NUTRITION INFORMATION Sri Lanka

of 52
-
Upload
tarake-dharmawardene -
Category
Documents
-
view
228 -
download
0
Transcript of NUTRITION INFORMATION Sri Lanka
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
1/52
NUTRITION INFORMATION
SYSTEM IN SRI LANKA
Dr. Renuka Jayatissa
(M.B.B.S., M.Sc, MD)
Department of Nutrition
Medical Research Institute
Department of Health services
Sri Lanka
in collaboration with
WORLD BANK
2002
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
2/52
NIS/MRI
2
CONTENTS
Acknowledgements 3
Chapter 1: Introduction... 4
Chapter 2: Development of NIS.... 6
Chapter 3: Findings of the baseline information .. 15
Chapter 4: Establishment of NIS and use of information . 44
Chapter 5: References 49
Annex 1:
Annex 2:
51
52
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
3/52
NIS/MRI
3
ACKNOWLEDGEMENTS
I wish to thank WORLD BANK for providing the funds to conduct the study. Special mention must be
made of Dr. Amarasinghe, Co-ordinator, World Bank project for the speedy course of action taken to
release funds.
The members of the Technical Advisory Committee provided an invaluable service in planning the study.
I thank them.
I sincerely thank Dr. C.D. Gunaratne, Director Nutrition, Dept. of Health, Colombo, for all the support,
Prof. Lalani Rajapaksa, Department of Community Medicine, Faculty of Medicine, Colombo and Mrs.
Soma de Silva, UNICEF for providing their expertise in selecting the sample for the study and Prof.
Dulitha Fernando, Professor of Community Medicine, Faculty of Medicine, Colombo, assisted in the
preparation of the Report.
I am grateful to Dr.Gaya Colambage, Director, Medical Research Institute. She gave her best to make
the study a success.
Last, but foremost in mind are the pivotal operators: the Provincial Directors, Principals of the schools,
teachers, parents, and children. To one and all I wish to say am deeply indebted to you for having been
partners in the study.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
4/52
NIS/MRI
4
CHAPTER 1
INTRODUCTION
Sri Lanka is an island with a population of approximately 18.7 million. For purposes of administration, Sri
Lanka is divided into 8 Provinces, 25 Districts and 315 Divisional Secretary areas. The Eight Provincial
Directors of Health Services (PDHS) are totally responsible for management and effective
implementation of health services in the respective provinces. Deputy Provincial Directors of Health
Services (DPDHS) assist the eight PDHSs. DPDHS areas are similar to administrative districts, except
for Kilinochchi and Ampara district. Each DPDHS area is sub-divided into several Medical Officers of
Health areas (MOH/DDHS), which are congruent with administrative units, i.e. Divisional Secretariats.
The MOH/DDHS is responsible for the preventive and promotional health care in a defined area, with a
population ranging from 60,000 to 80,000 and has trained staff working at field level (Annual Health
Bulletin, 2000).
Though Sri Lanka has achieved considerable success in the reduction of mortality with increase in the life
expectancy, the load of morbidity that is present in the community has not been commensurate with the
decline in mortality. An important and persisting problem has been the significant level of malnutrition,
affecting particularly infants, children of the younger age groups and pregnant women. Though poverty
does influence levels of under nutrition, poverty alone does not explain the high prevalence of
underweight that persists in Sri Lanka. Educational and cultural factors are likely to play a significant role,
which in turn affect infant and child feeding practices and family attitudes towards nutrition in general
(Ministry of Health Highways and Social services, 1995).
Nutrition information system (NIS) is a system designed to monitor, on a continuous and regular basis,
the food and nutrition situation of a country. It will watch over nutrition in order to make decisions, which
will in turn lead to improvements in nutrition in the population. Sri Lanka is relatively rich in nutritionrelevant data that can be used to build nutrition information system. There is a lot of information collected
routinely in the health sector by different categories of staff and different agencies at different times.
However, it is important to find out what information is really needed to assess the nutritional problems in
the community and what information is related to causality. The micro level assessment of nutritional
factors are very important to counteract the action oriented cycle because the decisions can be taken at
community level by the information collectors themselves rather than waiting till the national interventions
arrived.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
5/52
NIS/MRI
5
The following elements exist at present as nutrition information;
Food balance sheet - Statistics Department Data on growth monitoring, - Health Data on health indicators (birth weight, disease pattern) - Health Maternal and child health data - Health
In addition to the above survey data are also available, e.g.,
Socio-economic survey data - Central Bank Demographic and health survey data - Department of Census and Statistics National Health survey - Ministry of Policy Planning Anaemia, Iodine, Vit A surveys - Medical Research Institute
This is an analysis to show how we can use the routinely collected information and survey data as an
action oriented basis. It will be useful to Health workers, Medical officers of Health, Deputy Provincial
Directors, Provincial Directors and Nationally, to assess the situation and the monitoring and evaluating
of interventions to eliminate the nutritional problems in the country. In turn, this type of exercise will help
to improve the accuracy and quality of routinely collected data. The objectives of the nutrition information
system are as follows:
General objectives:
1. To develop a Nutrition Information System (NIS) with minimal additional inputs.Specific objectives:
1. To assess the nutritional status using a life style approach;
children under 5 years school children adolescents adults pregnant women
2. To develop indicators relevant to nutritional problems3. To identify trends in nutritional status and analyse associated factors4. To make recommendations regarding activities that should be undertaken to established a
surveillance system at MOH, district and provincial level.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
6/52
NIS/MRI
6
CHAPTER 2
DEVELOPMENT OF NIS
It was decided to study the nutritional problems using a life style approach. The following steps were
adopted to collect information to develop the NIS, i.e.,
1. Identification of information to be included in the NIS2. Discussion with Experts3. Collection of available information4. Collection of information on children aged 5-14 years.
Figure 1
Conceptual Framework for the Causes of Malnutrition in Society
Outcomes
Immediate
causes
Underlying
Inadequate Education causes
Basic causes
Malnutrition and death
Inadequate dietary
intake
Disease
Inadequate
access to food
Insufficient healthservices and unhealthy
environment
Inadequate care formothers and children
Formal and non formal institutions
Political and ideolo ical su erstructure
Economic structure
Potential resources
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
7/52
NIS/MRI
7
2.1. Identification of information to be included in the NIS
Conceptual framework of the causes of malnutrition was used to facilitate the identification of data on
assessment and analysis of the determinants of malnutrition (UNICEF 1990). The framework is shown in
Figure 1. In this framework, casual factors and their interactions are shown at three mains societal levels-
immediate, underlying and basic.
The synergistic interaction between the two immediate causes, inadequate dietary intake and disease,
fuels a vicious cycle that accounts for much of the high morbidity and mortality. Three groups of
underlying factors contribute to inadequate dietary intake and infectious disease: household food
insecurity, inadequate maternal and childcare and poor health services, and an unhealthy environment.
These underlying causes are in turn underpinned by basic causes that relate to the amount, quality,
control and use of various resources (United Nation 1997). The following indicators were identified tocollect information on causal factors.
2.2. Discussion with Experts
Core-group was formulated with Public Health specialists, Academics and other specialists with nutrition
background (Annex-1). Series of discussion sessions were conducted to gather information. Major
nutritional problems in Sri Lanka were identified and the following areas were prioritised.
