Nursing Concepts · C. Develop the written nursing care plan. ... other needs—and remember that...
28
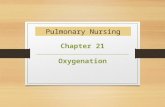
Nursing Concepts 41 Planning A. Assign priority to the nursing care activities. B. Specify goals reflecting desired outcome of nursing care. 1. Develop short-term and long-term goals. 2. Identify nursing interventions for goal attainment. 3. Establish outcome criteria. C. Develop the written nursing care plan. 1. Involve client and family in all aspects of planning. 2. Keep care plan current and flexible. Implementing A. Initiate and carry out planned nursing activities. B. Coordinate activities of client and family members along with health team members. C. Document client’s responses to nursing actions. Evaluating A. Collect objective and subjective data and determine if goals were achieved. B. Identify and make revisions to the nursing care plan. A. Maslow’s hierarchy of basic human needs. 1. Human behavior is motivated by a system of needs. 2. Clients will focus or attempt to satisfy needs at the base of the pyramid before focusing on those higher up (Figure 3-1). 3. Human needs are universal; however, some may be modified by cultural influence. 4. The nursing process is always concerned with phys- iological needs first; then progresses to teaching, decreasing anxiet y, etc. This is also true for the client with psychosocial needs; the client’s physi- ological needs must be met before progressing to the next level. NURSING PRIORITY: Pay attention to Maslow’s hierarchy of needs when answering test questions related to setting priorities. The physiological needs at the base of the pyramid must be satisfied first in order to focus on other needs—and remember that oxygenation is always the first physiological need or priority. STEPS OF THE NURSING PROCESS The categories of the nursing process and the activities in each category vary somewhat according to nursing authors. The nursing process as presented here correlates with the categories of the NCLEX-PN. Data Collection A. Collecting data. 1. Objective data are nursing observations. Example: Client weighs 125 lb; 50 ml of green drainage via the nasogastric tube. 2. Subjective data are information given by the client. Example: “My side hurts; I am scared about surgery.” 3. Client data are collected using three skills. a. Observation: what can be seen. Example: Is the client awake or asleep; is the client obese or underweight; is the client smiling or frowning? b. Auscultation: what can be heard. Example: Is the client laughing; are there breath sounds pres- ent; do you hear hyperactive bowel sounds? c. Palpation: what can be felt. Example: Is the client’s skin warm and dry; does the client have a pedal pulse; is the client’s abdomen soft? ✔ ✽ Figure 3-1 Maslow’s hierarchy of needs. (From Zerwekh J, Claborn J: Memory Notebook of Nursing, Vol 1, ed 4, Ingram, Texas, 2008, Nursing Education Consultants.)
Transcript of Nursing Concepts · C. Develop the written nursing care plan. ... other needs—and remember that...

Nursing Concepts
41
planningA. Assignprioritytothenursingcareactivities.B. Specifygoalsreflectingdesiredoutcomeofnursing care. 1. Developshort-termandlong-termgoals. 2. Identifynursinginterventionsforgoalattainment. 3. Establishoutcomecriteria.C. Developthewrittennursingcareplan. 1. Involveclientandfamilyinallaspectsofplanning. 2. Keepcareplancurrentandflexible.
ImplementingA. Initiateandcarryoutplannednursingactivities.B. Coordinateactivitiesofclientandfamilymembers alongwithhealthteammembers.C. Documentclient’sresponsestonursingactions.
evaluatingA. Collectobjectiveandsubjectivedataanddetermineif goalswereachieved.B. Identifyandmakerevisionstothenursingcareplan.
A. Maslow’shierarchyofbasichumanneeds. 1. Humanbehaviorismotivatedbyasystemofneeds. 2. Clientswillfocusorattempttosatisfyneedsatthe baseofthepyramidbeforefocusingonthosehigher up(Figure3-1). 3. Humanneedsareuniversal;however,somemaybe modifiedbyculturalinfluence. 4. Thenursingprocessisalwaysconcernedwithphys- iologicalneedsfirst;thenprogressestoteaching, decreasinganxiety,etc.Thisisalsotrueforthe clientwithpsychosocialneeds;theclient’sphysi- ologicalneedsmustbemetbeforeprogressingto thenextlevel.
NURSING PRIORITY: Pay attention to Maslow’s hierarchy of needs when answering test questions related to setting priorities. The physiological needs at the base of the pyramid must be satisfi ed fi rst in order to focus on other needs—and remember that oxygenation is always the fi rst physiological need or priority.
sTEPs OF THE NuRsiNg PROCEssThe categories of the nursing process and the activities
in each category vary somewhat according to nursing authors. The nursing process as presented here correlates with the categories of the NCLEX-PN.
data collectionA. Collectingdata. 1. Objectivedataarenursingobservations.Example: Client weighs 125 lb; 50 ml of green drainage via the nasogastric tube. 2. Subjectivedataareinformationgivenbytheclient.Example: “My side hurts; I am scared about surgery.” 3. Clientdataarecollectedusingthreeskills. a. Observation:whatcanbeseen.Example: Is the client awake or asleep; is the client obese or underweight; is the client smiling or frowning? b. Auscultation:whatcanbeheard.Example: Is the client laughing; are there breath sounds pres-ent; do you hear hyperactive bowel sounds? c. Palpation:whatcanbefelt.Example: Is the client’s skin warm and dry; does the client have a pedal pulse; is the client’s abdomen soft?
✔
✽
Figure 3-1 maslow’s hierarchy of needs. (From Zerwekh J, Claborn J: Memory Notebook of Nursing, Vol 1, ed 4, Ingram, Texas, 2008, Nursing Education Consultants.)

42 CHAPTER 3 Nursing Concepts
HEAlTH AssEssmENT
Health History
TEST ALERT: Collect baseline physical data on admission.
The health history is a primary source of client information. The source of the information can be the client, relatives, friends, old records, or any combination of these. A predetermined format should be used as a guide for the interview.A. Demographicdata. 1. Name,address,phonenumber,age,sex,marital status. 2. Race,religion,usualsourceofmedicalcare.B. Chiefcomplaint/reasonforvisit. 1. Chiefcomplaint(CC)ismainreasonclientsought healthcare. 2. CCisrecordedinclient’sownwords.Example: “I have been vomiting blood since this morning.”C. Historyofthepresentillness. 1. Chronologicalnarrativestoryofthehistoryofthe presentstateofhealth. 2. Includesrelevantfamilyhistory.D. Pasthistory. 1. Childhooddiseases. 2. Immunizations. 3. Allergies. 4. Hospitalizationsandseriousillnesses. 5. Accidentsandinjuries. 6. Medications. 7. Prenatal,laboranddelivery,orneonatalhistory (recordedforallchildrenunderage5andolder childrenwithacongenitalordevelopmental problem).E. Reviewofsystems(ROS). 1. Isaverballistingfromheadtotoeoftheclient’s overallstateofhealth. 2. Containssubjectivedatagivenbytheclient;does notcontaininformationfromthephysicalexamina- tion.Specificassessmentdataforeachbodysystem canbefoundatthebeginningofeachchapter.
HEAlTH TEACHiNg
Principles of Client EducationA. Commoncharacteristicsoftheadultlearner. 1. Theadultclient’sbackgroundofexperience,skills, andattitudeswillformthebasisforanynewinfor- mationreceived.Frequentlytheclienthashadno positiveexperiencesinahospitalenvironment. 2. Thelevelofadultdevelopmentwillgreatlyaffect theclient’sreadinesstolearn.Ifaclientisinamid- lifetransition,itmaybeverydifficulttolearnnew attitudesandskillsthatthreatenself-image.
✽
Example: A man in his early 40s may have difficulty accept-ing any education regarding his colostomy.B. Factorscontributingtotheteaching-learningprocess. 1. Readinesstolearn. a. Theclientmustfeelthematerialisrelevantto his/herhealth,andmustbewillingtoputforth theefforttolearn. b. Theclientmusthavethementalcapacityto learn,aswellasthephysicalabilitytoperform theskills. c. Theclientmusthavephysicalandsafetyneeds metbeforefocusingonlearning.Ifaclient exertsallofhis/herenergytocopewiththe physicalstress,thenhe/shehaslittleenergy forlearning. d. Comfort. (1) Physicalcomfort:discomforts(suchas pain,nausea,hunger,needtovoid)are distractorstothelearningprocess. (2) Psychologicalcomfort:anger,frustrations, fear,andguiltseverelyhamperthelearning process. e. Beforetheteaching-learningprocesscanbegin, theclientandthenurseneedtodiscussand agreeonspecificlong-termandshort-termgoals. Thenursemustcarefullyevaluatetheclient’s knowledgeoftheproblem.C. Factorsrelatingtothepresentation. 1. Statethespecificobjectiveofeachteachingsession: exactlywhattheclientistogain. 2. Usevocabularyandterminologyappropriatetothe client’sunderstandingandtohisorherdevelopmen- tallevel.Usecorrecttermsforbodyparts. 3. Trytostimulateasmanysensesaspossible.Use charts,handouts,andpiecesofequipmentwhen appropriate. 4. Repetitionisanintegralpartoflearning.Beready torepeatthematerialortohavetheclientrepeatthe skilluntilhe/shedoesitcorrectlyandbecomes comfortablewiththeskill. 5. Themoreactivetheclientisintheprocess,the betterhe/shewillretaintheinformation. 6. Planshortsessions;donotoverwhelmtheclient withtoomuchinformationatonetime. 7. Whenappropriate,activelyinvolvethefamilyand significantothers. 8. Begenerouswithpositivereinforcement.D. Pediatricfactorsinfluencingthelearningprocess. 1. Intellectualdevelopmentmovesfromtheconcrete totheabstract. 2. Thenurseneedstoassessthedevelopmentallevel ofthechildbeforeplanningtheeducational approach. a. Preschoolclient. (1) Thepreschoolchildfrequentlyexperiences fearsofbodyinjury.Explanationsshouldbe simple.

CHAPTER 3 Nursing Concepts 43
B. Bathing. 1. Typesofbath. a. Bedbath. b. Partialbath. c. Shower. d. Therapeuticbath:sitzbathormedicatedbath. 2. Nursingimplications. a. Roomshouldbekeptwarm,bathshouldbegin withcleanareasandprogresstodirtyareas. b. Topreventdryskin,irritation,andinfection, carefullyrinseallsurfaceareasanddrythem. c. Keepclientwarmbyusingabathblanketand controllingroomtemperature. d. Ensurequietandprivacy. e. Moisturizeskinwithlotion.
NURSING PRIORITY: Clients who are receiving external radiation therapy should not be bathed with soap over the area of the radiation, which will be marked. Lotions and powders should not be used on the area.
3. Levelsofpersonalcare. a. Completecare:Clientrequirestotalassistance fromnursebecauseclientisabletodolittleor nothingwithoutassistance. b. Partialcare:Clientperformsasmuchofhisor herowncareaspossible;nurseusually completesremainingcare. c. PMcare(bedtimeorhourofsleep):Isprovided toprepareclientforarelaxing,uninterrupted periodofsleep;includesoralcare,possible partialbathing,skincare,soothingbackmass- age,straighteningorchangingthebedlinen,and offeringthebedpanorurinal.C. Oralhygiene. 1. Includescareoftheclient’steethordentures,gums, tongue,andlips. 2. Whenprovidingoralcaretounconsciousclient, turntheclient’sheadtothesidetopreventaspira- tion.D. Haircare. 1. Newborninfantsneedscalpscrubbeddailytopre- ventcradlecap. 2. Adolescentsusuallyrequiremorefrequentsham- pooingbecauseofincreaseinoilysecretions. 3. Olderadultclientswillneedtoshampoolessoften.
Body Alignment and Range of Motion (ROM)A. Characteristicsofcorrectbodyalignmentinbed. 1. Headupwitheyeslookingstraightforward. 2. Neckandbackstraight. 3. Armsrelaxedandsupportedatsides. 4. Legsparalleltohipswithkneesslightlyflexed. 5. Feetseparatedandparalleltothelegswiththetoes pointedupwardandslightlyoutward.
✔
(2) Separationanxietyisaprobleminthisage group;includeparentsinteachingsession. (3) Thepreschoolchildisawareofthephysical andmechanicalcausesofproblemshe/she cansee;thechildisunawareofphysical andmechanicalforcesthathe/shecannot see. b. School-ageclient. (1) Benefitsfromtours,drawings,anatomical dolls. (2) Learnswellfromrole-playingandpuppets. (3) Needstoincludeparentsinteaching sessionforreinforcementandtomaintain consistency. c. Adolescentclient. (1) Needstobeasindependentaspossiblein managementofhealthproblem. (2) Needsassistanceincopingwithlossofin- dependenceandself-direction. (3) Educationalprogramsneedtohelpado- lescentdealwithchangesinbodyimage andinmaintainingego.E. Olderadultclient. 1. Determinetheolderadultclient’sfunctionallosses (i.e.,hearingorvisionimpairment,memoryloss). 2. Identifysocialsupporttoaidtheolderadult;this oftenincreasescompliancewithinformationbeing taught. 3. Determinehearingandvisualacuityandmake adjustmentstoleaningprocess. 4. Determineiftheclientisexperiencinganyconfu- sionordisorientation.Askclienttoincludefamily memberinteachingactivity.
BAsiC NuRsiNg skills
Hygienic Nursing Measures
TEST ALERT: Assist with activities of daily living.
A. Bedsandcomfortmeasures. 1. Avoidshakinglinens. 2. Holdallsoiledlinensawayfromyouruniform. 3. Mattresses. a. Alternatingpressuremattress. (1)Providesacontinuousshiftofpressureby alternatinginflationanddeflationofairor waterevery2to5minutes. (2) Usedtopreventdevelopmentofortotreat pressureulcers. b. Eggcratemattress. (1) Foamrubbermattresswithprojectionsthat looklikeaneggcrate. (2) Placedontopofaregularmattress. (3) Usedtopreventpressureareasfromdevel- opinginabedriddenclient.

