November 1997 Volume 56, No. 11 ISSN: 001 7-8594 …
36
HAWAII MEDICAL JOURNAL November 1997 Volume 56, No. 11 ISSN: 001 7-8594 0 CAL 4 s V I 1856
Transcript of November 1997 Volume 56, No. 11 ISSN: 001 7-8594 …

HAWAIIMEDICAL
JOURNALNovember 1997 Volume 56, No. 11 ISSN: 001 7-8594
0CAL 4s
V I1856

We cod sayou
a thousd
Wee the onethat saves youmoney
HMSA RewardsIn appreciation for all you do on belmif of our members and to help you lower your
business costs, HMSA is proud to introduce the HMSA Rewards program for
participating providers. As a valued partner in health care, you’re eligible for a host of
discounted services and supplies. With HMSA Rewards, you can enjoy savings on
national business services, administrative training and services, and the latest
information technology applications. It’s just our way of saying thanks for being a part
of the HMSA family.
For more information about the HMSA Rewards
program, please call 948-6330 on Oahu or
1 (800) 790-4672 toll-free from the Neighbor Islands.
HMSAJtx Blue CresstYj Blue Snei
01 Hawa
CJioice for a Ralth.ier Hdz.oaiihttp ://www, hmsa .cOm

HAWAIIMEDICAL
JOURNAL(USPS 237-640)
Published monthly by theHawaii Medical Association
Incorporated in 1856 under the Monarchy1360 South Beretania, Second Floor
Honolulu, Hawaii 96814Phone (808) 536-7702; Fax (808) 528-2376
EditorsEditor: Norman Goldstein MD
News Editor: Henry N. Yokoyama MDContributing Editor: Russell T. Stodd MD
Editorial BoardVincent S. Aoki MD, Benjamin W. Berg MD,
John Breinich, Satoru Izutsu PhD,James Lumeng MD, Douglas G. Massey MD,Myron E. Shirasu MD, Frank L. Tabrah MD,
Alfred D. Morris MD
Journal StaffManaging Editor: Becky KendroEditorial Assistant: Carol Uyeda
OfficersPresident: John S. Spangler MD
President-Elect: Leonard R. HowardSecretary: Roger T. Kimura MDTreasurer: Charles R. Kelley MD
Past President: Carl W. Lehman MD
County PresidentsHawaii: Lorraine Sonoda-Fogel MDHonolulu: William M. Dang Jr. MD
Maui: Jon Betwee MDWest Hawaii: Ali Bairos MDKauai: Gerald McKenna MD
Advertising RepresentativeRoth Communications
960 Prospect Street, Suite 11Honolulu, Hawaii 96822
Phone (808) 545-4061Fax (808) 545-4094
The Journal cannot be held responsible for opinions expressed inpapers, discussion, conimunications or advertisements. The advertising policy of the Hawaii Medical Journal is governed by therules of the Council on Drugs of the American Medical Association. The right is reserved to reject material submitted for editorialor advertising columns. The Hawaii Medical Journal (USPS237640)ispublishedmonthly bythellawaiiMedicalAssociation(ISSN 0017-8594), 1360 South Beretania Street, Second Floor,Honolulu, Hawaii 96814.
Postmaster: Send address changes to the Hawaii MedicalJournal, 1360 South Beretania Street, Second Floor, Honolulu,Hawaii 96814. Periodical postage paid at Honolulu, Hawaii.
Nonmember subscriptions are $25. Copyright 1995 by theHawaii Medical Association. Printed in the U.S.
Contents
EditorialNorman Goldstein MD 305
President’s MessageLeonard Howard MD 305
Medical School HotlineRichard V. Mitsunaga MD, FAAP 306
Military MedicineNathaniel B. Berg MD 307
Book Reviews 309
CommentaryRussell T. Stodd MD 311
Application of Informed Consent Priciples in the Emergency DepartmentEvaluation of Febrile Children at Risk for Occult BacteremiaLoren G. Yamamoto MD, MPH, MBA 313
Common Sports Injuries Seen by the Primary Care PhysicianPart I: Upper ExtremityJames F. Scoggin, HI MD 324
News and NotesHenry Y. YokoyamaMD 331
Classified Notices 332
HAWAII MEDICAL JOURNAL, VOL 56, NOVEMBER 1997303
WeathervaneRussell T StoddMD 334
Cover art and descriptive text by Dietrich Varez, Volcano, Hawaii.All rights reserved by the artist.
Ulu
Because Ulu branches break easily it is risky to climb for the fruit. A proverbsays the entrance to the underworld is from the end of the breadfruit (Ulu)branch.
HappyThanksgiving

Join us in the quest forcontinued medical excellence.
Join your Straub colleagues as we strive for
continuing medical excellence.
Straub Clinic & Hospital, Inc. is accredited by
the Hawaii Medical Association to sponsor
continuing medical education for physicians.
Straub designates this educational activity
for a maximum of one credit hour in
Category 1 of the Physician’s Recognition
Award of the American Medical Association.
Each physician should claim only those
hours of credit that he/she actually spent in
the educational activity.
StmubWhen it really mattersVisit Straubs homepage at httje//www.stmubhealtheons
You are invited to attend...
— Friday Noon Conference —
PRO Data on Pneumonia Therapy and
Congestive Heart Failure
Roger Kimura, MD and Nathaniel Ching, MDOctober 24, 1997, 12:30 - 1:30 p.m.
Doctors Dining RoomLearning Objectives —
At the conclusion, participants will be able to:• Evaluate treatment modalities in Congestive Heart
Failure in the Medicare population.• Emphasize the utilization of ACE Inhibitor or their
alternatives.• Determine improvement in the quality of care in
Pneumonia therapy.
— Friday Noon Conference —
One Year at the Kapolei Clinic
Charles Kelley, MD; Ramon Pajarillo, MDand Helen Aldred, MD
November 7, 1997, 12:30 - 1:30 p.m.
Doctors Dining RoomLearning Objectives —
At the conclusion, participants will be able to:• Understand the challenges and rewards of opening
a satellite clinic within the Straub System.• Discuss the problems and solutions that may be
applicable to a wide variety of practices throughoutthe Straub family of clinics.
— Friday Noon Conference —
Treatment of Acute Myocardial Infarction
Roger L. White, MDNovember 21, 1997, 12:30 1:30 p.m.
Doctors Dining RoomLearning Objectives —
At the conclusion, participants will be able to:• Describe current treatment and pathophysiology of
Acute Myocardial Infarction (MI).• Review PTCA in Acute MI.• Summarize the GUSTO Studies.
We would like to acknowledge the Educational Grantfrom Pfizer Pharmaceuticals.
Please call Fran Smith at 522-4471 for more information.

Editorial Presidents Message
The Harry L. Arnold Jr. MDHawaii Medical Journal Case of the Month
Norman Goldstein MDEditor
A new feature for the HawaiiMedical Journal will be introducedwith the January 1998 issue. Ournew monthly feature, “The HarryL. Arnold, Jr. MD! HMJ Case ofthe Month” will publish case reports from Hawaii.
Reports accepted for publication should represent uniquely Ha
L waiian, or Pacific Basin, subjectHarry L. Arnold Jr. MD matter. We encourage submissions
from Hawaii and other PacificBasin locations. Our medical practices are rich in content, and thisnew forum will allow sharing of topical issues in a brief report. Wewill limit the content to no more than 2 published pages, with nomore than 2 total figures, tables, or images, and 10 or fewerreferences. The Instruction to Authors are published in the June1997 HMJ issue on page 157.
The purpose of the column is to introduce a forum for presentationof medical problems which are of interest and importance in ourregion. There are many medical conditions in our region (e.g. Kavadermopathy, leptospirosis, Hansen’s disease, tropical pyomyositis)which are culturally or epidemiologically unique. A case reportformat allows academic discussion of some relatively rare conditions, and serves to refresh the knowledge of those geographicallysingular diseases we may have come to regard as commonplace. TheHMJ will thus become a repository for reports of those diseaseprocesses requiring unique knowledge for treatment and diagnosisin our Medical Ohana.
This new feature will honor the Editor of the Hawaii MedicalJournal for 41 years, Harry L. Arnold, Jr. MD.’ We are pleased thatBenjamin W. Berg, MD will serve as editor for this new section.
References1 Goldstein N. Editor: Harry L. Arnold, Jr. MD Festschrift; HMJ Nov 1982, 41, 387-454.
Leonard Howard MD
In this first message to you as your president, I would like to sharewith you my thoughts about the role of the HMA in the currentmedical practice environment. We constantly hear comments thatthe reason we don’t have physicians beating down our doors to joinis that we lack relevance. Is this really the case, or are other factorsimpacting on us? What does the charge mean? The term itself issimple: Relevant - bearing upon or relating to the matter in hand;pertinent; to the point. Let us look at some of the current and somecontinuing activities of the HMA and see if we lack relevance. Whatis going on now that is of concern to the HMA?
PGMA bankruptcy - When it was announced that PGMA wasfolding and that many thousands of patients would be without care,and that many physicians would not receive payment for carealready delivered to subscribers, the HMA got involved. We attended the court hearings, listened to the legal dealings, and realizedthat the physicians were going to take their place far down the lineof individual creditors if the stated goal of “Keeping the hospitalshappy” was carried out. When this was reported to HMA Council,Dr Ali Bairos reported his solution of filing a small group lawsuit.Council voted to join with Dr. Bairos and, in addition, survey allHMA physicians as to their outstanding claims. When all reportswere in, the HMA physicians, as a group, represented by far thelargest creditor. Dr Spangler and I set up a meeting with the StateInsurance Commissioner, Rey Graulty, and the lawyers handlingthe reorganization process. The concerns of the HMA were expressed, and we received assurances that the HMA would be treatedin the same manner as the hospitals, pharmacies, and other healthcare providers. In September we received aprogress report from MrGraulty’s office which affirmed this assurance. A summary of thisreport will be published in the Hawaii Medical Newsletter. Relevant? You bet!
Tort Reform - In mid-September we received a notice from theCommittee on Judiciary of the House that there would be a PublicHearing on Tort Reform held on Oahu Thursday, November 13,1997. Because we represent the physicians of Hawaii, we were sentthis notice, requesting us to testify. Our testimony is already drafted,and will be presented to Chairman Tom’s committee at the hearing.We were already aware of the Administrative interest in TortReform because of an invitation to join a coalition of interestedparties to lobby for tort reform in this coming session. Your HMAwas represented at the first two meetings of the coalition, where wewere very forthright in our insistence that relief from joint liabilitywould not be extended to the tobacco industry. When the tobaccolobbyist showed up at the second meeting and offered RJR moneyto put on a dinner on Maui, we withdrew from the coalition. HMACouncil approved this action. In this situation, the HMA willprovide strong testimony for tort reform as we did in the past. Ourlast involvement with tort reform resulted in the formation of thePatient Conciliation Panels, one of the most successful methods ofreducing the number of medical malpractice suits in Hawaii.
HAWAII MEDICALJOURNAL, VOL 56, NOVEMBER 1997305
-J
Until Ibere’s a cure,there’s the
American DiabetesAssociation

Relevant? You Bet!The Times are a-changin - Where is the HMA on the evolution
of managed care in Hawaii? We stand right alongside the AMA
insisting on physician control of managed care organizations.
AIvINews top story Jan 20, 1997 reported that for all physicians, the
percentage holding managed care contracts increased from 55.7%
in 1986 to 69.6% in 1992. I don’t think the direction has changed
since then. For the young physicians, 0-5 years in practice, the
figures are 56.5% and 72%, respectively. Maybe the reason we do
not attract young physicians as members is because we are being
perceived as a solo-practice-only organization, and the younger
physicians are not interested. If we are to represent and be advocates
for all the physicians of Hawaii, it is necessary that we not take a
strong stance on any position that positively affects one group of
physicians but negatively affects another. The HMA must support
the freedom of choice for patients to see the physician they want,
and the right of the physician to practice in the situation in which he!
she chooses. There are many issues that affect all physicians in
Hawaii. It is in these issues we find our relevance.
Medical School Hotline
Role of the Clinical Faculty in PediatricMedical Education
Richard Y. Mitsunaga, M.D., F.A.A.P.Clinical Professor, Department of Pediatrics
John A. Burns School of Medicine
University of Hawaii
In 1984, fewer than 5% of all physician-patient contacts resulted
in hospitalization. Nevertheless, clerkships for trainees at all levels
were predominantly hospital-based inpatient experiences.’ Over
time, academic departments and training programs evolved to be
subspecialty based and located in tertiary care centers which had
scant contact with the physicians who referred the cases.
Of course, many specialties require a primarily in-patient experi
ence of its trainees; this is particularly true of the surgical fields and
most medical sub-specialties. Practice in the primary care areas, on
the other hand, is mainly an out-patient experience and becoming
increasingly so because of medical advances and other forces
including managed care.Like other primary care specialists, pediatricians have noted that
a larger portion of their patients who previously required hospital
ization are now routinely managed on an out-patient basis. The
combination of the incfeasingly ambulatory nature ofpediatrics and
the validity of classic, in-patient based training of pediatricians was
generating more and more questions.2In Hawaii the Department of Pediatrics at the John A. Burns
School of Medicine (JABSOM) is the direct descendent of a
community hospital residency program at Kauikeolani Children’s
Hospital. The program was integrated into JABSOM 24 years ago
with Dr. Sherrel Hammar as Chairman and Professor. He made two
important decisions which have guided the program since its
inception as a university residency: (1) Every in-patient would be a
teaching patient and (2) Clinical faculty would be an integral part of
the program.The clinical faculty who augmented the small number of faculty
emphasized to the house-staff that patient care is a continuum which
starts with an out-patient diagnosis, admission and hospital treat
ment, and post-hospital follow-up. The manner in which clinical
faculty are utilized in the Department ofPediatrics has evolved over
the years by observing four principles:One, all pediatric admissions to Kapiolani Medical Center for
Women and Children are teaching patients. Admitting pediatri
cians, whether clinical or regular faculty are expected to interact
with residents of different levels according to a protocol designed to
maximize the teaching value of the patient for the resident. (This
protocol was redefined at a joint resident-faculty retreat in 1997).
This interaction determines the day-to-day management of the
patient.Two, teaching on the general pediatric ward is accomplished by
a team of two regular and two clinical faculty members who are
assigned one month rotations. Accordingly, twenty-four clinical
faculty members spend part of each week-day morning for a month
tending to teaching duties.The residents benefit from the perspective that the clinical faculty
can give on inpatients regarding pre and post hospital management,
family dynamics and use of community resources. The clinical
faculty benefits from the close exposure to residents, regular faculty
and the stimulus of working on a hospital service. The Department
of Pediatrics experiences no difficulty in obtaining volunteers for
this duty.Three, clinical faculty members provide community-based ambu
latory experience for residents as well as medical students. In
contrast to the hospital based ambulatory experience which pro
vides care for children who need primarily ongoing sub-specialty
care, the community-based ambulatory experience focuses on con
tinuity, weilness, family dynamics and common illnesses which are
managed in the office.The community-based ambulatory experience with clinical fac
ulty members offers residents more than patient management. It is
their introduction to office practice. Residents have their choice of
practice setting from solo or small group practice to large staff-
model multi-specialty groups. Residents are exposed for the first
time to considerations regarding an office’s physical design; busi
ness aspects such as employee matters, accounting, billing and
collections, and medical records systems; appointment systems and
telephone techniques; patient flow; purchasing; and office meet
ings. Residents can also learn about issues which confront physi
cians such as division of responsibilities, decision making, continu
ing medical education and dividing income; nursing job descrip
tions; special office areas (hearing and vision screening, minor
surgery); office laboratory procedures and relations with local
specialists such as pharmacists, school counselors and other com
munity resources.3 The rotation can be tailored to address each
resident’s interests and needs.Four, clinical faculty who are subspeciaLists provide rotations in
their offices or in the clinic for experience within their sub-special
ties.The validity of the educational approach utilizing clinical faculty
and community experience by the Department of Pediatrics has
HAWAII MEDICAL JOURNAL, VOL 56, NOVEMBER 1997
306

