Oliviero Bruni, Luigi Gallimberti Buona Notte: Il sonno tra fisiologia ... · Oliviero Bruni, Luigi...
50
Oliviero Bruni, Luigi Gallimberti Buona Notte: Il sonno tra fisiologia e disturbo Conduttore: Mattia Doria
Transcript of Oliviero Bruni, Luigi Gallimberti Buona Notte: Il sonno tra fisiologia ... · Oliviero Bruni, Luigi...

Oliviero Bruni, Luigi Gallimberti Buona Notte: Il sonno tra fisiologia e disturbo
Conduttore: Mattia Doria
Grazie per l’attenzione!
The Harvard sleep researcher Robert Stickgold has recalled his former
collaborator J. Allan Hobson joking that the only known function of sleep was
to cure sleepiness
ALLAN RECHTSCHAFFEN
“if sleep doesn’t serve an absolutely vital function, it is the
biggest mistake evolution ever made.”
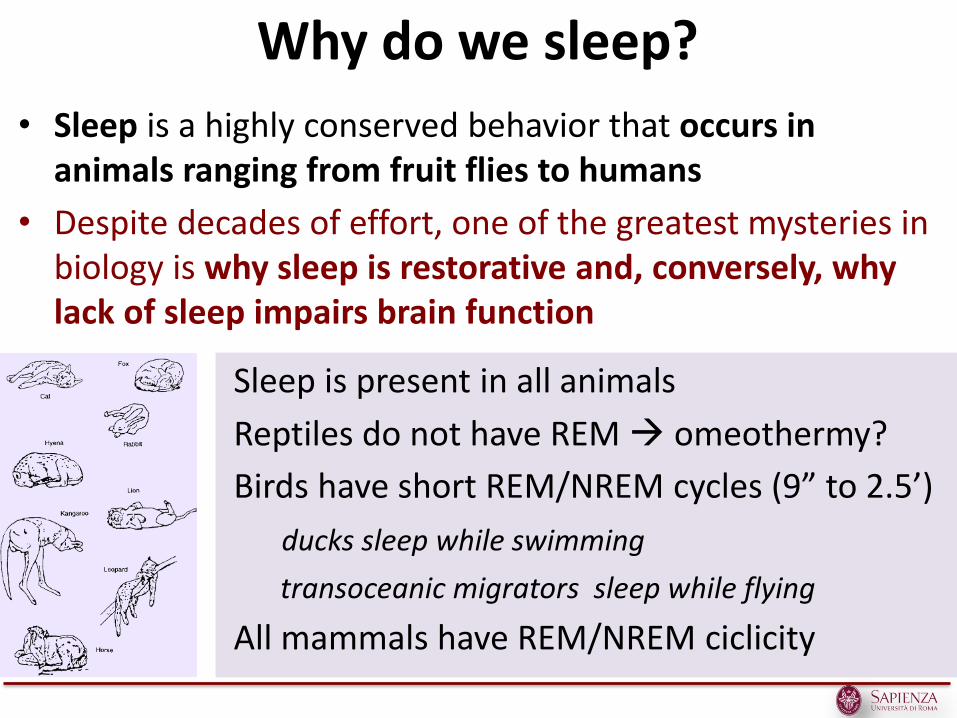
Sleep is present in all animals
Reptiles do not have REM omeothermy?
Birds have short REM/NREM cycles (9” to 2.5’)
ducks sleep while swimming
transoceanic migrators sleep while flying
All mammals have REM/NREM ciclicity
Why do we sleep?
• Sleep is a highly conserved behavior that occurs in animals ranging from fruit flies to humans
• Despite decades of effort, one of the greatest mysteries in biology is why sleep is restorative and, conversely, why lack of sleep impairs brain function
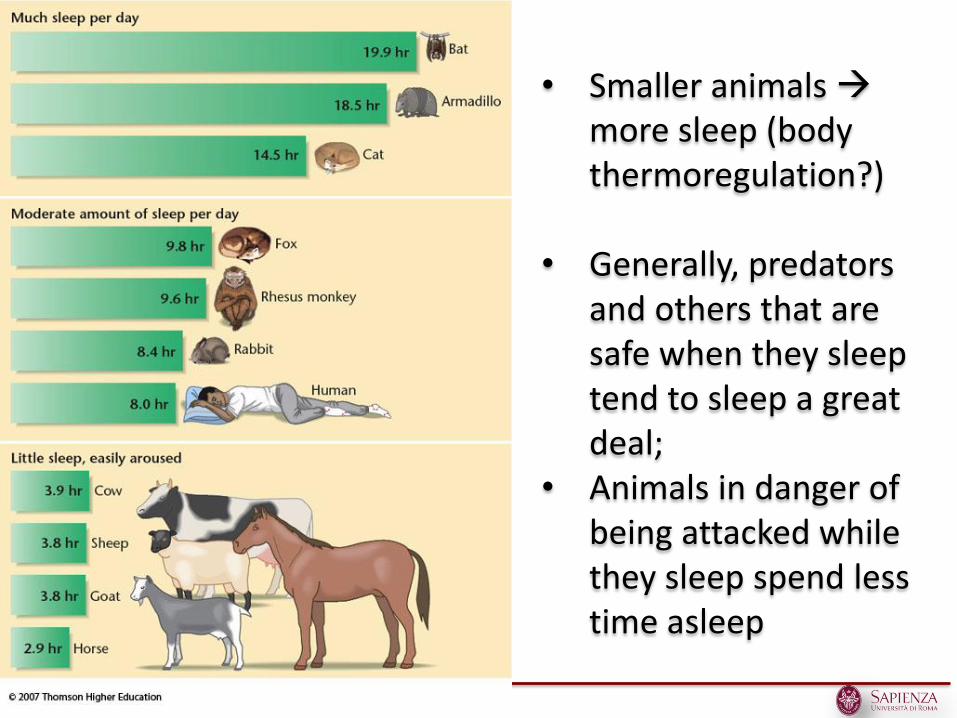
• Smaller animals more sleep (body thermoregulation?)
• Generally, predators and others that are safe when they sleep tend to sleep a great deal;
• Animals in danger of being attacked while they sleep spend less time asleep
Sleep is necessary for survival
• Whatever the reasons for sleeping, in mammals sleep is evidently necessary for survival. For instance, rats completely deprived of sleep die in a few weeks
• In humans, lack of sleep leads to impaired memory and reduced cognitive abilities, and, if the deprivation persists, mood swings and even hallucinations.
• The longest documented period of voluntary sleeplessness is 264 hours (approximately 11 days), a record achieved without any pharmacological stimulation.
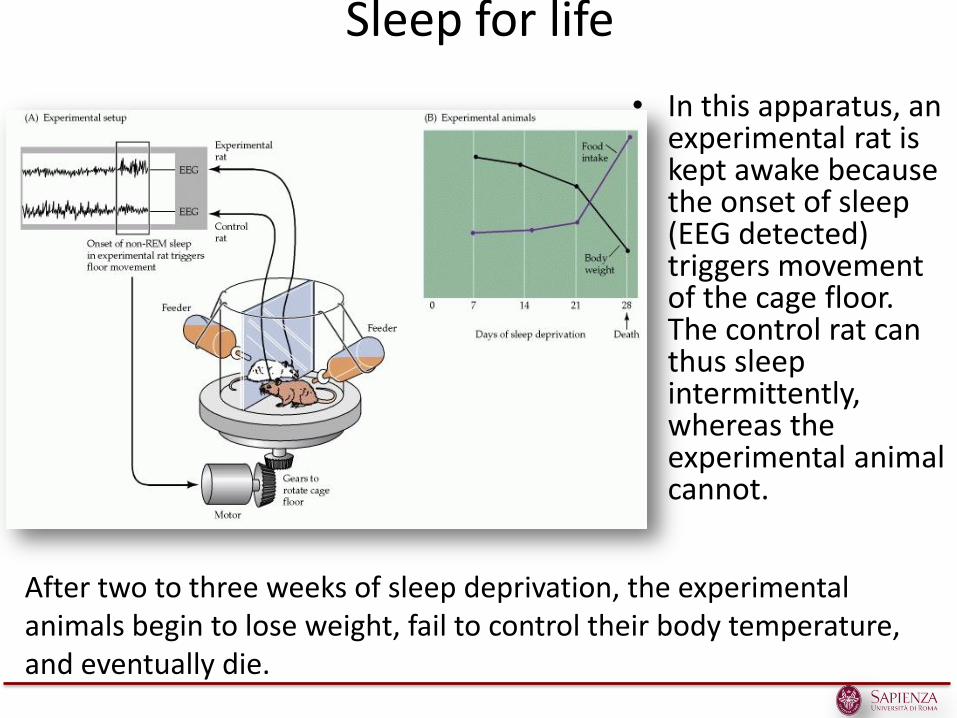
Sleep for life
• In this apparatus, an experimental rat is kept awake because the onset of sleep (EEG detected) triggers movement of the cage floor. The control rat can thus sleep intermittently, whereas the experimental animal cannot.
After two to three weeks of sleep deprivation, the experimental animals begin to lose weight, fail to control their body temperature, and eventually die.
What’s strange in this picture?
Birds at extreme sides have one eye opened
Does Unihemispheric Sleep Aid in Predator Detection? Unihemispheric SWS increase as predation risk increases
Sleep–wake patterns in nonhuman and human primates
• Sleep–wake patterns in nonhuman primates consist mainly of polyphasic episodes of rest and activity with frequent (up to 12) cycles of wakeful activity through- out the 24-hour day.
• The biphasic sleep–wake pattern probably began in human primates in the latter part of the Neolithic period (since 10.000 BC).
