Obstructive sleep apnea among patients seeking outpatient ......Obstructive sleep apnea among...
1
Andrew Fritz M.D. University of Texas Southwestern Obstructive sleep apnea among patients seeking outpatient treatment for mental disorders About obstructive sleep apnea OSA and other mental disorders Proposed relationship of psychiatric and other factors in OSA OSA screening tools Evaluation of existing OSA screening tools and item availability in EMR Proposed Methods Acknowledgements Citations Obstructive Sleep Apnea Hypopnea (OSA) is a breathing-related sleep disorder characterized by apneas and hypopneas occuring more than 15 times per hour (Apnea Hypopnea Index [AHI] ≥ 15) diagnosed by polysomnography, or, apneas and hypopneas occurring more than 5 times per hour (AHI ≥ 5) when sleep-related symptoms are reported such as nocturnal breathing disturbances (snoring, snorting, gasping, or observed paused breathing) or symptoms while awake (daytime sleepiness, fatigue, or unrefreshing sleep) that are not attributable to another sleep disorder, other mental disorder, or a medical disorder. 1 The condition was not well characterized until 1978 and non-invasive treatment with positive airway pressure was introduced in 1981, 2 though recognized at least as early as 11th Century C.E. by Persian philosopher and physician Ibn-Sina or Avicenna. 3 The prevalence of OSA in the general population using the lowest cut-off (AHI 5) estimated between 9-38% in developed countries. 4 Prevalence is higher in adult male and post-menopausal female, obese, and elderly individuals. Individual anatomic and neurologic factors also impact risk. Prevalence is increasing, likely related to increasing obesity, average age, and recognition. 5 Despite being so common, OSA is often undiagnosed and untreated. 6 Untreated OSA is associated with significant adverse health outcomes like cardiovascular diseases, cerebrovascular events, diabetes, cognitive impairment decreased quality of life, motor vehicle crashes and all-cause mortality. 5 Obstructive Sleep apnea is common among individuals with diagnosed mental disorders. Some disorders correlate more with OSA diagnosis than others. A review identified OSA prevalence of 0.7% to 47.8% in Schizophrenia, 3.2% in Schizoaffective Disorder, 4.52% to 48% in pooled psychotic disorders, 2.9% to 69% in Bipolar I and II Disorders, 0% to 66% in MDD, 6.4% to 58.1 % in Anxiety Disorders and 1.3% to 83% in PTSD in published studies examining prevalence of OSA among patients with mental disorders; studies performed in inpatient or sleep clinic-referred populations generally produced higher prevalences. 7 In a study of veterans seeking psychiatric treatment at the Dallas VA Medical Center, OSA was diagnosed by polysomnography in 37.8% of patients with MDD, 35.3% of patients with PTSD, and 16.7% of patients with BD; and mood disorder comorbid with PTSD had a higher association with OSA than mood disorder alone. 8 Symptoms of OSA like sleep arousal, abnormal sleep duration, fatigue, sleepiness, anergia, and diminished concentration overlap with those of many mental disorders such as Mood disorders, Anxiety Disorders, Trauma- and Stressor- Related Disorders, Neurocognitive disorders, Attention Deficit/Hyperactivity Disorder and other Sleep-Wake Disorders. The presence and attribution of symptoms common to OSA impacts diagnosis of OSA other mental disorders and assessment of treatment responsiveness of both OSA and other mental disorders. There exists a variety of evidence that the relationship between OSA and other mental disorders is beyond correlation but rather bi- or multi- directional. 7 ● Polysomnography is required to diagnose OSA but may be expensive, time consuming, and of limited availability ● There exist numerous tools developed and or used to screen for OSA such as the Berlin Sleep Questionnaire, BMI-Neck, Epworth Sleepiness Scale, GOAL, Multivariable Apnea Prediction Index, NAMES, No-Apnea, Lausanne NOSAS, OSA-50, STOP-BANG Questionnaire and it’s variations, and the Symptomless Multivariable Apnea Prediction Index. ● Most rely on a mix of both objective and patient-reported data ○ BMI Neck, SMVAP objective only ○ ESS, WSQ, STOP patient-reported only ● Validation studies typically performed in various, but limited, populations for given screening tools ○ Multidisciplinary Sleep Clinic Referrals ○ Pre-Anesthesia Assessment ○ Occupation ● Current evidence is insufficient to assess the benefits and harms of routine screening for OSA in asymptomatic adults in general population. 