OCULAR INFLAMMATORY DISEASE C. Stephen Foster, MD, FACS, FACR Harvard Medical School Massachusetts...
88
OCULAR INFLAMMATORY DISEASE C. Stephen Foster, MD, FACS, FACR Harvard Medical School Massachusetts Eye Research and Surgery Institution
-
Upload
leon-mealer -
Category
Documents
-
view
221 -
download
0
Transcript of OCULAR INFLAMMATORY DISEASE C. Stephen Foster, MD, FACS, FACR Harvard Medical School Massachusetts...

OCULAR INFLAMMATORY DISEASE
C. Stephen Foster, MD, FACS, FACRHarvard Medical School
Massachusetts Eye Research and Surgery Institution
Ocular Inflammatory Disease
• By far, the number one cause of blindness, worldwide
• Infection
• Trauma
• Cancer
• Autoimmunity




UVEITIS
• What is it?
• What is its importance?
• What is the history of its therapy?
• What does the future hold?

UVEITIS
• What is it?

Etymology
• Uvea, from uva (Latin = grape)
• itis, (Greek = inflammation)
Therefore, inflammation of the uvea
Ophthalmia and flegmoni, general terms

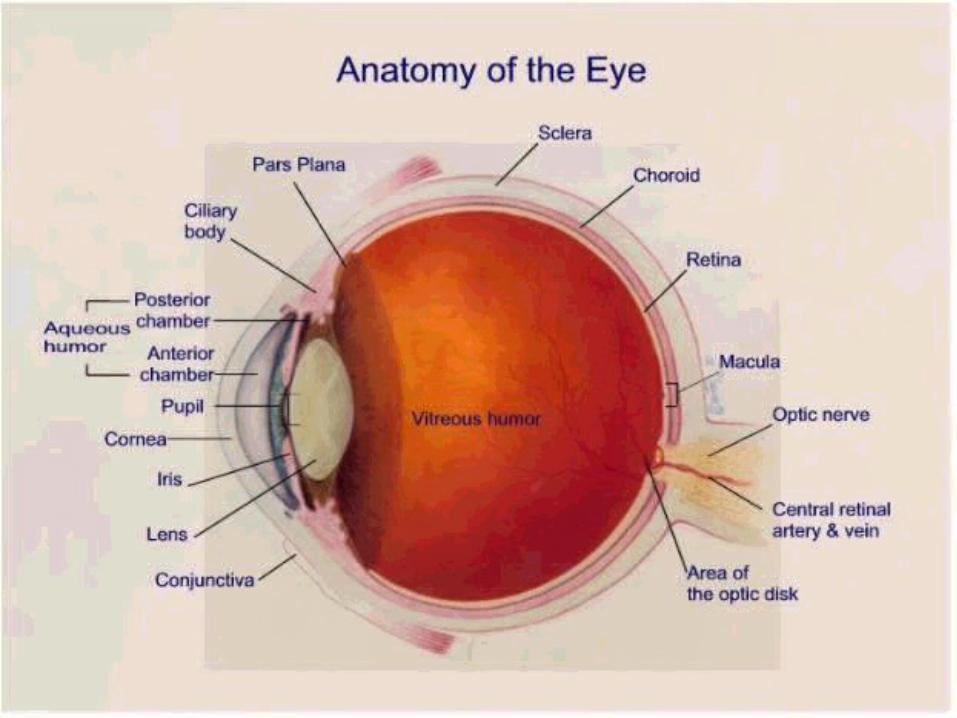
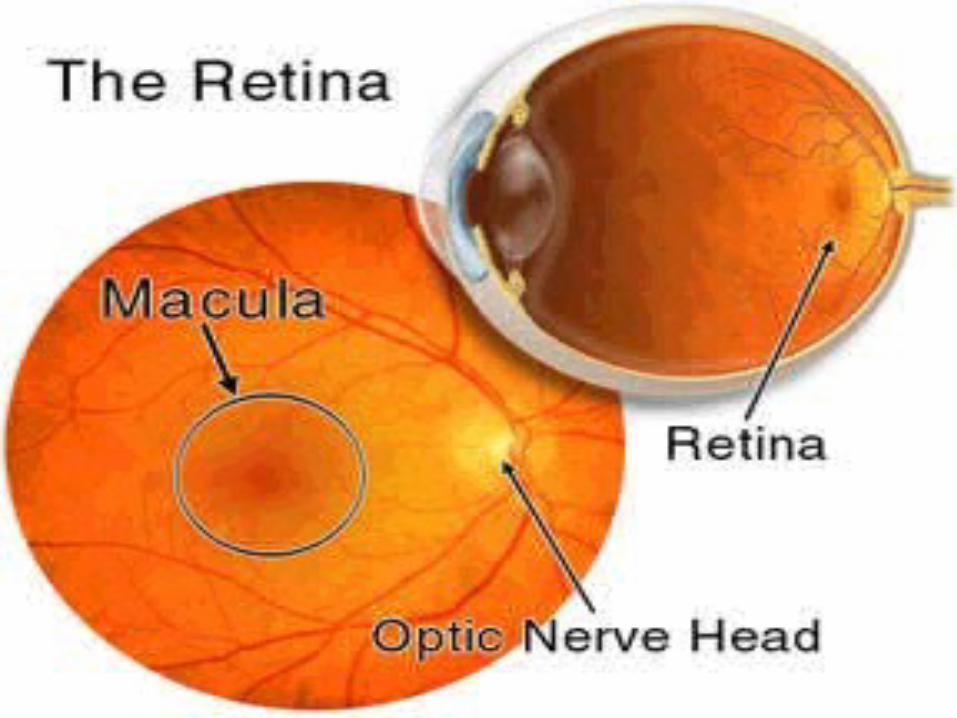
Anatomy
The uvea or uveal tract is the middle, highly vascular layer of the eyeball
• Iris
• Ciliary body
• Choroid



