OCULAR PHARMACOLOGY. Definitions 1) Bioavailability-% of unchanged drug delivered to site of...
69
OCULAR PHARMACOLOGY
-
Upload
ernest-willis -
Category
Documents
-
view
226 -
download
2
Transcript of OCULAR PHARMACOLOGY. Definitions 1) Bioavailability-% of unchanged drug delivered to site of...

OCULAR PHARMACOLOGY

Definitions 1) Bioavailability-% of unchanged drug delivered to site of potential
action regardless of route of administration 2) Compartment-body space in which drug is homogeneously distributed 3) Rate constants- Ka- absorption rate constant (fraction of drug entering compartment perunit time) Ke- elimination rate constant (fraction of drug eliminated fromcompartment per unit time) 4) Order of kinetics- First order-rate of absorption and elimination are proportional to drugconcentration Zero order-rates are independent of concentration, related to a functionalcapacity of body (true for most eyedrops) 5) Tissue binding-renders drug unavailable for elimination and prolongs
its retention in a compartment

Relevant anatomic characteristics of the eye Cornea-functions as a trilaminar permeability barrier (does not
allowanisocoria drugs to cross by simple diffusion)a) Properties of different corneal layers Epithelium- hydrophobic Stroma- hydrophilic Endothelium- hydrophobic
b) Epithelium is main barrier to hydrophilic molecules
c) Nonionized molecules penetrate epithelium/endothelium well, ionizedmolecules penetrate stroma well
d) For maximal corneal drug penetration a molecule must have optimum ratio of hydro- and lipo- philicity
Relevant anatomic continue…… 2) Sclera-due to intraocular pressure there is
typically a constant outward flow across the sclera, therefore even sub-Tenon’s
injections penetrate the globe slowly
3) Blood ocular barrier-present due to tight junctions of nonpigmented ciliary epithelium, retinal pigment epithelium, and retinal capillary endothelial cells

Vehicles of drug administration
Eyedrops-major route of ocular drug administration
a) Drops are advantageous because they avoid systemic toxicity by have the problem of a short duration of availability in the tear film and need to pass through a barrier with limited permeability
b) Characteristics of the cul-de-sac as a drug compartment

Factors affecting availability of topical meds 1. Surfactants-increase solubility of
hydrophilic drugs by alteringpermeability of epithelial membranes 2. Drug concentration-concentrated
solutions are used to maximize the amount of drug entering the eye during
the limited availability provided by a drop
Factors affecting availability of topical meds 3. Viscosity-high viscosity solutions increase drug contact
time on the cornea
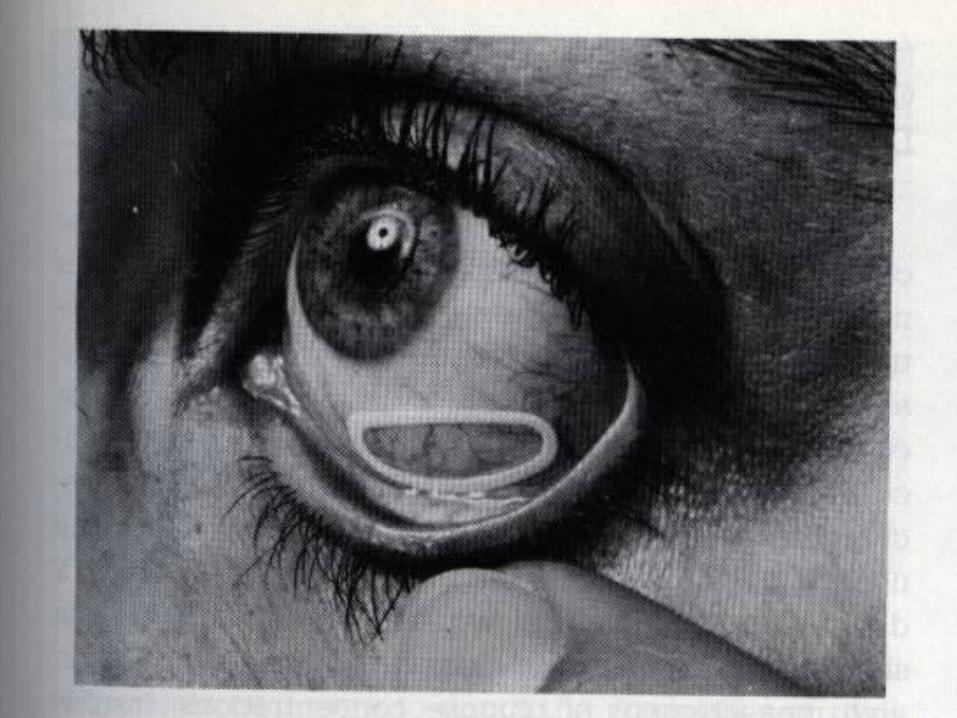
4. pH-determines degree of ionization of a drug (remember:
nonionized portion will be more lipid soluble, whileionized portion will be more stable in the tears and betterpenetrate stroma)- since the pH of tears is slightly alkaline(7.4) many oculardrugs are weak bases (alkaloids) existing in boththeir charged and uncharged forms at that pH- if the pH of the solution is made more basic then moreuncharged forms of the molecule are present, increasinglipid solubility and epithelial penetration

