
Notice of Intended Action and Cease and Desist Order...Auditor Joe Kylman sent a letter to NEMA...
240
1 STATE OF MICHIGAN DEPARTMENT OF ATTORNEY GENERAL CORPORATE OVERSIGHT DIVISION In the Matter of the: AG No. 2018-0217889-A National Emergency Medicine Association and Kelly Herzog Respondents. _________________________________________________/ Notice of Intended Action and Cease and Desist Order To: National Emergency Medicine Association Kelly Herzog 500 Edgewood Road, Suite 105 P.O. Box 1039 Edgewood, MD 21040 [email protected] Registered Agent Registered Agent Solutions, Inc. 2285 S. Michigan Road Eaton Rapids, MI 48827 Bill Schuette, Attorney General of the State of Michigan, under Section 20(4) of the Charitable Organizations and Solicitations Act, MCL 400.271 et seq., notifies National Emergency Medicine Association (“NEMA”) and its President Kelly Herzog of his intention to bring a civil action against NEMA and Herzog in Ingham County Circuit Court, and orders NEMA and Herzog to cease and desist all unlawful solicitations as described below. Before bringing a civil action, the Attorney General will consider accepting an assurance of discontinuance or other appropriate settlement agreement.
Transcript of Notice of Intended Action and Cease and Desist Order...Auditor Joe Kylman sent a letter to NEMA...

1
STATE OF MICHIGAN DEPARTMENT OF ATTORNEY GENERAL
CORPORATE OVERSIGHT DIVISION
In the Matter of the: AG No. 2018-0217889-A National Emergency Medicine Association and Kelly Herzog
Respondents.
_________________________________________________/
Notice of Intended Action and Cease and Desist Order
To: National Emergency Medicine Association
Kelly Herzog 500 Edgewood Road, Suite 105 P.O. Box 1039 Edgewood, MD 21040 [email protected] Registered Agent Registered Agent Solutions, Inc. 2285 S. Michigan Road Eaton Rapids, MI 48827
Bill Schuette, Attorney General of the State of Michigan, under Section 20(4)
of the Charitable Organizations and Solicitations Act, MCL 400.271 et seq., notifies
National Emergency Medicine Association (“NEMA”) and its President Kelly Herzog
of his intention to bring a civil action against NEMA and Herzog in Ingham County
Circuit Court, and orders NEMA and Herzog to cease and desist all unlawful
solicitations as described below. Before bringing a civil action, the Attorney General
will consider accepting an assurance of discontinuance or other appropriate
settlement agreement.
2
I. Jurisdictional Allegations
1. Respondent National Emergency Medicine Association (“NEMA”) is a
Maryland-based nonprofit corporation with 501(c)(3) tax-exemption status.
Its address is 500 Edgewood Road, Suite 105, P.O. Box, 1039, Edgewood,
Maryland 21040. Its President is Kelly Herzog. Its Michigan-based resident
agent is Registered Agent Solutions, Inc., 2285 S. Michigan Road, Eaton
Rapids, MI 48827.
2. According to NEMA’s website, it incorporated in 1982: “The National
Emergency Medicine Association is a 501(c)(3) nonprofit organization
founded in 1982, committed to trauma prevention and the delivery of quality
medical services at each stage of trauma with and [sic] emphasis on first
response at the time of the emergency.” Exhibit A, Website Screenshot of
9/6/18. NEMA fundraises under the names National Heart Council, National
Stroke Council, National Alzheimer’s Council, and Kids do Matter.
3. In 1989, NEMA first registered to solicit in Michigan under Michigan’s
Charitable Organizations and Solicitations Act (“Solicitations Act”). NEMA is
registered under the Solicitations Act as # 9773.
4. As a registered charitable organization soliciting in Michigan, NEMA is a
person subject to the authority of the Attorney General under the
Solicitations Act. MCL 400.271 et seq.; MCL 400.272(a) and (e).
5. Respondent Kelly Herzog is a director of NEMA, its President, and its
highest paid employee. Exhibit B, NEMA 2016 Form 990, p. 7. Section 20(1)

3
of the Solicitations Act, MCL 400.290(1), allows the Attorney General to seek
relief against an officer or director of a registered charity or against “any
other person that directly engaged in, authorized, or was legally responsible
for the prohibited act or practice; or against any combination of those
persons.”
II. Background Facts
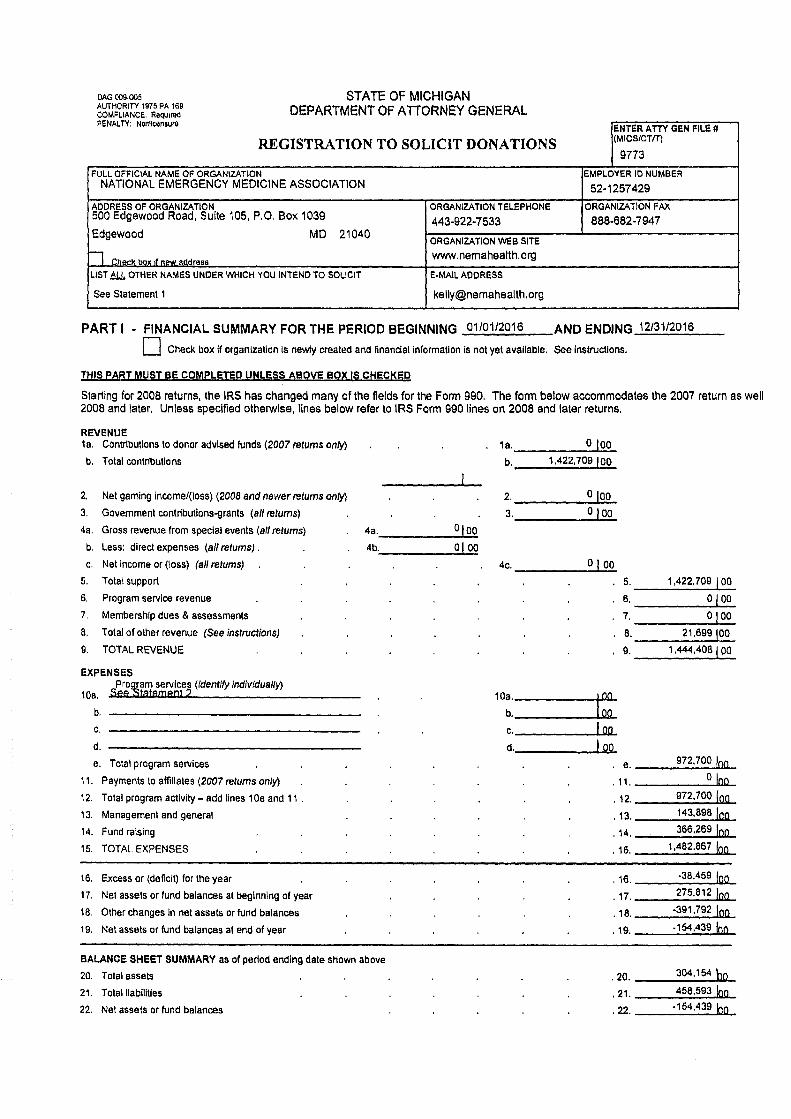
6. In 2017, the Attorney General’s Charitable Trust Section received NEMA’s
renewal registration form, including NEMA’s 2016 IRS Form 990 and
audited financial statements. Exhibit B.
7. NEMA’s 2016 Form 990 reported $1,422,709 in contributions received and
$1,482,867 in total expenses. Of these expenses, NEMA reported $364,772 in
fundraising, $143,898 in management and general, and $972,700 as program
service expenses. Exhibit B, pp. 1-2. NEMA’s program service expenses
resulted from two reported programs: (1) $8,675 for educating “the public on
physical and psychological health matters by using videos and internet;” and
(2) $964,025, including grants of $3,300, for providing “public health
educational info on first aid, heart, trauma, stroke prevention, alzheimers
disease, and emergency matters by mailing letters to the general public.” Id.
8. Of these reported $972,700 in program service expenses, $967,673 (or 99.5%)
resulted from joint cost allocations, an accounting method that, if certain
conditions are met, allows a charity to allocate a percentage of fundraising
costs to program services. Exhibit B, p. 9, lines 25(B) and 26(B). However, in

4
the Charitable Trust Section’s experience, charities that employ joint cost
allocations frequently don’t meet the necessary conditions or use an
unreasonable percentage allocation. In this way, such charities falsely
allocate fundraising expenses as program services, thereby minimizing their
reported fundraising expenses and increasing their program services and
making the charity appear more efficient than it is.1
9. Given the Charitable Trust Section’s experience regarding misuse of joint
cost allocations and the fact that 99.5% of NEMA’s charitable programs were
the result of joint cost allocations, on January 16, 2018, Charitable Trust
Auditor Joe Kylman sent a letter to NEMA President Kelly Herzog
questioning its joint cost allocation, requesting solicitation materials, and
requesting a schedule of NEMA’s $3,300 in grants made in 2016. Exhibit D,
1/16/18 Kylman Letter to Herzog.
10. Herzog responded for NEMA on March 20, 2018. Exhibit E, 3/20/18 Herzog
Letter to Kylman. NEMA’s response defended its joint cost allocations,
produced the requested solicitation materials, and listed its three charitable
grants, as follows:
a. “$200 to the Harford County, Maryland Chamber of Commerce to enable disabled and disadvantaged persons to attend the circus.”
1 In recognition of this potential problem, and to aid donors, the Charitable Trust Section’s online search feature at mi.gov/charitysearch breaks out joint cost allocations so donors can see the percentage of an organization’s program services that resulted during fundraising. The Attorney General’s website reports that $967,673 of NEMA’s program services were conducted during fundraising, representing 99.48% of all NEMA’s program services. See Exhibit C, 9/7/18 screenshot from mi.gov/charitysearch.

5
b. “$100 to Operation Support Our Troops for the purchase of sunscreen and other necessities for military personnel stationed overseas.”
c. “3,000 to Maryland Search and Rescue for the purchase/acquisition of
portable defibrillators, specialized backpacks for emergency medical service personnel and other first responders (ALS backpacks), special combat application (CAT) tourniquets, structural aluminum malleable (SAM) splints, first responder kits, and chemical warm packs.” Exhibit E, Response 4a.
11. NEMA’s response failed to satisfy the Charitable Trust Section’s concerns
regarding its activities and raised additional questions regarding its joint cost
allocations. Moreover, NEMA’s program activities (mostly educational
materials included within its solicitations) and its schedule of grants (just
three small grants of questionable purpose) appeared inconsistent with
NEMA’s solicitation materials, which made claims such as the following:
a. That NEMA’s “programs, educational materials and equipment grants” helped combat stroke; [Exhibit F.1, Mail package #7487 (dated 2/16/16)]
b. That NEMA raised “funds for the prevention of injury and illness by addressing health and social issues through education, applied research, technology, and equipment;” [Exhibit F.1, Mail package #7487 (dated 2/16/16)]
c. That NEMA had used past funds raised to “expand our grants for
stroke education and develop stroke prevention materials for individuals at risk.” [Exhibit F.2, Mail package #7578 (dated 5/5/16)]
d. That contributions to NEMA would “join in our effort to fight and win
the battle against heart disease” and “help us put an end to needless suffering.” [Exhibit F.3, Mail package #7411 NHC (dated 11/25/15)]
e. That contributions to NEMA would be used “to help end the tragedy of
Alzheimer’s Disease” and “will bring hope and happiness to many families struggling with this disease . . . even right there in [Michigan].” [Exhibit F.4, Mail package #7418 NAC (dated 12/1/15)]

6
f. That donations to NEMA would “continue to support our fight to end the tragedy of Alzheimer’s Disease” and “will bring hope to families struggling with the disease and help fund vital research to find a cure.” [Exhibit F.5, Mail package #7771 (4th quarter 2016)]
12. Of additional concern was the fact that a review of NEMA’s past IRS Form
990s showed that NEMA President Kelly Herzog, during years 2006 to 2016,
had earned total compensation and benefits of $1,786,826, an average of
$162,438 per year. Yet NEMA’s grants during those years averaged just
$14,521; and in five of the eleven years, NEMA made no grants or fewer than
$1,000 in grants.
13. On May 29, 2018, The Attorney General issued an investigative order to
NEMA further questioning NEMA’s joint cost allocations, requiring
production of additional solicitation materials and additional schedules of
grants, and requiring NEMA to identify any grants and program expenses
that corresponded to its various representations to donors. Exhibit G,
Investigative Order.
14. On August 16, 2018, Herzog responded for NEMA. With NEMA’s response,
the Attorney General now possessed all NEMA solicitation materials for the
years 2015 through 2017 and a complete list of NEMA grants for these years.
Exhibit H. 8/16/18 Herzog Response to Investigative Order.
A. NEMA’s Program Activities and Grants for 2015 to 2017
15. Before reviewing NEMA’s 2015 to 2017 solicitations, or NEMA’s response to
the Attorney General’s inquiries into specific NEMA solicitations for 2016,

7
it’s helpful to review NEMA’s reported program activities for the years 2015
to 2017.
16. 2015. In 2015, NEMA reported total program service expenses of $695,442,
all related to education of the public regarding health matters and including
grants of $650. Exhibit G, 2015 Form 990, p. 2. As with the 2016 Form 990
discussed above, nearly all NEMA’s program expenses—$694,792 of
$695,442, or 99.9%—were the result of dubious joint cost allocations.2
Regarding the $650 in grants, the Attorney General required NEMA to
produce a schedule of these grants. NEMA’s response states:
#2: In 2015, NEMA provided a grant to the Chamber of Commerce of Harford County, Maryland, in the amount of $200 to fund its yearly carnival for disabled children. The balance of $450 was recorded in error on NEMA’s books as grants. This amount should have been treated as amortization of the cost of gift software and should have been recorded as part of NEMA’s development costs. [Exhibit H]
In other words, even the reported grant of $650 overstated NEMA’s
charitable grants, which were limited to a single $200 grant to help
disabled children attend a carnival, and the purpose of this grant did
nothing to combat heart disease, stroke, or Alzheimer’s.
17. 2016. As discussed above, 99.5% of NEMA’s 2016 program activities came
from joint cost allocations for NEMA’s purported educational programs. In
2 NEMA’s August 16, 2018 response to the Attorney General’s Investigative Order advises that it will be amending its 2016 Form 990 to revise the joint cost allocation based on a review of mailing content rather than employee time. See Exhibit H, Response 19. Upon revision, the Attorney General expects that NEMA’s reported educational program service expenses will be sharply reduced. And as discussed below, the Attorney General believes NEMA does not meet the criteria to allocate any fundraising expenses as joint costs.

8
response to the Attorney General’s questions, NEMA has advised that it
intends to amend its 2016 Form 990, which will presumably result in a lower
allocation and lower program expenses. Exhibit H, Response 19. Apart from
NEMA’s educational activities, NEMA had just three grants for the year:
a. “$200 to the Harford County, Maryland Chamber of Commerce to enable disabled and disadvantaged persons to attend the circus.”
b. “$100 to Operation Support Our Troops for the purchase of sunscreen and other necessities for military personnel stationed overseas.”
c. 3,000 to Maryland Search and Rescue for the purchase of emergency
medical equipment. Exhibit E, Response 4a.
18. 2017. NEMA submitted its 2017 Form 990 in September 2018, i.e., following
its August response to the Attorney General’s investigative order. While
NEMA’s 2016 Form 990 allocated a smaller percentage of its fundraising
costs as program services (apparently responding to concerns raised in
correspondence from the Attorney General), NEMA’s program activities
again mostly resulted from its joint cost allocations. In 2017, NEMA reported
$1,812,105 in total expenses, including $1,391,882 as fundraising, $120,166
as management and general, and $300,057 as program services. Of these
$300,057 in program services, $289,478 (96.5%) resulted from joint cost
allocations; and NEMA’s reported programs were again all educational in
nature, and mostly resulted from its fundraising campaigns.
19. In 2017, NEMA reported on its Form 990 grants of $10,765. NEMA also
produced a schedule of these grants to the Attorney General, listing two and

9
totaling $10,465.36 (we’re unsure of the $300 discrepancy between the
schedule of grants and the 990):
a. $1,200 to Social Apostolate of Savannah, Georgia for 1 Philips HeadStart onsite AED; and
b. $9,265.36 to Memorial Health University Medical Center of Savannah, Georgia for 1 Mass Casualty Cart and all supplies. [Exhibit H, Response 8 attachment.]
20. In sum, NEMA’s charitable programs for the years 2015 to 2017 are its
purported educational programs, which are dependent on joint cost
allocations,3 and six grants totaling $13,965. Within these six grants were
two grants to attend the circus, one for sunscreen for troops, and three for
medical equipment. NEMA identified no recent research grants: NEMA
produced a list of grants going back to 1986, which identified 9 research
grants, but the most recent was in 1994—24 years ago. Nor did NEMA
identify any programs—other than the purportedly educational components
within its fundraising mailers, and its educational videos and information it
posts on the internet—that would combat or fight heart disease, stroke, or
Alzheimer’s. In other words, NEMA’s nearly exclusive charitable activity (the
value of which NEMA has for years falsely included or overstated on its
Forms 990), has been mailing sweepstakes and fundraising campaigns to the
public containing “educational” materials.
3 Later sections analyze the joint cost allocations and show that NEMA’s joint cost allocations were unjustified under the applicable criteria and, alternatively, excessive.

10
21. The next sections will look more closely at NEMA’s fundraising campaigns,
including their representations regarding NEMA’s activities—and whether
NEMA truly conducts these activities—and then will review the educational
materials NEMA includes within its fundraising campaigns.
B. NEMA’s Responses to the AG Regarding 2016 Solicitations
22. Within the Attorney General’s May 2018 investigative order, the Attorney
General questioned NEMA regarding specific representations NEMA made in
its 2016 solicitation materials. NEMA has made similar or identical
representations in its 2015 and 2017 solicitation materials—materials which
were received as part of NEMA’s response to the Attorney General’s
Investigative Order. The Attorney General’s questions, and NEMA’s
responses follow.
23. Mail packages #7487 (dated 2/16/16) and #7578 (dated 5/5/16) stated:
The Annual Fund Drive is our most important appeal of the year and your help is urgently needed now.
Over 100,000 Americans will die of stroke this year. Stroke (brain attack) is a leading cause of death and disability in adult Americans. We are winning the battles but have not yet won the war against stroke. Don’t let stroke disable or kill you or someone in your family. Follow the guidelines provided on the back of this letter. And, make a small gift so that others may live.
Our plans are in place for the programs, educational materials and equipment grants that are so vital to so many people – people in your local area- perhaps even someone in your own family.
With your past support Mr. Sampleperson, we have been able to expand our grants for stroke education and develop stroke prevention materials for individuals at risk.

11
Your 2016 Annual Fund gift is vital to our success in fighting stroke and so much more needs to be done.” [Exhibits G, F.1, and F.2 (emphasis added)]
a. The Attorney General asked: “For the years 2015 through present,
identify all NEMA programs, and the amount spent on such programs,
that combat stroke.” NEMA responded: “For 2015 to the present,
NEMA’s program, the National Stroke Council, combatted stroke via
the educational materials that were published and disseminated to the
public in connection with this program. During this period, NEMA
spent $11,751.75 in connection with the National Stroke Council.” In
other words, NEMA admitted that it has no programs to combat
stroke other than its educational materials, almost all of which are
mailed as part of fundraising campaigns.
b. The Attorney General asked: “For the years 2015 through present,
identify all NEMA equipment grants that combat stroke.” NEMA
responded:
NEMA typically does not make unsolicited grants in regard to its charitable programs and activities. NEMA relies on grant requests to identify those organizations in need of grant funds for purposes that advance NEMA’s charitable mission. From 2015 to the present, NEMA did not receive requests for grants for equipment that combat stokes [sic] and, for this reason, NEMA did not make grants that combat strokes during the above period. Previously, in 2002, NEMA made a grant in the amount of $61,232.90 to fun the purchase of equipment for rapid assessment and transient ischemic attack (“TIA”) for the Baltimore foundation of the University of Maryland that provides treatment and rehabilitation to stroke victims. (Emphasis added.)

12
In other words, NEMA admitted that it made no equipment
grants to combat strokes, and that its last such equipment grant
was in 2002—16 years ago.
c. The Attorney General asked: “For the years 2015 through present,
identify all Michigan residents and organizations that benefited from
NEMA programs or equipment grants.” NEMA responded:
From 2015 to the present, 47 residents of Michigan received educational and related materials from NEMA in connection with the National Stroke Council program. A copy of the list of recipients is attached. NEMA did not receive requests for equipment grants from organizations located in Michigan during the requested period. However, in previous years, grants were made to the following organizations. [NEMA then identified four grants, totaling about $18,000, in the years 1995, 2008, 2008, and 2012.]
d. In other words, NEMA has provided no equipment grants in
Michigan since 2012, and the benefit of its National Stroke Council
program is limited to the 47 Michigan residents that received
educational materials from NEMA, which presumably was part of a
NEMA fundraising campaign. (NEMA’s list of donors include an
amount next to each recipient of educational materials, suggesting
that each individual donated that amount to NEMA.)
e. In sum, NEMA told donors that donations would support “programs,
educational materials, and equipment grants” that could even support
people in the donors’ “local area,” but for years, NEMA has had no
programs to combat stroke, made no equipment grants to
combat stroke, and made no grants to individuals in Michigan;
13
and almost all of NEMA’s educational materials are included
within fundraising campaigns.
24. Mail packages #7487 (dated 2/16/16) and #7578 (dated 5/5/16) also included a
standard disclosure that NEMA included in many of its mailings, which
stated:
Through our mailings we raise the much needed funds for the prevention of injury and illness by addressing health and social issues through education, applied research, technology, and equipment. [Exhibits G, F.1, and F.2]
Similar language is also included on NEMA’s homepage at
www.nemahealth.org, which states under “Our Mission”: “Our mission is the
prevention of injury and illness by addressing health and social issues
through education, applied research, technology, and equipment.” Exhibit A,
Website Screenshot of 9/6/18. The Attorney General asked NEMA to identify
all instances of these activities.
a. “For the years 2015 through present, identify all NEMA funding of
applied research for the prevention of injury and illness.” NEMA
responded:
NEMA, as noted, typically does not make unsolicited grants in regard to its charitable programs and activities. NEMA relies on grants requests to identify those organizations in need of grant funds for purposes that advance NEMA’s charitable mission.
From 2015 to the present, NEMA did not receive requests for grants in regard to applied research to prevent injury and illness and, for this reason, NEMA did not fund applied research for the prevention of injury or illness during the above period. Previously, NEMA provided grants in 1993 in the amount of $13,000 to Jefferson Medical, located in Pennsylvania, for applied

14
focal cerebral ischemic II stroke research to prevent injury or illness. (Emphasis added).
In other words, NEMA did not make any applied research grants
during the period of its solicitations, nor has NEMA made an
applied research grant in twenty-five years.
b. “For the years 2015 through present, identify all NEMA funding of
technology for the prevention of injury and illness.” NEMA responded:
From 2015 to the present, NEMA did not receive requests in regard to technology to prevent injury and illness and, for this reason, NEMA did not fund technology for prevention of injury or illness during the above period. Previously, in 2002, NEMA provided grants to the University of Maryland in the amount of $61,232.90 for the purchase of technology equipment for rapid assessment and TIA research to prevent injury and illness. (Emphasis added.)
In other words, NEMA did not fund any technology for the
prevention of injury and illness during the period of its solicitations,
nor has NEMA funded such technology for sixteen years.
c. “For the years 2015 through present, identify all NEMA funding of
equipment for the prevention of injury and illness.” NEMA responded:
From 2015 to the present, NEMA did not receive requests for grants in regard to equipment to prevent injury and illness and, for this reason, NEMA did not fund equipment for prevention of injury or illness during the above period. Previously, in 1996, NEMA provided grants to the National Stroke Association in the amount of $5,000 for the purchase of equipment to permit EMS first responders to treat stroke victims to prevent or reduce injury and illness from strokes. (Emphasis added).
Again, NEMA has admitted that it did not perform the activity it told
donors, i.e., funding equipment for the prevention of injury or illness.

15
25. Mail packages #7487 (dated 2/16/16) and #7578 (dated 5/5/16) stated:
With your past support Mr. Sampleperson, we have been able to expand our grants for stroke education and develop stroke prevention materials for individuals at risk.
Your 2016 Annual Fund gift is vital to our success in fighting stroke and so much more needs to be done.
Please, won’t you help us continue to give the gift of life by making your 2016 Annual Fund gift today? Thank you, you are a lifesaver! [Exhibits G, F.1., and F.2 (emphasis added)]
a. The Attorney General asked NEMA to “identify all NEMA grants for
stroke education.” NEMA responded in a similar manner, explaining
that it doesn’t make unsolicited grants, hadn’t made any grants in
recent years, and that its most recent grants were in 1995. Exhibit H,
Response 7a.
b. The Attorney General next asked: “For the years 2015 through
present, explain how NEMA had ‘expand[ed]’ its grants for stroke
education compared to previous years.” NEMA responded:
From 2015 to the present, NEMA continued to provide educational materials to the public via solicitations and requests for information concerning stroke prevention and treatment. NEMA wanted to make grants and even expand its grant-making program for stroke education during these years. However, due to a failure to receive requests for grants for stroke education, NEMA, as noted, did not make grants for stroke education from 2015 to the present. [Exhibit H, Response 7b (emphasis added.]
In other words, despite telling donors that NEMA had “expand[ed]”
its grant programs for stroke education, NEMA had not only not
expanded its grant programs for stroke, NEMA had not made
any such grants since 1995.

16
26. Sweepstakes package #7411 National Heart Council (dated 11/25/15)
included a “winner announcement” regarding a $10,000 prize and stated:
When you send your reply and claim your prize, please send along a gift of $7, $10, or even $5 to join in our effort to fight and win the battle against heart disease. This is your chance to win a major prize and help us put an end to needless suffering. Please, your help is desperately needed. [Exhibits G and F.3 (emphasis added)]
The Attorney General asked: “For the years 2015 through present, identify
all NEMA expenditures ‘to fight and win the battle against heart disease.’ ”
NEMA responded, again citing the “valuable educational information” it
provides and listing all its grants since its founding in 1986. Exhibit H,
Response 8 (including attachment). But NEMA’s recent grants are few—just
three since 2015 totaling just $13,465—nor do they appear focused on
“fight[ing] and win[ning] the battle against heart disease” or of doing
anything concrete to “put an end to needless suffering.” NEMA’s last research
grants, which arguably did do something (even if minimal) in the battle
against heart disease, were in 1994—24 years ago. This leaves NEMA’s
“educational program,” a program that was almost exclusively accomplished
within fundraising campaigns and is not rightly considered a charitable
program. Moreover, in fundraising under the name “National Heart Council”
and speaking of putting “fight[ing] and win[ning] the battle against heart
disease” and “put[ting] an end to needless suffering,” NEMA implied to
donors that their donations do would do more than fund continued
sweepstakes and fundraising mailings. In sum, NEMA had no programs to

17
“fight and win the battle against heart disease” or to “put an end to needless
suffering.”
27. Sweepstakes package #7418 National Alzheimer’s Council (dated 12/1/15)
included an “award notification” regarding a $10,425.76 grand prize and then
asked for a donation “to help end the tragedy of Alzheimer’s Disease:”
Mr. Sampleperson, we also request your formal participation by enclosing a tax-deductible gift to help end the tragedy of Alzheimer’s Disease. A donation is not required and will not increase your chances of winning. But your gift of just MRC1, or MRC2 will bring hope and happiness to many families struggling with this disease . . . even right there in <ST>.” [Exhibit G and F.4]
The Attorney General asked NEMA to identify all expenditures, programs in
Michigan, and grants to people in Michigan for the purpose of helping “end
the tragedy of Alzheimer’s Disease.” NEMA’s response, similar to previous
NEMA responses, confirmed that NEMA’s only program to combat
Alzheimer’s Disease is the educational materials it sends (mostly within
fundraising campaigns). NEMA claimed that it spent $4,066,366 in
promoting awareness of Alzheimer’s, but as will be discussed in greater detail
below, these mailings were primarily fundraising campaigns and NEMA
should not have allocated its fundraising costs to program services, or
alternatively, NEMA excessively allocated fundraising costs to program
services. NEMA also confirmed that it made no grants to combat Alzheimer’s
in Michigan during the years 2015 to 2016. Exhibit H, Response 9.
28. Sweepstakes package #7771 (2016, quarter 4) included an announcement
that “the $9,452.51 check has been approved for payment” and stated:

18
Thank you for your previous donation to NAC, Mr. Sampleperson, we hope that you will continue to support our fight to end the tragedy of Alzheimer’s Disease. A gift is not required and won’t increase your chances of winning, but your donation will bring hope to families struggling with the disease and help fund vital research to find a cure. [Exhibits G and F.5 (emphasis added)]
NEMA mailed package #7771 to over 60,000 recipients nationwide in
December 2016, generating more than 6,000 donations. Regarding this
mailing, the Attorney General asked: “For the years 2015 through present,
identify all NEMA grants to fund vital research to find a cure for Alzheimer’s
Disease.” NEMA again responded stating that it does not make unsolicited
grants and confirmed that, during this period, “NEMA did not make grants
concerning Alzheimer’s disease.” Exhibit H, Response 10 (emphasis
added). In other words, a donation to NEMA did nothing to “help fund vital
research to find a cure” for Alzheimer’s, with NEMA’s last research grants
occurring 24 years ago in 1994. Instead, donations to NEMA were primarily
used to fund further NEMA sweepstakes and other fundraising mailings.
29. Mail package National Stroke Council #7266 from 2015 is an example of
another blatant deception by NEMA. Within this fundraising letter to
National Stroke Council “members,” NEMA stated:
Fighting stroke is very expensive. No matter how costly, we believe it’s vitally important. Stroke claims more than 400 American lives each day.
Whatever it takes, the National Stroke Council is dedicated to end stroke. And we’re proud to have you as a member and partner.
The National Stroke Council also works in communities like yours to prevent stroke and save lives of stroke victims. For example:

19
• Through your generosity, we have helped establish a new community service model for the rapid evaluation and treatment of patients experiencing a TIA or mini-stroke. Funding provided by the National Stroke Council to the Brain Attack Team at the University of Maryland Medical Center . . . [Exhibit F.9]
Omitted from NEMA’s fundraising letter is the relevant fact that NEMA’s
“new community service model” was a grant to the University of Maryland in
2002—thirteen years before the mailing. Exhibit H, List of NEMA
grants. Moreover, that 2002 grant appears to have been the last NEMA
grant to combat stroke, with NEMA confirming in its response to the
Attorney General that NEMA had made no grants to combat stroke between
2015 through 2018. Exhibit H, Response 5.e. Yet, thirteen years after its last
to combat stroke, NEMA is still telling donors that donations will support
NEMA in its work “in communities like yours to prevent stroke and save
lives of stroke victims.”
C. NEMA’s Other Solicitations and its “Educational” Materials
30. NEMA has produced solicitation materials to the Attorney General for the
years 2015 to 2017. The Attorney General has reviewed these materials and
finds that they include similar or identical representations to the 2016
materials discussed in detail above.
31. The overall message of NEMA’s many fundraising campaigns was that
donations would aid in the fight against Alzheimer’s, or heart disease, or
stroke, or would support NEMA’s Kids Do Matter program. But in fact,
NEMA’s only “programs” were the sweepstakes and fundraising campaigns
themselves and any educational materials therein. (Any other NEMA

20
educational materials, on its website or in videos or other mailings, were
insignificant in scope compared to NEMA’s fundraising campaigns, which is
generally how it conducted its educational program. See Exhibit E, Response
7.e. admitting that NEMA’s education program typically contained a
fundraising appeal.) NEMA’s equipment grants have been minimal—
especially in recent years—and are not coordinated by any clear purpose. And
NEMA has made no research grants in over twenty years.
32. Given that NEMA’s almost exclusive charitable program—and hence its
justification for its existence and its fundraising—is purportedly its
educational materials within its mailings, the following paragraphs review
some of these “educational” materials.
33. NEMA National Heart Council sweepstakes package #7041 from 2015
(Exhibit F.6), as its educational component includes the following:

21
We note that NEMA includes its “educational” message directly under its
boilerplate disclosures and (apparently) on the back of a sweepstakes prize
announcement form. That is, most people that received this “educational”

22
message likely threw the package away unopened; those that opened it likely
threw it away then; and those that responded with a donation are unlikely to
have ever read the fine print on the back or the “educational” message.
Moreover, the ten tips to a healthy heart are generic—don’t smoke, exercise
regularly, watch what you eat, stop to smell the roses—and do not amount to
a fight or battle that is likely to defeat heart disease.
34. NEMA National Alzheimer’s Council mailing #7061 from 2015 (Exhibit F.7)
is another sweepstakes. Here is the top of the front of the mailing.

23
Here’s the back:

24
Again, NEMA’s purported educational component of the mailing is on the
back of a sweepstakes mailing (that most would classify as junk mail) and
comprises a short paragraph entitled “What is Alzheimer disease?” under a
lengthy page of boilerplate disclosures in small print. Again, the
“educational” message is generic, stating:
Alzheimer disease, or Alzheimer’s as it is also referred to, is the leading cause of dementia. Named after the person who first described it, Alzheimer disease may be defined as a set of symptoms that include loss of memory, judgement, reasoning ability, and often changes in behavior. With the aging of the “baby boomers” the incidence of Alzheimer’s is expected to more than triple by the middle of the 21st century. At the present time, Alzheimer’s cannot be stopped or cured. Research, however, is resulting in greater understanding of the disease and identification of steps that may reduce your risk of experiencing Alzheimer’s.
And NEMA’s underlining of the last sentence regarding the importance of
research is itself misleading since NEMA conducts no such research and any
contributions to NEMA will almost exclusively be used to send more
fundraising and sweepstakes materials such as the present one. Nor does this
purportedly “educational” content include any call to action, so any joint cost
allocation for this particular mailing would be disallowed.
35. Other NEMA sweepstakes mailings, such as National Heart Council #7064 of
2015 (Exhibit F.8), included no educational content whatsoever.
D. Scope of NEMA’s Fundraising and Lack of Sweepstakes Winners
36. In response to the Attorney General’s investigative order, NEMA produced
spreadsheets detailing all its campaigns from 2015 through April 2018,
including the type of campaign and the result of each campaign. See Exhibit

25
H, NEMA Mail Packages Years 2015 to 2018. Over these three years and four
months, NEMA’s campaigns were almost all sweepstakes fundraising
campaigns, with a few straight fundraising appeals. The following chart
provides the totals for all campaigns for each year.
# Mailed Donors Income MI
donors
MI
income
Cost Net
income
2015 1,236,783 124,911 $823,269 7,263 $46,680 $782,935 $40,333
2016 2,023,398 235,046 $1,503,673 10,433 $67,228 $1,183,068 $320,605
2017 2,285,110 223,435 $1,418,569 10,604 $64,668 $1,366,404 $52,164
2018 612,012 74,815 $487,893 2,389 $14,079 $359,605 $128,287
Total 6,157,303 658,207 $4,233,404 30,689 $192,655 $3,692,012 $541,389
In sum, during this period, NEMA sent more than 6 million mailers
nationwide, raising more than $4 million, including nearly $200,000
in Michigan, yet apart from NEMA’s purported educational campaigns (of
dubious merit and almost exclusively within sweepstakes and other
fundraising campaigns), NEMA made just six grants totaling $13,965—or
0.3% of total funds raised—and conducted no research and made no
other efforts toward combatting stroke, heart disease, or Alzheimer’s.
37. The Attorney General also asked NEMA to identify its sweepstakes winners
in recent years. For the years 2015 to 2017, none of NEMA’s monthly
sweepstakes campaigns produced a sweepstakes winner.4 Exhibit I. That is,
4 NEMA has not produced sweepstakes winners for the current year of 2018. NEMA’s most recent sweepstakes winner was in 2013 for a $10,000 prize.

26
none of the 5.5 million NEMA sweepstakes mailings during the years
2015 to 2017 resulted in a claimed sweepstakes prize. Instead, the only
winners during these three years, were monthly “bonus” winners of $100
prizes, totaling $3,600 over three years.
E. NEMA’s Mailings do not Meet the Criteria for Joint Cost Allocations
38. As discussed above, NEMA’s educational content, which is found almost
exclusively in its many fundraising campaigns seeking donations, is of
dubious educational value and is mostly buried beneath disclaimers on the
back of sweepstakes prize announcements; and some fundraising campaigns
lack any educational content. Nevertheless, NEMA has been allocating joint
costs for years, thereby reporting millions of dollars of fundraising expenses
as “educational” programs on its IRS Form 990s.5 But for joint costs to be
allocable, Financial Standard Board’s Accounting Standards Codification’s
(ASC) threefold criteria of purpose, audience, and content must be met. ASC
958-720-45-29. NEMA’s joint costs do not meet this criteria; and
alternatively, NEMA’s joint cost allocations have been excessive.
Purpose Criterion
39. The ASC states:
To accomplish program functions, the activity shall call for specific action by the audience that will help accomplish the [nonprofit’s] mission. Actions that help accomplish the [nonprofit’s] mission are actions that do either of the following:
5 NEMA has been using joint cost allocations for at least the last ten years, and likely longer.

