October 29, 2012 Monday memo Health reform update · 2012. 10. 29. · -Updated recommendations for...
13
Deloitte Center for Health Solutions October 29, 2012 Monday memo Health reform update This week’s headlines: My take Implementation update - Study: premium rate review - CMS: 2.3 million Medicare beneficiaries saved an average of $657 on prescription drugs - Physicians hesitant to participate in Medicare with looming SGR fix - Study: safety net hospitals hurt by cuts in DSH payments, lower Medicaid enrollment Legislative update - Class action lawsuit settled, Medicare enrollees with long-term medical problems entitled to coverage - Study: Medicaid block grants could cut $1.7 trillion in Medicaid - Compounding update: compounding pharmacy license revoked, CDC finds facility contaminated - House GOP claims HHS improperly using tax dollars in promoting ACA - Senate HELP Committee seeks feedback on track and trace system policy change State update - State employee health costs - Massachusetts health department officials issued warnings to compounding center - State round-up Industry news - Report: decline in the number of employers offering retiree health benefits - Updated recommendations for cervical cancer screening and hormone therapy - Report: medical devices spending up almost 1% - Study: declines in U.S. biomedical and health R&D funding threaten global competition Quotable Fact file Subscribe to the Health Care Reform Memo Deloitte Center for Health Solutions research Upcoming life sciences and health care Dbriefs webcasts Deloitte contacts My take From Paul Keckley, Executive Director, Deloitte Center for Health Solutions I speak to groups about health care three to four times weekly, but in my 35 years, last Wednesday’s was a first. The topic was simple enough: “ what middle market employers should know about health reform and what they can do to prepare.” The audience: 1,100 business executives gathered at the Ohio State University-GE Capital 2012 National
Transcript of October 29, 2012 Monday memo Health reform update · 2012. 10. 29. · -Updated recommendations for...

Deloitte Center for Health Solutions
October 29, 2012
Monday memo
Health reform update
This week’s headlines: My take
Implementation update - Study: premium rate review - CMS: 2.3 million Medicare beneficiaries saved an average of $657 on prescription drugs - Physicians hesitant to participate in Medicare with looming SGR fix - Study: safety net hospitals hurt by cuts in DSH payments, lower Medicaid enrollment
Legislative update - Class action lawsuit settled, Medicare enrollees with long-term medical problems
entitled to coverage
- Study: Medicaid block grants could cut $1.7 trillion in Medicaid
- Compounding update: compounding pharmacy license revoked, CDC finds facility contaminated
- House GOP claims HHS improperly using tax dollars in promoting ACA
- Senate HELP Committee seeks feedback on track and trace system policy change
State update - State employee health costs
- Massachusetts health department officials issued warnings to compounding center
- State round-up
Industry news - Report: decline in the number of employers offering retiree health benefits
- Updated recommendations for cervical cancer screening and hormone therapy
- Report: medical devices spending up almost 1%
- Study: declines in U.S. biomedical and health R&D funding threaten global competition
Quotable
Fact file
Subscribe to the Health Care Reform Memo
Deloitte Center for Health Solutions research
Upcoming life sciences and health care Dbriefs webcasts
Deloitte contacts
My take
From Paul Keckley, Executive Director, Deloitte Center for Health Solutions
I speak to groups about health care three to four times weekly, but in my 35 years, last
Wednesday’s was a first. The topic was simple enough: “what middle market employers
should know about health reform and what they can do to prepare.” The audience: 1,100
business executives gathered at the Ohio State University-GE Capital 2012 National

Middle Market Summit in Columbus, Ohio. The agenda: some serious heavy weights—
Warren Buffett, Jeff Immelt, and rock star-entrepreneur Sammy Hagar—a/k/a The Red
Rocker—who I followed on the program.
I was probably the only one in the room that could not sing along with his 1984 hit “I Can’t
Drive 55” and my suit and tie definitely contrasted with his tee shirt and sandals. When I
took the stage, I had a sinking feeling that health care was last on the audience members’
minds: after all, they had just given the 65-year-old music legend a standing “O” as much
for his success as an entrepreneur (Cabo Wabo Tequila, Sammy’s Beach Bar Rum) as
his music. Sometimes I feel like a brown shoe at a white tie affair: it was certainly the case
last week.