UVEITIS
• What is it?
• What is its importance?

The ProblemUveitis continues to blind people, even 60 years
after the introduction of steroid therapy.
12.3 million cases in the USA
45,000 new cases/year in the USA alone
10% of all cases of blindness
Annual costs in the USA: $242.6 million

The ProblemUveitis is the third leading cause of preventable
blindness in developed countries

How Does Uveitis Blind?
• Glaucoma

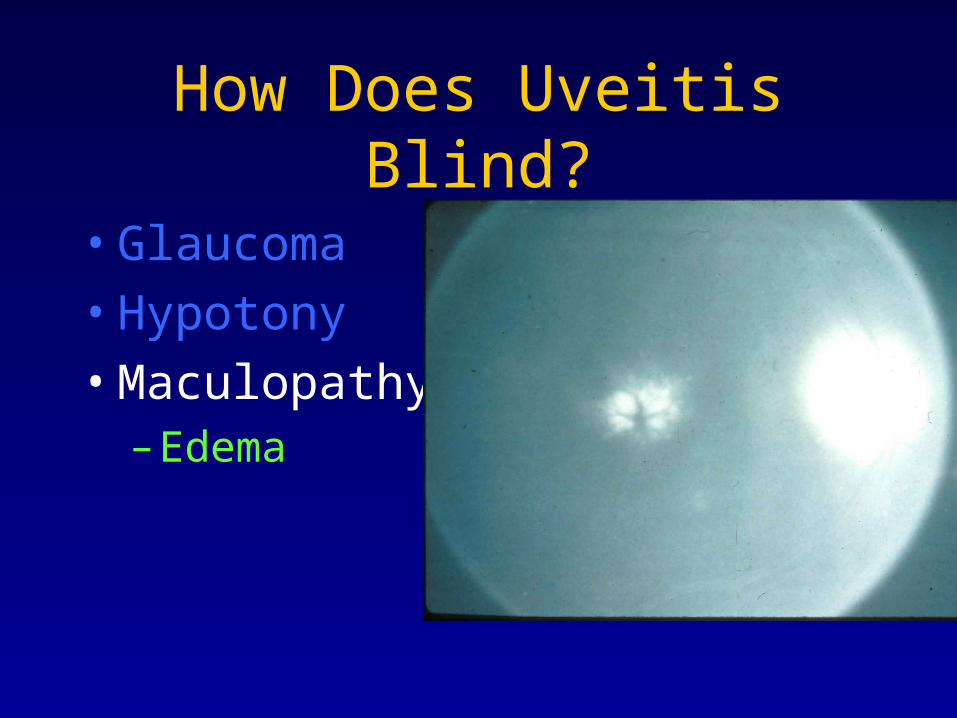
How Does Uveitis Blind?
• Glaucoma
• Hypotony
• Maculopathy– Edema

How Does Uveitis Blind?
• Glaucoma
• Hypotony
• Maculopathy– Edema
– Cysts/holes

How Does Uveitis Blind?
• Glaucoma
• Hypotony
• Maculopathy– Edema
– Cysts/holes
– Membrane

