
Lesioni cistiche pancreatiche: linee guida diagnostiche - Gastrolearning®

Pietro Maggi
MD, PhD
ECTRIMS Fellowship
Novità diagnostiche nella Sclerosi Multipla
Florence, April 8 2018

MS diagnostic criteria
McDonald et al. Annals of Neurology 2001
Schumacher et al. Annals New York Academy of Sciences 1965
• “On neurologic examination there must be evidence of involvement of 2 or more separate parts of the CNS”
• “The involvement of neuraxis must have occurred temporally…in two or more episodes of worsening ”
Polman et al. Annals of Neurology 2011
Reich D.S. et al. NEJM 2018Thompson et al. Lancet Neurology 2018
Magnetic Resonance Imaging can substitute for clinical findings in the determination of DIS and DIT in patient with a typical CIS.

MRI red flags: features atypical for MS but instead suggestive of an alternative diagnosis

Solomon A.J et al. Neurology 2016; 87:1393-1399

Phase@CHUVT2* MagFLAIR* @CHUV FLAIR* MRI in a patient with MS and systemic sarcoidosis

Imaging parenchymal veins in MS
Image courtesy of Martina Absinta (NIH)
The presence of a central vein within the
lesion is a pathological hallmark of MS
100um
LFB-PAS

1. Absinta M. et al. Nature Review Neurology
• The perivenular topography of MS lesions has been recently visualized in vivo using susceptibility based MRI at high field strength1: Magnitude T2* and Phase
• T2* relaxation: combination of “true T2 relaxation” and relaxation caused by magnetic field inhomogeneities2
• Due to the deoxyhemoglobin (paramagnetic molecule), central veins appear prominent within MS lesions.
2. Cavhan GB et al. Radiographics, RSNA 2009
• The susceptibility effect is more important at
higher field strength (3T & 7T)
Image courtesy of Dr Pascal Sati NINDS, NIH
Imaging parenchymal veins in MS

• Recently, the combination of FLAIR and T2*, so called FLAIR* image, allows to achieve an excellent lesion/WM contrast (FLAIR) and vein detection (T2*)
Sati et al. Radiology, 265 (2012) 926-932.
Images courtesy of Dr. Daniel Reich and Pascal Sati Translational Neuroradiology Unit, NIB, NINDS, NIH –Bethesda US
Imaging parenchymal veins in MS

FLAIR* @Lausanne University Hospital

Published 11 Nov
2016
Consensus criteria of the NAIMS cooperative

Consensus criteria of the NAIMS cooperative
• Individuals with cerebral small vessel disease, migraine, AQP4-IgG-positive NMOSD, Susac syndrome have a significantly lower proportion of brain lesions with a central vein compared to MS.
The central vein in other diseases:
• Other MRI mimics of MS, such as SAD, neurosarcoidosis and Sjogrensyndrome, should also be investigated.
Sati et al. Nature Review Neurology 2016
Mistry et al. MS Journal 2016
Tallantyre et al. Neurology 2011
Mistry et al. JAMA Neurology 2013
Accepted for publication in the Annals of Neurology on January 8, 2018

