Nursingcrib.com Nursing Care Plan - Bronchitis
2
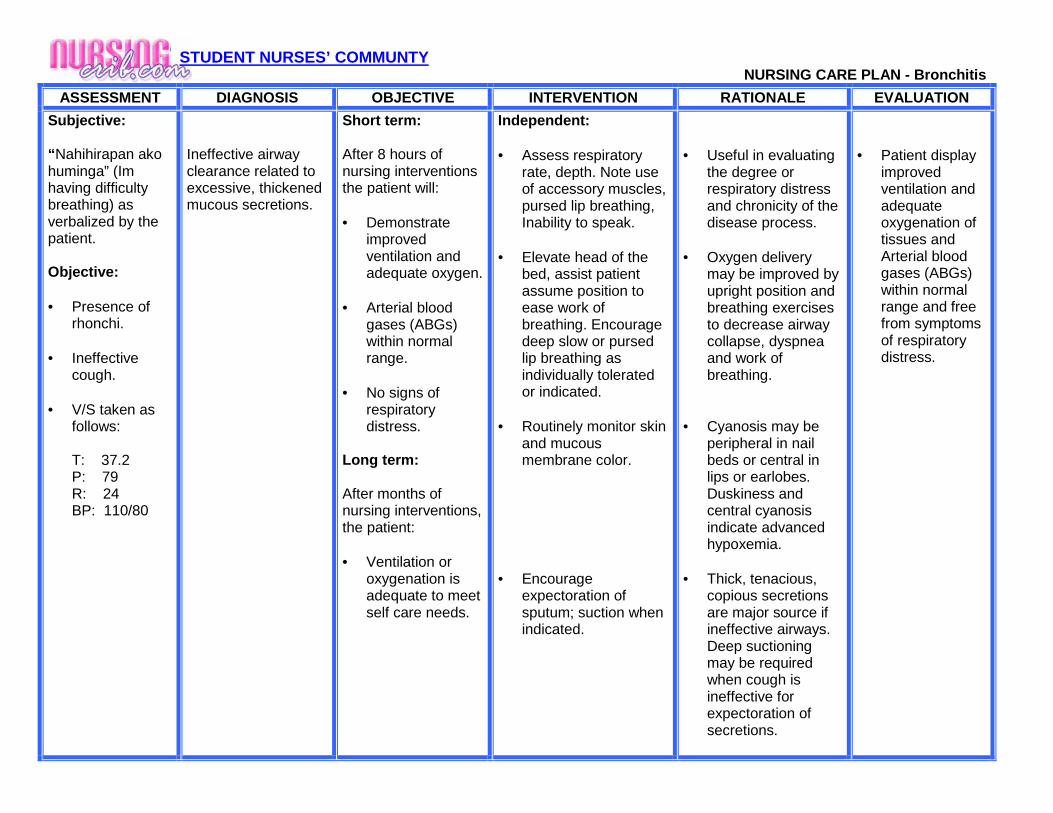
STUDENT NURSES’ COMMUNTY NURSING CARE PLAN - Bronchitis ASSESSMENT DIAGNOSIS OBJECTIVE INTERVENTION RATIONALE EVALUATION Subjective: “Nahihirapan ako huminga” (Im having difficulty breathing) as verbalized by the patient. Objective: • Presence of rhonchi. • Ineffective cough. • V/S taken as follows: T: 37.2 P: 79 R: 24 BP: 110/80 Ineffective airway clearance related to excessive, thickened mucous secretions. Short term: After 8 hours of nursing interventions the patient will: • Demonstrate improved ventilation and adequate oxygen. • Arterial blood gases (ABGs) within normal range. • No signs of respiratory distress. Long term: After months of nursing interventions, the patient: • Ventilation or oxygenation is adequate to meet self care needs. Independent: • Assess respiratory rate, depth. Note use of accessory muscles, pursed lip breathing, Inability to speak. • Elevate head of the bed, assist patient assume position to ease work of breathing. Encourage deep slow or pursed lip breathing as individually tolerated or indicated. • Routinely monitor skin and mucous membrane color. • Encourage expectoration of sputum; suction when indicated. • Useful in evaluating the degree or respiratory distress and chronicity of the disease process. • Oxygen delivery may be improved by upright position and breathing exercises to decrease airway collapse, dyspnea and work of breathing. • Cyanosis may be peripheral in nail beds or central in lips or earlobes. Duskiness and central cyanosis indicate advanced hypoxemia. • Thick, tenacious, copious secretions are major source if ineffective airways. Deep suctioning may be required when cough is ineffective for expectoration of secretions. • Patient display improved ventilation and adequate oxygenation of tissues and Arterial blood gases (ABGs) within normal range and free from symptoms of respiratory distress.
description
care plan for patients with bronchitis
Transcript of Nursingcrib.com Nursing Care Plan - Bronchitis
STUDENT NURSES’ COMMUNTY NURSING CARE PLAN - Bronchitis
ASSESSMENT DIAGNOSIS OBJECTIVE INTERVENTION RATIONA LE EVALUATION
Subjective: “ Nahihirapan ako huminga” (Im having difficulty breathing) as verbalized by the patient. Objective: • Presence of
rhonchi. • Ineffective
cough. • V/S taken as
follows:
T: 37.2 P: 79 R: 24 BP: 110/80
Ineffective airway clearance related to excessive, thickened mucous secretions.