been established in several ways. The graduates of the programcontinue to practice successfully in this State in both communityand academic settings. In addition, the Residency Review Committee (RRC) for Pediatrics requires increasing amounts of community-based experience of pediatric trainees. Finally, Pediatric Education in Community Settings is the topic of an increasing numberof papers and seminars.4
Ironically, many of our best clinical faculty are not well known inthe hospital. These are physicians who have outstanding out-patientskills and keep their patients out of the hospital. The departmenthopes to maximize resident exposure to such clinicians. Of course,all clinical faculty are expected to impart their techniques onremaining current in their specialty to the residents.
The role of the clinical faculty in pediatric education is subject toconstant evaluation, modification and improvement. The residentinitiated faculty-resident retreat of 1997 is the first of what is hopedwill be an ongoing process. The faculty must increasingly learnprinciples of adult education and improve on feedback mechanismsto validate continually the worth of its contributions to residenteducation.
References:1. Physicians for the Twenty-first Century: The GPEP Report: Report of the Panal on the General
Professional Education of the Physician and College Preparation for Medicine, 1984. Association ofAmedcan Medical Colleges, One Dupont Circle, NW., Washington, DC 20036.
2. Greenberg LW, Geton P, Brassiux C, et.al. How Are Pediatric Training Programs Preparing Residentsfor Practice? Am J Dis Child. 1991; 145:1389-1392
3. Sample Outline forOtfice Training from the Pediatdc Medicine Clinic, 19241 Montgomery VillageAve.,Suite F-b, Gaithersburg, Maryland 29879.
4. DeWitt, TG, Roberts KB, eds, 1996. Pediatdc Education in Community Settings: a Manual. Adington,Virginia: National Center for Education in Matemal and Child Health.
Military Medicine
Tragedy in Guam: One Doctor’s Chronicle
Nathaniel B. Berg MDMajor U.S. Army
U.S. Naval Hospital Guam
In the early morning hours of August 6, 1997,1 received a call thatbegan in a manner well familiar. The physician on duty in theemergency room at U.S. Naval Hospital Guam (USNH, GU) calledme to request an emergent non-contrast head CT. She was evaluating an elderly male who was found to be non-responsive and acerebral vascular accident was thought the likely etiology. I askeda few questions about the case and told her I’d be on my way in assoon as I called the CT technologist. The routine nature of thescenario for the late night encounter with my colleagues in theemergency ended with her next declaration. She had just receivedreport of a possible crash of a Boeing 747 passenger plane on NimitzHill. I live on the top of Nimitz Hill and had just fallen asleep whenshe called. I confidently informed her that no plane had crashed intoNimitz Hill. I surely would have awoken at the sound of such adisaster, particularly if one of the monstrous 747s that rumble overmy house many times a day was involved. I called the CT technolo
gist and dressed, with little thought of the tail end of my discussionwith the ER. As I opened my back door the smell ofjet fuel filled theair.
My route to the hospital takes me by a look-out in front of the laststand of the Japanese Imperial Army on Guam in World War II. Thevista is usually of the non-inhabited, jungle-covered side of NimitzHill, as it slopes into a ravine. Through the light rain, the entire sideof the hill seemed engulfed in flames. A Guam Police car had pulledover and an officer was standing in the road. As I approached his facespoke horrification. I stopped and realized that I was the onlyRadiologist for the hospital closest to a disaster the size of which Icould only guess. I continued to the hospital. I provided visualconfirmation of the crash and the entire hospital staff was recalled.The mass casuality drills we so diligently practice on Guam was now‘the real thing’. The crash site was difficult to access. The rescueeffort was completed in a cooperative manner by the United StatesMilitary and local civilian fire and rescue personnel.
As the sole Radiologist I remained predominately in the Emergency Department. A barrage of requests were relayed from the fiveemergency department exam rooms. Order was made of the requestsand films were completed and interpreted rapidly. The urgency tointerpret a large number of films rapidly while continuing tocoordinate the radiographic triage did not allow me to sit in a darkquiet room with my Dictaphone. Tread the films standing at the ERview box with surrounding light and mass commotion, accented byagonizing screams. I gave verbal reports to the physicians, as atechnologist wrote my opinion on the film jacker. CT scans werebrought for interpretation by runners. We could not spare a portablemachine for the intensive care unit. The few stable survivors hadtheir needed X-rays completed in the Radiology department. Theidentification of patients by name was usually not possible. Aspracticed in our drills, all patients were assigned numbers as theyentered the Emergency Department. This would prevent error inmatching patient to films.
Two days following the crash I received another unique phonecall. I was informed that I would need to complete X-rays on all ofthe remains of those who did not survive the crash. The exams wouldbe needed to aid in identification of the victims and would possiblyhelp in assessing the cause of the accident. The senior technologistsand I inspected the temporary morgue to assess our unfamiliar task.An enormous warehouse had been partitioned into areas labeledintake, medical photography, personal effects, pathology, anthropology, fingerprints, mortuary and data entry/processing. Beneatha sign labeled RADIOLOGY we were to set up shop. As explainedby the National Disaster Management System (NDMS) and Disaster Medical Operations Readiness Team (D-Mort) team leaders, thebody bags were brought from the crash site in refrigerated tractortrailers. They would be assigned a folder and would pass througheach section. We were to open the bags, inspect the contents andcomplete appropriate radiographs. Anything that might aid in identification was to be recorded. The task was to be completed asrapidly as possible without compromise of information. I knew wewould need off-island personnel and material resources to completethe task.
Building a radiology suite at the morgue site was not feasible. Wewould need three portable X-ray units. Two to run continuouslywhile a third charged. A processor, a label flasher and light boxes
HAWAII MEDICAL JOURNAL. VOL 56, NOVEMBER 1997
307

would need to be available. We borrowed portable units from Guam
Memorial Hospital (GMH), requisitioned a bathroom for the pro
cessor, and took the rest of the equipment from our own hospital. If
two units were to be running simultaneously, a large number of
cassettes would be needed, including scoliosis cassettes. Tripler
Regional Medical Center (TRMC) sent the cassettes and two near
new portable units to allow return of the GMH units. Three tech
nologists were needed for each machine. One to shoot and two to
position and hold cassettes and remains. One person was needed in
the darkroom and the another to keep order of the films and records.
The heat in the warehouse and the nature of the work made obvious
the need for frequent breaks. Several additional people would be
needed. A team leader and a Radiologist for each shift added to the
needed manpower. We were to work twelve hour shifts until the
work was done. A call went out for assistance from the U.S. military
facilities in the Pacific Rim.Harlan Herr, CDR, MC, USN, Radiology Department Head at
USNH, GU was on leave at the time of the accident and was on his
way back. Technologists from the 121St U.S. Army General Hospi
tal in Seoul, Korea and Naval Hospital Yokosuka, Japan arrived
within 24-hrs. With the arrival of Commander John Maher, MC,
USN from Naval Medical Center San Diego (NMCSD) we began
our work at the morgue, while continuing to manage the Naval
Hospital Guam Radiology Department. Terry Yeager, MAJ, MC,
USAR came from TRMC with three technologists from his facility
and two from Naval Clinic Pearl Harbor More technologists were
to arrive from NMCSD, Bremerton Naval Hospital and Naval
Hospital Camp Pendelton allowing us to run a normal schedule at
Naval Hospital Guam and crews at the morgue 24-hrs a day. CDR
Robert Parkinson, a radiologist from NMCSD possessed Korean
language skills that were to prove useful in comparing our exams to
antemortum radiographs that arrived from Korea, and in communi
cating with Korean nationals.The technologists and I shared a fear of the unknown. We knew
that we would be seeing things that we all had hoped to live and die
without seeing. Radiographing charred remains in various states of
decomposition was not something we had chosen to do, and no one
knew how we would react. The NDMS team leaders recommenda
tions were later given to all of our team members. He advised us to
focus on the importance of our work. Through high quality radio-
graphs, remains could be quickly and accurately matched with
available antemortum films. This would allow delivery of remains
to loved ones. The possession of remains, no matter their condition,
is essential to grieving and closure in virtually all cultures and
religions. Our work would clearly help the families of the victims.
Without our work, their suffering might be prolonged.
After a body bag was brought to our work area, we visually
examined the contents of the bag. A scoliosis film was used to
survey for radiodense components, personnel effects, and other
non-human elements, e.g. aircraft parts, that were not seen on
intake. Radiographs that might help in age or sex determination
were completed. Typically, these included views of the ends of the
long bones, hands, feet and spine if they were present. For matching
to antemortum exams, we would attempt standard positioning of the
LLTHEPA551
TAKE ONE A DAYAND GALL ME
ALOHALABORATORIES, I NC.
Oio tL Ctei E4 of 1J3ab’ofo
CAP Accredited Laboratory
Surgical Pathology
Dermatopathology
Cogy
Frozen Sections
Intraoperative Consultations
David M. Amberger, M.D.
.:E .
Harley-Davidson FAT BOY®
We can put the wind in your hair and the freedom back into your spiritwith Harley-Davidson, Kawasaki, Buell and Moto 6uzzi motorcycles parts,
accessories and professional service. We speak the lingo to bikers and welcomenew riders by walking you from school, to license, to the right bike.
) CITY
2965 N. Nimitz Highway(Near JN Chevrolet and the Airport)
Open daily
2036 Hau Street Honolulu, Hi 96819
(808) 842-6600 Fax: (808) 848-0663Phone: 831-2600

remains as for common clinical radiographs. Thus, if a skull waspresent, a paranasal sinus series and a skull series would be completed. Mastoid air cells and frontal sinuses have extraordinaryvariability and are excellent sources ofX-ray matching. As views ofthe chest, wrist, ankle, cervical and lumbar spine are common, thesewere completed when possible. The scout scoliosis films oftendemonstrated unexpected findings, such as osseous structures frommore than one victim. These were separated appropriately.
A group of psychiatrists, psychologists and social workers sentfrom NMCSD made up the U.S. Naval sprint team sent to providepsychological support. They were critical to help our teams workingfull time. They met with each individual at least once every threeshifts and with the entire team as a group daily. We followed theiradvice to take short breaks every two hours, change our clothesbefore going home, refrain from eating in the warehouse and to lookout for each other. To date, no team member has reported difficultyworking or sleeping, nightmares, or other signs indicative of lastingadverse emotional consequences of the work completed. We Xrayed every single remain brought to the morgue. Even the smallestfragments were examined with an attempt to identify anatomicorigin. The anthropologists would further examine the remains andnot infrequently would ask for additional views of individual bonesknown to aid in age estimation. As explained to us, all efforts wereto be made at identifying the remains including DNA testing of allremains not otherwise positively matched with a victim.
Several weeks later our job was complete. The Radiology teamwas made up of members from many different commands aroundthe Pacific Rim. All became quickly focused on expediently andexpertly doing everything we could to unite victim’s remains withloved ones. This maintained the esprit of the teams quite highthroughout. Many attributed the success of arduous work at themorgue site to military readiness training and attention to thepreventive measures recommended by the NMCSD sprint team. Wewere proud to learn that many of our exams had been critical inidentification of remains.
Major Berg is a Staff Radiologist assigned to U.S. Naval Hospital,Guam.
C Book Reviews
All Stings ConsideredFirst Aid and Medical Treatment of
Hawaii’s Marine InjuriesCraig Thomas MD and Susan Scott
Reviewed by Norman Goldstein MD
Craig Thomas MD, and emergency room physician, and SusanScott, a registered nurse and marine science writer, have created asuperb book in All Stings Considered. Their years of clinicalexperience and their participation in activities on, under, and aroundHawaii’s waters make them the authorities on marine injuries inHawaii.
This compendium, well researched and well written, is easy for
the general reader to understand and will be a handy reference forall water enthusiasts. It is also an excellent medical text for thehealth professional. No other book specifically addresses the Hawaii aquatic environment. The many articles on specific marineinjuries that exist in the medical literature are difficult for the layreader to obtain and understand.
Every emergency room and poison control center should have acopy of this book at hand. Paddling, sailing, and swimming clubs,along with high school and college athletic coaches, will use it foraccident prevention and quick treatment. First responders, emergency physicians and staff, pediatricians, family practitioners,internists, and dermatologists will find it valuable as a speedyreference.
In their first joint publication effort, the authors have compiled awealth of marine information.
Editor’s Note: This is a must-have and must read for every healthprofessional in Hawaii.
The Honolulu Heart Program,An Epidemiology Study of Coronary Heart Disease
and Stroke
Reviewed by Roger L. White MDDepartment of CardiologyStraub Clinic & Hospital
It is my pleasure to review and recommend strongly the newlypublished book, The Honolulu Heart Program, An Epidemiological Study of Coronary Heart Disease and Stroke as edited byDrAbraham Kagan. The Honolulu Heart Program study has gainedinternational recognition over the past 30 years for its thorough andongoing research and has become probably the second most frequently quoted study to the Framingham study on coronary arterydisease from Massachusetts. As a practicing cardiologist in Honolulu, I have had many patients who have been enrolled in this study,as I am sure most clinicians in our community have been touchedone way or another by this study. I have heard many of the authorsspeak at conferences over the years, and its is a pleasure to have thedata all in one place in a book form. It is much welcomed.
The book is edited by Dr Abraham Kagan who has coordinated theefforts of 13 contributing editors. It is 204 pages, well organized andvery readable. The Honolulu Heart Program has followed theepidemiology of coronary heart disease and stroke in 3,006 Hawaiian men of Japanese background for more than three decades. Thisis a monumental task of organization and persistence, and hasyielded some very valuable data which we can all translate into ourday-to-day care of patients in the prevention of heart attack andstroke. The most significant conclusion from this study was toconfirm a gradient in coronary heart disease prevalence, incidencein mortality among Japanese males living in Japan, Honolulu andCalifornia, with the highest incidence of cornary artery diseasebeing in California, the lowest in Japan, and moderate in Hawaii.The correlation with changes in diet and lifestyle with increasedWesternization correlates very well. There is also confirmed areverse gradient for the prevalence of stroke from the same three
HAWAII MEDICAL JOURNAL, VOL 56, NOVEMBER 1997309