44 CHAPTER 3 Nursing Concepts
B. Rangeofmotion(ROM). 1. ActiveROM. a. Clientperformsexercisewithoutassistance. b. Usedforclientwhoindependentlyperforms activitiesofdailyliving(ADLs),butforsome reasonisimmobilizedorlimitedregarding activity. c. Goalismusclestrengthening,aswellasmainte- nanceandpreventionofmuscleatrophy. 2. PassiveROM. a. Clientcannotactivelymove. b. Cannotcontractmuscles;thereforemuscle strengtheningcannotbeaccomplished. c. Goalistomaintainjointflexibilityandprevent contractures.C. PrinciplesofROMexercises. 1. Stretchmusclesbymovingthebodypart;avoid movementtothepointofdiscomfort. 2. PerformROMatleasttwicedailyonimmobile clients,withaminimumoffourtofiverepetitionsof eachexercise. 3. Alwayssupportextremityaboveandbelowthejoint whendoingpassiveROMonextremities. 4. Involvetheclientinplanningtheexerciseprogram.
TEST ALERT: Provide for mobility needs – ambulation, range of motion, repositioning.
AsepsisA. Medicalasepsis. 1. Designedtoreducethenumberofpathogensinan areaanddecreasethelikelihoodoftheirtransfer (e.g.,handhygiene).
NURSING PRIORITY: Proper hand hygiene is one of the most important procedures for the prevention of infection.
2. Oftenreferredtoascleantechnique. 3. Administeringoralmedications,givingenemas, providingtubefeedings,andpracticingdaily hygieneareallcarriedoutwiththecleantechnique.B. Surgicalasepsis. 1. Designedtonotjustsimplyreducethenumberof pathogensbuttomaketheobjectfreeofallmicro- organisms. 2. Alsoknownassteriletechnique. 3. Surgicalasepsisisimplantedforsterileprocedures, suchaschangingsteriledressings,completing sterilecatheterizations,andperformingsurgical proceduresintheoperatingroom(Box3-1).
TEST ALERT: Set up a sterile fi eld; use ap-propriate equipment to maintain asepsis; use
aseptic/sterile technique.
Postmortem CareA. Determinewhetherthereareanytissuesororganstobe donated.B. Consultwiththenursingsupervisortodetermine whethertheclient’sdeathneedstobereportedandorif theclient’sdeathnecessitatesanautopsy. 1. Deathresultingfromanaccidentor,homicide,or suicide. 2. Unattendeddeath;deathoccurringataworkplace orduringincarceration.C. Performpostmortemcareassoonaspossible. 1. Determinewhetherfamilywantstoparticipatein postmortemcare. 2. Unlessclientistohaveanautopsy,removeall equipmentaccordingtofacilitypolicy. 3. Cleansethebodyandcoverwithacleansheet. Placeapillowundertheheadandleavethearmson theoutsideofthesheet.Deodorizeroomifneces- sary. 4. Offerthefamilyanopportunitytobewiththe client.Provideprivacyinanunrushedatmosphere.
✔
procedures requiring Sterile technique • Surgicalproceduresintheoperatingroom (e.g.,transurethralprostatectomy[TURP], appendectomy). • Biopsiesintheoperatingroom,treatmentroom,or client’sroom. • Catheterizationsoftheheart,bladder,orotherbody cavities. • Injections:intramuscular(IM),subcutaneous(subQ), intradermal. • Infusions:IV,instillationsorinfusionsofmedicationor radioactiveisotopesintobodycavities. • Dressingchanges: • Usually,firstpostoperativedressingchangedoneby usingsteriletechnique. • Dressingsovercathetersinsertedintobodycavities (e.g.,Hickmancatheter,subclavianlines,dialysis accesssites). • Dressingsofclientswithburns,immunological disorders,andskingrafts.
guidelines for Sterile Field • Neverturnyourbackonasterilefield. • Avoidtalking. • Keepallsterileobjectswithinview(e.g.,belowwaistis notwithinsterilefield). • Moisturewillcarrybacteriaacross/throughaclothor paperbarrier. • Transferofobjectsfromsteriletocontaminated (notsterile)=contaminated. • Donotreachacrossasterilefield.
BOX 3-1 stERiLE tECHNiQuE: PROCEduREs ANd GuidELiNEs

CHAPTER 3 Nursing Concepts 45
5. Returnallpersonalbelongingstothefamily.Docu- mentwhatitemsweretakenandbywhom. 6. Attachidentifyingnametagtothebodyandtothe shroud.Shroudthebodyaccordingtofacility policy.
NURSING PRIORITY: Make sure there is correct identification attached to the body before allowing the body to be removed from the nursing unit.
Wound CareA wound is a disruption in normal tissue caused by
traumatic injury; also may be surgically created.A. Nursinggoals. 1. Promotehealing. 2. Preventfurtherdamage. 3. Preventinfection.B. Woundhealingisaffectedby: 1. Nutritionalstatus. a.Adequatecaloriesandproteinarenecessaryfor tissuehealing. b.Theobeseclientisatincreasedriskforpoor woundhealing. 2. Excessivewounddrainage:impairstissueregenera- tionandwillharborbacteria. 3. Aging:slowingoftissueregeneration. 4. Infection:prolongsinflammationanddelayswound granulation. 5. Locationandapproximationofwoundedges. 6. Circulationtothewound.C. Characteristicsofwoundhealing. 1.Blackwounds. a.Necroticdevitalizedtissue;highriskforinfec tion. b.Frequentlyrequiresharporsurgicaldebridement oftissueforhealingtooccur. 2. Yellowwounds. a.Containdevitalizedtissue;requirecleaningfor healingtooccur. b.Mechanicaldebridementrequiresirrigationsand dressingchanges.A19Fintravenous(IV)cath- eterona30-mLsyringeprovidessafepressure forirrigationandremovalofdevitalizedtissue. c.Wet-to-drydressings,wet-to-moistdressings, woundpacking,andenzymaticdebridement maybeusedtocleanseyellowwounds. d.Hydrocolloidaldressingstoretainmoisture. 3. Redwounds. a.Requireprotectionoffragilegranulationtissue. b.Topicalantibioticointmentandnonadhering dressingsmaybeusedonshallowwounds. c.Woundsshouldbekeptmoist(moisture-reten- tiondressings,hydrogeldressing);drydressings willdamagethenewgranulationtissue.
✔
✽
D. Processofwoundhealing. 1. Primaryintention:woundedgesapproximatedand closed(surgicalincision). 2. Secondaryintention:woundleftopentohealfrom theinsideoutwiththeformationofgranulation tissue.E Nursinginterventions.
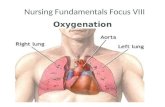
NURSING PRIORITY: When cleansing an area, always start at the cleanest area and work away from that area. Never return to an area you have previously cleaned. Discard the cleansing swab after each horizontal or vertical stroke.
1. Cleansingofwound.(Figure3-2) a. Horizontalwound:cleansedfromcenterofinci- sionoutward,thenlaterally. b. Verticalwound:cleansedfromtoptobottom, thenlaterally. c. Drainorastabwound:cleansedinacircular motion. 2. Woundirrigations:commonlyusedforlargeopen woundsthatarehealingbysecondaryintention. a. Directthesolutionfromthetoptothebottomof thewound,andfromcleantocontaminatedareas. b.Irrigationsolutionshouldbewarmedtopromote comfort. c.Positionclienttopromotegravitydrainagefrom wound. 3.Drainsareinsertedintoanopenwoundtoprevent theaccumulationofsecretionsandexudate.(Figure 3-3). a.Penrosedrain:softflexibledraininsertedinto wound.
✔
Figure 3-2 Wound cleansing. (From deWit, S. Fundamental skills and concepts for nursing, ed 3, St Louis, 2009, Saunders Elsevier).

46 CHAPTER 3 Nursing Concepts
NURSING PRIORITY: Avoid pooling of excessive drainage under saturated dressing; this can lead to skin irritation and infection.
(1) Asafetypinorclipmaybeinsertedthrough thePenrosedraintopreventitfromslipping furtherbackintothewound. (2) Frequentdressingchangesarepreferableto reinforcingthesamedressing. b. Jackson-Prattcatheterordrainagesystem:Bulb mustbecompressedtoallowairtoescapeand thenisrecappedtomaintainsuction. c. Hemovac:Evacuatormustbecompressedat leastevery4hourstoprovidesuction;besureto emptydrainagefrompouringspout. 4. Wet-to-drydressings. a. Purposeistotrapnecrotictissueinthedressing asitdries. b. Dressingshouldbemoistwhenappliedand allowedtodryfor4to6hours. c.Whendressingischanged,thepackeddressing shouldbegentlyremovedalongwithabsorbed drainageandnonviabletissue.Donotsoak packingbeforeremoval;thiswilldecreasethe removalofnonviabletissue.
NURSING PRIORITY: When performing wet to dry dressing change, wring out excessive moisture from dressings. The dressings should be thick and wet enough to dry between dressing changes.
5.Montgomerystraps:usedwhenfrequentdressing changesareneeded;helptopreventskinirritation thatcouldoccurwithtaperemoval.
✔
✔
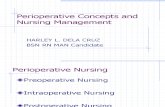
6. Elasticizedabdominalbindersassisttopreventten- siononthesutureline,especiallybeneficialin obeseclients.(Figure3-4) 7. Obtainaspecimenofwounddrainage. a. Gentlyrollasterileswabinthepurulentdrain- age. b. Obtainwoundspecimenbeforeanymedication orantimicrobialagenthasbeenappliedto woundareaoradministeredtoclient.
TEST ALERT: Perform wound care and/or dressing change.
Heat and Cold ApplicationsA. Heatapplications. 1. Purposeofheatapplicationistosoftenexudate,and increasebloodsupplytopromotehealing. 2. Unlessaphysicianorderscontinuousheatapplica- tions,treatmenttimeisusually20to30minutes. 3.Cautionclientregardinghotbathsandvasodilating effectthatmaycauseposturalhypotension. 4. Moistheatpenetratesdeeperthandryheat. 5. Donotuseheatonanareathatisbeingtreatedwith radiation,isbleeding,hasbeeninjuredwithinthe last24hours,orhasdecreasedsensation. 6. Typesofheatapplication. a.Moistheatpack. b.Padthatcirculateswarmedwatertodistribute dryheattobodyparts.Coverthesourceto protecttheskin. c.Heatlamporheatcradle. d.Sitzbath,usecleanwater,notwatertheclient hasusedforbathing.B. Nursingintervention–heatapplication. 1. Takevitalsignsbefore,during,andafterheatappli- cation,ifheatisappliedtoalargearea. 2. Unlessanorderisforcontinuousheatapplications, treatmenttimeisusually20minutes.
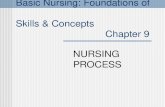
Figure 3-3 medical – Wound drain and suction devices. (From deWit, S, Surgical Nursing: Concepts and Practice, St Louis, 2009, Saunders Elsevier).
WOuNd dRAiN ANd suCtiON dEviCEs
A, Penrose drain.
B, Jackson-Pratt drain and reservoir.
C, T-tube drain.
D, Hemovac drainage system.
Figure 3-4 Abdominal binding. From deWit, S. Fundamental skills and concepts for nursing, ed 3, St Louis, 2009, Saunders Elsevier).

CHAPTER 3 Nursing Concepts 47
3. Closelyobserveskinunderareaofheatapplication. 4. Donotallowclienttoadjusttemperaturesettings.C. Coldapplications. 1. Icebag,icecollar,oriceglove. 2. Coldcompressorcoldpack. 3. Hypothermiablanket. 4. Reducesedema,swellingandpainifappliedimme- diatelyafteraninjury. 5. Maybeusedtodecreasetemperature.D. Nursingintervention–coldapplication 1. Frequentlycheckthetemperatureofaclientwitha hypothermiablanketfortreatmentofafever.
TEST ALERT: Provide cooling measure for elevated temperature.
2. Removethecoldpackif: a.Thereismottling,orrednessofskin. b.Clientcomplainsofburningpainornumbness.
3. Preventchilling, 4. Donotusecoldapplicationsonareasofdecreased circulation,openwounds,orareatreatedwith radiationtherapy.
NURSING PRIORITY: Do not use hot or cold applications with conditions of impaired circulation (e.g., peripheral vascular disease or diabetes).
specimen Collection
TEST ALERT: Collect specimens for diagnostic testing.
A. Generalprinciples. 1. Usesterileequipmenttoobtainspecimenandpre- ventcontaminationfromoutsidesources. 2. Usethecorrectcontainerforeachspecimen:Preser- vatives,anticoagulants,orchemicalsmaybere quired. 3. Alwaysobservestandardprecautionswhenobtain ingspecimens,keepoutsideofcontainercleanto preventcontaminationintransfertothelaboratory. 4. Properlylabelthespecimen.Collectthecorrect amountatthecorrecttime.B. Typesofspecimen. 1. Urine(seeAppendix18-3). 2. Stool(seeAppendix13-13). 3. Sputum:throatornasopharyngeal(seeAppendix 10-8). 4. Blood.
5. Woundspecimen.
✔ vital signs
TEST ALERT: Take client vital signs; compare changes in vital signs to client’s baseline; notify supervisor or health care provider for change in
client status.
A. Normalvalues(Table3-1).B. Assessment. 1. Respirations. a. Evaluateaninfant’srespiratorypatternbefore stimulation. b. Checkthoraciccavityforsymmetricalexcur- sion. c. Breathsoundsarebestevaluatedwithclientin sittingposition. 2. Pulserate. a. Irregularradialpulse(weakvolumeorlowrate) shouldbeassessedbytakinganapicalpulserate readingfor1fullminute. b. Apicalpulseisauscultatedatthefifthintercostal spaceatthemidclavicularline(pointofmaximal intensity,PMI). c. Apical-radialpulseisdeterminedbytwopeople countingboththeapicalandtheradialpulse ratesatthesametime.Thisprovidesinformation aboutpulsedeficit,whichisthedifferencein thetwovalues. d. Aweakperipheralpulsemaybeevaluatedbya Dopplerultrasound. e.Checkapicalpulseinneonates,infants,small childrenandinadultclientswithirregularpulse.
tABLE 3-1 NORMAL vitAL siGNs
NEONAtE Respiration 30-60breaths/min Pulse 120-140beats/min
CHiLd 2 tO 4 yEARs Respiration 24-32breaths/min Pulse 90-130beats/min
CHiLd 6 tO 10 yEARs Respiration 15-26breaths/min Pulse 70-110beats/min Bloodpressure 90/40-110/60mmHg
AduLt Respiration 12-18breaths/min Pulse 60-100beats/min Bloodpressure 100/60-120/80mmHg
NURSING PRIORITY: Know the range of normal values for vital signs at different age levels. This is critical for identifying changes in a client’s status as well as for determining specific criteria for medication administration.
✔