How Does Uveitis Blind?
• Glaucoma• Hypotony• Maculopathy
– Edema
– Cysts/holes
– Membrane
• Optic neuropathy
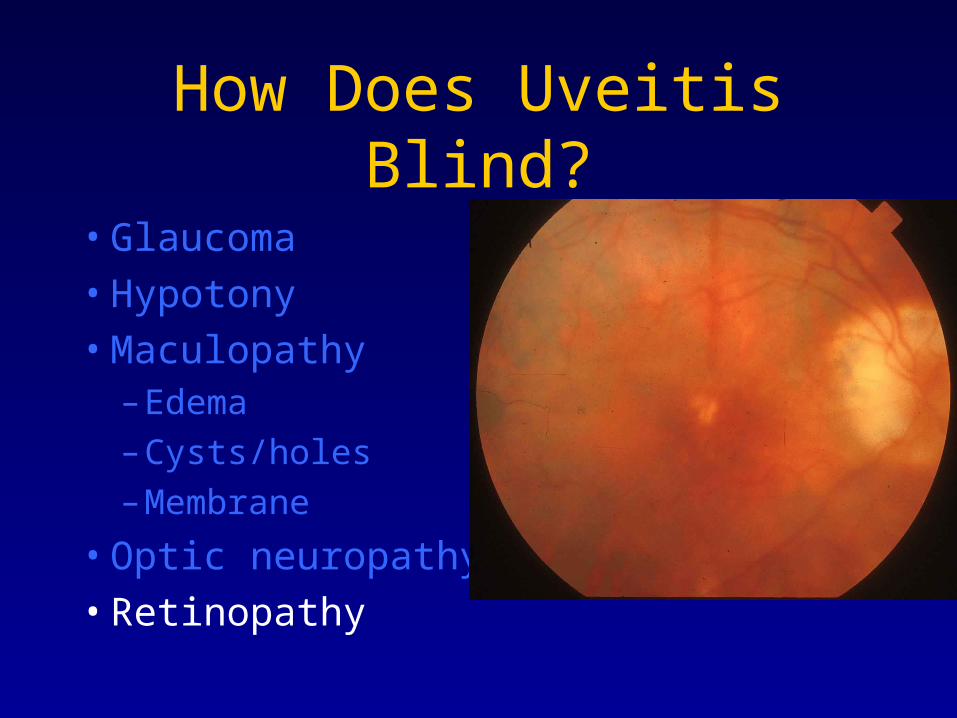
How Does Uveitis Blind?
• Glaucoma
• Hypotony
• Maculopathy– Edema
– Cysts/holes
– Membrane
• Optic neuropathy
• Retinopathy

How Does Uveitis Blind?• Glaucoma• Hypotony• Maculopathy
– Edema
– Cysts/holes
– Membrane
• Optic neuropathy• Retinopathy• Neovascularization

What Is the Evidence?• Smith RE. 1989. Pars Planitis. In: Medical Retina, chapter
96
• Laaksonen AL. 1966. A prognostic study of JRA. Analysis of 544 cases. Acta Paediatr Scand. 1966;Suppl:166
• Kanski JJ. JRA and uveitis. Surv Ophthalmol. 1990;34:253-67
• Rothova A, et al. 1996. Causes and frequency of blindness in patients with intraocular inflammatory disease. Br J Ophthalmol. 80
• 35% of uveitic eyes: blind

UVEITIS
• What is it?
• What is its importance?
• What is the history of its therapy?

Uveitis Therapy Through the Ages
• The Ebers Papyrus (1500 BC) - Egypt
• Hippocratic Corpus (4th century BC) - Greece
• Galen (AD 131-201) – Rome
• Aetius of Amida (AD 502-575) – Byzantium
• Yves (1772) – Paris
• Schmidt (1800) – Vienna
• Waldrop, Saunders, Travers, MacKenzia, Middlemore, Dalrymple (1808-1852) - England

Uveitis Therapy Through the Ages
• The Edwin Smith Surgical Papyrus
New York Academy of Medicine
1700 BC
The oldest known existing ophthalmic document
Based upon, among other things, writings from the time of Imhotep (2640 BC)

Uveitis Therapy Through the Ages
The Edwin Smith Surgical Papyrus contains references to inflammatory conditions of the eye.
Physicians with special interest in the eye were identifiable as early as the 6th Egyptian Dynasty (2400 BC).

