Obstructive Sleep apnoea – relevance to the general physician
27
Obstructive Sleep apnoea – relevance to the general physician Dr Sophie West Newcastle Regional Sleep Service [email protected]
Transcript of Obstructive Sleep apnoea – relevance to the general physician

Obstructive Sleep apnoea –
relevance to the general
physician
Dr Sophie West
Newcastle Regional Sleep Service


Obstructive sleep apnoea
• Common in the general population
- 4% men, 2% women
>70 year olds = 15-20%
Men with Type 2 diabetes = 23%
Diabetic macular oedema = 50%
Bariatric surgery waiting list = 70%
Bipolar disorders = 21% -51%
Marfan’s Syndrome =33%
AAA= 41%


Fat distribution is important
Visceral
obesitySubcutaneous
obesity
OSA
DM
Met synd


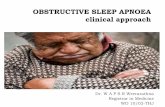
Overnight oxygen saturation levels in OSA: >400 dips/apnoeas in total
Beginning
of night
1st hr
2nd
hr
8th hr
End of
night
60 minutes
3rd hr



Red = SaO2, Blue = pulse rate
Episodic rise in pulse rate with each arousal from sleep (even if the
cortex is not ‘woken’ as well).

Arterial blood pressure during OSA
Rise with every
arousalRecurrent dips with every
obstructed breath

Kohler M, Stradling JR. Nature Rev Cardiol 2010


Symptoms of OSACommon (>60%)• Loud snoring• Excessive daytime sleepiness• Choking or shortness of breath sensations during sleep• Restless sleep• Unrefreshing sleep• Changes in personality• NocturiaLess common (10-60%)• Morning headaches Enuresis• Reduced libido Nocturnal sweating• Spouse worried by apnoeic episodesRare (<10%)• Recurrent arousals/insomnia • Nocturnal cough• Symptomatic oesophageal reflux

OSA in the medical clinic
• Snoring? Loud, nightly
• Witnessed apnoeas
• Unrefreshing sleep and daytime sleepiness
• Driving? Job? Shifts?
• Especially if associated other condition or difficult to control
Ask GP / Refer to Local
Sleep Service if suspicion
- we will do sleep study

Treatment of OSA
1. Weight loss (+bariatric surgery)
2. Sleep hygiene
– Avoidance of sedatives/alcohol
– Stop smoking
– Positional changes
3. Mandibular advancement device
(4. ENT Surgery)
5. CPAP

Nasal continuous positive airway pressure, CPAP
Newcastle > 5000 CPAP patients
c.£300
c.£100
c.£100

CPAP
Sullivan C et al. Lancet 1981



CPAP• Adjustment period – support from trained staff
• Side effects not severe – dry mouth/nose, red marks on face, air leak, noise
• Benefit generally proportional to OSA severity
• Generally well tolerated
Retrospective cohort analysis, n=640
• Average use 6.2 hours/night AIM 4 HRS
• 81% adherence at 5 years, 70% at 10 years
• Severity of OSA on sleep study determines long term adherence
Kohler M et al. Thorax 2010

CPAP
Could it be used to treat more than OSA?
Resolution of
intermittent hypoxia
Decreased sympathetic drive
Improved sleep architecture
Improved energy and activity
Decreased cellular inflammation

CPAP and other conditions
Robust RCT data:
• CPAP reduces BP – greatest if severe OSA,
high CPAP use, hypertension
Bazzano LA. Hypertension 2007
• CPAP reduces ESS in minimally symptomatic
people with OSA – cost effective
Craig S et al. Thorax 2012
• CPAP improves some measures of vascular
functionSchwarz EI et al. Respirology 2015

CPAP and other conditions
• CPAP probably improves cardiovascular risk
- But not yet demonstrated in RCT
- International trial ongoing
Marin JM et al. Lancet 2005

CPAP and diabetes
• Many RCTs show CPAP doesn’t improve glycaemic
control or insulin resistance
• – but one recent study 8 hrs CPAP /night for 2 weeks in
sleep lab N=39 “pre-diabetes” Insulin sensitivity improved,
p=0.04 Pamidi S. 2015;192:96-105.
• CPAP improved vision in patients with diabetic
macular oedema - small pilot study Mason RH et al. Respiration 2011

70 year old female
�Type 2 Diabetes Mellitus
�Blood Pressure 128/78mmHg
�HbA1c 55mmol/mol
ESS 5, ODI 57
….But, macular oedema

• Prevalent – especially if you see patients with
raised BMI, visceral obesity
• Relevant to general physician – association with
other conditions, may make them worse
• Treating OSA is straightforward, inexpensive, cost
effective
• Falls in sleepiness, better driving, Q of L
• Improved BP, ?CV disease
Refer to local sleep service to investigate
Obstructive Sleep apnoea