Novel Statistical Approach to Determine Inflammatory BowelPatients
11
ORIGINAL RESEARCH ARTICLE Novel Statistical Approach to Determine Inflammatory Bowel Disease: Patients’ Perspectives on Shared Decision Making Corey A. Siegel 1 • Jennifer H. Lofland 2 • Ahmad Naim 3 • Jan Gollins 4 • Danielle M. Walls 5 • Laura E. Rudder 6 • Chuck Reynolds 6 Ó Springer International Publishing Switzerland 2015 Abstract Background Limited information is available on patients’ perspectives of shared decision-making practices used in inflammatory bowel disease (IBD). Objective The aim of this study was to examine patient insights regarding shared decision making among patients with IBD using novel statistical technology to analyze qualitative data. Methods Two 10-patient focus groups (10 ulcerative colitis patients and 10 Crohn’s disease patients) were conducted in Chicago in January 2012 to explore patients’ experiences, concerns, and preferences related to shared decision making. Key audio excerpts of focus group in- sights were embedded within a 25-min online patient sur- vey and used for moment-to-moment affect trace analysis. Results A total of 355 IBD patients completed the survey (ulcerative colitis 51 %; Crohn’s disease 49 %; female 54 %; 18–50 years of age 50 %). The majority of patients (66 %) reported increased satisfaction when they par- ticipated in shared decision making. Three unique patient clusters were identified based on their involvement in shared decision making: satisfied, content, and dissatisfied. Satisfied patients (18 %) had a positive physician rela- tionship and a high level of trust with their physician. Content patients (48 %) had a moderate level of trust with their physician. Dissatisfied patients (34 %) had a life greatly affected by IBD, a low level of trust of their physician, a negative relationship with their physician, were skeptical of decisions, and did not rely on their physician for assistance. Conclusion This study provides valuable insights re- garding patients’ perceptions of the shared decision-mak- ing process in IBD treatment using a novel moment-to- moment hybrid technology approach. Patient perspectives in this study indicate an increased desire for shared deci- sion making in determining an optimal IBD treatment plan. This work has been presented in part at the American College of Gastroenterology Annual Meeting, Las Vegas, NV, USA, on 22 October 2012. Electronic supplementary material The online version of this article (doi:10.1007/s40271-015-0126-z) contains supplementary material, which is available to authorized users. & Jennifer H. Lofland jlofl[email protected] 1 Inflammatory Bowel Disease Center, Dartmouth–Hitchcock Medical Center, Lebanon, NH, USA 2 Health Economics and Outcomes Research, Janssen Scientific Affairs, LLC, 850 Ridgeview Drive, Horsham, PA 19044, USA 3 Incyte Corporation, Wilmington, DE, USA 4 Delta Modelling, Mt Prospect, IL, USA 5 BDJ Solutions, Melrose, MA, USA 6 The Benfield Group, St Louis, MO, USA Patient DOI 10.1007/s40271-015-0126-z
-
Upload
jangollins -
Category
Documents
-
view
77 -
download
1
Transcript of Novel Statistical Approach to Determine Inflammatory BowelPatients

ORIGINAL RESEARCH ARTICLE
Novel Statistical Approach to Determine Inflammatory BowelDisease: Patients’ Perspectives on Shared Decision Making
Corey A. Siegel1 • Jennifer H. Lofland2 • Ahmad Naim3• Jan Gollins4 •
Danielle M. Walls5 • Laura E. Rudder6 • Chuck Reynolds6
� Springer International Publishing Switzerland 2015
Abstract
Background Limited information is available on patients’
perspectives of shared decision-making practices used in
inflammatory bowel disease (IBD).
Objective The aim of this study was to examine patient
insights regarding shared decision making among patients
with IBD using novel statistical technology to analyze
qualitative data.
Methods Two 10-patient focus groups (10 ulcerative
colitis patients and 10 Crohn’s disease patients) were
conducted in Chicago in January 2012 to explore patients’
experiences, concerns, and preferences related to shared
decision making. Key audio excerpts of focus group in-
sights were embedded within a 25-min online patient sur-
vey and used for moment-to-moment affect trace analysis.
Results A total of 355 IBD patients completed the survey
(ulcerative colitis 51 %; Crohn’s disease 49 %; female
54 %; 18–50 years of age 50 %). The majority of patients
(66 %) reported increased satisfaction when they par-
ticipated in shared decision making. Three unique patient
clusters were identified based on their involvement in
shared decision making: satisfied, content, and dissatisfied.
Satisfied patients (18 %) had a positive physician rela-
tionship and a high level of trust with their physician.
Content patients (48 %) had a moderate level of trust with
their physician. Dissatisfied patients (34 %) had a life
greatly affected by IBD, a low level of trust of their
physician, a negative relationship with their physician,
were skeptical of decisions, and did not rely on their
physician for assistance.
Conclusion This study provides valuable insights re-
garding patients’ perceptions of the shared decision-mak-
ing process in IBD treatment using a novel moment-to-
moment hybrid technology approach. Patient perspectives
in this study indicate an increased desire for shared deci-
sion making in determining an optimal IBD treatment plan.
This work has been presented in part at the American College of
Gastroenterology Annual Meeting, Las Vegas, NV, USA, on 22
October 2012.
