NOTICE OF PUBLIC MEETING – DRUG USE REVIEW BOARD … · ii. Presentation of utilization and...
674
NOTICE OF PUBLIC MEETING – DRUG USE REVIEW BOARD REVISED AGENDA Date of Posting: xxxxx Date of Meeting: Thursday, January 22, 2015 at 5:30 PM Name of Organization: The State of Nevada, Department of Health and Human Services, Division of Health Care Financing and Policy (DHCFP), Drug Use Review Board (DUR). Place of Meeting: Silver Legacy Silver/Gold Room 407 N Virginia St Reno, Nevada 89501 AGENDA 1. Call to Order and Roll Call 2. Public Comment on Any Matter on the Agenda 3. Administrative a. For Possible Action: Review and Approve Meeting Minutes from July 24, 2014. b. Status Update by DHCFP i. Public Comment ii. Medicaid’s overview of the upcoming legislative session iii. Introduction of new member, Dr. Michael Owens. 4. Presentation and Discussion of Nevada’s Prescription Monitoring Program a. Jenine M. Davis, Pre-Criminal Intervention Officer, Controlled Substance Abuse Prevention Task Force 5. Clinical Presentations ROMAINE GILLILAND Director STATE OF NEVADA DEPARTMENT OF HEALTH AND HUMAN SERVICES DIVISION OF HEALTH CARE FINANCING AND POLICY 1100 E. William Street, Suite 101 Carson City, Nevada 89701 (775) 684-3600 BRIAN SANDOVAL Governor LAURIE SQUARTSOFF Administrator
Transcript of NOTICE OF PUBLIC MEETING – DRUG USE REVIEW BOARD … · ii. Presentation of utilization and...
-
NOTICE OF PUBLIC MEETING – DRUG USE REVIEW BOARD
REVISED AGENDA
Date of Posting: xxxxx Date of Meeting: Thursday, January 22, 2015 at 5:30 PM Name of Organization: The State of Nevada, Department of Health and Human
Services, Division of Health Care Financing and Policy (DHCFP), Drug Use Review Board (DUR).
Place of Meeting: Silver Legacy Silver/Gold Room
407 N Virginia St Reno, Nevada 89501
AGENDA 1. Call to Order and Roll Call
2. Public Comment on Any Matter on the Agenda
3. Administrative
a. For Possible Action: Review and Approve Meeting Minutes from July 24, 2014.
b. Status Update by DHCFP
i. Public Comment ii. Medicaid’s overview of the upcoming legislative session iii. Introduction of new member, Dr. Michael Owens.
4. Presentation and Discussion of Nevada’s Prescription Monitoring Program
a. Jenine M. Davis, Pre-Criminal Intervention Officer, Controlled Substance Abuse Prevention Task Force
5. Clinical Presentations
ROMAINE GILLILAND Director
STATE OF NEVADA DEPARTMENT OF HEALTH AND HUMAN SERVICES
DIVISION OF HEALTH CARE FINANCING AND POLICY 1100 E. William Street, Suite 101
Carson City, Nevada 89701 (775) 684-3600
BRIAN SANDOVAL Governor
LAURIE SQUARTSOFF Administrator
-
Page 2
a. For Possible Action: Discussion and proposed adoption of updated clinical prior
authorization criteria for sofosbuvir (Sovaldi®). i. Public comment on proposed clinical prior authorization criteria. ii. Presentation of utilization and clinical information. iii. Discussion by the Board and review of utilization data. iv. Proposed adoption of updated prior authorization criteria.
b. For Possible Action: Discussion and proposed adoption of prior authorization criteria
for Ledipasvir-Sofosubuvir (Harvoni®)
i. Public Comment on proposed clinical prior authorization criteria. ii. Presentation of utilization and clinical information. iii. Discussion by the Board and review of utilization data. iv. Proposed adoption of updated prior authorization criteria
c. For Possible Action: Discussion and proposed adoption of updated clinical prior authorization criteria for simeprevir (Olysio®). i. Public comment on proposed clinical prior authorization criteria. ii. Presentation of utilization and clinical information. iii. Discussion by Board and review of utilization data. iv. Proposed adoption of updated prior authorization criteria.
d. For Possible Action: Discussion and proposed adoption of updated prior authorization criteria for Oxycodone w/acetaminophen tab CR (Xartemis XR®)
i. Public Comment on proposed clinical prior authorization criteria. ii. Presentation of utilization and clinical information. iii. Discussion by the Board and review of utilization data. iv. Proposed adoption of updated prior authorization criteria.
e. For Possible Action: Discussion and proposed adoption of updated prior authorization criteria for apixaban (Eliquis®)
i. Public Comment on proposed clinical prior authorization criteria. ii. Presentation of utilization and clinical information. iii. Discussion by the Board and review of utilization data. iv. Proposed adoption of updated prior authorization criteria.
f. For Possible Action: Discussion and proposed adoption of updated clinical prior authorization criteria for the immunomodulator class of medication. i. Public comment on proposed clinical prior authorization criteria. ii. Presentation of utilization and clinical information. iii. Discussion by Board and review of utilization data.
-
Page 3
iv. Proposed adoption of updated prior authorization criteria.
g. For Possible Action: Discussion and proposed adoption of updated clinical prior authorization criteria for transdermal fentanyl. i. Public comment on proposed clinical prior authorization criteria. ii. Presentation of utilization and clinical information. iii. Discussion by Board and review of utilization data. iv. Proposed adoption of updated prior authorization criteria.
h. For Possible Action: Discussion and proposed adoption of updated clinical prior authorization criteria for palivizumab (Synagis®). i. Public comment on proposed clinical prior authorization criteria. ii. Presentation of utilization and clinical information. iii. Discussion by Board and review of utilization data. iv. Proposed adoption of updated prior authorization criteria.
6. DUR Board Requested Reports
a. Report on Top 10 Black Box warning medications: i. Public comment on Black Box warnings. ii. Discussion by the Board and review of utilization data.
b. Report on controlled substance utilization and trends. i. Public comment on controlled substance utilization and trends. ii. Discussion by the Board and review of utilization data.
c. Report on psychotropic drug use in children. i. Public comment on psychotropic drug use in children. ii. Discussion by the Board and review of utilization data.
d. Report on buprenorphine and buprenorphine/naloxone use. i. Public comment on buprenorphine and buprenorphine/naloxone use. ii. Discussion by the Board and review of utilization data.
e. Report on Nevada Medicaid Lock-in Program i. Public comment on Lock-in Program. ii. Discussion by the Board and review of utilization data.
f. Report on Asthma treatment utilization.
-
Page 4
i. Public comment on asthma treatment utilization. ii. Discussion by the Board and review of utilization data.
g. Report on Tussionex Utilization. i. Public comment on Tussionex Utilization. ii. Discussion by the Board and review of utilization data.
7. Standard DUR Reports
a. Review of Prescribing/Program Trends. i. Top 10 Therapeutic Classes for Q2 2014, Q3 2014, and Q4 2014 (by Payment and
by Claims). ii. Top 50 Drugs of Q2 2014, Q3 2014, and Q4 2014 (by Payment and by Claims).
b. Concurrent Drug Utilization Review (ProDUR)
i. Review of Q2 2014, Q3 2014, and Q4 2014. ii. Review of Top Encounters by Problem Type.
c. Retrospective Drug Utilization Review (RetroDUR)
i. Public comment on Retro DUR. ii. Status of previous quarter. iii. Status of current quarter. iv. Review and discussion of responses.
8. Closing Discussion
a. Public comments on any subject.
b. Date and location of the next meeting.
i. Discussion of the time of the next meeting.
c. Adjournment.
Nevada Medicaid is unaware of any financial impact to other entities or local government due to this public hearing, other than as stated above.
PLEASE NOTE: Items may be taken out of order at the discretion of the chairperson. Items may be combined for consideration by the public body. Items may be pulled or removed from the agenda at any time. If an action item is not completed within the time frame that has been allotted, that action item will be continued at a future time designated and
-
Page 5
announced at this meeting by the chairperson. All public comment may be limited to 5 minutes.
This notice and agenda have been posted at www.dhcfp.nv.gov and http://notice.nv.gov Notice of this meeting and draft copies of the changes will be available on or after the date of this notice at the DHCFP Web site www.dhcfp.nv.gov, Carson City Central office and Las Vegas DHCFP. The agenda posting of this meeting can be viewed at the following locations: Nevada State Library; Carson City Library; Churchill County Library; Las Vegas Library; Douglas County Library; Elko County Library; Lincoln County Library; Lyon County Library; Mineral County Library; Tonopah Public Library; Pershing County Library; Goldfield Public Library; Eureka Branch Library; Humboldt County Library; Lander County Library; Storey County Library; Washoe County Library; and White Pine County Library and may be reviewed during normal business hours. If requested in writing, a draft copy of the changes will be mailed to you. Requests and/or written comments on the proposed changes may be sent to the Rita Mackie at the Division of Health Care Financing and Policy, 1100 E. William Street, Suite 101, Carson City, NV 89701, at least 3 days before the public hearing. All persons that have requested in writing to receive the Public Hearings agenda have been duly notified by mail or e-mail. Note: We are pleased to make reasonable accommodations for members of the public who are physically challenged and wish to attend the meeting. If special arrangements for the meeting are necessary, please notify the Division of Health Care Financing and Policy, in writing, at 1100 East William Street, Suite 101, Carson City, Nevada 89701 or call Rita Mackie at (775) 684-3681, as soon as possible, or e-mail at [email protected]
mailto:[email protected]
-
1
Nevada Medicaid Drug Use Review (DUR) Board
Draft Meeting Minutes
The Division of Health Care Financing and Policy (DHCFP) Drug Use Review (DUR) Board conducted a public meeting on July 24, 2014 beginning at 5:30 pm at the following location:
Best Western Airport Plaza Hotel
1981 Terminal Way Reno, NV 89502-3215
Paul Oesterman, Pharm.D., Chairman; Dave England, Pharm.D.; James Marx, M.D; Larry Nussbaum, MD
Board Members Present:
Board Member Absent:
Jeff Zollinger, DO; Chris Shea, Pharm.D.
