
Nucleic Acid Testing vs Infectivity Michael P. Busch, M.D., Ph.D. Blood Centers of the Pacific Blood...
46
Nucleic Acid Testing vs Infectivity Michael P. Busch, M.D., Ph.D. Blood Centers of the Pacific Blood Systems, Inc. EPFA, Lisbon Portugal May, 2001
-
Upload
lindsey-reed -
Category
Documents
-
view
216 -
download
2
Transcript of Nucleic Acid Testing vs Infectivity Michael P. Busch, M.D., Ph.D. Blood Centers of the Pacific Blood...

Nucleic Acid Testing vs Infectivity
Michael P. Busch, M.D., Ph.D.Blood Centers of the Pacific
Blood Systems, Inc.
EPFA, Lisbon PortugalMay, 2001

NAT vs Infectivity Overview of stages of infections and importance
of understanding stage-specific gEq:infectivity ratios (concentration vs volume infused)
Review of NA dynamics (pre/peri/post-SC) for HIV, HCV and HBV
Review infectivity data for each stage Need for future studies
animal transmission models lookback studies (NAT/SC donors; recipient cases)
Stages of TTVIs and infectivity
• Pre-ramp-up viremia• Ramp-up viremia• Plateau phase / peak viremia• Peri-SC viremia• Post-SC viremia
– Persistent carrier (viral load set point)– “Resolved” infection?
• Immunosilent carrier• Transient Viremia w/o SC
Stages of TTVIs and infectivity
• Pre-ramp-up Viremia– Low-level, intermittent “blips” of RNA/DNA detected
prior to quantifiable ramp-up phase
– Innoculum vs focal replication that seeds dissemination vs abortive replication
– Can this occur transiently w/o subsequent ramp-up/SC?
– Is this viremia infectious?
– Kinetic, viral sequencing & infectivity studies in progress

Testing Algorithm for HCV NAT-conversion Panels
Alpha Therapeutic / NGI screening(Antibody & 512 Pool PCR)
63 HCV NAT-conversion Panels ( 774 Donations )5 Control Panels ( 54 Donations )
dHCV TMA Testing
Quantitative Viral Load( Roche Monitor )
Intermittent Pre-Ramp-Up Viremia * in 25/41 (61%) panels >3 pre-r/u units Ramp-Up & Plateau Phase
Replicate dTMA ( x 3 ) & NGI UltraQual PCR Testing
* Ramp-Up = consistent RNA detection with progressive increase in viral load.

Low-Level Intermittent HCV ViremiaPreceding Ramp-Up Phase
Assay sensitivity (6 x 102)
-60 -40 -20 0 10 20
% d
TM
A P
osit
ive
(4 r
epli
cate
s)
Days Pre/Post 1st Quantitative RNA+ Donation
x103
x102
x104
x106
x105
x108
HC
V M
onitor PC
R (gE
q/mL
)
100
50
75
25
NGI512 PCR
Neat PCR
x107
(BCP ID 10083)

Representative HIV Conversion Panels with Pre-Ramp-Up “Blip” Viremia
(RNA “blip” observed in 7/19 informative panels)
Days from First MP-PCR+ Test
p24 Ag HIV-1 Ab
HIV-1 RNA (copies / mL)
# Pos /
# Replicate PCR
- 21 Neg Neg < 100 1 / 10
- 19 Neg Neg < 100 7 / 8
- 14 Neg Neg < 100 0 / 8
- 11 Neg Neg < 100 0 / 8
- 7 Neg Neg < 100 0 / 8
- 4 Neg Neg < 100 3 / 8
0 Neg Neg 260 5 / 5
3 Neg Neg 27,000
7 Pos Neg 370,000
9 Pos Neg 2,800,000
16 Pos REACT 410,000
Alpha / BCP Case 1012

10
100
1,000
10,000
100,000
1,000,000
-37-35-29-26-21-18-11 -8 0 3 8
0.00
20.00
40.00
60.00
80.00
100.00
120.00
140.00
HB
V D
NA
Loa
d (
gEq
/mL
)Representative HBV Panel with Pre-Ramp-Up Viremia Representative HBV Panel with Pre-Ramp-Up Viremia
(pre-ramp-up viremia observed in 12/23 informative panels)(pre-ramp-up viremia observed in 12/23 informative panels)H
BsA
g S/C
Day from 1st + HBsAg test
Pre-Ramp-Up Ramp-Up
+ -