5 ○ Given elevated OSA prevalence among patients with mental disorders, this recommendation may not apply to that population * available by PHQ-9 but specific question may not apply directly to given screening tools † may be available for patients taking medications associated with weight gain Hypotheses 1. OSA is prevalent, underdiagnosed and undertreated among patients using general psychiatric services, including at our institution 2. Screening patients for OSA risk / referral for sleep medicine evaluation can be completed using objective and patient reported data already available in EMR with similar accuracy to alternative screening tools that require less frequently obtained subjective and objective data, and without adding to clinician workload. 3. Diagnosis and treatment of unrecognized OSA in patients with one or more co-occurring mental disorders may lead to diagnostic clarification, improvement of symptoms, treatment response, and or treatment remission of co-occurring mental disorders. Of identified OSA Screening tools currently in use or recently developed, only SMVAP makes use only of items that are readily available in the local EMR at present. Unfortunately, it does not include subjective data items, which has been identified as an important factor in developing an ideal OSA screening tool by a Task Force of the American Academy of Sleep Medicine. However, the Task Force did not find any tool in use that met all criteria necessary to be recommended by the AASM and actually recommended the continued development and investigation of alternative screening methods. 9 SMVAP was identified as one of the screening tools meeting a majority of criteria. SMVAP was developed from the Multivariable Apnea Prediction index 10 by omitting the subjective questionnaire. 9 This was done because the target population of the study was commercial truck drivers and it was felt they would be incentivized to underreport subjective symptoms due to the potential for study outcome to impact their livelihood. 9 Use of objective only items may be of benefit in particular patient populations such as those with impaired communication and thought process such as patients with Schizophrenia 11 or perhaps those with Neurocognitive Disorders. SMVAP has also been implemented in to screen for risk of post-operative complications among over 50,000 pre-surgical patients and validated the screening test by comparing index score to known OSA previously diagnosed OSA. 12 Screening Tool: Berlin BMI-NECK ESS GOAL MVAP NAMES No-Apnea NOSAS OSA 50 STOP STOP-BAG STOP-BANG SMVAP WSQ Screening Item: Readily available in EMR Age x x x x x x x x Blood pressure x x x x x BMI x x x x x x x x x Diabetes x Heart disease x Sex/Gender x x x x x x x Stroke x Not readily available in EMR Falling asleep during an activity x x Neck circumference x x x x x Observed apnea x x x x x x x x Oral airway evaluation x (Loud) Snoring x x x x x x x x x Snorting / Gasping x Tiredness* x x x x x Waist circumference† x Next Steps 1. Select suitable screening tool with data readily available in EMR a. Symptomless Multivariable Apnea Prediction Index b. Or, devise novel screening tool using readily available data points c. Or, work with psychiatry clinic to initiate routine collection of additional data point(s) relevant to existing screening tool 2. Obtain data required by selected tool from EMR of psychiatry outpatients not previously diagnosed with OSA utilizing REDCap and the Clinical Data Pull (CDP) via FHIR (Fast Healthcare Interoperability Resource) 3. Identify patients for further evaluation, Invite and consent for further participation; 4. Perform additional OSA screening tools to allow comparison of suitable screening tool to existing tools 5. Obtain additional data to allow for analysis of confounding factors a. Psychiatric Diagnoses and Treatments b. Medical Diagnoses and Treatments c. Demographic Factors 6. Refer identified patients for sleep study (likely will require referral for sleep clinic evaluation as well) a. Decide between home sleep study vs. in-lab study for use as Gold Standard to assess screening tool. 1. Hone Proposal a. Feedback appreciated! 