
Regional Vaccine Matching Results and Recommendations Regarding to Sample Submission

OFFICE OF THE ASSISTANT REGIONAL DIRECTOR
IMMUNIZATIONS AND VACCINE DEVELOPMENT PROGRAMME (IVD)
PANDEMIC INFLUENZA A (H1N1) 2009
VACCINE DEPLOYMENT ACTIVITY IN AFRICAN REGION
PART TWO: SUB-REGIONAL REPORTS
31 October 2010, Brazzaville, Republic of Congo

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 2
IST Central Africa
Technical Support to the Influenza H1N1 Vaccine Deployment
Program
Final Report of Mission: June - October 2010
Consultants:
Dr. ALOMBAH, Fozo Richard (MD, M.Sc.)
&
Mr. SEKA Nda Leonce (Ing. Logisticien)

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 3
Acknowledgements
The authors of this report wish to sincerely thank the WHO and USAID who provided the necessary financial and
logistics support that enabled the accomplishment of this assignment. Our special thanks go to Dr. Richard Mihigo,
Dr. Imboua Lucile and Dr. Norbert Ngendabanyikwa whose technical guidance and regular counsel was crucial in
surmounting certain obstacles.
Our thanks and appreciation also go to the WHO Country Representatives and IVD focal points, as well as the EPI
managers who were so instrumental as a liaison between us and the country coordinating committees and health
authorities in advocacy.
We equally want to thank our colleagues and support staff of the IST who enabled us to fully integrate the team and
receive all support necessary for daily activities.
Finally, we will like to thank Dr. Max Mondestin for the foundation he laid for this work. We also express special
appreciation to our colleagues Zenaw Adam and Chweya Amos of the AFRO office, Faich Hannah-Sarah, Ousmane
Dia, Robert Steinglass, Michel Othepa, Kathy Haines, Elena Kanevsky and Karlan Jankowski for continued
technical and logistics support during this assignment

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 4
Executive Summary
WHO declared Influenza A H1N1 pandemic in June 2009. Countries of the WHO/AFRO region joined the global
effort to contain the spread of the virus. In addition to implementing the general measures recommended by WHO,
countries subscribed to vaccinate 10% of their populations with the limited doses of H1N1 vaccine donated by the
WHO and partners. The United States government which donated a substantial amount of vaccine equally provided
financial assistance and recruited consultants to provide technical assistance. The main objective of this consultancy
was to provide complementary technical and programmatic support to the IST in the immunization preparedness and
response to the H1N1 influenza pandemic in all 10 Central African countries. After the Abuja workshop, eligible
countries were requested to finalize and submit national vaccines deployment plans (NDPs) and fulfill certain
conditions (signing of letters of intent and agreement, submission of validated plan, authorization of importation of
vaccines) in order to gain access to the donated vaccines.
After initial work done with support from the first USAID consultant from January to May 2010, countries of the
Central African sub-region variedly adhered to these conditions. From June to October 2010, this consultancy
continued to support countries to finalize and submit NDPs, submit documents for vaccine shipment, elaborate/adapt
training and management tools for the immunization campaigns, and field visits to support social mobilization and
organization of campaigns. Challenges included dysfunctional coordination committees, more urgent health
priorities, and shortage of staff, administrative and political bottlenecks and insufficient information on vaccines.
Apart from the DRC which signed only the letter of intent (LOI), all countries of the sub-region signed letters of
agreement (LOA), but only seven (Angola, Burundi, Cameroon, Congo, CAF, Eq. Guinea, Sao Tome & Principe)
succeeded to submit validated NDPs that were approved. Burundi later on withdrew from the process and 6
countries received the requested doses of vaccine accompanied by matching ancillary supplies and funds to support
operational deployment costs. By the time of this report, only three countries (Sao Tome & Principe, Congo and
CAF) actually organized vaccination campaigns and submitted termination reports. Results showed that vaccination
coverage was 53% in Congo, 81% in CAF and 80% in STP. In general, low coverage was reported among pregnant
women compared to other groups. Altogether, 180 cases of alleged AEFI were reported in CAF Congo, and STP.
None of these cases was confirmed by investigation reports as linked to the vaccine. In general, AEFI surveillance is
weak in the sub-region.
The support provided by USAID was crucial in achieving these results. Collaboration between consultants and IVD
staff at all levels, as well as between consultants and country teams greatly enhanced the achievement of results.
Countries that implemented NDPs showed a high capacity of rapid mobilization. However, it may be difficult to
determine the preparedness of the countries to react to a pandemic situation from this exercise, since the
implementation took place within a context of relaxed alert and urgency and persistent misinformation.
Continued support from USAID to the IST through consultants can strengthen other program areas.

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 5
Table of Contents
1 Introduction: ................................................................................................................................................ 7
1.1 BACKGROUND ........................................................................................................................................... 7 1.2 OBJECTIVE OF MISSION ............................................................................................................................. 7 1.3 SPECIFIC OBJECTIVES ................................................................................................................................ 7 1.4 SITUATION AT THE START OF THE MISSION (MAY 31ST
2010) ........................................................................ 8
2 Implementation of Technical Assistance Activities ....................................................................................... 8
2.1 TECHNICAL SUPPORT NEEDS OF MEMBER STATES, ..................................................................................... 8 2.2 TECHNICAL SUPPORT PROVIDED ................................................................................................................ 9 2.3 OTHER ACTIVITIES WITHIN THE IST ......................................................................................................... 10
3 Accomplishments ....................................................................................................................................... 10
3.1 DEPLOYMENT OF VACCINES AND ANCILLARY SUPPLIES............................................................................ 10 3.2 IMPLEMENTATION EXPERIENCES OF COUNTRIES THAT ORGANIZED VACCINATION CAMPAIGNS .................. 12
4 Results ........................................................................................................................................................ 15
4.1 VACCINE DOSES ADMINISTERED AND COVERAGE ..................................................................................... 15 4.2 LOST VACCINE DOSES PER COUNTRY ........................................................................................................ 17 4.3 ADVERSE EVENTS REPORTED (AEFI) ....................................................................................................... 17
5 Challenges, Constraints and Strengths ........................................................................................................ 18
5.1 CHALLENGES ENCOUNTERED, PROPOSED SOLUTIONS AND LESSONS LEARNED .......................................... 18 5.2 STRENGTHS ............................................................................................................................................... 0
6 Conclusion and Recommendations ............................................................................................................... 0
6.1 CONCLUSION ............................................................................................................................................. 0 6.2 RECOMMENDATIONS ................................................................................................................................. 0 USAID: ............................................................................................................................................................. 0 WHO: ................................................................................................................................................................ 0

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 6
List of Tables
Table 1: Completion of program activities by country on May 31st 2010..………………………………7
Table 2: Technical assistance by country…………………………………………………………………8
Table 3: Financial Resources Provided by Country…....…………………………………………………10
Table 4: Human and material resources mobilization by three Country.…………………………………11
Table 5: Vaccine uptake by country…………….. ….……………………………………………………11
Table 6: Attribution of vaccine doses to target groups in countries.………………………………….…..12
Table 7: Vaccination coverage in three countries……………………….…………………………..….…17
Table 8: Vaccination coverage by country and by target group…………………………………………..17
Table 9: Wastage rates and remaining doses……….…………………………………………….…….…18
Table 10: Adverse events registered after vaccination……………………………………………………19
Table 11: Challenges of NDP development and implementation process………………………………...20
List of Figures
Figure 1: Distribution of Influenza A H1N1 Cases in Central Africa………………….………..………..6
Figure 2: Training sessions in Central African Republic………………………………….…...…………13
Figure 3: Training session and launching of activities in Congo…..………………………………….….14
Figure 4: Campaign banner Central African Republic...………………………………………………….14
Figure 5: Ministers laucnhing campaign in Central African Republic……………………………………15
Figure 6: Turn-out at vaccination sites in Central African Republic…...…………………………………16
Figure 7: Status of completion of main program activities………………….…………………………….16
Figure 8: Overal vaccination coverage in each country…..……………….………………………………17
List of Acronyms
AFRO region African regional
AED Academy for Educational Development
AEFI Adverse Events Reported after Immunization
LOI Letter of intent
LOA Letter of agreement
IST/CA Inter-country Support Team Central Africa
CAF Central Africa Republic
DRC Democratic Republic of Congo
STP Sao Tomé & Principe
EPI Expanded Program of Immunization
JSI John Snow Inc.
NDP National Deployment Plan
IVD Immunization Vaccine Development
USAID United States Agency for International Development
WHO World Health Organization

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 7
1 Introduction:
1.1 Background
In June 2009, WHO declared Influenza A H1N1 a pandemic. As part of the effort to assist health systems in
resource-limited countries to prevent, detect, treat and mitigate cases of illness associated with the Influenza A
H1N1 pandemic virus, and to reduce the impact of the pandemic on society, WHO coordinated efforts to help
countries meet the challenges. WHO/AFR through its IST sub-regional offices has been supporting countries’
operational response strategies including the preparation, implementation and coordination of country response
plans, revamping surveillance systems, procurement and use of vaccines, antiviral, and infection control
commodities and laboratory equipment.
From surveillance data up to June 2010, the AFRO region had registered a total of 18,598 confirmed
Influenza A H1N1 cases in 35 countries, with 168 deaths. As shown in figure 1 below, the Central
African sub-region reported 40 cases distributed among all countries except Equatorial Guinea; and 1
death registered in Sao Tome and Principe. This may be an underrepresentation given that countries used
sentinel sites for surveillance.
To assist developing countries with limited
resources, the US government and other partners
donated vaccines through the WHO vaccines
donation program. Through USAID, the US
government, in addition to financial and logistics
support, collaborated with WHO to recruit and
deployed experts at all levels, including the sub-
regional levels to technically support the deployment
of these vaccines. It is within the framework of this
collaboration that two consultants, Dr. ALOMBAH Fozo Richard (Epidemiologist) and Mr. SEKA Nda
Léonce (Logistician) were deployed to the IST/CA in June 2006 to continue the support started by the
previous USAID consultant, Dr. Max Mondestin since January 2010.
1.2 Objective of Mission The overall objective of this mission was to provide complementary technical and programmatic support to the IST
and countries in the sub-region in their immunization preparedness and response to the H1N1 influenza pandemic.
1.3 Specific Objectives Provide technical assistance to countries to finalize national Influenza H1N1 pandemic vaccines
deployment plans (NDPs) drafted in Abuja ;
Track progress of countries towards meeting preconditions for vaccine donation;
Monitor the mobilization and allocation of local financial and human resources towards the implementation
of the NDPs ;
Provide technical support to ensure the readiness of the national logistics management systems to receive
and deploy vaccine;
Support the organization of the immunization campaigns including micro-planning, training, vaccines
deployment, monitoring and supervision, and elaboration of termination reports;
0
1-25
26-100
Number of Cases
> 100
37
222
1
44
4 21 66
7
Total= 402 cas dont un décès

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 8
1.4 Situation at the start of the mission (May 31st 2010)
The situation of each country with respect to program activities at the end of May 2010 when the previous
consultant ended his mission stood as follows:
Table 1: Completion of Program Activities by Country on May 31st 2010
This table shows that by end of May 2010:
9/10 countries in IST/Centre had issued LOAs (DRC did not submit)
7/9 countries (Angola, Burundi, Cameroon, Congo and Sao Tome and Principe, Gabon and Chad) had National
Deployment Plans technically reviewed by IST/CA, of which:
- Five were approved by the RO and HQ
- One (Gabon) was reviewed and awaiting political endorsement by the government
- One (Chad) was reviewed and sent back with comments to the country for corrections and
adjustment.
2 countries, (CAF, Eq. Guinea) had not submitted NDPs
One (1) country (Sao Tome and Principe) had already received vaccine and ancillary supplies but not yet
organized immunization campaign.
2 Implementation of Technical Assistance Activities
2.1 Technical Support Needs of Member States, Country teams remained in constant contact with the IST/CA office throughout the NDP development process.
Areas of need and challenges for which technical assistance was requested included;
- access to documentation at country level and in French language;
- elaboration/adaptation of tools and materials for training, social mobilization, data collection, and
reporting;
- providing responses to frequently asked questions and dissipating rumors and controversies about
H1N1 vaccination within countries;
- determining numbers and planning for the different target populations (pregnant women 2nd
&3rd
trimesters only, children from 6-59 months, chronic patients);
- resolving issues related to regulatory and legal bottlenecks;
- obtaining complete information on vaccines and planning arrival;
- orientating practical aspects of implementation especially social mobilization and training prior to
campaigns;
- advocacy in some countries to overcome political obstacles and gains support for program in
context of conflicting priorities and calendars;

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 9
2.2 Technical Support Provided Table 2: Technical Assistance by Country
Country Technical Assistance Requested Technical Assistance Provided
Angola Reference documents Documents transmitted and key information about
influenza H1N1 vaccine provided
Burundi Information and assistance to finalize and
submit vaccine importation documents
Liaison with Geneva to finalize documents and
provided more information for MOH to sign
importation documents
Cameroon Reference documents, support in reviewing
tools, support in organization of campaign
Translated documents transmitted, tools reviewed
and finalized, communication and social
mobilization materials shared, logistics tools
finalized.
Congo Reference documents, assistance to prepare
vaccine importation documents, support in
organizing campaign
Translated documents provided; tools reviewed and
finalized; follow up for vaccines arrival and
reception report; mission trip to support social
mobilization and training towards campaign; support
to finalize report and fill online evaluation tool.
Gabon Assistance to finalize plan Organized meeting with MOH
Continued follow-up with country team
Equatorial
Guinea
Assistance to finalize plan and complete
vaccine importation documents; reference
documents; liaison for vaccine shipment.
Reference documents provided, assistance to finalize
and validate plan, vaccine importation documents
facilitated; follow-up of shipment of donation
vaccine.
Central
African
Republic
Assistance in completing and validating
plan, transfer of funds, reference
documents, support to organize campaign.
Translated documents transmitted; tools reviewed
and finalized; follow up for vaccines arrival and
reception report; follow up of transfer of funds,
mission trip to support social mobilization and
training towards campaign; support to finalize report
and fill online tool
DRC None None
STP Clarification and support to elaborate
termination report
Provided report template and support to finalize
report and fill online tool
Chad Clarification about process and operational
costs
Continued contact and exchanges with the WR to
support process, reference documents shared,
To render technical assistance effective, consultants developed various strategies:
advocacy strategies were initiated to support process in-country
reference documents elaborated by WHO and partners were translated into French and
transmitted to the countries;
assistance was equally provided to the countries to elaborate other documents, including a
compilation of frequently asked questions and answers, training, communication and social
mobilization, management and data collecting tools;
permanent contact maintained with countries through e-mail, telephone (GPN and cell)
technical assistance visits were conducted to assist in advocacy, social mobilization, training,
supervision and other aspect of the immunization campaign;
Liaison with IVD colleagues on other TA visits to the various countries equally assisted in follow
up and feedback on pending issues;

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 10
weekly and monthly IVD technical staff meetings were tapped in to discuss challenges with other
colleagues and develop new strategies.
Quite often, technical assistance was effective in helping countries overcome challenges. In some case,
however, it was not enough to resolve all issues. Consultants frequently had to turn to the IST/IVD Focal
point and even the Coordinator to get more support especially in advocacy. Yet in other cases, it did not
yield fruit. Even interventions from the regional and headquarter offices in other cases were still not
sufficient to resolve outstanding issues and facilitate the process.
2.3 Other Activities within the IST
As integral part of the IST/IVD staff, consultant also participated in weekly and monthly IVD and inter-
divisional IST coordination meetings and related AFRO (Brazzaville)-level IVD teleconferences.
Contributions to and learning from data analysis, and validation of reports enriched both consultants and
the IVD team.
Within the IVD, consultants particularly got involved in IST monitoring of and monthly reporting on
country progress in implementing the four IVD priorities (interrupting the circulation of poliomyelitis,
reducing the number of unimmunized children, improving data quality and accelerated disease control)
and sat in for colleagues on mission to respond to all solicitations concerning these areas. Consultants
equally participated in the creation of IST sub-clusters.
Monthly update reports of progress in H1N1 activities were provided to the IST, AFRO and USAID.
3 Accomplishments
3.1 Deployment of Vaccines and Ancillary Supplies
3.1.1 Resolving Legal and Regulatory Issues The regulatory authorities in the countries were strict in applying regulation concerning importation of vaccines. The
pre-qualification certificate and the letter of agreement which served as a waiver were largely used to convince these
authorities to deliver importation authorizations.
IST facilitated the obtaining of other documents (airway bill, certificate of origin, package list, and customs value of
donation). Navigating through this process was a challenge because the country authorities requested to have these
documents before signing authorization to import the vaccines, while manufacturers requested the importation
authorization before releasing the vaccines along-side these documents.
3.1.2 Resources Mobilization for Vaccine Deployment In addition to vaccines and ancillary supplies, financial, human and other material resources were mobilized for the
campaigns. WHO mobilized resources to support countries conduct deployment operations. The following table
summarizes allocation of vaccines, ancillary supplies and funds for countries.
Table 3: Material and Financial Resources Provided by Country

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 11
Apart from Angola whose government promised f$211,293 for operational costs, no other country mobilized local
financial resources for this activity. However, human and material resources were mobilized in the countries for the
exercise.
Table 4: Human and Material Resources Mobilization
3.1.3 Reception, Storage and Distribution of Vaccines In general, analysis of reports of reception and distribution of vaccines, syringes, and safety boxes showed
satisfactory management of the process.
In addition to syringes and safety boxes received with the vaccines, some countries procured other ancillary
supplies such as cotton, soap, gloves and bin liners.
- To ensure appropriate storage temperatures and hence quality, countries generally stored the vaccine at the
central level, and dispatched them to the field less than a week before the organization of the campaign.
- Logisticians in general, used previously developed mass campaign distribution tools which were adapted to
this particular context to manage vaccine deployment. Supervisors and trainers used central, regional and
district service vehicles to transport vaccines. To close transportation gaps, rental vehicles were used.
Table 5: Vaccine Uptake by Country and wastage
- There were difficulty determining wastage rate with accuracy because children 6-35 months who received
½ doses were not accurately accounted for
- Wastage was increased by use of 0,5ml syringes without sub-graduation to administer ½ doses
- Of the 3,027,010 doses received, only 710, 490 doses have so far been used
- The remaining doses (153 510) in STP and CAF expired
- The 1 220 900 doses in Cameroon and Eq. Guinea will expire if not used by October 30th, thereby
increasing the wastage

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 12
Table 6: Attribution of Vaccine Doses to Target Groups in Countries
Since there were no established formulae to determine the population size within each priority group, random
attribution resulted in vaccination data significantly different from targets. In addition, during vaccination, off-
target persons were included either on instructions from authorities or due to difficulties screening.
3.2 Implementation Experiences of Countries that Organized
Vaccination Campaigns Three countries of the sub-region -Sao Tome & Principe (9-12 June 2010), Congo and Central African Republic
(25-30 August 2010) - so far have implemented NDPs. The context in each country was different and hence
experiences were varied.
3.2.1 Training, Micro Planning and Pre-Campaign Activities Consultants supported pre-campaign activities, including adaptation/elaboration of tools, logistics operational plans,
and communication/social mobilization materials.
To build capacity within country pandemic preparedness teams, training tools proposed by WHO were generally
adapted and used for training sessions. In addition to other materials and documents, IST consultants prepared and
delivered three presentations as part of the training of trainers in Congo and CAF, focusing on general updates on
Influenza H1N1 and vaccination, logistics management and social mobilization. Particularly these presentations
were geared towards dissipating rumors and gaining buy-in of stakeholders on the raison d’être of vaccination.
In general, countries waited for the arrival of vaccines and agreement on campaign days before initiating micro-
planning activities. These activities began 7 to 10 days before the launching of the campaign. Countries trained
national trainers/supervisors who in turn rolled out training in cascade together with assistance to districts in their
micro-planning activities. In Congo and Central African Republic where vaccines were received close to expiry
dates, the chronogram of activities was modified to accelerate these activities.
Central African Republic
In Central African Republic, one national training session was organized for all central level, regional and district
supervisors, who in turn organized regional and district-level training of supervisors and vaccinators. It was however
observed during supervision of the campaign that some vaccinators received a briefing instead of full training.
Because of this lacuna in training and given that this was a new vaccine with its specificity, some vaccinators had
difficulties in vaccine administration and data collection. For example, instead of giving 0.25ml to children of 6-35
months, some vaccinators administered 0.5ml to everybody. Some administered 0.25ml to children but did not
indicate on tally sheets.