27
a. Benefit the recipient (such as by improving the recipient’s physical, mental, emotional, or spiritual health and well-being).
b. Benefit society (by addressing societal problems). [ASC 958-720-45-35]
NEMA asserts that it meets this test because its mailings routinely include
calls to action such as
• the National Heart Council’s “Ten Steps to a Healthy Heart,” which advises to “exercise regularly” and “see your physician regularly”;
• the National Stroke Council includes a call to “have your blood cholesterol level checked” and recommending limiting consumption of high cholesterol food;
• the National Alzheimer’s Council states that “getting a diagnosis and
getting it early will help the affect person and their family make plans for the future” and “that’s why it is very important to see your doctor if you suspect Alzheimer’s disease.” Exhibit E, Responses 7c and 7d.
We note that our review found mailings that lacked any call to action, or
simply educated the audience about a particular disease, such as the mailing
whose only educational content was the paragraph regarding “What is
Alzheimer’s.” Nevertheless, even if NEMA’s above call to actions are
accepted, the purpose criterion is not established until all portions of the
criteria are satisfied, and NEMA fails the Separate and Similar Activities
Test and the Other Evidence Test.
40. Separate and Similar Activities Test. The test states: “The purpose
criterion is met if a similar program or management and general activity is
conducted separately and on a similar or greater scale.” ASC 958-720-45-45.
The Attorney General’s Charitable Trust Auditor asked NEMA regarding
this test: “Is the program, including the call to action, conducted on a similar
28
scale using the same medium without the fund-raising appeal?” Exhibit D.
NEMA responded: “No. NEMA’s program typically includes a fund-raising
appeal.” Exhibit E, Response 7e. Since NEMA failed the Separate and
Similar Activities Test, NEMA must past the Other Evidence Test (ASC 958-
720-45-47) or it fails the purpose criterion.
41. Other Evidence Test. Under this test, “[a]ll available evidence, both
positive and negative, shall be considered to determine whether, based on the
weight of that evidence, the purpose criterion is met.” ASC 958-720-45-47.
Implementation guidance for this test is found in ASC 958-720-55-6 to 55-9.
NEMA fails this test. ASC 958-720-55-7 states: “The facts may indicate that
the purpose criterion is met if the [nonprofit] measures program results and
accomplishments of the activity.” But apart from tracking whether a
particular mailing produces a donation, NEMA has no apparent means for
measuring the extent to which its audience has been educated or otherwise
taken action in response to NEMA’s calls to action. Nor does NEMA meet the
next part of the test, since NEMA does not conduct its calls for specific action
“without a significant fundraising component in a different medium.” Id. In
considering “all available evidence,” the Attorney General also again notes
that NEMA’s “educational” materials included generic information such as
“don’t smoke,” “watch your weight,” and “stay connected”; and these were
frequently found on the back side of sweepstakes mailers—mailers that
themselves generally produced no sweepstakes winners—under the small

29
print disclosures explaining that the person had in fact not won a major prize
and had a small likelihood of winning. NEMA’s mailings fail the Other
Evidence Test.
Audience
42. When the purpose criterion is not met, joint costs are not allocable to
program services and no further analysis need be done. Nevertheless, we will
analyze the “Audience” criterion, which also leads to the conclusion that joint
costs should not be allocated.
43. ASC 958-720-45-48 states:
A rebuttable presumption exists that the audience criterion is not met if the audience includes prior donors or is otherwise selected based on its ability or likelihood to contribute to the [nonprofit]. That presumption can be overcome if the audience is also selected for any of the reasons in the following paragraph. In determining whether that presumption is overcome, [a nonprofit] shall consider the extent to which the audience is selected based on its ability or likelihood to contribute to the NFP and contrast that with the extent to which it is selected for one or more of the reasons in the following paragraph. For example, if the audience’s ability or likelihood to contribute is a significant factor in its selection and it has a need for the action related to the program component of the joint activity, but having that need is an insignificant factor in its selection, the presumption would not be overcome.
The Attorney General asked NEMA how it selected its audience and how it
overcame this presumption. Exhibit D. NEMA’s response claimed that
NEMA’s lists are chosen “to identify people likely to have the interest and
ability to take independent action to further NEMA’s mission. . .” NEMA has
failed to rebut the presumption. NEMA’s “educational” mission and generic
calls to action are such that any adult member of the public would meet this

30
criterion. Additionally, NEMA’s response admitted that part of its strategy
for identifying recipients was whether that person had donated financially in
the past: “a strategy was developed to identify and contact those who have
supported NEMA in the past, either financially, by volunteering, or by taking
other independent actions on behalf of NEMA in furtherance of its mission . .
.” Exhibit E, Response 7f, 7g, and 7h. Considering our review of NEMA’s
activities, we are unpersuaded that a significant portion of NEMA’s lists
include NEMA volunteers or those that NEMA has confirmed have taken
“independent action” on NEMA’s behalf. In fact, NEMA’s response appears to
be a false statement since NEMA has not recently reported any volunteers on
its Forms 990. (Line 6 of NEMA’s 2015, 2016, and 2017 Forms 990 list zero
volunteers.) NEMA has failed to rebut the presumption that its audience was
chosen due to its likelihood to contribute and so fails the audience criterion.
44. Content. Because NEMA failed both the purpose and audience criteria, joint
costs are not allocable to program services, so no analysis of the content of the
joint activity is necessary.
45. Excessive. Alternatively, had NEMA satisfied the joint costs criteria, NEMA
excessively allocated these costs to program services. One of the accepted
methods for allocating joint costs is the physical units method, which involves
measuring the lines or square inches of a mailing that are dedicated to
program, which in NEMA’s instance would be its educational program
inviting its donors to a call to action. ASC 958-720-55-26. But NEMA did not

31
use this method or any of the accepted methods. Instead, NEMA used an
allocation of employee time and allocated as much as 75% of the cost of its
printed fundraising materials to its educational programs. Exhibit E,
Response 4e attachment; see also Exhibit H, Response 18. We find that this
method was neither rational nor systematic as a review of the mailings shows
that their primary purpose was fundraising, and any educational component
to the mailings was minimal, whether by the physical units method or any
other measure. Additionally, NEMA’s time allocation for President Kelly
Herzog is itself suspect since NEMA has almost no program activities; nor is
it clear that Herzog’s supposed time spent on programs is relevant to the cost
allocation of NEMA’s mailings, which have a primary purpose of fundraising
and include minimal educational materials and, sometimes, no educational
materials nor any call to action. And in responding to the Attorney General’s
investigative order, NEMA implies that it recognizes that its past allocations
were excessive since NEMA stated that it was revising its allocation method
for 2017 “to reflect not only personnel time but, also, the mailing content
breakdown.” Exhibit H, Response 18.
46. Using joint cost allocations over the last ten or more years—and even though
NEMA made almost no grants and conducted no research during this time—
NEMA has falsely reported hundreds of thousands of dollars (over a million
dollars in some years, see, e.g., 2013 Form 990) of its fundraising expenses
each year as charitable program service expenses. This has grossly inflated

32
NEMA’s charitable activities on its IRS Form 990 and was part of its scheme
to defraud donors.
III. Law
47. Section 18 of the Charitable Organizations and Solicitations Act (Solicitations
Act) prohibits persons from engaging in a variety of acts. MCL 400.288. These
prohibited acts include:
(j) Divert or misdirect contributions to a purpose or organization other than that for which the funds were contributed or solicited.
(n) Employ any device, scheme, or artifice to defraud or obtain money or property from a person by means of a false, deceptive, or misleading pretense, representation, or promise.
(o) Represent that funds solicited will be used for a particular charitable purpose if those funds are not used for the represented purpose.
(u)(ii) Submit any of the following to the attorney general . . . [a] document containing any materially false statement.
(y) For a charitable organization, submit financial statements, including IRS form 990, 990-EZ, 990-PF, or other 990- series internal revenue service return, or any other financial report required under this act, that contain any misrepresentation with respect to the organization’s activities, operations, or use of charitable assets.
IV. Alleged Violations
Every alleged violation below incorporates the facts alleged above and in
every other alleged violation.
48. Scheme to Defraud. MCL 400.288(1)(n).

33
a. Since at least 2015, NEMA has been raising funds with the express
purpose of fighting stroke, Alzheimer’s, and heart disease, and
supporting its Kids Do Matter program.
b. NEMA’s fundraising materials included generic representations, such
as that donations would “join in our effort to fight and win the battle
against heart disease” or to “help end the tragedy of Alzheimer’s
Disease” or to “fight stroke.” See, for example, Sweepstakes package
#7411 (dated 11/25/15) and Sweepstakes package #7418 (dated
12/1/15).
c. NEMA’s fundraising materials also included specific representations
regarding NEMA’s activities in “fighting” these diseases, including:
i. “Our plans are in place for the programs, educational materials
and equipment grants that are so vital to so many people –
people in your local area – perhaps even someone in your own
family.” Mail package #7487 (dated 2/16/16).
ii. “Through our mailings we raise the much needed funds for the
prevention of injury and illness by addressing health and social
issues through education, applied research, technology, and
equipment.” Mail package #7487 (dated 2/16/16).
iii. NEMA’s homepage at www.nemahealth.org stated, under “Our
Mission”: “Our mission is the prevention of injury and illness by
addressing health and social issues through education, applied

34
research, technology, and equipment.” And “The National
Emergency Medicine Association is a 501(c)(3) nonprofit
organization founded in 1982, committed to trauma prevention
and the delivery of quality medical services at each stage of
trauma with and [sic] emphasis on first response at the time of
the emergency.”
iv. “With your past support [Mr. XXX], we have been able to
expand our grants for stroke education and develop stroke
prevention materials for individuals at risk.” Mail package
#7578 (dated 5/5/16) (emphasis added).
v. “[W]e hope that you will continue to support our fight to end the
tragedy of Alzheimer’s Disease. A gift is not required and won’t
increase your chances of winning but your donation will bring
hope to families struggling with the disease and help fund
vital research to find a cure.” Sweepstakes package #7771
(2016, quarter 4) (emphasis added).
d. NEMA used false and excessive joint cost allocations on its IRS Form
990 in support of this scheme and to make it appear that it had
valuable charitable programs when, in fact, it had few to none.
e. NEMA’s fundraising campaigns were a device, scheme or artifice to
defraud or obtain money from Michigan (and nationwide) donors by

35
means of a false, deceptive, or misleading pretense, representation or
promise and so violated MCL 400.288(1)(n).
f. NEMA misled donors into believing that NEMA would use funds
raised to fight Alzheimer’s, heart disease, or stroke, or to support Kids
Do Matter. Instead, NEMA almost exclusively used funds raised to
fund additional sweepstakes campaigns—sweepstakes that themselves
produced no sweepstakes winners—and other fundraising campaigns
and pay NEMA administrative expenses, including a six-figure salary
for NEMA President Kelly Herzog.
g. NEMA’s purported “educational” benefit within its mailings was of
limited to non-existent value and was not properly categorized—or
excessively categorized—as a charitable program. To the extent that
NEMA’s mailings included some “educational” content that could be
considered a charitable program, NEMA nevertheless deceived donors
since NEMA’s mailings implied the existence of a charitable program
to “fight” or to “fight and win” the battle against Alzheimer’s, stroke, or
heart disease. NEMA had no such program.
h. Apart from NEMA’s educational programs, which were actually
fundraising campaigns, NEMA had no other programs to fight
Alzheimer’s, stroke, or heart disease. NEMA’s equipment grants are
minimal and have no apparent purpose in fighting Alzheimer’s, stroke,
or heart disease. And NEMA has not funded any research for more

36
than 20 years. Likewise, NEMA’s Kids Do Matter campaigns were
purely fundraising campaigns that supported none or, at best, de
minimis charitable activities.
i. For every solicitation NEMA made into Michigan for the years 2015 to
2018, NEMA violated MCL 400.288(1)(n). While NEMA has not
provided the precise number of mailings into Michigan, the numbers it
has provided the Attorney General suggest that NEMA obtains
approximately one donation for every ten mailings. Since NEMA has
obtained 30,689 donations from Michigan donors, the Attorney General
alleges 300,000 violations of MCL 400.288(1)(n). [300,000 violations]
49. Diversion of Funds Raised. MCL 400.288(1)(j).
a. In responding to NEMA solicitations, NEMA donors intended their
donations to be used for the purposes included in the solicitation
materials, i.e., to fight heart disease, stroke, and Alzheimer’s through
charitable programs that included research, education, and equipment
grants.
b. Apart from the “educational” materials NEMA sends within its
fundraising campaigns, NEMA has no charitable programs to combat
disease or support children. In recent years, NEMA has conducted no
research and it has made minimal equipment grants and ones that are
not targeted toward combatting disease, let alone defeating these

37
diseases; nor has it made grants in support of its Kids Do Matter
program.
c. For every donation raised in Michigan from 2015 through 2018, NEMA
diverted or misdirected contributions to a purpose or organization
other than that for which the funds were contributed or solicited in
violation of MCL 400.288(1)(j). For each of the 30,689 donations raised
in this period, the Attorney General alleges one violation of MCL
400.288(1)(j). [30,689 violations]
50. Misrepresentation of Use of Funds Donated. MCL 400.288(1)(o).
a. NEMA donors intended their donations to be used to support programs
to fight and win the battle against Alzheimer’s, heart disease, and
stroke; to fund research; to fund equipment grants to combat these
diseases; to support the safety and medical treatment of children; and
to expand NEMA’s grants.
b. NEMA’s sweepstakes and other fundraising campaigns represented
that funds raised would be used for these and other particular
charitable purposes, but NEMA did not use the funds raised for these
purposes.
c. For every solicitation NEMA made into Michigan for the years 2015 to
2018, NEMA violated MCL 400.288(1)(o). While NEMA has not
provided the precise number of mailings into Michigan, the numbers it
has provided the Attorney General suggest that NEMA obtains one

38
donation for every ten mailings. Since NEMA has obtained 30,689
donations from Michigan donors, the Attorney General alleges 300,000
violations of MCL 400.288(1)(o). [300,000 violations]
51. Submitting Documents with False Statements to Attorney General.
MCL 400.288(1)(u)(ii)
a. NEMA submitted its registration form in 2017 accompanied with its
2016 IRS Form 990 and audited financial statements. NEMA reported
on its IRS Form 990 and its audited financial statements that it
received $1,422,709 in contributions, $1,482,867 in total expenses, and
of these expenses, $972,700 in total program services. But NEMA’s
report of its total program services was false. Of the $972,700 in total
program service expenses, $967,673—99.5% of total program services
expenses—were reported as joint costs allocated to program services.
NEMA did not meet the purpose or audience criterion of SOP 98-2 and
should not have allocated any joint costs.
b. And to the extent that any of NEMA’s fundraising costs were properly
allocable as joint costs, NEMA falsely overstated its joint costs using
an allocation of employee time that was neither rational nor
systematic, an allocation which NEMA used even though some of its
mailings included no call to action and other mailings included no
educational content whatsoever.6
6 NEMA has admitted that it used employee time rather than mailing content to do the allocation and intends to amend its 2016 IRS Form 990 once it has recalculated the

39
c. 2 violations. In submitting its 2016 IRS Form 990 and audited
financial statements to the Attorney General as part of its registration,
NEMA submitted documents with false statements in violation of MCL
400.288(1)(u)(ii). [2 violations]
52. Submitting Financial Statements that Misrepresent NEMA’s
charitable activities. MCL 400.288(1)(y).
a. NEMA submitted its registration form in 2017 accompanied with its
2016 IRS Form 990 and audited financial statements. NEMA reported
on its IRS Form 990 and its audited financial statements that it
received $1,422,709 in contributions, $1,482,867 in total expenses, and
of these expenses, $972,700 in total program services. But NEMA’s
report of its total program services was false. Of the $972,700 in total
program service expenses, $967,673—99.5% of total program services
expenses—were reported as joint costs allocated to program services.
NEMA did not meet the purpose or audience criterion of SOP 98-2 and
should not have allocated any joint costs.
b. And to the extent that any of NEMA’s fundraising costs were properly
allocable as joint costs, NEMA falsely overstated its joint costs using
an allocation of employee time that was neither rational nor
allocation using mailing content. See Response #19 to Investigative Order. NEMA has also admitted that at least some of its solicitation materials included no call to action, hence any allocation for those materials was unjustified. See Response #16: “NEMA’s Kids Do Matter direct mail solicitations did not provide a call to action.” And our review has also shown that some of the mailings included no educational content, so no joint cost allocation for these mailings was justified. See, for example, National Heart Council #7064 of 2015.

40
systematic, an allocation which NEMA used even though some of its
mailings included no call to action and other mailings included no
educational content whatsoever.
d. 2 violations. In submitting its 2016 IRS Form 990 and audited
financial statements to the Attorney General as part of its registration,
NEMA submitted financial statements that misrepresented NEMA’s
charitable activities in violation of MCL 400.288(1)(y). [2 violations]
53. Total Violations. In total, and as described in the preceding paragraphs, the
Attorney General alleges that NEMA has violated the Solicitations Act
630,6937 times.
V. Attorney General’s Authority 54. Section 20 of the Charitable Organizations and Solicitations Act specifies
the Attorney General’s authority to redress violations of the Act, including:
a. Issuing a Notice of Intended Action, MCL 400.290(4);
b. Issuing a Cease and Desist Order, MCL 400.290(4);
c. Bringing a civil action in court with a fine of up to $10,000 per
violation, MCL 400.290(1);
d. Accepting an Assurance of Discontinuance, MCL 400.290(4); and
e. Requesting injunctive relief, attorney fees and costs, and restitution,
MCL 400.290(1).
7 At a maximum civil fine of $10,000 per violation, as alleged, NEMA faces a maximum penalty of $6,306,950,000. Even at a modest penalty of $10 per violation, NEMA faces a penalty of $6,306,950.

41
55. Section 20 of the Solicitations Act allows the Attorney General to proceed
against individual officers, directors, shareholders, or controlling members
of NEMA. MCL 400.290(1).
VI. Cease and Desist Order
56. The Attorney General HEREBY ORDERS National Emergency Medicine
Association (NEMA) to CEASE AND DESIST all unlawful solicitations as
described in the above violations. Within seven (7) days, NEMA must
confirm in writing to the Attorney General its compliance with this order.
57. Violations of this order may result in a civil action for restitution, civil fines,
litigation costs, and injunctive relief. Continuing violations may also result
in additional violations alleged in any civil action.
VII. Opportunity to Respond or to Confer with the Attorney General
58. Within twenty-one (21) days of receiving this Notice, Respondents have the
opportunity to respond to the undersigned Assistant Attorney General and
to confer with the undersigned Assistant Attorney General in reaching an
appropriate assurance of discontinuance or settlement agreement.
59. If no satisfactory resolution is reached during this period, the Attorney
General intends to bring a civil action against NEMA and its President
Kelly Herzog (and possibly other NEMA directors or officers) in Ingham


Exhibit A

'',.,
.;.:
;,,
NEM
A
Nat
iona
l H
eart
C
ounc
il L
earn
the
sig
ns o
f he
art
atta
ck, a
sses
s yo
ur r
fsk
fact
ors,
leam
abo
ut th
e vi
deo
Str
aigh
t fro
m t
he
Hea
rt
, !
I Sear
ch..
. .,
\
''-------:-
-::
-:-
:--c-,-
-,-
,;-c-,-
-,.
~ N
atio
nal
Hea
rt C
ou
nci
l
••••
Who
is th
e N
atio
nal
Em
erge
ncy
Med
icin
e A
ssoc
iatio
n {N
EMA
)?
Th-e
Na
tio
na
l Em
erge
ncy
Me
dic
ine
A.ss
odat
to~:
is a
501
{c){
3) n
o:-ip
rofit
or~
aniz
citio
,..i f
ou
nd
ed
1n
19S
2,
com
miu
ed t
o 1
raur
ra p
reve
r:1io
n ar
,c tt
:e C
eUve
ry o
f q1.
.:aU:
y 11
edj::
::al s
e.:-.
;i-ce
s a
t e~c
h s:
age
of e
aun:
a v,
.tith
and
emph
asis
on
firs
t :e
spo
nse
at
tr1E
tim
e o
" th
e e
rr.e
rgen
cy.
Our
Mis
sion
0 L~
t rris
sto1
is t
he p
reve
ntio
n o
f tnj
ur:/
a~C
n::1
ess
·oy
:aG
dres
s1ng
hea
t:::-,
a:-1
d so
cia~
1ss
ues
thror
...~9'"
"1 e
d'...
.!cat
ion.
aJpU
ed r
esea
rch.
tec
hnol
ogy,
a.,:
c eq
_uip
men
r_
Pl.E
ase
Co:
-,sic
e~ S
uppo
rtin
g O
ur
Eff
or.s

Exhibit B
DAGC09-005 AUTHORITY 1975 PA 169 COMFLIANCE: Required
STATE OF MICHIGAN DEPARTMENT OF ATTORNEY GENERAL
PENALTY: Nonllcensur8
REGISTRATION TO SOLICIT DONA TIO NS
FULL OFFICIAL NAME OF ORGANIZATION NATIONAL EMERGENCY MEDICINE ASSOCIATION
ADDRESS OF ORGANIZATION ORGANIZATION TELEPHONE 500 Edgewood Road, Suite 105, P.O. Box 1039 443-922-7533 Edgewood MD 21040
ORGANIZATION WEB SITE
n l"h .... l, hr,y d """' oririress www.nemahealth.org
LIST & OTHER NAMES UNDER WHICH YOU INTEND TO SOLICIT E-MAIL ADDRESS
See Statement 1 [email protected]
ENTER A TTY GEN FILE # (MICS/CT/T)
9773
EMPLOYER ID NUMBER
52-1257429 ORGANIZATION FAX 888-682-7947
PART I • FINANCIAL SUMMARY FORTHE PERIOD BEGINNING 01/01/2016 AND ENDING 12/31/2016
D Check box if organization is newly created and financial information is not yet available. See instructions.
THIS PART MUST BE COMPLETED UNLESS ABOVE aox IS CH§CK§D
Starting for 2008 returns, the IRS has changed many of the fields for the Form 990. The form below accommodates the 2007 return as well 2008 and later. Unless specified otherwise, lines below refer to IRS Form 990 lines on 2008 and later returns.
REVENUE 1a. Contributions to donor advised funds (2007 returns only)
b. Total contributions
2. Net gaming lncome/(loss) (2008 and newer returns only)
3, Government contributions-grants (a// retums)
4a. Gross revenue from special events (a// returns)
b, Less: direct expenses (a// returns) .
c. Net Income or (loss) (all returns)
5. Total support
6. Program service revenue
7. Membership dues & assessments
8. Total of other revenue (See instructions)
9. TOTAL REVENUE
EXPENSES Program services (identify individually)
10a. See -statement 2 b.
C,
d. -----------------e, Total program services
11. Payments to affiliates (2007 returns only)
12. Total program activity - add lines 1 Ce and 11 .
13. Management and general
14. Fund raising
15. TOTAL EXPENSES
16. Excess or (deficit) for the year
17. Net assets or fund balances at beginning of year
18. Other changes in net assets or fund balances
19. Net assets or fund balances at end of year
4a. ------0joo 4b. ------0100
BALANCE SHEET SUMMARY as of period ending date shown above
20. Total assets
21. Total liabilities
22. Net assets or fund balances
1a. 0 100
b. 1,422.109 I oo
2. 0100
3. 0100
4c. o I oo 5, 1 .422. 109 I oo 6, o I oo 7. 0100
8. 21,699100
9. 1,444.406100
10a. 1: b.
C, I aa d. I QQ
e. 912.100 Ice . 11. 0 loo . 12. 912.100 loo , 13. 143,698 lao .14, 366,269 laa , 15. 1,4s2.ss1 loo
. 16. -38.459 loo
.17. 21s.s12 loo
. 18. -391,792 loo
. 19. -154.439 loo
. 20. 304.154 ba , 21. 458.593 ~a '22. -154,439 bo

PART ll(A)
Yes No v'
PROFESSIONAL FUND RAISER
During the fiscal year reportgd in Part I, did the organization compensate a professional fund raiser as defined by Michigan law? (See instructions for definition).
If yes, complete Schedule A. Attach copies of all contracts, addendums, and Campaign Financial Statements (for type B contracts*) unless previously submitted. For type A contracts no longer in effect, enter date contract ended in End Date column at right. Use a separate line for each type B* campaign or event.
SCHEDULE A
Name, Address, & MIFR # of Professional Fund Raiser
Contract Type*
Period Covered or Date of Event
Sum of All Payments to professional Fund Raiser
-----Type A·---En d Date
If additional lines are needed, attach schedule using above format.
PART ll(B)
Yes No v' Does the organization currently have a contract with a professional fund raiser as defined by Michigan law?
(See instructions for definition).
If yes, complete Schedule B for each contract even if included on Schedule A above. For type B contracts*, complete a separate line for each campaign or event. Attach copies of all contracts and addendums not previously submitted.
SCHEDULE B
Name, Address, & MIFR # of Professional Fund Raiser
Contract Type*
Date of Contract
• - - - - - - - Type B only - - - - - - - -
Campaign end/ Show Date
•contracts with a professional fund raiser (PFR) are to be categorized according to the type of fund raising services described by the contract. Contract types which begin with the letter A (type A contracts) involve arrangements where the PFR does not come into contact with solicited funds. In contract types which begin with B (type B contracts), the PFR has access to the solicited funds.
A 1 - Consultant A2 - Solicits, does not handle funds B3 • Special event B4 - Sell coupon books
BS - Sell advertising space B6 - Sell other items B7 • Solicits, handles funds B8 • Other
PART Ill AUDIT OR REVIEW REQUIREMENT
The following schedule has been completed to show you if either audited or reviewed financial statements are necessary. If you already submitted an audit prepared in accordance with generally accepted auditing principles, you do not need to complete this section.
a. Total support Restricted grants from foundations (no longer used) Government grants
1.422,709 [oo b. c. d. e.
Add lines b & c . Subtract line d from line a • 1,422.70< O
If line e is $525,000 or more, you must provide financial statements prepared In accordance with generally accepted accounting principles audited by an independent certified public accountant. If line e is $275,000 or more, but less than $525,000, either reviewed or audited financial statements are required.
PART IV GENERAL INFORMATION
1. You .!!lldfil. designate a resident agent in Michigan. Provide name and physical address (not PO Box). Name National Registered Agents, Inc. National Registered Agents, Inc.
Address 40600 Ann Arbor Road E, Suite 201 Plymouth Ml 48170
b. Attach samples.
3, For renewal registrations only. If the answer to any of the following is yes, attach a detailed explanation. All questions relate to the period since the filing of the organization's last application.
PARTV
a. Has there been any change In the organization's tax status with the Internal Revenue Service?
b. Has there been a significant change in the purposes of the organization?
c. Has the organization's right to solicit funds been denied, suspended, revoked, or enjoined by any state agency or by any court, or are proceedings pending?
d. For entities filing on behalf of Michigan chapters, have there been any additions to, or deletions from, the subsidiaries included within your license?
CERTIFICATION
Yes No ti
ti
ti
Under penalties of perjury, I certify that I am authorized to sign this document for the organization and that to the best of my knowledge and belief the information provided, including all attachments, is true, correct, and complete. Original signature required, no photocopies will be accepted.
Signature: _________________ _ President
Title Date Print Name: Kelly Herzog
REMINDER: You must attach a fully completed copy of the appropriate IRS form in order for \he registration to be processed. A llstlng of your board of directors names and addresses must be attached to the 990 or the registration See Statement 3
THIS IS A PUBLIC RECORD, COPIES OF WHICH ARE SENT, UPON REQUEST, TO ANY INTERESTED PERSON.
REV 10/09
Return Completed Registration To: ATTORNEY GENERAL CHARITABLE TRUST SECTION PO BOX 30214 LANSING Ml 48909

Statement 1
Form: Ml (2016)
Page: 1
Othor Namo:
Other Namo:
Page:1
Other Names
National Heart Council NHC National Stroke Council NSC
National Alzheimer's Council NAC Kids Do Maller KDM
NATIONAL. EMERGENCY MEDICINE ASSOCIATION
EIN: 62-1257429
Hoader

Statement 2
Form: Ml (2016)
Page: 1
Description
Program Sorvlcos
NATIONAL EMERGENCY MEDICINE ASSOCIATION
EIN: 52-1257429
10A
Expensos
The organizalion educated the public on physlcal and psychological health matters by using videos and Internal 8,875
964,025 The organization provided public health educational info on first aid, heart, trauma, stroke prevenllon, alzhelrner's disease, and emergency matters by majling letters to the general public
Total:
Page:2
972,700

Statement 3
Form: Ml 12016)
Page:3
Officer Name
Kelly Herzog
Patricia Brookhart
Page: 3
Officers, Directors and Trustees
Address
500 Edgewood Road, Suite 105 P.O. Box 1039 Edgewood, MD 21040
2608 Hess Road Fallston, MD 21047
NATIONAL EMERGE:NCY MEDICINE ASSOCIATION
EIN: 52•1257429
CERTIFICAllON
lllle
President
Treasurer
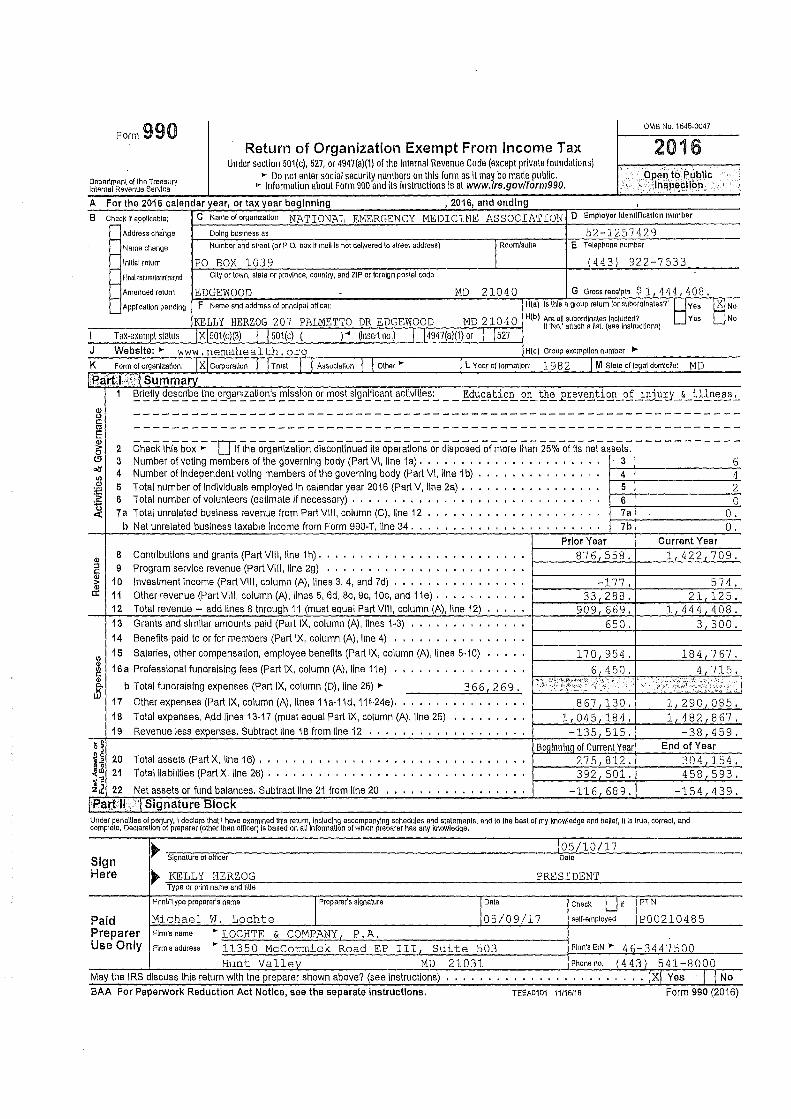
Form 990 0MB No. 1545-0047
2016 Return of Organization Exempt From Income Tax Under section 501(c), 527, or 4947(a)(1) of the Internal Revenue Code (except private foundations)
• Do not enter social security numbers on this form as IL may be made public. ~ft:rR~ti~~esr:~f;~ry • Information about Form 990 and its instructions Is at www.irs.gov/form990.
A For the 2016 calendar year, or tax year beginning , 2016, and ending B ChecK if applicable: C Name of organization NATIONAL EMERGENCY MEDICINE ASSOCIATION D Employer ldenuncallon number
...-Address change Doing business as 52-1257429 ..... I Room/sul\e E Telephone number Name change Number and s~eel (or P.O. box If mell ls no\ delivered lo street address) ,__ lnlllal return PO BOX 1039 ( 443) 922-7533 ...,_ final re\um/\ermlna\ad Cl\y or \own, slate or province, country, and ZIP or foreign postal code ,__
Gross receipts $ 1 , 4 4 4 , 4 0 8 , Amended return EDGEWOOD MD 21040 G - F Name and address of prtnclpal officer. H(a) Is \his a group return for subordinates?' ~Yes Appllca\lon pending ~No ..... H(b) Are all subordinates Included? Yes No KELLY HERZOG 207 PALMETTO DR EDGEWOOD MD 21040 If 'No,' a\\ach a list (sea lnslrucllons)
I Tax-exempt status IXl501(c)(3) I J 501(c) ( )• Onsert no.) I j4947(a)(1) or I 1s21 J Website: • www.nemahealth.orq H(c) Group exemption number • K Form of organlzallon: I xi Corµorallon I I Trust I I Assoclallon I I Olher • I L Year of fonnallon: 1982 j M Slate of legal domicile: MD
neart,L:S: I Summarv 1 Briefly describe the organization's mission or most significant activities: __ Education on the _rrevention of i.!!_JJ.ll)' & illness,
Ql ---------------------------------------------------------------0 C: C1l ---------------------------------------------------------------E <I)
_________ LJI _____________________________________________________ ~ 2 Check this box • If the organization discontinued its operations or disposed of more than 25% of Its net assets.
(!l 3 Number of voting members of the governing body (Part VI, line 1 a) , • • • • • , 3 6 «J 4 Number of independent voting members of the governing body (Part VI, line 1 b) 4 4 (/)
<I) 5 Total number of Individuals employed In calendar year 2016 (Part V, ilne 2a) • 5 2 :e ::,, 6 Total number of volunteers (estimate If necessary) • , •• , •• , 6 0 ~ 7a Total unrelated business revenue from Part VIII, column (C), line 12 7a 0.
b Net unrelated business taxable income from Form 990-T, line 34. 7b 0. Prior Year current Year
<I> 8 Contributions and grants (Part VIII, line 1h) .• , . , •• , • 876,558. 1,422,709.
:::J 9 Program service revenue (Part VIII, line 2g) •,Io I I I l C: ru
10 Investment income (Part VIII, column (A), lines 3, 4, and 7d) -177, 574, ai cc 11 Other revenue (Part Viii, column (A), lines 5, 6d, 8c, 9c, 10c, and 11e) . 33,288, 21 125. 12 Total revenue - add lines 8 through 11 (must equal Part Viii, column (A), line 12) 909,669, 1,444 408. 13 Grants and similar amounts paid (Part IX, column (A), lines 1-3) 0 0 I IO IO I l 650. 3 300. 14 Benefits paid to or for members (Part IX, column (A), llne 4) ' .... ' .. ' '.
"' 15 Salaries, other compensation, employee beneflts (Part IX, column (A), lines 5-10) 170,954, 184,767.
~ 16 a Professional fundraislng fees (Part IX, column (A), line 11 e) . . . . . . . . ' . 6 450. 4 715. <I>
b Total fundraising expenses (Part IX, column (D), line 25) • ii·· ·'f, It?:L'···.·· .''··•••· i<i?:t::.::z;; \; ...... i 0. 366,269. M 17 Other expenses (Part IX, column (A), lines 11a-11d, 11 f-24e). ''.'.' 8 67 130, J., 290 085, 18 Total expenses, Add lines 13-17 (must equal Part IX, column (A), line 25) 1,045,184, 1,482,867. 19 Revenue less expenses, Subtract llne 18 from line 12 '''' . . ' .. -135,515. -38 459.
5! Beqlnninq of Current Year End of Year d 20 Total assets (Part X, line 16) , • , Io o I Io Io 1 t .. 275 812. 304,154. 1~ 21 Total liabilities (PartX, line 26) , ••••• , •••.• .. 392 501. 458,593, j] 22 Net assets or fUnd balances. Subtract line 21 from line 20 -116 68 9, -154 439,
IP~rt-11\ I Signature Block Under pen allies of parjur;, I declare \hat I have examined \his return, Including accompanying schedules and s\alemanls, and lo \he bes\ of my knowledge and belief, II Is \rue, correct, and complete, Declarallon of preparer (other lhan officer) Is based on all lnformaUon of which preparer has any Knowledge,
• 105/10/17
Sign Signature of officer Dale
Here • KELLY HERZOG PRESIDENT Type or prlnl name and \Ille
PrtnVType preparers name I Preparers signature I Dale Check LJ1f I PTIN
Paid Michael w, Lochte 05/09/17 self-<>mployed P00210485 Preparer Firm's name • LOCHTE & COMPANY P.A. Use Only Firm's address • 11350 McCormick Road EP III Suite 503 Firm's EIN • 46-3447500
Hunt Vallev MD 21031 Phone no, {443) 541-8000 May the IRS discuss this return with the preparer shown above? (see Instructions) • • • • • • • ' .... '. . , , •, , , , , . !XI Yes · I I No BAA For Paperwork Reduction Act Notice, see the separate instructions. TEEA0101 11/16/16 Form 990 (2016)
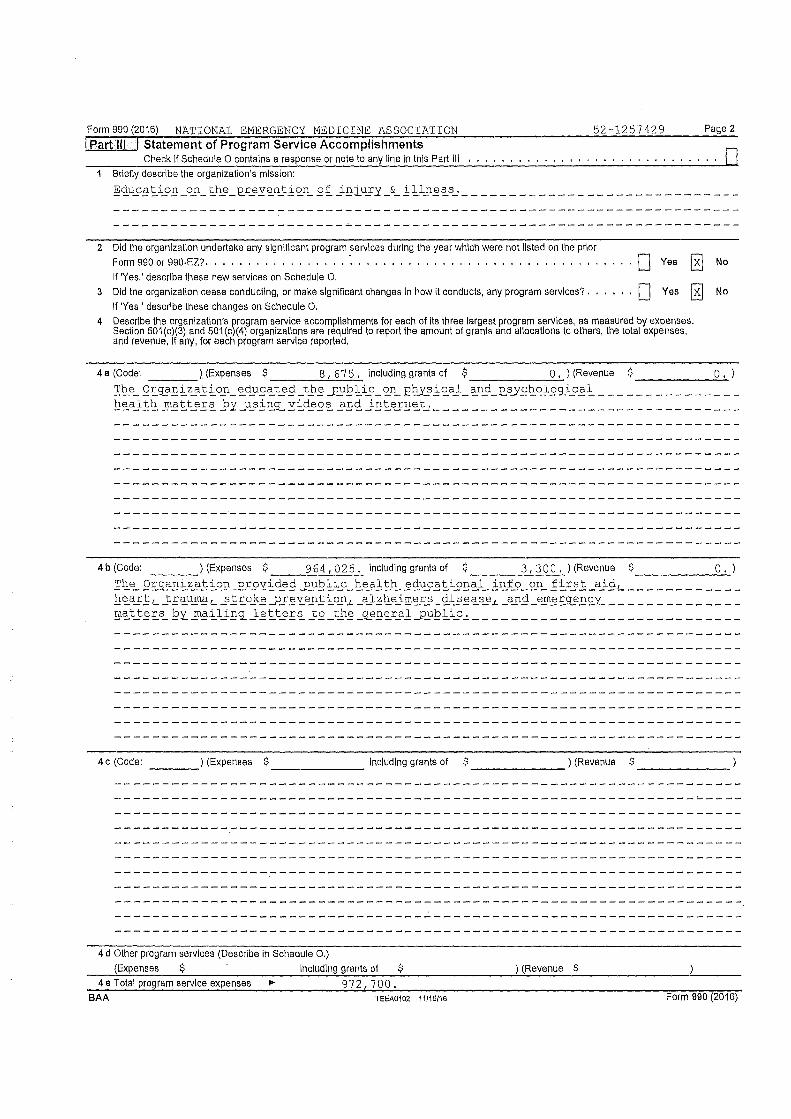
Form990(20i6) NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 Page 2
I.Part Ill I Statement of Program Service Accomplishments Check If Schedule O contains a response or note to any line In this Part Ill .... , ........ , .... , .... . "' •
Briefly describe the organization's mission: Education on the_12.revention of iniury & illness. ____________________________ _
2 Did the organization undertake any significant program sef\llces during the year which were not listed on the prior Form 990 or 990-EZ?. , . , . , ... , , . , • , , ..... , .. , .• , .. , , , ••..... , ... , ,
If 'Yes,' describe these new services on Schedule 0.
3 Did the organization cease conducting, or make significant changes In how It conducts, any program sef\llces?. If 'Yes,' describe these changes on Schedule O.
• ... ·D
Yes
Yes [ill
4 Describe the organization's program sef\llce accomplishments for each of Its three largest program sef\llces, as measured by expenses. Section 50i(c)(3) and 50i(c)(4) organizations are required to report the amount of grants and allocations to others, the total expenses, and revenue, If any, for each program service reported,
No
No
4a (Code: ) (Expenses $ 8 67 5. including grants of $ O. ) (Revenue $ O. ) ---- ____ _,___ ------- -------The OI3?nization educated the_pyblic_on El:u'J3ical_and .e_s_ys,holog_ical ______________ _ health matters by usillc'l., videos and internet, _______________________________ _
4 b (Code: ) (Expenses $ ---- 964,025. including grants of $ ____ 3~1 _3_0_0_.) (Revenue $ ______ 0_.)
The Org_anization_.e_rovided_pyblic_health educational info_ on first aidL ___________ _ heartL traumaL stroke_pJevention.L alzhe:i.mers_disease, and eme£g\"n<.::_y ____________ _ matters by_ mailing_ letters to the gs)neral_pyblic. ___________________________ _
4c (Code: ____ ) (Expenses $ _______ Including grants of $ _______ ) (Revenue $ ______ _
4 d Other program services (Describe In Schedule 0.) (Expenses $ Including grants of $ ) (Revenue $
4 e Total program service expenses • 9 7 2 '7 O O • BAA TEEA0102 11/16/16 Form 990 (2016)

