Ocular Trauma - Emergency Care and Management
6
- Fatures _ Bruce D. Nichols Ocular Trauma: Emergency Care and Management SUMMARY The emergency care and management of patients with ocular trauma can often be handled completely by the family physician, whose goal should be recognizing the nature and circumstance of the injury and subsequent decision making based on the inutial management steps. Obtaining a careful and thorough patient history is vital, as unsuspected trauma may be looked for based on historical dues. The initial examination is similarly crucial for determining the extent of the injury and for fornulating the treatment plan. Vety often, early and effective first-aid care can prevent future complications, which could otherwise lead to subsequent deterioration of the eye. (Can Fam Physician 1986; 32:1466-1471.) SOMMAIRE II est possible au medecin de famille de traiter en urgence et de facon complete les patients qui presentent un traumat-isme oculaire. L'objectif devient alors de reconnaitre la nature et les circonstances de la blessure et de prendre une decision sur la foi des premieres etapes du traitement. II est vital d'obtenir un dossier minutieux et complet du patient car celui-ci peut revdler un traumatisme insoupconne. II en est de meme de 1'examen initial destine a preciser l'extension d'une blessure et A formuler un plan de traitement. II arrive trbs souvent que des premiers soins precoces et efficaces puissent prevenir des complications futures; dans le cas contraire, il y aurait danger de d6t6rioration ult6rieure et de perte de l'oeil. Key words: ocular trauma, eye, ophthalmology .1 Dr. Nichols, a certificant of the College, was chief resident in the Department of Ophthalmology, University Hospital, University of Saskatchewan, Saskatoon, at the time of writing. He is currently undertaking a fellowship in corneal transplantation and anterior segment surgery at the University of Minnesota, Minneapolis, Minnesota. Reprint requests to: Department of Ophthalmology, University of Minnesota, Box 493, Mayo Memorial Building, 516 Delaware St. South East, Minneapolis, MN. U.S.A. 55455. T HE INCIDENCE OF ocular trauma is relatively common de- spite the anatomic and functional pro- tective mechanisms of the visual sys- tem.' The orbital rim prevents many direct injuries from affecting the eye, and reflex closure of the lids aids in insulating the globe. The upward rota- tion of the eye in response to a sudden stimulus and the cushioning effect of the retrobulbar fat also act as protec- 1486 tion. In spite of these facts and the great strides in the development of protective eye wear, the incidence of eye injuries remains high. Ocular History As with all injuries to the body, knowing the circumstances and subse- quent events under which an eye injury occurred is important for therapeutic decision making and for possible legal implications. The information required to document the patient's ocular his- tory is listed in Table 1. This informa- tion alone will often direct the physi- cian to examine specific anatomic areas or to check for specific func- tional deficits based on the situation and type of injury. It is very important to ask the patient about the health of the eye before the injury and to ask if the visual acuity has changed. Examination The visual acuity in each eye needs to be accurately tested and recorded before any treatment begins. If a Snel- len chart is unavailable, or if the pa- tient is confined to bed, a test card may be used to assess the near visual acuity. Ideally, the patient who wears glasses should wear them if they are available and not broken; however, if this is not possible, the pinhole acuity should be measured. If the patient is in pain, and especially if blepharospasm has occurred, a topical anesthetic such as proparacaine 0. 5% (Ophthaine) Table I Ocular History 1. When, where, how and with what did the injury occur? 2. Severity and duration of presenting complaint. 3. Symptoms (change in visual acuity). 4. Previous eye disease, injury, surgery. 5. Systemic diseases. 6. History of tetanus immunization. 7. Medications (including any eye drops). 8. Allergies. 9. Recent food and fluid intake (if general anesthesia is being considered). CAN. FAM. PHYSICIAN Vol. 32: JULY 1986
-
Upload
yogo-prabowo -
Category
Documents
-
view
218 -
download
0
description
j
Transcript of Ocular Trauma - Emergency Care and Management

- Fatures _Bruce D. Nichols
Ocular Trauma:Emergency Care and ManagementSUMMARYThe emergency care and management ofpatients with ocular trauma can often behandled completely by the family physician,whose goal should be recognizing the natureand circumstance of the injury andsubsequent decision making based on theinutial management steps. Obtaining a carefuland thorough patient history is vital, asunsuspected trauma may be looked for basedon historical dues. The initial examination issimilarly crucial for determining the extent ofthe injury and for fornulating the treatmentplan. Vety often, early and effective first-aidcare can prevent future complications, whichcould otherwise lead to subsequentdeterioration of the eye. (Can Fam Physician1986; 32:1466-1471.)
