Official Journal of the Aortic Institute at Yale-New Haven...
39
Editor-in-Chief: Co-Editor-in-Chief: Editors: Associate Editors: John A. Elefteriades, MD Michael Jacobs, MD Kim Eagle, MD Bart Muhs, MD Sandip Mukherjee, MD Santi Trimarchi, MD Mohamad Bashir, MD Emily A. Farkas, MD Bulat A. Ziganshin, MD A multi-disciplinary journal for clinicians and researchers with interest in the Aorta and its first-order branches, intended for cardiac surgeons, cardiologists, vascular surgeons, interventional radiologists, geneticists, molecular biologists, engineers, and industry scientists, among others. Publish Date: December 2013 Volume 1, Issue 6 Official Journal of the Aortic Institute at Yale-New Haven Hospital Accepting papers at: http://aorta.scienceinternational.org. ISSN 2325-4637
Transcript of Official Journal of the Aortic Institute at Yale-New Haven...

Editor-in-Chief:
Co-Editor-in-Chief:
Editors:
Associate Editors:
John A. Elefteriades, MD
Michael Jacobs, MD
Kim Eagle, MDBart Muhs, MDSandip Mukherjee, MDSanti Trimarchi, MD
Mohamad Bashir, MDEmily A. Farkas, MDBulat A. Ziganshin, MD
A multi-disciplinary journal for clinicians and researcherswith interest in the Aorta and its first-order branches,intended for cardiac surgeons, cardiologists, vascularsurgeons, interventional radiologists, geneticists, molecularbiologists, engineers, and industry scientists, among others.
Publish Date:December 2013
Volume 1, Issue 6
Official Journal of the Aortic Institute at Yale-New Haven HospitalAccepting papers at: http://aorta.scienceinternational.org.
ISSN 2325-4637

MAQUET Cardiovascular LLC
45 Barbour Pond Drive
Wayne, NJ 07470
Phone: +1 (408) 635-6800
www.maquet.com/int
Conform to the new standard for Left Atrial Appendage (LAA) Occlusion.
Angled jaw aligned with Fastener elbow aids in optimal placement
Soft silicone housing for tissue conformity
Available in 7 & 9 Connector configuration
1 Slater AD, Tatooles AJ, Coffey A, et al. Prospective clinical study of a novel left atrial appendage occlusion device.
Ann Thorac Surg. 2012 Jun;93(6):2035-8; discussion 2038-40.
Easy and rapid application (60 seconds or less)1
Conforms to variable LAA size and thickness with pliable silicone housing
Zero blood loss at device footprint
MAQUET — The Gold Standard.
The TIGERPAW® System II with its unique Fastener technology is designed with soft silicone housing
to minimize risk and damage to the friable LAA. Once implanted, the Fastener conforms to the shape
and thickness of the patient’s appendage, resulting in 100% clinically proven occlusion.1
MCV00020598 Rev A
Scan this QR to
learn more about
TIGERPAW® System II
MEASURED IN RESULTS.M E D T R O N I C S E T S T H E S TA N D A R D F O R G L O B A L A O R T I C C L I N I C A L E V I D E N C E L E A D E R S H I P.
Get results at www.medtronicendovascular.com
1. US IDE Trial. Endurant 2011 Clinical Update. 2. Data on file at Medtronic.3. BOXI data as of March 16, 2012.
Most comprehensive abdominal aortic clinical program: 1,500+ patients studied worldwide2
1 out of 2 EVAR patients worldwide receives an Endurant stent graft3
UC201301782aEN © Medtronic, Inc. 2013. All Rights Reserved.
At 1 and 2 Years1
MIGRATION
TYPE I ENDOLEAK
RUPTURE POST IMPLANT 0%
Innovating for life.
Endurant® II AAA STENT GRAFT SYSTEM

Medtronic Vascular, Inc.3576 Unocal PlaceSanta Rosa, CA 95403USA
Product Services Support CenterTel: 888.283.7868Fax: 800.838.3103
CardioVascular LifeLineCustomer SupportTel: 877.526.7890Tel: 763.526.7890
www.medtronic.comwww.medtronicendovascular.com
For distribution in the USA only.FTSOP113326-06 Rev 1B © Medtronic, Inc. 2013. All Rights Reserved.
IndicationsThe Endurant® II Stent Graft System is indicated for the endovascular treatment of infrarenal abdominal aortic or aorto-iliac aneurysms in patients with the following characteristics:
of 19 to 32 mm
Contraindications The Endurant II Stent Graft System is contraindicated in:
Warnings and Precautions
has not been established. All patients should be advised that endovascular
the performance of the implanted endovascular stent graft. Patients with
in the structure or position of the endovascular graft) should receive enhanced follow-up. Specific follow-up guidelines are described in the Instructions for Use.
secondary interventions or surgical procedures.
to undergo or who will not be compliant with the necessary preoperative and postoperative imaging and implantation studies as described in the Instructions for Use.
along the edge of the stent graft should be aligned immediately below the lower-most renal arterial origin.
increased duration of the procedure.
been evaluated in some patient populations. Please refer to the product Instructions for Use for details.
MRI Safety and CompatibilityNon-clinical testing has demonstrated that the Endurant II Stent Graft is MR Conditional. It can be scanned safely in both 1.5 T & 3.0 T MR systems under certain conditions as described in the product Instructions for Use. For additional information regarding MRI please refer to the product Instructions for Use.
Adverse EventsPotential adverse events include (arranged in alphabetical order): Amputation;
Aneurysm enlargement; Aneurysm rupture and death; Aortic damage, including perforation, dissection, bleeding, rupture and death; Arterial
Bleeding, hematoma or coagulopathy; Bowel complications (e.g., ileus,
attendant problems (e.g. arrhythmia, myocardial infarction, congestive heart failure, hypotension, hypertension);
hematuria, infection); Hepatic failure; Impotence; Infection of the aneurysm, device access site, including abscess formation, transient fever and pain;
paraparesis, paralysis); Occlusion of device or native vessel; Pulmonary
insufficiency, failure); Stent graft: improper component placement; incomplete
difficulties; graft material wear; dilatation; erosion; puncture and perigraft
including infection, pain, hematoma, pseudoaneurysm, arteriovenous fistula, dissection; Vascular spasm or vascular trauma (e.g., iliofemoral vessel dissection, bleeding, rupture, death); Vessel damage; Wound complications and
cellulitis)
Please reference product Instructions for Use for more information regarding indications, warnings, precautions, contraindications and adverse events.
CAUTION: Federal (USA) law restricts this device to sale by or on the order of a physician.

Edwards, Edwards Lifesciences, and the stylized E logo are trademarks of Edwards Lifesciences Corporation.
© 2012 Edwards Lifesciences Corporation. All rights reserved. AR08712
This is the moment your skill and technique
are complemented with the latest advances
in heart valve therapies. It’s the moment
world-class training, expert clinical support,
and meaningful innovations continue to
compliment your patient care. This is the
moment you partner with Edwards
Lifesciences along your path to success.
Progress Confidently
Learn more about the history, products,
and educational opportunities in this moment.
www.edwards.com/ThisMoment
Edwards Lifesciences Irvine, USA I Nyon, Switzerland I Tokyo, Japan I Singapore, Singapore I São Paulo, Braziledwards.com
your team meets our hands-on training
This moment
is everything.
Editorial Board
Editor-in-Chief
John A. Elefteriades Yale University(New Haven, CT)
Co-Editor-in-Chief
Michael Jacobs Maastricht UniversityHospital (Maastricht,Netherlands)
Editors
Alan Dardik Yale University(New Haven, CT)
Kim Eagle University of Michigan(Ann Arbor, MI)
Bart Muhs Yale University(New Haven, CT)
Santi Trimarchi Polilinico San Donato(Milan, Italy)
Sandip Mukherjee Yale University(New Haven, CT)
Editor Emeritus
Randall B. Griepp Mount Sinai MedicalCenter (New York, NY)
Associate Editors
Emily A. Farkas Saint Louis University(St. Louis, MO)
Bulat A. Ziganshin Yale University(New Haven, CT)
Mohamad Bashir Liverpool Heart andChest Hospital,(Liverpool, UK)
Editorial Board
Jean Bachet Zayed Military Hospital(Abu Dhabi, United ArabEmirates)
Steven Bailey University of TexasHealth Sciences Center(San Antonio, TX)
Paul Barash Yale University (NewHaven, CT)
Roberto DiBartolomeo
University of Bologna(Bologna, Italy)
Joseph BavariaUniversity ofPennsylvania(Philadelphia, PA)
Jean-PierreBecquemin
Henri Mondor Hospital(Creteil, France)
Harisios Boudoulas Aristolelian University(Columbus, OH)
Alan C. Braverman Washington UniversitySchool of Medicine(St. Louis, MO)
Duke Cameron John Hopkins Hospital(Baltimore, MD)
John Chang Long Island VascularCenter (Roslyn, NY)
Roberto Chiesa University di Bologna(Bologna, Italy)
Michael Coady Stamford Hospital(Stamford, CT)
Denton A. Cooley Texas Heart Institute(Houston, TX)
Joseph Coselli Texas HeartInstitute/Baylor College ofMedicine (Houston, TX)
Michael Dake Stanford University(Stanford, CA)
George Dallas Archimedes Analytical/Associate Yale Medical(Hickory, NC)
Tirone E. David Toronto General Hospital(Toronto, ON)
Dimitrios Dougenis Patras University Schoolof Medicine (Rio, Greece)
L. (Hank) Edmunds University of Pennsylvania(Philadelphia, PA)
Anthony Estrera University of Texas-Houston Medical School(Houston, TX)
Rosella Fattori S. Orsola UniversityHospital (Bologna, Italy)
Anthony Furnary Starr-Wood Cardiac Group(Portland, OR)
Valentin Fuster Mount Sinai MedicalCenter (New York, NY)
Leonard Girardi New York Weill CornellMedical Center (NewYork, NY)
Gary Grunkemeier Providence Health System(Portland, OR)
Richard Gusberg Yale New Haven Hospital(New Haven, CT)
Ala Sami Haddadin Yale University (NewHaven, CT)
Jay Humphrey Yale University (NewHaven, CT)
Olga A. Iakoubova Celera (Alameda, CA)

John S. Ikonomidis Medical University ofSouth Carolina(Charleston, SC)
Jeffrey Indes Yale University(New Haven, CT)
Eric Isselbacher Massachusetts GeneralHospital (Boston, MA)
Ion Jovin McGuire VA MedicalCenter (Richmond, VA)
Jes S. Lindholt University Hospital ofOdense (Odense, Denmark)
Matthias Karck University of Heidelberg(Heidelberg, Germany)
Nicholas Kouchoukos Missouri Baptist MedicalCenter (St. Louis, MO)
George Koullias Stony Brook University(Stony Brook, NY)
Johannes Lammer Medical University(Vienna, Austria)
Frank A. Lederle VA Medical Center(Minneapolis, MN)
Scott LeMaire Baylor College ofMedicine (Houston, TX)
George Letsou University ofTexas-Houston MedicalSchool (Houston, TX)
Bart Loeys Ghent University Hospital(Ghent, Belgium)
Wei-Guo Ma Anzhen CardiovascularSurgery (Beijing, China)
Jorge Mascaro Queen Elizabeth MedicalCentre (Birmingham, UK)
George Matalanis Austin Hospital(Heidelberg, Australia)
Dianna Milewicz University of Texas MedicalSchool (Houston, TX)
Raj K. Modak Yale New Haven Hospital(New Haven, CT)
Hamid Mojibian Yale University School ofMedicine (New Haven, CT)
Frans Moll University Medical CenterUtrecht (Utrecht,Netherlands)
Christoph Nienaber University HospitalRostock (Rostock,Germany)
Dimitris Nikas Athens Medical Center(Athens, Greece)
Takao Ohki Jikei University School ofMedicine (Tokyo, Japan)
Aung Oo Liverpool Heart andChest Hospital(Liverpool, UK)
John Pepper Imperial College(London, UK)
John A. Rizzo Stony Brook University(Stony Brook, NY)
Flavio Rocha Virginia Mason MedicalCenter (Seattle, WA)
Natzi Sakalihasan University of Liege(Liege, Belgium)
Hans-JoachimSchaefers
University of Saarlandes(Homburg, Germany)
Marc Schepens AZ St. Jan(Brugge, Belgium)
Oz Shapira Hebrew University(Jerusalem, Israel)
Bauer Sumpio Yale New Haven Hospital(New Haven, CT)
Li-Zhong Sun Capital Medical University(Beijing, China)
Wei Sun University of Connecticut(Storrs, CT)
Lars Svensson Cleveland Clinic(Cleveland, OH)
Robert Thompson Washington UniversitySchool of Medicine(St. Louis, MO)
M. David Tilson III Columbia University (NewYork, NY)
Britt H. Tonnessen Roper Heart and VascularCenter (Charleston, SC)
Ramesh K. Tripathi Narayana Institute ofVascular Sciences(Bangalore, India)
Marko Turina University Hospital(Zurich, Switzerland)
Yuichi Ueda Tenri Hospital(Nari, Japan)
Gilbert R. Upchurch,Jr.
University of VirginiaMedical Center(Charlottesville, VA)
Paul Urbanski Herz and Gefaess Clinic(Neustadt, Germany)
Hence Verhagen Erasmus UniversityMedical Center(Rotterdam, Netherlands)
Stephen Westaby The John RadcliffeHospital (Oxford, UK)
Christopher White Ochsner Medical Center(New Orleans, LA)
Simona Zannetti Medtronic Cardio Vascular(Santa Rosa, CA)

CME
CME
ORIGINAL RESEARCH ARTICLES
259 Inflammatory Cell Infiltrates in Acute and Chronic Thoracic Aortic DissectionDarrell Wu, Justin C. Choi, Aryan Sameri, Charles G. Minard, Joseph S. Coselli, Ying H. Shen, Scott A. LeMaire
268 Modeling the Growth of Infrarenal Abdominal Aortic AneurysmsMarc A. Bailey, Paul D. Baxter, Tao Jiang, Aimee M. Charnell, Kathryn J. Griffin, Anne B. Johnson,Katherine I. Bridge, Soroush Sohrabi, D. Julian A. Scott
LETTER TO THE EDITOR
274 Comment on “Modeling the Growth of Infrarenal Abdominal Aortic Aneurysms” by Bailey et al.Hai Fang, John A. Rizzo
STATE-OF-THE-ART REVIEW
276 Cardiovascular Collapse During Transcatheter Aortic Valve Replacement: Diagnosis andTreatment of the “Perilous Pentad”
Adam El-Gamel
IMAGES IN AORTIC DISEASE
283 Esophago-Pleural Fistula Caused by Compression Necrosis in a Patient With Acute Type BAortic Dissection
Toshiro Ito, Yohsuke Kuroda, Toshitaka Watanabe, Tetsuya Koyanagi, Tetsuya Higami
HOW I DO IT
286 Finger-Thumb Technique for Elephant Trunk RetrievalBulat A. Ziganshin, John A. Elefteriades
UPCOMING MEETINGS
289 List of Upcoming Meetings
AORTA (ISSN 2325-4637) is an online open-access journal issued bi-monthly (6 issues per year, one volume per year) by ScienceInternational Corporation.
All correspondence should be directed to: John A. Elefteriades, MD, Editor-in-Chief, AORTA Journal, 330 Cedar Street, BoardmanBuilding #204, New Haven, CT 06510. Tel.: �1-203-785-2551, Fax: �1-203-785-3346, E-Mail: [email protected]
All inquiries regarding copyrighted material from this publication should be directed to Science International Corporation: 31 Sun-set Court, Stamford, CT, 06903, USA. Tel.: �1-203-329-8842, Fax: �1-203-329-8846, E-Mail: [email protected]
Volume 1, Number 6, December 2013