THE SUPPORTWith 1,700 American ExpressTravel offices in 120 Countriesaround the world, we’re there tohelp you almost anywhere you go.American Express Travel is yourhome away from home.
THE VALUEThe volume of business we generatefor our travel partners provides usextensive price advantages that wepass on to you, our customer.Let us show you how you can savemoney on air, hotel, car, cruise andtour arrangements.
THE SERVICE & EXPERIENCEDedicated to providing localpersonalized service, yoirAmerican Express Travel team iscomposed of seasoned travelprofessionals. With over 250 yearsof experience among them,you can rest assured your travelarrangements will receive theattention to detail they deserve.
TRAVEL FINANCIAL SERVICESAmerican Express is your‘one stop shop” for all your travel
financial service needs. includingTravelers Cheques (7 majorcurrencies), Foreign Exchange,Gift of Travel certificates,Gift Cheques, MoneyGram. etc.
AMERICAN EXPRESSCARDMEMBERSWe also provide American ExpressCardmembers with services suchas emergency check cashing,emergency card replacementand exclusive offers forCardmembers.
sites, with the highest incidence of stroke beingin Japan, and a lower incidence in Hawaii. Theimportance of these studies and the influence ofdiet with increasing fat content, increasing myocardial infarction cannot be underestimated.
The chapters in the book are well organizedand review lipoprotein study analysis, hypertension, coronary heart disease, stroke, pathology,mortality rates, recent review of data, and looking to the future with regards to aging anddementia. The bibliography for each chapter iscomplete and helpful. The Honolulu Heart Program has had several firsts in the epidemiologyof beast disease. Some of these include theinverse relationship between alcohol and coronary artery disease, for which we can all begrateful in justifying one to two small drinks aday to prevent heart attacks (albeit, unfortunately the rates of hemorrhagic stroke, cancerand mortality increase with increased alcohol).Also, another first in The Honolulu Heart Program was to show the inverse risk factor relationship between HDL cholesterol, in that thehigher the HDL level, the lower the risk ofcoronary atherosclerosis. This is particularlywell documented in the chapter on PathologicalCorrelations by Dr Grant Stemmerman wherehe reviews the autopsy studies on 288 meninvolved in the study. The Honolulu Heart Program is also the first to document a correlationbetween a stressful lifestyle and what we calltype A behavior, and increased incidence ofcoronary artery disease.
I feel that this book should be on the bookshelfof every cardiologist, internist and family practitioner in Hawaii. It is unique to the region thatthe study as important on an international basis.This study helps lay the foundation for futureepidemiologic studies ofdifferent ethnic groups,gender, lifestyle, diet and exercise programs inthe prevention of coronary heart disease andstroke. As an example, we already know thatalthough coronary heart disease is less commonin women, its prevalence increases as womenget older, and women are more likely to have afatal myocardial infarction then men. Also, asour population ages, the effects of aging anddementia will be very important to study to look at epidemiologic
factors which may, if prevented, improve the quality of life. Hawaii
represents a unique community whereby different ethnic groups and
diet can be evaluated. As we move into the next century, we are truly
becoming a world community in the informational age, and by
doing epidemiologic studies one can better understand a disease
process, so that in the future better prevention can be done. The
Honolulu Heart Program has been a cornerstone and basis for future
studies.
YouMakePeopleWell.We MakeTravelEasyFor relief of travel headaches, take this ad and callus in the morning. Whether you’re traveling forbusiness or pleasure, nobody covers the worldlike American Express Travel.
TravelCOMMERCE TOWER1440 Kapiolani Blvd. • Suite 104(Corner of Kapiolani Blvd. and Keeaumoku Ave.)947-7171 and 941-0568
To learn more about brain attack or services for stroke
survivors, call the American Heart Association’s Stroke
Connection at 1-800-553-6321.
Stroke is a Brain Attack.Know the Warning Signs.
HAWAII MEDICAL JOURNAL, OL 56, NOVEMBER 1997
310
Commentary
Russell T. Stodd MD
My brother, John. was the oldest of four boys surviving in theStodd family. Partly because he was the oldest, but mostly becauseof his character and personality. John was the acknowledged leader,and commanded the most respect. From my earliest recollections,John was generous, kind and protective. He was wise, and seemedalways to be right, but he rarely offered advice. When asked hewould offer his opinion, but always with a few kind words andwithoutjudgment. He was a fighter pilot in the famous Black SheepSquadron during the war, and was a prisoner of war in Japan. He wascalled back in the Marine Corps and flew in Korea as well. Weadmired and revered him. After a lengthy legal career he retired toplay some golf and travel.
When John became ill last year with myeloma. his HMO doctorshad difficulty making a diagnosis. Because of severe neck and headpain, his initial “diagnostician” treated him with increasingly potentanalgesics, but never pursued a diagnosis. After several months,John was referred to a neurosurgeon for possible spinal fusionbecause of worsening and unrelenting pain. The surgeon obtainedradiographic studies which revealed the presence of a mass high inhis neck as the source of his difficulty. Biopsy of the mass revealedthe presence of myeloma. Strike one! He was treated with irradiation and chemotherapy which was debilitating, and precipitated apulmonary embolus. Strike two! Coumadin was added to his therapeutic program, but monitoring was careless, and his dose wasconstantly juggled. In May he became severely anemic. It wasevident that he was bleeding, and he was transfused three units.During this time, I advised him by telephone about medications andlab studies, and tried to be reassuring. In our last conversation it wasobvious that he was bleeding from his GI tract with hemorrhage intohis naso-pharynx and where else? I recognized that he was Coumadintoxic and I suggested that he question his doctor about that possibility. The following day he saw his last HMO doctor, who had neverseen John prior to that time. She advised him to continue theCoumadin. Strike three! You’re out, John. Three days later, on June16, Father’s Day, he died at home from a massive cerebral hemorrhage.
So our beloved family leader and hero was gone, quite suddenlyand before his time. Is there blame to be assigned here, and if so to
whom? The answer is, yes, there are plenty to blame. Specificallyhis doctors and their system of indifferent care are at fault. TheHMO and their nonchalant corporate practice of medicine wasdisgraceful. The initial internist was useless when he treated Johnwith increasingly strong pain medication while never seriouslyseeking a diagnosis. When the diagnosis was made by a neurosurgery consultant, John’s care was spotty at best. Still, after initialtherapy for his tumor, and the pulmonary embolus, he was gainingstrength. While on Maui in February his kidney function wasnormal, his calcium and serum proteins were okay and he appearedto have a good prognosis.
The matter of his coumadin therapy and the apparent disregard forobvious toxicity is shameful. Then, of course, there is blame formyself as well. I was certain he was toxic from coumadin, andshould have strongly recommended prompt remedial action butinstead merely made a weak recommendation to question the HMOdoctor.
I remain angry and sorrowful. I miss my brother every day, andfeel remorse at my failure. The anger is stored up for casual,insensitive practice of corporate medical care. Even if challengedabout this sad case, the corporate spokesman would merely state thatthis patient slipped through the cracks, and after all, he was 74 yearsold. He had a serious disease, so how much time did he have leftanyway? As an HMO executive once stated, “We see patients asnumbers, not individuals. We are a mass-production medical assembly line, and there is no room for the human equation in ourbottom line.”
What doctor really knew my brother? Who cared? A thoughtfulintelligent family doctor would have helped John stay alive for anindefinite time by simply paying attention. One patient and a caringphysician with an ongoing record, pertinent and calculated labwork, timely follow-up, proper advice on therapy and appropriateactivity; in other words, a doctor who cared. Make no mistake; astrong doctor-patient relationship is critical to successful treatment.Separated from a single, responsible physician, the patient is at greatrisk. Think about it. Where is the HMO going with the healingprocess?
Editor’s Note:Its not your failure, Russ. It is the failure of medicine today.Whether in a HMO, another type of group practice or solo practice,let us learn from the story of “Brother John.” Patients are notnumbers, they are individuals. Mahalo for sharing your sorrow withus.
Our public education programs teach people about cancer. Last year, 55• million people learned that with early detection we can win 87% of the battle.
FORMOREINFORMATIONL4ILTOLIFREE 1 8OACS.2345For more information on winning, call 1—800—ACS—2345
HAWAII MEDICAL JOURNAL, VOL 56, NOVEMBER 1997311

A $10 miffion renovation has just made thepre-eminent rehabilitationfacilityin Hawaii even better!
-1.1\ —
the Rehabilitation Hospital of the Pacific has served
Hawaii’s people with:
• highly experienced staff physicians and
psychologists
• a comprehensive team approach to
rehabilitation care
• highly trained therapy teams for each
disability
• a caring and compassionate staff
• a broad track record of successful
patient outcomes
• family involvement and training
• state-of-the-art technology and
equipment
We are proud to announce that our $10 million
renovation has given this esteemed hospital a
new face - inside and out.
Call 531-3511 for information.
%.Rehabffitation Hospital of the PacificREHAB‘Aiea • Hawaii Kai • Hilo • Kauai • Maui • Mifilani • Nu’uanu • Queens • St. Francis-West

Application of Informed ConsentPrinciples in the Emergency DepartmentEvaluation of Febrile Children at Risk for
Occult BacteremiaLoren G. Yamamoto MD, MPH, MBA*
Informed consent requires that the risks and benefits of a particulardiagnostic and therapeutic plan be reviewed with the patient,including the disclosure of alternative diagnostic and treatmentapproaches. Although it could be argued that it is difficult to presentall the diagnostic and therapeutic options to parents in the E. D.management of febrile children at risk for occult bacteremia, it is thepurpose of this report to describe the experience with followingthese principles of informed consent in a group of these children.
Methods: Convenience sample of febrile children presenting toan E.D. at risk for occult bacteremia. A standardized informationsheet was presented. A parent survey of preferences followed.
Results: In 37 patients, most of the parents chose no tests andpreferred to be involved in the medical decision making process fortheir child.
Conclusions: While preferred by parents and supported by AAP,the process of informed consent, for febrile children at risk foroccult bacteremia, is time consuming and often not possible whenthe E.D. is busy. Physicians may find it desirable to make decisionsfrom an informed consent perspective to a comfort level dependenton time availability, parents’ comprehension ability, and individualpersonal practice preference.
Keywords: informed consent, occult bacteremia, otitis media,blood culture, white blood count
*Emergency Services,Kapiolani Medical CenferFor Women And ChildrenDepartment of PediatricsUniversity of HawaiiJohn A. Burns School of Medicine
Correspondence:Loren 6. Yamamofo, MD, MPH, MBADepartment of Pediatrics1319 Punahou Street, #718Honolulu, Hi 96826(808)973-8387Fax (808)949-4232e-mail: [email protected]
IntroductionWhile the authority to make medical decisions used to rest solely
with the physician (doctor knows best theory), this is now considered to be unacceptable.’ In addition to sources in the medicalliterature26 and court conclusions,6 the American Academy ofPediatrics (AAP)’ and the Joint Commission on Accreditation ofHealthcare Organizations (JCAHO)7 have confirmed support ofinformed consent, which requires that the risks and benefits of aparticular diagnostic and therapeutic plan be reviewed with thepatient. This review should include the disclosure of alternativediagnostic and treatment approaches.’-7Decision-making power orauthority is increasingly seen as something to be shared by equalpartners in the physician-patient or physician-parent relationship.’While reports in the literature have indicated that this is the properapproach to take, such a practice is time consuming.
In the evaluation of the febrile child at risk for occult bacteremia,sources in the literature have recommended divergent diagnosticand therapeutic approaches (Table l).819 According to informedconsent principles, the management of such cases should includethe disclosure of all these approaches.’-7
While physicians may assume that patients generally want moretests and more treatment in order to avoid as much risk as possible,a published survey of parents showed that parents often preferredthe opposite of this (fewer tests, less treatment, more risk) in ahypothetical case scenario involving a 6-week old febrile infant.20This indicates that when a range of diagnostic and treatment optionsare presented to parents, they may often choose the less aggressivechoice even if it involves more risk. This also indicates that trueinformed consent with full disclosure of alternatives, is often notpracticed as a standard in this clinical scenario. Although it could beargued that it is difficult to present all the diagnostic and therapeuticoptions involved to parents, it is the purpose of this report to describethe experience with following the principles of informed consent ina group of actual children presenting to an E.D. with fever at risk foroccult bacteremia. Quality of care maybe improved by understanding this process better to determine ways ofoptimizing the informedconsent process.
BackgroundThe emergency department evaluation of young febrile children
(3 months to 3 years of age) at risk for occult bacteremia is arecognized controversy. Actual patient data supporting a singlestandardized diagnostic evaluation and treatment approach is lack-
HAWAII MEDICAL JOURNAL, VOL 56. NOVEMBER 1997313
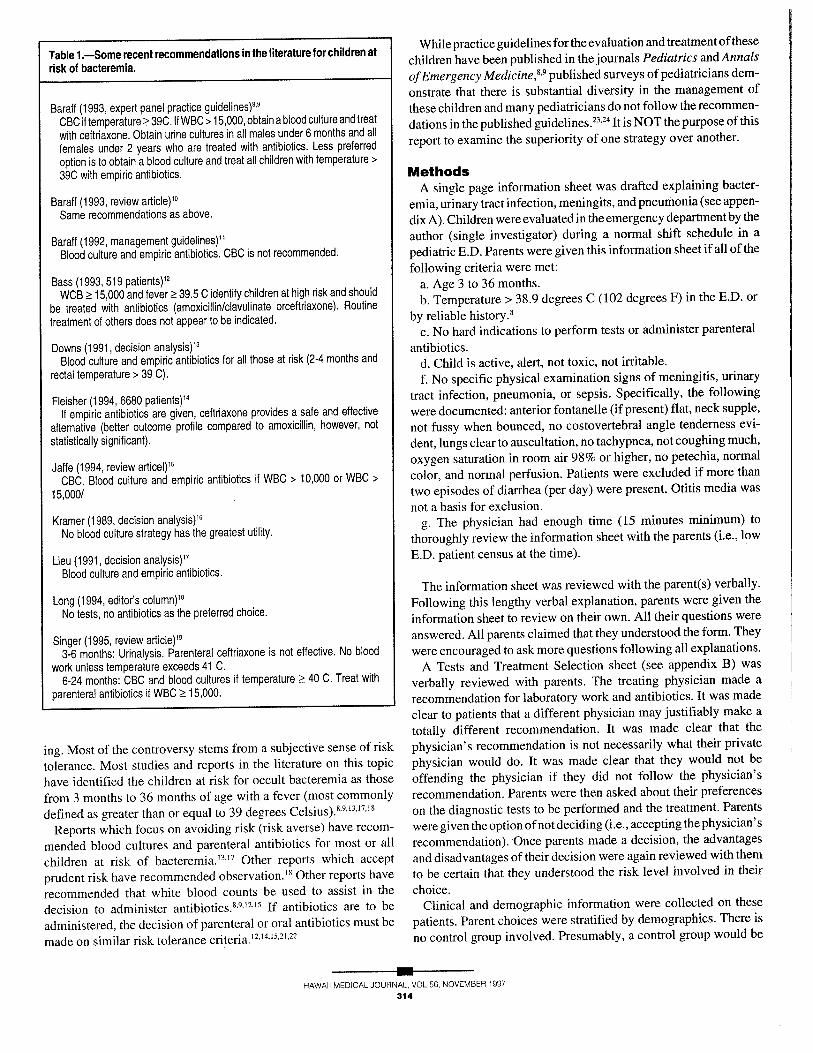
Table 1.—Some recent recommendations in the literature for children atrisk of bacteremia.
Baraff (1993, expert panel practice guidelines)8’9CBC if temperature 39C. If WBC>15,000, obtain a blood culture and treat
with ceftriaxone. Obtain urine cultures in all males under 6 months and allfemales under 2 years who are treated with antibiotics. Less preferred
option is to obtain a blood culture and treat all children with temperature>
39C with empiric antibiotics.
Baraft (1993, review article)10Same recommendations as above.
Baraff (1992, management guidelines)11Blood culture and empiric antibiotics. CBC is not recommended.
Bass (1993, 519 patients)12WCB 15,000 and fever 39.5 C identify children at high risk and should
be treated with antibiotics (amoxicillin/clavulinate orceftriaxone). Routinetreatment of others does not appear to be indicated.
Downs (1991, decision analysis)13Blood culture and empiric antibiotics for all those at risk (2-4 months and
rectal temperature > 39 C).
Fleisher (1994, 6680 patients)14If empiric antibiotics are given, ceftriaxone provides a safe and effective
alternative (better outcome profile compared to amoxicillin, however, not
statistically significant).
Jaffe (1994, review articel)10CBC. Blood culture and empiric antibiotics if WBC > 10,000 or WBC >
15,000/
Kramer (1989, decision analysis)16No blood culture strategy has the greatest utility.
Lieu (1991, decision analysis)17Blood culture and empiric antibiotics.
Long (1994, editor’s column)18No tests, no antibiotics as the preferred choice.
Singer (1995, review article)193-6 months: Urinalysis. Parenteral ceftriaxone is not effective. No blood
work unless temperature exceeds 41 C.6-24 months: CBC and blood cultures it temperature 40 C. Treat with
parenteral antibiotics if WBC 15,000.
ing. Most of the controversy stems from a subjective sense of risk
tolerance. Most studies and reports in the literature on this topic
have identified the children at risk for occult bacteremia as those
from 3 months to 36 months of age with a fever (most commonly
defined as greater than or equal to 39 degrees Celsius).8’9’13’17’8
Reports which focus on avoiding risk (risk averse) have recom
mended blood cultures and parenteral antibiotics for most or all
children at risk of bacteremia.’3”7Other reports which accept
prudent risk have recommended observation.’8Other reports have
recommended that white blood counts be used to assist in the
decision to administer antibiotics.8’9’2’5If antibiotics are to be
administered, the decision of parenteral or oral antibiotics must be
made on similar risk tolerance
While practice guidelines for the evaluation and treatment of these
children have been published in the journals Pediatrics and Annals
ofEmergency Medicine,8’9published surveys of pediatricians dem
onstrate that there is substantial diversity in the management of
these children and many pediatricians do not follow the recommen
dations in the published guidelines.23’24It is NOT the purpose of this
report to examine the superiority of one strategy over another.
MethodsA single page information sheet was drafted explaining bacter
emia, urinary tract infection, meningits, and pneumonia (see appen
dix A). Children were evaluated in the emergency department by the
author (single investigator) during a normal shift schedule in a
pediatric E.D. Parents were given this information sheet if all of the
following criteria were met:a. Age 3 to 36 months.b. Temperature> 38.9 degrees C (102 degrees F) in the E.D. or
by reliable history.8c. No hard indications to perform tests or administer parenteral
antibiotics.d. Child is active, alert, not toxic, not irritable.
f. No specific physical examination signs of meningitis, urinary
tract infection, pneumonia, or sepsis. Specifically, the following
were documented: anterior fontanelle (ifpresent) flat, neck supple,
not fussy when bounced, no costovertebral angle tenderness evi
dent, lungs clear to auscultation, no tachypnea, not coughing much,
oxygen saturation in room air 98% or higher, no petechia, normal
color, and normal perfusion. Patients were excluded if more than
two episodes of diarrhea (per day) were present. Otitis media was
not a basis for exclusion.g. The physician had enough time (15 minutes minimum) to
thoroughly review the information sheet with the parents (i.e., low
E.D. patient census at the time).
The information sheet was reviewed with the parent(s) verbally.
Following this lengthy verbal explanation, parents were given the
information sheet to review on their own. All their questions were
answered. All parents claimed that they understood the form. They
were encouraged to ask more questions following all explanations.
A Tests and Treatment Selection sheet (see appendix B) was
verbally reviewed with parents. The treating physician made a
recommendation for laboratory work and antibiotics. It was made
clear to patients that a different physician may justifiably make a
totally different recommendation. It was made clear that the
physician’s recommendation is not necessarily what their private
physician would do. It was made clear that they would not be
offending the physician if they did not follow the physician’s
recommendation. Parents were then asked about their preferences
on the diagnostic tests to be performed and the treatment. Parents
were given the option of not deciding (i.e., accepting the physician’s
recommendation). Once parents made a decision, the advantages
and disadvantages of their decision were again reviewed with them
to be certain that they understood the risk level involved in their
choice.Clinical and demographic information were collected on these
patients. Parent choices were stratified by demographics. There is
no control group involved. Presumably, a control group would be
HAWAII MEDICAL JOURNAL,
314
VOL 56, NOVEMBER 1997

