October 19, 2017 - Idaho Medicaid Pharmacy Program | … pain reliever for most state Medicaid...
103
October 19, 2017 1
Transcript of October 19, 2017 - Idaho Medicaid Pharmacy Program | … pain reliever for most state Medicaid...
October 19, 2017
1
Ongoing Reviews
Narcotic Prescribing Improvement Project
Top 150 Utilizers
Methadone
Buprenorphine and benzodiazepine concomitant use
Hepatitis C Update
2

OPIOID PATTERNS OF USE IN CHRONIC
NON-MALIGNANT PAIN Idaho Medicaid Participants
2016 Study
3
Profile Review
• Generated profiles for the 150 recipients with the highest morphine mg equivalents (MME) for the time period July 1, 2016 through December 31, 2016
• All profiles were hand reviewed by Idaho Medicaid Pharmacists
• All patients were re-evaluated for current utilization – August 2017
150 Top patients by Total MME
26 not used in evaluation• 5 had chronic use, but MME less than 90
• 13 had liquid opioids (false high quantity), but MME less than 90
and not chronic
• 8 did not have chronic use during study period
4
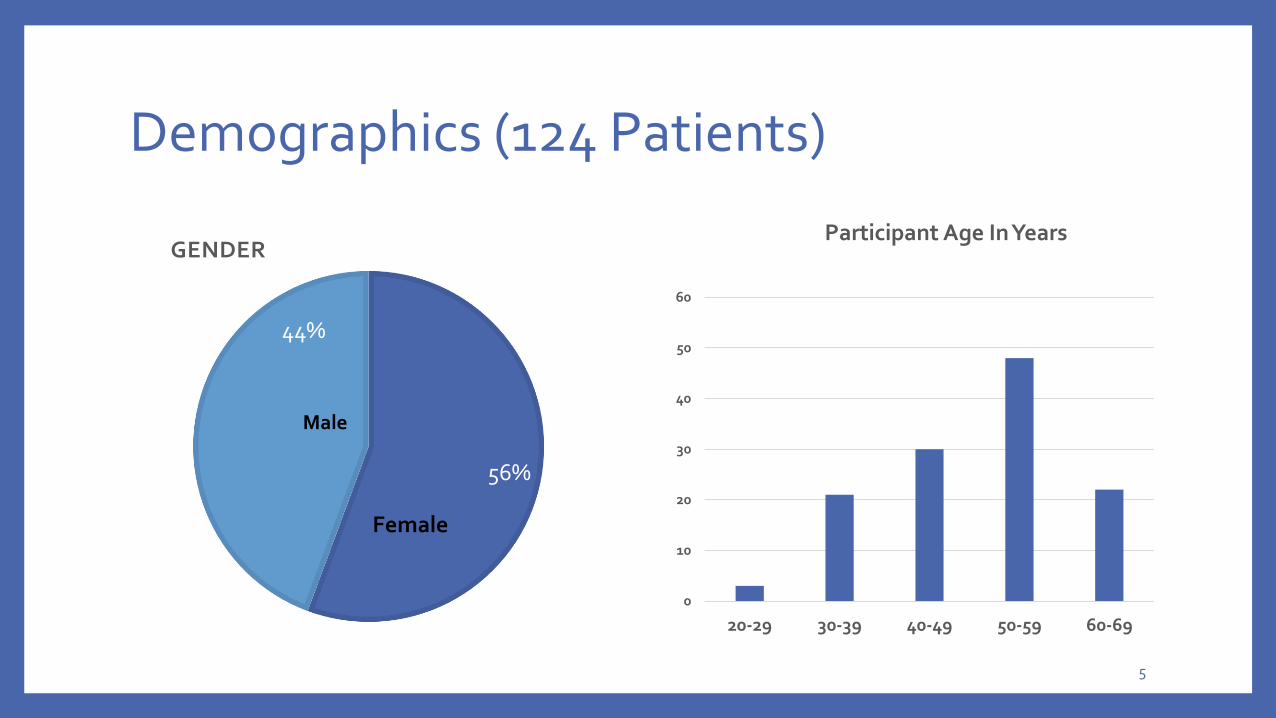
Demographics (124 Patients)
56%
44%
GENDER
Male
Female
0
10
20
30
40
50
60
20-29 30-39 40-49 50-59 60-69
Participant Age In Years
5
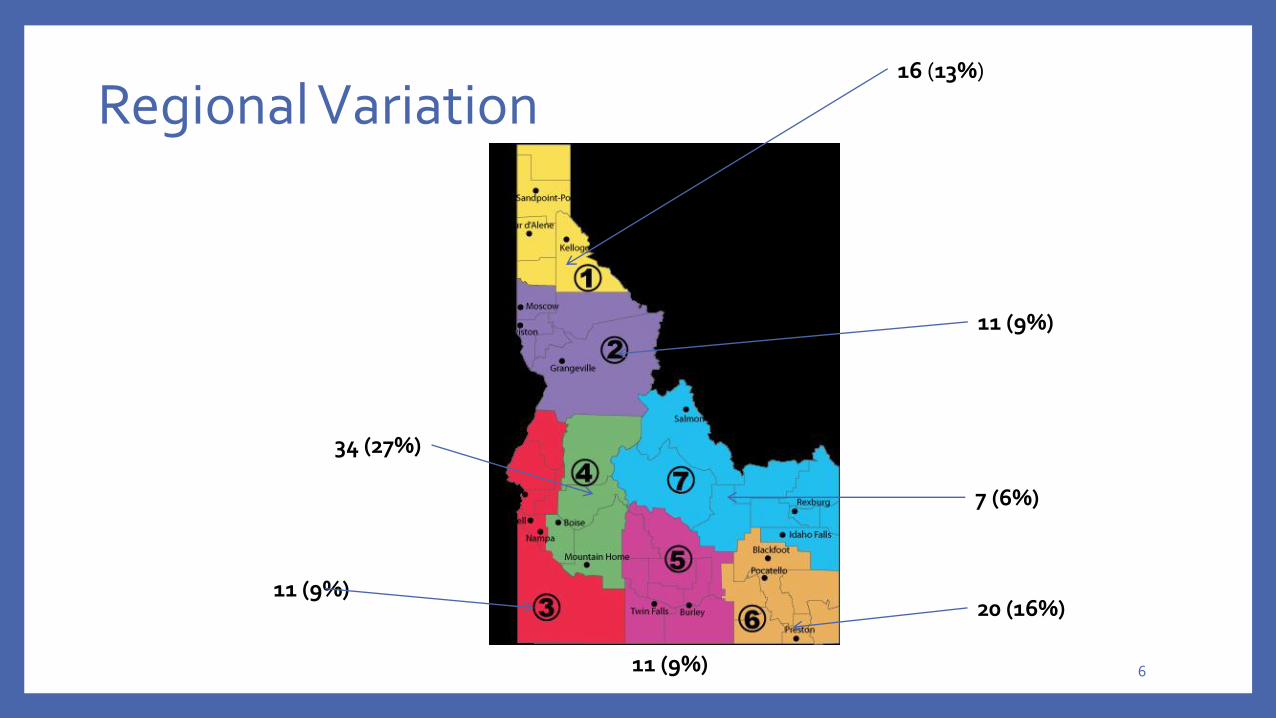
Regional Variation
11 (9%)
11 (9%)
34 (27%)
11 (9%)
20 (16%)
7 (6%)
16 (13%)
6
Patients With Cancer
Ten patients had a diagnosis of cancer
Five of the Ten had chronic non-malignant pain unrelated to cancer diagnosis so were kept in evaluation
Total in analysis for chronic non-malignant pain when pure cancer patients excluded: 119
7
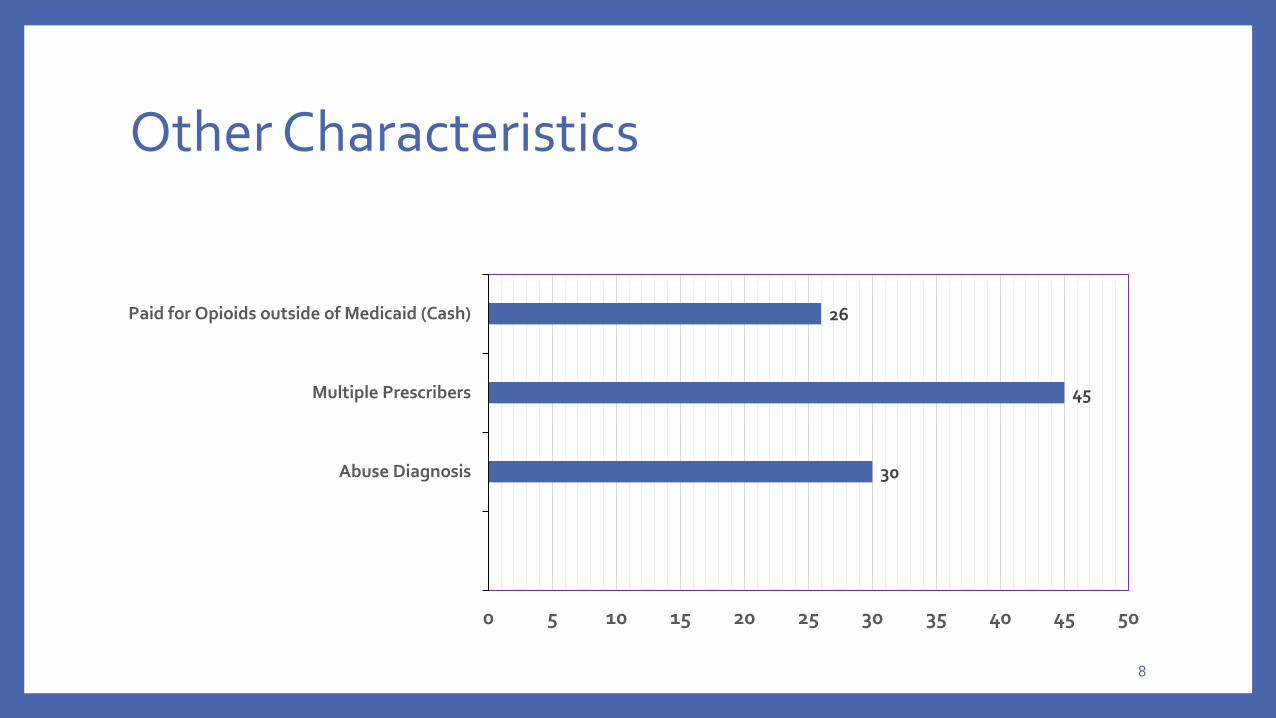
Other Characteristics
30
45
26
0 5 10 15 20 25 30 35 40 45 50
Abuse Diagnosis
Multiple Prescribers
Paid for Opioids outside of Medicaid (Cash)
8