• The monophasic sleep–wake pattern began with the advent of electric light and of the 24-hr society
Theogony, Hesiod
Notte generò Destino (Moros), Vendetta (Kere) e Morte, il Sonno e la specie dei Sogni
• Nyx (Notte) era la personificazione della notte terrestre, e suo fratello Erebo (Buio) era la notte del mondo infernale
• Da Nix nacquero: • Etere (luce) and Emera (giorno) • Eris (discordia), Kere o Nemesis (vendetta), Moros (destino o
fato) • Hypnos (sonno) e il gemello Thanatos (morte)
• Figlio delle Tenebre e della Notte, fratello della Morte (Thanatos) e del Destino (Moros) e padre dei Sogni
Hypnos - Sonno
Hypnos dormiva in una caverna in cui scorreva il Lete, fiume dell'oblio (Stazio, Tebaide, X, 84-90), e davanti alla quale crescevano piante di papavero (Ovidio, Metamorfosi, XI, 604-607). Hypnos aveva 3 figli :
• Morfeo • Phantasos • Phobetor
Thermoregulation (McGinty and Szymusiak, 1990) Adaptation to an ecological niche (Webb, 1974) “Instinctual behavior” (Meddis, 1977) Neuronal plasticity (Krueger et al., 1995) Processing of memory traces (Tononi, 2006)
THEORIES EXPLAINING THE FUNCTIONS OF SLEEP
1. Inactivity
2. Energy conservation
3. Restorative
4. Tissue repair
5. Brain plasticity
6. Cognition
Theories of Why We Sleep 1- Inactivity Theory
• This theory, sometimes called adaptive or evolutionary, suggests that inactivity at night is an adaptation that served a survival function by keeping organisms out of harm’s way at times when they would be particularly vulnerable.
• Sleep is analogous to the hibernation of animals
• The theory suggests that animals that were able to stay still and quiet during these periods of vulnerability had an advantage over other animals that remained active.
Frank MG. 2006. The mystery of sleep function: current perspectives and future directions. Reviews in the Neurosciences. 17:375-392.
Theories of Why We Sleep 2 - Energy Conservation Theory
• The energy conservation theory suggests that the primary function of sleep is to reduce an individual’s energy demand and expenditure during part of the day or night, especially at times when it is least efficient to search for food.
• The function of sleep is to conserve energy by: – decreasing body temperature 1-2 Celsius degrees in mammals – decreasing muscle activity
• Research has shown that energy metabolism is reduced during sleep (by 10% in humans and more in other species)
• NREM sleep uses much less energy than wakefulness and may provide time to restore our brains glycogen stores, which are depleted by the demands of wakefulness
• Recent studies suggest that sleep may strengthen our immune defenses and insufficient sleep impair them.
Frank MG. 2006. The mystery of sleep function: current perspectives and future directions. Reviews in the Neurosciences. 17:375-392.
Theories of Why We Sleep 3 - Restorative Theories
• Sleep in some way serves to "restore" what is lost in the body while we are awake and provides an opportunity for the body to repair and rejuvenate itself.
• Many of the major restorative functions in the body like muscle growth, tissue repair, protein synthesis, and growth hormone release, immune functions occur mostly, or only, during sleep.
• While we are awake, neurons in the brain produce adenosine, a by-product of the cells' activities. The build-up of adenosine in the brain leads to our perception of being tired (is counteracted by caffeine, which blocks the actions of adenosine and keeps us alert)
• During sleep, the body has a chance to clear adenosine from the system.
Frank MG. 2006. The mystery of sleep function: current perspectives and future directions. Reviews in the Neurosciences. 17:375-392.
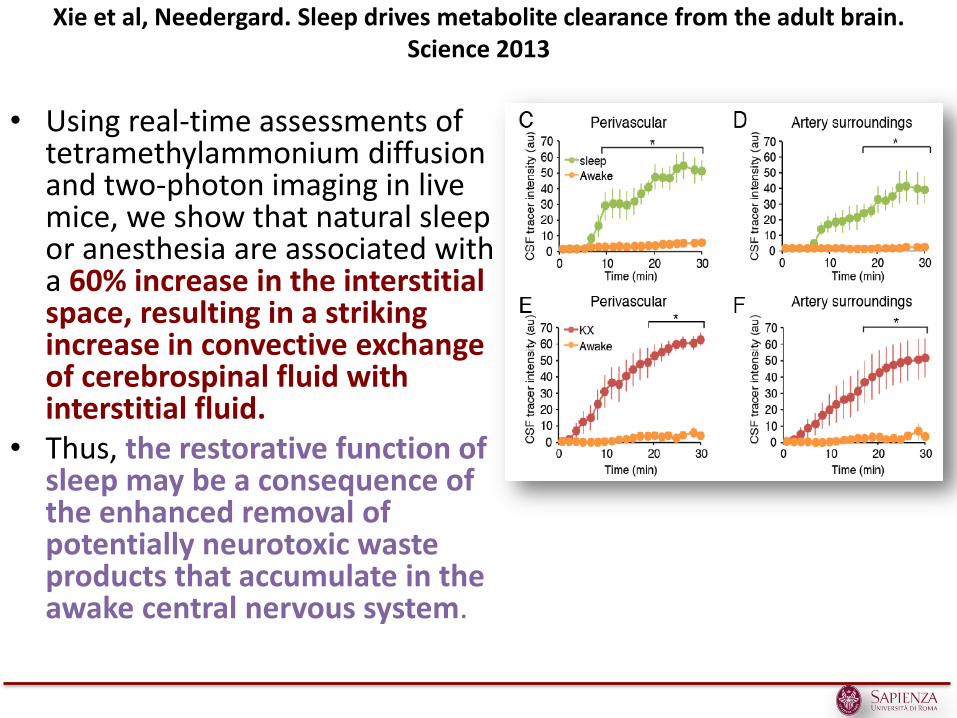
Xie et al, Needergard. Sleep drives metabolite clearance from the adult brain. Science 2013
• Using real-time assessments of tetramethylammonium diffusion and two-photon imaging in live mice, we show that natural sleep or anesthesia are associated with a 60% increase in the interstitial space, resulting in a striking increase in convective exchange of cerebrospinal fluid with interstitial fluid.
• Thus, the restorative function of sleep may be a consequence of the enhanced removal of potentially neurotoxic waste products that accumulate in the awake central nervous system.
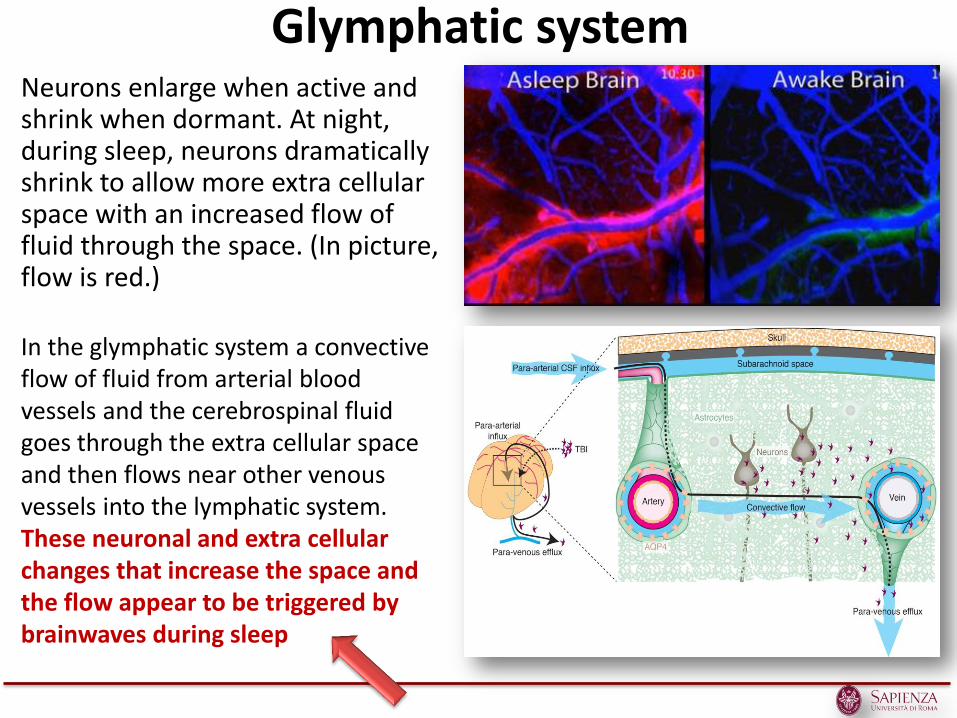
Glymphatic system Neurons enlarge when active and shrink when dormant. At night, during sleep, neurons dramatically shrink to allow more extra cellular space with an increased flow of fluid through the space. (In picture, flow is red.)
In the glymphatic system a convective flow of fluid from arterial blood vessels and the cerebrospinal fluid goes through the extra cellular space and then flows near other venous vessels into the lymphatic system. These neuronal and extra cellular changes that increase the space and the flow appear to be triggered by brainwaves during sleep
Theory Why we sleep 4 – Restoration somatic tissue repair (NREM)
1. Slow-wave sleep (SWS) increases following sleep deprivation
2. SWS percentage of is increased during development
3. Release of growth hormone occurs at sleep onset and peak during SWS in prepubertal children. The release of many endogenous anabolic steroids occurs in relation to a sleep cycle (prolactin, testosterone, and LH).
4. The nadir of catabolic steroid release, occurs during the first hours of sleep, coincident with the largest percentage of SWS. Increased mitosis of lymphocytes and increased rate of bone growth occur during sleep.
Theories of Why We Sleep 5 - Brain Plasticity Theory
• Sleep is correlated to changes in the structure and organization of the brain brain plasticity,
• REM sleep may have evolved in order to ‘reprogram’ innate behaviors and to incorporate learned behaviors and knowledge acquired during wakefulness
• Synaptic efficiency and efficacy of the brain depends on keeping the synaptic connections refined integrating new neuronal firing patterns. Sleep periodically occurs to allow the brain to do this, thus maintaining brain plasticity. This synaptic reorganization occurs during NREM sleep
Frank MG. 2006. The mystery of sleep function: current perspectives and future directions. Reviews in the Neurosciences. 17:375-392.
