Obesity: Objectives Causes and Consequences medical Jack A ... · 04.02.2014 · from L. obesitas...
13
1 Obesity: Causes and Consequences Jack A. Yanovski, M.D.. Ph.D. Chief, Section on Growth and Obesity Program in Developmental Endocrinology and Genetics National Institute of Child Health and Human Development Objectives • WHAT is obesity? • WHAT are the medical consequences of obesity? • WHY do some people become obese? What is Obesity? Obesity is an excess of body fat from L. obesitas "fatness, corpulence" Body Mass Index (BMI) • BMI = weight (kg)/height (m) 2 • Measure of weight adjusted for height • Highly correlated with body fat – Relationship varies with age, gender, ethnicity, and body build • Easy to obtain • Does not distinguish between body fat and muscle OVERFAT: 220 LBS One can be overweight but not overfat OVERWEIGHT: 220 LBS 0 10 20 30 40 50 60 70 Relationship Between BMI and Percent Body Fat in Men and Women Adapted from: Gallagher et al. Am J Clin Nutr 2000;72:694. Body Fat (%) Body Mass Index (kg/m 2 ) 0 10 30 40 60 20 50 Women Men
Transcript of Obesity: Objectives Causes and Consequences medical Jack A ... · 04.02.2014 · from L. obesitas...

1
Obesity:Causes and
ConsequencesJack A. Yanovski, M.D.. Ph.D.
Chief, Section on Growth and Obesity
Program in Developmental Endocrinology and Genetics
National Institute of Child Health and Human Development
Objectives
• WHAT is obesity?
• WHAT are the medical consequences of obesity?
• WHY do some people become obese?
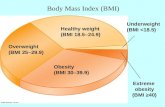
What is Obesity?
Obesity is an excess of body fat
from L. obesitas "fatness, corpulence"
Body Mass Index (BMI)
• BMI = weight (kg)/height (m)2
• Measure of weight adjusted for height
• Highly correlated with body fat– Relationship varies with age, gender, ethnicity, and
body build
• Easy to obtain
• Does not distinguish between body fat and muscle
OVERFAT: 220 LBS
One can be overweight but not overfat
OVERWEIGHT: 220 LBS
0
10
20
30
40
50
60
70
Relationship Between BMI and Percent Body Fat in Men and Women
Adapted from: Gallagher et al. Am J Clin Nutr 2000;72:694.
Bo
dy
Fa
t (%
)
Body Mass Index (kg/m2)
0 10 30 40 6020 50
Women
Men

2
By BMI, >65% of US Adults Are Overweight, >30% are Obese
Prevalence of obesity (BMI ≥ 95th percentile) in children has
tripled, but stable in girls over past 10 years
0
5
10
15
20
25
Boys Girls Boys Girls
1971-74 1976-80 1988-94 1999-2002
2003-2006 2006-2008 2009-2010
6-11 years 12-19 years
Ogden et al JAMA 307:483-490, 2012
BM
I ≥
95th
Per
cent
ile
BMI-Associated Disease Risk
Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults—The Evidence Report. Obes Res 1998;6(suppl 2).
Additional risks: Poor aerobic fitnessLarge waist circumference (men > 40 in; women > 35 in)
Classification BMI (kg/m2) Risk
Underweight < 18.5 Increased
Normal 18.5 – 24.9 Normal
Overweight 25.0 – 29.9 Increased
Obese I 30.0 – 34.9 High
II 35.0 – 39.9 Very high
III ≥ 40 Extremely high
Rel
ativ
e R
isk
of C
VD
Mor
talit
y
1
2
3
4
5
6
7
8
Lean Normal Obese
Body Fat Category (% Weight as Fat)
< 16.7% 16.7% – 24.9% 25%
Fatness, Fitness, and Cardiovascular Disease Mortality
Lee et al. Am J Clin Nutr 1999;69:373.
Aerobically fit
Unfit
Subcutaneous Fat
Abdominal Muscle Layer
Intra-abdominal Fat
Visceral Adiposity:
Amount of intra-abdominal (visceral) fat is well correlated to the complications of obesity
Medical Complications of Obesity
Phlebitisvenous stasis
Coronary heart disease
Pulmonary diseaseabnormal functionobstructive sleep apneahypoventilation syndrome
Gall bladder disease
Gout
Diabetes
Osteoarthritis
Nonalcoholic fatty liver diseasesteatosissteatohepatitiscirrhosis
HypertensionDyslipidemia
Cataracts
Skin
Pancreatitis
Idiopathic intracranial hypertension
Cancerbreast, uterus, cervix, prostate,kidney, colon, esophagus, pancreas, liver
Gynecologic abnormalitiesabnormal mensesinfertilitypolycystic ovarian syndrome
Stroke