SOMMAIREII est possible au medecin de famille de traiter enurgence et de facon complete les patients quipresentent un traumat-isme oculaire. L'objectifdevient alors de reconnaitre la nature et lescirconstances de la blessure et de prendre unedecision sur la foi des premieres etapes dutraitement. II est vital d'obtenir un dossier minutieuxet complet du patient car celui-ci peut revdler untraumatisme insoupconne. II en est de meme de1'examen initial destine a preciser l'extension d'uneblessure et A formuler un plan de traitement. IIarrive trbs souvent que des premiers soins precoceset efficaces puissent prevenir des complicationsfutures; dans le cas contraire, il y aurait danger ded6t6rioration ult6rieure et de perte de l'oeil.
Key words: ocular trauma, eye, ophthalmology
.1
Dr. Nichols, a certificant of theCollege, was chief resident in theDepartment of Ophthalmology,University Hospital, University ofSaskatchewan, Saskatoon, at thetime of writing. He is currentlyundertaking a fellowship in cornealtransplantation and anteriorsegment surgery at the Universityof Minnesota, Minneapolis,Minnesota. Reprint requests to:Department of Ophthalmology,University of Minnesota, Box 493,Mayo Memorial Building, 516Delaware St. South East,Minneapolis, MN. U.S.A. 55455.
T HE INCIDENCE OF oculartrauma is relatively common de-
spite the anatomic and functional pro-tective mechanisms of the visual sys-tem.' The orbital rim prevents manydirect injuries from affecting the eye,and reflex closure of the lids aids ininsulating the globe. The upward rota-tion of the eye in response to a suddenstimulus and the cushioning effect ofthe retrobulbar fat also act as protec-
1486
tion. In spite of these facts and thegreat strides in the development ofprotective eye wear, the incidence ofeye injuries remains high.
Ocular HistoryAs with all injuries to the body,
knowing the circumstances and subse-quent events under which an eye injuryoccurred is important for therapeuticdecision making and for possible legalimplications. The information requiredto document the patient's ocular his-tory is listed in Table 1. This informa-tion alone will often direct the physi-cian to examine specific anatomicareas or to check for specific func-tional deficits based on the situationand type of injury. It is very importantto ask the patient about the health ofthe eye before the injury and to ask ifthe visual acuity has changed.
ExaminationThe visual acuity in each eye needs
to be accurately tested and recordedbefore any treatment begins. If a Snel-len chart is unavailable, or if the pa-
tient is confined to bed, a test card maybe used to assess the near visualacuity. Ideally, the patient who wearsglasses should wear them if they areavailable and not broken; however, ifthis is not possible, the pinhole acuityshould be measured. If the patient is inpain, and especially if blepharospasmhas occurred, a topical anesthetic suchas proparacaine 0. 5% (Ophthaine)
Table IOcular History1. When, where, how and with what
did the injury occur?2. Severity and duration of presenting
complaint.3. Symptoms (change in visual
acuity).4. Previous eye disease, injury,
surgery.5. Systemic diseases.6. History of tetanus immunization.7. Medications (including any eye
drops).8. Allergies.9. Recent food and fluid intake (if
general anesthesia is beingconsidered).
CAN. FAM. PHYSICIAN Vol. 32: JULY 1986

may be instilled to allow for a betterexamination. Table 2 lists the steps ofthe ocular examination that should beperformed on any patient with an ocu-lar injury. Before treatment or duringtransport for treatment, a patient whohas a lacerated globe should have theeye protected with a hard shield to pre-vent further unnecessary injury.