48 CHAPTER 3 Nursing Concepts
3. Temperature. a. Temperatureisaffectedbymouthbreathingand temperatureoforalintake. b. Oraltemperatureistakenunlessotherwiseindi- cated. 4. Bloodpressure(BP)assessment(Box3-2).
NURSING PRIORITY: Know the range of normal values for vitas signs at different levels. This is critical for identifying changes in a client’s status as well as for determining criteria for medication administration.
immOBiliTYImmobility is the therapeutic or unavoidable restric-
tion of a client’s physical activity.A. Causesofrestrictedmovement. 1. Spinalcordorneurologicalinjury. 2. Presenceofseverepain:arthritis,surgery,orinjury.B. Therapeuticreasonsforrestrictedmovement. 1. Todecreasepain. 2. Toimmobilizeawound. 3. Tolimitexerciseandactivity(e.g.,clientswithcar- diacproblems). 4. Toreduceeffectsofgravityonedema,varicosities.
Adverse Physical Effects of immobilityTheprimarynursinggoalinthecareoftheimmobilizedcli-entisthepreventionofcomplications.Thisisachievedbyinitiatingnursingactivitiestopreventcomplicationsandbycarefulassessmentofmajororgansystemsforspecificdataindicatingtheeffectsofimmobility.A. Cardiovascularsystem. 1. Physicaleffects. a. Orthostatichypotension(dropinbloodpressure [BP]uponstanding). b. Decreaseinabilityofthehearttomaintainout- put. c. Venousstasis. d. Increaseincardiacworkload. 2. Nursingimplications. a. Positionbodytoenhancecirculation. b. Changepositionfrequently. c. Usepassiveandactiverangeofmotion. d. Beginactivitygradually;allowclienttositbe- forestanding.B. Respiratorysystem. 1. Physicaleffects. a. Decreaseinthoracicexcursion. b. DecreaseinO
2/CO
2exchange.
c. Increaseinpulmonaryinfections. d. Increaseincollectionoffluidsinthelung. 2. Nursingimplications. a. Elevateheadofbed. b. Maintainadequatehydration. c. Haveclientturn,cough,anddeepbreatheevery 2hours.
✔
✽
d. Promoteincreaseinactivityassoonaspossible; haveclientsitupinchairatbedside. e. Assesspulmonarysecretionsforinfection.
NURSING PRIORITY: Encourage mobility to facilitate improvement in respiratory status, to assist in removal of secretions, to prevent pressure areas on the skin, prevent constipation, and prevent contractures.
C. Urinarysystem. 1. Physicaleffects. a. Urinarystasis. b. Increasedcalciuminurinemayprecipitatestone formation. c. Urinarytractinfections. 2. Nursingimplications. a. Haveclientsituptovoid,ifpossible. b. Increasefluidintake. c. Decreasecalciumintake. d. Assessforurinaryretentionandurinarytract infection.D. Musculoskeletalsystem. 1. Physicaleffects. a. Demineralizationofbones:decreaseinbone strength.
✔
ProcedureClientshouldbeinasittingpositionwithoutlegscrossed.Theinflatablecuffiswrappedsnugglyaroundtheupperhalfofthearm.Thecuffisinflated20to30mmHgabovethepointatwhichradialpulsationdisappears.Asthecuffisdeflated,asoundisproducedwithinthebrachialarteryjustbelowthecuffandisaudiblewiththestethoscope.Thesounds(Korotkoffsounds)coincidewitheachpulsebeat.Usually,whenthecuffpressureisbelowdiastolic,thesoundswillceaseorbecomemuffled.
Nursing implicationsSizeofcuffshouldbe20%widerthanthediameterofthelimb.Ifthecuffistoolarge(e.g.,onachild’sarm),theBPobtainedwillbesubstantiallylowerthanthetrueBP.Ifthecuffistoosmall(e.g.,onanobeseperson’sarm),theBPobtainedwillbehigherthanthetrueBP.ThedifferenceinBPbetweentherightandleftarmsisnormally5to10mmHg.
BOX 3-2 BLOOd PREssuRE AssEssMENt
NURSING PRIORITY: It is important to ascertain and record when the sounds become muffl ed. If there is any doubt, the blood pressure (BP) may be recorded as a tripartite pressure (120/70/50 mm Hg), implying that the sound became muffl ed at 70 mm Hg and disappeared at 50 mm Hg.
✔

CHAPTER 3 Nursing Concepts 49
Figure 3-5 Considerations of the Pain Experience. From: Black J, Hawks, J: Medical Surgical Nursing: Clinical management for positive outcome, ed 7, 2005, Philadelphia, Saunders.
b. Muscleweaknessandatrophy,paralyticileus. c. Lossofmotioninjointsleadstofibrosisand contractures. 2. Nursingimplications. a. Performrangeofmotionexercises. b. Encourageactivecontractionandrelaxationof largemusclegroups. c. Positionbodytomaintainproperalignment. d. Encouragedailyweightbearing(standingat bedside)whenpossible.E. Gastrointestinalsystem. 1. Physicaleffects. a. Anorexia. b. Ineffectivemovementoffecesthroughcolonthat leadstoconstipation. c. Diarrheasecondarytoimpaction. 2. Nursingimplications. a. Establishbowelprogram;forexample,defecate everyotherdayorthreetimesaweek. b. Encouragedietwithadequateprotein,bulk,and liquids. c. Checkforimpaction.F. Integumentarysystem. 1. Physicaleffects. a. Decreaseintissueperfusionleadingtopressure ulcer. b. Decreaseinsensationinanareaofincreased pressure. 2. Nursingimplications. a. Maintaincleanliness.
b. Promotecirculationthroughfrequentposition- ingchanges. c. Protectbonyprominenceswhenturning. d. Preventpressureareasfromtightclothing,cast, orbraces. e. Performfrequentvisualinspectionofpressure areas.
TEST ALERT: Provide for mobility needs; main- tain skin integrity; identify signs and symptoms
of venous insufficiency.
PAiNPain is a complex, universal experience.
Pain is a sensory perceptual experience Pain is a totally subjective personal experience Pain is an early warning sign; its presence triggers awareness that something is wrong in the body (Figure 3-5).A. TypesofPain 1. Acutepain:hasanidentifiablecause;isprotective; short,predictableduration(lastinglessthan3 months);itfrequentlyhasanimmediateonsetandis reversibleorcontrollablewithtreatment.Most oftenhasanidentifiablesourcesuchaspostopera- tivepainthatdisappearsasthewoundheals. 2. Chronicpain:lastsmorethan6months;continual orpersistentandrecurrent.Painmaynotgoaway; periodsofdecreasedandincreasedpain.Originof painmaynotbeknown.
✽

50 CHAPTER 3 Nursing Concepts
3. Referredpain:painthatdoesnotoccuratthepoint ofinjury.Forexample,painrelatedtomyocardial ischemiamaybefeltintheleftarmorshoulder; cholecystitismaybefeltasshoulderpain. 4. Phantompain:painthatfollowstheamputationofa bodypart;maybedescribedasthrobbing,cramp- ing,orburninginthebodypartamputated. 5. Pretendedpain(malingering):clientexpressesthat thereispainwhenactuallyhasnopain. 6. Psychogenicpain:painduetoemotionalfactors ratherthanphysiologicaldysfunction.B. PainAssessment(Box3-3) 1. Patternofpain. a.Painonsetandduration:whenitstarted,precipi- tatingcauses,andhowlongitlasts. b.Breakthroughpain:transient;maybemoderate tosevereandoccursbeyondcurrentanalgesic treatment;usuallyrapidonsetandveryintense. 2. Areaofpain. a.Asktheclienttoidentifythepainsite. b.Painmaybereferredfromtheprecipitatingsite toanotherlocation—shoulderpainwith cholecystitis,leftarmpainwithMI. c. Sciaticapainfollowsanervepathwayofthe sciaticnerve,generallydownthebackofthe thighandinsidetheleg. d.Intensityofpain:useapainorratingscaleto helptheclientcommunicatethepainintensity.
TEST ALERT: Validate pain utilizing a rating scale.
3. Typeofpain-sharp,burning,throbbing,cramping. 4. Determineanyactivitiesandsituationsthatprecipi- tateorincreasethelevelofthepain—movement, ambulation,coughing. 5. Clientresponsestopain. a. Increasedbloodpressure,pulse,andrespira- tions. b.Diaphoresis,increasedmuscletension,nausea andvomiting. 6. Client’sinterpretationandmeaningofthepain experience. 7. Harmfuleffectsofpain.(Box3-4)
Cultural implications of PainA. Culturalbeliefsandvaluesaffecthowaclientresponds topain.B. Nursesfrequentlyassumethattheirownculturalimpli- cationsofpainandthewaystheydealwithpainare thesameasthoseoftheclient.C. Assessattitudesandbeliefsthatmayaffecteffective treatmentofthepain.Someclientsmaybelievethat takingpainmedicationswillcause“addiction”; otherclientsmaybelievethatcomplainingofpainis asignofweakness.D. Avoidstereotypingclientsbyassumingaspecificcul- turewillorwillnotexhibitmoreorlesspain.E. Nursingconsiderationsofpaincontrolassociatedwitha client’sculture: 1. Identifywhatthepainmeanstotheclient;for example,awomaninlaborwillperceivepaindif- ferentlythanaclientwhoexperiencespainasan indicationofadvanceddisease. 2. Identifyculturalimplicationsregardinghowaclient respondstoorexpressespain;someclientsmoan andcomplainloudlywhileothersmaybeveryquiet andstoic. 3. Individualizepaincontrolbasedontheclient’sre- sponsetopain. 4. Establishcommunicationmethodsfortheclientto expresslevelofpainandadequacyofpaincontrol (e.g.,painscales,FACESscale,pictures,images). 5. Expressionofpainissubjective;acceptclient’sper- ceptionandexpressionofpain,andfacilitate nursingcaretomeetclient’sculturalneedsin providingpaincontrol.
TEST ALERT: Recognize cultural diversity in client’s perception of and response to pain.
P:Provokingorpalliativefactors
Q:Quality
R:Region
S:Severity
T:Timing
BOX 3-3 MNEMONiC tO EvALuAtE PAiN
Acute PainDisturbssleepAppetitedecreasesFluidintakedecreasesNauseaandvomiting
Chronic PainFatigueWeightgainPoorconcentrationJoblossDivorceDepression
BOX 3-4 AssEssiNG tHE HARMfuL EffECts Of PAiN
NURSING PRIORITY: The nurse should ad-minister pain medication to clients experiencing acute pain without fear of addicting the client to the medication.
✔

CHAPTER 3 Nursing Concepts 51
Noninvasive Pain Relief MeasuresA. Nursinginterventionforpainrelief(nonpharmacologi- cal). 1. Changepositionsfrequentlyandsupportbodyparts. 2. Encourageearlyambulationaftersurgery. 3. Elevateswollenbodyparts. 4. Checkdrainagetubestoensurethattheyarenot stretched,kinked,orpulled. 5. Providecutaneousstimulationthroughpressure, massage,bathing,andheatorcoldtherapyto promoterelaxation.
NURSING PRIORITY: Low levels of anxiety or pain are easier to reduce or control than are higher levels; pain relief measures should be used before pain becomes severe.
B. Relaxationtechniques. 1. Relaxedmusclesresultindecreasedpainlevel. 2. Typicalrelaxationexercisesfocusondeepbreathing andalternatetensingandrelaxingofvariousbody partsinasystematicmanner. 3. Meditation:focusesattentionawayfrompain. 4. Rhythmicbreathing:methodofrelaxationanddis- tractionbyfocusingonthebreath. 5. Musicmayassistinrelaxation.C. Guidedimagery. 1. Creativevisualizationisthetherapeuticuseofim- agesfromone’simaginationtofocusawayfrom painsensationbyemphasizingpleasantmemories andexperiences. 2. Oftencombinedwithrelaxationandbiofeedback.D. Hypnosisisalsousedtoproduceastateofalteredcon- sciousnessthatischaracterizedbyextremeresponsive- nesstosuggestion.E. Biofeedback:providesclientwithinformationabout changesinbodyfunctionsofwhichclientisusually unaware(e.g.,bloodpressure,pulserate).F. Transcutaneouselectricnervestimulation(TENS). 1. Deliversanelectricalcurrentthroughelectrodes appliedtotheskinsurfaceofthepainfulregion ortoaperipheralnerve. 2. Identifytriggerpoints(areasthatareextremelysen- sitivewhenstimulated)andplaceelectrodes. 3. InstructclienttoadjustTENSunitintensityuntilit createsapleasantsensationandrelievesthepain.G. Acupuncture:mostcommoncomplementarytherapyto decreasepain. 1. Requiresinsertionofthinmetalneedlesintothe bodyatdesignatedpointstorelievepain. 2. Iseffectiveinpainmanagement,aswellasnausea andvomitingassociatedwithpostoperativeand chemotherapy. 3. Encourageclienttoreviewthecredentialsofthe practitioner,whoshouldhaveamaster’sdegreein orientalmedicineandberegisteredtopracticein thestate.
✔
TEST ALERT: Identify client need for PRN medications; provide non pharmacological mea-
sures for pain relief; use an alternative/complimentary nursing actions in providing pain control (e.g., imag-ery, massage, repositioning).
Medications for Pain ReliefA. Administeras-needed(PRN)analgesicmedications (seeAppendix3-2:Analgesics). 1. StepsinadministeringPRNmedications. a. Assessclienttodeterminesourceandquality andcharacteristicsofpain. b. Checkclient’schart. (1) Lastmedicationreceivedandrouteofad- ministration. (2) Thetimeadministered. (3) Client’sresponsetomedication c. Checkcurrentorderforpainmedication. d.Selectappropriatemedication. (1) Usenonopioidanalgesicsformildtomod- eratepain. (2) Avoidcombinationsofopioidsforolder adults. (3) IVmedicationsactmorerapidlyforacute painrelief. (4) AvoidIMinjectionsinolderadults. (5) Sustained-releaseandextended-releaseoral medicationsworkwellforchronicpain managementandwillprovidepainman- agementoveralongerperiodoftime.
NURSING PRIORITY: Use a preventive approach in alleviating pain by administering narcotics before the pain occurs (if it can be predicted), or at least before it reaches severe intensity. This is particularly important in regard to care of the new postoperative client.
e. Documentpainintervention. f. Decreasestimuliinroomanddetermineother factorsinfluencingdiscomfort. g. At15-and30-minuteintervals,assessclient’s responsetopaininterventionanddocument nursingactions.B. Typesofmedications. 1. Narcoticanalgesicsareusedforrelievingsevere pain.Example: Morphine, codeine, hydromorphone (Dilaudid), meperidine (Demerol), oxycodone (Percodan). 2. Nonnarcoticanalgesicsactatperipheralsitestore- ducepain.Example: Propoxyphene (Darvon), 3. Potentiatingdrugsareusedtointensifytheactionof thenarcoticagent.Example: Promethazine (Phenergan), hydroxyzine (Vistaril, Atarax), diazepam (Valium).
✔