Here’s what I told the group:
Health care is a big deal. It impacts everyone. It is the fastest growing line item
expense in the budgets of the federal and state government, and one of the fastest
for companies that provide insurance coverage and in the average U.S. household.
And it touches everyone.
Health costs can be reduced, but only if the health care system—including
individuals, policymakers, and employers—drive changes to the fundamentals of
the industry. Incentives based on volume must be replaced by incentives for doing
the right things that are evidence-based the first time. And the health system must
embrace accountability; adherence to evidence-based necessary care; mechanisms
to alter unhealthy behaviors; transparency for prices and quality; and technologies
that enable improved coordination, reduced error, and improved efficiency. To
embrace these changes, employers must understand the health system, not just
how their benefits are designed. There’s a difference.
The Affordable Care Act (ACA) is one of many legislative efforts to fix the system.
But transformation of the health system requires more than federal legislative
action: in most communities and states, employers are catalysts for meaningful
improvements.
Business leaders get it. They see a need to get the U.S. fiscal house in order. They
recognize the solution requires a combination of actions including tax reforms and
reduced government spending. And they understand health reform must be on the table
at the same time. Health costs impact corporate profits and global competitiveness for
large multi-nationals—that’s well documented. But even among smaller and mid-sized
companies, it’s about access to a productive workforce without being hampered by health
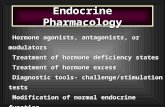
costs that defer growth and innovation. These findings from the National Center for the
Middle Market (NCMM) 3rd
quarter survey underscore the salience of health care to the
viability of mid-sized companies:

Source: NCMM Middle Market Indicator (MMI) 3Q 2012
Note: middle market companies have between $10 million and $1 billion in revenues.
As I reflect, it may have been the most challenging speech I’ve ever given, perhaps
because I followed Sammy, and perhaps because the topic is so delicate: employers have
a huge opportunity to impact reform of the health system, but they need to understand
health care—not just benefits design—and most don’t.
They know their costs are significant and growing: for single coverage, employers pay
83% of the $5,615 total premium and for family coverage, they invest 73% of the $15,745 total premium to get and keep a healthy, productive workforce (Source: Kaiser Family
Foundation, 2012 Employer Health Benefits Survey). They understand their employees
value health coverage as a benefit. Their issue is affordability: in the last decade, 10% of
employers dropped coverage due to costs, and in the decade ahead, we estimate 9%
more will drop simply due to costs (Source: 2012 Deloitte Survey of U.S. Employers).
They know it matters to their employees: only 20% of employees with employer-
sponsored coverage feel protected from health costs that might wipe out their household
financial security. But most don’t understand the health system—how it actually operates,
how clinical decisions are made, how necessary and unnecessary costs are incurred, or
how each of the system’s multiple sectors relate to each other or not.
I am going to download Sammy’s songs this week and learn the words to “I Can’t Drive
55” so I can sing along next time. I need to get out of my musical comfort zone.
And employers need to get out of their comfort zone and play an active role in fixing the
health system. They need to invest time in understanding the health system, not just its
costs, and become catalysts in its transformation.
return to top
75%
77%
81%
86%
92%
79%
70%
85%
85%
90%
76%
77%
84%
89%
91%
0% 20% 40% 60% 80% 100%
Commodity costs
Talent management
Uncertainty of government actions
Ability to maintain margins
Health care costs
Top Middle Market Business Challenges
Q3
Q2
Q1

Implementation update
Study: premium rate review Per Section 10003 of the ACA, health insurers must justify increases in premium rates
above 10% to either state or federal reviewers. Kaiser Family Foundation researchers
analyzed 846 rate filings from 41 states that were reviewed by state regulators (798) or
the U.S. Department of Health and Human Services (HHS) (448): “As of August 1, 2012,
44 states and DC have rate review programs that have been deemed by HHS to be
effective in at least one insurance market, meaning that they meet such criteria as having
the authority under state law to determine the reasonableness of rate increases, having a
transparent process for making the information publicly available, and allowing public
comment on proposed rate changes.”