Electronic supplementary material The online version of thisarticle (doi:10.1007/s40271-015-0126-z) contains supplementarymaterial, which is available to authorized users.
& Jennifer H. Lofland
1 Inflammatory Bowel Disease Center, Dartmouth–Hitchcock
Medical Center, Lebanon, NH, USA
2 Health Economics and Outcomes Research, Janssen
Scientific Affairs, LLC, 850 Ridgeview Drive, Horsham, PA
19044, USA
3 Incyte Corporation, Wilmington, DE, USA
4 Delta Modelling, Mt Prospect, IL, USA
5 BDJ Solutions, Melrose, MA, USA
6 The Benfield Group, St Louis, MO, USA
Patient
DOI 10.1007/s40271-015-0126-z

Key Points for Decision Makers
This study provides valuable patient insights
regarding the shared decision-making process in IBD
treatment using a novel moment-to-moment hybrid
research approach, which quantifies information
from focus groups using a large sample of cohorts.
Cluster analyses applied to the moment-to-moment
variables identified three unique patient clusters of
satisfaction with their role in decision making:
satisfied, content, and dissatisfied.
The majority of IBD patients want to be actively
involved in treatment decision making, want to be
well informed, and report increased satisfaction
when they participate in shared decision making.
However, a notable proportion of patients report
dissatisfaction with their role in shared decision
making, often resulting in a search for a new
physician.
Further research into the three distinct IBD patient
types, particularly the ‘Dissatisfied’ cluster of
patients who experience less shared decision making,
is warranted.
1 Introduction
Shared decision making is a collaborative engagement
process between patient and clinician through which de-
cisions are shared based on evidence-based medicine and
the values and needs of the patient [1]. Shared decision-
making tools, such as decision aids, are often used to
prepare patients for making a decision about a treatment
choice. Decision aids used in the decision-making process
have been shown to increase patient participation in deci-
sion making, reduce decisional conflict, and increase pa-
tient satisfaction [2–4]. Emerging evidence suggests that
other benefits of shared decision making and decision aids
include better self-management of disease, reduced medi-
cal costs, and physician satisfaction [5–7]. Shared decision
making is a model of healthcare that can promote quality
care and benefit multiple stakeholders throughout the
healthcare supply chain. Although existing data support the
benefits of implementing the shared decision-making
model, the model has not been widely adopted by health-
care practitioners [8]. The actual implementation of a
structured shared decision-making model will require a
paradigm shift among many stakeholders, and will need to
address the barriers that healthcare professionals have
identified in implementing a shared decision-making model
in clinical practice [8].
Inflammatory bowel disease (IBD) is comprised mainly
of two major chronic inflammatory disorders of the gas-
trointestinal tract—Crohn’s disease and ulcerative colitis.
IBD is a complex disease whose heterogeneous disease
process offers a clinical scenario that is unique for each
patient and requires long-term management. With the ad-
vent of biologic therapies (e.g. anti-tumor necrosis factor
[TNF] agents), which are currently considered standard
treatment for IBD, treatment options have greatly im-
proved. Furthermore, as a result of cumulative research that
has shown improved efficacy with early combined anti-
TNF and immunomodulator (thiopurine) therapy, a ‘top-
down’ versus ‘step-up’ approach to the use of anti-TNF
agents has become more accepted [9]. Based on the mul-
tiple medication options and different proposed treatment
algorithms, patients have a myriad of treatment choices
with varying risk–benefit profiles to consider, often leading
to patient psychosocial distress in the decision-making
process [10].
Because of the increasing complexity of IBD treatment
choices, it is critically important that patients with IBD
understand the potential benefits and risks of therapeutic
options prior to choosing an appropriate treatment. Shared
decision making is a collaborative way for IBD patients to
participate in choosing a treatment that best suits their
values and preferences. Unfortunately, prior research sug-
gests that individuals with IBD have brief, limited dis-
cussions with their gastroenterologists regarding treatment
options [11].
Siegel et al. have recently developed a shared decision-
making tool for patients with Crohn’s disease who are
contemplating a decision to use immunomodulators, anti-
TNF agents, or combination therapy [12, 13]. The decision
aid, using both pictorial and verbal explanations, offers
information regarding long-term treatment options, in-
cluding benefits and side effects. To date, limited infor-
mation is available on patients’ perspectives of shared
decision making or shared decision-making tools (i.e. de-
cision aids) used in IBD. In a survey conducted in over
1000 IBD patients, 81 % of respondents reported that it
was very important to be actively involved in the decision-
making process regarding treatment options [14]. There-
fore, additional research from the patient’s perspective is
needed to examine the barriers and motivations for im-
plementing shared decision making in the physician–pa-
tient conversation regarding IBD therapeutic intervention.
The objectives of the current study were to examine
patient insights about shared decision making among pa-
tients with IBD using novel statistical technology to ana-
lyze qualitative data. These patient-oriented data in the
C. A. Siegel et al.

current study are part of a three-phase, multi-stakeholder
research project that also includes physician research and
an expert consensus panel. It is hoped that the combined
data from these three research phases will offer key
learnings regarding stakeholders’ motivations and barriers,
and will generate recommendations for the effective and
efficient implementation of shared decision making.