one in which parents had no control in any of the clinical decisions.Such a control group would be highly biased by the treatment thatis imposed upon them by their physician. Thus, the statistics arepresented as descriptive only (no inferential statistics).
Antipyretics were administered to all patients (either at home orin the E.D.). Temperatures were rechecked in most patients beforedischarge.
This study was presented to the medical center’s institutionalresearch board (IRB) for review. IRB approval was obtained.
ResultsThe results of 37 E.D. patients are summarized in tables 2 and 3.
Ages ranged from 3.5 to 35.6 months of age (mean 14.4 months,standard deviation 9.4). Parents accompanying children ranged inage from 17 to 42 years of age (mean 28, standard deviation 7). Ininstances when both parents accompanied the child to the E.D., theage of the “dominant parent” was used as the parent’s age for thatchild (tables 2 and 3). The dominant parent was the one whoappeared to be making most of the decisions. Of the 37 patients,mothers were present alone in 21 cases, fathers were present alonein 2 cases, and both parents were present in 14 cases. Of the 14 caseswhen both parents were present, the mother was assessed as beingthe dominant parent in 6 cases and the father in 8 cases.
Maximum temperatures ranged from 38.9 to 41.1 degrees C(mean 39.8, SD 0.5). Otitis media with effusion was diagnosed in 22of the 37 patients. Five of the 37 patients presented with febrileseizures. Only one of the 37 patients was on antibiotics prior to theE.D. visit.
Table 2 stratifies the parental diagnostic test preferences bydemographic and clinical variables. In 2 of the 37 cases, parents didnot want to make a choice. In these two instances, no diagnostic testswere performed. In 31 of 37 cases, the physician made no recommendation on whether to do any tests. In 25 of these 31 instances,parents chose to do no tests. The physician recommended “no tests”in three cases. Urine studies only were recommended in one case (17month old female with fever and vomiting), however, parentselected for no tests in this instance. A CBC and blood culture wererecommended in one case (24 month old with a febrile seizure inwhom the child’s primary care physician requested the tests). Acomplete sepsis work up was recommended in one case (a 3.5 monthold). Parents concurred in these two cases.
When a diagnostic test recommendation was made by the physician (6 instances), parents agreed with this recommendation in fourinstances. In one case, urine studies were recommended and theparent declined this. In one case, the parent declined to make achoice and the physician’s recommendation was carried out. Thus,in no instance, did parents request more tests than that recommended by the physician.
Of the 31 cases where the physician did not make a diagnostic testrecommendation, there were four cases where parents requestedtests. One case was a 17-month old whose parents requested a chestradiograph. In two cases, parents (of an 11-month old and a 3.5-month old) requested a CBC and blood culture. The last case was 24-month old with a febrile seizure whose parents requested a completesepsis work-up.
Parental diagnostic test preferences did not differ significantly byany of the variables tabulated in table 2. However, the numbers here
Table 2.—Parental diagnostic study preferences (these tests were theones actually carried out)
Parents’ preference: No Tests Doesn’t want(studies consented to) Tests done to choose
All 29 6 2
Age3-5 months 3 2 16-12 months 14 1 013-36 months 12 3 1
SexMale 16 4 2Female 13 2 0
ParentMother 16 4 2Father 1 1 0Both 12 1 0Age24 13 1 0Age25 16 5 2
Medical InsurancePrivate 13 3 1Medicaid 15 2 0None 1 1 1
Doctors recommendationNo tests recommended 2 0 1Tests recommended 1 2 0No recommendation 26 4 1
Max temperature38.9to39.9 16 4 140.0 to 42.0 13 2 1
Otitis MediaPresent 16 4 2Not present 13 2 0
SeizurePresent 3 2 0Not present 26 4 2
are too small to come to any conclusion.Table 3 stratifies the parental antibiotic choices by demographic
and clinical variables. In three cases, parents declined to make anantibiotic choice. In two of these cases (with otitis media), oralantibiotics were prescribed. In the third case, no antibiotics wereprescribed.
There was a physician antibiotic recommendation in 31 of 37cases (no antibiotics in 1, oral antibiotics in 28, and parenteralantibiotics in 2). Antibiotics were recommended by the physician inall 22 cases in which otitis media with effusion was diagnosed.Parents followed the physician’s recommendation in most instances. However, in 8 instances, parents chose parenteral antibiotics when the physician recommended oral antibiotics. In one instance, parents chose no antibiotics when the physician recommended oral antibiotics. In one instance, parents chose oral antibi
HAWAII MEDICAL JOURNAL, VOL 56, NOVEMBER 1997315

office. All patients were informed to return to the ED. if their
condition worsened. No patient returned to the E.D. for a follow-up
visit or to the hospital for hospitalization.
otics when the physician recommended parenteral antibiotics.
Parents of 34 of the 37 children indicated that they liked helping
the physician decide the treatment for their child. In two cases,
parents indicated that they did not like helping the physician decide
the treatment for their child. In one instance, a parent could not
decide.Temperatures at discharge declined in 31 of 37 patients compared
to their admission temperature. Discharge temperatures were not
obtained in two patients who presented with admission E.D. tem
peratures of 38 degrees or less rectally (fever documented at home).
The temperature in one child did not decline. Discharge tempera
tures in the other three patients were not recorded on the charts. It
is possible that the discharge temperatures were not obtained, or
they were obtained, but not recorded.All blood cultures obtained (five) were negative. Follow-up was
arranged for all patients in a clinic or their primary care physician’s
DiscussionThe possibility that the wording of the information sheet used in
this survey may be biasing the decisions of parents is acknowl
edged25 The information sheet was written to remain as neutral as
possible. Yet the infomation sheet had to be simple and short. It
would be impossible to write an information sheet that is simple,
short, and perfectly accurate while satisfying all experts that its
wording is perfectly neutral. This less than perfectly accurate and
less than perfectly neutral information sheet was adopted realizing
its limitations.It is likely that the preference choices made by parents were
substantially influenced by the recommendation of the treating
physician. However, the noted trend is that most parents chose no
tests in the absence of a physician’s recommendation. While most
parents followed the physician’s antibiotic treatment recommenda
tion, some parents chose more aggressive antibiotic treatment
options (parenteral) than the physician’s recommendation (oral).
The high number of antibiotic recommendations by the physician
makes it difficult to determine what the true antibiotic preferences
of the parents were. However, many children in this cohort were
diagnosed with otitis media with effusion and the risk factors ofeach
individual case had to be weighed by the physician making the
individual treatment recommendation to fit the ethical standard of
what was felt to be best for the individual child.
While the informed consent information disclosed during this
survey was largely limited to that listed in appendix A for most
cases, some parents asked for more details regarding specific
aspects of their child’s condition. The following issues were dis
closed in lay terms on an as needed basis. It is obvious, that the
disclosure of all these details would not be possible during a single
patient encounter.The frequency of otitis media with effusion2627 in this group of
patients was high. In all instances, the severity of the otitis media
was felt to be low (otitis media with effusion as opposed to acute
otitis media).26’27 Parents were informed of this and in every case,
they were informed that such mild otitis media does not reliably
account for the fever28’29and their child’s risk for bacteremia and its
complications are no different than a child without otitis media.3°In
patients with otitis media, empiric antibiotics were recommended
whether or not blood cultures were obtained. The high frequency of
otitis media with effusion accounts for most ofthe empiric antibiotic
recommendations without obtaining a blood culture. Yet in one case
of otitis media with effusion, parents declined antibiotics when they
were informed that the likelihood of recovery following a course of
antibiotics was only slightly better than the likelihood of spontane
ous recovery26’27’334(all parents of children with otitis media were
advised of this).While patients with otitis media may be considered by some to be
a “source” of fever, it is often considered to be a source that is not
clinically useful in modifying risk since otitis media is associated
with a similar risk of bacteremia compared to febrile children
without otitis media.3°Fever without a source can be defined as an
instance in which the etiology of the fever is not apparent after a
careful history and physical examination.10In most instances, it is
Table 3.—Parents antibiotic (Abx) preferences (the actual treatmentscarried out)
Parents’ preference: No Oral Parenteral Doesn’t want(treatment consented to) Abx Abx +PO Abx to choose
All 4 20 10 3
Age3-5 months 1 2 3 06-12 months 3 6 5 113-36 months 0 12 2 2
SexMale 3 11 6 2Female 1 9 4 1
Medical insurancePrivate 2 10 4 2Medicaid 2 9 5 0None 0 1 1 1
Tests done(parents’ preference)
Notests 3 19 6 1Tests done 1 1 3 1Doesn’t want to choose 0 0 1 1
Physician’s antibioticrecommendation
No recommendation 2 2 1 1No antibiotics 1 0 0 0Oral antibiotics 1 17 8 2Parenteral antibiotics 0 1 1 0
Max temperature38.9to39.9 3 11 5 2
40.0to42.0 1 9 5 1
Otitis MediaPresent 1 13 6 2Not present 3 7 4 1
SeizurePresent 0 4 0 1Not present 4 16 10 2
HAWAII MEDICAL JOURNAL, VOL 56, NOVEMBER 1997
316

Appendix A - Information Sheet
HAWAII MEDICAL JOURNAL,317
Information: Tests and Treatment For ChildrenWith Fever Physician’ s Name, MD, Pediatrician
The doctor has examined your child and has found that the cause ofyour child’s fever is probably not serious, Most of the fever is mostlikely caused by a virus (like the flu virus). Antibiotics will not help yourchild get rid of the virus. Since no doctor can be absolutely sure that thisfever is only caused by a virus, we must discuss some other possibilitieswith you.
get worse and spread infection to the blood and brain. Children withkidney infections often have abnormal kidneys. We won’t know aboutthis since you can’t feel the kidneys. You can only see them with specialX-rays with X-ray dye. To check for urine or kidney infection, we needa sample of urine. We can’t ask small children to urinate in a cup so forsmall children, we get a urine sample by putting a tube in the bladder tolet some urine out. Your child won’t like this, but it is quick and it won’tcause any harm. Sometimes there is some bleeding from this, but thiswill go away on its own.
3. Meningitis (infection in the brain). There are many types ofmeningitis. Some meningitis is not too bad, but the bad form ofmeningitis can kill you or cause permanent brain damange unless it istreated early. Children with meningitis usually look very, very sick.They usually have vomiting, a stiff neck, a bulging soft spot, or a badheadache. They are usually fussy, drowsy, or don’t look at you well.Since they have a bad headache, this gets worse if you bounce themwhile carrying (they get more fussy if you do this) or if they jump up anddown. A spinal tap is needed to find meningitis. A spinal tap is painful,but it is usually quick (1 to 3 minutes), and it will not harm your child.
4. Pneumonia (lung infection). Most pneumonias are not serious ifyour child’s oxygen level is normal (we measured this with the redlight). To find out if your child has pneumonia, we need to do a chestX-ray. X-rays can be harmful, but the dose of X-rays in a chest X-rayis very small. Doctors believe this to be very safe.
1. Bacteria in the blood (bacteremia). There is roughly a 2% to 10%chance that your child may have bacteria in the bloodstream. This is notnecessarily bad. Children with bacteria in the bloodstream will curethemselves most of the time (even without antibiotics). However, about1% to 5% of the time, a child may get a complication from this (such asone of the infections below). To find out if your child has bacteria in thebloodstream, we must draw a blood sample and grow this sample in thelab for 2 days to see if any bacteria will grow out. We will not be ableto find out today ifyour child has bacteria in the bloodstream. It will take2 days. We could do a blood count test today to find out if your child isat high risk or low risk of bacteria in the bloodstream, but this test is notalways accurate. Many children with bacteria in the bloodstream havenormal blood counts and many children with abnormal blood counts donot have bacteria in the bloodstream. If we give your child someantibiotics, this might lower the chance that your child will get worse ifyour child has bacteria in the bloodstream. An antibiotic shot seems tobe better than antibiotics by mouth. If your child has had all his/herimmunizations (RIB vaccine), then his/her risk of complications frombacteria in the blood is even lower.
2. Kidney infection. There is a small chance that your child mighthave an infection in the urine or kidneys. Young children don’t usuallytellus that itburns when they urinate. Ifuntreated, a kidney infection can
Doctor’s Survey: Since your child has fever, you should know thatthe tests and treatment for this are very controversial. If you ask 10pediatricians what to do, you will get many different answers. Mostoffice or clinic pediatricians would not do any tests. Some would doblood tests only. Some would do blood tests and a urine test. Otherdoctors would do all the tests. We would like to give you some choiceson how to approach this.
Please understand that all of these tests are safe.
Appendix B - Tests and Treatment SelectionSheet
Doing all these tests is the safest approach. On the other hand, we don’twant to do any unnecessary tests.
The doctorrecommends:
Do you want us to treat your child with antibiotics?D No antibiotics
Antibiotic shots (high dose) - treats some hidden infections, butnot guaranteed to prevent worsening
Antibiotics by mouth - might treat some hidden infectionsL I don’t want to choose. I want the doctor’s Recommendation
If you would like us to do more tests or less tests than the doctorrecommends, please tell us and we can discuss this.
Check one:I don’t like helping the doctor decide the treatment for my child.
J I like helping the doctor decide the treatment for my child.
Do you want us to do these tests?I don’t want to choose, I want the doctor’s recommendation.Yes L No Blood tests - checking for bacteria in the bloodstreamYes No Urine test - checking for urine or kidney infectionYes No Spinal tap - checking for meningitis (brain infection)
D Yes No Chest X-ray - checking for pneumonia (lung infection)
You are child’s: Mother LI Father LI Other
How old are you?
I understand that doctors do not agree on which tests should be donefor fever.I understand that the doctor has offered me all of these choices.I understand that no choice is guaranteed to be perfect.
VOL 56. NOVEMBER 1997

[aste,BenzamYCifl® worksFor visible results in as little as 2 weeks.1• More than 12 million prescriptionSwritten in the U.S. since introduction?
•Large size (46.6 g) for addedconvenience.

Adverse conditions infrequently reported include dryness,erhema, and pruritus.Artistic representation, not an actual case. Treatmentoutcomes varyPlease see references and prescribing informationon adjacent page.
than the speed oflife.tZAMYCIN®Topical
(3% erythromydn, 5% benzoyl peroxide)
Better results faster3