Findings from 32 states and DC, which had publically available rate review data:
One in five resulted in a lower premium increase than the insurer initially requested
Individual group premium: 8.9% average rate increase requested, 6.3% average
rate increase approved
Small group premium: 5.2% average rate increase requested, 4.7% average rate
increase implemented
Findings in states where federal reviews were conducted:
The average premium rate request was 16%. Note: the average rate request is
higher for federal reviews because HHS can only review rate increases at or above
10%; states with rate review programs in place monitor all increases
77% of filings were determined unreasonable by HHS
19% were found to be “not unreasonable” by HHS
Background: prior to the passing of the ACA, many states had rate review programs in
place; Section 10003 set a floor of requirements. States with effective programs in place
began reviewing proposed increases in September 2011. HHS conducts reviews in states
without effective programs in place, but does not have the authority to deny rate
increases. HHS and states are required to make information publicly available for
requests at or above 10%.
(Source: Kaiser Family Foundation, “Quantifying the Effects of Health Insurance Rate
Review,” October 2012)
return to top
CMS: 2.3 million Medicare beneficiaries saved an average of $657 on
prescription drugs Thursday, the Centers for Medicare & Medicaid Services (CMS) reported that in the first
nine months of 2012, 2.3 million beneficiaries in the Medicare prescription drug “donut
hole” saved an average of $657, and 20.7 million beneficiaries received at least one
preventive service with no deductible or co-payment as a result of Sections 3301, 4103,
4104, and 4105 of ACA. To date, CMS reports that 5.6 million beneficiaries have saved
$4.8 billion on prescription drugs since the enactment of these provisions.
return to top
Physicians hesitant to participate in Medicare with looming SGR fix According to a Medical Group Management Association (MGMA) survey of physicians,
82% of practices would be likely to participate in accountable care organizations, patient-
centered medical homes, or bundled payment and shared savings pilots if Congress

passed legislation to override mandated sustainable growth rate (SGR) reductions for the
next five years. Key findings:
If the scheduled 27% reduction in Medicare reimbursement takes place on January
1, 2013: 45% of practices say they are very likely to reduce the number of
appointments for new Medicare patients, 27% say they probably would reduce the
number of appointments available for their current Medicare patients, 31% are very
likely to stop accepting new Medicare patients altogether.
More than half would likely reduce size of their staff; 75% say they would reduce
employee salaries or benefits.
In the past five years, 60% percent of practices reported reducing staff salaries,
benefits, or delaying buying new clinical equipment or facilities.
(Source: MGMA, “Performance and Practices of Successful Medical Groups: 2012 Report
Based on 2011 Data,” October 2012)
Note: stay tuned for an upcoming Issue Brief from the Deloitte Center for Health
Solutions—“Understanding the Sustainable Growth Rate: Analyzing the `Doc Fix.’”
return to top
Study: safety net hospitals hurt by cuts in DSH payments, lower Medicaid
enrollment Thursday, the National Association of Public Hospitals and Health Systems (NAPH)
released its analysis of the Congressional Budget Office’s forecast of insurance coverage
for fiscal year (FY) 2014 to FY2019, concluding hospitals will spend $53.3 billion more on
uncompensated care by 2019 than estimated prior to the enactment of ACA. Two major
factors were cited for the increase: reductions in Medicaid disproportionate share hospital
(DSH) payments to safety net hospitals starting in FY2014, and lower participation in
Medicaid as a result of the June 28 Supreme Court ruling that disallowed mandatory
eligibility at 133% of the federal poverty level (FPL).
Background: beginning in FY2014, per Section 2551 of the ACA, CMS will reduce DSH
Medicaid allotments by a total of $18.1 million. States with a lower percentage of their
population uninsured will receive a 50% reduction, and states with a larger percentage of
uninsured will receive a 25% reduction. Per Section 3133 of ACA, CMS will reduce DSH
Medicare payments by a total of $22 billion over ten years. Initially CMS will reduce
Medicare DSH payments by 75% in FY2014, and subsequently increase payments based
on the percent of the population uninsured and the amount of uncompensated care.
return to top
Legislative update
Class action lawsuit settled, Medicare enrollees with long-term medical
problems entitled to coverage Last Monday, the U.S. Department of Justice announced the proposed settlement of a
class action lawsuit brought on behalf of Medicare plaintiffs that, if approved by the U.S.
