Oikawa et al nt J rain Disord Treat 21, 31 Volume ssue 2 ... · 14. Morotti A, Liberini P, Padovani...
2
International Journal of Brain Disorders and Treatment Oikawa et al. Int J Brain Disord Treat 2019, 5:031 Volume 5 | Issue 2 DOI: 10.23937/2469-5866/1410031 • Page 1 of 2 • Oikawa et al. Int J Brain Disord Treat 2019, 5:031 Open Access ISSN: 2469-5866 Citaon: Oikawa JET, de Souza JGL, Ferreira VCC, Wille PR, Parolin LF, et al. (2019) Opc Perineuris Secondary to Sjogreen’s Syndrome: Case Report. Int J Brain Disord Treat 5:031. doi.org/10.23937/2469- 5866/1410031 Accepted: November 02, 2019: Published: November 04, 2019 Copyright: © 2019 Oikawa JET, et al. This is an open-access arcle distributed under the terms of the Creave Commons Aribuon License, which permits unrestricted use, distribuon, and reproducon in any medium, provided the original author and source are credited. Opc Perineuris Secondary to Sjogreen’s Syndrome: Case Report Juliana Emy Tolachinski Oikawa 1* , Julia Gomes Leite de Souza 1 , Vitória Caroline Cardoso Ferreira 1 , Paulo Roberto Wille, MD, PhD 2 , Laura Fiuza Parolin, MD 3 and Marcus Vinícius Magno Gonçalves, MD, PhD 3 1 Medical Students, Universidade da Região de Joinville, Brazil 2 Department of Radiology, Universidade da Região de Joinville, Brazil 3 Department of Neurology, Universidade da Região de Joinville, Brazil *Corresponding author: Juliana Emy Tolachinski Oikawa, Medical Students, Universidade da Região de Joinville, Joinville, SC 89219-710, Brazil positive (23.6) and anti-RO/LA antibody positive. Cra- nial MRI showed very thin and intense contrast en- hancement along both optic nerve sheath and parot- id edema associated (Figure 1) meeting the criteria of Sjogren syndrome (SS) [19]. We found no evidence of secondary SS suggesting a form primary. Paent had clinical improvement of visual acuity and retroocular pain parally aſter pulse therapy with methylprednisolone. Rituximab maintenance paent every 6 months. SS is a rare cause and should not be forgoen as a differenal diagnosis of opc perineurit. References 1. Lai C, Sun Y, Wang J, Purvin VA, He Y, et al. (2015) Optic perineuritis in behçet disease. J Neuroophthalmol 35: 342- 347. 2. Lana-Peixoto MA (2002) Sistema sensorial-parte I-Re- visão 1997-1999. Neurooftalmologia. Arquivos Brasileiros de Oftalmologia. 3. Tatsugawa M, Noma H, Mimura T, Funatsu H (2010) High- dose steroid therapy for idiopathic optic perineuritis: A case series. J Med Case Rep 4: 404. 4. Purvin V, Kawasaki A (2009) Optic perineuritis secondary to wegener’s granulomatosis. Clin Exp Ophthalmol 37: 712-717. 5. Toshniwal P (1987) Optic perineuritis with secondary syph- ilis. J ClinNeuroophthalmol 7: 6-10. 6. Lim SH, Heng LK, Puvanendran K (1990) Secondary syph- ilis presenting with optic perineuritis and uveitis. Ann Acad Med Singapore 19: 413-415. Keywords Optic perineurits, Sjogreen, Neuroimmunology CASE REPORT Check for updates Opc perineuris (OPN) is a rare inflammatory dis- ease involving the opc nerve sheath [1], causing pain and disc edema and is oſten bilateral [2]. The diagnosis of OPN is commonly based on magnec resonance im- aging (MRI) findings and clinical features [3]. In MRI it is possible to visualize a circumferenal enhancement around the intraorbital opc nerve with preservaon of the nerve itself (doughnut sign) [4]. This is beer seen in contrast-enhanced and suppressed coronal MRI se- quences with fat. Magnec resonance imaging may also show enhancement of orbital fat and slight increase in extraocular muscles [1]. The eologies of OPN include syphilis [5,6], tuberculosis [7,8], herpes zoster [9], sar- coidosis [10,11], Wegener’s granulomatosis [12], gran- ulomatosis associated with polyangiis [13], giant cell arteris [14,15] Crohn’s disease [16], Behçet’s disease [1], acute renal necrosis [17]. However, in most cases, no specific eology is idenfied and these cases are cat- egorized as idiopathic OPN [18]. A 68-year-old woman started with a subacute onset of progressive visual acuity worsening associ- ated with bilateral retrobulbar pain about 4 months ago. Fundoscopy was normal and reduced direct and consensual photo motor reflex. Sicca syndrome was confirmed in Schirmer test. Rheumatoid factor was
Transcript of Oikawa et al nt J rain Disord Treat 21, 31 Volume ssue 2 ... · 14. Morotti A, Liberini P, Padovani...