52 CHAPTER 3 Nursing Concepts
4. Nonsteroidalanti-inflammatorydrugshaveanalge- sic,anti-inflammatory,andantipyreticproperties.Example: Acetylsalicylic acid (ASA) or aspirin, acetamino-phen (Tylenol), ibuprofen (Motrin, Advil), naproxen (Naprosyn).C. Patient-controlledanalgesia(PCA). 1. Clientcontrolsdeliveryofpainmedicationviaa PCApump. 2. Acommonorderisfor1to4mgofmorphineevery 10minutesuntilpainisrelievedwithalockoutdose of10mgperhour. 3. Checkforparametersforbolusdoseofmedication. a.Shouldbeavailableforepisodesofincreased pain(dressingchanges,chesttubeinsertion,etc. b.Fortheclientwhogoestosleepandawakens withseverepainunrelievedbyPCA. c. Forcancerclientswhoexperiencebreakthrough pain. 4. AdvantagesofPCA. a. Moreeffectivepaincontrol. b. Decreasedclientanxiety,clientcontrolspain moreeffectively. c. Increasedclientindependence. d. Decreasedlevelofsedation. e. Clienttendstouselessnarcotic. 5. Instructanyfamilymemberorsignificantothersnot toadministermedication(documentthatyouhave donethis).ExplainthatPCAworksontheprinciple thatwhentheclientisuncomfortable,heorshewill usethePCA.
NURSING PRIORITY: Fear of addiction is often major concerns of clients (and their families) who are receiving pain medications. The nurse should administer PRN pain medication to clients experiencing acute pain without the fear of addicting the client to the medication.
D. PalliativePainRelief 1. Thepreventionorreliefofpainwhenacureforthe client’sillnessisnotfeasible.
TEST ALERT Palliative/comfort care: assess client for nonverbal signs of pain/discomfort.
Assess, intervene, and educate client/family about pain management.
2. Administeranalgesicsbasedonclient’slevelof pain;medicationisincreasedasclient’spainin- creases. 3. Painmedicationisfrequentlyadministeredonan around-the-clockscheduleratherthanaPRN scheduletomaintaintherapeuticlevelsofmedica- tion.Painmedicationisadministeredintheabsence ofpain.
✔
4. Anurse’sorclient’sfearthattheclientwillbecome dependenton,addictedto,ortoleranttomedication isinappropriateintheprovisionofpaincontrolin palliativecare. 5. Breakthroughpainfrequentlyoccursinclientswith cancer;painmayoccurspontaneously,maybepre- cipitatedbycoughing,mayoccuratanytimeduring thedosinginterval,ormayoccurtowardtheendof thedose. 6. Fearthatopioidswillhastendeathisunsubstanti- ated,eveninclientsattheveryendoflife.Itisim- portantthatnursesprovideadequatepainrelieffor theterminallyillclient.
OLdER AdULT PRIORITY: Analgesics tend to last longer and there is an increased risk for side effects and toxic effects in the older client.
E. EvaluationofPainControl 1. Identifyclientbehaviorresponsebeforetheinter- ventionandcomparewithresponsefollowingthe intervention. 2. Basedonassessmentofpainpriortomedication, determineifpainhasbeenresolved. 3. Chartclientresponsetopainmedication.
END-OF-liFE CAREA. Providepsychosocialsupporttoclientandfamily
TEST ALERT: Provide care and support to clients and families at end-of-life; identify
client’s end-of-life needs and ability to cope with end of life interventions.
1. Assistfamilytoidentifyresourcesfordecisions abouttreatmentandtoprepareadvancedirectives. 2. Assistclienttoidentifyandtocontactspiritualad- visors. 3. Respondquicklytocalllights,checkonclient often,thishelpstokeeptheclientfromfeeling abandonedorisolated. 4. Encouragefamilytoparticipateincareassisting withfood,hygienemeasures,physicalcontact.B. Assistclienttounderstandimplicationsofresuscitation andassociatedterms.
NURSING PRIORITY: It is important that clients understand that full comfort and physical assistance will continue to be provided regardless of their choice to be resuscitated or not. Respect client choices for palliative care.
1. Allownaturaldeath(AND),andordonotresusci- tate(DNR):maintaincomfortmeasures,hygiene andpaincontrol;ordermustbewrittenonchart.
✔
✔

CHAPTER 3 Nursing Concepts 53
2. Fullcode:fullCPRandresuscitationactions. 3. Hospicecareorpalliativecare a.Doesnotrefertoaplace,butrathertoaconcept ofcarethatprovidessupportfortheclientwhois dying. b.Caremaybeprovidedinlong-termcarefacility, hospital,orathome. c. Criteriaforhospicecareincludestheclient’s desirefortheserviceandaphysician’sstate- mentthattheclientwillprobablynotsurvive beyondthenext6months(theallowedtime frameissomewhatflexiblesinceactualamount oftimecannotbepredicted).
Physical Management of symptomsA. Physicalsymptomsofimpendingdeath. 1. Sensory. a.Hearingisusuallythelastsensetodisappear –alwaysconsidertheunconsciousclientcan hear. b.Taste,smellarediminished. c.Visionisoftenblurred,blinkreflexmaybeab- sent. 2. Integumentary:skinisoftencoolandclammy; mottlingoccursonextremities;cyanosisoccurs aroundmouthandnoseandonnailbeds. 3. Respiratory a.Respirationsbecomeshallowandirregular; CheyneStokes—periodsofapneaalternating withdeeprapidbreathing. b. Increasedmucusinupperairwaycausing gurgling,noisyrespirations. c. Inabilitytocoughorclearairway. 4. Cardiovascular. a.Heartratemayvaryfromaregular,increased ratetoaslowingandirregularheartbeatbefore death. b.Decreasedbloodpressureandtissueperfusion. 5. Elimination. a.Urinary:outputdecreases,incontinenceoccurs. b.Bowel:monitorforconstipation;bowelinconti- nencemayoccur. 6. Musculoskeletal. a.Graduallossofabilitytomove,lossoffacial muscletone. b.Difficultyspeaking,unawareofbodyposition. 7. Neurological. a.Decreasedlevelofconsciousness. b.Decreasedreflexes:gag,cough,swallow.B. Nursinginterventions. 1. Providepalliativepainmanagement—thepreven- tionorreliefofpainwhenacurefortheclient’s illnessisnotfeasible. a.Painmedicationisfrequentlyadministeredon anaround-the-clockscheduletomaintainthera- peuticlevelsofmedication;donotdelayordeny painreliefmeasurestoadyingclient.
b.Moderatetolargeamountsofopioidsmaybe requiredtomaintainclient’scomfort. c.Administeranalgesicsbasedonclient’slevelof pain;medicationisincreasedasclient’spain increases. d.Adjuvantmedicationstoincreaseeffectiveness ofanalgesics—antiemetics,antidepressants, corticosteroids. e.Anurse’sorfamily’sfearthattheclientwill becomedependenton,addictedto,ortolerantto painthemedicationisinappropriateinprovision ofpaincontrolinpalliativecare. 2. Dehydration:maintainoralhygiene;donotforcethe clienttoeatordrink.Theoptiontowithhold artificialnutritionorhydrationshouldbemade bytheclientintheadvancedirective,orbythe persondesignatedinadvancedirective. 3. Respiratorydistress:elevatetheheadofthebed, offeroxygen,providemedicationstodecrease apprehension. 4. Elimination. a.Utilizeincontinencepads,preventskinirrita- tion,followfacilityprotocolforindwelling catheters. b.Monitorbowelfunction,assessforimpaction, promotenormalfunctionwithinclient limitations. 5. Anorexia,nauseaandvomiting. a.Assessforprecipitatingcauseandadminister medicationstodecreasenausea. b.Offersmall,frequentmeals,butdonotfocuson client’sneedtoeat. 6. Determineclient’spersonalpreferencesandcultural implicationsregardingdeath.Providefamilycare regardingculturalneeds.
PERiOPERATivE CARESurgicalprocedures,whetherplannedoranemergencyinter-vention,representacrisisinaclient’slife.Howeverminor,surgicalproceduresalwayscarrysomedegreeofrisk,physi-caldiscomfort,andfinancialstress.A. Perioperativereferstotheentireoperativeexperience (preoperative,intraoperative,andpostoperativecare).B. Preoperativephase:theperiodoftimebeforethesurgi- calprocedure. 1. Assessmentandcorrectionofphysiologicaland psychologicalproblemsthatmayincreasethe client’sriskfactors. 2. Clientteachingregardingthesurgery. 3. Clientteachingregardingpostoperativecareand activities.C. Intraoperativephase:theperiodoftimetheclientisin theoperatingroom.D. Postoperativephase:thisperiodbeginswiththeadmis- sionoftheclienttothepostanesthesiacareunit(PACU) andincludestheremainderoftheclient’shospitaliza- tionandrecoveryperiod.

54 CHAPTER 3 Nursing Concepts
Preoperative Care
TEST ALERT: Perform care for client before and after surgical procedure.
A. Clientprofile. 1. Age:Theolderadultandtheinfanthavemoredif- ficultymaintaininghomeostasisthandothe adultandchild.Theolderadultismorelikelyto havechronichealthproblemscomplicatingsurgery (Box3-5). 2. Weight:Obesitypredisposestheclienttopostopera- tivecomplicationsofinfectionandwounddehis- cence.Fattytissueismoresusceptibletothe infectiousprocess. 3. Preoperativeinterview. a. Chronichealthproblemsandprevioussurgical procedures. b. Pastandcurrentdrugtherapy,includingover- the-counter(OTC)medications.
NURSING PRIORITY: Evaluate client’s current medications, be sure to include OTC medications as well as any alternative medications (herbal remedies).
c. Historyofdrugallergiesanddietaryrestrictions. d. Client’sperceptionofhisorherillnessandim- pendingsurgery. e. Client’sleveloforientationandanyvisualor auditoryproblemsthatwouldhinder communication. f. Discomfortorsymptomsclientiscurrentlyex- periencing. g. Religiousaffiliation. h. Familyorsignificantothers. 4. Psychosocialneeds:Fearoftheunknownisthe primarycauseofpreoperativeanxietyinthemen- tallystableclient.Thesurgicalexperienceisunique toeachclientandrepresentsatimeofcrisis. 5. Checkroutinelaboratorystudies–mayvary accordingtoclient’sdiagnosis,valuesshouldbe availabletosurgicalteam. a. Completebloodcount(CBC),bloodtype. b.Clottingstudies(PT,PTT,INR,seeAppendix 11-1). c. Urinalysis. d. Chestx-ray–especiallyforolderadults e. Serumelectrolytes,serumcreatinineandblood ureanitrogen(seeAppendix18-1). f. Electrocardiogram(ECG)-generallyforclients over40yearsorunlessotherwiseindicated.
✔
NURSING PRIORITY: Anticipate questions re-garding basic pre and postoperative nursing care as well as questions that apply to a specifi c surgical condition or procedure. Nursing implications for specifi c surgical procedures may be found under the major systems in the care of the medical-surgical client.
B. Preoperativeteaching:Thegoalistodecreasethe client’sanxietyandtopreventpostoperativecomplica- tions. 1. Evaluatetheclient’scurrentunderstandingofhis/ herillnessandoftheanticipatedsurgicalinterven- tion. 2. Useterminologytheclientwillunderstand. 3. Donotoverwhelmtheclientwithtoomuchinfor- mationatonetime;allowadequatetimeforclient questions. 4. Involvetheclient’ssignificantothersinthepreop- erativeteaching. 5. Preoperativeteachingcontent. a. Deepbreathingandcoughingexercises. b. Turningandextremityexercises. c. Painmedicationpolicy,forexample,PRN,PCA.
✔
Olderadultclientsareatincreasedriskfordeveloping postoperativecomplicationsbecauseofthedecreased responseoftheimmunesystem(whichdelayshealing) aswellastheincreasedincidenceofchronicdisease. • Cardiovascular:decreasedcardiacoutputandperipheral circulation,arrhythmiasaremorefrequentandcanlead toadecreasedcardiacoutput.Thereisanincreased incidenceofarteriosclerosisandatherosclerosiswhich canleadtohypertension. • Respiratory:decreasedvitalcapacity,reducedoxygen exchange,anddecreasedcoughreflexcanleadtoan increasedriskforatelectasis,pneumonia,andaspiration. • Renal:decreasedrenalfunctioncanleadtofluid overload,dehydration,andelectrolyteimbalance. • Musculoskeletal:increasedincidenceofarthritisand osteoporosisleadtoanincreasedriskoffallsand decreasedmobility. • Sensory:decreasedvisualacuityandhearingaffectthe client’sreactiontimeandcanleadtosafetyproblems associatedwithfallsandinjuries. Poornutritionalstatuswhichcanaffecthealingaswellas postoperativerecovery. Theolderclientmayrequirerepeatedexplanation, clarification,andpositivereassurance.
TEST ALERT: Provide care that meets the special needs of the older adult client.
BOX 3-5 OLdER AduLt CARE fOCus preoperative and postoperative considerations