3
Why do people become obese?
Obesity Is Caused by Long-Term Positive Energy Balance
FatStores
America’s Weapons of Mass Destruction
• 50 - 80% of the variance in human body weight is accounted for by genetic variation
• The remainder is explained by common environmental factors
Genetic Epidemiology of Human Obesity: Twin studies
Indianfamily from
Mexico
Pima Indianfamily in the
US
Portion size and pediatric obesity
0
10
20
30
40
50
60
70
Nu
mb
er o
f L
arge
-Siz
e P
orti
ons
Intr
odu
ced
1970 - 74 1975 - 79 1980 - 84 1985 - 89 1990 - 94 1995 - 99
0
3
6
9
12
15
Per
cen
t O
verw
eigh
t (>
95t
h c
enti
le)
1970 - 74 1975 - 79 1980 - 84 1985 - 89 1990 - 94 1995 - 99
12-19 year olds
6-11 year olds

4
Portion sizes have increased over the years
100
200
300
400
500
600
700 19552001
Ca
lori
es
McDonald’sFries
Coca-Cola Snickers
2.3 oz 6.9 oz 6.5 oz 20 oz 1.1 oz 3.7 oz
Nutrition Action, 2001.
Environmental Changes in Physical Activity
• Decreased physical activity in schools/workplace/communities– Few schools offer daily P.E.– Fewer jobs require manual labor– Lack of sidewalks
• Increased sedentary behavior– Office and home– Computer, video games, television
Relative Risk of Developing Obesity and TV Viewing in Adults
Nurses Health Study (1992-1998)
0
0.5
1
1.5
2
2.5
0 to 1 2 to 5 6 to 20 21 to 40 >40
Hu et al., JAMA; 2003:1785
P<0.001
Hours per Week
Season Matters: Weight change is
greatest during thewinter holiday season
Yanovski et al
NEJM 342
861-72000
Sept - Nov Holiday Jan - March March - Nov
0.00
0.25
0.50
0.75
p < .001
Wei
gh
t C
han
ge
(kg
)

5
Why Do People Become Obese?
• Changes in our environment explain why obesity has become more common over the last 40 years
• Our genes make us respond to our current environment by becoming obese
Identical Twins Fraternal Twins
Effects of Parental Obesity on Child Body Adiposity
0
5
10
15
20
25
Per
cen
t of
Cas
es
-3 -2 -1 0 1 2 3
Triceps fatfold SDS
two lean parents
0
5
10
15
20
25
Per
cen
t of
Cas
es
-3 -2 -1 0 1 2 3
2 obese parents
Garn and Clark, Pediatr. 57: 443, 1976
<15% >75%
Age 14y Height 172 cm, weight 166 kg, BMI 56.3 kg/m2
• Endocrinologic abnormalities• Medication-related• Hypothalamic damage related• Genetic
– Established syndromes– Leptin signaling pathway defects
Differential Diagnosis of Obesity Classical Endocrinologic causes of obesity
• Hypothyroidism– weight gain
– fatigue
• Hypercortisolism– 1 in 1,000,000 prevalence
– weight gain, striae, depression…
• Hyperinsulinemia (insulinoma)– Hypoglycemic episodes with
weight gain
Before After