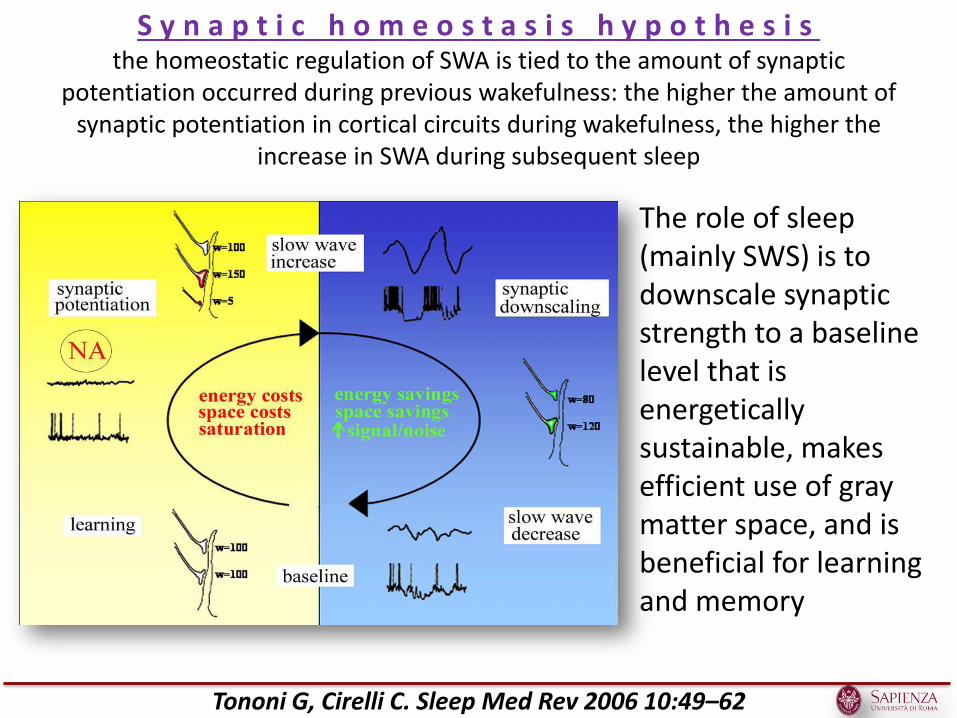
S y n a p t i c h o m e o s t a s i s h y p o t h e s i s the homeostatic regulation of SWA is tied to the amount of synaptic
potentiation occurred during previous wakefulness: the higher the amount of synaptic potentiation in cortical circuits during wakefulness, the higher the
increase in SWA during subsequent sleep
Tononi G, Cirelli C. Sleep Med Rev 2006 10:49–62
The role of sleep (mainly SWS) is to downscale synaptic strength to a baseline level that is energetically sustainable, makes efficient use of gray matter space, and is beneficial for learning and memory
Per capire a cosa seve il sonno basta vedere cosa succede quando il sonno è disturbato /alterato
• Sleep apnea has been associated with diabetes and cardiovascular disease and lead to cognitive impairment.
• Chronic insomnia has been linked to low quality of life, depression, increases in cardiovascular disease and hypertension, cognitive and motor impairment
• REM-sleep behavior disorder is a reliable predictor of neurodegenerative disease like Parkinson’s or Alzheimer’s.
Il sonno tra fisiologia e disturbo
• Quale è la prevalenza dei disturbi del sonno nell’infanzia e nell’adolescenza?
• Quanto devono dormire i bambini e gli adolescenti?
• Quali sono le conseguenze di un sonno insufficiente o disturbato nel bambino?
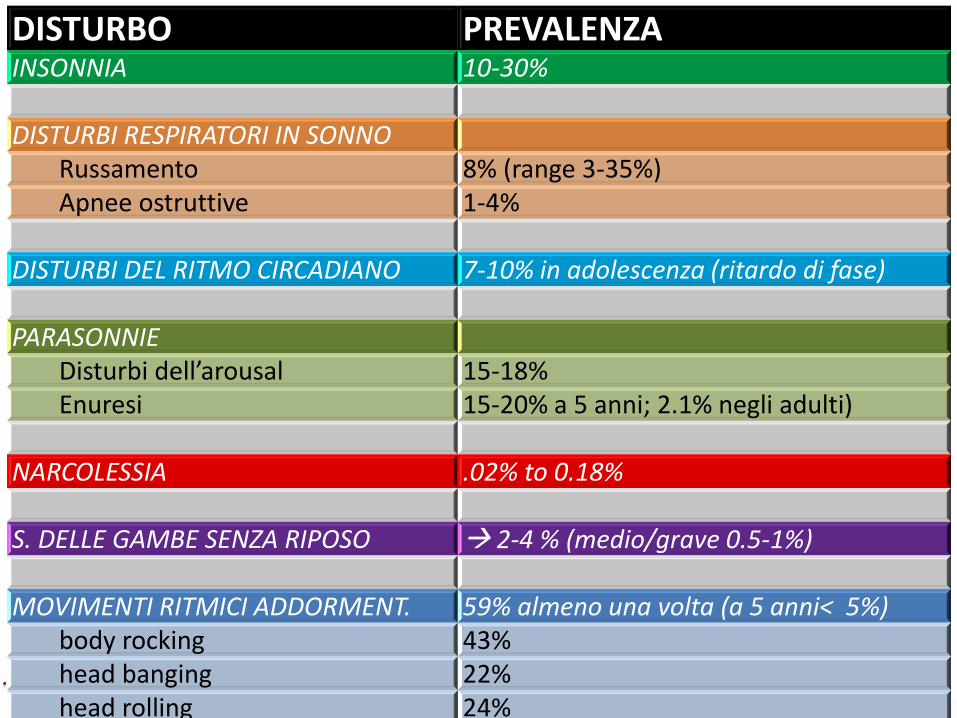
DISTURBO PREVALENZA INSONNIA 10-30%
DISTURBI RESPIRATORI IN SONNO Russamento 8% (range 3-35%) Apnee ostruttive 1-4%
DISTURBI DEL RITMO CIRCADIANO 7-10% in adolescenza (ritardo di fase)
PARASONNIE Disturbi dell’arousal 15-18% Enuresi 15-20% a 5 anni; 2.1% negli adulti)
NARCOLESSIA .02% to 0.18%
S. DELLE GAMBE SENZA RIPOSO 2-4 % (medio/grave 0.5-1%)
MOVIMENTI RITMICI ADDORMENT. 59% almeno una volta (a 5 anni< 5%) body rocking 43% head banging 22% head rolling 24%
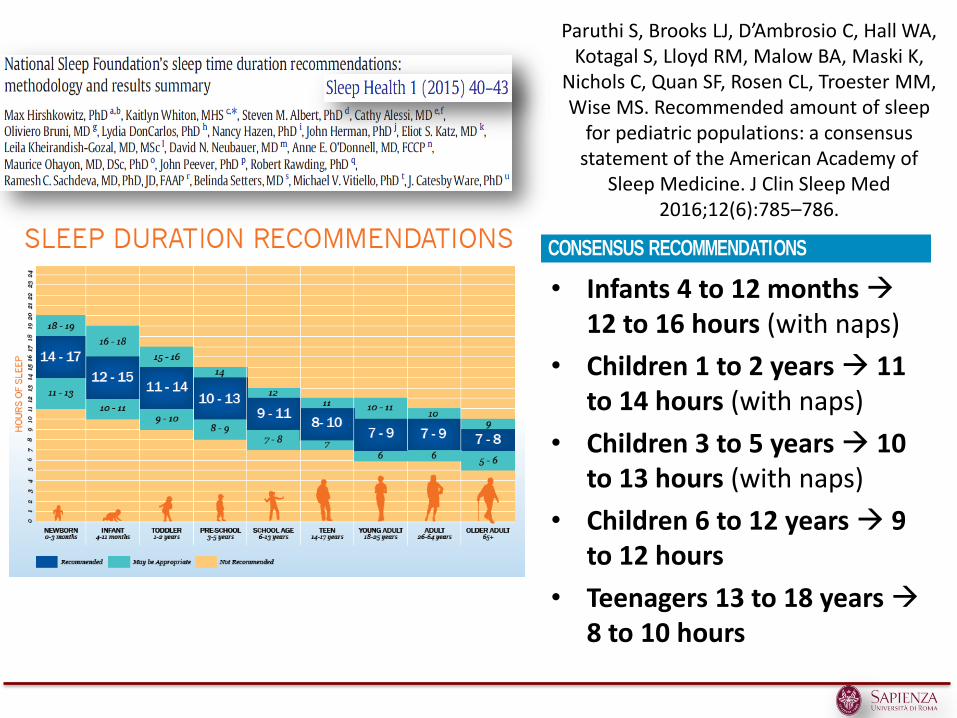
Paruthi S, Brooks LJ, D’Ambrosio C, Hall WA, Kotagal S, Lloyd RM, Malow BA, Maski K,
Nichols C, Quan SF, Rosen CL, Troester MM, Wise MS. Recommended amount of sleep
for pediatric populations: a consensus statement of the American Academy of
Sleep Medicine. J Clin Sleep Med 2016;12(6):785–786.
• Infants 4 to 12 months 12 to 16 hours (with naps)
• Children 1 to 2 years 11 to 14 hours (with naps)
• Children 3 to 5 years 10 to 13 hours (with naps)
• Children 6 to 12 years 9 to 12 hours
• Teenagers 13 to 18 years 8 to 10 hours
785 Journal of Clinical Sleep Medicine, Vol. 12, No. 6, 2016
Sleep is essential for optimal health in children and adolescents. Members of the American Academy of Sleep Medicine developed consensus
recommendations for the amount of sleep needed to promote optimal health in children and adolescents using a modified RAND Appropriateness Method.
The recommendations are summarized here. A manuscript detailing the conference proceedings and the evidence supporting these recommendations will be
published in the Journal of Clinical Sleep Medicine.
Keywords: pediatric, sleep duration, consensus
Citation: Paruthi S, Brooks LJ, D’Ambrosio C, Hall WA, Kotagal S, Lloyd RM, Malow BA, Maski K, Nichols C, Quan SF, Rosen CL, Troester MM, Wise
MS. Recommended amount of sleep for pediatric populations: a consensus statement of the American Academy of Sleep Medicine. J Clin Sleep Med
2016;12(6):785–786.
CONSENSUS RECOMMENDATIONS
• Infants* 4 months to 12 months should sleep 12 to 16
hours per 24 hours (including naps) on a regular basis
to promote optimal health.
• Children 1 to 2 years of age should sleep 11 to 14 hours
per 24 hours (including naps) on a regular basis to
promote optimal health.