Some Characteristics of Ocular Routes of Drug Administration
ROUTE: Topical
ABSORPTION PATTERN: Prompt, depending on formulation
SPECIAL UTILITY: Convenient, economical, relatively safe
LIMITATIONS AND PRECAUTIONS: corneal and conjunctival toxicity, nasal mucosal toxicity, systemic side effects from nasolacrimal
absorption
Some Characteristics of Ocular Routes of Drug Administration
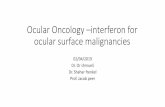
ROUTE: Subconjunctival, sub-Tenon's, and retrobulbar injections
ABSORPTION PATTERN: Prompt or sustained, depending on formulation
SPECIAL UTILITY: Anterior segment infections, posterior uveitis, cystoid macular edema
LIMITATIONS AND PRECAUTIONS: Local toxicity, tissue injury, globe perforation, optic nerve trauma, central retinal artery and/or vein occlusion, direct retinal drug toxicity with inadvertent globe perforation, ocular muscle trauma, prolonged drug effect

Some Characteristics of Ocular Routes of Drug Administration
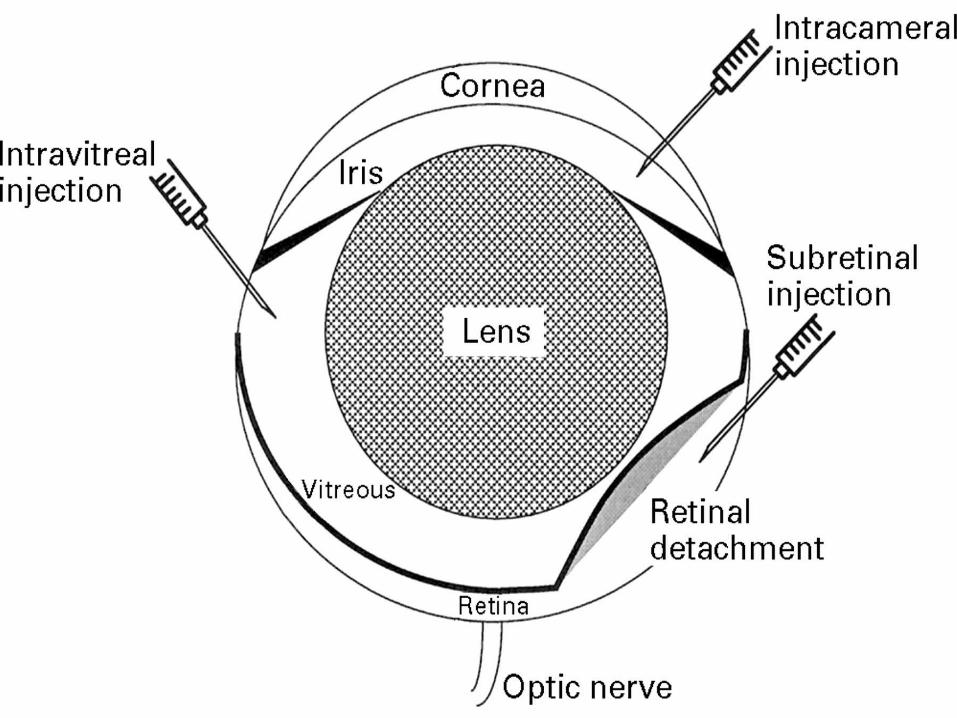
ROUTE: Intraocular (intracameral) injections
ABSORPTION PATTERN: Prompt
SPECIAL UTILITY: Anterior segment surgery, infections
LIMITATIONS AND PRECAUTIONS: Corneal toxicity, intraocular toxicity, relatively short duration of action