Others Present:
Coleen Lawrence, Chief, Program Services; Mary Griffith, RN, Pharmacy Services Specialist; Darrell Faircloth, Senior Deputy Attorney General;
DHCFP:
Beth Slamowitz, Pharm.D. HPES:
Carl Jeffery, Pharm.D. Account Manager Catamaran:
Lori Howarth, Bayer; Scott Larson, BMC; Lisa Borland, Vertex; Cathy Gross, Vertex; Joe Hubbard, CNUCOR; Sandy Sierawski, Pfizer
Others:
ROMAINE GILLILAND Director
LAURIE SQUARTSOFF
Administrator
STATE OF NEVADA DEPARTMENT OF HEALTH AND HUMAN SERVICES
DIVISION OF HEALTH CARE FINANCING AND POLICY 1100 E. William Street, Suite 101
Carson City, Nevada 89701 www.dhcfp.nv.gov BRIAN SANDOVAL
Governor
-
2
1. Call to Order and Roll Call Meeting called to order at 5:32PM. Roll Call: Carl Jeffery - Catamaran Jim Marx - Las Vegas Pain Management Physician Larry Nussbaum - Reno School of Medicine David England - Las Vegas Pharmacist Paul Oesterman - Pharmacist Reno Chair Darrell Faircloth – Senior Deputy Attorney General Beth Slamowitz – HP Mary Griffith – Nevada Medicaid Coleen Lawrence – Nevada Medicaid
2. Public Comment Sandy Sierawsky – Pharmacist in Nevada – Pfizer/Medical Division: Requested board review prior authorization criteria for the oral anticoagulants Pradaxa, Xarelto, and Eliquis. Eliquis has been approved by the FDA for an additional indication, so we would like the criteria used so that it could potentially be incorporated in that criteria. PO: Because it’s not an agenda item, we will add it for the agenda for next time, that way it will be actionable.
3. Administrative Review and approve April 24, 2014 meeting minutes. JM: Motion to approve minutes. DE: Seconded. Discussion: None. Board votes unanimous, “Aye.” Minutes approved.
4. Status Update by DHCFP Mary Griffith – RN, Pharmacy Services Specialist: Provided the following updates: OPR, (Ordering Prescribing Referring) physicians, we’ve been talking about that for several months now and we actually have the implementation date. There are web announcements in the back. It’s going to be effective/ soft edit/ a portion of it goes into effect August 18th, 2014. That means that if there is a drug that is prescribed by someone who is not a Medicaid provider, there will be a message that comes up that says “This prescription is prescribed by someone who is not enrolled in Medicaid”. Next time that fill comes in, if it’s after October 1st, it’s going to deny. October 15th is the hard edit. So for
-
3
October 1st
Board: When is that effective?
too, it’s going to be effective for everybody, not just pharmacy, so if you have any physicians that you go and visit, they will be effected by this also.
Mary: October 15thColeen: It’s common obviously, already, in the pharmacy world, this is on the record, and Medicare has already implemented it. It’s implemented in other states and has been implemented in other states for years. I think pharmacy is going to be a natural transition. It’s expected in the pharmacy world. I expect that we’re going to see unknown impact. It’s going to be in other areas in healthcare where there’s what I call the triad. And the triad would be physician, or a prescriber; a supplier; and then another provider, so a direct service provider. A good example would be a home health provider, or a DME company. That’s where it’s going to get a little trickier because the ordering and the direct servicing is going to be a little bit different. As a physician, it’s going to be an education pattern that we’re going to have to get out there with.
. That is when the hard edit hits. The soft edit starts next month.
Mary: The hope is that when the pharmacist sees that new message that they inform the recipient. “Hey your doctor is not a Medicaid provider. Next time, if you need a refill on this, it’s going to get denied.” so that the recipient can go to their own doctor and get them on our enrollment. PO: Is there a bypass mechanism for somebody who is taking call or covering for a Medicaid provider who is himself not a provider? Coleen: The only way that I would say in that kind of a scenario, is interns, such as in the emergency room, hospitalists and interns are not applicable to this rule. They fall under the hospital benefit themselves, so that’s the only caveat, if you want to say taking call for somebody, that’s the only exception to this rule. LN: So trainees, like residents? Coleen: Residents are not applicable, interns… LN: Even if they’re in a clinic, not in a hospital? Coleen: If they fall under the resident role, and I mean the Medicare Resident role, those are the only ones. You’re required to have your NPI and follow those rules, you must fall under the OPR. Mary: Also, there is going to be a mechanism for 30 days after the hard edit for the pharmacist to be able to override, if they come across someone that doesn’t have that provider enrollment. They will be able to override that, but that’s only going to happen for the first 30 days and then it’s going to be turned off. Coleen: That’s only for Pharmacy. DE: And that’s until 11/15, they can override if they need to? Mary: Right. The Governor has created a controlled substance task force. Very high level, different political people that are involved in it. Our administrator Laurie Squartsoff is involved in it also. I’m not sure how often they meet, but it’s definitely something that we’re following because it’s gone to the Governor’s level on this. We’re still involved with the substance abuse task force for the Board of Pharmacy. They haven’t had a meeting recently, I don’t think, but we’re definitely involved with that in encouraging physicians to enroll in the PMP program. JM: There actually is movement afoot through the Pharmacy Board to be registered at the time of medical licensing (and possibly DOs), or will be required to do that as a part of their relicensure. There will be virtually 100% enrollment. That doesn’t mean 100% participation.
-
4
Mary: Next month we have someone from the Board of Pharmacy that is familiar with the PMP program to come talk to us [about the changes being made] in October. Coleen: We’re continuously recruiting for positions, whether it’s on this board, or the P&T, because we have an open position that will be on the P&T for a psychiatrist. Our goal is to expand the participation on this board by statute of ten members. If there are any nominations, please send them to our office and we’ll work with our director for this board, and we’ll work with the Governor’s office for the P&T. For this board, we’re looking for Best Practice and Standards of Care for clinical criteria and utilization and the P&T is strictly for the Preferred Drug List. PO: Any updates in terms of Healthcare Reform? Coleen: Last month they hosted the National Association of Medicaid Directors conference in Tahoe. We had feedback from all the different states about what was going on with Healthcare Reform. I will state that Nevada ranked as one of the only states that did a full Medicaid expansion duplicating the current Medicaid benefit. So we’re still really proud of that decision by our Director and our Governor to fully replicate our current Medicaid benefit plan as a single Medicaid program. What we have learned from all the other states, if they chose to expand Medicaid, that was step one. Step two was really narrowing their benefit plan. Although there have been hurdles of what’s happened on the Medicaid side, I will definitely say that it’s been very seamless as to what has happened with our Medicaid expansion. Our eligibility population has grown tremendously. They’re projecting somewhere in the area of 500,000 by the end of the year for Medicaid expansion. I can get you the exact numbers, but they are posted on our DHS website, but those are the numbers I keep hearing. On a positive note, at our lowest point of Medicaid expansion, we had up to 60,000+ applications in the queue for our backlog of eligibility. I was at a meeting on Tuesday, and the Division of Welfare and Supportive Services said that they have approximately 6,000 applications in the queue which is by far the best they have ever had in their history. So this administration and DWSS’s administration have definitely put all of their resources forward in doing improvements on their welfare process to really streamline what’s going on in there. Whoever touches the application is the one who finishes the application. It’s very positive on the eligibility side. We’re hearing that there are literally determinations that day on eligibility now, so it’s very positive. Very big push for us, on the Medicaid side, to work with our providers to encourage providers to actually accept Medicaid patients. What we’re trying to do is figure out what are the barriers. We wake up every day saying “We’re not that system who wants to deny patients, or deny care. And we don’t want to deny payment.” So what we’re doing is going out there and in meetings like this, I was in a meeting for the last two days where the federal government is trying to figure out why people are not taking Medicaid. So what we ask for is any feedback as to what are barriers of why people are not taking Medicaid. Our administrator has really put the focus on us to figure out, whether it’s prior authorizations, myths…that’s our biggest focus right now. JM: Is there any type of formula for how patients are distributed to managed care verses indemnity? How is that working out? Coleen: For managed care verses fee for service? JM: Right. Coleen: I’ll have to get you what the actual numbers are. I do believe that the majority of them are going into the Managed care system because of the dynamics of the state. They’re going into urban Washoe, or urban Las Vegas, and well the last numbers I saw, that’s what
-
5
they were. I would have to get you those specific numbers, but that’s what the projections were because Fee for Service would be the (rural). They are falling into the newly eligible calculation which is going into managed care. They are not coming into Fee for Service. JM: In Managed care, there are panels. Is the problem recruiting into those panels? Coleen: What we are finding is that it doesn’t matter whether you are cash patient, if you are Managed care, fee for service, Medicare. We have a stress on our entire healthcare system right now. Honestly, our own employee system is having a hard time finding doctors right now. Everyone has a long wait list right now. It’s not just Medicaid, but my issue is to be concerned with anything we can do to reduce any type of barriers that are out there. So one of our largest focuses right now is to make sure that managed care and fee for service are as streamlined as possible, so Beth and Carl took on a very large project and they are trying to make sure that, for example, our PDLs looked similar, so when a physician looks at it, it looks somewhat seamless. So we’re looking at even those types of minute little things to make sure that we are streamlined. But yes. They are going primarily into managed care.
5. Presentations:
a. (Carl hands out packet to board members) This is a late addition that we’ve added here, so I apologize for not getting it to you guys sooner for you to review it. This is due September 30, 2014 to CMS Since this is the last meeting before that date, we scrambled to get this put together. Standard answers, very similar to what it was last year. I think the numbers that we’ll call out that are different that I think are improving are like the generic trend. So if you look, starting on page 7, see the number of generic claims. It’s on the very bottom and then it splits and carries over to page 8. Our generic dispense rate is 80.5%. And this is 2013. We’re pushing 82% now and this continues to climb as more generics are available. But still it only makes up 22% of our total expenditure, so that’s a huge difference. As more specialty products and biologics hit on the market, the brand names are really pushing the prices up.