CHAPTER 3 Nursing Concepts 55
d. Adjunctequipmentusedforbreathing:incentive spirometry,nebulizer,O
2mask.
e. ExplanationofNPOpolicyifindicated.C. Physicalpreparation. 1. Skinpreparation. a.Theoperativesiteandthesurroundingarea shouldbecleanedeitherbytheclientorby specificcleansingofthesitebyamemberof thesurgicalteam. b.Shavingtheoperativeareaisnolongerrecom- mendedtobedonebynursingstaff;ifareaisto beshaveditshouldbedoneinthepreoperative holdingareaorintheoperatingroom. 2. Foodandfluidsarerestrictedforapproximately6 hourspreoperatively. 3. Enemasorsometypeofgastrointestinalcleansing isusuallyadministeredtheeveningbeforesurgery involvingtheGItract,pelvicarea,orretroperitoneal area.Thisassiststopreventfecalcontaminationin theperitonealcavity.Takesafetyprecautionswith olderadultclient,bowelpreparationcanbeexhaust- ing. 4. Promotesleepandrest:Afterthepreoperativepro- ceduresarecompleted,theclientgenerallyreceives asleepingmedicationtopromoterest.Common medicationsusedarebarbiturates.D. InformedConsent 1. Thephysicianisresponsibleforhavingthecon- sentformsigned.Itmustbesignedbeforesedation isgiven.Thesurgeonshouldgivetheclientafull explanationoftheprocedure,includingcompli- cations,alternatives,andrisksinvolved. 2. Theclient’sinformedconsentrecord(permit)must besignedbythephysician,theclient,andawitness; thewitnessisfrequentlythestaffnurse.
NURSING PRIORITY: The informed consent record (permit) must be signed before the client receives the preoperative medication.
3. Thesignedconsentrecord(permit)ispartofthe permanentchartrecordandmustaccompanythe clienttotheoperatingroom.
day of surgeryA. Nursingresponsibilities. 1. Haveclientfollowroutinehygienecareorshower withanantisepticsolutionorbactericidalsoap. 2. Reviewclient’sregularlyscheduledmedications anddetermineifanymedicationsaretobeheldon thedayofsurgery,orifallmedicationsshould begiven. 3. Recordvitalsignswithin1hourofclientbeing transportedtosurgery. 4. Secureand/orremovevaluablesaccordingtohospi- talpolicy;weddingbandsmaybetapedonfinger.
✔
5. Facilitymayrequiretheclienttoremovefingernail polishorartificialnailfromatleastonefinger. 6. Mostoftendenturesandremovablebridgeworkare removedtopreventbreakage,aspirationorairway obstruction.Checkyoungchildrenforthepresence oflooseteeth. 7. Removecontactlens,prostheticdevices,glasses, hairpiecesandgivethemtotheclient’sfamily. Removeanymetalhairpinsorclips. 8. Checkclient’sidentificationforfirstandlastname, dateofbirth,physician,andhospitalnumber. 9. Identifyfamilyandsignificantotherswhowillbe waitingforinformationregardingclient’sprogress. 10. Checkthechartforcompletenessregardinglabora- toryreports,signedconsentform,significantclient observations,historyandphysicalrecords. 11. Makesurethesurgicalteamisawareofadvanced directives,oranyreligiousbeliefsthatcouldimpact surgery(bloodtransfusions).B. Preoperativemedications(seeAppendix3-3). 1. Purpose. a. Decreaseanxietyandprovidesedation. 2. Nursingresponsibilities. a. Askclienttovoidbeforeadministrationofmedi- cation. b. Obtainbaselinevitalsigns. c. Medicationisusuallyadministeredaboutan hourbeforesurgery.Manyinstitutionsare administeringthemedicationintheoperative suitesotheclientcanparticipateinthe“time out”processforidentificationofoperativesite. d. Raisethesiderailsandinstructtheclientnotto getoutofbed. e. Removedenturesandpartialplates. f. Observefordesiredresponseaswellasundesir- ablesideeffectsofmedication. g. Maintainquietenvironmentbeforebeingtrans- portedtotheoperatingroom. h. Allowparenttoaccompanychildasfaraspos- sible.C. The“timeout”istheprotocolforpreventingwrong site,wrongprocedure,wrongpersonsurgery;itmust occurinthelocationwheretheprocedureisperformed. Allmembersofthesurgicalteamareinvolvedinthe positiveidentificationofthepatient,thenameofthe intendedprocedure,andthesiteoftheprocedure.D. Nursingconsiderationsforspinalanesthesia. 1. Clientwillnotbeabletofeelanysensationbelow levelofanesthesia. 2. Vasodilationbelowlevelofanesthesiamayprecipi- tatehypotension. 3. Clientmayexperiencepostanesthesiaheadache (“spinal”headache). 4. Clientmayremainawakethroughoutprocedure. 5. Maybeusedinmajorsurgicalproceduresbelowthe levelofthediaphragm.

56 CHAPTER 3 Nursing Concepts
OLdER AdULT PRIORITY: Spinal anesthesia may be used for clients undergoing transurethral resection of the prostate (TURP), inguinal herniorrhaphy, or orthope-dic procedures, as well as for poor-risk clients who would not tolerate inhalation anesthesia very well.
E. Conscioussedation:theadministrationofanIVmedi- cationtoproducesedation,analgesia,andamnesia. 1. Characteristics a. Clientcanrespondtocommands,maintains protectivereflexes,anddoesnotneedassistance tomaintainairway. b. Amnesiamostoftenoccursaftertheprocedure. c.Slurredspeechandnystagmusindicatetheend ofconscioussedation 2. Nursingimplications. a. Clientisassessedcontinuously;vitalsignsare recordedevery5to15minutes. b. Monitorlevelofconsciousness;clientshouldnot beunconscious,butrelaxedandcomfortable. c. Clientshouldrespondtophysicalandverbal stimul;protectiveairwayreflexesremainintact. d. Potentialcomplicationsincludelossofgagre- flex,aspiration,hypoxia,hypercapnia,andcar- diopulmonarydepression. e. Doesnotrequireextensiverecoverytimefollow- ingsurgery.
immediate Postoperative RecoveryA. Admissionofclienttorecoveryarea. 1. Obtainbaselineassessment. a. Vitalsigns. b. Statusofrespirations. c. Generalcolor. d. Typeandamountoffluidinfusing. e. Specialequipment. f. Dressings. 2. Notifysupervisororsurgeonregardinganydeterio- rationofclient’sconditionduringthepostoperative recoveryperiod.
Nursing Interventionsv Goal: Tomaintainandsupportrespiratoryfunction.A. Leaveairwayinplaceuntilpharyngealreflex(gagref- lex)hasreturned.B. Positionclienttomaintainventilationandpreventaspi- ration.C. Encouragecoughinganddeepbreathing.D. Administerhumidifiedoxygenasnecessary.E. Reportsignificantchangesinrespiratorystatus.F. Listentothechestforadecreaseinbreathsounds. NotifysupervisororPCPiftherearesignificant changesinrespiratorystatus.G. Monitorstatusandchangesinpulseoximetry.
✔ NURSING PRIORITY: The client’s respiratory status is a priority concern throughout the client’s entire stay in the postoperative recovery area.
v Goal: Tomaintaincardiovascularstability.A. Checkvitalsignsevery15minutesuntilstable;com- parewithpreoperativevitalsigns.B. Reportbloodpressuremeasurementthatiscontinually dropping5to10mmHgwitheachreading.C. Reportconsistentlyincreasingbradycardiaortachycar- dia.D. Evaluatequalityofpulseandpresenceofirregular pulse.v Goal: Tomaintainadequatefluidstatus.A. MonitorrateofIVinfusion.B. Measureurineoutputifbladdercatheterispresent (minimumof30mlperhourforanadult).C. Evaluateforbladderdistentionifthereisnocatheter.D. Observeamountandcharacterofdrainageondressings ordrainageincollectingcontainers.E. Assessamountandcharacterofgastricdrainageif nasogastrictubeisinplace.F. Nauseaandvomitingmayoccurasclientisrecovering fromanesthesia.v Goal: Tomaintainincisionalareas.A. Evaluateamountandcharacterofdrainagefrominci- sionanddrains.B. CheckandrecordstatusofHemovac,Jackson-Pratt,or anyotherwounddrains.v Goal: Tomaintainpsychologicalequilibrium.A. Speaktoclientfrequentlyincalm,unhurriedmanner.B. Continuallyorientclient.C. Maintainquiet,restfulatmosphere.D. Promotecomfortbymaintainingproperbodyalign- ment.E. Explainallprocedures,evenifclientisnotfullyawake.F. Rememberthatintheanesthetizedclient,thesenseof hearingisthelasttobelostandthefirsttoreturn.v Goal: Clientmeetscriteriatoreturntoroom.A. Vitalsignsarestableandwithinnormallimits.B. Clientisawakeandreflexeshavereturned.C. Dressingsareintactwithnoevidenceofexcessive drainage.D. Clientcanmaintainapatentairwaywithoutassistance.
General Postoperative Carev Goal: Tomaintaincardiovascularfunctionandtissueperfusion.A. Monitorvitalsigns,usuallyevery4hours,afterfull recovery.B. Evaluateskincolorandnailbedsforpalenessand cyanosis.C. Assessclient’stolerancetoincreasingactivity.D. Encourageearlyactivityandambulation.E. Monitorforcirculatorycomplicationsofimmobility.
✔

CHAPTER 3 Nursing Concepts 57
tABLE 3-2 COMMON POstOPERAtivE COMPLiCAtiONs
COMPLiCAtiON siGNs ANd syMPtOMs NuRsiNG iNtERvENtiONAtelectasis-acollapseofaportionofthelungproducinganairlessstateinthealveoli.(Chapter10)
Pulmonaryemboli(PE)movementofathrombusintothepulmonaryartery.(Chapter10)
Pneumonia–anacuteinflammatoryprocesswherealveolifillwithfluid.(Chapter10)
Shock-adecreaseincardiacoutputduetolossofcirculatingbloodvolume.(Chapter11)
Wound infection-aninfectionofthesurgicalincisionarea.
Wound dehiscence
Wound evisceration
Dyspnea,decreasedorabsentbreathsoundsoveraffectedarea,asymmetricalchestexpansion,hypoxia.
Chestpain,dyspnea,tachycardia,increasedanxiety,decreasedpulseoximetry,decreasedbloodpressure.
Fever,shallowrespirations,wetbreathsounds,coughproductiveofthickyellowmucus,mayprogresstohypoxia.
Decreasingbloodpressure,weakpulse,restless,confusion,oliguria.
Poorwoundhealing,redness,tenderness,fever,tachycardia,leukocytosis,purulentdrainage.
Unintentionalopeningofthesurgicalincision.
Protrusionofaloopofbowelthroughthesurgicalwound.
Positionclientonunaffectedside.Maintainhumidification,oxygen(seeChapter15).Administernarcoticscautiouslyifclientisatincreasedrisk.Prevention:assistclienttoturn,cough,anddeepbreath;provideadequatehydration;encourageambulation,preventabdominaldistention.
NotifyRNimmediatelyofanychestpainordifficultybreathinginclientsatincreasedrisk.Placeclientinsemi-Fowlerspositionandbeginoxygen.Maintainbedrest.RemainwithclientinrespiratorydistressPrevention:Encourageambulationassoonaspossible,positionclienttopreventvenousstasis.
Maintainclientinloworsemi-Fowlers,monitorpulseoximetrylevels.Humidifiedoxygenandmaintaingoodhydration.Prevention:coughanddeepbreath,encourageincentivespirometry.Olderadultclientsareatincreasedrisk;encouragepostoperativeactivityassoonaspossible.
AnticipateRNwillinitiateIVaccessifnotpresent,maintainNPOandbedrest.Positionclientsupine.Preventhypoxiaandmonitorvitalsigns.(seeChapter11).Prevention:closelymonitordrainsandincisionsforbleeding,identifyclientsatincreasedrisk.
Cultureincisiontodetermineorganism.Evaluateprogressofwoundhealing.Prevention:identifyhigh-riskclients;maintainsteriletechniquewithdressingchanges;goodhandhygiene.
Evaluateforbleeding;maintainbedrestandorpositionclienttopreventfurtherpressureatincisionsite.Prevention:identifyclientsatincreasedriskforstressonincisionandpoorhealing;assistclienttosplintincisionwhencoughing;useabdominalbinders.
Coverbowelwithsterilesalinesoakeddressing.Donotattempttoreplaceloopofbowel.Notifyphysician;clientwillmostlikelyreturntosurgeryforfurtherexploration.
TEST ALERT: Monitor wounds for signs and symptoms of infection.
Continued