Benzamycinn(erythromycin-benzoyl persxkle topical gel)
Topical gel: Orrfthrnmycin (3%), benznyl peroxide (5%)For Dermalsingical Use Only — Not fur Ophthalmic Use
Reconslilute Before Dispensing
Brief Summary—Cnnselt package insert fsr full prescribing informal ion,
INDICATIONS AND USAGEBENZAMVCIN Topical Gel is indicated for the topical treatment of acne vulgaris.
CONTRAINDICATIONSBENZAMYCIN5Typical Gel is csntraindicatod in those individuals whn have shows hyporsonsitisiny to any slits companents.
WARNINGSPsendamembrannns culitis has been repnrlod with nearly all antibacterial agents, including eryfhmmgciu, and may range in neverityfrom mild In life-threatening. Therefore, it is important to cnnsider this diagnosis in palients who present with dianirea sobsequonl Inthe administratimr of antihactorfal agents.Treatment with antibacterial agents alters the normal flora at the colon and may permit nsergrowth of clnstridia. Stadien indicate that a tosin produced by Clsatridiam difficile is nno primary casse at “antibiotic-asnsciatod colitis.”After the diagnosis at pseadsmembranoas colitis has been established, therapeatic measares ohnold be initiated. Mild cases ofpseudomembransan colitis asually respond In drug discnntinaatisn alone. In mnderate In severe cases, consideration shsald begiven ts management with tlaids and electrolytes. prstein supplementation and treatment with as antibacterial drag clinically effective against C. difticile cnlitis.
PRECAUTIONSGeneral: Far tnpical use nn’; nut toe ophthalmic ave. Cancnmdant tapical acne therapy shnuld beaned ssdh cautian because a possible cumulative irritancy effect ivay occur, especially with the use of peeling, denqaamating nr abrasive agents. If severe irritationdevelops, discontinue use and institute appropriate therapy.The use of antibiotic agents may be assnciated with the svergrnwth of nonousceptible nrganisms including fungi. It this accurs,discontinue sue and take appropriate measures.Avoid contact wdh eyes and all macnun membranes.Infnrmalion fur Patients: Patients using 8ENZAMYCINS Topical Gel shsuld receive the fslluwing intormatiun and instructions:
1, This medication is to be used as directed by the physician. It is tsr estersal use nnly Assid contact with the eyes. nsse, mseth.and all macset membranes.
2. This medication should not be used tsr any disorder other than that tsr which it was prescribed.3. Patients shusld nut sue any ather topical acne preparation unless stherwise directed by physician.4. Patients should report tn their physician any signs of local adverse reactions.5. 8ENZAMYClN Tspical Gel may bleach hair ar colored fabric6. Keep product refrigerated and discard after 3 months
CARCINOGENESIS, MUTAGENESIS AND IMPAIRMENT OF FERTILITYData from a study using mice known to be highly susceptible to cancer suggests that benzuyl persuide acts as a Iumnr pro-muter. The clinical significance of this is unknswn.Nu animal studies have bees performed to evaluate the carcinugenic and mutagenic putential ur effects on fertility ut tspical erythrnmycio. However, lung-term (2-year) oral studies in rats with eiethrumycin ethylsuccisate and erythrsmycin base did nutprsside evidence of tumorigenicity. There was sa apparent effect us male or female fertility in rats ted erythromycis (base) atlesols up ts 025% at diet.Pregnancy: Toratngenic Effects: Pregnancy CATEGORY C: Animal reproduction studies haue nut been cnnducted wdh BENZAMYCIN5Tupical Gel sr benzuyl peroside.There seas no evidence uf teratsgenicity or any nther adverse effect an reproduchon in female rats ted erythrnmycin base (uptn 0.25% diet) prinr tn and during matiag, during gentatisn and through weaning nf two successive lifters.There are us well-csntrolled trials in pregnant wumen with BENZAMyCIN5Tspical Gel. It also is not known whether BENZAMYCIN5Tspicsl Gel can cause fetal harm when administered to a pregnant woman yr can affect repruductive capacity. BENZAMYClN TnpicalGel should be given to a pregnant woman unly if clearly needed.
Nnrsing Women: It is nut iowo whether BENZAMYClN Typical Gel is eacreted is human milk after tepical applicaban. Howevecerythrsmycin is eucreled in human milklsllnwing oral and parenteral erythrsmycis administratiun. Therefsre, caution shnuld be eoercised when orythrsmycis is administered Is a nursing woman.
Podiatric Use: Safety and effectiveness of this pruduct in pediatric patients below the agent f2 have not been established.ADVERSE REACTIONSIn csnfrolled clinical trials, the total incidence of adverse reactions associated with the use ut BENZAMYClN Topical Gel wasapprooimstsly 3%. These were dryness and urticarial reactiun.The tolluwing additional local adverse reactions hase been reported sccasiunally: irritation of the skin including peeling, itching,
burning sensation, erythema, inflammation of the face, eyes and nose, and irrfatiun at the eyes. Skin dincnloration, oiliness andtenderness of the skin have also been reported.
DOSAGE AND ADMINISTRATIONBENZAMYCIrTspMicaI Gel ohould be applied twice dady, morning and evening, or as directed by a physician, In affected areasafter the skin is thoroughly washed, rinsed with warm water and gently patted dry.
Important In the PharmacistPrior In dispensing, lap vial until puwdor Ilaws freely. Add indicated amend of ethyl alcnhnl (70%) In vial (le Ihe mark) andimmediately shake In cumpletely dissalve erytfrromycin. Add this solution to gel and stir until homogeneous is appearance
)f tu 1½ minutes). BENZAMYClN Tspical Gel shnuld then be stored under refrigeration. Do not freeze. Place a 3-mnnth enpiration date on the label.
NOTE: Prior to reconstitution, store stream temperature I,etween 15arro’ 311 ‘C (59’— 86’r7.After reconsilIntion, store under refrigeralinn between 2’ and 8’C (36’ — 46’F).
On not freeze. Koop lighlly claned. Keep net of the reach of children.
Caotioe: Federal (U.S.A.) law prohibits dispensing witheul prescription.U.S. Palest Nns. 4,307,107 and 4.497.794Manufactured by RhOne-Poulenc Rorer Puerto Rico Inc.Manati, Puerto Rico
Fsr DERMIK LABORATORIES, INC.A Rhhne-Psulenc Rarer Company DERMIK LABORATORIES, INC.Csllegevifle, PA 19426 dieesdisDsvioyy
Rev. 12/95 19-712W
tbr
Cost EffectiveAlternativesto Hospitalization
Call Hawaii’s mostexperienced provider
of home infusion therapies
PHARMACAFEWE MAKE YOUR JOB EASIER
SERViNG ALL ISLANDSJCAHO Accredited with Commendation
99-1260 Iwaena St., #100, Aiea, HI 96701Main Office (808) 488-9446Hilo Branch Office (808)961-5115
child’s temperature decreased. Parents were in
formed that such a favorable temperature re
sponse to antipyretics does not rule out the
possibility of serious infection.3541 Similarly, aclinical observation scale was not found to beuseful in detecting bacteremia.42Despite these
limitations, documentation of the child’s vital
signs and general appearance at discharge, if all
favorable, are added evidence to support a be
nign clinical assessment. It is common for an
hour to elapse following an admission dose of
antipyretics because ofpatient registration, phy
sician availability, review of the necessary in
formation, family discussion, charting, discharge
instructions, etc. Even in cases where antipyretics
were given late in the ED. visit, or the duration
of the E.D. visit was briefer than usual, all parents were willing to
stay in the E.D. for up to 45 minutes for a period of observation and
follow-up vital signs and clinical assessments.
Parents were informed that “expert” recommendations vary. This
listing in table 1 is not meant to be complete, but rather to illustrate
the spectrum of recommendations (for a more complete reference
list, refer to Singer, et alt9). Note that most of these reports are not
publishing recommendations based on newly acquired data, but
rather rely on data collected in the past. The two recent studies of
children (Basst2 and Fleishert4)both focused on comparing oral
antibiotics with parenteral antibiotics. Given the widespread use of
not convincing that otitis media is the source of a high fever28’29and
bacteremia risk is not altered by the presence of otitis media.3°
Additionally, otitis media is poorly defined and it ranges from
minimal to severe without an objective standardized severity scale.26’27
Otitis media results in fever in roughly 50% of cases.28’29 Febrile
children with otitis media often have a concurrent viral infection28’29
(and occasionally bacteremia30)which may be the actual cause of
the fever rather than the otitis media itself. Because otitis media
cannot be reliably considered to be the source of a fever, these
children should be considered at similar risk for bacteremia.
Anecdotally, parents seemed to feel some relief when their
HAWAII MEDICAL JOURNAL, VOL 56, NOVEMBER 1997
320

H. influenzae B vaccine in infants, it is likely that the most virulentof the common bacteremial organisms is likely to be less prevalentif a study of bacteremia were to be repeated today. Thus, theconclusions reached by even the most recent of studies available tous may only have limited applicability to the contemporary cohortof children. The likelihood of a bad outcome is likely to be lowercurrently, than it has been in the past)8
Although empiric antibiotics are often administered withoutobtaining a blood culture, this choice receives negative reviewsfrom most experts, because it does not permit clinicians to identifypatients with bacteremia.8”8It may also mask other existing infections such as meningitis and urinary tract infections. The magnitudeof this potential problem is difficult to measure. In discussions withparents, this issue does not appear to concern them as much as otherissues. In fact, the most frequent diagnostic/therapeutic choice wasthat of no tests with oral antibiotics (most of these cases had otitismedia). It should be noted that:
1. The practice of administering a 10-day course oforal antibioticswithout a blood culture is done very frequently in offices andemergency departments in the routine treatment of fever associatedwith otitis media. The frequency of bacteremia and its complications in children with otitis media is argued to be roughly similar tothat of similar children without otitis media.’4’3°The number ofthese febrile children who are not cultured probably greatly outnumbers patients in the E.D. identified as at risk for occult bacteremia. Yet there has been no substantial published concern recommending blood and/or urine cultures for febrile children prior toantibiotic treatment for otitis media.
2. Despite obtaining a blood culture, the decision of whether tohospitalize a patient with pneumococcal bacteremia is based on thepatient’s clinical status (persistent fever vs. afebrile and well-appearing) at the time of the positive blood culture (ito 3 days later)and not solely on the blood culture (unless it is positive for a morevirulent organism).8’9Thus, regardless of the blood culture results(positive, negative, or not obtained) and regardless of whether apatient is on antibiotics at the time of follow-up, patients who are notdoing well, should be investigated and treated more aggressively.8’9
This small survey of patients and parents described in this reportdemonstrates that most parents are willing to digest substantialamounts of medical information in a reasonably short period oftime. The degree to which they understand this information was notmeasured in this survey. In the typical patient encounter, comprehension cannot always be objectively and accurately assessed.Clinicians must generally rely on communication skills and feedback from the patient/parents to assess comprehension. In thissurvey, once parents received the information, nearly everyone waswilling to express a preference and in most instances, their preference was not in favor ofperforming tests. Nearly everyone preferredto participate in the medical decision making involving their child.While this process was extremely time-consuming for the clinicianand possible only during periods of low ED. census, most parentsseemed to appreciate the information and time spent.
Since the diagnostic and therapeutic decisions involved in thefebrile child at risk for occult bacteremia are controversial, it isdifficult to say with certainty that any given approach is scientifically superior to all other approaches. Despite the lack of scientificcertainty, practice guidelines have been published.8’9Practicingpediatricians do not appear to consistently follow these guide-
lines23’24 and thus, the controversy has not ended.4345 While physicians may often feel the need to obtain a blood culture and administerceftriaxone to febrile children who do not appear ill, would theytake this same approach for their own son or daughter? One studyindicates that they would not follow the practice guidelines for theirown child.46 Regardless, this choice, which is available to physicians, may not be offered to other patients if the practice guidelinerecommendations are imposed upon patients without disclosure ofalternatives. Informed consent contemplates that patients shouldcollaborate with physicians in developing and evaluating treatmentoptions, with patients having a veto over any proposed treatment.2
Similarly in this report, parents were given information on theissue of febrile children (without a source). Informed consentshould disclose to patients all information “material” to making adecision whether to undergo or forgo a proposed treatment ordiagnostic procedure.”2This would include the disclosure of risks,benefits, and alternatives.”2
Medical legal liability concerns with informed consent raiseadditional controversy.6Are parents capable of making informedconsent decisions? Will physicians be held liable if physicianscomply with parents’ preferences? Does involving the parents in thedecision making process result in more liability risk or less liabilityrisk?
The above questions are difficult to answer and these issues arebeyond the scope of this report. However, if the choice is to discloseor withhold information about alternative approaches (discussion ofthe range of diagnostic and therapeutic strategies), the doctrine ofinformed consent states that we must not withhold the information,regardless of what one’s opinion of the medical legal liabilityconsequences is.2While this may be ideal from an informed consentperspective, most practicing physicians find this to be extremelytime consuming and often not possible in their practice.
A general principle of reducing malpractice risk is to disclose andacknowledge the presence of uncertainty with patients. Whilephysicians prefer to form clear and accurate diagnoses and treatment plans for their patients, uncertainty exists.47 It should beaccepted by and acknowledged by the physician and the patient.Disclosing the issues of controversy acknowledges this uncertainty.47When uncertainty presents choices, people make decisionsappropriate to a level of risk that they can tolerate. The “processmodel” of informed consent (where patient and physician interact inan ongoing relationship sharing information, clinical results, diagnostic/therapeutic choices/recommendations, and personal/culturalperferences2)provides an opportunity to establish a therapeuticalliance between physician, patient, and family48 where the physician, patient, and family are all co-active in sharing responsibility49and hence, risk. Many health care risk managers agree that such aprocess might reduce malpractice risk.48
In this survey, patients weighed the potential harm and discomfortto their child from tests and treatments against the potential benefitof the same. Since the tests and treatments are largely harmless, thedominant negative factor remaining is pain sustained by their child.Thus, most parents did not perceive the benefits of blood culture tooutweigh the pain consequence. The practice guidelines recommending blood work on all these patients8’9would suggest that thewisdom of experts should outweigh the wisdom of parents. Themonetary cost of the tests was never considered by patients in thissurvey. Nearly all the patients were insured and their out of pocket
HAWAII MEDICAL JOURNAL, VOL 56, NOVEMBER 1997321

expenses for a CBC and blood culture would range from zero in
most instances to up to 20% of the insurance carrier’s pre-negotiated
preferred laboratory rates. Thus, most parents declined the tests
even if their out of pocket expenses were zero or a minimal cost.
These results are consistent with those found in a focus group of
33 parents choosing treatment options for a hypothetical 6-week old
infant with fever, in which parents tended to choose options that
involved less testing and more risk.20 Another study demonstrated
that parents and physicians differ in the way they value the benefits
and consequences of the tests, treatments, and outcomes of children
at risk of bacteremia.5°Parents emphasize the short-term pain,
discomfort, and inconvenience of the tests and are more willing to
risk rare but severe long-term morbidity to avoid the short-term
consequences of testing.5°These factors account for the findings of
our survey.While physicians may find it less time consuming (and often
preferable) to impose their diagnostic and therapeutic plans upon
patients, informed consent requires that we spend more time with
patients discussing significant alternatives. This report shows that
this can be done even in a complex and controversial clinical
decision making scenario such as this. This process, however, is
very time consuming. A standardized information sheet reviewed
by a nurse may be a more efficient way of insuring informed
consent. This process would be similar to condition specific dis
charge information sheets that are reviewed with patients by nurses
or physicians at discharge. Such condition specific information
sheets can be composed for other conditions where decision making
is complex and controversial to optimize and document the process
of informed consent.In summary, favorable points of informed consent are presented
where risks, benefits, and alternatives are disclosed. From the data
presented, we can conclude the following: 1) Parents overwhelm
ingly prefer to be included in the medical decisions affecting their
child. 2) Under the circumstances of this study, most parents were
not in favor of obtaining CBC’s and/or blood cultures. 3) No
conclusion can be drawn regarding the empiric antibiotic prefer
ences ofparents since antibiotics were recommended by the treating
physician in most instances. 4) The process of informed consent is
time consuming and often not possible when the E.D. is busy.
Physicians may find it desirable to make decisions from an informed
consent perspective to a comfort level dependent on time availabil
ity, parents’ comprehension ability, and individual personal prac
tice preference.
References1. Committee on Bioethics, American Academy of Pediatrics. Informed consent, parental permission, and
assent in pediatric practice. Pediatrics 1995;95(2):314-317.
2. Lidz CW, Appelbaum PS, Meisel A: Two models of implementing informed consent. Arch tnt Med
1 988;148:1385-1389.3. Beauchanp TL, Childress JF. Principles of Biomedical Ethics, third edition, NewYork: Oxford University
Press; 1986.4. Applebaum PS, Lidz CW, Meisel A. Informed Consent: Legal Theory and Clinical Practice, New York:
Oxford University Press; 1987.5. additional informed consent source.6. Bussey GD. Informed consent: Its legal history and impact on medicine. Hawaii Med J 1 995;54:472-
475.7. JointComrnission on Accreditation of Healthcare Organizations. ComprehensiveAccreditation Manual
for Hospitals, The Official Handbook. Joint Commission on Accreditation of Healthcare Organizations,
Oabrook Terrace, IL, 1996, Standard Rl.1.2.1, p. Rt-9.
8. Baraft U, Bass JW, FleisherGR, etal. Practice guidetine forthe management of children 01035 months
of age with fever without a source. Ann Emerg Med 1993;22:1 198-1210.
9. Baraff U, Bass JW, Fleisher GR, et at. Practice guideline for the management of intants and children
01036 month of age with fever without a source. Pediatrics 1993;92(1):1-12.
10. Baraff U. Management of infants and chitdren 3 to 36 months of age with feverwithout source. Pediatr
Annals 1 993;22(8):500-504.11. Baraff U, Lee SI. Feverwithouta source: Management of children 3 to 36 months of age. Pediatrlnfect
Dis J 1992;11(2):146-151.12. Bass JW, Steele RW, Wittier BIt, et al. Anfimicrobial treatment of occult bacteremia: a muitcenter
cooperative study. Pediatr Infect Dis J 1 993;12(6):466-473.
13. Downs SM, McNuff RA, Margolis PA. Management of infants at risk for occult bacteremia: A decision
analysis. J Pediafrl99l;118(1):11-20.14. FleisherGR, Rosenberg N, Vinci R, et at. tntramuscularversus oral antibiotictherapyforthe prevention
of meningitis and other bacterial sequelae in young, tebrile children at risk for occult bacteremia. J
Pediatr 1 994;124(4):504-512.15. Jaffe DM. Occult bacteremia in children. Adv Pediatr Infect Die 1994;9:237-260.
16. Kramer MS Lane DA, Mills EL. Should blood cultures be obtained in the evaluation of young febrile
children without evident focus ot bacterial infection? A decision anatysis of diagnostic management
strategies. Pediatrics 1 989;84(1 (:18-27.17. Lieu TA, Schwartz JS, Jaffe DM, FLeisher GB. Strategies for diagnosis and treatment of children at
risk for occult bacteremia: Clinical effectiveness and cost-effectiveness. J Pediatrl 991:118(1 (:21-29.
18. Long SS.Antibiotictherapyintebritechildren: “Best-laid schemes . JPediatrl994;124(4):585.588.
19. SingerJl, VestJ, PrintsA. Occult bacteremia and septicemia in the febrile child youngerthan twoyears.
Emerg Med Clin North Am 1995;13(2):381-416.20. Oppenheim P1, Sotiropoulos G, Baraft U: Incorporating patient preferences into practice guidelines:
Management of children with fever without a source. Ann Emerg Med 1 994;24:836-841.
21. Wald ER, Dashefsky B. Cautionary note on the use of empiric ceftriaxone for suspected bacteremia.
AnrJDis ChildlQ9f;f45:1359-1361.22. Baratf U, Oslund 5, Prather M. Effect of antibiotic therapy and etiologic microorganism on the risk of
bacterial meningitis in children with occult bacteremia. Pediatrics 1993;92:140-143.
23. Ros SP, Herman BE, Beissel TJ. Occult bacteremia: Is there a standard of care? PediafrEmerg Care
1994; 10(5):264-267.24. Young PC. The management ot febrile infants by primary-care pediatricians in Utah: Comparison with
published practice guidelines. Pediatrics 1995;95(5):623-627.
25. McNeil BJ, Parker SG, Sox HC, Tversky A. On the elicitation of preferences tor alternative therapies.
NEngIJMed 1982;306:1259-1262.26. Paradise JL. Treatment guidelines for otitis media: the need for breadth and flexibility. PediaIr Infect
Dis J 1995;14(5):429-435.27. Stool SE, Berg AO, Berman 5, et al. Managing otitis media with effusion in young children. Quick
reference guide tor clinicians. AHCPR Publication 94-0623. Rockville, MD: Agency for Health Care
Policy and Research, Pubtich Health Service, US Department of Health and Human Services. July
1994. (Alternative citation: Pediatrics 1994;94(5):766-773.)28. Niemeta Mario, Multi Uhari M, Jounio-Ervasti K, et. al. Lack of specific symptomatology in children with
acute otfis media, Pediatr Infect Dis J 1 994;1 3:765-768.29. Ruuskanen 0, Heikkinen T. Otitis media: etiology and diagnosis. Pediatr Infect Dis J 1994:13:S23-
S26.30. Schutzman SA, Pelrycki 5, Fleisher GR. Bacleremia with ottis media. Pediatrics 1991 ;87(1):48.53.
31. Rosenfeld RM, Vertrees JE, Carr J, et al Clinical efficacy of antimicrobial drugs for acute otitis media:
Metaanalysis of 5400 children from thirty-three randomized trials. JPecliatrl994;124:355-367.
32. Cantekin El, McGuire TW, Griffith TL. Antimicrobial therapy for otifis media with effusion (‘secretory’
otitis media(. JAMA 1991 ;266(23(:3309-3317.33. Paradise JL. Managing otitis media: A time for change (commentary). Pediatrics 1995;96(4):712-715.
34. Cunningham AS. Antibiotics for ofitis media: Restraint, not routine. Contemp Pediatrl994;11(3):17-
30.35. Bonadio WA, Bellomo T, Brady W, Smith D. Correlating changes in body temperature with infectious
outcome in febrile children who receive acetaminophen. Clin Pediafrl993;32(6):343-346.
36. Yamamoto LT, Wigder HN, Fligner DJ, ef al. Relationship of bacteremia to antipyrefictherapy in tebrile
children. PediatrEmerg Care 1987;3(4):223-227.37. Baker MD, Fosarelli PD, Carpenter RO. Childhood fever: Correlation of diagnosis with temperature
response to acetaminophen. Pediatrics 1987;80(3):315-318.
38. Baker BC, Tiller T, Bausher JC. Severity of disease correlated with fever reduction in febrile infants.
Pediatrics 1989;83(6):101 6-1019.39. Weisse ME, MillerG, Brien JH. Feverresponse to acetaminpt’ren in viral vs. bacterial intectons. Pediatr
Infect Dis J 1 987;6(12(:1 091-1094.40. Torrey SB, Henretig F, Fleisher G, ef al, Temperature response to antipyrefic therapy in children:
Relationship to occult bacteremia. Am J E,nerg Med 1 985;3(3):1 90-192.
41. MazurLJ, KozinetzCA. Diagnostictests toroccultbacteremia: Temperature responsetoacetaminphen
versus WBC count. Am J Enierg Med 1 994;12(4):403-406.42. Teach SJ, FLeisherGR, etal. Efficacy of an observation scalein defecting bacteremia infebnile children
three to thirty-six months of age, treated as outpatients. J. Pediatr 1 995;1 26(6):877-81.
43. Kramer MS, Shapiro ED. Management of the young febrile child: a commentary on recent practice
guidelines. Pediatrics 1997;1 00:(1 );1 28-134.44. BaratfUJ, BassJW, FleisherGR, etal. Commentaryon practiceguidelines. Pediatrics 1 997;100:(1 );134-
136.45. Bauchner H, Pelfon SI. Management of the young febnle child: a continuing controversy. Pediatrics
1997;100:(1);137-138.46. Yamamoto LG, Boychuk RB. Emergency Department versus Office Setting and Physidan/Patient
Kinship Effects in the Diagnostic and Therapeutic Choices of Febrile Children at Risk For Occult
Bacteremia. Hawaii Med J. 1997; 56:209-214.47. Carmi A. Medical decisions under uncertainty. Med Law 1993;12(3-5):277-281.
48. Hotzer JF. A new approach to informed consent can reduce claims. Pediatr Ann 1991 ;20(2):64-68.
49. Leaman TU, Saston JW. Preventing Malpractice: The Co-active Solution. New York, Plenum Medical
Book Company, 1993, pp.89-120.50. Kramer MS., Efezadi-Amoti J, Ciampi A, et at. Parents’ versus physicians’ values for clinical outcomes
in young tebrile children. Pediatrics 1994;93(5):697-702.