Stages of TTVIs and Infectivity
• Ramp-up viremia– Persistent viremia with progressive increase in
viral load leading to peak or plateau viremia – Doubling time used to project WP differences
of ID-NAT, MP-NAT and Ag assays– Presumed infectious (chimp study in progress)
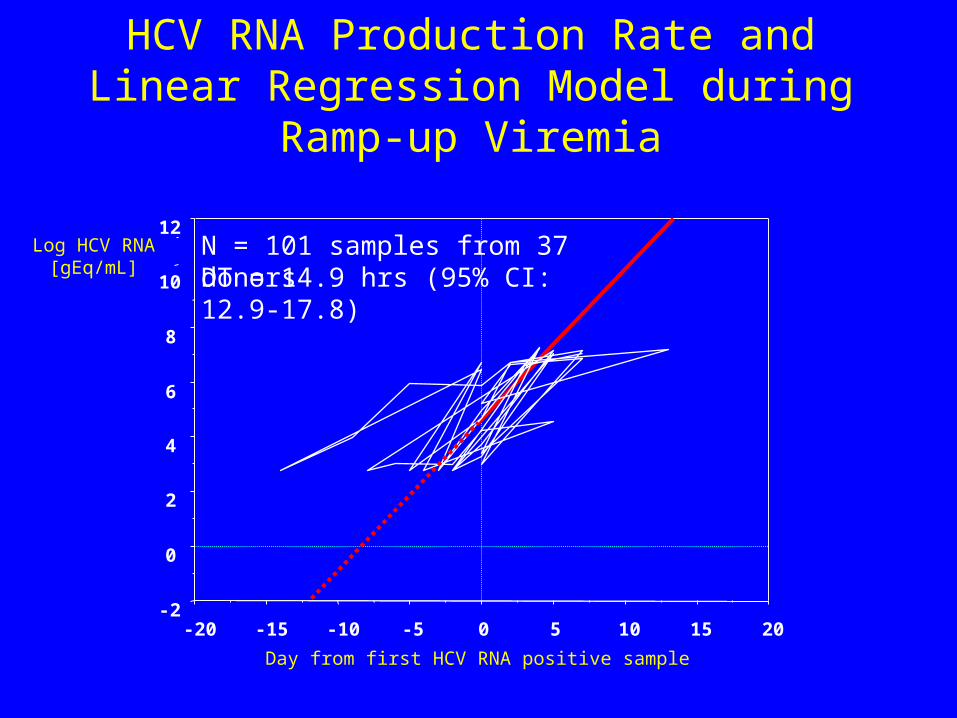
HCV RNA Production Rate and Linear Regression Model during Ramp-up Viremia
-2
0
2
4
6
8
10
12
-20 -15 -10 -5 0 5 10 15 20
Day from first HCV RNA positive sample
N = 101 samples from 37 donorsLog HCV RNA[gEq/mL] DT = 14.9 hrs (95% CI: 12.9-17.8)
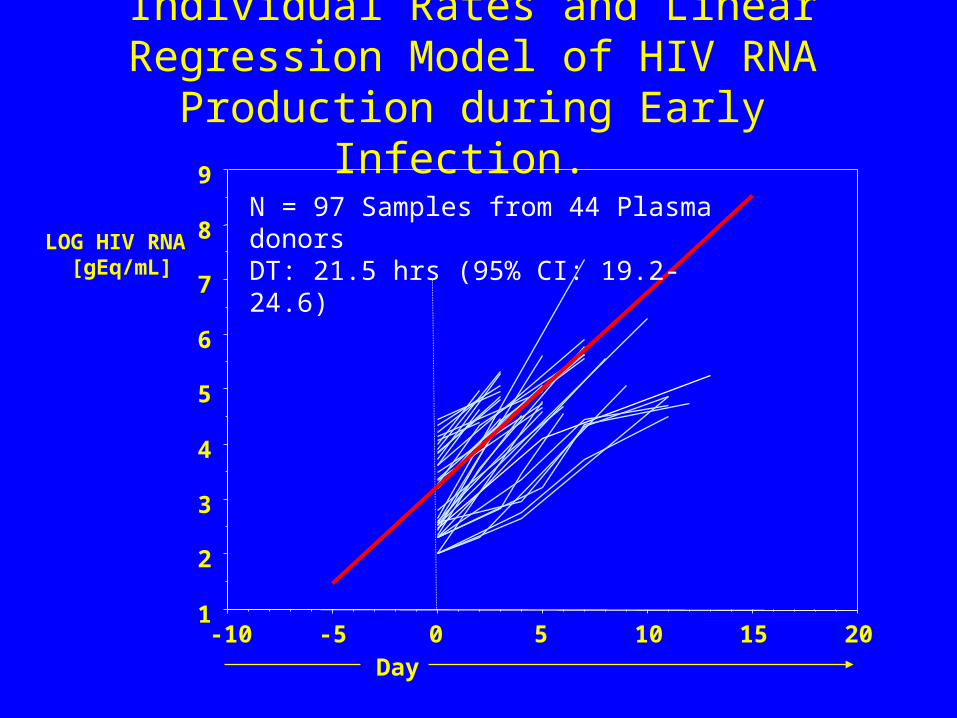
Individual Rates and Linear Regression Model of HIV RNA Production during Early Infection.
LOG HIV RNA [gEq/mL]
1
2
3
4
5
6
7
8
9
-10 -5 0 5 10 15 20Day
N = 97 Samples from 44 Plasma donorsDT: 21.5 hrs (95% CI: 19.2-24.6)

Individual Rates and Linear Regression Model of HBV DNA Production during Early HBV Infection
0
1
2
3
4
5
6
7
8
-60 -50 -40 -30 -20 -10 0 10 20 30
Day from first HBsAg positive sample
Log HBV DNA[gEq/mL]
N = 70 samples from 21donorsDT: 2.6 days (95% CI: 2.6-3.2)