Annual DUR Report Presentation – Carl Jeffery - Catamaran
PO: Carl, for that 80% is that for those products that have a generic available, or all dispensed? Carl: That’s all dispensed generics. Our rate of dispense when there’s a generic available is over 99 percent. There’s not too many and think most of those are on the preferred list. We have a little bit more work to do for cost savings and cost avoidance. These are numbers we’ve shared before with the DUR board. We’re just going to roll those into an annual report instead of the quarterly. CJ: On the early refill, what is the rationalization for utilizing 80% for one class of drug and 90% for another? Coleen: The DUR board actually made that recommendation back in 2007 or 2008. There was one tolerance level. At the very beginning when the controlled substance focus started. We started that. That’s when the recommendation happened because that’s what a lot of states do. They tighten it up on that side. Carl: CMS is doing a better job about getting these every year they update these reports and ask for different information, for example this year they are asking for e-prescribing trends. They’ve asked for these cost savings numbers for retro-DUR before and they are doing a better job of rolling these in and getting them back out to the public. We should be seeing standardization across the board.
-
6
PO: We need to approve this report for submission, so I’ll ask for a motion to approve it. LN: Motion to Approve. PO: We have a motion, do we have a second? DE: Second. PO: We have a motion and a second to approve the Preliminary Annual DUR Report for CMS. Any additional discussion? Voted: Unanimously to Approve.
b.
Public Comment: None
Discussion of proposed adoption of updated clinical prior authorization criteria for the medications used for acne – Carl Jeffery – Catamaran
Carl:
PO: There was some consideration for possibly utilizing the oral tretinoin products for just grade 3 or grade 4. Do you know if any of the other programs do anything like that?
The first page in there is chapter 1200 as it is now only one criteria is that they have to be under 21. So our proposed criteria is to add some criteria to those 22 and over, because we do receive periodic requests and I think there are adults with acne that can lead to infection and scarring, so we want to make sure we have the option available to treat these, so our proposal is that we add the criteria here that would 22 or over with a diagnosis of moderate to severe acne grade 2 or higher. I included a graph if you want to look at the utilization. Almost all of these are going to be patients that are 21 and under. But still the high ones are the Clindamycin, but they are appropriate levels after working through the topicals and then our oral tretinoin are very few. They are following the appropriate guidelines.
Carl: It’s across the board. Some other Medicaid programs don’t cover these at all because they see them as strictly cosmetic, other ones are pretty open to adults. The criteria that is proposed here is by the clinical call center who does handle other Medicaid programs. This is pretty standard to what they are accustomed to seeing. They’ve got such a strict REM’s set up for the oral tretinoins anymore, we’re just adding more hoops to jump through to get those medications. CL: You already have an overarching criteria that drugs can’t be used for cosmetic reasons the call center will be looking at this in addition to that, correct? PO: In essence we are looking at allowing those patients who fit the criteria of twenty two and over and with grade 2 or higher to include them in being eligible. JM: Is there any P&T guidance? The thing that really jumps out, other than that tretinoin compound is the benzoyl peroxide – Clindamycin combinations being 100 times more expensive than the individual components. Is there any sort of step type therapy? Carl: We do have a couple of classes, topical retinoid and combination agents. We’ve got Retin-A micro, Tazorac, and Ziana as preferred. JM: Not as much concerned about the Retin-A as the clindamycin. Carl: We’ve got the topical benzoyl peroxide antibiotic and combination products out there too. JM: Those are like dirt cheap and until they combine them and then all of the sudden… Carl: We’ve got the BenzaClin as one of our preferred agents. CL: If you wanted to make a clinical step, you guys could do that, because they are just doing it for an entire class. JM: The Clindamycin phosphate, for 921 Claims is $41,000, but for the BenzaClin, for 250, it’s twice that.
-
7
Carl: What you’re not seeing is the rebates coming back in. By having a preferred list, that’s the whole point of it. CL: The history of it is this. In many states, the reason the criteria is set under 21 is because it is looked at as cosmetic. Then states had to allow it for children because of the EPSDT rule. Then it was kind of pushed on throughout the years to where adults can have it. Now we’ve been pushed on and said “What do you do?” Some states allow it and some states stick with saying it’s cosmetic for adults. If you treat the acne early…you get pushed on enough and say “What do you want to do?” There are still those cases on the edge. So I think we have a protection in the regulations so it can’t be cosmetic, I won’t get in trouble on the regulatory side. If we can put something in there that says medically that over 21… PO: Is there going to be any kind of issue with the grading, the four grades of acne? Carl: Moderate to Severe means grade two or higher. We can be more aggressive to start. It’s always easier to be more aggressive then back off, then we can try to ramp up if we find out that utilization is going crazy. I think by the time they get moderate to severe grade acne, it’s to the point of fulminating cystic acne where it’s going to cause health issues. DE: That’s where grade two starts anyway. Carl: I believe so. PO: Cystic – I think that’s three. Would it be possible for grades 1 and 2 to have certain medications available, then three and four, other medications are available? Set it up that way as opposed to anything’s available? Carl: There are clinical guidelines from the American Academy of Pediatrics that defines mild to moderate to severe and also there are some dermatology guidelines. The American Academy of Dermatology also has some recommendations. DE: Could we possibly make an amendment to section B to make that grade 3 or higher as opposed to grade 2? Carl: Certainly. DE: I would think that by the time the patient reached 22, they would have already been on some sort of therapy and persisting after that age, it would be more severe therefore it would justify going to that. Whether they have come to and began a Medicaid program or had been in a Medicaid program, there would have been some treatment prior to that. What we’ve got is a revision to the proposed prior authorization criteria with the new addition being the recipient is 22 years of age or older, and has a diagnosis of grade 3 or higher. Prior authorization would be good for one year. Can I get a motion for these proposed criteria? PO: Can I get a motion for these revised proposed criteria, with the addition being the recipient is 22 or older and a diagnosis of grade 3 or higher of acne. The prior authorization would be good for one year? DE: So moved. JM: Second. PO: We have a motion and a second. Any further discussion? None. All those in favor of the revised proposed prior authorization criteria Voted: Unanimously to Approve. Motion carries.
c.
Clinical review – Xolair – Carl Jeffery – Catamaran
Public Comment: None
-
8
Carl Jeffery – Catamaran - Proposed addition for treatment of the urticaria as a new indication for this product. No changes to the actual treatment of asthma, just the addition of the urticaria. I did look into other treatments with H2 blockers for treatment of urticaria. It’s really not indicated for that, but they’ve done some studies and a lot of studies are really old and not well controlled. They weren’t blinded or anything. A lot of them were done with hydroxyzine. They think it had more to do with the cimetidine boosting the effects of the hydroxyzine, than the cimetidine having an effect itself. It’s really not that much of an impact. But still the criteria is to have the H1s first, oral antihistamines first then go on to the two. DE: This would still be a relatively limited access anyway. Even using Xolair, even for the asthma. Carl: We average in the low 20’s the number of people who are on this. PO: Do you recall what the rationalization was for the prior authorization being 3 months? Would it make it easier on the call center if it was one year? Carl: Yes. It would mean fewer calls. DE: What I don’t recall of the top of my head is where it says chronic idiopathic urticaria I don’t remember the underlying passage of what is causing it. It doesn’t make sense. By the virtue of saying chronic idiopathic, it would make sense to say the one year approval time as opposed to three months if it’s going to be an ongoing process. But I can’t recall what would stimulate this, if there was any seasonal variability with it. Carl: I’m not familiar enough with it either. DE: I like the criteria though. CL: The first part of it wasn’t for someone who was chronic. DE: The first part was for persistent asthma that can flare up, but at the same time with chronic idiopathic urticaria…I’ve dispensed it for patients with asthma, but never for a patient with chronic idiopathic urticaria (CIU), so I’m not that familiar with that utilization of it. If I remember correctly, even when we were using the Xolair, the patient had to meet all of the criteria too. Plus it is limited as to who can prescribe it. Up here we see that it has to be prescribed by the pulmonologist, allergist, and immunologist. We’re leaving it pretty open down here in the CIU. Would we want to add the allergist, immunologist section and/or rheumatologist down there as opposed to leaving it for anyone to order because the criteria for Xolair is quite extensive? It has a black box warning. Would we want to add dermatologist, allergist, and immunologist down in the criteria part B in the ‘iii’ section, moved down one level? Put who can prescribe it in there like we’ve included up above. In addition we have that the recipient’s current weight must be recorded. I think that should be added to the CIU indication also because it’s weight based. Carl: Dosage is also dependent on pretreatment IGE results. PO: So we’ve revised the proposed prior authorization criteria, we’re not touching the indication for severe persistent asthma, What we’re looking at doing is adding the diagnosis of chronic idiopathic urticaria with the proposed criteria of the present here and adding that the prescriber must be either a pulmonologist, dermatologist, or a rheumatologist and recipient’s current weight must be recorded. Also extend the prior authorization period to one year. For both. Carl: For the chronic urticaria, it’s not weight based dosing. It’s just 150 or 300 mg dosing once every 4 weeks.
-
9
PO: How do they determine whether it’s for 150 or 300? [Drug information] says dosage of Xolair in CIU patients is not dependent on serum IGE level, or body weight. It just says 150 or 300, but doesn’t give any criteria. Not going to add the weight. Carl: Just to be clear, the motion is to add the specialist, dermatologist, pulmonologist, rheumatologist, the CIU indication, and to increase the prior authorization to 12 months. DE: I’ll move we accept this JM: Second PO: Motion and second. No further discussion, Advised Proposed prior authorization criteria for the use of Xolair for both the severe persistent asthma and chronic idiopathic urticaria, with 12 month approvals with prior authorization. Board: Voted unanimously – Aye PO: Motion carries.
d.