Some Characteristics of Ocular Routes of Drug Administration
ROUTE: Intravitreal injection or device
ABSORPTION PATTERN: Absorption circumvented, immediate local effect, potential sustained effect
SPECIAL UTILITY: Endophthalmitis, retinitis
LIMITATIONS AND PRECAUTIONS: Retinal toxicity
Absorption. After topical instillation of a drug, the rate and
extent of absorption are determined by :1-the time the drug remains in the cul-de-sac and
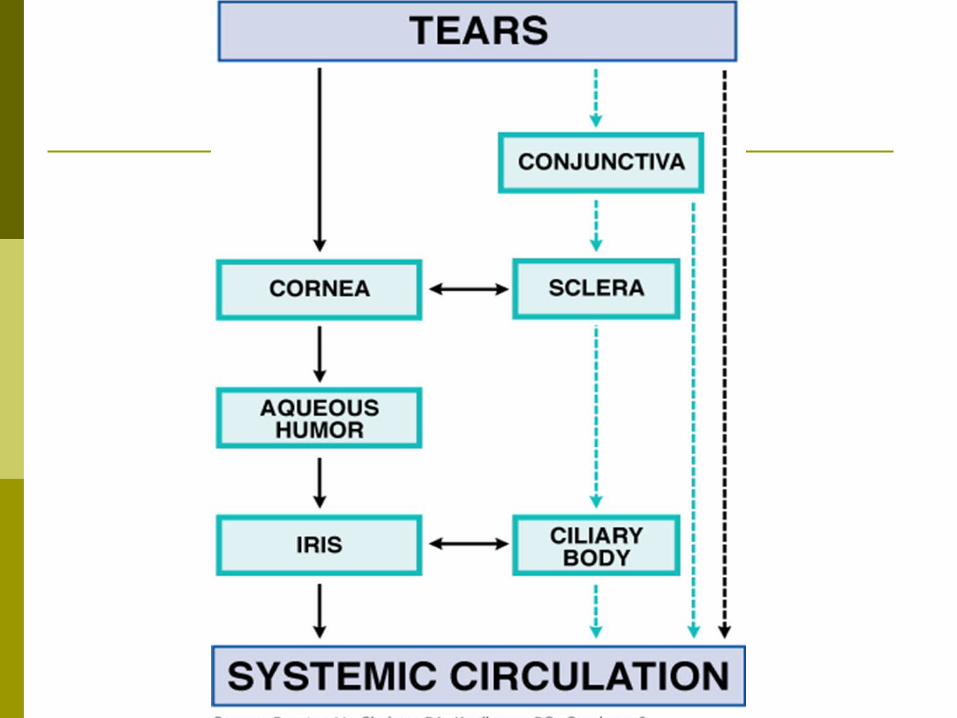
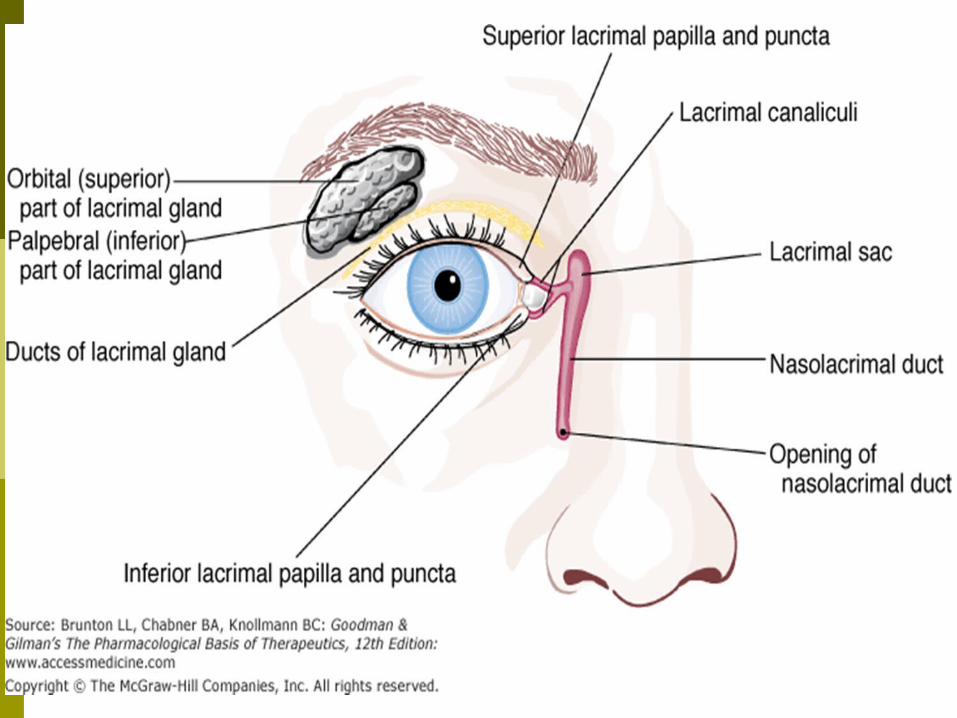
precorneal tear film 2-elimination by nasolacrimal drainage 3-drug binding to tear proteins4- drug metabolism by tear and tissue proteins 5-diffusion across the cornea and conjunctiva