District Court judge, will change a long-standing policy toward payments for certain home,
skilled, and long-term care services for Medicare enrollees whose health status was not
deemed to be “improved” as a result of the services. The proposed settlement agreement
requires that CMS re-write the Medicare manual for nursing and therapy services to make
clear that provision of these services no longer requires evidence that their provision is directly linked to health status improvement. Note: the settlement will be most meaningful
to patients and family members with Alzheimer’s/Parkinson’s, stroke, spinal cord and
traumatic brain injuries, and others. The settlement stemmed from a case where an 81-

year-old woman was denied home health services through Medicare because her multiple
sclerosis was not improving.
return to top
Study: Medicaid block grants could cut $1.7 trillion in Medicaid Block grants to states for Medicaid could cut $1.7 trillion from the Medicaid program over
the next ten years ($932 billion from repealing the ACA and $810 billion from transitioning
to a block grant), per an analysis by the Urban Institute and the Kaiser Commission on
Medicaid and the Uninsured. Key findings:
Hospitals payments could be reduced $363.8 billion and nursing home payments
$220.2 billion from 2013-2022 under a block grant scenario
Medicaid enrollment could be reduced by 17 million if the ACA is repealed
77% increase in state spending with no efficiency gains; 46% if Medicaid spending
per enrollee was held to the rate of growth in GDP per capita under a block grant
scenario
(Source: Kaiser Commission on Medicaid and the Uninsured and the Urban Institute,
“National and State-by-State Impact of the 2012 House Republican Budget Plan for
Medicaid,” October 2012)
return to top
Compounding update: compounding pharmacy license revoked, CDC finds
facility contaminated The fallout continued last week for the Massachusetts compounding pharmacy linked to
the multi-state fungal meningitis outbreak responsible for 294 known cases of fungal
meningitis and 24 deaths. Tuesday, the Massachusetts Board of Pharmacy permanently
revoked the New England Compounding Center’s (NECC) license after several health and
safety violations were discovered. An inspection conducted by the Massachusetts
Department of Public Health and U.S. Food and Drug Administration (FDA) found that
black fungus particles were visible in sealed vials of the recalled steroid, NECC distributed
products on 13 separate occasions before receiving sterility test results, large batches of
compounded sterile product were distributed directly to facilities for general use without
requiring a prescription for an individual patient, and sterilization procedures were not
followed properly.
Related: members of the U.S. House Energy and Commerce Committee sent a letter to
NECC’s owner and former owner seeking documents related to the recent outbreak as
well as the history of investigations and operations of the NECC and associated entities
dating back to 2002. NECC’s owner declined to comply with the Committee’s earlier
request for a briefing on the outbreak. The letter highlighted that prior to the meningitis
investigation, joint federal and state inspections of the NECC facility occurred in 2002,
2003, and 2004 in response to an adverse event reported to the FDA. Public Citizen’s
Health Research Group issued a letter to HHS Secretary Kathleen Sebelius requesting
that the HHS Office of Inspector General (OIG) investigate whether the FDA exerted full
use of its legal authority to regulate NECC after prior inspections discovered violations.
return to top
House GOP claims HHS improperly using tax dollars in promoting ACA Last week, GOP Chairmen of the House Subcommittee on Oversight Dave Camp (R-MI)
and Charles Boustany (R-LA) sent HHS Secretary Kathleen Sebelius a letter inquiring
about the status of materials requested in May 2012 regarding the use of taxpayer dollars

on the promotion of the ACA. The Subcommittee claims HHS is improperly using taxpayer
dollars to promote “Obamacare.” The information is requested by October 31, 2012.
return to top
Senate HELP Committee seeks feedback on track and trace system policy
change The Senate Committee on Health, Education, Labor, and Pensions (HELP) released a
draft proposal on drug distribution security, referred to as a “track and trace” system, last
week requesting comments from stakeholders on the policy options proposed in the
report. Comments are due November 7, 2012, the day after the election, and
policymakers hope to draft and pass legislation by the end of the year. Congress
attempted to address drug distribution safety earlier this year, but efforts were stalled due
to disagreements on the requirements and implementation of a track and trace system.