Clinical review – Ivacaftor
Public Comment: Lisa Borland – Medical Affairs with Vertex Pharmaceuticals – Addressing the committee in reference to Ivacaftor. It’s known commercially as Kalydeco. First and only available therapy that targets the underlying causes of cystic fibrosis. The underlying cause in a defect in what is called the CF Terra protein. CF terra protein primarily functions as a chloride ion channel. This is really important in regulating fluid and electrolytes across various epithelial tissues – the lung, the pancreas, and the digestive system. Estimated 30,000 persons with cystic fibrosis in the United States. According to the 2012 Cystic Fibrosis Foundation patient registry, there are an estimated 186 patients in the state of Nevada. Kalydeco is indicated for a very specific subset of the CF population. It was originally approved in January of 2012 for persons 6 years of age and older with a mutation known as G551D. That mutation is present in less than 4% of the overall CF population. In February of this year, the label was expanded to include 8 additional mutations. These 8 additional mutations account for less than 1% of the overall CF population. That indication was added for 6 and older for those 8 additional mutations. Should also add that it is not effective for those who have 2 copies of the 508 Dal mutation. That’s the most common CF causing mutation. The efficacy of Kalydeco in persons with the G551D mutation was supported by two phase 3 clinical trials – one in persons 12 years of age and older, the other in patients 6-11. In both those studies there was a statistically significant improvement in lung function as measured by percent predicted FEV-1. That was assessed at 24 weeks. The treatment effect was 10.6 in the adolescent population and 12.5% in the pediatric population. Those levels of lung improvement were sustained through 48 weeks of therapy. Those were seen regardless of age, sex, level of disease severity, or geographic location. Patients treated with Kalydeco also saw improvements in weight. In both the adolescent and adult population there was a decrease in risk of pulmonary exacerbations, as well as improvement in patient’s respiratory symptoms. The study evaluating and supporting the efficacy for the 8 additional mutations, for which Kalydeco recently gained approval. In the smaller study, because those mutations are very rare, 39 patients, it was an 8 week cross over study. Those patients responded very similarly as the G551D population. So an improvement in percent predicted FEV-1, 10.7%, we didn’t see the reduction in risk of pulmonary exacerbations, because the study was only 8 weeks and was too short, but an improvement in MMI and patient reported respiratory symptoms. The safety profile is really based on the three original registration
-
10
studies. The discontinuation rate due to adverse events; in the Kalydeco treated patient, it was 2%, that’s compared to 5% in the placebo treated patients. The serious adverse events that occurred more commonly with Kalydeco than with placebo, whether or not they were determined to be drug related by the investigator, were increased liver enzymes, abdominal pain, and hypoglycemia. The small study - safety profile was very similar to what was seen in the G551 population. DE: This basically improves quality of life, but about longevity? Lisa Borland: The therapy has been on the market for two years, so there isn’t enough information to prove its effect on survival. We do have modeling data that suggests that, based on the improvement in just FEV-1. DE: With the patient being required to be 6 years of age or older, were tests not done on anyone younger than that? Or are there possible studies to be done on younger patients? Lisa Borland: The dose is the same in those 6-11 as in those 12 and older. The pill is about the size of a large multi vitamin. The pediatric patients just can’t take those. The pediatric patients have not been evaluated yet and it would require a different formulation. As of now, though it’s outside of the labeled indication, a pediatric study has been conducted in 2-5 year olds with a different formulation. DE: It’s probably a “Do not crush” then. Lisa Borland: I don’t know that the formulation has been released publically, but it is not a large multi vitamin. It’s a pediatric formulation. DE: In the studies do you also see a decrease in hospitalizations? Lisa Borland: In the phase 3 studies, particularly in the adolescent and the adult population, we didn’t see very many pulmonary exacerbations in the pediatric patients, in general. Lung function doesn’t start to decline until adolescence. Pediatric patients have healthier lungs. What we saw with hospitalization was a tertiary endpoint in the adolescent and adult population. I didn’t see a significantly decreased rate of hospitalizations themselves, but in the duration of the hospitalizations and duration of IV antibiotics, and the duration of those pulmonary exacerbations, when they occurred, and how they were treated, but not the numbers or the even rate. DE: With this onboard, were there any issues with the patients, if there were a hospitalization, or even outpatient, were they still able to use the inhaled antibiotics, or did it always require, if they had exacerbation, hospitalization where they had to have IV antibiotics as opposed to inhaled or oral. Lisa Borland: There’s no standard definition of pulmonary exacerbation. The way that they were evaluated or defined in clinical trials was 4 of 12 sinopulmonary symptoms and either a change in antibiotics, or an addition of an antibiotic. It wasn’t necessarily related to IV antibiotics. PO: So what we have in front of us is the proposed criteria, amended from what we did have to include the new mutations, as well as the inclusion of the 6 years of age or older criteria. Motion to accept and seconded. No further discussion DE: Motion to accept LN: Second Board: Voted Unanimously - Aye PO: Motion carries.
-
11
e.
PO: We have the previous criteria that was last reviewed in January of 2008. No proposed changes. Just time to take a look at the criteria for review. Call for anyone in the public domain that wishes to speak.
Clinical review – Updated prior authorization criteria for those medications used to treat ADD/ADHD
Sandy Sierawsky – Pharmacist in Nevada – Pfizer/Medical Division: This was addressed in the April meeting, but one of the things that the state wanted to see changed was the removal of the DSM terminology. That’s what was discussed. The other issue I wanted to resurface is that it’s pretty restrictive criteria for those who are not psychiatrists. If you look at the data that IMS provides, prescriptions for long acting stimulants make up about 60% of treatment for ADHD. Out of that 28% is prescribed by psychiatrists. 72% is prescribed by pediatricians, primary care physicians, etc. Nationally, psychiatrists aren’t prescribing the bulk of these medications. The American Academy of Pediatrics require pediatricians to diagnose and treat ADHD. They provide guidelines for them to follow to identify causes, symptoms, vulnerabilities, etc. Nationally, pediatricians provide about 66% of all office visits for children in Medicaid. I feel that the criteria is too restrictive to allow for those healthcare providers to provide treatment. LN: Is this still being done like this? Where, when I’m writing a prescription, I’m still having to get a prior authorization even when putting down a diagnosis? Coleen: Top prescribers in Nevada are psychiatrists, not pediatricians. Sandy Sierawsky: Right because it’s too difficult for the pediatricians to write the prescription because the criteria doesn’t allow it. They probably just pass on the patients to a psychiatrist. Coleen: We’ve also talked about the overall behavioral health of the children. We still have a very high utilization of these medications in Nevada, if you look at the data. DE: The point of the criteria is to have a psychiatrist in the mix, so that the patient can be evaluated for need. This prevents a child being put on the medication just because there was a complaint from a teacher. Board discussion: Reviewed Prior Authorization form. How Nevada differs from other states in this matter is the requirement of follow up care. Patients must be seen during a certain timetable. How do we assure that people get appropriate treatment? Board discussion: Use of the DSM 4 – Updating policies. If the ICD-9 language can be taken out of the policy, (where it’s not applicable to the actual policy) it will be removed. If it is pertinent with ICD-9 and it needs to be updated with ICD-10, we cannot make that change because ICD-9 and ICD-10 cannot be run at the same time and it can’t be changed to ICD-10 until next October. Board: Board acknowledges the fact that they have reviewed the updated prior authorization criteria for those medications used to treat ADD/ADHD, but no changes will be made. Board: No action being taken.
f. Call for public representation: None
Clinical review – Prior authorization criteria for transdermal fentanyl system
Board discussion: Last review by the DUR Board was July 30th
, 2009. No proposed changes.
-
12
Discussion of criteria of using multiple long acting pain medications and limits set up by the criteria. Suggestion of eliminating item 1C from criteria. Need a better way to handle multiple drug prescriptions for pain, so that abuse can be stopped and doctors can actually prescribe what the patients need. Carl to bring this discussion back to the next meeting for review. Mentioning morphine equivalent dosing that is ok to move to transdermal fentanyl. Criteria stating the prescriber has checked the PMP. No action being taken to modify the criteria at this time.
g.
DUR Board Requested Reports
1. Top 10 Black Box Warning Medications – Being deferred until next meeting. Open to audience discussion.
2. Controlled Substance Utilization on Trials Report – Carl Jeffery – Same report as was presented during last meeting. Hydrocodone and Acetaminophen are the highest prescribed medications. 500 mg Acetaminophen is no longer available after January, so it’s not on the report. Pretty significant spike in drug utilization, but there has been an increase in Medicaid membership as a whole. Promethazine with Codeine has really dropped off. • Carl to bring criteria next meeting to discuss Lock-in program. Consider
amending criteria. 3. Psychotropic medication use in Children – Report filters diagnosis by age.
Appears that the adolescent population is spiking. Count of diagnosis by specialty. The program that pulls the reports doesn’t duplicate the numbers. The primary diagnosis is captured. If the child is on an additional medication for another diagnosis, that diagnosis is not captured on the report. The population of children on psychotropic medications is very high.
4. Pro-DUR edit on late refill correlation to ER visits – still pending. 5. Buprenorphine and Buprenorphine-naloxone use – 2 reports and the Board is
asked to return the color coded copies when finished in insure no potential HIPAA violations. Looking at continuity of care with these products. Reports show that the patients are very compliant in taking the medications, or at least getting them filled. Possible criteria for initial fill to limit the quantity for the first 30 days with the requirement of ongoing 30 day fills after the initial fill. Main concern is paying a dispensing fee each time. There are other states that limit the dispensing fee to once a month. Will evaluate how it is done in other states.
h. DUR Board Standard Report Carl presented drugs by diagnosis. Top 10 prescribed. Everything looks consistent. Hepatitis agents have moved up while Hemophilia has dropped off since the first quarter. Abilify is one of the top medications. Significant change in amount+ spent can be attributed to a few new members that require a very large dose of medication at a time. Abilify to go generic in 2015. Oxycontin should be going generic soon. Generics have been approved. Purdue has a competing product with Zohydro coming out.
-
13
Request: Tussionex report
Request: Albuterol or asthma medicines as a whole – breakdown of how patients are using the drug and how effective it is for treatment.
Retro DUR Report: Looking at A-typical antipsychotics in pediatric patients. If they are on 2 or more a-typicals outside of their approved age. Study is not finished. Hoping for feedback by next meeting. Possibility of going paperless discussed.