2 Materials and Methods
2.1 Study Design
This was a mixed-methods research study consisting of
qualitative and quantitative components. This hybrid ap-
proach consisted of the following: (1) a qualitative com-
ponent—two focus groups; and (2) a quantitative
component—an online patient survey using key focus
group insights with moment-by-moment rated discussion.
2.2 Participants and Recruitment
Qualitative After approval from the Dartmouth College
Committee for the Protection of Human Subjects, two fo-
cus groups (one group of 10 ulcerative colitis patients and
one group of 10 Crohn’s disease patients) were conducted
in January 2012. Focus group patients were recruited
through Schlessinger Associates, a professional research
panel (Iselin, NJ, USA). Qualified focus group participants
were 18 years of age or older and resided in the US. Par-
ticipants had been diagnosed with Crohn’s disease and/or
ulcerative colitis by a gastroenterologist for 2 or more
years, had tried three or more different treatments since
IBD diagnosis, and had participated in an IBD focus group
no more than six times. Participants could also not be a
medical or market research professional. Potential par-
ticipants answered a brief screener survey to identify if
they qualified and were interested in participating in the
focus group.
Quantitative Survey participants were recruited in April
2012 through Research Now (Plano, TX, USA), a profes-
sional research panel. Qualified focus group participants
were 18 years of age or older and lived in the US. Par-
ticipants had been diagnosed with Crohn’s disease and/or
ulcerative colitis. If the participant had been diagnosed
with ulcerative colitis, the patient could not have had a
colectomy. Neither the participant nor a member of their
household could have been a medical professional.
2.3 Data Collection
Qualitative The purpose of the recorded focus group dis-
cussion was to explore patients’ experiences, concerns, and
preferences related to shared decision making in order to
identify how shared decision making tools can be more
commonly used and effectively and efficiently imple-
mented. Participants were asked about perception of their
disease, its management, and decision-making practices (if
any), relationship with their physician, knowledge of
shared decision making, and their insights towards imple-
mentation of shared decision making in their treatment
decision planning. The guiding principle in the focus
groups was to elicit both similar and contrasting opinions.
The focus group discussion followed the following format
(see online supplementary appendix for focus group mod-
erator guide): (1) began broadly by asking patients what
they considered to be a successful outcome of their
treatments; (2) explored patients’ knowledge level of IBD
and what actions they take to understand their disease and
its treatments; (3) moderated an in-depth discussion about
patients’ experiences with decision making; (4) discussed
patients’ assumptions about providers to understand per-
ceptions and attitudes that may impact the decision-mak-
ing process (from the patient perspective); (5) explored
patient ideas and recommendations regarding the approach
and processes that physicians and clinical staff should
have in place to promote patient engagement in decision
making; (6) focused on how treatment benefits and risks
should be addressed during the decision-making process;
and (7) included rating and prioritization of specific
treatment risks and benefits. The focus group discussion
lasted 2 h.
Quantitative The 25-min online patient survey consisted
of two audio clips featuring key excerpts taken from de-
identified focus group recordings, as well as 40 demo-
graphic and quantitative questions. Key audio excerpts (see
online supplementary appendix for survey details and au-
dio transcripts) were identified based on comments relative
to objectives of the research, comments about experiences
that might be relevant to large numbers of IBD patients,
and different opinions about common IBD-related issues.
Survey participants answered demographic and back-
ground health questions before they watched a 1-min video
tutorial that explained the use of a media rating tool and
allowed participants to practice using the tool (see online
supplementary appendix for audio training video script). A
total of 355 IBD patient participants were then asked to
‘listen and rate’ the key audio excerpts from the two focus
groups. The excerpts were approximately 8 and 4 min,
respectively. The content of the focus group excerpts re-
flected a range of patients’ perspectives on shared decision
making and experiences with IBD as described above in
the objectives of focus groups discussions.
The purpose of the media rating tool was to capture
participants’ ongoing reactions to what they were hearing
in a media stimuli. For this research application, a 0–10
Patients’ Perspectives on Shared Decision Making

Likert agreement scale was used, with ‘0’ representing
strongly disagree, ‘5’ representing neutral, and ‘10’ rep-
resenting strongly agree. Participants moved their pointing
device (mouse or touchpad) up and down to register their
agreement or disagreement while listening to the audio.
The rating tool was located directly under the media and
participants had easy visual clues, including a position
marker on the large scale and a number representing their
current rating position. Participants were instructed to re-
turn their mouse to a neutral position (5 on the 1–10 scale)
when the moderator was speaking, otherwise participants
could rate their level of agreement at any time during the
audio. Participant media rating position was recorded every
second, and up to 240 distinct data points were possible for
a 4-min media clip. The range of possible values was 0 and
10 with precision of 2 decimal points.
Following the rating of the audio, participants were asked
a set of discrete follow-up questions related to the focus
group discussion topics (see survey in the online supple-
mentary appendix for further details). No formal pilot study
was conducted; however, after 50 survey completions by
IBD patients, researchers reviewed the responses to assess
the quality of the data. Finding no discrepancies in patient
responses, no modifications to the survey were made and the
survey was continued to the conclusion of the study.