Blunt TraumaBlunt trauma causes a contusion in-
jury that usually does not lacerate thesurface of the eye. This form of traumacan result in such injuries as cornealabrasions, subconjunctival hemor-rhages, hyphemas and blowout frac-tures.2
Corneal abrasionsCorneal abrasions are usually
caused by minor superficial trauma butnevertheless they can be quite sympto-matic. The epithelium is debrided, andthis may sometimes be caused by aforeign body in the conjunctival sac oron the cornea. Symptoms may includesevere pain or a sensation of a foreignbody in the eye. There may be exces-sive lacrimation, blepharospasm andphotophobia. The conjunctiva is oftenhyperemic, and visual acuity may benormal or slightly reduced, dependingon the area of comeal involvement.
Examining a patient with a cornealabrasion is often difficult as patientsare usually unwilling to open theireyes because of the pain they are ex-periencing. A topical anesthetic agentoften obliterates the symptoms and issomewhat diagnostic. These dropsshould not be instilled repeatedly for
analgesia, as corneal epithelial toxicityand interference with epithelial healingare known side effects. Examining thecornea with a pen light may show neg-ative results for any epithelial defectson initial cursory examination, how-ever, fluorescein dye instilled intoconjunctival sac will easily identifyareas of denuded epithelium. (See Fig-ure 1.) Cobalt blue illumination facili-tates the observance of corneal stain-ing with fluorescein, but is not alwaysrequired. An irregular light reflex thatis often seen on close examination isindicative of a break. in the epitheliallayer. The treatment for a cornealabrasion is described in Table 3.3 Cor-neal abrasions generally heal quickly-within 24-48 hours, but patientsshould be monitored until completehealing has occurred.
Although long-term problems arerare, scarring and subsequent reducedvisual acuity may occur if the initialinjury involved Bowman's membrane.Recurrent epithelial erosions may alsocomplicate a simple abrasion withsuch symptoms as sharp pain, tearing,
Table 2Examination
1. Corrected visual acuity in each eye.2. Pinhole acuity if / 20/20.3. External exam including pupillary
reactions.4. Extraocular movements.5. Ophthalmoscopy.6. Confrontational fields.7. Palpation (integrity of orbital rim).8. Assessment of neurological status if
indicated (possible intracranialtrauma).
photophobia, and blurred vision. Thepatient will complain of these symp-toms occurring, usually on arising inthe morning or suddenly during thenight. The attacks may be short-lived,or may last several hours. Graduallythey become less frequent and oftensubside; however, treatment with so-dium chloride drops and "bandage"soft contact lenses is sometimes re-quired.
Table 3Treatment of Corneal Abrasions
1. Instill a topical anesthetic.2. Clean any debris out of conjunctival
sac with an ophthalmic irrigatingsolution (Eye-Stream) or cottonswabs.
3. Instill a cycloplegic agent(cyclopentolate 1% or homatropine2%) to relieve ciliary spasm andreduce secondary iridocyclitis.
4. Instill a broad-spectrum antibioticointment such as gentamicin sulfate(Garamycin) or chloramphenicol(Chloroptic).
5. Patient should wear a doublepressure patch for twenty-fourhours.
6. Administer oral analgesics ifnecessary.
Subconjunctival hemorrhageSubconjunctival hemorrhages may
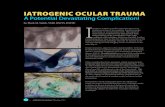
be caused by minor trauma or mayarise spontaneously. Rarely, the causemay be an underlying blood dyscrasialeading to a bleeding diathesis. Sub-conjunctival hemorrhage may resultfrom an episode of raised venous pres-sure, for example, following coughingor lifting. The presentation may bequite striking (see Figure 2) with hem-
Figure l Figure 2Corneal abrasion showing irregular light reflex, Subconjunctival hemorrhage extending to the limbus,denuded epithelium and fluorescein staining. with an uninvolved inferior area.
- X 7;;.;A:1 v
CAN. FAM. PHYSICIAN Vol. 32: JULY 1986 1 467

orrhage usually extending to thelimbus, but with uninvolved areas be-neath the lids. If no posterior limit tothe hemorrhage is seen, the blood mayhave resulted from a middle or anteriorcranial fossa fracture, and appropriateadditional investigations will be re-quired.4 The possibility of infectionshould be considered because hemor-rhagic conjunctivitis caused by entero-viruses and coxsackieviruses maypresent a similar picture; however, thepatient usually has pain, photophobia,the sensation of a foreign body in theeye, tearing and lid edema. In the ab-sence of significant trauma or infectionto the eye, the patient needs only to bereassured that the blood will clear intwo to three weeks time, and no othertreatment is required.