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 13
Fig. 2: Training Sessions in Central African Republic
The implication of representatives of priority groups (security forces and health personnel) in training and operations
at all level contributed to the success of the campaign in CAF, where IST consultants also supported the country
team to organize a special training session for media professionals and other social mobilization activities in
response to the general apprehensive atmosphere surrounding the arrival of the vaccine. This training of media
professionals was the turning point in sensitization and social mobilization.
Congo
In Congo, the country team opted for two pooled training sessions in Brazzaville and Pointe Noire where central-
level and regional supervisors were trained, to roll out cascade training in the country. Much of micro-planning was
discussed during these training sessions.
Fig. 3: Training session and launching of activities in Congo
3.2.2 Social Mobilization and Launching Ceremony: Campaign activities were launched in Congo and CAF in a context characterized by apprehensions and questioning
especially from university circles following rumors and misinformation propagated by foreign media. The necessity
to vaccinate after the WHO had declared the end of pandemic, why vaccines are coming in almost expired, why only
10% of population and why the specific groups were some of the questions asked. In addition, the fact that vaccines
had no control patch on vials compounded these apprehensions. It took tactful advocacy and social mobilization
strategies from the IST in support of the country teams for the governments to accept to vaccinate and for the target
groups to adhere.
All three countries developed social mobilization support materials including banners, posters, essential messages,
radio spots in local languages and television spots. Apart from Sao Tome & Principe (STP) the other two countries
of the sub-region officially launched vaccination campaigns with a public
ceremony.
Sao Tome & Principe
In STP, due to lack of a budget for a public launching, the Minister of
health launched activities through a radio and television communiqué
which was relayed by news papers and local radio stations.
Congo

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 14
In Congo, officials limited the scope of public launching to a low-key ceremony for fear that a massive turn-out and
subsequent stock-out of vaccines may lead to unforeseen consequences. In addition, diffusion of social mobilization
messages which were prepared ahead of time was limited to regions outside of Brazzaville.
Activities in Congo started up timidly on the first day, limited to health workers with more passive supervision.
With health workers’ acceptance, vaccination was progressively extended to other priority groups. But it was clear
that this approach adversely affected social mobilization and popular adhesion to the program.
Central African Republic
In Central African Republic, after officials and the population were convinced through targeted advocacy social
mobilization, a very high profile launching ceremony was organized with both the ministers of Public Health and
Interior giving the first doses of vaccine in front of a crowd and representatives of major media outlets in the
country. Subsequent to this launching and the press conference which the minister of health gave within the training
of trainers, massive turn out was observed.
Fig 5: Ministers Launching Campaign in CAF
The implication of leaders within priority groups (security officers, health workers) in training activities was equally
instrumental in galvanizing the population.
3.2.3 Supervision and Monitoring of Campaign Activities Central level supervisors were dispatched to regions to support regional and district level supervisors. Monitoring of
activities was done through a permanent campaign secretariat that was on telephone contact with field actors to
register any issues and bring them to the national coordination committee for discussion.
In CAF, mobile telephone network was reinforced by a command radio system which exchanged information every
morning. Supervisors were particularly instructed to ensure that any adverse events were notified and properly
investigated and managed. From supervision of activities in CAF it was noted that there was massive turn-out at
vaccination sites leading to stock out of vaccine in some health areas on the second day. Few cases of adverse events
and insufficient transportation were notified, but not investigated. Training gaps were also noted in some areas.
In Congo, an assessment of the first day by the coordination committee formulated recommendations that were
relayed to the field. This subsequently reinvigorated activities that had started timidly.
Fig 6: Turn-out at Vaccination Sites in CAF
CAF: Minister of Health administering first dose of vaccine to
a security officer with The Minister of Interior on standby
(25/08/25)
CAF: Launching of vaccination campaign: From right to left:
WHO Representative, Minister of Health, Minister of Interior,
and Director of Community Hospital (25/08/2010)

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 15
3.2.4 Healthcare Waste Management Waste management remains a challenge in the sub-region as a whole due to absence of operational national waste
management plans and infrastructure. Burning and burying as well as transportation to designated burning sites were
methods used. Off-site transportation of waste was not regularly ensured and this accounted for waste accumulation
at some health facilities.
4 Results The key accomplishments of this mission were:
Seven of the ten countries successfully had plans approved, 6 of which received vaccines and 3 completed
vaccination campaigns
A total of 587,074 persons (210,379 in Congo, 364,476 in CAF, 12,219 in STP) were vaccinated against
the Influenza H1N1 virus, of which 26,327 were health workers
More awareness was raised and capacity was built within pandemic readiness teams in the three countries
to organize pandemic vaccine deployment activities. A total of 317 trainers and supervisors, 2130
vaccinators, 1067 volunteers and social mobilization agents were trained.
The following table and figures present the key results obtained in the countries that completed campaign activities
by the end of October 2010 when the program closed down:
Fig. 7: Status of Completion of Main Program Activities
This graph shows that significant progress was made during the period June through October. Seven countries in all
had NDPs approved, six (Angola, Burundi, Cameroon, Congo, Central African Republic, Equatorial Guinea and Sao
Tome and Principe) received vaccines and three (Central African Republic, Congo and Sao Tome and Principe)
organized vaccination campaigns.
4.1 Vaccine Doses Administered and Coverage Vaccination coverage for the three countries which completed activities is represented below. However, because
targets were arbitrarily set, coverage figures are not representative.
Table 7: Vaccination Coverage in Three Countries

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 16
Fig 8: Overall Vaccination Coverage and in each Country
Table 8: Vaccination Coverage by Country and by Target Group
Country
Priority Groups covered
Health
staff
Pregnant
women
Children
6-59
months
Chron.
diseases Others Total
Congo 14494 12266 157952 0 25667
210,379
Central
African
Republic 10783 26861 232511 78854 15467
364,476
Sao Tome
and Principe 1050 1759 6868 2542 0
12,219
Total 26327 40886 397331 81396 41134
587,074
These results show:
low turn-out among pregnant women in all three countries - pregnant women usually get vaccinated during
prenatal consultations over longer periods;
high turn-out in the target groups “others” and “chronic patients” in which were included security and
emergence personnel in Congo and CAF. But also people who were not eligible (government officials,
emergency and security personnel) and managed to get vaccinated were recorded as others or chronic patients
Massive participation of among health workers (146%) - vaccination in this group was extended to all hospital
workers without distinction.

WHO/IST/C.A Mission Report Influenza H1N1 Support Mission June- October 2010 17
4.2 Lost vaccine doses per country Table 9: Wastage Rates and Remaining Doses
- No cases of lost or damaged vaccines were reported during reception and deployment.
- The remaining doses in Congo and STP (153 510) could not be used at a later time due to short shelf life.
- Of 3,027,010 doses received, only 710, 490 doses have so far been used
- Also, if Cameroon, Eq. Guinea, do not organize vaccination activities by the end of October, a substantial
number of doses (1 220 900) will expire.
- Concerns raised by countries about the vaccine included the absence of control patches on the vials,
absence of graduation on 0.5ml syringes to enable the use of ½ doses, which accounted for the high
wastage rate in some countries.
- In general, the wastage ratio could not be accurately determined for the three countries that organized
campaigns because the total number of children who received ½ doses was not recorded in data collection.
- Tools were revised for the remaining countries eventually organizing campaigns, to take into account these
children
4.3 Adverse Events Reported (AEFI) The following chart represents the principal types of supposed adverse events recorded during the campaigns in the
three countries (CAF, Congo and STP).
Table10: Adverse Events Registered After Vaccination
During training, emphasis was placed on the need to monitor, notify properly investigate and manage all AEFI
cases. However, no country conducted investigations of supposed AEFI cases. Hence it will be difficult to link the
180 cases notified in the three countries to the vaccin. The AEFI surveillance systems in the sub-region need
strengthening not only for vaccines but to ensure good pharmacovigilance.

5 Challenges, Constraints and Strengths
5.1 Challenges Encountered, Proposed Solutions and Lessons learned The challenges encountered during this process, solutions applied and lessons learned are presented in table 10 below.
Table 11: Challenges of the NDP Development and Implementation process
Country Major Challenges/Constraints Action Taken Results Lesson learned
Sao Tome
&
Principe
A documentary diffused over national television at the eve
of the launching of immunization campaign, attributing
abortions to H1N1 vaccine. This reinforced circulating
misinformation
Intensified sensitization
campaign during the
immunization campaign
Some pregnant women
accepted to be vaccinated but
this negatively affected
coverage
Social mobilization and sensitization
towards immunization campaign
should be initiated early enough
before the event and the media
should be provided with accurate
information
Central
African
Rep.
Vaccines received close to the end of shelf life, vaccines
without control patch, and the announcement of the end of
pandemic were all factors that contributed to reinforce
skepticisms and questions
A technical assistance visit
focused on advocacy and
social mobilization. Special
training/information session
organized for media
professionals to gain their
support
Convinced, the ministers of
health and interior provided
the political backing while the
media sensitized the
population, leading to massive
participation of the population
Developing strategies to gain
support from political authorities
and the media is crucial in the
success of a mass health action,
especially in the face of
controversies
Congo Just like CAF, Congo received vaccine close to expiry date.
In addition, vaccines came in after the declaration of end of
pandemic. These factors coupled with the already
circulating misinformation about the vaccines created
reticence among some authorities. Authorities decided to
limit social mobilization. In addition, children who
represented 60% of the target population were on school
holidays and difficult to reach
Technical assistance was
provided to the IVD country
team to organize advocacy
towards authorities to accept
to vaccinate as planned
After intense effort,
vaccination was launched
starting with health workers so
as to test acceptability.
Eventually children were
vaccinated but the target was
not met
Various factors, related or not to the
program do influence the decision-
making process of political
authorities and must be considered
during planning
Angola Because of the intense polio riposte activities, Angola was
unable to find an opening on the calendar to organize a
campaign. The plan was to integrate the H1N1 vaccine into
routine immunization, contrary to plan.
While providing continued
support to the polio
immunization campaigns,
IST advocated for the
organization of the H1N1
campaign but never found a
window of opportunity
Since the H1N1 vaccines
could not be integrated into
routine Immunization, the
country conserved the vaccine
while waiting for an
opportunity.
Countries dealing with several
health challenges balance the costs
and benefits of investing resources
in each new program
19
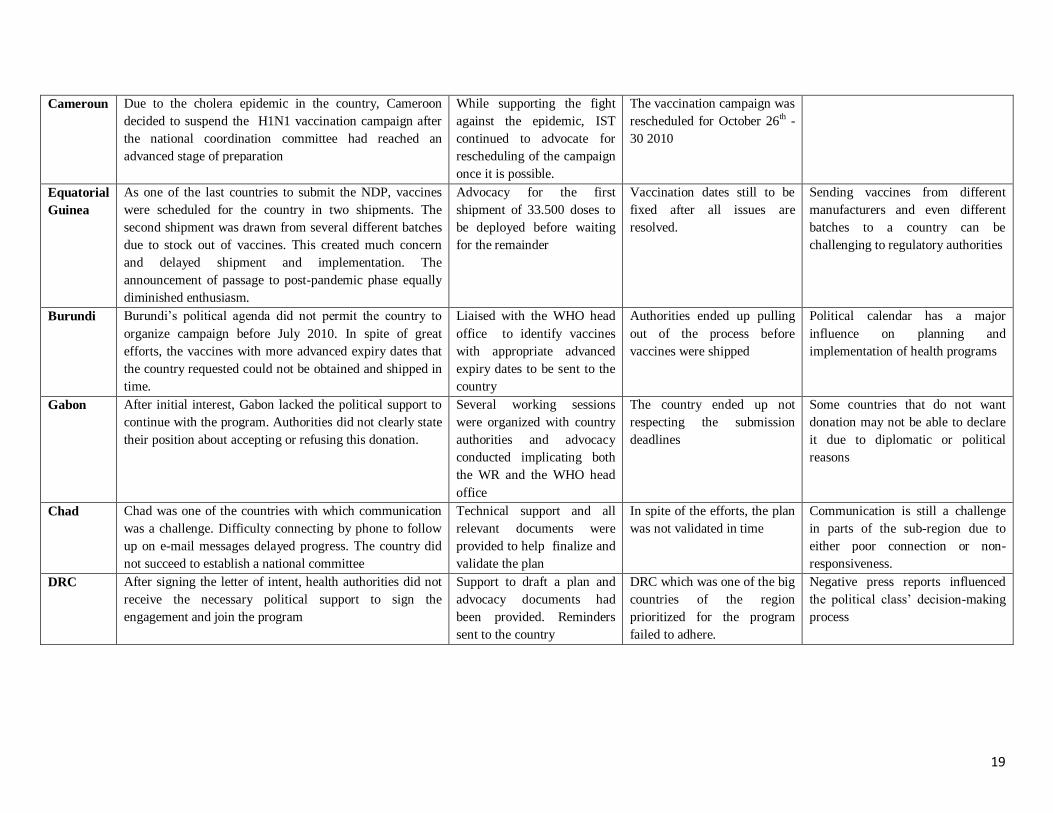
Cameroun Due to the cholera epidemic in the country, Cameroon
decided to suspend the H1N1 vaccination campaign after
the national coordination committee had reached an
advanced stage of preparation
While supporting the fight
against the epidemic, IST
continued to advocate for
rescheduling of the campaign
once it is possible.
The vaccination campaign was
rescheduled for October 26th -
30 2010
Equatorial
Guinea
As one of the last countries to submit the NDP, vaccines
were scheduled for the country in two shipments. The
second shipment was drawn from several different batches
due to stock out of vaccines. This created much concern
and delayed shipment and implementation. The
announcement of passage to post-pandemic phase equally
diminished enthusiasm.
Advocacy for the first
shipment of 33.500 doses to
be deployed before waiting
for the remainder
Vaccination dates still to be
fixed after all issues are
resolved.
Sending vaccines from different
manufacturers and even different
batches to a country can be
challenging to regulatory authorities
Burundi Burundi’s political agenda did not permit the country to
organize campaign before July 2010. In spite of great
efforts, the vaccines with more advanced expiry dates that
the country requested could not be obtained and shipped in
time.
Liaised with the WHO head
office to identify vaccines
with appropriate advanced
expiry dates to be sent to the
country
Authorities ended up pulling
out of the process before
vaccines were shipped
Political calendar has a major
influence on planning and
implementation of health programs
Gabon After initial interest, Gabon lacked the political support to
continue with the program. Authorities did not clearly state
their position about accepting or refusing this donation.
Several working sessions
were organized with country
authorities and advocacy
conducted implicating both
the WR and the WHO head
office
The country ended up not
respecting the submission
deadlines
Some countries that do not want
donation may not be able to declare
it due to diplomatic or political
reasons
Chad Chad was one of the countries with which communication
was a challenge. Difficulty connecting by phone to follow
up on e-mail messages delayed progress. The country did
not succeed to establish a national committee
Technical support and all
relevant documents were
provided to help finalize and
validate the plan
In spite of the efforts, the plan
was not validated in time
Communication is still a challenge
in parts of the sub-region due to
either poor connection or non-
responsiveness.
DRC After signing the letter of intent, health authorities did not
receive the necessary political support to sign the
engagement and join the program
Support to draft a plan and
advocacy documents had
been provided. Reminders
sent to the country
DRC which was one of the big
countries of the region
prioritized for the program
failed to adhere.
Negative press reports influenced
the political class’ decision-making
process