2.4 Data Analyses
Survey and media rating data were analyzed using a variety of
techniques, including descriptive statistics, crosstabs, sig-
nificance testing including Chi-square test for independence,
cluster analysis, and multiple discriminant analysis. The Chi-
square test for independence helped identify significant rela-
tionships between variables, while cluster analysis and mul-
tiple discriminant analysis were used exclusively for
analyzing media rating data. Simple descriptive statistics were
used to summarize demographics and discreet choice re-
sponses. An average of all participants’ second-by-second
ratings/traces were presented as a single ‘all-trace’ line. Ad-
ditional moment-to-moment trace lines using demographic
and other discrete variables were created to examine subseg-
ments of the sample such as gender, income, and age.
Cluster analysis was employed in order to detect distinct
patterns in media rating data that could not otherwise be
uncovered by looking at demographic or other quantitative
segments. The specific method of clustering used was
K-means, a non-hierarchical mutually exclusive clustering
method which allows cases to be reassigned until an opti-
mal cluster solution is reached. The clusters were not re-
quired to be of equal sizes. There was one outlier whose
data were not used or analyzed.
For each cluster, average moment-to-moment traces
were created and the patterns of response for each
individual cluster were examined on a second-by-second
basis over the audio portion of the survey. The mutually
exclusive cluster groups contain respondents who have a
similar response pattern. Specifically, patient response
patterns within a cluster group are more similar to each
other than the patterns identified in the other clusters. The
consistent pattern of the moment-to-moment traces is an
overall reflection of the group’s attitudinal and cognitive
response and reaction to the issues put forth in the focus
group audio excerpts. The different response patterns of
each cluster are remarkably different from the ‘all’ trace or
any other trace pattern generated by standard demographics
or a priori participant segments. Examining the trace pat-
terns of all the clusters over the course of an entire audio
discussion visually illustrates where clusters converge on a
common point of view (i.e. agree) and where their views
dramatically differ (i.e. disagree).
Clusters were named based on their respective cognitive
responses and attitudes inherent in moment-to-moment
trace patterns. Each cluster name was based upon the
unique response pattern and reaction (i.e. positive/nega-
tive) related to the content discussed throughout the
discussion.
Cross-tabs were used to identify significant relationships
between clusters in terms of demographics, attitudinal,
behavioral, and other relevant participant data to profile the
distinguishing characteristics of each cluster segment. The
frequency distribution (percentage of population) was re-
ported for categorical variables and descriptive statistics
(mean, standard deviation) were reported for continuous
variables. The Chi-square test for independence was used
to determine if there was a statistically significant rela-
tionship between the cluster group and other categorical
variables.
Multiple discriminant analysis was used to determine
divergent points of discussion between the three clusters.
The potency index was calculated based upon the structure
matrix and eigenvalues to determine the overall impact of
each second of the discussion group. Statistically sig-
nificant subsegments (blocks of time in seconds) within the
discussion were identified as the most divisive and dis-
criminating opinions among the clusters.
3 Results
Of the 355 IBD patients who completed the survey, mean
age was 49 years (range 18–50; 54 % female), 51 % had
ulcerative colitis, 49 % had Crohn’s disease, 21.4 % were
diagnosed less than 2 years ago, 39.4 % were diagnosed
between 2 and 10 years ago, and 39.2 % were diagnosed
10 or more years ago. Respondents represented different
levels of severity, as measured by abbreviated Mayo Clinic
C. A. Siegel et al.

and Crohn’s Disease Activity Index (CDAI) scores. The
majority of patients were well-educated (57 %) with a
bachelor’s or post-graduate degree. Almost half (47 %) of
IBD patients received insurance coverage through an em-
ployer. The majority of patients (55 %) had never used a
biologic medication. One-third of patients had used or were
using a biologic medication to treat their IBD, and 12 %
responded ‘don’t know’.
3.1 Quantitative Survey Results
3.1.1 Patient Knowledge of Inflammatory Bowel Disease
Almost all patients responded that they had some knowl-
edge of their IBD. The majority of patients said they were
knowledgeable to very knowledgeable about their disease
(66 %). Over three-quarters of patients had some knowl-
edge of the IBD treatment available to them; however, less
than half (41 %) said they were knowledgeable to very
knowledgeable about their treatment options.
3.1.2 Sources of Shared Decision-Making Information
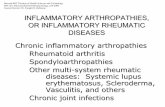
The vast majority of patients receive information about
IBD from their physicians (88 %), and half of the patients
used health information websites to learn about IBD
(Fig. 1). Physicians are patients’ most trusted source of
shared decision-making information (high trust 49 %).
Almost three-quarters of patients would prefer to receive
information about how shared decision making can help
them make decisions about IBD treatment from a face-to-
face conversation with physicians or their staff (74 %).
However, a large percentage are also comfortable learning
more about shared decision making and IBD from the In-
ternet (63 %).
3.1.3 Patient Satisfaction with Shared Decision Making
The majority of patients (66 %) reported increased satis-
faction with their care when they participated in shared
decision making. Many patients believe that they are al-
ready experiencing a form of shared decision making, with
72 % of patients indicating that their physician practices
shared decision making regularly or even more frequently.
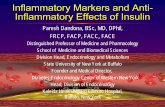
The majority of patients believe that their physicians treat
them with respect and listen to what they have to say
(Fig. 2).
Patients were largely satisfied with their role in decision
making and said that they have satisfactorily experienced
or understood components of the decision-making process.