HyphemaA hyphema results when blood is re-
leased into the anterior chamber, oftenfollowing blunt trauma. It must be re-membered, however, that other causesof hyphema, especially retinoblastomaand juvenile xanthogranuloma in chil-dren, may present spontaneously, withno history of injury.5 Evidence ofblood in the anterior chamber can bestriking or slight and seen only withslit lamp examination. A distinct fluidlevel of settled red blood cells is oftenthe presenting picture (see Figure 3),but the entire chamber may be filledwith blood, which is described as an"eight ball hemorrhage". Fifty-eightpercent of hyphemas fill less than one-third of the anterior chamber.6 Thesource of the anterior chamber hemor-rhage is thought to be from concussiveforces that displace the iris and lensposteriorly and result in a tear of the
ciliary body or other angle structures.Patients with hyphema need to bethoroughly evaluated for unsuspecteddamage that may be present and causelong-term complications. In additionto the ocular examination listed inTable 2, intraocular pressure should bemeasured and recorded; it may be ele-vated in up to 32% of patients.7 Eleva-tion of intraocular pressure may be alate complication that arises because ofa post-traumatic deformity of the an-terior chamber angle, which is knownas angle recession. Secondary hemor-rhage occurs in approximately 25% ofall hyphema patients, most frequentlybetween three and five days post-
8injury, and is associated with amarkedly worse prognosis in terms ofeventual visual outcome, and with arecurrent increase in the intraocularpressure.
Although the treatment of traumatichyphemas has many controversialaspects, including whether hospitaliza-tion is necessary, the goal is still topromote resorption of the blood and toprevent rebleeding. One treatment reg-imen is listed in Table 4, but it must beborne in mind that other modalitiesexist. Various medications includingcycloplegics, miotics, topical steroidsand estrogens have been suggested,but there is no definite evidence of
Table 4Treatment of Traumatic Hyphema
1. Put patch and shield on injured eye.2. Sedation only if patient exhibits
extreme agitation.3. Acetaminophen plus codeine for
analgesia (avoid ASA).4. Elevate head of bed 30- 46y.
their benefit. Aminocaproic acid hasbeen shown to decrease the incidenceof secondary hemorrhage by its antifi-brinolytic effect.9
Surgical intervention may be re-quired if medical therapy fails to con-trol the intraocular pressure, or if othercomplications such as corneal bloodstaining occur.
Blow-outfracturesOrbital floor fractures occur when
non-penetrating trauma transmitsforces to the orbital soft tissues, whichresults in increased hydrostatic pres-sure within the confines of the bonyorbit. The usual site of fracture is theposterior medial orbital floor in themaxillary bone. Rupture of the globeis uncommon in blow-out fracturesand has been reported in only nine per-cent of cases.10
Clinical findings include localizedpain, ecchymosis and lid swelling,epistaxis, orbital emphysema, en-ophthalmos, diplopia and hypoesthesiain the distribution of the infraorbitalnerve.11 The inferior rectus and the in-ferior oblique muscles or orbital fi-brous connective tissue may becomemechanically entrapped in the fracturesite and result in diplopia. The restric-tive ophthalmoplegia can be demon-strated on ocular version testing as isshown in Figure 4. It should be re-membered that other ocular injuriesare associated with 24-30% of blow-out fractures,1 2 including retinaledema and hemorrhage, hyphema,comeal laceration, choroidal rupture,glaucoma, and retinal detachment.
Radiologic evaluation is importantbecause up to 72% of fractures can be
Figure 3 Figure 4Hyphema illustrating the aqueous-blood fluid level in Blow-out fracture. Left orbit demonstrates restrictivethe anterior chamber. ophthalmoplegia in upgaze.
CAN. FAM. PHYSICIAN Vol. 32: JULY 19861468

diagnosed with certainty by usingWaters, Caldwell, lateral, basal andoptic foramen views.'3 CAT scanningin axial and coronal views is also ofbenefit.The emergency care of patients with
blow-out fractures centres aroundmedical or surgical treatment of asso-ciated ocular traumas, however, thefracture itself is never an immediateconcern. Indications for surgical cor-rection of blow-out fractures are con-troversial, but the guidelines suggestthat enophthalmos and/or diplopia inthe primary and reading positions maybe just cause for intervention.14 Thenatural history of untreated blow-outfractures has shown that many patientsimprove without undergoing surgery.