• Children 3 to 5 years of age should sleep 10 to 13 hours
per 24 hours (including naps) on a regular basis to
promote optimal health.
• Children 6 to 12 years of age should sleep 9 to 12 hours
per 24 hours on a regular basis to promote optimal
health.
• Teenagers 13 to 18 years of age should sleep 8 to 10
hours per 24 hours on a regular basis to promote
optimal health.
◦ Sleeping the number of recommended hours on a
regular basis is associated with better health outcomes
including: improved attention, behavior, learning,
memory, emotional regulation, quality of life, and
mental and physical health.
◦ Regularly sleeping fewer than the number of
recommended hours is associated with attention,
behavior, and learning problem s. Insufficient sleep also
increases the risk of accidents, injuries, hypertension,
obesity, diabetes, and depression. Insufficient sleep in
CONSENSUS STATEMENT
Recommended Amount of Sleep for Pediatric Populations:
A Consensus Statement of the American Academy of Sleep MedicineShalini Paruthi, MD1,*; Lee J. Brooks, MD2,3; Carolyn D’Ambrosio, MD4; Wendy A. Hall, PhD, RN5; Suresh Kotagal, MD6; Robin M. Lloyd, MD6;
Beth A. Malow, MD, MS7; Kiran Maski, MD8; Cynthia Nichols, PhD9; Stuart F. Quan, MD10; Carol L. Rosen, MD11; Matthew M. Troester, DO12;
Merrill S. Wise, MD13
1Saint Louis University, St. Louis, MO; 2Children’s Hospital of Philadelphia, Philadelphia, PA; 3Liaison for the American Academy of Pediatrics, Elk Grove Village, IL; 4Brigham and
Women’s Hospital, Boston, MA; 5University of British Columbia School of Nursing, Vancouver, BC; 6Mayo Clinic, Rochester, MN; 7Vanderbilt University Medical Center, Nashville,
TN; 8Boston Children’s Hospital, Boston, MA; 9Munson Sleep Disorders Center, Traverse City, MI; 10Harvard Medical School, Boston, MA; 11Rainbow Babies and Children’s Hospital,
Cleveland, OH; 12Barrow Neurological Institute at Phoenix Children’s Hospital, Phoenix, AZ; 13Methodist Healthcare Sleep Disorders Center, Memphis, TN; *moderator of the
Consensus Conference Panel
pii: jc-00158-16 http://dx.doi.org/10.5664/jcsm.5866
teenagers is associated with increased risk of self-harm,
suicidal thoughts, and suicide attempts.
◦ Regularly sleeping more than the recommended hours
may be associated with adverse health outcomes such
as hypertension, diabetes, obesity, and mental health
problems.
◦ Parents who are concerned that their child is sleeping
too little or too much should consult their healthcare
provider for evaluation of a possible sleep disorder.
* Recommendations for infants younger than 4 months are not
included due to the wide range of normal variation in duration
and patterns of sleep, and insufficient evidence for associa-
tions with health outcomes.
BACKGROUND AND METHODOLOGY
Healthy sleep requires adequate duration, appropriate timing,
good quality, regularity, and the absence of sleep disturbances
or disorders. Sleep duration is a frequently investigated sleep
measure in relation to health. A panel of 13 experts in sleep
m edicine and research used a m odified R AND Appropriate-
ness Method1 to develop recommendations regarding the sleep
duration range that promotes optimal health in children aged
0◦18 years. The expert panel reviewed published scientific evi-
dence addressing the relationship between sleep duration and
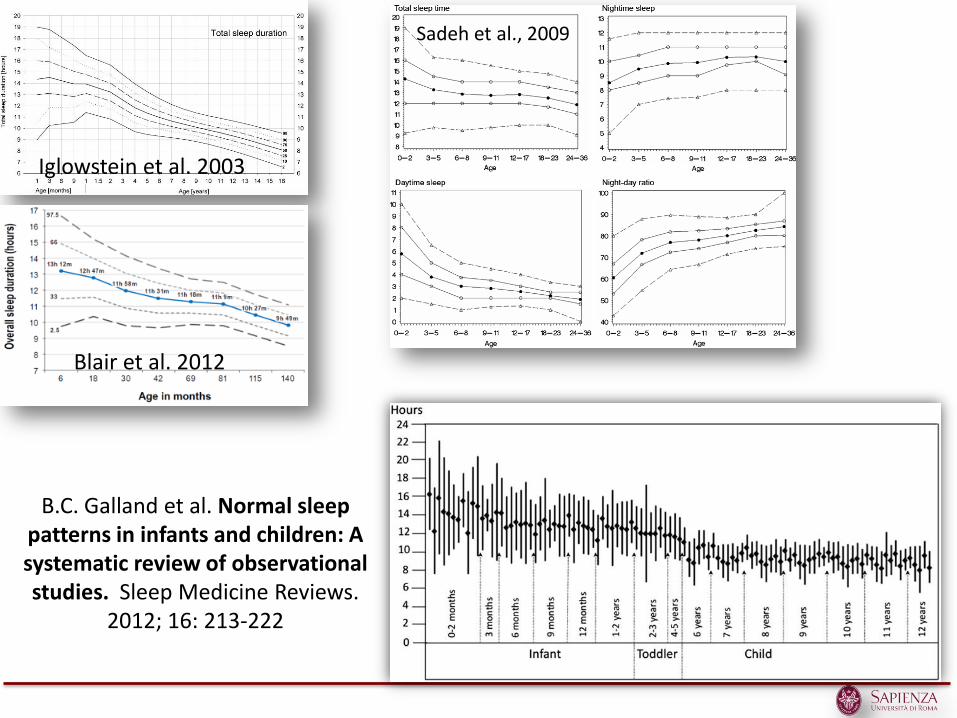
Iglowstein et al. 2003
Sadeh et al., 2009
Blair et al. 2012
B.C. Galland et al. Normal sleep patterns in infants and children: A systematic review of observational studies. Sleep Medicine Reviews.
2012; 16: 213-222
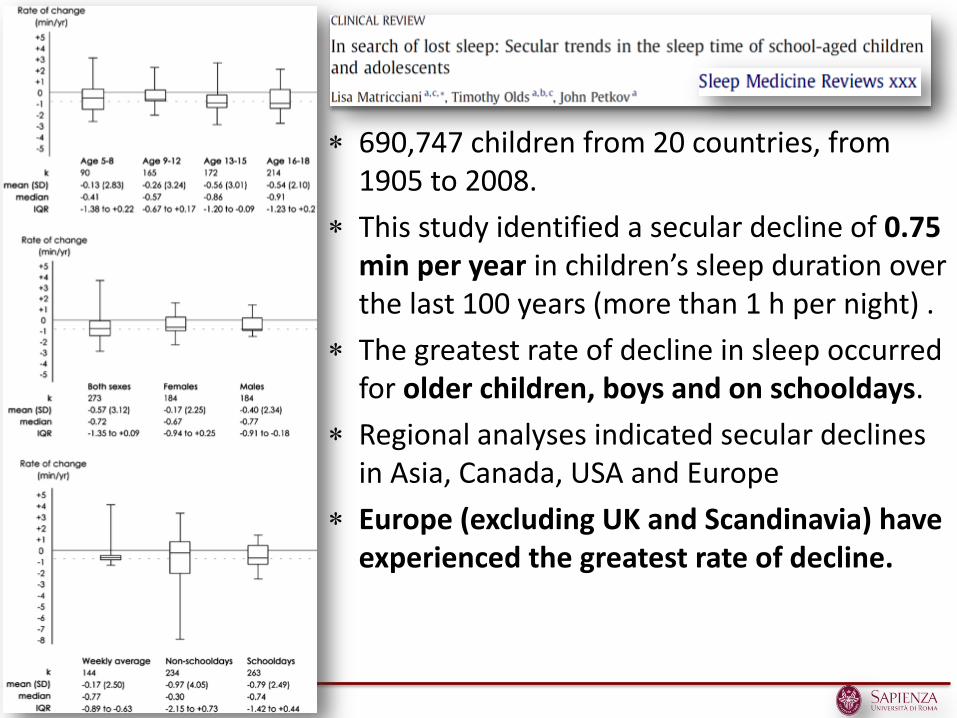
690,747 children from 20 countries, from 1905 to 2008.
This study identified a secular decline of 0.75 min per year in children’s sleep duration over the last 100 years (more than 1 h per night) .
The greatest rate of decline in sleep occurred for older children, boys and on schooldays.
Regional analyses indicated secular declines in Asia, Canada, USA and Europe
Europe (excluding UK and Scandinavia) have experienced the greatest rate of decline.
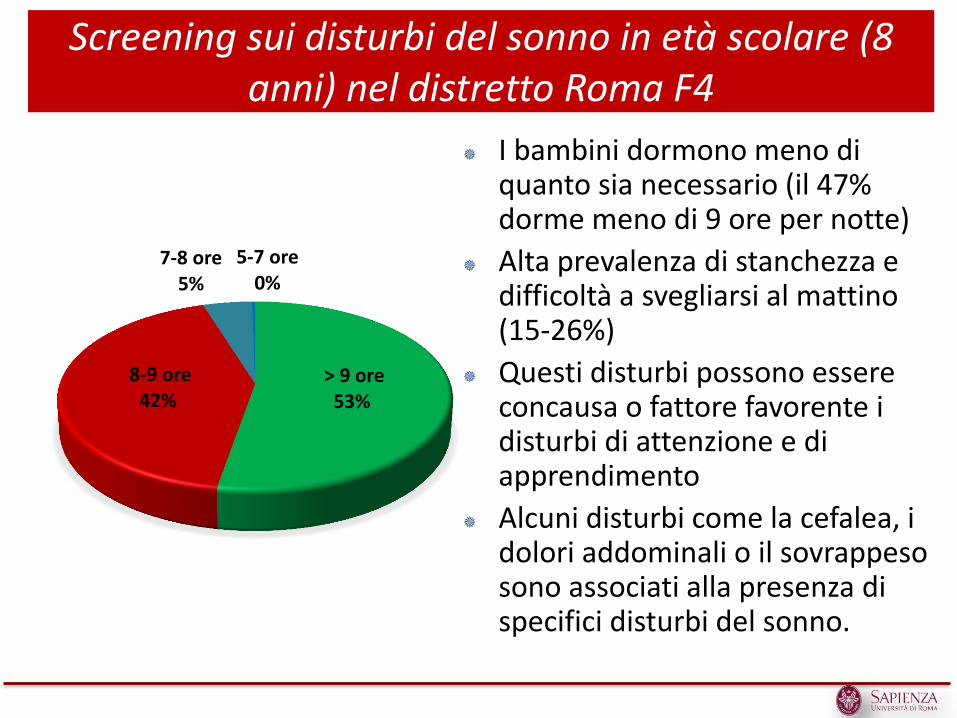
> 9 ore 53%
8-9 ore 42%
7-8 ore 5%
5-7 ore 0%
I bambini dormono meno di quanto sia necessario (il 47% dorme meno di 9 ore per notte)
Alta prevalenza di stanchezza e difficoltà a svegliarsi al mattino (15-26%)
Questi disturbi possono essere concausa o fattore favorente i disturbi di attenzione e di apprendimento
Alcuni disturbi come la cefalea, i dolori addominali o il sovrappeso sono associati alla presenza di specifici disturbi del sonno.