However, approximately one-third of patients did not un-
derstand the benefits, risks, and side effects of each treat-
ment option, and 19 % were not satisfied with how much
they were participating in making decisions about their
IBD treatment. Approximately one-third of patients (32 %)
switched physicians because of the way the physicians
made IBD decisions. Patients who did not experience
shared decision making were interested in making shared
decisions more frequently (extremely interested 42 %).
When answering the question ‘‘What would you change
Fig. 1 Sources of IBD
information. IBD inflammatory
bowel disease
Patients’ Perspectives on Shared Decision Making

between you and your physician to make shared decision
making a positive experience for you?’’, patients had bal-
anced and pragmatic expectations of decision-making roles
and responsibilities (Fig. 3).
3.1.4 Patient Clusters
Cluster analyses applied to the moment-to-moment vari-
ables identified three unique patient clusters of satisfaction
with their role in decision making: satisfied (17.5 %),
content (47.7 %), and dissatisfied (34.7 %) (Fig. 4;
Table 1). Clusters were named based on their respective
cognitive responses and attitudes inherent in moment-to-
moment trace patterns. Each cluster name was based upon
the unique response pattern and reaction (i.e. positive/
negative) related to the content presented throughout the
discussion.
Satisfied patients (18 %) were characterized as having a
positive physician relationship and a high level of trust
with their physician. Ninety-seven percent of satisfied pa-
tients indicated high trust in their physician as an infor-
mation source compared with 81 % of content and 66 % of
dissatisfied patients (p\ 0.001). Satisfied patients
(n = 62) were more likely to agree with a set of statements
in the survey that generally indicated more confidence in
their decision making about their IBD and more
23%
19%
18%
14%
26%
27%
25%
25%
27%
30%
38%
45%
0% 20% 40% 60% 80% 100%
Agree Strongly Agree Completely Agree
My doctor treats me with respect
My doctor listens to what I have to say
in making decisions about my IBD treatment
Overall, I am confident in my IBD treatment decisions
84%
80%
76%
76%
Fig. 2 Decision-making
process between physician and
patient. IBD inflammatory
bowel disease
Fig. 3 Moment-to-moment of patient ideal scenario of shared decision making. SDM shared decision making
C. A. Siegel et al.

understanding of the risks and benefits. A higher percent-
age of satisfied patients (66 %) indicated that their physi-
cian practices shared decision making compared with
content (53 %) and dissatisfied (33 %) patients
(p\ 0.001).
Satisfied patients were more likely to be male (60 %;
p\ 0.001), older (52 % over 60 years of age), insured
through Medicare (42 %; p\ 0.001), and be diagnosed 10
or more years ago (52 %; p = 0.006). Disease severity was
generally mild to moderate, with the majority of satisfied
patients reporting a normal number of daily stools (ul-
cerative colitis, n = 180, 56 %; p\ 0.001). A majority of
satisfied Crohn’s disease patients (47 %; p = 0.019) indi-
cated that their overall well-being was ‘well’. Ap-
proximately three-quarters of satisfied patients indicated
that IBD had little effect on their work (77 %; p\ 0.001).
IBD had the least effect on satisfied patients, 74 % of
whom indicated that IBD had little effect on daily life
(p\ 0.001) compared with 64 % of content and 29 % of
dissatisfied patients.
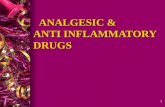
Figure 5 features a cluster trace for a key section of
audio related to physician–patient relationship. Table 2
contains the quotes associated with the Fig. 5 rated audio
clip. This audio clip demonstrates how the clusters’ cog-
nitive responses and inherent attitudes differed from each
other. When responding to audio about physician–patient
relationships, the satisfied cluster showed a significantly
more positive relationship with their physician and the
dissatisfied cluster had less trust and a weaker relationship
overall with their physician. For example, the satisfied
Fig. 4 Patient moment-to-moment responses based on cluster analysis-audio segment: perspectives on treatment decisions with physicians
Table 1 Cluster profiles
Cluster description
Satisfied cluster
(17.5 %)
More positive relationship with physician
Higher level of trust with their physician
Older and more likely to have been diagnosed
10 or more years ago
Less severe and better managed IBD
Content cluster
(47.7 %)
More or less content
Moderate level of trust in their physician
Dissatisfied cluster
(34.7 %)
Dissatisfied and negative relationship with
physician
Life and work more affected by IBD
Lower level of trust in their physician
More skeptical about decisions made by
physician
More interested in getting information about
IBD from sources other than their physician
IBD inflammatory bowel disease
Patients’ Perspectives on Shared Decision Making

cluster agreed very strongly with the sentiment ‘‘I had a
wonderful doctor who was all about health…I trust his
opinion and his treatment choices…’’, moving from an
average rating near 2 to an average rating near 9. The
content cluster also agreed with this statement, shifting
from an average rating of approximately 5 to almost 7.
Meanwhile, the dissatisfied cluster was the only cluster
where the average rating decreased (from approximately 8
to 7).