5.2 Strengths Complete integration of the consultants into the IVD team enabled consultants to benefit from the support
of team members and to contribute to strengthen aspects of other vaccination programs.
The communications structure of the WHO (GPN, cell phone and e-mail system) put at the disposal of
consultants facilitated exchanges with country teams
The support of the IVD focal point and the IST coordinator was crucial in resolving difficult issues
The available reference documents on websites (WHO, CDC, USAID, JSI), as well as technical back-up
from the regional and head offices
The WHO country representatives were very instrumental in advocacy and creating collaborative links with
ministries of health
Technical expertise at IST level in addition to the pool of trainers trained at Abuja at country levels were
readily tapped into during implementation
6 Conclusion and Recommendations
6.1 Conclusion Even though the performances of this program are mitigated, the presence of USAID consultants at the IST was
crucial to the successes registered. The integration of consultants into the IVD team equally contributed in
reinforcing other IST programs. With the challenge of staff shortages at the IST and country levels, coupled with
competing priorities, providing financial support and technical assistance through consultants can improve
outcomes. In addition, direct collaboration between the team of consultants at the IST, AFRO and head office in
Geneva facilitated analysis and problem-solving.
Even though three countries were able to successfully deploy vaccines in the field, it may be difficult to assess the
emergency preparedness and the rapid deployment capacity of these countries through this program. The
implementation of NDPs intervened after the global alert had relaxed. Three main factors influence rapid
deployment: availability of human and allocation of financial resources, and presence political will.
6.2 Recommendations
USAID: Continue partnership with WHO to provide technical support to health programs through consultants
WHO: In collaboration with USAID, support the elaboration /finalization and implementation of national waste
management plans in countries of the sub-region in order to alleviate the waste management challenges
observed.
Support countries to strengthen AEFI surveillance systems in the sub-region
COUNTRIES:
Maintain H1N1 surveillance and general preventive measures
Organize immunization campaigns before vaccines expire (Cameroon, Angola and Eq. Guinea)
Destroy expired vaccines with destruction reports
Elaborate/finalize and implement national healthcare waste management plans
Strengthen adverse event (AEFI) surveillance systems
Reference:
1. Final Mission Report, Max Mondestin
2. National Deployment Plans
3. Personal experience, trip reports, meetings and other communications
4. Progress and coverage reports, vaccine arrival reports and other documents from countries
5. Resource persons at country level (phone, e-mail etc)

1
Pandemic Influenza A H1N1 (2009),Vaccine
Deployment Activity in East and Southern African
Countries (IST ESA) End of mission report
Abdulquadir Oni and Afework Assefa November 2009 – October 2010
Harare, Zimbabwe

2
Executive summary
Since the confirmation of the first case of the novel Influenza A H1N1 (2009) infection in April 2009, the
intensified surveillance showed rapid transmission of the virus and by June 11 2009 all the scientific and
epidemiologic criteria for a pandemic level were met which led the World Health Organization (WHO) to
declare the beginning of the AH1N1 pandemic.
The global collaboration to mitigate the effect of the emerging pandemic had been extraordinary and
vaccines were licensed for use as early as October 2009. In view of the shortage of vaccines, donor
countries pledged to support the provision of vaccines, technical and financial assistance through WHO to
developing countries to vaccinate 10% of the population. Through this partnership two consultants were
seconded by USAID to support 19 countries in the WHO Eastern and Southern Africa (ESA) sub-region
to review and fast track national deployment plans, give technical advice and training, assess the logistic
capacities and planning before the arrival of vaccines to the countries.
By May 2009 a total of 15,969 confirmed cases and 108 deaths were reported in the sub-region. Of the
18 eligible countries for the donation of vaccines in the sub-region, 17 (with the exception of Uganda)
submitted their National deployment plans and 15 were eventually approved (Eritrea withdrew in the
process and Tanzania did not finalize the plan).
Fifteen countries received the vaccines and implemented/are implementing the vaccination. Uganda,
Tanzania, Eritrea and Mozambique are the four countries which did not receive the vaccines. 9 countries
have completed the vaccination exercise; 4 are still ongoing and 2 will start in November.
Reported coverage from the 9 countries with completed vaccination showed coverage of 66.89% (ranging
from 4% in Mauritius to 83.4% in Kenya and 82.5% in Zimbabwe)
A total of 13,918,890 doses of vaccines were deployed 11,695,300 0.5 ml AD syringes, 358,200 5ml
syringes and 141,150 safety boxes were deployed. The reported operational cost amounted to USD
11,591,338 of which 38.7% were reported contributions from governments.
Oversight of the vaccination in the 6 remaining countries currently conducting the vaccination, termination
reports from all countries and sharing the final report with stake holders are the remaining unfinished
tasks.
Despite negative rumors and controversies it was encouraging to finally see that most countries in the
sub-region vaccinated some of the vulnerable groups.
It is recommended that countries should continue surveillance of influenza due to H1N1 and other viruses
as part of their integrated surveillance system and improve on data recording and reporting including the
vaccination report. The low incidence of severe adverse events following immunization (AEFI) should be
shared with all stake holders.
3
Introduction ........................................................................................................................................................ 5
Objectives and scope of work ......................................................................................................................... 6
Inter country Support Team –Eastern and Southern Africa sub-region (IST ESA) ............................... 6
Background information on influenza A H1N1 (2009) infection in the sub-region ................................ 7
Activities ............................................................................................................................................................. 9
ABUJA WORKSHOP ............................................................................................................................................. 9
VACCINE DEPLOYMENT PLAN ............................................................................................................................ 10
Letter of intent (LOI): .................................................................................................................................. 10
Letter of Agreement (LOA): ....................................................................................................................... 10
National Deployment Plan (NDP): ............................................................................................................ 10
LESSONS LEARNT IN THE DEVELOPMENT OF THE NDP ..................................................................................... 11
IMPLEMENTATION ............................................................................................................................................. 12
Microplans .................................................................................................................................................. 12
Training ....................................................................................................................................................... 12
Brief summary of countries‟ activities in relation to the National deployment plan and vaccination .... 12
Work remaining ................................................................................................................................................ 18
Strengths/Weaknesses ................................................................................................................................... 18
General Coordination (clear understanding of responsibilities): ............................................................. 18
Outcomes of Abuja Meeting: ..................................................................................................................... 18
MOH involvement/coordination: ................................................................................................................ 18
COUNTRIES SPECIFIC STRENGTH/WEAKNESS: .................................................................................................. 19
Strengths: ................................................................................................................................................... 19
Challenges/weaknesses: ........................................................................................................................... 19
WHO COUNTRY LEVEL ..................................................................................................................................... 20
WHO IST LEVEL .............................................................................................................................................. 20
W.H.O/HQ: ..................................................................................................................................................... 20
OTHER PARTNERS (USAID, UNICEF, ETC): ................................................................................................... 21
USAID/Deliver: ........................................................................................................................................... 21
USAID mission: .......................................................................................................................................... 21
Conclusion and recommendations: ............................................................................................................. 22
Acknowledgements: ....................................................................................................................................... 24
Annex 1: Summary of main activities of the consultants for the period ............................................... 24
Annex 2: Summarized H1N1 2009 NDP Profile in ESA/IST Countries .................................................... 28

4
Annex 3 : Summarized Deployed Vaccine and Ancillaries by ESA/IST Countries .............................. 31
Annex 4: Vaccines doses (10 dose vials) by types shipped to 15 countries ........................................ 32
Annex 5: Ancillaries Shipment by Donors .................................................................................................. 32
Annex 6: Summarized Financing Profile of Operational Cost Contributions ....................................... 32
Annex 7: Interim Report of Vaccine Doses Administered ........................................................................ 34
Annex 8: Reported ESA/IST Countries Funding of Essential functions of H1N1 Vaccine NDP ................................ 34

5
Report on Pandemic Influenza A H1N1 (2009),
Vaccine Deployment Activity in IST ESA
7 Introduction
Worldwide, pandemic influenza outbreaks have killed millions of persons in the past. In 2005 there was a Global concern on an impending influenza pandemic and all countries were alerted on this potential global heath problem. On the back ground of this in April 2009, H1N1 was first detected in the United States. This virus was a unique combination of influenza virus genes which was never identified previously in either animals or people. The virus genes were a combination of genes most closely related to North American swine-lineage H1N1 and Eurasian lineage swine-origin H1N1 influenza viruses. Because of this, initial reports referred to the virus as a swine origin influenza virus. However, investigations of initial human cases did not identify exposures to pigs and it became apparent that this new virus was circulating among humans and not among pig herds.
The world Health Organization was monitoring the situation very closely and updating and guiding countries on the measures and steps to mitigate the spread and fatal outcomes. On April 25, 2009, under the rules of the International Health Regulations, the Director-General of WHO declared the 2009 H1N1 outbreak a Public Health Emergency of International Concern and recommended that countries intensify surveillance for unusual outbreaks of influenza-like illness and severe pneumonia.
On April 29, 2009 WHO raised the influenza pandemic alert from phase 4 to phase 5, signaling that a pandemic was imminent, and requested that all countries immediately activate their pandemic preparedness plans and be on high alert for unusual outbreaks of influenza-like illness and severe pneumonia.
On June 11, 2009 WHO raised the pandemic alert to phase 6 indicating a global pandemic as a result of the spread of the virus to more than 2 WHO regions. By then 74 countries had reported more than 74000 confirmed cases.
In view of the possibility of change in severity of illness and anticipation of the worst, the global partnership was intensified with the aim of providing adequate preventive and treatment capacity to countries. As a result of a remarkable partnership vaccines were licensed and made available for public use from October 2009.
Considering the shortage in the supply of vaccines, WHO in collaboration with the united states and other governments and partner agencies pledged to support the effort to stop the global spread of the H1N1 influenza pandemic by providing an amount of vaccine equivalent to 10 percent of their domestic vaccine supply available to assist countries that will not otherwise have direct access to the vaccine through the world health organization.
In the context of the WHO declaration of 2009 Influenza A H1N1 pandemic African countries (including all the 19 countries of the East/Southern African sub-region) agreed to collaborate with WHO and other international partners to reduce the morbidity and mortality of disease. In principle they took national responsibilities for the rapid deployment of the newly developed AH1N1 vaccines to protect prioritized/targeted population (in the absence of sufficient vaccine for the populace) in their respective countries. This was with due consideration of Scientific Advisory Group of Experts‟ recommendations.
As part of this effort to control the spread and impact of influenza A H1N1(2009) pandemic, two consultants were seconded by USAID to WHO office for Southern and Eastern Africa sub region

6
(IST-SEA) to provide technical and programmatic support to countries in the sub region in their preparation, deployment and implementation of vaccination against influenza A H1NI1(2009).
This report summarizes the activities that were carried out from December 2009 to October 2010 by the countries in East and Southern Africa, the support that was provided by IST team, the achievements, the challenges and recommendations
8 Objectives and scope of work
Under the general leadership of the Coordinator of the East and Southern Africa Inter-Country Support Team (ESA/IST), direct supervision of ESA/IST EPI Team leader, general guidance of WHO/AFRO and collaboration with WHO/HQ, the H1N1 team provided technical and programmatic support to 19 countries in the sub-region (through their respective WHO country offices) for H1N1 influenza immunization supply chain activities in general with the following activities:
Review and facilitate approval of the national vaccine deployment plans
Track progress in preparation of country H1N1 vaccination plans and assignment of roles/responsibilities (with contact information) in all countries in the sub-region.
Perform gap analysis in areas of management, organization, human resources, information, storage, transport, and waste management to support deployment of H1N1 vaccine and ancillary equipment.
Provide technical support in training and vaccine logistics for preparation of country plans
Maintain data base of country requests for technical assistance and status in filling requests
Track operational costs requested in country plans and the country channels proposed for receiving and disbursing these external funds.
Track country readiness to receive, store and distribute shipments of vaccines and related equipment and supplies.
Submit interim and termination reports on the status of vaccine deployment
9 Inter country Support Team –Eastern and Southern Africa sub-region (IST ESA)
IST-ESA Is one of the three sub-regional WHO offices under the regional office. The coordinating office is located at Harare, Zimbabwe and supports19 countries in the sub-region. The EPI unit is one of the major departments under the IST coordinator and is led by a unit head with different program supporting officers. The two consultants to support H1N1 vaccination activities were part of the EPI team and were directly working with the staffs in the unit and report to the unit head

7
.
10 Background information on influenza A H1N1 (2009) infection in the sub-region
Following the confirmation of cases of influenza A H1N1 (2009) in other regions, the countries in the sub-region have been reporting confirmed cases of influenza A H1N1 (2009) infections. The number of confirmed cases sharply rose between the end of July to end of September and peaked at around the beginning of October. From then on the number of reported cases
showed a progressive decline as shown in the chart below
Chart 1: The number of confirmed cases reported to WHO regional office from end of June 2009 to end of May 2010
Looking into the number of cases reported from individual countries show that the majority of the cases in the sub-region were reported from South Africa. Out of a total of 15969 cases (as of May 26, 2010)* reported from the region, 12640 (79.2%) were reported from South Africa. The relative advance of the country in terms of laboratory supported case surveillance may
account for the high proportion of the reported cases from South Africa.
010002000300040005000600070008000
Cases
deaths
The countries in the sub-region:
Eritrea, Ethiopia, Kenya, Uganda,
Tanzania, Rwanda. Zambia, Malawi,
Mozambique, Zimbabwe,
Botswana, Namibia, South –
Africa, Swaziland, Lesotho,
Madagascar, Comoros,
Seychelles, and Mauritius

8
The chart below illustrates the cumulative number of cases in the sub-region with the total number of cumulative cases from all countries on the top. It clearly shows that most of the cases were reported from South Africa.
CHART 2: Total cumulative number of reported cases of Influenza A (H1N1) 2009 in countries
from Eastern and Southern African Sub-region from June 2009 to May 2010.
*data source WHO AFRO- weekly update
The breakdown of confirmed cases and deaths by country in the sub-region
Country As of June 29, 2009, As of May 26, 2010,
Cumulative total Cumulative total
Cases Deaths Cases Deaths
Botswana 0 0 23 0
Ethiopia 2 0 19 0
Kenya 1 0 417 0
Lesotho 0 0 65 0
Madagascar 0 0 877 3
Malawi 0 0 4 0
Mauritius 1 0 69 8
Mozambique 0 0 57 2
Namibia 0 0 75 1
Rwanda 0 0 524 0
Seychelles 0 0 33 0
South Africa 7 0 12640 93
Swaziland 0 0 2 0
Tanzania 0 0 770 1
Uganda 0 0 263 0
Zambia 0 0 90 0
Zimbabwe 0 0 41 0
TOTAL 11 0 15969 108
The pandemic remained largely mild in terms of mortality. The total number of reported deaths due to influenza A H1N1(2009) in the sub-region as of end of May 2010 was 108 giving a
02000400060008000
1000012000140001600018000
Botswana
Ethiopia
Kenya
Lesotho
Madagascar
Malawi
Mauritius1
Mozambique
Namibia

9
mortality rate of 0.7%. Most deaths (86.1%) were also reported from South Africa but even then
the mortality rate was 0.73%.
In general the reported confirmed cases (and deaths) from many of the countries may be a gross underestimation and may not reflect the actual number of cases. This may be related to the weak surveillance and reporting system, the mild nature of most infections, the lack of
laboratory facilities to confirm suspected cases.
11 Activities
11.1 Abuja workshop
A training workshop was organized by WHO regional office in collaboration with WHO head quarters. The main purpose of the workshop was to bring focal points on EPI and epidemic preparedness from ministries of health and WHO country offices to draw up plans for the deployment of a pandemic influenza vaccine. The vaccine deployment plan is to be part of the pandemic preparedness plan of each country.
All countries from the sub-region (except Comoros which could not make it due to flight problems) participated in the workshop through EPI and/or Epidemic/surveillance unit personnel. Focal points from WHO country offices also participated in the workshop.
At the end of the workshop almost all countries in the sub-region submitted a first draft of vaccine deployment plan. However the plans needed finalization and it was agreed that countries will finalize and submit the plans to respective IST offices in 2 weeks following the workshop.
The workshop was very important and timely to give emphasis, review and update the pandemic preparedness plan in general and the vaccine deployment plan in particular.
However some participants were not the focal points or were not available to follow and finalize the deployment plan upon return to their countries. This was further complicated by shifting responsibilities to epidemic preparedness/ surveillance departments to finalize the plan in some countries.
It will be good to emphasize on the utilization of the existing ministry structure and committees and build up on previous experience in responding to outbreaks with mass vaccination (measles, polio…). Practically in most countries the personnel, equipment and logistic system was the same to that of other mass vaccination.
The logistic tool was a very good introduction but a bit complex for many participants to make use of it. It will be worth if the training on it gets repeated in other EPI meetings.
The recommendation not to include wastage factor in the calculation of vaccine requirement did not sunk well into participants and became one of the controversial issues during the screening and approval
The workshop did not discuss well on the modalities of funding. Some countries assumed all funding will come with the donation and were not showing or putting effort to get funding from the respective governments.