Screening sui disturbi del sonno in età scolare (8 anni) nel distretto Roma F4
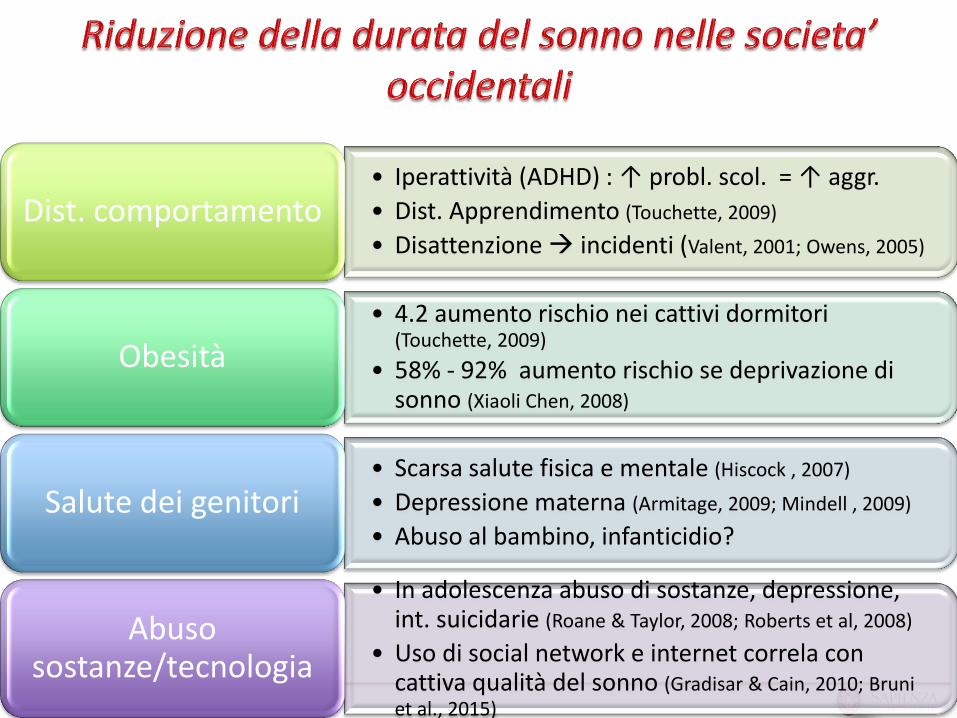
• Iperattività (ADHD) : ↑ probl. scol. = ↑ aggr.
• Dist. Apprendimento (Touchette, 2009)
• Disattenzione incidenti (Valent, 2001; Owens, 2005)
Dist. comportamento
• 4.2 aumento rischio nei cattivi dormitori (Touchette, 2009)
• 58% - 92% aumento rischio se deprivazione di sonno (Xiaoli Chen, 2008)
Obesità
• Scarsa salute fisica e mentale (Hiscock , 2007)
• Depressione materna (Armitage, 2009; Mindell , 2009)
• Abuso al bambino, infanticidio? Salute dei genitori
• In adolescenza abuso di sostanze, depressione, int. suicidarie (Roane & Taylor, 2008; Roberts et al, 2008)
• Uso di social network e internet correla con cattiva qualità del sonno (Gradisar & Cain, 2010; Bruni et al., 2015)
Abuso sostanze/tecnologia
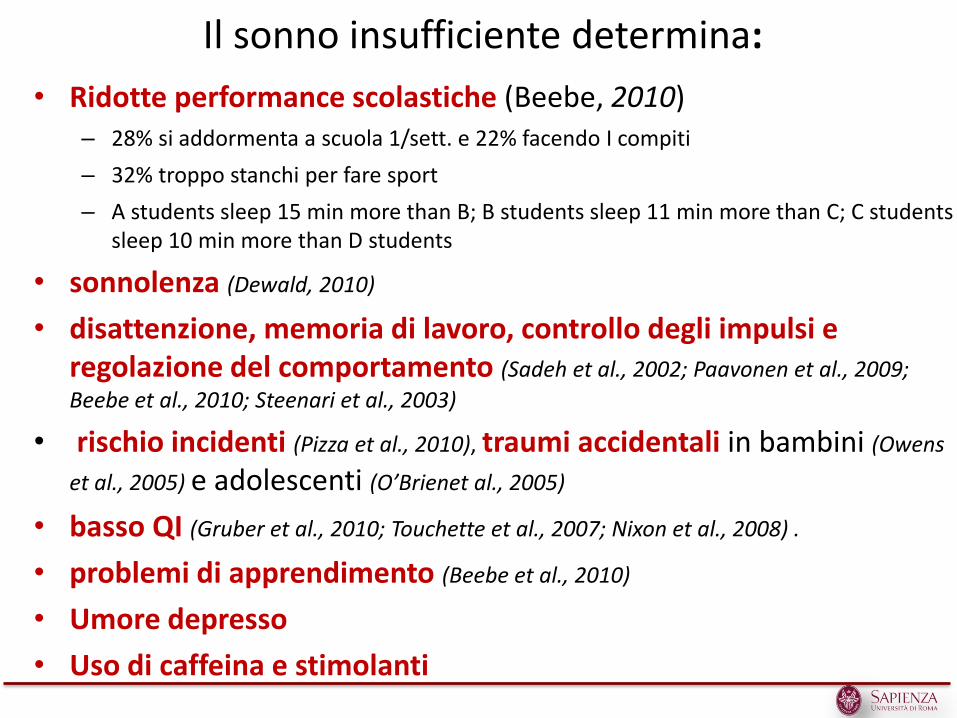
Il sonno insufficiente determina:
• Ridotte performance scolastiche (Beebe, 2010) – 28% si addormenta a scuola 1/sett. e 22% facendo I compiti
– 32% troppo stanchi per fare sport
– A students sleep 15 min more than B; B students sleep 11 min more than C; C students sleep 10 min more than D students
• sonnolenza (Dewald, 2010)
• disattenzione, memoria di lavoro, controllo degli impulsi e regolazione del comportamento (Sadeh et al., 2002; Paavonen et al., 2009;
Beebe et al., 2010; Steenari et al., 2003)
• rischio incidenti (Pizza et al., 2010), traumi accidentali in bambini (Owens
et al., 2005) e adolescenti (O’Brienet al., 2005)
• basso QI (Gruber et al., 2010; Touchette et al., 2007; Nixon et al., 2008) .
• problemi di apprendimento (Beebe et al., 2010)
• Umore depresso
• Uso di caffeina e stimolanti
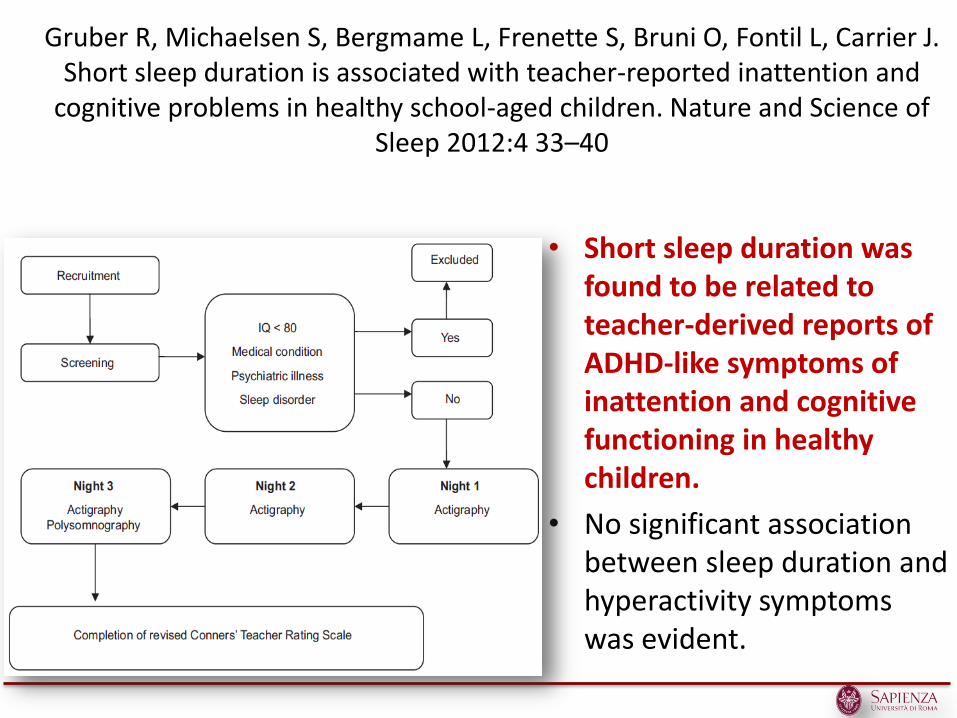
Gruber R, Michaelsen S, Bergmame L, Frenette S, Bruni O, Fontil L, Carrier J. Short sleep duration is associated with teacher-reported inattention and
cognitive problems in healthy school-aged children. Nature and Science of Sleep 2012:4 33–40
• Short sleep duration was found to be related to teacher-derived reports of ADHD-like symptoms of inattention and cognitive functioning in healthy children.