Inflammatory Cell Infiltrates in Acute and ChronicThoracic Aortic Dissection
Darrell Wu, MD1,2,3,†, Justin C. Choi, MD1,2,†, Aryan Sameri, BS1,2, Charles G. Minard, PhD4,Joseph S. Coselli, MD1,2, Ying H. Shen, MD, PhD1,2, Scott A. LeMaire, MD1,2,3*1Division of Cardiothoracic Surgery, Michael E. DeBakey Department of Surgery, Baylor College of Medicine, Houston, Texas;2Department of Cardiovascular Surgery, The Texas Heart Institute, Houston, Texas; 3Department of Molecular Physiology andBiophysics, Baylor College of Medicine, Houston, Texas; and 4Dan L. Duncan Institute for Clinical and Translational Research, BaylorCollege of Medicine, Houston, Texas
AbstractBackground: Thoracic aortic dissection (TAD) is a highlylethal cardiovascular disease. Injury to the intima andmedia allows pulsatile blood to enter the media, leadingto dissection formation. Inflammatory cells then infiltratethe site of aortic injury to clear dead cells and damagedtissue. This excessive inflammation may play a role inaneurysm formation after dissection. Methods: Using im-munohistochemistry, we compared aortic tissues from pa-tients with acute TAD (n � 11), patients with chronic TAD(n � 35), and donor controls (n � 20) for the presence ofCD68� macrophages, neutrophils, mast cells, and CD3� Tlymphocytes. Results: Tissue samples from patients withacute or chronic TAD generally had significantly moreinflammatory cells in both the medial and adventitiallayers than did the control samples. In tissues from pa-tients with acute TAD, the adventitia had more of theinflammatory cells studied than did the media. The pat-tern of increase in inflammatory cells was similar inchronic and acute TAD tissues, except for macrophages,which were seen more frequently in the adventitial layerof acute TAD tissue than in the adventitia of chronic TADtissue. Conclusions: The inflammatory cell content of bothacute and chronic TAD tissue was significantly differentfrom that of control tissue. However, the inflammatorycell profile of aneurysmal chronic TAD was similar to thatof acute TAD. This may reflect a sustained injury responsethat contributes to medial degeneration and aneurysmformation. Copyright © 2013 Science International Corp.
Key WordsInflammation · Thoracic aortic dissection
Macrophage · Mast cell · Neutrophil · T lymphocyte
Introduction
Aneurysm formation after thoracic aortic dissec-tion (TAD) is a deadly cardiovascular disease and amajor cause of morbidity and mortality [1]. Aorticdissections occur when pulsatile blood enters an in-timal tear and causes the medial layer to split alongthe length of the aorta. Weakening of the aortic wallcan be caused by medial degeneration, which is char-acterized by vascular smooth muscle cell depletionand elastic fiber depletion and fragmentation [2,3].Concurrently, inflammatory cells can infiltrate the in-jured aortic wall, clear the dead cells, remove dam-aged matrix proteins, and remodel the extracellularmatrix [4]. However, uncontrolled inflammatory pro-cesses can lead to tissue destruction in the aorta [5,6],which in turn may lead to the formation of an aneu-rysm after aortic dissection. The role of inflammationafter dissection as a cause of aneurysm formation hasnot been well characterized.
Previous studies have shown that CD68� macro-
Fax �1 203 785 3346E-Mail: [email protected]://aorta.scienceinternational.org
© 2013 Aorta.Published by Science International Corp.ISSN 2325-4637
Accessible online at:http://aorta.scienceinternational.org
*Corresponding author:Scott A. LeMaire, MDDivision of Cardiothoracic SurgeryMichael E. DeBakey Department of SurgeryBaylor College of MedicineOne Baylor Plaza, BCM 390, Houston, TX 77030Tel.: �1 832 355 9942, Fax: �1 832 355 9928, E-Mail: [email protected]†These authors contributed equally to this study.
Original Research Article
Aorta, December 2013, Volume 1, Issue 6: 259 –267DOI: http://dx.doi.org/10.12945/j.aorta.2013.13-044
Received: August 22, 2013Accepted: November 27, 2013Published online: December 2013

phages [7], neutrophils [8], mast cells, and CD3� [5,6]and CD4� T lymphocytes [9] are significantly in-creased in the aortic wall of patients with abdominalaortic aneurysms or ascending thoracic aortic aneu-rysms (TAAs) (both heritable and sporadic), as well asin patients with Type A dissections [5,6]. However, theinflammatory infiltrates present in acute TAD and de-scending TAA due to chronic TAD are not well docu-mented. In this study, we examined aortic tissues frompatients with acute ascending TAD or descendinganeurysms after TAD for the presence of CD68� mac-rophages, neutrophils, mast cells, and CD3� T lym-phocytes in both early and late phases of the dissec-tion. We hypothesized that chronic TAD tissues wouldexhibit reduced inflammation and an altered inflam-matory cell profile compared to acute TAD tissues.
Materials and Methods
Study Enrollment and Tissue CollectionThe institutional review board at Baylor College of Medicine
approved this study. Informed written consent was obtainedfrom all subjects. We enrolled 46 patients who underwentrepair of an acute or chronic TAD and who did not haveaortitis, dissection variants such as intramural hematoma orpenetrating aortic ulcer, or a dissection caused by trauma.Tissue samples obtained within 14 days of TAD onset wereconsidered acute (n � 11), whereas those obtained more than60 days after TAD onset were considered chronic (n � 35); wedid not enroll patients in whom tissue samples would beobtained during the subacute phase (ie, between 14 and 60days after TAD onset). During dissection repair, we excisedtissue samples from the outer wall of the false lumen. Controlaortic tissues (n � 20) were obtained from organ or tissuedonors who had no aortic aneurysm, dissection, coarctation, orprior aortic repair and no evidence of sepsis.
Histology and Immunohistochemical StainingAortic tissues were paraffin-embedded and sectioned. En-
dogenous peroxidase activity in aortic sections was quenchedby 3% hydrogen peroxide treatment. Citric acid antigen re-trieval was performed. Tissue sections were blocked in 5%normal horse serum and incubated overnight with primaryantibodies (Table 1). Samples were then incubated with the
appropriate biotin-conjugated anti-mouse IgG secondary anti-bodies (Vector Laboratories, Inc., Burlingame, CA, USA). Normalmouse immunoglobulin G (Vector Laboratories) served as thenegative control for immunostaining. Inflammatory cells werevisualized by using peroxidase substrate 3,3=-diaminobenzi-dine (DAB; Vector Laboratories), and cell nuclei were counter-stained with hematoxylin (Sigma Aldrich, St. Louis, MO, USA).Image Pro-Plus 4.5 (Leica Microsystems, Bannockburn, IL, USA)was used to quantify the positive-staining inflammatory cellswithin the medial and adventitial layers. Three microscopicfields (400�) were randomly selected from each layer foranalysis. Positive-staining areas were then normalized to anobserved tissue area within the same sample.
Statistical AnalysisAll quantitative data are presented as the mean � standard
deviation. Data were analyzed with SPSS software, version 20.0(SPSS Inc., Chicago, IL, USA). The difference between the meanratios of positively stained area (�m2) to observed tissue area(�m2) among the groups was compared by using the Mann-Whitney or Kruskal-Wallis nonparametric test with Bonferronicorrection. The representative non-normal distribution of thepositive-staining area was depicted by using boxplots with afive-point summary scale.
Results and Discussion
In response to aortic injury, inflammatory cells in-filtrate the aortic wall to aid in tissue repair [4]. In thisstudy, we characterized the inflammatory infiltrate ob-served in aortic tissues from acute and chronic TADpatients by means of immunohistochemistry; all TADtissues showed significantly more CD68� macro-phages, neutrophils, mast cells, and CD3� T lympho-cytes in both the medial and adventitial layers ascompared to the same vessel layer in aortic tissuesfrom controls (Figs. 1A and 1B, 2A and 2B, 3A and 3B,and 4A and 4B, respectively). Moreover, we found agreater abundance of all inflammatory cell types in theadventitia than in the media (Figs. 1C, 2C, 3C, and 4C,respectively); this finding suggests that inflammatorycells infiltrate the aortic wall from the vasa vasoruminto the media [10]. This increased inflammatory infil-
Table 1. Primary Antibodies Used for Immunohistochemical Analysis
Antibody Cell type Source Clone Manufacturer Dilution factor
CD 68� Macrophage Monoclonal mouse anti-human KP1 Dako (Carpinteria, CA) 1:50Mast cell tryptase Mast cell Monoclonal mouse anti-human AA1 Dako 1:200Neutrophil elastase Neutrophil Monoclonal mouse anti-human NP57 Dako 1:125CD3� T Lymphocyte Monoclonal mouse anti-human F7.2.38 Dako 1:50
260 Original Research Article
Wu, D. et al. Inflammatory Cell Infiltrates in TAD

trate at the site of either acute or chronic dissectionsuggests that an uncontrolled or chronic inflammatoryresponse may contribute to aortic destruction andmaladaptive remodeling of the aortic wall. Our find-ings support previous reports of a similar increase ininflammatory infiltrates in thoracic and abdominalaortic aneurysms [5,6], suggesting a possible sharedmechanism of aortic degeneration among thoracic
and abdominal aortic aneurysms and acute andchronic TAD.
Patient CharacteristicsThe clinical characteristics and demographics of
the TAD patients and control donors are shown inTable 2. Patients with acute TAD tended to beyounger, and the percentage of smokers was similaracross the three groups. No patient in the chronic TADgroup had diabetes. As expected, the time to surgerywas longer for the chronic TAD patients than for theacute TAD patients (5 � 3 days versus 1730 � 2088days), and we had a higher number of ascending aortasamples (n � 10) collected from acute TAD patientsand a higher number of descending aorta samples(n � 20) from chronic TAD patients. The aortic diam-eters were similar for acute and chronic TAD patients.
Macrophages in TAD TissuesMacrophages are one of the most abundant inflam-
matory cells in the media and adventitia of abdominalaortic aneurysms (AAAs), TAA [5,6], and TAD tissues[5]. Because they secrete proteases such as collage-nases, elastase, and matrix metallopeptidase-9(MMP-9) that directly destroy the extracellular matrix[7] and cytokines and chemokines such as interleukin6 (IL-6) and monocyte chemotactic protein-1 (MCP-1)that recruit cells, macrophages are instrumental inmaintaining and amplifying the inflammatory cascade[11]. Using a marker for phagocytic cells, our immu-nohistochemical analysis showed that more areas inthe media and adventitia in both acute and chronicTAD tissues stained positively for CD68� macro-phages than did areas of control tissues (Fig. 1A).Although CD68 is not a macrophage-specific antigen,in this instance, sampling of the outer wall minimizesthe presence of any lipid-rich regions, limiting anycross-reactivity with CD68� smooth muscle cells [12].On quantification, we also found a significant increasein CD68� macrophage content in the media andadventitia of acute and chronic TAD tissues (Fig. 1B) ascompared to that in control tissues. Medial macro-phage content did not differ significantly betweenacute and chronic TAD tissues, but we found signifi-cantly higher levels of macrophages in the adventitiaof acute TAD tissues than in chronic TAD tissues. Inboth acute and chronic TAD tissues, the adventitiacontained significantly more areas that stained posi-tive for macrophages than did the media. These find-
Figure 1. CD68� macrophages are increased in the mediaand adventitia of acute and chronic TAD tissues. A. Immuno-histochemistry staining and comparison of macrophages in themedial and adventitial layers of the aortas from tissue samplesfrom donor controls and acute and chronic TAD patients.Original magnification, 200�. B. Comparison of the positive-staining areas of control, acute, and chronic dissection tissuesin the media and adventitia. C. Comparison of the positive-staining areas of the media and adventitia in acute and chronicTAD. The tips of the projecting bars represent the minimumand maximum values, and the box depicts the interquartilerange, with the solid middle line representing the median.Circles and asterisks represent 1.5� and 3� the interquartilerange, respectively.
Original Research Article 261
Aorta, December 2013 Volume 1, Issue 6: 259 –267

ings support the role of macrophages in ongoingaortic tissue destruction after dissection formation.
When evaluating the potential effects of macro-phages, it is important to consider the two differentsubpopulations of macrophages: the proinflammatoryM1 macrophages and the anti-inflammatory M2 mac-rophages. Studies have shown that an extensive pres-ence of the cytotoxic M1 subtype can further contrib-ute to tissue injury and destruction because thesemacrophages can release reactive oxygen species andnitric oxide synthase [13]. In contrast, M2 macro-phages have been shown to resolve inflammation byinhibiting T cell proliferation, phagocytizing apoptoticneutrophils, reducing the production of proinflamma-tory cytokines, and secreting and stabilizing matrixcomponents [13]. Therefore, comparing the levels ofproinflammatory M1 macrophages and anti-inflamma-tory M2 macrophages in TAD tissue could help deter-mine whether or not a chronic inflammatory state islikely to lead to an altered tissue homeostasis domi-nated by destructive factors.
Neutrophils in TAD TissuesNeutrophils are key regulators of sterile vascular
inflammation [14] and are capable of secreting serineproteases, cathepsins, and reactive oxygen intermedi-ates that can damage the extracellular matrix [8,14]. Ina mouse study, neutrophil depletion prevented AAAdevelopment [8], suggesting that neutrophil recruit-
ment is critical for the development of aortic aneu-rysms. Furthermore, doxycycline therapy has beenshown to improve proteolytic balance by reducing theneutrophil content in patients undergoing electiverepair of AAA [15]. In the present study, we observedan increase in neutrophil cells in the media and ad-ventitia of both acute and chronic TAD tissues (Fig.2B). Our findings support those of Cohen et al. [16],who also reported an increase in neutrophil levels inAAA. Thus, we believe that neutrophils may play a rolein the inflammatory cascade after an acute dissectionand that increased neutrophil levels in chronic TADtissues could suggest ongoing vascular injury, reflect-ing an acute-on-chronic inflammatory response thatcontributes to aneurysm formation.
Mast Cells in TAD TissuesLike macrophages and neutrophils, mast cells have
been shown to play a significant role in the develop-ment of AAA. Mast cells are capable of secreting chy-mases, which can activate matrix metalloproteinases,and angiotensin II, both of which contribute to aneu-rysm formation [17,18]. Additionally, mast cells cansecrete tryptases and proinflammatory signaling fac-tors, such as interferon-gamma (IFN�), IL-6, and tumornecrosis factor-� (TNF�), which can lead to an increasein monocyte infiltration, chemokine production, andvascular cell injury [19]. Furthermore, treatment withtranilast, a mast cell degranulation inhibitor, attenu-
Table 2. Characteristics of TAD Patients and Control Tissue Donors
Control n � 20 Acute TAD n � 11 Chronic TAD n � 35 p-value**
Age (years)* 57 � 9 49 � 16 54 � 14 0.2Hypertension 11 (55%) 9 (82%) 32 (91%) 0.006Smoking 8 (40%) 5 (46%) 19 (54%) 0.60Diabetes 6 (30%) 2 (18%) 0 0.001Stroke 8 (40%) 0 2 (6%) 0.002Coronary artery disease 0 1 (9%) 9 (26%) 0.02Peripheral vascular disease 0 0 4 (11%) 0.3Chronic obstructive pulmonary disease 1 (5%) 0 4 (11%) 0.6Confirmed diagnosis of Marfan syndrome 0 2 (18%) 5 (14%) 0.1Bicuspid valve disease 0 0 0 1.00Aortic diameter (cm)* 5.5 � 1.6 6.0 � 1.4 0.3Interval to surgery from time of dissection (days)* 5 � 3 1730 � 2088 �0.001Sample site
Ascending aorta 10 (50%) 10 (91%) 15 (43%)0.02Descending aorta 10 (50%) 1 (9%) 20 (57%)
*Data are presented as mean � standard deviation.
**p-values comparing groups by using Kruskal-Wallis tests (continuous variables) or Fisher’s exact test (discrete variables).
262 Original Research Article
Wu, D. et al. Inflammatory Cell Infiltrates in TAD

ates aneurysm formation [20]. In the present study, wefound a significant increase in mast cells in the aorticmedia and adventitia of both acute and chronic TADtissues (Fig. 3B). Given the critical role of mast cells invascular destruction, we believe they may be impor-tant contributors to the continued dilation and de-struction of the aortic wall.
CD3� T Lymphocytes in TADCD3� T lymphocytes are capable of secreting cy-
totoxic mediators such as Fas/FasL and perforin, whichcan cause cell death and have been reported to be themost prominent inflammatory cell in the media of TAD[6]. Furthermore, CD3� T lymphocyte activation canlead to the secretion of proteases that can weaken theaortic wall. For example, contact between mast cells
Figure 2. Neutrophils are increased in the media and adven-titia of acute and chronic TAD tissues. A. Immunohistochemis-try staining and comparison of neutrophils in the medial andadventitial layers of the aortas from donor controls and acuteand chronic TAD patients. Original magnification, 200�. B.Comparison of the positive-staining areas of control, acute, andchronic dissection tissues in the media and adventitia. C. Com-parison of the positive-staining areas of the media and adven-titia in acute and chronic TAD. The tips of the projecting barsrepresent the minimum and maximum values, and the boxdepicts the interquartile range, with the solid middle linerepresenting the median. Circles and asterisks represent 1.5�and 3� the interquartile range, respectively.
Figure 3. Mast cells are increased in the media and adventitiaof acute and chronic TAD tissues. A. Immunohistochemistrystaining and comparison of mast cells in the medial and ad-ventitial layers of the aortas from donor controls and acute andchronic TAD patients. Original magnification, 200�. B. Com-parison of the positive-staining areas of control, acute, andchronic dissection tissues in the media and adventitia. C. Com-parison of the positive-staining areas of the media and adven-titia in acute and chronic TAD. The tips of the projecting barsrepresent the minimum and maximum values, and the boxdepicts the interquartile range, with the solid middle linerepresenting the median. Circles and asterisks represent 1.5�and 3� the interquartile range, respectively.
Original Research Article 263
Aorta, December 2013 Volume 1, Issue 6: 259 –267