Window Period Viremia Parameters Derived from NAT Analysis of
Plasma Donor Panels
Virus N High-Titer Plateau Phase
Ramp-up Phase Doubling Time
pre-Ramp-up Viremia
HIV 43 N.A. 21.5 hrs (19.2-24.6) 7 / 19
HCV 63 57 days * 17.7 hrs (17.1-18.3) 25 / 41
HBV 23 N.A. 2.8 days (2.6-3.2) 12 / 23
* Based on follow-up of 30 plasma donors detected as MP-NAT-pos by Alpha and Bayer (95% CI 29-85 days)
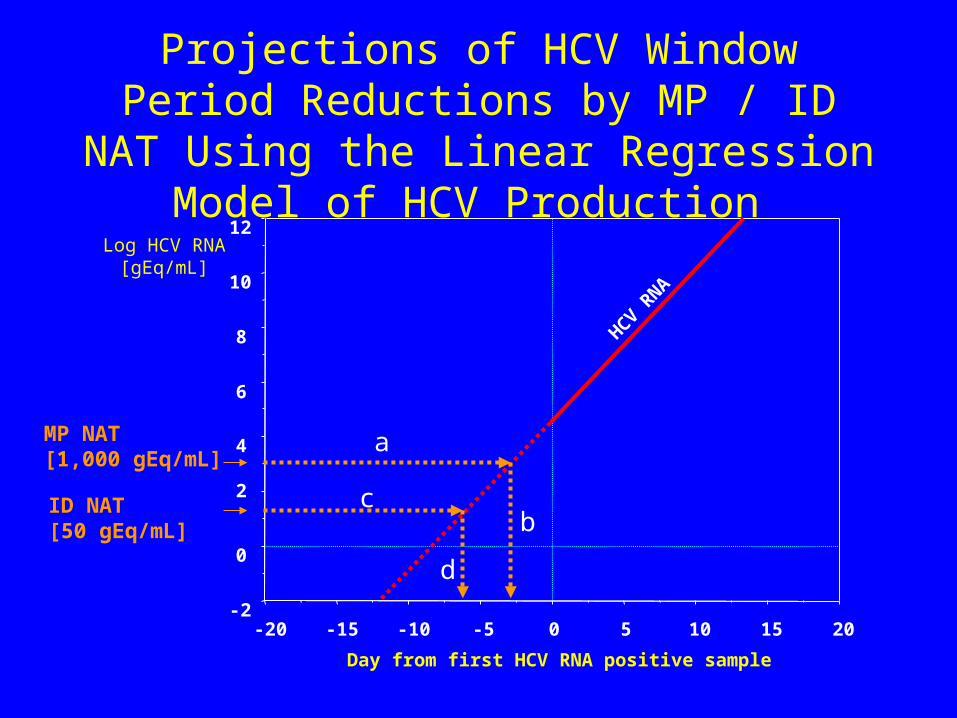
Projections of HCV Window Period Reductions by MP / ID NAT Using the Linear
Regression Model of HCV Production
-2
0
2
4
6
8
10
12
-20 -15 -10 -5 0 5 10 15 20
Day from first HCV RNA positive sample
Log HCV RNA[gEq/mL]
MP NAT[1,000 gEq/mL]
ID NAT[50 gEq/mL]
a
bc
dHCV R
NA
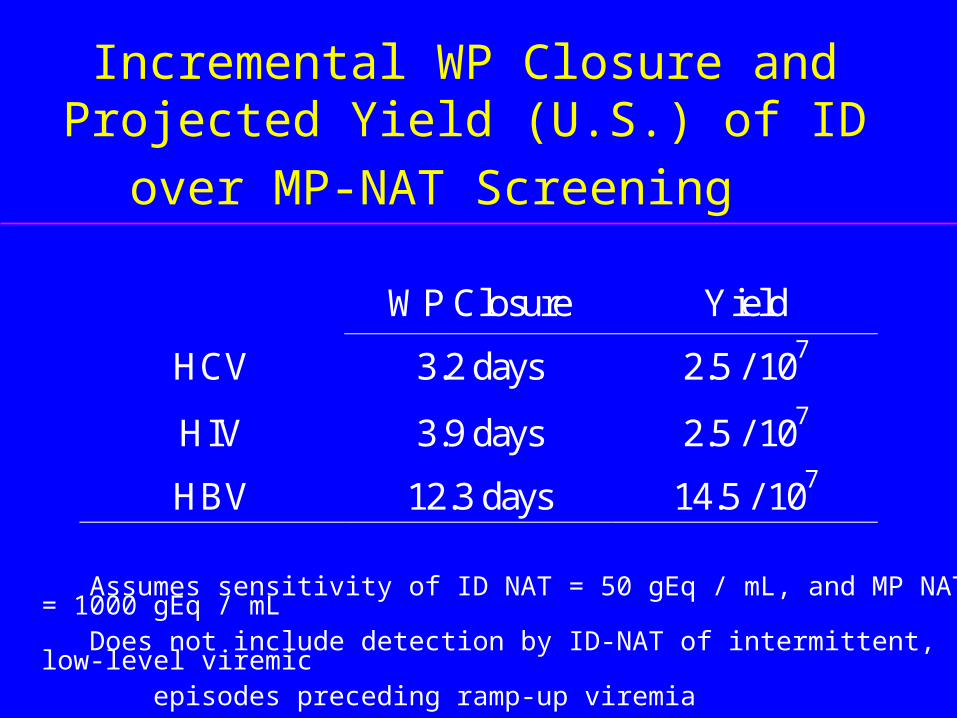
Incremental WP Closure and Projected Yield
(U.S.) of ID over MP-NAT Screening
WP Closure Yield
HCV 3.2 days 2.5 / 107
HIV 3.9 days 2.5 / 107
HBV 12.3 days 14.5 / 107
Assumes sensitivity of ID NAT = 50 gEq / mL, and MP NAT = 1000 gEq / mL Does not include detection by ID-NAT of intermittent, low-level viremic episodes preceding ramp-up viremia