Multiple Sclerosis:
Background
Recurrent focal neurological symptoms associated to focal CNS lesions
Sagittal
Coronal
Image courtesy of Dr. Martina Absinta (NIH, 2016)
FLAIR* MRI @3Tesla
CNS vasculitis:
Neurological presentation variable & non-specificPossible recurrent focal neurological symptoms Possible association to focal CNS lesions
Giannini et Al. Acta Neuropathologica 2012
FLAIR* MRI @3Tesla
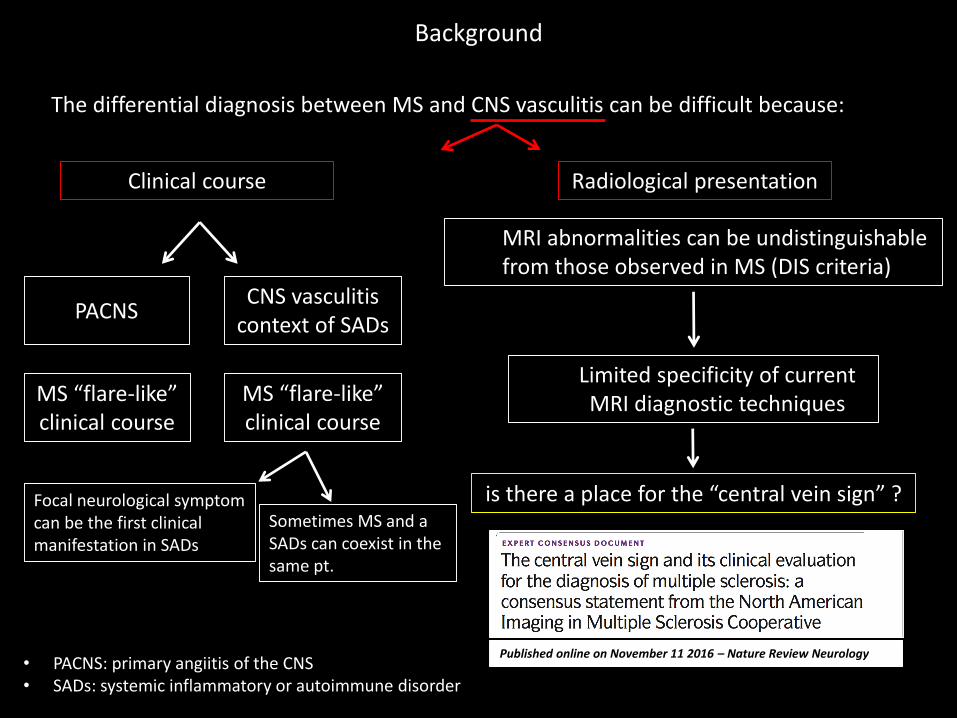
Background
The differential diagnosis between MS and CNS vasculitis can be difficult because:
Focal neurological symptom can be the first clinical manifestation in SADs
Sometimes MS and a SADs can coexist in the same pt.
Limited specificity of current MRI diagnostic techniques
Published online on November 11 2016 – Nature Review Neurology
is there a place for the “central vein sign” ?
CNS vasculitis context of SADs
MS “flare-like” clinical course
Clinical course Radiological presentation
MRI abnormalities can be undistinguishable from those observed in MS (DIS criteria)
PACNS
MS “flare-like” clinical course
• PACNS: primary angiitis of the CNS• SADs: systemic inflammatory or autoimmune disorder

83 patients were included in this study:
Patients and Methods
31 patients with systemic autoimmune disease and clinical/MRI evidence of brain involvement or with PACNS (“inflammatory vasculopathies”)
52 patients with RRMSaccording to McDonald’s criteria
Patients where recruited from: • the Careggi Hospital (Florence)• the Erasme Hospital (Brussels)• the San Raffaele Hospital (Milan)
vasculitis patients: • 9 patients with SLE• 7 patients with APS• 10 patients with Behçet disease• 2 patients with Sjögren Disease• 3 patients with PACNS
Post processing:T2*w EPI FLAIR
FLAIR*
MRI scanners:• 3T Philips Intera MRI scanners (Brussels and Milan) • 1.5T Philips Achieva MRI scanner in Florence.
MRI acquisition protocol :• 3D T2*-w EPI images acquired during Gd injection• and 3D T2-FLAIR images acquired after Gd injection
MRI acquisition and image post-processing:
Sati P et al. Nature reviews Neurology. 2016;12(12):714-22. Sati P et al. Radiology. 2012;265(3):926-32.

“central vein” assessment on FLAIR* images: MS vs. SADs with CNS involvment
Multiple Sclerosis Sjögren disease
APS SLE
Axial
Sagittal
Axial
Sagittal
Axial
Coronal
Axial
Coronal
Coronal Coronal
Sagittal Sagittal