2. REDcap Training for data collection 3. Identify, Recruit, and seek input from additional stakeholders a. Rising PGY-3 and PGY-4 psychiatry residents interested in UTSW Sleep Medicine elective b. Representatives of UTSW Psychiatry and Sleep Medicine Clinics c. Statistical analysis support 4. Identify need for, obtain funding 5. IRB Consultation and Submission when regular clinical research activities resume Venkata Mukkavilli MD, University Hospital Sleep and Breathing Disorders Clinic, Department of Psychiatry, University of Texas Southwestern Medical Center, Dallas, TX Cisco Fritz 1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington D.C.: 2013. 2. Ralls F, Cutchen L. A contemporary review of obstructive sleep apnea. Curr Opin Pulm Med. 2019;25(6):578‐593. doi:10.1097/MCP.0000000000000623 3. BaHammam AS, Almeneessier AS. Dreams and Nightmares in Patients With Obstructive Sleep Apnea: A Review. Front Neurol. 2019;10:1127. Published 2019 Oct 22. doi:10.3389/fneur.2019.01127 4. Senaratna CV, Perret JL, Lodge CJ, et al. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med Rev. 2017;34:70‐81. doi:10.1016/j.smrv.2016.07.002 5. US Preventive Services Task Force, Bibbins-Domingo K, Grossman DC, et al. Screening for Obstructive Sleep Apnea in Adults: US Preventive Services Task Force Recommendation Statement. JAMA. 2017;317(4):407‐414. doi:10.1001/jama.2016.20325 6. Young T, Evans L, Finn L, Palta M. Estimation of the clinically diagnosed proportion of sleep apnea syndrome in middle-aged men and women. Sleep. 1997;20(9):705‐706. doi:10.1093/sleep/20.9.705 7. Gupta MA, Simpson FC. Obstructive sleep apnea and psychiatric disorders: a systematic review. J Clin Sleep Med. 2015;11(2):165‐175. Published 2015 Jan 15. doi:10.5664/jcsm.4466 8. Fehr BS, Katz WF, Van Enkevort EA, Khawaja IS. Obstructive Sleep Apnea in Posttraumatic Stress Disorder Comorbid With Mood Disorder: Significantly Higher Incidence Than in Either Diagnosis Alone. Prim Care Companion CNS Disord. 2018;20(4):18m02281. Published 2018 Aug 9. doi:10.4088/PCC.18m02281 9. Gamaldo C, Buenaver L, Chernyshev O, et al. Evaluation of Clinical Tools to Screen and Assess for Obstructive Sleep Apnea. J Clin Sleep Med. 2018;14(7):1239‐1244. Published 2018 Jul 15. doi:10.5664/jcsm.7232 10. Maislin G, Pack AI, Kribbs NB, et al. A survey screen for prediction of apnea. Sleep. 1995;18(3):158‐166. doi:10.1093/sleep/18.3.158 11. Szaulińska K, Wichniak A. BMI-NECK: A simple assessment of risk of obstructive sleep apnea in schizophrenia. J Psychiatr Res. 2020;125:33‐37. doi:10.1016/j.jpsychires.2020.03.005 12. Lyons MM, Keenan BT, Li J, et al. Symptomless Multi-Variable Apnea Prediction Index Assesses Obstructive Sleep Apnea Risk and Adverse Outcomes in Elective Surgery [published correction appears in Sleep. 2017 Jul 1;40(7):] [published correction appears in Sleep. 2017 Sep 1;40(9):]. Sleep. 2017;40(3):zsw081. doi:10.1093/sleep/zsw081 13. Rein K. Beyond Heart Health: Consequence of Obstructive Sleep Apnea [Internet]. Consult QD. Consult QD; 2020 [cited 2020May29]. Available from: https://consultqd.clevelandclinic.org/beyond-heart-health-consequences-of-obstructive-sleep-apnea 14. Green-Jones A. Science in the City brings research to life for the public to explore - CT Plus - UT Southwestern [Internet]. UT Southwestern Medical Center - The future of medicine, today! 2019 [cited 2020May29]. Available from: https://www.utsouthwestern.edu/ctplus/stories/2019/science-in-the-city.html Figure created by Gupta and Simpson demonstrating their proposed feed-forward pathway for the development of symptoms of upper airway instability and OSA from biological, psychiatric and metabolic dysregulation. 7 “Each symptom cluster is an independent entry point to the cycle. If left untreated, the presence of a risk factor increases the likelihood of the synergistic development of more symptoms from each cluster, resulting in OSA. The bolded arrows denote the most salient associations in the model.” 7 Depiction of airway obstruction as would occur in obstructive sleep apnea. Note the prone position of the sleeping figure, and the increased neck circumference. The figure is overlaid with examples of electrophysiological recordings representative of those of a polysomnogram. 13 Visitors ascending stairs at the UTSW North Campus. 14
Transcript of Obstructive sleep apnea among patients seeking outpatient ......Obstructive sleep apnea among...