6. Date and Location of next meeting October 23, 2014, at the Best Western in Reno.
7. Adjournment Meeting Adjourned at 7:53PM
-
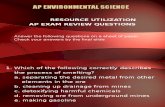
Sovaldi Utilization ‐ 2014
YearMonth Filled Drug Label Name
Count of Claims
Count of Members Qty Disp
Days Supply Paid Amt
201401 SOVALDI TAB 400MG 10 10 280 280 228,525.28$ 201402 SOVALDI TAB 400MG 16 16 448 448 428,475.00$ 201403 SOVALDI TAB 400MG 33 30 924 924 856,953.60$ 201404 SOVALDI TAB 400MG 52 45 1,456.00 1,456 1,428,245.20$ 201405 SOVALDI TAB 400MG 42 41 1,176.00 1,176 1,171,158.76$ 201406 SOVALDI TAB 400MG 62 55 1,736.00 1,736 1,628,888.36$ 201407 SOVALDI TAB 400MG 62 53 1,736.00 1,736 1,629,221.40$ 201408 SOVALDI TAB 400MG 63 56 1,764.00 1,764 1,544,886.16$ 201409 SOVALDI TAB 400MG 59 55 1,652.00 1,652 1,429,951.20$ 201410 SOVALDI TAB 400MG 38 38 1,064.00 1,064 1,000,449.72$ 201411 SOVALDI TAB 400MG 27 27 756 756 714,462.36$ 201412 SOVALDI TAB 400MG 34 28 952 952 942,976.84$
-
0
10
20
30
40
50
60
70
201401 201402 201403 201404 201405 201406 201407 201408 201409 201410 201411 201412
Count of Sovaldi Claims
-
Page 1 of 1
Copyright 2015 • Completed on 01/13/2015
DIVISION OF HEALTH CARE FINANCING AND POLICY NEVADA MEDICAID
DRUG USE REVIEW (DUR) BOARD PROPOSED PRIOR AUTHORIZATION CRITERIA
Sovaldi (Sofosbuvir)
No Changes Proposed at this time.
-
APPENDIX A – Coverage and Limitations
DIVISION OF HEALTH CARE FINANCING AND POLICY
MEDICAID SERVICES MANUAL
January 1, 2015 PRESCRIBED DRUGS Appendix A Page 76
VV.
1. Recipients with a diagnosis of Chronic Hepatitis C Genotype 1 infection and combination therapy with ribavirin.
Sovaldi® (sofosbuvir)
Therapeutic Class: Anti-Hepatitis Agents-Polymerase Inhibitor AgentsLast Review by the DUR Board: April 24, 2014
Sovaldi® (sofosbuvir) is subject to prior authorization and quantity limitations based on the Application of Standards in Section 1927 of the Social Security Act and/or approved by the DUR Board. Refer to the Nevada Medicaid and Check Up Pharmacy Manual for specific quantity limits.
1. Coverage and Limitations:
Approval for Sovaldi® (sofosbuvir) for mono-infected or HCV/HIV-1 co-infectedrecipients will be given if the following criteria are met and documented:
a. The recipient has a diagnosis of chronic hepatitis C Genotype 1 infection; and the recipient will be treated in combination with peginterferon alfa and ribavirin or, if the recipient is ineligible to receive peginterferon alfa, in combination with ribavirin; or
b. The recipient has a diagnosis of Chronic Hepatitis C Genotype 2 or 3 Infection; and the recipient will be treated in combination with ribavirin; or
c. The recipient has a diagnosis of Chronic Hepatitis C Genotype 4 Infection; and the recipient will be treated in combination with peginterferon alfa and ribavirin; or
d. The recipient has a diagnosis of Chronic Hepatitis C Genotype 1, 2, 3, or 4 infection; and the recipient has a diagnosis of hepatocellular carcinoma and is awaiting a liver transplant; and the recipient will be treated in combination with ribavirin.
2. Prior Authorization Guidelines:
a. Prior Authorization approval will be for 12 weeks for ALL of the following:
1. Recipients with a diagnosis of Chronic Hepatitis C Genotype 1 infection and combination therapy with peginterferon alfa and ribavirin.
2. Recipients with a diagnosis of Chronic Hepatitis C Genotype 2 infection and combination therapy with ribavirin.
b. Prior Authorization approval will be for 24 weeks for all of the following:
-
APPENDIX A – Coverage and Limitations
DIVISION OF HEALTH CARE FINANCING AND POLICY
MEDICAID SERVICES MANUAL
January 1, 2015 PRESCRIBED DRUGS Appendix A Page 77
2. Recipient with a diagnosis of Chronic Hepatitis C Genotype 3 infection and combination therapy with ribavirin.
c. Prior Authorization approval will be for up to 48 weeks or until liver transplantation for recipients with a diagnosis of hepatocellular carcinoma and is awaiting a liver transplant combination therapy with ribavirin.
d. Prior Authorizations will be renewed in 12 week intervals based on genotype.
e. Prior Authorization forms are available at: http://www.medicaid.nv.gov/providers/rx/rxforms.aspx
-
Page 1 of 3
Copyright 2014 • Review Completed on 07/01/2014
Therapeutic Class Overview Hepatitis C Polymerase Inhibitors
Therapeutic Class • Overview/Summary: Sovaldi® (sofosbuvir) and Harvoni® (ledipasvir/sofosbuvir) are once-daily
nucleotide analog inhibitors of hepatitis C virus (HCV) nonstructural protein 5B (sofosbuvir) and 5A (ledipasvir) ribonucleic acid (RNA) polymerase, which is essential for viral replication of HCV.1,2 The efficacy of sofosbuvir has been established in patients with HCV genotype 1, 2, 3 or 4 infection, including those with hepatocellular carcinoma meeting Milan criteria (awaiting liver transplantation) and those with HCV/human immunodeficiency virus-1 co-infection.1 Ledipasvir/sofosbuvir has been proven safe and effective only in genotype 1 infection.1,2
• Several treatment guidelines were recently updated to include recommendations on the use of sofosbuvir in the treatment of HCV infection.3-6 The consensus guidelines from the American Association for the Study of Liver Diseases (AASLD) and the Infectious Diseases Society of America (IDSA) prefer sofosbuvir-based combination therapy for most patients with chronic HCV genotype 1 through 6 infection. Telaprevir- and boceprevir-containing regimens are considered inferior to the preferred and alternative regimens and are no longer recommended for the treatment of HCV genotype 1 infection.3
Table 1. Current Medications Available in Therapeutic Class1 Generic
(Trade Name) Food and Drug Administration Approved
Indications Dosage
Form/Strength Generic
Availability Sofosbuvir (Sovaldi®)
Treatment of chronic HCV genotype 1 infection, including HCV/HIV-1 co-infection, in combination with peginterferon alfa and ribavirin; treatment of chronic HCV genotype 1 infection, including HCV/HIV-1 co-infection, in combination with ribavirin alone (without peginterferon alfa) in patients who are ineligible to receive an interferon-based regimen; treatment of chronic HCV genotype 4 infection, including HCV/HIV-1 co-infection, in combination with peginterferon alfa and ribavirin; treatment of chronic HCV genotype 2 or 3 infection, including HCV/HIV-1 co-infection, in combination with ribavirin; prevention of post-transplant HCV reinfection in combination with ribavirin in patients with hepatocellular carcinoma meeting Milan criteria (awaiting liver transplantation), including patients with HCV/HIV-1 co-infection
Tablet: 400 mg
-
Ledipasvir/ sofosbuvir
Treatment of chronic HCV genotype 1 infection in adults
Tablet: 90/400 mg
-
HCV=hepatitis C virus, HIV=human immunodeficiency virus Evidence-based Medicine • The Food and Drug Administration (FDA) approval of the polymerase inhibitor sofosbuvir was based
on the results of six clinical trials consisting of 1,947 patients who were treatment-naive or had not responded to previous treatment with peginterferon alfa and ribavirin (treatment-experienced), including patients with hepatitis C virus (HCV) and human immunodeficiency virus co-infection. In addition, sofosbuvir was effective in patients who were not eligible for an interferon-based treatment regimen and in patients with hepatocellular carcinoma awaiting liver transplantation, addressing unmet medical needs in these populations.1,7-9
-
Therapeutic Class Overview: hepatitis C polymerase inhibitors
Page 2 of 3
Copyright 2014 • Review Completed on 07/01/2014
• The addition of sofosbuvir to standard therapy (i.e., ribavirin or peginterferon alfa and ribavirin) resulted in significantly higher sustained virologic response rates compared to standard therapy alone in adults with chronic HCV genotype 1, 2, 3 and 4 infections.1,6-8
• The FDA approval of Harvoni® (ledipasvir/sofosbuvir) was based on the results of three phase III trials (N=1,518) in HCV mono-infected subjects with genotype 1 infection with compensated liver disease. All three phase III trials evaluated efficacy of ledipasvir 90 mg/sofosbuvir 400 mg fixed-dose tablet administered once daily with or without ribavirin. Treatment duration was fixed in each trial and was not guided by subjects’ HCV RNA levels. Sustained virologic response (SVR) was the primary endpoint and was defined as HCV RNA 95% of the patients across the three trials. This included patients that were treatment-naïve and –experienced and patients who both had and did not have cirrhosis.2,10-12
• Treatment with Ledipasvir/sofosbuvir for eight weeks was noninferior to both the 8-week ledipasvir/sofosbuvir + ribavirin treatment arm (treatment difference 0.9%; 95% CI, -3.9 to 5.7%) and the 12-week ledipasvir/sofosbuvir treatment arm (treatment difference -1.4%; 95% CI, -6.4 to 3.6%).11
• The most commonly reported adverse events in clinical studies of sofosbuvir and ribavirin were fatigue and headache. In patients treated with sofosbuvir, ribavirin and peginterferon alfa, the most commonly reported adverse events included fatigue, headache, nausea, insomnia, and anemia. Adverse effects for Ledipasvir/sofosbuvir are similar to sofosbuvir alone.1,2,7-12
Key Points within the Medication Class • According to Current Clinical Guidelines:3-6
o The most efficacious therapy for the treatment of hepatitis C virus (HCV) genotype 1 through 6 is the use of sofosbuvir-based combination therapy.