Uveitis Therapy Through the Ages
Pepi-Ankh-Or-Iri, physician to the Pharaoh
The most ancient identifiable ophthalmologist
Royal Oculist
Palace Eye Physician and Guardian of the Anus

Uveitis Therapy Through the Ages
Pepi-Ankh-Or-Iri embraced the concept of whdw (ukedhu), “the rotten stuff par excellence”
He subscribed to the practice of expurgation therapy for uveitis.
This practice continued through the next 3900 years for a variety of ailments.
Uveitis Therapy Through the Ages
Additional therapies evolving through time included employment of poltices and solutions
100 of the 237 medication recipes in the Ebers papyrus are for eye disease
Zinc, antimony, copper, aloe, yellow ochre, red ochre, myrrh, malachite, ink powder, galena and djaret were predominant.

Uveitis Therapy Through the Ages
Roman period : 2ndC BC – 4thC AD
• Cannabis, opium, plant extracts
• Cathartics and enemas
Uveitis Therapy Through the Ages
Byzantine period : 4thC AD – 15thC AD
• Opium, barley, milk, honey, oil, breast milk, egg white, iron, copper, pepper drops and poltices
• Blood letting
• Oral and rectal administration of antidotes

Uveitis Therapy Through the Ages
Modern period (15thC AD to present)
Scarpa, 1806 : “A strong countrywoman, 35 years old, was brought into the hospital in April 1796, on account of violent, acute ophthalmia in both her eyes, with great tumefaction of the eyelids, redness of the conjunctiva, pain, and fever”


Uveitis Therapy Through the Ages
Scarpa, 1806 : “I took away blood abundantly from the arm, foot, and also locally by means of leeches applied near both the angles of the eyes, and I also purged her” These remedies helped to abate the inflammatory stage of the violent ophthalmia.
Emollient herbs boiled in milk; quince seed mucilage; bags of tepid mallows; blistering


Louis Braille – 1809-1852
It was during this era that a very young French boy was blinded in one eye by an accidental puncture of that eye with an awl in his father’s saddle shop.
Sympathetic ophthalmia uveitis blinded the other eye by the time the child was 9 years old

Uveitis Therapy Through the Ages
MacKenzie, 1830.Dilation of the pupil with tincture of
belladonna, bloodletting, purging, blister therapy
1900 – Fever therapy: fever induced by intramuscular injections of milk and subsequently with typhoid protein. Sometimes fatal; persisted into the early 1950’s
Uveitis Therapy Through the Ages
1949 – Hensch – Corticosteroid therapy
1950 – Dan Gordon – Cornell University, New York City


The History of Immunosuppressive Therapy for Uveitis
E. Roda-Perez. El tratamiento de las uveitis de etiologia ignota con mostaza nitrogenada. Arch Soc Oftal Hisp Am. 1952; 12: 131-151

The History of Immunosuppressive Therapy for Uveitis
Wong – 1965
Newell – 1966
Moore – 1968
Gills – 1970
Mamo – 1970
Godfrey – 1974
Andrash - 1978
Martinez - 1978

Prevalence of Visual Disability and Blindness Despite Corticosteroid
Therapy:It’s a Disgrace!
Evidence-based analysis of peer-reviewed literature indicates that the prevalence of visual disability and blindness secondary to uveitis has not measurably changed in the past 40 years.
Why is that? How can that possibly be?

Steroid MonotherapyStuck in second gear
• Few departments of Ophthalmology have an Ocular Immunologist on their faculty
• Therefore,
Steroid MonotherapyStuck in second gear
Most ophthalmologists completing their residency training have never been exposed to uveitis patient management with anything other than with steroids

Lessons from Rheumatology
• Rheumatologists learned the lesson the hard way too: steroid and NSAID therapy first, reserving immunomodulatory therapy for patients with advanced disease, resulted in progressive joint damage and great disability.