If your small business needs more financial resources and flexibffity, First Hawaiian Bank has theanswer — Business FirstLine, an unsecured, revolving line of credit. It offers the following features:
•Your own personal Business Banker • Overdraft protection• No collateral requirements • Business MasterCard• Cash when you need it • Combined statement• Simple one page application • And more
To apply for a Business FirstLine or to talk with a business bankingexpert like Rae, call 525-6262 (neighbor islands call collect) or visit anyconveniently located branch.
Yes, we have answers.

Common Sports Injuries Seen bythe Primary Care Physician
Part I: Upper ExtremityJames F. Scoggin, III, MD*
From a lecture presented at the 1996 Hawaii Medical Association Annual Meeting in Lihue, Kauai
Sports medicine is the care of medical and surgical needs ofathletes. Common sports injuries of the upper extremity includetraumatic and atraumatic dislocations and subluxations of theshoulder. Many traumatic dislocations in young athletic individualswill reoccur unless surgically corrected.
Rotator cuff problems commonly interfere with activities whichrequire overhead motion, Injuries of the acromioclavicular joint arebest categorized by their radiographic appearance.
Tennis elbow can usually be treated by a stepwise conservativeapproach. Skiers thumb is a sprain of the ulnar collateral ligamentof the first metacarpophalangeal joint. The Stener lesion should beruled out.
The ulnar nerve may be compressed in the palm of the hand incyclists. This usually responds to decreasing mileage and increasing padding of the hands. Oarsman’s wrist is a tenosynovitis of thewrist seen in paddlers.
Athletic, or sports injuries are primarily injuries of the musculosk
eletal system. These may be seen and treated either in the office of
the primary care physician, or of the specialist. Whether treating the
elite world class athlete or the weekend warrior, the following
principles of diagnosis and treatment generally apply. A thorough
history and physical examination will usually make precise diagno
sis of the injury possible. An anatomic approach follows.
Shoulder dislocations and subluxations in sports are quite com
mon and have affected the careers of many athletes. Two important
subgroups should be identified: 1) acute traumatic dislocations;
and, 2) atraumatic subluxations.
Traumatic Shoulder DislocationThe first group, acute traumatic shoulder dislocations, are ap
proximately 98% anterior in direction.’ There is usually a history of
injury with an abduction and external rotation force applied to the
shoulder. The physical examination of these patients should always
include evaluation of the neurovascular status of the limb. The
axillary nerve is the most common associated neurologic injury
*Department of Orthopaedic Surgeryand Sports MedicineStraub Clinic & Hospital888 S. King StreetHonolulu, Hawaii 96813
with acute traumatic shoulder dislocations. Evaluation of the axil
lary nerve should include testing of the autonomous sensory zone
located on the lateral deltoid. Numbness in this area will suggest
damage to the axillary nerve.2X-ray evaluation of the acutely dislocated shoulder should in
clude the “trauma series” ofx-rays. The trauma series includes a true
A.P. x-ray of the shoulder, an axillary or “West Point” view of the
shoulder, and a true lateral view in the scapular plane. This series
gives views of the shoulder at right angles to one another and, in
general, should be performed whenever evaluating acute traumatic
episodes of the glenohumeral joint.3Most shoulder dislocations are acutely reduced in the emergency
room and these patients are then followed as outpatients, often in the
primary care physician’s office. Outpatient follow up is extremely
important because acute anterior shoulder dislocations have a 94%
recurrence rate, if the patient is under 20 years of age. In patients
over 40 years of age, there is a lower recurrence rate,4 but a higher
instance of rotator cuff tears associated with the traumatic episodes.
The patient needs to be counseled regarding the likelihood of
recurrence. In the older patient, rotator cuff tear must be suspected
and ruled out by physical examination, or, if necessary, by further
diagnostic testing.5After an acute shoulder dislocation, it is common practice to treat
the initial injury with a sling or shoulder immobilizer, ice, and
analgesics as required. Gradual return to function occurs after
approximately three weeks. The length of the immobilization re
quired is controversial and probably does not influence the likeli
hood of reoccurrence.Recurrent shoulder dislocation is an indication for referral to the
orthopedic surgeon. Recurrent shoulder dislocations are a disabling
and disconcerting condition in the life of an athlete or active person.
They can be surgically repaired with a 96-97% success rate.67
Atraumatic Shoulder SubluxationA second subgroup of shoulder instabilities is the atraumatic
subluxation. These may be anterior, posterior, or inferior, and may
also be multidirectional. The typical patient in this subgroup,
however, presents to the office with a history of the shoulder
slipping in and out of joint without an initial traumatic episode
preceding it. Commonly, this is associated with chronic repetitive
stretching injuries, such as occur in baseball pitchers, tennis players,
and other overhead athletes. The patient often states that the shoul
der slips in and out ofjoint or feels “dead”, especially with a pitching
or throwing motion.8’9
HAWAII MEDICAL JOURNAL, VOL 56. NOVEMBER 1997
324

HAWAII EMERGENCY
— — — — —
•PHYSICIANS • ASSOCIATED
HawaiiEmergency Physicians Associated, Inc.
HEPAServing:
Established: 1971Castle Medical CenterWahiawa General HospitalHilo Medical CenterNorth Hawaii Community Hospital
HEPA Is a Participating Provider With:
HMSA - continuous since 1971KAISER - continuous since 1971
MedicareCHAMPUS
DHSFederal Employee Program (Blue Cross)
Kaiser of Southern CaliforniaMainland Blue Cross Plans (through HMSA)
Veteran’s AdministrationWorker’s Compensation
HMSA - 65C PlusStraubCare QuantumQueen’s Hawaii Care
Queen’s Preferred Plan (formerly PGMA)Aloha Care Quest
Kaiser QuestHMSA Quest
HMAAQueen’s HMSA Premier Health Plan
Physicians Health Hawaii Inc.University Health Alliance/HDS
Kapiolani Health HawaiiHawaii Laborers Health & Welfare Trust Fund
P.O. Box 1266 • KsUua, HI 96734 • 18081 261-3326 • Fax: 8081 262-0514

Figure 1.—To test for anterior shoulder instability, the patient’s arm is abducted andexternally rotated gently. The patient will display a look of apprehension as the shouldernears a position of dislocation.
On physical examination, there is a positive apprehension sign(Figure 1). The patient indicates apprehension when the arm isabducted and externally rotated. Pain is often reproduced with adislocation maneuver, and relieved by a reduction maneuver. Oneshould always check for generalized ligamentous laxity, includinga sulcus sign, hyperextension of the elbow joint, or the ability totouch the thumb to the wrist. In some athletes, the shoulder slips inand out ofjoint because the ligaments are so lax that they just do nothold the joints in place.
Radiographic evaluation, once again, should consist of the “traumaseries.” A pneumonic. “AMBRI,” outlines the treatment of atraumaticsubluxations. If the initiating event is Atraumatic, and especially ifthe direction of instability is Multidirectional; if the condition isBilateral, then the treatment is Rehabilitation with dynamic stabilization of the shoulder in physical therapy. An Inferior capsular shiftmay be necessary if surgery is performed.3
Rotator Cuff InjuriesThe next group of shoulder injuries which we will discuss in
cludes acute and chronic injuries to the rotator cuff. This broad areaincludes acute strains or tears of the rotator cuff, and chronicrepetitive attrition of the rotator cuff associated with impingement.The rotator cuff is composed of the tendons of the supraspinatus,infraspinatus, subscapularis, and teres minor. These tendons coalesce at their insertion on the greater tuberosity of the humerus.During abduction of the shoulder, the supraspinatus is exposed tofriction against the undersurface of the acromion. Sudden pain, orchronic pain with throwing, paddling, tennis serve, bench press, orother shoulder activity, may indicate a strain or tear of the rotatorcuff. The diagnosis of this disorder continues with the physicalexamination. There is often a painful arc of motion between 70degrees of abduction and 120 degrees of abduction. There may bea positive impingement sign. The impingement sign is elicited byhaving the patient abduct his shoulder 90 degrees, while the examiner gently internally rotates the arm. In the presence of a rotator cufftear or other rotator cuff injury, this usually will reproduce painwhich the patient can pin point at the top of the shoulder, or rotator
cuff region. There is often weakness or pain with abduction of theshoulder or with forward flexion against resistance. In an acuterotator cuff tear, there is often a positive “drop arm test”. In this test,the physician elevates the patient’s arm passively. If he then beginsto remove his support from the patient’s arm, the patient reports thesensation that his arm will “drop”.’°3
Plain film x-rays, the trauma series, are again indicated in mostcases. The treatment for acute shoulder strains is rest, ice, analgesics
as needed and gradual return to function as pain subsides. In the faceof an acute full thickness rotator cuff tear, surgical repair is indicatedin most young athletic individuals. Conservative management ofthe full thickness rotator cuff tear might be considered in debilitated,elderly, or otherwise low activity patients, or if the patient is a poorsurgical candidate.
Rotator cuff problems do not always present with an acute injuryas those described above. There is often a history of chronic painwith certain activities, such as throwing, swimming, weight lifting,etc. The physical examination should include evaluation of strengthand range of motion of the shoulder, with testing for an impingement sign and instability. If the pain or weakness is severe, anarthrograrn or MRI might be considered to rule out rotator cuff tear.If the pain is milder, or if a rotator cuff tear is not suspected,nonsteroidal anti-inflammatory drugs and a shoulder rehabilitationprogram to emphasize internal and external rotation strengtheningshould be performed. If no relief is obtained, a subacromial cortisone injection should be considered. Obviously, rest from aggravating activities or modification of the activity itself, should be addressed. If the pain cannot be resolved with conservative management, arthroscopic examination is considered. In most cases, withchronic impingement, six months of conservative management andmodification of activities will precede consideration of arthroscopicevaluation, unless suspicion of a torn rotator cuff or damage to othersignificant shoulder structures is strongly suspected. The arthroscopehas proven extremely valuable in evaluation of the shoulder and intreatment of certain rotator cuff lesions. Diagnostically, thearthroscope can be used to evaluate the rotator cuff and confirm orexclude the presence of partial or full thickness rotator cuff tears.
Figure 2.—Tennis elbow pain may be relieved by a tennis elbow splint or Nirschl bandplaced snugly about the forearm.
HAWAII MEDICALJOURNAL VOL 56. NOVEMBER 1997
326