Concurrent Benzodiazepine Use
Percent with concurrent consistent benzodiazepine usage 53%
Of those using benzodiazepines, percent where prescriber is same 34%
9
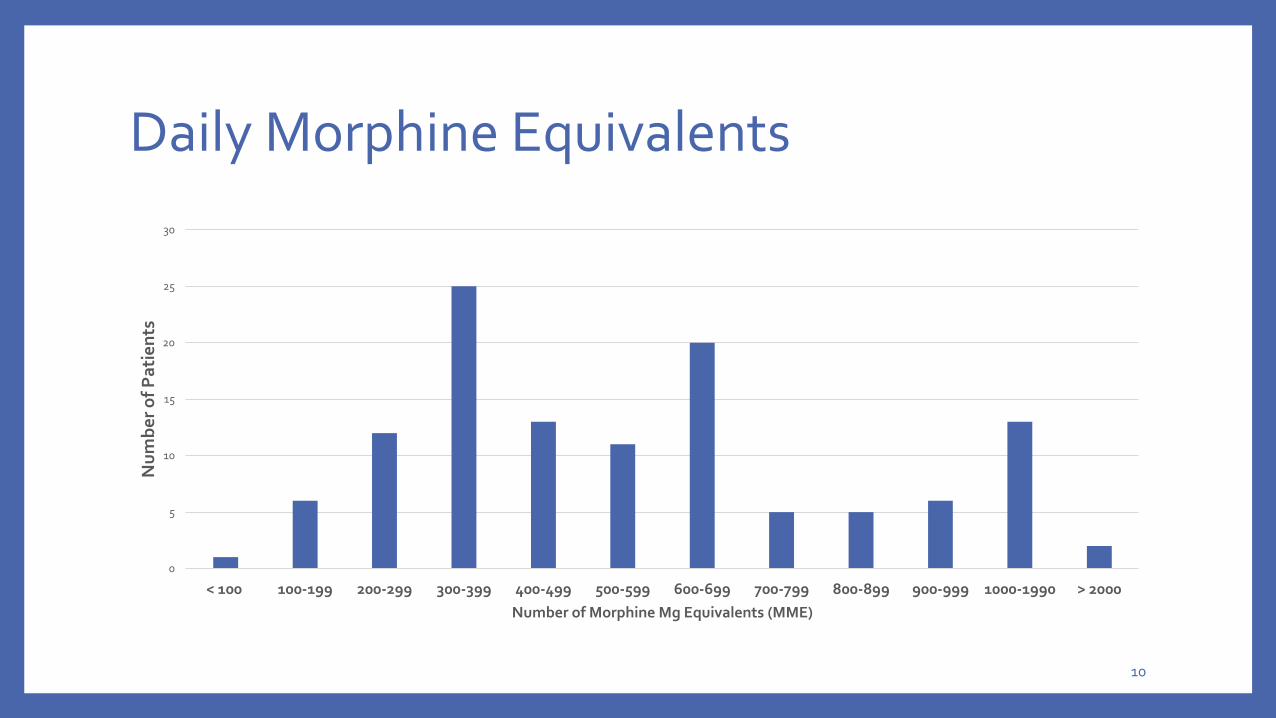
Daily Morphine Equivalents
0
5
10
15
20
25
30
< 100 100-199 200-299 300-399 400-499 500-599 600-699 700-799 800-899 900-999 1000-1990 > 2000
Nu
mb
er
of
Pa
tie
nts
Number of Morphine Mg Equivalents (MME)
10
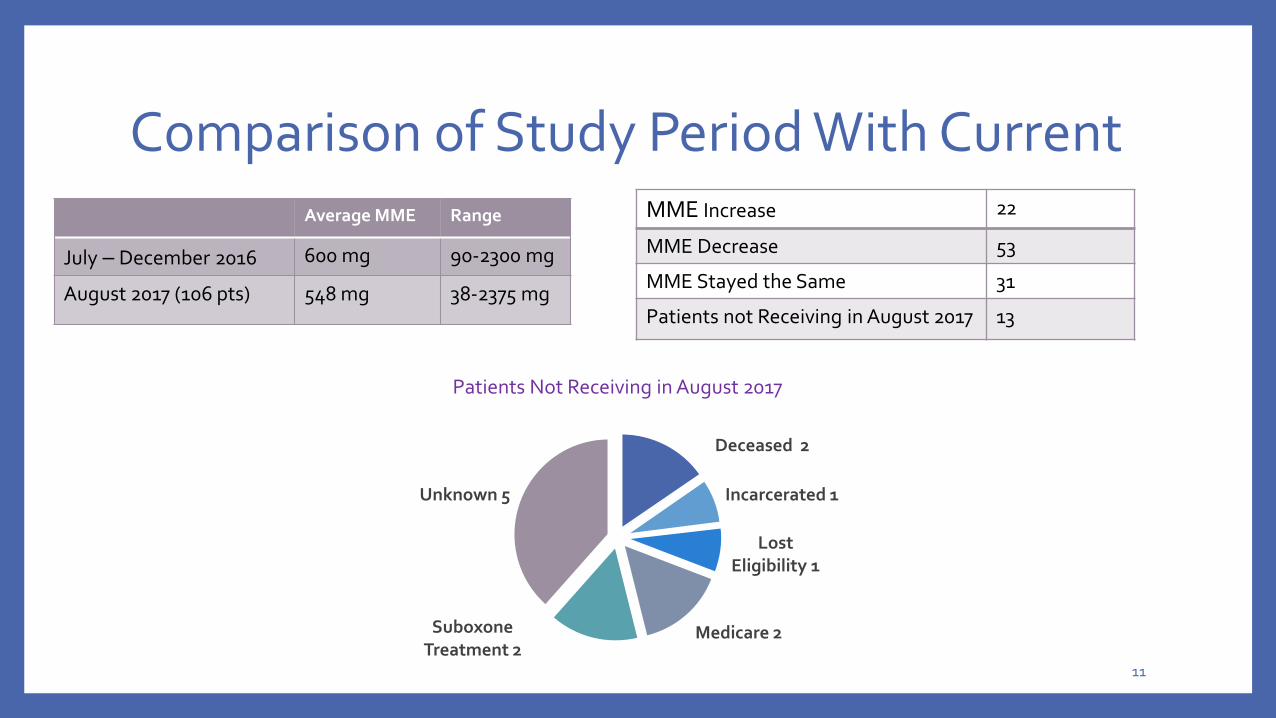
Comparison of Study Period With CurrentAverage MME Range
July – December 2016 600 mg 90-2300 mg
August 2017 (106 pts) 548 mg 38-2375 mg
MME Increase 22
MME Decrease 53
MME Stayed the Same 31
Patients not Receiving in August 2017 13
Deceased 2
Incarcerated 1
Lost Eligibility 1
Medicare 2Suboxone Treatment 2
Unknown 5
Patients Not Receiving in August 2017
11

