Objectives - Caribbean...
16
Transcript of Objectives - Caribbean...


ObjectivesAfter completing this module, the learner will be able to:
1. Discuss the history of dialyzer reprocessing.
2. List two reasons why dialysis centers reprocess dialyzers.
3. Explain the steps involved in dialyzer reprocessing.
4. Discuss the hazards to patients and staff that can occur with dialyzer reprocessing.
5. List the required documentation for dialyzer reprocessing.
Dialyzer Reprocessing
208
Module 7 cover photo credit:
Renaclear® Dialyzer Cleaning System reprinted with permission from Minntech Renal Systems, 2005.

IntroductionThe dialyzer is a feat of engineering: complexenough to do some of the work of a humankidney, yet simple enough to be mass-produced, and reliable enough to be used manytimes. For medical and non-medical reasons,many dialyzers are reprocessed: cleaned anddisinfected to be used again by the same patientinstead of being thrown out after a single use.This is called reuse.
Dialyzer reprocessing is regulated by the federaland some state governments. Regulationsinclude the standards and conditions centersmust follow so reuse is as safe and effective aspossible for both patients and staff.
A reprocessing technician has the immense job ofmaximizing patient benefits of reuse and reducingthe risks. This is done by carefully following all ofthe guidelines, regulations, and center procedures.
This module covers the history of the reasonsfor reprocessing, the role of regulations andguidelines, and the steps used to reprocess dialyzers.
History of DialyzerReprocessingDialyzer reprocessing has been around since the late1960s. At first done by hand, reprocessing is nowmost often done with a machine. Many factors aidedthe development and types of reuse equipment;one was the evolution of dialyzers themselves.
By the mid-1960s, most patients were treatedwith Kiil dialyzers (see Figure 1). A Kiil was a“sandwich” made of layers of membrane sheets
held apart by grooved boards of polypropyleneplastic. Rubber gaskets and metal clamps heldthe sandwich together. The Kiil had to beassembled and pressure tested before eachuse—a slow and complex technique. Often—10%–20% of the time—it would fail thepressure test, and the whole process would haveto start over with fresh sheets of membrane.
In 1967, Dr. Belding Scribner (who helpeddevise the vascular access) reported that theblood compartment of a Kiil could be filledwith a germicide (germ-killing solution),rinsed, and used for the next treatment. TheKiil did not have to be taken apart and rebuilt.This was one of the first examples of dialyzerreprocessing. For Dr. Scribner, the main reasonfor reusing Kiils was to save home patients the time and trouble of “tearing down”and rebuilding them. At that time, most of Dr. Scribner’s patients were doing homehemodialysis in his Seattle program.1
3209
Figure 1: Kiil dialyzer
Latches Inside the Kiil, two pairs of membranesheets (4 sheets) were separated bythree grooved polypropylene boards

By the late 1960s, new coil dialyzers werepreferred for reuse. Coils were easier to set upand prime (fill and rinse with normal saline)than Kiils, but too costly for many hospitals to use as disposable or single-use products, asmanufacturers suggested. Prior to reuse, theywere filled with a disinfecting solution to killgerms and kept in a refrigerator with sterilewater in the blood compartment.2
By the late 1970s, “disposable” parallel platedialyzers were being reused. The dialyzer couldbe sealed off with germicide in both the bloodand dialysate sides. This reduced the chances of contamination by bacteria.
When hollow fiber dialyzers came on themarket in 1970, they proved to be well-suitedfor reuse. With strong structural integrity, theywere easy to rinse. Water pressure could beused to wash fibrin and blood out of thedialyzer fibers. Reused hollow fiber dialyzersperformed better than other types. Cell volume(fiber bundle volume) was easy to measure.Since the fiber bundle volume could bemeasured and used to decide when thedialyzers should be discarded, the hollow fiberdialyzer became the preferred choice for reuse.
From 1964 to 1976, dialyzer reuse evolved; it wasstudied, changed, refined, tested, and practiced.Researchers looked at how reprocessed coil,parallel plate, and hollow fiber dialyzers differedfrom new dialyzers in clearance and removal of small molecules. They tried a number ofgermicides, dwell times, concentrations, andtemperatures. In time, they found ways toreliably kill and prevent the growth of bacteria.
Companies built single-station and multi-station automated systems for reprocessing.
Single-station systems were used for dialysis centersand home hemodialysis. These included the ECHO™by Mesa Medical, Inc., and the Renatron® byRenal Systems. A few companies made multi-station systems of varying sizes for center use.The ADR-22 by Texas Medical Devices, SeratronicsDRS-4, and the Lixivitron 2 by Harco MedicalElectronic Devices were four-station systems.The Belro Company built a six-station machine.Computer Dialysis Systems made largersystems; the Compudial KP-1 was 12 stations.