Sharp TraumaLid lacerations
Sharp trauma to the lids shouldarouse suspicion of further damagethan is immediately obvious andshould alert the emergency care physi-cian to take a thorough history and doa complete ocular examination. Gener-ally, the type of surgical repair of eye-lid lacerations depends on the depthand location of the injury. Superficiallacerations that are remote from the lidmargin and involve only the skin andorbicularis usually require skin suturesonly. A search for imbedded foreignbodies should be carried out. Deeperlacerations involving the levator mus-cle require extra care in suturing, andthe patient may need to be referred toan ophthalmologist. Lacerations in-volving the lid margin that are centraland do not involve the lacrimal system
can be repaired by precise suture align-ment and tension to avoid lid notches.If the lacrimal system is involved andthe laceration extends through the can-aliculus, intubation tubes will likelyneed to be placed and a referral wouldbe warranted. Figure 5 illustrates anavulsion type of lid laceration involv-ing the inferior canaliculus.
Conjunctival, corneal andscleral lacerations
If a subconjunctival hemorrhage isassociated with a conjunctival lacera-tion, a penetrating injury to the eyemay be present.15 Small conjunctivallacerations will often heal by them-selves without suturing. Sharp andblunt trauma may cause scleral ruptureand other associated eye injuries.Similarly, comeal lacerations (with orwithout iris prolapse) may be asso-ciated with anterior chamber hemor-rhage and intraocular foreign bodies.The fundamental point in managingthese injuries is recognizing the extentof the trauma so that appropriate man-agement plans can begin. Topical anti-biotic drops should be instilled eachhour, intravenous antibiotics should bestarted, and a protective shield shouldbe placed over the injured eye. Thesepatients will require an urgent ophthal-mology consultation.
Ocular Foreign BodiesHistorical details will often help to
indicate the most probable site of anocular foreign body. The location de-pends on the velocity of impact and theweight of the particle.16 If the objectwas propelled by great force it will
likely be intraocular, whereas withsuperficial foreign bodies this historyis rare.
Corneal and conjunctivalforeign bodies
Foreign material on the cornea andconjunctiva cause such symptoms aspain, tearing, lid squeezing and thesensation of a foreign body in the eye.These symptoms often worsen uponblinking and may be accompanied byphotophobia. The conjunctiva isusually injected and the visual acuitymay be reduced if the foreign body isnear the visual axis.The patient should be examined
under magnification, preferably a slitlamp, which will aid in determiningthe extent and depth of the corneal in-jury. Vertical scratches may indicate aforeign body under the upper lid and,accordingly, both the upper and lowerfornices should be examined for re-tained foreign material. Iron-contain-ing foreign bodies in the cornea willoften be surrounded by a rust ring inthe epithelium, which may retard heal-ing and cause irritation. (See Figure6.) These rings are best removed witha 25 g needle or dental burr 24-48hours after the removal of the foreignbody.'7 Care should be taken not to betoo aggressive so as to avoid scarring.The *treatment steps for removing
superficial corneal and conjunctivalforeign bodies are outlined in Table 5.
Intraocular foreign bodiesPatients may have an intraocular
foreign body without being aware thatthe eye was penetrated. A history ofhammering metal on metal should alert
Figure 5Lid laceration due to an avulsion injury involving thecanalicular system.
..# ._v. Jri
Figure 6Metallic corneal foreign body with a rust ring.
CAN. FAM. PHYSICIAN Vol. 32: JULY 1986 1469

the clinician to search for an intraocu-lar foreign body. (See Figure 7.) Thetype of material will dictate the type ofreaction: silver, aluminum, platinumand gold are rather inert and cause lit-tle reaction, but iron can lead tosiderosis bulbi and eventual loss of theeye.A high index of suspicion coupled
with examination and various diagnos-tic tests including X-rays, CAT scans,and ultrasound will serve to diagnosethe presence of an intraocular foreignbody. Emergency care includes topicaland intravenous antibiotic coverage(although many high velocity missilesare sterile), tetanus prophylaxis if re-quired, and a protective eye shield.Ophthalmological consultation for sur-gical evaluation should be arranged ur-gently.