Detection of HIV in antibody negative
window phase
1
10
100
1000
10000
100000
1000000
-4 -3 -2 -1 0 1 2 3 4 5 6 7 8 9 10 11 12
geq/ml
Days
infectious window
NucliSens-Ampliscreen 1:48
TMA single
TMA 1:16
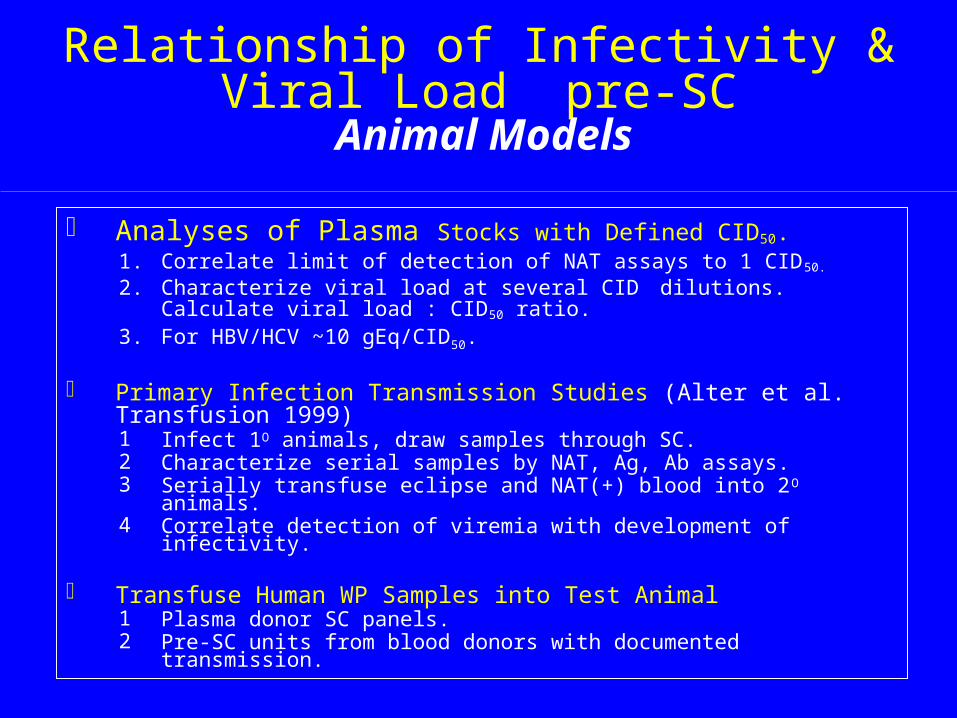
Relationship of Infectivity & Viral Load pre-SC Animal Models
Analyses of Plasma Stocks with Defined CID50.1. Correlate limit of detection of NAT assays to 1 CID50. 2. Characterize viral load at several CID dilutions. Calculate viral load :
CID50 ratio. 3. For HBV/HCV ~10 gEq/CID50.
Primary Infection Transmission Studies (Alter et al. Transfusion 1999)1 Infect 1O animals, draw samples through SC.2 Characterize serial samples by NAT, Ag, Ab assays.3 Serially transfuse eclipse and NAT(+) blood into 2O animals. 4 Correlate detection of viremia with development of infectivity.
Transfuse Human WP Samples into Test Animal1 Plasma donor SC panels.2 Pre-SC units from blood donors with documented transmission.
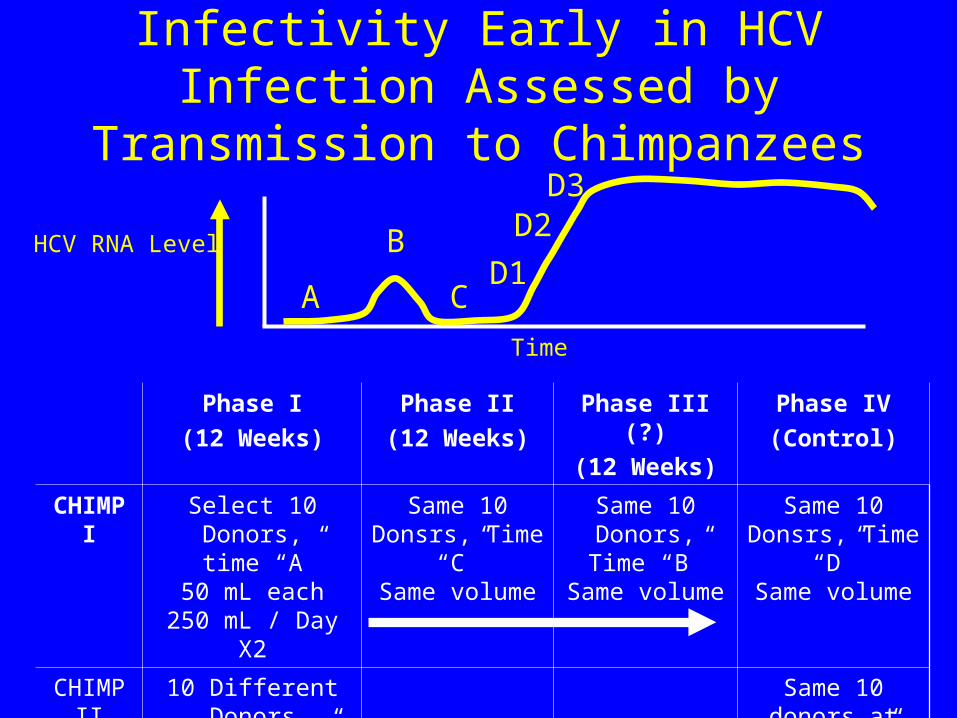
Infectivity Early in HCV Infection Assessed by Transmission to Chimpanzees
Phase I
(12 Weeks)
Phase II
(12 Weeks)
Phase III (?)
(12 Weeks)
Phase IV
(Control)
CHIMP I
Select 10 Donors, time “A”
50 mL each250 mL / Day X2
Same 10 Donsrs, Time
“C”Same volume
Same 10 Donors, Time
“B”Same volume
Same 10 Donsrs, Time
“D”Same volume
CHIMP II
10 Different Donors
with no “B” peak at time “C”
Same 10 donors at time
“D”
HCV RNA Level
A C
B
D3D2D
1Time