58 CHAPTER 3 Nursing Concepts
v Goal: Tomaintainrespiratoryfunction.A. Haveclientturn,cough,anddeepbreatheevery2 hours.B. Encourageuseofincentivespirometrytopromotedeep breathing.C. Maintainadequatehydrationtokeepmucussecretions thinnedandeasilymobilized.D. Encourageearlyambulation.E. Evaluatesputumforpresenceofinfection.v Goal: Tomaintainadequatenutritionandelimination.A. Assessforreturnofbowelsoundsandnormalperistal- sis.B. Assesstheclientwithanasogastrictubeforreturnof peristalsis.C. Encouragefluidsafterclientdemonstratestoleranceto fluids.D. Assessclient’stoleranceoforal(PO)fluids;usually beginwithclearliquids.E. Dietisusuallyprogressiveasclient’sconditionand appetiteindicate.F. Recordbowelmovements;normalbowelfunction shouldreturnasevidencedbynormalbowelmovement onthesecondorthirdpostoperativeday(provided theclientiseating).G. Assessurinaryoutput.
1. Clientshouldvoid8to10hoursaftersurgery. 2. Ifbladdercatheterispresent,clientshouldaverage atleast30mlperhour. 3. Promotevoidingbyallowingclienttostandoruse bedsidecommode,ifnotcontraindicated. 4. Avoidcatheterizationifpossible.v Goal: Tomaintainfluidbalance.A. MonitorIVinfusionsforcorrectfluidandrateof infusion.B. Assessforadequatehydration. 1. Moistmucousmembranes. 2. Adequateurineoutputwithnormalspecificgravity. 3. Goodskinturgor. 4. Stablevitalsigns. 5. Alertandoriented.C. Assesscharacterandamountofgastricdrainage throughthenasogastrictube.v Goal: Topromotecomfort.A. Anticipatepain;assessandadministerappropriate analgesics.B. Administerantiemeticfornauseaandvomiting.C. Maintaingoodhygiene(e.g.,cleandressings,clean gown).D. Changeclient’spositionevery2hours.E. Allowforperiodsofrestafteradministrationof analgesics.
tABLE 3-2 COMMON POstOPERAtivE COMPLiCAtiONs—cont’d.
COMPLiCAtiON siGNs ANd syMPtOMs NuRsiNG iNtERvENtiONUrinary retention
Gastric dilatation
Paralytic ileus-causedbydecreasedperistalsis,orintestinalobstruction,leadingtogastricdistention.
Inabilitytovoid8hoursaftersurgery;bladdermaybepalpable;voidingsmallamounts,dribbling
Nausea,vomiting,abdominaldistension,decreasedbowelsounds.
Determineamountoffluidintakeandwhentoanticipateclienttovoid—generallywithin8hr.Palpatesuprapubicareatoevaluateforbladderdistention.Assistclientintonormalvoidingpositionifpossible,runtapwater,provideprivacy.Catheterizeonlyifnecessary.Prevention:Determinepreoperativerisks:medications,lengthofsurgery,historyofpros-tateproblems.
Clientswithabdominalorbowelsurgeryareatincreasedrisk.Positionclientinsemi-Fowlerstodecreaseriskofaspiration.MaintainclientNPO.Prevention:Olderadultclientsareatincreasedrisk;andclientswithabdominalorbowelsur-geryareatincreasedrisk;encourageactivityassoonaspossible;carefullymonitoranalgesics.
Prevention:sameasforgastricdistention.MaintainnasogastrictubesuctionandNPOsta-tus.IfNGtubeisnotpresent,maybeginearlyfeedingofclearliquidstoincreaseintestinalmotility.Evaluatefordistention,statusofbowelsoundsandabdominaldiscomfort.Monitorforpossiblecompromisedrespirations.
IV, Intravenous; NPO, nothing by mouth; NG, nasogastric

CHAPTER 3 Nursing Concepts 59
NURSING PRIORITY: In addition to the pain and discomfort associated with a surgical procedure, it is important to assess other possible sources of discomfort, such as full bladder, occluded catheter or tube, gas accumulation, IV infiltration, or compromised circulation due to position/pressure.
Postoperative Complications – see Table 3-2
disaster Planning
TEST ALERT: Participate in preparation for internal and external disasters – participating in safety drills, identifying safety manager, locating
Material Safety data Sheet (MSdS).
A. Fire 1. Immediatelyreturntoyourunitifafirecodeis called. 2. Iffireislocalized(inoneroomorarea),removethe clientsfromtheimmediatearea. 3. Ifclientsonyourunitarenotinimmediatedanger, closeallofthedoorstotheclient’sroomsandtothe unit. 4. Ifyouneedtoevacuateyourunitbecauseofanim- mediatedangertostaffandclients,evacuateclients inthisordertoprovideforthemostrapidremoval ofthemostclientsinashortperiodoftime: a. First:Ambulatoryclientsarefirstbecausethey canmovethequickestandyoucanremovemore clientsquickly. b. Second:Clientsinwheelchairsorwalkersor clientsthatneedassistancearenexttobe evacuated. c. Third:Clientsthatrequirethemostassistance, forexample,ventilatorclientsorthosewhoare totallybedridden,arethenexttobeevacuated. 5.Knowthetypesoffireextinguishers: a.ClassA:waterorsolutionforpaperorlinenfires. b.ClassB:foamextinguisherforgrease,chemical, orelectricalfires. c. ClassC:multipurposeforpaper,linen,orelectri- calfires. 6. Usingafireextinguisher—rememberPASS: Pullthepin. Aimatthebaseofthefire. Squeezethetrigger. Sweepfromsidetoside.B. Responseacronym:RACE Rescue—removeallclientsinimmediatedanger. Alert—initiatethealarm. Confine—closealldoorsandwindows;turnoff oxygenvalvesandelectricalequipment. Extinguish—usetheappropriateextinguisherfor typeoffire.
✔ lEgAl imPliCATiONs
Responsibility for PracticeA. Individualliability. 1. Everynurseisliableforhisorherownconduct. 2. Liabilitymaybesharedbyanotherpersonorgroup (e.g.,thedoctor,anothernurse,orthehospital),but itcannotberemovedbythestatementsoractionsof another. 3. IfanRNisnotavailable,thepracticalnursemay notcarryoutfunctionsthatarerecognizedtobe outsidethescopeofpracticeofapracticalnurse.
TEST ALERT: Identify your professional prac-tice limitations (refuse to perform tasks outside your scope of practice); report a health care pro-
vider’s unsafe practice.
B. Unethicalnursingcare. 1. Medicationerrorsthataremadeandnotreported/ corrected. 2. Physicalandverbalclientabuse. 3. Providingcarewhileundertheinfluenceofalcohol ordrugs. 4. Breachofclientconfidentiality. 5. Jeopardizingaclient’swell-beingbywithholding careortreatment. 6. Providingcareoutsidetheprotocolforsafe,ethical nursingpracticeaccordingtotheindividualstate nursepracticeact. 7. Thepractical/vocationalnurseshouldfollowthe lineofauthoritywithintheinstitutionforreporting anincident.C. Standardofcare:Thelegalconceptofafictional,rea- sonable,prudentindividualofthesameeducationand professionagainstwhichanotherprofessional’s performanceisjudged. 1.Statementofnursingstandards. a.Practiceacts,andrulesandregulations. b.JointCommission(JC). c. Policyandprocedures’manuals. d. Priorcourtdecisions. 2. Usedtodeterminewhenabreachofdutyhas occurred.D. GoodSamaritanlaws:enactedbyindividualstateswith thepurposeofprotectinghealthcareproviderswhoas sistataccidentsandemergencies. 1. Careprovidedingoodfaith. 2. Caremustbegratuitous;nocompensationis receivedforthecarerendered. 3. Careprovidedshouldnotbenegligent. 4. Knowthestatusinyourstate.

60 CHAPTER 3 Nursing Concepts
Legal Considerations A. Negligence:Unintentionalharmtoanotherthatoccurs throughfailuretoactinareasonableandprudent manner.B. Malpractice:Unprofessionalnursingpracticethatfails tomeettheproperstandardofcare.C. Invasionofprivacy:Protectionofconstitutionalrightto befreefromundesiredpublicityandexposuretopublic view. 1. Propercoveringofphysicalbody. 2. Medicalrecords. a. Releasewithsignedclientconsentform. b. Releaseformedical“needtoknow”limitedto caregiversonly. 3. Belongingsmustbeprotectedandmaynotbe searchedwithoutspecificauthorization.Aclient’s listofbelongingsshouldbeexplainedtoandsigned bytheclient. 4. Conversationsconfidential;insomestatesprotected byspecificstatute. 5. Photographsandviewingofproceduresrequire consentofclient. 6. Controlofvisitoraccesstoclientandclientinfor- mation. 7. Reportinglawsareanexception–someinformation isrequiredbylawtobereported.
TEST ALERT: Follow regulation/policy for reporting specific issues (abuse/neglect, gunshot wound, or communicable disease, etc.)
a. Communicablediseases. b. Injuriesordeathsthatare,orcouldbe,causedby physicalviolence(gunshotandknifewounds). c. Clientabuse-childrenandolderadult. d. Othersdefinedbystatestatute. 8. Rightsmaybewaivedbytheclientbutneverby medicalpersonnel. 9. Nursesareobligatedtomaintainconfidentialityof client’shealthinformationinaccordance withtheHealthInsurancePortabilityandAccount abilityAct(HIPAA)of1996.D. Validconsent(informedconsent).
TEST ALERT: Obtain client’s signature on consent form. The signed informed consent form provides evidence the consent process has
occurred. The nurse should verify with the client that the physician has discussed the risks and benefits of the surgery and the client understands his/her rights.
1. Timely:Somestatesorinstitutionshavespecific timerestrictionsonwhenconsentsaresigned. 2. Written:Thisisrequiredforallinvasiveprocedures.
3. Witnessedsignature:Donotsignaninformedcon- sentasawitnessunlessyouknowclienthasall informationandunderstandstheinformationneces- sarytoaninformeddecision. 4. Procedurespecifiedintermstheclientcanunder- stand. 5. Clientunderstandingofsignificantrisksofproce- dure. 6. Signedwhileclientisfreefrommind-alteringdrugs orconditions. 7. Withdrawalofconsentcanbewrittenorverbaland mayoccuratanytimebeforetheprocedure.E. Orders:doctors/primaryhealthcareprovider.
TEST ALERT: Evaluate appropriateness of an order.
1. Questionanyorderthatisnotclearlywrittenand understood. 2. Eachmedicationordershouldcontainthecorrect medicationname,therouteofadministration,the dosageamount,andthetimeofadministration. 3. Single-doseordersareforamedicationtobegiven onetime. 4. “Stat”orders:procedureormedicationshouldbe given/carriedoutimmediately;newordersshould bescannedinitiallytodetermineifany“stat” ordersarepresent. 5. Thenurseisresponsibleforquestioninganymedi- cationorderiftheorderisnotclear,orifthenurse feelstheremaybeanerrorintheorder.
Protective ProceduresA. Documentation:writtenrecordofeventssurrounding client’shospitalstay. 1. Protectsclientbypromotinggoodcommunication amonghealthcareproviders. 2. Providesevidenceincourtofcaregiven. a. Courtswillnotassumecareisgivenunlessitis recorded. b. Demonstratesmeetingofstandardofcare.B. Howtodocument(Box3-6). 1. Usetheagencyformatcorrectly. 2. Completeallportionsofformat. a. Useopinionsonlyinassessmentportionof charting,neverinareasrequiringfactualdata. b. Completeanhonestrecordofevents. (1) Donotalterrecordatanytime. (2) Recordallevents,evenunusualevents, factually. (3) Giveallappropriateinformationabouteach note(e.g.,statusofincision:presenceofand typeofdrainage,inflammationofarea,foul odor,andtypeofdressingifany). (4) Explainomissionsincare. 3. Time,date,andsignallentries.

CHAPTER 3 Nursing Concepts 61
4. Donotskiplines;donotleaveanyblankspacesfor otherpeopletochart. 5. Correcterrorsproperly. a. Drawastraightlinethrougherror;dateand initial. (a) Nowhite-outonerror. (b) Noobliterationorerasureoferror. (c) Norecopyingofpagetoomitnote. b. Addomittedinformationbyan“addendum”or “lateentry”;givedateandtimeoforiginalnote aswellasdateandtimeofaddendum. 6. Usemeaningful,specificlanguage,donotuse wordsyoudonotunderstandorunacceptable abbreviations.C. Incidentreports.
TEST ALERT: Report incidents/events/irregular occurrences according to facility guidelines.
1. Onlythepersondirectlyinvolvedintheincident shoulddocumentthefactsinthereport. 2. Donotcompleteanincidentreportforsomeone else. 3. Documentthefacts. a.Donotdrawconclusionsorspeculateonwho causedorwhowasresponsiblefortheincident. b.Donotstateopinionsormakejudgments. 4. Reportdoesnotreplacethedocumentationofthe incidentinthechart. 5. Donotdocumentanyreferencetotheincidentre- portinthechart;thesamefactualinformationfiled ontheincidentreportshouldbeincludedonthe chart. 6. Failuretocompleteanincidentreportcouldbecon- sideredacover-up. 7. Completeanincidentreportforanyunusualoccur- renceoraneventinwhichclientorfamilysafety wascompromised.Followthelineofauthority withintheinstitutionforreportinganincident.D. Knowyourlimits.
TEST ALERT: Recognize task/assignments you are not prepared to perform and seek assistance.
1. Physical-emotional:beawareoffatigueandexhaus- tionandcompensateforthem. 2. Practicecompetency. a.Donotperformprocedureswithoutadequate preparation,knowledge,andexperience. Requestsupervisionifyouareunsureofyour skills. b.Reportunsafepracticestoyoursupervisor. c.Donotallowanyonetotalkyouintodoing somethingyouarenotsureofbylettinghim orheragreetotaketheliabilityortellingyou thatyoushoulddoit.
• Allentriesshouldbeaccurateandasobjectiveas possibe. • Makecorrectionsappropriatelyandaccordingtoagency orhospitalpolicies.Donotobliterateanyinformation thatiswrittenonthepaperchart. • Ifthereisinformationthatshouldhavebeenchartedand wasnot,makea“lateentry,”indicatingthetimethe chartingactuallyoccurredandthespecifictimethe chartingreflects.Example:10/13/09.10:00a.m.late entry,chartingtoreflect10/12/09. • Allidentifiedclientproblems,nursingactionstaken, andclientresponsesshouldbenoted.Donotdescribea clientproblemandleaveitwithoutincludingnursing actionstakenandtheclient’sresponse. • Beasobjectiveaspossibleincharting.Ratherthen charting“Theclienttoleratedtheprocedurewell,”chart thespecificparameterscheckedtodeterminethat conclusion.Achartentryworded“ambulated,tolerated well”wouldbemoreeffectiveifcharted“ambulated completelengthofhall,noshortnessofbreathnoted, pulserateat98,respirationsat22.” • Eachpageofthepaperchartoreachcomputerentry shouldcontainthecurrentdateandtime.Eachtime informationisenteredonanewpage,makesureit reflectsthecurrenttimeofcharting. • Documentwhosawtheclientandwhatmeasureswere initiated.Particularlynotewhenthedoctorsvisited; ifyouhadtocalladoctorbecauseofaproblem,record thedoctor’sresponse.Iforderswerereceived,besure theyaresignedaccordingtopolicy.Thisisespecially importantifyouhadtomakeseveralcallstothedoctor. • Makesureyournotesonthepaperchartarelegibleand clearlyreflecttheinformationyouintended.Itisagood ideatoreadoveryournurse’snotesfromtheprevious daytoseewhethertheystillmakesenseandaccurately portraythestatusoftheclient.Ifthenotesdonotmake sensetoyouthenextday,imaginehowdifficultitwould betodeciphertheinformationatalaterdate,orincourt. • Chartingbyexceptionmaybeavailableonelectronic charts,aswellaspapercharts.Inthiscase,thenurse mayberequiredtodocumentonlysignificantfindingsor exceptions.Itisimportantthatexceptionnotesare enteredandprovideaclearpictureoftheclient’scare orstatus. • DonotgiveyourcomputerpasswordorIDtoanyone, anddonotchartforanyotherhealthcareperson. • Ifchartingbycomputerintheclient’sroom,makesure thenursingormedicalrecordhasbeenclosedbefore leavingtheroom. AdaptedfromIrvin,Judy:Legalissues.InZerwekhJ, ClabornJ,editors:Nursing today: Transitions and trends, ed6,St.Louis,2009,Saunders.
BOX 3-6 GuidELiNEs fOR EffECtivE dOCuMENtAtiON