Low birth weight Protein energy malnutrition of children under 5 years and school children Iron deficiency anaemia throughout the life cycle Iodine deficiency among school children Vitamin A deficiency among children under five years
The following activities were identified under the design of the NIS.
development of indicators relevant to each nutrition problem to make decisions. needed data for selected information. sources of data,
administrative sources (data already being gathered routinely) household surveys
Responsibility of institutions.During the sessions of discussions the above activities were followed for the above-mentioned nutritional
problems as shown in Table 1.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
8/52
NIS/MRI
8
Table 1
Identification of nutritional problems, indicators, source of data and responsibilities of
institutions using a lifecycle approach
Problem Definition of indicator Source of data Responsibility
Children under five years1.Low BirthWeight
% of new-borns below 2500g Monthly data fromFHB by DDHS area(H-509)
Monthly returnsfrom hospital
Birth weightSurveillance
D/FHB
Director/MS/DMO/MOIC/RMO
D(FHB)/MRI
II. Stunting(6-59 months)
% of children below -2SD from themedian of the NCHS/WHO height
for age reference population
Special surveys andsurveillance at
every 5 years
Existing researchdata/DHS/MRI/
NHSIII.Underweight(under 5years)
% of children below -2SD from themedian of the NCHS/WHO weightfor age reference population
% of children under 5 years whoattended clinics and below the 3rdcentile
Special surveys andsurveillance atevery 5 years
Monthly data fromFHB by DDHS area(H-509)
Existingresearchdata/DHS/MRI/NHS
FHBIV. Wasting(under 5
years)
% of children below -2SD from themedian of the NCHS/WHO weight
for height reference population
Special surveys andsurveillance at
every 5 years
Existing researchdata/DHS/MRI/
NHS
Primary school childrenV. Stunting atSchool entry( year 1, 4)
% of children below -2SD from themedian of the NCHS/WHO heightfor age reference population
Monthly data fromFHB by DDHS area(school healthreturn)
Special surveys andsurveillance atevery 5 years
D/FHB
MRIVI. Wasting(year 1,4)
% of children below -2SD from themedian of the NCHS/WHO weightfor height reference population
Monthly data fromFHB by DDHS area(school healthreturn)
Special surveys andsurveillance atevery 5 years
D/FHB
MRIVII.Overweight(year 1,4)
% of children above +2SD fromthe median of the NCHS/WHOweight for height referencepopulation
Monthly data fromFHB by DDHS area(school healthreturn)
D/FHB
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
9/52
NIS/MRI
9
Special surveys andsurveillance atevery 5 years
MRI
AdolescentsVIII. Thinness
in adolescents(year 7)
% of adolescents below the 5th
percentile from the referencepopulation for under nutrition forBMI for age
Monthly data fromFHB by DDHS area(school healthreturn)
Special surveys andsurveillance atevery 5 years
D/FHB
MRI
IX. Overweightin adolescents
(year 7)
% of adolescents at and above85th percentile from the reference
population for BMI for age
Monthly data fromFHB by DDHS area
(school healthreturn)
Special surveys andsurveillance atevery 5 years
D/FHB
MRI
Pregnant womenX.Underweight
% of pregnant women below 18.5of BMI at first trimester
Monthly data fromFHB by DDHS area
(H-509 return) Special surveys and
surveillance atevery 5 years
D/FHB
MRIXI. Weightgain inpregnancy
% of pregnant women with weightgain during the pregnancy
Monthly data fromFHB by DDHS area(H-509 returns to beincluded)
Special surveys andsurveillance atevery 5 years
D/FHB
MRI AdultsXII. Dietrelated chronicdegenerativediseases
Rates of morbidity and mortality ofchronic degenerative diseases:cardiovascular disease, diabetes,obesity, some cancers:comparison with some infectiousdisease rates
Hospital data fromhealth bulletin
D/information
XIII.Underweight
% of adults below the 18.5 BMI Special surveysandsurveillance atevery 5 years
MRI
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
10/52
NIS/MRI
10
XIV.Overweight
% of adults above the 24.9 of BMI Special surveysandsurveillance atevery 5 years
MRI
XV. Changingdietary
patterns
1. Food availability by food groupsin the country.
2. Per capita daily energy intakefor selected food items by sector3. Contribution of each foodgroups to the overall calorie intakewith income
Food balancesheet
Socio-economicsurvey Socio-economic
survey
Censusand
statistics Central
Bank
CentralBank
Micro nutrient deficienciesXVI. Anaemia % of children with haemoglobin
below the cut-off value. Special surveys
andsurveillance atevery 5 years
MRI
XVII. Vitamin Adeficiency
% of children with the prevalenceof serum retinal mol/LMild =>0-=10-=20
Special surveysandsurveillance atevery 5 years
MRI
XVII.Iodinedeficiency-
1. % of children of 6-12 years ofage with urine iodine levels
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
11/52
NIS/MRI
11
infectious disease rates Health Bulletin MOHHouseholdfood security
dietary energy supply; food intake relative to need, Percent below poverty line,
Socio-economicsurvey
CentralBank
Inadequatematernal andchild care
Breast feeding (duration andpercentage);
Mean age of introduction ofcomplementary foods;
Usage of oral RehydrationFluids (ORT)
Health Bulletin/ H-509
Special surveys andsurveillance atevery 5 years
H-509
MOH/FHB
MRI
FHBAccess tobasic health
services
Coverage of measlesvaccination,
Births attended by a trainedhealth staff,
H-509
H-509
FHB
FHB
Healthyenvironment
Availability of clean water, Availability of sanitary latrines
PHI sanitationrecord
PHI sanitationrecord
D/Environment/MOH
The identified indicators to assess nutritional problems, source of data and responsibilities of the
collection of data were finalised with Experts. Since information regarding to children less than 5 years is
available at the moment, it was decided to use secondary data as baseline information. To carry out the
school based study to collect information on children aged 5-18 years due to the importance of problems
in that group and lack of current data.
2.3. Collection of available information
Information was collected with regard to each indicator by identified data sources and literature review,
including reviews of "grey" or unpublished literature and by interview with key informants. Due to the
methodology adopted in the Demographic Health Survey (DHS), it was not possible to identify the
prevalence of nutritional problems and the determinants by districts or provinces. Therefore other
available studies were used.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
12/52
NIS/MRI
12
The following data was available (routine and survey data):
Children under 5 years Adults Micro nutrient deficiencies Causes of malnutrition under 5 years
Following information is not available:
Primary school children Adolescence Pregnant women
Therefore simple method was adopted to collect information on primary school children and adolescence
at school level.
2.4. Collection of information on children aged 5-14 years
Information was collected cross-sectionaly in 7 districts of the country due to logistic reasons. The
districts were selected by considering the following factors:
High and low prevalence of stunting and wasting of children under 5 years for last 20 years Prevalence of stunting/ wasting/ underweight has not been changed much during the last 20
years.
Prevalence of Vitamin A deficiency in the area Prevalence of anaemia in the area Deficiency of iodine in the area Presence of representative data by district and Province.
The following districts were selected.
Anuradhapura, Polonnaruwa, Badulla, Moneragala, Colombo, Hambantota, Kurunagala.
2.4.1. Data collection
Data were collected among school children aged 5-14 years because 90% of children belonged to the
particular age group could easily met in the schools. The required sample size for each district was
calculated on the basis of the prevalence of underweight among children less than 5 years. This was 800
children from 5-14 year old age group giving a total sample size of 5600 for all 7 districts. The schools
were selected from a list of all schools in Sri Lanka that was provided by the Department of Education. A
multi-stage stratified sampling technique was used to identify the sample. During the first stage the
proportionate stratification was done to identify the number of schools in the urban and rural areas in
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
13/52
NIS/MRI
13
each district according to the population of children in selected age group. In the second stage, types of
schools were considered. During the third stage, required number of schools was identified using
population proportion to sampling technique. During the fourth stage of sampling, all classes of grade 1, 4
and 7 were listed out and one class from each grade was randomly selected from each school. Grade 1,4
and 7 was selected to study by considering the school health programme in the country to adopt that
data into the NIS in the future. All the children in each selected class were included in the assessment
nutritional status.
The following information was obtained:
1. Basic information: birthday and sex and other identifying information2. Biochemical assessment for anaemia3.
Measurement of height and weight
2.4.1.1. Basic information
All children in selected classes who had obtained the consent of their parents and were present on the
day of the study were identified as participants. A structured format was developed to obtain identification
data, age and sex of children in the selected classes. The information was obtained from the attendance
register and marked on the format by a member of the study team.
2.4.2.2. Biochemical assessment for anaemia
Sample of capillary blood for estimating haemoglobin was obtained from 10 children, selected at random
from each selected class (grade 1,4 and 7) in each school. Haemoglobin was assessed by Haemocue
method. A total of 30 haemoglobin from each school was estimated. The following procedure was used
to detect anaemia by using HaemoCue method: A finger-pricked drop of capillary blood was taken by
using a disposable lancet. The function of the HaemoCue photometer was checked on a daily basis by
measuring the control cuvette.
2.4.2.3. Measurement for height and weight
All the children in selected classes were measured for height and weight. Measurements were taken by
the field investigators who had been trained and standardised before the study. Height was recorded to
the nearest centimetre by using anthropometrics rod. The children were weighed with the use of an
electronic balance to the nearest 0.01kg after they removed their shoes and socks. The observer
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
14/52
NIS/MRI
14
variation was assessed by duplicating the measurement by the same observer and repeating the 10% by
the best investigator.