Simeprevir, peginterferon alfa, and ribavirin triple therapy regimen is generally recommended as an alternative, rather than a preferred regimen.
The use of sofosbuvir plus simeprevir (with or without ribavirin) off-label regimen is recommended in genotype 1 HCV infected patients who are either peginterferon alfa ineligible, prior null or partial responders to peginterferon alfa and ribavirin dual therapy, or liver transplant recipients.
In the treatment of HCV genotype 1 infection, telaprevir- and boceprevir-containing regimens are considered inferior to the preferred and alternative regimens and are either no longer recommended or are reserved for patients who are not candidates for the preferred and alternative regimens.
No one peginterferon alfa or ribavirin product is preferred or recommended over another.
• Other Key Facts: o Sofosbuvir is available as a 400 mg tablet and is dosed 400 mg once daily.1 o Ledipasvir/sofosbuvir is available as a 90/400 mg tablet and is also dosed once dialy.2 o The standard drug regimen for chronic hepatitis C requires 24 to 48 weeks of treatment, with
self-injections of peginterferon alfa which is associated with a number of side effects including nausea, mood swings and severe flu-like symptoms. Sofosbuvir combination therapy shortens the treatment duration to only 12 week in genotype 1, 2 and 4 HCV infections and offers an interferon-free regimen in genotype 2 and 3 HCV infections.1,3
o Sofosbuvir is a substrate of P-glycoprotein (P-gp). Thus, coadministration of potent P-gp inducers such as rifampin and St. John’s wort should be avoided. Nevertheless, there are fewer drug interactions with sofosbuvir compared to the HCV protease inhibitors.1,2,15-17
o Compared to combination therapy with HCV protease inhibitors for the treatment of genotype 1 HCV infection, sofosbuvir combination therapy offers potential for improved efficacy, shorter duration of treatment that is not response-guided, no viral resistance, favorable safety profile, reduced pill burden, and fewer drug-drug interactions (no CYP450 hepatic metabolism).1,13-15
-
Therapeutic Class Overview: hepatitis C polymerase inhibitors
Page 3 of 3
Copyright 2014 • Review Completed on 07/01/2014
References 1. Sovaldi® [package insert on the internet]. Foster City (CA): Gilead Sciences, Inc.; 2013 Dec. 2. Harvoni® [package insert]. Foster City (CA): Gilead Sciences, Inc.; 2014 Oct. 3. American Association for the Study of Liver Diseases (AASLD), Infectious Diseases Society of America (IDSA), International
Antiviral Society-USA (IAS-USA). Recommendations for testing, managing, and treating hepatitis C [guideline on the Internet]. Alexandria (VA): AASLD/IDSA/IAS-USA 2014 Apr [cited 2014 Nov 11]. Available at: http://www.hcvguidelines.org.
4. European Association for the Study of the Liver (EASL): Treatment of Hepatitis [guideline on the Internet]. Geneva (Switzerland): EASL 2014 Apr [cited 2014 Nov 11]. Available at: http://files.easl.eu/easl-recommendations-on-treatment-of-hepatitis-C.pdf.
5. Department of Veteran Affairs National Hepatitis C Resource Center Program and the Office of Public Health. Chronic hepatitis C Virus (HCV) infection: Treatment considerations [guideline on the Internet]. Washington (DC): VA 2014 May [cited 2014 Nov 11]. Available at: http://www.hepatitis.va.gov/pdf/2014hcv.pdf.
6. World Health Organization (WHO). Guidelines for the screening, care and treatment of persons with hepatitis C infection [guideline on the Internet]. Geneva (Switzerland): WHO 2014 Apr [cited 2014 Nov 11]. Available at: http://www.who.int/hiv/pub/hepatitis/hepatitis-c-guidelines/en/.
7. Lawitz E, Mangia A, Wyles D, Rodriguez-Torres M, Hassanein T, Gordon SC, et al. Sofosbuvir for previously untreated chronic hepatitis C infection. N Engl J Med. 2013 May 16;368(20):1878-87.
8. Jacobson IM, Gordon SC, Kowdley KV, Yoshida EM, Rodriguez-Torres M, Sulkowski MS, et al. Sofosbuvir for hepatitis C genotype 2 or 3 in patients without treatment options. N Engl J Med. 2013 May 16;368(20):1867-77.
9. Zeuzem S, Dusheiko GM, Salupere R, Mangia A, Flisiak R, Hyland RH, et al. Sofosbuvir and ribavirin in HCV genotypes 2 and 3. N Engl J Med. 2014 May 22;370(21):1993-2001.
10. Afdhal N, Zeuzem S, Kwo P, Chojkier M, Gitlin N, Puoti M, et al. Ledipasvir and sofosbuvir for untreated HCV genotype 1 infection. N Engl J Med. 2014 May 15;370(20):1889-98.
11. Kowdley KV, Gordon SC, Reddy KR, Rossaro L, Bernstein DE, Lawitz E, et al. Ledipasvir and sofosbuvir for 8 or 12 weeks for chronic HCV without cirrhosis. N Engl J Med. 2014 May 15;370(20):1879-88.
12. Afdhal N, Reddy KR, Nelson DR, Lawitz E, Gordon SC, Schiff E, et al. Ledipasvir and sofosbuvir for previously treated HCV genotype 1 infection. N Engl J Med. 2014 Apr 17;370(16):1483-93.
13. Victrelis® [package insert]. Whitehouse Station (NJ): Merck & Co., Inc.; 2014 Apr. 14. Incivek® [package insert]. Cambridge (MA): Vertex Pharmaceuticals Incorporated; 2013 Oct. 15. Olysio® [package insert]. Titusville (NJ): Janssen Therapeutics; 2013 Nov.
-
Page 1 of 34
Copyright 2014 • Review Completed on 11/17/2014
Therapeutic Class Review Hepatitis C Polymerase Inhibitors
Overview/Summary The hepatitis C polymerase inhibitors include sofosbuvir (Sovaldi®) alone and the combination product ledipasvir/sofosbuvir (Harvoni®) which are used for the treatment of chronic hepatitis C infection.1,2 The hepatitis C virus (HCV) is an enveloped ribonucleic acid virus that is transmitted through exposure with infected blood. It causes chronic infection in 70 to 85% of infected persons and the Centers for Disease Control and Prevention estimates 3.2 million persons are chronically infected. Chronic HCV infection can lead to the development of active liver disease, and accounts for up to 40% of all patients undergoing liver transplantation.3,4 There are seven genotypes of HCV (genotypes 1 to 7), with genotype 1 being the most common in the United States, followed by genotypes 2 and 3.4,5 The goal of hepatitis C treatment is HCV eradication in order to prevent complications and death. Genotyping is helpful in the clinical management of patients with hepatitis C for determining the choice of therapy. Assessment of liver disease severity is also recommended for predicting prognosis and determining the timing of therapy.6,7 Due to the slow evolution of chronic infection, it is difficult to demonstrate if treatment prevents complications of liver disease; therefore, response to treatment is defined by surrogate virological parameters. Sustained virologic response (SVR), defined as the absence of HCV ribonucleic acid (RNA) 24 weeks following discontinuation of treatment, has historically been the most important primary endpoint in clinical trials. Recently, SVR 12 (undetectable HCV RNA 12 weeks after the end of therapy) has also been accepted as a primary endpoint for regulatory approval in the US due to concordance with SVR 24.6 Prior to the availability of direct-acting antiviral agents, combination of peginterferon alfa and ribavirin has been the standard of care for the treatment of chronic hepatitis C.4-12 The other direct-acting antiviral agents include the nonstructural protein 3 protease inhibitors boceprevir, telaprevir and simeprevir.13-15 Several other direct-acting antiviral agents are in the final stages of development that aim to improve efficacy, ease of administration, tolerability and patient adherence, as well as to shorten treatment duration.6 The consensus guidelines from the American Association for the Study of Liver Diseases (AASLD) and the Infectious Diseases Society of America (IDSA) give preference to sofosbuvir-based combination therapy for most patients with chronic HCV genotype 1 through 6 infections. The choice of treatment regimen is primarily determined by HCV genotype, response to prior treatment (in any), the stage of liver disease, HCV viral load as well as patient’s ability to tolerate and be adherent treatment.1,2,7 For genotype 1 infection, telaprevir- and boceprevir-containing regimens are considered to be markedly inferior to the preferred and alternative regimens due to higher rates of serious adverse events, longer treatment duration, high pill burden, numerous drug-drug interactions, frequency of dosing, intensity of monitoring for continuation and stopping of therapy, and dietary requirements.7 Treatment guidelines do not give preference to one specific peginterferon alfa or ribavirin product over another.4-12
Sofosbuvir (Sovaldi®) is a nucleotide analog inhibitor of HCV nonstructural protein 5B RNA polymerase, which prevents viral replication of the HCV. The efficacy of sofosbuvir has been established in patients with HCV genotype 1, 2, 3 or 4 infection, including those with hepatocellular carcinoma meeting Milan criteria (awaiting liver transplantation) and those with HCV/human immunodeficiency virus (HIV)-1 co-infection. Prescribing information does not restrict sofosbuvir use to either treatment-naïve or experienced patients.1 The combination product, Harvoni®, adds ledipasvir to sofosbuvir. Ledipasvir is similar to sofosbuvir; however, it inhibits HCV nonstructural protein 5A.2 Specific Food and Drug Administration-approved indications are outlined in Table 2. Compared to combination therapy with HCV protease inhibitors for the treatment of HCV genotype 1 infection, sofosbuvir combination therapy offers potential for improved efficacy, shorter duration of treatment that is not response-guided, no viral resistance, favorable safety profile, reduced pill burden, and fewer drug-drug interactions (no CYP450 hepatic metabolism).1,2,13-15 Table 1. Medications Included Within Class Review
Generic Name (Trade name) Medication Class Generic Availability Sofosbuvir (Sovaldi®) Hepatitis C virus NS5B polymerase inhibitor -
Ledipasvir/sofosbuvir (Harvoni®) Hepatitis C virus HCV NS5A inhibitor/ NS5B polymerase inhibitor -
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 2 of 34
Copyright 2014 • Review Completed on 11/17/2014