and T lymphocytes can result in the release of MMP-9from mast cells [21]. In the current study, we foundthat CD3� T lymphocytes were significantly increasedin the media and adventitia of acute and chronic TADtissues compared to control tissues (Fig. 4B). Our find-ings, combined with those showing increased CD3� Tlymphocyte levels in both sporadic and heritable as-cending TAA and Type A dissections [6], suggest that
the pathogenesis of sporadic and heritable aneurysmsand dissection may share a common immune mech-anism.
Media versus AdventitiaIn the traditional view of vascular inflammation,
chemoattraction results in the movement of immunecells through the endothelium to the media. However,growing evidence indicates that the adventitia mayplay a more prominent role in maintaining an inflam-matory response [22]. The adventitia is a major site ofinflammatory cell accumulation, and an extensive in-filtration of macrophages has been linked to aorticaneurysm development [23]. In this study, we foundsignificantly more CD68� macrophages, neutrophils,and CD3� T lymphocytes in the adventitia than in themedia in both acute and chronic cases of TAD (Figs.1C, 2C, and 4C). The abundance of inflammatory cellsin the adventitia indicates that the adventitia is adynamic microenvironment intimately involved in aor-tic wall homeostasis.
EosinophilsOne cell type that was not studied was eosinophils.
Eosinophils are capable of degranulating cytotoxic pro-teins that can damage tissue, produce superoxide andtransforming growth factor-�, and be stimulated by neu-trophils to produce proinflammatory cytokines to furtherperpetuate an inflammatory response [24]. Despite thesenumerous functions, the precise role of eosinophils incausing aortic aneurysms or dissection is not well under-stood, although eosinophils are present in the media ofacute ascending dissection, suggesting a potential roleof eosinophils in causing aortic dissection [25].
Study LimitationsTissue samples in the TAD group were obtained
from patients who had other underlying diseases inaddition to the dissection, and some patients experi-enced dissection after aneurysm formation. Thus, pa-tient heterogeneity and comorbidity factors may haveaffected the inflammatory response to dissection;however, this study was not powered to assess theclinical correlations between the degree of inflamma-tory infiltration and patient comorbidities. Further-more, we evaluated only end-stage aortic tissue; therole of inflammatory cells in the early stages of thedisease process needs to be studied to determinewhether their presence is a contributing factor to
Figure 4. CD3� T lymphocytes are increased in the media andadventitia of acute and chronic TAD tissues. A. Immunohisto-chemistry staining and comparison of CD3� T lymphocytes in themedial and adventitial layers of the aorta from donor controls andacute and chronic TAD patients. Original magnification, 200�. B.Comparison of the positive-staining areas of control, acute, andchronic dissection tissues in the media and adventitia. C. Com-parison of the positive-staining areas of the media and adventitiain acute and chronic TAD. The tips of the projecting bars repre-sent the minimum and maximum values, and the box depicts theinterquartile range, with the solid middle line representing themedian. Circles and asterisks represent 1.5� and 3� the inter-quartile range, respectively.
264 Original Research Article
Wu, D. et al. Inflammatory Cell Infiltrates in TAD

the initial development of TAD or solely a response toaortic injury after TAD. We also did not include ananalysis of tissue from the interim subacute periodafter acute (�14 days) and before chronic (�60 days)dissection. Although these definitions of acute andchronic are arbitrary, tissue is more friable and difficult tooperate on during this time frame, suggesting that theremay be an immense amount of remodeling. For thisreason, one might expect there to be even largeramounts of inflammatory cells present in these subacutecases than in acute or chronic cases. Additionally, we didnot delineate subpopulations of inflammatory cells. Fi-nally, technical limitations of our analysis based on themean ratios of positively stained area (�m2) to observedtissue area (�m2) precluded a comparison of the relativedistribution between cell types. Despite these limita-tions, the results of our study support the important roleof the inflammatory response in TAD.
Conclusion
We observed a significant increase in CD68� mac-rophages, neutrophils, mast cells, and CD3� T lym-phocytes in the media and adventitia of acute andchronic TAD tissues. The pattern of increase in inflam-matory cells was similar in acute and chronic dissec-tion tissue. The significant difference between thenumber of inflammatory cells seen in the medial andadventitial layers suggests that the cells infiltrate the
media through the vasa vasorum. Overall, this studysuggests that inflammation may play a role in tissuedestruction and the development of aortic aneurysmafter dissection.
Acknowledgments
This study was supported by NIH Grants K08HL080085 and R01 HL085341 (to S.A.L.). The ThoracicAortic Disease Tissue Bank at Baylor College of Medi-cine was supported in part through the Tissue BankingCore of the Specialized Center of Clinically OrientedResearch in Thoracic Aortic Aneurysms and Dissec-tions (NIH P50 HL083794). Darrell Wu was supportedby a training grant (NIH T32 HL007676) through theDepartment of Molecular Physiology and Biophysics atBaylor College of Medicine. We thank Guanghui Liu,MD, PhD, Jun Song, MD, PhD, and Mary T. Nguyen forassisting with immunostaining. We thank LudivineRussell and Laura C. Palmero for assistance in patientenrollment and tissue collection. We gratefully ac-knowledge Scott A. Weldon, MA, CMI, of Baylor Col-lege of Medicine, for assistance with illustrations, andStephen N. Palmer, PhD, Rebecca Bartow, PhD, andHeather Leibrecht, MS, of the Texas Heart Institute, forproviding editorial support.
Comment on this Article or Ask a Question
References
1. Centers for Disease Control and Preven-tion. National Center for Health Statistics.Compressed Mortality File 1999-2007. CDCWONDER On-line Database, compiled fromCompressed Mortality File 1999-2007 Se-ries 20 No. 2M, 2010. 2007.
2. Schlatmann TJ, Becker AE. Pathogenesis ofdissecting aneurysm of aorta. Comparativehistopathologic study of significance of me-dial changes. Am J Cardiol. 1977;39:21–26.10.1016/S0002-9149(77)80005-2
3. Schlatmann TJ, Becker AE. Histologicchanges in the normal aging aorta: implica-tions for dissecting aortic aneurysm. Am JCardiol. 1977;39:13–20. 10.1016/S0002-9149(77)80004-0
4. Mitchell RN, Libby P. Vascular remodeling intransplant vasculopathy. Circ Res. 2007;100:967–978. 10.1161/01.RES.0000261982.76892.09
5. He R, Guo DC, Estrera AL, Safi HJ, Huynh TT,Yin Z, et al. Characterization of the inflam-matory and apoptotic cells in the aortas of
patients with ascending thoracic aortic an-eurysms and dissections. J Thorac Cardio-vasc Surg. 2006;131:671–678.e2. 10.1016/j.jtcvs.2005.09.018
6. He R, Guo DC, Sun W, Papke CL, DuraisamyS, Estrera, AL, et al. Characterization of theinflammatory cells in ascending thoracic aor-tic aneurysms in patients with Marfan syn-drome, familial thoracic aortic aneurysms,and sporadic aneurysms. J Thorac Cardio-vasc Surg. 2008;136:922–929e1. 10.1016/j.jtcvs.2007.12.063
7. Thompson RW, Holmes DR, Mertens RA, LiaoS, Botney MD, Mecham RP, et al. Productionand localization of 92-kilodalton gelatinasein abdominal aortic aneurysms. An elasto-lytic metalloproteinase expressed by aneu-rysm-infiltrating macrophages. J Clin Invest.1995;96:318 –326. 10.1172/JCI118037
8. Eliason JL, Hannawa KK, Ailawadi G, Sinha I, FordJW, Deogracias MP, et al. Neutrophil depletioninhibits experimental abdominal aortic aneu-
rysm formation. Circulation. 2005;112:232–240.10.1161/CIRCULATIONAHA.104.517391
9. Xiong W, Zhao Y, Prall A, Greiner TC, BaxterBT. Key roles of CD4� T cells and IFN-gamma in the development of abdominalaortic aneurysms in a murine model. J Im-munol. 2004;172:2607–2612.
10. Majesky MW, Dong XR, Hoglund V, Ma-honey WM, Daum G. The adventitia: a dy-namic interface containing resident pro-genitor cells. Arterioscler Thromb Vasc Biol.2011;31:1530 –1539. 10.1161/ATVBAHA.110.221549
11. Tieu BC, Lee C, Sun H, LeJeune W, RecinosA, Ju X, et al. An adventitial IL-6/MCP1amplification loop accelerates macro-phage-mediated vascular inflammationleading to aortic dissection in mice. J ClinInvest. 2009;119:3637–3651. 10.1172/JCI38308
12. Andreeva ER, Pugach IM, Orekhov AN. Sub-endothelial smooth muscle cells of human
Original Research Article 265
Aorta, December 2013 Volume 1, Issue 6: 259 –267

aorta express macrophage antigen in situand in vitro. Atherosclerosis. 1997;135:19 –27. 10.1016/S0021-9150(97)00136-6
13. Duffield JS. The inflammatory macrophage:a story of Jekyll and Hyde. Clin Sci. 2003;104:27–38. 10.1042/CS20020240
14. Phillipson M, Kubes P. The neutrophil in vas-cular inflammation. Nat Med. 2011;17:1381–1390. 10.1038/nm.2514
15. Abdul-Hussien H, Hanemaaijer R, Verheijen JH,van Bockel JH, Geelkerken RH, Lindeman JH.Doxycycline therapy for abdominal aneurysm:Improved proteolytic balance through re-duced neutrophil content. J Vasc Surg. 2009;49:741–749. 10.1016/j.jvs.2008.09.055
16. Cohen JR, Parikh S, Grella L, Sarfati I, CorbieG, Danna D, et al. Role of the neutrophil inabdominal aortic aneurysm development.Cardiovasc Surg. 1993;1:373–376.
17. Li M, Liu K, Michalicek J, Angus JA, Hunt JE,Dell’Italia LJ, et al. Involvement of chymase-mediated angiotensin II generation in bloodpressure regulation. J Clin Invest. 2004;114:112–120. 10.1172/JCI200420805
18. Tchougounova E, Lundequist A, Fajardo I,Winberg JO, Abrink M, Pejler G. A key role formast cell chymase in the activation of pro-matrix metalloprotease-9 and pro-matrixmetalloprotease-2. J Biol Chem. 2005;280:9291–9296. 10.1074/jbc.M410396200
19. Zhang J, Sun J, Lindholt JS, Sukhova GK,Sinnamon M, Stevens RL, et al. Mast celltryptase deficiency attenuates mouse ab-dominal aortic aneurysm formation. Circ Res.2011;108:1316 –1327. 10.1161/CIRCRESAHA.111.243758
20. Tsuruda T, Kato J, Hatakeyama K, Kojima K,Yano M, Yano Y, et al. Adventitial mast cellscontribute to pathogenesis in the progres-sion of abdominal aortic aneurysm. Circ Res.2008;102:1368 –1377. 10.1161/CIRCRESAHA.108.173682
21. Baram D, Vaday GG, Salamon P, Drucker I,Hershkoviz R, Mekori YA. Human mast cellsrelease metalloproteinase-9 on contact withactivated T cells: juxtacrine regulation byTNF-alpha. J Immunol. 2001;167:4008 –4016.
22. Maiellaro K, Taylor WR. The role of the ad-ventitia in vascular inflammation. Cardiovasc
Res. 2007;75:640 –648. 10.1016/j.cardiores.2007.06.023
23. Zhao L, Moos MP, Gräbner R, Pédrono F, FanJ, Kaiser B, et al. The 5-lipoxygenase pathwaypromotes pathogenesis of hyperlipidemia-dependent aortic aneurysm. Nat Med. 2004;10:966 –973. 10.1038/nm1099
24. Hiraguchi Y, Nagao M, Hosoki K, Tokuda R,Fujisawa T. Neutrophil proteases activate eo-sinophil function in vitro. Int Arch AllergyImmunol. 2008;146 Suppl 1:16 –21. 10.1159/000126055
25. Xu L, Burke A. Acute medial dissection of theascending aorta: evolution of reactive histo-logic changes. Am J Surg Pathol. 2013;37:1275–1282. 10.1097/PAS.0b013e318294adc3
Cite this article as: Wu D, Choi JC, SameriA, Minard CG, Coselli JS, Shen YH, LeMaireSA. Inflammatory Cell Infiltrates in Acuteand Chronic Thoracic Aortic Dissection.Aorta 2013;1(6):259–267. DOI: http://dx.doi.org/10.12945/j.aorta.2013.13-044
EDITOR’S COMMENTS AND QUESTIONS
Editor’s Comments:The authors are to be congratulated on this impor-
tant study, making stronger the link between inflam-mation, aortic aneurysm, and aortic dissection.
Editor’s Questions:
1. Why did you sample only the outer layer inyour dissection patients? We know the dissec-tion occurs in mid-media. Why not sample andexamine the inner layer as well?
We are primarily interested in what drives aorticdilatation after aortic dissection has occurred. Wefocused on the outer wall of the false lumen be-cause this is the region primarily responsible foraneurysm expansion and rupture in patients withdissection, and the region that would be the targetfor pharmacologic treatment designed to preventdilatation after dissection. Changes involving theinner dissecting membrane (or dissection “flap”)would have limited clinical relevance in chronicdissection.2. Is it fair to include a preponderance of de-
scending dissections as your control groupwhen the acute dissections were all ascending?Information is mounting that ascending anddescending dissections are different diseases
(embryology, genetics, morphology, patho-physiology [1,2], so one worries to have a dis-parate control group.
The editor makes a valid point. Our goal was to seewhether the inflammatory response persists inchronic dissection patients. A set of patients withacute descending thoracic aortic dissection wouldbe the ideal and proper controls for the group ofpatients with chronic descending thoracic aorticdissection; however, because it is very rare thatthese patients require open operative intervention,acutely dissected descending thoracic aortic tissuewas not available for analysis. Although we ac-knowledge that acutely dissected aorta is not theideal control, we believe it is a reasonable alterna-tive at this stage, given that the inflammatory re-sponse to the tissue injury caused by acute dissec-tion may be similar in different segments of theaorta, despite differences in underlying embryology,morphology, and pathophysiology; this suppositionwill require investigation.3. You indicate that your controls were organ
donors. Why did they have so much diabetesand stroke?
This was not intentional. Our main inclusion crite-rion for controls was that they had no evidence ofaortic disease. Many of the control subjects weredonors of non-vital organs and tissues. Selecting acontrol group with an age that matched the age of
266 Original Research Article
Wu, D. et al. Inflammatory Cell Infiltrates in TAD

our patient population (�65 yr) resulted in a rela-tively high prevalence of comorbidities.4. Is it fair to say that your hypothesis that chronic
dissection patients would have less inflamma-tion than acute dissection patients was notborne out? Any comments on this?
Our findings did not support our original hypothe-sis. In inflammation, a basic tenet is that after 24-48hours, the predominant inflammatory cell infiltrateis macrophages, which progressively phases outover the next 7-14 days. We were surprised that theentire spectrum of inflammatory cells was presenteven in chronic dissection tissue samples, suggest-ing a sustained active inflammatory response.5. Does the association you show us between
inflammation and dissection inform us aboutcausation? That is to say, which is the chickenand which is the egg? Does the inflammationcome first, or the dissection?
We do not believe our findings provide informa-tion about the role of inflammation in the initia-tion of aortic dissection. Although aortic wallinflammation may certainly be a factor in theinitial intimal/medial tear from which the dissec-tion propagates, we purposely focused on tissuefrom the outer wall of the false lumen distal tothe initial entry site to better understand theinflammatory response to dissection. We view theacute longitudinal splitting of the media as aform of severe vascular wall trauma that wouldbe expected to spark a major acute inflammatoryresponse, and we were particularly interested inhow the inflammatory cell profile might changewhen moving into the chronic phase. Our findingssuggest that a continued inflammatory responsemay contribute to progressive weakening of theouter aortic wall in patients who develop aneu-rysms caused by chronic dissection.
References
1. Elefteriades JA, Farkas EA. Thoracic aortic an-eurysm clinically pertinent controversies anduncertainties. J Am Coll Cardiol. 2010; 55:841–857. 10.1016/j.jacc.2009.08.084
2. Ruddy JM, Jones JA, Ikonomidis JS. Patho-physiology of thoracic aortic aneurysm (TAA):is it not one uniform aorta? Role of embryo-
logic origin. Prog Cardiovasc Dis. 2013; 56:68 –73. 10.1016/j.pcad.2013.04.002
Original Research Article 267
Aorta, December 2013 Volume 1, Issue 6: 259 –267