2.3.2. Field level activities
The field investigators, all of whom have previous experience in field research activities, were responsible
for all components of the study (Annex-2). Investigators were trained in testing the capillary blood
samples for haemoglobin content. All selected schools were informed about the study. The consent
forms were distributed to all children in the selected classes prior to the study to obtain the consent of the
parents/guardians. The schools were informed of the date of the visit. All fieldwork was completed during
a 6-month period, November 2001 - April 2002.
2.3.3. Collection of data in Colombo district:Five schools from urban sector were covered by the study team. Rural sector schools were not studied
due to the school vacation.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
15/52
NIS/MRI
15
CHAPTER 3
Findings of the baseline information
A nutrition information system requires; correct assessment of the problem; an appropriate analysis of
the causes of the problem on a provincial or district basis; and the resources available to combat theproblem. Based on these causes of the problems and the resource analysis, action would then be taken
and the results, including the achievements of a particular desirable outcome, measured. This would in
turn provide an opportunity for further analysis and better action to improve the nutrition situation -"Triple
A cycle" (Asian Development Bank 1999).
3.1. Assessment of the problem
The results are presented according to the following order by considering the lifecycle approach: low birth
weight, protein energy malnutrition (PEM) of children under 5 years, nutritional problems among school
children, nutritional problems among adults, Vitamin A deficiency, iodine deficiency. This section includes
a presentation of prevalence and trends of the nutritional status.
3.1.1. LOW BIRTH WEIGHT
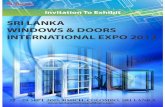
Most children are born with low birth weight and become increasingly malnourished. Figure 2 shows that
the highest low birth weight is in the Central Province and then in Uva Province. The lowest is in Western
Province. But it had declined in all the Provinces.
Figure 3 and 4 shows the geographical distribution of the prevalence of low birth weight. Annual health
bulletin provides the registrar General's data, which are originally taken from hospital statistics and not
validated, for districts. Therefore this data should be interpreted cautiously. WHO (1995) recommended,
Figure 2
Trends in prev alence of Low Birth Weight in Provi
of Sri Lanka, 1975-2000(Source: Annual Health Bulletin 1984-2000, Ministry
of Poli cy planning 1988/89)
0
10
20
30
40
50
60
70
80
1984 1988-89 1991 1992 1993 2000Year
%
Central
North central
Sabaragamuwa
Uva
Southern
North Western
Western
Eastern
Nothern
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
16/52
NIS/MRI
16
prevalence of >15% of LBW as the cut-off for triggering public health action. Therefore the arbitrary cut-
offs were used as =20% as low, moderate, high and very high prevalence of
LBW in the population. The very high prevalence was detected in NuwaraEliya, Badulla, Monaragala and
Batticaloe districts. Almost all the districts show the prevalence higher than 10%. When the data was
compared with the 1988/89, an improvement was detected in some districts like Polonnaruwa, Matale,
and Puttulum etc.
Figure 3 and 4
Prevalence of low birth weight by district, 1988-2000
(Source: Ministry of policy planning 1988/89 and Annual health bulletin 2000)
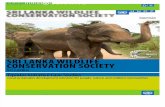
3.1.2. PROTEIN ENERGY MALNUTRITION OF CHILDREN UNDER 5 YEARS
Figure 5
Child malnutrition (0-4.99 years)
in Sri Lanka, 1975-2000
0
10
20
30
40
50
60
70
1975-76
1977-78
1980-82
1987
1993
1995-96
2000
Year
Percentagebelow
median
(-2SD)
Underweight
Stunting
Wasting
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
17/52
NIS/MRI
17
As shown in Figure 5, stunting among Sri Lankan children has improved from 49.9% to 13.5% since 1975
but wasting has not improved during this period, i.e. 13.9% to 14%. Though the underweight is a complex
index to interpret it has also declined from 57.3% to 29.4%.
There are wide variations in the prevalence of stunting and wasting among the different Provinces in Sri
Lanka, the Uva Province having the highest rate of stunting and the Western Province having the lowest.
But all the Provinces have shown a marked improvement (Figure 6). Wasting among children has
increased in Sabaragamuwa Province. But in all other Provinces it has gone up in 1988/89 and come
down to the 1980-82 level in 1995. There has been no improvement at all in the North Western Province
since 1980 (Figure 7).
Figure 7
Trends in prevalence of Child wasting (0-4.99 years) in
Provinces of Sri Lanka, 1980-2000
0
5
10
15
20
25
1980-82 1988-89 1995 Year
Percen
tage
be
lowme
dian
(-2SD)
Central
North central
Sabaragamuwa
Uva
Southern
North Western
Western
Figure 6
Trends in prevalence of Child stunting (0-4.99 years) in
Provinces of Sri Lanka, 1980-1995(Source:Ministry of policy planning 1980/2,1988/9 and MRI 1998
0
10
20
30
40
50
60
1980-82 1988-89 1995 Year
Percen
tage
be
low
me
dian
(-2SD)
Central
North central
Sabaragamuwa
Uva
Southern
North Western
Western
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
18/52
NIS/MRI
18
Figure 8 and 9
Prevalence of stunting among children less than 5 years by district, 1987-2001
(Source: Ministry of policy planning 1988/89 and MRI 2001-unpublished )
The prevalence of wasting and stunting by districts were mapped out to assess the problem at micro
level. The degree of stunting and wasting was classified as low, moderate, high and very high to assess
the severity of malnutrition in the provinces and districts (the classification currently used by WHO Global
database was taken). As the district data is not available after the year 1988/89 the unpublished data on
the anaemia status survey report was analysed by district to be used but this data are not representative
of district. Therefore this information should be interpreted cautiously. It is interesting to note that the
level of stunting ranges from low to high and that very high level of stunting is not detected at present.
NuwaraEliya district still shows a high level of stunting. The reason may be due to the fact that in this
district whose population consists of estate workers, infrastructure is lacking when compared to other
districts. Kandy, Badulla and Monaragala districts have a moderate degree of stunting and the rest of the
districts have a low degree of stunting. When these findings are compared with 1988/89 data, it shows a
tremendous improvement.
However, the geographical distribution of stunting and low birth weights by districts are compared (Figure
4 and 9), it showed somewhat similar distribution. Low birth rate may be a causal factor for the stunting.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
19/52
NIS/MRI
19
Figure 10 and 11
Prevalence of wasting among children less than 5 years by district, 1987-2001 (Source: Ministry of
policy planning 1988/89 and MRI 2001-unpublished)
In 1988/9, most of the districts had a very high level of wasting except in 5 districts. At present there is a
marked improvement and only 6 districts still maintain a very high level of wasting. Gampaha district has
changed from a high degree of wasting to medium degree of wasting and Matale district has changed
from very high level to a low level of wasting during the last 13 years (this observation may be related to
low sample size in Matale district in 2001). Though the national level of wasting has not got changed, the
district level improvements are remarkable. At present, more concentration should be focussed on the
districts, which still maintain very high levels of wasting, i.e., Kurunagala, Anuradhapura, Polonnaruwa,
Kandy, Monaragala and Hambantota.
3.1.3. NUTRITIONAL PROBLEMS AMONG SCHOOL CHILDREN
The data were collected from 7687 school children in 7 districts. Two age groups were identified and
classified into groups, primary school children (5-9.9 years) and adolescents (10-14.9 years). Number
of children in each age group was 4876 (63.4%) and 2811 (36.6%).
3.1.3.1. UNDER NUTRITION
I. Primary school children
The nutritional status was assessed by calculating the wasting and stunting of children aged 5-9.9
years and it was graded according to WHO classification and shown in the Figure 12 and 13 to illustrate
the geographical distribution.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
20/52
NIS/MRI
20
Figure 12 and 13
Prevalence of stunting and wasting among school children aged 5-9.9 yearsby districts, 2002
Badulla district has moderate degree of stunting and it is the highest rate reported in this school study.
All the other districts surveyed have mild degree of stunting. These findings are comparative with the
stunting rates among children under 5 years of age except in Monaragala district, which showed a
moderate degree of stunting prevalence among children less than 5 years (Figure 12). In that case it is
interesting to note that there is an improvement of stunting from pre-school to school children in
Monaragala district.