DIALYZERREPROCESSINGDEMOGRAPHICS
In 1976, about 18% of U.S. dialysis patients weretreated with reused dialyzers. In the 1980s, manystudies found that reuse with proper quality controlwas safe. Machines that made reprocessing easierand more efficient aided growth of the practice. In1983, dialysis payment from Medicare was changed:centers were paid a fixed sum—the compositerate—for each treatment. The change to acomposite rate may have been the single largestreason for the rapid growth of reuse, whichreached a peak in 1997, with 82% of centersusing it. In 2002, this dropped to 63%.3 In 2001,the largest dialysis company in the United Statesannounced a change to single-use dialyzers.4
Their market share ensures that dialyzer reusewill continue to drop in the United States.
Why DialyzersAre ReusedThe reasons for dialyzer reuse, both medicaland non-medical, have changed over time.
Dialyzer Reprocessing
210
MEDICAL REASONS FOR DIALYZER REUSE
The main medical reason to reuse dialyzers is to reduce hypersensitivity reactions. A patientmay have such a reaction in the first 15–30minutes of treatment with a new dialyzer.Symptoms include anxiety, itching, and troublebreathing, which can lead to respiratory failure.This is also called “first-use syndrome.” In rarecases, patients may have an anaphylacticreaction to a new dialyzer; this is a severe,sometimes fatal allergy, which may includehives and respiratory failure.
The most severe hypersensitivity reactions are dueto ethylene oxide (ETO). ETO is used to sterilizemost new dialyzers in the United States.5,6 Thechance of a reaction is less with a reused dialyzerbecause the repeated rinsings can lower the levelsof ETO.6 Rinsing new dialyzers can also reducereactions. The rinsing done for preprocessingand reprocessing can also remove other noxioussubstances from the dialyzers.
Some centers reuse dialyzers because they want toremove more middle molecules, such as beta-2-microglobulin (β2m). Reuse makes it possible forthese centers to afford the costly high-flux dialyzersthat do a better job of removing middle molecules.
SAFETY OF REUSEIn 1997, the National Kidney Foundation’sCouncil on Dialysis had an expert panel reviewclinical experience with dialyzer reuse since1988. The group looked at patient symptoms,death, chemical toxicity, and dialyzer clearance.While the Council did not take a stand for oragainst reuse, they found no effect of reuse onpatient illness or death.7 It has recently been
suggested that there was a patient survivaladvantage when dialyzer use was switched fromreuse to single-use.8 On the other hand, studiessuggesting that patients who reuse dialyzers do not have a higher mortality rate thanpatients on single-use dialyzers continue toemerge.9-11 Many authors believe reuse is safeand can deliver quality care if it is done usingrecognized reprocessing protocols such as those recommended by the Association for theAdvancement of Medical Instrumentation(AAMI) guidelines (as well as dialyzermanufacturers’ instructions).3,12-15
NON-MEDICAL REASONSFOR DIALYZER REUSE
The most common non-medical reason fordialyzer reuse is cost. Reusing a dialyzer canreduce the cost per dialysis treatment, evenincluding the staff time that is used.
Another argument for reuse is the environmentalimpact. Throwing out dialyzers can be a majorproblem and expense. Reusing them reducesthe amount of biohazardous waste.5
DialyzerReprocessingProcedureDialyzers should be reprocessed using theAAMI standards and recommendations. TheCenters for Medicare and Medicaid Services(CMS) adopted the AAMI guidelines as aCondition for Coverage for dialysis centers, andas federal regulations. The AAMI guidelinescover equipment, cleaning and disinfecting,
5211

labeling, record keeping, supplies,environmental safety, staff qualifications,training, and quality assurance (see Figure 2).15
All water used for reprocessing must meetAAMI standards.15
TYPES OF DIALYZERSIn 1996, the Food and Drug Administration(FDA) required that a dialyzer’s label mustreflect its commercial marketing and clinicaluse. Therefore, each dialyzer must be labeledfor “single” or “multiple” use. Companies whosell dialyzers to centers that reuse them mustgive instructions for safe and effective reuse.The label must have at least one recommended
way to reprocess the dialyzer and scientificdocumentation that it is safe and effective. Not all dialyzers are approved for use with allgermicides used in reprocessing. Only dialyzersthat can be reused can be labeled for “multipleuse.”16 Before you start to prepare a dialyzer forreprocessing, check the label for “multiple use.”