Background: “track and trace” language was included in the re-authorization of the
Prescription Drug User Fee Act (PDUFA) of 2012 this summer, but was removed due to
industry opposition. Manufacturers oppose the use of individual identifiers that require
tracking of single packages of drugs but favor tracking at the lot level.
A federal track and trace system would allow the FDA to track a drug from its origination,
through the manufacturing process, to the point of sale. If a counterfeit, diverted, stolen, or
otherwise damaged product is reported, the FDA would be able to ensure timely
intervention to prevent the damaged product from being distributed widely. Currently,
some states have laws in place to enhance drug security, but a federal system would
standardize processes across state lines. In 2015, California will require unique identifiers
to be placed on all drugs.
return to top
State update
State employee health costs State government workers have richer health benefits than the private sector, but the gap
has narrowed from $1,523 in 2007 to $891 in 2012 while the numbers of state workers not
paying a co-payment or premium has shrunk from 39% in 2007 to 30% in 2012 with an average of $425/month out-of-pocket (vs. 17% in the private sector). (Source: Bureau of
Labor Statistics [BLS] National Compensation Survey)
return to top
Massachusetts health department officials issued warnings to
compounding center Massachusetts Department of Health officials notified the NECC of safety and quality
improvements dating back to 1999. Per the Department’s records, each citation was
resolved. To date, nearly 300 cases of fungal meningitis and 24 deaths have been linked
to the tainted injectable from NECC.
return to top
State round-up Tuesday, an Indiana law preventing Planned Parenthood from obtaining
reimbursement from the state Medicaid program because it provides abortion
services was overturned by the Seventh Circuit U.S. Court of Appeals. The ruling
differs from a Fifth Circuit U.S. Court of Appeals decision to uphold legislation that
refuses state funding to Planned Parenthood and other abortion providers in Texas.
A settlement between legal advocates and the state of Pennsylvania's public

welfare office acknowledges up to 100,000 individuals may have been wrongly
terminated from the state’s Medicaid program due to eligibility. The state agreed to
increase use of electronic databases to more accurately verify Medicaid eligibility. If
re-enrolled, beneficiaries may submit receipts for reimbursement for any cost
incurred for Medicaid covered expenses during the period they were without
coverage.
Enrollees in California's Major Risk Medical Insurance Program will see reduced
premium rates in 2013 matching the Pre-Existing Condition Insurance Plan (PCIP),
the federal program established per Section 1101 of the ACA for individuals with
pre-existing health conditions unable to access affordable coverage. This measure
will serve as a stopgap until 2014 when high-risk subscribers may purchase
coverage through the state Health Benefit Exchange.
Mississippi estimates more than 300,000 residents could be added to its Medicaid
program by 2025 with projected cumulative state costs (2014-2025) of $1.07 billion.
The cost to state government will be just under $100 million in 2017 when the
federal match is reduced to 95%.
In a letter to Governor Mary Fallin (R-OK), Senator Tom Coburn (R-OK)
recommended Oklahoma not expand Medicaid to 133% of the FPL and instead
work on improving public programs already in place.
return to top
Industry news
Report: decline in the number of employers offering retiree health benefits The number of private businesses offering retiree health benefits decreased significantly
between 1997 and 2010, and employers that still offer retiree health benefits have
generally adapted benefit packages resulting in increased retiree premiums, decreased
eligibility, or reduced coverage features. Notable findings:
Private firms offering retiree health benefits decreased from 29% to 17% resulting in
a net 4% decrease in the percentage of retirees over age 65 with health benefits.
Most employers (78%) are very or somewhat likely to increase retiree contributions
to premiums in the future.
Employees expecting health benefits upon retirement have decreased, from 45% to
32% of workers.
While 35% of current employees age 45 to 64 expected to receive health benefits
upon retirement, 25% of early retirees and 16% of Medicare-eligible retirees actually
received them in 2010.
(Source: Employee Benefit Research Institute, “Employment-Based Retiree Health
Benefits: Trends in Access and Coverage, 1997‒2010,” October 2012)
return to top
Updated recommendations for cervical cancer screening and hormone
therapy Last Monday, the American College of Obstetricians and Gynecologists (ACOG) issued
new guidelines recommending that most women should be screened for cervical cancer
(Pap test) once every three to five years, instead of annually. The new guidelines also
recommend that women over the age of 30 receive the Pap test and the human
papillomavirus (HPV) test simultaneously every five years.