62 CHAPTER 3 Nursing Concepts
E. Clientidentification—TheJointCommissionrequire- ments: 1. Twoidentifiersarerequired;forexample,the hospitalidentificationnumberandtheclient’sname onthearmband.Physiciansnameandclient’sdate ofbirtharecommonlyonidentificationarmbands. 2. Ifclientdoesnothaveanarmband,thentheindi- vidual’sstatednamewouldbeoneidentifier; theclient’sdateofbirth,socialsecuritynumber, address,orphonenumbercouldserveasthesecond identifier. 3. Client’scurrentphotographorvisualrecognition maybeusedasoneidentifierinlong-termcare facilities,homecaresettings,orbehavioralcare facilities.Forshort-termclients,facilitieswith unstablestaffing,and/orhigh-riskmedications,the two-identifierrequirementisnecessary. 4. Theclientdoesnothavetostatehisorhernameas anidentifier.
NURSING PRIORITY: Always check client identifi -cation according to the Joint Commission guidelines.
specifi c situations at RiskA. Physicalinjurytotheclient. 1. Inappropriatesiderailuse. 2. Inadequatesupervisionduringambulation. 3. Obstacleordangersonfloororinpathofclient. 4. ImpropertransportationB. Improperuseofrestraints-maybephysicalorchemi- calrestraintsandareusedonlytoprotectthephysical safetyoftheclientandothers. 1. Useofarestraintonaclientrequiresaphysician’s orderfor: a.Typeandlocationofrestraint. b.Typeofbehaviorforwhichrestraintistobeused. c.Timeframethattheorderfortherestraintcovers. 2. Inanemergencysituation,physicalrestraintsmay beusedwithoutadoctor’sorderforaverylimited periodoftime. 3. Safenursingpracticeforthecareofaclientinre- straintsincludes: a.Checkrestrainedclientevery30minutesand provideforphysiologicalneeds. b.Removerestraintsandproviderangeofmotion every2hours. c.Documentthetimeofeachcheckandtheneuro- vascularstatusofclient’sextremities. d.Removerestraintsassoonaspossible. e.Securerestraintstothebedframe,nottotheside rails. f.Discusswithfamilytherationaleforandpur- poseofrestraints. g.Investigateallalternativestorestraints:family involvement,methodstoincreaseclient orientation,scheduledtoiletingactivities.
✔B. Medicationerrors(seeChapter4). 1. Followthesevenrightsofmedicationadministra- tiontoprotecttheclient. 2. Haveabasicknowledgeofmedicationsadminis- tered. a.Reasonclientisreceivingthemedication. b.Majorsideeffectsofmedication. c.Anticipatedclientresponsetomedication. 3. Neveradministeramedicationwithoutacomplete order. 4. Notify the supervisor or RN if there is a obvious contraindication to the administration of a medication. C. Administrationofnarcotics 1. Neversignoutforanarcoticyoudonotpersonally administer. 2. Donotsignasawitnessfornarcoticwastingunless youactuallyobservethewasting. 3. Alwayshaveanotherlicensedpersonwitnessand co-signwheneveritisnecessarytowasteanarcotic.D. Telephoneandotherverbalorders(Box3-7).
TEST ALERT: Take a verbal or phone order; transcribe a physician’s order.
1. Practicalnursesmustbeawareofthepoliciesand proceduresoftheinstitutionregardingtelephone orders.SomeinstitutionsdonotallowthePNto takedoctor’sorders.Thepracticalnurseislegally obligatedtofollowthepolicyoftheemploying institution. 2. Writedownthetelephoneorderandreaditback; receiveconfirmationthattheorderiscorrect. 3. Donottakeverbalorderswiththephysicianpresent whenitisnotanurgentsituation. 4. Ordersleftonvoicemailarenotacceptable;the nursemustcallthehealthcareprovidertoobtain theorderdirectly.
• Saywhoyouarerightaway. • Donotapologizeforphoning. • Stateyourbusinessbrieflybutcompletely. • Ifyouwantthedoctortoassessthepatient,sayso. • Ifthedoctoriscoming,askwhentoexpecthimorher. • Ifyougetdisconnected,callback. • Documentattemptstoreachadoctor. • Ifadoctorisrudeorabusive,tellhimorhersoand reportittothenursingmanager. • Ifyoucannotreachadoctororgetwhatyouneed, alwaystellyournursingmanager. FromRosser,Cathy:Building Nursing Management Skills. InZerwekhJ,ClabornJ,editors:Nursing today: Transitions and trends,ed6,St.Louis,2009,Saunders.
BOX 3-7 tiPs fOR COMMuNiCAtiNG WitH PHysiCiANs ON tHE tELEPHONE

CHAPTER 3 Nursing Concepts 63
5. Verbalordersleftwithpatientsorfamilymembers arenotacceptable;thenursemustcallthehealth careproviderandobtaintheorderdirectly. 6. Obtainneededsignaturepromptlyfortelephone orders.D. Changesinclient’scondition.
NUIRSING PRIORITY: Identify and report signifi-cant changes in client condition.
1. Notify appropriate individuals of changes – RN, unit supervisor, physician, or other health care provider. 2. Followthechainofcommandifthereisfailure toprovideappropriatecareafternotificationofsig- nificantchangeinclientcondition. 3. Documentchangesandeventssurroundingthe changeintheclient’sstatus. 4. Thepracticalnurseisresponsibleforevaluating clients,andobtainingassistance,ornotifying appropriateindividualsofthechangeinclientcon- dition. 5. Followuponassessmentsofclientproblemsand whatnursingactionwastakentoresolvetheprob- lem.Forexample,thenursemayverycarefully documenttheeventssurroundingaclient’sfall, butitisalsocriticaltofollowuponwhatwasdone toprovidecareandtoprotecttheclientafterthe fall.E. Hand-off(shift)report:purposeistoprovideaccurate informationandsafequalitycarethroughouttheclient’s hospitalization. 1. Useaninteractivecommunicationmethodunder standableforallinterdisciplinaryteams—SBAR: Situation—Whatishappeningatthepresent time? Background—Whatarethecircumstances leadinguptothissituation? Assessment—WhatdoIthinktheproblemis? Recommendation—Whatshouldwedoto correcttheproblem? 2. Theoncomingnurseisresponsibleforthenursing carerequiredonhisorhershift. a.StatusofIVsandamountoffluidtocount. b.Anyabnormalconditions(vitalsigns,pain, specialtreatments). c. Statusofclientwithregardtodiagnosis.For examples,cardiacclient—presenceorabsence ofchestpainanddysrhythmias;surgical client—voiding,incisionstatus;orthopedic client—circulationdistaltocastortraction. d.Psychosocialstatusoftheclient.
TEST ALERT: Provide and receive report on assigned clients.
✔
Legal documentsA. Client’smedicalrecordorchart.B. Advancemedicaldirective(AD):awrittendocument regardingaclient’sdesiresforprovisionofmedicalcare ifthatpersonisunabletomakehisorherownchoices ordecisions. a. Livingwill(naturaldeathact):awrittendocument describingtheclient’swishesandspecialinstruc- tionsregardinglifesupportmeasuresintheevent thattheclientisincapacitated. b. Medicalpowerofattorneyforhealthcare. (1) Identifiesthepersondesignatedbytheclient toensurethatpreviouslyagreedADsare carriedoutaccordingtotheclient’sdirection. (2) Identifiesthepersondesignatedtomake healthcaredecisionsfortheclientiftheclient isincapacitated. c. ADsmaybechangedorrevokedbytheclientatany time.
TEST ALERT: Provide information about advance directives (Ad).
C. Donotresuscitate(DNR)orders. 1. Writtenbythephysicianbasedontheclient’swrit- tenmedicaldirectives. 2. Nursesareobligatedtorespectandobservethe DNRorder. 3. Healthcarepersonnelshouldbeadvisedofthe DNRorder.
mANAgEmENT OF HEAlTH CARE WORkERs
A. Delegationistransferringtoacompetentindividualthe authoritytoperformaselectednursingtaskina selectedsituation,theprocessfordoingthework. Thenurseretainsaccountabilityforthedelegation, mostoftendelegationistheroleoftheRN.B. Assignmentdescribesthedistributionofworkthateach staffmemberistoaccomplishinagiventime.Toas- signistodirectanindividualtodoactivitieswithinan authorizedscopeofpractice.C. Supervisionistheprovisionofguidanceordirection, oversight,evaluationandfollow-upbythelicensed nursefortheaccomplishmentofanursingtask delegatedtonursingassistivepersonnel.(NCSBN, 2004).D. Roleofthepracticalnurse(PN)insupervision 1. ThePNshouldensuretheunlicensedassistive personal(UAP)understandstheassignedtask, andtheUAPshouldacknowledgetothePNthat he/sheunderstandsthedirections. 2. ThePNshouldmakeperiodiccheckstodetermine thattheUAPisperformingthetasksasdirected.

64 CHAPTER 3 Nursing Concepts
3. IftheUAPdoesnotcarryoutthetaskscorrectly, thePNshouldcorrecttheactioninatimelyprofes- sionalmanner.Iftheproblemisnotresolved,the RNshouldbenotified. 4. ThePNshouldassigntaskstotheUAPthatare clearlydefined,arewithintheexpectedexpertise oftheUAP,andhaveveryspecificguidelines:for example,bathing,ambulating,clienthygiene.
TEST ALERT: Make client care or related task assignment.
study Questions: Concepts of Nursing management
4. Thenurseenterstheclient’sroomanddiscoversthe clientonthefloorbesidethebed.Thesiderailsareup, andtheclientisconfusedanddisoriented.What informationwouldbeincludedinthenurse’sdocumen- tationintheincidentreport? 1 Uponenteringtheroom,Idiscoveredtheclienton theflooratthesideofthebed;thesiderailswere up. 2 Theclientfelloutofthebedafterthenursingassis- tanthadexplainedtohimtheimportanceofnot gettingup. 3 Theclientwasconfusedandapparentlytriedto climboutoverthesiderailsofthebed. 4 Evidentlythepreviousnursedidnotcheckonthe clienttoseethathewasconfused,andhefelloutof bed.5. Theolderadultclientisbeingdischargedwithapre- scriptionforhydrocodone(Vicodin)forpaincontrol. Whatinformationwillthenurseincludewhendiscuss- ingwiththeclientthepossibleadverseeffectsofthe medication? 1 Increaseintakeofbulkandfibertopreventconsti- pation. 2 Thepaincontrolcanbeincreasedbytakinganad- ditionalacetaminophen500mg. 3 Returntotheclinicforserumlabstudiestodeter- minetoxicitylevels. 4 Increasedbruisingmayoccurbecauseofchangesin theskin.
E. Prioritizingclientcareassignments. 1. Identifythemostillorunstableclientofyouras signedclients–evaluateandcareforthatclient first. 2. Physiologicalneedsarethepriority–educationand communicationneedscanusuallywaituntilthe physiologicalneedsaremet. 3. Initiallyreviewtheassignedclientlist–consider thereportreceivedoneachclient.Determinewhich clientneedsimmediatephysicalassistanceinorder tomaintainsafety.(Reviewprioritysettingin Chapter1).
TEST ALERT: Organize and prioritize care of assigned group of clients.
1. Bedrestisfrequentlyprescribedforclientswhohave hadabrainaccidentorstrokeuntiltheircondition stabilizes.Howcanthenurseavoidpotentialproblems? 1 Insertanindwellingcatheter 2 Helptheclientbathetwotimesdaily 3 Placetheclientonacirculatingairmattress 4 Developanactivityschedulewiththeclient2. Thenursebeginschartingonaclient’spaperchartand afterenteringdatadiscoversithasbeenwrittenon thewrongchart.Whatisthebestwaytocorrectthis error? 1 White-outthewronginformationandwriteoverit. 2 Recopythepagewiththeerrorsothatthechartwill beneat. 3 Drawastraightlinethroughtheerror,initial,and date. 4 Obliteratetheerrorsothatitwillnotbeconfusing.3. Aclientisnauseatedandhasvomitedalargeamount offoulsmellingdarkgreenbilefluidtwiceinthepast hour.Whatisthebestnursingaction? 1 Positiontheclientinasupinepositionandmaintain bedrest. 2 Placeclientonnothingbymouth(NPO)statusand notifythesupervisor. 3 Encourageclearliquidstohelpsettlethestomach. 4 Ambulateclienttostimulatedevelopmentofperi- stalsis.