Modeling the Growth of Infrarenal AbdominalAortic Aneurysms
Marc A. Bailey, BSc, MBChB, MRCS1,2*, Paul D. Baxter, PhD, CStat3, Tao Jiang, MSc3,Aimee M. Charnell, BSc, MBChB1,3, Kathryn J. Griffin, MA, MBBChir, MRCS1,2,Anne B. Johnson, SVN1, Katherine I. Bridge, MBChB, MRCS1,2, Soroush Sohrabi, PhD, MRCS1,D. Julian A. Scott, MD, FRCS, FEBVS1,2
1Multidisciplinary Cardiovascular Research Centre, Division of Cardiovascular and Diabetes Research, The Leeds Institute of Genetics,Health and Therapeutics, The University of Leeds, Leeds, United Kingdom; 2The Leeds Vascular Institute, The General Infirmary atLeeds, Leeds, United Kingdom; and 3The Division of Epidemiology and Biostatistics, The Leeds Institute of Genetics, Health andTherapeutics, The University of Leeds, Leeds, United Kingdom
AbstractBackground: Abdominal aortic aneurysm (AAA) growthis a complex process that is incompletely understood.Significant heterogeneity in growth trajectories be-tween patients has led to difficulties in accurately mod-eling aneurysm growth across cohorts of patients. Weset out to compare four models of aneurysm growthcommonly used in the literature and confirm which bestfits the patient data of our AAA cohort. Methods: Pa-tients with AAA were included in the study if they hadtwo or more abdominal ultrasound scans greater than 3months apart. Patients were censored from analysisonce their AAA exceeded 5.5 cm. Four models wereapplied using the R environment for statistical comput-ing. Growth estimates and goodness of fit (using theAkaike Information Criterion, AIC) were compared, withp-values based on likelihood ratio testing. Results: Of510 enrolled patients, 264 met the inclusion criteria,yielding a total of 1861 imaging studies during 932cumulative years of surveillance. Overall, growth rateswere: (1) 0.35 (0.31,0.39) cm/yr in the growth/time cal-culation, (2) 0.056 (0.042,0.068) cm/yr in the linear re-gression model, (3) 0.19 (0.17,0.21) cm/yr in the linearmultilevel model, and (4) 0.21 (0.18,0.24) cm/yr in thequadratic multilevel model at time 0, slowing to 0.15(0.12,0.17) cm/yr at 10 years. AIC was lowest in thequadratic multilevel model (1508) compared to other
models (P < 0.0001). Conclusion: AAA growth was het-erogeneous between patients; the nested nature of thedata is most appropriately modeled by multilevel mod-eling techniques. Copyright © 2013 Science International Corp.
Key WordsAbdominal aortic aneurysm · Growth rate · Quadratic ·Multilevel modeling
Introduction
An abdominal aortic aneurysm (AAA) is a focal dila-tation of the abdominal aorta, greater than 3 cm indiameter or 1.5 times the diameter of the adjacent nor-mal aorta. In clinical practice and in the UK AAA NationalScreening Programme (http://aaa.screening.nhs.uk),once the infrarenal aorta reaches 3.0 cm in its maximalanteroposterior (AP) diameter, it is classified as aneurys-mal. The event(s) that trigger AAA development remainunknown. Important clinical risk factors include malesex, smoking, hypertension, and a family history of thecondition [1]. Once established, AAA progressivelyevolves toward rupture, which confers high mortality.
Rupture risk is positively associated with aneurysm
Fax �1 203 785 3346E-Mail: [email protected]://aorta.scienceinternational.org
© 2013 Aorta.Published by Science International Corp.ISSN 2325-4637
Accessible online at:http://aorta.scienceinternational.org
*Corresponding author:Marc A. Bailey MBChB, BSc, MRCS, BHF FellowThe Leeds Vascular InstituteThe General Infirmary at LeedsGreat George StreetLeeds LS1 3EX, United KingdomTel: �1 441133923196, Fax: �1 441133922624, E-Mail: [email protected]
Original Research Article
Aorta, December 2013, Volume 1, Issue 6: 268 –273DOI: http://dx.doi.org/10.12945/j.aorta.2013.13-036
Received: July 25, 2013Accepted: December 11, 2013Published online: December 2013

size. Presently, the mainstay of clinical managementinvolves active monitoring, smoking cessation thera-pies, and cardioprotective medication, with prophy-lactic repair once the annual risk of rupture outweighsthe mortality risk of intervention. This interventionthreshold is currently set at 5.5 cm (on abdominalultrasonography) in otherwise fit patients, based onrandomized trial data [2]. Aneurysm screening is ef-fective at reducing mortality from AAA rupture in menand is being increasingly adopted in many developedcountries [3]. The recent report from the RESCAN col-laborators suggests surveillance intervals could besafely increased, with significant cost savings [4].
Aneurysm growth is a complex process that is notnecessarily linear and remains a relatively poorly ex-plored area in the literature. Many authors have notedsignificant heterogeneity in aneurysm growth patternsbetween patients [5–7]. This has led to difficulties inattempts to report pooled growth estimates for patientcohorts [7]. A variety of growth modeling strategies havebeen reported previously [8], but direct comparisonswithin a single-center patient cohort are lacking. Theaims of this study were (1) to compare a range of modelsto estimate aneurysm growth and (2) to confirm themost appropriate modeling strategy for estimatinggrowth in a cohort of patients by testing the goodness-of-fit of each model to data derived from our patientcohort.
Materials and Methods
PatientsConsecutive patients referred to our institution, a university
hospital vascular surgery unit, serving a local population of800,000 in the United Kingdom with a diagnosis of AAA betweenJanuary 1, 2003 and April 31, 2010 were invited to participate inthe Leeds Aneurysm Development Study (LEADS) on a voluntarybasis. The inclusion and exclusion criteria for LEADS have previ-ously been reported [9–11]. Ethical approval was given by theinstitutional ethics committee (Project Reference: 03/142). At re-cruitment, all patients gave written, informed consent and com-pleted a standardized health questionnaire which was adminis-tered face-to-face by a research nurse (A.J.).
ImagingMaximal aortic diameter in the anteroposterior plane was
measured with B mode abdominal ultrasound (USS) using anAcuson Antares scanner (Siemens Healthcare, Malvern PA,USA). Calipers were placed on the outer wall of the sac, pro-ducing outer wall- to-outer wall (OTO) maximal aneurysmdiameter measurements, which reflected departmental prac-
tice during the study period. Scanning intervals were based onthe UK Small Aneurysm Trial [12], arranged by the clinician incharge of the patient’s care. Enrollment in the study had noimpact on normal clinical care. Patients received surveillanceuntil they underwent aortic repair, died, or withdrew from thestudy. Scans performed in our department prior to recruitmentwere also included, with patient consent, and thus the earliestimaging study dates from February 1994. All USS were per-formed by experienced vascular sonographers; variability forthe department has been previously reported [13].
Inclusion and Exclusion CriteriaPatients from LEADS were included in the present study if
they had an infrarenal abdominal aortic aneurysm (defined asan infrarenal aortic diameter � 3 cm or 1.5 times the diameterof the adjacent aorta) and agreed to participate in the study[10,11]. We only included imaging data from patients with twoor more USS performed a minimum of 3 months apart, whilethe aneurysm was � 5.5 cm in maximal diameter for themodeling comparisons. Patient data were censored from theanalysis once the aneurysm exceeded the 5.5 cm interventionthreshold on USS, as it is possible that growth patterns in largeaneurysms, above the intervention threshold, differ from thosebeneath it, and this falls outside the remit of the present study.
StatisticsWe applied four growth models to the data: (1) simple
growth/time analysis, (2) ordinary linear regression model, (3)linear multilevel model (MLM), and (4) quadratic MLM. All modelswere constructed by a biostatistician (P.B., T.J.) using the R envi-ronment for statistical computing (www.R-project.org).
Simple growth/time analysis (1) involved dividing the differ-ence between the first and last aortic diameters (centimeters) bythe length of time between the two measurements (years). Anordinary linear regression model (2) [14] was fitted with aorticdiameter as the response element and time from the initial scanas the predictor. A parametric, linear MLM (3) with two levels andmeasurements nested within patients [15,16] was fitted by fullmaximum likelihood, with aortic diameter as the response ele-ment and time from the initial scan as the fixed predictor. Arandom, normally distributed intercept term and a random, nor-mally distributed slope term were added for each patient. Aquadratic MLM (4) [15,16] was also fitted using the same basicstructure as the linear MLM, with the addition of both a fixedeffect and a random, normally distributed slope term that werequadratic in time (modeled up to 10 years).
Model comparisons were conducted using the Akaike In-formation Criterion (AIC) together with p-values based on like-lihood ratio testing. Lower values of AIC represent a moreparsimonious fit of the model to the data set and provide ameasure of how well the model represents the patient data onwhich it is based. Data are presented as mean (95% confidenceintervals) or mean � standard deviation unless otherwisestated. A p-value �0.05 was set as the predetermined level ofstatistical significance.
Original Research Article 269
Aorta, December 2013 Volume 1, Issue 6: 268 –273

Results
Study PopulationFive hundred and ten patients with AAA were en-
rolled in LEADS during the study period. Of these, 264met the inclusion criteria for the present analysis. Datawere available from 1861 suitable imaging studies formodeling comparison. Each patient contributed anaverage of 7 � 3 USS measurements to the studyduring 932 cumulative years of surveillance (mean3.5 � 2.5 years/patient). The mean aneurysm size atrecruitment to the study was 3.8 � 0.7 cm, increasingto 4.7 � 0.7 cm at the end of the study period. Themean age of the study population was 74 � 2 years atrecruitment; 81% were men. The results of the medicalquestionnaire are provided in Table 1. As expected,there was a high proportion of hypertensive ex-smokers (mean pack years smoked, 43) with a range ofcardiovascular comorbidities. Of these, 197 of 264(74.6%) were receiving antiplatelet therapy, 175 of 264(66.3%) statins, and 181 of 264 (68.6%) at least oneantihypertensive medication (beta blockers, angioten-sin converting enzyme inhibitors, angiotensin II recep-tor antagonists, or calcium channel blockers).
Growth Modeling EstimatesAs expected, aneurysm growth was heterogeneous
across the study population. Illustrative scatter plots ofpatients exhibiting slow, moderate, and rapid aneurysmgrowth are provided in Figure 1. Overall growth esti-
mates for the cohort by model were: (1) simple growth/time model: 0.35 (0.31,0.39) cm/yr, (2) ordinary linearregression model: 0.056 (0.042,0.068) cm/yr, (3) linearMLM: 0.19 (0.17,0.21) cm/yr, and (4) quadratic MLM: 0.21(0.18,0.24) cm/yr, at time zero (see Fig. 2), slowing to 0.15(0.12,0.17) by year 10 (see Fig. 3). The residuals werenormally distributed for models (2), (3), and (4).
Goodness-of-Fit AnalysisIt is not possible to calculate the AIC for the simple
growth/time model (1). For the ordinary linear regres-sion model (2), AIC: 3819. For the linear MLM (3), AIC:1527, P � 0.0001 compared to model (2). For thequadratic MLM (4), AIC: 1508, P � 0.0001 compared tomodel (2) and P � 0.0001 compared to model (3).
Discussion
In this study, we have modeled aneurysm growth ina cohort of 264 patients with infrarenal AAA below or atthe intervention threshold and compared four statisticalmodeling approaches which have been previously usedin the literature. We have demonstrated that the fourdifferent models applied to our data produced hetero-geneous estimates of aneurysm growth.
The simple growth/time calculation produced anoverestimate of growth compared to the MLM esti-mate. We relate this to the observation that the lastscan in the series is more likely to be an overestimate(due to observer variability in measurement) that trig-gered intervention and hence was never corrected byfurther scans. When used as the second of two datapoints to calculate growth, this leads to bias in favor ofoverestimation. It is also possible that negative growthrates could be produced by this method; however, wedid not observe this in our analysis. Further, themethod is significantly weakened by the fact that itignores the majority of the data points (71.6% of datapoints in our study are ignored by this method, forexample). AIC cannot be calculated for this method ofgrowth estimation as there is no statistical modelunderlying the growth process that can be tested.
When applied to our data, an ordinary linear regres-sion model underestimated growth as compared to allother models with heavily autocorrelated residuals.We hypothesize that this may be related to the differ-ences in individual growth trajectories that are atten-uated when trajectories are pooled across patients,coupled with the fact that the model ignores the
Table 1 Clinical Characteristics of the Study Population
n %
Ever smoker 238 90.2Hypertension 157 59.5Peripheral vascular disease 86 32.6Myocardial infarction 69 26.1Current smoker 66 25.0Cerebrovascular disease 53 20.1Diabetes mellitus 37 14.0CABG 28 10.6Family history AAA 16 6.1DVT/PE 15 5.7
Hypertension was defined as a clinical history of the condition or the use of antihy-
pertensive medication. Peripheral vascular disease was defined as a clinical history of
claudication or an ankle-brachial pressure index of � 0.8. Myocardial infarction was
defined as a known clinical history of the condition or q waves on the recruitment
ECG. Cerebrovascular disease included both completed stroke and transient isch-
emic attack. CABG � coronary artery bypass grafting, DVT � deep venous
thrombosis, PE � pulmonary embolism.
270 Original Research Article
Bailey, M.A. et al. AAA Growth Modeling

multilevel structure of these data. Patients with slow-growing AAA tend to have a larger number of scans intotal, which may compound bias in the model towardslow growth. Using a linear regression model doesinclude all data, in contrast to the growth/time calcu-lation, but analyzes all scan data for all patients to-gether. This represents a statistical error; the assump-tions of the model are not met by these data, as scansfrom the same patient are related through growth andthus are not independent, as is required for simple
linear regression analysis. We suggest that this istherefore an invalid method of modeling this type ofdata, the growth estimate of which is completely in-accurate and should be ignored.
In MLM, each patient contributes to the overallgrowth estimate, but an individual regression line ismodeled for each patient. The effects of covariates canthen be added as interactions with the overall growthestimate observed (although this covariate analysisrequires a large number of patients). MLM better rep-resents the correlated nature of these data, and animproved AIC is apparent for the linear MLM as com-
Figure 1. Example growth trajectories of patients with slow growth (left), moderate growth (center), and rapid growth (right).
Figure 2. Comparison plot of growth estimates by model.Each point represents growth estimate with 95% confidenceintervals. Dist. Time � (1) growth/time calculation, Lin. Reg. �(2) ordinary linear regression model, Lin. MLM � (3) linearmultilevel model, Quad. MLM. � (4) quadratic multilevel model(estimate at time zero).
Figure 3. Aneurysm growth estimates for the quadratic mul-tilevel model plotted at annual intervals over a 10 year qua-dratic growth model. Each point represents growth estimatewith 95% confidence intervals.
Original Research Article 271
Aorta, December 2013 Volume 1, Issue 6: 268 –273