AUTOMATED VERSUSMANUAL SYSTEM
Dialyzer reprocessing can be done with amachine (see Figure 3) or manually (by hand).All the tasks done by the machine can also bedone by hand, but the automated system offersbetter quality control. Use of an automatedreprocessing machine is more efficient, moreconsistent, provides better records, and is saferfor patients.17
Preparing for the First Use of a Dialyzer
DIALYZER LABELINGPut the patient’s name on a dialyzer before you use it for the first time. If you have patientswith the same or similar last names, thedialyzer label must have a warning or alert. The label should also have extra informationsuch as the first name and middle initial, colorcode, or medical record number, to preventmix-ups (see Figure 4). The label will needspace for the number of uses, date and time ofthe last reuse, an identifier for the reprocessingstaff member, and results of tests done on thedialyzer.18
Dialyzer Reprocessing
212
Figure 2: Systems diagram for
reprocessing dialyzersDrawing adapted with permission from AAMI
REJECT DIALYZER – REMOVE FROM SERVICE* This step may be done later but must precede initiation of dialysis.
Initiate dialysis
Germicide/disinfectant test
Germicide/disinfectant rinseGermicide/disinfectant test
Patient ID check*
Inspection
MIN TIME
TIME LIMIT
Storage
InspectionGermicide/disinfectant fillPerformance test(s) (leak test)
Rinse/pre-clean
First useTermination of dialysis
Preprocessing (optional)
Re-label
Storage
New dialyzer
Storage
Check
Supplies
Fails specs
Water treatment
Tap water
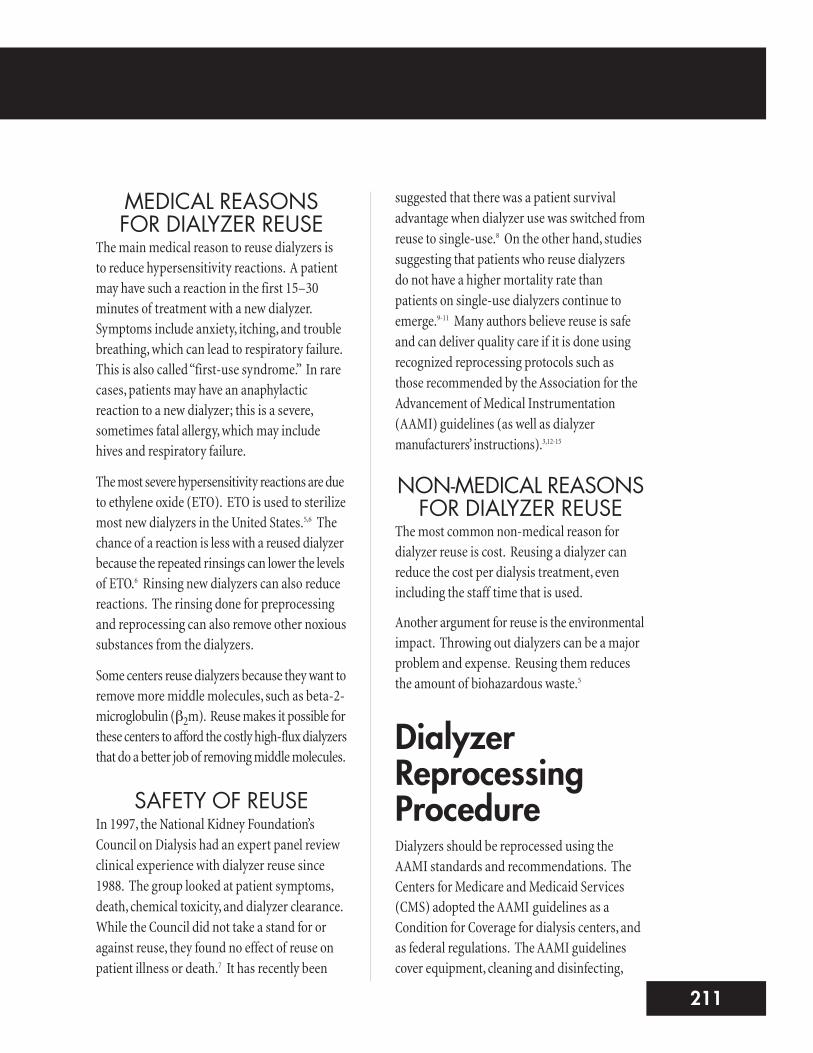
Labels need to stay readable throughreprocessing and dialysis. The label should notcover up the model number, lot number, arrowsfor direction of blood and/or dialysate flow, orother key data. Labels on dialyzers with clearcasings should be small enough that you cansee the blood path.