Related: the U.S. Preventive Services Task Force (USPSTF) recommended against the

use of combined estrogen and progestin hormone therapy treatments for the prevention of
chronic conditions in postmenopausal women, and the use of estrogen for the prevention
of chronic conditions in postmenopausal women who have had a hysterectomy. Both
treatments received a grade “D” rating from the Task Force based on the evidence of both
the benefits and harms of the service.
Background: per Section 2713 of ACA any group health plan or insurer in the group or
individual market must provide preventive health services rated grade “A” or “B” by
USPSTF with no cost sharing or co-payment beginning August 1, 2012.
return to top
Report: medical devices spending up almost 1% In 2010, medical device spending was 6% ($156 billion) of the $2.6 trillion the nation
spent on health care, representing an increase of 0.7% from 1989 to 2010. During this
time, the Health Care Consumer Price Index (MC-CPI) increased 4.7%, and the Medical
Care Services Consumer Price Index (MCS-CPI) increased 5%
(Source: Gerald Donahoe, Guy King, “Estimates of Medical Device Spending in the
United States,” October 2012)
return to top
Study: declines in U.S. biomedical and health R&D funding threaten global
competition A Research!America analysis of biomedical and health research and development (R&D)
spending in the U.S. revealed that R&D declined 3% ($4 billion) in FY2011, the first
spending decline since 2002. The report noted that much of this decline comes from the
expiration of $10.4 billion in funding designated to the National Institutes of Health (NIH)
by the American Recovery and Reinvestment Act. Per the report, sequestration might
threaten the nation’s biomedical and health research capacity and ability to compete
globally by reducing federal biomedical and health research funding by 8-10%. Notable
findings:
Federal funding for research declined 14% in FY11, totaling $39.5 billion in 2011
Overall industry investment in R&D increased 1.4% from 2010, $77.6 billion in 2011
Pharmaceutical industry investment in R&D increased 3% from 2010, $38.5 billion
in 2011
Biotechnology investment in R&D declined 3% ($800 billion) from 2010, $29.2
billion in 2011
Medical device industry investment in R&D increased 7.4% from 2010, $9.8 billion
in 2011
(Source: Research!America, “2011 U.S. Investment in Health Research,” October 2012)
return to top
Quotable “Congress needs to grant the FDA whatever additional powers it deems necessary to
inspect the pharmacies, monitor their sales and judge the safety or effectiveness of their
products. The problems need to be addressed on a nationwide basis, not just through states, which often have limited resources and expertise.”—The New York Times,
Editorial Page, “Deeper Concerns about Drug Compounding,” October 26, 2012
“I was always confident that the Affordable Care Act, a.k.a. Obamacare, was

constitutional. It was interesting to see them, or Justice Roberts in particular, take the
approach that this was constitutional under the taxing power. The truth is that if you look
at the precedents dating back to the 1930s, this was clearly constitutional under the
Commerce Clause. I think Justice Roberts made a decision that allowed him to preserve
the law but allowed him to keep in reserve the desire, maybe, to scale back Congress’
power under the Commerce Clause in future cases.”—President Barack Obama, Rolling
Stone, October 2012
return to top
Fact file Economic outlook: the GDP is expected to grow 2.3% next year, up from 1.65%
in first half of 2012; unemployment is expected to end 2013 at 7.6% vs. 7.8% in
2012; job growth is expected to average 175,000/month. (Source: USA Today
survey of 48 economists, October 15-18, 2012)
Obesity and school food: kids consume 30-50% of their calories at school; one in
three is overweight or obese. (Source: U.S. Department of Agriculture [USDA])
High caffeine sports drinks: emergency room (ER) visits attributable to sports
drinks increased ten times from 1,128 in 2005 to 13,114 in 2009. (Source:
Substance Abuse and Mental Health Services Administration [SAMHSA],
November 22, 2011)
Debate viewership: October 3 (domestic policy)—67.2 million, October 11
(domestic and foreign policy)—51.4 million, October 22 (foreign policy)—65.6
million. (Source: Nielsen)
College tuition: average cost for tuition, room, and board after financial aid is
$12,110 vs. sticker price of $17,860 for public four-year schools and $23,840 for