Andrew Fritz M.D. University of Texas Southwestern
Obstructive sleep apnea among patients seeking outpatient treatment for mental disorders
About obstructive sleep apnea
OSA and other mental disorders
Proposed relationship of psychiatric and other factors in OSA
OSA screening tools
Evaluation of existing OSA screening tools and item availability in EMR
Proposed Methods
Acknowledgements
Citations
Obstructive Sleep Apnea Hypopnea (OSA) is a breathing-related sleep disorder characterized by apneas and hypopneas occuring more than 15 times per hour (Apnea Hypopnea Index [AHI] ≥ 15) diagnosed by polysomnography, or, apneas and hypopneas occurring more than 5 times per hour (AHI ≥ 5) when sleep-related symptoms are reported such as nocturnal breathing disturbances (snoring, snorting, gasping, or observed paused breathing) or symptoms while awake (daytime sleepiness, fatigue, or unrefreshing sleep) that are not attributable to another sleep disorder, other mental disorder, or a medical disorder.1
The condition was not well characterized until 1978 and non-invasive treatment with positive airway pressure was introduced in 1981,2 though recognized at least as early as 11th Century C.E. by Persian philosopher and physician Ibn-Sina or Avicenna.3
The prevalence of OSA in the general population using the lowest cut-off (AHI 5) estimated between 9-38% in developed countries.4 Prevalence is higher in adult male and post-menopausal female, obese, and elderly individuals. Individual anatomic and neurologic factors also impact risk.
Prevalence is increasing, likely related to increasing obesity, average age, and recognition.5
Despite being so common, OSA is often undiagnosed and untreated. 6
Untreated OSA is associated with significant adverse health outcomes like cardiovascular diseases, cerebrovascular events, diabetes, cognitive impairment decreased quality of life, motor vehicle crashes and all-cause mortality. 5
Obstructive Sleep apnea is common among individuals with diagnosed mental disorders. Some disorders correlate more with OSA diagnosis than others.
A review identified OSA prevalence of 0.7% to 47.8% in Schizophrenia, 3.2% in Schizoaffective Disorder, 4.52% to 48% in pooled psychotic disorders, 2.9% to 69% in Bipolar I and II Disorders, 0% to 66% in MDD, 6.4% to 58.1 % in Anxiety Disorders and 1.3% to 83% in PTSD in published studies examining prevalence of OSA among patients with mental disorders; studies performed in inpatient or sleep clinic-referred populations generally produced higher prevalences.7
In a study of veterans seeking psychiatric treatment at the Dallas VA Medical Center, OSA was diagnosed by polysomnography in 37.8% of patients with MDD, 35.3% of patients with PTSD, and 16.7% of patients with BD; and mood disorder comorbid with PTSD had a higher association with OSA than mood disorder alone.8
Symptoms of OSA like sleep arousal, abnormal sleep duration, fatigue, sleepiness, anergia, and diminished concentration overlap with those of many mental disorders such as Mood disorders, Anxiety Disorders, Trauma- and Stressor- Related Disorders, Neurocognitive disorders, Attention Deficit/Hyperactivity Disorder and other Sleep-Wake Disorders. The presence and attribution of symptoms common to OSA impacts diagnosis of OSA other mental disorders and assessment of treatment responsiveness of both OSA and other mental disorders.
There exists a variety of evidence that the relationship between OSA and other mental disorders is beyond correlation but rather bi- or multi- directional.7
● Polysomnography is required to diagnose OSA but may be expensive, time consuming, and of limited availability ● There exist numerous tools developed and or used to screen for OSA such as the Berlin Sleep Questionnaire, BMI-Neck,
Epworth Sleepiness Scale, GOAL, Multivariable Apnea Prediction Index, NAMES, No-Apnea, Lausanne NOSAS, OSA-50, STOP-BANG Questionnaire and it’s variations, and the Symptomless Multivariable Apnea Prediction Index.