Lessons from Rheumatology
• Early employment of steroid-sparing immunomodulatory, disease-modifying agents results in vastly superior outcomes
• The toxicity of medication side effects is less with this approach too

Lessons from Rheumatology
• The battle-cry throughout the world of rheumatology has, therefore, become: “The Mission is Remission”
• Ophthalmologists can and should learn from them

Lessons from RheumatologyThe battle-cry throughout the world of rheumatology
has, therefore, become: “The Mission is Remission”
Disease remission should be the goal for allrheumatologists treating childhood arthritis >> By Carol A. Wallace, MD

Lessons from Rheumatology
• Ophthalmologists should embrace this model of early steroid-sparing, remission-inducing therapy with even more vigor than does rheumatology, since the eye is so much less forgiving of chronic inflammation than is the joint, with profound life-altering consequences
So, Where Are We Today?
IMMUNOMODULATORY THERAPY
• Clear evidence for safety and effectiveness in saving vision in selected populations with uveitis patients doomed to a life of blindness without such therapy

So, Where Are We Today?
IMMUNOMODULATORY THERAPY
• Clear evidence for insufficient employment of such therapy by ophthalmologists worldwide

A View to the Future
Increased emphasis on education by subspecialty learned societies
• International Uveitis Study Group
• International Ocular Inflammation Society
• American Uveitis Society
• Uveitis Subspecialty Day – American Academy of Ophthalmology

A View to the Future
Increased emphasis on recruitment of fellowship trained ocular immunologists onto faculties of departments of ophthalmology

A View to the Future
New initiatives by “Big Pharma” on clinical trials of medications capable of affecting the immune system and ocular inflammatory disease.

A View to the Future
Basic tissue, cellular and molecular research on the causes and the mechanisms of ocular inflammatory disease eye tissue damage
A View to the Future
Basic research on the immune system and mechanisms of regulation

A View to the Future
My fantasy
Re-education and autoregulation

Re-educaton and Autoregulation
• Identification of target molecule involved in the autoimmune inflammation


OCP Target Antigen Identification
We have identified the β-4 subunit of α-6/ β-4 integrin as the target antigen in patients with ocular cicatricial pemphigoid


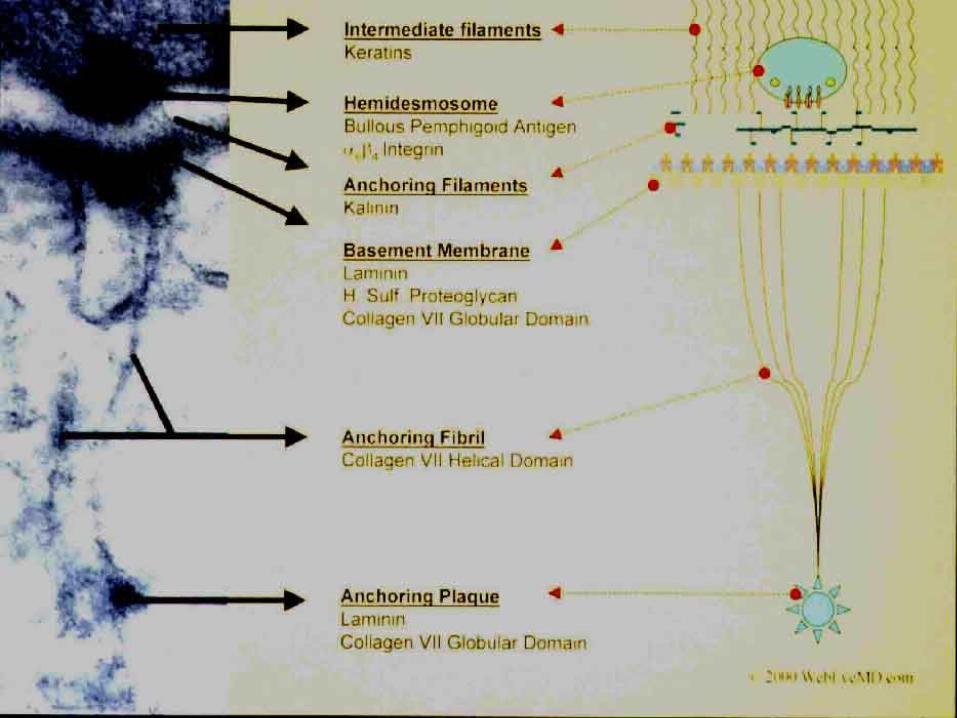
Laminin 5
BP180
PLECTINBP230
Collagen VII
Plasma MembranePlasma Membrane
?
IFIFss


Laminin 5
BP180
PLECTINBP230
Plasma MembranePlasma Membrane
Laminin 5
BP180
PLECTINBP230
Plasma MembranePlasma Membrane
Add Antibodies
?
Disassociation of hemidesmosome components