Relationship of Infectivity & Viral Load pre-SC Human Transmission Data
1. Investigate Recipients of Prior Donations by NAT / Ab SC Donors (Donor directed lookback)
Model Duration of "Infectious WP" Based on Rate of Recipient Infection Relative to ID Intervals
Petersen, et al. Transfusion 1993;33:552-7 For Cases with Documented Transmission and Available Plasma,
Characterize Viral Load and Detection by MP/SD NAT TestsSchttler, et al. Lancet 2000Robbins, et al. JAMA 2000Roth, et al. submitted
Transfuse human infectious plasma with low viral load into animals to validate sensitivity of the models

HIV Test Results for Donor, Recipients in Singapore Transmission Case
Robbins, et al. JAMA, 2000
Patient CollectionDate
HIVCopies / mL
HIVAb
p24Ag
AmplicorQuan.
NucliSensQuan.
NucliSensQual.
RT-PCRQual.
6 / 97 5 - 39 - - - - + +
10 / 31 / 97 16,000 + nd nd + nd +
10 / 28 /97 2,800 + nd nd + nd +
10 / 3 / 97 13,000 + nd nd + nd +
BD = Blood Donor; PR = Platelet Recipient; RBCR = Red Blood Cell Recipient
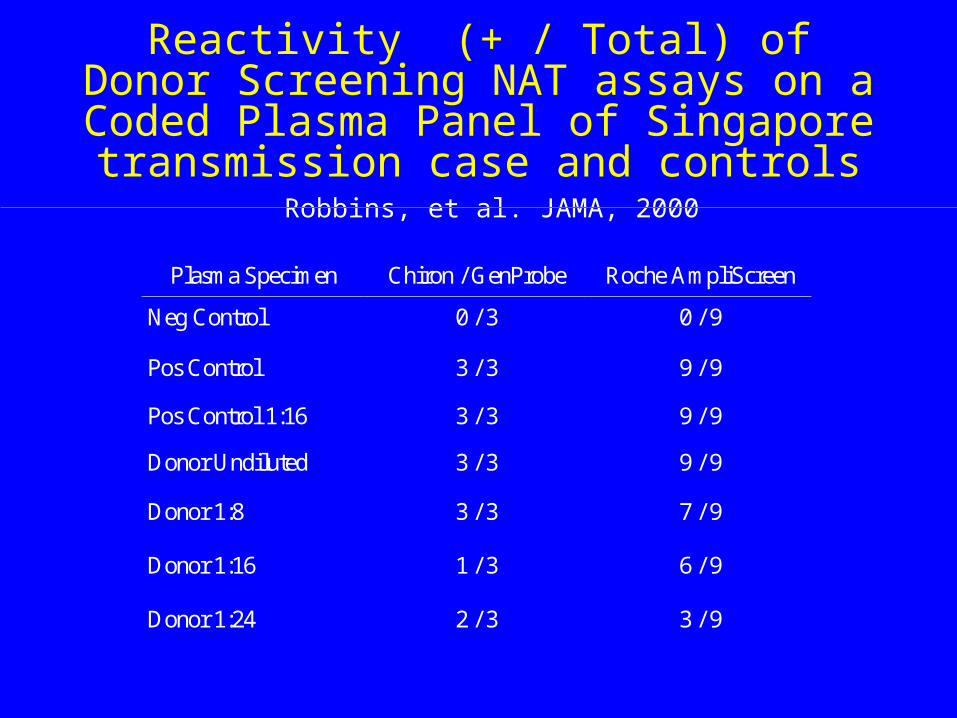
Reactivity (+ / Total) of Donor Screening NAT assays on a Coded Plasma Panel of Singapore transmission case and controls
Robbins, et al. JAMA, 2000
Plasma Specimen Chiron / GenProbe Roche AmpliScreen
Neg Control 0 / 3 0 / 9
Pos Control 3 / 3 9 / 9
Pos Control 1:16 3 / 3 9 / 9
Donor Undiluted 3 / 3 9 / 9
Donor 1:8
Donor 1:16
Donor 1:24
3 / 3
1 / 3
2 / 3
7 / 9
6 / 9
3 / 9
HCV Transmission by Blood Donation Negative by NAT
Schüttler CG, et al. Lancet 2000; 355:41-2
• Donation 8 weeks prior to SC donation
• HCV transmission by platelet concentrate (~50mL plasma) but not RBC (~5mL plasma)
• NAT studies of FFP, incl. “enhanced input” PCR assays, negative for HCV RNA
• Conclusion: “Even a negative NAT test cannot completely prevent transmission of HCV.”