Figure 13 shows the wasting prevalence in the surveyed districts. A very high grade of wasting has
been found in Kurunagala, Monaragala and Hambantota districts according to the population
prevalence. All the other districts, which were studied, also have a high degree of wasting. A similar
pattern is observed when we compare this with the wasting prevalence among children less than 5
years. In Anuradhapura district of course, there is a difference. There is a shifting from very high
prevalence to high prevalence from pre-school to school (Figure 11).
II. Adolescents
When NCHS/WHO reference was applied to classify the under nutrition and over nutrition among
adolescents, 44.7% and 84.0% of records in the studied population was flagged at the age of 10 years
and 11 years respectively. Therefore the BMI-for-age-sex was taken as a reference and thinness was
calculated by districts and shown in Figure 14.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
21/52
NIS/MRI
21
Figure 14Prevalence of thinness among schoolchildren aged 10-14.9 years by district, 2002
The proportion of the population with thinness was
classified by WHO (1995) as low, medium, high and
very high prevalence to classify the severity of the
thinness. It would also define a public health
problem and this classification is closely linked to
available resources for correcting problems, the
stability of the environment and government
priorities (Figure 14). Hambantota district has
shown a very high level of thinness and all the other
districts studied have indicated high level. It isinteresting to note that this observation is
comparative with the pattern observed among
primary school children except in Monaragala and Kurunagala districts. In these districts there is an
improvement from very high level to high level from primary school to adolescents. This finding
indicates that when children are close, at, or passing the growth spurt they have caught up the growth.
3.1.3.2. OVER NUTRITION
I. Primary school children and adolescents
Primary school children whose Wt/Ht is >2SD in the NCHS/WHO reference and the adolescents whose
BMI>=85th percentile in WHO 1995 reference, was classified as overweight children. Geographical
distribution is shown in Figure 15 and 16. The proportion of the school children with overweight was
classified by taking arbitrary cut-off points to reflect the distribution of overweight among children as
shown in Figure 15 and 16 (low, medium, high and very high prevalence). In this study it was found
that there is low prevalence in all the districts studied except in Colombo district. Figure 16 shows the
increasing pattern among adolescents. Colombo district has a very high level of overweight prevalence
among adolescents children. But it showed a medium prevalence with primary schoolchildren. Even
the Badulla and Polonnaruwa districts have increasing trends from low to high prevalence. This is a
situation to be aware of with the decreasing trend of under nutrition in the country.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
22/52
NIS/MRI
22
Figure 15 and 16Prevalence of overweight among schoolchildren aged 5-9.9 years and 10-14.9 years
by district in year 2002
3.1.3.3. ANAEMIA
Anaemia was assessed by measuring haemoglobin levels of school children. Total number of children
tested for anaemia was 1448 and 766 from primary school children and adolescents respectively. Age
dependent haemoglobin levels were taken to detect anaemia by adjusting the altitude. The proportion of
the school children with anaemia was classified by taking WHO cut-off points to reflect the distribution of
anaemia among children as shown in Figure 17 and 18 (low, medium, high and very high prevalence).
Figure 17 and 18Prevalence of anaemia among schoolchildren aged 5-9.9 years and 10-14.9 years
by district in year 2002
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
23/52
NIS/MRI
23
Very high levels of anaemia were not seen in any district. A high degree of anaemia has been shown in
Anuradhpura and Kurunagala districts. Thalasaemia is more prevalent in these districts. When it comes
to the adolescent group Colombo district has a low level of anaemia and other districts have a medium
level of anaemia prevalence.
3.1.4. NUTRITIONAL PROBLEMS AMONG ADULTS
3.1.4.1. Diet related chronic degenerative diseases among adults
The most prominent chronic degenerative diseases - cardiovascular disease, cancer and diabetes
mellitus - are linked by unhealthy diet and physical inactivity. Actions to prevent these diseases should,
therefore, focus on controlling the risk factors in an integrated manner. Therefore the disease pattern and
causal factors are analysed under selected indicators.
3.1.4.1.i. Morbidity and mortality rates among major chronic degenerative diseases
There is an upward trend of Diabetes Mellitus, Hypertension and Ischaemic Heart disease among
hospital admissions and in contrast to that there is a downward trend in helminthiasis and vitamin
deficiencies and intestinal infections (Figure 19). This pattern clearly shows the double burden of
diseases in Sri Lanka. At one end diseases related to poverty and at the other end diseases due to
prosperity.
Figure 19Trends in Hospitalisation of selected disease
in Sri Lanka, 1975-2000( Source:Health bulletin 2000 )
0
200
400
600
800
1000
1200
1975 1980 1985 1990 1995 2000 Year
Casesper100,0
0
population
Intestinalinfec dis
Helminthiasis
Nutr. Defi.
Diabetes
Hypertension
IHD
(Exclude: Jaffna, Kilinochchi, Mullativu and Ampara Districts)
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
24/52
NIS/MRI
24
3.1.4.1.ii. Changing dietary patterns
The eating habits of people are changing. More people are eating out more frequently or eating foods
that are not nutritionally balanced. They are consuming more of animal fats, sugar and fried foods and
less of fresh fruits and vegetables (WHO 2001).
Food availability in Sri Lanka since last two decades clearly shows this changing pattern (Figure 20). The
availability is directly related to the consumption pattern of the population. The oils, fats, sugar and meat
availability has increased in contrast to the decreased trend of the availability of pulses, nuts. Vegetable
and fruit availability has not changed much during this period.
Figure 20
Changes in percapita availability of foo
(gms/day) in Sri Lanka, 1982-1999(Source: Food balance sheets 1982-1999)
0
100
200
300
400
500
600
700
800
900
1000
1982 1984 1991 1995 1997 1999 Year
Gms
/day
Oils & Fats
Milk
Fish
Eggs
Meat
Fruits
Vegetables
Pulses & Nuts
Sugar
Roots & TubersCereals
Figure 21
Contribution from urban, rural and estate sect
(% of deaths) from diseases of the circulator
system in 1991 in males and females(Source:Cardiovascular research in Sri Lanka 1998)
0
20
40
60
80
Urban Rural Estate Sector
%
Male
Female
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
25/52
NIS/MRI
25
The mortality rates due to diseases of the circulatory system by sector suggest a higher mortality rate
among urban population than among rural and estate population (Figure 21). When we compare this
finding with per capita daily energy intake for selected food items, it shows that the urban population
consumes more animal food like meat, fish, sugar and milk than rural and estate population (Figure 22).
Coconut consumption is highest among rural population. This findings support the study carried out
among Polynesian islanders who obtain 34-63% of their food energy from coconut and found vascular
diseases uncommon among them (Prior 1981). Though the vegetable is grown in the estate sector, the
vegetable consumption is lowest among the estate population.
Figure 23
Components of diet in re lation to income deci
of spending units(Source: Consumer finance and socio economic survey 1996-97)
0%
20%
40%
60%
80%
100%
1 2 3 4 5 6 7 8 910
Income deciles of spending units
%
ofenergy
Others
Carbohydrate
Animal Fat
Vegetable Fat
Figure 22
Per capita daily energy consumption of select
food items by sector(Source: Socio-economic finance sur vey 1996/97)
0%
20%
40%
60%
80%
100%
Urban Rural Estate Sector
%o
fenergy
Others
Vegetable
Meat,Fish,Milk
Sugar
Coconut
Wheat Flour andBread
Rice
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
26/52
NIS/MRI
26
When the contribution of each food group to the overall calorie intake with rising income shows a
marked variation (Figure 23). The spending units at the upper income deciles derived higher proportion
of animal fat compared to others. In contrast, the lower deciles derived more energy from vegetable fat.
Rice, bread and wheat flour accounted for the highest proportion of energy derived for all groups.
3.1.4.2. Overweight and obesity
Inactive life is attributed to high body mass index (BMI) and the high rate of overweight and obesity in
the society. The changing pattern of prevalence of overweight among males and females in different
age groups in urban areas is illustrated in Figure 24. Though the study methodologies were not
comparative, it showed the high prevalence of overweight among females than males. The prevalence
of overweight is more among the 40-49 year age group. From then the reducing trend of overweight
has observed. This is an alarming situation when compared with the increasing trend of non-communicable diseases. This is one of the issues to be addressed urgently.