Distribution Melanin binding of certain drugs is an
important factor in some ocular compartments. For example, the mydriatic effect of a adrenergic receptor agonists is slower in onset in human volunteers with darkly pigmented irides compared to those with lightly pigmented irides.

Distribution continue…………….. Another clinically important consideration
for drug-melanin binding involves the retinal pigment epithelium. In the retinal pigment epithelium, accumulation of chloroquine causes a toxic retinal lesion known as a "bull's-eye" maculopathy, which is associated with a decrease in visual acuity

Ointments
Ointments usually contain mineral oil and a petrolatum base and are helpful in delivering antibiotics, cycloplegic drugs, or miotic agents
Ointments a) Advantages1. Increase drug contact time b) Disadvantages1. May act as a barrier to vision and
penetration of other drops2. Slow release of some meds from ointment
may result insubtherapeutic levels of drug
3) Gel-made of high viscosity acrylics (ex. Ocuserts)- slowly releases drug at a
steady state level at overall lower conc. and less systemic side-effects
4) Liposomes-synthetic lipid microspheres into which drugs may be incorporated for sustained release
5) collagen shields-also provide prolonged drug contact time (rate of drug release may not be constant)
6) Subconjunctival/retrobulbar injection-allows drug to bypass conj/corneal epithelial barriers, can allow meds to reach therapeutic levels behind the lens/iris diaphragm
7) Intraocular injection 8) Systemic administrationAbility of blood borne agents to reach the
globe depends on: a) lipid solubility b) plasma protein binding (only unbound
form is bioavailable) c) molecular weight
MISCELLANEOUS Packs
Sustain-release devices
Irrigations
Hypertonic agents
Chelating agent

Metabolism. Enzymatic biotransformation of ocular
drugs may be significant since a variety of enzymes,including esterases, oxidoreductases , lysosomal enzymes, peptidases , glucuronide and sulfate transferases , glutathione-conjugating enzymes,catechol-O-methyl-transferase, monoamine oxidase, and 11b-hydroxysteroid dehydrogenase are found in the eye.

Metabolism continue…….. The esterases have been of particular interest because
of the development of prodrugs for enhanced corneal permeability; for example, dipivefrin hydrochloride is a prodrug for epinephrine, and latanoprost is a prodrug for prostaglandin F2a; both drugs are used for glaucoma management.
Topically applied ocular drugs are eliminated by the liver
and kidney after systemic absorption, but enzymatic transformation of systemically administered drugs also is important in ophthalmology.
Toxicology. All ophthalmic medications are potentially
absorbed into the systemic circulation , so undesirable systemic side effects may occur.
Most ophthalmic drugs are delivered locally to the eye, and the potential local toxic effects are due :
hypersensitivity reactions
direct toxic effects on the cornea, conjunctiva, periocular skin, and nasal mucosa.
Local toxicity of topically applied ocular drugs Some drugs are more prone to produce
hypersensitivity reactions such as neomycin.
Unfortunately some eyes, and some individuals, have a genetic predisposition to allergic reactions, particularly those subjects who suffer from atopy or allergy affecting other systems.