HCV Transmission by Blood Donation Negative by NAT Schüttler CG, et al. Lancet 2000; 355:41-2
Follow-up study in collaboration w/ Dr. Gerlich
• Coded panel with 3 aliquots (2.5 mL) of implicated plasma and 2 positive (low-level HCV RNA ramp-up) and 1 negative controls.
• GenProbe, NGI
• Controls correctly identified by both assays
• GenProbe HCV dTMA (+) in 2 of 3 replicates; NGI Ultraqual PCR (-) on all 3 replicates
• Sequencing and chimp transmission studies in progress

Donor directed lookback studies from NAT+/SC donors
Roth et al. Lancet (submitted)
Virus # units/recips evaluated
# units/ recipients infected
HCV 22 0
HIV 11 0
HBV 13 0
Relationship of Infectivity & Viral Load pre-SC
Human Transmission Data
2. Investigate Donors to Recipients with reported post-transfusion infections (Recipient traceback)
Retest stored aliquots of donation plasma Recall implicated donors Perform sequencing/phylogenetic analysis to
confirm linkage

Analysis of Reported Post-Tx Cases in Japan Matsumoto et al. Transfusion 2001
• 141 “TA-HBV” cases reported ’97-99– 103 fully investigated: donation samples & f/u available– 15 HBV DNA(+) donations linked to 14 cases
• 9 WP units - donors SC to anti-HBc/anti-HBc on f/u– 5 tested HBsAg EIA+, all w/ >4,000 gEq/mL
• 2 units anti-HBc+ at donation and f/u• 3 low-level HBV DNA(+) donations w/ HBV(-) donors on f/u
– 1 case w/ 43 HBV DNA- donations, 1 donor SCd on f/u
• 92 reported “TA-HCV” cases: all donations NAT(-) and all donors (-) on f/u
• 0 cases of “TA-HIV” reported

Stages of TTVIs and infectivity
• Plateau phase (HCV)– Prolonged, stable high-titer viremia preceding SC
– Minor fluctuations in viral load may reflect host cell capacity to support viral replication
• Peak viremia (HIV & HBV)– Rapid rise then fall in viral load corresponding to
immune control and clearance of virus
– Results in clearance or post-SC steady state viremia

Stages of TTVIs and infectivity
• Peri-SC phase– cellular and humoral immune response results
in down-modulation of viral production and, in some cases, clearance
– Smooth decline in viral load to clearance or steady state viremia in most cases
– Some cases evidence marked fluctuation in viremia including intermittent neg-pos ID NAT results
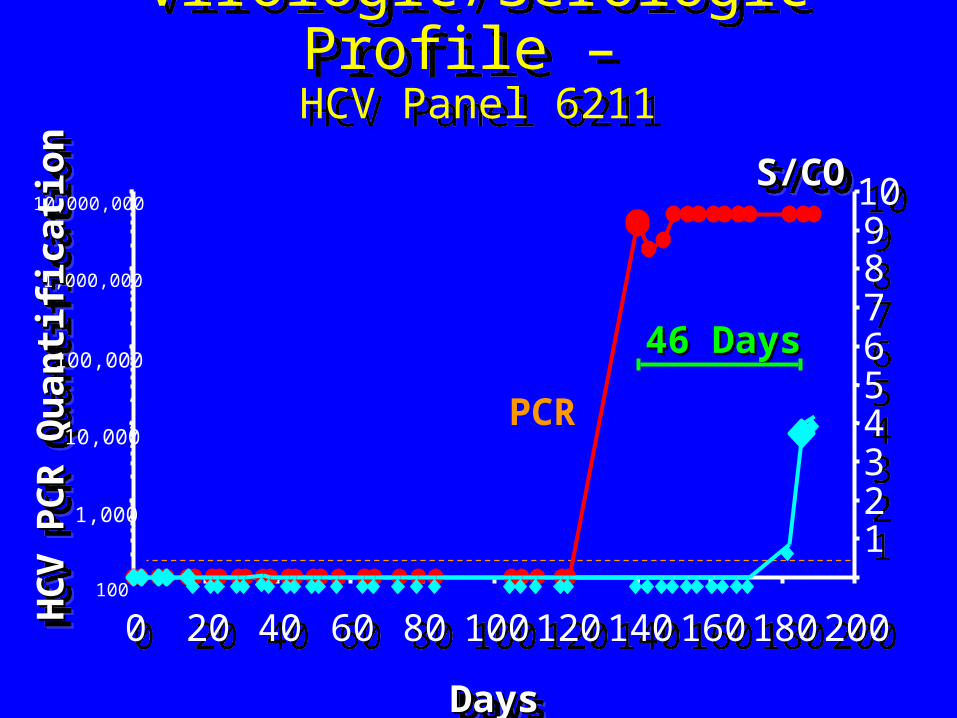
Virologic/Serologic Profile – HCV Panel 6211
Virologic/Serologic Profile – HCV Panel 6211
DaysDaysDaysDays
S/COS/COS/COS/CO
HC
V P
CR
Qu
anti
fica
tio
nH
CV
PC
R Q
uan
tifi
cati
on
HC
V P
CR
Qu
anti
fica
tio
nH
CV
PC
R Q
uan
tifi
cati
on
46 Days46 Days
100
1,000
10,000
100,000
1,000,000
10,000,000
00 2020 4040 6060 8080 100100 120120 140140 160160 180180 200200
1122334455667788991010
PCR