pared to a linear regression model. However, a linearMLM still presumes aneurysm growth to be a linearprocess, and this is not necessarily the case [17]. Wetherefore also tested a quadratic basis to the MLM. Inour patient cohort, a quadratic basis to MLM demon-strated a small but significant improvement in AICwhen compared to a linear MLM. Both the linear andquadratic MLM demonstrated significantly improvedAIC compared to the ordinary linear regression model.It is noteworthy that the growth estimate in the qua-dratic MLM slows over time. This is not suggestingthat aneurysm growth slows in individual patients, butrather reflects the observation in the fixed effects partof the model, that patients with slower growing an-eurysms will remain in the cohort for longer timeperiods, whereas those with rapidly growing aneu-rysms will leave the cohort to undergo repair.
Our data support the notion that AAA growth exhibitssignificant variation between patients, is not necessarilylinear, and is more suitably represented by MLM tech-niques. Our AIC data suggest that quadratic as opposedto linear modeling strategies most accurately representthe growth of AAAs within a cohort of patients over time.However, it is difficult to be certain if the quadratic MLMprovides a more accurate growth estimate than a linearMLM or simply better detects the selection effects intro-duced by slow-growing aneurysms persisting in the dataset for a longer time. Our data add weight to the previ-ous work using MLM techniques, and we suggest thatfuture studies aiming to identify factors which may in-fluence growth must use MLM to reach valid conclu-sions. Relatively few groups have previously used MLM[5,18–21], possibly because this requires access to a suit-ably experienced biostatistician, which is not always pos-sible. Reassuringly, the MLM generated growth estimatesfor our patient cohort which were similar to previoushigh-quality reports using large patient numbers withlinear MLM [17,19].
There are clear limitations to this work. We have useda cohort of patients from a single center in the UK. Ourfindings are therefore specific to this cohort of patients,which may differ compared to other AAA patient groupsaround the globe. While the overall sample size wasrelatively small, it was large enough to estimate the fixedeffects of the model [22]. It would have been beneficialto include relevant clinical risk factors for AAA (e.g.,gender, smoking, hypertension) in the model; however,the sample was likely underpowered for looking at in-teraction terms, as would be required for subgroup anal-
ysis, so this was not possible. It is noteworthy that aproportion of patients recruited to the study were ex-cluded from the growth modeling analysis (48%). Thesepatients tended to have an incidental large aneurysmdetected with a single scan that went straight for inter-vention; thus no growth data were available. Anotherproblem is the fact that patients with fast-growing an-eurysms are selected out of the data (to go for interven-tion) and thus have fewer data points included. Jointmodeling [23,24] is an appealing approach to try tobroach this problem, as it would allow correction for thisselection effect. Joint modeling allows the analysis of thedata taking into account both the autocorrelation in therepeated measures as well as the time-to-event outcome(aortic intervention). We chose to censor any measure-ment data from AAAs above the traditional interventionthreshold of 5.5 cm. Very little is known about thegrowth patterns of these large AAAs and it is possiblethat these aneurysms exhibit a growth pattern differentfrom smaller aneurysms which would require an alterna-tive modeling technique. This is an important, separatearea for further study. We also set a minimum standardof scans required to meet inclusion criteria (two or moreUSS which were at least 3 months apart). This approachwas taken to ensure enough data were available toestimate a growth trajectory for each patient. Few pa-tients contributed only the minimum number of scans(n � 16, 6% of the study population), with the averagecontribution being 7 scans per patient. It has been es-tablished that USS aneurysm measurement from innerwall to inner wall (ITI) is more reproducible than OTO[25]. As our study began in 2003, we have used OTOmeasurements for the purposes of the present analysis.The data used for analysis reflect the duration of OTOmeasurement policy in our department. All patients nowreceive ITI measurements as per the UK National AAAScreening Programme (http://aaa.screening.nhs.uk), butnone of these measurements were included in the pres-ent analysis.
Conclusion
AAA growth is a complex process that varies sig-nificantly patient-to-patient. Between 3.0 and 5.5 cm,the heavily nested structure of the data is best repre-sented with multilevel modeling techniques. Furtherwork should focus on joint modeling approaches andon aneurysms above the intervention threshold.
272 Original Research Article
Bailey, M.A. et al. AAA Growth Modeling

Acknowledgments
This work was supported by funding from TheGarfield Weston Trust for Medical Research into Dis-eases of the Heart and The Circulation Foundation(UK). This work was presented at the Society for Aca-demic and Research Surgery Jan 2012, Nottingham,UK and the International Workshop on Statistical Mod-elling July 2013, Palermo, Italy. The authors confirmthat the work is all their own and has not been
submitted for publication or previously published inany other journal. D.J.A.S. is a RESCAN collaborator.No authors have any conflict of interest to declare.M.A.B., K.J.G., and K.I.B. are British Heart Foundationfunded Clinical Research Training Fellows; S.S. is aNational Institute of Health Research funded ClinicalLecturer.
Comment on this Article or Ask a Question
References
1. Vardulaki KA, Walker NM, Day NE, Duffy SW,Ashton HA, Scott RA. Quantifying the risks ofhypertension, age, sex and smoking in pa-tients with abdominal aortic aneurysm. Br JSurg. 2000;87:195–200. 10.1046/j.1365-2168.2000.01353.x
2. Filardo G, Powell JT, Martinez MA, Ballard DJ.Surgery for small asymptomatic abdominalaortic aneurysms. Cochrane Database SystRev. 2012;3:CD001835.
3. Thompson SG, Ashton HA, Gao L, Buxton MJ,Scott RA. Final follow-up of the MulticentreAneurysm Screening Study (MASS) random-ized trial of abdominal aortic aneurysmscreening. Br J Surg. 2012;99:1649 –1656. 10.1002/bjs.8897
4. Bown MJ, Sweeting MJ, Brown LC, Powell JT,Thompson SG. Surveillance intervals forsmall abdominal aortic aneurysms: a meta-analysis. JAMA. 2013;309:806 –813. 10.1001/jama.2013.950
5. Brady AR, Thompson SG, Fowkes FG, Green-halgh RM, Powell JT. Abdominal aortic aneu-rysm expansion: risk factors and time intervalsfor surveillance. Circulation. 2004;110:16–21.10.1161/01.CIR.0000133279.07468.9F
6. Darwood R, Earnshaw JJ, Turton G, Shaw E,Whyman M, Poskitt K, et al. Twenty-yearreview of abdominal aortic aneurysmscreening in men in the county of Glouces-tershire, United Kingdom. J Vasc Surg. 2012;56:8 –13. 10.1016/j.jvs.2011.12.069
7. Dunne JA, Bailey MA, Griffin KJ, Sohrabi S,Coughlin PA, Scott DJ. Statins: the holy grailof abdominal aortic aneurysm (AAA) growthattenuation? A systematic review of the lit-erature. Curr Vasc Pharmacol. 2012.
8. Bailey MA, Charnell AM, Griffin KJ, Czoski-Murray CJ, Sohrabi S, Rashid ST, et al. Asystematic review of the methodology em-ployed to calculate abdominal aortic aneu-rysm (AAA) growth rate. Ultrasound. 2011;19:197–202. 10.1258/ult.2011.011040
9. Bailey MA, Griffin KJ, Sohrabi S, Whalley DJ,Johnson AB, Baxter PD, et al. Plasma throm-bin-antithrombin complex, prothrombinfragments 1 and 2, and D-dimer levels are
elevated after endovascular but not openrepair of infrarenal abdominal aortic aneu-rysm. J Vasc Surg. 2013;57:1512–1518. 10.1016/j.jvs.2012.12.030
10. Parry DJ, Al-Barjas HS, Chappell L, Rashid ST,Ariëns RA, Scott DJ. Markers of inflammationin men with small abdominal aortic aneu-rysm. J Vasc Surg. 2010;52:145–151. 10.1016/j.jvs.2010.02.279
11. Parry DJ, Al-Barjas HS, Chappell L, Rashid T,Ariëns RA, Scott DJ. Haemostatic and fibrino-lytic factors in men with a small abdominalaortic aneurysm. Br J Surg. 2009;96:870 –877.10.1002/bjs.6632
12. Powell J, Brown LC, Forbes JF, Fowkes FG,Greenhalgh RM, Ruckley CV, et al. Final 12-year follow-up of surgery versus surveillancein the UK Small Aneurysm Trial. Br J Surg.2007;94:702–708. 10.1002/bjs.5778
13. Foo FJ, Hammond C, Goldstone A, Abuham-diah M, Rashid S, West R, et al. Agreementbetween computed tomography and ultra-sound on abdominal aortic aneurysms andimplications on clinical decisions. Eur J VascEndovasc Surg. 2011;42:608 –614. 10.1016/j.ejvs.2011.07.003
14. Draper NR, Smith H. Applied regression anal-ysis, 3rd edition. Chichester: Wiley Inter-science. 1998.
15. Goldstein H. Multilevel statistical models,4th edition. Chichester: Wiley Interscience.2011.
16. Pinheiro JC, Bates DM. Mixed-effects modelsin S and S-PLUS. New York: Springer-Verlag.2000.
17. Powell JT, Sweeting MJ, Brown LC, Goten-sparre SM, Fowkes FG, Thompson SG. Sys-tematic review and meta-analysis of growthrates of small abdominal aortic aneurysms.Br J Surg. 2011;98:609 –618. 10.1002/bjs.7465
18. Sweeting MJ, Thompson SG, Brown LC,Greenhalgh RM, Powell JT. Use of angioten-sin converting enzyme inhibitors is associ-ated with increased growth rate of abdom-inal aortic aneurysms. J Vasc Surg. 2010;52:1–4. 10.1016/j.jvs.2010.02.264
19. Sweeting MJ, Thompson SG, Brown LC, Pow-ell JT. Meta-analysis of individual patientdata to examine factors affecting growthand rupture of small abdominal aortic aneu-rysms. Br J Surg. 2012;99:655–665. 10.1002/bjs.8707
20. Thompson A, Cooper JA, Fabricius M,Humphries SE, Ashton HA, Hafez H. An anal-ysis of drug modulation of abdominal aorticaneurysm growth through 25 years of sur-veillance. J Vasc Surg. 2010;52:55-61.e2.
21. Thompson AR, Cooper JA, Ashton HA, HafezH. Growth rates of small abdominal aorticaneurysms correlate with clinical events. Br JSurg. 2010;97:37–44. 10.1002/bjs.6779
22. Bell BA, Morgan GB, Schoeneberger JA, Lou-dermilk BL, Kromrey JD, Ferron JM. Dancingthe sample size limbo with mixed models:how low can you go? SAS Global Forum.Seattle, Washington. 2010;1–11.
23. Diggle PJ, Sousa I, Chetwynd AG. Joint mod-elling of repeated measurements and time-to-event outcomes: the fourth Armitage lec-ture. Stat Med. 2008;27:2981–2998. 10.1002/sim.3131
24. Henderson R, Diggle P, Dobson A. Jointmodelling of longitudinal measurementsand event time data. Biostatistics. 2000;1:465–480. 10.1093/biostatistics/1.4.465
25. Hartshorne TC, McCollum CN, Earnshaw JJ,Morris J, Nasim A. Ultrasound measurementof aortic diameter in a national screeningprogramme. Eur J Vasc Endovasc Surg. 2011;42:195–199. 10.1016/j.ejvs.2011.02.030
Cite this article as: Bailey MA, BaxterPD, Jiang T, Charnell AM, Griffin KJ,Johnson AB, Bridge KI, Sohrabi S, D. Ju-lian A. Scott. Modeling the Growth ofInfrarenal Abdominal Aortic Aneurysms.Aorta 2013;1(6):268–273. DOI: http://dx.doi.org/10.12945/j.aorta.2013.13-036
Original Research Article 273
Aorta, December 2013 Volume 1, Issue 6: 268 –273

Comment on “Modeling the Growth ofInfrarenal Abdominal Aortic Aneurysms” byBailey et al.
Hai Fang, PhD,1 John A. Rizzo, PhD2,3*1China Center for Health Development Studies, Peking University, Beijing, China; 2Stony Brook University, Stony Brook, New York;and 3Aortic Institute at Yale-New Haven Hospital, Yale University School of Medicine, New Haven, Connecticut
Dear Editor:The authors [1] have provided some
interesting results and furthered under-standing of the statistical challenges andappropriate procedures for estimating an-eurysm growth rates. We have learned agreat deal from this study and applaudtheir efforts. But after reviewing their studycarefully, we feel that an exponential mod-eling approach, as applied in some previ-ous research [2,3], is preferable because itmodels a more realistic pattern of aneu-rysm growth, in which growth dependsnot only on duration but on initial aneu-rysm size. The exponential model positsthat the last measured aneurysm size, Al,and the first measured size, Af, are relatedas follows: (1)
Al � Afe�T, (1)
where T � the time between the first andlast tests and � is a coefficient to be esti-mated. This approach is implemented bytaking the natural logarithm of bothsides of Equation 1 and then estimatingby ordinary least squares (OLS), allowingfor no intercept term. This functional re-lationship has the properties that aneu-rysm growth is larger, the greater theinitial aneurysm size and the longer thepatient is followed.
One criticism of this approach is that itdoes not use all available data, such aswhen patients have more than two imag-
ing studies. But if patients have severalmeasured sizes, one may still apply thismethod, taking advantage of these multi-ple measurements to enlarge the samplesize. Suppose, for example, that there arethree measured sizes for the same patientand that we also know the dates for eachmeasurement. One can then obtain twoobservations for this patient. The first ob-servation relates the difference betweenthe 1st and 2nd size to the time betweenthe first and second tests, while the secondrelates the difference between the 2ndand 3rd size to the time between the sec-ond and third tests. For the first observa-tion, the first size can be regarded as Af
and the second size can be regarded as Al,where T is the time between the first andsecond tests according to Equation 1above. For the second observation, thesecond size can be regarded as Af and thethird size can be regarded as Al, where T isthe time between the second and thirdtests. However, this modeling approachmay suffer from the fact that the samepatient appears in the data set more thanonce (Gujarati and Porter 2009). The errorterms in the linear regression will then becorrelated because several error terms arefrom the same patient. A model clusteringthe error terms and controlling for auto-correlation should be applied. Clusteringthe error terms enables us to control forthe correlations between several error
terms from the same patients. Autocorre-lation occurs because the different obser-vations from the same patients are alsocorrelated. For example, the size differ-ence for the first observation is corre-lated with that of the second observationfrom the same patient. This approachusing all available data increases statisti-cal power and precision of the estimates.However, it may exacerbate selection ef-fects. For example, if patients with mul-tiple imaging studies tend to have stable,slow-growing aneurysms while fast-growing aneurysm patients are selectedout for surgery after fewer imaging stud-ies, this approach will overweight theslow-growing aneurysms, biasing growthestimates downward.
In prior correspondence, the authorshave argued that the exponential model isno better than the OLS estimates they pro-vided and which they considered to beinferior to their preferred models; namely,the linear multilevel model (MLM) andquadratic MLM models. The authors alsonoted that they estimated the exponentialmodel, finding that for a person with a 1cm aneurysm, the annual growth would be0.052 cm, increasing to 0.088 cm after 10years. However, this example is misleadingbecause it uses patients with aneurysmsizes that were not in the database. To beenrolled in their study, patients had to
Fax �1 203 785 3346E-Mail: [email protected]://aorta.scienceinternational.org
© 2013 Aorta.Published by Science International Corp.ISSN 2325-4637
Accessible online at:http://aorta.scienceinternational.org
*Corresponding author:John A. Rizzo, PhDProfessor of Preventive Medicine and EconomicsStony Brook UniversityStony Brook, NY, 11794 USATel: �1 631 741 8539, Fax: �1 347 848 0884, E-Mail:[email protected]
Letter to the Editor
Aorta, December 2013, Volume 1, Issue 6: 274 –275DOI: http://dx.doi.org/10.12945/j.aorta.2013.0056
Received: December 1, 2013Accepted: December 17, 2013Published online: December 2013

have an initial aneurysm size � 3 cm or 1.5times the size of the adjacent aorta. Itseems doubtful that more than a few, ifany, patients with an aorta � 1 cm wereincluded in the analysis. It would be morereasonable and informative to apply aneu-rysm sizes actually observed in the data tothe exponential model estimates.
When one does this, their results usingthe exponential model indicate the follow-ing:
Initial Aneurysm Size Annual Growth3 cm 0.16 cm4 cm 0.21 cm5 cm 0.26 cm5.5 cm 0.29 cm
These growth rates are consistent withthe values in their preferred models;namely, the MLM linear and MLM qua-dratic models. But, unlike their models, theexponential approach shows that growthincreases as the aneurysm size is greater,which we believe makes compelling clini-
cal and anatomical sense. Their MLM linearmodel concludes that growth is the sameregardless of aneurysm size, while theMLM quadratic model estimates thatgrowth actually declines over time as theaneurysm is increasing in size. We find thisimplausible and believe it may just betracking a selection effect in the data, e.g.,patients with large unstable aneurysms aredifferentially selected out for surgery, leav-ing a disproportionate share of large aneu-rysm patients whose aneurysms are morestable.
The authors do not include further im-aging studies once a patient has an imag-ing study that measures the aorta as being� 5.5 cm. They note that this is becausegrowth of large aneurysms may be differ-ent. We concur and, in fact, their statementon this point is really an admission thataneurysm growth does depend on aneu-rysm size, most probably with larger aneu-rysms growing faster. But none of theirmodels capture this effect. The exponentialmodeling approach does.
The authors’ decision to exclude fur-ther imaging studies once patients havepassed the size threshold for interventionmay, however, be justifiable on thegrounds that it mitigates selection effects.If patients with large unstable aneurysmsare differentially selected out for surgery,including the remaining large stable aneu-rysms in the study may exacerbate selec-tion effects, and one might erroneouslyestimate that larger aneurysms grow moreslowly. While statistical methods for deal-ing with selection effects are well known inthe literature [4], this would require esti-mating an equation predicting the proba-bility that a patient is selected out for sur-gery in addition to estimating growth. Thedata requirements to implement this selec-tion correction, both in terms of samplesize and variables needed, can be quiteformidable.
Comment on this Article orAsk a Question
References
1. Bailey MA, Baxter PD, Jiang T, Charnell AM,Griffin KJ, Johnson AB, et al. Modeling thegrowth of infrarenal abdominal aortic aneu-rysms. Aorta. 2013;1:268-273. 10.12945/j.aorta.2013.13–056
2. Rizzo JA, Coady MA, Elefteriades JA. Proce-dures for estimating growth rates in thoracicaortic aneurysms. J Clin Epidemiol. 1998;51:747–754. 10.1016/S0895-4356(98)00050-X
3. Coady MA, Rizzo JA, Hammond GL, KopfGS, Elefteriades JA. Surgical interventioncriteria for thoracic aortic aneurysms: astudy of growth rates and complications.Ann Thorac Surg. 1999;67:1922–1926;discussion 1953-1958. 10.1016/S0003-4975(99)00431-2
4. Heckman J. Sample selection bias as a spec-ification error. Econometrica. 1979;47:153–161. 10.2307/1912352
Cite this article as: Fang H, Rizzo JA.Comment on “Modeling the Growth ofInfrarenal Abdominal Aortic Aneurysms” byBailey et al. Aorta 2013;1(6):274–275. DOI:http://dx.doi.org/10.12945/j.aorta.2013.0056
Letter to the Editor 275
Aorta, December 2013 Volume 1, Issue 6: 274 –275