Content patients had less severe or more controlled
cases of IBD. Furthermore, the effect of IBD on the life of
content patients was generally moderate or minimal. Fifty-
eight percent (58 %) of content ulcerative colitis patients
indicated a normal number of stools. This percentage is
similar to the 56 % of satisfied patients but quite different
from the 23 % of dissatisfied patients (p\ 0.001). Almost
two-thirds (64 %) of content patients indicated that IBD
had little effect on work compared with 77 % of satisfied
patients and 39 % of dissatisfied patients (p\ 0.001). Over
one-third of content patients (36 %) indicated that IBD had
some effect on their daily life compared with 26 % of
satisfied patients and 71 % of dissatisfied patients
Fig. 5 Audio snapshot of moment-to-moment response regarding the doctor–patient relationship
Table 2 Cluster trace quotes for Fig. 5
Marker Quote
G I don’t trust them. I want to know what they’re up to and what they’re thinking and I want to talk to another doctor if I don’t think I’m
getting enough information from them
H I’ve seen a few doctors that I feel like are a bit arrogant and they talk to you like you’re an idiot, and at times I won’t listen to advice
that I’ve been given
I I had a wonderful doctor who was all about health, restoration, and prosperity. Because of that, I trust his opinion and his treatment
choices, and if it’s not broke, don’t fix it
J I think maybe if I had more trust in my doctor then I wouldn’t be so skeptical of his suggestions
K I try to take as little prescription drugs as possible. I’d rather have a doctor that’s going to help me treat myself
L I am not saying I don’t believe in doing all I can to help control my disease, but at the end of the day, I trust my doctor to prescribe
medications that will help me get better
M Sometimes when I ask for the options, he might tell me, with this percentage of your colon being inflamed, this is the only option you
have, he’ll explain it to me. But, I have to push for that, for him to say, these are all the options that are available to you and this is the
percentage of good they would be by treating it or not
C. A. Siegel et al.

(p\ 0.001). Content patients (48 %) were characterized as
having a moderate level of trust with their physician.
Eighty-one percent (81 %) of content patients indicated a
high level of trust in their doctor compared with 97 % of
satisfied patients and 66 % of dissatisfied patients
(p\ 0.001). Gender distribution was skewed slightly to-
wards males in content patients (56 %; p\ 0.001).
Dissatisfied patients were characterized by the follow-
ing: (1) being dissatisfied; (2) having a life that is greatly
affected by IBD; (3) having a low level of trust of their
physician; (4) having a negative relationship with their
physician; (5) being skeptical of decisions made by their
physician; and (6) not relying on their physician for as-
sistance. Dissatisfied patients were more likely to be female
(76 %; p\ 0.001), younger (over 60 years of age, 12 %;
35 years of age or younger, 32 %; p\ 0.001), and not as
likely to be diagnosed 10 or more years ago (27 %;
p = 0.006) compared with satisfied patients.
Only one-third (33 %; p\ 0.001) of dissatisfied patients
indicated that their physician almost always practices
shared decision making with them. Dissatisfied patients
(59 %; p = 0.022) were also more likely than the other
clusters to get information about their IBD from health
information websites. Approximately 95 % of patients in
the satisfied and content patient clusters thought that the
physician was the most useful information source com-
pared with 85 % of dissatisfied patients (p = 0.004). In
general, dissatisfied patients reported higher severity of
disease compared with satisfied patients. Unlike satisfied
patients, fewer dissatisfied patients had normal stools (ul-
cerative colitis, 23 %; p = 0.001). Similarly, only 16 %
(p = 0.019) of dissatisfied Crohn’s disease patients indi-
cated that their overall well-being was ‘well’. Ap-
proximately one-third of dissatisfied patients indicated that
IBD had little effect on their work (39 %; p\ 0.001) and
daily life (29 %; p\ 0.001). Thirty-nine percent (39 %) of
dissatisfied patients indicated that IBD had a moderate
effect on daily life compared with less than 15 % for sat-
isfied and content patients.
4 Discussion
The results of this study offer unique insights into IBD
patients’ perspectives on shared decision making as it re-
lates to treatment of their disease. Although IBD patients
are knowledgeable about their disease, they fall short of
understanding the risks and benefits of IBD treatment op-
tions. IBD patients value their physicians’ support and
expertise as a trusted source of information and prefer face-
to-face conversations. The majority of patients use Internet
resources to gather shared decision making and IBD in-
formation. These IBD patients want to be actively involved
in treatment decision making, want to be well informed,
and report increased satisfaction when they participate in
shared decision making. However, the data show that a
notable proportion of patients report dissatisfaction with
their role in shared decision making, often resulting in a
search for a new physician.
The three distinct clusters of patients identified were
those who were satisfied, content, or dissatisfied with the
shared decision-making process with regard to the deter-
mination of an optimal IBD treatment strategy. The dif-
ference in demographics and disease characteristics
between satisfied and dissatisfied patients are notable yet
inconclusive. The dissatisfied cluster of IBD patients de-
scribes a population of patients who tend to be younger,
female, have greater disease severity, and report less shared
decision making. The reasons for these patients’ dissatis-
faction are unknown. However, contributing factors may
include, but are not limited to, patients not participating in
shared decision making with their physicians, or severity of
disease (i.e. patients’ disease process was less treatable).
Regardless of the reason for the dissatisfaction in the shared
decision-making process, these patients are clearly suffer-
ing to a greater degree than other patients and deserve closer
examination. More research is needed to learn more about
this dissatisfied cluster of patients, their current experi-
ences, and how systematic shared decision making may
improve their future experiences. Similarly, further research
on the satisfied and content clusters of patients may enhance
understanding around the favorable aspects of the shared
decision-making process from the patient’s perspective.