Form 990 (2016) NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 Page 3
I Part IV :I Checklist of Required Schedules Yes No
1 Is the organization described In section 501(c)(3) or 4947(a)(1) (other than a private foundation)? ff 'Yes,' complete X Schedule A. . . . . . , . . . , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , 1
2 Is the organization required to complete Schedule B, Schedule of Contributors (see Instructions)? ... '.'' '' 2 X
3 Did the organization engage In direct or Indirect ~ol\tlcal campaign activities on behalf of or In opposition to candidates X for public office? ff 'Yes,' complete Schedule C, art I, . . . . • • , , • , , , , , . . . . . . . . , . . , • , , , , . , IO O' 3
4 Section 501(c)\3l organizations. Did the or~anlza\lon e~'We In lobbying activities, or have a section 501(h) election X In effect during he tax year? If 'Yes,' compfe e Schedule , art If • • • . • • • • • . • • • • . . • . • • • • . • . • . IO O I 4
5 Is the organization a section 501 (c)(4), 501 (c)(5~, or 501 (c)(6) organization that receives membership dues, X assessments, or similar amounts as defined in evenue Procedure 98-19? If 'Yes,' complete Schedule C, Part Ill ... ••I' 5
6 Did the organization maintain any donor advised funds or any similar funds or accounts for which donors have the right to provide advice on the distribution or investment of amounts In such funds or accounts? If 'Yes,' complete Schedule D,
X Part I, ........ , , • , , , , • , , . , , ..... , , , , , , , , , , ........•••. , , , , , , ''. ' .. ' 6
7 Did the organization receive or hold a conservation easement, including easements to ~reserve open space, the environment, historic land areas, or historic structures? If 'Yes,' complete Schedule D, art fl ........... I• f IO I' 7 X
8 Did the organization maintain collections of works of art, historical treasures, or other similar assets? ff 'Yes,' complete Schedule D, Part Ill. . . • . , , • , , . . . . . . . . . , , , , , • • , , , , , , , . , . , , . , , . '.' '.'.' 8 X
9 Did the organization report an amount In Part X, line 21, for escrow or custodial account liability, serve as a custodian for amounts not listed in Part X; or provide credlt counseling, debt management, credit repair, or debt negotiation
X services? If 'Yes,' complete Schedule D, Part IV , • , , , , , , , ..•. , .. , , , , , , , , , , , , , , , , , . ' I I I I I 9
10 Did the organization, directly or through a related organization, hold assets In temporarily restricted endowments, permanent endowments, or quasi-endowments? If 'Yes,' complete Schedule D, Part V , , .......... , , . '' '' . ' 10 X
If the organization's answer to any of the following questions is 'Yes', then complete Schedule D, Parts VI, VII, VIII, IX, ,,'._:, ' ,::··,,
,, :'."I 11 I , .. or X as applicable. lcii k_: ~
a Did the organization report an amount for land, buildings, and equipment In Part X, line 107 If 'Yes,' complete Schedule D, Part VJ. , , ....• , , , , , , , , . , , , .. , ... , , , , , , , • , , , • , ......•. , , , , , , , •. ... 11 a X
b Did the organization report an amount for Investments - other securities In Part X, line 12 Iha\ is 5% or more of its total assets reported In Part X, line 16? If 'Yes,' complete Schedule D, Part VII ................•....... . '' 11 b X
c Did the organization report an amount for Investments - program related in Part X, line 13 that Is 5% or more of its total assets reported in Part X, line 167 if 'Yes,' complete Schedule D, Part VIII , , , • . . . . . . . . . . . . . . . . . • . .. ' 11 C X
d Did the orTianlzatlon report an amount for other assets in PartX, line 15 that Is 5% or more of Its total assets reported in Part X, lne 16? ff 'Yes,' complete Schedule D, Part IX . . . . • • • , , • . . • , • • • . . • • • • . , • , , , • , '' 11 d X
e Did the organization report an amount for other liabilities In Part X, line 25? ff 'Yes,' complete Schedule D, Part X , , , . ' 11 e X
f Did the organization's separate or consolidated financial statements for the tax year include a footnote that addresses the organization's liability for uncertain tax positions under FIN 48 (ASC 7 40)? ff 'Yes,' complete Schedule D, Part X . ' ... ' 11f X
12 a Did the organization obtain separate, independent audited financial statements for the tax year? If 'Yes,' complete Schedule D, Parts XI and XII . • . . • , • , , , , , , , • , , , . • , . . . • • . , , , , , , , , • . • • . , , , . '' I I I! 12a X
b Was the organization included in consolidated, Independent audited financial statements for the tax year? If 'Yes,' and ff the organization answered 'No' to line 12a, then completing Schedule D, Parts XI and XII is optional 12b X
13 Is the organization a school described In seclion 170(b)(1 )(A)(II)? If 'Yes,' complete Schedule E, , , , . , •.•.. , , 13 X
14a Did the organization maintain an office, employees, or agents outside of the United States?, ..•....... , .. , . ' 14a X
b Did the or~anlzatlon have aggregate revenues or expenses of more than $10,000 from grantmaklng, fundralsing, business, nvestment, and program service activities outside the United States, or aggregate foreign Investments valued at $100,000 or more? If 'Yes,' complete Schedule F, Parts I and IV , • , , , , , , • , , •. , ••. , . , , . , , , , , , '.' 14b X
15 Did the organization rerort on Part IX, column (A), line 3, more than $5,000 of grants or other assistance to or for any foreign organization? / 'Yes,' complete Schedule F, Parts fl and IV • , , , . , . • . . . . . • • • . . . • • . , , , . • . '. 15 X
16 Did the organization report on Part IX, column (A), line 3, more lhan $5,000 of aggregate grants or other assistance to or for foreign Individuals? If 'Yes,' complete Schedule F, Parts Ill and IV • , ........ , , , . , . , , , •.. , .. '' 16 X
17 Did the or~anlzatlon r1ort a total of more than $15,000 of expenses for professional fundraislng services on Part IX, column (A, lines 6 an 11e? If 'Yes,' complete Schedule G, Part I (see Instructions) . , ...... , •.. , , .. , ... 17 X
18 Did the organization report more than $15,000 total of fundraising event gross Income and contributions on Part VIII, lines 1c and Ba? If 'Yes,' complete Schedule G, Part fl , •• , , •• , , , , , , , , • , ••.•...•. , , , ,'. .. ' 18 X
19 Did the organization report more than $15,000 of gross Income from gaming activities on Part VIII, line 9a? If Yes,' complete Schedule G, Part /II . .. , , , •• , , •. , ........•..• , ...•...•... , • , . , •. • I• I I I 19 X
BAA TEEA0103 11/18/18 Form 990 (2016)

Form 990 (2016) NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 Page 4
I-Part IV .1 Checklist of Required Schedules (continued) Yes No
20a Did the organization operate one or more hospital facilities? If 'Yes,' complete Schedule H . 20a X
b If 'Yes' to line 20a, did the organization attach a copy of Its audited financial statements to this return? 20b
21 Did the organization report more than $5,000 of grants or other assistance to any domestic organization or domestic government on Part IX, column (A), line i 7 If 'Yes,' complete Schedule I, Parts I and If , , , • , , i--.:::21,;,_,;f---,;,_,;'--X_
22 Did the organization report more than $5,000 of grants or other assistance to or for domestic individuals on Part IX, column (A), line 2? If 'Yes,' complete Schedule I, Parts I and Ill , .. , , . , .•.• , , , . , , • , ....•..... , •. , i-;:2::;.2-1-_-1-_X_
23 Did the organization answer 'Yes' to Part VII, Section A, line 3, 4, or 5 about compensation of the organization's current and former officers, directors, trustees, key employees, and highest compensated employees? If 'Yes,' complete Schedule J , . , . , . , , , . , , . , . . , . • . , , , • , , , • . . • • , , , . , , , , , , , , , • , , • , , , , ,
24 a Did the organization have a tax-exempt bond Issue with an outstanding principal amount of more than $100,000 as of the last day of the year, that was Issued after December 31, 20027 If 'Yes,' answer /Ines 24b through 24d and complete Schedule K. If 'No, 'go to 1/ne 25a , , ,. . , , , , , . . . , . , , , , . • , , , • , , . . . . , . , . , . . .
b Did the organization Invest any proceeds of tax-exempt bonds beyond a temporary period exception? . . • . , , . .
c Did the organization maintain an escrow account other than a refunding escrow at any time during the year to defease any tax-exempt bonds?. , , .•• , . , . , ..... , •.•••.•••. , .••......•.. , . , • ,
d Did the organization act as an 'on behalf of Issuer for bonds outstanding at any time during the year? , , , , , , , , ,
'. 23 X
. ' 24a X
'' 24b
'' 24c
'' 24d
25a Section 501(cl(3), 501(c)(4), and 501(c)(29) organizations. Did the organization engage In an excess benefit transaction with a disqualified person during the year? If 'Yes,' complete Schedule L, Part I , • , , , , , , , • , , , •• , • , , .-,;;;,25,.,;a'+--+--X_
b Is the organization aware that it engaged in an excess benefit transaction with a disqualified person In a prior year, and that the transaction has not been reported on any of the organization's prior Forms 990 or 990-EZ? If 'Yes,' complete Schedule L, Part I , , . , , , , , , , , , , , , , , , , , , , , • , , • • , , , , , • • • , • , , • , , , , , , , , , , , , , , f--'-25-'b-+--+--X_
26 Did the organization report any amount on Part X, line 5, 6, or 22 for receivables from or payables to any current or former officers, directors, trustees, key employees, highest compensated employees, or disqualified persons? If 'Yes,' complete Schedule L, Part II , • • , • , , , . • • . . • . . . • . . . • • • . . • • • . • • • , , . . . . , • . • , , ..,_26__._-"-_X_
27 Did the organization provide a grant or other assistance to an officer, director, trustee, key employee, substantial contributor or employee thereof, a grant selection committee member, or to a 35% controlled entity or family member of any of these persons? If 'Yes,' complete Schedule L, Pait Ill , • , , , , , , , , • , , , •• , , • , . , • , , , , . , , ..
28 Was the organization a party to a business transaction with one of the following parties (see Schedule L, Part IV instructions for applicable filing thresholds, conditions, and exceptions):
a A current or former officer, director, trustee, or key employee? If 'Yes,' complete Schedule L, Part IV • , , , • , , , , , , , ,
b A family member of a current or former officer, director, trustee, or key employee? If 'Yes,' complete Schedule L, Part IV, , , , , • , , , , , • , , , , , , , , • , , , , , , , , , , , , , , , , , , . ,
c An entity of which a current or former officer, director, trustee, or key employee (or a family member thereof) was an officer, director, trustee, or direct or Indirect owner? If 'Yes,' complete Scheciule L, Part IV • . , , • . . . . . , , ,
29 Did the organization receive more than $25,000 in non-cash contributions? If 'Yes,' complete Schedule M .. , , . ,
27 X
!tl'"{;"IIW'{ 1
.• _. f 1 28a X
28b X
28c X f ~2-9 -+----+--x--
30 Did the organization receive contributions of art, historical treasures, or other similar assets, or qualified conservation contributions? If 'Yes,' complete Schedule M . . . . , , , , . • . , . . . . . • • . . , , . • , , • . . . • • , , ..,_30__. _ _,,__x_
31 Did the organization liquidate, terminate, or dissolve and cease operations? If 'Yes,' complete Schedule N, Part I , f---31--1--+-X_
32 Did the organization sell, exchange, dispose of, or transfer more than 25% of its net assets? If 'Yes,' complete Schedule N, Part II , • , , , • , , , • • • , , , , , , , , , , , • , , , , , , • , • , , , • • , , , • • , , , , , , , , , , 1--32--1_-+_X_
33 Did the organization own 100% of an entity disregarded as separate from the organization under Regulations sections 301.7701-2 and 301.7701-3? If 'Yes,' complete Schedule R, Part I , , , , .. , , ••..... , ...• , . , ... ,
34 Was the organization related to any tax-exempt or taxable entity? If 'Yes,' complete Schedule R, Part II, Ill, or IV, and Pait V, line 1 , , , , , , , , , , , , , . , . . , , , • • , . • . , , , • . . • . . . . . , . , , , , , , . ,
35a Dld the organization have a controlled entity within the meaning of section 512(b)(13)7, , •• , , , • , , , , ,
b If 'Yes' lo line 35a, did the organization receive any payment from or engage in any transaction with a controlled entity within the meaning of section 512(b)(13)? If 'Yes,' complete Schedule R, Part V, line 2 , , , • , . , , , ,
36 Sectlon 501(c)(3) organizations. Old the organization make any transfers to an exempt non-charitable related organization? If 'Yes,' complete Schedule R, Pait V, line 2 . , , • • , • , • , , . . • , , , , , , , , , , , • ,
37 Did the organization conduct more than 5% of Its activities through an entity that Is not a related organization and that Is treated as a partnership for federal income tax purposes? If 'Yes,' complete Schedule R, Part VI , , , . , • , . , , • ,
38 Did the organization complete Schedule O and provide explanations in Schedule O for Part VI, lines 11 b and 197 Note, All Form 990 fliers are required to complete Schedule O •. , , , , • , , •• , ..••. , , • , ••. , •. , ,
BAA
TEEA0104 11/16/16
' .. '
''
''
''
0 t t I
33 X
34 X
35a X
36b X
36 X
37 X
38 X
Form 990 (2016)

Form 990 (2016) NATIONAL EMERGENCY MEDICINE ASSOCIATION
!Pa.rtV I Statements Regarding Other IRS Filings and Tax Compliance Check If Schedule O contains a response or note to any line in this Part V ,
1 a Enter the number reported In Box 3 of Form 1096. Enter -0- if not applicable , , b Enter the number of Forms W-2G Included in line 1 a. Enter -0· If not applicable,
52-1257429
1 a
1 b
c Did the organization comply with backup withholding rules for reportable payments to vendors and reportable gaming (gambling) winnings to prize winners? , , , , ...• , , , , , , , , , , , ..• , , , , , , , . , .. , , , . , , .
2 a Enter the number of employees reported on Form W-3, Transmittal of Wage and Tax State-ments, filed for the calendar year ending with or within the year covered by this return , , , .___2_a._L_ ______ --=2;.,i
b If at least one Is reported on line 2a, did the organization file all required federal employment tax returns? Note. If the sum of lines 1a and 2a Is greater than 250, you may be required to e-f//e (see Instructions)
3 a Did the organization have unrelated business gross Income of $1,000 or more during the year? .. , . , , b If 'Yes,' has It flied a Form 990-T forthis year? If 'No' to line 3b, provide an explana(/on In Schedule 0, , ......• , . ,
4 a At any time during the calendar year, did the organization have an Interest In, or a signature or other authority over, a financial account In a foreign country (such as a bank account, securities account, or other financial account)? . . . . .
b If 'Yes,' enter the name of the foreign country: .,.
. See Instructions for fillng_requirements for FlnCEN Form 114, Report of Foreign Bank and Financial Accounts (FBAR). Sa Was the organization a party to a prohibited tax shelter transaction at any time during the tax year? ...• ,
b Did any taxable party notify lhe organization that It was or Is a party to a prohibited tax shelter transaction? , . , , , c If 'Yes,' to line 5a or 5b, did the organization file Form 8886-T? , • , , . . . . . . . . , . , . . . . . . . . . , , .
6 a Does the organization have annual gross receipts that are normally greater than $100,000, and did the organization solicit any contributions that were not tax deductible as charitable contributions? , , , , ..... , , , , •.. , .
b If 'Yes,' did the organization Include with every solicitation an express statement that such contributions or gifts were not tax deductible? . , , , , , , , , . . , , , , , , , , , . . , . , • , , , , , , , . . . , , , , , , , , • , , , , ,
7 Organizations that may receive deductible contributions under section 170(c).
a Did the organization receive a payment In excess of $75 made partly as a contribution and partly for goods and services provided to the payor?. , , , , , . , . . , , , , , , , , . , , . . . , , , , , • , , . . . , , , , , ,
b If 'Yes,' did the organization notify the donor of the value of the goods or services provided? , , , , . , ••• ,
c Did the organization sell, exchange, or otherwise dispose of tangible personal property for which It was required to file Form 8282? , ... , ... , . , •.• , . , , , , , , , . , .. , , , , , , , , . , . , , , , , , , • , , , , , , , ,
d If 'Yes,' Indicate the number of Forms 8282 filed during the year , ..• , , . , , , , . , .. , ,__7__,d'---------1 e Did the organization receive any funds, directly or Indirectly, to pay premiums on a personal benefit contract?, f Did the organization, during the year, pay premiums, directly or Indirectly, on a personal benefit contract?, , ,
g If the organization received a contribution of qualified Intellectual property, did the organization file Form 8899. as required? , • • , , , , . . , . , , , , , , , , , , . , , , , , , , , , , , , , , • , • , , , , , • , • • •
h If the organization received a contribution of cars, boats, airplanes, or other vehicles, did the organization file a form 1098-C? . , . , . , . , , , .. , , • , , , , , , ... , . , , • , , , , , .... , , , , . , , . , . ,
8 Sponsoring organizations maintaining donor advised funds, Did a donor advised fund maintained by the sponsoring organization have excess business holdings at any time during the year? , . . . , • . , , , . , . . . . , , , . , , . . .
9 Sponsoring organizations maintaining donor advised funds,
a Did the sponsoring organization make any taxable distributions under section 4966? . b Did the sponsoring organization make a distribution to a donor, donor advisor, or related person?,
10 Section 501 (c)(7) organizations. Enter:
Sa
Sb Sc
Sa
Sb
7g
7h
a Initiation fees and capital contributions Included on Part VIII, line 12 •.. , • , , . , , r-10_a-+---------,··,, b Gross receipts, included on Form 990, Part VIII, line 12, for public use of club facilities ..__10-'b_,_ ______ ---1
11 Section 501 (c){12) organizations. Enter: a Gross income from members or shareholders. . . . . , , , , . . , , , , , . , , , , 11 a
----------1°,c:,::ic.i. b Gross Income from other sources (Do not net amounts due or paid to other sources
against amounts due or received from them.) , , , , , , , , , , • , . , , , . . , , • ...__11"'-b"-'------------1 12a Section 4947(a)(1) non-exempt charitable trusts, Is the organizationjiling Form 990 In lieu of Form 1041?,
b If 'Yes,' enter the amount of tax-exempt interest received or accrued during the year . , , , , . .__12_b_,_ ______ --t•.
13 Section 501 (c)(29) qualified nonprofit health Insurance issuers. a Is the organization licensed to Issue qualified health plans In more than one state? . . , , , , . .
Note. See the Instructions for additional Information the organization must report on Schedule 0.
b Enter the amount of reserves the organization Is required to maintain by the states in which the organization Is licensed to issue qualified health plans • , , , , , , . , ... , , 13 b
c Enter the amount of reserves on hand , , , , , , , , .. , ..• , , , • , , , , , , .• , r-13-c-+----------1
14 a Did the organization receive any payments for Indoor tanning services during the tax year? ,
b If 'Yes,' has It flied a Form 720 to report these payments? If 'No,' provide an exp/anal/on In Schedule O, 14a
14b
Page 5
Yes No
X X
X
BAA TEEA0105 11/16/16 Form 990 (2016)

Form 990 (2016) NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 Page 6 I Part VI•:! Governance, Management, and Disclosure For each 'Yes' response to fines 2 through 7b below, and for
a 'No' response to line Ba, Bb, or 10b below, describe the circumstances, processes, or changes in Schedule 0. See instructions.
Yes No 1 a Enter the number of voting members of the governing body al the end of the tax year, 1 a
If there are material differences In voting rights among members ,____. _______ ___, of the ~overnlng body, or if the governing body delegated broad aulhonly lo an executive committee or similar committee, explain In Schedule 0.
b Enter \he number of voting members included In line 1 a, above, who are Independent .__1_b__,_ _______ 4 2 Did any officer, director, trustee, or key employee have a family relationship or a business relationship with any other
officer, director, trustee, or key employee? ... , ...... , ......••.... , .. , , . , , . , ... , .
3 Did the organization delegate control over management duties customarily performed by or under the direct supervision of officers, directors, or trustees, or key emplo_yees to a management company or other person? .... , , ... , ..
4 Did the organization make any significant changes to its governing documents since the prior Form 990 was filed? •• , , , . , , .•.. , .•.•••..• , , , , • , , , , , , , , •
5 Did the organization become aware during the year of a significant diversion of the organization's assets? 6 Did the organization have members or stockholders? . . . , • , . , . • . . . • , , • . • . . . . . , , . 7 a Did the organization have members, stockholders, or other persons who had the power to elect or appoint one or more
members of the governing body? • . • , • • . . . . . . . . • . • . • , . . . • , • , . • • . , . • .
b Are any governance decisions of the organization reserved lo (or subject to approval by) members, stockholders, or persons other than the governing body? . . , • . , • • • . • . . , . • . . • • • . . , . . , . , , , ,
8 Did the organization contemporaneously document the meetings held or written actions undertaken during the year by the following:
3
4 6 6
7a
7b
a The governing body? . . • • , , , . • . . . . , . . • . . . . • . . . • . , • • • . • . . . . • • . . . . . . . . 8 a X
b Each committee with authority lo act on behalf of the governing body? • . . • • . , , . . . , . • , , , . . , . . 8 b X
9 Is there any officer, director, trustee, or key employee listed in Part VII, Section A, who cannot be reached at the
X
X
X X
X
X
organization's mailing address? If 'Yes,' provide the names and addresses in Schedule O • • • . . , , 9 X
Section B. Policies This Section B re uests information about olicies not re uired b the Internal Revenue Code.
1 O a Did \he organization have local chapters, branches, or affiliates? .••• , •••• , .••..•••..•..••...
b If 'Yes,' did the organization l1ave written policies and procedures governing the activities of such chapters, afllllates, and branches to ensure their operations are consistent with the organization's exempt purposes?, , , • • , , . , • . , , . , • , , , , , . • ,
11 a Has the organization provided a complete copy of this Form 990 to all members of Its governing body before filing the form? , • , . . , , , , b Describe In Schedule O the process, If any, used by the organization to review this Form 990.
12 a Did the organization have a written conflict of interest policy? If 'No,' go to fine 13 . , . . . • . • . . . • . • . , . . b Were officers, directors, or trustees, and key employees required to disclose annually Interests thal could give rise
to conflicts 7 • , . , . , . , . , , . • . , , . , . , , • , . , , . , , • , , • • . . • • • , • • . , . . , , , , . •
c Did the organization regularly and consistently monitor and enforce compliance with the policy? If 'Yes,' describe in Schedule O how this was done . . • • , . • , • , . • • • . • , , . • • • . • •
13 Did the organization have a written whlstleblower policy? , • , , . . . . . . . . . . , • . . . . . • • • . . . . . • 14 Did the organization have a wril\en document retention and destruction policy? ••...• , .•••..... , ••
15 Did the process for determining compensation of lhe following persons Include a review and approval by independent persons, comparability dala, and contemporaneous substantiation of the deliberation and decision?
a The organization's CEO, Executive Director, or top management official ..• , • b Other officers or key employees of \he organization. . . • . • . • , • • • . . . . . • • • . . . . .
If 'Yes' to line 15a or 15b, describe the process in Schedule O (see Instructions). 16 a Did \he organization Invest In, contribute assets to, or participate in a joint venture or similar arrangement with a
Yes 10a
10b
11 a X
12a X
12b X
12c X 13 14 X
No
X
X
taxable entity during the year? . , • . . . . . . , • • • . . • . . . , . . . • . . . . . . . . . • . . . . . . . • . . . . , ,___,..,__,___
b If 'Yes,' did the organization follow a written policy or procedure requiring \he organization to evaluate its participation In Joint venture arrangements under applicable federal tax law, and take steps to safeguard the or anlzalion's exem t status with res ect to such arran ements?. . . . • . • • . . , . . . . • • . . . . . . • . . . , . . . ,
Section C. Disclosure 17 List lhe stales with which a copy of this Form 990 is required to be filed • See Form 990, Pa..11e 6, Line 171con\inued) , ________ _
18 Section 6104 requires an organization to make lls Forms 1023 (or 1024 if applicable), 990, and 990-T (Section 501(c)(3)s only) available for public Inspection. Indicate how you made these available. Check all that apply. ~ Own website O Another's website ~ Upon request O Other (explain in Schedule 0)
19 Describe in Schedule o whether (and if so, how) the organization made its governing documents, conflict of interest policy, and nnancial statements available to the public during the tax year.
20 Slate lhe name, address, and telephone number of \he person who possesses the organization's books and records: • Kelly Herzog 207 Palmetto Drive Edgewood MD 21040 (443) 922-7533
BAA TEEA0100 11/16/16 Form 990 (2016)

Form990(2016) NATIONAL EMERGENCY MEDICINE ASSOCIA'l'ION 52-1257429 Page7
I Part Vtl1 I Compensation of Officers, Directors, Trustees, Key Employees, Highest Compensated Employees, and Independent Contractors Check if Schedule O contains a response or note lo any line In this Part VII ....... , •..•.. , . , , , . , ....... , . IBJ
Section A. Officers, Directors, Trustees, Key Employees, and Highest Compensated Employees 1 a Complete this table for all persons required to be listed. Report compensation for the calendar year ending with or within the organization's tax year.
"' List all of the organization's current officers, directors, trustees (whether Individuals or organizations), regardless of amount of compensation. Enter -0- in columns (D), (E), and (F) if no compensation was paid.
• List all of the organization's current key employees, If any. See instructions for definition of 'key employee.' • List the organization's five current highest compensated employees (other than an officer, director, trustee, or key employee)
who received reportable compensation (Box 5 of Form W-2 and/or Box 7 of Form 1099-MISC) of more than $100,000 from the organization and-any related organizations.
0 List all of the organization's former officers, key employees, and highest compensated employees who received more than $100,000 of reportable compensation from the organization and any related organizations,
• List all of the organization's former directors or trustees that received, in.the capacity as a former director or trustee of the organization, more than $10,000 of reportable compensation from the organization and any related organizations. List persons in the following order: Individual trustees or directors; Institutional trustees; officers; key employees; highest compensated employees; and former such persons.
n Check this box ii neither the organization nor any related organization compensated any current officer, director, or trustee. (C)
(A) (B) Poslllon ~o not check more (D) (E) than one ox, unless person Name and TIiie Average Is both an officer and a Reportable Reportable
hours dlrectorllnJstee) compensation from compensellon from per
Is.~ ::, j :;,; (1) :c i the orgenlzallon related organl20llons
week ~ ..lg 3 -· (W-211099-MISC) (W.211099-MISC)
(11st any i~ i C,
~ m. '§-
hours for 9l !~ related fii "Q. SJ(
orn~~l;a- ~ ,Q below I i ~ i dolled line) (1)
* a.
_ (1) THOMAS BLAIR ______________ - ~ :..DJ) CHAIRPERSON X 0. o.
_(2)_HOWARD WEINERT ____________ -~:..DJ). DIRECTOR X 0, 0,
_(3)_SUZANNE LEVIN _____________ 2,00 SECRETARY X X 0, 0.
-~)_ PATJUCIA_BROOKHART _________ _ l ,_OJ) TREASURER X X o. o.
_(5)_KELLY HERZOG ______________ 35.00 PRESIDENT X X X X 127,950. o.
_(6)_LAURA PFISTER _____________ ..?l :..OJ), DIRECTOR X 20,450. o.
_Q)_ _______________________ ----·
_ (8)_ - - - - - - - - - - - - - - - - - - - - - - - ----· -~l _______________________
----·
(10)_ --- -- --- -- __ ------ _____ ----· (11) ___ _ ---- ___ -- ____ -- _ -- -- ----·
0~------------------------ ----·
(13)_ ---- _ --- -- ---- _ --- __ -- _ ----0~ ---------------------------BAA TEEA0107 11/16/16
(F) Esllmaled
amount of other compensallon
fromlhe organization and related
organlzallons
o.
0.
o.
o.
24,820,
182.
Form 990 (2016)

Form 990 (2016) NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 Page 8
I Part Vil :I Section A. Officers, Directors, Trustees Kev Emplovees, and Hi!:.lhest Compensated Employees (con//nued)
(B) (C) Posl\lon
(D) (E) (F) (A) Average (do not check more than one
Name and lille hours box, unless person Is both an Reportable Reportable Estimated per officer and a director/trustee) compensation from compensation rrom amount of other
week ~i j
the organlzaUon related organizations compensation (list any Q ~ ::l 0 ?: (W-2/1099-MISC) (W-2/1099-MISC) rromthe hours ~s \fl-, ~ ~ :g.::r organlzaUon
ror
~~ i ~ I i~ ~ end related related organizations o!~~~~za ~ i ~ l i below i dotted
line) "' gi
II ~SL _______________________ ----
(16) -------------------------- ----(17) -------------------------- ----(18) _______________________
----(19) -------------------------- ----(20) -------------------------- ----(21) -------------------------- ----
(22) -------------------------- ----(23) -------------------------- ----(24) -------------------------- ----(25) _______________________
----1 b Sub-total, , . , ................... . • 148 400, o. 25 002.
c Total from continuation sheets to Part Vil, Section A • dTotal(addlines1band1c),,.,,.,,,.,.,. • 148 400. 0. 25 002,
2 Total number of Individuals (Including but not limited to those listed above) who received more than $100,000 of reportable compensation from the organization • 1
... '.' . 3 Did the organization list any former officer, director, or trustee, key employee, or highest compensated employee on line 1 a? If 'Yes,' complete Schedule J for such individual • , . , • , . • • . . . . , . . • . , . . . , ...,..__,,.,,-.....----,,-,...._,
4 For any Individual listed on line 1a, is the sum of reportable compensation and other compensation from the organization and related organizations greater than $150,0007 If 'Yes,' complete Schedule J for such Individual , , • . . • • • . • . . , . . . . . , • . , , . , • . . . . , • , . , , , , . , , , . • • •
5 Did any person listed on line 1 a receive or accrue compensation from any unrelated organization or individual for services rendered to the or anizatlon? If 'Yes,' com lete Schedule J for such erson • . . . . . . , . . . · 5 X
Section B. Independent Contractors . 1 Complete this table for your five highest compensated independent contractors that received more than $100,000 of
compensation from the organization. Report compensation for the calendar year ending with or within the organization's tax year,
(A) Name and business address
(B) Description of services
(C) Compensation
He~POrt Creative Consultants 3 5 Railroad Ave Duxbury MA 02332 Karketinq and education materials productin 1,196,598.
2 Total number of Independent contractors (Including but not limited to those listed above) who received more than ·· · ··· i,: · •· .·. ·· $100,000 of compensation from the organization • 1 :t .. :.;i: ... . ,, ...
BAA TEEA0108 11/16/16 Form 990 (2016)

Form 990 (2016) NATIONAL EMERGENCY MEDICINE ASSOCIATION !Part VIII! Statement of Revenue
Check If Schedule O contains a response or note to any line In this Part VIII ,
b Membership dues . ,
c Fundralslng events .. d Related organizations e Government grants (contributions)
f All other contributions, gifts, grants, and similar amounts not incfuded above , ,
1 C
1 d
1 e
1 f g Noncash contributions included in lines 1a-1f: $ ______ _ h Tota I. Add lines 1 a-1 f • , , • , , , , . •
2a
(A) Total revenue
52-12574?.9
(C) Unrelated business
Page 9
...... • (D)
Revenue excluded from tax
under sections 512-514
------------------1-------1-__;_------+-------t--------+-------b ------------------1-------1--------+-------t--------+-------c ------------------1-------1-------+------+------+-------d ------------------1---------------+-------t--------+-------e ------------------1-----------------------------------f All other program service revenue , . . ...... ------1-------+,.,,...,.,....,.,.....,._,,.....,.,..,,;-.,,_.,.,..,,.,..._,.._,..,,_.+,,-,-,---,.....,-,..,..., g Total. Add lines 2a-2f , , . , , • , . , • , .... , ,•
3 Investment lncor:ne (Including dividends, Interest and other similar amounts) ....... , .. , .... .
6 a Gross rents b Less: rental expenses c Rental Income or (loss) , •
,•
(I) Real
d Net rental Income or (los~s'-) _. ------.------· -•+,,=----
7 a Gross amount from sales of assets other than inventory
b Less: cost or other basis and sales expenses ,
(I) Secunlles (II) Olher
c Gain or (loss) •.•
d Net gain or (loss) •. . ' ' ' ... ' ' . •
8 a Gross Income from fundralsing events (not Including. , $ ______ _ of contributions reported on line 1 c),
See Part IV, line 18, • , • , •. , . , a 1-------b Less: direct expenses . , • . . • . b'-------•··
. . ' ' . '• c Net Income or (loss) from fundralsing events . r------M===-=~=1~ 9 a Gross Income from gaming activities,
See Part IV, line 19, • . • . . , . . • a 1------b Less: direct expenses , , .... , , b~-----c Net Income or (loss) from gaming activities ... , ..• , •
r------+-,--,----,--,....,..-,..,.,,;,....,..,,..-,--.,-,-,----,-+--:c:-c,-c"'7""'"-:--,.,-,::+-:-c,---,..,,.,,,,----71 1 O a Gross sales of inventory, less returns
and allowances • . , • , . . • , . , a --------<
b Less: cost of goods sold , . . • • . . b.,_ _____ ~,~~--~---~~-~,., .... ,~~~~~---~-·~, c Net Income or (loss) from sales of Inventory
Miscellaneous Revenue Business Code
C -----------------------------------------------------d All other revenue . • • • , . . ,
e Total. Add lines 11a-11d, . , •
12 Total revenue. See Instructions BAA
. . • 2 ,,• 1444
TEEA0109 11/16/16