Indications Table 2. Food and Drug Administration Approved Indications1,2,16
Indication Sofosbuvir Ledipasvir/ sofosbuvir Treatment of chronic HCV genotype 1 infection in adults Treatment of chronic HCV genotype 1 infection, including HCV/HIV-1 co-infection, in combination with peginterferon alfa and ribavirin; treatment in combination with ribavirin alone (without peginterferon alfa) can be considered for hepatitis C patients with genotype 1 infection who are ineligible to receive an interferon-based regimen
Treatment of chronic HCV genotype 4 infection, including HCV/HIV-1 co-infection, in combination with peginterferon alfa and ribavirin
Treatment of chronic HCV genotype 2 or 3 infection, including HCV/HIV-1 co-infection, in combination with ribavirin
Prevention of post-transplant HCV reinfection in combination with ribavirin in patients with hepatocellular carcinoma meeting Milan criteria (awaiting liver transplantation), including patients with HCV/HIV-1 co-infection
HCV=hepatitis C virus, HIV=human immunodeficiency virus Pharmacokinetics
Table 3. Pharmacokinetics1,2,16
Generic Name
Bioavailability (%)
Protein Binding (%)
Renal Excretion (%) Metabolism
Serum Half-Life (hours)
Sofosbuvir Not reported
61to 65
80
hydrolysis and phosphorylation
(active metabolite: GS-461203)
0.5
Ledipasvir/ sofosbuvir Not reported
>99.8/ 61 to 65
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 3 of 34
Copyright 2014 • Review Completed on 11/17/2014
While sofosbuvir was not specifically studied in treatment-experienced patients with HCV genotype 1 infection, the estimated response rate in patient who previously failed treatment with peginterferon alfa and ribavirin is 71% according to the prescribing information. This is based on the observed response rate in NEUTRINO subjects with multiple baseline factors associated with a lower response to interferon-based treatment (i.e., IL28B non-C/C alleles, HCV RNA >800,000 IU/mL and F3 to F4 fibrosis).1 FISSION (N=499) was a randomized, open-label noninferiority Phase 3 trial that compared treatment with sofosbuvir plus ribavirin for 12 weeks to peginterferon alfa plus ribavirin for 24 weeks in treatment-naïve patients with HCV genotype 2 or 3. A SVR12 was achieved in 67% of patients in both groups. Response rates in patients receiving sofosbuvir plus ribavirin were lower among patients with HCV genotype 3 than among those with HCV genotype 3 (56 vs 97%). Among patients with cirrhosis at baseline, 47% of patients receiving sofosbuvir plus ribavirin had a SVR compared to 38% of those receiving peginterferon alfa plus ribavirin.17 No resistance-associated mutations were detected among patients in either NEUTRINO or FISSION trials who received sofosbuvir and had a relapse after virological suppression; the precise reason for relapse is unknown.17 POSITRON (N=278) was a randomized, double-blinded Phase 3 trial that compared 12 weeks of treatment with sofosbuvir and ribavirin to placebo in patients with HCV genotype 2 or 3 who were interferon intolerant, ineligible or unwilling. A SVR was achieved in 78% of patients treated with sofosbuvir and ribavirin compared to 0% of those receiving placebo (P
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 4 of 34
Copyright 2014 • Review Completed on 11/17/2014
were receiving antiretroviral therapy for their HIV infection. The most common HIV treatment regimens included emtricitabine/tenofovir administered with efavirenz, atazanavir/ritonavir, darunavir/ritonavir or raltegravir.20 In this trial, SVR was achieved by 76% (87/114) of treatment-naïve patients with HCV genotype 1 receiving 24 weeks of therapy, 88% of treatment-naïve patients with HCV genotype 2 receiving 12 weeks of therapy, and 92% of treatment-experienced patients with HCV genotype 3 receiving 24 weeks of therapy. HIV rebound occurred in two patients (0.9%) on antiretroviral therapy.1 An unpublished open-label Phase 2 clinical trial evaluated sofosbuvir plus ribavirin in patients with HCV genotypes 1 to 6 and hepatocellular carcinoma prior to undergoing liver transplantation. Patients meeting the MILAN criteria (a single tumor ≤5 cm in diameter or ≤3 tumors each ≤3 cm in diameter and no extra hepatic manifestations of the cancer or evidence of vascular invasion of tumor) were treated for 24 to 48 weeks or until the time of liver transplantation. The post-transplant virologic response (pTVR) rate was 64% in the 36 evaluable patients who have reached the 12 week post-transplant time point. The safety profile of sofosbuvir and ribavirin was similar to that observed in Phase 3 clinical trials.1 An unpublished, ongoing, single-arm, open-label interferon-free Phase 2 pilot study is evaluating 24-week regimen of sofosbuvir plus ribavirin in naïve and treatment-experienced patients with recurrent HCV infection (any genotype) after liver transplantation. The interim SVR4 rate was 80.8% (21/26). There were no episodes of acute or chronic rejection. No drug interaction dose adjustments of immunosuppression have been required.20 LONESTAR-2 is an unpublished, ongoing open-label Phase 2 study evaluating a 12-week regimen of sofosbuvir 400 mg once daily added to peginterferon alfa (180 μg/week) and weight-based ribavirin twice daily (1,000 or 1,200 mg/day) among 47 treatment-experienced patients with HCV genotype 2 or 3 infection. In this study 55% of patients had cirrhosis. SVR12 occurred in 83% (20/24) of genotype 3 patients achieved and 96% (22/23) of HCV genotype 2 patients.22 The COSMOS trial is an unpublished, randomized, open-label, Phase 2a trial evaluating a once daily combination of simeprevir 400 mg and sofosbuvir 150 mg with and without ribavirin for 12 and 24 weeks in HCV genotype 1 patients. The four-point score METAVIR scale was used to quantify the degree of inflammation and fibrosis of the liver. Cohort 1 (N=80) included prior null responders with METAVIR scores F0 to F2 and Cohort 2 (N=87) included prior null responders and treatment-naïve patients with METAVIR scores F3 to F4.23 In the Cohort 1, SVR12 was achieved by 96% (26/27) of patients receiving a 12-week simeprevir added to sofosbuvir and ribavirin regimen and 93% (13/14) of patients receiving a 12-week simeprevir and sofosbuvir regimen without ribavirin. In the Cohort 2, SVR12 was achieved by 93% (25/27) of patients receiving a 12-week simeprevir added to sofosbuvir and ribavirin regimen and 93% (13/14) of patients receiving simeprevir and sofosbuvir regimen without ribavirin. Treatment was found to be generally safe and well tolerated. There was little to no benefit from adding ribavirin in this difficult to treat groups of hepatitis C patients and 12 week treatment provided similar clinical benefit to 24 week treatment.23-25
The FDA approval of Harvoni® (ledipasvir/sofosbuvir [LDV/SOF]) was based on the results of three phase III trials (N=1,518) in HCV mono-infected subjects with genotype 1 infection with compensated liver disease. All three phase III trials evaluated efficacy of ledipasvir 90 mg/sofosbuvir 400 mg fixed-dose tablet administered once daily with or without ribavirin. Treatment duration was fixed in each trial and was not guided by subjects’ HCV RNA levels. Sustained virologic response (SVR) was the primary endpoint and was defined as HCV RNA
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 5 of 34
Copyright 2014 • Review Completed on 11/17/2014
cirrhosis, gender, baseline HCV RNA level and IL28B status. The SVR rates in the four treatment groups ranged from 94 to 100% among subjects with cirrhosis, although the study was not designed or powered to formally compare the SVR rates among subjects with cirrhosis and those without cirrhosis.26 ION-3 (N=865) was a phase III, randomized, open-label study that evaluated eight weeks of LDV/SOF ± ribavirin and 12 weeks of LDV/SOF in treatment-naïve, non-cirrhotic subjects with HCV genotype 1 infection. The SVR rate was 94% with eight weeks of LDV/SOF, 93% with eight weeks of LDV/SOF+ ribavirin, and 95% with 12 weeks of LDV/SOF. Treatment with LDV/SOF for eight weeks was noninferior to both the 8-week LDV/SOF+ ribavirin treatment arm (treatment difference 0.9%; 95% CI, -3.9 to 5.7%) and the 12-week LDV/SOF treatment arm (treatment difference -1.4%; 95% CI, -6.4 to 3.6%).27 ION-2 (N=440) was a phase III, randomized, open-label study that evaluated 12 to 24 weeks of LDV/SOF ± ribavirin in genotype 1 subjects with or without cirrhosis who failed prior therapy with an interferon-based regimen, including those containing an HCV protease inhibitor. The SVR rates was 94% in the group that received 12 weeks of LDV/SOF; 96% in the group that received 12 weeks of LDV/SOF + ribavirin; 99% in the group that received 24 weeks of LDV/SOF; and 99% in the group that received 24 weeks of LDV/SOF+ ribavirin.28 Treatment with LDV/SOF± ribavirin for 12-weeks resulted in lower SVR rates in cirrhotic subjects (82 to 86%) compared to non-cirrhotic subjects (95 to 100%). In contrast, 24-week treatment with LDV/SOF± ribavirin resulted in comparable SVR rates amongst subjects with cirrhosis (100%) and without cirrhosis (99%). The difference in SVR rates among subjects with cirrhosis receiving 12 and 24 weeks of treatment was statistically significant (P=0.007).28 ELECTRON-2 (N=90) was an unpublished, open-label, phase II study evaluating 12-week regimen of LDV/SOF± ribavirin in treatment-naïve and treatment-experienced subjects with genotype 1 and in treatment-naïve genotype 3 subjects. Treatment with LDV/SOF + ribavirin in subjects with genotype 1 and prior SOF failure lead to an SVR12 of 100% (19/19). Treatment with LDV/SOF in subjects with genotype 1 and Child Pugh Class B cirrhosis led to an SVR12 of 65% (13/20). Treatment with LDV/SOF in treatment-naïve subjects with genotype 3 lead to an SVR12 of 64% (16/25) Treatment with LDV/SOF + ribavirin in treatment-naïve subjects with genotype 3 lead to an SVR12 of 100% (26/26).29 In the Synergy (N=14), treatment with LDV/SOF in subjects with genotype 1 and prior SOF failure lead to an SVR12 of 100% (14/14); of 14 subjects, seven had cirrhosis.30