TOTAL CELL VOLUMEBefore using a new dialyzer for the first time,you will need to test it for baseline total cellvolume (TCV)—also called fiber bundlevolume (FBV)—or a baseline clearance value(e.g., urea, sodium, or ionic clearance).15 TheTCV measures the ability of the dialyzer totransport solutes and ultrafilter at its next use.Compare the baseline TCV or a baselineclearance with the TCV or clearance result aftereach reprocessing. Check each dialyzer against
its own TCV or its own clearance value. Thereare differences between dialyzers in TCV orclearance value that you will miss if they areonly measured in a batch.19
7213
Figure 3: Automated reprocessing
systemsDrawings adapted with permission
from Seratronics and Renal Systems, respectively
Figure 4: Example of a reprocessing label
Drawing adapted with permission from Seratronics

PREPROCESSMany centers preprocess new dialyzers.Preprocessing removes more residualgermicides, such as ETO, or other products ofmanufacturing, such as spallated particles, bore fluid, cleaning chemicals, phthalates,bisphenols, and other noxious substances thatcould cause harmful reactions the first time a dialyzer is used. Preprocessing allows for anaccurate measure of a dialyzers total cell volume.6
After DialysisAt the end of a treatment, blood in the dialyzeris “rinsed back”—returned to the patient. It is important to rinse as much of the blood aspossible back to the patient. A rinseback that is fair or poor leaves blood in the dialyzer (see Figure 5). Fair or poor rinseback leads topatient blood loss and is a reason to discard adialyzer. After rinseback, a dialyzer that passesinspection is taken off of the extracorporealcircuit and brought to the reprocessing room.
PRE-CLEANINGThe first step in reprocessing is to pre-clean the dialyzer. Pre-cleaning removes some of the blood from the blood compartment. Pre-cleaning may use reverse ultrafiltration; you do this by placing a cap on one of the dialysateports and sending a controlled supply of waterinto the other port.17 For some dialyzers, youmay need to remove the header (see Figure 6).6
If the header of the dialyzer is removed to allowfor cleaning, take special care to rinse anddisinfect the area, including the O-rings, beforeputting the headers back on the dialyzer.Germicides may be used during pre-cleaning.6
PERFORMANCE TESTSAfter you rinse and clean the dialyzer, you will needto test its functional and structural integrity.Federal and state regulations require measuringthe TCV after each reuse. You will also need todo a leak test; this measures how well thedialyzer can withstand a pressure load, andprotects the patient from a dialyzer blood leak.Finally, inspect the dialyzer for cracks, chips, ordefects in the plastic housing.18
DIALYZER REJECTIONIf a dialyzer fails the performance tests or visualinspection, throw it away. KDOQI guidelinesrecommend that dialyzers with less than 90% of the original clearance value (whether urea,sodium, or ionic clearance measures are used),or with less than 80% of the original TCV value, should be thrown out.19 Note: Loss of adialyzer’s transport capacity does not directlyrelate to fiber clotting because the (now) greaterblood flow velocity in the remaining unclottedfibers will cause a higher diffusion rate inside
Dialyzer Reprocessing
214
Figure 5: Good, fair, and poor rinsebacks
Good rinseback –a few streaks of blood
Fair rinseback –several streaks, possibly
in different places
Poor rinseback –many streaks
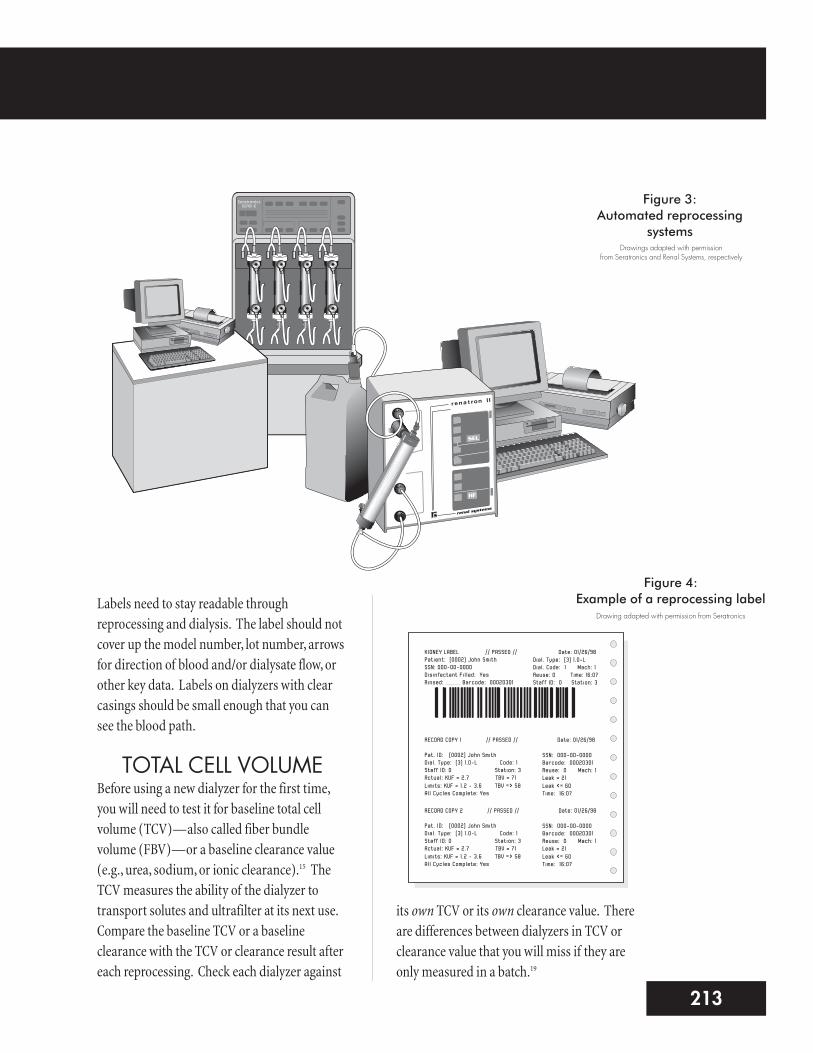
each such fiber. So, when the residual TCVvalue of a hollow fiber dialyzer is 80% of theoriginal TCV, the relative fall in urea, sodium, orionic clearance will only be about 10%.15
You will also discard dialyzers that have reachedtheir maximum number of uses (per yourcenter’s policy); fail the leak test; have cracks,chips, or defects in the plastic housing; havebeen exposed to more than one germicide; orhave many discolored fibers.18