• No significant association between sleep duration and hyperactivity symptoms was evident.
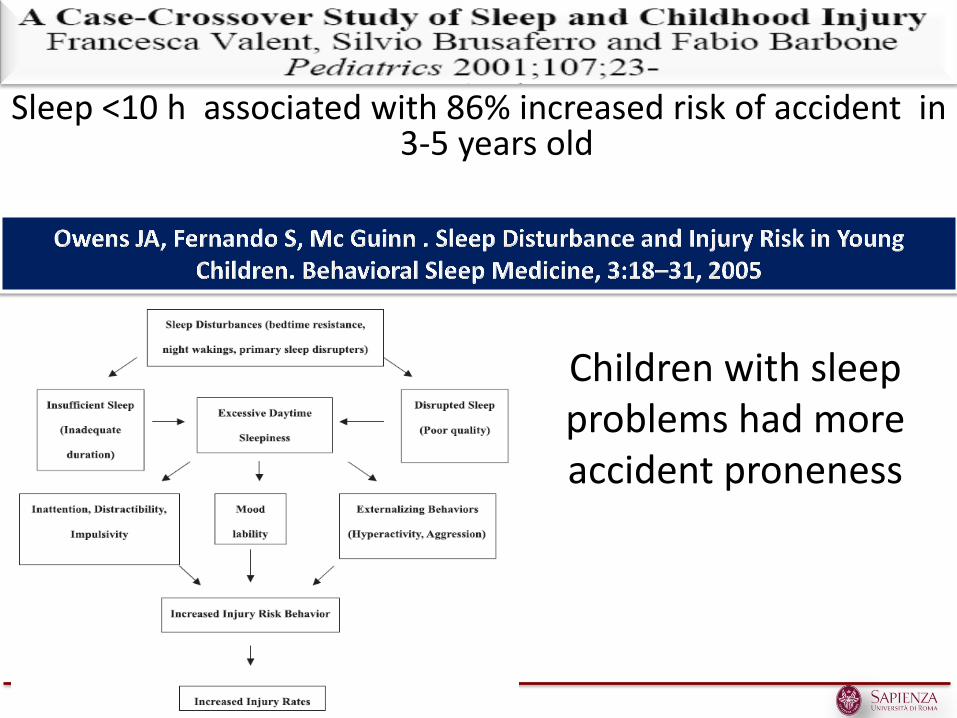
Sleep <10 h associated with 86% increased risk of accident in 3-5 years old
Children with sleep problems had more accident proneness
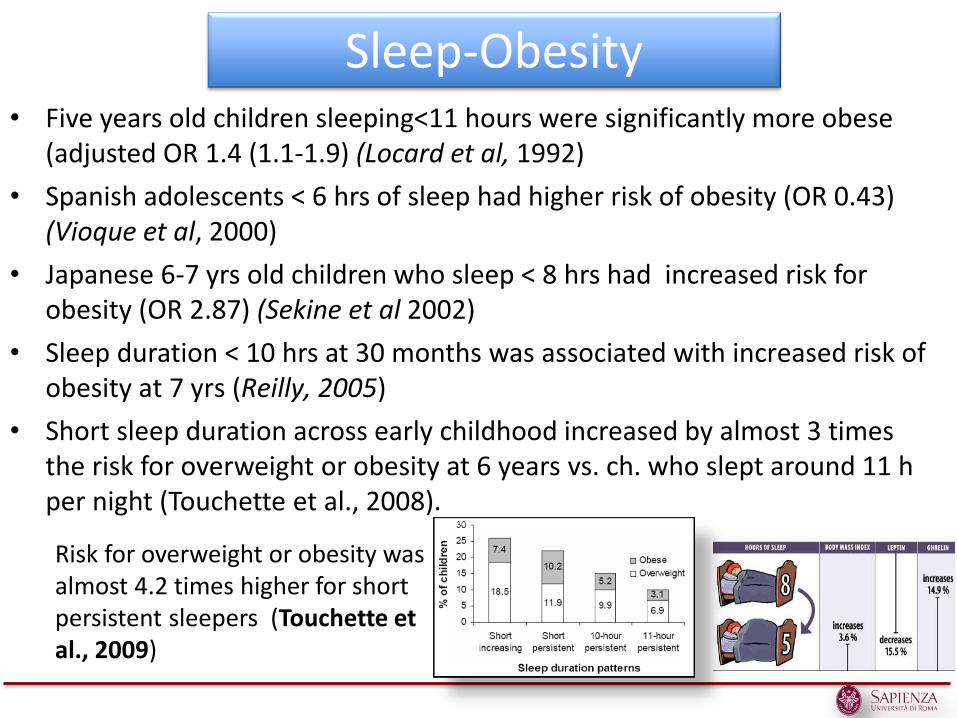
• Five years old children sleeping<11 hours were significantly more obese (adjusted OR 1.4 (1.1-1.9) (Locard et al, 1992)
• Spanish adolescents < 6 hrs of sleep had higher risk of obesity (OR 0.43) (Vioque et al, 2000)
• Japanese 6-7 yrs old children who sleep < 8 hrs had increased risk for obesity (OR 2.87) (Sekine et al 2002)
• Sleep duration < 10 hrs at 30 months was associated with increased risk of obesity at 7 yrs (Reilly, 2005)
• Short sleep duration across early childhood increased by almost 3 times the risk for overweight or obesity at 6 years vs. ch. who slept around 11 h per night (Touchette et al., 2008).
Sleep-Obesity
Risk for overweight or obesity was almost 4.2 times higher for short persistent sleepers (Touchette et al., 2009)
Parent’s health and infant’s sleep
• 70% of mothers with colicky infants have aggressive thoughts/fantasies towards their children
• 26% admit to toughts of infanticide during colic episodes (Levistsky et al., Clin Pediatr, 2000)
• Increased maternal depression and disorganized parent attachment (Stifter et al., Infancy, 2002; Armitage, 2009)
• Life stress and symptoms of depression and anxiety in the mothers were negatively related to preschool child's sleep duration (Caldwell Radekers, 2014)
• Infant sleep problems were associated with poor general health in mothers and in fathers and with severe psychological distress (Hiscock et al., 2007)
SLEEP and Maternal Depression Armitage R; Flynn H; Hoffmann R; Vazquez D;
Lopez J; Marcus S. Early developmental changes in sleep in infants: the impact of maternal
depression. SLEEP 2009;32(5):693-696.
• Maternal depression is associated with significant sleep disturbance in infancy at 2 weeks postpartum that continues through 24 weeks. It remains to be determined if sleep disturbance in infancy confers a greater risk of developing early-onset depression in childhood.
Mindell JA; Telofski LS; Wiegand B; Kurtz ES. A nightly bedtime routine: impact on sleep
in young children and maternal mood. SLEEP 2009;32(5):599-606
• These results suggest that instituting a consistent nightly bedtime routine, in and of itself, is beneficial in improving multiple aspects of infant and toddler sleep, especially wakefulness after sleep onset and sleep continuity, as well as maternal mood.
• 20/2/2007: Madre uccide figlio di un anno (ANSA) - VERONA, 20 FEB - Una donna ha ucciso il proprio figlio di un anno e ha poi tentato di suicidarsi.
• 2/12/2008: L’infanticidio di Catanzaro e depressione post partum – La morte della neonata di appena due settimane, sbattuta sul pavimento
dalla madre perché piangeva troppo, avvenuta a Catanzaro è l’ennesimo infanticidio commesso da una mamma.
• 20/7/2009: Madre uccide figlio di 4 anni (ANSA) MILANO, 20 LUG - E' stata arrestata la donna di 36 anni che nel pomeriggio ha ucciso il proprio bambino di 4 anni
• 26/8/2009 Genova, madre uccide figlio neonato poi si toglie la vita
• Early childhood sleep disturbance is more closely associated with anxiety, whereas adolescent sleep problems are closely linked to depression (Dahl, 1996; Alfano et al., 2009).
• Chronic poor sleep in adolescents was associated with depression (Roberts et al, 1995; 2001), with anxiety or depression (67%) (Manni et al, 1997; Morrison et al, 1992) and/or somatic concerns (Marks and Monroe, 1976) and lower self-esteem (Price et al, 1978; Kirmil-Gray, 1984)
• The magnitude of depressive symptoms in adolescents are related to the presence of sleep problems
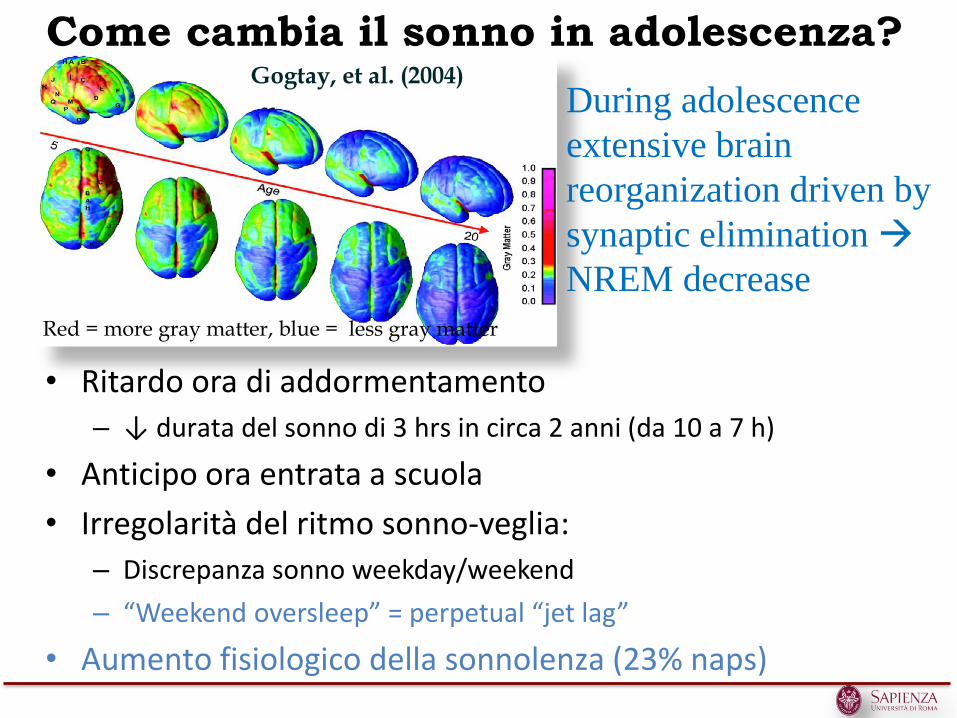
Come cambia il sonno in adolescenza?