Short term: After 8 hours of nursing interventions the patient will: • Demonstrate
improved ventilation and adequate oxygen.
• Arterial blood
gases (ABGs) within normal range.
• No signs of
respiratory distress.
Long term: After months of nursing interventions, the patient: • Ventilation or
oxygenation is adequate to meet self care needs.
Independent: • Assess respiratory
rate, depth. Note use of accessory muscles, pursed lip breathing, Inability to speak.
• Elevate head of the
bed, assist patient assume position to ease work of breathing. Encourage deep slow or pursed lip breathing as individually tolerated or indicated.
• Routinely monitor skin
and mucous membrane color.
• Encourage
expectoration of sputum; suction when indicated.
• Useful in evaluating
the degree or respiratory distress and chronicity of the disease process.
• Oxygen delivery
may be improved by upright position and breathing exercises to decrease airway collapse, dyspnea and work of breathing.
• Cyanosis may be
peripheral in nail beds or central in lips or earlobes. Duskiness and central cyanosis indicate advanced hypoxemia.
• Thick, tenacious,
copious secretions are major source if ineffective airways. Deep suctioning may be required when cough is ineffective for expectoration of secretions.
• Patient display
improved ventilation and adequate oxygenation of tissues and Arterial blood gases (ABGs) within normal range and free from symptoms of respiratory distress.
STUDENT NURSES’ COMMUNTY
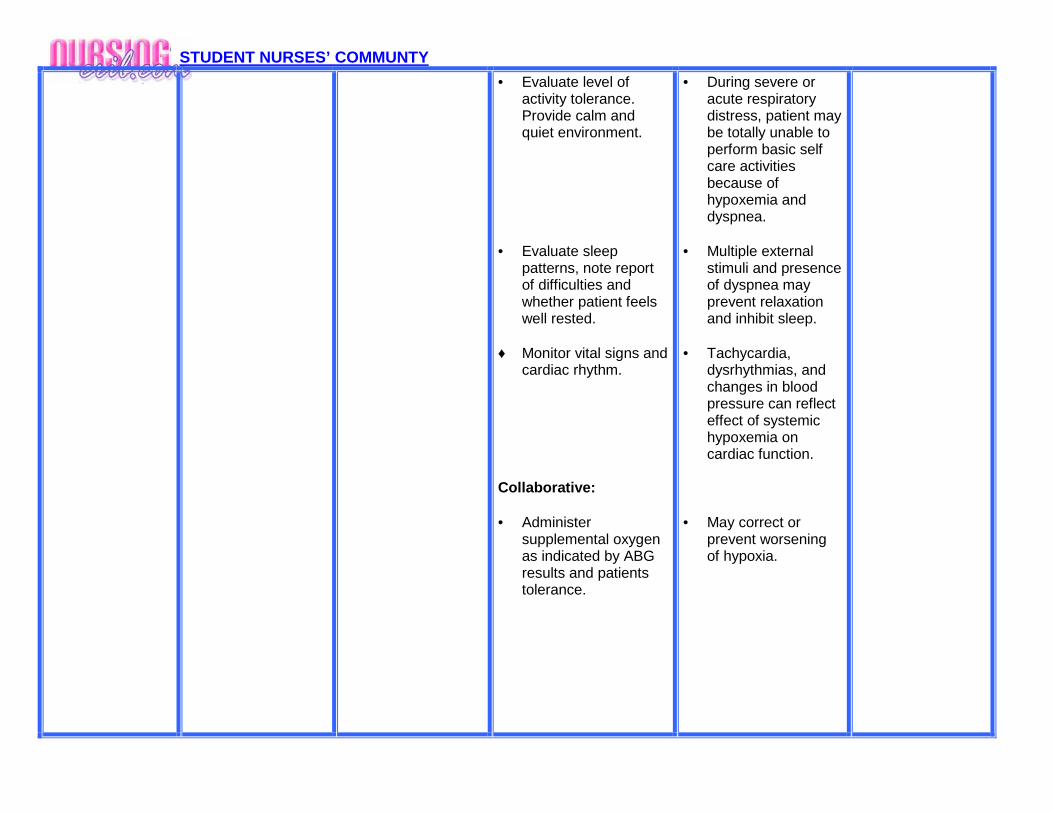
• Evaluate level of activity tolerance. Provide calm and quiet environment.
• Evaluate sleep
patterns, note report of difficulties and whether patient feels well rested.
♦ Monitor vital signs and
cardiac rhythm. Collaborative: • Administer
supplemental oxygen as indicated by ABG results and patients tolerance.
• During severe or acute respiratory distress, patient may be totally unable to perform basic self care activities because of hypoxemia and dyspnea.
• Multiple external
stimuli and presence of dyspnea may prevent relaxation and inhibit sleep.
• Tachycardia,
dysrhythmias, and changes in blood pressure can reflect effect of systemic hypoxemia on cardiac function.
• May correct or
prevent worsening of hypoxia.