Another unpublished study, ERADICATE (N=50), was an open-label phase II trial evaluating once-daily LDV+SOF for 12 weeks in treatment-naïve subjects with HCV genotype 1 infection (F0 to F3 liver fibrosis) and HIV co-infection. Cohort A included subjects who were not previously treated with HIV antiretrovirals who either had a stable CD4 count and HIV RNA 500 cells/mm3. Cohort B included subjects on HIV antiretrovirals for at least eight weeks, CD4 count >500 cells/mm3 and HCV RNA
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 6 of 34
Copyright 2014 • Review Completed on 11/17/2014
Table 4. Clinical Trials
Study and Drug Regimen Study Design and Demographics Sample Size and Study Duration
End Points Results
Treatment of Genotype 1, 2, 3, 4, 5, and 6 Chronic Hepatitis: Treatment-Naïve Patients Lavitz et al17 (NEUTRINO and FISSION) NEUTRINO: Sofosbuvir 400 mg once daily for 12 weeks and peginterferon alfa-2a 180 µg once weekly for 12 weeks and ribavirin 1,000 mg/day (weight
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 7 of 34
Copyright 2014 • Review Completed on 11/17/2014
Study and Drug Regimen Study Design and Demographics Sample Size and Study Duration
End Points Results
ribavirin 800 mg/day in two divided doses for 24 weeks
infection Secondary: Not reported
Afdhal et al26 (ION 1) Ledipasvir 90 mg and sofosbuvir 400 mg once daily for 12 weeks vs ledipasvir 90 mg and sofosbuvir 400 mg once daily for 12 weeks and ribavirin 1,000 mg (weight
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 8 of 34
Copyright 2014 • Review Completed on 11/17/2014
Study and Drug Regimen Study Design and Demographics Sample Size and Study Duration
End Points Results
weeks Kowdley et al27 (ION 3) Ledipasvir 90 mg and sofosbuvir 400 mg once daily for 8 weeks vs ledipasvir 90 mg and sofosbuvir 400 mg once daily for 8 weeks and ribavirin 1,000 mg (weight
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 9 of 34
Copyright 2014 • Review Completed on 11/17/2014
Study and Drug Regimen Study Design and Demographics Sample Size and Study Duration
End Points Results
and ribavirin 1,000 mg (weight
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 10 of 34
Copyright 2014 • Review Completed on 11/17/2014
Study and Drug Regimen Study Design and Demographics Sample Size and Study Duration
End Points Results
≥75 kg) for 12 weeks vs placebo FUSION: Sofosbuvir 400 mg once daily for 12 weeks and ribavirin 1,000 mg/day (weight
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 11 of 34
Copyright 2014 • Review Completed on 11/17/2014
Study and Drug Regimen Study Design and Demographics Sample Size and Study Duration
End Points Results
of response was 66% (78% with HCV genotype 2 infection and 61% with HCV genotype 3 infection) as compared to 76% among patients without cirrhosis (100% with HCV genotype 2 infection and 63% with HCV genotype 3 infection). Secondary: Not reported
Zeuzem et al19 (VALENCE) Sofosbuvir 400 mg once daily for 12 weeks and ribavirin 1,000 mg/day (weight
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 12 of 34
Copyright 2014 • Review Completed on 11/17/2014
Special Populations
Table 5. Special Populations14
Generic Name
Population and Precaution Elderly/ Children Renal Dysfunction
Hepatic Dysfunction
Pregnancy Category
Excreted in Breast Milk
Sofosbuvir No evidence of overall differences in safety or efficacy observed between elderly and younger adult patients. No dosage adjustment required in the elderly. Safety and efficacy in children
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 13 of 34
Copyright 2014 • Review Completed on 11/17/2014
Adverse Event(s) Sofosbuvir Ledipasvir/sofosbuvir Neutropenia
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 14 of 34
Copyright 2014 • Review Completed on 11/17/2014
Drug Interactions Table 7. Drug Interactions (Not All Inclusive)1,2,37
Generic Name
Interacting Medication or Disease Potential Result
Ledipasvir Antacids: aluminum and magnesium hydroxide
Coadministration may result in decreased plasma concentrations of ledipasvir. It is recommended to separate antacid and ledipasvir/sofosbuvir administration by four hours.
Ledipasvir H2-receptor antagonists: famotidine
H2-receptor antagonists may be administered simultaneously with or 12 hours apart from ledipasvir/sofosbuvir at a dose that does not exceed doses comparable to famotidine 40 mg twice daily.
Ledipasvir Proton-pump inhibitors: omeprazole
Proton-pump inhibitor doses comparable to omeprazole 20 mg or lower can be administered simultaneously with ledipasvir/sofosbuvir under fasted conditions.
Ledipasvir Antiarrhythmics: digoxin
Coadministration with digoxin may increase the concentration of digoxin. Monitor therapeutic concentration of digoxin during coadministration.
Ledipasvir, Sofosbuvir
Carbamazepine, oxcarbazepine, phenobarbital, phenytoin
Coadministration may result in decreased plasma concentrations of sofosbuvir and/or ledipasvir leading to loss of therapeutic effect of sofosbuvir. Coadministration is not recommended.
Ledipasvir, Sofosbuvir
Rifampin, rifabutin, rifapentine
Coadministration may result in decreased plasma concentrations of sofosbuvir leading to reduced therapeutic effect of sofosbuvir. Coadministration is not recommended.
Ledipasvir, Sofosbuvir
St. John's wort (Hypericum perforatum)
Coadministration may result in decreased plasma concentrations of sofosbuvir leading to reduced therapeutic effect of sofosbuvir. Coadministration is not recommended.
Ledipasvir, Sofosbuvir
Tipranavir/ritonavir Coadministration may result in decreased plasma concentrations of sofosbuvir and/or ledipasvir leading to reduced therapeutic effect of sofosbuvir. Coadministration is not recommended.
Dosage and Administration Table 8. Dosing and Administration1,2
Generic Name Adult Dose Pediatric Dose Availability
Sofosbuvir Treatment of chronic HCV genotype 1 infection, including HCV/HIV-1 co-infection, in combination with peginterferon alfa and ribavirin; treatment in combination with ribavirin alone (without peginterferon alfa) can be considered for hepatitis C patients with genotype 1 infection who are ineligible to receive an interferon-based regimen: Tablet: 400 mg once daily for 12 weeks (with peginterferon alfa and ribavirin) or 24 weeks (with ribavirin alone in patients ineligible to receive an interferon-based regimen) Treatment of chronic HCV genotype 4 infection, including HCV/HIV-1 co-infection, in combination with peginterferon alfa and ribavirin: Tablet: 400 mg once daily for 12 weeks
Safety and efficacy in children have not been established.
Tablet: 400 mg
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 15 of 34
Copyright 2014 • Review Completed on 11/17/2014
Generic Name Adult Dose Pediatric Dose Availability
Treatment of chronic HCV genotype 2 or 3 infection, including HCV/HIV-1 co-infection, in combination with ribavirin: Tablet: 400 mg once daily for 12 weeks (genotype 2) or 24 weeks (genotype 3) Prevention of post-transplant HCV reinfection in patients with hepatocellular carcinoma meeting Milan criteria (awaiting liver transplantation), including patients with HCV/HIV-1 co-infection: Tablet: 400 mg once daily for up to 48 weeks or until liver transplantation, whichever occurs first
Ledipasvir/ sofosbuvir
Treatment of chronic HCV genotype 1 infection: Tablet: 90/400 mg once daily for 12 weeks (treatment-naïve with or without cirrhosis* or treatment-experienced without cirrhosis) or 90/400 mg once daily for 24 weeks (treatment-experienced with cirrhosis).
Safety and efficacy in children have not been established.
Tablet: 90/400 mg
HCV=hepatitis C virus, HIV=human immunodeficiency virus *Ledipasvir/sofosbuvir may be considered for 8 weeks of therapy in treatment-naïve patients without cirrhosis who have pre-treatment HCV RNA less than 6 million IU/mL. Clinical Guidelines Table 9. Clinical Guidelines
Clinical Guideline Recommendation(s) American Association for the Study of Liver Diseases, Infectious Diseases Society of America, and International Antiviral Society-USA: Recommendations for testing, managing, and treating hepatitis C (2014)5
• Current consensus guidelines provide guidance regarding optimal hepatitis C virus (HCV) treatment assuming that the decision to treat has already been made; guidance regarding in whom and when to initiate treatment will be provided in a future consensus guideline update.
• It may be advisable to delay treatment for some patients with documented early fibrosis stage (F0 to 2), because waiting for future highly effective, pangenotypic, direct-acting antiviral combinations in interferon-free regimens may be prudent. Potential advantages of waiting to begin treatment will be provided in a future consensus guideline update.
• A regimen is classified as either "recommended" when it is favored for most patients or "alternative" when optimal in a particular subset of patients in that category. When a treatment is clearly inferior or is deemed harmful, it is classified as "not recommended."
• Recommendations for peginterferon alfa and ribavirin relapsers are the same as for treatment-naïve persons as described below.
• Interferon ineligible criteria: o Intolerance to interferon alfa. o Autoimmune hepatitis and other autoimmune disorders. o Hypersensitivity to peginterferon alfa or any of its components. o Decompensated hepatic disease. o Major uncontrolled depressive illness. o A baseline neutrophil count below 1,500/μL, a baseline platelet count
below 90,000/μL, or baseline hemoglobin below 10 g/dL. o A history of preexisting cardiac disease.
Treatment of HCV genotype 1 in treatment-naïve patients and relapsers with prior peginterferon alfa and ribavirin • Recommended treatments:
o Interferon eligible: sofosbuvir plus peginterferon alfa and ribavirin for
-
Therapeutic Class Review: hepatitis C polymerase inhibitors
Page 16 of 34
Copyright 2014 • Review Completed on 11/17/2014
Clinical Guideline Recommendation(s) 12 weeks.
o Interferon ineligible: sof