● Most rely on a mix of both objective and patient-reported data○ BMI Neck, SMVAP objective only○ ESS, WSQ, STOP patient-reported only
● Validation studies typically performed in various, but limited, populations for given screening tools○ Multidisciplinary Sleep Clinic Referrals○ Pre-Anesthesia Assessment○ Occupation
● Current evidence is insufficient to assess the benefits and harms of routine screening for OSA in asymptomatic adults in general population.5
○ Given elevated OSA prevalence among patients with mental disorders, this recommendation may not apply to that population
* available by PHQ-9 but specific question may not apply directly to given screening tools† may be available for patients taking medications associated with weight gain
Hypotheses1. OSA is prevalent, underdiagnosed and undertreated among patients using general
psychiatric services, including at our institution
2. Screening patients for OSA risk / referral for sleep medicine evaluation can be completed using objective and patient reported data already available in EMR with similar accuracy to alternative screening tools that require less frequently obtained subjective and objective data, and without adding to clinician workload.
3. Diagnosis and treatment of unrecognized OSA in patients with one or more co-occurring mental disorders may lead to diagnostic clarification, improvement of symptoms, treatment response, and or treatment remission of co-occurring mental disorders.
Of identified OSA Screening tools currently in use or recently developed, only SMVAP makes use only of items that are readily available in the local EMR at present.
Unfortunately, it does not include subjective data items, which has been identified as an important factor in developing an ideal OSA screening tool by a Task Force of the American Academy of Sleep Medicine. However, the Task Force did not find any tool in use that met all criteria necessary to be recommended by the AASM and actually recommended the continued development and investigation of alternative screening methods.9 SMVAP was identified as one of the screening tools meeting a majority of criteria.
SMVAP was developed from the Multivariable Apnea Prediction index10 by omitting the subjective questionnaire.9 This was done because the target population of the study was commercial truck drivers and it was felt they would be incentivized to underreport subjective symptoms due to the potential for study outcome to impact their livelihood.9
Use of objective only items may be of benefit in particular patient populations such as those with impaired communication and thought process such as patients with Schizophrenia11 or perhaps those with Neurocognitive Disorders.
SMVAP has also been implemented in to screen for risk of post-operative complications among over 50,000 pre-surgical patients and validated the screening test by comparing index score to known OSA previously diagnosed OSA.12
Screening Tool: Berlin BMI-NECK ESS GOAL MVAP NAMES No-Apnea NOSAS OSA 50 STOP STOP-BAG STOP-BANG SMVAP WSQ
Screening Item:
Readily available in EMR
Age x x x x x x x x
Blood pressure x x x x x
BMI x x x x x x x x xDiabetes x
Heart disease x
Sex/Gender x x x x x x x
Stroke x
Not readily available in EMR
Falling asleep during an activity x x
Neck circumference x x x x x
Observed apnea x x x x x x x x
Oral airway evaluation x
(Loud) Snoring x x x x x x x x x
Snorting / Gasping x
Tiredness* x x x x x
Waist circumference† x
Next Steps
1. Select suitable screening tool with data readily available in EMR
a. Symptomless Multivariable Apnea Prediction Index
b. Or, devise novel screening tool using readily available data points
c. Or, work with psychiatry clinic to initiate routine collection of additional data point(s) relevant to existing screening tool
2. Obtain data required by selected tool from EMR of psychiatry outpatients not previously diagnosed with OSA utilizing
REDCap and the Clinical Data Pull (CDP) via FHIR (Fast Healthcare Interoperability Resource)
3. Identify patients for further evaluation, Invite and consent for further participation;
4. Perform additional OSA screening tools to allow comparison of suitable screening tool to existing tools
5. Obtain additional data to allow for analysis of confounding factors
a. Psychiatric Diagnoses and Treatments
b. Medical Diagnoses and Treatments
c. Demographic Factors
6. Refer identified patients for sleep study (likely will require referral for sleep clinic evaluation as well)
a. Decide between home sleep study vs. in-lab study for use as Gold Standard to assess screening tool.
1. Hone Proposal
a. Feedback appreciated!