Cardiovascular Collapse During TranscatheterAortic Valve Replacement: Diagnosis andTreatment of the “Perilous Pentad”
Adam El-Gamel, MBBCh, MD, FRCS Ed., FRCS Eng.*
Waikato Hospital, Cardiothoracic Surgery, Auckland University, Hamilton, New Zealand
AbstractTranscatheter aortic valve replacement (TAVR) has, with-out a doubt, brought an unprecedented excitement to thefield of interventional cardiology. The avoidance of a ster-notomy by transfemoral or transapical aortic-valve im-plantation appears to come at the price of some seriouscomplications, including an increased risk of embolicstroke and paravalvular leakage. The technical challengesof the procedure and the complex nature of the high-riskpatient cohort make the learning curve for this procedurea steep one, with the potential for unexpected complica-tions always looming. Although most commonly relatingto vascular access, these complications can also resultfrom prosthesis-related trauma or malposition, or fromunanticipated trauma from the pacing wire or the superstiff wire. Sudden and unexplained hypotension is oftenthe earliest indicator of major complication and mustprompt an immediate and detailed exclusion of five majorpathologies: retroperitoneal bleeding from access siterupture, aortic dissection or rupture, pericardial tampon-ade, coronary ostial obstruction, or acute severe aorticregurgitation. In most cases, these can be dealt withquickly, and by percutaneous means, although open sur-gery may occasionally be necessary. Increased operatorand team experience should make prevention and recog-nition of these catastrophic complications more complete.For this reason, the importance of specific training, suchas that provided by the valve manufacturers throughworkshops and proctorship, cannot be overemphasized.It is essential that all operators, and indeed all membersof the implant team, exert extreme vigilance to the de-
velopment of intraprocedural complications, which couldhave rapid and potentially lethal consequences. Greaterexperience with an improved understanding of theserisks, along with the development of better devices, de-liverable through smaller and less traumatic sheath tech-nology, will undoubtedly improve the safety and, poten-tially, widen the applicability of TAVR in the future.Forthcoming innovations include a newer generation ofthe valves with operator-controlled steerability to facili-tate negotiation of tortuous aortic anatomy, as well asfully retrievable and resheathable devices to accommo-date the events of dislocation or embolization. The factthat Transcatheter aortic valve implantation (TAVI) is newimplies learning from experience but also from mistakes.The TAVI team must be vigilant to recognize and diag-nose intraprocedure severe hypotension. The “perilouspentad” of catastrophic causes must be constantly bornein mind: retroperitoneal bleeding from access site rup-ture, aortic dissection or rupture, pericardial tamponade,coronary ostial obstruction, and acute severe aorticinsufficiency. Copyright © 2013 Science International Corp.
Key WordsTranscatheter aortic valve replacement · Complications ·Aortic valve
Introduction
Transcatheter aortic valve replacement (TAVR) hasbecome a major clinical reality in the management of
Fax �1 203 785 3346E-Mail: [email protected]://aorta.scienceinternational.org
© 2013 Aorta.Published by Science International Corp.ISSN 2325-4637
Accessible online at:http://aorta.scienceinternational.org
*Corresponding author:Adam El-Gamel, MBBCh, MD, FRCS Ed., FRCS Eng.Waikato Hospital, Cardiothoracic Surgery, Auckland UniversityPembroke StreetHamilton 3876, New ZealandTel.: �1 647 839 8899, Fax: �1 647 839 8631, E-Mail: [email protected]
State-of-the-Art Review
Aorta, December 2013, Volume 1, Issue 6: 276 –282DOI: http://dx.doi.org/10.12945/j.aorta.2013.13-027
Received: June 17, 2013Accepted: November 27, 2013Published online: December 2013

patients with severe aortic stenosis who are deemedto be a high or indeed a prohibitive surgical risk [1,2].Current understanding of the likely complications as-sociated with this procedure is rapidly evolving. TAVR-adverse events differ markedly from those related tosurgical intervention.
Awareness of how complications occur may help intheir recognition, management, and ultimately, avoid-ance, thus improving patient outcomes and facilitat-ing the safe application of this novel therapy.
TAVR continues to be associated with the potentialfor serious complications [3,4] including vascular in-jury, stroke, cardiac injury such as heart block, coro-nary obstruction, cardiac or aortic perforation, para-valvular leak, and valve misplacement.
Within this article we review the complications ofTAVR and discuss possible prevention, diagnosis, andmanagement.
Hypotension
Although, most often, relieving aortic stenosis isassociated with spontaneous improvement of left ven-tricular (LV) function and hemodynamics, patientswith severe aortic stenosis may be extremely sensitivehemodynamically. This is particularly true in the pres-ence of coronary artery disease and LV systolic ordiastolic dysfunction. Whatever the primary cause, hy-potension or tachycardia may initiate a downwardspiral of ischemia and severe pump failure. Vasopres-sor agents (phenylephrine or norepinephrine), whichmaintain adequate perfusion pressure, are often help-ful. Chronotropic and inotropic agents should beavoided as they tend to increase myocardial oxygendemands, which may intensify myocardial ischemiaand induce a downward spiral which may not berecoverable without cardiopulmonary bypass [5].
Unexplained severe hypotension should promptconsideration for an immediate diagnostic strategy toidentify and treat the cause [6] (Table 1), which enu-merates the “perilous pentad” of potential cata-strophic sources of hypotension during TAVR . Thischecklist may serve as a useful mental map during theacute hypotensive event.
Retroperitoneal Bleeding from Access Site RuptureThe relatively large diameter of the delivery cathe-
ter, the frequent presence of severe arteriosclerosis,
along with the common factor of patient fragility cancombine to create major vascular problems at theaccess site. Access for the delivery sheath has provento be a major limitation of transarterial TAVR. Earlysystems used 22 gauge to 25 gauge French sheaths(outer diameter 9-10 mm), and in the absence ofadequate screening, the incidence of arterial dissec-tion and perforation was relatively high [6,7].
To determine the feasibility of an arterial approach,careful and meticulous assessment of the arterialtree— using multi-slice computed tomography andangiography—is mandatory. The images should beused to evaluate the presence and severity of arterialaccess pathology and arterial size [8,9].
Minimal lumen diameter, as well as the amountand distribution of atheroma, tortuosity, and calcifica-tion, will determine the risk of vascular injury relatedto sheath insertion. Ideally, the minimal lumen diam-eter should exceed the diameter of the delivery sys-tem.
As a rule, in borderline cases, regarding size orsignificant pathological findings, one should use ac-cess alternatives, which include the apical, subclavian,open iliac, or ascending aorta approaches [9,10]. An-other option in such circumstances is reconstructionof the ilio-femoral axis with stents or grafts. Althougha large body of knowledge exists for the apical pro-cedure, clinically documented experience with otherapproaches is still rapidly growing.
After uncomplicated vascular closure, ilio-femoralangiography should be performed from the contralat-eral femoral access site, which allows rapid identifica-tion and, if necessary, ongoing management of vas-cular complications.
Dissection or perforation of the ilio-femoral arteriesmay occur in the presence of excessively traumaticsheath insertion. Dissection of the ascending or de-scending aorta can similarly occur due to cathetertrauma. Hypotension, hypovolemia, or cardiac tam-ponade are the common clinical scenarios whenever avascular perforation or dissection takes place [11].
Retroperitoneal hemorrhage is one of the dramaticpotential complications of TAVR. Successful manage-ment requires a high level of suspicion should suddenunexplained hypotension occur [12].
When the large arterial sheath is occlusive, perfo-ration may become evident only after sheath removal.Volume expansion and angiographic assessmentshould be performed without delay.
State-of-the-Art Review 277
Aorta, December 2013 Volume 1, Issue 6: 276 –282

Immediate reinsertion of the occlusive sheath overa guide wire or placement of a highly compliant oc-clusion balloon, proximal to the area of suspectedperforation, typically provides rapid and relatively re-liable control of bleeding, allowing time for definitivemanagement [11].
Covered stents or percutaneous endografts mightserve as adequate therapy and should be available inthe catheterization laboratory for prompt interven-tion, although formal surgical repair might be neces-sary.
Aortic Dissection or RuptureUnexplained hypotension after balloon dilation or
valve expansion should prompt echocardiographic orangiographic assessment of the LV outflow tract andaortic root.
Rupture of the aortic annulus can occur follow-ing aortic balloon valvuloplasty or valve deploy-ment. Accurate choice of the valve and balloon size,
avoiding excessive balloon dilation and valve over-sizing, may decrease the likelihood of this uncom-mon but deadly complication. Particular attention isrequired where the annulus and/or subannular tis-sues are markedly calcified or when the root isunusually small [14,15].
These same traumatic forces during forceful ma-nipulation of the aortic root can produce aortic dis-section, with distal propagation from the aortic root.Like aortic rupture, this should be sought and diag-nosed from the intraoperative transesophageal echo-cardiogram. Open surgical correction will usually berequired.
Pericardial TamponadeThe reported incidence of tamponade after TAVR
varies from 0% to 7%. Typically, pericardiocentesis isadequate; however, thoracotomy might be required.The use of a stiff wire with an appropriately shapedcurve and a standard J-curve at the tip is likely to be
Table 1. Causes of Severe Intraoperative Hypotension During TAVR (and Other Less Acute Complications)
Condition Treatment Comment
(1) Retroperitoneal bleeding fromiliac artery access site rupture
Balloon occlusion Precise imaging of access ileofemoral vesselscan decrease the likelihood of thiscomplication
Surgical control
(2) Aortic dissection or rupture Surgical control will likely be necessary,although this scenario is often lethal
Avoid oversizing, overballooning
(3) Pericardial tamponade Pericardial drainage or open surgicalcontrol may be required, depending onscenario
Causes range from RV wire perforation to LVwire perforation, to aortic or LV rupture
(4) Coronary ostial obstruction Percutaneous angioplasty mayoccasionally be of benefit
Components of valve, or, more likely, abulky leaflet atheroma may overlie andocclude a coronary osSurgical conversion is often necessary
(5) Acute severe aorticinsufficiency
A second transcatheter valve may needto be delivered
Usually due to “frozen leaflet”
Surgical conversion may be necessaryApical access site problems Surgical control Late pseudoaneurysm may resultInternal cardiac tears (VSD or LV
to LA fistula)Individualized
Acute mitral insufficiency Surgery may be required From chordal tear during antegrade apicalapproach
Positioning and deploymentproblems
Individualized
Stroke MultifactorialAcute kidney injury MultifactorialConduction disturbances Close monitoring More commonly noted with Medtronic
CoreValve devicePacemaker as neededSuicidal LV Fluid administration
VSD, ventricular septal defect; LV, left ventricle (ventricular); LA, left atrium.
278 State-of-the-Art Review
El-Gamel, A. Complications of Transcatheter Valve Replacement

the best method to avoid perforation of the LV. Rightheart perforation by the transvenous pacemaker isalso possible [14].
Coronary Ostial ObstructionCoronary obstruction may occur if an obstructive
portion of the valve frame, or the sealing cuff, isplaced directly over a coronary ostium; however, thisis exceedingly rare. The presence of open cells over acoronary ostium is well tolerated. Although percuta-neous coronary interventions have been performedsuccessfully after valve implantation, it is likely thatframe struts will prevent or complicate selective cor-onary cannulation.
A greater concern is the possibility of displacing anunusually bulky, calcified native leaflet over a coronaryostium.
The diagnosis of coronary ostial obstruction maybe reflected in the EKG trace or via sudden depressionin left ventricular function on the echocardiogram.The echo may actually demonstrate the displacementof a calcified leaflet onto the coronary os.
Although acute coronary ostial obstruction maywell prove fatal, some cases have been successfullymanaged by immediate percutaneous angioplastyor open bypass surgery. The risk of coronary occlu-sion is low, but difficult to assess, and most likelydepends on the bulkiness of the native leaflets,height of the coronary ostia, and dimensions of thesinus of Valsalva.
Acute Severe Aortic InsufficiencyAcute severe aortic insufficiency after TAVR may
produce hypotension and shock. Diagnosis may besuggested by hypotension and a wide pulse pressureon the arterial trace, with failure to maintain a gooddiastolic pressure after TAVR.
Significant transvalvular regurgitation is rare afterTAVR, and is usually related to acute structural valvefailure. This may include prosthesis rupture or mal-functioning leaflet (“frozen leaflet”), which is rare but,nevertheless, a possible complication after TAVR. De-ployment of a second valve may be necessary. Alter-natively, prompt cardiopulmonary bypass and surgicalvalve replacement may be required to sort out theproblem (see below for a discussion of less severeparavalvular aortic regurgitation).
Other Potential Technical Problems
Apical Access IssuesDirect access to the left ventricular apex is
achieved through an anterior mini- thoracotomy.The most common concern is chest wall discomfortwith the associated potential for respiratory com-promise and prolonged ventilation. Identifying thecardiac apex with transthoracic echo or fluoroscopyin two dimensions allows more direct access with-out the need for rib spreading other than by a softtissue retractor [13].
On completion of the procedure, the apex is re-paired with preinserted pledgeted sutures. A shortburst of rapid ventricular pacing (rate between 130and 140) is used to decrease LV systolic pressureduring tying of these sutures.
Postprocedural low-grade bleeding from the ac-cess site may result in cardiac tamponade and requirefurther repair and prophylactic use of a biologicalglue. A pericardial patch cover can reduce this risk.Management of large tears might require institutionof cardiopulmonary support [12].
Delayed pseudoaneurysm formation at the site ofventricular repair has been reported. Although pseu-doaneurysms might be initially asymptomatic, theyare typically progressive and require surgical interven-tion.
Internal Cardiac TearsA tear created at the level of the valve inflow can
result in either ventricular septal defect or a LV to leftatrial shunt.
Mitral Valve InjuryDuring an antegrade apical approach, a wire can
be passed below a mitral chorda, leading to distor-tion or avulsion of the mitral chordae. This maycause acute mitral regurgitation. Resistance to cath-eter advancement through the ventricle or transientmitral regurgitation assessed by transesophagealechocardiography should alert the operator to thispossibility. Rewiring or use of a balloon flotationcatheter may be considered to avoid subchordalpassage [15].
Surgical treatment may be required if the mitralregurgitation is acute and severe.
State-of-the-Art Review 279
Aorta, December 2013 Volume 1, Issue 6: 276 –282