Table 5Treatment of Corneal andConjunctival Foreign Bodies
1. Instill a topical anesthetic.2. Irrigate eye with saline to try and
wash foreign body away.3. Wipe off conjunctival foreign bodies
with a moistened cotton swab.4. Remove comeal foreign bodies with
a 25 g needle.5. Treat the same as a corneal
abrasion. See Table 3.6.- Remove rust rings after 24- 48
hours.
Chemical BurnsThe emergency care of chemical
burns of the eye is one of the few situa-tions where treatment preceeds a de-tailed history and examination. Once ithas been established that the eye has
been exposed to toxic products, theimmediate treatment is copious irriga-tion with any available source of cleanwater. Attempts to neutralize the of-fending chemical with special solu-tions should not be made as furtherdamage may result.
The severity of any burn depends onthe concentration of the chemical, theduration of exposure, and the pH ofthe solution. Weak acids penetrate bio-logic tissues poorly. The hydrogen ionprecipitates protein and thus providessome protection to the corneal stromaand deeper tissues. Alkalis as well asstrong acids will penetrate tissues rap-idly and combine with the lipid of cellmembranes and denature collagen andcause vascular thrombosis in the con-junctiva, episclera and even the an-terior uvea.18 Patients with chemicalburns usually have intense pain, lacri-mination and blepharospasm.
The emergency care of patients withchemical injuries is outlined in Table6. The natural clinical history showsthat when burns are severe, especiallythose due to alkalis, there is an imme-diate rise in intraocular pressure.19This rise in pressure may be severeenough to require surgical interventionafter a trial of medical therapy. Pa-tients with the most severe alkali burnswill present with an opaque cornea,absent epithelium and ischemic ne-crosis of the perilimbal conjunctiva.These eyes often go on to perforationdue to the release of collagenase fromhealing inflammed tissue. The best re-sult that one can hope for after a severealkali bum is a totally vascularized andscarred cornea that has not undergoneperforation or developed glaucoma.
(See Figure 8.) Various medicationssuch as acetylcysteine, L-cysteine, andEDTA have been shown to inhibit colla-genase and reduce the incidence of ul-cerations.20 Topical and systemicsteroids as well as topical ascorbic andcitric acids have also been used in thecare of chemically injured eyes. 21' 22
Table 6Treatment of Chemical Burns1. At the scene of injury, immediately
irrigate the eye(s) with any sourceof clean water.
2. Instill a topical anesthetic, retractthe lid(s), then irrigate the eye(s)with at least 2000 ml of 0.9%normal saline over one hour (to pHof 7.3-7.7 in the cul-de-sac).
3. Remove all particulate matter fromfomices with a cotton swab.
4. Instill cycloplegic such ascyclopentolate 1% to preventsynechiae and decrease ciliaryspasm.
5. Instill antibacterial ointment such asgentamicin sulfate (Garamycin) orchloramphenicol (Chloroptic), thenpatch the eye(s).
6. Administer systemic analgesics forpain.
AcknowledgementsFigures 1, 3, 5, 6 and 8 have been
reprinted by permission from theAmerican Academy of Ophthal-mology. I wish to thank Dr. C. C.Ewing for reviewing this paper, andMs. D. Meyer for typing the manu-script.
References1. Gombos GM. Nonpenetrating and non-
Figure 7Intraocular foreign body.
l. M..
Figure 8Vascularized and scarred cornea secondary to a severealkali burn.