• Ritardo ora di addormentamento
– ↓ durata del sonno di 3 hrs in circa 2 anni (da 10 a 7 h)
• Anticipo ora entrata a scuola
• Irregolarità del ritmo sonno-veglia:
– Discrepanza sonno weekday/weekend
– “Weekend oversleep” = perpetual “jet lag”
• Aumento fisiologico della sonnolenza (23% naps)
Gogtay, et al. (2004) During adolescence
extensive brain
reorganization driven by
synaptic elimination
NREM decrease
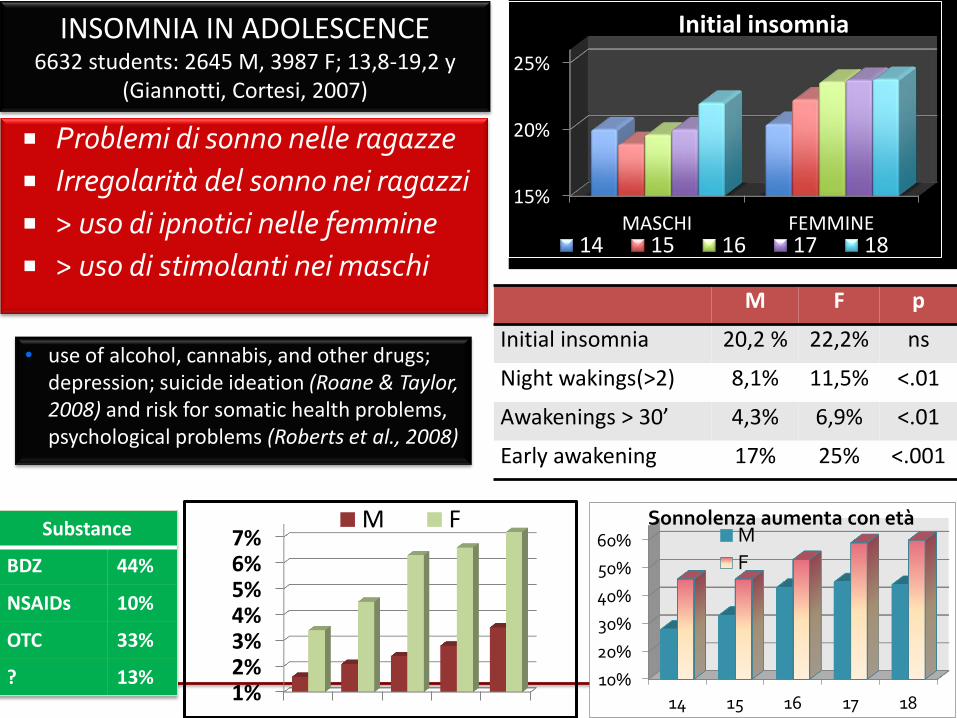
INSOMNIA IN ADOLESCENCE 6632 students: 2645 M, 3987 F; 13,8-19,2 y
(Giannotti, Cortesi, 2007)
15%
20%
25%
MASCHI FEMMINE
Initial insomnia
14 15 16 17 18
Problemi di sonno nelle ragazze
Irregolarità del sonno nei ragazzi
> uso di ipnotici nelle femmine
> uso di stimolanti nei maschi
10%
20%
30%
40%
50%
60%
14 15 16 17 18
Sonnolenza aumenta con età M
F
1%2%3%4%5%6%7%
14 15 16 17 18
M FSubstance
BDZ 44%
NSAIDs 10%
OTC 33%
? 13%
M F p
Initial insomnia 20,2 % 22,2% ns
Night wakings(>2) 8,1% 11,5% <.01
Awakenings > 30’ 4,3% 6,9% <.01
Early awakening 17% 25% <.001
• use of alcohol, cannabis, and other drugs; depression; suicide ideation (Roane & Taylor, 2008) and risk for somatic health problems, psychological problems (Roberts et al., 2008)
• 34% of US adolescents reported text messaging and 44% talking on the telephone after 9 pm (Calamaro et al., 2009)
• 30% woken up by text messages [Van den Bulck, 2003, 2007]
• Mobile phone use associated with shorter sleep duration, later wake-up times (Punamaki et al. 2007; Harada et al. 2002) and with school bullying in adolescents (Tochigi et al., 2012)
• 64% of children had one or more electronic devices in their bedroom shortened sleep duration, excess body weight, and lower physical activity (Chalal et al., 2012)
• Unlike passive technological devices (e.g., TV, mp3), the more interactive technological devices (i.e., computers, cell phones) before bed, the more likely difficulties falling asleep and unrefreshing sleep (Gradisar et al., 2013)
Mobile phones?
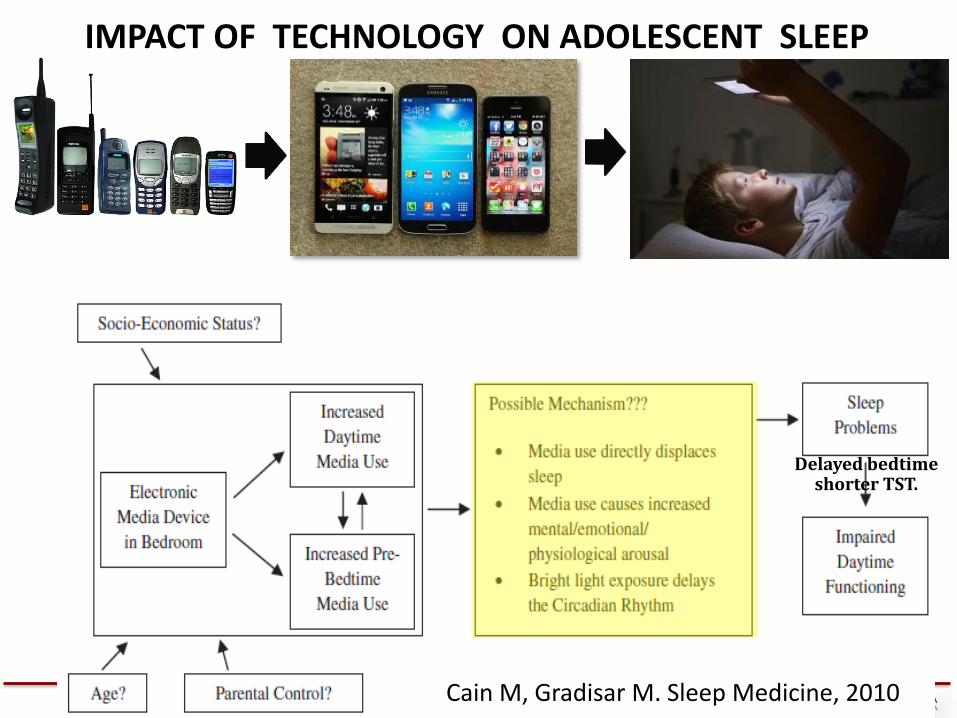
Cain M, Gradisar M. Sleep Medicine, 2010
Delayed bedtime shorter TST.
IMPACT OF TECHNOLOGY ON ADOLESCENT SLEEP
Mechanisms of technology affecting sleep 1. Reduce sleep length (Custers & Van den Bulck, 2012), increase sleep
latency (Higuchi et al., 2005) delay bedtimes (Van den Bulck, 2004).
2. Directly displace sleep, and replace activities that promote good sleep (< physical activity obesity) (Stepanski & Wyatt, 2003).
3. Cause physical discomfort, such as muscular pain and headache, which can negatively affect sleep (Thomée et al., 2010).
4. The bedroom is not sleep-inducing stimuli (Hauri & Fisher, 1986).
5. Induce cognitive and emotional arousal and impair sleep (Cain &
Gradisar, 2010; Gellis & Lichstein, 2009; Higuchi, 2005)
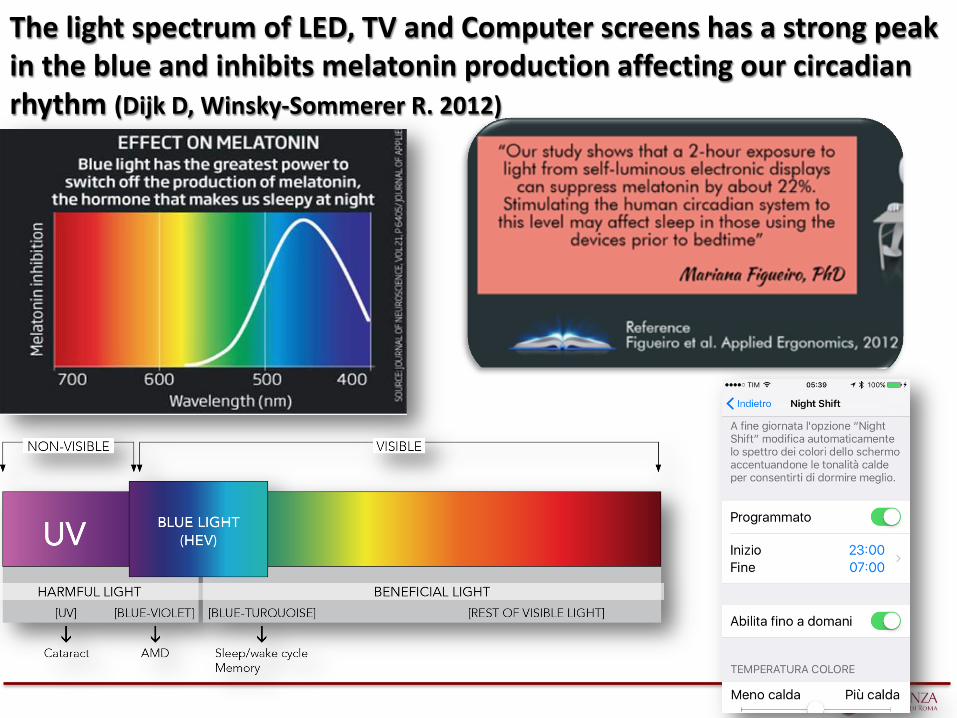
6. Bright light emitted by many electronic devices, especially with short wavelengths, can cause phase delays, (Cain & Gradisar, 2010;
Bjorvatn & Pallesen, 2009; Khalsa, et al., 2003; Zeitzer, et al. 2000).