Positioning and Deployment Problems
Improper PositioningA valve extending excessively into the ventricle or
the aorta may be associated with adverse events suchas mitral insufficiency, arrhythmia, or aortic injury.
Prosthesis embolization immediately after deploy-ment is generally the result of a gross error in posi-tioning or ejection of the device by an effective ven-tricular contraction during deployment.
Embolization to the aorta is well tolerated so longas coaxial wire position is maintained, preventing thevalve from flipping over and obstructing the ante-grade flow. Typically, the valve can be snared or re-positioned with a partially inflated valvuloplasty bal-loon into a stable position in the aorta. A TAVRreattempt is often successful, although an alternativeapproach might be advisable when the reason forinitial failure cannot be identified. Embolization to theLV is far less likely, but in such cases, surgical removalmight be the only option available.
Paravalvular regurgitation, due to incomplete an-nular sealing, is common. Some degree of paravalvularaortic regurgitation is reported in 80-96% of cases. Inmost cases, the degree of regurgitation is trivial ormild. Grade �2� regurgitation is found in 7-24% ofpatients. Although no trial has directly compared theEdwards SAPIEN and Medtronic CoreValve devices, therates of regurgitation reported in the literature seemto be similar for the two devices. Appropriate sizingwith multiple imaging modalities is one way of reduc-ing this problem, which adversely impacts long-termsurvival. Sometimes further ballooning may reduce orabolish the aortic regurgitation.
Paravalvular RegurgitationMild to moderate paravalvular regurgitation usually
does not produce severe, acute hemodynamic de-rangement. During follow-up, regurgitation is moreoften reduced, rather than becoming worse. The im-portance of paravalvular leak has been emphasized inseveral reports in which grade �2� regurgitation hasbeen shown to be an independent predictor of short-and long-term mortality [16].
StrokeNeurological events are generally mulifactorial,
with some related to the procedure. Manipulation of awire and/or large-diameter catheter through the aor-
tic arch, positioning of the device, performance ofballoon aortic valvuloplasty, and inadequate bloodflow to the brain during rapid pacing and devicedeployment are all potential causes of neurologic in-jury. Factors related to the very elderly patient sub-strate, in whom the incidence of atrial fibrillation andatherosclerotic disease is high, contribute to the risk ofperi-procedural cerebrovascular events. Reported inci-dence of clinical stroke in the current literature variesbetween 1.7% and 8.4% [17].
Initially, it was anticipated that stroke associatedwith TAVR occurred during the procedure, but in-depth analysis of this issue has demonstrated a con-tinuous hazard extending beyond the early phase.This hazard was thought to be higher after Transcath-eter aortic valve implantation (TAVI) in comparisonwith surgical aortic valve replacement (SAVR). How-ever, recent data have shown that although the dif-ference is significant in the first 30 days, the latehazard is in fact similar between TAVI and SAVR.
The role of atrial fibrillation as a potential mecha-nism for stroke after TAVI has been emphasized in tworecent reports, which show a fourfold increased risk ofstroke.
There are several embolic protection devices cur-rently under investigation. Reports have not shown aclinical impact on reducing the incidence of overt orsilent neurological events after TAVR.
Acute Kidney InjuryThe incidence of acute kidney injury (AKI), accord-
ing to multiple reports, lies around 7-8%. Many ofthese studies have been consistent in identifyingblood transfusion as a predictor of AKI. Transfusionsare most likely related to bleeding resulting from thevascular access site. The dye load certainly contributesto kidney injury. Predisposing factors include hyper-tension, chronic obstructive pulmonary disease, andabnormal baseline renal function. Toggweller S. et al.reported that TAVR patients who had AKI had signifi-cantly higher in-hospital mortality and worse long-term survival [18,19].
Conduction DisturbancesIt has now been identified that the self-expandable
Medtronic CoreValve system (because of the higher andlonger-lasting radial forces as well as the deeper implan-tation site in the left ventricle outflow tract) has a higherrate of pacemaker requirement than the Edwards SAPIEN
280 State-of-the-Art Review
El-Gamel, A. Complications of Transcatheter Valve Replacement

system. The incidence is higher in patients who have aleft or right bundle branch block prior to implantation.
A recent meta-analysis reported that 28.9% (23-36%) of patients implanted with the MedtronicCoreValve valve and 4.9% (4-6%) of patients im-planted with the Edwards SAPIEN valve will require anew permanent pacemaker [19].
Given the variable timing of the possible occur-rence of high-degree AV block, continuous postpro-cedural ECG monitoring should be performed for atleast 72 hours for those patients considered to be atincreased risk for this complication. Avoiding over-sizing and deep implantation in the outflow tractcan reduce the incidence of this complication [19].
The “Suicidal LV”In rare circumstances, after sudden reversal of
chronic, severe aortic stenosis, the sudden disappear-ance of afterload can permit the hypertrophied leftventricle to contract so forcefully and completely thatit obstructs forward flow. The subvalvular hypertrophyobstructs outflow from the LV. This has been elo-quently termed the “suicidal LV” post-TAVR.
Treatment involves fluid administration and avoid-ance of diuretics.
Conclusion
TAVR has become the standard of care for thosepatients for whom the surgical risk is deemed prohib-itive. TAVR is also emerging as a reasonable alternativefor those selected, operable patients in whom the riskof either mortality or morbidity is “high.” Althoughbleeding and vascular complications are decreasing asTAVR technology improves and continues to miniatur-ize, significant and potentially catastrophic mechani-cal complications may still occur. Having a clear, fo-cused, prepared outlook to the recognition andtreatment of these TAVR-related catastrophes is essen-tial for the care team. This article has provided aframework for such a perspective.
Conflict of Interest
Adam El-Gamel is a proctor and consultant forEdwards Life Science.
Comment on this Article or Ask a Question
References
1. Rodés-Cabau J, Webb JG, Cheung A, Ye J,Dumont E, Feindel CM, et al. Transcatheteraortic valve implantation for the treatmentof severe symptomatic aortic stenosis in pa-tients at very high or prohibitive surgicalrisk: acute and late outcomes of the multi-center Canadian experience. J Am Coll Car-diol. 2010;55:1080 –1090. 10.1016/j.jacc.2009.12.014
2. Lefèvre T, Kappetein AP, Wolner E, Nataf P,Thomas M, Schächinger V, et al. One year fol-low-up of the multi-centre European PARTNERtranscatheter heart valve study. Eur Heart J.2011;32:148–157. 10.1093/eurheartj/ehq427
3. Moussa ID. Complications of transcatheteraortic valve implantation with the Cor-eValve-what have we learned so far? Cathe-terization Cardiovasc Interv. 2010;76:767–768. 10.1002/ccd.22837
4. Zahn R, Gerckens U, Grube E, Linke A, SievertH, Eggebrecht H, et al. Transcatheter aorticvalve implantation: first results from a multi-centre real-world registry. Eur Heart J. 2011;32:198 –204. 10.1093/eurheartj/ehq339
5. Huffmyer J, Tashjian J, Raphael J, Jaeger JM.Management of the patient for transcatheteraortic valve implantation in the perioperative
period. Semin Cardiothorac Vasc Anesth. 2012;16:25–40. 10.1177/1089253211434966
6. Franco A, Gerli C, Ruggeri L, Monaco F. An-aesthetic management of transcatheter aor-tic valve implantation. Ann Cardiac Anaesth.2012;15:54 –63. 10.4103/0971-9784.91484
7. Van Mieghem NM, Tchetche D, Chieffo A,Dumonteil N, Messika-Zeitoun D, van derBoon RM, et al. Incidence, predictors, andimplications of access site complicationswith transfemoral transcatheter aortic valveimplantation. Am J Cardiol. 2012;110:1361–1367. 10.1016/j.amjcard.2012.06.042
8. Ramlawi B, Anaya-Ayala JE, Reardon MJ.Transcatheter aortic valve replacement(TAVR): access planning and strategies.Methodist DeBakey Cardiovasc J. 2012;8:22–25.
9. Alsac JM, Zegdi R, Blanchard D, Achouh P,Cholley B, Berrebi A, et al. Complications of theaccess during aortic valve implantationthrough transfemoral access. Ann Vasc Surg.2011;25:752–757. 10.1016/j.avsg.2010.11.020
10. Etienne PY, Papadatos S, El Khoury E, PietersD, Price J, Glineur D. Transaortic transcathe-ter aortic valve implantation with the Ed-wards SAPIEN valve: feasibility, technicalconsiderations, and clinical advantages. Ann
Thorac Surg. 2011;92:746 –748. 10.1016/j.athoracsur.2011.03.014
11. Nuis RJ, Piazza N, Van Mieghem NM, OttenAM, Tzikas A, Schultz CJ, et al. In-hospitalcomplications after transcatheter aorticvalve implantation revisited according tothe Valve Academic Research Consortiumdefinitions. Catheterization Cardiovasc In-terv. 2011;78:457–467.
12. Vallabhajosyula P, Bavaria JE. Transcatheteraortic valve implantation: complications andmanagement. J Heart Valve Dis. 2011;20:499 –509.
13. Strauch JT, Scherner M, Haldenwang PL,Madershahian N, Pfister R, Kuhn EW, et al.Transapical minimally invasive aortic valveimplantation and conventional aortic valvereplacement in octogenarians. Thorac Car-diovasc Surg. 2012;60:335–342. 10.1055/s-0032-1304538
14. Tchetche D, Van der Boon RM, Dumonteil N,Chieffo A, Van Mieghem NM, Farah B, et al.Adverse impact of bleeding and transfusionon the outcome post-transcatheter aorticvalve implantation: insights from thePooled-RotterdAm-Milano-Toulouse In Col-laboration Plus (PRAGMATIC Plus) initiative.
State-of-the-Art Review 281
Aorta, December 2013 Volume 1, Issue 6: 276 –282

Am Heart J. 2012;164:402–409. 10.1016/j.ahj.2012.07.003
15. Webb JG, Wood DA. Current status of trans-catheter aortic valve replacement. J Am CollCardiol.2012;60:483–492.10.1016/j.jacc.2012.01.071
16. Sponga S, Perron J, Dagenais F, MohammadiS, Baillot R, Doyle D, et al. Impact of residualregurgitation after aortic valve replacement.Eur J Cardiothorac Surg. 2012;42:486 –492.10.1093/ejcts/ezs083
17. Nombela-Franco L, Webb JG, de Jaegere PP,Toggweiler S, Nuis RJ, Dager AE, et al. Timing,predictive factors, and prognostic value ofcerebrovascular events in a large cohort ofpatients undergoing transcatheter aortic valveimplantation. Circulation. 2012;126:3041–3053. 10.1161/CIRCULATIONAHA.112.110981
18. Salem JE, Paul JF, Caussin C. Transfemoralaortic valve implantation in a renal trans-plant patient with a Dacron aorto-bi-iliacbypass. J Invasive Cardiol. 2012;24:667–670.
19. Toggweiler S, Webb JG. Challenges in trans-catheter aortic valve implantation. SwissMed Wkly. 2012;142:w13735. 10.4414/smw.2012.13735
Cite this article as: El-Gamel A. Cardio-vascular Collapse During TranscatheterAortic Valve Replacement: Diagnosis andTreatment of the “Perilous Pentad”.Aorta 2013;1(6):276 –282. DOI: http://dx.doi.org/10.12945/j.aorta.2013.13-027
EDITOR’S COMMENTS AND QUESTIONS:
Editor’s Comments:This excellent article by Dr. El-Gamel provides a
clear diagnostic and therapeutic approach for cata-strophic complications, which can occur during orimmediately after TAVI. Having this clear diagnosticand therapeutic map in mind is likely to save lives. Thisarticle is recommended for all teams starting or per-forming TAVI.
Editor’s Questions:As the indication for TAVI has classified the patients
into two different groups—the first being the inoperableAS patients and the second group being the high-riskoperable surgical patients, the team has to make anindividual call before the procedure if surgical interven-tion has a place in an individual patient; it makes nosense to perform an emergency procedure on a patientwho was rejected for an elective operation (inoperablepatient). It is imperative that the Heart Team, the pa-tient, and the patient’s family are aware of the limit tothe extent of surgery that will be offered in the event ofa significant complication. For example, we feel thatredo sternotomy and repair of a type A dissection in anonagenarian is inappropriate and would not be under-taken. Prevention of complications required during TAVIappears to be of critical importance. As the outcome ofemergency surgical intervention offers poor outcome,this should be discussed at length with all parties and
then documented in the patient’s file prior to the proce-dure.
1. Is it worth operating for rupture of the aorticroot from TAVI? Is there any meaningfulchance of salvage?
Reported 30-day mortality of TAVI complicationsneeding surgical intervention from the Europeansource registry was high (51.9%) and showed cause-specific differences, with 100% mortality in patientswith aortic rupture or cardiac tamponade, 0%death in those with acute aortic regurgitation, andintermediate risk of death or intermediate mortalityrisk in those with aortic injury or valve emboliza-tion/migration. So the experience and data do notsupport surgery for aortic or cardiac rupture.2. Is it worth operating for non-ruptured aortic
dissection occurring during TAVI?The decision to operate on acute dissection is com-plicated by the patient characteristics, pervious op-eration, and age. For example, we feel that redosternotomy and repair of a type A dissection in anonagenarian is inappropriate and would not beundertaken. However, an 80-year-old with no pre-vious history of cardiac surgery, considered opera-ble but high risk for conventional surgery, may beoffered surgical repair.3. Is it worth operating for coronary ostial occlu-
sion occurring during TAVI?Operating for coronary occlusion and aortic incom-petence has the best outcomes, so surgery shouldbe offered in the operable patients who are ac-cepted for TAVI.
282 State-of-the-Art Review
El-Gamel, A. Complications of Transcatheter Valve Replacement
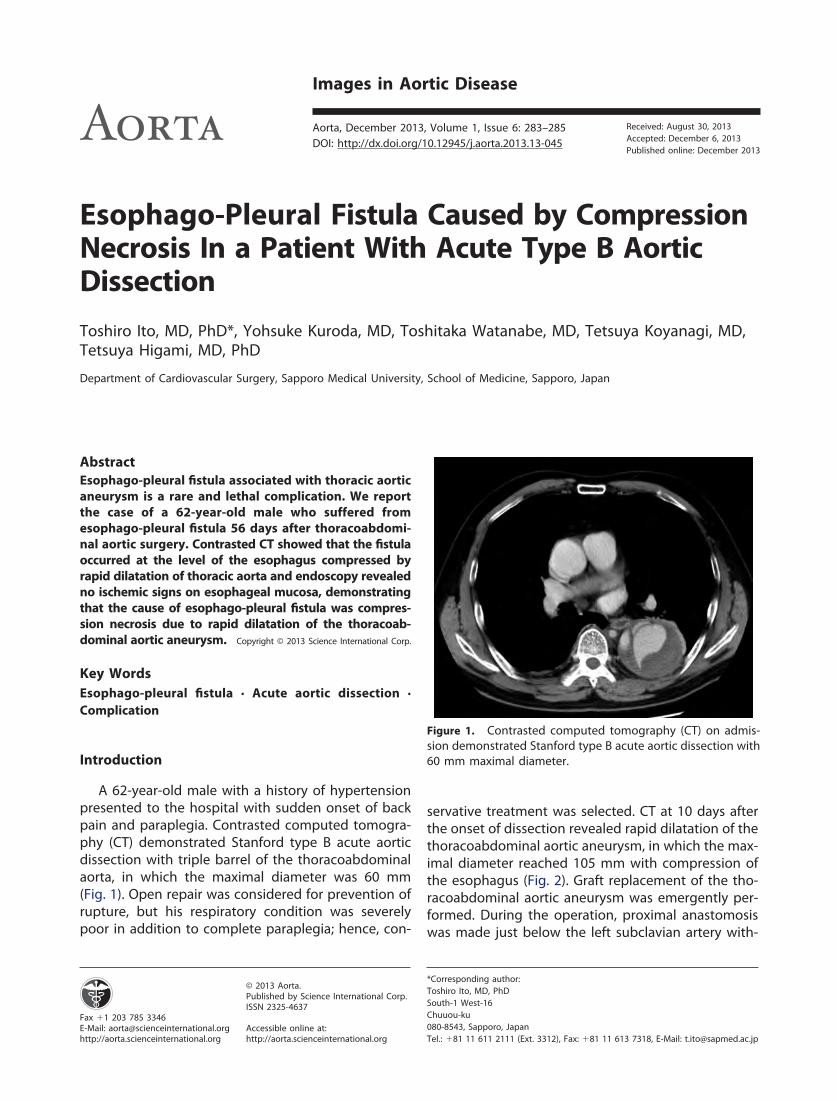
Esophago-Pleural Fistula Caused by CompressionNecrosis In a Patient With Acute Type B AorticDissection
Toshiro Ito, MD, PhD*, Yohsuke Kuroda, MD, Toshitaka Watanabe, MD, Tetsuya Koyanagi, MD,Tetsuya Higami, MD, PhD
Department of Cardiovascular Surgery, Sapporo Medical University, School of Medicine, Sapporo, Japan
AbstractEsophago-pleural fistula associated with thoracic aorticaneurysm is a rare and lethal complication. We reportthe case of a 62-year-old male who suffered fromesophago-pleural fistula 56 days after thoracoabdomi-nal aortic surgery. Contrasted CT showed that the fistulaoccurred at the level of the esophagus compressed byrapid dilatation of thoracic aorta and endoscopy revealedno ischemic signs on esophageal mucosa, demonstratingthat the cause of esophago-pleural fistula was compres-sion necrosis due to rapid dilatation of the thoracoab-dominal aortic aneurysm. Copyright © 2013 Science International Corp.
Key WordsEsophago-pleural fistula · Acute aortic dissection ·Complication
Introduction
A 62-year-old male with a history of hypertensionpresented to the hospital with sudden onset of backpain and paraplegia. Contrasted computed tomogra-phy (CT) demonstrated Stanford type B acute aorticdissection with triple barrel of the thoracoabdominalaorta, in which the maximal diameter was 60 mm(Fig. 1). Open repair was considered for prevention ofrupture, but his respiratory condition was severelypoor in addition to complete paraplegia; hence, con-
servative treatment was selected. CT at 10 days afterthe onset of dissection revealed rapid dilatation of thethoracoabdominal aortic aneurysm, in which the max-imal diameter reached 105 mm with compression ofthe esophagus (Fig. 2). Graft replacement of the tho-racoabdominal aortic aneurysm was emergently per-formed. During the operation, proximal anastomosiswas made just below the left subclavian artery with-
Fax �1 203 785 3346E-Mail: [email protected]://aorta.scienceinternational.org
© 2013 Aorta.Published by Science International Corp.ISSN 2325-4637
Accessible online at:http://aorta.scienceinternational.org
*Corresponding author:Toshiro Ito, MD, PhDSouth-1 West-16Chuuou-ku080-8543, Sapporo, JapanTel.: �81 11 611 2111 (Ext. 3312), Fax: �81 11 613 7318, E-Mail: [email protected]
Figure 1. Contrasted computed tomography (CT) on admis-sion demonstrated Stanford type B acute aortic dissection with60 mm maximal diameter.
Images in Aortic Disease
Aorta, December 2013, Volume 1, Issue 6: 283–285DOI: http://dx.doi.org/10.12945/j.aorta.2013.13-045
Received: August 30, 2013Accepted: December 6, 2013Published online: December 2013