DISINFECTIONThe next step is to disinfect the dialyzer. Theautomated system fills dialyzers with agermicide or disinfectant (agent that killspathogenic microorganisms). Dialyzers mustbe exposed to only one germicide duringreprocessing. Use of more than one germicidemay damage a dialyzer.20 The four main typesof germicides used in the U.S. are peraceticacid, formaldehyde, glutaraldehyde, and heatdisinfection with citric acid. Peracetic acid isthe most-commonly-used germicide.3 Eachgermicide has pros and cons (see Table 1).17
To ensure proper disinfection, the germicidemust stay in the dialyzer for a certain amount of time. The contact time (amount of time thegermicide remains in the dialyzer) differs foreach germicide (see Table 1).17
9215
Figure 6: Parts of hollow fiber dialyzer
Plastic casing, or housing
Hollow fibers
Header
Translucent polyurethane or polycarbonate (plastic) potting material.If endotoxin leaches into the potting material, it is difficult to remove it.
Dialyzerreprocessing
label
Blood may clot inside the hollow fibers,making the dialyzer difficult to rinse andclean completely.
Blood clotting may occur at the ends of the hollow fibers between the pottingmaterial and header.
Germicide Pro Con ContactTime
Peracetic acid •When diluted,breaks down tobiodegradableacetic acid,oxygen, and water
•Cost 11 hours
Formaldehyde •Cost • Technician mustuse a respirator
•Quick drenchshower needed inthe center
•May causecancer
• Disposal costs
24 hours
Glutaraldehyde •Cost • Linked withrespiratory andskin problems
• Disposal costs
10 hours
Heatdisinfection withcitric acid
•No staff safetyconcerns
•No environmentalconcerns
•Not all dialyzerscan be heatdisinfected
20 hours
Table 1: Germicide Pros, Cons, and Contact Time

Dialyzer Reprocessing
216
HANDLING HAZARDOUS MATERIALS
Germicides for reuse kill microorganisms—and they can also harm you and your patients.Occupational Safety and Health Administration(OSHA) Standards require centers to tell staff about allhazardous chemicals in the workplace. The centermust provide a list of all chemicals and keep itcurrent. One copy of the material safety data sheet(MSDS) for each substance must be kept in a filethat you can read. Another must be posted nearwhere a chemical is used, so you can find theinformation quickly in an emergency. All containersshould be labeled clearly to avoid mix-ups.21
Your center must train you in its procedures forhandling hazardous materials.21 The center mustalso encourage you to read its written policies.You should know where policies, emergencyprocedures, and training materials are kept inyour center. A center with more than 10 staffmust also keep records of occupational illnessesand injuries. It is the employer’s duty to ensurecompliance with safety practices and policies.
Procedures alone cannot prevent worker injuryfrom toxic substances. Each staff member mustlearn the steps and follow them. Taking shortcuts
with hazardous materials is not a time-saver ifit causes an accident. You must protect yourselfand others around you by learning how tohandle hazardous materials safely.
STORAGE OFREPROCESSED DIALYZERSBefore being stored, the outside of the dialyzer mustbe wiped or soaked clean with a disinfectant.Don’t store reprocessed dialyzers with new ones.Storage conditions should keep deterioration,contamination, and breakage to a minimum.Reprocessed dialyzers can be stored on wall racksor in carts until they are needed. The storagesystem should be designed to be easy to clean.Always follow your center’s policies and procedures.17
Preparing forNext Use
DIALYZER INSPECTIONThe first step in getting a dialyzer ready for its nextuse is looking at it (see Figure 7) to be sure that:
n It is labeled properly.
n No structural damage or tampering has occurred.
Figure 7: Reprocessed dialyzer
Verify correct patient name.