Continue…… Others may have known but atypical and
undesirable reactions to topical drops, such as marked elevation of intraocular pressure (IOP) associated with topical corticosteroids.

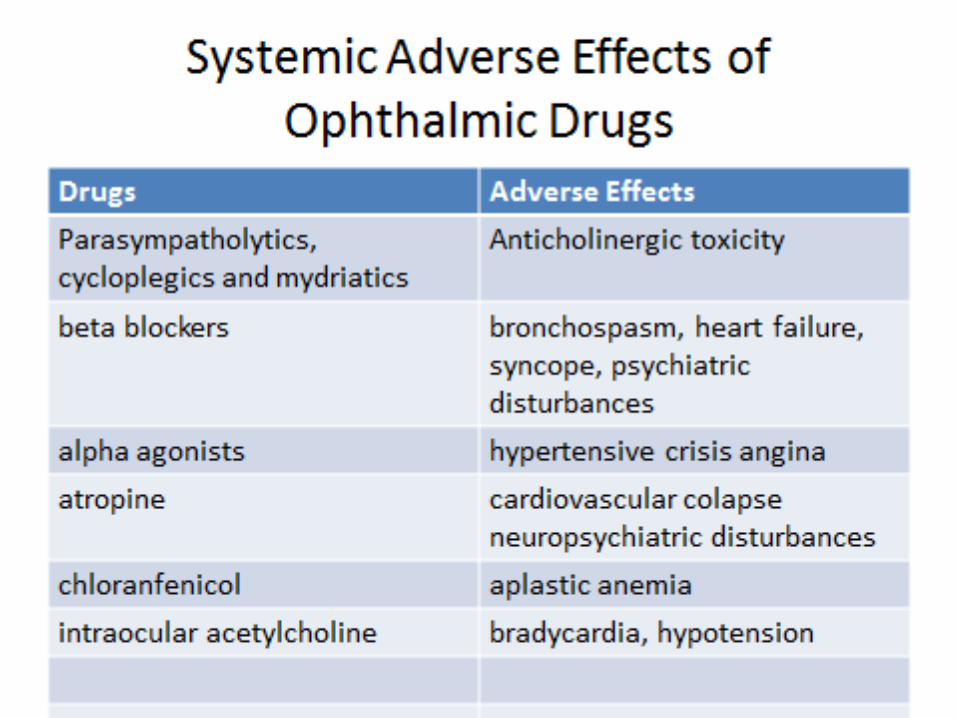
systemic toxicity of topically applied ocular drugs The systemic toxicity of topical ocular
drugs can be significant, and topical betablockers have been associated with marked respiratory and cardiac depression and exacerbation of respiratory conditions such as asthma.
Presevatives Eyedrops and contact lens solutions commonly
contain preservatives such as benzalkonium chloride, chlorobutanol, chelating agents, and thimerosal for their antimicrobial effectiveness. In particular, benzalkonium chloride may cause a punctate keratopathy or toxic ulcerative keratopathy Thimerosal currently is used rarely due to a high incidence of hypersensitivity reactions.
APPLICATIONS OF DRUGS IN OPHTHALMOLOGY
THERAPEUTIC DIAGNOSTICSome drugs have both effects therapeutic
and diagnostic( e.g. atropine homatropine physostigmine and pilocarpine)
Chemotherapy of Microbial Diseases in the Eye
Appropriate selection of antibiotic and route of administration is dependent on
the patient's symptoms, the clinical examination, and the culture/sensitivity
results.
Topical Antibacterial Agents Commercially Available for
Ophthalmic Use Chloramphenicol, 0.5% solution,
Conjunctivitis, keratitis
Ciprofloxacin hydrochloride (CILOXAN). 1% ointment 3% solution, Conjunctivitis, keratitis

Topical Antibacterial Agents Gentamicin sulfate (GARAMYCIN) 0.3%
solution Conjunctivitis, blepharitis, keratitis
Erythromycin 0.3%& 5% ointment Blepharitis, Conjunctivitis

Topical Antibacterial Agents Sulfacetamide sodium, 10, 15, 30%
solution Conjunctivitis, keratitis
Polymyxin B 10% ointment ,Various solutions , Conjunctivitis, blepharitis, keratitis
Antiviral Agents for Ophthalmic Use Trifluridine Topical (1% solution) Herpes
simplex keratitis Herpes simplex conjunctivitis
idoxuridine-IDU-topical 0.1%, ointment 0.5%
Acyclovir Oral, intravenous 400- and 800-mg Herpes zoster ophthalmicus Herpes simplex iridocyclitis
Valacyclovir Oral Herpes simplex keratitis , Herpes zoster ophthalmicus