Fossum, et al. The Association Between Use of Electronic Media in Bed Before Going to Sleep and Insomnia Symptoms, Daytime Sleepiness, Morningness, and Chronotype. Behav Sleep Med, 2014; 12:343-357
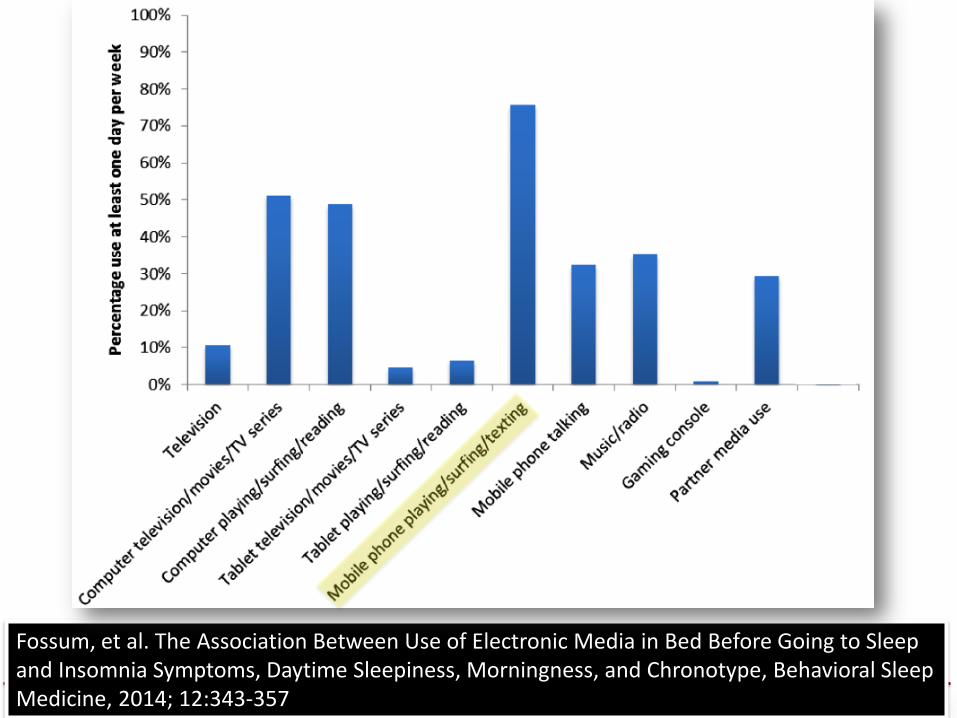
Fossum, et al. The Association Between Use of Electronic Media in Bed Before Going to Sleep and Insomnia Symptoms, Daytime Sleepiness, Morningness, and Chronotype, Behavioral Sleep Medicine, 2014; 12:343-357
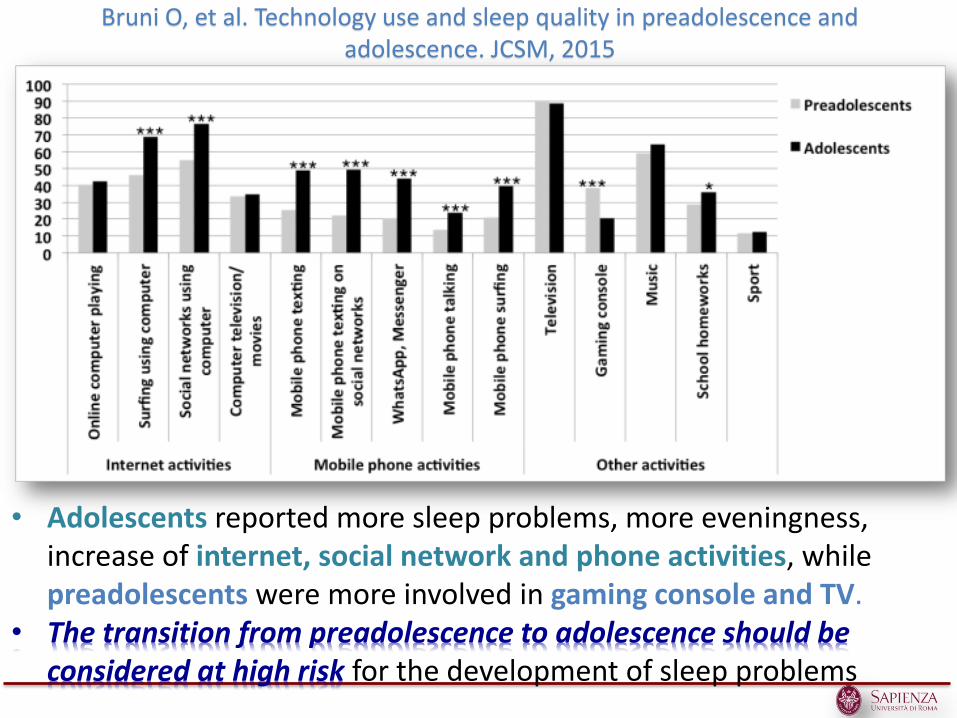
Bruni O, et al. Technology use and sleep quality in preadolescence and adolescence. JCSM, 2015
• Adolescents reported more sleep problems, more eveningness, increase of internet, social network and phone activities, while preadolescents were more involved in gaming console and TV.
• The transition from preadolescence to adolescence should be considered at high risk for the development of sleep problems
Hysing et al. Sleep patterns and insomnia among adolescents: a population-based study. J Sleep Res. (2013)
• To obtain the recommended sleep duration of 8–9 h, which was also in accordance with their self-perceived sleep need, they should have gone to bed at around 22:00 hours.
• At weekends, their sleep duration was in accordance with their subjective sleep need, with a shift towards later bedtime of more than 2 h and an even later rise time.
Sleep deprivation affects frontal areas and executive functioning especially in infants
• The impact of sleep deprivation is more prominent in frontal than posterior brain areas (Cajochen, et al., 2001) and frontal brain regions seem to have a higher need for recovery during sleep than posterior areas (Beebe & Gozal, 2002; Dahl, 1996; Horne, 1993).
• Given that major advances in EF take place between 1 and 6 years of age (Zelazo et al., 2008), and that neural density of the frontal lobes begins to decline at about 7 years of age (Huttenlocher, 2002), the potential impact of sleep on frontal⁄executive functions may be especially potent earlier in development, when the brain shows substantial dynamic plasticity (Singer, 1995).
The mechanisms by which sleep deprivation and disruption, determine neurocognitive deficits are similar to those of
intermittent hypoxia
• Sleep-deprivation determined cellular injury (Everson, 2005), hippocampal oxidative stress (Gopalakrishnan et al., 2004; Silva et al., 2004), suppression of neurogenesis and long-term potentiation in the hippocampus (Hairston, 2005) and affect brain structures involved in motivation, goal direction, reward, and attentional capacity.
• In the developing brain, exposure to sleep deprivation during sensitive periods may result in morbid and potentially irreversible changes in neural organization in these brain sectors (Frank et al., 2003)
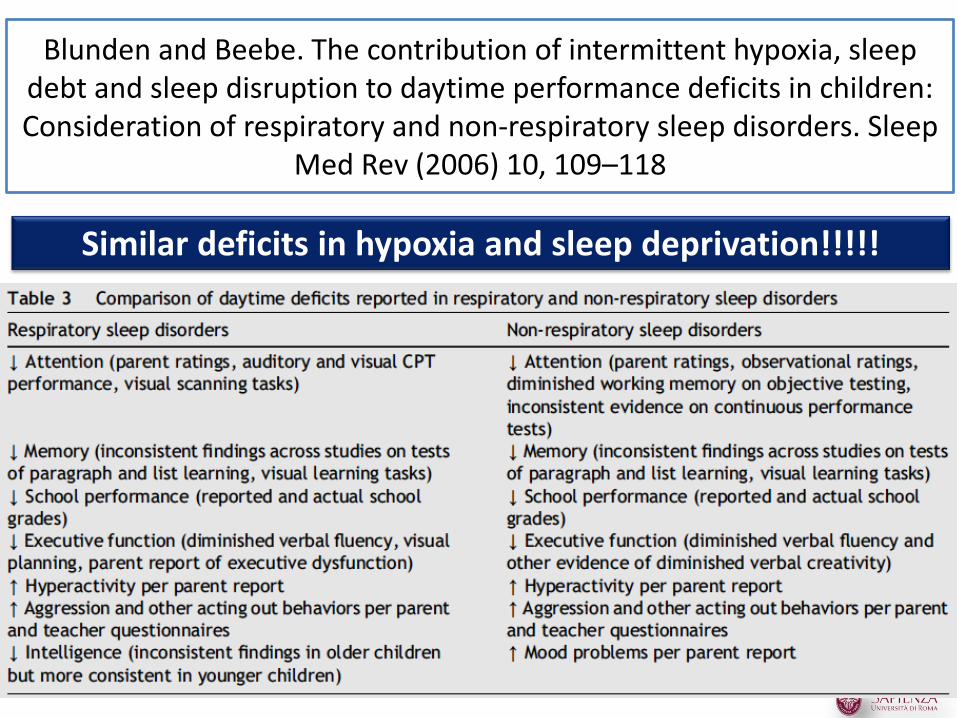
Blunden and Beebe. The contribution of intermittent hypoxia, sleep debt and sleep disruption to daytime performance deficits in children: Consideration of respiratory and non-respiratory sleep disorders. Sleep
Med Rev (2006) 10, 109–118
Similar deficits in hypoxia and sleep deprivation!!!!!
Thanks for your
attention!