6
Medications associatedwith pediatric obesity
• Glucocorticoids
• Psychotropic Agents– Antipsychotics: phenothiazines, clozapine,
resperidone
– Mood stabilizers: lithium, gabapentin
– Antidepressants: amitryptiline, mirtazapine
• Anticonvulsants: valproate, carbamazepine
• Serotonin Receptor Antagonist: cyproheptadine
• Antihypertensives: propranolol, nifedipine, clonidine
Genetic Syndromes Associated with Obesity
– Down Syndrome (trisomy 21)
– Prader Willi - (15 q 11.2-12)
– Bardet Biedl Syndromes
– Pseudohypoparathyroidism - inactivation of the stimulatory G protein subunit (20-q13.3)
– Achondroplasia - FGF-R3 (4p16.3)
– Turner Syndrome (45 XO)
Brushfield spot
Epicanthal fold
Palmar Crease
Cupped pinnae
Down Syndrome
Prader Willi Syndrome• Hypotonia, poor feeding neonatal period,
• After age 2y, obesity, “insatiable appetite, small hands/feet, hypogonadism,
• Abnormalities of 15q11-q12– Paternal deletions
– Uniparental (maternal)disomy
– Abnormal methylation
Bardet Biedel Syndromes
• Obesity
• Retinal degeneration
• Extra digits hands/toes
• Genital hypoplasia or hypogonadism (most males, 50% females)
• Mental retardation 75%
New Genetic Syndromes Associated with Obesity
• Leptin deficiency
• Leptin Receptor Deficiency
• Prohormone Convertase 1 deficiency
• POMC processing mutation
• Melanocortin 4 Receptor mutation
• Melanocortin 3 Receptor mutation

7
Wild-Type Mice ob/ob (leptin deficient)
Discovery of Leptin, Dec. 1994Transforming Event in Obesity Research
Zhang et al, Nature 372:425 (1994)
Leptin
Hypothalamic Leptin
receptors
PC-1POMC
Neuropeptide Y
α - MSH
Melanocortin Receptors
NPY Receptors
Autonomic Nervous System
Beta-3 Adrenergic receptors
Appetite
CRH,GnRH,TRH
Leptin Signaling and Obesity
Leptin Gene Deletion
Montague et al, Nature 387:903-908, 1997
• 2 cousins from a highly consanguineous Pakistani family
• Normal at birth, rapid weight gain
• Very low leptin despite high % fat
• Single base deletion introducing a premature stop codon
Plasma Leptin
0
15
30
45
60P
lasm
a L
epti
n (n
g/m
L)
10 20 30 40 50 60
DXA Percent Fat
Leptin Mutation
Healthy Children
Leptin-Deficiency
Farooqi et al, NEJM 341:879-884, 1999
0
10
20
30
40
50
60
70
80
90
100
Wei
ght
(kg)
0 1 2 3 4 5 6 7 8 9 10
Age (years)
98thPercentile
50thPercentile
2ndPercentile
Leptin treatment

8
Leptin treatment
Farooqi et al J Clin Invest; 106: 1093-1103, 2002
Effects of leptin
injections in a child
with leptin
deficiency
Little efficacy of leptin in obese humans who are not leptin deficient
Hypothalamic Leptin
receptors
PC-1
Leptin
POMC
Neuropeptide Y
α - MSH
Melanocortin Receptors
NPY Receptors
Autonomic Nervous System
Beta-3 Adrenergic receptors
Appetite
CRH,GnRH,TRH
Leptin Signaling and Obesity
Human Leptin Receptor Mutations
• Early-onset obesity
• High leptin
• Failure to enter puberty normally
Clement et al. Nature 392, 398–401, 1998
z
500 kcal/d diet
Patients with leptin receptor deficiency (LEPR-/-) have significant hyperleptinemia
LEPR-/- Controls0
25
50
75
100
125 p=0.003
Ser
um
Lep
tin
(n
g/m
L)
Adapted from Farooqi et al. N Engl J Med 2007Adjusted for fat mass