Hollow fibers should be relativelyfree of clotted blood.
Dialyzerreprocessing
label
Complete andlegible label.
There should be no visibledamage to the dialyzer.
All capsshould betight with no
leakage.
Thereshould beno clots inthe header.
Is aesthetic appearance acceptable to patient?

n Ports are capped, and there is no leakagefrom the ports or other parts of the dialyzer.
n It was stored long enough for the germicide towork, but not so long as to exceed acceptableshelf life.
n The cosmetic appearance is acceptable—itlooks clean.
After you look at the dialyzer, use a positive indicatortest strip or ampule to confirm that germicide ispresent and strong enough to work. Looking at thedialyzer cannot tell you how strong or concentratedthe disinfectant is. You must test the fluid itself toconfirm the presence and strength of germicide.15
REMOVAL OF GERMICIDEThe next step is to thoroughly rinse thegermicide out of the dialyzer before it is used,using the center’s procedure. Then, test thedialyzer to make sure the residual germicide is at or below the manufacturer’s and center’sspecifications, using a residual germicide test.It is important to keep fluids flowing in theextracorporeal circuit after you test for removalof the germicide. If not, you will need to retestfor germicide before starting the treatment. If you don’t rinse the dialyzer well enough, thepatient could be exposed to the toxic germicide.
PRIOR TO TREATMENTJust before the start of treatment, two people (staffand/or patient) must check the patient information onthe dialyzer to make sure it matches the patient.Record this step on the reprocessing record or dialysisflowsheet, and sign it to show who did the check. Staffmembers should ensure that the dialyzer has beenprepared for use. The dialyzer must be properlylabeled, structurally sound (no cracks or leaks, allcaps in place, etc.), free of germicide, and clean.15
Potential HazardsDialyzer reprocessing is safe and effective if it is done correctly. If it is done wrong, dialyzerreprocessing poses hazards to patients.
BACTERIA AND ENDOTOXINThe greatest risk of reuse comes fromcontamination of a dialyzer with bacteria orendotoxin (toxins on the membranes of certainbacteria). Bacteria and endotoxin may enter thedialyzer from the water used to make dialysate.After a treatment, some bacteria in the dialysatecompartment may stay in the dialyzer. If bacteriaand endotoxin multiply in the dialyzer and enterthe patient’s body, pyrogenic reactions (fever,chills, nausea, vomiting, hypotension, musclepain) or septicemia (blood infection) couldoccur. For patients, this can be life-threatening.18
Problems with bacterial or endotoxincontamination may occur due to:
n Improperly prepared germicide
n Use of outdated germicide
n Not enough contact time between the dialyzer and germicide
n Improper storage conditions
n Inadequate filling of the dialyzer
Dialyzer housings, support structures, andmembranes can adsorb (attract and hold)endotoxin. This makes endotoxin hard to rinseout. So, levels of bacteria and endotoxin in thewater used for reprocessing must be kept as lowas possible. Bacteria in water used to reprocessdialyzers must not exceed the AAMI standard of 200colony forming units (CFU).15 The AAMI action levelis 50 CFU for bacteria in water used for dialysate.
11217

The endotoxin level should be <2 endotoxin units/mL (EU/mL) with an action level of 1 EU/mL.22
If it is found that a patient had a pyrogenic reaction orsepticemia due to dialyzer reprocessing, the centermust stop reusing dialyzers. Reuse may not restartuntil the whole reprocessing system has been checked.20
CHEMICALSReprocessing germicides are toxic if they enter thepatient’s blood, even in small amounts (see Figure 8).If allof the germicide is not rinsed out before thenext treatment, the patient may have burning in the access limb, blurred vision, or numbnessin the lips. Death can occur from poisoning. Acute(sudden) toxicity may also occur if dialysis doesnot start right after an acceptable residualgermicide test; waiting may cause a rebound ofthe germicide in the blood compartment. Small
amounts of some germicides that don’t causeacute symptoms may still cause long-termproblems, such as trouble sleeping and changesin the body’s immune system. You must followcenter policies and procedures for chemical useexactly to avoid the risks and hazards of chemicaluse in reprocessing. More importantly, youmust test every dialyzer before use to be sure all of the chemicals have been removed.18
ALTERED DIALYZERPERFORMANCE
In time, reprocessing and reusing dialyzers reducesand alters their membrane surface area. This cancause poor solute transport and ultrafiltration, sothe dialysis prescription is not delivered. Reprocessingdialyzers can change their performance fromthe manufacturer’s specifications in a numberof ways. Contact with cleaning agents andgermicide can harm the membrane, causingleaks and reducing clearance. During reuse,hollow fibers can clog with blood, or membranesurfaces may be coated with blood products orother material. This can reduce flow and/or thesurface area of the dialyzer. A slower flow rateor smaller surface area can reduce clearance as well as the ultrafiltration rate (UFR).6
DocumentationDialyzer reuse is a vital part of hemodialysis in manycenters today. While reuse is a medical procedure, thereprocessing is much like a manufacturing process.Centers should follow the “good manufacturingpractice” standards used by dialyzer makers. Thismeans that a lot of documentation is needed(see Table 2).23 The staff person who documentsreprocessing and reuse must be diligent and precise.