10
11.2 Vaccine deployment plan
Letter of intent (LOI): one of the requirements by member countries to get the donated
vaccines was to officially write a letter of intent to the Director General of WHO confirming the country‟s need to protect the most vulnerable. In this regard all the 19 countries in the sub-region submitted the letter of intent and most of them in the first few weeks after the Abuja workshop.
Letter of Agreement (LOA): All the countries in the sub-region with the exception of Uganda
and Mozambique submitted a letter of agreement countersigned by the Ministers of Health (or their delegates). This was one of the prerequisites to receive the financial and material support and outlines all the procedures and legal concerns in case of liability. In the sub-region, some countries went ahead and submitted their deployment plan before submitting the LOA on the assumption that the letter will ultimately be signed by the highest official in the ministry. However, it was mandatory that the letter of agreement be submitted for the country to receive the donations even if the plan was done and approved. In the case of Mozambique for example the plan was approved at all levels and implementation was supposed to follow; but due to failure in signing the LOA the donations and financial support could not be provided for the country.
National Deployment Plan (NDP): during the course of the Abuja workshop all countries
developed a draft deployment plan. The status of the draft plans vary from country to country. Some of the factors that were observed to negatively affect the development of the plan include
Some of the participants‟ did not have some important facts and data.
Some were not confident in what they should plan for and had to consult their supervisors by phone
There was some confusion and reluctance in taking responsibility between the EPI managers and the disease prevention/ surveillance officers.
In general, the draft plans were grossly incomplete with the logistic/distribution, finance and budget and timeline being some of the major sticking points. It was therefore agreed that countries will be further working on the plan and officially submit to WHO-IST offices within the two weeks of the completion the workshop.
However the plans were not submitted in the two weeks because of various reasons
Some of the participants in Abuja on return to their country were not able to continue work as a team and bring on partners together to finalize the plan
Other competing priorities- like outbreaks cholera (Kenya), Measles in Southern Africa
The funding component and getting pledges from partners was not easy for many countries
Christmas and new year break which unfortunately coincided with the planned period, might also have contributed because of the fact that many partner agencies and personnel were not available for consultation
Of the 19 countries in the sub-region 14 officially submitted the National deployment plan between January and June, 2009.
Kenya was in the group A countries which were prioritized to receive the vaccines earlier than others. Hence a team from the consultants was on ground to support the country in finalizing the vaccine deployment plan in December and early January. It was the first country to submit the
11
plan and get the approval after some amendments to the initial plan following reviewers comment both at the regional and HQ level.
The delay in submitting the national deployment plan was raised as an issue and discussed in the ESA/IST EPI meetings 2010, Maputo Mozambique (10 -12) March 2010 where all sub region countries were in attendance. Side meeting discussions and agreement were held with specific countries‟ current situation and way forward. These countries were Botswana, Comoros, Ethiopia, Madagascar, Malawi, Mauritius, Namibia, RSA, Seychelles, Tanzania, Mozambique, Lesotho, Uganda, Zambia & Zimbabwe,
Following the meeting and further follow-ups, countries submitted the NDP which was reviewed at IST level and forwarded to the regional office after feedbacks were accommodated. General review of NDP was based on the 8 essential elements of viable deployment plan but with specific focus on the defined target population of prioritized group, vaccination strategy to reach them and illustrated budget elaboration (2 tranches of 2 and 8 %) for deployment at all level of activities.
Funding proposals were also discussed, reviewed and finalized. The plans came in phases, 14 countries‟ plan were reviewed and approved before June 30 while plans from Comoros, Rwanda and Zambia were reviewed and approved at the IST after June 30. Uganda and South Africa did not submit their NDP officially,
11.3 Lessons learnt in the development of the NDP
The team which participated in Abuja workshop was not available for the finalization of the planning- “other priorities”
There was no clarity in who is going to take the leadership- between the EPI team and the disease prevention department
Involvement of partners at country level was minimal and was very difficult to get their support in funding some of the activities
There were negative rumors about the pandemic and the vaccine. Though their effect at that stage were minimal, there was less enthusiasm and interest from some partner agencies and personnel to be fully engaged
Countries submitted the NDP much later than the anticipated period. Uganda and Tanzania are the only two countries which did not submit the plan officially. Eritrea withdrew its interest but had submitted the national deployment plan.
Most countries followed the SAGE recommendations on prioritizing high risk groups. But few countries (Botswana, South Africa, Mauritius, Rwanda) had wanted more vaccines for other groups as well. The strategies on how to reach these groups were not well depicted in some of the plans.
Almost all countries had to revise their plan (including the budget) to clearly show the two phases of deployment - the initial 2% and the remaining 8% because most have lumped the 10% request altogether.
The logistic plan was not very clear as to whether there will be a need for surging the cold chain storage capacity or not
Communication and information aspect including its funding was not given due emphasis in some of the plans

12
Post marketing surveillance was also not as emphasized as one would expect during introduction of a new vaccine
11.4 Implementation
Microplans were developed by countries using the existing national EPI planning capacities
and mechanism of planning for supplementary immunization. Due consideration was given to the priority groups for H1N1 vaccination, vaccine surge delivery approach to impact on the distribution plans and relative capacities at service delivery levels. Guidelines and tools were shared with countries for consideration, adaptation/adoption to facilitate all the related activities of H1N1 vaccine deployment. The WHO official logistic tool was used to support countries lacking logistics skills, and validate countries plans in conjunction of the verification of the budgeted activities in the 8 essential deployment elements. Countries distribution plans were verified on country support visit and attuned with countries‟ peculiar situations
Training was conducted in all the 15 countries which participated in the vaccination
exercise.13 countries adopted a cascaded training of trainers approach while South Africa and Swaziland trained all their supervisors and vaccinators at selected locations in their respective countries. The IST team supported 15 participating countries with the training of their respective health workers prior to deployment efforts with emphasis on epidemiology of the disease, vaccine handling, interpersonal communication and side effects/AEFI monitoring and reporting. The facilitation was provided directly or through remote support of training of national trainers supervisors. Directly supported countries include Botswana, Kenya, Malawi, Namibia, Swaziland, South Africa and Zimbabwe. In countries where direct support was not provided, training manuals, agenda, power-point presentation and publications were shared with country teams.
11.4.1 Brief summary of countries’ activities in relation to the National
deployment plan and vaccination
(Refer to annexes 2-6 for details)
BOTSWANA:
Submitted 1st draft on: April 19, 2009
Finalized and approved at IST: May 13, 2009
Major issues in the plan:
The country showed interest to vaccinate the entire population and was ready to purchase the doses vaccines outside the 10% donation
The budget needed clarification on whether it was for 10% or for the planned 100%
The planned procurement of 214,800 AD syringe was grossly inadequate to meet 90% extra population targeted.
Overall reconciliation of the excel figures with the narrative plan figures in the vaccination strategies was redone with the team during the H1N1 vaccine deployment training support mission to Gaborone Botswana.
Training was conducted on three different sessions and venues from May 18-20 for national officers (TOT) and the remaining two days for District health officers
The training was supported by IST consultants

13
Implementation: The H1N1 vaccination was conducted in 5 phases beginning early June targeting all residents of Botswana
Support provided: Several telephone calls and e mail support on the development and finalizing the NDP
Two missions to Botswana were made by IST consultants to support the country team on ground: one on planning and assessing the logistic needs (one week) and the other on training and microplanning (5 days)
COMOROS
Submitted 1st draft on: March 22 (it was initially sent to HQ)
Finalized and approved at IST: July 8, 2010
Major issues in the plan:
After the first draft a feedback was given on March 24 to the country team on some of the important issues but there was a long delay in accommodating some of the important points and hence the delay in the final approval. There were no delegates from Comoros in Abuja and this may have contributed to the fact that the initial plan did not follow the general format and was lacking specificity on selection of priority groups, the details of transportation and cost for ancillary equipment was not estimated
Details of supply and cold chain, legal issues, communication and waste management were missing and operational cost was not separated into the 2 tranches of 2% and 8% by activities with the contribution of the government and partners.
Implementation: ongoing- vaccines arrived August 29, 2010
Support provided: remotely by e mail and telephone calls
ETHIOPIA
Submitted 1st draft on: February 15, 2010
Finalized and approved at IST: March 20
Major issues in the plan: the contribution of government and other partners in funding the costs
Training: conducted in 1st week of July
Implementation: started on 13th of July in the capital and is now completed in Addis but is still ongoing in other regions
Support provided: review of the plan, feedback through e mails and telephone, training materials
Data on coverage: currently only from 4 regions available- 40.7%
ERITREA
Submitted 1st draft on: February 5 (was actually sent on 13th of January but was not traced until February 5. The country withdrew its application and letter of intent by a letter of withdrawal written to WHO –HQ on February 8 (dated January 19). Hence the country was removed from the tracking list of countries.
KENYA

14
Submitted 1st draft on: 14 January 2010
Finalized and approved at IST: 15 January 2010
Major issues in the plan: The plan was developed for the first phase only 2% and did not show
the government and other partner contribution in funding
Training: was conducted from April 17
Implementation: started April 21, 2010
Support provided: 2 missions to Kenya were made. One in the initial development of the plan
and the second during implementation
Data on coverage: 83.4%
LESHOTHO
Submitted 1st draft on: January 15, 2010
Finalized and approved at IST:
Major issues in the plan: Estimation of pregnant women, budget clearly
Training: 20 May 2010
Implementation: starting from end of May-(May 28)
Support provided: through teleconferences and e- mails
Data on coverage: 81.1%
MADAGASCAR:
Submitted 1st draft on: 16 Feb, 2010
First review and feedback by IST: 22 February 2010
Finalized and approved at IST:
Major issues in the plan:
The priority groups and the order of implementation was not clearly indicated and the initial plan did not show the two phases (2% and 8%) clearly
The contribution of government and partners in funding some of the activities
Training: 23rd August
Implementation: started September 6 – major issue for delay was difficulty of sourcing a long
expiry date vaccine to meet the whole shipment requirement for Madagascar. Proposed short dated vaccine was rejected
Support provided: remotely through telephone and e mail
Data on coverage to date: 40.4%
MALAWI
Submitted 1st draft on: February 25

15
First review and feedback by IST:: 1st March 2010
Finalized and approved at IST:
Major issues in the plan: an underestimate of pregnant women, funding from other sources
Training: Sept 6-13
Implementation: vaccination to be conducted beginning the first week in October. It was delayed because of a measles outbreak which was prioritized over the H1N1 vaccination
Support provided: Mission on ground for 10 days to support the planning and logistic aspect
Data on coverage:
MAURITIUS
Submitted 1st draft on: May 12 (but country had purchased vaccines by its own and had started
vaccination of high risk group by the time it submitted the NDP
First review and feedback by IST::May 14
Finalized and approved at IST: May 14
Major issues in the plan: reconciliation of the budget figures on the vaccination strategies and AEFI sections with those on the summarized budget
Implementation: is still going on
Support provided: review of the plan, feedback, training materials, slides
Data on coverage: MOZAMBIQUE
The country had gone through all the processes for approval of the deployment plan- submitted Letter of Intent and the National deployment plan. The plan was reviewed and approved. However it did not progress to signing/submitting the letter of agreement and hence the vaccination exercise did not take place NAMIBIA
Submitted 1st draft on: January 29, 2010 (the Abuja draft plan)
First review and feedback by IST: Feb 4, 2010
Finalized and approved at IST:
Major issues in the plan: estimate of pregnant women; specific strategies to reach the target
population, legal issue, budget and gap in funding
Training: April 22 at central level and from April 25-27 to district officers Implementation
Support provided: several feedback and exchange of e mails on the plan; a mission to the country from April 20-28 to support training and updating the microplan
Data on coverage: 84%
RWANDA

16
Submitted 1st draft on: Rwanda shifted from IST central to ESA after it had submitted the plan to
IST Central and AFRO
First review and feedback by IST: June 23
Finalized and approved at IST: July 5, 2010
Major issues in the plan: vaccination strategies, budget
Training: ongoing
Implementation: is ongoing
Support provided: reviewing and updating the plan, sharing training materials
Data on coverage:
SEYCHELLES
Submitted 1st draft on: April 15
First review and feedback by IST: April 16
Finalized and approved at IST: April 18
Major issues in the plan: estimation of pregnant women; budget for transporting, capacity to receive 10% was not confirmed in the initial plan
Training: June 2-4
Implementation: From June 11, 2010
Support provided: Generic resource materials/tools were shared, policies issues/concerns were clarified
Data on coverage to date: 37% SOUTH AFRICA
Though the country was not in the initial list of countries to be supported, special arrangement was made by WHO HQ and the government to support South Africa due to the FIFA World cup 2010.
Though the country did not submit LOI, LOA and NDP to IST, a request for technical support was made and the two IST consultants have made a mission to support the planning and preparedness before receiving the vaccines.
Country received 3.5 million doses of vaccines in addition to the ones purchased by the government. It had conducted vaccination since April but no report have been received.
SWAZILAND
Submitted 1st draft on: March 5
First review and feedback by IST: March 17
Finalized and approved at IST: March 31, 2010

17
Major issues in the plan: The country was planning for 40% of its population while the donation
was only for 10%. Cold chain capacity in the districts were limited
Training: conducted from June 1-4
Implementation: vaccination started on June 4
Support provided: in addition to the review and feedbacks on the plan, a mission to the country
was made to support the training
TANZANIA
Though an attempt was made to get engaged with the country team several times through reviewing the initial draft plan, there was no response from the country and hence the deployment plan could not be realized
UGANDA
Though delegates from Uganda participated in Abuja and there was a letter of intent from the country, the national deployment plan was never submitted officially. Repeated attempts to reactivate the process failed .
ZAMBIA
The draft plan prepared in Abuja was reviewed and feedback given to the country in April to reactivate the process. An updated version was submitted on May 23:
Finalized and approved at IST: July 9, 2010
Major issues in the plan: the target figures were not very clear, budget for all activities were not well delineated
Training:
Implementation: on going
Support provided: several exchange of e mails and telephone conversations with the country team to reconcile data and assumptions
Data on coverage: ZIMBABWE
The Abuja draft plan was reviewed and feedback given in March but the country was facing a huge measles outbreak and attention was diverted
Finalized and approved at IST: April 3
Major issues in the plan: strategies on how to select school children and distribution of vaccines
Training: July 22-25 Implementation: Delayed response to MCAZ (NRA) requirements for donated new vaccines and delayed supply of AD syringes
Support provided: In addition to the reviews and feedback on the plans, supported the training in Harare and Bulawayo for all provincial trainees
Data on coverage – 82%

18
12 Work remaining
Of participating countries with completion of deployment only Kenya and Zimbabwe provided viable summary reports of the deployment exercise. The remaining 6 countries with completion of the vaccination exercise (Botswana, Lesotho, Mauritius, Namibia, Seychelles and Swaziland) are yet to provide official termination report but provided somewhat interim report.
The remaining 7 participating countries are either with ongoing vaccination (Ethiopia, Madagascar and South Africa) or are yet to commence (Comoros, Malawi, Rwanda & Zambia) at the time of the finalization of this report.
Given the poor country feedback (in spite the persistent follow up) attempt at quantitative data analysis of outcomes was difficult and may not reflect the actual realities at country levels.
13 Strengths/Weaknesses
General Coordination (clear understanding of responsibilities): Most of the 19
member representatives were ably represented at the Abuja meeting (except Rwanda who later joined the IST sub region and comoros). However, some countries‟ representatives were not necessarily part of the team members working on the NDP in their respective countries (e.g. Kenya and South Africa)
In some countries apparent delay of take off were observed with reluctance by the EPI program to own the leadership and kick start the planning and implementation process. Examples of the countries include Kenya, Botswana and Namibia. However with the IST level interventions, the national health authorities in these countries corrected the situation and joint planning and coordination through constituted national committee commenced.
Outcomes of Abuja Meeting: December deadline for NDP submission was met only
by Kenya out of 19 countries the rest were late and 3 were very late.
Countries were well aware about the essential components, strategies, context of SAGE prioritization, financing options and regulatory issues for surge deployment of the H1N1 vaccines. However refresher meetings and pre vaccinators training had to be conducted to update knowledge obtained at the Abuja training
General awareness of H1N1 vaccines novel nature made health workers/authorities to be wary of its potential side-effects, curious of communication strategies with stakeholders and to have mixed feeling of hope/doubt of its demand uptake by target population
MOH involvement/coordination: The ministries of Health owned the deployment
effort in all the 19 countries signing the LOI and 18 countries signing the LOA. Funding ownership was however very poor (see annex 5 for details).
Botswana initially planned for self procurement of vaccines but later on negotiated and obtained 1.6million doses to vaccinate its entire population.
Swaziland established a budget line of R 14million for vaccination of target population before full collaboration with W.H.O. commenced. However IST efforts to convince the GOS to reprogram this budget in support of delivery efforts and eventually strengthen the routine programme proved abortive.

19
South Africa self procured 1.1million doses of vaccines (before securing additional 3.5million doses of H1N1 vaccines in anticipation of the FIFA 2010 through a separate negotiating mechanism with W.H.O.)
Countries vaccine financing contributions to operational cost were below average with only Botswana, Mauritius, and South Africa with full responsibilities of their respective operational cost. Available data indicate that major part of the operational cost in most countries were financed by W.H.O. and with some support from USAID (for in country vaccine and ancillary deliveries) in some prioritized countries
Health workers perception: varies from in deferent countries. This ranges from poor
demand in Botswana to high uptake in Zimbabwe
13.1 Countries Specific strength/weakness:
13.1.1 Strengths:
High motivation for deployment efforts in Southern African countries
Existence of identified focal points at country levels (WCOs and national committee) for follow ups
Existing EPI structure and system used as H1N1 vaccine delivery mechanism
Ownership (substantial government contribution) of deployment efforts in several Southern Africa countries: Some of these include health workers mobilization (all participating countries), inter-sectoral collaboration (BOT, MAL, NAM, ZIM, SOA) high level advocacy all participating countries)
The national drug regulatory authorities reviewed materials on vaccine safety in almost all countries
Previous experiences on SIAs have a remarkable positive contribution on the planning, implementation and waste management
FIFA 2010 world cup in South Africa further enhanced the country‟s motivation on the deployment effort requesting additional 3.5 million doses donation from W.H.O.
13.1.2 Challenges/weaknesses:
Countries competing priorities delayed (e.g. measles outbreak in all participating countries except Kenya where there was a cholera outbreak, though small scale).
New vaccine requires new experience documentation (regulatory, inclusion in AEFI monitoring system, other programmatic issues e.g. vaccine handling policies).
Bureaucratic administrative issues at country levels slowed/delayed deployment operational issues. Lead time of review/approval lengthens as delays are experienced from country levels
Full donor dependency of most countries limits participating countries ownership of the deployment process
Prevailing poor planning capacities in some countries (with no national logistician) hampered the planning process in some countries (Botswana, Lesotho, Namibia & Zambia).