Figure 24
Prevalence of overwe ight and obesity among males
females, 1993-2001(Source: MRI, Lipid profile study 1993 & MRI 2002)
0
5
10
15
20
25
30
35
40
45
50
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 >=60
Age groups
%
Male overweight
2001 male overweight
Female overweight
2001 female overweight
Male obese
2001 male obesity
Female obesity
2001 female obesity
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
27/52
NIS/MRI
27
3.1.4.3. Underweight
Figure 25
Prevalence of underweight among adults over 40 years of age
in different populations, 2001 (Jayatissa 2002-unpublished,n=720)
The prevalence of underweight is also high among adults especially in the rural population. Figure 25
shows that the proportion of underweight is decreasing with the urbanisation. There are no existing
programmes to address this problem.
3.1.5. VITAMIN A DEFICIENCY STATUS (VAD)
The clinical signs of VAD include night blindness, Bitots spots, corneal xerosis and corneal scars orulcers. The prevalence of clinical deficiency is estimated by combining night blindness and eye
changes, primarily Bitots spot to form a total Xerophthalmia prevalence (United Nation 2001). Clinical
VAD assessed by eye deficiency (Xerophthalmia) is considered a public health problem at more than
1% prevalence (Asian Development Bank 1999).
The trend in clinical VAD prevalence was assessed in Sri Lanka from 1975 to 1996. It has reduced from
1.1% in 1975 to 0.3% in 1987 and 0.8% in 1995/96. It showed there is an improvement of clinical VAD.
The provincial estimates from previous surveys since 1975 was compared (Table 1).
The improving trend is apparent, except in the Western Province. When the provincial trends are taken
into consideration, we can see that the clinical VAD is a public health problem in the Southern and the
Sabaragamuwa Provinces in 1995, but not in the whole country. It is noted that the sub clinical VAD is
increasing. Sub clinical VAD is defined as the prevalence of serum retinol concentration below 0.70
mmol/l (20 g/dl) minus the percentage of individuals with clinical VAD (ACC/SCN paper No.19).
28.6
11.29.4
16.3
0
5
10
15
20
25
30
35
Rural
Office
wo
rkers
Semi-
urban
Total
Population categories
underweight%
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
28/52
NIS/MRI
28
Table 1
Vitamin A deficiency: prevalence trends in children (6-70) months since 1975
PROVINCE CLINICAL SUB CLINICAL
1975 1995 1975 1995
Western0.9 1 - 23.3
Central1 0.5 - 21.8
North Central0.7 0.5 - 56.8
Southern1.8 1.3 - 41
Northern0.6 _ - _
Eastern1 _ - _
North western0.7 0.3 - 46.0
Uva0.9 0.0 - 35.0
Sabaragamuwa2 1.8 - 49.5
SRI LANKA 1.1 0.8 3.9 32.5
Sri Lanka has initiated the supplementation with high-dose Vitamin A capsules in the year 2000, but the
reports are not available on capsule coverage. Though the clinical deficiency was low in North Central
Province, the sub clinical deficiency was higher. The Sabaragamuwa Province has shown both clinical
and sub clinical deficiency. All the Provinces have shown a severe sub clinical VAD.
The estimated prevalence of clinical VAD in 1995 is 0.95% in South Asia and the sub clinical deficiency
is around 10 20% (Asian Development Bank 1999). It is interesting to note that the sub clinical
deficiency in Sri Lanka is higher than the estimates.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
29/52
NIS/MRI
29
3.1.6. IODINE DEFICIENCY
Iodine deficiency control is being tackled in the country through salt iodisation, which is supported by
legislation. Three indicators were used to assess the magnitude of the problem and as the process
indicators, i.e. goitre rates among school children, median urinary iodine concentration among school
children and the percentage of households consumption of adequately iodised salt.
3.1.6.1. Goitre rates
The rate of goitres in school children aged 8-14 years is a convenient way to assess the iodine status of
a community. Figures 26 and 27 show the past and present distribution of goitre rates by districts. It
shows the decline of goitre rates in some districts and the increase in some districts namely
Anuradhapura and Polonnaruwa. But not a single district shows less than 5% of goitre rates, which is
the indicator to the elimination of iodine deficiency. The major cause for this is that the iodine content
varies very widely among manufacturers, wholesalers, and retailers and at household levels.
Figure 26 and 27
Prevalence of goitre by districts (Source: Fernando et al. 1989 and MRI 2001)
3.1.6.2. Median urinary iodine concentration
Figure 28 shows that the Badulla and Matara districts have mild iodine deficiency according to median
urinary iodine concentration, which indicates the most recent iodine nutritional status.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
30/52
NIS/MRI
30
Figure 28: Prevalence of median urinary iodine concentration by districts
Figure 29: Percentage of households used the adequately iodised salt by district
(Source: MRI 2001)
3.1.6.3. Household consumption of adequately iodised salt
The percentage of households that use the adequately iodised salt is only below 50% in Badulla and 50 -
69% in Matara (Figure 29). This may be the cause of mild iodine deficiency in these districts. In the
districts, which have shown more than the adequate level in urine the percentage of households, which
use iodised salt, are less than 50% except in Polonnaruwa district. This may be due to high level of
mineral content in drinking water.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
31/52
NIS/MRI
31
3.2. Appropriate analysis of the causes of the problem by provinces or districts
The results are presented only with the causes of protein energy malnutrition (PEM) of children less than
5 years. It includes the appropriate analysis of description of the causes of malnutrition.
3.2.1. CAUSESOFPROTEINENERGYMALNUTRITIONOFCHILDRENUNDER5YEARS
Conceptual framework of the causes of malnutrition was used to facilitate the assessment and analysis of
the causes of malnutrition (Figure 1). In this framework, casual factors and their interactions are shown at
three main societal levels-immediate, underlying and basic.
3.2.1.i. Immediate causes
The immediate causes of malnutrition are the inadequate dietary intake and disease.
3.2.1.i.a. Dietary intake: dietary energy consumption,
This was used as an indicator to assess the dietary intake of the population. National data on dietary
energy consumption by the sector is presented in Figure 30. Estate sector showed the highest intake of
energy but the activity levels are very high among them due to the nature of manual work involved.
However, the energy level has not reached the Recommended Dietary Allowances (RDA) of active male.
Rural sector has shown an improvement of energy intake from 1969-1997. Literature suggests that when
there is an inadequate dietary intake, it is not only the intake of energy and protein, which is low, but also
the intake of some micronutrients.
Figure 30
Trends in pe rcaput dietary energy consumptio
sector, 1969-97(source: Central Bank, 1998)
1500
1700
1900
2100
2300
2500
2700
2900
3100
3300
3500
1969/70 1978/79 1981/82 1996/97
Year
Kcal
URBAN
RURAL
ESTATE
RDA(sedentary male)
RDA(active male)
RDA (sedentaryfemale)
RDA (active female)
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
32/52
NIS/MRI
32
3.2.1.i.b. Diseases:
Diarrhoea and Acute Respiratory Infection (ARI) contribute significantly to the high prevalence of PEM.
There is an important relationship between infections and dietary intake. Therefore the following
indicators were assessed to determine the relationship.
infectious disease rates - Figure 31,
The infectious disease rate was assessed by using the hospital data on national basis because the
reliable district data was not available. The districts, which have major hospitals, have higher rates of
cases because the data provided by the hospital indoor morbidity mortality register is not validated
according to the residence. However, Figure 31 clearly showed that there is a decreasing trend in
hospital admissions with infectious diseases and that admissions due to nutritional deficiencies and
helminthiasis are negligible.
3.2.1.ii. Underlying causes
Household food insecurity, inadequate caring practices and inadequate access to basic health services,
together with an unhealthy environment, are the underlying causes of inadequate dietary intake and
diseases and consequently of malnutrition.
3.2.1.ii.a. Household food insecurity
This was assessed by per-capita food availability (measured in total energy) in the country as shown in
Figure 32. Per capita food availability has not got changed much during last 20 years. But the availability
of animal foods has increased a little during this period.
Figure 31
Trends in Hospitalisation of infectious disea
in Sri Lanka, 1975-2000
( Source: Annual Health Bulletin,2000)
0
100
200
300
400
500
600
700
800
900
1000
1975 1980 1985 1990 1995 2000
Year
Casesper
100
,000
popu
lation Intestinal infec
dis
Helminthiasis
Nutr. Defi.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
33/52
NIS/MRI
33
Figure 32Change in per-captia food availability (in total energy) in Sri Lanka, 1982-1999
(Source: Sri Lanka food balance sheet 1982-1999)
Two other indicators were identified to analyse the household food insecurity, i.e., the percentage of poor
household and average per capita calories consumption for poor households. The geographical
distribution was also analysed (Figure 33 and 34).