Dialyzer Reprocessing
218
Figure 8: Medical risks of incorrect
dialyzer reprocessing
Sleep problems and changes in theimmune system caused by exposure tosmall amounts of germicide over time
Shortness of breath,respiratory distress
Burning in the vascular access
Anaphylaxis (severe,immediate allergicreaction), which may include:• Hives• Rapidly falling blood pressure
•Muscle spasmsin breathingpassages, GI tract, or uterus
• Swellingin the throat

Quality Assuranceand Quality ControlA center must prove it can safely and effectivelyreprocess dialyzers. Federal regulations requirea center that reuses dialyzers to have a programto monitor the system. Quality assurance andquality control are the two parts of the program.
The center needs to develop, implement, andevaluate policies and procedures on reuse. Allstandards, as well as state and federal regulations,must be included in the policies and procedures.Quality assurance provides the proof that policiesand procedures have been written and are beingimplemented. AAMI standards on reprocessing
have details on all aspects of a quality assuranceprogram (see Table 3 on page 220).15
Quality control shows that the materials, processes,and final product meet set standards. Examplesof quality control for dialyzer reprocessing are TCVmeasurement, bacterial and endotoxin tests, andtests for the presence or absence of germicide.
ConclusionDialyzer reprocessing, done correctly, is safeand effective for patients. If done incorrectly, itcan pose a hazard to patients and staff. As adialysis technician, your role is to follow thecenter’s policies and procedures on dialyzerreprocessing to ensure patient and staff safety.
13219
Document DescriptionDialyzer ReprocessingManual
A summary of all reuse specifications, policies, procedures, training materials,manuals and methods, and samples of forms and labels
Reprocessing Log Record of every step in the use of a dialyzer – from entry in the center to allperformance testing, to disposal
Water Quality Record of water treatment system maintenance and operation to meet AAMIstandards and the center’s policies and procedures
Complaint Investigation Fileand Special Incident Report
Record of all complaints by patients and staff about dialyzer failures or possibleharmful reactions, which includes results of any investigation of the complaintsand any actions taken to correct the problem
Environmental Testing Record of testing required by regulatory agencies on any germicides or cleaningagents used in dialyzer reuse
Equipment Maintenance Log of the dates of preventive maintenance, repairs, and results of scheduledtesting on all reprocessing equipment
Incoming Materials Log/Material Quality Records
Log of incoming materials such as dialyzers, port caps, disinfectants, otherreprocessing supplies, and results of any quality control tests
Personnel HealthMonitoring Records
Record of the results of medical exams of workers to monitor exposure tosubstances that may be toxic, as required by regulatory agencies
Training Records Record of staff’s completion of a training course in dialyzer reprocessing andproven ability to do reuse correctly
Quality Assurance andQuality Control
Record of the dates and results of all quality assurance and quality controlevaluations
Table 2: Dialyzer Reprocessing Documents

Dialyzer Reprocessing
220
Center Name: ____________________________________________
Q.A. Monitoring Activity Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Water culture/LAL testing (monthly)
Water chemical analysis (annually)
Level of airborne toxic chemicals
Complaint file audit & trend analysis
Physical plant audit
Personnel protection equipment(environment) audit
Dialyzer labeling parameters audit
Reprocessing technique audit
Reprocessing technique trend analysis
Preparation for dialysis audit
Germicide concentration verification(before dialysis)
Patient monitoring procedures audit
QA & QC procedures audit
Validation of clearance vs. TCV or FBV
General environmental safety audit
Audit of validation procedures(performance & germicide)
Reprocessing supplies parameters audit
Master record review & audit
Job descriptions audit
Training materials & trainingdocumentation auditAudit of compliance with informed consent policy
Audit of written policies & procedures
Audit of written maintenance & repair policiesAudit & trend analysis of maintenance & repair records
Table 3: Quality Assurance Schedule – Dialyzer Reprocessing
Table adapted with permission from the Association for the Advancement of Medical Instrumentation

15221
References1. Pollard TL, Barnett BMS, Eschbach JW, Scribner BH: A technique for storage and multiple re-
use of the Kiil dialyzer and blood tubing. Trans Amer Soc Artif Int Organs 13:24-28, 1967.
2. Deane N, Wineman RJ, Bemis JA (eds): Guide to Reprocessing of Hemodialyzers (Developmentsin Nephrology). Norwell, MA, Martinus Nijhoff Publishing, 1986, p 4.