20
Confirmation of cold chain adequacy for 2%, 8% or 10% in some countries was challenging due to the limited capacity available to assess existing cold chain capacities (e.g. Botswana and Lesotho).
Decentralization (Central medial store handling of vaccine distribution) in some countries (e.g. Namibia & Botswana) hampered monitoring/quality assurance of distribution procedure
Letter of agreement requirements/conditions (absolving manufacturers, WHO and countries taking full responsibilities) delayed response time of some countries to the deployment process.
NRAs requirements delayed some countries involvement in the deployment process (e.g. Zimbabwe required for the summary lot protocol before licensing waiver could be given and insisted that cohort event monitoring be part of the activities to be implemented during vaccination). In Kenya the vaccination of pregnant women was put on hold because the information from the manufacturers stated that it has no information on safety in that group.
Social mobilization and communication activities were planned and budgeted for in most countries. However these activities were poorly implemented in almost all countries due to inability to provide robust target mobilization to the targeted population.
13.2 WHO country level
Existence of country offices in all participating countries gave a closer support hand to the deployment process. In all countries (participating and non participating) the country offices were pivotal to communication, facilitation, training, implementation and termination in the respective countries
Indeed WCO was the lead agency in the deployment process in all 14 participating countries. The process was led by the country in SOA
WCOs in Namibia, Seychelles, and Kenya made additional local financial contributions to the national operational cost of their respective countries.
13.3 WHO IST level
IST coordinator, EPI team leader and the whole EPI team were generally involved with deployment exercise with update shared at EPI monthly meeting and administrative backup support provided (access to the electronic share drive, internal communication loop & facilitation of country mission trips)
Existing ESA/IST EPI administrative & infrastructural support system/protocol were exploited to support all participating countries
Existing countries‟ acceptability of W.H.O. global leadership on health issues
13.4 W.H.O/HQ:
Provided/developed deployment guidelines, training support, vaccine/ancillary shipments with manufacturers, allocated funding (in the context of the developed/approved national deployment plan and other resource materials for the facilitation of the deployment process at country levels via the regional and IST
Provided global reference to countries needs e.g. Kenya‟s concern on possible contraindication of Fluvirin in pregnancy (and under 4 yrs) clarified in reference to SAGE position and recommendations of prioritizing pregnant women and safety

21
Frequent direct communication with countries excluding the IST (letter of agreement, vaccine delivery dates, funding support to countries) created some communication/operational gaps initially but later rectified. Examples are its direct communication with Rwanda, direct negotiation with SOA (for 3.5million doses), direct negotiation with Botswana to immunize total population and change of its vaccine type with no communication with the IST
Generated minor/uncomfortable controversy by suggesting short dated vaccine to some countries (e.g. Madagascar and Rwanda refusal of some short dated vaccines) in attempts to ensure a single vaccine type shipment to countries)
Protracted international controversy generated by Council of Europe impacted negatively on some countries demand and may have been responsible for the withdrawal of Eritrea, poor motivation of Mozambique and no follow up by Tanzania and Uganda
Delayed release of vaccine to countries de-motivates country teams for the deployment exercise e.g. Kenya
WHO/HQ last minute changes on vaccine type and delivery dates poses operational and regulatory challenges in recipient countries
Early release of funds (at least 2 weeks prior to vaccine shipment would have facilitated activities like training and microplanning to be conducted before the arrival of the vaccines.
13.5 Other Partners (USAID, UNICEF, etc):
Visible/tangible presence of partners in most countries to provide complementary support (e.g. funds disbursement management by JSI in Kenya, MCHIP support on supervision and monitoring activities in Kenya, USAID support in Namibia and Malawi, UNICEF support of social mobilization in Malawi etc)
Provision of countries funding support to bridge gaps of specific line items e.g. USAID for in-country supply chain
Partners‟ support of W.H.O. in funding technical assistance to countries via the IST (secondment of an epidemiologist and a logistician)
USAID and UNICEF facilitation at the Abuja workshop
Vaccine manufacturers technical and operational back up of implementation through vaccine shipment and release of licensing dossiers to countries NRAs
USAID/Deliver: Supported in-country vaccines distribution in prioritized vaccines
through developed/validated funding plans in a number of countries. These are Ethiopia, Kenya, Malawi, Namibia and Swaziland?.
Provided/funded the ancillaries supply in Ethiopia, Kenya, Lesotho, Malawi, Namibia, Rwanda and Swaziland
USAID mission: Although most of the local missions expressed readiness to support
the efforts in their respective countries their support were limited to those provided and initiated by USAID/Deliver. The missions in Kenya and Namibia made a notable interest and contribution to the campaign
Coordinated support by DELIVER/JSI from planning stage was reported in Malawi, Kenya, Ethiopia and Swaziland. Planned support in Zimbabwe was suspended due to prevailing country‟s relationship with the U.S government.

22
Other Partner‟s involvement: The support of CDC-Kenya (coverage survey in Kenya), MCHIP- Kenya (supervision) UNICEF (communication in Malawi), AED-US (communication in Kenya) and JSI (in country vaccine deployment in Namibai) were reported. Level of partners involvement varies from country to country based on advocacy efforts of the respective national committees as defined in their respective national deployment plans. (Summary details of established partnership is illustrated in annex 4 and 5)
14 Conclusion and recommendations:
By the time the vaccines were deployed in most of the countries, there was a decline in the number of reported cases worldwide and because of this the activity period was marred by many controversies and negative rumors. Nevertheless, 16 of the 19 countries went through all the processes to deploy Pandemic Influenza A H1N1 (2009) vaccines. High risk groups were prioritized and vaccinated in these countries with no report of major/serious advent events. However there are lessons to be learnt from this exercise for future similar scenarios and we would like to make the following recommendations:
To Countries:
1. Although the Abuja training workshop was well conducted within the shortest time permitted, some countries‟ representatives with hands on responsibility of NDP finalization appears not to be well represented at the workshop (e.g. Kenya, South Africa are 2 case in point). Defined clear terms of reference of participants (e.g. known focal points responsible for accelerated vaccination) should be complied with by countries. This is a crucial step in the planning process and could define the success of the deployment process.
2. Clear country leadership should be defined and the national health authority to avoid ambiguity and delay as observed in some countries (Botswana, Zimbabwe) with hesitation to lead the process. It took the intervention of the Director of Public Health (at the instance of the IST H1N1 focal point team) before rapid progress could be observed in the finalization of the planning stage in a country.
3. Country ownership of the deployment process should be negotiated right from the outset e.g. as part of the legal agreement by W.H.O. and partners. This could be in terms of operational cost contribution to ensure commitment throughout the process of deployment. The withdrawal of 4 countries after massive investment in training would thus be discouraged in future.
4. Delays experienced in some countries (e.g. Zimbabwe) due to regulatory demand for summary protocol and the need to add additional function (cohort event monitoring) should be negotiated in advance between the countries and their respective NRAs to avoid unnecessary delay and concern by stakeholders to the surge deployment effort recommended for the pandemic situation
5. The level of inter-sectoral collaboration was not adequate in almost all participating countries with partners limited to only WHO, UNICEF and USAID. Given the experience of these countries in supplemental immunization activities, adequate communication to all immunization & disease control partners, ministry of education, transport, finance etc potentials to optimize all potentials stakeholders‟ comparative advantage.
6. Although national committees for the deployment effort were strong and well coordinated at the national levels but this strength and organization were observed to diminish downwards toward the peripheral levels. Future participating countries national committees should ensure duplication of strength of the committees at peripheral levels to enhance compliance with the deployment guidelines

23
7. Peripheral levels should be involved in the development of district microplan for vaccination efforts to ensure viability of the deployment effort within the specified time of 7 days. In most countries a macroplan adaptation was used for the deployment effort
8. Given the passive approach of most developing countries to emergencies, (pandemics inclusive) active integrated surveillance of the AH1N12009 virus should be continuous in all countries in addition to the recommended incorporation of H1N1 vaccination with the seasonal flu vaccine in countries with existing in seasonal flu vaccination (e.g. South Africa) as a trivalent vaccine.
9. Countries are encouraged to use post pandemic vaccine balance for non prioritized populations provided expiry dates still permits with full notification of their respective NRAs (where applicable).
To W.H.O.:
10. Financing support and deployment to countries should be sent at least 2 weeks in advance (by W.H.O. and partners) to facilitate pre vaccination preparation such as social mobilization, training and tools developments
11. Frequent vaccine type changes experienced in countries should be avoided at worst communicated in advance to countries to facilitate and fast track regulatory issues and training implications of such changes.
12. Delays in ancillary deployment to countries experienced in Zimbabwe, Malawi, Botswana, and Namibia should be communicated in advance in future for quick options identification by countries
13. Apparent differences in countries technical, infrastructural and systemic capacities should be taken into consideration at the strategies developmental stage to ensure favorable endpoints. Absence of national and W.H.O. logistician in Botswana, Namibia, South Africa and Zambia, constituted major challenge to the pace of planning and implementation in these countries. In addition the decentralization of vaccine distribution in Botswana, Namibia (with the Central Medical Store) being the main entity responsible for distribution but without being involved in the training, planning and implementation could not assure the vaccine handling quality assurance of delivered vaccine. Adequate viable strategies should be made to support such countries right at the training/planning stage
14. Countries sole legal responsibilities for the deployment of the new vaccines caused some concerns in some countries (e.g. Uganda). If stakeholders‟ consensus on the terms of the legal instrument cannot be jointly agreed before finalization at least advance notification of countries should be ensured before finalization. This ensures involvement in the terms of agreement by all countries in taking full responsibilities of the deployment process.
15. All the training/resource materials were found to be very simple and practical. However some of them need to be updated for consistency of information and standards (e.g. national training manual on the MDVP compared with the WHO MDVP recommendations
16. The level of social mobilization activities for the mobilization of the new vaccines was observed to be inadequate in almost all the participating countries. Given the apparent inexperience of countries in targeted mobilization, a section of the workshop should be dedicated to mainly to enhance country capabilities in this effort.
17. While there is enough feedback and responses at HQ levels to the international controversy generated by council of Europe, continuous information and active collaboration with the media, from outset and throughout the implementation process at all levels (HQ, AFRO, IST and country) would have made a major difference to the protracted controversy.

24
18. The AEFI profile from most countries indicated high vaccine tolerance with reported low rate of severe AEFI incidence similar to what was obtainable to seasonal flu vaccines. The positive outcome should be documented (from feedback survey) and shared with all stakeholders as evidence of the safety and high tolerance of the vaccine for future reference.
19. Countries‟ feedback had been very poor with delay in response and limited information in most of the feedbacks in spite of a simplified version to facilitate the feedbacks. Traditional reporting channels for SIAs in countries may be explored for possible improvement.
20. IST mission support to countries would be strengthened and fast tracked through provision of UNLP as some delay were experienced due to visa requirements during implementation period
21. Consideration should be given to identification of a focal point to oversee deployment completion by the remaining countries (COM, ETH, MAD, MAL, RWD & ZAM) and consolidate the outstanding reports with this summary as part of the regional level report.
15 Acknowledgements:
We would like to thank the IST coordinator Dr O. Walker, the EPI team leader Dr. N. Shivute and all EPI team members for their guidance and support throughout our stay. We would also like to extend our gratitude to USAID for funding our activities and supporting the travel arrangements to the countries.
16 Annex 1: Summary of main activities of the consultants for the period
Workshop/Meetings Participation in the sub-region:
o Participated/facilitated at the AH1N1 training workshop in Abuja Nigeria 23 - 27
November 2009 for 20 English speaking countries (Botswana, Ethiopia, Eritrea,
Gambia, Ghana, Kenya, Lesotho, Liberia, Malawi, Namibia, Nigeria, Sierra
Leone, Seychelles, South Africa, Swaziland, Zambia and Zimbabwe) in the
African region.
o Participated and facilitated at the ESA/IST EPI meetings 2010, Maputo
Mozambique (10 -12) March 2010 (Trip report available on request)
o Participated at Regional H1N1 vaccine deployment monthly teleconference
o Participated at National H1N1 committee meetings of Botswana, Malawi,
Namibia, Rep South Africa, Zimbabwe
Support of training of national trainers supervisors in most IST H1N1 vaccine
deployment participating countries
Supported member countries to develop district micro-plans, training plans/agenda, tools
for monitoring and supervision for the deployment effort
Tracked countries feedback on signed Letters of Intent (LOI), Letters of Agreement
(LOA) and order planning forms
Reviewed, feedback follow up (with participating countries) and approved national
deployment plans (NDPs) and forward to AFRO for consideration/approval to the next
level (WHO/HQ)
25
Provided direct/remote support to country preparedness: Commodity specifications, cold
storage needs, tracking/Distribution, training etc
Developed funding proposals with USAID prioritized countries in context of USAID H1N1
funding focus with countries and shared with USIAD/DELIVER-TO2 for consideration.
Submitted monthly activity report to the USAID, ESA/IST, and WHO/AFRO for
orientation
Handled emanating issues, concerns, queries, resistance and policies from countries to
facilitate the deployment exercise at all levels of deployment
Performed other assigned tasks by the ESA/IST management, USAID/JSI and WHO
(AFRO & HQ) as designated
Submitted a final ESA/IST summary report of H1N1 2009 vaccine deployment to
ESA/IST, WHO/AFRO and USAID/JSI.
IST situational reports of major activities pertaining H1N1 vaccine deployment was
discussed with key observation and interventions at the monthly Regional
teleconference
All implementing countries were provided with tracking support of vaccine and ancillary
shipments, national regulatory authority (NRA) registration waiver, in country
receipt/clearance and finance deployment/disbursement (including Mozambique that
later lost interest in the deployment process)
In concert with the WHO H1N1 country focal points and within the context of the
approved National Deployment plans of USAID prioritized countries, funding proposals
were developed and shared with USAID/Deliver project for its consideration. The summary
of the financial costs and funding sources is shown in Annex 5
Monthly situational and activity update were shared with USAID/Deliver project, the
ESA/IST team leader, the ESA/IST coordinator and the WHO/AFRO H1N1 coordinating
unit. The situation update is illustrated in annex 1
Country trip reports, generic training manuals, pre-vaccination/in process supervisory
tools, Q/A for journalists, MDVP policies, generic communication materials, opt out form,
and post pandemic Q/A were shared with all stakeholders in the deployment process.
Copies of these are attached.
Estimation of pregnant women population as part of the prioritized group were either
over or underestimated. UNFPA population baseline assumption was used to resolve
and provide a common baseline for all implementing countries.
Countries with policy on parental consent for targeted children were provided with
generic „opt out‟ policy for their possible adoption and in use in their respective
deployment exercise. This was applicable in Seychelles and South Africa
Supposedly contraindication of „Fluvirin‟ in pregnancy led to initial exclusion of pregnant
women from the prioritized group but later included after close discussion with national

26
authorities on the SAGE position and recommendation on all H1N1 vaccine. Indeed this
had a negative impact on the overall uptake of the vaccine by this target group in Kenya.
Sudden change of vaccine type from the scheduled type (after or during training
exercise) in more than one country (e.g. Botswana, Madagascar, Mozambique,
Zimbabwe) posed
programmatic challenges (during and after training) necessitating addressing formative
supervision during implementation (in post training countries)
regulatory challenges by the NRA of the countries in question as registration waiver is
often specific for the filed type of vaccine for which application is sought leading to
shipment delay (e.g. Rwanda and Zimbabwe).
Deployed H1N1 vaccine types to countries with target age group of 6 months - 3years as
part of the prioritized group requires 0.25ml administration in 2 doses spaced at least 3
weeks apart. Hence pediatric AD syringe were needed for administration. Since
countries were not provided pediatric AD syringe they had to source locally (e.g.
Botswana Sanofi non adjuvanted vaccine)
Local and international issues on the H1N1 vaccines safety, pandemic status, were
tackled and addressed in local context, but with reference to global experience/situation.
Some of these include the raised issue of contraindication of Fluvirin in pregnancy
(clarified with SAGE recommendations), international controversy on the need for
vaccination (clarified with historical perspective of influenza pandemics), safety of H1N1
vaccines (clarified with safety profile of seasonal influenza vaccine with same production
mechanism) etc
The council of Europe protracted controversy (questioning the authenticity of WHO
AH1N1 pandemic declaration) may have influenced the withdrawal of Eritrea (after NDP
submission, signing of LOI and LOA), inaction of Mozambique (after NDP approval and
receipt of WHO support funds), Tanzania and Uganda (after submission of draft of their
respective NDP).
Countries were encouraged to use post pandemic vaccine balance for non prioritized
populations provided expiry dates still permits with full notification of their respective
NRAs (where applicable).
Expired short dated vaccines were encouraged to be destroyed at local levels in the
context of countries‟ prevailing waste management guidelines and disposal.
Supported the IST country members in logistics preparation of Measles campaign on
same mission support to countries with H1N1 deployment efforts (e.g. Malawi and
Republic of South Africa)
Developed the concept note and logical frame work for the deployment project at the
instance of the IST coordinator to guide the mechanism and schedules of activities
within the sub region

27
Followed up of participating countries contribution to the IST summary/termination report
met with very poor response. Interim report template to facilitate feedback was shared
with all participating countries. However feedbacks were provided only by Botswana,
Ethiopia, Kenya, Lesotho, Mauritius, Madagascar, Namibia, Swaziland and Zimbabwe.
Of these only Kenya and Zimbabwe reports were informative enough. The rest have
several missing elements yet to be furnished.