Results: “central vein” assessment
Central vein sign assessment
Vasculitis MS
% p
eri
venula
rle
sio
ns
leukocortical/cortical lesions *
subcortical/deep WM lesions *periventricular lesions *
infratentorial lesions *
Vasculitis MS
13%
69%
20%
14%
32%
41%
7%
* Mann-Whitney p£0.001
3%
Vasculitis MS
Juxtacortical/ leukocortical lesions *
Subcortical/deep white matter lesions *
Periventricular lesions *
Infratentorial lesions *
Topographical distribution of brain lesions
vascu
litis MS
0
20
40
60
80
100
% p
erive
nula
r le
sions
% p
eri
venula
rle
sio
ns
APS
SLE
Sjögr
en
Behçet
PACN
S MS
0
20
40
60
80
100
% p
erive
nula
r le
sions
• The percentage of perivenular lesions was significantly higher in MS vs. vasculitis (p<0.0001)
• Among vasculitides, Behçet disease showed the highest percentage of perivenular lesions
• The separation between the two groups was complete when “50% rule” is applied.
• The frequency of perivenular lesions did not differ significantly between 1.5T and 3T MRI
88%
14%
Tallantyre EC et al. Neurology. 2011;76(6):534-9.
40%50%
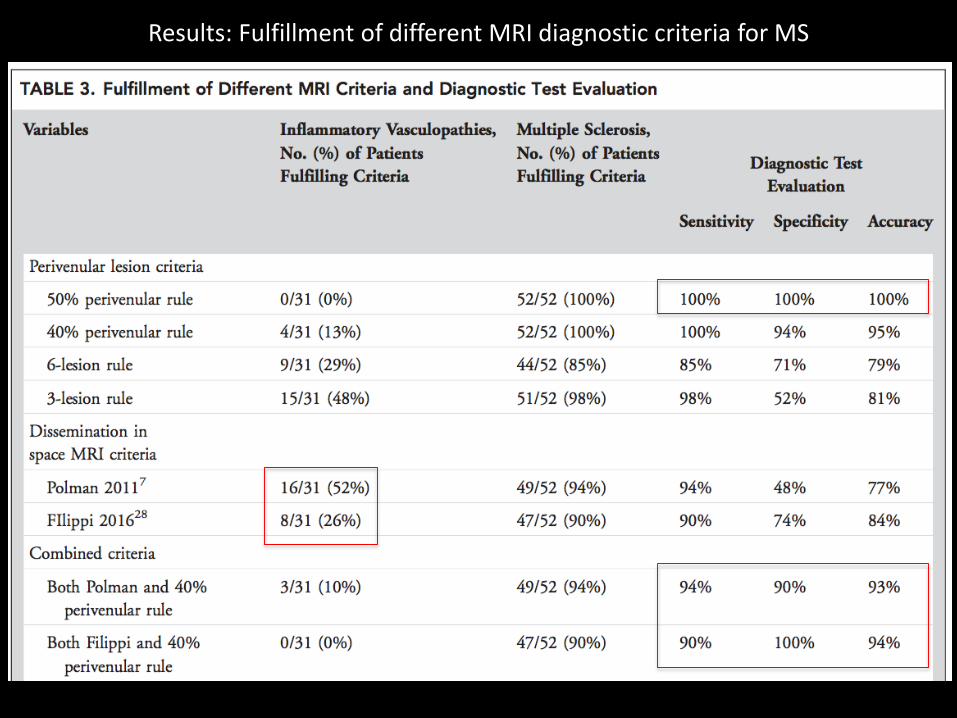
Results: Fulfillment of different MRI diagnostic criteria for MS
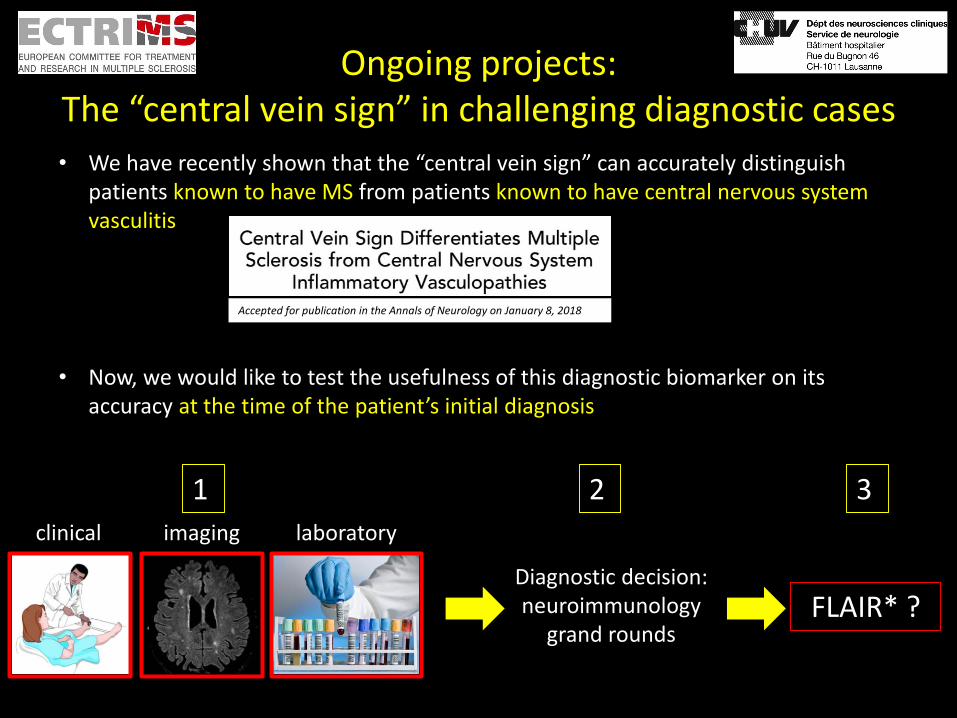
• We have recently shown that the “central vein sign” can accurately distinguish patients known to have MS from patients known to have central nervous system vasculitis
Accepted for publication in the Annals of Neurology on January 8, 2018
• Now, we would like to test the usefulness of this diagnostic biomarker on its accuracy at the time of the patient’s initial diagnosis
Aim of the study is to prospectively assess the value of a single 3T FLAIR* MRI scan for:
1. predicting an eventual diagnosis of MS in patients with possible MS but atypical
clinical, biological and/or radiological presentation
2. Predict or confirm an MS diagnosis in patients with both a possible or established
MS diagnosis and a concomitant systemic autoimmune disorder (potentially
affecting the central nervous system)
Ongoing projects:The “central vein sign” in challenging diagnostic cases
clinical imaging laboratory
Diagnostic decision: neuroimmunology
grand roundsFLAIR* ?
1 2 3