Antiviral Agents continue…………. Famciclovir Oral Herpes simplex keratitis Foscarnet IV , Intravitreal Herpes zoster ophthalmicus
Cytomegalovirus retinitis Ganciclovir IV, oral Cytomegalovirus
retinitis Formivirsen Intravitreal injection
Intravitreal implant Cytomegalovirus retinitis

Antifungal Agents for Ophthalmic Use Polyenes Amphotericin B 0.1-0.5% (typically 0.15%)
topical solution , 0.8-1 mg subconjunctival , 5-ug intravitreal & intravenous injection Yeast and fungal endophthalmitis
Natamycin 5% topical suspension ,Yeast and fungal blepharitis, conjunctivitis, keratitis

Antifungal Agents for Ophthalmic Use Imidazoles Fluconazole oral,, Itraconazole oral Ketoconazole oral Miconazole 1% topical solution Yeast and
fungal keratitis subconjunctival (5-10 mg)
intravitreal (10 ug) injection Yeast and fungal endophthalmit

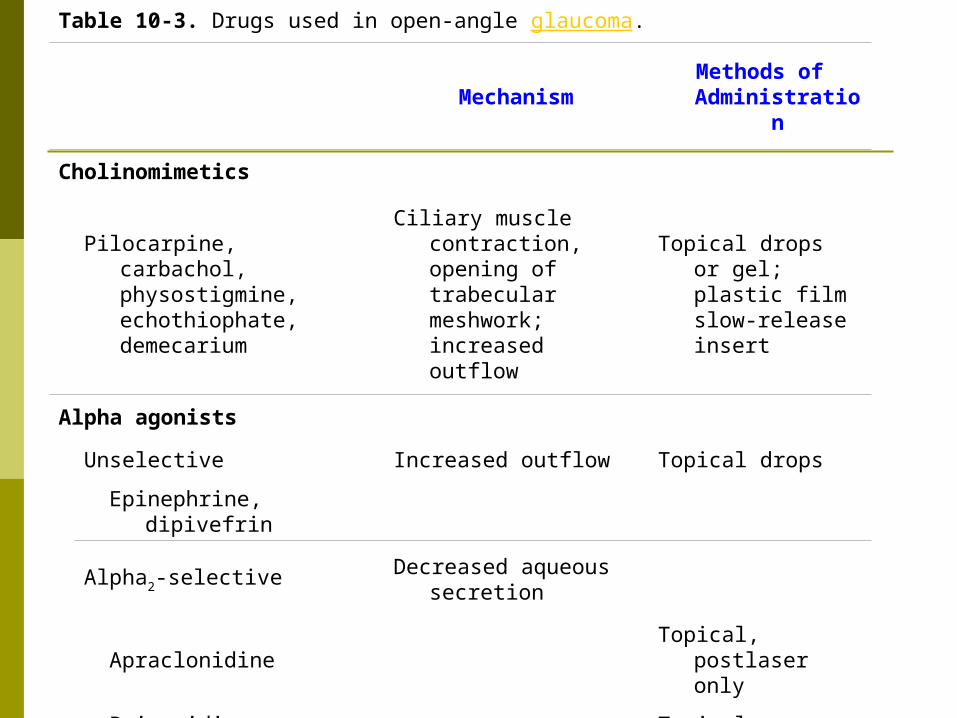
Table 10-3. Drugs used in open-angle glaucoma.
MechanismMethods of Administratio
n
Cholinomimetics
Pilocarpine, carbachol, physostigmine, echothiophate, demecarium
Ciliary muscle contraction, opening of trabecular meshwork; increased outflow
Topical drops or gel; plastic film slow-release insert
Alpha agonists
Unselective Increased outflow Topical drops
Epinephrine, dipivefrin
Alpha2-selective Decreased aqueous secretion
Apraclonidine Topical, postlaser
only
Brimonidine Topical
Beta-blockers
Timolol, betaxolol,
carteolol, levobunolol, metipranolol
Decreased aqueous secretion from the ciliary epithelium
Topical drops
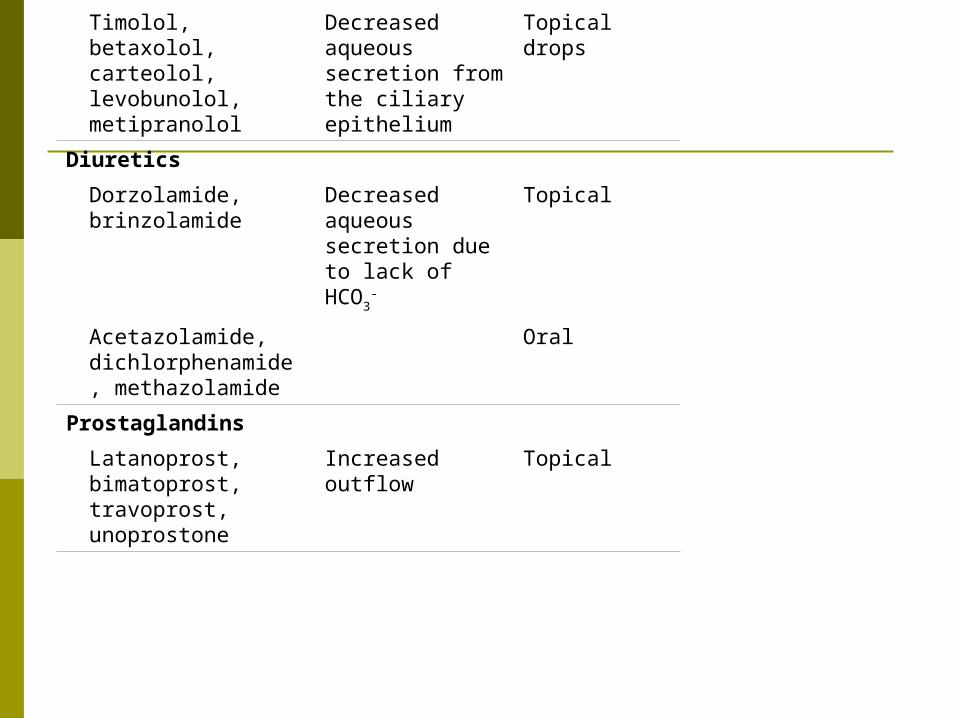