28
17 Annex 2: Summarized H1N1 2009 NDP Profile in ESA/IST Countries
Countries 1st Date of
NDP
Submission
Last Date
of
Submission
of NDP
approved
version
Observed
Strength/weakness in
NDP
General Comments
on NDP
Interim/Termination
reports status
Botswana
JAN_2010 MAY_2010
Plan for 100% total
population; Budget
clarification for 10 or
100%; 5 months for 1st
draft correction
Challenge of
planning capacity,
No National
logistician; Pledge of
100% funding of
operational cost was
not redeemed hence
surge strategy was
compromised, op
cost about
USD1.0/dose
No termination
report nor interim
report submitted in
spite of several
follow ups
Comoros
MAR_2010 MAY_2010
Fully donor dependent;
No budget for AEFI &
waste management;
Need to reconcile total
target population
Late submission of
revised budget
beyond the deadline;
operational cost
about USD 0.8/dose
Yet to commence
vaccination exercise
(planned for
October)
Eritrea NDP submitted but followed with a formal withdrawal from deployment exercise
Ethiopia
MAR_2010 MAR_2010
All essential elements
attended to except for
minor issues on human
resource,
communications and
surveillance for AEFI
A well written plan
but no funding
support from the
government
Preliminary report
indicated that all
vaccines had been
distributed;
vaccination started
in 4 of 7 regions;
interim coverage of
47%
Kenya
DEC_2009 DEC_2009
Complied with all
essential functions; No
GOK funding
commitment
Only country that
met the deadline of
Dec 2009 for NDP
submission
Terminal report
submitted with
national coverage of
83.4%
Lesotho
DEC_2009 MAR_2010
Duplication of
appropriate committees
at provincial and district
level were well
articulated in plans; No
details of cold chain
adequacy.
Operational cost of
about USD
0.712/dose;
Submitted interim
report indicated
coverage of 74.8%;
details of
Government and
other partners
funding contribution
missing
Madagascar
FEB_2010 MAY_2010
Target population
redefined; Few errors of
addition in plan; Source
of available funds not
specified as separate
summary;
No government
contribution
Commenced
vaccination exercise
(Sept); interim report
indicate 45.5% for
Health worker and
pregnant women
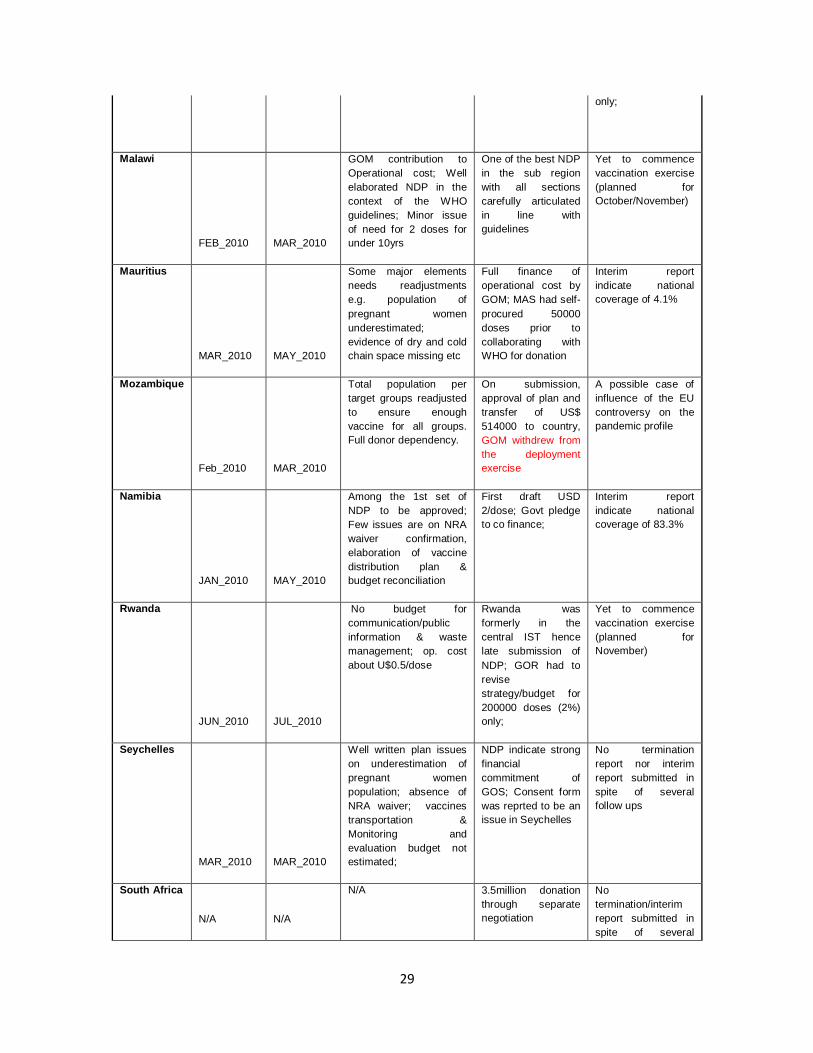
29
only;
Malawi
FEB_2010 MAR_2010
GOM contribution to
Operational cost; Well
elaborated NDP in the
context of the WHO
guidelines; Minor issue
of need for 2 doses for
under 10yrs
One of the best NDP
in the sub region
with all sections
carefully articulated
in line with
guidelines
Yet to commence
vaccination exercise
(planned for
October/November)
Mauritius
MAR_2010 MAY_2010
Some major elements
needs readjustments
e.g. population of
pregnant women
underestimated;
evidence of dry and cold
chain space missing etc
Full finance of
operational cost by
GOM; MAS had self-
procured 50000
doses prior to
collaborating with
WHO for donation
Interim report
indicate national
coverage of 4.1%
Mozambique
Feb_2010 MAR_2010
Total population per
target groups readjusted
to ensure enough
vaccine for all groups.
Full donor dependency.
On submission,
approval of plan and
transfer of US$
514000 to country,
GOM withdrew from
the deployment
exercise
A possible case of
influence of the EU
controversy on the
pandemic profile
Namibia
JAN_2010 MAY_2010
Among the 1st set of
NDP to be approved;
Few issues are on NRA
waiver confirmation,
elaboration of vaccine
distribution plan &
budget reconciliation
First draft USD
2/dose; Govt pledge
to co finance;
Interim report
indicate national
coverage of 83.3%
Rwanda
JUN_2010 JUL_2010
No budget for
communication/public
information & waste
management; op. cost
about U$0.5/dose
Rwanda was
formerly in the
central IST hence
late submission of
NDP; GOR had to
revise
strategy/budget for
200000 doses (2%)
only;
Yet to commence
vaccination exercise
(planned for
November)
Seychelles
MAR_2010 MAR_2010
Well written plan issues
on underestimation of
pregnant women
population; absence of
NRA waiver; vaccines
transportation &
Monitoring and
evaluation budget not
estimated;
NDP indicate strong
financial
commitment of
GOS; Consent form
was reprted to be an
issue in Seychelles
No termination
report nor interim
report submitted in
spite of several
follow ups
South Africa
N/A N/A
N/A 3.5million donation
through separate
negotiation
No
termination/interim
report submitted in
spite of several

30
follow ups
Swaziland
MAR_2010
Separation planned govt
procurement from
donation from plan,
confirmation of NRA
approval, Details of
intersectoral
collaboration, distribution
plan were missing, Cold
chain capacity at
provincial level was a
challenge;
NDP elaborate GOS
intention of self
procurement of up to
41.5% total
population and
finance the
additional cost of
operational
Interim report
indicate a coverage
of 21.1%;
Termination report
yet to be submitted
Tanzania
These two countries did not conclude the NDP submission/approval process
Uganda
Zambia
FEB_2010 JUL_2010
Target population for
phase II & III missing;
Details of cold chain
adequacy missing;
Details on the budget
missing; (Management &
coordination); Initial op
cost >US$1/dose;
NDP planed to take care
of waste management
and AEFI within normal
routine system.
NDP was not in
recommended
format; was
submitted beyond
the deadline and
vaccination planned
for post pandemic
period; Operational
cost per dose is
estimated at USD
0.9_(USD206, 964
for 230,000 doses);
Yet to commence
vaccination exercise
(planned for
November)
Zimbabwe
JAN_2010 MAY_2010
Vaccination strategies,
priority groups target
populations
reconciliation, budget
summary are the key
issues on the NDP
NDP could not be
finalized on time
because of massive
measles outbreak
and the deployment
of the EPI staff to
contained the
outbreak
Interim report
indicate 79.4%;
Termination report
yet to be submitted

31
18 Annex 3 : Summarized Deployed Vaccine and Ancillaries by ESA/IST
Countries
Countries Shipp
ed
Vaccin
e Qty
(by
HQ)
receiv
ed in
countr
y
Source of
Vaccine/
Type
Vol/
dose
Cm3
Vaccine arrival date
versus date expected
(March)
Quantity:
AD
Syringes
(0.5mL)
Quantity:
RUP
Syringes
(5mL)
(with
Pandemr
ix only)
Quantit
y:
Safety
Boxes
Ancillaries
Donor
Botswana 16128
00
Sanofi
France
non
adjuvante
d
(Panenza)
5.2 Jun-19 1695200 n/a 22000 WHO
Comoros 65000 CSL
Panvax
3.4 Aug-29 68900 n/a 825 WHO
Eritrea Officially withdrew from deployment effort
Ethiopia 30000
00
GSK
Pandemri
x
5.7 June 313200 3151200 39850 USAID
Kenya 73000
0
Norvatis
Fluvirin
Mar-24 768000 n/a 8850 USAID
Lesotho 19500
0
Panvax 3.4 May-07 163200 n/a 1900 WHO/USAI
D
Madagascar 10560
90
Sanofi US 5.2 Aug-20 2145600 n/a 24675 WHO
Malawi 13000
00
Sanofi US 5.2 0.3million (Jun19) 1million
(Aug)
1051200 n/a 12100 USAID
Mauritius 32700
0
Panenza 5.2 127000 (June); 200000
(August)
134400 n/a 1550 WHO
Mozambique Discontinue follow up for deployment efforts
Namibia 216000 Pandemr
ix
5.7 cm3 May-10 228000 23400 2900 USAID
Rwanda 200000 Pandemr
ix
5.7 cm3 Sep-10 211200 21600 2575 USAID
Seychelles 9000 Panvax 3.4 cm3 Apr-10 9600 n/a 125 WHO
South Africa 358420
0
Sanofi
US
5.2cm3 May-10 n/a n/a n/a n/a
Swaziland 117000 Panvax 3.4 cm3 Jun-10 98400 n/a 1125 WHO/USAI
D
Tanzania Country did not progress on deployment process
Uganda Country did not progress on deployment process
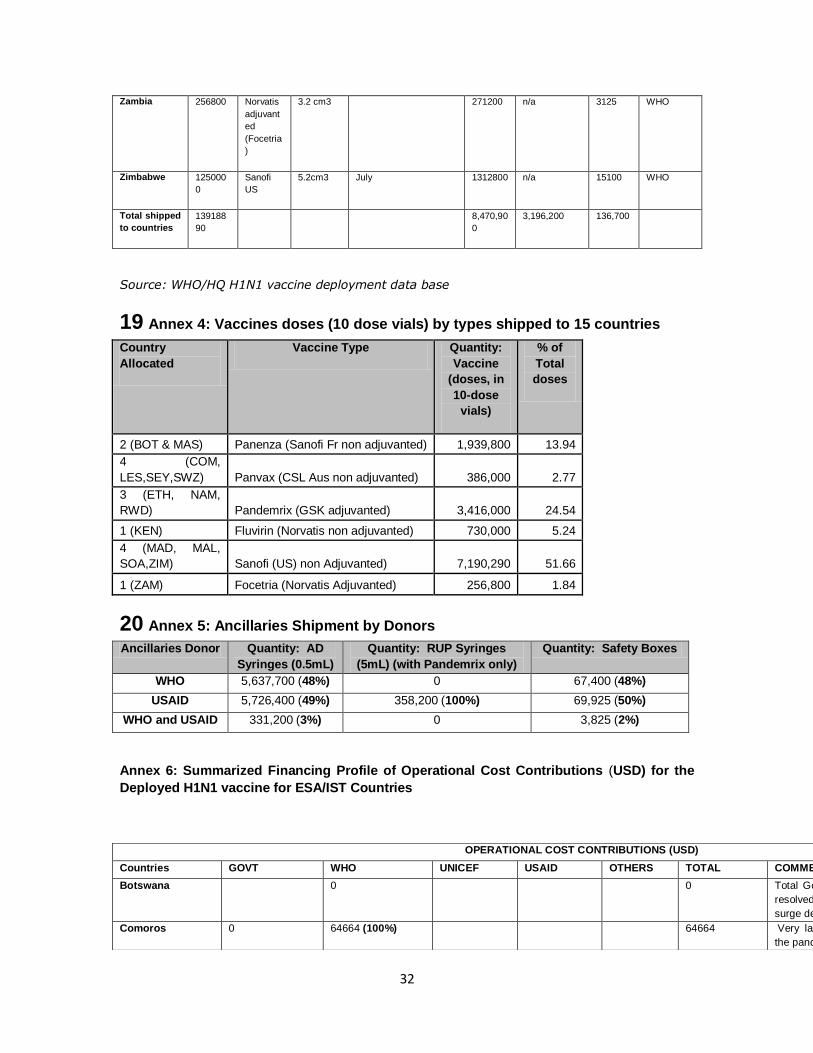
32
Zambia 256800 Norvatis
adjuvant
ed
(Focetria
)
3.2 cm3 271200 n/a 3125 WHO
Zimbabwe 125000
0
Sanofi
US
5.2cm3 July 1312800 n/a 15100 WHO
Total shipped
to countries
139188
90
8,470,90
0
3,196,200 136,700
Source: WHO/HQ H1N1 vaccine deployment data base
19 Annex 4: Vaccines doses (10 dose vials) by types shipped to 15 countries
Country
Allocated
Vaccine Type Quantity:
Vaccine
(doses, in
10-dose
vials)
% of
Total
doses
2 (BOT & MAS) Panenza (Sanofi Fr non adjuvanted) 1,939,800 13.94
4 (COM,
LES,SEY,SWZ) Panvax (CSL Aus non adjuvanted) 386,000 2.77
3 (ETH, NAM,
RWD) Pandemrix (GSK adjuvanted) 3,416,000 24.54
1 (KEN) Fluvirin (Norvatis non adjuvanted) 730,000 5.24
4 (MAD, MAL,
SOA,ZIM) Sanofi (US) non Adjuvanted) 7,190,290 51.66
1 (ZAM) Focetria (Norvatis Adjuvanted) 256,800 1.84
20 Annex 5: Ancillaries Shipment by Donors
Ancillaries Donor Quantity: AD
Syringes (0.5mL)
Quantity: RUP Syringes
(5mL) (with Pandemrix only)
Quantity: Safety Boxes
WHO 5,637,700 (48%) 0 67,400 (48%)
USAID 5,726,400 (49%) 358,200 (100%) 69,925 (50%)
WHO and USAID 331,200 (3%) 0 3,825 (2%)
Annex 6: Summarized Financing Profile of Operational Cost Contributions (USD) for the
Deployed H1N1 vaccine for ESA/IST Countries
OPERATIONAL COST CONTRIBUTIONS (USD)
Countries GOVT WHO UNICEF USAID OTHERS TOTAL COMMENTS
Botswana 0 0 Total Govt pledge could not be redeemed; deployment
resolved to health facility delivery without the proposed
surge delivery strategy
Comoros 0 64664 (100%) 64664 Very late submission of NDP deployment well beyonf
the pandemic period

33
Sources: Countries H1N1 vaccine deployment interim reports and WHO/HQ funds transfer
correspondence
Eritrea 0 0 0 0 0 0 Withdrew
Ethiopia 0 3000000 (93.52%) 207742
(6.48%)
3207742 Regionally phased rollout from Addis Ababa to others.
Deployment beyond the pandemic period
Kenya 107914 (23.83%) 143000
(31.58%)
201864
(44.58%)
452778 Delayed release of funds and vaccine to country;
Lesotho 0 128090 (100%) 128090 WHQ fully funded financial gaps (USD128090), little
support from GOL for training of health workers; UNICEF
pledged could not be accessed because govt
bureaucratic process
Madagascar 768887 (100%) 768887 Budget of US$ 768,887 approved and transferred to
MAD; Only about a million doses could be deployed due
to short date of the required balance.
Malawi 15000 (1.74%) 621000 (72.22%) 223646
(26.02%)
859646 Vaccine deployment beyond the pandemic period due to
response to measles outbreak;
Mauritius 51830 (100%) 51830 Fully funded operational cost aside from the self
procured 50,000 doses prior to WHO donation of 327000
doses
Mozambique Country did not progress on deployment process
Namibia 2025789 (91.4%) 170000 (7.67%) 20000
(0.9%)
2215789 First phase of deployment exercise was integrated with
NID hence Government contribution is inclusive of its
support during this phase
Rwanda 163404 (100%) 163404 Deployment and vaccination well beyond the pandemic
period,; Late submission of plan and presidential election
in country contributed to delay in deployment
Seychelles 13367.6 (21.6%)
7,860 (12.7%) 40794 (65.8) 62021.59
South Africa 0 RSOA fully responsible for all operational cost; Disposal
syringe is till the policy of choice in country;
Swaziland 2376083 (93.4%) 168759 (6.63%) 2544842 Initial Govt established budget line for H1N1
(R14million) was not used and could not be
reprogrammed for strategic cold chain support of the
programme
Tanzania Country did not progress on deployment process
Uganda Country did not progress on deployment process
Zambia 206964 (100%) 206964
Zimbabwe 804080 (100%) 804080 Total sum received in 2 phases from WHO/HQ (USD 698,080;
USD 106,000 (for in-country delivery
GRAND TOTAL 4482070 6211672 203550 633252 60794 11591338
% Total
contribution 38.7 53.6 1.8 5.5 0.5 100
# Countries
contributed to
5 12 2 3 2 GOVT: MAL, NAM, SEY, SWZ; WHO: ALL except BOT, MAS &
SOA; UNICEF:KEN; USAID: ETH, KEN & MAL; OTHERS (CDC):
NAM
% of countries
contributed to
33.33 80.00 13.3 20 13.33