Figure 33 and 34
Percentage of poor households by district and average per capita calories consumption for poor
households by district
(Source: Consumer Finance Survey 1999, statistical abstract, 2000)
Note: Those households spending more than 50%, of the expenditure on food and adult equivalent food expenditure is less
than Rs. 743 per adult per month (excluding non-food) are considered as poor households.
More than 40% of the population were categorised as poor households in Matale, Monaragala and
Ratnapura districts. It is interesting to note that the per capita calorie intake of the poor in these districts
0
500
1000
1500
2000
2500
1982 1984 1995 1997 1999
Year
C
alor
ies
/day
Vegetable
Animal
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
34/52
NIS/MRI
34
is between 1600-1699 except in Monaragala district. This calorie intake is not at all adequate for very
active manual workers who live in these districts. It is interesting to note that in the Colombo district the
per capita calorie intake is between 1500-1599 calories (the lowest intake reported in the country) in spite
of only less than 10% of the population being considered poor.
3.2.1.ii.b. Adequate care for children and mother
Caring practices constitute the most neglected determinant of young child malnutrition, but it is the least
satisfactory condition at present. Caring practices can be divided into four major components: (United
Nation 1997)
- Feeding practices, including breast-feeding and complementary feeding practices.- Hygiene practices, including personal, food and household hygiene.-
Home based health care, including ORT, early detection of illness and health seekingbehaviour.
- Psycological practices, including early childhood stimulation.The National data on exclusively breast-feeding pattern shows the proportion for infants in the age group
of (5-11) months was 55% in 2000. Seventy-five percents of mothers have provided their infants below
four months with only breast-feeding and 90% of children are breast-fed for more than one year.
However, the district data varies a lot (DHS 2001). In Sri Lanka, 60% of children of 4-6 months aged
were introduced complementary foods in 1994. But the data related to the quantity, quality and frequency
are also equally important and the data are lacking.
Very few localised studies were carried out about hygiene practices. Both households and personal
hygiene are very important aspects of care. This may be one explanation of the big difference in
malnutrition between districts.
The indicator to assess the home-based care is use of Oral Rehydration Therapy (ORT) by mothers. This
information is collected by the Public Health Midwife.
The above information related to caring practices were not available by district it was decided to assess
the situation by taking an indirect indicator as shown below.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
35/52
NIS/MRI
35
I. Child and maternal mortality rates
Figure 35 shows that the child and maternal mortality rates had declined since 1945. At present it is at a
minimum level. Therefore the geographical distribution was assessed to detect the micro level problem.
Figure 36 and 37
Infant Mortality Rate (IMR) per 1000 live births by district from 1988-1997
(Source: Registrar General's Data from Statistical Abstract 2000)
Figure 35
Infant mortality (IMR), Neonatal mortality rate (N
and M aternal mortality rate (MMR) in Sri Lanka,1
2000(Source:Registrar general department, Annual health bull etin 1999)
0
20
40
60
80
100
120
140
160
180
1945
1950
1955
1960
1965
1970
1975
1980
1985
1990
1995
1997
Year
per
live
births
NMRIMRMMR
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
36/52
NIS/MRI
36
Figure 38 and 39
Maternal Mortality Rate (MMR) per 10,000 live births by district from 1988-1996
(Source: Registrar General's Data from statistical abstract 2000)
Figure 36, 37, 38 and 39 show the infant mortality rate and maternal mortality rate respectively. IMR is
higher in Rathnapura, Nuwaraeliya, Kandy, Badulla, Anuradhapura, Mullativ and Kilinochchi than in other
district. MMR is highest among the Ampara, Mullative and Kilinochchi districts, which are war torn areas.
3.2.1.ii.c. Access to basic health services and a healthy environment
These are underlying determinants of young child malnutrition. Coverage of measles immunisation and
percentage of births attended to by a trained health staff are two indicators of the access to basic health
services.
I. Access to basic health services
In Sri Lanka the percentage of births attended to by a trained health staff is almost 99%. Figure 39 and
40 shows the coverage of measles immunisation in 1995-2000. The immunisation was initiated in 1985
and the coverage is above 95% in most of the districts. But Kandy district has a low coverage, which is
below 85%. While Vavuniya district, which is an area ravaged by war has a level about 80-89%.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
37/52
NIS/MRI
37
Figure 40
Measles immunisation coverage by districts from 1995-2000
Coverage of measles immunisation and percentage
of births attended to by a trained health staff showed
the sufficient level of basic health services in all the
districts of Sri Lanka. However, these data do not
show anything about the quality of services provided.
II. Healthy environment
availability of clean water, availability of sanitary latrines
Figure 41, 42, 43 and 44
Availability of safe drinking water and adequate sanitary latrines by districts from 1981-2000
(Source: Census of population and housing 1981 from Annual Health Bulletin 1994-2000)
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
38/52
NIS/MRI
38
The data on water and sanitation are shown in Figure 41, 42, 43 and 44. While access to water has
improved significantly since 1981, access to sanitary facilities is still very low.
3.2.1.iii. Basic causes
Education and information are crucial in determining how resources are used.
3.2.1.iii.a. Literacy rate
Sri Lanka has a very high rate of literacy as shown in Figure 45. There is no significant difference
between male and female literacy.
Figure 45
Literacy rate by sex in Sri Lanka from 1881-1996/7(Source: Annual Health Bulletin 1999, North and East not include
0
10
20
30
40
50
60
70
80
90
100
1881
1891
1901
1911
1921
1946
1953
1963
1971
1981
1994
1996/97
Year
%
Male
Female
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
39/52
NIS/MRI
39
Educational attainment is shown in Figure 46. About 40% attained education up to primary level in Uva,
North Central and Central provinces. About 30-35% have received an education up to secondary level
except in Western Province. This is also an important determinant during the nutrition education.
Figure 46
Educational attainment by Provinces 1996/97(Source: Central Bank of Sri Lanka 1996/97)
0
5
10
15
20
25
30
35
40
45
Weste
rnNW
P
South
ern NCP
Sabara
gamuw
aCe
ntral Uv
a
Provinces
%
No schooling
PrimarySecondary
Tertiary
3.2.1.iii.b. Maternal education
Female literacy is now widely recognised to be an important determinant of the health of the Nation.
Female literacy is lowest in the Uva Province and highest in the Western Province (Figure 48). Control of
resources at household level is as important as their availability in the household. In households, wherewomen control more resources, therefore the female education is an important determinant of child
malnutrition.
Figure 48
Literacy rate by sex by Provinces 1996/(Source: Central Bank of Sri Lanka 1996/97)
75
80
85
90
95
100
Weste
rnNW
P
South
ern NCP
Sabar
agamuwa
Centr
al Uva
Provinces
%
Male
Female
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
40/52
NIS/MRI
40
3.3. Resources available to combat the problem
Resources are required to fulfil the necessary conditions of food, health and care. Both the availability
and control of resources are important. Resources can be divided into human, economic and
organisational resources. This section is not dealt due to limited logistics.
The summary of findings is tabulated in the Table 3.
Table3
Summary findings of the NIS
Group Problem Findings
Pre-school
children
Low Birth Weight It is still a public health problem in Sri Lanka. Highest
prevalence was detected in NuwaraEliya, Badulla,
Monaragala and Batticaloe district. High proportions ofestate workers are residing in these districts. The data
screening should be done at district level to get more
accurate information.
Stunting NuwaraEliya district still shows a high level of stunting.
Kandy, Badulla and Monaragala district have moderate
degree of stunting and rest of districts have low degree of
stunting.
Wasting Though national level of wasting has not got changed, the
district level improvements are remarkable. At present,
the more concentration should be focussed on the
districts, which still maintain the very high levels of
wasting, i.e., Kurunagala, Anuradhapura, Polonnaruwa,
Kandy, Monaragala and Hambantota.
Primary-school
children
Stunting Badulla district has moderate degree of stunting and it is
the highest rate reported. All the other districts surveyed
are having mild degree of stunting. This finding is
comparative with the stunting rates among children under
5 years of age except in Monaragala district.