Form 990 (2016) NATIONAL EMERGENCY MEDICiNE ASSOCIATION 52-1257429 Page 10
Do not Include amounts reported on lines 6b, 7b, 8b, 9b, and 10b of Part Viii.
Grants and other assistance to domestic organizations and domestic governments, See Part IV, line 21 , • , .. , . , ••. ,
2 Grants and other assistance to domestic Individuals. See Part IV, line 22 . . . . • ,
3 Grants and other assistance to foreign organizations, foreign governments, and foreign Individuals. See Part IV, lines 15 and 16 ,
4 Benefits paid to or for members. , • , . , , 5 Compensation of current officers, directors,
trustees, and key employees , . , . , • ,
6 Compensation not Included above, to disqualified persons (as defined under section 4958(1)(1 )) and persons described in section 4958(c)(3)(8). , , , .....
7 Other salaries ,and wages, .. , .. , •
8 Pension plan accruals and contributions (Include section 401 (k) and 403(b) employer contributions) ..
9 Other employee benefits . . . , , . 1 O Payroll taxes , , , , , , , , . . . .
11 Fees for services (non-employees): a Management , b Legal. , , ,
c Accounting . . d Lobbying • • ,
e Professional fundralsing seNlces. See Part IV, line 17 f Investment management fees •.. , .. ,
(A) (B) (C) Total expenses Program service Management and
expenses general expenses
3 300, 3 300,
148 455. 89 454, 29 501.
3 036. 1 8 6. 610 22 454. 13 112. 4 671. 10 822. 6 478. 2 172,
13 740. 1 847. 10 592. 17 905. 0, 17 905.
4 715.
JD) Fun raising
expenses
29 500,
610. 4 671, 2 172,
1 301.. 0.
4 715,
g Other. (If line 11~ amount exceeds 10% of line 25, column (A) amount, list hne 11g expenses on Schedule O.) , . , 1---~"-"--(...,L"'""'--'-!----~ls.c4'-'--'3"'8"-1"'-'-. 1------~1=-'4"-'2"---'--' 1----------"-!.. 14 523. o.
12 Advertising and promotion • 13 Office expenses . . . . 14 Information technology ·. 15 Royalties • • 16 Occupancy . . . , . • , 17 Travel , , • • , . • , •
18 Payments of travel or entertainment expenses for any federal, state, or local public officials , , . , . , . . . • • • ,
19 Conferences, conventions, and meetings , 20 Interest, ........ , , , . , , .• ,
21 Payments to affiliates. . . . . , , • . • ,
22 Depreciation, depletion, and amortization, 23 Insurance , , , . • . . . , , . . . • . . 24 Other expenses, Itemize expenses not
covered above (List miscellaneous expenses In line 24e, If line 24e amount exceeds 10% of line 25, column (A) amount, list line 24e expenses on Schedule 0.) . , • , .•...
15 737, 1 799.
11 033.
2 760.
7 500, 6 910. 1 327, 1 799, o. 0,
6 621. 2 206. 2 206,
2 208, 276. 276,
a Da t_a l(roces s in,q_ _________ 4'"" ___ _.,_,.,_.,_.....,..,...,__.+----.k.<...,-..,.--"'-::t....L+----~~c:;,...."-'-1----L..J-.,-.,.,.~~ b List_ Costs _____________ ..}-___ ...,..;...,._:...u ....... +-----...,_,.,..,,...........,1---------'"'-'+-----'~'-'-"'""'-~
c Mailin,g_ Services _________ 4----.1..lL'1-f-.~.C,,...+----..::wc...,...,"'-"-.,_._+----.....,..,+-'-'-"'-"'-'-i---'---''-'-,-.,.,.::u..~ d Bank Fees ______________ ...,_ ___ _.........,_J..W.J.u....+--------'......YI-----......,+-'-''-"-''--'-+-------..:.~
e All other expenses • . , . • , . . • . , . ,
26 Total functional ex enses, Add lines 1 throu h 24e.
26 Joint costs. Complete this line only if the organization reported In column (B). Joint costs from a combined educational campaign and fundralslng solicitation. Check here • IB] if following SOP 98-2 ASC 958-720 , .. , , ...
BAA
1 001 610. 1 482 867.
1 473 506, TEEA0110 11/16/16
747 525, 3 134. 250 951. 972 700. 143 898. 366 269,
967 673, 141 061, 364 772. Form 990 (2016)

Form 990 2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION
PartX < Balance Sheet
(/l
-m ~-~
(/l
:~ r= .0 (IJ
::i
(/l
~ C (IJ
iii co 'ti § u. .. 0 $ w
:R .... C1) z
BAA
Check if Schedule O contains a response or note to any line in this Part X ,
Cash - non-interest-bearing , , , , , , ,
2 Savings and temporary cash Investments 3 Pledges and grants receivable, net,· , . , 4 Accounts receivable, net . , . , . , . . ,
6 Loans and other receivables from current and former officers, directors, ~~~t1i8gt ~~hi~f!o~e.e~, ~~d .hl.g~e~t_c?IT;P~~s~t~d. e_m~l~y.e~s: ~o.m~l~t~ .
6 Loans and other receivables from other disqualified persons (as defined under section 4958(1)(1)), persons described In section 4958(c)~3)t, and contributing employers and sponsoring organizations of section 501 (c (9 volunta~ employees' beneficiary organizations (see Instructions). Complete Part I of Sche ule L . . . .
7 Noles and loans receivable, net I I Io t
8 Inventories for sale or use , . , ..•. , , . , . ,
9 Prepaid expenses and deferred charges . . . • . •
10a Land, buildings, and e;\;1\pment: cost or other basis. Complete Part VI of Sc edule O , , , , . , • . . • 10a 8 572.
b Less: accumulated depreciation . , .. , •.••• 10 b 5 564. 11 Investments - publicly traded securities . . . . . .
12 Investments - other securities. See Part IV, line 11
13 Investments - program-related. See Part IV, line 11
14 Intangible assets , , •. , .••.......•..•..
16 other assets. See Part IV, line 11 IO I• 0 IO O • 0 0 0
16 Total assets. Add lines 1 throu h 15 must e ua\ line 34 17 Accounts payable and accrued expenses. 18 Grants _payable. . . . . . . 19 Deferred revenue 0 0 0 0 o O I• 0 t t I
20 Tax-exempt bond \lablllt\es , .•• , ...
21 Escrow or custodial account liability. Complete Part IV of Schedule o 22 Loans and other payables to current and former officersd directors, trustees,
key employees, hl~hest compensated employees, and isqua\ified persons . Complete Part II o Schedule L •...••..•• ·, ......•••.•.
23 Secured mortgages and notes payable to unrelated third parties ......
24 Unsecured notes and loans payable to unrelated third parties 0 I I I IO 0
25 Other liabilities (Including federal Income tax, payables to related third parties, and other llabilitIes not included on lines 17-24). Complete Part X of Schedule D ••
26 Total liabilities. Add lines 17 through 25. , , • , , ..•..•..•.••..•.
Organizations that follow SFAS 117 (ASC 968), check here • g)and complete lines 27 through 29, and \Ines 33 and 34.
27 Unrestricted net assets. . . . , .
28 Temporarily restricted net assets .
29 Permanently restricted net assets
Organizations that do not follow SFAS 117 (ASC 958), check here • 0 and complete lines 30 through 34 .
30 Capital stock or trust principal, or current funds, . , , •.. , .•.••
31 Paid-In or capital surplus, or land, building, or equipment fund .•..
32 Retained earnings, endowment, accumulated income, or other funds. 33 Total net.assets or fund balances, ••.•..
34 Total llabllttles and net assets/fund balances ... , .........
TEEA0111 11/16/16
52-1257429
(A) Beginning of year
129 110.
4 723. 25 850,
92 339. 275 812. 392 501.
-116 689. 275 812.
2
10c
11 12 13
14
16 16 17 18 19
20
22
23 24
25
30 31
32 33
34
Pa e 11
(B) End of year
168 421.
3 008, 27 100,
91 568. 304 154, 458 593.
-154 439. 304 154.
Form 990 (2016)

Form 990 (2016) NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 Page 12
!'Partxi<I Reconciliation of Net Assets Check If Schedule o contains a response or note lo any line In this Part Xi. .n
1 Total revenue (must equal Part VIII, column (A), line 12) 1 1 444 408. 2 Total expenses (must equal Part IX, column (A), line 25) 2 1 482 867. 3 Revenue less expenses. Subtract line 2 from line 1 . 3 -38 459, 4 Nel assets or fund balances al beginning of year (must equal Part X, line 33, column (A)). 4 -.116 689. 5 Net unrealized gains (losses) on Investments. 6 709. 6 Dona led services and use of facilities. ., 6 7 Investment expenses . 7 8 Prior period adjustments . 8 9 Other changes In net assets or fund balances (explain in Schedule O) 9
10 Net assets or fund balances at end of year. Combine lines 3 through 9 (must equal Part X, line 33, column (B)). . . . . . , . . . . . . . . . . • . . . . . 10 -154 439,
I PartXll I Financial Statements and Reporting
Check If Schedule O contains a response or note to any line In this Part Xii ........................ .
Accounting method used lo prepare the Form 990: •cash (ill Accrual Oother
If the organization changed Its method of accounting from a prior year or checked 'Other,' explain In Schedule 0.
2 a Were the organization's financial statements complied or reviewed by an Independent accountant?.
If 'Yes,' check a box below lo Indicate whether the financial statements for the year were compiled or reviewed on a s~arate basis, consolidated basis, or both: LJ Separate. basis Oconsolldated basis Osoth consolidated and separate basis
Yes No
' ... '' ,-....-1----1----
b Were the organization's financial statements audited by an Independent accountant? . • . . . . . • . . . . . . . . , . . , i-_,__..__ if 'Yes,' check a box below lo Indicate whether the financial statements for the year were audited on a separate basis, consol\dated basis, or both: D Separate basis [ill Consolidated basis D Both consolidated and separate basis
c If 'Yes' to line 2a or 2b, does the organization have a committee that assumes respons\bll\ly for oversight of the audit, review, or compliallon of Its financial statements and selection of an Independent accountant? ..•..•.• , •.•
if the organization changed either Its oversight process or selection process during the tax year, explain in Schedule 0,
3 a As a result of a federal award, was the organization required to undergo an audit or audits as set forth In the Single Audit Act and 0MB Circular A--133?, ..........•.....•.........••......•.....
b If 'Yes,' did the organization undergo the required audit or audits? If the organization did not undergo the required audit or audits, ex lain wh In Schedule 0 and describe an ste s taken to under o such audits . . . . . . • . . . . . . , .
BAA
TEEA0112 11/16/16
3a X
3b Form 990 (2016)

SCHEDULE A (Form 990 or 990-EZ)
Public Charity Status and Public Support Complete If the organization Is a section 501(c)(3) organization or a section
4947(a)(1) nonexempt charitable trust.
0MB No. 1545-0047
2016 . •. •' ',,'.
Department of the Treasury Internal Revenue Service
• Attach to Form 990 or Form 990-EZ.
• Information about Schedule A (Form 990 or 990-EZ) and Its Instructions Is at www.lrs.gov/form990,
Qpen tp. F?ubUq ·, •. . lnspectloh . ,•:·,: •.· .
Name of the organlrntlon I Employer ldent!Ocatlon number
NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 )Partl I Reason for Public Charity Status (All organizations must complete this part.) See instructions. The organization Is not a private foundation because It ls: (For lines 1 through 12, check only one box.)
2 A school described In section 170(b)(1)(A)(ll). (Attach Schedule E (Form 990 or 990-EZ).) 3 A hospital or a cooperative hospital service organization described In section 170(b)(1)(A)(III).
1 ~ A church, convention of churches, or association of churches described in section 170(b)(1)(A)(I).
4 A medical research organization operated In conjunction with a hospital described In section 170(b)(1 )(A)(III). Enter lhe hospital's name, city, and state:
5 0 An organization operated for the benefit of a college or university owned or operated by a governmental unit described In section 170(b)(1 )(A)(lv). (Complete Part II.)
6 0 A federal, state, or local government or governmental unit described In section 170(b)(1)(A)(v). 7 59 An organization that normally receives a substantial part of Its support from a governmental unit or from the general public described
In section 170(b)(1)(A)(vi). (Complete Part II.)
8 0 A community trust described In section 170(b)(1)(A)(vl), (Complete Part II.)
9 O An agricultural research organization described In section 170(b)(1)(A)(ix) operated In conjunction with a land-grant college or university or a non-land-grant college of agriculture (see Instructions). Enter the name, city, and state of the college or university: _________________________________________________________ _
10 0 An organization that normally receives: (1) more than 33-113% of its support from contributions, membership fees, and gross receipts from activities related to Its exempt functions-subject to certain exceptions, and (2) no more than 33-113% of Its support from gross Investment income and unrelated business taxable Income (less section 511 tax) from businesses acquired by the organization after June 30, 1975. See section 509(a)(2). (Complete Part Ill.)
11 D An organization organized and operated exclusively to test for public safety, See section 509(a)(4).
12 0 An organization organized and operated exclusively for the benefit of, to perform the functions of, or to carry out the purposes of one or more publicly supported organizations described In section 509(a)(1) or section 509(a)(2), See section 509(a)(3). Check the box in lines 12a through 12d that describes the type of supporting organization and complete lines 12e, 12f, and 12g.
A
B
C
D
E
a O Type 1. A supporting organization operated, supervised, or controlled by Its supported organizatlon(s), typically by giving the supported organlzation(s) the power to regularly appoint or elect a majority of the directors or trustees of the supporting organization. You must complete Part IV, Sections A and B.
b O Type II. A supporting organization supervised or controlled in connection with Its su1ported organizatlon(s), by having control or management of the supportln~ organization vested In the same persons that contra or manage the supported organlzation(s). You must complete Part IV, Sections A and C,
c O Type Ill functionally Integrated. A supporting organization operated In connection with, and functionally Integrated with, Its supported organiza\lon(s) (see Instructions). You must complete Part IV, Sections A, D, and E.
d O Type Ill non-functionally Integrated, A supporting organization operated In connection with Its supported organizatlon(s) that is not functionally integrated. The organization generally must satisfy a distribution requirement and an attentiveness requirement (see Instructions). You must complete Part IV, Sections A and D, and Part V.
e O Check this box if the organization received a written determination from the IRS that It is a Type I, Type II, Type Ill functionally Integrated, or Type Ill non-functionally Integrated supporting organization.
f Enter the number of supported organizations . , , . , . , ........ . g Provide the following information about the supported organization(s).
(I) Name of supported organization (ti) EIN (Ill) Type of organlzaUon (described on lines 1-10 above (see Instructions))
(Iv) Is the organization listed In your governing
document?
Yes No
(v) Amount of monetary support (see Instructions)
(vi) Amount of other support (see instructions)
Total
BAA For Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990-EZ, · TEEA0401 09/28/16
Schedule A (Form 990 or 990-EZ) 2016

Schedule A (Form 990 or 990-EZ) 2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257 42 9
IParrn lsupport Schedule for Organizations Described In Sections 170(b)(1)(A){iv) and 170(b)(1)(A)(vi) (Complete only If you checked the box on line 5, 7, or 8 of Part I or if the organization failed lo qualify under Part Ill. If the organization falls to qualify under the tests listed below, please complete Part Ill.)
Section A, Public Support
Calendar year (or fiscal year beginning In) • (a) 2012 (b) 2013 (c) 2014 (ct) 2015 (e) 2016
Page 2
(f) Total
1 Gifts, grants, contributions, and membership fees received. [Do not include any 'unusual grants,') , , , • 1 368 940. 1 525 120. 1 123 297. 876 558. 1 422 709, 6 316 624.
2 Tax revenues levied for the organization's benefit and either paid to or expended on Its behalf , , . . . ,
3 The value of services or facilities furnished by a government_a\ unit to the ·organization without charge,
4 Total. Add lines 1 through 3
5 The portion of total contributions by each person (other than a governmental unit or publicly supported organization)· Included on line 1 that exceeds 2% of the amount shown on line 11, column (f) , •
6 Public support. Subtract line 5 from line 4 . , , , , , , • •
Section 8. Total Support
Calendar year (or fiscal year beginning In) •
7 Amounts from line 4 • ,
8 Gross Income from Interest, dividends, payments received on securities loans, rents, royalties and Income from similar sources . . . . , . , .
9 Net income from unrelated business activities, whether or not the business is regularly carried on , . • . • • , , , ,
10 Other income. Do not Include gain or loss from the sale of capita\ assets (Explain In PartVI.) ... , , , , , . ,
11 Total support, Add lines 7 through 1 o , , , . . , , , ,
12
(a) 2012 (b) 2013 (c) 2014 (d) 2015 (e) 2016
l 368,940. 1,525,120, 1 123 297, 876 558. 1 422,709,
3. 6. 315. 828, 574,
13 First five years. If the Form 990 Is for the organization's first, second, third, fourth, or fifth tax year as a section 501 (c)(3) organization, check this box and stop here. . . , . , , . . . , , , . , . . , . . , , , , . . . , . . , . . . . . . . . . , ,
Section C. Computation of Public Support Percentage
6 316 624.
6 316 624,
(f) Total
6 316 624,
1 726.
14 6 451.
6 464,801.
'. '. •
14 Public support percentage for 2016 (line 6, column (0 divided by line 11, column (D) >-1_4 __ ~9~7~·~7~1~%_
15 Public support percentage from 2015 Schedule A, Part II, line 14 . , , •. , , , , , '-'-1..;..5_.__-"9'-'7....,.~4'--"8'--%-
16a 33-1/3% support test-2016, If the organization did not check the box on line 13, and line 14 ls 33-1/3% or more, check this box and stop here. The organization qualifies as a publicly supported organization •. , , , ... , . , , , , . , , , , , , , , , , , ,• ~
b 33-1/3% support test-2015. If the organization did not check a box on line 13 or 16a, and line 15 Is 33-1/3% or more, check this box D and stop here. The organization qualifles as a publicly supported organization , , , , , , , . , , , , . , , , , , , , , , , , , , , , , , •
r
17a 10%-facts-and-clrcumstances test-2016, If the organization did not check a box on line 13, 16a, or 16b, and line 14 ls 10% or more, and If the organization meets the 'facts-and-circumstances' test, check this box and stop here. Explain in Part VI how D the organization meefs the 'facts-and-circumstances' test. The organization qualifies as a publicly supported organization , . , , , , .•• •
b 10%-facts-and-clrcumstances test-2015. If the organization did not check a box on line 13, 16a, 16b, or 17a, and line 15 is 10% or more, and If the organization meets the 'facts-and-circumstances' test, check this box and stop here. Explain In Part VI how the
8 organization meets \lie 'facts-and-circumstances' test. The organization qualifies as a publicly supported organization . , , • . . , • , , , • . 18 Private foundation. If the organization did not check a box on line 13, 16a, 16b, 17a, or 17b, check this box and see Instructions , .. , , •
BAA Schedule A (Form 990 or 990-EZ) 2016
TEEA0402 09/28/16

Schedule A (Form 990 or 990-EZ) 2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1.257 4 2 9
!Part Ill ;!support Schedule for Organizations Described in Section 509(a)(2) (Complete only \fyou checked the box on line 10 of Part I or If the organlza\lon failed to qualify under Part II. If the organization fails to qualify under the tests listed below, please complete Part II.)
Section A. Public Support
Page 3
Calendaryear(orfiscalyearbeglnning in) • (a) 2012 (b) 2013 {c) 2014 (d) 2015 (e) 2016 (f) Total 1 Gifts, grants, contrlbu\lons, f----'-'-------ie---'--'-----t---'-~---1--~----+---~-----t-------
and membership fees received. (Do not include any 'unusual grants.') , , , , , •
2 Gross receipts from admissions, merchandise sold or services performed, or facllltles furnished in any activity that is related to the organization's tax-exempt purpose , , , , •
3 Gross receipts from activities that are not an unrelated trade or business under section 513
4 Tax revenues levied for the organization's benefit and either paid to or expended on Its behalf . . , . • . , ,
5 The value of services or facilities furnished by a governmental uni\ to the organization without charge.
6 Total. Add lines 1 through 5 7a Amounts Included on lines 1,
2, and 3 received from disqualified persons . • • . ,
b Amounts Included on lines 2 and 3 received from other than disqualified persons that exceed the greater of $5,000 or 1 % of the amount on line 13 for the year. . • • • , , , . ,
c Add lines 7a and 7b • . , , ,
8 Public support. (Subtract line 7cfromllne6,),., .....
S I BTtlS ect on o a uooort Calendar year (or fiscal year beginning in) •
9 Amounts from line 6 '' ' ... 10a Gross income from interest, dividends,
paymonts roceived on securities loans, rents, royalties and income from similar sources , , • , • • • . ''
b Unrelated business taxable Income (less section 511 taxes) from businesses acquired after June 30, 1975 .
c Add lines 10a and 10b . , , . 11 Net income from unrelated business
acllvllles not included In line 1 Ob, whether or not the business Is regularly carried on • . . . , • .
12 Other income. Do not Include gain or loss from the sale of capital assets (Explain In Part VI.) . , . . , , , , . , ,
13 Total support. fdd lines 9, 1 0c, 11, and 12, . , • , , . ,
(a) 2012 (b) 2013 (c)2014 (d) 2015 (e) 2016 (f} Total
14 First five years. If the Form 990 Is for the organization's first, second, third, fourth, or fifth tax year as a section 501 (c)(3) ......... • n ornanlzation, check this box and stop here. , •... , , • , .. , , • , ..• , . , , • , •• , .• , . , , , . , , • ,
Section C. Com utation of Public Su ort Percenta e 16 Public support percentage for 2016 (line 8, column(!) divided by line 13, column(!)) 15 % 16 Public support percentage from 2015 Schedule A, Part Ill, line 15 •••• , • . • • • 16 %
Section D. Computation of Investment Income Percentage 17 Investment income percentage for 2016 (line 10c, column(!) divided by line 13, column (f}), , ••.••.• , •. , • , 17 %
18 Investment Income percentage from 2015 Schedule A, Part Ill, line 17 . . • • . . • . • . . . . . . . • . . • • • . . . 18 % 19a 33-1/3% support tests-2016, If the organization did not check the box on line 14, and line 15 Is more than 33-1/3%, and line 17
Is not more than 33-1/3%, check this box and stop here. The organization qualifies as a publicly supported organization . . . . . • • 0 b 33-1/3% support tests-2015. If the organization did not check a box on line 14 or line 19a, and line 16 is more than 33-1/3%, and
line 18 is not more than 33-1/3%, check this box and stop here. The organization qualifies as a publicly supported organization • • . • 20 Private foundation. If the organization did not check a box on line 14, 19a, or 19b, check this box and see Instructions, , , , , , . , •
BAA TEEA0403 09128116 Schedule A (Form 990 or 990-EZ) 2016

Schedu\eA(Form990or990-EZ)2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 Page4
!Part IV· j Supporting Organizations (Complete only if you checked a box in line 12 on Part I. If you checked 12a of Part I, complete Sections A and B, If you checked 12b of Part I, complete Sections A and C. If you checked 12c of Part I, complete Sections A, D, and E. If you checked 12d of Part I, complete Sections A and D, and complete Part V.)
Section A. All Supporting Organizations
Are all of the organization's supported organizations listed by name In the organization's governing documents? If 'No,' describe In Part VI how the supported organizations are designated. If designated by class or purpose, describe the designation, If historic and conl/numg relationship, explain.
2 Did the organization have any supported organization that does not have an IRS determination of status under section 509(a)(1) or (2)7 if 'Yes,' explain in Part VI how the organization determined that the supported organiza/lon was described in sec/Ion 509(a)(1) or (2),
3a Did the organization have a supported organization described in section 501 (c)(4), (5), or (6)7 If 'Yes,' answer (b) and (c) below,
b Did the organization confirm that each supported organization qualified under section 501(c)(4}, (5), or (6) and satisfied the public support tests under section 509(a)(2}7 If 'Yes,' describe In Part VI when and how the organize/Ion made the determination.
c Did the organization ensure that all support to such organizations was used exclusively for section 170(c)(2)(8) purposes? If 'Yes,' explain In Part VI what controls the organization put In place to ensure such use,
4a Was any supported organization not organized in the United States ('foreign supported organization')? If 'Yes' and If you checked 12a or 12b in Part I, answer (b) and (c) below,
b Did the organization have ultimate control and discretion in deciding whether to make grants to the foreign supported organization? If 'Yes,' describe in Part VI how the organization had such control and discretion despite being controlled or supervised by or In connec/lon with its supported organizations,
c Did the organization support any foreign supported organization that does not have an IRS determination under sections 501(c)(3) and 509(a)(1) or (2)? If 'Yes,' explain in Part VI what controls the organization used to ensure that all support to the foreign supported organization was used exclusively for section 170(c)(2)(B) purposes,
Sa Did the organization add, substitute, or remove any supported organizations during the tax year? If 'Yes,' answer /b) and (c) below (If applicable), Also, provide detail In Part VI, including (i) the names and EIN numbers of the supported organizations added, substituted, or removed; (ii) the reasons for each such action; (///) the authority under the organization's organizing document authorizing such action; and (Iv) how the action was accompllshed (such as by amendment to the organizing document),
b Type I or Type II only. Was any added or substituted supported organization part of a class already designated In the organization's organizing document?
c Substitutions only. Was the substitution the result of an event beyond the organization's control?
6 Did the organization provide support (whether in the form of grants or the provision of services or facilities) to anyone other than (I) Its supported organizations, (ii) Individuals that are part of the charitable class benefited by one or more of Its supported organizations, or (Ill) other supporting organizations that also support or benefit one or more of the filing organization's supported organizations? If 'Yes,' provide detail In Part VJ.
7 Did the organization provide a grant, loan, compensation, or other similar payment to a substantial contributor (defined in section 4958(c)(3)(C}}, a family member of a substantial contributor, or a 35% controlled entity with regard lo a substantial contributor? If 'Yes,' complete Part I of Schedule L (Form 990 or 990-EZ).
s Did the organization make a loan to a disqualified person (as defined in section 4958) not described in line 7? If 'Yes,' complete Part I of Schedule L (Form 990 or 990-EZ),
9a Was lhe organization controlled directly or indirectly at any time during the tax year by one or more disqualified persons as defined in section 4946 (other than foundation managers and organizations described In section 509(a)(1) or (2))7 If 'Yes,' provide detail In Part VJ,
b Did one or more dls~ualified persons (as defined In line 9a) hold a controlling interest In any entity in which the supporting organization had an interest? If 'Yes,' provide detail in Part VI.
c Did a disqualified person (as defined In line 9a) have an ownership Interest In, or derive any personal benefit from, assets In which the supporting organization also had an interest? If 'Yes,' provide detail In Part VJ,
1 0a Was the organization subject to the excess business holdings rules of section 4943 because of section 4943(!) (regarding certain Type II supporting organizations, and all Type Ill non-funcllonally Integrated supporting organizations)? If 'Yes,' answer 10b below,
b Did the organization have any excess business holdings In the lax year? (Use Schedule C, Form 4720, to determine whether the organization had excess business holdings.) 1 Ill
Yes No
BAA TEEA0404 09128116 Schedule A (Form 990 or 990-EZ) 2016

Schedule A (Form 990 or 990-EZ) 2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 !Part IV· 1 Suooortina Oraanizations (continued)
11 Has the organization accepted a gift or contribution from any of the following persons?
a A person who dlreclly or indirectly controls, either alone or together with persons described in (b) and (c) below, lhe governing body of a supported organization?
b A family member of a person described in (a) above?
c A 35% controlled entity of a person described In (a) or (b) above? /f 'Yes' to a, b, or c, provide detail in Part VI.
Section B. T
Did the directors, trustees, or membership of one or more supported organizations have the power to regularly appoint or elect al least a majority of the organization's directors or trustees al all limes during the tax year? If 'No,' describe in Part VI how the supported organization(s) effectively operated, supe!Vised, or controlled the organization's activities, If the organization had more than one supported organization, describe how the powers to appoint and/or remove directors or trustees were allocated among the supported organizations and what cond/1/ons or restrictions, if any, applied to such powers during the tax year.
2 Did the organization operate for the benefit of any supported organization other than the supported organlzatlon(s) that operated, supervised, or controlled the supporting organization? If 'Yes,' explain in Part VI how providing such benefit carried out the purposes of the supported organizatlon(s) that operated, supe1Vised, or controlled the supporting organization.
Section C. Type II Sup orting Organizations
Were a majority of lhe organization's directors or trustees during the tax year also a majority of the directors or trustees of each of the organization's supported organlzatlon(s)? If 'No,' describe in Part VI how control or management of the su ortin or anizat/on was vested in the same ersons that controlled or mana ed the su orted or anization s .
Section D. All Type HI Supporting Organizations
Did the organization provide to each of Its supported organizations, by the last day of the fifth month of-the organization's tax year, (i) a written notice describing the type and amount of support provided during the prior tax year, (Ii) a copy of the Form 990 lhat was most recently flied as of lhe dale of notification, and (Ill) copies of the organization's governing documents In effect on the date of notification, to the extent not previously provided?
2 Were any of the organization's officers, directors, or trustees either (I) appointed or elected by the supported organlzatlon(s) or (ii) serving on the governing body of a supported organization? /f 'No,' explain in Part VJ how the organization maintained a close and continuous working relationship with the supported organization(s).
3 By reason of the relationship described In (2), did the organization's supf orted organizations have a significant voice In the organization's investment policies and In directing the use o the organization's income or assets at all times during lhe tax year? If 'Yes,' describe In Part VI the role the organization's supported organizations played In this regard.
Section E. Type ill Functionally Integrated Supporting Organizations
1 Check the box next to the method that the organization used to satisfy the Integral Part Test during the year (see instructions).
a D The organization satisfied \he Activities Test. Complete line 2 below.
b D The organization Is the. parent of each of its supported organizations, Complete line 3 below.
-···---'~,
11a
11b
11c
3
c D The organization supported a governmental entity. Describe In Part VI how you supported a government entity (see Instructions),
2 Activities Test. Answer (a) and (b) below.
a Did substantially all of the organization's activities during the tax year directly further the exempt purposes of the supported organlzatlon(s) to which the organization was responsive? If 'Yes,' then In Part VI identify those supported organizations and explain how these activities directly furthered their exempt purposes, how the organization was responsive to those supported organizations, and how the organization determined that these activities constituted substantially all of its activities.
b Did the activities described in (a) constitute activities that, but for the organization's Involvement, one or more of the organization's supported organization(s) would have been engaged In? If 'Yes,' explain In Part VI the reasons for the organization's position that its supported organ/zatlon(s) would have engaged in these activities but for the organization's Involvement.
3 Parent of Supported Organizations. Answer (a) and (b) below.
a Did lhe organization have the power to regularly appoint or elect a majority of the officers, directors, or trustees of each of the supported organizations? Provide details in Part VI.
b Did the organization exercise a substantial degree of direction over the policies, programs, and activities of each of Its supported organizations 7 if 'Yes,' describe in Part VJ the role played by the organization in this regard, 3b
Page 5
Yes No . - ': .. ~. : ;~cLJ
Yes No
BAA TEEA0405 09/28/16 Schedule A (Form 990 or 990-EZ) 2016

Schedule A (Form 990 or 990-EZ) 2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 Page 6
IPartV I Type Ill Non-Functionally Integrated 509(a)(3) Supporting Organizations
0 Check here If the organization satisfied the Integral Part Test as a qualifying trust on Nov. 20, 1970 (explain In Part VI). See Instructions. All other Type Ill non-functionally Integrated supporting organizations must complete Sections A through E.
Section A - Adjusted Net Income
Net short-term capital gain
2 Recoveries of prior-year distributions
3 Other gross Income (see Instructions)
4 Add lines 1 throu h 3,
5 Oepreciallon and depletion
6 Portion of operating expenses paid or Incurred for production or collecllon of gross Income or for management, conservation, or maintenance of property held for production of Income (see Instructions)
7 Other expenses (see Instructions)
8 Ad usted Net Income subtract lines 5, 6, and 7 from line 4 .
Section B - Minimum Asset Amount
1 Aggregate fair market value of all non-exempt-use assets (see Instructions for short tax year or assets held for part of year):
a Average monthly value of securities
b Average monthly cash balances
c Fair market value of other non-exempt-use assets
d Total (add lines 1a, 1b, and 1c)
e Discount claimed for blockage or other factors (explain In detail In Part VI):
2 Acquisition indebtedness applicable to non-exempt-use assets 3 Subtract line 2 from line id.
4 Cash deemed held for exempt use. Enter 1-1/2% of line 3 (for greater amount, see Instructions),
5 Net value of non-exempt-use assets (subtract line 4 from line 3)
6 Multiply line 5 by ,035,
7 Recoveries of prior-year distributions
8 Minimum Asset Amount (add line 7 to line 6)
Section C - Distributable Amount
Adjusted net Income for prior year (from Section A, line 8, Column A)
2 Enter 85% of line 1.
3 Minimum asset amount for rior ear from Secllon B, line 8, Column A
4 Enter realer of line 2 or line 3,
6 Income tax imposed in prior year
6 Distributable Amount. Subtract line 5 from line 4, unless subject to emergency temporary reduction (see Instructions),
(A) Prior Year
2
3
4
5
6
7
8
(A) Prior Year
2 3
4
5
6
7
8
2
3 4
5
6
7 Check here if the current year Is the organization's first as a non-functionally integrated Type Ill supporting organization see Instructions ,
(B) Current Year (opllonal)
(B) Current Year (optional)
Current Year
BAA Schedule A (Form 990 or 990-EZ) 2016
TEEA0406 09/28/16

52-1257429 Page 7
Section D - Distributions Current Year
Amounts paid to supported organizations to accomplish exempt purposes
2 Amounts paid lo perform activity that directly furthers exempt purposes of supported organizations, in excess of income from activity
4 Amounts paid lo acquire exempt-use assets 5 Qualified set-aside amounts (prior IRS approval required) 6 Other distributions (describe In Part VI). See instructions. 7 Total annual distributions. Add lines 1 lhrough 6.
8 Distributions to attentive supported organizations to which the organization Is responsive (provide details In Part Vt). See Instructions.
9 Distributable amount for 2016 from Section C, line 6
1 O Line 8 amount divided by Line 9 amount
Section E - Distribution Allocations (see instructions}
Distributable amount for 2016 from Section C, line 6
2 Underdis\ributlons, If any, for years prior to 2016 (reasonable cause required - explain In Part VI). See instructions.
d From 2014 .
e From 2015 .
f Total of lines 3a through e
g Applied lo underdlstrlbullons of prior years
h Applied lo 2016 distributable amount
I Car over from 2011 no\ a lied see Instructions
Remainder. Subtract lines 3 , 3h, and 31 from 31.
4 Distributions for 2016 from Section D, line 7: $
a Applied to underdistribulions of prior years
b A lied to 2016 distributable amount c Remainder. Subtract lines 4a and 4b from 4.
5 Remaining underdlstrlbutions for years prior lo 2016, If any. Subtract lines 3g and 4a from line 2, For result greater than zero, ex lain In Part VI. See Instructions.
6 Remaining underdlstrlbutlons for 2016. Subtract lines 3h and 4b from line 1. For result greater than zero, explain In Part VI. See Instructions.
7 Excess distributions carryover to 2017. Add lines 3] and 4c.
8
c Excess from 2014
d Excess from 2015
e Excess from 2016 BAA
(i) Excess
Distributions
TEEA0407 09/28/16
(II) Underdlstrlbutlons
Pre-2016
(Ill) Distributable
Amount for 2016
Schedule A (Form 990 or 990-EZ) 2016

Schedule A (Form 990 or 990-EZ) 2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-12 57 429 Page 8
I Part VI cjsupplem,ental Information. Provide the BJmlanations required by Part )11 line 10; Par:\ II, line 17a ?r 17br·Part Ill,. line 1 ~; Pa~ IV, Sec lion A, lines 1, 2, 3b, 3c, 4b, 4c, 5a, 6, 9a, 9b, gc, 11 a, 11 b, and 11 c, Part Iv, Section B, lines 1 and 2, Part V, Section C, line 1, Part IV, Section D, lines 2 and 3; Part IV, Section E, lines 1c, 2a, 2b, 3a, and 3b; Part V, line 1; Part V, Section B, line 1e; Part V, Section D, lines 5, 6, and B; and Part V, Section E, lines 2, 5, and 6, Also complete this part for any add\lional Information. (See instructions,)
Pt II Ln 10 Other Income Part II, Line 10 Description: Mail List Rentals 2012: 24038, 2013: 26653, 2014: 41347, 2015: 33288, 2016: 21125, Description:
BAA
Sale of Inventory 2012: 0, 2013: 0. 2014: 0, 2015: 0. 2016: 0, Description: Miscellaneous 2012: 0. 2013: 0, 2014: 0. 2015: 0. 2016: 0,
TEEA0408 09/28/16 Schedule A (Form 990 or 990-EZ) 2016