Time to Detection of Transfusion-Transmitted HCV Infection by Test
RNA
0
.2
.4
.6
.8
1
Cum
. S
urvi
val
0 20 40 60 80 100 120 140 160Days post-transfusion
EIA 3.0
ALT
Time to Mean 95% CIRNA 12.6 1.5-23.7ALT 51.5 18.5-84.5EIA3.0 70.7 32.8-128.6

HEPATOLOGY Vol. 29, No. 3, 1999

HCV NAT-Positive Donor HCV NAT-Positive Donor with fluctuating viremia during plateau-SC phase
0
250
500
750
1,000
1,250
1,500
0 30 60 90 120
ALT
0
5
10
15
20
25
30
(S/CO)
-147
102
103
104
105
106
-365
Viral load
RIBA – – – – – – Ind Ind + +
ALT
TMA
EIA
Viralload
Stages of TTVIs and infectivity
• Immunosilent carriers– Persistent viremia in absence of detectable SC
• Case reports for HIV, HCV and HBV• Recipient infection documented for HCV
– Durand et al. Ann Intern Med 2000– Peoples et al. Transfusion 2000
• Transient Viremia without SC– Confirmed by alternate sample and f/u with serotyping– Frequency in HR populations detectable by high
sensitivity NAT is now under study.

0 25 50 75 100
125
150
175
200
225
250
275
300
325
350
375
400
425
450
475
500
525
550
575
600
CP9TN78
TN104CP3
TN107TN49
TN113TN31TN90TN71
TN119TN110TN33CP8
TN69TN123TN95
TN120TN80TN83TN91TN43CP2
TN136TN27TN29
Seroreactive
Seronegative
Seroreactive, NAT Negative
Seronegative, NAT Negative
ARC HCV NAT Reactive Donations Confirmed with Follow up Sample(s) N = 25
Number of Days

Stages of TTVIs and infectivity
• Post-SC– Chronic seropositive carrier state
• Set-point viral load (NA vs Ag levels)• Variable infectivity to NA/Ag ratio
– Defective viral particles– Excess Ag production– Neutralizing Ab– Impact of unit storage and recipient susceptibility
– “Resolved” infection • Sensitivity of NAT vs infectivity in blood?• Persistence of infections virus in liver or other tissues• Waning Ab titers w/ persistent cellular immune responses

Rate of HCV Viremia (dHCV TMA) among Seropositive Subjects with Divergent Risk
Factors and Immune Status
Study Category Sero+
No.
RNA -pos
No. ( % )
ARC Donors 4,565 3,653 (80%)
BSI Donors 1,514 1,193 (79%)
UHS IVDU 300 255 (85%)
VATS HIV+ Patients
112 93 (83%)

Systematic Review of Role of Polymerase Chain Reaction in Defining Infectiousness
among People Infected with Hepatitis C VirusDore GJ, Kaldor JM, McCaughan GW
Br Med J 1997; 315:333-7
•2022 people exposed to anti-HCV(+) sources•1148 exposed to PCR(+) sources: 148
transmissions•874 exposed to sources (-) for HCV: 0
transmissions•Transmission rates after:
•Perinatal exposure 6.2%
•Needlestick 6.1%
•Solid organ / bone marrow transplantation 78%
•Blood components 88%
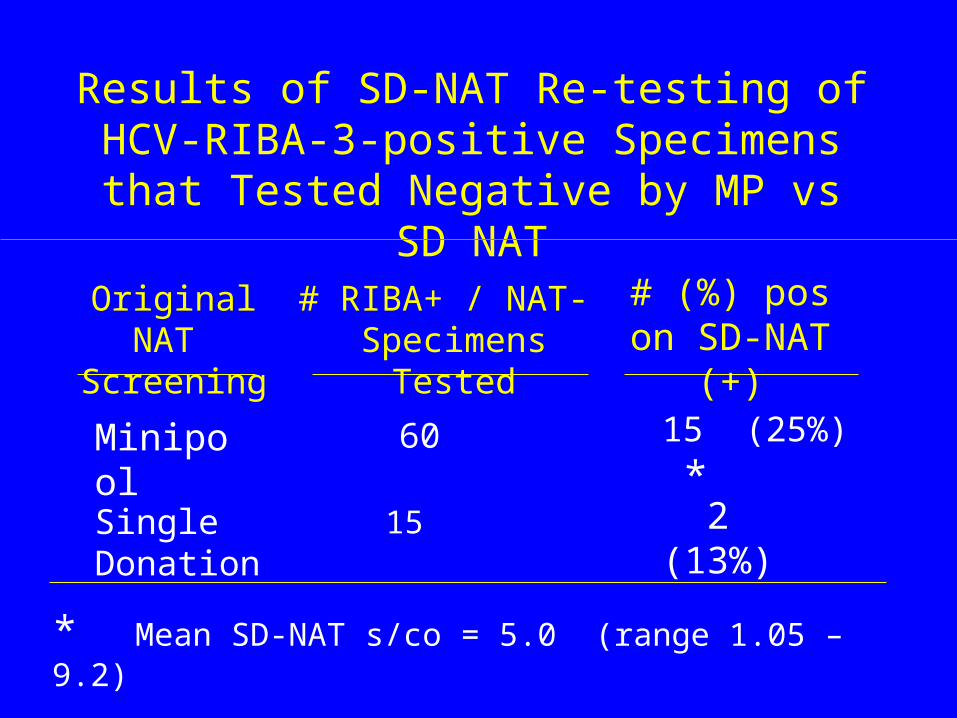
Results of SD-NAT Re-testing ofHCV-RIBA-3-positive Specimens that Tested Negative by MP vs SD NAT
Original NAT Screening
# RIBA+ / NAT- Specimens Tested
# (%) pos on SD-NAT (+)
Minipool
Single Donation
60
15
15 (25%) *
2 (13%)
* Mean SD-NAT s/co = 5.0 (range 1.05 – 9.2)