International Journal of
Brain Disorders and Treatment
Oikawa et al. Int J Brain Disord Treat 2019, 5:031
Volume 5 | Issue 2DOI: 10.23937/2469-5866/1410031
• Page 1 of 2 •Oikawa et al. Int J Brain Disord Treat 2019, 5:031
Open Access
ISSN: 2469-5866
Citation: Oikawa JET, de Souza JGL, Ferreira VCC, Wille PR, Parolin LF, et al. (2019) Optic Perineuritis Secondary to Sjogreen’s Syndrome: Case Report. Int J Brain Disord Treat 5:031. doi.org/10.23937/2469-5866/1410031Accepted: November 02, 2019: Published: November 04, 2019Copyright: © 2019 Oikawa JET, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Optic Perineuritis Secondary to Sjogreen’s Syndrome: Case ReportJuliana Emy Tolachinski Oikawa1*, Julia Gomes Leite de Souza1, Vitória Caroline Cardoso Ferreira1, Paulo Roberto Wille, MD, PhD2, Laura Fiuza Parolin, MD3 and Marcus Vinícius Magno Gonçalves, MD, PhD3
1Medical Students, Universidade da Região de Joinville, Brazil2Department of Radiology, Universidade da Região de Joinville, Brazil3Department of Neurology, Universidade da Região de Joinville, Brazil
*Corresponding author: Juliana Emy Tolachinski Oikawa, Medical Students, Universidade da Região de Joinville, Joinville, SC 89219-710, Brazil
positive (23.6) and anti-RO/LA antibody positive. Cra-nial MRI showed very thin and intense contrast en-hancement along both optic nerve sheath and parot-id edema associated (Figure 1) meeting the criteria of Sjogren syndrome (SS) [19]. We found no evidence of secondary SS suggesting a form primary.
Patient had clinical improvement of visual acuity and retroocular pain partially after pulse therapy with methylprednisolone. Rituximab maintenance patient every 6 months. SS is a rare cause and should not be forgotten as a differential diagnosis of optic perineurit.
References1. Lai C, Sun Y, Wang J, Purvin VA, He Y, et al. (2015) Optic
perineuritis in behçet disease. J Neuroophthalmol 35: 342-347.
2. Lana-Peixoto MA (2002) Sistema sensorial-parte I-Re-visão 1997-1999. Neurooftalmologia. Arquivos Brasileiros de Oftalmologia.
3. Tatsugawa M, Noma H, Mimura T, Funatsu H (2010) High-dose steroid therapy for idiopathic optic perineuritis: A case series. J Med Case Rep 4: 404.
4. Purvin V, Kawasaki A (2009) Optic perineuritis secondary to wegener’s granulomatosis. Clin Exp Ophthalmol 37: 712-717.
5. Toshniwal P (1987) Optic perineuritis with secondary syph-ilis. J ClinNeuroophthalmol 7: 6-10.
6. Lim SH, Heng LK, Puvanendran K (1990) Secondary syph-ilis presenting with optic perineuritis and uveitis. Ann Acad Med Singapore 19: 413-415.