Re-educaton and Autoregulation
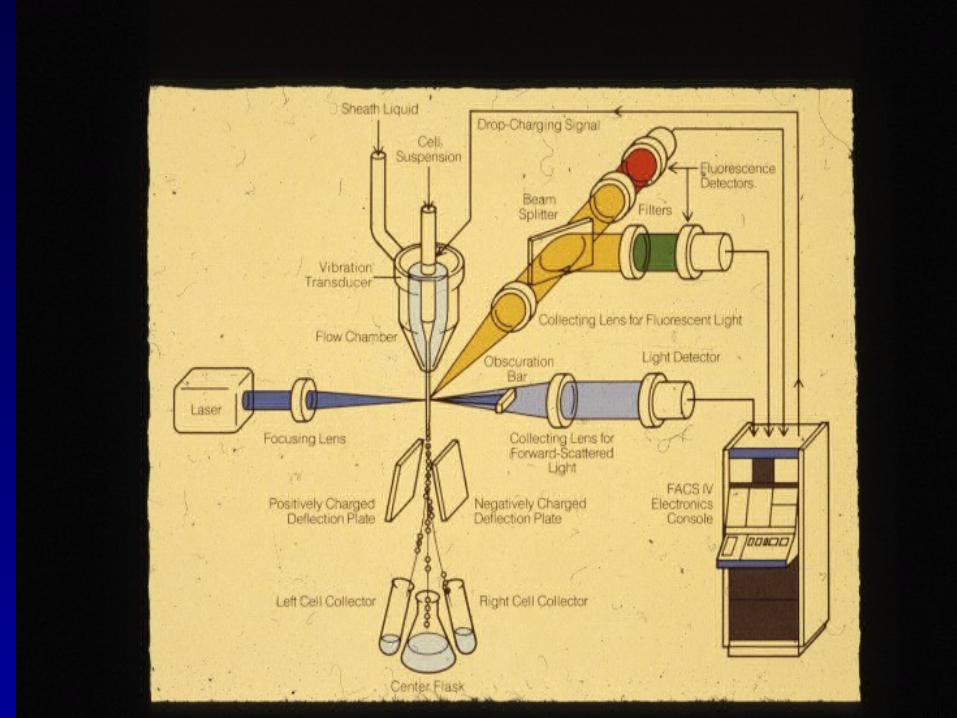
• Isolation of patient white blood cell lymphocyte popluation




Re-educaton and Autoregulation
• Incubation of patient regulatory lymphocytes with the relevant target of the immune inflammation attack, combined with molecules known to promote development of regulatory T lymphocytes


Re-educaton and Autoregulation
Transfusion of the re-educated regulatory T lymphocytes back into the patient

Re-educaton and Autoregulation
The newly re-educated regulatory T lymphocytes regulate or suppress the autoaggressive cells, thereby abrogating the autoimmune attack on the eye.
No chemotherapy. No drugs.
Resetting the immune system
Re-educaton and Autoregulation
Alternatively, what about this?

Re-educaton and Autoregulation
Sir Peter Medawar, a British zoologist, was awarded the Nobel Prize in Physiology or Medicine in 1960 for his seminal work on the immunology of the eye.

Re-education and Autoregulation
Sir Medawar’s work led to the concept of immunologic privileged sites, the eye being one such site, and of immunologic tolerance in such sites, i.e., foreign material tolerated rather than rejected when placed in such sites

Re-education and Autoregulation
Sir Medawar’s work led to an entire field of research over the ensuing 60 years on the mechanism of immunologic tolerance, and to the discovery in the 1970’s by Baruj Benacerraf of a unique popluation of white blood cells now called regulatory or suppressor T lymphocytes

Re-education and Autoregulation
Anterior chamber inoculation of protein can lead to the development of very potent regulatory T lymphocytes which regulate or suppress inflammation directed against the protein employed for that inoculation.


Re-education and Autoregulation
Might one be able, then, to induce immunologic tolerance in a patient with autoimmune disease by inoculating that patient, in the anterior chamber of the eye, with the protein against which the autoimmune reaction has developed?

Summary
• Uveitis is a potentially blinding eye problem
• It is a problem of great epidemiologic and economic importance
• Excellent therapy exists today for uveitis
• Yet far too few ophthalmolgists avail themselves and their patients of such therapy
Conclusions
PRESCRIPTIONS FOR PROGRESS• Training of ocular immunologists• Training of ophthalmology residents by ocular
immunologists• Research dedicated to uveitis; especially
identification of relevant antigen targets• Continued research dedicated to the immune
system and to regulation of it.