HCV viral load in anti-HCV+ donors and outcome in recipients
Operskalski et al. AABB 2001
Donation HCV
RNA level
# recipients
exposed
# (%) recipients
infected
Neg (<102.2) 15 6 (40%)
102.2 – 103.9 18 15 (83%)
104.0 – 106.3 53 49 (92%)

Correlation of HIV NAT withSupplemental HIV Serological Data
ARC 09/08/99 – 08/31/0009/08/99 – 08/31/00
Western Blot ResultNATResult
Pos
Neg
Total
Pos Ind Neg
213(94%)
13
226(5.6%)
38
1,901
1,939
21
1,856
1,877
(1.5%)
Total
272
3,770
4,042

Characteristics of WB Pos/TMA Neg Samples identified by ARC NAT Screening
All samples p24 Ag negativeAll samples p24 Ag negative
Sample Pool Neat HIV-1/HIV-2 WB HIV PCR
1 NR 1.43 41, 120, 160 Neg
2 NR 1.03 41, 160 Neg
3 NR 1.62 41, 160 Neg
4 NR 1.11 41, 55, 160 Neg
5 NR 2.50 24, 41, 51, 61, 160 Neg
6 NR 20.18 all bands Neg
7 NR 1.22 24, 41, 160 Neg
8 NR 1.11 17, 41, 120, 160 Neg
9 NR 1.84 41, 160 Neg
10 NR 1.40 24, 41, 160 Neg
11 NR 1.70 17, 24, 41, 51, 160 Neg
12 NR 20.00 all bands Pos (200 copies/mL)
13 NR 17.84 all bands Neg
09/08/99 – 08/31/0009/08/99 – 08/31/00

HIV-1 Transmission vs RNA Load and Storage
0 10
30
50
1
2
3
4
5
6 RBC (+)
RBC (–)
Platelets (+)
FFP (+)
FFP (–)
Days to Administration HIV
-1 R
NA
Load (
Log
10)
Cop
ies/
mL
Busch et al. JID 1994

HBV DNA Detection in anti-HBc+HBsAg- US blood donations
Kleinman et al. AABB 2001• 5121 anti-HBc-only donations from 5 REDS sites
tested• 1231 anti-HBc+, anti-HBs <100 IU/mL by Prism• 395 rep samples screened by PCR (<10 IU/mL) w/
confirmation by 2 PCR assays on sep aliquot• 4 HBV DNA+ detected (4/107 anti-HBs-neg)
– HBV DNA load 10-100 copies/mL
• Project 1 HBV DNA+ per 48,955 Tx units, similar to projected yield of HBV DNA+ pre-HBsAgWP units

Infectivity of HBV DNA PCR+, HBsAg-, anti-HBc+ blood
Prince et al. Transfusion 2001
• 3 patients sampled 25-30 years post acute HBV
• HBsAg-/anti-HBc+/anti-HBs+• HBV DNA+ w/ 200-1300 copies/mL• 1.35 mL serum + 2-4 x 107 PBMC
inoculated• Chimps monitored 15 months • All chimps neg for HBsAg, HBV DNA, etc.

Infectivity of HBsAg (-) Hepatic Allografts with Antibodies to HBV
Dodson, et al. Transplantation 1997;64:1582-4
Donor Recipient N InfectedN (%)
anti-HBc
anti-HBs
anti-HBc
anti-HBs
- + - - 25 0
+ - - - 25 18* (72%)
+ - - + 7 0
+ - + - 15 2* 4/18 transmitting donors had low-titer anti-HBs

Conclusions
Relationship between infectious units and RNA/DNA levels varies by stage of infection
During primary (pre-SC) infection, 1-10 gEq/mL plasma appears able to transmit infection
Ab+/NAT- donations must be presumed infectious (can’t d/c serology or reenter donors)
Need for future studies at international level1. animal transmission model systems2. donor lookback studies (prior units from NAT+ and Ab
SC donors)3. investigation of donors in TA-recipient infections


