KeywordsOptic perineurits, Sjogreen, Neuroimmunology
CaSE REPORT
Check forupdates
Optic perineuritis (OPN) is a rare inflammatory dis-ease involving the optic nerve sheath [1], causing pain and disc edema and is often bilateral [2]. The diagnosis of OPN is commonly based on magnetic resonance im-aging (MRI) findings and clinical features [3]. In MRI it is possible to visualize a circumferential enhancement around the intraorbital optic nerve with preservation of the nerve itself (doughnut sign) [4]. This is better seen in contrast-enhanced and suppressed coronal MRI se-quences with fat. Magnetic resonance imaging may also show enhancement of orbital fat and slight increase in extraocular muscles [1]. The etiologies of OPN include syphilis [5,6], tuberculosis [7,8], herpes zoster [9], sar-coidosis [10,11], Wegener’s granulomatosis [12], gran-ulomatosis associated with polyangiitis [13], giant cell arteritis [14,15] Crohn’s disease [16], Behçet’s disease [1], acute retinal necrosis [17]. However, in most cases, no specific etiology is identified and these cases are cat-egorized as idiopathic OPN [18].
A 68-year-old woman started with a subacute onset of progressive visual acuity worsening associ-ated with bilateral retrobulbar pain about 4 months ago. Fundoscopy was normal and reduced direct and consensual photo motor reflex. Sicca syndrome was confirmed in Schirmer test. Rheumatoid factor was

ISSN: 2469-5866DOI: 10.23937/2469-5866/1410031
Oikawa et al. Int J Brain Disord Treat 2019, 5:031 • Page 2 of 2 •
phenolate mofetil combination therapy. Eur J Rheumatol 4: 70-72.
14. Morotti A, Liberini P, Padovani A (2013) Bilateral optic peri-neuritis as the presenting feature of giant cell arteritis. BMJ Case Rep.
15. Pappolla A, Silveira F, Norscini J, Miquelini L, Patrucco L (2019) Bilateral optic perineuritis as initial presentation of giant cell arteritis. Neurologist 24: 26-28.
16. Mcclelland C, Zaveri M, Walsh R, Fleisher J, Galetta S (2012) Optic perineuritis as the presenting feature of crohn disease. J Neuroophthalmology 32: 345-347.
17. Byon IS, Jung JH, Kim HY, Park SW, Lee JE (2013) Op-tic perineuritis secondary to acute retinal necrosis. J Neu-ro-Ophthalmology 33: 419-421.
18. Hickman SJ (2016) Optic perineuritis. Curr Neurol Neurosci Rep 16: 16.
19. Vitali C, Bombardieri S, Jonsson R, Moutsopoulos HM, Al-exander EL, et al. (2002) Classification criteria for sjögren’s syndrome: A revised version of the European criteria pro-posed by the American-European consensus group. Ann Rheum Dis 61: 554-558.
7. Raghibi A, Wan Hitam WH, Noor RAM, Embong Z (2012) Optic perineuritis secondary to tuberculosis: A rare case presentation. Asian Pac J Trop Biomed 2: S1206-S1208.
8. Yates WB, Nothling S, Lawlor M (2019) Optic perineuritis due to tuberculosis. J Neuro-Ophthalmology 39: 257-259.
9. Bansal R, Singh R, Takkar A, Lal V (2017) Combined cen-tral retinal artery and vein occlusion with optic perineuritis following herpes zoster dermatitis in an immunocompetent child. Indian J Ophthalmol 65: 1233-1235.
10. Yu-Wai-Man P, Crompton DE, Graham JY, Black FM, Dayan MR (2017) Optic perineuritis as a rare initial pre-sentation of sarcoidosis. Clin Exp Ophthalmol 35: 682-684.
11. Kidd DP, Burton BJ, Graham EM, Plant GT (2016) Optic neuropathy associated with systemic sarcoidosis. Neurol Neuroimmunol Neuroinflammation 3: e270.
12. Takazawa T, Ikeda K, Nagaoka T, Hirayama T, Yamamoto T, et al. (2014) Wegener granulomatosis-associated optic perineuritis. Orbit 33: 13-16.
13. Yoshitaka K, Kurumi A, Hirotoshi K, Hajime K (2017) Re-fractory optic perineuritis due to granulomatosis with poly-angiitis successfully treated with methotrexate and myco-
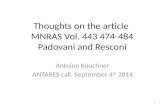
Figure 1: Axial A) T1-spin echo, after gadolinium iv injection and axial; B) T2 with fat saturation show a very thin and intense symmetrically contrast enhancement along both optic nerve sheath as well a high intensity thickening along of both optic perineural CSF space. Coronal C) T1-spin echo, after gadolinium i.v. injection and coronal; D) T2 with fat saturation reveal a symmetrical increase of parotidite glands.