private four-year school sticker price of $39,520; represents a sticker price increase of 3% and actual price increase of 4.8% over prior year. (Source: The College
Board)
Multigenerational homes: 4.3 million U.S. households—5.6% of total—have three
or more generations—up from 3.7% in 2000. (Source: U.S. Census Bureau 2009-
2011 American Community Survey)
Campaign 2012 polling: 31.6% of the samples used in polling in this cycle are on
mobile devices. (Source: Real Clear Politics average of the eight polls it follows)
Medicare appeals: Part A hospitals: 14.1 million Medicare claims were denied,
295,000 were appealed, 40% of the appeals were successful; Part B physicians:
93 million claims denied, 2.4 million appealed, 53% reversed. (Source: CMS)
Lower income household consumption: households with incomes in the bottom
fifth account for 8.7% of total consumption—unchanged since 2000; 47.7% have
personal computers vs. 19.8% in 2000, households with six or more rooms increased from 21.9% to 30%, 75.5% have cell phones. (Source: American
Enterprise Institute, BLS Consumer Expenditure Survey)
Medicaid enrollment: Medicaid spending increased 2% in FY2012 with a 3.2%
increase in enrollment compared to a 9.7% increase in spending and a 4.4%
increase in enrollment in FY2011. (Source: Kaiser Commission on Medicaid and
the Uninsured, October 2012)
Medical school applicants: 45,266 applicants for 2012 school year, a 3.1%
increase from 2011. Total enrollment is projected to increase by 30% within the
next three to four years. In 2013, four new medical schools are scheduled to open.

(Source: Association of American Medical Colleges [AAMC], “Medical School
Enrollment Continues to Climb with New Diversity Gains,” October 2012)
Medical cost burden: the recession did not increase the percentage of individual
discretionary spending for health care over 10% because individuals decreased
out-of-pocket spending overall to adjust to their lower compensation; 19% of
people under age 65 spend more than 10% of their discretionary income on health
care. (Source: Health Affairs, “Despite the Recession’s Effects on Incomes and
Jobs, the Share of People With High Medical Costs Was Mostly Unchanged,”
October 2012)
Adverse birthing events: on average 52,000 women experience severe maternal
morbidity per year; 114% increase in 2009 from 1998 for postpartum
hospitalizations. (Source: Obstetrics & Gynecology, “Severe Maternal Morbidity
Among Delivery and Postpartum Hospitalizations in the United States,” November
2012)
Health insurance coverage: in 2011, 92.5% of children had access to health
insurance. Significant drop in health insurance coverage for kids occurred in 20
states, down from 34 states between 2009 and 2010. (Source: Georgetown
University Health Policy Institute Center for Children and Families, “Uninsured
Children 2009-2011: Charting the Nation’s Progress,” October 2012)
Access to orthopedic surgeons for Medicaid enrollees: in the past six years
the number of orthopedic surgeons accepting children enrolled in Medicaid with a
broken arm dropped 40%; access to orthopedic surgeons for children with private
insurance decreased 10% since 1996. (Source: American Academy of Pediatrics,
“Fewer Orthopedic Surgeons Accepting Pediatric Medicaid Patients,” October
2012)
Consumer reaction to health information exchange: 86% want personal health
information (PHI) to be protected, 86% want to be continually informed about who
has seen their health information, and 78% want to control what information is shared. (Source: Annals of Family Medicine, “Health Care Consumers’ Preferences
Around Health Information Exchange,” October 2012)
Global comparisons: the U.S. spends 2.5 times more than the average health
expenditure per person of the 34 Organisation for Economic Co-operation and
Development (OECD) countries. Notable comparisons: physicians/1,000: U.S. 2.4
vs. OECD 3.1; hospital beds/1,000: U.S. 2.6 vs. OECD 3.4; life expectancy at birth:
U.S. 78.7 vs. OECD 79.8. (Source: OECD Health Data 2012)
return to top
Subscribe to the Health Care Reform Memo
Health Care Reform Memo — The weekly Health Care Reform Memo is available for
subscription. Please visit www.deloitte.com/us/healthmemos/subscribe. First, confirm
your sector(s) of interest. Then, select the Health Care Reform Memo as one of your
Email Newsletters (under Health Sciences). return to top
Deloitte Center for Health Solutions research To learn more about recent Deloitte thought leadership, please visit Deloitte University
Press (www.DUPress.com).