The condition of the biceps tendon and other potentially involvedstructures can be evaluated. Furthermore, the arthroscope can beused in conjunction with specialized instruments to decompress theundersurface of the acromion where bony structures may be impinging on the rotatorcuff.11’12Arthroscopically assisted rotator cuffrepair methods are available.
Acromioclavicular Joint SeparationAcromioclavicularjoint separation, also known as shoulder sepa
ration, commonly occurs as a result of athletic injury. The athletemay present with pain and swelling at the end of the collar bone.These injuries often occur with a direct force to the point of theshoulder, such as a tackle or fall resulting in a direct impact betweenthe shoulder and the ground. This force is directed from the point ofthe shoulder to the AC joint, causing the ligaments to tear in avariable pattern with the end of the clavicle popping out of place.These injuries are graded from 1-VI, depending upon their severity.5For the most part, the grading of these injuries is based on theirradiographic appearance. The type I AC joint separation is a mildsprain of the joint. It is treated with a sling and rest for one to twoweeks or until the tenderness resolves. The type II AC jointseparation is a slight elevation of the clavicle seen on x-ray. Theseare commonly treated with a sling and rest for three to six weeks,followed by progressive strengthening. Often the athlete will needto wait eight to twelve weeks for return to contact sports.’° The typeIII shoulder separation represents a more significant injury. In typeIII separation, the distal clavicle is elevated completely above thesuperior border of the acromion. The type IV AC joint separationpresents with the end of the clavicle impaled through the trapezius.the type V shoulder separation is one in which a severe dislocationof the joint leaves the end of the clavicle elevated, almost to the baseof the neck, and the type VI AC joint separation is an inferiordislocation of the distal end of the clavicle to a subcoracoid position.In general, the type I and II AC joint separations are always treatedconservatively with a sling and rest for a few weeks, depending onthe severity of the injury, followed by progressive strengthening andgradual return to sports. The treatment of the grade IV through VIinjuries is always surgical, for these represent severe disruption ofthe normal anatomy. The treatment of the grade III separation issomewhat controversial, although more physicians are leaningtowards the conservative management of these injuries. This, however, should be individualized, depending upon the specific characteristics of the injury and the demands or requirements of the patient.The above described evaluation of the AC joint is very dependentupon obtaining high quality x-rays. X-ray evaluation of the ACjointrequires less x-ray penetration than x-ray evaluation of the shoulderjoint itself. Specific radiographic evaluation of the acromioclavicular joint is required.3’5
Tennis ElbowTennis elbow is a term that is usually synonymous with lateral
epicondylitis. Occasionally, the term tennis elbow may be used todescribe pain of the medial epicondyle of the humerus. This lattercondition is also known as golfer’s elbow. The patient with tenniselbow usually complains of pain at the lateral epicondyle of thehumerus which may radiate proximally or distally. In tennis, thepain is often associated with the backhand stroke. l3,l4
Physical examinationThe athlete will complain of pain with resisted extension of the
wrist. The pain should localize to the epicondyle region, and shouldreproduce the patient’s symptoms.
TreatmentThe initial treatment of tennis elbow should include stopping or
modifying the offending activity. Abstaining from, or at leastreducing the amount of tennis may be helpful. In milder cases,simply adjusting the tennis stroke and correcting training errors maybe helpful. In tennis this is especially important in the backhandstroke. The player should be instructed in using less wrist extensionin his stroke, or switching to a racquet that is not as stiff. Nonsteroidal anti-inflammatory drugs are often utilized initially. Counterforcebracing, utilizing a tennis elbow splint or “Nirschl” band (Figure 2),is inexpensive and protects the origin of the extensor tendons at thelateral epicondyle during healing.
If the above measures do not result in improvement, one mightconsider a cortisone injection, further rest from the offendingactivities, or possibly a course of formal physical therapy. Eighty toninety percent of appropriately treated tennis elbow cases shouldresolve within six months with conservative measures alone.
Surgical treatment is indicated in those cases of tennis elbowwhich do not respond to six months of appropriate conservativemanagement.
Skier’s Thumb“Skier’s thumb,” or “gamekeeper’s thumb,” is a sprain of the
ulnar collateral ligament at the base of the thumb metacarpophalangeal joint. This is considered to be the most common skiinginjury, and may occur with forced abduction of the thumb associatedwith a fall while holding the ski pole. Milder sprains are usuallytreated with splinting or protective taping. It is important to distinguish between a partial and a complete rupture of the medialcollateral ligament. In certain more severe sprains, the tendon maybecome interposed between the proximal and distal ends of the tornmedial collateral ligament. This is the so-called “Stener lesion.” Inthese cases, surgical repair is often needed to restore pinch strengthand prevent chronic instability and pain of the joint.10”6
Ulnar Nerve Compression In CyclistsCyclists may develop numbness in the ulnar nerve innervated
digits from chronic compression of their ulnar nerve in the palm ofthe hand which occurs while riding. In addition to numbness,intrinsic muscle weakness of the hand may also occur. Treatmentshould include thickly padded handlebar cushions or tape, paddedcycling gloves, and restricting mileage.
Oarsman’s WristOarsman’s wrist is an extensor tenosynovitis of the radial wrist
extensors seen primarily in rowers and paddlers, and sometimes inracquet sports. Pain, tenderness, and swelling may be present at thedorsal wrist, the treatment is rest, splinting, and nonsteroidal anti-inflammatory drugs. Occasionally a steroid injection might beconsidered. Correction of training errors, with adequate rest periodsand more gradual building of strength and endurance are helpful inprevention.’0
HAWAII MEDICAL JOURNAL, VOL 56. NOVEMBER 1997327

This series on common sports injuries for theprimary care physician will be continued withpart II, Lower Extremity, in a subsequentissue.
References1. Rowe, C. Prognosis in Dislocations of the Shoulder. J. Bone Joint
Surg. 1956, 38-A: 957-977.2. Hoppenteld, S. Orthopaedic Neurology. Philadelphia: J.B. Lippincott
Co; 1977: 7-42.3. Rockwood, C. The Shoulder, Philadelphia: W.B. Saunders Co., 1990.4. Rowe, C. Acute and Recurrent Anterior Dislocations of the Shoulder.
Orthop Clin of North Amer. 1980, 11(2): 253-270.5. Rockwood, C. Fractures in Adults, Vol 1. Philadelphia: J.B. Lippincott
Co; 1991: 1021-1179.6. Rowe, C. The Bankart Procedure. J. Bone Joint Surg. 1978,60-A: 1-
16.7. Caspad, R. Arthroscopic Reconstwction for Anterior Shoulder Insta
bility. Techniques Orthop., 1988,3:59-66.8. Jobe, F. Shoulder Pain in the Overhand or Throwing Athlete. Orthop
Review. 1989, 18(9): 963-975.9. Rowe, C. Recurrent Transient Subluxation of the Shoulder, J. Bone
Joint Surg. 1981, 63-A: 863-871.10. Kulund, D. The Injured Athlete. Philadelphia, J.B. Lippincott Co.,
1988.11. Beach, W. Arthroscopic Management of Rotator Cuft Disease. Ortho
pedics. 1993, 16(9): 1007-1015.12. Gartsman, G. Arthroscopic Acromioplasty for Lesions of the Rotator
Cuff. J. Bone Joint Surg. 1990,72-A: 169-1 80.13. Nirschl, R. Tennis Elbow, Orthop. Clin. North Am. 1973,4(3): 787-
800.14. Coonrad, R. Tennis Elbow: Ifs Courses, Natural History, Conserva
tive and Surgical Management J. Bone Joint Surg. 1973,53-A: 1177-1182.
15. Froimson, A. Tenosynovitis andTennis Elbow, in Green, D: OperativeHand Surgery, New York: Churchill Livingstone, lnt., 1988, 2117-2134.
16. Green, D. Fractures and Dislocations in the Hand, in Rockwood, C:Fractures in Adults, Vol 1. Philadelphia: J.B. Lippincott Co., 1991,441-561.
Kahu Malama Nurses, Inc.cures atlEyour staffing ills!1k
REGISTEREDNURSES
LICENSEDPRACTICAL
NURSES
CERTIFIEDNURSE AIDES
MEDICALASSISTANTS
NURSE AIDES
SPECIALTYMEDICAL
PERSONNEL
Serving all islands 24 hours every day since 1982
Temporary staffing:to support and/or supplement your workforce
Long-term staffing:to assist on an on-going basis (contract)
Employee leasing:to provide you with needed employees for part or allofyour workforce
Permanent placement:To allow you to consider afulltime employment relationship
Private Duty:for individuals in need of one-on-one assistance
Special needs:such as immunizations, drug screening, patient transport,case review and utilization review
c:se Fore
r%41TaJania
Kahu Malama Nurses, Inc.1357 Kapiolani Blvd., Suite 850
Honolulu, HI 96814
(808) 951-0111 • Fax (808) 949-3834
Toll-Free Inter-island 1-800-773-9021
Email: [email protected]
SHOW YOURMOTHER YOU
LOVE HER.Make sure she gets her mammogram.
It can spot trouble years before she can.For free information about a quality
mammogram that’s safe and reliable,call 1 -800-ACS-2345.
THERE’S NOTHINGMIGHTIER THAN THE SWORD
AMERICAN9CANCERf SOCIETY®
WANTED32 Athletes in peak condition to win the America’s Cup.
Requirements:• Extraodinaiy cardiovascular capacity & warp-speed reflexes• Able to climb 100-foot mast suspended fiom metal wire• Musthoist 150 lbs. of sail l00ftJnunder8sec.• Able to spin loaded winches at 120 rpm for up to two hours• Able to withstand extremely coId/et conditions• Must work 14-hour days, 7 days,ik.• Three year mm. committment req.
What does it take to bring the America’s Cup to Hawaii? Join the Aloha Racing teamand find out. Aloha Racing corporate sponsor HEALTHSOUTH Corp., the nationslargest rehabilitation provider and undisputed leader in sports medicine, has joinedour Hawaii America’s Cup Team. As members of the Hawaii healthcare industry youtoo can benefit during the next three years from an association with one of the mostexciting and physically demanding sports in the world ... the America’s Cup.
If you’d like to find out how you can race with the team aboard the Aloha Racingyacht during the next America’s Cup in Ankland, New Zealand; how your healthcarebusiness can capitalize on the international marketing opportunities of this ‘healthychallenge’ or how you can personally support the effort to bring the America’s Cup toHawaii, contact D. J. Cathcart with Aloha Racing at (808) 3664259.
AAWAIKIKI YACHT CLUB
AMERICA’s CuP CHALLENGE

If a physician you care about is at risk...If you need someone to turn to...
COMMITTEE ON PHYSICIANS’ HEALTHA Confidential Program of the HMA
For physicians and theirfamilies
Members of the HMA Committee on Physicians’ Health are available by phone to colleagues and theirfamily members who feel they need help with their situation. We assist physicians who become unableto practice medicine with reasonable skill and ignore the safety of their patients. Chemical, mental,emotional and physical impairment are considered by the Committee. The Committee will assist withina confidential system to restore the physician to a state where he or she will be able to practice medicine.
YOU ARE WELCOME TO CALL ANY OF THE FOLLOWING:
Gabrielle Bemis Batzer, M.D.Ed Gramlich, M.D.William Haning, M.D.Leonard S. Jacobs, M.D.Virgil Jobe, M.D.Roger Kimura, M.D.Gerald McKenna, M.D.Ronald Peroff M.D.S. Larry Schlesinger, M.D.Stephen Wallach, M.D.
or call or write to:Hawaii Medical Association
1360 South Beretania Street, Second FloorHonolulu, HI 96814
(808) 536-7702, ext 2234 or ext 2230fax (808) 528-2376
Contact Island
OahuOahuOahuOahuOahuOahuKauaiOahuMauiOahu
Phone #
(808) 566-1403(808) 956-7457(808) 236-8497(808) 254-5385(808) 522-3220(808) 523-6966(808) 246-0663(808) 231-1333(808) 871.7502(808) 521-3851

regret to say we don’t offer message in a bottle. But we do offer plenty of other ways to communicate, like fax
ing, caller l.D., paging, voice messaging, Internet service, the list goes on and on. And they’re all from one company.
GTE Hawaiian Tel. We’ve been helping businesses communicate for over a century. To improve your own communication
skills, stop by any GTE Phone Mart, visit our web site at www.gte.com, or call 643-4411. ici I i Hawaiian TelBeyond the call
Products and services available in most areas.

News and Notes Henry N. Yokoyama MD
Life in These Parts
A Prayer for Tom FrissellGod of all mankind, Creator of the UniverseWe thank you for this day in Hawaii-nei.We thank you for this occasion: a celebrationOf Tom’s life, for having known Tom as a friend.A cantanicerous friend, a kind and generous friend.
This was the noblest fisherman of them allThis was a giant of a manThis was an Ahi among Menpachi
Tom is now for the ages. No one quite like himWill walk the face of the earth or sail theSeven seas, FOREVER MORE.Best his memory will linger with us
With a smile on our lipsWith a twinkle in our eyesWith a twinge in our hearts.
We rejoice that he is in the company of Capt. Bill,Pres, Mr Mahi, Mr Ahi, Mr Uhu, Mr Paka
May the wine there be vintage and everfiowingMay the sashimi be fresh and plentifulMay the chops be thick and tasty.
Help us remember that he was your gift to us.Help us keep his memory precious as we returnHis ashes to you, remembering that we,In the not too distant future,Will be joining Tom in your Happy Fishing
Grounds.This we pray.
The Duchess
Theodore K.L Tseu MD(Tom’s fishing buddy)Aboard the Kuu Huapalaoff Kalaupapa, MolokaiJuly 8, 1997
(Condensed version from Stitches July-August1997)
The subject of the day was “Limericks” at anursing home activities session. A very quietwithdrawn lady resident who rarely spoke a word,put up her hand and began to recite:
“I sat with the duchess at tea;She was gracious as gracious could be,But her rumblings abdominalWere something phenomenal,And everyone thought it was me!”
The Nervous Mountie(A very condensed version ofa Stitches story byRobbie Newton Druinmond MD)
Daniel Dumas was the true general surgeonwho could and did everything. He knew gynecology and urology and plastics. He could drill burrholes and anastamose the ends of resected bowels. Daniel had been in every major conflict inWWII. He’d trained in France, and alas althoughhis grammar was unimpeachable, his accent wasan atrocious blend of Hercule Poirot and Inspector Clouseau.
A frightened, burly 6 ft. 3 Royal CanadianMountie needed a vasectomy. The procedurewent smoothly and painlessly and Daniel usedLgto close the final layer. In a benighted effort to
placate the patient, he leaned over the drape withhis masked face and said matter of factly, “Zee
fall off in ten days.”The patient bolted upright, the whites of his
horrified eyes filled my field of vision. I grabbedhis shoulders, locked my gaze with his and translated: “The knots, the knots will fall off in tendays.”
AnecdotesA young man from the outback decides to get
some learning in Sydney. He meets a hooker in abar and they go up to a hotel room. He starts to runaround in the room. First he grabs the dresser andthrows it out the window. A few minutes later, hepicks up the bed and throws it out the balcony.The hooker asks in astonishment: “What’s happening?” The young man replies, “Never beenwith a woman before. If it’s anything like beingwith a kangaroo, we need lots of room.”(As told by Jon Isenberg, Professor ofMedicine,UC San Diego lecturing at the 7th Annual Hawaii Gastroenterology Symposium at KahalaMandarin on Sat. Aug. 23. Jon explained that heneeds “lots of room” to discuss NSAIDS andHelicobacter Ulcers)
Uncle Dick noticed that everytime he ate chitlins, his favorite food, his foot would pain himthat evening. The family doctor confirmed hissuspicion that it was pork-induced gout. When hereturned from the doctor’s, my aunt asked himhow the appointment had gone. Uncle Dickplopped down on the sofa, kicked off his shoesand replied, “the doctor said I’m going to havegout about three times a week.” (Reader’s DigestSeptember 1997)
The Latest News on Gerd(Keith Tolman MD; Chiefof Endoscopy at University of Utah; Dinner lecture at Pacific CafeOahu, August 7)
Rules in Medicine1. Above all, do no harm2. Cover your ass
Re Behavioral Modification“The only reason I would take up jogging
again; so that I can hear heavy breathing again.”Erma Bombeck
Re SucralfateTwo questions you never ask at a meeting
1. How does sucralfate work?2. What are the ingredients in German sausage?
Esophagitis Therapy“Step up approach is a product of marketing.
It’s biologic nonsense. The proton pump inhibitors are better for all grades of esophagitis. Wecan heal esophagitis, but the relapse rate is 70%.Reflux is a chronic disease. Continuous treatmentis necessary.
Zsa Zsa’s 6th husband:“I know what to do, but I don’t know how to
make it exciting.”
Re Proton Pump InhibitorGive it in the morning 1/2hr before breakfast.
GERDIt is a lifetime disease requiring lifetime medi
cation. 79% of patients improve on therapy.Surgery is not curative. We need to reevaluate therole of surgery in GERD: viz Laproscopicfundoplication vs proton pump inhibitor.
The Last Rule of Medicine“Never ask a surgeon if you need an operation.”Likewise: “Never ask a gastroenterologist if
you need endoscopy.”Step-down therapy is also a marketing strat
egy. Maintenance therapy for GERD is full dosedaily therapy.
Goals of Maintenance Therapy for GERD• Improve quality of life• Prevent complications• Safety• Cost effectiveness
“The best therapy is the therapy that works.”“The most expensive therapy is therapy thatdoesn’t work.”Yogi Berra said, “Predictions are always dangerous, especially about the future.”
MiscellanyPaddy had just arrived in New York from
Ireland and was invited by one of his Americancousins to go to his first baseball game. Seated inthe Yankee Stadium bleachers, he watched as aman swung a stick, hit a ball and started toward awhite bag. Everyone stood up and yelled, “Run,run!”
Then a second guy came up to the plate, whackedthe ball and started down toward the white bag.Everyone stood again and yelled, “Run, run!”
A third batter came up, but this one didn’t hit theball. He didn’t even swing. Four times the pitcherpitched, four times the catcher caught. Paddy wascompletely confused when the batter dropped thestick and started strolling toward the white bag.“Run, run!” Paddy shouted.
“No, he doesn’t have to run,” his cousin informed him. “He’s got four balls.” Paddy’s eyeswidened as he stood. “Walk with pride, man!” heshouted. “Walk with pride!”
(Fro,n Playboy April 1997)
Chemists synthesize marvelous chemicals thesedays. There is the story that one synthesized anaphrodisiac for men that is so powerful that it hadto be swallowed very quickly to avoid a stiffneck.
Continued on Next Page
HAWAII MEDICAL JOURNAL. VOL 56, NOVEMBER 1997331