34
Annex 7: Interim Report of Vaccine Doses Administered with Coverage by Countries
BOT COM ETH KEN LES MAD MAL MAS NAM RWD SEY SOA SWZ ZAM ZIM TOTAL
Vaccine doses shipped (10-dose vials) 1612800 65000 3000000 730000 195000 1056090 1300000 327000 216000 200000 9000 3584200 117000 256800 1250000 13918890
Vaccine doses deployed in country 6900 6900
Health workers Vaccinated 8314 16645 3968 16000 819 7482 87513 140741
Target health workers 52697 15000 15526 1000 15500 55000 154723
%HW Coverage 31.59 26.45 103.05 81.90 48.27 159.11 90.96
Pregnant Women vaccinated 7011 173066 766 24149 262 4846 36776 246876
Target Pregnant Women 416856 36000 42505 400 19036 150080 664877
%Coverage Pregnant Women 41.52 2.13 56.81 65.50 25.46 24.50 37.13
Persons with chronic medical condition vaccinated 61332 719 41255 810 9810 200707 314633
Target Person with chronic medical condition 73000 40000 3711 70138 69920 256769
% Coverage PCMC 0.98 103.14 21.83 13.99 287.05 122.54
Others vaccinated 15595 55207 0 706777 777579
Target of Others 65970 0 975000 1040970
% coverage Others 83.69 72.49 74.70
Total vaccine doses administered 0 0 0 609344 92252 189711 0 5453 136611 0 1891 0 22138 0 1031773 2248197
Total Target 0 0 0 730720 123300 469553 0 124000 164001 0 5111 0 104674 0 1250000 3360989
%Overall Coverage 83.39 74.82 40.40 4.40 83.30 37.00 21.15 82.54 66.89
Source: Interim report from countries
21 Annex 8: Reported ESA/IST Countries Funding of Essential functions of H1N1
Vaccine NDP
Countries
Vaccination
Strategies
Management
and
Organization
Communication
and Information
Human
resource
and security
Public
Information
Supply and
Cold Chain
Waste
Management
Post
marketing
Surveillance Evaluation Total
Botswana 0
Comoros 0
Eritrea
0
Ethiopia 0
Kenya 2700 19147 19000 150659 117333 50405 800 30000 31920 421964

35
Lesotho 0 27855 3660 53735 0 10033 154 0 0 95437
Madagascar 145343 2689 12637 31766 40530 41105 4940 0 4527 283539
Malawi 0
Mauritius 14175 8418 572 4209 20202 30 4242 505 0 52353
Mozambique 0
Namibia 145500 38800 55300 172000 6000 135772 0 0 20000 573372
Rwanda 0
Seychelles 41761 3565 6522 2727 6498 0 395 158 395 62022
South Africa 0
Swaziland 14593 7485 4242 19030 7749 425641 5566 278 0 484584
Tanzania 0
Uganda 0
Zambia 0
Zimbabwe 200100 0 100000 154000 0 181960 15000 20500 0 671560
Total 564172 107958 201933 588127 198312 844947 31098 51442 56843 2644831
% 21.33 4.08 7.63 22.24 7.50 31.95 1.18 1.94 2.15 100.00
Source: Submitted interim reports of ESA/IST Countries. NB: These are the available figures

36

37
END OF ASSIGNMENT REPORT ON H1N1 VACCINE
DEPLOYMENT AND UTILIZATION ACTIVITIES
Dr Patrick BYARUHANGA Jean NGANTCHOU
October 2010

38
Table of contents Page
Introduction ………………………………………………………………………………………… 3
Epidemiologic situation of H1N1 prior to vaccine deployment activities.. 4
West Africa Map…………………………………………………………………………………… 4
Epidemic preparedness and response to H1N1 pandemic ……………………. 5
Abuja H1N1 workshop ………………………………………………………………………… 5
Vaccine deployment plan ……………………………………………………………………. 6
Funding vaccine deployment activities in IST member countries ………….. 8
Implementation ………………………………………………………………………………… 10
Results ……………………………………………………………………………………………. 15
Challenges of assignments ……………………………………………………………….. 19
Evaluation activities ………………………………………………………………………….. 22
Conclusion and recommendations ………………………………………………… 22
Word of appreciation ……………………………………………………………………… 23

39
1 Introduction The WHO IST sub region comprises of 17 countries with a total population of approximately 340,867,787.
The countries of the sub region include: Algeria, Benin, Burkina Faso, Cape Verde, Cote D’Ivoire, Gambia,
Ghana, Guinea Bissau, Guinea Conakry, Liberia, Mali, Mauritania, Niger, Nigeria, Sierra Leone, Senegal,
and Togo. All the countries in the sub region with the exception of Algeria were eligible for the WHO
H1N1 vaccine donation. The WHO IST West sub region therefore was expected to plan to immunize about
31 million people; the equivalence of 10% of the total population of all eligible countries in the sub region.
This report is a brief on the steps followed to deploy and utilize WHO donations of H1N1 vaccines to
countries of the WHO IST West sub region.
1.1 Epidemiologic situation of H1N1 prior to vaccine deployment activities On 15th and 17th April 2009 novel swine influenza virus A H1N1 was identified in two epidemiologically
unlinked patients in the USA. The same strain was identified in Mexico, Canada and elsewhere as the
cause of outbreaks of influenza infections. The rapid human to human spread of the outbreak across
countries and continents led to WHO declaration of H1N1 pandemic.
West African countries were not spared of this epidemic. Table 1 below shows the cases and deaths due to H1N1 prior to H1N1 vaccine deployment activities. Table 1 Cumulative cases of H1N1 in WHO IST West sub region
Country Cumulative H1N1 (as 7th Dec 2009)
Cases Deaths
Algeria 276 3
Cape Verde 62 0
Cote D'Ivoire 3 0
Ghana 52 0
Nigeria 2 0
Total 395 3
By the end of November 2009 the sub region had recorded a total of 395 H1N1 cases and three deaths in
5 countries (see table 1 above). All evidence was pointing to a rising number of cases with more countries
reporting new cases.
By May 23, 2010 10 countries had reported 2,192 cases and 56 deaths due to H1N1 pandemic. See table 2
below. Ghana is reported to have continued to report H1N1 activity up to August 2010.

40
Figure 1 Map of West Africa showing H1N1 cases and deaths by May 23, 2010
Key: Numbers in black= H1N1 cases; in red deaths due to H1N1 infection By the end of November 2009 the sub region had recorded a total of 395 H1N1 cases and three deaths in 5 countries (see table 1 above). All evidence was pointing to a rising number of cases with more countries reporting new cases. By May 23, 2010 10 countries had reported 2,192 cases and 56 deaths due to H1N1 pandemic. See table 2
below. Ghana is reported to have continued to report H1N1 activity up to August 2010.
Table 2 cumulative cases of H1N1 in IST West as of May 2010
Country Cumulative H1N1 (as 23rd May 2010)
Cases Deaths
Algeria 916 54
Cape Verde 118 0
Cote D'Ivoire 30 0
Ghana 720 0
Guinea Conakry 3 0
Mauritania 15 0
Niger 49 0
Nigeria 11 2
Senegal 325 0
Togo* 5 0
Total 2,192 56
Togo* cases not on WHO website list

41
1.2 Epidemic preparedness and response to H1N1 pandemic The rapid spread of the disease and the severity of the condition caused some panic among populations
and countries had to intervene very fast to allay fears caused by this new pandemic.
Countries, with support from partners, developed epidemic preparedness response plans to the
pandemic. The plans included the clinical identification (signs and symptoms); laboratory
diagnosis/confirmation, the curative component (anti viral drugs) and the health information and public
awareness on how to prevent H1N1 infection. Countries that were financially able to afford the cost of
vaccines like Algeria bought them and vaccinated their populations. However the majority could not and it
is such countries that benefited from the donation of vaccines and operational costs from WHO, USAID
and other partners.
2. Abuja H1N1 Workshop Since H1N1 was a new pandemic with new vaccines being developed, it was necessary to call countries for
an orientation on H1N1 pandemic updates and also on how to develop country vaccine deployment and
utilization plans.
2.1 Trainees Trainees were selected by respective governments and included WHO country IVD focal points/DPC and
government Ministry of Health staff responsible for immunization and control epidemics.
Some of the staff selected as government representatives unfortunately did not participate in the
development of the NDPs on returning home.
2.2 Training workshop This was a 5 days’ workshop held in a serene environment suitable for serious work
2.2.1 Workshop components and effectiveness Considering the four objectives of the workshop; they were all met and the workshop was successful.
The workshop had the necessary and experienced experts who performed their tasks well
2.2.2 Workshop materials The workshop materials and tools were sufficient and appropriate.
2.2.3 Suggestions for future workshops Like in most workshops, a lot of information was availed to participants and this tended to stretch the
workshop time to beyond the usual working hours.
In future facilitators should work within the allocated time by minimizing introduction of
other topics though relevant but may not be directly related to the theme of the
workshop
In some countries participants selected to attend the Abuja workshop would not participate in the
development of country deployment plans. Others selected had different assignments that were
considered important and urgent.
Care should be exercised when selecting participants. Countries should be guided on the
process of selection of their staff so that only committed workers, who will be available,
can attend.

42
3. Vaccine deployment plan
3.1 Letters of intent and of agreement.
o These are documents that were supposed to have been written or signed prior
to Abuja workshop. They were countries’ expression of willingness and
commitment to accept and use the vaccines. Most countries had responded
except a few that needed reminding to sign letters of agreement. Francophone
countries generally wished that they had been sent the letters of agreement
written in French. In the end all 16 countries signed the LOI and all except Mali
and Benin signed the LOA.
3.2 Status of NDP at IST.
o Although it was assumed that countries would have developed their NDPs up to
almost completion before they left Abuja workshop, this was not the case. In IST
West it had been planned that Togo would be the first followed by Nigeria in
submission of the plan and implementation however by end of December 2009
no NDP plan had been submitted for IST to review. Togo invited H1N1
consultants to support the country to finalize their NDP and by mid January
2010 their plan was ready and submitted. All
countries submitted their NDPs late and the reasons for late submission were
many but included competing programs like NIDS, the task was time consuming
and staff to develop the plans were busy with other activities. In some countries
the people who attended Abuja workshop had abandoned the task.
o In IST West all 16 countries developed NDP. However 15 NDPs were approved. Cape Verde NDP was sent back to the country for them to develop a plan to cover the entire population 6months and above. The country did not do as advised and was assumed to have lost interest in the donation of H1N1 vaccines.
3.3 The level of technical support that was needed in member countries
o Apart from Togo, Mali and Senegal the rest of the countries were supported by
remote mechanisms that included phone calls and internet. The remote
process followed when at the IST level the plans submitted by the countries
were found to be unclear or generally wanting. This process had limitations. It
required that the Country WHO focal point was available on phone and internet
and had a good working relationship with the government (Ministry of Health)
staff as some suggested changes had to be approved by the government.
3.3.1Technical support, effectiveness, Problems and Solutions
o Technical support followed the country's request to IST for support. The consultant upon arrival arranged a meeting of all stakeholders to review and workout modalities to complete the deployment plans using the knowledge and skills acquired from Abuja workshop and from previous

43
plans that had been approved. Problems arose if the country team had hidden interests in the plan or if the team involved was new to the task; in countries where those who attended the Abuja workshop had abandoned the exercise. More time would be spent explaining the whole process from the rationale for selection of target population and all other aspects of the plan write up. Once basic concepts were explained the planning process was easier to accomplish. Approval at IST was faster when the consultants were directly involved in the development of the plan.
3.3.2 Challenges encountered and suggested solutions:
o Most countries didn’t request for support and the remote support to such
countries was often slow because the focal points were in the field engaged in
other programs.
o Controversial areas in the deployment plans included the inclusion in the NDPs
of irrelevant activities and also overpricing certain activities and items. It took
some time to convince countries to adjust accordingly
o Some countries were reluctant to give a breakdown of the cost of activities
preferring to allocate large sums of money along each activity without any
justification. Some persuasion was necessary to get the corporation of the
countries
3.3.3 Support from WHO Regional and Headquarter Office
o The constant pressure for NDPs from the RO and HQ was also transmitted to
countries and this helped in hastening the process of developing and finalizing
NDPs. The HQ and RO supported by providing updates on H1N1 and vaccines
and documents like training materials.
o Teleconferences and daily updates helped consultants to share information and
to appreciate what is going on in other sub regions.
3.4 General observations and lessons learnt from each country during planning and
approval process including the adequacy of the check list
o Although it was an emergency activity countries that had not seen any case
were slow at developing their plans. Those that had seen many cases were
initially active in developing the plans but as time passed and the cases started
to reduce, they also become relaxed and reluctant to develop their deployment
plans. Some withdrew altogether. This demonstrates the importance of
intervening at optimum times.
o Countries where the country WHO IVD focal persons and government EPI
managers were responsible for H1N1 NDPs, the process of developing the plans
was faster and easier to follow up at IST level. Similarly implementation
(vaccination campaign) was also better organized.
o Approval of NDPs at IST was not entirely dependent on the screening approval
tool. Other issues of plans being feasible/doable were also put into

44
consideration at IST level. Repetition of activities and costing them twice were
some of the observations made at IST level for correction by the countries.
o Generally the checklist was a good guiding tool to assist in approval of the NDPs.
3.5 Experiences of countries pertaining to plan components enabling and hindrances
other key issues of relevancy to document in each component.
o The components formed a good basis for NDP development and most of the
countries followed them step by step
o Communication and information was understandably often confused with
public information
o Under supply of cold chain, some countries had hoped to improve on their cold
chain capacity by procuring cold chain equipment but were disappointed to
learn that the emergency exercise couldn’t cater for heavy developmental costs.
o Few countries included evaluation as an activity in their NDPs.
It is important to note that some countries made very nice plans that were duly
approved. However when it came to implementation some aspects of the above
components were not implemented as planned. This was observed mainly in the
following components: management and organization, public information or social
mobilization, and waste management.
4 Funding vaccine deployment activities in IST member countries
4.1 Resource mobilization
o All countries in this region, with the exception of Niger, indicated in their plans
that H1N1 NDP was a new activity that had not been included in their National
budgets and didn’t make much effort to fund it. In this sub region only Togo
received funding from partners-UNDP.
o Countries that were among the first to submit NDPs had their budgets
scrutinized more than those that sent theirs later on when WHO had increased
funding for deployment activities. This had the effect of delaying the planning
process at country level as the countries were advised to review their budgets
downwards.
4.2 Budget allocation patterns
o Most countries allocated a lot of money (more than expected) for management
and organization, supply chain processes, waste management and post
marketing surveillance. After some discussions and guidance from IST the
allocations were appropriately adjusted.
o The bulk of funding came from partners: WHO and USAID
Table 3 Funding of H1N1 deployment and utilization

45
Operational costs
Vaccine shipment
Syringes and other ancillaries
Vaccine and ancillaries distribution
Comments
Funding (USD)
Partner
Funding (USD)
Partner
Funding (USD) Partner
Funding (USD) Partner
Country
Benin -
Burkina
Faso
971,790 WHO Not available 267,569
USAID/DELIVER
Included in the O.F.
Cape Verde
-
Côte
d'Ivoire
988,054 WHO Not available 303,312
USAID/DELIVER
Included in the O.F.
Gambia 140,132 WHO
Not available
Not available
Included in the O.F.
Ghana
1,058,000 WHO Not available 61,900
USAID/DELIVER 102,900
USAID/DELEVER
Guinea 425,986 WHO
Not available
Not available
Included in the O.F.
Guinea-
Bissau
243,012 WHO Not available
Not available
Included in the O.F.
Liberia 109,200 WHO
Not available 15,239
USAID/DELIVER
Included in the O.F.
Mali
- Included in the O.F.
Mauritania
200,578 WHO
Not available
Not available
Included in the O.F.
Niger 454,804 WHO
Not available
Not available
Included in the O.F.
Nigeria 1,000,000 WHO
Not available
Not available
Included in the O.F.
Senegal 376,823 WHO
Not available 31,100
USAID/DELIVER 67,336
USAID/DELEVER
Sierra Leone
396,159 WHO
Not available
Not available
Included in the O.F.
Togo 358,200 WHO
Not available 122,891
USAID/DELIVER 55,456
USAID/DELEVER
TOTAL
6,722,738
802,011
225,692 O.F.: Operational fund
5 Implementation
5.1.1 Training, Micro Planning and Pre-Campaign Activities
Micro planning:
Micro-planning as an activity has been a weak link before the campaign itself. Indeed
the deployment plans of countries were simply the outcomes of Abuja’s workshops. The
compilation of needs was made at the central level with very few information about the
real problems of the operational level. In all sub-region countries, the campaign of
vaccination against influenza was not part of the activities planned and budgeted for the
year 2009-2010. The pandemic has been declared, the need for a vaccination campaign
against influenza A (H1N1) failed as an emergency. The Abuja’s workshops were

46
organized in order to standardize deployment plans. Our expectation was to see every
country to organize a micro-planning session. Unfortunately lack of time and resources,
this operation could not take place, and it is for these reasons that deployment plans
were realized at the central level, contrary to the rationale that the activities would be
designed at the operational level. It is important to remember that wherever the
activities were developed at the central level, the WHO country office has been obliged
to finance few workshop days in order to allow the EPI staff to develop the plans.
This deviation from the development of micro-plans was responsible for not taking into
the consideration specificities of some health facilities (distance, number of teams,
number of syringes compared to children who were to receive only a half-dose).
We hope that the micro-planning will often retain the attention of policymakers on
funding and timing of implementation.
Training:
In all countries of the region involved in vaccination against influenza A (H1N1), training
was effective at central, regional and district level. But after the training of health unit’s
responsible, the cascade didn’t continue in order to allow other contributors of these
centers, to be at the same level of information. This deficiency was felt in the use of vials
or management of interpersonal communication.
We have noted in some countries visited that the delay between training day at central
level and commencement of immunization activities was so short that the cascade
training couldn’t be good. It is also important to recall that among the training tools
were missing in our view the local name of the flu that could have facilitated the
dissemination of messages in the local language.
As training tools, efforts have been made at the IST to gather all the tools developed by
WHO, DELIVER, AED or Manufacturers to make them available to all countries willing to
switch to the active phase of vaccination.
Training of journalist by AED Training of Central Facilitators

47
5.1.2 Vaccination Campaign
Human Resources Mobilization in Countries:
Following their different plans, countries anticipate to mobilize vaccinators, supervisors,
drivers, relays and few agents. They were respectively in charge of vaccinating the
populations, supervising the teams during activities, mobilizing the targets, selecting
those who are concerned and incinerating safety boxes. Their number depends on the
target population at the area and the intensity of the job.
Social Mobilization and Launching Ceremony:
Social mobilization is essential for the success of a mass campaign. From the success of
its implementation depends the density of the queue during the implementation, even
the goals of vaccination. During the first phase of vaccination in Togo, as during the
implementation in Ghana, this fact has been neglected, and the results were not
conclusive. But during the second phase still in Togo, all aspects of mobilization have
been integrated and good the results followed.
People tend to evaluate every movement of the Administrative Authorities, and their
attendance or not at official launch of the campaign demonstrates the seriousness and
the height they give to the activity. In Togo, Mauritania, Sierra Leone, Ministers of
Health together with partners (WHO, UNICEF) have personally launched the activities of
vaccination against influenza A (H1N1). The actual attendance have boosted some
skeptics, and helped to improve attendance. By contrast in a country like Ghana, where
there has been no official launch by the authorities, attendance has taken a hit, and the
rumors could only increase. Vaccination of authorities before the national television can
convince people that the vaccine they are offered has nothing harmful. Opposite to
what is claimed in newspapers or Internet.