Coming soon: Understanding the Sustainable Growth Rate: Analyzing the “Doc Fix”

2012 Survey of U.S. Health Care Consumers – INFOBrief series and Five-year report
Currently available: Impact of Health Care Reform on Insurance Coverage: Projection Scenarios Over
10 Years – Update 2012—October 2012. Available online at
www.deloitte.com/us/2012coveragemodel
State Medicaid Program Management: Update and considerations—September 2012.
Available online at www.deloitte.com/us/2012statemedicaid
Meeting the Challenge: Maximizing the value of employer-sponsored health care—
August 2012. Available online at www.deloitte.com/us/meetingthechallenge
2012 Deloitte Survey of U.S. Employers: Opinions about the U.S. health care system
and plans for employee health benefits—July 2012. Available online at
www.deloitte.com/us/2012employersurvey
Deloitte 2012 Survey of U.S. Health Care Consumers: The performance of the health
care system and health care reform—June 2012. Available online at
www.deloitte.com/us/2012consumerism
Health Care Reform: Center Stage 2012 Perspectives from consumers, physicians
and employers—June 2012. Available online at
www.deloitte.com/us/healthcarecenterstage2012
return to top
Upcoming life sciences and health care Dbrief webcasts Anticipating tomorrow's complex issues and new strategies is a challenge. Stay fresh with
Dbriefs – live webcasts that give you valuable insights on important developments
affecting your business.
November 13: Market Forces at Work: Life Sciences Implications of Changes in Health
Care Delivery, Access, and Coverage
December 11: What's Around the Corner for Health Care Organizations and
Policymakers?
return to top
Deloitte contacts
Paul H. Keckley, Ph.D., Executive Director, Deloitte Center for Health Solutions
Jessica Blume, U.S. Public Sector National Industry Leader, Deloitte LLP
Bill Copeland, U.S. Life Sciences and Health Care National Industry Leader, Deloitte LLP
Jason Girzadas, National Managing Director, Life Sciences & Health Care, Deloitte
Consulting LLP ([email protected])
Harry Greenspun, M.D., Senior Advisor, Health Care Transformation and Technology,
Deloitte Center for Health Solutions ([email protected])
Mitch Morris, M.D., National Leader, Health Information Technology, Deloitte Consulting
LLP ([email protected])
George Serafin, Managing Director, Health Sciences Governance Regulatory & Risk
Strategies, Deloitte & Touche LLP ([email protected])

Rick Wald, Director, Human Capital, Deloitte Consulting LLP ([email protected])
To receive email alerts when new research is published by the Deloitte Center for Health Solutions, please register at www.deloitte.com/centerforhealthsolutions/subscribe.
To access Center research online, please visit www.deloitte.com/centerforhealthsolutions.
To arrange a briefing for your team, contact Jennifer Bohn ([email protected]).
return to top
Deloitte.com | Security | Legal | Privacy
30 Rockefeller Plaza New York, NY 10112-0015 United States
About Deloitte Deloitte refers to one or more of Deloitte Touche Tohmatsu Limited, a UK private company limited by guarantee, and its network of member firms, each of which is a legally separate and independent entity. Please see www.deloitte.com/about for a detailed description of the legal structure of Deloitte Touche Tohmatsu Limited and its member firms. Please see www.deloitte.com/us/about for a detailed description of the legal structure of Deloitte LLP and its subsidiaries. Certain services may not be available to attest clients under the rules and regulations of public accounting.
Disclaimer This publication contains general information only and Deloitte is not, by means of this publication, rendering accounting, business, financial, investment, legal, tax, or other professional advice or services. This publication is not a substitute for such professional advice or services, nor should it be used as a basis for any decision or action that may affect your business. Before making any decision or taking any action that may affect your business, you should consult a qualified professional advisor.
Deloitte shall not be responsible for any loss sustained by any person who relies on this publication.
Copyright © 2012 Deloitte Development LLC. All rights reserved. Member of Deloitte Touche Tohmatsu Limited
To unsubscribe, reply to this message and add “Unsubscribe” in the subject line.