out aortic clamping under deep hypothermic circula-tory arrest. Distal anastomosis was made just abovethe renal arteries in the retroperitoneal space. Recon-struction of the intercostal arteries was not done be-cause of preoperative paraplegia. Although leftrecurrent laryngeal nerve paralysis occurred as acomplication, the operation was successful. The pa-tient underwent rehabilitation up until dischargewhile on nasal tube feeding. At 39 days postopera-tively, spiking fever occurred a few times per day.White blood cell count and C-reactive protein levelwere 7500 � 103/�L and 9.97 mg/dL, respectively.Pseudomonas aeruginosa was cultured from blood, butthere was no obvious focus of infection identified onCT. Antibiotic treatment was initiated, and spikingfever gradually abated. Antibiotic treatment was con-tinued for prophylaxis of graft infection. At 56 dayspostoperatively, contrasted CT as part of periodic in-spection revealed pleural abscess around the vascularprosthesis, and perforation of the esophagus was sus-pected (Fig. 3). Endoscopy demonstrated the vascularprosthesis through a large esophago-pleural fistula(Fig. 4). The patient underwent emergent video-assisted thoracoscopic esophagectomy and thoracicdrainage. Cervical salivary fistula was then establishedby use of the oral end of the esophagus, and anenteral feeding tube was placed in the jejunum. Afterthe operation, intrathoracic irrigation from the tho-racic tube was performed and antibiotic treatment
was maintained. However, Pseudomonas aeruginosawas again detected in the culture of thoracic drainage.We recommended performing a graft replacement ofthe infected vascular prosthesis with omental plom-bage, but his family did not consent. He suffered fromsepsis due to infection of the vascular prosthesis anddied at 4 months after the surgery.
Figure 2. CT at 10 days after the onset of dissection demon-strated compression of the esophagus by the aortic aneurysmwith 105 mm diameter (white arrow).
Figure 3. Postoperative contrasted CT at 56 days revealedpleural abscess around the vascular prosthesis, and perforationof the esophagus was suspected (white arrow).
Figure 4. Endoscopy demonstrated the large esophago-pleural fistula.
284 Images in Aortic Disease
Ito, T. et al. Esophago-Pleural Fistula In Acute Aortic Dissection

This case is our experience of a large esophago-pleural fistula in a patient with acute Type B aorticdissection. The causes of the esophago-pleural fistulawere not believed to be due to surgical trauma duringthe operation or mechanical stimulation of the vascu-lar prosthesis. Surgical procedures which could inducedamage to the esophagus, such as resection of theaortic wall, aortic clamping, and reconstruction of theintercostal arteries, were not performed, and the vas-cular prosthesis was not in contact with the fistula asdemonstrated by postoperative CT. Esophageal isch-emia due to malperfusion may have influenced theperforation of the esophagus. However, endoscopydid not show necrotic or ulcerated esophageal mu-cosa around the fistula. Therefore, it is considered thatthe cause of the esophago-pleural fistula was the
compression necrosis due to rapid dilatation of the tho-racoabdominal aortic aneurysm. A small esophago-pleural fistula occurred on the 39th postoperative daywhen spiking fever appeared. However, it was discov-ered only after the fistula became large because infec-tion was controlled initially by nasal tube feeding andappropriate antibiotic treatment.
Comment on this Article or Ask a Question
Cite this article as: Ito T, Kuroda Y, Watanabe T, Koyanagi T,Higami T. Esophago-Pleural Fistula Caused by Compression Ne-crosis In a Patient With Acute Type B Aortic Dissection. Aorta 2013;1(6):283–285. DOI: http://dx.doi.org/10.12945/j.aorta.2013.13-045
EDITOR’S QUESTIONS
1. Did you consider intervening initially with fen-estration or endograft to try to reverse theparaplegia?
No, I didn’t. Actually, when he was admitted to ourhospital, 8 hours had passed since the paraplegia hadoccurred. Then, cerebrospinal fluid drainage was per-formed for 72 hours, but the paraplegia was notrecovered.
2. You intervened at ten days to replace theaorta, so the native aorta was then �depressur-ized�. How, then, could the aortic wall producepressure to result in esophageal necrosis?
There are some possibilities that could cause perfo-ration of the esophagus such as rupture of the aneurysmto the esophagus, surgical trauma during the operation,esophageal necrosis due to malperfusion, or compres-
sion necrosis due to rapid dilatation of the aneurysm.During the operation, there were no signs of aneurys-mal rupture. On the other hand, any surgical proce-dure which could induce damage to the esophagus,such as resection of the aortic wall, aortic clamping,and reconstruction of the intercostal arteries, was notperformed. Therefore, it is not considered that thecause of esophageal perforation was the rupture tothe esophagus from the surgical trauma. It is possiblethat esophageal ischemia due to malperfusion mayhave influenced the perforation of the esophagusbecause the intrathoracic esophagus is mainly sup-plied by the intercostal arteries which were occludedby the thrombosed false lumen of aortic dissection.However, endoscopy did not show necrotic or ulcer-ated esophageal mucosa around the fistula. There-fore, it is considered that the cause of esophagealperforation was the compression necrosis due to rapiddilatation of the thoracoabdominal aortic aneurysm.
Images in Aortic Disease 285
Aorta, December 2013 Volume 1, Issue 6: 283–285

Finger-Thumb Technique for Elephant TrunkRetrieval
Bulat A. Ziganshin, MD, John A. Elefteriades, MD*
Aortic Institute at Yale-New Haven Hospital, Yale University School of Medicine, New Haven, Connecticut, USA
AbstractIn this report we present a brief video illustrating the“Finger-Thumb Technique” that we have used extensivelyat our institution for elephant trunk retrieval during sec-ond stage elephant trunk procedures. Although only safein experienced hands, this technique is a viable option inthe arsenal of a cardiothoracic surgeon, especially in caseswhen proximally surrounding a massively enlarged aortais unappealing. Copyright © 2013 Science International Corp.
Key WordsDescending aorta · Thoracic aortic aneurysm · Surgi-cal treatment · Stage II elephant trunk procedure
Staged open surgical treatment of aneurysms ofthe aortic arch and descending aorta was first de-scribed by Borst [1], and then modified by Crawford[2] and Svensson [3]. The essence of the two-stageprocedure is in the “elephant trunk” graft that isinserted into the descending aorta during arch re-placement surgery. The elephant trunk graft is lefthanging in the lumen of the descending aorta inanticipation of the second stage intervention (per-formed usually a few weeks or months later), duringwhich another graft will be attached to this elephanttrunk. Anastomosing the descending aortic graft to thepreplaced elephant trunk is often preferable to anasto-mosing to a dilated distal aortic arch under deep hypo-thermic arrest. Identifying and retrieving the elephanttrunk graft safely during the second stage intervention iskey to making this operation successful, perhaps itsmost critical step. Retrieval of the elephant trunk for
performance of a Stage II procedure is not trivial, espe-cially because the elephant trunk is often left short, inorder to discourage paraplegia due to coverage of manypairs of intercostal arteries. Often the elephant trunkterminates just beyond the aortic arch.
There are several technical options for elephanttrunk retrieval:
1. The aorta and the contained elephant trunkcan be surrounded above the terminus of theelephant trunk as described previously [3].However, this is not entirely benign, as theaorta may be very large at that level and therewill be local inflammation from the Stage Iprocedure. Aortic, esophageal, or recurrent la-ryngeal injury may be incurred.
2. A second alternative is that the entire proce-dure may be done under deep hypothermiccirculatory arrest (DHCA), but that defeats therationale of the elephant trunk procedure,which is meant to facilitate conduct of Stage II.Once the elephant trunk is safely controlled,there is no need for any DHCA.
3. A third alternative is to use high-dose adenosine[4,5] (or rapid ventricular pacing) to producetransient cardiac standstill, during which theaorta may be opened without exsanguination.
4. The Finger-Thumb technique.In this report we present the fourth alternative,
illustrated in this brief video (http://dx.doi.org/10.12945/j.aorta.2013.13.064.vid.01). We call this tech-nique the “Finger-Thumb” technique. As the nameimplies, the index finger and the thumb enter the
Fax �1 203 785 3346E-Mail: [email protected]://aorta.scienceinternational.org
© 2013 Aorta.Published by Science International Corp.ISSN 2325-4637
Accessible online at:http://aorta.scienceinternational.org
*Corresponding author:John A. Elefteriades, MDAortic Institute at Yale-New Haven HospitalYale University School of Medicine330 Cedar Street, Boardman Building 204New Haven, CT 06510 (USA)Tel: �1 203 785 2551, Fax: �1 203 785 3346, E-Mail: [email protected]
How I Do It
Aorta, December 2013, Volume 1, Issue 6: 286 –288DOI: http://dx.doi.org/10.12945/j.aorta.2013.13-064
Received: December 1, 2013Accepted: December 17, 2013Published online: December 2013

Figure 1. Illustrated is the transesophageal echocardiogra-phy-guided approach to the elephant trunk graft. Please notethe location of the recurrent laryngeal nerve, which can beinjured while encircling the proximal descending aorta.
Figure 2. Schematic illustration of elephant trunk graft re-trieval in preparation for clamping.
Figure 3. Intraoperative transesophageal echocardiography image showing the elephant trunk graft (indicated by red arrow)in the lumen of the descending aorta. Transesophageal and direct epi-aortic echocardiography confirm appropriate location ofthe incision for the Finger-Thumb technique.
How I Do It 287
Aorta, December 2013 Volume 1, Issue 6: 286 –288
descending aorta via a small vertical incision on theaorta and locate and retrieve the elephant trunk graftby direct palpation (Fig. 1 and Fig. 2). We alwaysidentify the end of the elephant trunk by intraopera-tive transesophageal and epi-aortic echocardiography(Fig. 1 and Fig. 3), so that an incision in the aorta canbe made at the ideal level.
Here are a few practical tips that we would like toshare:
● There is no margin for error, as the patient canexsanguinate in seconds if this procedure goesawry.
● The graft may adhere to the wall of the aorta,making identification and retrieval more diffi-cult. It can be teased away during Finger-Thumb retrieval process.
● In dissection cases, one must be certain to
explore for the graft in the true lumen (theaorta will have been fenestrated as far as pos-sible during Stage I).
● When the aorta is ultimately opened after con-trol of the elephant trunk, high intercostal ar-teries may be hard to identify if they originateat the top of the elephant trunk.
In conclusion, we believe that the “Finger-Thumb”is an extremely useful technique for elephant trunkretrieval during a second stage procedure. Althoughonly safe in experienced hands, this technique is aviable option in the arsenal of a cardiothoracic sur-geon, especially in cases when proximally surroundinga massively enlarged aorta is unappealing.
Comment on this Article or Ask a Question
References
1. Borst HG, Walterbusch G, Schaps D. Extensiveaortic replacement using “elephant trunk”prosthesis. Thorac Cardiovasc Surg. 1983;31:
37–40. 10.1055/s-2007-10202902. Crawford ES, Coselli JS, Svensson LG, Safi HJ,
Hess KR. Diffuse aneurysmal disease (chronicaortic dissection, Marfan, and mega aorta syn-dromes) and multiple aneurysm. Treatmentby subtotal and total aortic replacement em-phasizing the elephant trunk operation. AnnSurg. 1990;211:521–537. 10.1097/00000658-199005000-00002
3. Svensson LG. Rationale and technique for re-placement of the ascending aorta, arch, anddistal aorta using a modified elephant trunkprocedure. J Cardiac Surg. 1992;7:301–312.10.1111/j.1540-8191.1992.tb01020.x
4. Plaschke K, Bockler D, Schumacher H, MartinE, Bardenheuer HJ. Adenosine-induced car-diac arrest and EEG changes in patients withthoracic aorta endovascular repair. Br J An-aesth. 2006;96:310 –316. 10.1093/bja/ael002
5. El-Menyar A, Gehani A. Adenosine-inducedtachyarrhythmia and cardiac arrest. FutureCardiol. 2010;6:433–436. 10.2217/fca.10.66
Cite this article as: Ziganshin BA,Elefteriades JA. Finger-Thumb Tech-nique for Elephant Trunk Retrieval.Aorta 2013;1(6):286 –288. DOI: http://dx.doi.org/10.12945/j.aorta.2013.13-064
288 How I Do It
Ziganshin, B.A. et al. Finger-Thumb Technique for Elephant Trunk Retrieval

Upcoming Meetings
February 2014
1. 43rd Annual Meeting of the German Societyfor Thoracic and Cardiovascular SurgeryFebruary 9 –12, 2014Messe Freiburg, GermanyMeeting information available at:www.dgthg-jahrestagung.de/
March 2014
1. Aortic Valve Repair: A Step by Step ApproachMarch 6 –7, 2014Paris, FranceMeeting information available at:www.caviaar.com
2. The Houston Aortic Symposium: Frontiers inCardiovascular Diseases, the Seventh in theSeriesMarch 6 – 8, 2014Houston, TexasMeeting information available at:www.promedicacme.com
3. Advanced Module: Open and EndovascularAortic TherapyMarch 19 –21, 2014Windsor, United KingdomMeeting information available at:www.eacts.org/academy/2014-program/
April 2014
1. American Association for Thoracic SurgeryAortic SymposiumApril 24 –25, 2014New York, New YorkMeeting information available at:www.aats.org/aortic
2. American Association for Thoracic Surgery An-nual Meeting 2014April 26 –30, 2014Toronto, CanadaMeeting information available at:www.aats.org/annualmeeting/
3. 61st Annual Conference of the Israel HeartSocietyApril 30 –May 1, 2014Tel-Aviv, IsraelMeeting information available at:http://en.israelheart.com/
Upcoming Meetings
Aorta, December 2013, Volume 1, Issue 6: 289DOI: http://dx.doi.org/10.12945/j.aorta.2013.13-063
Received: November 29, 2013Accepted: November 29, 2013Published online: December 2013