1470 CAN. FAM. PHYSICIAN Vol. 32: JULY 1986

perforating injuries of the eyeball. In:Gombos GM, ed. Handbook of ophthal-mologic emergencies. New Hyde Park,NY: Medical Examination Publishing,1977:98- 120.2. Benson WE, Shakin J, Sarin LK. Blunttrauma. In: Duane TD, ed. Cliniccal oph-thalmology. Philadelphia: Harper andRow, 1985, vol 3:1- 14.3. Paton D, Goldberg MF. Corneal abra-sion. In: Paton D, Goldberg MF, eds.Manlagemenit of ocular injuries. Philadel-phia: Saunders, 1976:194- 8.4. Spalton DJ, Hitchings RA, Hunter PA.The conjunctiva: diseases and tumors. In:Spalton DJ, Hitchings RA, Hunter PA,eds. Atlas of c linic al ophthalmology.Philadelphia: Lippinccott, 1984:2- 20.5. Zimmerman LE. Ocular lesions of ju-venile xanthogranuloma, nevoxanthoen-dothelioma. Trans Ain Acad OphthalmnolOtolaryngol 1965; 69:412- 22.6. Read JD, Crouch ER Jr. Trauma: rup-tures and bleeding. In: Duane TD, ed.Clinical ophthalmology. Philadelphia:Harper and Row, 1985, vol 4:1- 18.7. Read JE, Goldberg MF. Traumatic hy-phema: comparison of medical treatment.
Traitis Am Accad Ophthalhnol Otolaryngol1974; 78:799- 815.8. Pilger IS. Medical treatment of trauma-tic hyphema. Surv' Ophthal,nol 1975;20:28- 34.9. Crouch ER Jr, Frenkel M. Aminoca-proic acid in the treatment of traumatichyphema. Am/n J Ophthal/nol 1976;81:355- 60.10. Cherry PMH. Rupture of the globe.Alrc h Ophthilnol 1972; 88:498- 507.11. Greenwald HS Jr, Kenney AH, Shan-non GM. A review of 128 patients withorbital fractures. Ain J Ophthillmnol 1974;78:655- 64.12. Wilkins RB, Havens WE. Currenttreatment of blow-out fractures. Ophth/l-mology 1982; 89:464- 6.13. Emery JM, Von Noorden GK, Schler-nitzauer DA. Orbital floor fractures: long-term followup of cases with and withoutsurgical repair. Trants Ain Aca(td Ophthtal-miol 1971; 75:802- 12.14. Hawes MJ, Dortzbach RK. Surgeryon orbital floor fractures. Ophthalnology1983; 90:1066- 70.15. Lichtenstein SB. Management of pen-
etrating and perforating injuries to the an-terior segment. In: Duane TD, ed. Clini-c'Cl ophthailmology. Philadelphia: Harperand Row, 1985, vol 5:1-9.
16. Chisholm IA. Intra-ocular metallicforeign bodies. Blr J Ophth(liniol 1964;48:364- 72.17. Paton D, Goldberg MF. Cornealforeign bodies. In: Paton D, GoldbergMF, eds. Mana,gentent oj ocul(ar inzjurl-ies.Philadelphia: Saunders, 1976:198- 204.18. Pfister RR. Chemical injuries of theeye. Ophthtdiaology 1983; 90:1246- 53.19. Paterson CA, Pfister RR. Intraocularpressure changes after alkali bums. ArchOphthalmnol 1974; 91:211-8.20. Brown SI, Weller CA. Collagenaseinhibitors in prevention of ulcers of alkali-burned cornea. Arch Ophthalmiiol 1970;83: 352- 3.21. Lass JH, Campbell RC, Rose J, et al.Medroxyprogesterone on corneal ulcer-ation; its effects after alkali burns on rab-bits. Arch Ophthalmniol 1981; 99:673- 6.22. Pfister RR, Paterson CA. Ascorbicacid in the treatment of alkali burns of theeye. Ophthalnology 1980; 87:1050- 7.