9
Leptin Receptor Deficiency –NIH Family
• Two siblings with early-onset obesity
• High leptin, even forobese children
Gil et al, Obesity, In Press, 2014
Leptin Receptor Deficiency –NIH Family
• Two siblings with early-onset obesity
• High leptin, even forobese children
• Consanguinity
Gil et al, Obesity, In Press, 2014
Whole Exome Sequencing of affected siblings
• 36,100 shared single nucleotide variants– 1537 rare and non-synonymous
• 4,702 shared recessive indels– 1,213 both rare and functional (frameshift, amino acid
insertion or deletion, or splice site)
• Filtering by pathogenicity and conservation: – Homozygous for 15 potentially damaging variants (10
SNVs and 5 indels)
• 1 Homozygous leptin receptor change
Mutation in Leptin Receptor
Premature stop codon after insertion of 9 novel amino acids
Gil et al, Obesity, In Press, 2014
Some obese humans with normal leptin receptor sequence are as obese and hyperleptinemic as those with leptin receptor deficiency
Farooqi et al, NEJM 356: 237-247, 2007
10
100
1000
Normal leptinreceptor sequence
Leptin receptordeficiency
Se
rum
Le
pti
n (
ng
/mL
)
Bardet-Biedl syndrome (BBS):Obesity, leptin resistance & hyperleptinemia
• BBS: a pleiotropic, polygenic obesity syndrome

10
Bardet-Biedl syndrome (BBS):Obesity, leptin resistance & hyperleptinemia
• BBS: a pleiotropic, polygenic obesity syndrome
• BBS proteins essential for normal function of primary cilium
• Inactivation of BBS proteins in miceleads to aberrant leptin receptor trafficking in hypothal impaired
Bardet-Biedl syndrome (BBS):Obesity, leptin resistance & hyperleptinemia
• BBS: a pleiotropic, polygenic obesity syndrome
• BBS proteins essential for normal function of primary cilium
• Inactivation of BBS proteins in miceleads to aberrant leptin receptor trafficking in hypothalamic neurons, impaired leptin signaling, and hyperleptinemia
Hyperleptinemia consistent with leptin resistance in patients with
Bardet-Biedl syndrome
Obese Controls BBS0
10
20
30
40
50 p<0.001
(n=63) (n=37)
Lep
tin
(n
g/m
L)
J Clin Endocrinol Metab; 96:E528-35, 2011
Adjusted for age, sex, race, & body fat %
Leptin
Hypothalamic Leptin
receptors
PC-1POMC
Neuropeptie Y
α - MSH
Melanocortin Receptors
NPY Receptors
Autonomic Nervous System
Beta-3 Adrenergic receptors
Appetite
CRH,GnRH,TRH
Leptin Signaling and Obesity
NH3 COOH
ß-lipotropin
BetaMSH
BetaEndorphin
GammaMSH
ACTH
Alpha MSH
16 K Fragment
Mutations disrupting ACTH / alpha MSH synthesis
= normal processing cleavage sites
Krude et al, Nature Genetics 19: 155-157, 1998
Pro-opio-melanocortin (POMC)
POMC Processing Human POMC Mutations
Krude et al, Nature Genetics 19: 155-157, 1998
• Can interfere with Processing of POMC into ACTH, alpha MSH, and beta-endorphin
• Red Hair (MC-1R)
• Congenitaladrenal hypoplasia(MC-2R)
• Obesity(MC-4R)