Wasting Very high grade of wasting has found in Kurunagala,
Monaragala and Hambantota districts. All the other
districts, which were studied also having high degree of
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
41/52
NIS/MRI
41
wasting. Similar type of pattern is observed when
compared with the wasting prevalence among children
less than 5 years except in Anuradhapura district, which
shows the shifting from very high prevalence to high
prevalence from pre-school to school.
Adolescents Thinness Hambantota district has shown a very high level of
thinness. All the other districts studied were indicated
high level, which is comparative with the pattern observed
among primary school children except in Monaragala and
Kurunagala districts, which shows the improvement from
very high level to high level from primary school to
adolescents. This finding indicates when the childrenclose, at or passing the growth spurt that they had
catches up the growth.
Overweight The increasing pattern was observed among adolescents.
Colombo district has a very high level that is shifted from
medium to very high levels with primary schoolchildren.
Even the Badulla and Polonnaruwa districts have
increasing trends from low to high prevalence. This is the
situation to be aware and alert with the decreasing trend
of under nutrition in the country.
Adults Diet related chronic
degenerative diseases
There is an upward trend of Diabetes Mellitus,
Hypertension and Ischaemic Heart disease among
hospital admissions and contrast to that the downward
trends of helminthiasis and vitamin deficiencies and
intestinal infections.
Changing dietary
patterns
The oils, fats, sugar and meat availability has increased in
contrast to the decreased trend of the availability of the
pulses, nuts. Urban population consumes more animal
food like meat, fish and milk than rural and estate
population.
Overweight and
obesity
The high prevalence of overweight among females than
males. The prevalence of overweight is more among the
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
42/52
NIS/MRI
42
40-49 years age groups and then the reducing trend has
observed. This is an alarming situation when compared
with the increasing trend of non-communicable diseases.
This is one of the issues to be addressed urgently.
Underweight The prevalence of underweight is also high among adults
especially in the rural population. There are no existing
programmes to address this problem.
Vitamin A deficiency Sri Lanka has initiated the supplementation with high-
dose Vitamin A capsules in year 2000, but the reports are
not available on capsule coverage. Though the clinical
deficiency is low in North Central Province, the sub
clinical deficiency was higher. Sabaragamuwa Provincehas shown both clinical and sub clinical deficiency. All the
Provinces had shown a severe sub clinical VAD.
Iodine deficiency Sri Lanka has shown a tremendous improvement towards
the elimination of iodine deficiency through the salt
iodisation programme. Moderate degree of goitre
prevalence has detected in the country. The major cause
for this is that the iodine content varies very widely among
manufacturers, wholesalers, and retailers and at
household levels. Quality control and monitoring of salt
iodine levels are the priority. To reduce the level of iodine
in salt at household and production sites should be
concerned.
Causes of protein
energy malnutrition of
children under 5 years
1. Estate sector showed the highest intake of energy.However, the energy level has not reached the
Recommended Dietary Allowances (RDA) of active
male.
2. There is a decreasing trend in hospital admissionswith infectious diseases and the admissions due to
nutritional deficiencies and helminthiasis are
negligible.
3. Per capita food availability has not got changed much
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
43/52
NIS/MRI
43
during last 20 years. But the availability of animal
foods has increased a little during this period.
4. More than 40% of the population were categorised aspoor households in Matale, Monaragala and
Ratnapura districts.
5. Per capita calorie intake of the poor in these districtsis between 1600-1699 except in Monaragala district.
This calorie intake is not at all adequate for very
active manual workers who live in these districts.
6. In the Colombo district the per capita calorie intake isbetween 1500-1599 calories (the lowest intake
reported in the country) in spite of only less than 10%of the population being considered poor.
7. Data related to the quantity, quality and frequency ofcomplementary feeding is lacking.
8. While access to water has improved significantlysince 1981, access to sanitary facilities is still very
low.
9. Female literacy is lowest in the Uva Province andhighest in the Western Province.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
44/52
NIS/MRI
44
CHAPTER 4
Establishment of NIS and use of information
Mock and Mason stated in 1999, Nutrition information systems are an essential component of national
investment programmes aimed at reducing the incidence and prevalence of malnutrition in Asia (Asian
Development Bank 1999). The analysis presented in Chapter 3 uses the UNICEF conceptual framework
to develop the NIS across Provinces and districts and it explores relationships, especially between
immediate, underlying and basic causes and malnutrition.
The last 10-12 years data was used to develop this information system. This clearly shows that routinely
collected data can be used to gather information for following indicators:
Infants and preschool children: Low Birth Weight Underweight
School children Stunting (year 1, 4) Wasting (year 1,4) Overweight (year 1,4)
Adolescence Thinness (year 7) Overweight (year 7)
Pregnant women Underweight
Adults Diet related chronic degenerative diseases
Causes of malnutrition under 5 years Inadequate maternal and child care Access to basic health services Healthy environment
Sri Lanka has routine on-going data collection by the Public Health Midwives (PHM) and Public Health
Inspectors (PHI) and sends to the Medical Officer of Health (MOH) monthly or quarterly to compile. Data
related to the above indicators, which were used to build up the NIS could be collected from PHM or PHI
level. Some of the data are already collecting to use for Maternal and Child Health activities, i.e., Growth
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
45/52
NIS/MRI
45
monitoring data (number of under weight children), number of low birth weight children, number of infant
deaths, number of neonatal deaths, number of maternal deaths, breast feeding, measles immunisation
coverage, percentages of births attended by a trained health staff, safe drinking water, adequate sanitary
facilities etc. By building the NIS from these data will enhance the quality and use of routine data by the
data collectors themselves.
In general, the approaches should be explored to strengthen these data sources whereverpossible to join into the system.
Attempt should be made to obtain comparable data from other surveys and studies e.g. DHS In Sri Lanka
Demographic and Health Survey tend to collect detailed information on population and health, socio-
economic status and household food access etc. but it was designed to collect the information onEcological Zone basis. Therefore this information is not possible to use by Provincial or district's policy
makers. In addition to this survey income and expenditure survey is going on every 10 yearly by Central
Bank of Sri Lanka. Medical Research Institute has undertaken the nationally representative surveys on
Iodine, Anaemia and Vitamin A. National sample surveys are necessary to build up the Project's nutrition
information strategy, preferably within five-year intervals. Therefore NIS will help the comparability across
districts and Provinces quarterly or yearly.
Changing of methodological issues in DHS survey to collect data by Provinces. This can validatewith routinely collected information to facilitate accurate reporting. It is a big assert to the
decision makers.
Policymaking requires information that addresses causality, and that demonstrates the consequences of
various policy options to policymakers (Asian Development Bank 1999). Prevalence and causes of
malnutrition in districts varied. It is important to prioritise the causes accordingly. Then the interventions
varied from district to district. NIS will directly support to identify the priorities on district basis. Then it is
easy for policy makers to deviate from the common policies relevant to nutrition like food subsidies and
poverty alleviation programme. The following issues were highlighted in the analysis which can be used
during the policy decisions:
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
46/52
NIS/MRI
46
The universal availability of drinking water and sanitary toilets to all households should beensured because it was found lacking in most districts. It will help to reduce of malnutrition in
children linked with water-born infections.
Female education should be upgraded in Uva and Central province to facilitate the nutritioneducation and essential childcare support.
Since per capita calorie consumption is very low in poor households of Colombo district,targeting of nutrition interventions should be carried out to reach children from those households.
Associated problems like food security; caring practice data should be linked to the routineinformation collection by adding the identified indicators to the system.
Awareness should be created among urban sector people the high consumption of meat andsugar may relate to cardiovascular disease morbidity.
Screening of adult population after 40 years of aged is important due to increase overweightprevalence from 35 years and obesity since 55 years, this may be linked to well women clinic
with the concept of upgrading family health. This may be related to rising level of non-
communicable diseases.
The absence of data for evaluation of nutrition and community based programmes, is a major constraint
to the design of Provincial or district programmes. This is true in the area of under nutrition reduction, low
birth weight reduction, anaemia and care of young children. NIS will address this information gap, which
is a priority.
An important information tool, which is used in this NIS, is Geographical Information system. In Chapter
3, most of the information is mapped out by districts to detect the problem and determinants. Same
system can be extended to MOH and PHM areas because the maps and geographical boundaries are
already available. It can be done manually or if the resources are available by using the computer.
Programme planners, policy makers and Funding agents can use the mapping and analytical products
regularly for programme design and implementation.