Methadone Use
Patients on Methadone
68
Patients not on Methadone 51
12
Current Targeted Interventions
• MME Edit for < or = 90 implemented July 19, 2017• New patients and patients with dose increases subjected to edit
• Existing patients exceeding 90 given a one year temporary prior authorization
• Methadone Case Management
• Educational Lettering• Treatment Duration
• Opioid Dosage
• Multiple Prescribers
• Paying Cash for additional Opioids
• Concurrent Benzodiazepines and Opioids
13
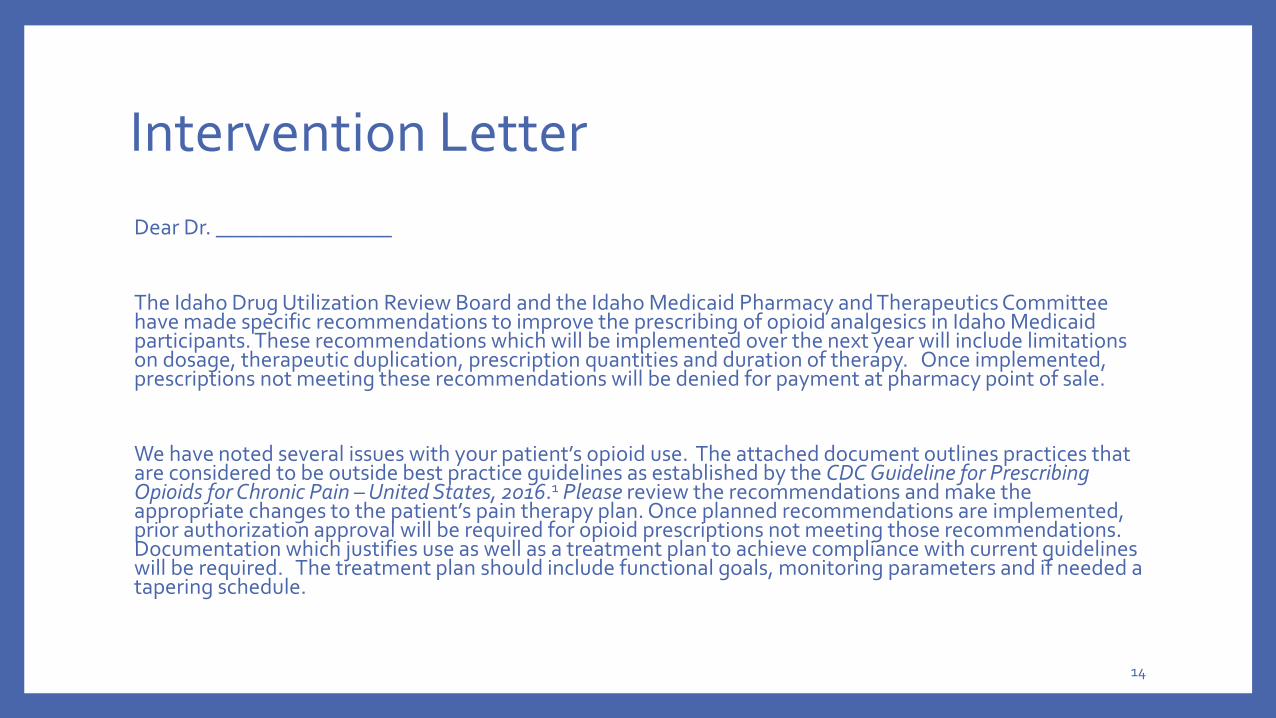
Intervention Letter
Dear Dr. ________________
The Idaho Drug Utilization Review Board and the Idaho Medicaid Pharmacy and Therapeutics Committee have made specific recommendations to improve the prescribing of opioid analgesics in Idaho Medicaid participants. These recommendations which will be implemented over the next year will include limitations on dosage, therapeutic duplication, prescription quantities and duration of therapy. Once implemented, prescriptions not meeting these recommendations will be denied for payment at pharmacy point of sale.
We have noted several issues with your patient’s opioid use. The attached document outlines practices that are considered to be outside best practice guidelines as established by the CDC Guideline for Prescribing Opioids for Chronic Pain –United States, 2016.1 Please review the recommendations and make the appropriate changes to the patient’s pain therapy plan. Once planned recommendations are implemented, prior authorization approval will be required for opioid prescriptions not meeting those recommendations. Documentation which justifies use as well as a treatment plan to achieve compliance with current guidelines will be required. The treatment plan should include functional goals, monitoring parameters and if needed a tapering schedule.
14
Treatment Duration
Finding: Your patient has been receiving continuous opioid therapy for > 1 year.
Guidelines/Evidence: While opioids may provide short-term pain relief, there is no evidence that they maintain pain relief, improve a patient’s ability to function or improve quality of life over long periods of time. Studies do show however that long-term use is associated with an increased risk of overdose, opioid related adverse events and opioid use disorder.
Recommendations/Action Needed:
• Evaluate whether this patient is experiencing clinically meaningful improvements in both pain and function compared to their baseline prior to initiation of opioid therapy.
• Maximize non-pharmacological interventions and non-opioid medications.
• If benefits in pain relief and functional improvement do not outweigh harms of continued opioid therapy, consider tapering to a lower dosage and possible discontinuation of the opioid.
15
Opioid Dosage
Finding: We calculate that your patient is currently receiving a total daily morphine equivalent dose of _____ mg.
This includes:
• The use of more than one short-acting opioid concurrently for greater than 2 months.
• Use of more than on long-acting opioid concurrently for greater than 2 months.
• Use of a combination of both long-acting and short-acting agents for greater than 2 months.
• Inclusion of a round the clock short-acting opioid.
Guidelines/Evidence: The CDC Guidelines recommend that providers should prescribe the lowest effective dosage when starting an opioid. Providers should use additional precaution when increasing dosage to > 50 morphine milligram equivalents/day and should generally avoid increasing dosage to > 90 morphine milligram equivalents/day. Opioid overdose risk increases in a dose-response manner. Dosages of 50-99 morphine milligram equivalents/day have been found to increase risks for opioid overdose by factors of 1 to 4.6 compared with dosages of 1-19 morphine milligram equivalents per day. Dosages of > 100 morphine milligram equivalents per day are associated with increased risks of overdose 2 -8.9 times the risk of 1-19 morphine milligram equivalents per day.
16
Opioid Dosage -2
Recommendations/Action Needed: Within the next year, Idaho Medicaid will be limiting daily cumulative opioid doses to < 90 daily morphine equivalents.
• Consolidate to not more than one long-acting and one short-acting opioid.
• Evaluate the monthly quantity used of the short-acting opioid. For example, a patient on a short-acting opioid with a dosing schedule of four times daily as needed should not require 120 tablets for 30 days of the month.
• Taper to a safer dosage. Submit this tapering plan to Idaho Medicaid.
• In evaluating this patient, consider performing frequent urine tests.
• Consider the possibility of diversion such as sharing or selling.
• Evaluate the patient for possible substance use disorder.
17
Multiple Prescribers
Finding: Multiple prescribers of opioids have been noted through the Idaho Prescription Monitoring Program (PMP) report which is attached.
Guidelines/Evidence: The use of multiple prescribers potentially puts a patient at risk for overuse of opioid analgesics resulting in overdose, other adverse effects and development of opioid use disorder. The coordination of the patient’s opioid use by one prescriber minimizes the occurrence of these potential harms as well as maximizing the ability to evaluate improvements in pain and function.
Recommendations/Action Needed:
• Review the attached PMP report to coordinate care with other prescribers.
• Discuss with the patient the importance of utilizing one prescriber for their pain medication.
18
Paying Cash for Additional Opioids
Finding: Our review through the Idaho Prescription Monitoring Program (PMP) report shows that your patient is paying cash for opioids in addition to those paid for by Medicaid.
Guidelines/Evidence: Paying for additional opioids above those allowed by Medicaid exceeds recommended dosage limitations of a > 90 mg morphine equivalent daily dose. Higher opioid doses put patients at risk for overuse of opioid analgesics resulting in overdose, other adverse effects and development of opioid use disorder.
Recommendations/Action Needed:
• If both Medicaid and cash prescriptions are being prescribed by yourself, evaluate the total daily cumulative opioid dose and if it is greater than 90 daily morphine mg equivalents: • Taper to a safer dosage. Submit this tapering plan to Idaho Medicaid.
• Consider performing frequent urine tests.
• Consider the possibility of diversion such as sharing or selling.
• Evaluate the patient for possible substance use disorder.
• If the additional prescriptions for which the patient is paying cash for are being prescribed by a different prescriber, consider coordination of therapy with that prescriber who is identified on the PMP. Idaho Medicaid can also work with you to “lock-in” the patient to one prescriber and one pharmacy.
19
Concurrent Benzodiazepine
Finding: Your patient is receiving one or more benzodiazepines concomitantly with opioids on a continuous basis.
Guidelines/Evidence:
• The combined use of opioids and benzodiazepines or other CNS depressant drugs or alcohol has resulted in serious side effects including extreme sleepiness, slowed or difficult breathing, coma and death. Medical studies have shown the rates of overdose death of these drugs used concomitantly were up to 10 times higher than use of opioids alone. The risk of drug overdose death increases as the daily benzodiazepine dose increases.
• The FDA has recently added a boxed warning to the drug labeling of both prescription opioids and benzodiazepines outlining the dangers of using these medication drug classes concurrently.
• Most guidelines for the treatment of anxiety disorders recommend selective serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors or pregabalin as first-line pharmacological treatments. Benzodiazepines are generally recommended to be used only on short-term basis of 3-6 months.
20
Concurrent Benzodiazepine -2
Recommendations/Action Needed:
• Weigh the patient’s need versus risks of concurrent benzodiazepine and opioid exposure.
• Communicate with other prescribers managing the patient’s care to discuss the patient’s needs and prioritize the patient’s needs for opioid and/or benzodiazepines.
• For patients receiving both benzodiazepines and opioids requiring tapering, it is generally considered safer and more practical to taper opioids first.
• If benzodiazepines are tapered or discontinued or if your patient receiving opioids requires treatment for anxiety, evidence-based psychotherapies such as cognitive behavioral therapy and/or specific anti-depressants or other non-benzodiazepine medications approved for anxiety should be offered.
• Discuss with the patient safety concerns including an increased risk for respiratory depression and overdose with the concurrent use of opioids and benzodiazepines.
21
Ongoing Review
October 19, 2017
22
MethadoneGrowing Public Health Concern
More than 16,500 people in the United States die each year from opioid-related prescription drug overdoses.
Methadone is responsible for nearly 1/3 of these deaths but accounts for only 2% of opioid pain reliever prescription.
Centers for Disease Control and Prevention. “Opioids Drive Continued Increase in Drug Overdose Deaths” (2013). http://www.cdc.gov/media/relases/2013/p0220_drug_overdose_deaths.html.
23
MethadonePreferred pain reliever for most state Medicaid programs.
Idaho Medicaid removed Methadone preferred status October 2015.
Prior authorization required
Informed methadone providers of implementation of methadone prior authorization and requested tapering off of methadone.
24
MethadoneMethadone Prior Authorization Request Forms
Methadone, Initial Request
States initial criteria for review:
Failure of all alternative long acting narcotic agents.
Electrocardiogram (QTc interval documentation).
Pain score and functionality documentation.
Other active concurrent opioids (immediate release)
Documentation of failure/intolerance to non-opioid or opioid agents.
Limit to 30 mg/day maximum dose.
Cancer pain treatment is excluded from monitoring criteria.
25
Methadone Methadone, Reauthorization
Emphasizes monitoring and recommends dose tapering:
Electrocardiogram (QTc interval annual review).
Doses greater than 30 mg/day will require documentation of medical necessity and clinical reason why dose reduction cannot be employed.
History of failure/intolerance to non-opioid or other opioid agents.
Only prescribers who are familiar with methadone’s titration and risks, or those who are able to consult with a pain specialist or clinical pharmacist, should prescribe or make changes to methadone treatment.
Medicaid is monitoring active patients on methadone.
26
MethadoneAmerican Society of Interventional Pain Physicians (ASIPP) Guidelines
Recommend methadone only for use after failure of other opioid therapy and only by clinicians with specific training in its risks and uses, within FDA recommended doses. (Evidence: Level I; Strength of Recommendation: Strong)
Pain Physician. 2017 Feb;20(2S):S3-S92. Responsible, Safe, and Effective Prescription of Opioids for Chronic Non-Cancer Pain: American Society of Interventional Pain Physicians (ASIPP) Guidelines.
27
MethadoneReview of Methadone drug utilization after changing to non-preferred agent.
Calendar Quarters Reviewed:
4th Quarter 2015 (Oct-Dec)
2nd Quarter of 2016 (Apr-Jun)
3rd Quarter of 2016 (Jul-Sept)
4th Quarter of 2016 (Oct-Dec)
1st Quarter of 2017 (Jan-Feb)
2nd Quarter of 2017 (Apr-Jun)
3rd Quarter of 2017 (Jul-Sept)28
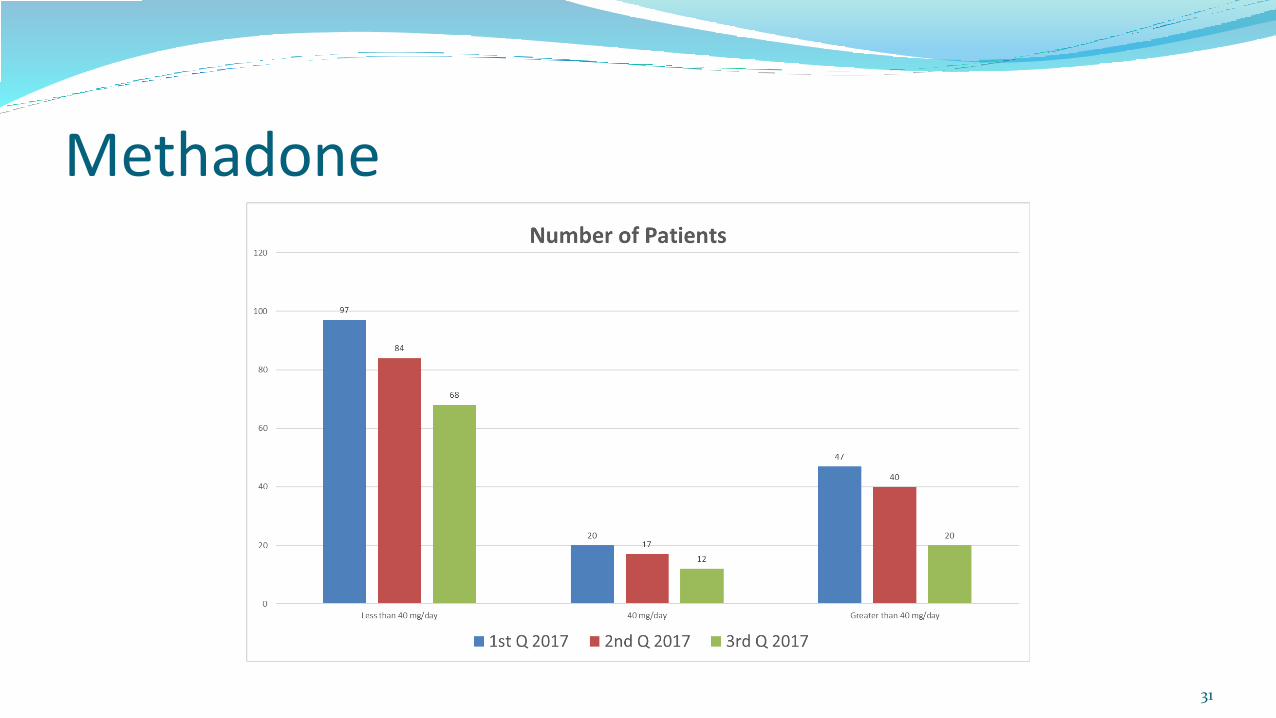
Methadone
29
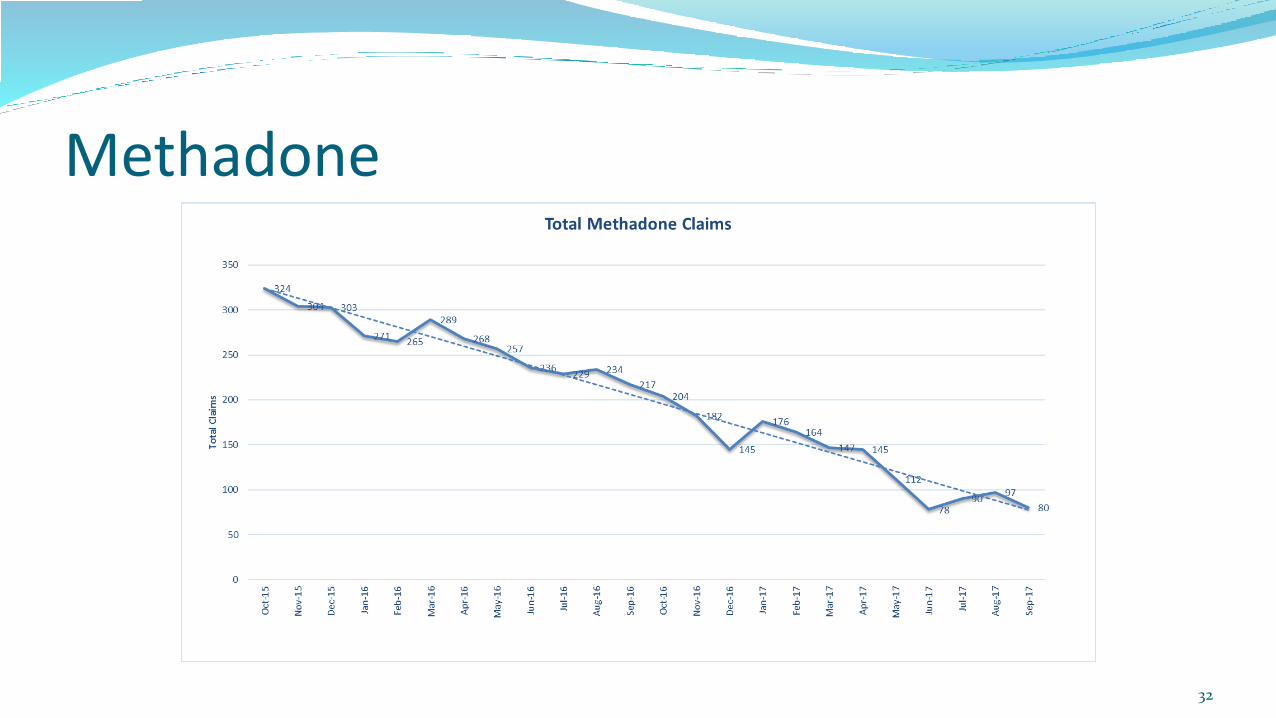
Methadone
30
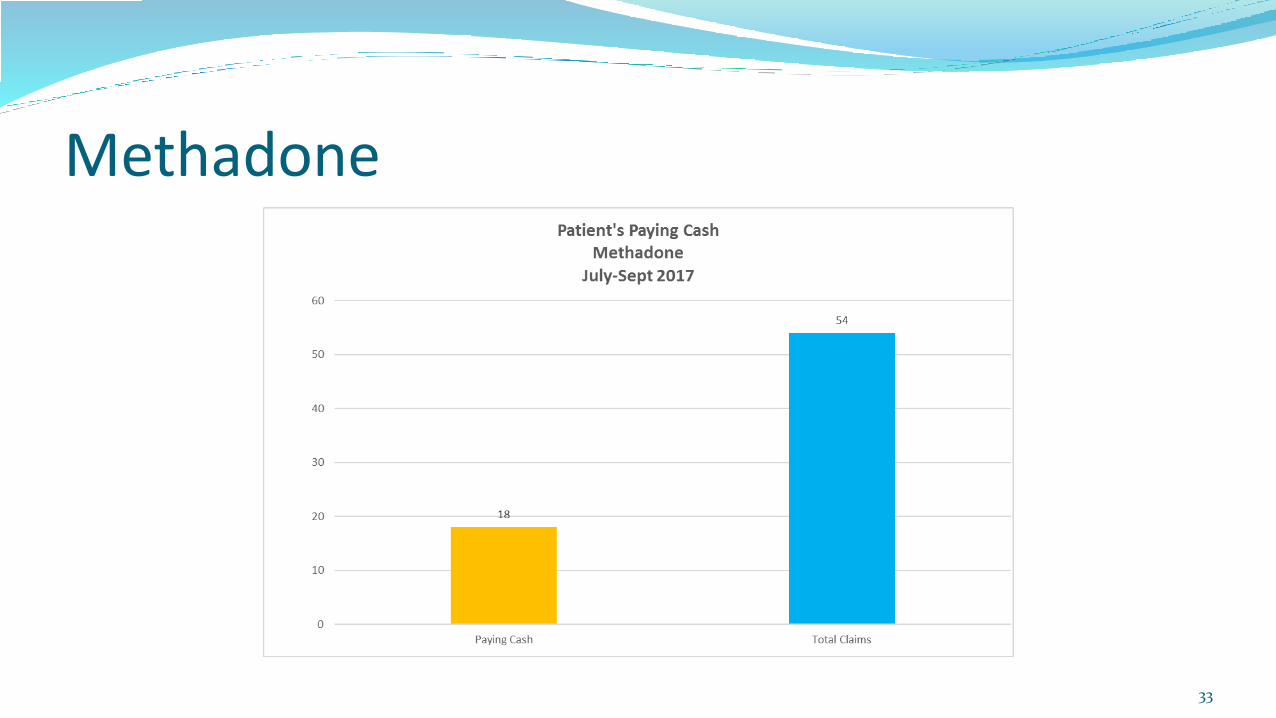
Methadone
31
Methadone
32
Methadone
33