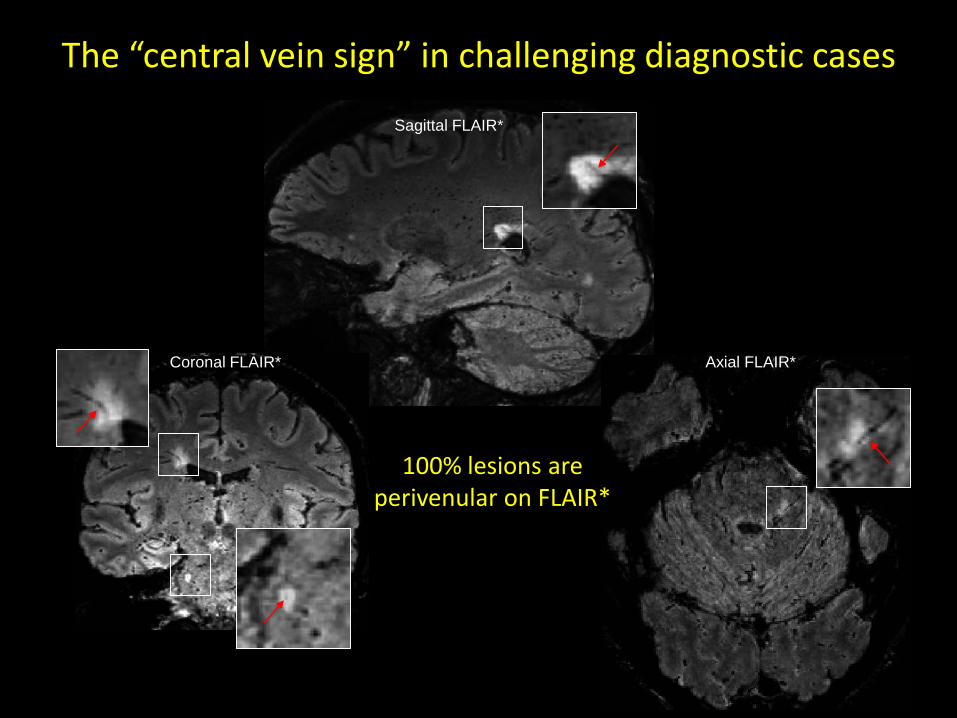
The “central vein sign” in challenging diagnostic cases
Clinical neurological features : 1. (age 48): hemi-face numbness/hypoesthesia2. (age 50): visual deficit (no better specified)3. (age 51): right sup limb hypoesthesia with ataxia4. (age 52) right inferior limb weakness with abnormal gait
Other, systemic symptoms : • Bilateral hands pain (joints ?) improved after steroid therapy• No other systemic symptoms
Male, 52 years old patient
Imaging work-up : • Brain MRI: several infratentorial and supratentorial WM lesions suggestive of MS• Spinal cord MRI: multiple discrete (<3 segm.) cervical and thoracic cord lesions; one
lesion showing contrast enhancement (Gd+)
Laboratory work-up : • LP: Absence of OCB; elevated protein concentration 1000mg/dl; leuco count<5 cells• Infectious and autoAb work-up is negative; serologic AQP4 Ab is negative
EDSS: 2.5 (pyramidal 2; sensitive 2; cerebellar 1)
The “central vein sign” in challenging diagnostic casesMale, 52 years old patient
Imaging work-up n2: • Brain MRI: one new Gd enhancing periventricular lesion• Spinal cord MRI: multiple discrete (<3 segm.) cervical and thoracic cord lesions
(3 cervical lesion showed mild Gd enhancement)
Laboratory work-up n2: • LP: Absence of OCB; elevated protein concentration 1300mg/dl
Considering the clinical and imaging features highly suggestive of MS and the exclusion of alternative diagnosis (NMOS, Sarcoidosis, Sjogren..)
The neuroimmunology round (blinded to FLAIR* results) decided for an MS diagnosis
T2w T1w Gd T1w Gd FLAIR
100% lesions areperivenular on FLAIR*
Sagittal FLAIR*
Coronal FLAIR* Axial FLAIR*