CHAPTER 3 Nursing Concepts 65
6. Thenurseisexplainingtotheclienttheimportanceof voidingpriortosurgery.Whatwouldthenurseinclude inthisexplanation? 1 ItisimportanttohaveanaccurateaccountofI&O forthatday. 2 Voidingbeforesurgerywillreducetheriskof bladderpainduringsurgery. 3 Voidingpriortosurgerywillpromotethephysi- ologicalsafetyduringsurgery. 4 Priortosurgeryitisimportanttovoidtodecrease thepossibilityofinfection.7. Thenursehasbeenassignedan86-year-oldclientwho hassufferedastroke.Theclientisnotorientedtoper- son,place,ortimeandispullingathisIVcatheterand tryingtoclimboutofthebed.Thenursehasapplieda vestrestraintandbilateralsoftwristrestraints.Which ofthefollowingnursingactionswouldbeappropriate? Selectallthatapply:____ 1 Providefornutritionandeliminationneedsevery2
hours.____ 2 Obtainaphysicianordereveryshiftforcontinua-
tionofrestraints.____ 3 Securetherestraintstothesiderailsofthebed.____ 4 Tietherestraintsinquickreleaseknots.____ 5 Assessanddocumentbehaviorsthatrequirecontin-
ueduseofrestraints.8. Whatpotentialproblemshouldthepracticalnursean- ticipatewhentoomuchstrainisplacedonthesuture line? 1 Thrombosis. 2 Infection. 3 Evisceration. 4 Dehiscence.9. Postoperativepainandcancerpainmaybeconsidered predictable.Howcanthenurseincreasetheeffective- nessoftheanalgesics? 1 GivethemPRN. 2 Administeronceaday. 3 Planaround-the-clockdosing. 4 Administertwiceaday.10. Awoundisleftopenaftersurgeryandallowedtoheal fromtheinsidetotheoutside.Thisdescribeswhattype ofhealing? 1 Firstintention. 2 Secondintention. 3 Primaryhealing. 4 Superficialhealing.
11. Aclienthasexperiencedadehiscenceandthenurse placestheclientonbedrest.Whatisthepurposeofbed restforthisclient? 1 Todecreaseoxygenconsumption. 2 Toincreasethehealingofthesite. 3 Topreventdevelopmentofpneumonia. 4 Topreventtheoccurrenceofevisceration.12. Thenurseiscaringforanimmobilizedclient.What nursingmeasureisusedtopreventthecomplicationsof atelectasisandpneumonia? 1 Turn,cough,anddeepbreathe. 2 Rangeofmotionexercises. 3 Clearliquiddietwithfrequentsuctioningofsecre- tions. 4 Bedrestwithfrequentvitalsignmeasurements.13. Beforeasurgicalprocedure,thenurseasksaclientto signaninformedconsentform.Whatisimportantfor thenursetovalidatebeforetheclientsignsthisform? 1 Thephysicianhasdiscussedthesurgerywiththe client. 2 Theclientunderstandsthepostoperativenursing care. 3 Thephysicianhasdiscussedthepossiblecomplica- tions. 4 Theclientunderstandsthesurgeryandtherisks involved.14. Olderadultclientsareconsideredhighriskforrespira- toryproblemsbasedonproblemsofimmobilityand agingchanges.Whatarethesechangesrelatedto? 1 Decreasedlungexpansionandreducedbreathing capacity. 2 Increasedbreathingandlungcapacity. 3 Poorpostureanddecreasedsizeofchestcavity. 4 Increasedlungsizeanddecreasedtidalvolume.15. Withtheclientintheproneposition,whichbony prominenceswouldthenurseidentifyasbeingmost susceptibletoskinbreakdown? 1 Sacrumandelbows. 2 Shoulderareaandtrochanter. 3 Anterioriliacspinesandpatellae. 4 Trochanter.
Answers and rationales to these questions are in the section at the end of the book titled Chapter Study Questions: Answers and Rationales.

66 CHAPTER 3 Nursing Concepts
Continued
Appendix 3-1 POsitiONiNG ANd BOdy MECHANiCs
POsitiON PLACEMENt usEFowler’s
Semi-Fowler’s
Low Fowler’s
Lateral (side-lying)
Semi-prone (Sims’)
Lithotomy
Prone
Supine
Headofbedat45-to60-degreeangle;hipsflexed
Headofbedat30-to45-degreeangle;hipsflexed
Headofbedat15-to30-degreeangle;hipsmayormaynotbeflexed
Headofbedlowered;pillowsunderarmandlegsandbehindback;flexkneeofanteriorside
Headofbedlowered;clientplacedonsidewithdependentshoulderliftedoutandlyingpartiallyonabdomen;placepillowunderflexedarmandunderupperflexedknees
Onbackwiththighflexedagainstabdomenandlegssupportedbystirrups.
Headofbedflat,clientonabdomen,headturnedtoside
Bedinflatposition,smallpillowunderhead
Theheightmaybedeterminedbyclientprefer-enceortolerance;frequentlyusedforclientwithrespiratorycompromise.
Cardiac,respiratory,neurosurgicalconditions,orclientcomfort.
PostoperativeandclientswithGIproblems.
Forclientcomfort;increasesuterineandrenalperfusioninpregnancyandpreventssupinevenacavasyndromeduringlabor.
Preventspressureareas,usedforcomfort
Forgynecologicalexaminationandsurgicalproceduresintheperinealarea.
Usedtopromotedrainageafteroralsurgeryortonsillectomy;usedtopreventcontracturesinclientswithabove-the-kneeamputation.Positionwillprotectinfantwithimperforateanus,orspinabifida.
Forclientcomfort.
TEST ALERT: Position client to prevent complications after tests, treatments, or procedures.
BOdy MECHANiCs—PREvENtiON Of iNjuRyManualliftingofaclientshouldbeavoided.Ifitisnecessarytomanuallyliftmostoralloftheclient’sweight,obtainliftequipmentand askforadequateassistance.
Body mechanics: 1. Avoidtwistingyourbody;keepyourheadandneckalignedwithyourspine.2.Flexyourkneesandplaceyourfeetwideapartforgoodbaseofsupport.3. Positionyourselfclosetothebedorclosetotheclient.4.Usearmsandlegstoassistinliftingclient,notyourback.5.Usepullsheetorslideboardtomoveclienttosideofbedand/ortomoveupinbed.
4 key Points: Assisting the Client to move up in Bed• Lowertheheadofthebedsothatitisflatoraslowastheclientcantolerate;raisethebedframetoapositionthatdoesnotrequireleaning.• Ifmorethanonepersonisneededforassistance,obtainaliftingdevice.• Determinetheclient’sstrongsideandhavehimorherassistwiththemove.• Instructtheclienttobendlegs,putfeetflatonbed,andpush.• With2people,useadrawsheetoraliftsheet.• Neverpullaclientupinbedbyhisarmsorbyputtingpressureunderhisarms.
4 key Points: logrolling the Client• Spinalimmobilization—useateamapproach.• Maintainproperalignmentonheadandbackareaswhileturning.• Beforemovingpatient,placeapillowbetweenclient’sknees.• Moveclientinonecoordinatedmovement,usingaturn/liftsheet.
TEST ALERT: Use transfer assistance device (roller, client lifts).

CHAPTER 3 Nursing Concepts 67
Appendix 3-1 POsitiONiNG ANd BOdy MECHANiCs—cont’d.
4 key Points: moving from Bed to Chair• Moveclienttothesideofthebed(bedwheelslocked),closesttotheedgewheretheclientwillbegettingup,placeachairwith armsatbedside.• Planonassistingclienttogetoutofbedonhisstrongestside.• Raiseheadofbed,assistclienttosideofthebed.• Moveclienttoedgeofbedandplaceyourhandsunderclient’slegsandshifthisweightforward,pivottheclient’sbodysoheis sittingpositionandhisfeetareflatonthefloor.• Haveclientreachacrosschairandgraspthearmofthechair.• Stabilizeclientbypositioningyourfootattheoutsideedgeofclient’sfoot.• Pivotclientintochairusingyourlegmusclesinsteadofyourbackmuscles.• Assistclienttomovebackandupinthechairforbetterposition.
Tips for moving and Positioning Clients• Useaturnsheettoprovidemoresupportforclient.• Encourageclienttoassistinmovebyusingthesiderailsandstrongsideofhisorherbody.• No-liftpolicy:useliftequipmentandassistancewheneveraclientrequiresmostofhisweighttobesupportedorliftedbysomeone.• Usetrochanterrollmadefrombathblanketstoaligntheclient’shipstopreventexternalrotationwheninthesupineposition.• Usefoldedtowels,blankets,orsmallpillowstopositionclient’shandsandarmstopreventdependentedema.
TEST ALERT: Maintain correct body alignment.
Continued
Appendix 3-2 ANALGEsiCs
general Nursing implications• Assess client for pain parameters: blood pressure, pulse, and respiratory status before and periodically after administration.• Use a scale to determine level of pain. • For more effective analgesic effect, administer medication before pain is severe. • Older or debilitated clients may require decreased dosage.
Medications side Effects Nursing implications
Narcotic Analgesics:Bindtoreceptorsinthecentralnervoussystem(CNS),alteringtheperceptionofandemotionalresponsetopain.Con-trolledsubstances(ScheduleII).
StroNg opIoId ANAlgeSIcS
Morphine sulfate:PO,subQ,IM,IV,epiduralanalgesia
Meperidine(Demerol):PO,subQ,IM
Fentanyl(Fentanyl,Sublimaze,Duragesic):IM,IV,PO,transdermal
RespiratorydepressionOrthostatichypotensionSedation,dizziness,lightheadedness,IncreasedtendencyforseizuresConstipationTolerance,physicalandpsychologicaldependenceMaydecreaseawarenessofbladderstimuli
1.MorphineismostcommonlyusedforPCA.2.Demerol:Notcommonlyusedforcontrolofchronicpainduetoneurotoxiceffect;usewithcautioninchildrenandelderlyclientsbecauseofincreasedriskfortoxicityandseizures.3.Allopioids:Usewithcautioninclientswhohaverespiratorycompromise.4.Pediatricimplications:Medicationdosageiscalculatedaccordingtobodysurfaceareaandweight.
5.Assessvoidingandencourageclienttovoidevery4hours.6.RequiresdocumentationasindicatedbyControlledSubstanceAct.7.Instructclienttochangepositionslowlytominimizeorthostatichypotension.
NURSING PRIORITY: Advise clients using fentanyl patches not to expose patch to heat (hot tub, heating pad) since this will accelerate the release of the fentanyl.
✔OLdER AdULT PRIORITY:
Prevent problems with constipation, monitor respiratory status.
✔
HIGH
ALERT

68 CHAPTER 3 Nursing Concepts
Appendix 3-2 ANALGEsiCs—cont’d.
Medications side Effects Nursing implications
ModerAte opIoIdS
Butorphanol(Stadol):IM,IV,nasalsprayNalbuphine(Nubain):subQ,IV,IM
Dizziness,drowsiness 1.Monitorclientforeffectivepaincontrol.2.Abruptwithdrawalafterprolongedusemayproducesymptomsofwithdrawal.
NURSING PRIORITY: Pain will return when Narcan is administered.✔
NArcotIc ANtAgoNISt - Antagonistscompetitivelyblocktheeffectsofnarcoticswithoutproducinganalgesic.
Naloxone(Narcan):IV,IM,subQ
Hypotension,hypertension,dysrhythmias. 1.Assessrespiratorystatus,bloodpressure,pulse,andlevelofconsciousnessuntilnarcoticwearsoff.Repeatdosesmaybenecessaryifeffectofnarcoticoutlaststheeffectofthenarcoticantagonist.2.Rememberthatnarcoticantagonistsreverseanalgesiaalongwithrespiratorydepression.Titratedoseaccordinglyandmonitorpainlevel.3.Uses:UsedtoreverseCNSandrespiratorydepressioninnarcoticoverdose.4.Contraindications and precautions:Usewithcautioninnarcotic-dependentpatients;maycauseseverewithdrawalsymptoms.
CDC, Centers for Disease Control and Prevention; CNS, central nervous system; IM, intramuscularly; IV, intravenously; PCA, patient-controlled analgesia; PO, by mouth (orally); subQ, subcutaneously
ModerAte to StroNg opIoId ANAlgeSIcSCodeine:PO,subQ
Hydromorphone(Dilaudid):PO,subQ,IM,IV,suppository
Oxycodone(Percodan,combinationwithibuprofen;Percocet,Tyloxcombinationswithacetaminophen;OxyContin):PO
Hydrocodone(Vicodin,Lorcetcombinationswithacetaminophen;Vicoprofen,combinationwithibuprofen):PO
Propoxyphene(Darvon,Darvocet):PO
Sedation,euphoria,respiratorydepression,constipation,urinaryretention,coughsup-pression
1.Usuallyadministeredbymouth.2.Codeineisanextremelyeffectivecoughsuppressant.3.Donotconfusehydromorphonewithmorphine.4.Warnpatienttoavoidactivitiesrequiringalertnessuntileffectsofdrugareknown.5.Medicationsareofteninvariousstrengthcombinationswithacetaminophenand/oribuprofen
NURSING PRIORITY: Help client to identify OTC medications that contain acetaminophen or ibuprofen – increased risk of overdose if taken in addition to combination opiod analgesics.
✔
HIGH
ALERT