MethadoneIn conclusion:
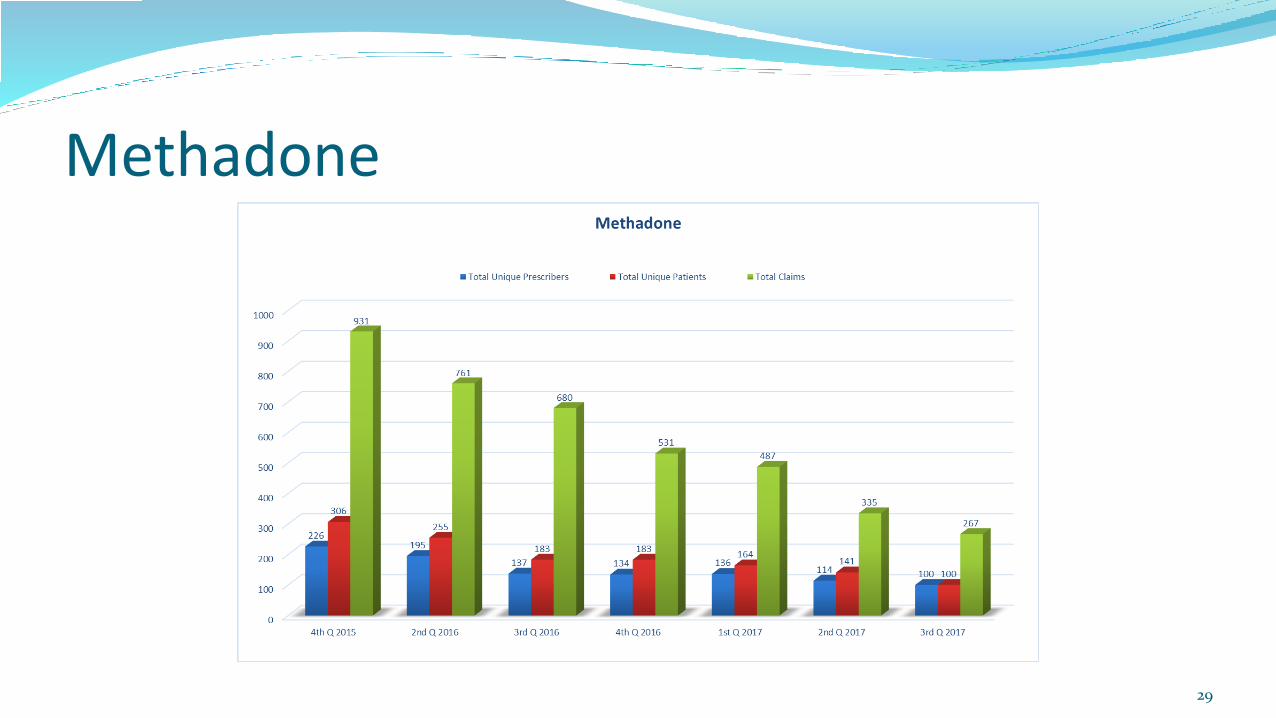
Continued decrease in Methadone claims since incorporation of prior authorization and monitoring criteria implementation.
Some decreased utilization noted due to patients paying cash for methadone.
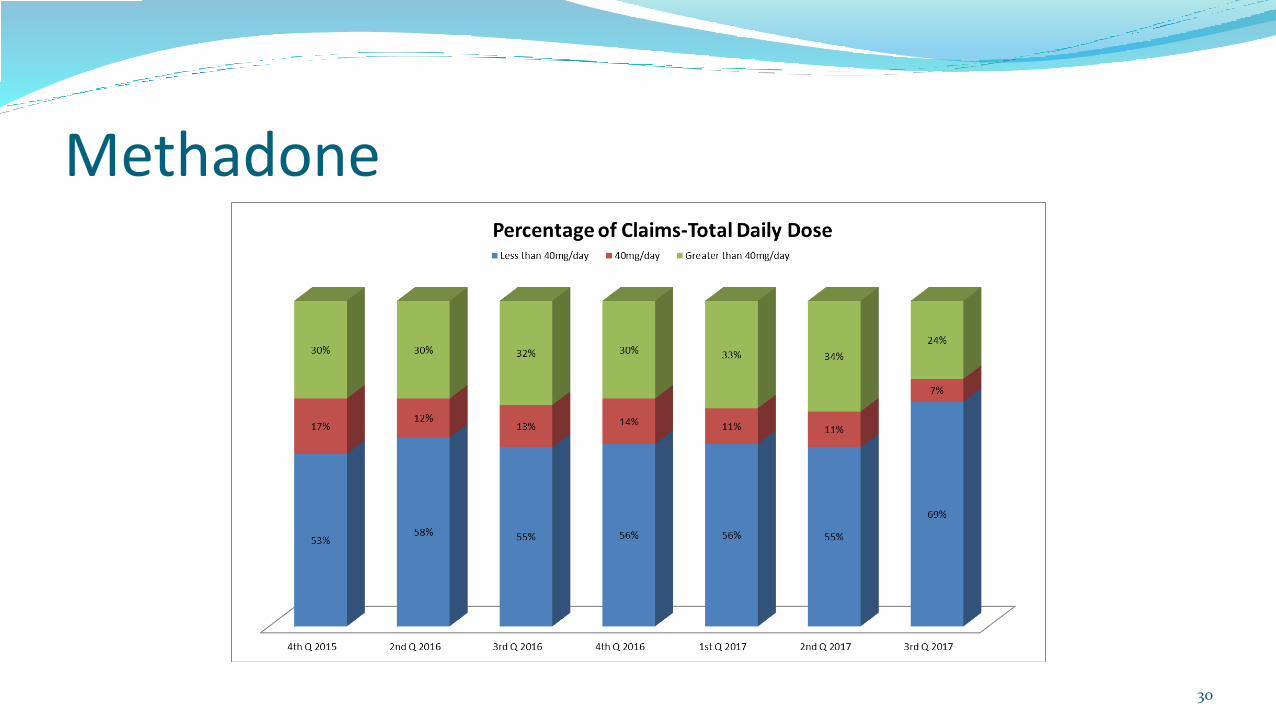
Patients taking more than 40 mg/day of methadone has decreased.
Continue to recommend tapering agent down to acceptable Morphine Daily Equivalents.
34
Methadone Questions/Comments??
35

October 19, 2017
36
Buprenorphine and benzodiazepine concomitant use
37
Suboxone Package Insert
Buprenorphine in combination with benzodiazepines or other CNS depressants including alcohol has been associated with significant respiratory depression and death.
Patients should be warned of the potential of self-administration of benzodiazepines or other depressants while under treatment with Suboxone.
Buprenorphine and benzodiazepine concomitant use
38
Payment block went in to effect 1/6/16 requiring prior authorization for payment for either buprenorphine or benzodiazepine with overlapping days of service.