11
Leptin
Hypothalamic Leptin
receptors
PC-1POMC α - MSH
Melanocortin Receptors
NPY Receptors
Autonomic Nervous System
Beta-3 Adrenergic receptors
Appetite
CRH,GnRH,TRH
Leptin Signaling and Obesity
Neuropeptide Y
NH3 COOH
ß-lipotropinACTH
Alpha MSH
GammaMSH
BetaMSH
BetaEndorphin
16 K Fragment
Mutations disrupting prohormone convertase 1
= normal processing cleavage sites
Krude et al, Nature Genetics 19: 155-157, 1998
Pro-opio-melanocortin (POMC)
POMC Processing
x x x x
Human Prohormone Convertase 1 Mutations
Jackson et al. Nature Med 16, 303-306, 1997
• Early-onset Obesity
• Abnormal post-translational hormone processing:– Hypogonadotropic hypogonadism
– Low cortisol
– Low insulin
– High pro-insulin
– High POMC
Leptin
Hypothalamic Leptin
receptors
PPAR--2 receptors
PC-1POMC α - MSH
Melanocortin Receptors
NPY Receptors
Autonomic Nervous System
Beta-3 Adrenergic receptors
Appetite
CRH,GnRH,TRH
Leptin Signaling and Obesity
Neuropeptide Y
MC4R -/-
Wild Type
Photograph courtesy of Daniel Marks, M.D., Ph.D.
Melanocortin 4 Receptor Knock-Out
Mouse
9y old with homozygous MC4-R mutation and 16y old normal brother
Farooqi et al NEJM 348:1085-1095,2003

12
Melanocortin 4 receptor heterozygous inactivating
mutations are common• 1.4% of 140 obese adults Gu et al Diabetes 48:635-9, 1999
• 0.7% of 306 children with BMI 34 ± 7 kg/m2
Hinney et al, J Clin Endocrinol Metab 84:1483-6;1999
• 4.0% of 209 French adults with BMI > 40 kg/m2
Vaisse et al, J Clin Invest 106:253-62, 2000
• 3.3% of 243 UK adults with history of onset of obesity before age 10y Farooqi et al, J Clin Invest 106:271-9, 2000
2.4% of severely obese may have heterozygous mutations of MC4 receptor
Melanocortin 3 ReceptorMC3R Knock-out
mice:• Increased fat mass• Reduced lean mass• Higher feeding
efficiency
– Chen AS, et al. Nature Genetics, 2000; 26:97-102
BMI-SD and DXA Fat Mass by Genotype of Function-Altering
MC3R Polymorphisms in African American and Caucasian Children
BMI-SD Score
African American Caucasian0
2
4
6
8Wt/WtWt/PP/P
BM
I-S
D S
core
DXA Fat Mass
African American Caucasian0
10
20
30
40
50
60Wt/WtWt/PP/P
DX
A f
at m
ass
(kg
)
P = 0.024 P = 0.041
P = 0.017P = 0.021
Double Mutant hMC3R knockin mice are more adipose than Wild Type hMC3R knockin mice
MC3RhWT/hWTMC3RhDM/hDM MC3RhWT/hWTMC3RhDM/hDM
…Back to our patient
Plasma Leptin
OurPatient
0
15
30
45
60
Pla
sma
Lep
tin
(ng/
mL
)
10 20 30 40 50 60
DXA Percent Fat
Leptin Mutation
Healthy Children

13
Our Patient
• He has a function-altering variant of the melanocortin 3 receptor, (Thr6Lys+Val81Ile)
• He has hyperinsulinemia and hypercholesterolemia
How should he be treated?
AAP Recommended Weight Goals for Overweight Children and
Adolescents
Weight Maintenance
BMI95th Percentile
Mild complication=hypertension, dyslipidemia, increased liver enzymes, and insulin resistance
Barlow and Dietz. Pediatrics 1998;102:e29.
Age 2–7 y: Weight Maintenance
Age >7 y: Weight Loss
Mild Complication
Yes
Mild Complication
No
BMI85th–94th Percentile
Mild Complication
No
Mild Complication
Yes
Age 2–7 y: Weight Maintenance
Age >7 y: Weight Loss
Weight Loss
Our Patient
• Enrolled in a 6 month randomized placebo-controlled trial of orlistat
• Lost 7 kg over first 3 months
• Lost 2 kg over months 3-6
• Regained all of his lost weight over the next 24 months