The management of a chronic condition such as IBD,
with cycles of severe symptoms and remission, is par-
ticularly challenging to treat and manage long term. This
makes IBD well-suited to a comprehensive shared deci-
sion-making approach to treatment. A fundamental re-
quirement of effective shared decision-making practice is a
strong doctor–patient relationship. The cluster analysis has
enabled us to identify and begin to describe the relationship
between shared decision making, patient–physician inter-
actions, and disease severity. Although this relationship
seems intuitive, the research confirms that shared decision
making for a chronic condition such as IBD is likely easier
and more effective among patients who have a strong
positive relationship with their physician [15, 16]. The
satisfied cluster of patients in this study illustrates one end
of a spectrum featuring a patient group with a high level of
trust in their physician and less severe or better-managed
IBD. In contrast, the dissatisfied cluster is on the other end
of the spectrum and is characterized by a poor relationship
and less trust in their doctor, more severe IBD, more
skepticism of the information provided by their physician,
and a greater desire to get information from alternative
sources.
Patients’ Perspectives on Shared Decision Making

Shared decision-making tools, such as treatment deci-
sion aids, can increase patient involvement and satisfaction
in the shared decision-making process [3, 4]. However,
understanding patients’ perspectives on shared decision
making is the essential first step for implementing the ap-
propriate shared decision-making tools and decision aids in
patients with IBD. Patients with IBD have been shown to
misperceive the benefits and risks of IBD treatment options
and demand a high remission rate before they are willing to
accept treatment-related risks [11]. Although there is a
paucity of data on the subject of shared decision making in
IBD patients, the conclusions of the few existing reports
support those of the current study in that patients are often
confused about the benefit–risk profiles of IBD treatments,
and they feel it is important to be actively involved in
making decisions regarding treatment of IBD [14].
Focus groups are a widely used research method to gain
various patient insights and provide qualitative in-depth
learning of behaviors, attitudes, and perceptions. However,
due to the small number of participants (usually 10–12) in a
focus group, qualitative information derived from these
groups lacks the empirical robustness of traditional quan-
titative approaches. Furthermore, researchers struggle to
quantify, analyze, and interpret focus group research re-
sults in order to generalize qualitative opinions to larger
populations. Therefore, the objective of the online-rated
focus group discussion was to understand why IBD patients
think and feel the way they do about shared decision
making and IBD and to quantify those emotions.
The online-rated focus group discussion is a research
method that generates a moment-to-moment tracking pro-
cess similar to the research method currently used to track
the level of positive or negative affect that a consumer
experiences and displays while watching a television ad-
vertisement. This technology has also been used to visu-
alize feedback to candidates’ comments from opposing
party focus groups during a political debate. Prior research
using moment-to-moment evaluations of television adver-
tisements has typically used this methodology to link key
aspects of the affect trace to retrospective evaluations of
the advertisement [17]. Similarly, this approach in the
current study assumes that participants listening and rating
an IBD patient focus group discussion are integrating both
positive and negative emotional content in forming their
overall evaluation of the focus group discussion. The novel
hybrid research methodology used in this study, which
integrates traditional qualitative and quantitative research
in a single process, has identified varying patient shared
decision-making needs based on patient characteristics,
perceptions, and beliefs of different IBD populations.
Media rating technology has been employed most ex-
tensively in the testing of commercials by major advertisers
and for political research [17, 18]. The use of the media
rating technology specifically for longer form audio such as
focus groups is, to our knowledge, not common. The value
of applying this methodology to patient research is poten-
tially enormous and still not fully realized. Better under-
standing of patient experience is critical to better disease
management and patient outcomes. Standard qualitative
research, including interviews and focus groups, is effec-
tive at getting in-depth patient perspectives. However, this
kind of research is difficult to generalize and to know how
representative these perspectives are to the patient
population as a whole. Quantitative research, including
surveys, can provide a summary overview of a wide range
of topics but provides shallow understanding. The media
rating technology seeks to bridge this gap by quantifying
qualitative data. A more nuanced and complex under-
standing of patients’ feelings about their disease, their re-
lationship with their doctor, and the overall treatment
process can be achieved through examination of overall
average, segment, and cluster media rating data.
Interpretations of the results of this study may be limited
by the following factors. First, this moment-to-moment
hybrid approach is a novel statistical method, particularly
in the field of shared decision making, and few published
data are available by which to compare the results of the
current study. To our knowledge, there is no published
literature where moment-to-moment trace methodology is
used to measure cognitive responses in either focus group
or in-depth interview research. Second, the views repre-
sented by the few patients in this study may not be repre-
sentative of the entire population of patients with IBD.
Third, only patients who had a computer and Internet ac-
cess were eligible to participate. Finally, some participants
may not have completely understood the moment-to-mo-
ment technology required for appropriate response and
participation.
5 Conclusions
This study provides valuable patient insights regarding the
shared decision-making process in IBD treatment using a
novel moment-to-moment hybrid technology approach.
Patient perspectives in this study indicate an increased
desire for shared decision making in determining an opti-
mal IBD treatment plan. Further research into the three
distinct IBD patient types, particularly the ‘Dissatisfied’
cluster of patients who experience less shared decision
making, is warranted. Finally, results from the online-rated
focus group discussions support the shared decision-mak-
ing model approach to IBD treatment.