Buprenorphine and benzodiazepine concomitant use
39
PMP Interconnect Search
Twenty-two States now on the list (must select each individual state to search) – including Idaho
Alaska Massachusetts North Dakota
Arizona Michigan Ohio
Arkansas Minnesota Oklahoma
Colorado Mississippi Rhode Island
Illinois Montana South Carolina
Indiana Nevada Texas
Kansas New Mexico Utah
Buprenorphine and benzodiazepine concomitant use
40
FDA Drug Safety Communication – 9/20/2017
FDA Drug Safety Communication: FDA urges caution about withholding opioid addiction medications from patients taking benzodiazepines or CNS depressants: careful medication management can reduce risks
Based on our additional review, the U.S. Food and Drug Administration (FDA) is advising that the opioid addiction medications buprenorphine and methadone should not be withheld from patients taking benzodiazepines or other drugs that depress the central nervous system (CNS). The combined use of these drugs increases the risk of serious side effects; however, the harm caused by untreated opioid addiction can outweigh these risks. Careful medication management by health care professionals can reduce these risks. We are requiring this information to be added to the buprenorphine and methadone drug labels along with detailed recommendations for minimizing the use of medication-assisted treatment (MAT) drugs and benzodiazepines together.
Buprenorphine and benzodiazepine concomitant use
41
FDA Drug Safety Communication – 9/20/2017
Many patients with opioid dependence may also use benzodiazepines or other CNS depressants, either under a health care professional’s direction or illicitly. Although there are serious risks with combining these medicines, excluding patients from MAT or discharging patients from treatment because of use of benzodiazepines or CNS depressants is not likely to stop them from using these drugs together. Instead, the combined use may continue outside the treatment setting, which could result in more severe outcomes.
Buprenorphine and benzodiazepine concomitant use
42
FDA Drug Safety Communication – 9/20/2017
Health care professionals should take several actions and precautions and develop a treatment plan when buprenorphine or methadone is used in combination with benzodiazepines or other CNS depressants. These include:
Educating patients about the serious risks of combined use, including overdose and death, that can occur with CNS depressants even when used as prescribed, as well as when used illicitly.
Developing strategies to manage the use of prescribed or illicit benzodiazepines or other CNS depressants when starting MAT.
Tapering the benzodiazepine or CNS depressant to discontinuation if possible.
Verifying the diagnosis if a patient is receiving prescribed benzodiazepines or other CNS depressants for anxiety or insomnia, and considering other treatment options for these conditions.
Recognizing that patients may require MAT medications indefinitely and their use should continue for as long as patients are benefiting and their use contributes to the intended treatment goals.
Coordinating care to ensure other prescribers are aware of the patient’s buprenorphine or methadone treatment.
Monitoring for illicit drug use, including urine or blood screening.
Buprenorphine and benzodiazepine concomitant use
43
FDA Drug Safety Communication – 9/20/2017
Our subsequent review of a published study3 and other drug use data showed that buprenorphine and benzodiazepines frequently have been prescribed for the same patient, often by the same prescriber, and these drugs are usually dispensed by the same pharmacy. An epidemiological study from Sweden found that receiving MAT with benzodiazepines or other CNS depressants such as drugs to treat insomnia appears to increase the risk of death.
Buprenorphine and benzodiazepine concomitant use
44
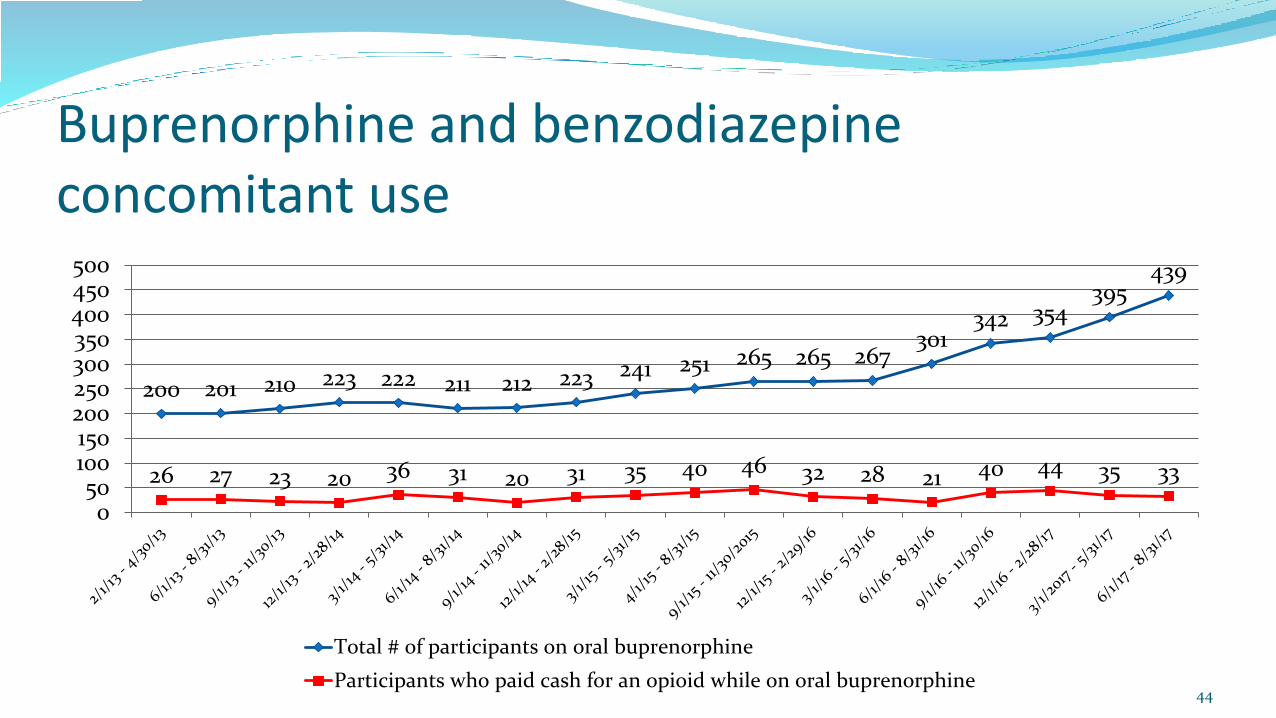
200 201 210 223 222 211 212 223 241 251 265 265 267301
342 354395
439
26 27 23 20 36 31 20 31 35 40 46 32 28 21 40 44 35 33
050
100150200250300350400450500
Total # of participants on oral buprenorphine
Participants who paid cash for an opioid while on oral buprenorphine
Buprenorphine and benzodiazepine concomitant use
45
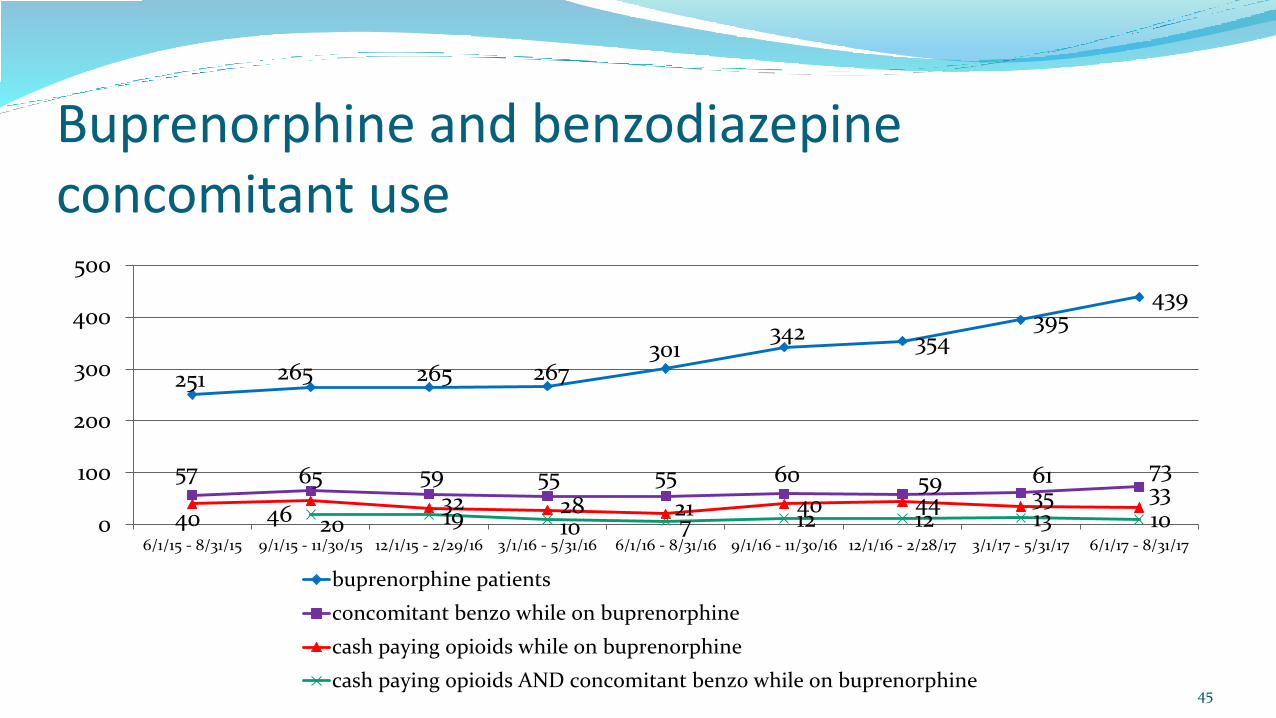
251 265 265 267301
342 354395
439
57 65 59 55 55 60 59 61 73
40 4632 28 21 40 44 35 33
20 19 10 7 12 12 13 100
100
200
300
400
500
6/1/15 - 8/31/15 9/1/15 - 11/30/15 12/1/15 - 2/29/16 3/1/16 - 5/31/16 6/1/16 - 8/31/16 9/1/16 - 11/30/16 12/1/16 - 2/28/17 3/1/17 - 5/31/17 6/1/17 - 8/31/17
buprenorphine patients
concomitant benzo while on buprenorphine
cash paying opioids while on buprenorphine
cash paying opioids AND concomitant benzo while on buprenorphine

Buprenorphine and benzodiazepine concomitant use
46
107
4
52
00
10
20
30
40
50
60
Buprenorphine and benzodiazepine June 2017 – August 2017
Buprenorphine prescriber justified ongoingbenzo usage
Buprenorphine prescriber is weaning benzoor has discontinued benzo
Patient no longer on buprenorphine butcontinuing benzo
Paying cash for benzo while onbuprenorphine (see detail next slide)
Prescriber never returned phone call