48
Poster for the campaign People rushing after a radio announcement
WRs being vaccinated during lunching ceremonies
Supervision and Monitoring of Campaign Activities
Among the fifteen countries which submitted their plans for approval, thirteen
definitely signed letters of agreement and received funds and vaccines to organize
vaccination against H1N1. By the middle of October 2010, eleven of them have already
vaccinated.
The strategy developed for the vaccination by most of countries consisted on mobilizing
fixed teams in health units; and depending on countries’ policy, either fixed teams were
also mobilized in private units, or mobile teams were designated to cover these units.
During the campaign, IST team supported technically five countries (Ghana, Mauritania,
Sierra Leone, Senegal and Togo). Our main duty was conducted at the central level
during training, social mobilization and planning of activities. Supervision went on at
central, regional and district levels.
All along supervision of activities we visited health centers and hospitals. We were
always accompanied by a WHO or EPI staff. Observations were noted and feedback
always given to the district, region then central level.
During supervision the following observations were globally made:
Funds were disbursed to enable operational level functioning,
Training of actors took place at all levels as expected,
The distribution of ancillaries followed the "bundling" policy only in few
countries (Togo, Senegal), except for the vaccination cards in Senegal,

49
At most of vaccination posts, the job was well organized and material correctly
disposed of,
Vaccine safety rules were observed, and there was communication between the
vaccinator and the person vaccinated,
Sending daily data to the central level was not effective for most of countries,
The waste storage varied from one country to another, but nowhere, we had a
specific room for the storage of safety boxes,
There was no particular vaccine storage problem at the health units; but many
fridges were not functioning (Togo, Ghana, Senegal)
It was obviously our duty to correct deficiencies, and congratulate health
workers when work was well done.
Similarly when it was useful we didn’t hesitate to change orientation
Our supervision in most cases was conducted in public and private health
centers.
After the campaign IST team usually:
o Met the WHO IVD Focal Point to make the point on what happened on the field
and make few suggestions,
o Debrief the WHO WR, during this we gave point on our findings, and present our
recommendations for future activities,
o Back to our base, we debrief also the IST Focal Point with whom we discussed
the issue of the remaining vaccines in countries where there was.

50
Attendance varied from country to country
Supervisors at H1N1 immunization/vaccination post
Results
Vaccination Coverage
Eleven countries out of thirteen are formally said have so far organized campaign of
vaccination against H1N1. Some of them have not yet communicated their final results.
The table 1 below summarizes countries’ results. It contents also the AEFI cases where
they are available.

51
COUNTRIES Parentage of vaccine received
POPULATION
Information on vaccines and ancillaries Comments
Type doses
received Doses
remained Wastage rate in %
Management of AEFI Cases
Vaccination group Target Immunized Coverage
Declared Investigated
Benin
Burkina Faso 10.1%
GSK Adj 1,450,000
Côte d'Ivoire 10.3%
Sanofi France n. adj 1,942,300
Gambie 9.9% CSL, non-adjuv. 164,500
Health Workers, 9,073 8,544 94.2%
Pregnant Women 18,881 16,669 88.3%
Diabetics, 6,420 4,834 75.3%
Chronically Ill and 13,370 12,281 91.9%
Children10–12 Years 61,090 52,804 90.1%
TOTAL 170,000 152,494 89.7% 3100 5,5 Not avail.
Ghana 10% GSK, adjuv. 2,300,000
Health Workers, 105,231
Pregnant Women 180,645
chronic disease 149,312
Security Officers 30,953
Inter. Travellers 1,068
Others 675,054
TOTAL 2,300,000 1,142,263 Not available 2 397
Not available
Guinée Bis. 9.7%
Sanofi France, n-adj. 160,000
Guinée Cona 0.114 GSK, adjuv. 1049000
Femmes enceintes 313,674 206566

52
Personnels santé 50,000 30673
Malades chroiniques 15,000 46104
Dépendants pers.santé 670,000 240758
Autres 448512
Total 1048874 972613 92 4.6 1068
Libéria 2.2% CSL, non-adjuv. 78,000
Health Workers, 9,534 15,334 160.83%
Pregnant women 64,446 48,297 75%
im. border pers§others 5,000 11,175 223.5%
TOTAL 79,000 71,629 90.66% Not available
Not available
Not avail. Not avail.
Mali
Mauritanie 9.7% CSL, non-adjuv. 296,400
Health workers 8,000 1,683 21.03%
Pregnant women 153,370 6,309 4.11%
security personnal 2,000 1,071 53.55%
Others with C.D 133,370 3,324 2.49%
TOTAL 296,740 12,387 4.17% 248,400 Not available
Not avail.
Niger 10.0% Sanofi US, n-adj. 1,374,900 Deux districts
Personnels santé 19,262 33,721 175% n'ont pas
Enfants 6-11 mois 481,709 594,964 124% encore vacciné
Femmes enceintes 683,816 265,363 39% Filingué et
Malades chroniques 296,938 286,845 97% Arlit
TOTAL 1,481,725 1,180,893 80% 2.31 3
Nigeria 2%
Sanofi US, n-adj. 2,880,000
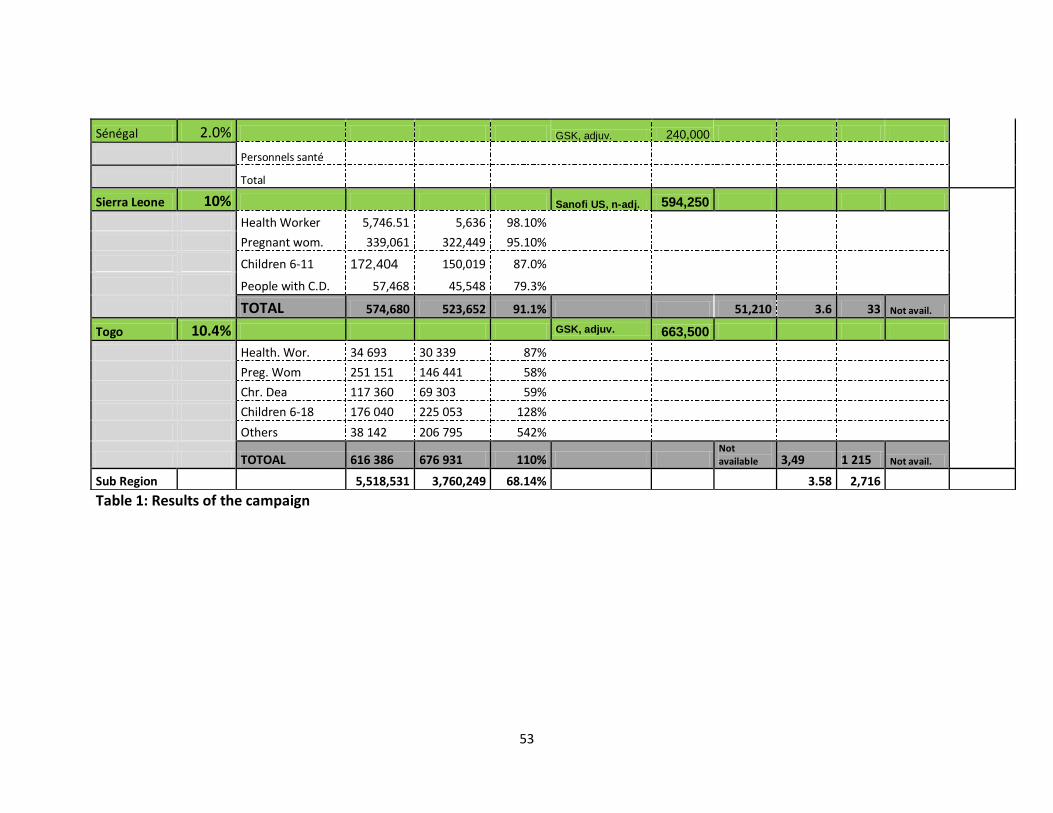
53
Table 1: Results of the campaign
Sénégal 2.0% GSK, adjuv. 240,000
Personnels santé
Total
Sierra Leone 10% Sanofi US, n-adj. 594,250
Health Worker 5,746.51 5,636 98.10%
Pregnant wom. 339,061 322,449 95.10%
Children 6-11 172,404 150,019 87.0%
People with C.D. 57,468 45,548 79.3%
TOTAL 574,680 523,652 91.1% 51,210 3.6 33 Not avail.
Togo 10.4% GSK, adjuv. 663,500
Health. Wor. 34 693 30 339 87%
Preg. Wom 251 151 146 441 58%
Chr. Dea 117 360 69 303 59%
Children 6-18 176 040 225 053 128%
Others 38 142 206 795 542%
TOTOAL 616 386 676 931 110% Not available 3,49 1 215 Not avail.
Sub Region 5,518,531 3,760,249 68.14% 3.58 2,716

54
Adverse Events Reported (AEFI):
Minor AEFI cases were reported here and there, but no serious cases have been investigated to
our attention. Cases of headache, fever or muscle pain have been reported. The availability of
“paracétamol” has contributed to keep the pain away. We would like to report a practice that
has been put in place in Togo, which has helped reduce cases of AEFI. It was after the
vaccination of children aged 6-18 months, mothers were systematically given “paracétamol”.
With these tablets, moms no longer need to return to the clinic when the child cries. Similarly it
is important to recall the formula for the management of AEFI cases in Ghana. First to each
vaccination post the list of side effects was displayed, and all without exception AEFI were
documented at each clinic, and all such information has been put together to develop the final
document on the AEFI cases for this vaccination.
Rumors of deaths ran in Ghana, but the investigations failed to blame the vaccine.
AEFI management during campaign
5.1.3 Challenges of Assignment
5.2 Vaccines and ancillary supplies
Regarding the storage of vaccines, all deployment plans have integrated this issue and
measures have been taken to avoid exposing vaccines for lack of space in the cold chain or dry
store. The scenarios were developed for the consideration of low storage capacity at central,
regional and district levels.
The vaccines and ancillaries distribution respected the process prescribed in various
deployment plans, namely delivering of vaccines and ancillaries to the operational units in brief

55
delays. It is important to remember that the provision of prepaid cards to most of responsible
helped to secure vaccines, and even to send data to the central level.
Health units that had cold chain problems resorted to nearest neighbors. However, we found
weaknesses in the maintenance of equipment and gas supplies to health units. To permanently
reduce these problems, we suggested the management of the issue at central level. This option
will ensure that all health units receive their monthly allocation of gas. Regarding maintenance,
there is a lack of funds for the parts and payment of bills. Which solution to optimize the
functionability of the cold chains? It is left to EPI managers to discuss with partners.
Concerning the wastage, It varied from country to country. It should be noted that, in Togo an
error on the expiry date of vaccine received for Phase One activities, contributed to the
destruction of a large stockpile of vaccine, which could only increase the wastage rate. In a
separate document (table of results), we synthesize the wastage rate by country, and the
number of doses of vaccine remaining where available.
5.2.1 Legal and Regulatory Issues
The vaccine against the flu was a new vaccine for the EPI. Its entry and qualification could be a
problem for the EPI authorities. To avoid surprises in the vaccine arrival at the airport, steps
have been taken in all countries to facilitate this entry; and where taxes were mandatory, as in
Senegal, measures have been taken to meet timing. To our knowledge, no cargo has been stuck
at the airport for procedural reasons.
5.2.2 Reception, Storage and Distribution of Vaccines
After the vaccine arrival in the country, a distribution plan was built following the targets.
Depending of the situation of the regions, districts or the health centers, axes of distribution
were drawn from the central level to the health unit.
List of needs follows then (human resources, vehicles, fuel etc.). It is important to recall that
DELEVER funded this activity in some countries; it has been successful and there was no
complaint as far as vaccine and ancillaries’ distribution are concerned. Before that issue, an
evaluation went on in order to address the storage capacity. We have not noted a specific
problem concerning the domain. Where there was a shortage, health unit used the neighboring
unit to store the vaccine

56
5.2.3 Healthcare Waste Management
Every country of the sub region has an internal policy for the waste management with regard to
past campaigns they have conducted. Overall it is within the health districts that safety boxes
will be destroyed. The main problem regarding the waste management was the absence of a
specific storage room to secure safety boxes. Used syringes were immediately put into safety
boxes. Concerning waste collection, most of countries planned to collect of safety boxes by
supervisors within the districts. Every district has the responsibility to destroy those safety
boxes.
Storage of safety boxes in the open an incinerator
5.3 Major Event that Influenced Activities
. When we do a turn in different health units, observe the head of Unit at work, even without
going into the calendar of events, the only daily tasks adequately show the stress of host. When
you have to add the various mass campaigns that must be organized, and sometimes without
any assistant, the heavy burden responsibility of the health worker is evident. By introducing
vaccination against influenza on one side, while on the other it is imperative to eradicate polio,
not to mention a possible mop up for measles, as well as the introduction of vaccination against
meningitis, the challenge is not easy to meet. The interweaving of these various activities
explains the delays in the development of deployment plans, also quality of results regarding
pressures responsible of health units are facing. It is important to recognize that with the
multitude of activities, outcomes and monitoring are not always obvious and for this reason, we
sometimes welcome the willingness of some unit leaders who seek excellence. This explains the
difficulty today in some countries to decide a date for the vaccination. We trust that they will
find ways to make available to AFRO and HQ information they need for further activities.
Similarly it is also important to note events outside our control that have violated the due

57
performance of certain timing in some countries (elections in Guinea Conakry, strike within the
medical community in Senegal, stopping of vaccination campaign in Mauritania).
Rain did not only disturb the vaccination, but also daily activities (Flooded compound of hospital)
6. Evaluation activities On completion of the vaccination campaigns most countries sent coverage results on excel. A few also sent written
reports and filled the evaluation tool sent by HQ. Countries however complained that they experienced difficulties
filling the tool online.
6.1 Surveillance for AEFI Information on AEFI is shown on a table attached; but it’s important to note that there was no significant AEFI that
was found to be directly connected to the vaccine. Surveillance continues.
7.0 Conclusion and Recommendations
7.1 Conclusion The report gives a brief of the steps and actions followed in the process of developing country H1N1 vaccine
deployment and utilization plans. Generally the whole exercise has been a success in the WHO IST West with 13
out of 16 countries reaching implementation/vaccination stage. There has been no serious AEFI that has so far
been detected and linked to the H1N1 vaccine.

58
Effort has been made, in the report; to highlight what went right and where things may have gone wrong with a
view to perform better should a similar situation arise in future.
7.2 Recommendations
Personal involvement of the WR ensured a successful campaign. Hence in future such
emergency activities should involve WRs.
Launching activities in which the WR and the Minister and his Senior staff were vaccinated
against H1N1 boosted the turn up for vaccinations.
Where the WHO IVD focal point was involved as the focal point for H1N1 the deployment, the
activities were better organized than when other officers were given that assignment.
There is need to strengthen public awareness and social mobilization for emergency activities.
The Officer responsible for social mobilization at IST West should have been facilitated by the
program to support some countries that needed support
Emergency activities like this one should be carried out swiftly and fast while the pandemic is
still on. Some delays in sending vaccines and releasing of funds were noted.
It was increasingly difficult to convince country decision makers to conduct a campaign after
cases had come down and during the post pandemic period.
Correspondences to countries were often made from HQ without copying to IST. The IST office
came to know about them when things didn’t work out. The IST officers involved should be
copied to.
There were many competing programs and this affected the deployment process right from
planning to implementation
Late submission to IST of requests for Technical support by countries was seen as a problem
because the administrators facilitating the travel arrangements were not given ample times to
process them.
Rainy season interfered with campaign activities in some countries.
8. Word of appreciation We are grateful to WHO AFFRO and WHO Headquarter for the support and guidance they provided to us. Our
appreciation go to the Coordinator of WHO IST West, the IVD Focal person and her staff in Ouagadougou and all
the countries in IST West for hosting us and making our work easy and successful.
Last but not least our sincere appreciation goes to MCHIP and DELIVER for employing us and attending to all our
day to day administrative needs and requirements promptly. God bless you all.
References B Source of information
WHO website
Country/National deployment plans
Resource persons at IST and country offices
Country progress and coverage reports


