The “central vein sign” in challenging diagnostic cases
Neurological symptoms : • Progressive walking impairment since 8 years• Constant bilateral assistance required to walk since 1 year
Female, 68 years old patient
Neurological examination: moderate paraparesis with tetrapiramidal syndrome (pronunced jaw-jerk reflex) and spastic gait
FLAIR images
Imaging work-up : • Brain MRI: several supratentorial periventricular and center semi-ovale WM lesions
without Gd enhancement• Spinal cord MRI: absence of spinal cord lesions

Sagittal FLAIR* Coronal FLAIR*Axial FLAIR*
13% lesions areperivenular on FLAIR*
Differential diagnosis: • Primary Progressive MS: but negative OCB and spinal cord MRI• Inflammatory, metabolic, degenerative, genetic disease
The “central vein sign” in challenging diagnostic casesFemale, 68 years old patient
Laboratory work-up : • LP: Absence of OCB; normal IgG index; leuco count<1 cells
Diagnostic work-up: • Immune, infectious, metabolic and genetic work-up showed an SPG4 mutation • Hereditary spastic paraplegia (autosomal dominant and incomplete penetrance.. )

Acknowledgment
Vita-Salute San Raffaele UniversityNeuroimaging Research Unit
• Massimo Filippi
• Martina Absinta
Department of Neuroradiology
• Roberta Scotti
Department of Neurology
• Vittorio Martinelli
University of FlorenceDepartment of Neurology, Careggi Hospital
• Luca Massacesi
• Matteo Grammatico
• Luisa Vuolo
National Institutes of Health (NIH)Translational Neuroradiology Section, NINDS
• Martina Absinta
• Pascal Sati
• Daniel Reich
Université Libre de Bruxelles (ULB)Department of Radiology, Hopital Erasme
• Niloufar Sadeghi
Department of Neurology, Hopital Erasme
• Gaetano Perrotta
Department of Neurology, CHU Brugmann
• Bernard Dachy
Lausanne University Hospital (CHUV)Department Neurology CHUV
• Renaud Du Pasquier
• Marie Theaudin
• Team NIS
Department of Radiology
• Merixtell Bach Cuadra
• Hagmann Patric
Ecole Polytechnique de Lausanne (EPFL)Siemens Healthineers
• Tobias Kober
• Jonas Richiardi
• Mario Fartaria de Oliveira


