Buprenorphine and benzodiazepine concomitant use
47
2 2
2325
0
5
10
15
20
25
30
Procedural, no PA submitted < 6 tablets Patient told to discontinue benzo No PA request submitted Prior auth request denied
Buprenorphine and benzodiazepine concomitant use
48
Online advice on taking benzos with Suboxone:
I've been seeing a lot of posts regarding taking benzos while on Suboxone. It is ok to take a benzo w/ suboxone - as long as you're taking the prescribed dosages you'll be fine. Now if you're taking 3 or 4 8mgs of Suboxone and say 5 or 6 Xanax that's not good, that's where the reported deaths have come from. I've been on Subs for 5 yrs. I've also been subscribed klonopin and am currently taking valium w/ it and it's fine. I'm on a low dose and only take what I am prescribed.
Editor's note: We do not verify the credentials of our users and nothing stated is intended to be taken as medical advice.
http://www.medschat.com/Discuss/Can-you-take-benzos-while-youre-on-suboxone-192505_p1_s2.htm
Buprenorphine and benzodiazepine concomitant use
49
Online advice on taking benzos with Suboxone:
I actually would suggest to take the Xanax first, so the bupe will bring you up. If you take the Xanax after the bupe there might be some dulling of the opioid effects, of course with a large benzo tolerance, and with bupe, I don't think it would be that much of an issue. Try both, see which you prefer.
http://www.bluelight.org/vb/threads/616086-Xanax-and-Suboxone-Which-to-take-first
Buprenorphine and benzodiazepine concomitant use
50
Online advice on taking benzos with Suboxone:
I want to know if I take the benzos will it be a problem when I see my doctor for Suboxone and test positive for them. He didn't prescribe me benzos because he said taking them is like walking on thin ice with suboxone. I have panic attacks and xanax helps stop them. Should I just stop weeks before the drug test or come clean and tell him the truth?
https://www.drugs.com/answers/i-get-xanax-and-temazepam-from-one-doctor-and-223285.html
If you're seeking xanax or "alprazolam" you would have to see another doctor and not mention you take suboxone.
Could not find this website when I went back to look for the citation.
Buprenorphine and benzodiazepine concomitant use
51
Questions/Comments ??
October 19, 2017
3rd Quarter 2017
(Calendar Year)
52
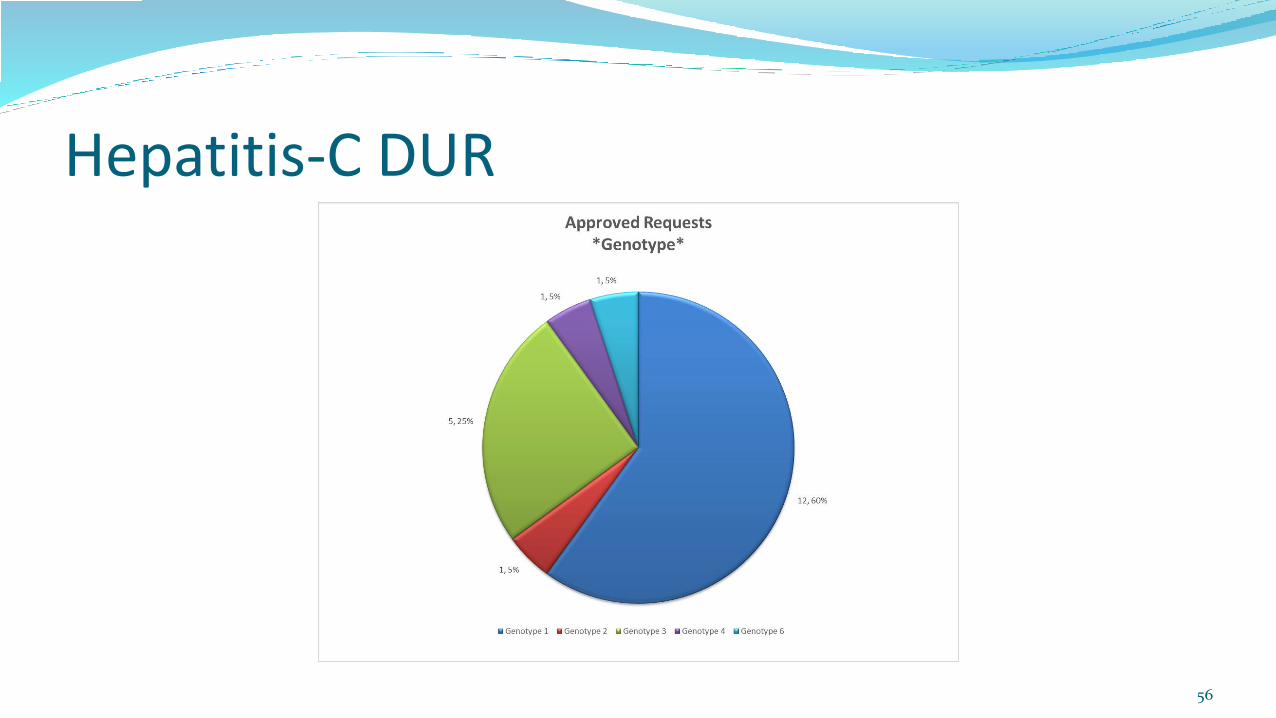
Hepatitis-C DUR
53
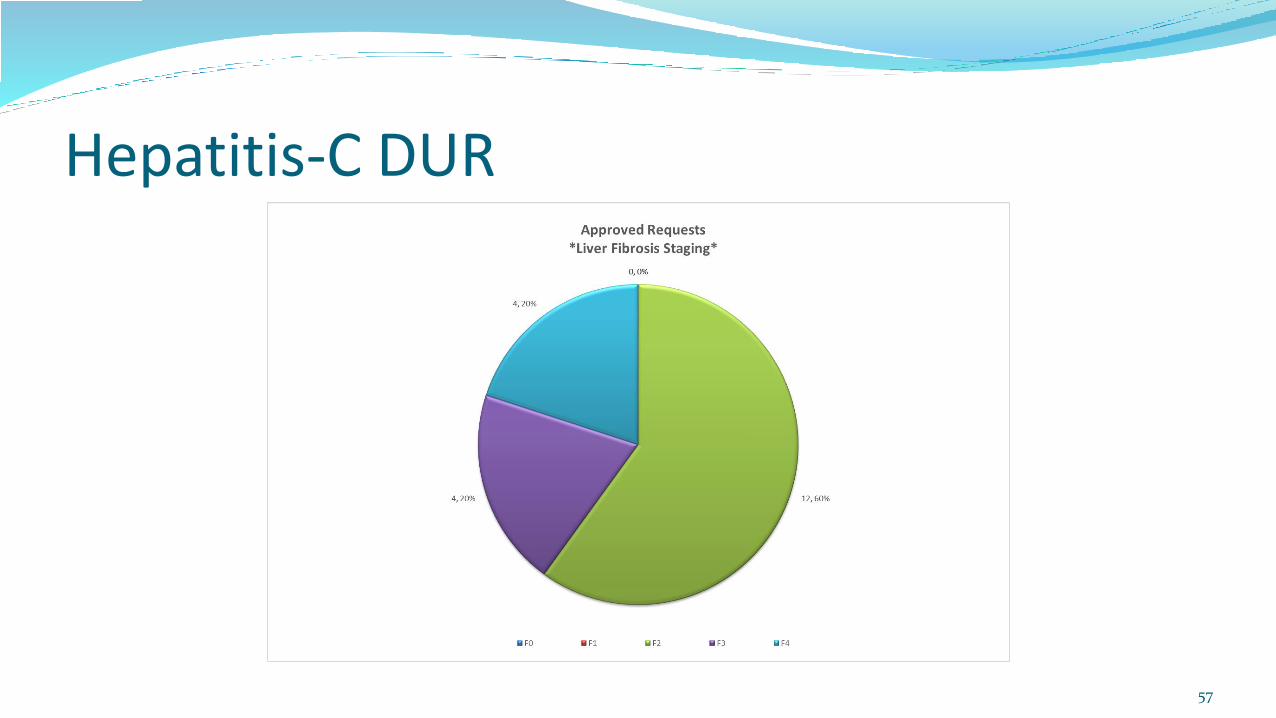
Hepatitis-C DUR
54
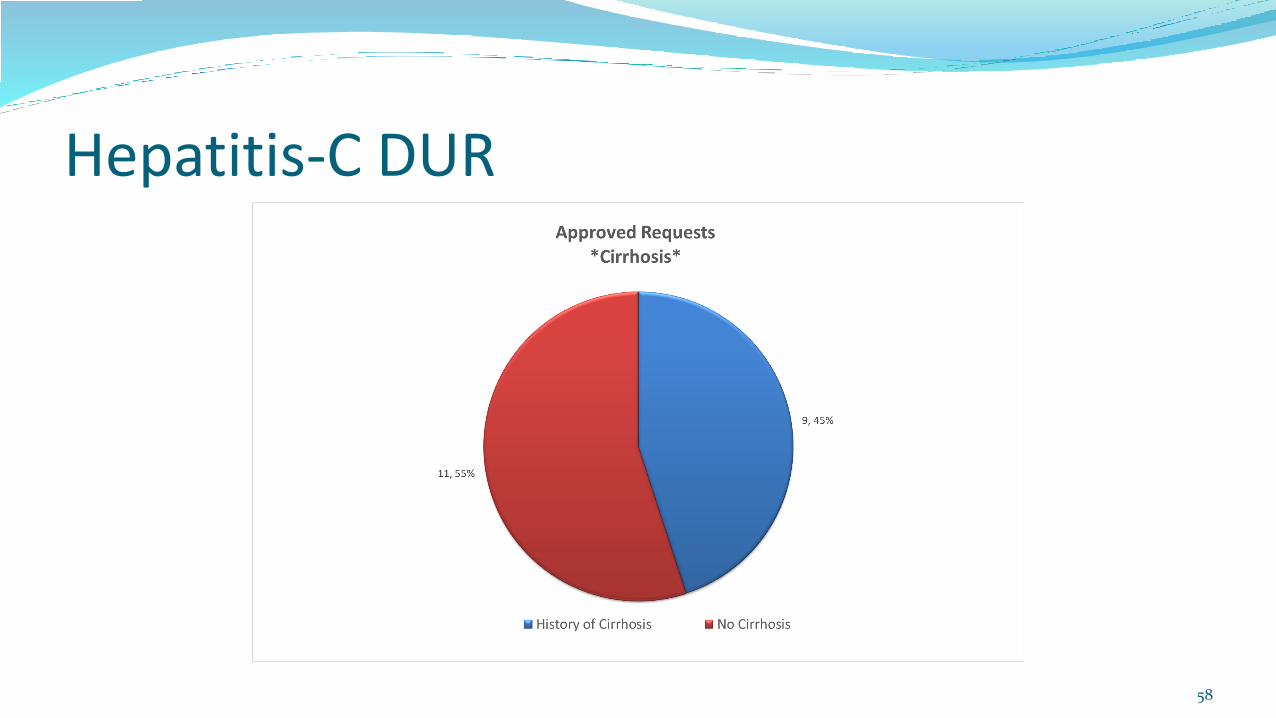
Hepatitis-C DUR
55
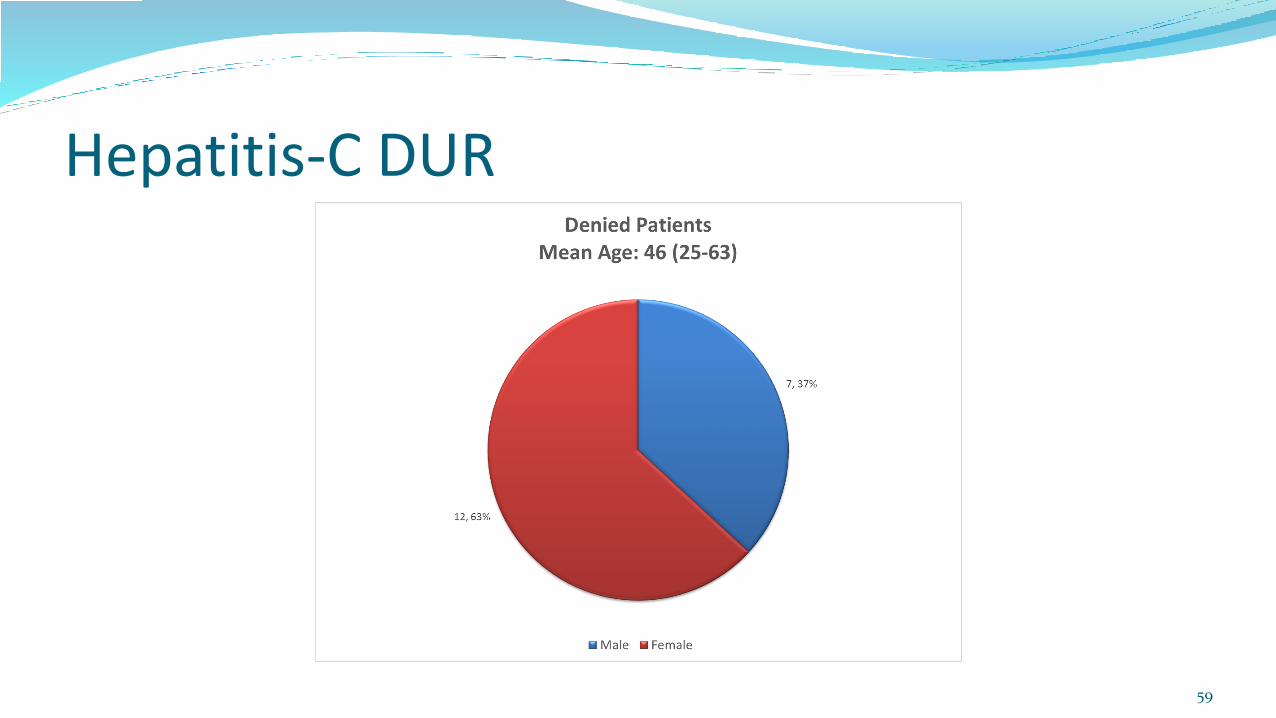
Hepatitis-C DUR
56
Hepatitis-C DUR
57
Hepatitis-C DUR
58
Hepatitis-C DUR
59
Hepatitis-C DUR
60
Hepatitis-C DUR
61
Hepatitis-C DUR
62
Hepatitis-C DUR
63
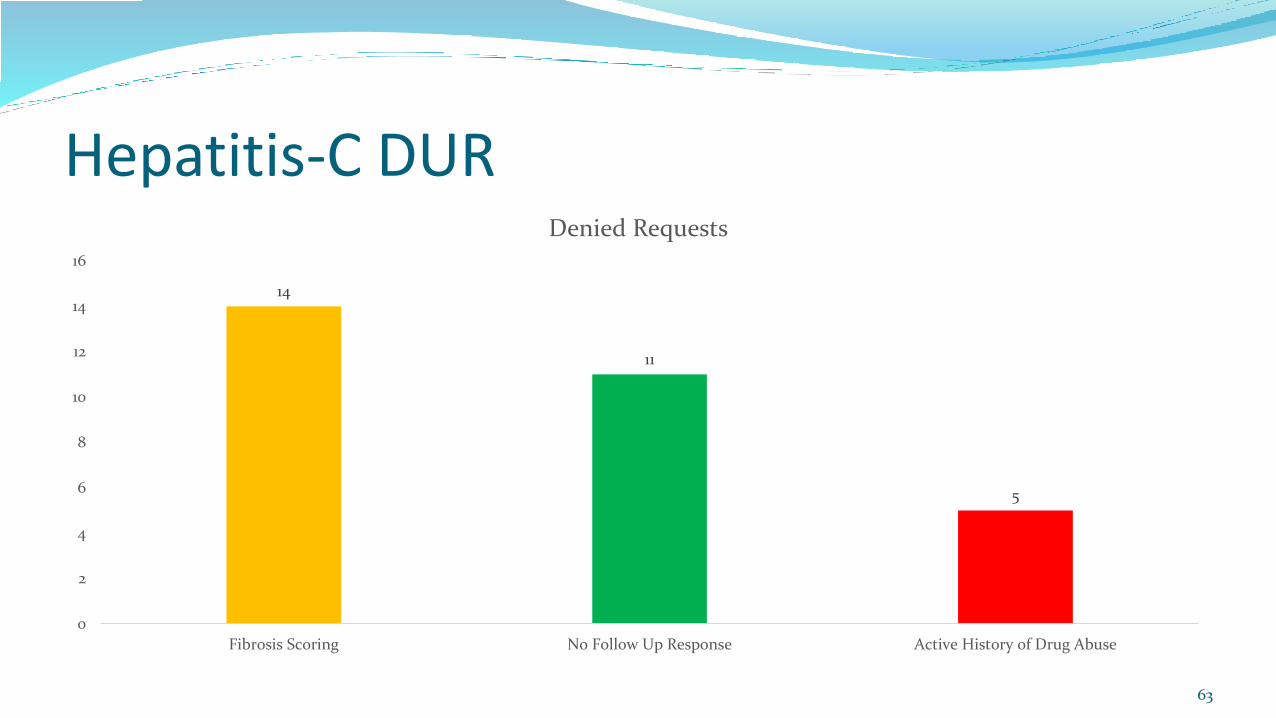
14
11
5
0
2
4
6
8
10
12
14
16
Fibrosis Scoring No Follow Up Response Active History of Drug Abuse
Denied Requests
Hepatitis-C DUR
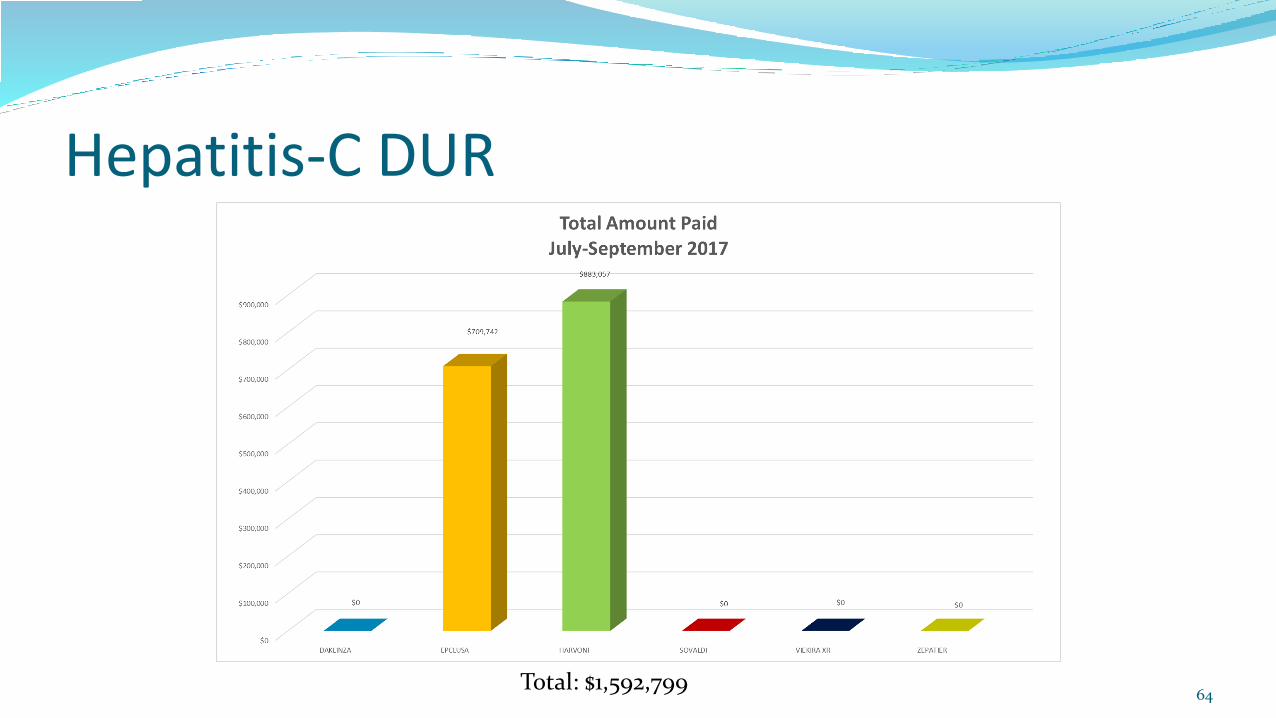
Total: $1,592,79964
Hepatitis-C DURFDA approved August 3, 2017
AbbVie Inc: Mavyret™ (glecaprevir, pibrentasvir)
Mavyret™ is the first treatment approved for 8 weeks duration.
Treatment duration with Mavyret™ differs depending on treatment history, viral genotype, and cirrhosis status.
Genotypes 1 thru 6
Dosing of 3 tablets once a day for 8 week treatment
Patient’s with no cirrhosis and naïve to therapy
Dosing of 3 tablets once a day for 12 week treatment
Compensated cirrhosis and naïve to therapy (Child-Pugh A)
Dosing can range from 8 weeks to 16 weeks based upon genotype and previous HCV regimens.
Mavyret™ is not recommended in patients with moderate cirrhosis and contraindicated in patients with severe cirrhosis. It is also contraindicated in patients taking the drugs atazanavir and rifampin. 65
Hepatitis-C DUR Questions/Comments??
66
Current Interventions/Outcomes Studies
Temazepam
Nifedipine IR / Methyldopa
67