SCHEDULED (Form 990)
Supplemental Financial Statements • Complete If the organization answered 'Yes' on Form 990,
Part IV, line 6, 7, B, 9, 10, 11a, 11b, 11c, 11d, 11e, 11f, 12a, or 12b.
0MB No. 1645-0047
2016 Department of the Treasury Internal Revenue Service
• Attach to Form 990, 1,: Open to Public . . ;
• Information about Schedule D (Form 990) and Its Instructions Is at www.irs.gov/form990. •.·· Inspection - • . • Name of tho organltntfon Employer loenlfficatlon nurnber
NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 !Part I I Organizations Maintaining Donor Advised Funds or Other.Similar Funds or Accounts.
Complete if the organization answered 'Yes' on Form 990, Part IV, line 6. (a) Donor advised funds (b) Funds and other accounts
1 Total number at end of year t O I• I I
2 Aggregate value of contributions to (during year) 3 Aggregate value of grants from (during year) 4 Aggregate value at end of year . , . . .
5 Did the organization Inform all donors and donor advisors In writing that the assets held In donor advised funds are the organization's property, subject to lhe organization's exclusive legal control? , . , , . , .. , ..... , 0Yes
6 Did the organization inform all grantees, donors, and donor advisors In writing that grant funds can be used only for charitable purposes and not for the benefll of the donor or donor advisor, or for any other purpose conferring impermissible private benefit? ... , ... , .. , .... , . , •.• , .... , ...•.•....... , . Yes No
Pa'i ·• ,: Conservation Easements. Complete if the organization answered 'Yes' on Form 990, Part IV, line 7.
Purpose(s) of conservation easements held by lhe organization (check all \hat apply).
§ Preservation of land for public use (e.g., recreation or education) • Preservation of a historically Important land area Protection of natural habitat D Preservation of a certified historic structure Preservation of open space
2 Complete lines 2a through 2d if the organization held a qualified conservation contribution In the form of a conservation easement on the last day of the tax year.
a Total number of conservation easements . , . . . . . , . . . , • . . . . . . . . b Total acreage restricted by conservation easements , . . . . . • . . . , . • . .
c Number of conservation easements on a certified historic structure Included In (a)
d Number of conservation easements included In (c) acquired after 8/17/06, and not on a historic structure listed In the National Register , .•.. , ... , •...••...••.•.. , •.•.
I\}\' Held at the End of the Tax Year 2a
2b
2c
2d 3 Number of conservation easements modified, transferred, released, extinguished, or terminated by the organization during the
tax year • _____ _ 4 Number of states where property subject to conservation easement is located • 5 Does the organization have a written policy regarding the periodic monitoring, Inspection, handling of violations,
and enforcement of the conservation easements it holds? • , ..•. , ......•..••....•... , .... 0Yes D No 6 Staff and volunteer hours devoted to monitoring, Inspecting, handling of violations, and enforcing conservation easements during the year
• 7 Amount of expenses incurred in monitoring, Inspecting, handling of violations, and enforcing conservation easements during the year
• $ ______ _
B Does each conservation easement reported on line 2(d) above satisfy the requirements of section 170(h)(4)(B)(I) and section 170(h)(4)(B)(II)? , ... , .... , • , , ... , ..........• , .. , .....••.. , , . , . 0Yes
9 In Part XIII, describe how the organization reports conservation easements In its reveriue and expense statement, and balance sheet, and Include, if applicable, the text of \he footnote to the organization's financial statements that describes the organization's accounting for conservation easements.
IPaif,111 I Organizations Maintaining Collections of Art, Historical Treasures, or Other Similar Assets. Complete if the organization answered 'Yes' on Form 990, Part IV, line 8.
1 a If the organization elected, as permitted under SFAS 116 (ASC 958), not to report In Its revenue statement and balance sheet works of art, historical treasures, or other similar assets held for p[1blic exhibition, education, or research In furtherance of public service, provide, In Part XIII, the text of the footnote to Its financial statements that describes these items,
b If the organization elected, as permitted under SFAS 116 (ASC 958), lo report in its revenue statement and balance sheet works of art, historical treasures, or other similar assets held for public exhibition, education, or research In furtherance of public service, provide the following amounts relating to these Items: (I) Revenue Included on Form 990, Part VIII, line 1 .. , ....•. , .••..... , , •......... , , , , • $ _______ _
(ii) Assets Included In Form 990, Part X ...... , , ••..•. , , •••. , ... , .••. , .•..• , , .. • $ _______ _ 2 If the organization received or held works of art, historical treasures, or other similar assets for financial gain, provide the following
amounts required to be reported under SFAS 116 (ASC 958) relating to these Items: a Revenue Included on Form 990, Part VIII, line 1 ... , .....•••• , , • . . • . . . • . . • • • . . , • $ _______ _ b Assets Included in Form 990, Part X ..• , , . , , , , , • , ...••• , • . .•• , . , . , . . . • $
BAA For Paperwork Reduction Act Notice, see the Instructions for Form 990. TEEA3301 08/16/16 Schedule D (Form 990) 2016

ScheduleD(Form990)2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 Page2
!Part Ill I Organizations Maintaining Collections of Art, Historical Treasures, or Other Similar Assets (continued) 3 Using the organization's acquisition, accession, and other records, check any of the following that are a significant use of Its collection
Items (check all that apply):
a § Public exhibition d O Loan or exchange programs
b Scholarly research e O Other ------------------~----c Preservation for future generations
4 Provide a description of the organization's collections and explain how they further the organization's exempt purpose In Part XIII.
5 During the year, did lhe organization solicit or receive donations of art, historical treasures, or other similar assets to be sold to raise funds rather than to be maintained as part of the organization's collecllon?, , . , , , . , , , , Yes No
Part 1\/, Escrow and Custodial Arrangements. Complete if the organization answered 'Yes' on Form 990, Part IV, line 9, or reported an amount on Form 990, Part X, line 21.
1 a Is \he organization an agent, trustee, custodian or other intermediary for contributions or other assets not Included D on Form 990, Part X?, , , , , , , , , , , , , , , , , , , , , , , , , , , . , , , , , . , , , , , . , , , , , , • , , , , Yes
b If 'Yes,' explain the arrangement In Part XIII and complete the following table:
c Beginning balance .....
d Additions during the year . ,
e Distributions during the year f Ending balance, , , , , , ,
Amount 1 C
1 d 1 e
1 f 2 a Did the organization include an amount on Form 990, Part X, line 21, for escrow or custodial account
b If 'Yes,' explain the arrangement In Part Xiii. Check here if the explanation has been provided on Part liability?
XIII ''
'' , LJ Yes .·, ~No
'' I I I I Io
IPartV :I Endowment Funds. Complete if the organization answered 'Yes' on Form 990 Part IV line 10. (a) Current vear (b) Prior vear (c) Two vears back (d) Three vears back
1 a Beginning of year balance ... b Contributions , , •• , , , . , .
c Net Investment earnings, gains, and losses . , , , , . , , , , ,
d Grants or scholarships .....
e other expenditures for facilities and programs , , , , ,
f Administrative expenses g End of year balance . ,
2 Provide the estimated percentage of the current year end balance (line 1g, column (a)) held as: a Board designated or quasi•endowment • ______ % b Permanent endowment • ______ %
c Temporarily restricted endowment • ______ %
The percentages on lines 2a, 2b, and 2c should equal 100%.
3 a Are there endowment funds not In the possession of the organization that are held and administered for the organization by: (i) unrelated organizations . . . . • . . . , . , . . • , . . . • , . . • . . . . , , (ii) related organizations , , , , , , , , , , , , , , , , , , , , , , , , , , , , , , ,
b If 'Yes' on line 3a(II), are the related organizations listed as required on Schedule R? ,
4 Describe In Part XIII the Intended uses of the organization's endowment funds,
IPartVlil Land, Buildings, and Equipment.
(e) Four vears back
Yes No 3a(l) 3a(li)
3b
Complete if the organization answered 'Yes' on Form 990, Part IV, line 11 a. See Form 990, Part X, line 10. Description of property a) Cost or other basis (bb Cost or other (c) Accumulated (d) Book value
(investment) asis (other) depreciation 1 a Land , 0 0 >>IO O O I 0 •;//\1Ii/i\t\;'':?••'{,,,· .• kr·.
b Buildings • . • . . . . , ,
c Leasehold improvements , d Equipment . , , , . . , , e Other. , . , . , , .. , , 8 572. 5 564. 3 008.
Total, Add lines 1a throu1.1h 1e. (Column (dJ must equal Form 990, Part X, column (BJ, line 10c.) . ,·, . '' .... ''' .. • 3 008. BAA Schedule D (Form 990) 2016
TEEA3302 08/15/16

ScheduleD(Form990)2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 Page 3
IPartVll<I Investments - Other Securities. Com lete if the or anization answered 'Yes' on Form 990, Part IV, line 11b. See Form 990 Part X line 12.
(a) Description of security or category (Including name of security)
(1) Financial derivatives • , . , , , . , . , ,
(2) Closely-held equity Interests • , , , , , , , , . , , , ,
(b) Book value (c} Method of valuation: Cost or end-of-year market value
~O~r -----------------------~------------------------
~-------------------------------------------------~-------------------------------------------------~-------------------------------------------------~-------------------------------------------------~-------------------------------------------------~--------------------------~-----------------------~-------------------------------------------------~--------------------------------------------------00 --------------------------~-----~=----~-~--~-~--~ Total. {Column (b) must e ua/ Form 990, Pa/1 X, column (BJ line 12,) •• • Part vnf Investments - Program Related.
- C I t 'f th . t' . d 'Y ' F ompe et e orQanrza 10n answere es on orm '
a ne C, ee orm a , 1ne 990 P rt IV II 11 S F 990 P rt X 1· 13 (a) Description of Investment (b) Book value (c) Method of valuation: Cost or end-of-year market value
(1)
(2)
(3)
(4)
(5)
(6) (7)
(8)
/9) (10)
Total. (Column (b) must eaua/ Form 990 Part X column (81 line 13,J. .• .,._;,':;;/.•·:. ,.:..:c.:. ., •ci'?\i";',:.i;' ' ' · · .. ,_.•.••,·;::.·:w<i'-'';,._.,,. .•.. · ··,:'.·.)
!Part IX"il Other As~ets. ' ' PartX line 15.
b Book value in Limited rtment Pro·ects 36 77
Restricted Cash 53 926. Securit De osits 867,
Total. {Column (b) must equal Form 990, Part X, column (B) line 15,) . , • , , , , . , , • , ... , . , , • , , ••. , , . • 91 568. PaHX''• Other Liabilities.
Com lete if the or anization answered 'Yes' on Form 990, Part IV, line 11e or 11f. See Form
(2) (3)
(4)
11
Total. Column must e ua/ Form 990, Part X, column B line 25. , , . , • 2. Llabfl\ty for uncertain tax positions. In Part XIII, provide the text of the footnote to the organization's financial statements that reports the organization's liability for uncertain tax positions under FIN 48 (ASC 740). Check here If the text of the footnote has been provided in Part XI\\, , • , •••• , , , • , , , •• , , , • , , , , , , .. , , D BAA TEEA3303 08115/16 Schedule D (Form 990) 2016

Schedule D (Form 990) 2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257 429 !Part XI I Reconciliation of Revenue per Audited Financial Statements With Revenue per Return.
Complete if the organization answered 'Yes' on Form 990, Part IV, line 12a. 1 Total revenue, gains, and other support per audited financial statements , '' '.' ..... ' .. 1 2 Amounts Included on llne 1 but not on Form 990, Part VIII, line 12:
a Net unrealized gains (losses) on Investments, . , 2a ' ' . . ' . ' ' '. ' ; b Donated services and use of facilities. • .. . ' .. . .. 2b .. i c Recoveries of prior year grants , , . . . ' .. . . . . . ' . '. . . 2c '
d Other (Describe in Part XIII.) .... •.•. . . . ' . '. . ' 2d 1. tz: e Add lines 2a through 2d I 1 • • • ' .. ' .. '. .. ' . ' . . . . ' . .. . ' 2e
3 Subtract llne 2e from llne 1 . , . , . '.' ' ... . . . . '. . . . '. .. . . 3 4 Amounts Included on Form 990, Part VIII, llne 12, but not on llne 1:
a Investment expenses not Included on Form 990, Part VIII, line 7b. , . . . . .. I ··I -709. , ,"
b Other (Describe In Part XIII.) .....• , t •II I IO I . ' .. ' ... . ' '; 4b ., c Add lines 4a and 4b '. . ' ... '. '. . . '. . ' . '' . ' ... . . ... .. o O I I '.' 4c
5 Total revenue, Add lines 3 and 4c, (This must equal Form 990, Part I, line 12.), . '. '. '' '.' '' 5
I.Part)Ol I Reconciliation of Expenses per Audited Financial Statements With Expenses per Return. Complete if the organization answered 'Yes' on Form 990, Part IV, line 12a.
Total expenses and losses per audited financial statements •....•.•
2 Amounts Included on llne 1 but not on Form 990, Part IX, llne 25: a Donated services and use of facllllies. b Prior year adjustments . , , . c Other losses . , , . • . . • .
d Other (Describe In Part XIII.) .
e Add lines 2a through 2d , ..
3 Subtract line 2e from line 1 . .
2a 2b
2c 2d 370,
4 Amounts Included on Form 990, Part IX, line 25, but not on line 1; a Investment expenses not Included on Form 990, Part VIII, line 7b. b Other (Describe In Part XIII.) ..... , ..... , ... , ...
. . . . . . . l-4al -• , , · · · · 4 b ~~-------c Add lines 4a and 4b . . . , . , , . . . . . . , , , . . , , . . ,
5 Total ex enses. Add lines 3 and 4c. This must e ua/ Form 990, Part I, fine 18. 4c 5
Page 4
1,445,118,
1. 1,445,117 .
-709, 1 444,408,
370. 1 482 867 .
1 482 867.
Provide the descriptions required for Part II, lines 3, 5, and 9; Part Ill, lines 1 a and 4; Part IV, lines 1b and 2b; Part V, llne 4; Part X, line 2; Part XI, lines 2d and 4b; and Part XII, \Ines 2d and 4b. Also complete this part to provide any additional Information,
Pt XI, Line 2d Pt XII, Line 2d
BAA
OTHER ENTITY REVENUES INCLUDED IN CONSOLIDATED AUDIT OTHER ENTITY EXPENSES INCLUDED IN CONSOLIDATED AUDIT
TEEA3304 08/15/16
Schedule D (Form 990) 2016

SCHEDULE G (Form 990 or 990-EZ)
Supplemental Information Regarding Fundraising or Gaming Activities 0MB No. 1545-0047
2016 Complete If the organization answered 'Yes' on Form 990, Part IV, line 17, 18, or 19, or if the organization entered more than $15,000 on Form 990-EZ, line 6a,
• Attach lo Form 990 or Form 990-EZ, • ._· Op~n. 'to Public_ Department of Iha Treasury I ti· · Internal Revenue service • Information about Schedule G (Form 990 or 990-EZ) and Its instructions is at www.irs.gov/form990. .: : nspec on Name of the organization I Employer Identification number
NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429
IP rt I ,j Fund raising Activities, Compl?te if the organizall,on answered 'Yes' on Form 990, Part IV, line 17. . 8 ·- Form 990-EZ filers are not regutred lo complete this part.
1 Indicate whether the organization raised funds through any of lhe following activities. Check all that apply.
a ~ Mall solicltatlons e § Solicitation of non-government grants b Internet and email solicitations f Solicitation of government grants c Phone solicitations g Special fundralslng events
d In-person sollcltatlons
2 a Did lhe organization have a written or oral agreement with any Individual (Including officers, directors, trustees, or key employees listed In Form 990, Part VII) or entity In connection with professional fund raising services? , , , , , , , ,
b If 'Yes,' list the 1 o highest paid Individuals or entitles (fundralsers) pursuant to agreements under which the fund raiser Is to be compensated at least $5,000 by the organization.
, G]Yes ONo
(I) Name and address of Individual (Ill) Did fundraiser (Iv) Gross receipts {v) Amount paid to (vi) Amount paid to
(II) Activity (or retained by) or entity (fundralser) have custody or control from activity fundralser listed In (or retained by)
of contritiutlons? column (I) organization
NEWPORT CREATIVE COMMUNICATIONS Yes No 1
MAIL EDUC/ X 1 422 709, 19 239, 1 403 470.
2
SOLICITATIONS
3
4
5
6
7
8
9
10
Total, , , .. , , , , .... , , , , , , , , , , , , , , , , , , , ... , • 1 422 709, 19 239, 1 403 470. 3 List all states In which the organization Is registered or licensed to solicit contributions or has been notified It Is exempt from registration
or llcenslng. Ark~nsas __________________________________________________________ _ Cali.tornia ________________________________________________________ _ Colorado __________________________________________________________ _ Florida __________________________________________________________ _
See Part I, Line 3 List of States Registered or Licensed lo Solicit Funds BAA For Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990-EZ,
TEEA3701 09/23/16
Schedule G (Form 990 or 990-EZ) 2016
Schedule G (Form 990 or 990-EZ) 2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-12 57 4 2 9 Page 2
!Part IF! Fundra!sing Events. Complete if the organization answered 'Yes' on Form 990, Part IV, line 18, or reported more than $15,000 of fundraising event contributions and gross income on Form 990-EZ, lines 1 and 6b. List events with gross receipts greater than $5,000.
(a) Event #1 (b) Event #2 (c) Olher events \d) Total events add column (a)
through column (c)) R {evenl \ype) {even! type) (Iola! number) E V E
1 Gross receipts N ... . . u E
2 Less: Contributions • .. 3 Gross Income (line 1 minus line 2).
4 Cash prizes . . . . . . . .. 5 Noncash prizes • ..
D I
6 RenVfaclilty costs . R . . .. E C T 7 Food and beverages . . .. E X 8 Entertainment. . . . .. p E N
9 Other direct expenses. s .. E s
10 Direct expense summary. Add lines 4 through 9 In column (d) .• 0 IO O O O IO O. 0 I IO O O O O I IO O O 0 • 11 Net Income summary. Subtract line 10 from line 3, column (d) •• . '.' .. '.' ............... •
I Parl: 1111 Gaming. Complete if the o~ganization answered 'Yes' on Form 990, Part IV, line 19, or reported more than $15,000 on Form 990-EZ, line 6a.
R (b) Pull tabs/instant (d) Total gaming
E (a) Bingo btngo/progresslve (c) Other gaming (add column (a) V bingo through column (c)) E N u E
1 Gross revenue ... . . . . 2 Cash prizes . • ... . .
E o X I p 3 Noncash prizes . . . . . .. . . R E E N C S, T E 4 RenVfacility costs , ' . . . s . .
5 Other direct expenses. .. . . HYes % HYes % HYes % ·::• ',, ,__ ''
--- ---6 Volunteer labor . . . . ' . . . . No No No .
7 Direct expense summary. Add lines 2 through 5 In column (d) . . . . '. . . . . . .. •
8 Net gaming income summary, Subtract line 7 from line 1, column (d) . . . . . . ... •
9 Enter the state(s) In which the organization conducts gaming activities: a Is the organization licensed to conduct gaming activities In each of these states? ........••.••....••... O Yes O No b If 'No,' explain:
10a Were any of the organization's gaming licenses revoked, suspended or terminated during the tax year? •......... O Yes ONo b lf'Yes,' explain: ________________________________________________________ _
BAA TEEA3702 09/23/16 Schedule G (Form 990 or 990-EZ) 2016

Sc.hedule G (Form 990 or 990-EZ) 2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 11 Does \he organization conduct gaming activities with nonmembers? , , , , .. , , , , , , , , , , , ,
12 Is \he organization a grantor, beneficiary or trustee of a \rust, or a member of a partnership or other entity formed lo administer charl\able gaming? . , , , . , , . , , , , , , , , .. , , , , , , , , ... , , , , , . , . , , , , .
. QYes
, 0Yes
13 Indicate \he percentage of gaming activity conducted in: I I a The organization's facility ......... , . , ..... , , . , , , , . , , , , , . , . , , , , , , , , . , , , , ,__13_a__. _______ %_ b An outside facility .. , , ... , ... , , , , , , , . , , , , , , , , . , , , , , , , , , , , , , , , , , , , , , , '--13_b__c.. _______ %_
14 Enter the name and address of \he person who prepares \he organization's gaming/special events books and records:
Name •
Address •
15a Does \he organization have a contract with a third party from whom the organization receives gaming revenue? , , , . , . , QYes b If 'Yes,' enter the amount of gaming revenue received by the organization • $ ___________ and the amount
of gaming revenue retained by the third party • $ __________ _ c If 'Yes,' enter name and address of the third party:
Name • ------------------------------------------------------------, I
Address • I
16 Gaming manager Information:
Name •-------------------------------------------------------------
Gaming manager compensation • $ __________ _
Description of services provided •
0 Director/officer 0Employee 0 Independent contractor
17 Mandatory distributions
a Is the organization required under state law to make charitable distributions from the gaming proceeds to retain the state gaming license? ---------------------------------DYes 0No
b Enter the amount of distributions required under state !aw to be distributed to other exempt organizations or spent In the organization's own exempt activities during the tax year • $
IPartJV I Supplemental Information. Provide the explanations required by Part I, line 2b, columns (iii) and (v); and Part Ill, lines 9, 9b, 10b, 15b, 15c, 16, and 17b, as applicable. Also provide any additional information. See instructions
Line 2b col(v)
BAA
THE ORGANIZATION PAID THE FUNDRAISER $1,196,596 FOR EXPENSES INCLUDING PRINTING, PAPER, MAIL LIST RENTAL, AND POSTAGE, THE CONSULTANT ITEMIZES
THESE ITEMS IN ADDITION TO HIS CONSULTING FEE ON THE INVOICE. CONSULTING FEES FOR 2016 TOTALED $19,239 OF WHICH $4,715 WERE ALLOCATED TO FUNDRAISING, $142 WAS ALLOCATED TO ADMINISTRATIVE, AND $14,381 WAS ALLOCATED TO PROGRAM EDUCATIONAL MAILING COSTS.
TEEA3703 09/23/16 Schedule G (Form 990 or 990-EZ) 2016

SCHEDULE J (Form 990)
Department of the Treasury Internal Revenue Service
Compensation Information For certain Officers, Directors, Trustees, Key Employees, and Highest Compensated Employees
• Complete If the organization answered 'Yes' on Form 990, Part IV, line 23. • Attach to Form 990.
• Information about Schedule J (Form 990) and Its Instructions Is at www.irs.gov/form990.
0MB No. 1545-0047
2016
Name of the organization Employer ldentlncatlon number
NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429
Pant Questions Regarding Compensation
1 a Check the appropriate box(es) If the organization provided any of the following to or for a person listed on Form 990, Part VII, Seclion A, line 1a. Complete Part Ill to provide any relevant information regarding these Items.
D First-class or charter travel 0Housing allowance or residence for personal use
D Travel for companions D Payments for business use of personal residence
D Tax indemnification and gross-up payments D Health or social club dues or initiation fees
D Discretionary spending account D Personal services (such as, maid, chauffeur, chef)
b If any of the boxes on line 1 a are checked, did the organization follow a written policy regarding payment or reimbursement or provision of all of the expenses described above? If 'No,' complete Part Ill to explain
2 Did the organization require substantiation prior to reimbursing or allowing expenses incurred by all directors, trustees, and officers, Including the CEO/Executive Director, regarding the Items checked In line 1a? ...• ,
3 Indicate which, if any, of the following the filing organization used to establish the compensation of the organization's CEO/Executive Director. Check all that apply. Do not check any boxes for methods used by a related organization to establish compensation of the CEO/Executive Director, but explain in Part Ill.
D Compensation committee Owritten em~loyment contract
D Independent compensation consultant D Compensation survey or study
D Form 990 of other organizations IE]Approval by the board or compensation committee
4 During the year, did any person listed on Form 990, Part VII, Section A, line 1a, with respect lo the filing organization or a related organization:
a Receive a severance payment or change-of-control payment? ••.• , • , .• , • ,
b Participate In, or receive payment from, a supplemental nonqual\fied retirement plan? c Participate In, or receive payment from, an equity-based compensation arrangement?
If 'Yes' to any of lines 4a-c, list the persons and provide the applicable amounts for each item In Part Ill.
Only section 601(c)(3), 501(c)(4), and 501(c)(29) organizations must complete lines 5.9,
5 For persons listed on Form 990, Part VII, Section A, line 1a, did the organization pay or accrue any compensation contingent on the revenues of:
a The organization? • • . . • . • , • . , . •
b A~y related organization? • . . . . . , , •
If 'Yes' on line 5a or 5b, describe In Part Ill.
6 For persons listed on Form 990, Part VII, Section A, line 1a, did the organization pay or accrue any compensation contingent on the net earnings of:
a The organization? • , , . . . . , . . , . .
b Any related organization? , , . , , , , , •
If 'Yes' on line 6a or 6b, describe In Part Ill.
7 For persons listed on Form 990, Part VII, Section A, line 1a, did the organization provide any nonfixed payments not described on lines 5 and 67 If 'Yes,' describe In Part Ill , •..••... , ..•.. ,
8 Were any amounts reported on Form 990, Part VII, paid or accrued pursuant to a contract that was subject to the initial contract exception described in Regulations section 53.4958-4(a)(3)? If 'Yes,' describe in Part Ill • , . , , . , .• , , , •.. , .••...•... , , . , ...•.... , •.
9 If 'Yes' on line 8, did lhe organization also follow the rebutlable presumption procedure described In Regulations section 53.4958-B(c)? ..••.•.• , •. , ..•. , •• , , ..• , , .•. , , , , • , ••••. , . , . , .
7
8
9
X
X
BAA For Paperwork Reduction Act Notice, see the Instructions for Form 990. Schedule J (Form 990) 2016
TEEA4101 0B/19/16

Sch
ed
ule
J (Form
990) 20
16
N
AT
ION
AL
E
ME
RG
EN
CY
M
ED
ICIN
E
AS
SO
CIA
TIO
N
52
-12
5 7 42
9 P
ag
e2
Jffli!'fJrj Offic
ers
, Directo
rs, Tru
ste
es
, Ke
y E
mp
loy
ee
s, a
nd
Hig
he
st C
om
pe
ns
ate
d E
mp
loyees_ U
se d
up
licate
cop
ies if a
dd
ition
al sp
ace
is ne
ed
ed
.
Fo
r ea
ch in
dM
du
al w
ho
se co
mp
en
satio
n m
ust b
e re
po
rted
on
Sch
ed
ule
J, rep
ort co
mp
en
satio
n fro
m th
e o
rga
niza
tion
on row
(i) and from
related org
an
izatio
ns. d
escrib
ed
in th
e instructions.
on
row
00-D
o n
ot list a
ny in
divid
ua
ls tha
t are
no
t listed on Fo
rm 9
90
, Pa
rt Vil.
Note: T
he
sum
of colum
ns (B)(i)-(iii) fo
r each listed ind
ividu
al m
ust e
qu
al th
e total a
mo
un
t of F
orm
990, Pa
rt VII, S
ectio
n A
, line
1a, ap
plica
ble
colu
mn
(D) and (E
) am
ou
nts fo
r tha
t ind
ividu
al.
KE
LL
Y
HE
RZ
OG
1
PR
ES
IDE
NT
2
3 4 5 6
7 8 9
10
11
12
13
14
15
16
BA
A
(A) N
am
e and T
itle
(B) B
reakdown ofW
-2 and/or1099-MIS
C com
pensation
(i) Base
compensation
(iJ 1-_ u_s_, 1 Q.o~ L@
L _ _ _ o __
(i} 1-------
j(ii)
{i) 1-------
l(ii)
(i) 1--------
L@
(i} 1--------
1 (ii) (i) 1
-------
l(ii)
(i} 1
-------
l(ii)
(i) 1--------
L@
(i) 1-------
lfii)
(i} 1-------
l(ii)
(i) t-------
l(ii}
(i) 1-------
l(ii}
(i) 1-------
l(iiJ (i) 1
--------
l(ii)
(i) 1-------
i(ii) (i) 1
-------
(ii}
(ii) Bo
nu
s & in
centive
compensation
(Iii) Oth
er
reportable co
mp
ensatio
n
__
_ 9
L6
5Q
-1------Q
_ Q
_ Q
_
TE
EA
41
02
0B
J19/16
(C} R
etire
me
nt
and oth
er
de
ferre
d
com
pe
nsa
tion
(D) N
on
taxa
ble
b
en
efits
(E) T
ota
l of
colu
mn
s(B)(i}-(D
) (F
) Co
mp
en
satio
n
in co
lum
n (B
) reported as
deferred on prio
r F
orm
990
__
__
__
o~
--2
4..L
s20
-.1-._
1sz.., 77
0-J
__
__
__
o_ o_ I
_ _ _ o. J _ ·
_ o -1
_ o _
-------~
--------r-------~
--------
-------~
--------~
-------~
--------
-------~
--------r-------~
--------
-------~
--------r--
----•--
-----
-------~--------r-------~
--------
-------~--------r-------~
--------
-------~--------~
-------~--------
-------~
--------r-------~
--------
-------~--------~
-------~--------
Sch
ed
ule
J {Fo
nn
990} 2016
Schedule J (F
orm 990) 2016
NA
TIO
NA
L
EM
ER
GE
NC
Y
ME
DIC
INE
A
SS
OC
IAT
ION
5
2-1
25
74
29
jlf?a.Tl:]11-/j S
up
ple
me
nta
l Info
rma
tion
Pro
vide
the
information, explanation, o
r descriptions required for P
art I, lines 1a, 1b, 3, 4a, 4b, 4c, S
a, 5b, 6a, 6b, 7, and 8, an
d fo
r Pa
rt IL A
lso
com
ple
te this p
art fo
r an
y additional information.
Pa
ge
3
BA
A
Sch
edu
le J {Form
990) 2016
TE
EA
41
03
08/19/16
SCHEDULE L (Form 990 or 990-EZ)
Department of the Treasury Internet Revenue Service
Transactions With Interested Persons • Complete If the organization answered 'Yes' on Form 990, Part IV, line 25a, 25b, 26, 27, 28a,
28b, or 28c, or Form 990-EZ, Part V, llne 38a or 40b. • Attach to Form 990 or Form 990-EZ.
• Information about Schedule L (Form 990 or 990-EZ} and Its Instructions Is at www.Jrs.gov/form990.
0MB No. 1545-0047
2016 Operi To,~u~nC ·•
)n~pecUon ·.· l Name of the organl2etlon I Employer Identification number
NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 I Part I J Excess Benefit Transactions (section 501 /c)(3), section 501 (c)(4), and 501 !c)(29) organizations only).
Complete if the organization answered 'Yes' on Form 990, Part IV, line 25a or 25b, or Form 990-EZ, Part V, nne 40b.
\bl Relationship between disqualified (c) Description of transaction
(d) Corrected? 1 (a) Name of dlsqua\lfled person person and organization
Yes No
(1)
(2)
(3)
(4)
(5)
(6)
2 Enter the amount of tax incurred by the organization managers or disqualified persons during lhe year under section 4958 ......•...•..........•..• , . . • . . . . . . • $ _______ _
3 Enter the amount of tax, If any, on line 2, above, reimbursed by the organization . . . . . . . . • . . . . • . . • $
I Par1::IH;;) Loans to and/or From Interested Persons. Complete if the organization answered 'Yes' on Form 990-EZ, Part V, line 38a or Form 990, Part IV, line 26; or if the organization reported an amount on Form 990, Part X, line 5, 6, or 22.
ta) Name of Interested parson (bl Relationship (c) Purpose td) Loan to or (e) Original (f) Balance due (g) In default? (h) Approved wl h organization al loan from the pnnctpel amount by board or
org anlzatlon? commlttea?
To From Yes No Yes No
(1) (2) (3) (4)
(5)
(6)
(7) (8)
(9)
(10) Total. IO O O I .. . . . . . ' ..... '''.' ' .... ' ... . .. • $ bt::;._; '!ii
' :n:;;, liPart.111\11 Grants <;>r Assist~n~e Benefiting Interested Persons_.
Complete if the organization answered 'Yes' on Form 990, Part IV, line 27.
(!)Written agreement?
Yes No
(\'i\t:\'."''\:i\
(a) Name of Interested person (b) Relationship between Interested person and the organization
(c) Amount of assistance (d) Type of assistance (e) Purpose of asststance
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
BAA For Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990-EZ. Schedule L (Form 990 or 990-EZ) 2016
TEEA4501 08/09/16

Schedule L (Form 990 or 990-EZ) 2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 Page 2
I Part IV I Business Transactions Involving Interested Persons. Complete if the organization answered 'Yes' on Form 990, Part IV, line 28a, 28b, or 28c, (a) Name of lnlerested person (b) Relationship beh•1een (c) Amount of (d) Description of transaction (e) Sharing of
Interested person and Iha transaction organlz.atlon's organizaUon revenues?
Yes No
(1) KELLY HERZOG BOARD OF DIRECTORS 0, DIRECTOR IN COMMON X
(2) SUZANNE, LEVIN BOARD OF DIRECTORS o. DIRECTOR IN COMMO\\i X
(3) THOMAS BLAIR BOARD OF DIRECTORS o. DIRECTOR IN COMMON X (4) (5) (6)
(7)
(8)
(9)
(10)
I Part V I Su~plem~~tal ,Information Provide add1t1onal information for responses to questions on Schedule L (see 1nstruct1ons),
Schedule L (Form 990 or 990-EZ) 2016 TEEA4601 08/09/16

SCHEDULE 0 (Form 990 or 990-EZ)
Department of the Treasury Internal Revenue Service
Supplemental Information to Form 990 or 990-EZ Complete to provide Information for responses to specific questions on
Form 990 or 990-EZ or to provide any additional Information. • Attach to Form 990 or 990-EZ,
• Information about Schedule O (Form 990 or 990-EZ) and Its Instructions Is at www.lrs.aov/form990,
0MB No. 1545-0047
2016 Open.to Pubil~ : !
·• • 111spectfon .. · ·· -.· , Name of the organlzallon I Employer tdentlncatJon number
NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429
Pt VI, Line Pt VI, Line Pt VI, Line Pt VI, Line Pt VI, Line
Pt VI, Line
Pt VII, Col
llb 12c 15a 15b 18
19
(F)
FORM 990 IS REVIEWED BY EXEC DIRECTOR & DISCUSSED BY PHONE WITH BOARDS MEMBERS PRIOR TO FILING, CONFLICT OF INTEREST STATEMENTS ARE COMPLETED BY BOARD MEMBERS ANNUALLY. CEO COMPENSATION IS APPROVED BY BOD, EMPLOYEE COMPENSATION IS DETERMINED BY CEO, FORM 990 IS AVAILABLE BY REQUEST AND THEY ARE ON GUIDESTAR, ORGANIZATIONAL DOCUMENTS, CONFLICTS OF INTEREST POLICIES &PROCEDURES AND AUDITED FINANCIAL STATEMENTS ARE AVAILABLE TO THE PUBLIC UPON REQUEST, CONTRIBUTIONS TO A 401(K) PLAN, HEALTH INSURANCE PREMIUMS,LONG TERM CARE PREMIUMS, LIFE INSURANCE PREMIUMS & HSA CONTRIBUTIONS
BAA For Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990-EZ, TEEA4901 08/16/16 Schedule O (Form 990 or 990-EZ) (2016)

SC
HE
DU
LE
R
(Fo
rm 990)
Re
late
d O
rga
niza
tion
s a
nd
Un
rela
ted
Pa
rtne
rsh
ips
•
Co
mp
lete
if the
org
an
izatio
n a
ns
we
red
'Ye
s' o
n F
orm
99
0, P
art IV
, line
33
, 34, 35
b, 36, o
r 37
. •
Atta
ch
to F
orm
99
0.
De
pa
rtme
nt of th
e T
reasury' Internal R
eve
nu
e S
ervice
•
Info
rma
tion
ab
ou
t Sc
he
du
le R
(Fo
rm 9
90
) an
d its
ins
truc
tion
s is
at w
ww
.irs.go
v/form
990.
Na
me
of the
organization
NA
TIO
NA
L
EM
ER
GE
NC
Y
ME
DIC
INE
A
SS
OC
IAT
ION
!Part! >j Id
entificatio
n o
f Disreg
arded
-En
tities. Co
mp
lete
if the
org
an
izatio
n a
nsw
ere
d 'Y
es' on F
orm
990, Pa
rt IV, lin
e 33.
(a) N
ame, address, and E
IN (ff applicable) o
f disregarded entity
(1) -
------
(2) -------------------------------
(3) --
--
--
--
--
--
--
--
--
--
--
--
--
--
--
-
(b)
Prim
ary activity (c)
Legal domicile (state
or foreign country)
(d)
To
tal incom
e
0M
B N
o. i54
5-0
04
7
2016 "<, ~~1~~:i:k>~k
1 Em
plo
yer iden
tification
nu
mb
er
52
-12
57
42
9
(e) E
nd-of-year assets (f)
Direct controlling
entity
j,l;clttll j Iden
tification
of R
elated T
ax
-Ex
em
pt O
rga
niza
tion
s. C
om
ple
te if th
e o
rga
niza
tion
an
swe
red
'Ye
s' on
Fo
rm 990, P
art IV
, line
34
be
cau
se it h
ad
o
ne
or m
ore
rela
ted
tax-e
xem
pt o
rga
niza
tion
s du
ring
the
tax year.
(a) {b)
{c) (d)
{e) (f)
(g)
Nam
e, address, and ElN
of related organization
Prim
ary activity Legal dom
icile (state E
xempt C
ode P
ub
lic charity status D
irect controlling
Sec 512{b)(13) o
r foreign country) section
(if section 501 (c)(3)) entity
controlled entity?
Ye
s
No
j1_lEM
ER
GE
NC
Y
ME
DIC
INE
SU
PPOR
T
FOU
ND
ATIO
N
__
PO
BO
X
10
39
__
__
__
__
__
__
__
__
_
__
EDG
EWO
OD
..L M
D 2
10
40
__
__
__
__
__
__
ED
UC
AT
ION
TO
5
2-2
32
04
38
PREVENT IN
JUR
Y/ILLN
ESS VA
5
01
rel /3
) lla
N
EMA
X
J~
--------------------------
--------------------------------------------------------
J~
--------------------------
--------------------------------------------------------J~
--------------------------
--------------------------------------------------------
BA
A F
or P
ap
erw
ork R
ed
uctio
n A
ct N
otice
, see
the
Instru
ction
s for F
orm
990. T
EE
A500i
09/09/16 S
chedule R (F
orm 990) 2016
Sch
ed
ule
R(F
orm
99
0)2
01
6
NA
TIO
NA
L
EM
ER
GE
NC
Y
ME
DIC
INE
A
SS
OC
IAT
ION
5
2-1
25
74
29
P
ag
e2
li8i:ir1:]tk pd
en
tific~
tion
of R
elated O
rgan
ization
s .Taxab
le as
a Partn
ership
C
?mple~
e if the
org
an
izatio
n a
nsw
ere
d 'Y
es' on F
orm
99
0, P
art IV
, line 34
· ·
be
cau
se 1t had o
ne
or m
ore
related org
an
izatio
ns tre
ate
d a
s a pa
rtne
rship
du
nn
g th
e ta
x yea
r.
(a} (b}
(c} (d}
(e} (f}
(g} (h}
(i) (j)
(k) N
am
e, a
dd
ress, a
nd
EIN
of
Prim
ary a
ctivity L
eg
al
Dire
ct Predom
inant income
Share o
f total S
ha
re o
f D
ispro
po
r-C
od
e V
-UB
I G
en
era
l or
Percentage re
late
d o
rga
niza
tion
d
om
icile
con
trollin
g
(related, unrelated, in
com
e
en
d-o
f-yea
r tio
na
te
am
ou
nt in
bo
x m
an
ag
ing
ow
nership (sta
te o
r e
ntity
excluded from tax
asse
ts a
lloca
tion
s?
20
of S
che
du
le
pa
rtne
r?
fore
ign
under sections
K-1 (F
orm
co
un
try) 572-514)
Yes
No
10
65
) Y
es N
o 111 _
__
__
__
__
__
_
-----------------------------
121 _ --------
--
--
----------------------------
J3l _ --
--
--
--
--
--
-----------------------------jP
atfl'i(q l.den
tification
o~ Related
Org
an
izatio
ns
Taxab
~e a:5 a Co
rpo
ratio
n o
r Tru
s~ Co
mp
lete
if th.e org
an
izatio
n a
nsw
ere
d 'Y
es' o
n F
orm
990, Pa
rt IV,
·· · ··
· · lme
34
be
cau
se 1t h
ad
on
e o
r mo
re related o
rga
niza
tion
s trea
ted
as a co
rpo
ratio
n o
r trust d
urin
g th
e ta
x year.
(a} (b}
(c} (d
} (e)
(f} (g)
(h)
(i) N
am
e, a
dd
ress, a
nd
ElN
of re
late
d o
rga
niza
tion
P
rima
ry activity
Le
ga
l do
micile
D
irect
Typ
e o
f en
tity S
ha
re o
f S
ha
re o
f en
d-o
f-Percentage
Sec 512(b)(13) (state o
r fore
ign
co
ntro
lling
(C
corp
, S co
rp,
tota
l inco
me
ye
ar a
ssets
ownership
controlled entity? co
un
try} e
ntity
or tru
st} Y
es N
o
0) __
__
__
__
__
__
__
__
__
__
__
_
--------------------------------------------------
(2) -----------------------
--------------. ----------
-------------------------
(3) -----------------------
-------------------------
-------------------------B
AA
T
EE
A5
00
2
09/09/16 S
che
du
le R
(Fo
rm 9
90
) 20
16