Establishment of the NIS and the regular mapping of the prevalence of malnutrition at PHM, PHI,MOH, DPDHS and PDHS level should be done. Following indicators can be used at each level.
PHM level:
Infants and preschool children: Low Birth Weight
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
47/52
NIS/MRI
47
Underweight Pregnant women
Underweight Causes of malnutrition under 5 years
Inadequate maternal and child care Access to basic health services
PHI level:
School children Stunting (year 1, 4) Wasting (year 1,4) Overweight (year 1,4)
Adolescence Thinness (year 7) Overweight (year 7)
Causes of malnutrition under 5 years Healthy environment
MOH level:
Infants and preschool children:
Low Birth Weight Underweight
School children Stunting (year 1, 4) Wasting (year 1,4) Overweight (year 1,4)
Adolescence Thinness (year 7) Overweight (year 7)
Pregnant women Underweight
Causes of malnutrition under 5 years Inadequate maternal and child care Access to basic health services Healthy environment
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
48/52
NIS/MRI
48
DPDHS level:
Infants and preschool children: Low Birth Weight Underweight
School children Stunting (year 1, 4) Wasting (year 1,4) Overweight (year 1,4)
Adolescence Thinness (year 7) Overweight (year 7)
Pregnant women Underweight
Adults Diet related chronic degenerative diseases
Causes of malnutrition under 5 years Inadequate maternal and child care Access to basic health services
Healthy environmentMaps should be up-dated periodically (quarterly, annually) to identify the areas representing pockets of
severely malnutrition in children less than 5 years and school children and nutrition programmes should
be targeted on such areas.
To complete the process of Triple A cycle, dissemination of information generated from NIS to policy
makers by a Newsletter or bulletin quarterly is needed. Then information can be use to evaluation of
programmes. The evaluations of impact of nutrition interventions are required to identify the gaps.
However, evaluation research is the weakest element of nutrition information strategies in Asia and
elsewhere. It is unwise to assume that well-established interventions are always contributing to reducing
deficiency, especially as circumstances change, and light of the growing knowledge of interactions
among nutritional deficiencies and the complexity of human biochemistry (Asian Development Bank
1999). Evaluation designs can be developed through NIS by MOH, District, Provincial and National level
yearly.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
49/52
NIS/MRI
49
CHAPTER 5
REFERENCES
1. Annual Health Bulletin, Ministry of Health, Planning unit, Sri Lanka;2000.2. Ministry of Health Highways and Social Services, Project Proposal for the Nutrition component-
World Bank assisted Sri Lanka health services development project;1995
3. UNICEF. Strategy for improving nutrition of children and women in developing countries, UnitedNations Children's Fund, New York, USA:1990.
4. World Health Organisation, Physical status: The use and interpretation of anthropometry - Report ofa WHO Expert Committee, WHO Technical Report series 854, Geneva;1995.
5. Asian Development Bank, Asian Development Review- Studies of Asian and Pacific EconomicIssues,17(1,2);1999.
6. World Health Organisation, Global database for malnutrition among children under 5 years, 2002.7. Sri Lanka Demographic and Health Survey, Department of Census and Statistics;20018. Ministry of Policy Planning and Implementation, Nutritional status survey report, Nutrition and
Janasaviya Division;1980/2
9. Ministry of Policy planning 1988/910.Medical Research Institute, Vitamin A deficiency status of children Sri Lanka 1995/6, A survey report,
Ministry of Health and Indigenous Medicine;1998.
11.Medical Research Institute, Anaemia status report in Sri Lanka, unpublished;2002
12.Annual Health Bulletin, Ministry of Health, Planning unit, Sri Lanka;199113. Annual Health Bulletin, Ministry of Health, Planning unit, Sri Lanka;199214.Annual Health Bulletin, Ministry of Health, Planning unit, Sri Lanka;199315.Annual Health Bulletin, Ministry of Health, Planning unit, Sri Lanka;1999.16.ACC/SCN,. ACC/SCN Symposium Report. UN Sub-committee on Nutrition. Nutrition policy paper
#19; 2001.
17.Prior IA, Davidson F, Salmond CE, Czochanska Z. Cholesterol coconut and diet in Polynesian atollsa natural experiment tye Pukapuka and Tohaleau island studies. American Journal of Clinical
Nutrition; 1981;32:1552-1561.
18.Mendis S. Cardiovascular researches in Sri Lanka. Review and Bibliography (1905-1998). Ministry ofHealth, Colombo, Sri Lanka; 1998.
19.World Health Organisation. Non communicable diseases prevention and management. South-EastAsia Region; 2001.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
50/52
NIS/MRI
50
20.Department of census and statistics. Statistical Abstract of the Democratic Socialist Republic of SriLanka, Sri Lanka Food balance sheet 1982-1984, Ministry of Plan implementation; 1985.
21.Department of census and statistics. Statistical Abstract of the Democratic Socialist Republic of SriLanka, Food balance sheet, Ministry of Finance and planning; 1997.
22.Department of census and statistics. Statistical Abstract. Ministry of Finance and planning Sri Lanka;2000.
23.ACC/SCN, Nutrition and Poverty. ACC/SCN Symposium Report. UN Sub-committee on Nutrition.Nutrition policy paper #16; November: 1997.
24.Central Bank of Sri Lanka, Socio-economic and Finances survey-1996/7;1998.25.Fernando MA, Balasuriya S, Herath KB, Katugampola S, Endemic Goitre in Sri Lanka, Asia Pacific
Journal of Public Health,3(1);1989
26.Medical Research Institute, Iodine deficiency status in Sri Lanka 2000/1, Survey Report, Ministry ofHealth;2001.
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
51/52
NIS/MRI
51
ANNEX-1
MEMBERS OF THE CORE-GROUP
1. Dr. Aberra Bekale - Head, Nutrition and Estate programme, UNICEF2. Mrs. Soma De Silva - Ex-Head, Evaluation and statistics unit, UNICEF3. Prof. D.N. Fernando - Professor of Community Medicine, Faculty of Medicine, Colombo.4. Dr. H.M. Fernando - Deputy Director General of Public Health Services, Department of health5. Dr. S.A.P. Gnanissara - Ex-Deputy Director General (ET&R), Department of health6. Dr. C.D. Gunaratne - Director Nutrition, Department of health7. Dr. V. Karunaratna - Director, Family Health Bureau8. Dr. Nynt Nynt Yi - Ex-Head, Nutrition and Estate programme9. Dr. S. Manikkarajha - Ex-Director, Estate and Urban health, Department of health10. Dr. C. Piyasena - Head, Nutrition Department, Medical Research Institute11. Prof. L. Rajapaksa - Associate Professor of Comm. Medicine, Faculty of Medicine, Colombo.12. Mr. N. Sumanaratne - Director, Ministry of Plan Implementation13. Dr. Vidyasagara - Ex-Director, Family Health Bureau14. Dr. K.P. Wickramasuriya - Ex-Director, Family Health Bureau15. Prof. T.W. Wikramanayake - Emirates Professor of Biochemistry
-
7/29/2019 NUTRITION INFORMATION Sri Lanka
52/52
NIS/MRI
52
ANNEX-2
Study Team
Dr. Renuka Jayatissa - Consultant Nutritionist (Principal Investigator)
Dr. C.L. Piyasena - Head
Dr. A.M.A.S.B. Mahamithawa - Medical officer
Dr. I. Warnakulasuriya - Medical officer
Mr. J.M.Ranbanda - Nutrition Assistant
Mr. K.D. Chandrathilaka - Public Health Inspector
Mr. A.P. Seneviratne - Public Health Inspector
Mr. H.K.T. Wijesiri - Public Health Inspector
Mr. H.N.P. Caldera - Public Health Inspector
Mr. P.V.N. Ravindra - Public Health Inspector
Mr. E.G.S. Kulasingha - Public Health Inspector
Mr. M.A.M.P.K. Marasingha - Public Health Inspector
Mr. W.A.P.I. Pieris - Public Health Inspector
Mr. J.S.Dean - Secretary
Laboratory team:
Mrs. T. Amarasena - Research Officer
Mrs. K.S.N. Jayaratne - Medical Laboratory Technologists
Mrs. B.Y. Gamage - Medical Laboratory Technologists
Miss. H. Kulathunga - Medical Laboratory Technologists
Mr. P. Gamage - Laboratory Orderly
Mrs. W. Polpitiya - Laboratory Orderly
Mrs. A.G. Sriyani - Labourer