October 19, 2017
68
Temazepam
69
Prior to 6/1/2017, temazepam 15mg and 30mg capsules were a preferred sedative for Idaho Medicaid.
Temazepam 7.5mg and 22.5mg were non-preferred due to cost.
At the 11/18/2016 P&T Committee meeting, the recommendation was made to not have any benzodiazepine as a preferred sedative due to safety concerns.
Temazepam
70
Letters were sent to prescribers on 3/9/2017 informing them that temazepam was being switched from preferred to non-preferred status.
Current patients were not automatically grandfathered.
The majority of the patients now on temazepam have tried and failed a preferred sedative (zolpidem and/or Rozerem) and therefore meet Idaho Medicaid’s criteria for payment of a non-preferred sedative.
71
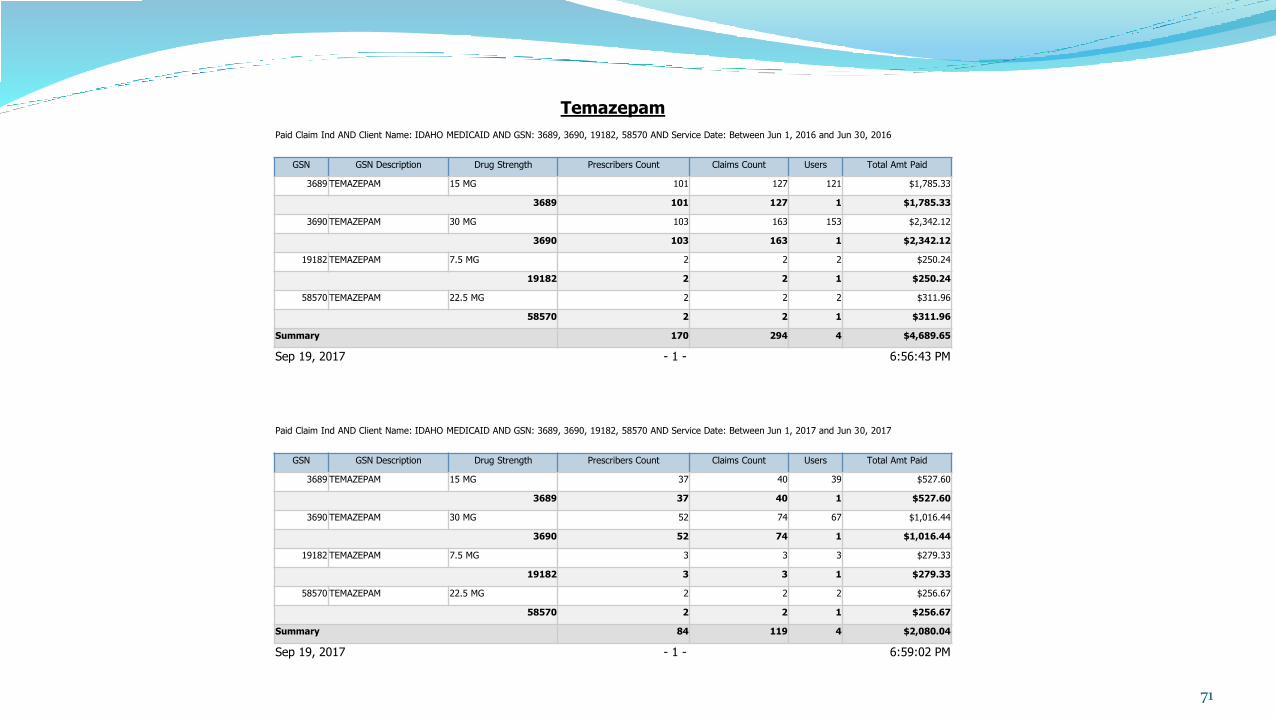
Temazepam
Paid Claim Ind AND Client Name: IDAHO MEDICAID AND GSN: 3689, 3690, 19182, 58570 AND Service Date: Between Jun 1, 2016 and Jun 30, 2016
GSN GSN Description Drug Strength Prescribers Count Claims Count Users Total Amt Paid
3689 TEMAZEPAM 15 MG 101 127 121 $1,785.33
3689 101 127 1 $1,785.33
3690 TEMAZEPAM 30 MG 103 163 153 $2,342.12
3690 103 163 1 $2,342.12
19182 TEMAZEPAM 7.5 MG 2 2 2 $250.24
19182 2 2 1 $250.24
58570 TEMAZEPAM 22.5 MG 2 2 2 $311.96
58570 2 2 1 $311.96
Summary 170 294 4 $4,689.65
Sep 19, 2017 - 1 - 6:56:43 PM
Paid Claim Ind AND Client Name: IDAHO MEDICAID AND GSN: 3689, 3690, 19182, 58570 AND Service Date: Between Jun 1, 2017 and Jun 30, 2017
GSN GSN Description Drug Strength Prescribers Count Claims Count Users Total Amt Paid
3689 TEMAZEPAM 15 MG 37 40 39 $527.60
3689 37 40 1 $527.60
3690 TEMAZEPAM 30 MG 52 74 67 $1,016.44
3690 52 74 1 $1,016.44
19182 TEMAZEPAM 7.5 MG 3 3 3 $279.33
19182 3 3 1 $279.33
58570 TEMAZEPAM 22.5 MG 2 2 2 $256.67
58570 2 2 1 $256.67
Summary 84 119 4 $2,080.04
Sep 19, 2017 - 1 - 6:59:02 PM
72