Sch
ed
ule
R(F
orm
99
0)2
01
6
NA
TIO
NA
L
EM
ER
GE
NC
Y
ME
I)_I_C_IN
E_ _
AS
SO
CIA
TIO
N
52
-12
57
42
9
Pa
ge
3
IR~
tfWC
jTran
saction
s With
Related
Org
anizatio
ns. C
om
ple
te if th
e o
rga
niza
tion
an
swe
red
'Ye
s' on Fo
rm 990, P
art IV
, line
34, 35b, or 36_
No
te. Com
plete line 1 if any entity is listed in Parts II, Ill, o
r IV o
f this schedule_
1 D
uring the
tax year, did th
e organization engage in
any of th
e follow
ing transactions with one o
r mo
re related organizations listed in
Parts II-IV
?
a R
eceipt of (i) interest, (ii) annuities, {iii) royalties, o
r (iv) rent from a controlled entity •
b G
ift, grant, or capital contribution to
related organization(s)
c G
ift, grant, or capital contribution from
related organization(s)
d Loans o
r loan guarantees to or fo
r related organization(s)
e Loans or loan guarantees b
y related organization(s)
f D
ividends from related organization(s) .
• . .
. g
Sale o
f assets to related organizatior:i(s) • .
••
h P
urchase of assets from
related organization(s)
Exchange o
f assets with related organization(s)
Lease of facilities, equipm
ent, or other assets to related organization(s)
k Lease of facilities, equipm
ent, or other assets from
related organization(s) .
I P
erformance o
f services or mem
bership or fundraising solicitations for related organization(s)
m P
erformance o
f services or m
embership o
r fundraising solicitations by related organization(s)
n Sharing o
ffacilitie
s, equipment, m
ailing lists, or other assets w
ith related organization(s) •
o
Sharing o
f paid employees w
ith related organization(s)
p
Reim
bursement paid to
related organization(s) for expenses •
q R
eimbursem
ent paid by related organization(s) fo
r expenses
r O
the
r transfer of cash o
r property to related organization(s) •
s O
the
r tran
sfer o
f cash or property from
related organization(s)
2 If th
e a
nsw
er to a
ny o
f the
above is 'Yes,' see th
e instructions fo
r information on w
ho
mu
st complete th
is line, including covered relationships and transaction thresholds.
(a) (b)
(c) N
am
e o
f related organization T
ransaction typ
e (a-s)
Am
ou
nt involved
(1) EM
ER
GE
NC
Y
ME
DIC
INE
S
UP
PO
RT
F
OU
ND
AT
ION
rn
{2)E
ME
RG
EN
CY
M
ED
ICIN
E
SU
PP
OR
T
FO
UN
DA
TIO
N
n
(3) EM
ER
GE
NC
Y
ME
DIC
INE
S
UP
PO
RT
F
OU
ND
AT
ION
0
(4)
(5)
(6)
---
Ye
s N
o
1a
X
1
b
X
1c
X
1d
X
1
e
X
1f
X
1g
X
1
h
X
1 i -21-
1 k I
X
1 I I
X
1m
X
1
n
~
1o
X
1 r X
1
s
X
(d) M
ethod of determ
ining a
mo
un
t involved
0. 11\C
TU
AL
BA
LA
NC
E
0. A
.CT
UA
L
BA
LA
NC
E
0. iA
.CT
UA
L
BA
L.A
NC
E
BA
A
TE
EA
50
03
09/09116
Schedule
R (F
orm 990) 2016

Sch
ed
ule
R (F
orm
990) 20
16
N
AT
ION
AL
E
ME
RG
EN
CY
M
ED
ICIN
E
AS
SO
CIA
TIO
N
52
-12
57
42
9
Pa
ge
4
j:iBartNE I Un
related O
rgan
ization
s Ta
xa
ble
as a Partn
ership
. Co
mp
lete
if the
org
an
izatio
n a
nsw
ere
d 'Y
es' o
n F
orm
990, Pa
rt IV, line 37.
Pro
vide
the
follo
win
g in
form
atio
n fo
r ea
ch e
ntity taJC
ed as a p
artn
ersh
ip th
rou
gh
wh
ich th
e o
rga
niza
tion
con
du
cted
mo
re th
an
five p
erce
nt o
f its activities (measured b
y total assets or g
ross
revenue) tha
t wa
s no
t a related organization. Se
e in
structio
ns re
ga
rdin
g e
xclusio
n fo
r certain inve
stme
nt partnerships.
(a) I
(b) j
(c)
I (d)
(e) {f)
(g)
(h) (i)
I (j)
I (k)
Nam
e, address, an
d E
IN o
f entity P
rimary activity
Legal do
micile
P
redominant
Are all partners S
ha
re o
f S
ha
re o
f D
ispro
po
r-C
od
e V
-UB
I G
en
era
l or
Percentage
(state or fo
reig
n
income
section to
tal in
com
e
en
d-o
f-yea
r tio
na
te
am
ou
nt in
bo
x m
an
ag
ing
ow
nership country)
(related, unre-501(c)(3)
assets a
lloca
tion
s?
20
of S
che
du
le
pa
rtne
r?
laled, excluded organizations?
K-1
from tax under
(Form
1065) sections 512-514)
Ye
s
No
Y
es
N
o
I Ye
s I
No
(1) ---------------·
(2) ---------------
(3) ---------------·
(4) ---------------
(5) __
__
__
__
__
__
__
_
(6) ---------------·
m _______________ _
(8) ---------------
BA
A
TE
EA
50
04
09/09/16
Sch
ed
ule
R (F
orm
990) 20
16

Schedule R (Form990)2016 NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429 Page 5
I PartVll I Supplemental Information. Provide additional information for responses to questions on Schedule R. See instructions,
BAA TEEA6005 09/09/16 Schedule R (Form 990) 2016

Form 88]9~E 0 IRS e-:file Si9n1;1.Jµre Ail~hJdi1atipn
for an Ex.empt OrganJza,t1,pn Fat ctilondaryoor :z&iei o/flseill year bei)lnnlno . , .... ,• , , 2018, and on<llng ,,.!?O · . . . .
· . .· ~ Oci hot sert~ lq ~1ffi«i~~ ~~y'~·~r:r~oTds.- - ,,-<~.. ~ c,; ~ -" lnfomp.ttoi) ·a~o.ut rqrm as79,g<;l imd lts Instruction$ ls :ii www-1rf,govlfptin007.0eo, .·
2'016 ...... ' . . · , rrtr,loyer id?l1ilf1"'1ilon numl>er,
NA.TI.ONA!, EMEB,GE\NCY MED'.Ic:1'.Nm ASSOCIATION . ,52~.12574 2,9• . ifome M<J lttle of o(ncr,r · ·
£<ELtY .HERZOG ,. .. .. . . .. . . .. . . .. . PRES!DENT [~11~Jiml Tys,e of Return and Return lnformi:ition (Whbte. Do·llam Only) . Check the bo:<:fodhe r~lifin for ~hlc\'i y6u ate, uslpg this .Form as79;EO. an~ entedhe applfooble arnoulih i( ahy_, :rfom. lhe return. If you . check the box on 11.ne.1a,, 2a, 3<'1,.4~, or. Sa, 1:ielow, and Iha amount on \ha\ hne fodhe return being ftled,yi~h this forrl\.was blank, then le'"v$ lhil;i .1 b; 2b.,·3bi4b, _or. Sb, 'Nf11che~r is. appficable, blanl< (do not enter -o+ Bu!, if you entereq -Q, OfJ \.he i:eturn, \hen .anter-0- on . lhe)pp/lrable line below: Do 1,1bt complete more than 1 line lr1 Part I. · · ·
1.i Forrrt 9M checl<-fW;1ra • , , ,;. [!l I? T9t1ll r~i/eiltie, tf~hy (Form 9~0, P.atfVllt,·column ·(A); ilne f2) , , , , '. .. 2. a F.otD'l 990;Ez 9h~ck here, . , • 0 b Total revenue, If any \form 990-EZ,-llne 9) •. ; •• ,, , ; • .- ; , , , , , 3 H·orm 1120-P()L ohebk here , , • ,• • b Total tax (Form 1i20-p61,,, line 22) .. : ., , , , r:, •• , , , , •
4 a form 990-PF :a~ecik here ...•. ~ D b • Tt)X .b.ased.'ot\jrwestmeritinoorna (Fohn 990-PF, Pait v,; lin.~ 5);. , • ·• fa Fonn8'868 check here , , ,.. 0 b Balancia Dµe.'{Forrn 8868, ifne Jo .- , ......•...... , . , , ....
!t-· -~:i,~,_4_4~} . .,.,,-.~~-o-.a-..
3b --~--'-..;....-...c.-.
4 b·-· ·,--..-'---+o--""--'--'-'-
6 b .
. fill]JlllDetlaratiort and Sliinatur~ Authorlzoitio.n ofQffkitW • · .·.. •. ·. . ·. · · · .· · · · <: : : : .' ·: .· · •· · · ·.· .· • · · . . . · · Unde.(P,e~altles of perlUr,i; .f~eclare thal !_am :an o.ffi~r of\he.;~~~va 6rg~nlzalion ahd ihat I, hr;iy~ e,cami~erl a.P.<iPY.~fihef:~rgan~:~~loi\i~. ~01¢: ', · · (;l/e;etron!i; ret4r,:i !J.11.d acoomp_~11Ylng sche(\uj~s an_ci lltf:ltem.e~ts 1;1ntl.t9 the \je~t of my ~OOWIE!qge_imd )lehef, they a.~m!~( f~iwqt,·.a,nct.··CQX!)p!ete. l fMh.E?f ~$~1e,t~-lhat lhE\ _i/J).1Qunt ),n F' art __ I a~.o~e fs Jhe amoµ_nt _show~ on the. .oopy of \ha o~gilhl~a\lon's electron.le ~\lllJ1,, cq_n.s13n_\ ;t_o ~IJpw;nw: intemiedlate. ll~r,.'I~ proV1qer,Ji:a.\1s\l:i.~te.r·, o,r Ei!e~r:oplo r,13tµrn._of]glq~t,;ir (i;;,Rc:_))'to send ihe. organization's return. t<)-_l~e ,IF:{~ .~r1~ l.o-recelv1ffrgm the lRS (a) ·;w acKnbwledgement of.receipt at.reason for reJemtorrof the tr\'\11~mfs$lor\, (b} the reason for any delay tri.processtng the return or. reftHid,•arid (c)'tiie a ale of.a.9Y teftihil' lf·appllta,pli'(,I.'a~l~otfa;:e,-\J\e. b}.i$! rr~~-~9rl i(nd_ its.c\¢..sktna_\et.l, flna11,9lal A,g~nlJc1,\f!'W~t.e, .. a:n, al~cfroh' le funds wijhdrawal (cllreat deo1l)'entry _t9Jhe·flnanc)aJlns.htutlot1.:ac.cotml'.lndloated (n the. Ii½ p_rej:>9fii,1\o.n !l.oftware fo.r paY,r.;)8,J~!:9fJh.e, ..... . organiza,tlop's f.~_d!'lr~l taxes owr,id:oni#.iJs .. rE:Jlum; and.the•fin1;1t)ctal ln$t\lUH?l'l tq 'dellit tn,e entfY .. toothfs a:c~•\t!lj, To revok~.,apay,rn,en.\,:I n:il!.!i!. can lain Hie u,s, 'f r~sury F.!r.u:m!)l!il ·/°}~!l,Ot. a~ 1.-/W~03$'.½1JS~7, t\O l<)ter th~n 2 ~U_$ln~~ c.fayir prlor.,!9 the pavm~nt (s~t~ernep1) d").tl31 J..~ls,p. . . . . . authorize. tn.e ·finil.liolal lnstl!J..ttl.o_n.~ Involved ln-the.prqqe~mg of the ~l~Wo.nto•p/lyrn~nt of t.p/es fo recell/e aoofldenUal lnfonnalj9n·i:ie.r;essary 1o arisw¢r l~qume~ an~. ta.so lye \ssties' U,Jatp:d l9 thE:i .payni(;IOI;_ 1. p~~e ~ele.9-!$.(,i _a pe(~:onal ld,¢lJl)~qa,tJ_ql:i nlililb~r (PlN) as illf sf~.natute for the ·· . organiz.at1on's e!ectronlc return and, lf applicable; the l:i1gan12ai1on1s.'~fls_e9U\l:131_s~t.ronle; fU_T)~~ Wl\htjf~\'11£\l, • · ·
officer's PIN: check.one box oniy . o,f!.~\h~r~e . --.,.....-~,.,.,-·-· ~~~=,.,,_. __ ......_ __ _,._......,._.......,~"'-foenterm~•p1B' ·I.... ·:lasrnYi1lgnature
·ERO .. finnnamn ;"·· · · ··. l:hl~dlva·num!wt'll,"bul ,, :: : • ; · · . · . ~b n·~! onlera\li!i'!"I
Cl\1 llie.6tganiia,i(ori'li ~~_xy~ar 2016 ~leci(~<in!::ally filed return,, lfl ha;y~ lh~(qalerj wjthln !hi!} re.tum That/} (){)py:o:itthe. re!qrn is beJng Hied wtth . a. a tale agenoy(1es). ragµlatmg chari\las as part of \.he JRS'feclJS~ale prograiri,.l ~ls\J l!l.lthorizfi! ll)e ~fors,m~!J!tonl:!<;i EP.O to. enter my PIN on
.. \he. re\urn\\ disclo$ure·consent screen. · ·
@A~ -~11 offipaTofihij ·qrga~lt!ltioh, i will enter my Pl_N ai tnl/'$1gn~tllre on)i)e·~rg~nfi:~tion's tsxy1:\ar,201'e ~°Je~rorilcally flied re\urn, it I hi,we ·. · · :if1dfc1;1lec/ .wtthlil .thlsJetum.th):ll a. ~opy :of th_e. re(Ull) fs._,Pelns ijl_ad.vi!lh _Ii state. ~gency(lea) regQlaUJ}g 01:taolles as. pl:lrl of the IR$ Fad/Slate
• Promarn, I wlll entan~y PIN on the retum1s dJs re coru;ent screen. · · ·,·· . ,'. '• ' :, '· ..
bate·•
'·'·,. •· •• ,.,,,.,, ,oc, •···,,;·I • Wi'55tl'J,3;:l•: I ·,. ; , o T\Q\ ~n et ~.11 zoro:>
i_csnlfy Iha): iti~ ~bpva nume"no-<;')nny::innY,' PIN; wh!9h Is my' sig~atllre on· the 2016"/ileclrQriloaii,i flied returi:i forlhe ilffl~ri!zailon lndioate_d · above. I confirm t\iat ! am .subm1~lln9 this return .In aopordano'a wllh the requ1rernej1\s o!Pu~;. 416?,· Moderi11z1'lq \¼-r.iJ~.(M'~f) lnforrns.lion·for Authorized lRS.:e~lil!-l Provldl'\@fod30alness Retumsi · · · · · · · · ··· ··
bale •, 05/09/ZOf?

NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429
Schedule O (Form 990), Supplemental Information to Form 990 Form 990, Page 6, Line 17 (continued)
Alabama Indiana Ore on Washington Illinois New Mexico Maryland Minnesota New Hampshire Pennsylvania New York South Carolina Connecticut Rhode Island Wisconsin Mississippi
North Carolina Missouri California Ohio Vir inia Massachusetts Oklahoma Geor ia Tennessee Arizona Florida West Virginia Arkansas Alaska Colorado
District of Columbia Hawaii Idaho
Kansas Louisiana Maine Michigan Montana Nebraska Nevada New Jersey North Dakota South Dakota Texas Utah Vermont Wyoming

NATIONAL EMERGENCY MEDICINE ASSOCIATION 52-1257429
Schedule G(Form 990 or Form 990-EZ), Supplemental Information Regarding Fundraising or Gaming Activities Part I, Line 3 List of States Registered or Licensed to Solicit Funds
Hawaii Illinois Indiana Kansas Kentucky Maine Maryland Massachusetts Michigan Minnesota Mississippi New Hampshire New Jersey New York North Carolina North Dakota Pennsylvania Rhode Island South Carolina Tennessee Utah Virginia West Virginia
Schedule O (Form 990 or 990-EZ), Supplemental Information to Form 990 or 990-EZ Form 990, Page 10, Line 24e All Other Expenses (continued)
(A) (B) (C) Description Total Program Management
services and general
SweeEstakes Prizes 4,037. 0. 2,837. Postage & ShiEEing 399,018. 298,754. o. Printing & Publications 597,948. 448,461. o. INTERNET EDUCATION 12, 12. 0. Land Deals 595. 298. 297.
(D) Fundraising
L 200, 1001264, 149 487.
o. o.
2

NATIONAL EMERGENCY MEDICINE ASSOCIATION
AND AFFILIATE
Consolidated Financial Statements
For the Year Ended December 31, 2016

NATIONAL EMERGENCY MEDICINE ASSOCIATION AND AFFILIATE
Independent Auditor's Report
Financial Statements
Consolidated Finandal Statements
For the Year Ended December 31, 2016
Table of Contents
Consolidated Statement of Financial Position Consolidated Statement of Activities Consolidated Statement of Functional Expenses Consolidated Statement of Cash Flows
Notes to Financial Statements
3 4 5 6
7
T ochte L & Company, P.A. Certijied Public Accountants
INDEPENDENT AUDITOR'S REPORT
Board of Directors National Emergency Medicine Association and Affiliate Edgewood, Maryland
11350 McConnick Road Exec. Plaza III, Suite 503 Hunt Valley, MD 21031
443.541.8002 ph. 443.281.8115 fax
www, lochtecpa.com
We have audited the accompanying consolidated financial statements of National Emergency Medicine Association and Affiliate (a nonprofit organization), which comprise the consolidated statement of financial position as of December 31, 2016, and the related consolidated statements of activities, functional expenses, and cash flows for the year then ended, and the related notes to the consolidated financial statements.
Management's Responsibility for the Consolidated Financial Statements
Management is responsible for the preparation and fair presentation of these consolidated financial statements in accordance with accounting principles generally accepted in the United States of America; this includes the design, implementation, and maintenance of internal control relevant to the preparation and fair presentation of consolidated financial statements that are free from material misstatement, whether due to fraud or en-or.
Auditor's Responsibility
Our responsibility is to express an opinion on these consolidated financial statements based on our audit. We conducted our audit in accordance with auditing standards generally accepted in the United States of America, Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements are free from material misstatement.
An audit involves perfonning procedures to obtain audit evidence about the amounts and disclosures in the consolidated financial statements. The procedures selected depend on the auditor's judgment, including the assessment of the risks of material misstatement of the consolidated financial statements, whether due to fraud or en-or. In making those l'isk assessments, the auditor considers internal control relevant to the entity's preparation and fair presentation of the consolidated financial statements in order to design audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the entity's intemal control. Accordingly, we express no such opinion. An audit also includes evaluating the appropriateness of accounting policies used and the reasonableness of significant accounting estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements.
We believe that the audit evidence we have obtained is sufficient and appropriate to provide a basis for our audit opinion.

T ochte L & Company, P.A. Certified Public Accountants
Opinion
In our opinion, the consolidated financial statements referred to above present fairiy, in all material respects, the financial position of National Emergency Medicine Association and Affiliate as of December 31, 2016, and the changes in their net assets and their cash flows for the year then ended in accordance with accounting principles generally accepted in the United States of America.
Emphasis-of-Matter Regarding Going Concern
The accompanying financial statements have been prepared assuming that the Organization will continue as a going concern. As discussed in Note 14 to the financial statements, the Organization continues to incur deficits in net assets and is heavily reliant on its mail order consultant vendor to continue to extend credit to the organization. The Organization has little liquidity \n the event of an unanticipated expenditure or a decrease in contribution revenue. These events raise substantial doubt about its ability to continue as a going concem. Management's plans regarding these matters are also described in Note 14. The financial statements do not include any adjustments that might result from the outcome of this uncertainty. Our opinion is not modified with respect to this matter.
Hunt Valley, Maryland May 1, 2017
NATIONAL EMERGENCY :MEDICINE ASSOCIATION & AFFILIATE Consolidated Statement of Financial Position
Current Assets Cash & Cash Equivalents Other Receivables
Marketable Equity Securities Prepaid Expenses
Total Ciwrent Assets
Property & Equipment
Furniture & Fixtures
Computer Hardware & Software Less: Accumulated Depreciation
Net Property & Equipment
Other Assets
Restricted Cash
December 31, 2016
ASSETS
Investments in Limited Partnerships - Apartment Projects Security Deposits
Total Other Assets
Total Assets
Current Liabilities Accounts Payable Accrued Expenses
Total Current Liabilities
Long-'Term Liabilities
Total Liabilities
Net Assets Unrestricted Temporarily Restricted
Total Net Assets
LIABILITIES AND NET ASSETS
Total Liabilities and Net Assets
$ 171,289 5,294
27,100 8,763
212,446
3,403
5,169 (5,564)
3,008
53,926
36,775 867
91,568
$ 307,022
$ 455,920 2,673
458,593
458,593
(176,857) 25,286
(151,571)
$ 307,022
The accompanying notes are an integral part of these financial statements. 3

NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE
Consolidated Statement of Activities
For the Year Ended December 31, 2016
Temporarily
Changes in Net Assets: Unrestricted Restricted
Public Support & Other Revenues Public Suppo1i:.
Contributed Public Support $ 1,388,282 $ -Bequests 25,000 9,427
Total Public Support 1,413,282 9,427
Other Revenues: Mail List Rentals 21,125 Investment Income 1,284
Total Other Revenues 22,409
Total Public Support & Othel' Revenues 1,435,691 9,427
Net Assets Released from Restriction 10 887 (10,887)
Total Public Support, Other Revenues & Reclassifications 1,446,578 (1,460)
Expenses Program Services:
Public Health Education 973,070
Supp01ting Services: Development 366,269 Management & General 143,898
Total Supporting Services 510,167
Total Expenses 1,483,237
Change in Net Assets (36,659) (1,460)
Net Assets - Beginning of Year (140,198) 26,746
Net Assets - End of Year $ ~176,857) $ 25,286
The accompanying notes are an integral pa1t of these financial statements. 4
$
$
$
Total
1,388,282 34,427
1,422,709
21,125 1,284
22,409
1,445,118
1,445,118
973,070
366,269 143,898
510,167
1,483,237
(38,119)
(113,452)
(151,571)

Allocated Joint Costs:
Data Processing
Producation Expense
List Costs
Mailing Services
Occupancy Expense
Office Expense
Postage & Shipping
Printing & Publications
Prof Fees & Contracts
Salaries, Taxes & Benefits
Subtotal
Other Expenses:
Grants
Land Deals
Sweepstakes Prizes
Subtotal
TOTAL COSTS
NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE
Consolidated Statement of Functional Expenses
For the Year Ended December 31, 2016
PROGRAM SERVICES SUPPORT SERVICES p ti b Ii C Health Education
Video I
Pr/111 Media I Other Radio/ TOTAL Mgmt
Ed11c11tio11 Pti11t llltemel PROGRAM a11d
/11(ormatio11 Ed11catio11 Ed11catio11 SERVICES Develop111e11t General
$ 21,822 $ 191 $ 191 $ 22,204 $ 11,660 $ 22,343
400 400
9,865 9,865 14,798
39,812 1,835 41,647 41,648 20,824
6,621 6,621 2,206 2,206
11,115 1,024 512 12,651 1,739 30,095
298,366 298,366 100,264
448,461 448,461 149,487
16,174 212 212 16,598 6,016 28,640 95,340 7,760 7,760 110,860 36,954 36,953
947,976 11,022 8,675 967,673 364,772 141,061
5,099 5,099
298 298 297
1,200 2,837
5,397 5,397 1,497 2,837
$ 953,373 $ 11,022 $ 8,675 $ 973,070 $ 366,269 $ 143,898
The accompanying notes are an integral part of these financial statements. 5
TOTAL
SUPPORT
SERVICES
$ 34,003
14,798
62,472
4,412
31,834
100,264
149,487
34,656
73,907
505,833
297
4,037
4,334
$ 510,167
TOTAL
EXPENSES
$ 56,207
400
24,663
104,119
11,033
44,485
398,630
597,948
51,254
184,767
1,473,506
5,099
59:i
4,037
9,731
$ 1,483,237

NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE
Consolidated Statement of Cash Flows
For the Year Ended December 31, 2016
Cash Flows From Operating Activities
Change in Net Assets
Adjustments to Reconcile Change in Net Assets
to Net Cash Provided by Ope1"ating Activities:
Depreciation Expense
Unrealized Gain on Marketable Equity Securities
Inventory Obsolescence (Increase) / Decrease in Operating Assets:
Other Receivables
Prepaid Expenses
Restricted Cash
Increase/ (Decrease) in Operating Liabilities:
Accounts Payable
Accrued Expenses
Net Cash Provided by Operating Activities
Cash Flows From Investing Activities
Purchase of Marketable Equity Securities
Net Cash Used by Investing Activities
Net Increase in Cash & Cash Equivalents
Cash & Caslt Equivalents - Beginning of Year
Cash & Caslt Equivalents - End of Year
The accompanying notes are an integral part of these financial statements, 6
$
$
(38,119)
1,715
(709)
2,714
4,877
2,142
771
66,380
(288)
39,483
(541)
(541)
38,942
132,347
171,289

NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE Notes to Financial Statements
December 31, 2016
NOTE 1: Description of Business and Summary of Significant Accounting Policies
Purpose of the Association and Related Organization
The National Emergency Medicine Association was incorporated in the District-of Columbia in 1982. Its special prngrams are concerned with the prevention of injury and illness by addressing health and social issues through education, applied research, tech11ology, and equipment. The Organization also exists to develop and support low-income housing projects for persons of limited financial means and other persons in need of safe and adequate housing.
Emergency Medicine Support Foundation, 1nc. was established to support the charitable purposes of the National Emergency Medicine Association. The Organization primarily will promote the Association's charitable purposes by providing funds and other support to enable the Association to carry out its taxexempt mission. The Organization also may provide grants to universities, institutions and scientists engaged in cardiac-related clinical and applied research, including research on the causes, treatment, and prevention of cardiovascular diseases.
Principles of Consolidation
The consolidated fmancial statements include the accounts of National Emergency Medicine Association and Emergency Medicine Support Foundation, foe. (the "Organization"). National Emergency Medicine Association has both an economic interest in Emergency Medicine Support Foundation, Inc. and control of the Organization through a majority voting interest in its governing board. All material inter-organization transactions have been eliminated.
Basis of Presentation
The Organization follows the Financial Accounting Standards Board (F ASB) Accounting Standards Codification (ASC) 958, Not-for-Profit Entities. I11 accordance with FASB ASC 958, the Organization is required to report information regarding its financial position and activities according to tlu-ee classes of net assets: umestricted net assets, temporarily restricted net assets, and permanently restricted net assets.
Net assets of the two restricted classes are created only by donor-imposed restrictions on their use. All other net assets, including board-designated or appropriated amounts, are legally umestricted, and are reported as part of the umestricted class. The organization has no permanently restricted net assets.
Use o(Estimates
The preparation of consolidated financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and assumptions that affect the 1'epo1ied amounts of assets and liabilities, the disclosure of contingent assets and liabilities, and the reported amounts of revenues and expenses. Accordingly, actual results could differ from those estimates.
Cash Equivalents
For the purpose of the statement of cash flows, the Organization considers all highly liquid sho1i-term investments purchased with maturities of three months or less to be cash equivalents.
7

NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE Notes to Financial Statements
December 31, 2016
NOTE 1: Description of Business and Summary of Significant Accounting Policies (Cont,)
Inventories
Inventories during 2016 consisted entirely of finished goods comprised of cards, informational booklets, and videos, Inventories are valued at the lower of cost or market. Cost is determined by the first-in, firstout method (FIFO). Inventory was written down by $2,714 in 2016 to reflect obsolescence, There is no inventory on hand as of December 31, 2016,
Allowance for Doubt/ii! Accounts
Receivables are stated at unpaid, balances, less an allowance for doubtful accounts. The Organization provides for losses on contribution and list receivables using the allowance method. The allowance is based on experience, a review of each individual receivable, and the Organization's history of uncollectible accounts, It is the Organization's policy to charge off receivables when management determines the receivable will not be collected. All of the Organization's receivables are deemed collectible as of December 31, 2016,
Fixed Assets
Expenditures for fixed assets purchased are recorded at cost and are depreciated on the straight-line basis over their estimated useful lives of three to seven years. Depreciation expense for the year ended December 31, 2016 amounted to $1,715. The Organization capitalizes all individual purchases with a cost over $500.
Investments
Investments in all debt and equity securities with readily determinable fair values are reported at fair value and totaled $27,100 at December 31, 2016,
Investments in apartment project limited patinerships, received as donations to the Organization, ai·e stated at estimated fair value as of the date of receipt and accounted for by use of the cost method whereby income is recognized based solely on cash distributions (see Note 4).
All other investments are repo1ied at historical cost, if purchased, or, if contributed, at fair value at the date of contribution,
Investment income, gains, and losses ai·e reported as increases or decreases in unrestricted net assets if the restrictions are met (either a stipulated time period ends or a purpose restriction is accomplished) in the reporting period in which the income 01· gains are recognized, Investment Income totaled $1,263 for the year ended December 31, 2016 and was comprised of$393 in dividends and interest income, $161 in capital gain and $709 in umealized gain in mutual and government securities funds.
Advertising Costs
Direct response advertising costs totaled $394,586 for the year ended December 31, 2016, and relates to the Organization's direct and sweepstakes mailings through a consultant. These costs are expensed as incurred since the advertising is primarily fund-raising in nature.
8
NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE Notes to Financial Statements
December 31, 2016
NOTE 1: Description of Business and Summary of Significant Accounting Policies (Cont.)
Donated Goods and Services
Donated materials and equipment are recorded at their estimated value at date of receipt. No amounts are recognized for donated services since no objective basis is available to measure the value of such services.
Contributed Public Support
The Organization recognizes all contributed public suppoti, including unconditional promises to give, as revenue in the period received. Contributed public supp01i is rep01ied as umestricted or restricted depending on the existence of donor stipulations that limit the use of the support. Support that is restricted by the donor is reported as an increase in umestricted net assets if the restrictions are met in the reporting period in which the support is recognized.
Donated assets are recorded at estimated fair value on the date of donation. It is the Organization's policy to repo1i the receipt of long-lived assets as umestricted support, absent explicit donor stipulations about how the assets must be used or how long these assets must be maintained.
Grants Awarded
The Organization recognizes the expense of the program grant and the associated liability in the year in which the Board of Directors awards the grant. The Organization awards grants for heati, stroke and other medical and social emergency related issues. Grants are awarded by the Board of Directors based on recommendations made by the Grant Advisory Council, which is separate from the Board. The responsibility of the Council is to revie_w grant requests and to advise the Board of Directors. Both the Board and the Council are subject to a conflict of interest policy under which a member is disqualified from evaluating any grant proposal submitted by an organization or institution with which the patiicular member is affiliated.
Jncoine Taxes
Under section 501(c)(3) of the Internal Revenue Service Code, the Organization is exempt from ta,"'\:es on income other than umelated business income. The Organization has been classified as an organization that is not a private foundation under Section 509(a)(2).
As required by the F ASB ASC regarding income taxes, the Organization is required to disclose any ta.,'s. positions that would result in unrecognized tax benefits. The Organization has no positions that would require disclosure or recognition under the topic. Generally, the exempt tax returns filed by the Organization are subject to examination by the Internal Revenue Service for a period of three years after they are filed. The Organization is subject to examination of its Forms 990 for the years ended December 31, 2013, 2014, 2015, and 2016.
9

NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE Notes to Financial Statements
December 31, 2016
NOTE 1: Description of Business and Summary of Significant Accounting Policies (Cont.)
Functional Allocation of'Expenses
In the consolidated statement of activities, all expenses, including salaries, taxes and benefits, are charged to the various programs, development, and management and general expenses on the basis of actual expense,
Subsequent Events
Subsequent events are evaluated through May l't, 2017 which is the date the financial statements were available to be issued,
NOTE 2: Other Receivables
Other receivables at December 31, 20 l 6 are comprised of $5,294 in mail list rentals, These receivables are scheduled to be collected in calendar year 2017, are unsecured, and have no stated interest rate,
NOTE 3: Restricted Cash
The Organization maintains two restricted cash accounts at December 31, 2016. One account is comprised of current and prior year donor contributions with restricted uses. This account is designated to be used strictly for activities related to the National Stroke Council. The restricted balance in this account amounts to $25,286 as of December 31, 2016,
The Organization stmied a new mail program in 2015 called "Kids Do Matter," The organization and the program and development consultant entered into an agreement in which the consultant required that all collections related to program and development mailings related to this new mail program be escrowed while the success of the program is evaluated. The expenses related to this program will be paid to the consultant out of this account. The organization's liability under this program is limited to funds escrowed, The balance in this account at December 31, 2016 totaled $28,640, The agreement can be terminated at any time by either pmiy.
NOTE 4: Investments in Limited Partnerships -Apartment Projects
In prior years, the Organization received an assignment of an interest in a federally assisted multi-family housing project as a charitable contribution, The total estimated fair market value assigned to this interest was $36,775, which was net of fees upon collection. The estimated fair value of this interest was based on prior year audited partnership financial statements on dates of contribution and property appraisals in most cases, less a significant discount since these units were of uncertain value because there is no readily available secondmy market. The limited partnership interest is accounted for on the cost basis of accounting because of the lack of control exercised by the Organization and the fact that there is no readily available secondary market, The original assigned fair market value has remained unchanged. While the fair value of the remaining limited partnership interest is still not readily determinable, management monitors the estimated fair market value based on info11nation repo1ied on Form 1065, Schedule K-1, which informs the Organization of its annual po1iion of the related tax. gain or loss and its
10

NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE Notes to Financial Statements
December 31, 2016
NOTE 4: Investments in Limited Partnerships -Apartment Projects (Cont.)
capital account balance. There have been no partnership distributions since the Organization obtained the partnership interest. Management believes that the value is reasonable.
At December 31, 2016, the following limited pa1inership interest was accounted for on the cost basis of accounting:
Partnership Name
Stratton Hill Associates, LLC
Ownership%
6.786%
NOTE 5: Direct Mail Development and Educational Program
Cost
$ 36.775
The Organization conducts its own mail program activities with the counsel and management suppo1i from a single direct mail marketing organization. These mailings are the method in which the Organization generates the majority of its public suppoti.
NOTE 6: Allocation of Joint Costs
In 2016, the Organization incunedjoint costs of$1,473,506 for informational materials and activities that included fundraising appeals. The cost of providing the various programs and activities has been summarized on a functional basis in the consolidated statement of functional expenses. These joint costs have been allocated to the various program and supporting services by the Organization's management.
The basis of allocation was as follows:
a. Grant Programs - costs involved in selecting and approving grant recipients.
b. Print Media Education - content of mailings directed at fund raising appeals, public awareness and education, and on allocated salaries and related indirect costs based on employee time.
c. Other Print Education and Information - printed materials addressing heart trauma, stroke trauma, parenting skills and children's concerns. Salaries and other related costs allocated based on employee time.
d. Video, Internet and Other Education - costs attributable to alerting the American Audience of emergency medical care, hea1i trauma, stoke prevention, parenting skills and children's concerns.
11

NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE Notes to Financia.l Statements
December 31, 2016
NOTE 6: Allocation of Joint Costs (Cont.)
The costs were allocated as follows:
Program Se1·vices Print Media Education Other Print Education
Yid~o, Internet and Oth~r Edll'3atf on ..
;Support ~e_1Y.,i~e!. . ...... . Development Management ~11_<:l_ C}eneral
Total Allocated Joint Costs
NOTE 7: Allocation of Functional Expenses
$
$
947,976
11,022
8,675 967,673
- ,,. - . --- . - -~-" .,. ....... --- ..
' 3~1,Tt} 141,061
505,833
1,473,506
64%
1%
1%
66%
25%
9% 34% ·
100%;
The costs of providing the various programs have been summarized on a functional basis in the consolidated statement of functional expenses. Accordingly, certain costs have been allocated among the programs and suppo1ting services benefited.
NOTE 8: Concentration of Suppliers
The Organization utilizes one marketing agency to print all of its educational and fundraising mailings. The total expense incurred to this marketing agency in 2016 was $1,196,598 which represents 83% of the total expenses in 2016.
NOTE 9: Net Assets
The Organization classifies net assets into three categories: ·unrestricted, temporarily restricted and permanently restricted. All net assets are considered to be available for umestricted use unless specifically restricted by the donor or by law. Temporarily restricted net assets include contributions with temporary, donor-imposed time or purpose restrictions. Temporarily restricted net assets become unrestricted and are reported in the statement of activities as net assets released from restrictions when the time restrictions expire or the contributions are used for the restricted purpose.
It is the policy of the Organization to treat the temporarily restricted contributions for which the restrictions were satisfied in the year received as unrestricted support.
12

NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE Notes to Financial Statements
December 31, 2016
NOTE 9: Net Assets (Cont,)
Temporarily restricted net assets are comprised of current and prior year contributions that were restricted to be spent on the National Stroke Council, plus interest earned on these restricted funds. The balance at December 31, 2016 was $25,286.
All of the Organization's other assets as of December 31, 2016 were umestricted.
NOTE 10: Defined Contribution Plans
The Organization commenced a Safe Harbor 40 l(k) plan for its employees in 2007. The plan covers employees who work in excess of 1,000 hours per year. Employees can make contributions to the plan up to the maximum amount allowed by the Internal Revenue Code. The employer contributes matching amounts equal to 100% of employee elective defe11'als to the extent that such elective deferrals do not exceed 3% of compensation for the plan year and 50% of elective deferrals to the extent such elective deferrals exceed 3% but do not exceed 5% of employee compensation for the plan year. The employer, at its discretion, can make profit sharing contributions to the plan based upon employee compensation for the year. Profit sharing contributions are subject to a vesting schedule in which employees vest at 20% per year of service with full vesting achieved after six years of service.
Employer matching contributions totaled $2,548 in 2016. There were no employer profit sharing contributions in 2016.
NOTE 11: Operating Lease
The Organization signed a five year, non-cancelable operating lease in December 2013 and moved its office from the President's house to a commercial building. Rental expense totals $919 per month, including all utilities. The rent increases 3 % per annum over the term of the lease. Rental expense in 2016 under this agreement totaled $11,033.
Future minimum lease payments for the initial term under this lease agreement as of December 31, 2016 is as follows:
2017 · 11,364 • 2018 10,730
Total $ 22,094
NOTE 12: Fail' Value Measurements
13

NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE Notes to Financial Statements
December 31, 2016
Financial Accounting Standards Board (F ASB) Accounting Standards Codification (ASC) 820, Fair Value Measurements and Disclosures, provides the framework for measming fair value, That framework provides a fair value hierarchy that prioritizes the inputs to valuation teclmiques used to measure fair value. The hierarchy gives the highest priority to unadjusted quoted prices in active markets for identical assets or liabilities (level 1 measurement). And the lowest priority to unobserved inputs (level 3 measurements). The three levels of the fair value hierarchy under FASB ASC 820 are described as follows:
Inputs to the valuation methodology are unadjusted quoted prices for identical assets or liabilities in active markets that the Organization has the ability to access.
Level 2 Inputs to the valuation methodology include: • Quoted prices for similar assets or liabilities in active markets; • Quoted prices for identical or similar assets or liabilities in inactive markets; • Inputs other than quoted prices that are observable for the asset or liability; • Inputs that are derived principally from or corroborated by observable market data by
correlation or other means. If the asset or liability has a specified ( contractual) term, the level 2 input must be observable for substantially the full term of the asset or liability.
Inputs to the valuation methodology are unobservable and significant to the fafr value measurement.
The asset or liability's fair value measurement level within the fair value hierarchy is based on the lowest level of any input that is significant to the fair value measurement. Valuation techniques used need to maximize the use of observable inputs and minimize the unobservable lnputs,
Following is a description of the valuation methodology used for assets measured at fair value, There have been no changes in the methodologies used at December 31, 2016,
},;Janey market funds are valued at cost, which approximates fair value, These assets were measured within Level l of the hierarchy described above.
U.S. government securities are valued at the closing price repo1ted on the active market on which the individual securities are traded.
Mutual fimds are valued at the net assets value ("NA V") of shares held by the plan at year end.
The investment in Limited Partnerships - Apartment Projects was measured at cost which approximates fair value based on management's estimates. These assets were measured within Level 3 of the hierarchy described above.
The preceding methods described may produce a fair value calculation that may not be indicative of net realizable value or reflective of future fair values, Fu1thermore, although the Organization believes its valuation methods are appropriate and consistent with other market paiticipants, the use of different
NOTE 12: Fair Value Measurements (Cont.) .
14

NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE Notes to Financial Statements
December 31, 2016
methodologies or assumptions to determine the fair value of certain financial instruments could result in a different fair value measurement at the reporting date.
The following tables set forth by level, within the fair value hierarchy, the Organization's assets at fair value as of December 31, 2016:
Fair Value Measurements at Decembe1· 31, 2016
Level 1 Level2 Level 3 Total
Money Market $ 57,838 $ - $ - $ 57,838
".2-27.Y.~f!.11:?:,~!!!?JS~Xt~x. , .. · .. •. ••· .,· ,oc~•••=t2,874_ - - ..1?.,~24., '-'-'__::::::-...;:._-= •• ~ ·_-;-_ ... ____ ;::-== .. - - .,.
Mutual Fund 14,226 - - 14,226
Limited Partnership Stratton Hill Associates - - 36,775 36,775
Total Investment $ 84,938 $ - $ 36,775 $ 121,713
There was no change in value on the level 3 investment.
NOTE 13: Schedule of Changes in Consolidated Net Assets
The Schedule of Changes in Unrestricted Net Assets for the year ended December 31, 2016 by organizational entity is as follows:
NEMA EMSF TOTAL
Unrestricted Net Assets 01/01/16 $ <
$ 3,237 $
143,435> <140,198>
Decrease for the Year Ended 12/31/15 <36,290> <369> <36,659>
Unrestricted Net Assets 12/31/15 $ <179,725> $ 2,868 $ <176,857>
All of the temporarily restricted net assets in 2016 relate to National Emergency Medicine Association (NEMA),
15
NATIONAL EMERGENCY MEDICINE ASSOCIATION & AFFILIATE Notes to Financial Statements
December 31, 2016
NOTE 14: Contingency - Going Concern
As indicated in the accompanying financial statements, the Organization incurred an operating deficit in 2016, and has a deficit of $176,857 in unrestricted net assets at December 31, 2016. There are few remaining expenses that can be further reduced without affecting operations. The organization has little liquidity as evidenced by a current ratio of .46.
Additionally, the mail order consultant is the Organization's largest creditor with a payable balance of $455,717 at December 31, 2016. The consultant has verbally indicated that they will continue to work with the Organization, but there is no contractual obligation. The Organization is heavily reliant on the mail order consultant's continued collaboration in regards to extension of credit and continued willingness to initially fund mailings so that the organization can continue to generate contributions.
Management continues to monitor expenses and the success of the direct mail program. Management, in conjunction with the mail order consultant, initiated a new program in 2015. Gross revenues to the Organization increased in 2016 and management anticipates this trend continuing in 2017. The ability of the Organization to continue as a going-concern is dependent on the success of management's effotis to manage costs and increase its revenue base, in addition to the willingness of the mail order consultant to continue working with the Organization to raise funds. The :financial statements do not include any adjustments that might be necessary if the Organization is unable to continue as a going concern.
16

Exhibit C

9/7/2018 Charities: Entity Detail
cs 9773
Office of the Attorney General Bill Schue1te 1 Attorney Gonflrnl
National Emergency Medicine Association, Inc.
Mailing Address: National Emergency Medicine Association, Inc. 500 Edgewood Rd. Ste. 105 Edgewood, MD 21040
Phone:
Email:
Website:
ORGANIZATIONAL INFORMATION
( 443)922-7533
www.nemahealth.org
Entity Type: Corporation State Established: DC Date Created: 01/20/1982
501(c)(3): Yes EIN: 52-1257429
Purpose Statement: EDUCATION ON THE PREVENTION OF INJURY AND ILLNESS.
FILING STATUS
Solicitation Registration Status
Expiration Date: 12/31/2017 Renewal Registration Pending
Charitable Trust Registration Status
Exempt
FINANCIAL INFORMATION Data is taken from the organization's IRS return or, if no return
was filed, from its solicitation registration or financial statements.
Period Ending 12/31/2016 Reports Filed 990/CPA Audit
Total Revenue
Total Expenses
Revenue Less Expenses
$1,444,408.00
$1,482,867.00
($38,459.00)
Total Assets
Net Assets
Expense breakdown
Charitable Programs Program Services
Supporting Services Mgt & General* Fun draising *
http://www.ag.state.mi.us/CharitableTrust/frmSearchResults.aspx
$972,700.00
$143,898.00 $366,269.00
$304,154.00
($154,439.00)
% of Total Expenses
65.60 %
9.70 % 24.70 %

9/7/2018 Charities: Entity Detail
Total Supporting Services $510,167.00 34.40 %
*If an organization files IRS Fonn 990-EZ or 990-PF, Supporting Services expenses may not be broken down into Mgt & General and/or Fundraising.
The information in this report is taken fi·om i11formation provided to the Michigan Attorney General by the organization or its agents. The Attorney General's office does not guarantee the accuracy or completeness of any of the information included. ff you notice any errors, please contact the Charitable Trust Section.
Additional Program Services Infonnation This organization claims that when it is soliciting or fundraising it is also can-ying out its charitable mission.
For example, a mailing may include infonnation about a medical condition or remind you to pull over when you hear a siren. Or, a telephone solicitor, while asking for a contribution, might ask if you know someone who could use the charity's services.
Thus, if you received a mailing or were called on the telephone, a portion of the cost of that mailing or telephone call may have been counted as part as of its charitable program (and also not counted as a fundraising cost).
Why should you know? For some charities, their largest charitable activity consists of services they provide while soliciting contributions. A very high percentage in the box below means that, according to its own financial reports, this charity perfmmed few program services outside of those conducted during solicitations.
You should know the facts so that you can decide if this activity is something you want to support.
Program Services Conducted During Fundraising
$967,673.00
PROFESSIONAL FUNDRAISERS
As% of All Program Services
99.48 %
This organization has, or recently had, contracts with the following professional fundraisers. Contact the Charitable Trust Section if you would like a copy of a contract or other information.
Charity/ Professional Fundraiser
Nat'l Emergency Med Assoc./ Newport Creative
National Emergency Medicine Association/ Aegis3 Fundraising Group
Contract Type
Consulting
Consulting
The information on these pages is taken from information provided to the Michigan Attorney General by the organization or its agents. The Attorney General's office does not endorse or promote any of the organizations or professional fundraisers listed on these pages. The Attorney General's office does not guarantee the accuracy or
completeness of any of the infonnation included. If you notice any errors, please contact the Charitable Trust Section.
http://www.ag.state.mi.us/Charitab\eTrustifrmSearchResults.aspx 2

Exhibit D
ST ATE OF MICHIGAN DEPARTMENT OF ATTORNEY GENERAL
BlLL SCHlJE'ITE ATTORNEY GENER.AL
January 16, 2016
Kelly Herzog, President National Emergency Medicine Association 500 Edgewood Road, Suite 105 PO Box 1039 Edgewood MD 21040
Re: National Emergency Medicine Association ("NEl\,L~") MICS 9773
Dear M. Herzog:
P.O. Box 30214 LANsn~G. MICHIGAN 48909
Last year, we received the Registration to Solicit Donations form of the above organization. Please also provide the following additional information with respect to the organization's submission:
1. The solicitation form indicated that NEMA neither had a contract during 2016 nor a contract at the time of submitting the form with a professional fundraiser. Has the organization's contract with Newport One ended? If so, please provide the date the contract ended. In either event, also complete he enclosed professional fund raiser schedule for Newport.
2. Similarly, our records reflect that NEJVIA had a contract with Aegis3 Fundraising Group. Please complete the enclosed schedule with respect to this contract.
3. According to Part VII, Section B of the Form 990, NEMA compensated Newport One $1,196,598. However, Schedule G, Part I reports that Newport only retained $19,239 of gross receipts. This discrepancy appears to be explained in Schedule G, Part IV which states that Newport's invoices breakout consulting fees from other costs. Regarding this matter:
a. Does NEMA separntely pay printing, postage, paper, mail list rental costs?
b. Provide a representative copy of a Newport 2016 invoice.
c. Provide a copy of the 1099 submitted to the IRS for Newport's fees for 2016.

Kelly Herzog, President National Emergency Medicine Association Page 2 January 16, 2018
4. Please provide the following information with respect to the organization's 2016 Form 990:
a. Prnvide a schedule of grants or assistance given with respect to the $3,300 reported on Part IX, line 1.
b. Part IX, line llb reports $13,740 in legal fees of which $1,847 was allocated to program services. Explain and justify the allocation to program services of legal fees.
c. Provide a schedule of Other fees reported on line 11g in the amount of $14,523. The schedule should include the name of each payee, the services provided, and the dollar amount paid.
d. Provide a schedule of other expenses reported on Part IX, line 24e. The schedule should itemize the expenses and show how each was functionally allocated. Note that, according to the form instructions, this information should have been reported on Schedule 0
e. Explain the basis for the percentage allocated to program services of each item that comprises line 24e.
5. Provide copies of all solicitation materials used by NEMA during 2016 including all versions of telemarketing scripts, internet solicitations (webbased and email), invoices or any other fulfillment requests, letters, envelopes, brochures, pamphlets and all other printed material.
6. Provide copies of all solicitation materials used by NEMA during 2017 including all versions of telemarketing scripts, internet solicitations (webbased and email), invoices or any other fulfillment requests, letters, envelopes, brochures, pamphlets and all other printed material.
7. We note that, according to its Form 990 and financial statements, NElVIA has allocated joint costs to program services. Please provide the information and supporting documentation requested below:
a. Provide a schedule that shows all expenses considered joint costs included in the joint costs allocation and that shows how each line was allocated with an explanation as to how the allocation was cletrmined.
b. Describe the program service that was conducted during the solicitations.

Kelly Herzog, President National Emergency Medicine Association Page 3 January 16, 2018
c. What was the purpose of the joint activity? What evidence did the auditor use or see that showed that the purpose of the activity was to further the mission of the organization?
d. What was the "call to action'' requested of the audience in the solicitations?
e. Is the program, including the call to action, conducted on a similar scale using the same medium without the fund-raising appeal? If so, please provide details and samples of materials used in that program.
f. Describe how the audience was selected for campaigns in which costs were allocated to program services. Provide names and descriptions of all donor lists acquired.
g. Identify which lists include persons that previously made contributions to NEMA.
h. For the lists that include previous donors, explain in detail how the presumption that the audience criterion was not met was overcome.
1. Provide the name and address of the owner of each contact, or donor, list.
J. Note 6 to the audited financial statements, which explains the joint cost allocations, includes Grant Programs in the discussion. Explain why Grant Programs are considered as part of joint costs. What solicitation activity takes place during Grant Programs?
k. Note 6 states that joint costs have been allocated based on employee time. With respect to this matter:
1. Provide the names and titles of the employees whose time was used to determine the joint cost allocation.
n. Provide details of the time study that was used to determine the joint cost allocation.
m. Explain how it was determined that certain employee time was program, management & general, OT fundraising related.
1v. Explain in detail the calculation of the joint cost allocations.

Kelly Herzog, President National Emergency Medicine Association Page 4 January 16, 2018
v. Which expense items were allocated based on employee time?
JJK
Please provide the requested information by February 16, 2018.
Very truly yours,
; -( >; l/1l /,:'.•'·c-'0 -· : -r'I--J;/f _,.--· ( '"_::::,. -·1 · \ __ ,_..,.. .. ~
JosepiJ/ Kylman Auditor Charitable Trust Section (517) 373-1152
Exhibit E
National Emergency Medicine Association Edgewood Professional Building
500 Edgewood Road, Suite 105 P.O. Box 1039 · Edgewood, MD 21040
443-922-7533 Fax: 888-682-7947 Web Address: www.nemaheaJth.org ~ E-mail: [email protected]
March 20, 2018
VIA E-MAIL
Mr. Joseph J. Kylman Audhor, ChmitabJe Trust Section State of Michigan Depruiment of Attorney General P.O. Box 30214 Lansing, Ml 48909
Re: National Emergency Medicine Association ("NEMA") MICS 9773
Dear Mr. Kylman:
Jam in receipt of your January 16, 2018 letter in which you requested additional information in connection with NEMA's 2017 Registration to Solicit Donations form ("Fom1") and NEMA's 2016 IRS Form 990. Thank you for agreeing to ru1 extension of time until March 23, 2018 to submit this response. NEMNs responses are set forth below:
Question 1: The indication in the Form that NEMA neither had a contract with a professional fundraiser during 2016 nor had a contract with a professional fundraiser when the Form was submitted was an inadvertent error. NEMA used Newport Creative Communications C'NCC") as its fundraising consultant during 2016. A copy of the contract between NEMA and NCC is included with this response. Also attached is the completed professional fundraiser schedule, item #9 of the F01n1> for NCC ("Schedule").
Question 2: NEMA retained Aegis3 Fundraising Group as its fundraising consultant effective January 1, 2017 and this contract covers the period Jrumary 1, 2017 - December 31 > 2019. A copy of this contract is included-with this response. NEMA cannot complete the Schedule for Aegis 3 Fundraising Group until NEtv'lA's 2017 audit is completed and its 2017 IRS Fonn 990 is filed. After such time, NEMA will be able to complete and submit the Schedule to you in regard to Aegis3 Fundraising Group .
.$.Qecia/ Prog_rams
N,\TION.-\L f}(•:,~'1'. cou.~uL." l"
l NNl'.lONAL . · S'l'lWiffi .. I COUNCIL ..
Questilin 3: Compensation paid to NCC.
a. NEMA did not pay printing, _postage; paper, or mail list rental costs separately. All such costs were included with the payments sent to NCC.
b, Attached is a copy ofNCC's December 2016 invoice which includes a spreadsheet "breakout" for each cost item.
c. NCC is a corporation. NEMJ-\ was not required to and did not submit Form 1099-MlSC in regard to the payments it made to NCC for the services NCC provided to NEMA in 2016,
Question 4: 2016 Fo1m 990
a, The itemization of the $3,300 in grants made in 2016 is set forth below:
May 24, 2016-NEMA made a grant in the amount of $200 to the Harford,County, Maryland Chamber of Connnerce to enable disabled and disadvantaged persons to attend the circus.
June 21, 2016- NEMA made a grant in the amount of $100 to Operation Support Our Troops for the purchase of sunscreen and other necessities for military personnel stationed overseas,
October 18, 2016 - NEMA made a grant in the amount of $3,000 to Maryland Search and Rescue for the purchase/acquisition of portable defibrillators, specialized backpacks for emergency medical service perso1111el and other first responders (ALS backpacks), special combat application (CAT) tourniquets, structural aluminum malleable (SAM) splints, first responder kits, and chemical wam1 packs.
b. Prut IX, line 11 b, reported $13,740 in 1egal fees of which $1,847 was allocated for program services. See, attached excerpt from NEMA's general ledger which sets fotth an itemization/schedule that explains this allocation. ·
c. Other fees reported on line 1 lg in the amount of $14,523 are listed in the attached excerpt frorn NEMA' s general ledger which sets forth an itemization/schedule that explains these fees.
d. Part IX, line 24e, reported other expenses, The schedule of itemized expenses for line 24e is included in Schedule 0. See, the attached document which sets forth an itemization/schedule that explains these expenses.
e, The percentage allocated to program services in regard to the items set forth in line 24e is based on an employee time study, a copy of which is included. Also attached is the 2016 allocation spreadsheet.
Question 5: Copies of all solicitation materials for 2016 are included. No internet solicitations; invoices, or any other fulfillment requests, letters, envelopes, brochures, pamphlets or other printed materials were -used for solicitation purposes by NEMA in 2016,
Question 6: Copies of all solicitation material for 2017 included. No intemet solicitations, invoices, or any other fulfillment requests, letters, envelopes, brochures, pamphlets or other printed materials were used for solicitation purposes by NEMA in 2017.
Question 7: Infom1ation and suppo1iing documents in regal'd to joint cost allocations to program services are set forth below.
a. The schedule that sets forth al! expenses considered joint costs and that was used for allocating joint costs is the same 2016 allocation spreadsheet that is provided in response to question 4e. The percentages allocated are determined by the employee time study that is also being provided in response to question 4e.
b. The program services that were conducted in connection \.Vith the solicitation$ include providing educational materials concerning heart attacks, strokes and other cardiovascular events and Alzheimer's disease. All such material was provided free-of-charge to the public.
c. and d. The purpose of the joint activity was to advance NEMA's charitable purposes of providing information to the public concerning various diseases, health emergencies and related trauma situations and prophylactic measmes to take to prevent and reduce the incidence and severity of such diseases, emergencies and trauma situations. See below in regard to further information concerning such purposes and the "ca!J to action'' requested of the audience in the solicitations.
NEMA determined for 2016 and 2017 that it satisfied the three criteria set forth in FASB ASC 958-720-45, subsection 45-28, namely the purpose, audience and content criteria regarding Accounting for Costs of Activities that include Fundraising. These determinations were based on the nature and content of the combined educational campaigns and fundraising solicitations ("Mailings") sent by NEMA in 2016 and 2017, representative copies ofwhicliare being provided to you. As noted, attached are the detailed calculations concerning the allocation of joint costs from NEMAS)s combined educational campaigns and fundraising Mailings.
As set forth in F ASB ASC 958-720-45, subsections 45-33 thorough 37, the purpose criterion is satisfied "if the putpose of the joint activity includes accomplishing program or management and general functions." Subsection 45-35 states that to "accomplish program functions, the activity shall call for specific action by the audience that will help accomplish the [nonprofit organization's] mission. Actions that help accomplish the [nonprofit organization's] mission are actions that do either of the following: a. [b ]enefit the recipient (such as by improving the recipient's physical, mental, emotional, or spiritual health and we11-being) [;] [or] b. [b]enefit society (by addressing societal problems)." ·
FASB ASC 958-720-55, Implementation Guidance and Illustrations, sets fo1ih numerous examples in regard to when the purpose, audience and content criteria are satisfied. Subsection 55-4 states, in regard to an organization whose mission is to improve individuals' physical health, that "motivating the audience to take specific action that will improve their physical health is a call for specific l'l.ction by the audience that will help accomplish the [nonprofit organization's] mission. An example ... is sending the audience a brochure that urges them to stop smoking and suggests specific methods ... that may be used to stop smoking."
NEMA' s mailings routinely include calls to action that satisfy the purpose test set forth above. For example, in its Mailings concerning its National Heart Council ('iNHC") project, NEMA satisfies the purpose criteria with calls to action from the "Ten Steps to a Healthy Heart" brochure, included with the Mailings, to "exercise regularly" and "see your physician regu!arly.'1 In its Mailings concerning its National Strnke Council ('.'NSC") project, there is a call to "htwe your blood cholesterol level checked" and the statement that "limiting the amount of high cholesternl foods in your diet will bring your cholesterol to a more desirable level." NEMA's National Alzheimer's Council ("NAC") mailings state that "getting a diagnosis and getting it early will help the affected person and their family make plans for the future" and "that's why it is very important to see your doctor if you suspect Alzheimer's disease."

FASB ASC 958-720-45, subsection 45-48-49, states that the audience test may be satisfied if the audience is selected for any of the following reaso'ris, even if previous donors are selected: a. "the audience's need to use or reasonable potential for use of the specific action called for by the program component of the joint activity[;] [and] b. the audience's ability to take specific action to assist the [nonprofit organization] in meeting the goals of the p1'ogrnm component of the joint activity.,."
e. No. NEMA's program typically includes a fund-raising appeal.
f., g., and h. List selection of persons to whom NEMA's Mailings are sent i~ managed by its 11st broker and manager Infogroup. All lists are approved by NEMA prior to mailing. Lists are chosen to identify people likely to have the interest and ability to take independent action to further NEMA's mission of promoting health by preventing injury and illness and addressing health and social issues through education, applied research, technology and equipment. This is an overwhelmingly significant factor used in ide11tifying such persons. In cases vvhere NEMA sent Mailings to previous responders, a strategy was developed to identify and contact those who have supported NEMA in the past, either financially, by volunteering, or by taking other independent actions 6n behalf ofNEMA in furtherance of its mission and to assist NEMA in meeting program goals .. NEMA, like many organizations, uses its own mailing list but also rents and exchanges lists from other organizations whose missions are congruent with NEMA' s mission. The audience criter.ion 1s met because the audience selected is based on its ability to take action to assist NEMA in fulfilling its charitable mission. See, FASB ASC 958-720•55, subsection 55.122. Potential responders represent approximately forty percent ( 40%) and previous responders represent approximately sixty percent ( 60%) of the individuals who receive NEMA's Mailings.
FASB ASC 958-720-45 subsection 45-50 states "the content criterion is met if the joint activity ... calls for specific action by the recipient that will help accomplish the [nonprofit organization's] mission, .. If the need for and benefits of the action are not clearly evident1 information describing the action and explaining the need for and benefits of the action is provided ... " FASB ASC 958-720-55, subsection 55-17, states that "the action should benefit the recipient or society" citing subsection 958-720-45-35. Subsection 55-17 states that actions that benefit the recipient include the following: "1. Stop smoking ... 2. Do not use alcohol or drugs. 4." '""'
NEMA's mailings meet the content criteria with their calls to action that will assist NEMA in fulfilling its mission. NEMA's NHC Mailings motivate NEMA's audience to take actions related to reducing the incidence of heart-related diseases. NEMA's NAC Mailings motivate NEMA's audience to take actions to reduce the incidence of Alzheimer's disease. NEMA's NSC Mailings motivate NEMA's audience to take action related to reducing the incidence of strokes and related cardio-vascular diseases.
Question 7i: A list of the owners of names used for prospecting in 2016 and 2017 is attached.
Question 7j: Note 6 to Audited Financial Statements-Joint Cost Allocation:
The reference to "Grant Programs" in Note 6 was made to include another example ofNE.MA's charitable activities concerning awards to first responders who play a critical role in preventing heart-related deaths and deaths from other catdfo-vascular events. Such inclusion was not meant to imply that such grants are considered an activity to which joint costs apply. No solicitation activity takes place in connection with NEMA's grant program.
Question 7k: Note 6 to Audited Financial Statements - Joint Cost Allocations Based on Employee Time,

i. Kelly Herzog, President and Laura Pfister, Donor Services/ Office Manager.
ii. Included with this response is a copy of the time study used to determine the allocation percentages.
ill. NEMA has only two (2) employees who pe1fo1·m all duties related to programs, management, general, etc. Their expenditure of time concerning programs, management; general etc. are set forth on time sheets to calculate the amow1t of time they expend in connection ,vith each of these categories. The time study is performed during a one month period, one time per year. From this calculation; a daily average is computed and the percentages of employee time devoted to the above categories for each year is detennined.
iv. See, responses set forth above and documents included with this request. To summarize, joint cost allocations are calculated based on the nature of the expense, i.e., whether it is one hup.dred percent (l 00%) program, fundraising, etc., or whether the expense must be allocated among these various categories based on the joint cost percentages discussed above.
v. The joint cost allocation spreadsheet included with this response sets fo1ih all expense hems and demonstrates where joint allocation of costs, based on employee time expended, was applied in regard to program, management arid fundraising expenses.
Please let us know if you have any fi.irther questions regarding the above responses.
Enclosures

-·--~··
\
C 1) (' Ir?'.°: .1\·_ '( (', c• ,1 -·· J .___,_::, ,.,v l -.J..•
6. List all current officers and directors unless they are Included on your IRS return, Marl< the box to indicate whether the person is an officer, director, or both. Provide.an additional sheet if necessary.
Name . -~ -· Officer Directp( Name . -
7. Is there any officer or director who cannot be reached at the organizatJon's mailing address?, If "yes," provide the names and addresses on an additional sheet.
Officer
8. Since your last registration form, has the organization or any of its officers, directors, employees or fundraisers:
A Been enjoined or otherwise prohibited by a government agency/court from soliciting?
B. Had its solicitation registration or license denied or revoked by any jurisdlctlon?
C. Been the sut5jectof a proceeding rega(d\hg ahy license~· registration, or solicitation?
D, Entered into a voluntary agreement of compliance with a government agency or in a case before a court or administrative agency? . . . . . . . . , . , . . . .
if any "yes" box is checked, provide a complete exPlanation on a separate sheet.
Director
Yes No
• •
Yes No
• • • • • • • •
Yes No
Qt • Has the organization engaged a professional fundraiser or fundraising consultant for Michigan fund raising activity for either the financial accounting period reported in item 10 or the current period? If no, go to question10,
Under Michigan law, fundraising consultants are considered professional fundralsers (PFRs). See instructions for definition. ·
If yes, in the chart below list all PFRs that your organization has engaged for Michigan fundralslng activity. Provide additional sheets if necessary. Provide copies of contracts for each PFR listed If not already provided.
Contract types: A - ConsuWng - See instructions for definition B - Solicitation / Event
~0.11, Pine,Rit\ij1:- ~d '.:).Ic,1\<"., 2,0\ '
l'-h, ;::,k.:."> r;:: L. 3q l I c
End date: y [S;I/
n D
AW B D
A [SJ!
B D
,_ .. \ \
y • n D
End date: A D
B D

l:i l2
l9
l1
0
L1
1
l12
l.1
3
L14
l15
L
16
L
17 L
18
L
19
L
20
TO
TA
LS
QU
AN
TIT
Y
0
11311 7,732 24,120 12,641 11,714 18,301 21,657 24,309
0 20,411 18,973 21,640
0
18
2,8
09
BR
DIR
EC
T
PO
ST
AG
E
$0.00 -
1191.41 $1,059.28 $3,304.44 $1,731.82 $1,604.82 $2,507.24 $2,967.01 $3,330.33
$0.00 $2,796.31 $2,599.30 $2,964.68
$0.00
$2
5,0
56
.64
PR
OD
UC
TIO
N
$0.00 $
42
2.1
4
$3,780.95 $7,573.68 $3,965.48 $3,678.fa $5,746.52 $6,800.30 $7,633.02
$0.00 $6,409.06 $5,957.52 $6,794.96
$0.00
$5
8,7
61
.82
De
ce
mb
er, 2
01
6
WIT
CO
C
AG
ING
$0.00 _ $0.00
$502.59 $1,567.80
$821.66 $761.41
$1,189.55 $1,407.70 $1,580.09
$0.00 $1,326.72 $1,233.24 $1,406.60
$0.00
$1
1,7
97
.36
DM
I D
AT
A
$0.00 }39.33
$208.76 $651.24 $345.10 $316.28 $494.13 $584.74 $656.34
$0.00 $551.10 $512.27 $584.28
$0.00
$4
,94
3.5
7
$38.66 I
~'
·/
' /
\ '
NC
C
\
I DE
SIGN
\
I $0.00 l
/ $124.54
$120.60 $63.21 $58.57
TO
TA
l $0.00 $777.42
$5,590.24 $13,217.76
$6,927.27 $6,419.27
$91.51 \
$10,028.95 $108.29
-$11,868.04 $121.55
$13,321.33 $0.00
$0.00 $102.04
$11,185.23 $94.87
I $10,397.20
$108.20 /
$11,858.72 $0.00
$0.00
\ . $
1,0
32
.04
/
$1
01
,59
1.4
3
't-"" J 1\ /
\ \I I-"'
R
• ·
/'~
\'
I ~
' !__.,.1.H1 llb'rlJ~
\ ':'(} u
)lt~
r~-1'
Qu e-s-h or-i
3h
-·
,...,. .
Sx.,,, ,~tfvP t-P
u..,,
\ ~

Ac
co
un
t 1D A
cc
ou
nt D
escrietion
D
ate 6
30
00
Legal F
ees -D
aily 1•2116/16
63
00
0
Le
ga
l Fees -
Daily
1·3114/16 6
30
00
Legal F
ee
s -D
aily 1• 3/24/16
63
00
0
Le
ga
l Fees -
Daily
1 ~/11/16
63
00
0
Legal Fe
es -
Daily
1· 5/10/16 6
30
00
L
eg
al F
ee
s • Daily
1·5/10/16 6
30
00
Legal F
ee
s -D
aily 1•6/13/16
63
00
0
Legal Fe
es -
Daily
1•6/13116 6
30
00
Legal F
ees -D
aily 1•6/13/16
63
00
0
Legal Fees -
Daily
1•7111[16 6
30
00
Legal F
ee
s-
Daily
1• 8/15116 6
30
00
Legal F
ees -D
aily i· 8115/16
63
00
0
Le
ga
l Fe-es -
Daily
1·9115/"16
63
00
0
Legal Fe
es -
DalJy
1·9115/16 6
30
00
Legal F
ee
s• D
aily 1• 9/15/16
63
00
0
Legal Fe
es-
Daily
1• 10111/16 6
30
00
Legal F
ee
s -D
aily 1• 11/10/16
63
00
0
Legal Fe
es -
Dally
1'1
1/1
0/1
6
63
00
0
Le2a1 Fees -
Dail)'.
1• 11110/16 6
30
~
Legal Fees -
Other
• 2/18[16 6
30
04
Legal F
ee
s-
Other
'21
18
/16
6
30
04
L!:l!al F
ee
s -O
ther -511or1s
63
00
6
Legal Fe
es-
Service
9/16/16
03/09118( O
PM
Na
tion
al E
me
rge
ncy M
ed
icin
e A
sso
c.
Gen
eral Led
ger
Fo
r the
Pe
riod
Fro
m Ja
n 1
, 2016 to D
ec 31, 2016
Tran
s Descri:etio
n
Am
ou
nt
Copilevilz &
Canter, L
LC
(DC
) -W
INC
OR
ES
TA
TE
$
23
7.5
0
Copllevitz &
Canter. LLC
(DC
) -M
cCA
LL ES
TA
TE
$1,235.00 C
opilevitz & C
anter, LLC
(DC
) -R
egistered Ag
en
l Fee for 2 yrs 2
01
6 &
20· $
50
0,0
0
Copilevitz &
Canter, L
LC
(DC
)-D
on
oh
oe
/Win
corW
ill $
1,9
00
.00
C
opilevltz & C
anter, LL
C
(DC
) -N
EM
A F
IS Legal opinion
$5
00
,00
C
opilevitz & C
anter, LL
C (D
C) -
McC
all Estate
$1
50
.00
C
opilevitz & C
anter, LL
C (D
C)-
NH
C R
EG
MA
RK
RE
NE
WA
L
$1
,18
7.5
0
Capilevilz &
Canter, L
LC
{DC
)-W!N
CO
R E
ST
AT
E
$2
,13
7.5
0
Capilevitz &
Canter, LLC
(DC
}-M
CA
LL ES
TA
TE
$
75
.00
C
opilevitz & C
anter, LLC
{DC
)-M
cCA
l!.L ES
TA
TE
$
78
.60
C
apilevitz & C
anter, LLC
(DC
)-M
cCaa E
state
$
17
5.0
0
Copilevilz &
Canter, LLC
(D
C)-
oth
er co
nce
rns
$1
42
.50
C
opilevttz & C
anter. LL
C (D
C)-
NH
C R
eview R
eg
Mar!<
$3
56
25
C
opilevitz & C
anter, LLC (D
C)-T
romblay E
state
$
83
1.2
5
Copilevilz &
Canter, LLC
(DC
)-W
inco
ur E
state $
23
7.5
0
Copilevitz &
Canter. LLC
{D
C)-
NH
C R
EN
EW
RE
GIS
TE
RE
D M
AR
K
S1,781.25
Copilevitz &
Canter. LLC
(D
C)-
CO
UR
IER
CH
AR
GE
S
S5
6.9
9
Copllevitz &
Canter, LLC
(D
C)-
NH
C R
EG
IST
ER
ED
CO
MP
LIAN
CE
$
23
7.5
0
Coellevitz &
Canter, LLC
(D
C)-T
RO
MB
LA
Y E
ST
AT
E
$1
,18
7.5
0
S13,006.84
Cow
ard, Hicks &
Siler, P
A -
McC
all Esta
te
$5
6.6
7
Cow
ard, Hlci<
s&S
iler, P
A-V
OID
ED
(S
00.67) A
lliance Land Surve)'.!ng, P
.C. -
2 Charities failure to
ea
l balance of $
93
4 d
$2
33
.50
$
23
3.5
0
Dir. O
flhe
US
Pa
ten
t $
50
0.0
0
$5
00
.00
$
13
,74
0.3
4
$1
3,7
40
.00
{10.3<
,)
$1
,30
0.6
8
$4
6.7
0
$5
00
.00
$
1,8
47
.38
$
1,8
47
.00
{S
0.33)
QveSkoJ') 4 b
10
% B
equest to National S
troke Council
20
%
10
0%
Nationel H
eart Council rel)_islered m
ark renew
al
Pag
e: 1