3. Finelli L, Miller JT, Tokars JI, Alter MJ, Arduino MJ: National surveillance of dialysis-associateddiseases in the United States, 2002. Semin Dial 18(1):52-61, 2005.
4. [No authors listed]: Fresenius phasing out reuse at its dialysis clinics. Nephrol News Issues15(5):8, 2001.
5. Parks MS: Reuse: is it right for your facility? (Part 1.) Nephrol News Issues 17(6):72-75, 2003.
6. Clark WR, Scott MK, Leypoldt JK: Methods and complications of dialyzer reuse, in Nissenson AR,Fine RN (eds): Dialysis Therapy (3rd ed). Philadelphia, PA, Hanley & Belfus, Inc., 2002, pp 199-203.
7. Task Force on Reuse of Dialyzers, Council on Dialysis, National Kidney Foundation: NationalKidney Foundation report on dialyzer reuse. Am J Kidney Dis 30(6):859-871, 1997.
8. Lowrie EG, Li Z, Ofsthun N, Lazarus JM: Reprocessing dialyzers for multiple uses: recentanalysis of death risks for patients. Nephrol Dial Transplant 19(11):2823-2830, 2004.
9. Port FK, Wolfe RA, Hulbert-Shearon TE, et al: Mortality risk by hemodialyzer reuse practiceand dialyzer membrane characteristics: results from the USRDS dialyzer morbidity andmortality study. Am J Kidney Dis 37(2):276-286, 2001.
10. Collins AJ, Liu J, Ebben J: Dialyzer reuse-associated mortality and hospitalization risk in incidentMedicare haemodialysis patients, 1998-1999. Nephrol Dial Transplant 19(5):1245-1251, 2004.
11. Fan Q, Liu J, Ebben JP, Collins AJ: Reuse-associated mortality in incident hemodialysispatients in the United States, 2000 to 2001. Am J Kidney Dis 46(4):661-668, 2005.
12. Murthy BVR, Pereira BJG: Effects of reuse on dialyzer function. Semin Dial 13(5):282-286,2000.
13. Kaufman AM, Levin NW: Dialyzer reuse, in Daugirdas JT, Blake PG, Ing TS (eds): Handbook of Dialysis (3rd ed). Philadelphia, PA, Lippincott, Williams & Wilkins, 2001, pp 169-181.
14. Light PD: Reuse of hemodialysis membranes in chronic dialysis therapy, in Henrich WL (ed).Principles and Practice of Dialysis (3rd ed). Philadelphia, PA, Lippincott, Williams & Wilkins,2004, pp 16-27.

Dialyzer Reprocessing
222
15. Association for the Advancement of Medical Instrumentation: Reuse of hemodialyzers(ANSI/AAMI RD47:1993). Arlington, VA, American National Standard, 2000.
16. U.S. Food and Drug Administration. Guidance for hemodialyzer reuse labeling. Available at:www.fda.gov/cdrh/comp/2507.pdf. Accessed July 2005.
17. Parks MS: Reuse: is it right for your facility? (Part 2.) Nephrol News Issues 17(7):30-34, 2003.
18. Shusterman NH, Feldman HI: Methods and complications of dialyzer reuse, in Nissenson AR,Fine RN (eds): Dialysis Therapy (2nd ed). Philadelphia, PA, Hanley & Belfus, Inc., 1993, pp 133-138.
19. National Kidney Foundation. KDOQI clinical practice guidelines and clinical practicerecommendations for 2006 updates: hemodialysis adequacy, peritoneal dialysis adequacy,and vascular access. Am J Kidney Dis 48(1 Suppl 1):S1-S322, 2006.
20. Centers for Medicare and Medicaid Services, HHS. Reuse of hemodialyzers and other dialysissupplies. Code of Federal Regulations, 42 CFR Ch. IV 405.2150, 168-169. Available at:www.access.gpo.gov/nara/cfr/waisidx_04/42cfr405_04.html. Accessed July 2005.
21. U.S. Department of Labor, Occupational Safety and Health Administration: Hazardcommunication (29 CFR Part 1910.1200). Federal Register, 61, 5507, 1996. Available at:www.osha.gov. Accessed October 2005.
22. Association for the Advancement of Medical Instrumentation: Dialysate for hemodialysis(ANSI/AAMI RD52:2004). Arlington, VA, American National Standard, 2004.
23. Taaffe VS: Quality assurance for hemodialyzer reprocessing: minimizing risks. Nephrol NewsIssues 15(7):36-40, 2001.
For more information on reuse and its history, two recent references are available:
1. Twardowski ZJ: Dialyzer reuse—part I: historical perspective. Semin Dial 19(1):41-53, 2006.
2. Twardowski ZJ: Dialyzer reuse—part II: advantages and disadvantages. Semin Dial19(3):217-226, 2006.