2. REDcap Training for data collection
3. Identify, Recruit, and seek input from additional stakeholders
a. Rising PGY-3 and PGY-4 psychiatry residents interested in
UTSW Sleep Medicine elective
b. Representatives of UTSW Psychiatry and Sleep Medicine
Clinics
c. Statistical analysis support
4. Identify need for, obtain funding
5. IRB Consultation and Submission when regular clinical research
activities resume
Venkata Mukkavilli MD, University Hospital Sleep and Breathing Disorders Clinic, Department of Psychiatry, University of Texas Southwestern Medical Center, Dallas, TX
Cisco Fritz
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington D.C.: 2013.2. Ralls F, Cutchen L. A contemporary review of obstructive sleep apnea. Curr Opin Pulm Med. 2019;25(6):578‐593. doi:10.1097/MCP.00000000000006233. BaHammam AS, Almeneessier AS. Dreams and Nightmares in Patients With Obstructive Sleep Apnea: A Review. Front Neurol. 2019;10:1127. Published 2019 Oct 22.
doi:10.3389/fneur.2019.011274. Senaratna CV, Perret JL, Lodge CJ, et al. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med Rev. 2017;34:70‐81.
doi:10.1016/j.smrv.2016.07.0025. US Preventive Services Task Force, Bibbins-Domingo K, Grossman DC, et al. Screening for Obstructive Sleep Apnea in Adults: US Preventive Services Task Force Recommendation
Statement. JAMA. 2017;317(4):407‐414. doi:10.1001/jama.2016.203256. Young T, Evans L, Finn L, Palta M. Estimation of the clinically diagnosed proportion of sleep apnea syndrome in middle-aged men and women. Sleep. 1997;20(9):705‐706.
doi:10.1093/sleep/20.9.7057. Gupta MA, Simpson FC. Obstructive sleep apnea and psychiatric disorders: a systematic review. J Clin Sleep Med. 2015;11(2):165‐175. Published 2015 Jan 15. doi:10.5664/jcsm.44668. Fehr BS, Katz WF, Van Enkevort EA, Khawaja IS. Obstructive Sleep Apnea in Posttraumatic Stress Disorder Comorbid With Mood Disorder: Significantly Higher Incidence Than in Either
Diagnosis Alone. Prim Care Companion CNS Disord. 2018;20(4):18m02281. Published 2018 Aug 9. doi:10.4088/PCC.18m022819. Gamaldo C, Buenaver L, Chernyshev O, et al. Evaluation of Clinical Tools to Screen and Assess for Obstructive Sleep Apnea. J Clin Sleep Med. 2018;14(7):1239‐1244. Published 2018
Jul 15. doi:10.5664/jcsm.723210. Maislin G, Pack AI, Kribbs NB, et al. A survey screen for prediction of apnea. Sleep. 1995;18(3):158‐166. doi:10.1093/sleep/18.3.15811. Szaulińska K, Wichniak A. BMI-NECK: A simple assessment of risk of obstructive sleep apnea in schizophrenia. J Psychiatr Res. 2020;125:33‐37. doi:10.1016/j.jpsychires.2020.03.00512. Lyons MM, Keenan BT, Li J, et al. Symptomless Multi-Variable Apnea Prediction Index Assesses Obstructive Sleep Apnea Risk and Adverse Outcomes in Elective Surgery [published
correction appears in Sleep. 2017 Jul 1;40(7):] [published correction appears in Sleep. 2017 Sep 1;40(9):]. Sleep. 2017;40(3):zsw081. doi:10.1093/sleep/zsw08113. Rein K. Beyond Heart Health: Consequence of Obstructive Sleep Apnea [Internet]. Consult QD. Consult QD; 2020 [cited 2020May29]. Available from:
https://consultqd.clevelandclinic.org/beyond-heart-health-consequences-of-obstructive-sleep-apnea14. Green-Jones A. Science in the City brings research to life for the public to explore - CT Plus - UT Southwestern [Internet]. UT Southwestern Medical Center - The future of medicine,
today! 2019 [cited 2020May29]. Available from: https://www.utsouthwestern.edu/ctplus/stories/2019/science-in-the-city.html
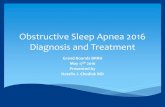
Figure created by Gupta and Simpson demonstrating their proposed feed-forward pathway for the development of symptoms of upper airway instability and OSA from biological, psychiatric and metabolic dysregulation.7
“Each symptom cluster is an independent entry point to the cycle. If left untreated, the presence of a risk factor increases the likelihood of the synergistic development of more symptoms from each cluster, resulting in OSA. The bolded arrows denote the most salient associations in the model.”7
Depiction of airway obstruction as would occur in obstructive sleep apnea. Note the prone position of the sleeping figure, and the increased neck circumference. The figure is overlaid with examples of electrophysiological recordings representative of those of a polysomnogram.13
Visitors ascending stairs at the UTSW North Campus.14