73

Temazepam
74
Discussion topic – do we want to institute any other criteria such as trial and failure of two sedatives before payment for a benzodiazepine sedative will be approved ?

October 19, 2017
75
76
Concern May 2017 P&T. Committee expressed concern of use of immediate release
nifedipine.
DUR to look at utilization to see if use went beyond use in pregnancy related conditions
77
FDA Indications Nifedipine IR Chronic, stable angina
Variant angina
Although FDA indicated the IR is not recommended because of association with excess mortality in patients with acute phase MI or unstable angina
IR not indicated for hypertension
78
Select Off-Label IndicationsPregnancy
Hypertension (although IR discouraged)
Pre-term Labor
As effective as beta agonists for reducing rate of delivery within 48 hours and more effective in reducing the delivery within 7 days
No better than placebo in maintenance tocolysis – use progesterone
Guidelines do not indicate any drug of choice for pre-term labor
May give enough time to give antenatal steroids to improve infant lung maturity between 24-34 weeks gestation
79
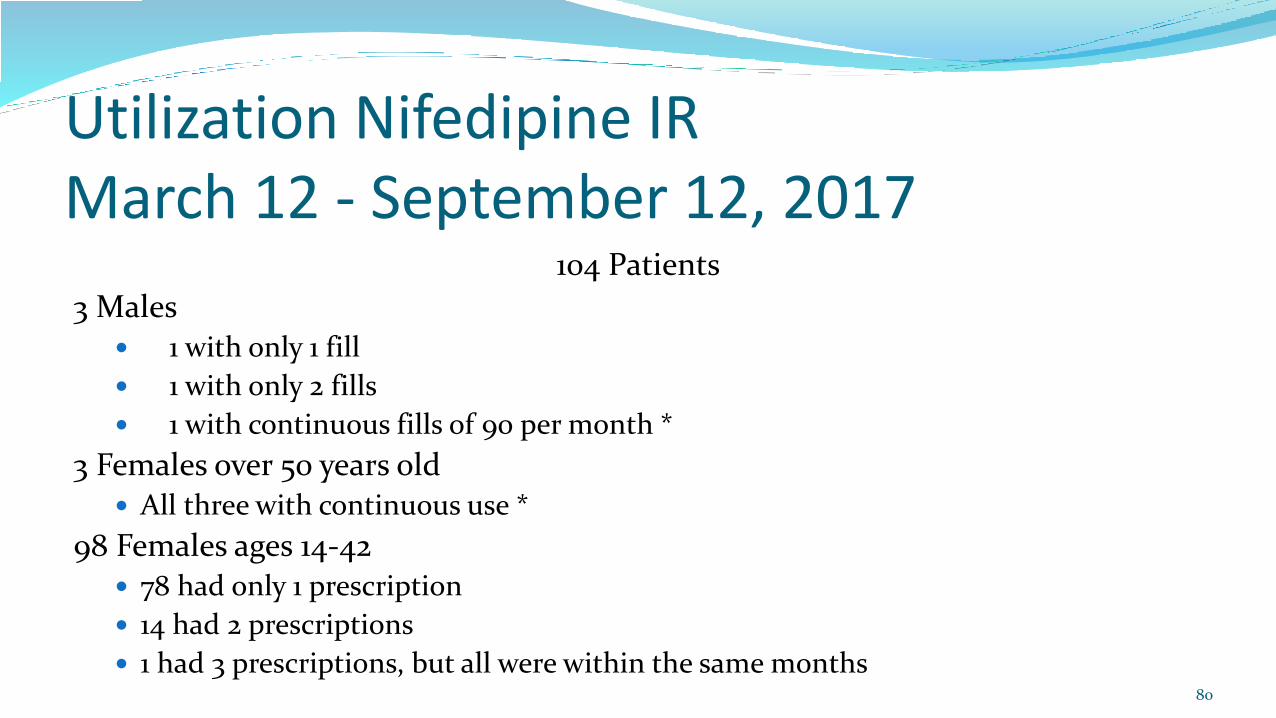
Utilization Nifedipine IR March 12 - September 12, 2017
104 Patients
3 Males 1 with only 1 fill
1 with only 2 fills
1 with continuous fills of 90 per month *
3 Females over 50 years old All three with continuous use *
98 Females ages 14-42 78 had only 1 prescription
14 had 2 prescriptions
1 had 3 prescriptions, but all were within the same months80

81
82
Concern Pharmacy and Therapeutics Committee at May 2017 meeting concerned
about use since not usually the drug of choice for hypertension
Suspected that use for hypertension associated with pregnancy
DUR to review diagnoses associated with use
83
Methyldopa UtilizationMarch 12, 2017 – August 12, 2017
17 individual patients
All female
Age Range 27-47 years
84
Associated Diagnoses Pregnancy Associated Hypertension in 12 patients
2 patients started during pregnancy, but continued to receive for continuing essential hypertension
1 patient received for maternal hypertension for pregnancy in 2013, 2015 and 2017. In between pregnancies received labetalol, lisinopril and nifedipine
1 patient (age 44) receiving continuously for essential hypertension
1 patient (age 41) had no listed diagnosis in record, but receiving continuously with other antihypertensives
85
86
Study Proposals for Upcoming Quarters:
87
Benzodiazepines
Buprenorphine vs. buprenorphine/naloxone for treatment of substance use disorder
Deprescribing Proton Pump Inhibitors
Buprenorphine without naloxone
Buprenorphine and Presence or Absence of Adjunct Therapy
Benzodiazepines
NICE (National Institute for Health and Care Excellence) – 2007
Generalized Anxiety Disorder
SSRIs for 12 weeks then if not effective switch to another for at least 6 months
Benzodiazepines for no more than 4 weeks in combination with SSRI only if adjunctive therapy is needed
Venlafaxine second line agent88
Benzodiazepines
NICE (National Institute for Health and Care Excellence) – 2007
Panic Disorder
SSRIs for 12 weeks to assess efficacy, duration of therapy of at least 6 months
Tricyclic antidepressants if multiple SSRIs fail
Benzodiazepines not recommended
89

Benzodiazepines
NICE (National Institute for Health and Care Excellence) – 2007
PTSD
SSRIs and mirtazapine as first line agents
Tricyclic antidepressants if first line agents fail
Benzodiazepines not recommended
90

Benzodiazepines
91
Benzodiazepines are a seductive but risky treatment for anxiety.
Quickly effective with few initial side effects.
BUT: Therapeutic effects lessen and side effects increase over time.
They also impede effectiveness of psychotherapies.
Reference: UW Telepain Webinar – 9/13/17 - Treatment of Anxiety
Plan for January 2018: Review national and international guidelines for treatment of anxiety and panic disorder with emphasis on the role of benzodiazepine therapy.
Observation: Many Idaho Medicaid participants are on chronic, scheduled, high dose benzodiazepine therapy who are NOT on any other anti-anxiety medication such as SSRIs, SNRIs, or buspirone.
92
93
Buprenorphine vs. buprenorphine/naloxone for treatment of substance use disorder
94
September 2017 POS Claims Data
Buprenorphine vs. buprenorphine/naloxone for treatment of substance use disorder
95
Criteria as stated on the PDL:
Oral buprenorphine/naloxone combination products are preferred except in pregnant women to minimize the possibility of diversion of buprenorphine single entity via the injection route.
This statement was copied from the SAMSHA website.
Buprenorphine vs. buprenorphine/naloxone for treatment of substance use disorder
96
The issue: Idaho Medicaid is getting many requests for single entity buprenorphine stating that the patient has had adverse effects to the naloxone component (not sure how the prescriber can tell that it is related to just the naloxone component) or that the patient is “allergic” to naloxone.
Data points to be collected: MID
Prescriber NPI
What is the reaction to naloxone – nausea, headache, something else
Incidence of report allergy or intolerance to Suboxone film
Patient currently pregnant or breastfeeding

October 19, 2017
97
October 19, 2017
98
October 19, 2017
99
Prospective DUR Report
100
History Errors:
• DD – drug-to-drug
• PG – drug to pregnancy
• TD – therapeutic duplication
• ER – early refill
• MC – drug-to-disease
Non-History Errors:
• PA – drug-to-age
• HD – high dose
• LD – low dose
• SX – drug-to-gender
Prospective DUR Report
101
DUR Board Meeting October 19, 2017
102
Next Meeting January, 2018
Location moving back to the Idaho Medicaid Offices at:
3232 Elder St.
Boise, ID 83705
103