Table 10-3. Drugs used in open-angle glaucoma.
Mechanism Methods of Administrat
ion
Cholinomimetics
Pilocarpine, carbachol, physostigmine, echothiophate, demecarium
Ciliary muscle contraction, opening of trabecular meshwork; increased outflow
Topical drops or gel; plastic film slow-release insert
Alpha agonists
Unselective Increased outflow
Topical drops
Epinephrine, dipivefrin
Alpha2-selective Decreased aqueous secretion
Apraclonidine Topical, postlaser only
Brimonidine Topical
Beta-blockers
Timolol, betaxolol, carteolol, levobunolol, metipranolol
Decreased aqueous secretion from the ciliary epithelium
Topical drops
Diuretics
Dorzolamide, brinzolamide
Decreased aqueous secretion due to lack of HCO3
-
Topical
Acetazolamide, dichlorphenamide, methazolamide
Oral
Prostaglandins
Latanoprost, bimatoprost, travoprost, unoprostone
Increased outflow
Topical

Glaucoma young patients usually are intolerant of
miotic therapy secondary to visual blurring from induced myopia
direct miotic agents are preferred over cholinesterase inhibitors in "phakic" patients (i.e., those patients who have their own crystalline lens) because the latter drugs can promote cataract formation

Glaucoma continue….. in patients who have an increased risk of
retinal detachment, miotics should be used with caution because they have been implicated in promoting retinal tears in susceptible individuals (such tears are thought to be due to altered forces at the vitreous base produced by ciliary body contraction induced by the drug)