Joe Camel Sent PackingThe AMA was pleased that RJ Reynolds is
dropping the cartoon character, but it maintains,“It gives us no reason to believe that his creatorshave quit. Let’s hope this is a step in the rightdirection rather than the beginning of a new andequally sinister campaign to addict our youngpeople to deadly tobacco.”
The French ParadoxGenial nephrologist Eugene Wong who was
honorary chairman (for the 4th time) of the 8thAnnual Honolulu Wine Festival (A benefit of theHawaii Lupus Foundation) says: “The only paradox between wine and health is the “FrenchParadox.” Despite their rich, high fat diet, theFrench have a low rate of heart disease. Theydrink a lot of red wine which is rich in flavanoidsand falvanoids are antioxidants preventing LDLfrom exercising its bad effects. The flavanoidsare primarily found in the skin of grapes and redgrapes have more than white grapes.”
“One of my philosophies is to experience themost out of my life. And there is always something new to learn about food and wine. Anyonewho thinks he is an expert in food and wine is a
jdc. There is so much to learn, and that’s whatmakes it great.”
“The best thing about wine is that it’s an areawhere you can share with other people. I’m apeople person and sharing my knowledge aboutfood and win through combined fellowship is
Office Space
Liliha Medical Bldg.—Share a 1,397 sq. ft. medicaloffice with free visitor parking. Call Chaney, Brooks &Company. 544-9557.Surgeon looking to share an office.—in the Queen’sPOB I or II. Fax information to 951-5538.
Locum Tenens
Locum Tenens available—Board-certified familypractice, 14 yrs clinical experience in Hawaii. Officecoverage, Deborah C. Love MD; home Oahu: (808)637-8611; cell ph: (808) 295-2770.Take an Afternoon Off.—While your office staysopen. Part-time primary care office coverage on aregular or occasional basis by longtime Honolulu physician. Contact John Wichmann-Walczak MD at 739-9483 or 524-2575.Wanted: Locum Tenens position.—Board-certifiedfamily practitioner with considerable experience inlocum tenens work. Desires position for 1, 2 or manyweeks. Call Kit Glover 668-7337 or the Phy Ex 524-2575.
Business Opportunity
Veteran Certified Petroleum Geologist.—Wishes toteam up with oil and gas investment capital finder.Excellent remuneration. (614) 453-9231 or fax (614)450-7507.
what it’s all about.”In 1994, Eugene was named “Mr Gourmet of
the Year” by the Society of Bacchus America, anelite New Orleans wine and food club.
Health Briefs(Pacific Business News, Oct. 6, 1997)
The Physician Compensation and ProductionSurvey 1997 Report by Medical Group Management Association summarizes the incomes of30,000 physicians as follows:
During the period 1992 to 1996: Primary physicians’ income rose 17%, Specialists’ incomerose 5.5%.
Four specialities, ophthalmology, neurology,anesthesiology and pulmonary medicine reporteda 2% income loss and work increase of 18%.
Appointed, Elected & HonoredThe 1997 United Chinese Society electedDavid
Lee Pang, 86, Father of the Year.Osamu Fukuyama, cardiologist and Associ
ated Clinical professor of Medicine at the UHSchool of Medicine was elected KMC’s 1997Physician of the Year.
Announcement
General Practice OpenecL—ln Kapahulu area by 20-year veteran of St. Francis ER. New patients welcomed; free parking; convenient hours; house calls(downtown Honolulu-Ama Haian). John WichmannWalczak MD at 750 Palani Avenue, Honolulu 96816.739-9483.Relocation.—for Jennifer Frank MD, Family Practiceand Tyronne Dang MD, Internal Medicine. EffectiveOct. 13, 1997. Their new office is Artesian Plaza, 1907S. Beretania SI, 5th fIr, Honolulu, HI 96826.
Misc.
Latex Glove Relief.—Latex glove sensitivity protectantspray, immediate reduction of Type I irritation fromlatex gloves, duration 100+ hand washes/4/8/16 hrs.Free evaluation sample to USNAPO address physicians. Limited time, 1 sample per office. Otherproducts: Scalp Itch Reducer gel and Skin Itch Reducer gel, soothing relief, duration varies from 8-48hrs, results vary per individual, Sahara Cosmetics,(808) 735-8081, P0 Box 10869, Honolulu, Hawaii96816-0869, USA, leave name on answering machineor send letterhead or business card to above address.Opoid Analgesics—Appropriate use vs Abuseseminar coming to Maui Waikapu Country Club onTuesday, Nov.18 at 5pm and to Kauai Marriott on Nov.20 also starting at 5pm. This outstanding seminar, with3 speakers from the mainland, was a big hit on Oahuand the Big Island. Watch for special mailing. Markyour calendar now. This seminar will be made possibleby an educational grant from Knoll Pharmaceutical Co.Invited to attend are physicians, nurses, pharmacistsand dentists.
For Sale
Wanted
HMA employees.—Looking for a good physician’s-type scale for monitoring our weight. If you have oneyou’d like to donate, please call or bimg to HMA office.Mahalo!Two professionals seeking—3/4 bedroom, 2 bathhouse to rent. Prefer peaceful setting. Dependable, nopets, no children. Call 737-4217 (bus ph).
Classified NoticesTo place a classified notice:
HMA members —Please send a signed and typewritten ad to the HMA office. As a benefit of membership,HMA members may place a complimentary one-time classified ad in HMJ as space is available.
Nonmembers —Please call 536-7702 for a nonmember form. Rates are $1.50 a word with a minimum of 20words or $30. Not commissionable. Payment must accompany written order.
HAwAIIPATHOLOGISTS’LABORATORY
The Full Service Lab
Offering ComprehensiveServices in. -
• Clinical Pathology• Surgical Pathology• Frozen Section Diagnosis• Pap Smears• Special Cytology• Flow Cytometry• Fine Needle Aspiration• Bone Marrow Interpretation• Specimen Photography• Image Analysis
1301 Punchbowl StreetHonolulu, Hawaii 96813547-4271 Fax 547-4045
Misc for Sale.—Desk 60 x 30 $50.; Credenza 71 x18’ $100, Xerox Model 5309, 1 yr old , $525. Ask forNelson 536-7702.Give-A-Way.—Burroughs Pegboard accounting system. Call Jean Frissell 536-0779.
HAWAII MEDICAL JOURNAL, VOL 56, NOVEMBER 1997
332

Your Success is Our GoalAmerican Medical AssociationOrganized Medical Staff Section(AMAOMSS)*Assembly Meeting
December 4-8, 1997Wyndham Anatole HotelDallas, Texas
• Joint Commission’s ORYX initiative• CPT coding changes and self audits• Measuring and managing outcomes• Group dynamics and team building• Fraud and abuse compliance
• Advocating your issues at home• New legislation and AMA action• Medical staff reengineering and bylaws• Forming a physician organization• Patient involvement in medical decision-making
In addition to these educational offerings, as an AMA-OMSS representative of your medical staff,you can participate in advocacy, policy-making and networking activities. Our goal is to work with youto identity and address medicine’s most pressing issues. We also want to help you increaseyour knowledge and skill so that together we can best serve the needs of patients, physicians,and the profession.
To achieve this goal you can:
‘ Submit resolutions and participate in mode-of-practice and general interestforums to bring your concerns to the forefront.
V Testify at reference committee hearings and vote on actions in a democraticassembly to further AMA’s advocacy agenda.
V Attend practical education programs to improve your medical practice,earn 10.5 hours of CME credit** and pay no fee to register!
Your success depends on your involvement! Plan today to attend the 1997 Interim AMAOMSS Assembly Meeting on December 4-8, 1997, at the Wyndham Anatole Hotel in Dallas, Texas.To receive more information and registration materials, please call 800 621-8335 and ask for theDepartment of Organized Medical Staff Services.
The American Medical Association Organized Medical Staff Section (AMA-OMSS) leads and assists grassroots physicians, individually and in groups,to organize and reclaim their role as medical leaders and advocates for excellence in patient care, professionalism, and the integrity of the patient-physicianrelationship, We proside practical educational forums, focused policy development, and grassroots support through the Federation.
The AMA designates this education activity for a maximum of 10.5 hours in category 1 credit towards the AMA Physician’s Recognition Award.Each physician should claim Only those hours of credit that he/she actually spent in the educational activity.
American Medical Association FEoIPhysicians dedicated to the health of America
VVVVV
To succeed in today’s health care environment, your medical staff needs the latest information andappropriate skills for meeting the day-to-day challenges of medical practice. By attending this meeting,you can learn about:

The Weathervane Russell F Stodd MD
No matter how cynical you get, it is impossible to keepup.
The Optima Health Plan, an HMO in Virginia with 242,000 members, has
begun fining capitated doctors $100/day when the doctor keeps the patient in the
hospital too long. Nurses from the HMO visit the hospitals and determine for the
plan what is the appropriate length of stay. If the nurse also decides the hospital
was in some way responsible for the overstay, the carrier will refuse to pay the
hospital. Not surprisingly, many of the 13,000 physicians are angry, because they
believe they are providing appropriate hospitalization. However, physicians must
recognize the doctor’s vulnerability when he sells his volition to the corporation.
The unspoken managed care motto is “profits, not patients.”
Progress is an illusion.In today’s high tech tools of computerized imaging, the barrage of lab studies
and the laptop, the practice of laying on the hands (and the other senses), is
disappearing. In a recent report in JAMA, both students and residents failed to
recognize and understand heart sounds of valve disease. 453 physicians in training
and 88 medical students were in the study. ffi evaluating 12 detectable important
abnormal heart sounds, the average grade was 20%. As the professor at Allegheny
University of Health Sciences in Philadelphia noted, “The stethoscope is an
accurate, sensitive and specific way of malcing a bedside diagnosis, but that skill
is fading in our times of high technology.” The critical point is that the increasing
use of primary care physicians as “gatekeepers” (I hate that word), shifts more
responsibility for diagnostic acumen to the general physician or internist. One
more caveat to consider in shopping for medical plan.
It is the ability to deceive oneself that one shows thegreatest talent.
A woman underwent a breast implant procedure. Subsequently, she sought to
bring a malpractice complaint against the surgeon. Her attorney obtained a
physician expert to provide testimony on her behalf. The “expert” submitted an
affidavit of credentials, but the court determined that the physician had not been
in active practice for ten years. Moreover, it was found that his recent professional
activity consisted solely of providing testimony in cases such as this one. The
affidavit was struck, and the expert not accepted by the court. Since the statute of
limitations had run out, the malpractice action was dismissed. We really do have
whores in our midst, and it is so refreshing when the court applies the label.
Our ability to delude ourselves is an important survival toolMedical records and peer review actions are not discoverable, that is, they are
confidential, right? Well, yes, or are they? A patient had a craniotomy and
developed an infection three weeks after the procedure. The patient and his wife
learned that there might have been a break in sterile technique during the
operation, and that there had been four other similar cases, resulting in both
hospital and state investigations. The patient got a copy of the government agency
report and used some of that information in his complaint. The hospital objected,
stating the report was privileged as part of the peer review mechanism. The court
disagreed and stated that the government investigation could have come from
other sources and it was up to the hospital to prove that the information came from
the peer review process.
The simpler it looks, the more problems it hides.In response to ballot initiatives in California and Arizona, the National
institutes of Health (NIH) empaneled 9 experts for 2-day session to evaluate
various hypotheses concerning the potential use of marijuana in therapeutic
settings. Five areas were defined; appetite stimulation, nausea and vomiting of
anticancer therapy, analgesia, neurologic disorders and glaucoma. After 2 days,
the panel came up with no recommendations and the chairman stated, “We need
to get some decent research done and get closure on this.” The major problem for
research scientists relates to obtaining a drug supply. Even if one is granted state
funding for a scientific study, then goes through the vexation of a schedule 1 Drug
Enforcement Agency (DEA) clearance, and then writes a protocol approved by
the Food and Drug Administration (FDA), there still remains the difficulty of
obtaining legal, certified grade marijuana to do the study. Over and above a drug
supply, research based upon an inhaled smoke delivery mechanism does not make
sense when we are in the midst of a massive anti-tobacco campaign.
If you think you did something wrong, you’re right.An Additional embarrassment for the elected hierarchy of our American
Medical Association in relation to the proposed endorsement of Sunbeam
products, is that the arrangement was not managed and not even known by the
officers nor the trustees. It would have been unexplainable for the officers to enter
into any such a cozy deal, but even more shocking is to learn that they did not even
know about it. Kirk Johnson, AMA general counsel, is heading an internal inquiry
into how the agreement was forged. Obviously, management must be tightened
up and functionaries apprised of the limitations in their work areas.
Without a government the nation would instantly collapse.With too much government it takes a little longer.
While Congress dithers and tinkers with the Social Security System by raising
taxes and cutting benefits, hardly a baby boomer or a generation X-er has any faith
that Social Security will be there for them. To seriously approach the problem, our
elected officials should look south. Mexico is solving it by going private.
Mexicans are now allowed to pullout of thepublic system and put aportion of their
income (with matching employer contribution) into private accounts. To no one’s
surprise they are jumping at the chance with $400 million deposited when the
accounts were opened, and the government anticipates another $4.7 billion by
January. Along with Mexico and Great Britain, 7 Latin American countries have
privatized their retirement programs.
Truth is the most valuable thing we have. Let us economize it.
Patients who enroll with Kaiser Foundation Health Plan must agree to accept
the HMO’s arbitration agreement to resolve malpractice disputes. Each side
selects its own arbitrator and works with the other to decide on a third panel
member. Kaiser’s own patient protocol promises to appoint a neutral arbitrator
within 60 days. In California, the Supreme Court found that Kaiser may have
engaged in fraudulent conduct. Kaiser knowingly permitted widespread delays in
the arbitration process, and the Court found that the mediator was neutral in 1%
of the cases. The average claim takes 863 days (that’s almost 2-1/2 years) to reach
a hearing.
Nobody is interested in sweetness and light.To no one’s surprise, the abiding big winners in the photorefractive keratec
tomy excimer laser business are the lawyers. While surgeons struggle to provide
good patient care with predictable outcomes at a fair cost, anyone transgressing
Pillar Point Partners $250 charge for each laser use, is promptly sued. But now the
federal lawyers are on the scene. Investigators for the Federal Trade Commission
are prepared to recommend that the FTC file an antitrust complaint against PPP.
How robust our economy would be if we could but listen to Shakespeare.
Addenda—+ Abraham Lincoln suffered from intermittent double vision due to hypertropia.
When he told his wife Mary that he saw his mirror image with a “ghost” she
believed it was a sign that he would die in office.
+ Patients who make prolonged use of inhalers with high concentration of
glucocorticoids will increase the risk of ocular hypertension or open-angle
glaucoma.+ What distinguishes humans from lower animals is the desire to take drugs.
+ Football combines the two worst things in America - violence and committee
meetings.
Aloha and Keep the faith.—rts •
HAWAII MEDICAL JOURNAL, VOL 56, NOVEMBER 1997
334

PromisesPromises
Competitive Rates and Premium Credits
Specialized Claims Management
Policyholder Involvement
We haven’t raised rates in 12 years, and 1997 marks the ninthconsecutive year of premium credits.
Our claims staff works exclusively in medical malpractice, and weretain law firms who specialize in representing physicians. Wemaintain a claims office in Honolulu.
MIEC policyholders continue to own and govern MIEC through aBoard of Governors they elect. Our physicians participate in peerreview, claims analysis and settlement decisions. No claim issettled without the policyholder’s consent.
MIEC has provided advice and certainty of protection to Hawaiipolicyholders for more than 16 years. If you’re not already an MIECpolicyholder, we invite you to apply. Call us toll-free 800-227-4527,or contact Hawaii Medical Association, 808-536-7702. Informationalso is available on our web site: http://www.miec.com.
MIECMedical Insurance Exchange of California6250 Claremont Avenue, Oakland, California 94618Fax: 510-654-4634Telephone: 800-227-4527
Hawaii Claims Office1360 South Beretania, Suite 405, Honolulu, Hawaii 96814Telephone: 808-545- 7231
MIECc 5,000+ policyholders get more than just a promise todefend malpractice claims.

The Future Horizons 401(k), developed
by Pacific Century Trust (formerly
Hawaiian Trust), a unique retirement plan
specially designed to meet the needs of
Hawaii’s employers and employees:
• It’s a flexible, comprehensive nvestment
program, tailored to meet the needs of
individual Hawaii businesses
• Our Plan Specialists make sure your
employees understand the program,
which encourages high participation
• We take care of the details, so you can
take care of your company’s business
FREE! AWARD-WINNING ENROLLMENT VIDEO!
To get one, or to find out more about the
Future Horizons 40 1(k), call the Retirement
Experts at (808) 538-4400. Neighbor Islands
call toll-free 800-272-7262.
() PACIFIC CENTURYTRUST
A DIVISION OT BANK or HAVvAii
k)
Any investments in stocks and bonds are subject to risks that may result Th loss of principa and are not depositsor obligations ol or en( orsed or guaranteed by Bank of HawaII or Pacific Century Trust and are not insured by
the FDIC, the Federal ?eserve Board or any other government agency















![P053 Fonds René Bélanger · P053/001/002 Biographies et curriculum vitae (copie [après 1945]-1993) P053/001/003 Sacerdoce ([après 1925]-copie 1997) P053/001/004 Implications sociales](https://static.fdocuments.in/doc/165x107/5f91279f84f3ea1a400d5913/p053-fonds-ren-b-p053001002-biographies-et-curriculum-vitae-copie-aprs.jpg)