Acknowledgments The authors wish to acknowledge the following
individuals for their contributions and critical review during the
C. A. Siegel et al.

development of this manuscript on behalf of Janssen Scientific Af-
fairs, LLC: Kim Poinsett-Holmes, PharmD, Poinsett Publications,
Inc., for medical writing and editorial assistance. This study was
sponsored by Janssen Scientific Affairs, LLC (Horsham, PA, USA).
Corey Siegel contributed to the study concept and design. Jennifer
Lofland and Ahmad Naim contributed to the study concept, design,
methods, and analyses. Jan Collins and Danielle Walls contributed to
the study design, methods, data collection, and analyses. Laura
Rudder and Chuck Reynolds contributed to the study design, meth-
ods, and data collection. All authors discussed the results and im-
plications, and commented on the manuscript at all stages. All authors
reviewed the final manuscript. Jennifer Lofland is the guarantor for
the study.
Conflict of interest Corey Siegel has received consulting fees from
Abbvie, BiolineRX, Given Imaging, Lilly, Janssen, Salix, Millenium,
Pfizer, Prometheus, Takeda, and UCB, as well as grants from the
Crohn’s and Colitis Foundation of American (CCFA), the Agency for
Healthcare Research and Quality (AHRQ) [1R01HS021747-01],
Abbvie, Janssen, Salix, Warner-Chilcott, and UCB.
Jennifer Lofland is an employee of Janssen Scientific Affairs, LLC.
At the time of the study, Ahmad Naim was an employee of Janssen
Scientific Affairs, LLC. Danielle Walls, Jan Collins, Laura Rudder,
and Chuck Reynolds were employed as subcontractors by Janssen
Scientific Affairs, LLC.
References
1. Towle A, Godolphin W. Framework for teaching and learning
informed shared decision making. BMJ. 1999;319:766–71.
2. O’Connor AM, Bennet CL, Stacey D, et al. Decision aids for
people facing health treatment or screening decisions. Cochrane
Database Syst Rev. 2009;(3):CD001431.
3. Glass KE, Wills CE, Holloman C, et al. Shared decision making
and other variables as correlates of satisfaction with health care
decisions in a United States national survey. Patient Educ Couns.
2012;88:100–5.
4. Lim E. Patients’ perspective in the surgical decision-making
process. Thorac Surg Clin. 2012;22:539–43.
5. Kennedy ADM, Sculpher MJ, Coulter A, et al. Effects of decision
aids for menorrhagia on treatment choices, health outcomes, and
costs. JAMA. 2002;288:2701–9.
6. Sullivan MD, Leigh J, Gaster B. Brief report: training internists in
shared decision making about chronic opioid treatment for non-
cancer pain. J Gen Intern Med. 2006;21:360–2.
7. Sieber W, Newsome A, Lillie D. Promoting self-management in
diabetes: efficacy of a collaborative care approach. Fam Syst
Health. 2012;30(4):322–9.
8. Legare F, Ratte S, Gravel K, et al. Barriers and facilitators to
implementing shared decision-making in clinical practice: update
of a systematic review of health professionals’ perceptions. Pa-
tient Educ Couns. 2008;73:526–35.
9. Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab, aza-
thioprine, or combination therapy for Crohn’s disease. N Engl J
Med. 2010;362:1383–95.
10. Lipstein EA, Lovell DJ, Denson LA, et al. Parents’ information
needs in tumor necrosis factor-a inhibitor treatment decision.
J Pediatr Gastroenterol Nutr. 2013;56:244–50.
11. Baars JE, Siegel CA, Kuipers EJ, et al. Patient’s perspectives
important for early anti-tumor necrosis factor treatment in in-
flammatory bowel disease. Digestion. 2009;79:30–5.
12. Siegel CA, Siegel LS, Hyams JS, et al. Real-time tool to display
the predicted disease course and treatment response for children
with Crohn’s disease. Inflamm Bowel Dis. 2011;17:30–8.
13. Siegel CA. Review article: explaining risks of inflammatory
bowel disease therapy to patients. Aliment Pharmacol Ther.
2011;33:23–32.
14. Baars JE, Markus T, Kuipers EJ, et al. Patients’ preferences re-
garding shared decision-making in the treatment of inflammatory
bowel disease: results from a patient-empowerment study.
Digestion. 2010;81:113–9.
15. Falke SI, Lawson L. Couples with diabetes and health-care pro-
viders: a grounded theory of preferential relating. Health Expect.
2014. doi:10.111/hex.12302 (Epub 10 Nov 2014).16. Shay LA, Lafata JE. Understanding patient perceptions of shared
decision making. Patient Educ Couns. 2014;96:295–301.
17. Baumgartner H, Sujan M, Padgett D. Patterns of affective reac-
tions to advertisements: the integration of moment-to-moment
responses into overall judgments. J Mark Res. 1997;34:219–32.
18. Elpers JLCMW, Wedel M, Pieters RGM. The influence of mo-
ment-to-moment pleasantness and informativeness on zapping
TV commercials: a functional data and survival analysis ap-
proach. In: Broniarczyk SM, Nakamoto K, editors. Advances in
consumer research. Valdosta: Association for Consumer Re-
search; 2002. p. 57–58.
Patients’ Perspectives on Shared Decision Making