Prolopa®Rx SummaryIndicationsTreatment of Parkinson's syndrome when not drug-induced.ContraindicationsKnown hypersensitivity to levodopa or benserazide; inpatients in whom sympathomimetic amines are contra-indicated; concomitantly with, or within 2 weeks of,MAOI administration; uncompensated cardiovascular,endocrine, renal, hepatic, hematologic or pulmonarydisease; narrow-angle glaucoma.WarningsDiscontinue levodopa at least 12 hours before initiating'Prolopa'. See Dosage section for substitution recom-mendations.Not indicated in intention tremor, Huntington's chorea ordrug-induced Parkinsonism.Increase dosage gradually to avoid CNS side effects(involuntary movements). Observe patients for signs ofdepression with suicidal tendencies or other seriousbehavioural changes. Caution in patients with history ofpsychotic disorders or receiving psychotherapeutic agents.In patients with atrial, nodal or ventricular arrhythmias orhistory of myocardial infarction initiate treatment cau-tiously in hospital. Caution in patients with history ofmelanoma or suspicious undiagnosed skin lesions.Safety in patients under 18 years has not been established.In women who are or may become pregnant, weigh bene-fits against possible hazards to mother and fetus. Notrecommended for nursing mothers.PrecautionsMonitor cardiovascular, hepatic, hematopoietic and renalfunction during extended therapy. Caution in patients withhistory of convulsive disorders. Upper gastrointestinalhemorrhage possible in patients with a history of pepticulcer.Normal activity should be resumed gradually to avoid riskof injury.Monitor intraocular pressure in patients with chronicwide-angle glaucoma. Pupillary dilation and activation ofHorner's syndrome have been reported rarely. Exercise
caution and monitor blood pressure in patients on anti-hypertensive medication. 'Prolopa' can be discontinued12 hours prior to anesthesia. Observe patients on con-comitant psychoactive drugs for unusual reactions.Adverse ReactionsMost common are abnormal involuntary movements,usually dose dependent, which necessitate dosage reduc-tion. Other serious reactions are periodic oscillations inperformance (end of dose akinesia, on-off phenomenonand akinesia paradoxica) after prolonged therapy, psy-chiatric disturbances (including paranoia, psychosis,depression, dementia, increased libido, euphoria,sedation and stimulation), and cardiovascular effects(including arrhythmias, orthostatic hypotension, hyper-tension, ECG changes and angina pectoris).Neurologic, intellectual, gastrointestinal, dermatologichematologic, musculoskeletal, respiratory, genitourinaryand ophthalmologic reactions have also been reported.Consult Product Monograph for complete list.DosageIndividualize therapy and titrate in small steps to maxi-mize benefit without dyskinesias. Do not exceed therecommended dosage range.Initially, one capsule 'Prolopa' 100-25 once or twicedaily, increased carefully by one capsule every third orfourth day (slower in post-encephalitic Parkinsonism)until optimum therapeutic effect obtained without dyski-nesias. At upper limits of dosage, increment slowly at2-4 week intervals. Administer with food.Optimal dosage Is usually 4-8 'Prolopa' 100-25capsules daily, in 4-6 divided doses.'Prolopa' 200-50 capsules are intended for maintenancetherapy once optimal dosage has been determined using'Prolopa' 100-25 capsules. No patient should receivemore than 1000 - 1200 mg levodopa daily during the firstyear of treatment. 'Prolopa' 50-12.5 capsules should beused when frequent dosing is required to minimizeadverse effects.For patients previously treated with levodopa, allow atleast 12 hours to elapse and initiate 'Prolopa' at 15% ofprevious levodopa dosage.During maintenance, reduce dosage slowly, if possible,to a maximum of 600 mg levodopa daily.
Supply'Prolopa' 50-12.5 capsules containing 50 mg levodopaand 12.5 mg benserazide.'Prolopa' 100-25 capsules containing 100 mg levodopaand 25 mg benserazide.'Prolopa' 200-50 capsules containing 200 mg levodopaand 50 mg benserazide.Bottles of 100.Product Monograph available on request.References:1. Editorial Parkinson's disease, 1984. Lancet 1984;1:
829-30.2. Lieberman AN, Goldstein M, Gopmathan G, et al.
Combined use of benserazide and carbidopa inParkinson's disease. Neurology 1984;34:227-9.
3. Rinne UK, M6lsa P. Levodopa with benserazide orcarbidopa in Parkinson's disease. Neurology 1979;29:1584-9.
4. Weiner WJ, Nausieda PA. Carbidopa - levodopa ratioin Parkinson's disease. Arch Neurol 1981; 38:534.
5. Hoehn MM. Increased dosage of carbidopa in patientswith Parkinson's disease receiving low doses oflevodopa. A pilot study. Arch Neurol 1980; 37:146-9.
Hoffmann-La Roche LimitedEtobicoke, Ontario M9C 5J4
® Registered Trade Mark© Copyright 1985 Hoffmann-La Roche Limited
5034
PAABCCPP
Original Research in Medicine and Chemistry
CAN. FAM. PHYSICIAN Vol. 32: JULY 1986 1471