Uveitis
Cyclopentolate (CYCYLOGYL, others), tropicamide (MYDRIACYL) Atropine, scopolamine and homatropine
frequently are used to prevent posterior synechia formation between the lens and iris margin and to relieve ciliary muscle spasm that is responsible for much of the pain associated with anterior uveitis.
Uveitis
If posterior synechiae already have formed, an adrenergic agonist may be used to break the synechiae by enhancing pupillary dilation.
A solution containing scopolamine 0.3% in combination with 10% phenylephrine
Topical steroids usually are adequate to decrease inflammation, but sometimes they must be supplemented with systemic steroids.
Use of Autonomic Agents in the Eye Cholinergic agonists Acetylcholine (MIOCHOL-E) 1% solution Intraocular
use for miosis in surgery (OCULAR SIDE EFFECTS): is Corneal edema
Carbachol Intraocular use for miosis in surgery, glaucoma
(O.S.E.) Corneal edema, miosis, induced myopia, decreased vision, brow ache, retinal detachment
Anticholinesterase agents Physostigmine (ESERINE) Glaucoma,
accommodative esotropia, louse and mite infestation of lashes
(O.S.E.) Retinal detachment, miosis, cataract, pupillary block glaucoma iris cysts, brow ache, punctal stenosis of the nasolacrimal system
Echothiophate Glaucoma, accommodative esotropia (O.S.E.) Same as for physostigmine
Muscarinic antagonists Atropine Cycloplegic retinoscopy, dilated
funduscopic exam, (O.S.E.) Photosensitivity, blurred vision
Scopolamine , Homatropine , Cyclopentolate , Tropicamide effect and side effect Same as for atropine
Sympathomimetic agents Dipivefrin , Epinephrine , Brimonidine
Glaucoma (O.S.E.)Photosensitivity, hypersensitivity
Phenylephrine Mydriasis Apraclonidine Glaucoma, pre- & postlaser
prophylaxis of intraocular pressure spike

Sympathomimetic agents Cocaine Topical anesthesia, evaluate
anisocoria Hydroxyamphetamine Evaluate anisocoria Naphazoline , Tetrahydrozoline
Decongestant (O.S.E.) Same as for dipivefrin

THE EYE

Use of Immunomodulatory Drugs for Ophthalmic Therapy Glucocorticoids. Glucocorticoids have an important role in
managing ocular inflammatory diseases Therapeutic Uses. antiinflammatory effects, topical
corticosteroids are used in managing significant ocular allergy
Toxicity of Steroids. open-angle glaucoma cataract c) ptosis d) mydriasis e) delayed wound healing f) enhanced microbial proliferation g) punctate keratopathy
Nonsteroidal Antiinflammatory Agents. General Considerations Ketorolac is given for seasonal allergic
conjunctivitis. An ophthalmic preparation is available for ocular inflammatory conditions
Diclofenac is used for postoperative inflammation.
Both ketorolac and diclofenac have been found to be effective in treating cystoid macular edema occurring after cataract surgery.
Diclofenac (Nonselective COX Inhibitors)
A 0.1% ophthalmic preparation is recommended for prevention of postoperative ophthalmic inflammation and can be used after intraocular lens implantation and strabismus surgery.
A topical gel containing 3% diclofenac is effective for solar keratoses.

Bromfenac Ophtalmic Bromfenac is a non-steroidal anti-
inflammatory drug (NSAID). Bromfenac ophthalmic (for the eyes) is used to treat swelling and pain caused by cataract surgery.
Side effect:hives;difficult breathing;swelling of your face, lips, tongue, or throat.

Nepafenac Nepafenac is a
nonsteroidal anti-inflammatory drug (NSAID).
It reduces pain and inflammation in the eyes.

Nepafenac Nepafenac ophthalmic suspension is used
to reduce pain and swelling after cataract surgery.
Nepafenac is a prodrug,after use penetrates the cornea and is converted by ocular tissue hydrolases to amfenac,


Antihistamines and Mast-Cell Stabilizers Pheniramine and antazoline, both H1-receptor
antagonists, are formulated in combination with naphazoline, a vasoconstrictor, for relief of allergic conjunctivitis.
Cromolyn sodium (CROLOM), which prevents the release of histamine and other autacoids from mast cells , has found limited use in treating conjunctivitis that is thought to be allergen-mediated, such as vernal conjunctivitis.
Lodoxamidetromethamine and pemirolast , mast-cell stabilizers, also are available for ophthalmic use.



![NANOSUSPENSION: BIOAVAILABILITY ENHANCING NOVEL … · or previous GI surgery (e.g. bariatric surgery) can also affect drug bioavailability [23]. Improvement of bioavailability: The](https://static.fdocuments.in/doc/165x107/5eb46ef2a9b685351d4067b1/nanosuspension-bioavailability-enhancing-novel-or-previous-gi-surgery-eg-bariatric.jpg)