Acco
un
t ID
Acco
un
t De
scrip
tion
D
ate 6
24
10
C
on
sult-
Prin
t Me
dia
1
1/4
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
1/4
/16
6
24
10
C
on
sult-
Prin
t Me
dia
1
1/4
/16
6
24
10
C
on
sult-
Prin
t Me
dia
1
1/4
/16
6
24
10
C
on
sult-
Prin
t Me
dia
1
2/1
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
2/1
/16
6
24
10
C
on
sult-
Prin
t Me
dia
1
2/1
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
3/1
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
3/1
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
3/1
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
3/2
2/1
6
62
41
0
Co
nsu
lt -P
rint M
ed
ia
13
/22
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
3/2
2/1
6
62
41
0
Co
nsu
lt -P
rint M
ed
ia
13
/22
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
5/2
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
5/2
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
5/2
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
6/2
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
6/2
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
6/2
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
7/1
/16
6
24
10
C
on
sult-
Prin
t Me
dia
1
7/1
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
7/1
/16
6
24
10
C
on
sult-
Prin
t Me
dia
1
7/1
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
8/1
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
8/1
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
8/1
/16
6
24
10
C
on
sult-
Prin
t Me
dia
1
9/1
/16
6
24
10
C
on
sult-
Prin
t Me
dia
1
9/1
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
9/1
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
10
/3/1
6
62
41
0
Co
nsu
lt-P
rint M
ed
ia
1 "i0/3/16 6
24
10
C
on
sult -
Prin
t Me
dia
1
10
/3/1
6
62
41
0
Co
nsu
lt-P
rint M
ed
ia
11
0/3
/16
624:10
Co
nsu
lt-P
rint M
ed
ia
11
1/1
/16
6
24
10
C
on
sult -
Prin
t Me
dia
1
11
/1/1
6
62
41
0
Co
nsu
lt-P
rint M
ed
ia
11
1/1
/16
6
24
10
C
on
sult-
Prin
t Me
dia
1 12/1116
62
41
0
Co
nsu
lt-P
rint M
ed
ia
11
2/1
/16
6
24
10
C
on
sult-
Prin
t Me
dia
1
12
/1/1
6
62
41
0
Co
nsu
lt-P
rint M
ed
ia
11
2/2
8/1
6
62
41
0
Co
nsu
lt -P
rint M
ed
ia
112/28116
03
/20
/18
at 2
:05
PM
Na
tion
al E
me
rge
ncy M
ed
icine
Asso
c. G
eneral Le
dg
er
Fo
r the
Pe
riod
Fro
m Ja
n 1, 2016 to D
ec 31, 2016
Tran
s Descrip
tion
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
l-15
TR
AD
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-L-15 N
HC
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-L-15 N
AC
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-L-15 K
DM
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-A
-16
KD
M D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -A
-16
NH
C D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -A
-16
NA
C D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
B-1
6 N
HC
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-B
-16 NA
C D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
B-1
6 K
DM
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-C
-16 NH
C D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
C-16 N
AC
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-C
-16 KD
M D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
C-16 T
RA
D D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
0-1
6 N
HC
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-D
-16 NA
G D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
D-1
6 K
DM
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-E
-16
NH
C D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
E-1
6 N
AG
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-E
-16 KD
M D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
F-16 T
RA
D D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
F-16 N
HC
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-F
-16 NA
C D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
F-16 K
DM
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-G
-16
NH
C D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
G-1
6 N
AG
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-G
-16 KD
M D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
H-16 N
HC
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-H
-16 NA
C D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
H-16 K
DM
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-1-16 T
RA
D D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -1
-16
NH
C D
ES
IGN
N
ew
po
rt Creative C
om
mu
nica
tion
-1-16 N
AC
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-1-1
6 K
DM
DE
SIG
N
Ne
wp
ort C
reative Co
mm
un
icatio
n -
J-16 NH
C D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
J-16 NA
G D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
J-16 KD
M D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
K-16 N
HC
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-K
-16
NA
G D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
K-16 K
DM
DE
SIG
N
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-L-16 T
RA
D D
ES
IGN
N
ew
po
rt Cre
ative
Co
mm
un
icatio
n -
L-1
6 N
HC
DE
SIG
N
Qucshrn Lfc_
Am
ou
nt
$1
06
.59
$
17
5.8
5
$2
27
.05
$
24
2.1
5
$3
60
.85
$
17
9.1
3
$2
29
.34
$
16
9.0
0
$224.81' $334.23 $199.11 $
27
8.7
2
$3
19
-24
$106.31 $
18
7.4
6
$2
43
.76
$
29
7.1
4
$1
92
.63
$
23
9.3
6
$3
02
.75
$
10
5.4
5
$1
98
.95
$
27
1.3
7
$3
05
.66
$
27
5.4
5
$2
92
.73
$33b.11 $267.41 $347.15 $312.99 $
12
5.4
9
$312.04 $
35
1.9
6
$292.11 $
27
1.4
6
$3
26
.13
.$
32
3 .. 0
8
$2
76
:35
$
33
4.4
5
$3
56
.87
$
12
4.5
4
$2
81
.04
Pa
ge
:1

Na
tion
al E
me
rge
ncy M
ed
icine
Asso
c. G
en
era
l Le
dg
er
Fo
r the
Pe
riod
Fro
m Ja
n 1, 2
01
6 to D
ec 3
1, 2
01
6
Acco
un
t ID
Acco
un
t De
scriptio
n
Da
te
Tra
ns D
escrie
tion
A
mo
un
t 6
24
10
C
on
sult -
Prin
t Me
dia
i 12/28/16
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-L
-16 NA
C D
ES
IGN
$
32
i.35
6
24
10
C
on
sult -
Prin
t Media
11
2/2
8/1
6
Ne
wp
ort C
rea
tive C
om
mu
nica
tion
-L
-16 KD
M D
ES
IGN
$305.11
62
41
0
Co
nsu
lt -P
rint M
edia 1
12
/31
/16
to reverse p
rior yr a
dju
stmn
t {f:5175.85)
62
41
0
Co
nsu
lt -P
rint M
ed
ia
11
2/3
1/1
6
to re
verse
prio
r yr ad
justm
nt
($2
27
.05
) 6
24
10
C
on
sult -
Prin
t Me
dia
1
12
/31
/16
to reverse p
rior yr a
diu
stmn
t {$142.~IS}
$10,679-68 7
5%
$8,009.76
67
10
8
Ship/P
ostage -A
dm
inistr
1/29/16 R
ecla
ss Postage to M
aterials ($'!8'.23)
67
10
8
Sh
ip/P
osta
ge
-A
dm
inistr
1/29/16 S
hip
/po
stag
e -
Adm
in $
79
.24
6
71
08
S
hip
/Po
stag
e -
Ad
min
istr 2/29/16
Re
class P
osta
ge
t6 M
ate
rials
($4
6.8
7)
67
10
8
Sh
ip!P
osta
ge
-Ad
min
istr 2/29/16
Sh
ip/p
osta
ge
-Ad
min
$
50
.00
6
71
08
S
hip
/Po
stag
e -
Ad
min
istr 3/31/16
Sh
ip/p
osta
ge
-Ad
min
$
15
0.0
0
67
10
6
Sh
ip/P
osta
ge
-Ad
min
istr 3/31/16
Re
class P
osta
ge
to M
ate
rials
{$1
0.5
0)
67
10
8
Sh
ip/P
osta
ge
-A
dm
inistr
4/29/16 R
ecla
ss Po
stag
e to
Ma
teria
ls ($42.24)
67
10
8
Sh
ip/P
osta
ge
-A
dm
inistr
4/29/16 S
hip
/po
stag
e -
Ad
m in
$5
0.0
0
67
10
8
Sh
ip/P
osta
ge
-Ad
min
istr 5/31/16
Re
class P
osta
ge
to Ma
teria
ls ($43.69)
67
10
8
Sh
ip/P
osta
ge
-A
dm
inistr
5/31/16 S
hip
lpo
stag
e -
Ad
min
$
25
0.0
0
67
10
8
Sh
ip!P
osta
ge
-A
dm
inistr
6/10116 P
etty C
ash -S
hip
/Po
stag
e -
Ad
min
istr 1
6
$6.00 6
71
08
S
hip
/Po
stag
e -A
dm
inistr
6/30116 R
ecla
ss Po
stag
e to
Ma
teria
ls {$24.51)
67
10
8
Sh
ip/P
osta
ge
-Ad
min
istr 7/29/16
Re
class P
osta
ge
to M
ate
rials
($21A3)
67
10
8
Sh
ip/P
osta
ge
-Ad
min
istr 7/29/16
Sh
ip/p
osta
ge
-Ad
min
$
10
0.0
0
67
10
8
Sh
ip/P
osta
ge
-Ad
min
istr 8/31116
Re
class P
osta
ge
to Ma
teria
ls ($26.03)
67
10
8
Sh
ip! P
ostage -A
dm
inistr
9/30/16 S
hip
/po
stag
e -A
dm
in
$5
0.0
0
67
10
8
Sh
ip/P
osta
ge
-A
dm
inistr
9/30116 R
ecla
ss Po
stag
e to
Ma
teria
ls ($"14.96)
67
10
8
Sh
ip/P
osta
ge
-Ad
min
istr 10/31/16
Re
class P
osta
ge
to M
ate
rials
($21.52) 6
71
08
S
hip/Postage -A
clmin
istr 10/31116
Ship/postage -A
dm
in
$5
0.0
0
67
10
8
Sh
ip/P
osta
ge
-Ad
min
istr 11/30/16
Re
class P
ostage to M
ate
rials
($18~59) 6
71
08
S
hip
/Po
stag
e -A
dm
inistr
11/30/16 S
hip
/po
stag
e -
Adm
in $
90
.00
6
71
08
S
hip
/Po
stag
e -
Ad
min
istr 12/20/16
Pe
tty Cash -
Postage
$5
0.6
5
67
10
8
Sh ip
f Postage -
Ad
min
istr 12130/ 16
R
ecla
ss Postage to
Ma
teria
ls ($"14.96)
67
10
8
Sh
ip/P
osta
ge
-Ad
min
istr 12130/16
Sh
ip/p
osta
ge
-A
dm
ln
$90.00 $711.36
10
0%
$711.36
69
80
0
Registration -
States
1! 1/13/16 W
Y S
ecretary of S
tate -R
eg
istratio
n -
States
16
$
27
.00
6
98
00
R
egistration -S
tate
s 1!3/23116
SO
Secretary o
f Sta
te -
Registration -
Sta
tes
16
$
10
.00
6
98
00
R
egistration -S
tate
s 1!3/23/16
NV
Secretary o
f Sta
te -
Re
gistra
tion
-S
tate
s 1
6
$400.00 6
98
00
R
egistration -S
tate
s 1!3/23/16
NV
Legal Pre
ss -R
egistration -S
tate
s 1
6
$4
0.0
0
69
80
0
Registration -
Sta
tes
1!3/24/16 W
V S
ecretary of S
tate
$
75
.00
6
98
00
R
egistration -S
tate
s 1!3/24/16
DC
Tre
asu
rer -
Registration -
Sta
tes
16
$B
O.D
O
69
80
0
Registration -
Sta
tes
1!3/24/16 U
T S
tate
-R
egistration -S
tate
s 1
6
$1
0.0
0
69
80
0
Registration -
Sta
tes
113/24/16 C
O S
ecretary of S
tate
-R
egistration -S
tate
s 1
6
$1
0.0
0
69
80
0
Registration -
Sta
tes
1!3/24/16 O
R S
ecre
tary o
f Sta
te -
Registration -
Sta
tes
16
$
50
.00
6
98
00
R
egistration -S
tate
s 114/6/16
DC
Tre
asu
rer -
Registration -
Sta
tes
16
$40.00
69
80
0
Registration -
Sta
tes
114/6/16 C
A A
ttorney General -
Registration -
Sta
tes
16
$150.00
69
80
0
Registration -
States
1{ 416/16 M
T S
ecretary of S
tate
-R
eg
istratio
n -
Sta
tes
16
$2Q
_QQ
6
98
00
R
egistration -S
tate
s 1 ( 5/1/16
ND
Se
creta
ry of S
tate
-R
eg
istratio
n -
States
16
$
15
.00
03/20118 at 2
:05
PM
P
ag
e:2

---
-
... ~
Na
tion
al E
me
rge
ncy M
ed
icine
Asso
c. G
en
era
l Le
dg
er
. F
or th
e Period fro
m Jan
1, 2016 to Dec 31, 2016
Ac
co
un
t ID
Ac
co
un
t De
sc
riptio
n
Da
te
Tra
ns
De
sc
riptio
n
Am
ou
nt
69
80
0
Registration -
Sta
tes
115/2/16 A
l Office
of th
e A
ttorn
ey G
en
e -
Registration -
Sta
tes
16
$25_00
69
80
0
Registration -
States
115/2116 C
A F
ranchise Ta
x Bo
ard
-R
egistration -sta
tes
16
$10.00
69
80
0
Registration -
States
115/10/16 F
L Dept. o
f Ag
ricultu
re &
Cnsm
-R
egistration -S
tate
s 1
6
$300.00 69800
Registration -
States
115/10/16 M
A S
ec. of th
e C
rnmnw
lth -R
egistration -S
tates 1
6
$250.00 69800
Registration -
States
115/10/16 P
A C
om
mo
nw
ea
lth o
f Pennsylvani -
Registration -
States
16
$250.00
69800 R
egistration -S
tate
s 115/11/16
NH
State o
f New
Ham
pshire -R
egistration -S
tates 1
6
$75.00 69800
Registration -
States
115/12/16 N
YS
Office
of the 1;-ttom
ey Gen -
Registration -
States
16
$25.00
69
80
0
Registration-: S
tate
s 1
[5/1
2/1
6
NC
State -
Registration -
States
16 $200_00
69
80
0
Registration -
States
1[5
/12
/16
O
R D
ep
t Of Ju
stice -
Registration -
States
16
$25-00
69
80
0
Registration -
States
115/12/16 V
A T
rea
sure
r of V
irgin
ia -
Registration -
States
16
$325.00
69
80
0
Registration -
States
115/12/16 C
T D
ep
t of C
on
sum
er P
rotectio -R
egistration -S
tates 1
6
$50.00 6
98
00
R
egistration -S
tates 1
(5/1
2/1
6
OH
State T
rea
sure
r-R
egistration -S
tate
s 1
6
$200.00 69800
Registration -
States
1!5
/12
/16
S
C S
ecre
tary o
f Sta
te -
Registration -
States
16
. $51-85
69800 R
egistration -S
tates 115/23/16
IL C
harity Bureau F
und -2
01
6 R
EG
RE
NE
WA
L
$15.00 6
98
00
R
egistration -S
tates 116/13/16
MD
Secretary o
f Sta
te -
Registration -
States
16
$300_00
69800 R
egistration -S
tates 116/13/16
NJ D
iv. of C
on
sum
er A
ffairs -
Registration -
States
16 $250_00
69800 R
egistration -S
tates 116/14/16
CA
Se
creta
ry of S
tate
-R
egistration -S
tate
s 1
6
$25.00 6
98
00
R
egistration -S
tates 1
(6/1
4/1
6
KS
Secretary o
f Sta
te -
Registration -
States
16
$40.00
69
80
0
Registration -
States
1(6
/14
/16
M
E S
ecre
tary o
f Sta
te -
Registration -
States
16
$60_00
69
80
0
Registration -
Sta
tes
1{6
/28
/16
M
N A
ttorney General's O
ffice -
Registration -
States
16
-
$25_00 69800
Registration -
Sta
tes
116/28/16 T
N S
ecretary of S
tate
-R
egistration -S
tates 1
6
$240.00 69800
Registration -
States
116/28/16 W
I State -
Registration -
States
16
$54.00
69800 R
egistration -S
tates 117/25/16
National R
egistered Agents, In -
RE
GIS
TE
RE
D A
GE
NT
ST
AT
E F
EE
~ $1,798.00
69
80
0
Registration -
States
119/22/16 M
S S
ecre
tary o
f Sta
te -
Registration -
States
16
$53.14
69800 R
egistration -S
tate
s 1
(9/2
2/1
6
LA S
ecretary of S
tate
-R
egistration -S
tate
s 16
$35.00 69800
Registration -
States
1111/15/16 H
I Departm
ent of Co
mm
erce
an
d -
Registration -
States
16 $3_50
69800 R
egistration -S
tates 1111/15/16
RI S
tate -R
egistration -S
tates 1
6
$93.98 69800
Registration -
States
1111/17/16 M
l State o
f Michigan -
Registration -
States
16
$20.00
69
80
0
Registration -
States
1111/17/16 O
K S
ecretary of S
tate
-R
egistration -S
tates 1
6
$65.00 69800
Registration -
States
1111/17/16 W
A S
tate -R
egistration -S
tates 1
6
$40.00 6
98
00
R
egisir§tion -S
tates 1112130/16
Registration E
xpe
nse
_
_ _ _
_ $1,421.00
$7,252.47 8
0%
$5,801.98
$18,643-5"1 $18,643.51
$14,523.10 11g
03
/20
/18
at 2
:05
PM
P
ag
e:3

NATIONAL EMEHGENCY MEDICINE ASSOCIATION 52•'1257429
Schedule G(forrn 990 or Form 990-EZ), Supplemental lnfomiation Regarding Fundralsing or Gaming Activities Part I, Line 3 List of States Registered or Licensed to Solicit Funds
Hawai:i. Illinois Indiana Kansas Kentuoky Maine Maryland Massachusetts Michigan Minnesota Mississippi New Hampshi~e _________ _ New Jersey New York North Carolina North Dakota Pennsylvania Rhode Island South Carolina Tennessee Ul:ah .................................... ·· ·v1..rgrn1·a·· ...................... . West Virginia
Schedule O (Form 990 or 990-EZ), Supplemental Information to Form 990 or 990-EZ Form 990, Page 1 o, Line 24e All Other Expenses (continued)
-.:.....-~
Description
Sweepstakes Prizes Postage & Shipping Printing & Publications INTERNET EDOCATION Land Deals
(A) Total
4,037. 399,018. 597,948.
12. 595,
(13) (C) Program Management services and general
o. 2,837. 298,754. o. 448,461. o.
12. o. 298. 297.
Q. 0 e.s+1 uY1
(D) Fundraislng
1,200. 100,264, 1491 487.
o. o.
Lf d
2

/--\ W-e,,
7-------r r-
I \) L' :i c.J-1 iJI>
.,
C1......' -r ,:_ N
AT
ION
AL
EM
ER
GE
NC
Y M
ED
IC1N
E A
SS
OC
IAT
ION
~
L,._,,--~ ' •
J \
' '
AL
LO
CA
TIO
N O
F F
UN
CT
ION
AL
EX
PE
NS
ES
BY
AC
CO
UN
T
CA
TA
GO
RY
D
AT
A P
RO
CE
SS
ING
(10) N
UM
BE
R
TO
TA
L
%
PR
OG
RA
M
¾
DE
VE
LO
PM
EN
T
%
MG
T.G
EN
. ¾
D
IFF
D
IFF
%
DA
TA
MA
IL-P
RIN
T M
ED
IA
10
5
4,6
12
.09
1
00
.00
%
.21
,92
4.6
4
40
.00
%
10
,96
2.4
2
20
.00
%
21
,92
4.8
4
40
.00
%
0.00 0
.00
%
DA
TA
MA
IL-U
ST
RE
NT
AL
10
1,394.61
10
0.0
0%
2
78
.92
2
0.0
0%
6
97
.31
50.00%
4
18
.38
3
0.0
0%
0
.00
0
.00
%
DA
TA
-PR
EM
IUM
1
0
0.0
0
10
0.0
0%
0
,00
6
0.0
0%
o.oa
40.0Q~/Q
, 0
,00
0
.00
%
0.0
0
0.0
0%
D
AT
A P
RO
C. 1
st AID
K!T
1
0
0.0
0
100.-00%
0.00 100.00"/4
0.0
0
0.0
0%
0
.00
0
.00
%
00
0
0.0
0%
D
AT
A P
RO
C. H
RT
/ST
K LIM
ES
10
0.00 10(l.00%
0,00
100_,:)0%
0.0
0
0.0
0%
0
.00
0
.00
%
0.0
0
0.00%.
DA
TA
PRO
C.11'1 H
OU
SE
10
0.0
0
10
0.0
0%
0
.00
1
00
.00
%
0.0
0
0.00%
0,0
0
0.0
0%
0.00
C,00%
:O
TA
L{-H
}) 5
o .. W
'3.7
0
·[ll[L00%
7
?_20:: . .7-11 39.50'%
·J·l/35:':;.72
20
]~%
2:2,3!/.:;L11
.:::-l•.ro'k G
.OU
(J,OU
~/.,
LIS
TC
OS
T (11)
NU
MB
ER
T
OT
AL
%
P
RO
GR
AM
%
D
EV
EL
OP
ME
NT
%
M
GT
. GE
N.
%
DIF
F
DlF
F¾
M
AIL
l.lST
RE
.NT
AL-H
OU
SE
'\1
24
,66
3.0
8
10
0.0
0%
9,865.23
40
.00
%
14
,79
7.8
5
60
.00
%
0,0
0
0.0
0%
0
.00
0.00%
M
AIL
US
T R
EN
TA
L-
Ol'liE
R
'!1 0
.00
100..po%
0.00
40
.00
%
0.0
0
60
,00
%
0.0
0
0.0
0%
0
.00
0
.00
%
MA
IL U
ST
-P
RE
MIU
M
11 0
.00
1
00
.00
%
0.00 6
0.0
0%
0.00
40,00%
0.0
0
0.00%
0.0
0
0.00%
TO
TA
L{'!i]
2.41 663.,D
S
·((!0.00%
S,S
65.13 .:10.00¾
·rJ..)"97.S
5 fi{lJ}(}<
lf.J U
.Of.l
0.00%.
t1.0G
OJJ0'1/,,
MA
ILIN
G S
ER
VIC
ES
(12)
NU
MB
ER
T
OT
AL
%
P
RO
GR
AM
%
D
EV
EL
OP
ME
NT
%
M
GT
.GE
N..
%
DlF
F
DiF
F%
C
AG
ING
/CA
SH
ING
1
2
10
4,1
19
.40
1
00
.00
%
41,647.76 4
0.0
0%
41,647.76
40
.00
%
20,823.88 2
0.0
0%
0
.00
0
.00
%
SH
IPP
ING
/STO
RA
GE
1
2
0.0
0
10
0.0
0%
0
.00
80_00%
0
.00
2
0.0
0%
0
.00
0
.00
%
0.0
0
0;00%
MA
JL HO
US
E F
EE
S P
RlN
T M
ED
IA
12
0
.00
100.00%
0
.00
70.00%
0
.00
3
0.0
0%
0
.00
0.00%
0
.00
0.00%
M
AIL H
OU
SE
FE
ES
PR
EM
IUM
1
2
0.0
0
·wo.00%
0
,00
60~
00%
0.0
0
40
.00
%
o.oo 0
.00
%
0.0
0
0.00%
MA
IL H
OU
SE
FE
ES
HR
T/S
TK
FF
1
2
0.00 100.00%
0
.00
1
00
.00
%
a.co 0.00%
0.00
0.0
0%
0
.00
0
.00
%
MA
IL HO
US
E F
EE
S N
WS
LT
R.
\2
0.0
0
10
0.0
0%
0
.00
100.00"/o
0.0
0
0.0
0%
0
.00
0
.00
%
0.0
0
0.00%
row,:.. {iZ
i 1
04
/iiS.4
(! ic,C
.00%
-t•ilt54.7.7S 40.00°/1)
<~i;G47.7r5
i!Q.00%
2G
J~13 . .BD 20.iJO~,;_.
D.G
O
O.{l0%
,
OF
FIC
E E
XP
EN
SE
(13) N
UM
BE
R
TO
TA
L
%
PR
OG
RA
M
%
DE
VE
LO
PM
EN
T
%
MG
T.G
EN
. %
D
IFF
D
IFF
%
AD
VE
RT
ISIN
G
13
Q
,00 1
00
.00
%
0.00 0
.00
%
0.0
0
0,00%
0,0
0
10
0.0
0%
0
,00
0.00'%
B
AN
K C
HA
RG
ES
1
3
21,209.31 1
00
.00
%
o.oo 0
.00
%
0.0
0
0,0
0%
21,209.31
10
0.0
0%
0
.00
0
.00
%
BA
NK
FE
ES
(ME
RC
HA
NT
) 1
3
45
6.1
9
10
0.0
0%
0
.00
0.00"/4
0.0
0
0.0
0%
4
56
.19
1
00
.00
%
0.0
0
0.0
0%
D
ON
ATlO
N
13
149.54
10
0.0
0%
74.77
50
.00
%
0.0
0
0.0
0%
7
4.7
7
50.00%
0.0
0
0.00%
DU
ES
ISU
BS
CR
IP.
13
2
,87
4.9
6
10
0.0
0%
0
.00
0
.00
%
0.0
0
0.0
0%
2
,87
4.9
6
10
0.0
0%
0
.00
0
.00
%
lNS
VR
AN
CE
1
3
2,6
07
29
1
00
.00
%
2,0
65
.83
8
0.0
0%
2
60
.73
1
0.0
0%
2
60
.73
1
0.0
0%
0
.00
0.00°/c-
LIBR
AR
Y I S
OF
TW
AR
E
13 2
.40
9.2
2
10
0.0
0%
1,204.61
50.00%
0.0
0
0.00'%
1,204.61 5
0.0
0%
0
.00
0.00%
M
ISC
ELLA
NE
OU
S
13
0
.00
1
00
.00
%
0.DO
-80.00%
0.0D
1
0.0
0%
0.0D
1
0.0
0%
0
.00
0
.00
%
MO
VIN
G/O
FFICE
1
3
0.0
0
10
0.0
0%
.0
.00
5
0.0
0%
0
.00
1
0.0
0%
o.oo
40
.00
%
0.0
0
0.00°/i; O
FF
ICE
SU
PP
LIES
1
3
4,4
76
.15
1
00
.00
%
2.238.08 5
0.0
0%
~
47
.82
1
0.0
0%
1
,79
0.4
6
40
.00
%
0.0
0
0.0
0%
P
AR
KIN
GIT
OllS
/GA
S
13
768.01
10
0.0
0%
614.41
80.00%
76
.50
10.00%
7
6.8
0
10
.00
%
0.0
0
0,0
0%
E
DU
CA
110N!TU
ITION
1
3
0.0
0
10
0.0
0%
0
.00
5
0.0
0%
0
.00
0
.00
%
0.0
0
50
.00
%
0.00 0
.00
%
BR
EA
KR
M/S
UP
PLIE
S E
XP
EN
SE
1
3
59
0.3
0
10
0.0
0%
295.15
50
.00
%
59
.03
1
0.0
0%
2
36
.12
4
0.0
0%
0
.00
0
.00
%
?H
ON
E/ IN
TE
RN
ET
1
3
1,6
75
.34
1
00
.00
%
83
7.6
7
50
.00
%
16
7.5
3
10
.00
%
67
0.1
4
40.QQ
C/t>
0.0
0
0.00°/n-R
EN
TA
L-E
XP
EN
SE
S
13
1
1,0
33
.28
·100.00%
5
,6H
l.97
6
0.0
0%
2
,20
6.6
5
20
.00
%
2,2
06
.66
2
0.0
0%
0
.00
0.00~·0
RE
NT
AL
-PO
BO
X
13 Q
.00 1
00
.00
%
0.00 5
0.0
0%
0
.00
10.00%
0
.00
4
0.0
0%
Q
.00 0
.00
%
EQ
UIP
ME
NT
-O
FF
lCE
1
3
0.0
0
10
0.0
0%
0
,00
5
0.0
0%
0
.00
1
0.0
0%
0
.00
4
0.0
0%
0
.00
0
.00
%
EQ
UIP
ME
NT
-S
ER
VIC
E
13
0
.00
1
00
.00
%
0.0
0
50
.00
%
0.0
0
10
.00
%
0,0
0
40
.00
%
0.0
0
0.0
0%
R
EP
AJR
S &
MA
INT
. 1
3
79
.99
1
00
.00
%
63
.99
8
0.0
0%
8
.00
.1
0.0
0%
8
,00
1
0.0
0%
0.00
0.0
0%
S
EM
INA
RS
1
3
0.00 1
00
.00
%
0.0
0
0.0
0%
0
.00
0
.00
%
0.0
0
10
0.0
0%
0
.00
0
.00
%
TR
AV
EL
1
3
0.0
0
10
0.0
0%
0
,00
8
0.0
0%
0
.00
1
0.0
0%
0
.00
1
0.0
0%
0
.00
0
.00
%
ME
ET
ING
S
13
2
,75
9.9
6
100_00%
2,2
07
.97
6
0.0
0%
276_00
10
,00
%
27
6.0
0
10
.00
%
0.0
0
O.O
D%
IN
TE
RE
ST
1
3
0.00 100.00%
0
.00
8
0.0
0%
0
.00
1
0.0
0%
0
.00
1
0.0
0%
Q
,00 0
.00
%
TA
XE
S/L
ICE
NS
ES
1
3
0.0
0
10
0.0
0%
0
.00
0
.00
%
0.0
0
0.0
0%
0
.00
1
00
.00
%
0.0
0
0.0
0%
T
AX
ES
/PR
OP
ER
TY
1
3
O,O
Q
10
0.0
0%
0
.00
8
0.0
0%
0.00
10
.00
%
0.0
0
10
.00
%
0.0
0
0.0
0%
D
EP
RE
CIA
TIO
N
13
i.714.51
10
0.0
0%
8
57
.26
50.00%
-1
71
.45
1
0.0
0%
6
85
.80
4
0.0
0%
0
,00
0
.00
%
SE
CU
RIT
Y
13
o.oo
10
0.0
0%
0.00
80.00'/o 0
.00
10.00%
O
.DO
. 10.00
1f,> 0
.00
0.00%
G
AIN
/LOS
S O
N S
AL
E O
F A
SS
IT
13
2,714.24
10
0.0
0%
2. 1
71
.39
80,00Y
c 271.42
10
.00
%
27
1.4
2
10,00%1
O.Q
O
0.0
0%
U
NR
EA
LIZE
D G
AIN
/LO
SS
INV
ES
T
13
£708.7~:ij
10
0.0
0%
:50!.D
0J 8
0.0
0%
f7:)ftG
"l 10.00%
171)_;:",~}
10.00~'o 0
.00
0
.00
%
TOTi-l.L {i3J
.S.1:1)1-09-,5:T-11,0.oa:;.,
"i8:YO..:: •• (tfl
3..'.:.·l:3%,
3/!f.:J .. 3-Q 7
.07
%
J1>23~LO.S
58.8~1%
alJjil G
.DO
%
PO
ST
AG
E &
SH
IPP
ING
{14) N
UM
BE
R
TO
TA
L
%
PR
OG
RA
M
%
DE
VE
LO
PM
EN
T
%
MG
T.G
EN
. %
D
IFF
D
IFF
%
PO
ST
AG
E-
OT
HE
R
14
4
,04
4.0
0
10
0.0
0%
2
,42
6.4
0
60
.00
%
1,6
17
.60
4
0.0
0%
0
.00
0
.00
%
0.0
0
0.0
0%
P
OS
TA
GE
-P
RIN
T M
ED
l'<
·14 3
94
,58
6.2
1
10
0.0
0%
2
95
,93
9.6
6
75
.00
%
98
,64
6.5
5
25.00%
0.0
0
0.0
0%
0
.00
0
.00
½
i a
f4
f I '·
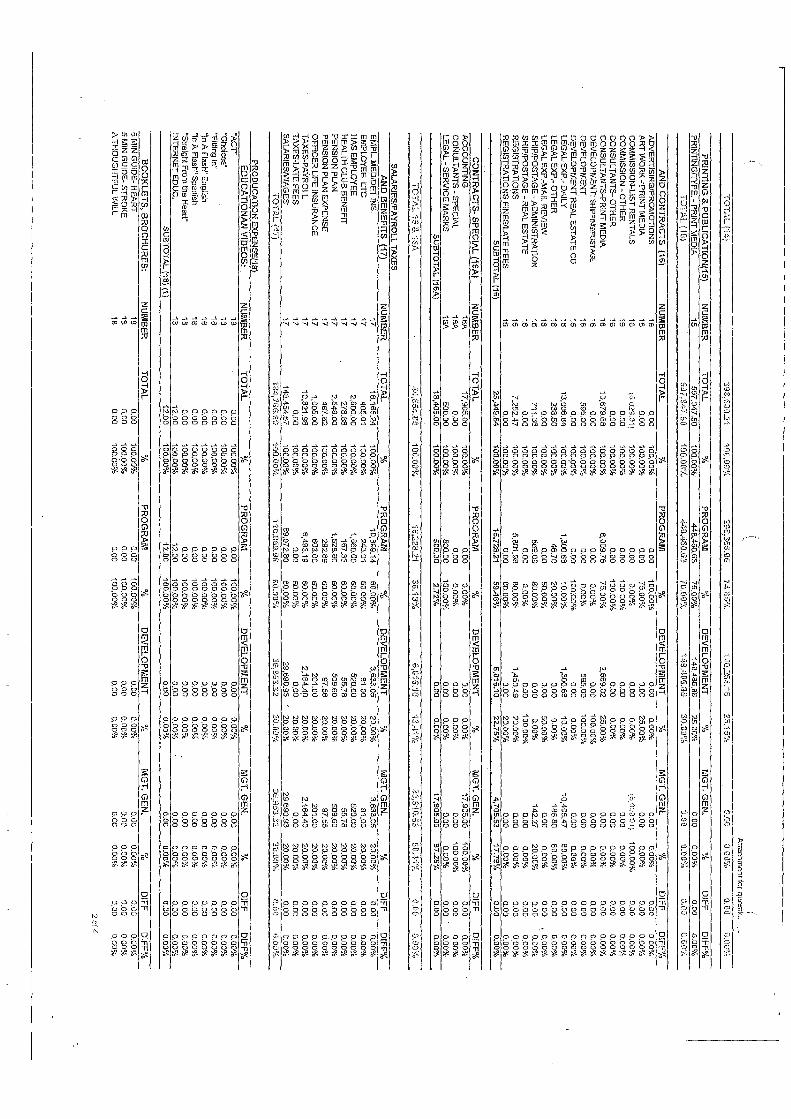
Attachm
ent for ques.tk,. , ....
TO
TI-.L
j·\4} 39•:630..21
1(18.00"'/t. 2S
B~
366.06 74-35·1/•
-; OD
,26~ :t 6 15.•i5"/.HT
CwOC O
.i:nJ.%
o.no O
.li0%
PR
INT
ING
& P
UB
L!C
AT
ION
(15
) N
UM
BE
R
TO
TA
L
%
PR
OG
RA
M
., D
EV
EL
OP
ME
NT
%
M
GT
.GE
N.
%
DIF
F
DIF
F¾
JO
PR
INT
ING
/TY
PE
. -P
RIN
T M
ED
IA
15
597,947.50
100.00%-
44s. • .:-50_53 75_00%
149.486_8'6
25.00%
0.00 0_00%
o_oo
0.0
0%
TO
TA
L(15l
597tfl--:'.-7.SO
rno_ono/. .. : .... -i..G.,1160.63
7Q.(l(!l~;,_
~i i1.9J'WG
.G5
3,iJ.OU
%
(J_(i{! ll.Uct:-'~
O.UG {i.i~, .... n.,,
AN
D C
ON
TR
AC
TS
(1
6)
NU
MB
ER
T
OT
AL
¾
P
RO
GR
AM
%
D
EV
EL
OP
ME
NT
%
M
GT
_G
EN
. %
D
IFF
D
lFF¾
AD
VE
RT
ISIN
G/P
RO
MO
TIO
NS
1
6
o_oo 100.00%
0,00
100,00%
o_oo 0_00%
0.00
0.0
0%
0
,00
0 0
0%
A
RT
WO
RK
--PR
INT
ME
DIA
1
6
0.00 100.00%
0,00
75
.00
%
0.00 25.00%
0,00
0.00%
0.00 0.00%
C
OM
MIS
SIO
N-LIS
T R
EN
TA
LS
16
F-, o:;;£.011
100.00%
D.00
0.00%
0.00 0
.00
%
;,~•;,i)::i):D1}
100.00%
o_oo 0.00%
C
OM
MIS
SIO
N -
OT
HE
R
15 o_oo
100.00"k 0.00
100_00%
0.00 0
.00
%
0.00 0.00%
0.00
0.00%
CO
NS
UL
TA
NT
S-O
TH
ER
1
6
0,0
0
100.00%
o_oo 1
00
,00
%
0.00 0.00%
o_oo
0.0
0%
0,00
0.0
0%
C
ON
SU
LT
AN
TS
-PR
INT
ME
DIA
1
5
1D,579,68
100.00%
8,009.76 7
5.0
0%
2,669.92
25.00%
0.0
0
0_00%
0.00 0.00%
D
EV
ELO
PM
EN
T: SH
IPPING
/POSTAG
E 1
6
0,0
0
100,00%
0.00 0.00%
0
.00
100-00%
0,00
0.00%
0.0
0
0_00%
DE
VE
LO
PM
EN
T
16
595,00
100.00%
a.co 0,000/.'.I
59
5,0
0
10
0.0
0%
0.00
0.0
0%
0.00
0.00%
DE
VE
LO
PM
EN
T R
EA
L E
ST
AT
E C
O
16
o_oo
100-p0%
a_oo 1
00
:00
%
0.0
0
0.00%
o_oa Q_OQo/o
0_00 0
.00
%
LE
GA
LE
<P
_-
DA
ILY
16
13,006_84
100.00%
1,300_68 1
0,0
0%
1,300_68
10.00%
10
,40
5.4
7
80
.00
%
0,0
0
00
0%
LE
GA
LE
XP
.-OT
HE
R
16
2
33
.50
100.00%
46.70
20_00%
D.00
0.00%
186_80 80.00%
0,00
0,00%
LE
GA
LE
XP
.-MA
IL R
EV
IEW
1
6
0.0
0
10•
-00%
0,00 50.00%
0.00
50.00%
0,00 0
.00
%
0.0
0
0.00%
SH
IPJP
OS
TA
GE
-AD
MtN
IST
RA
T!O
N
16
7
11
.36
100.00%
569-09
80_00%
o_oo Q
_OQ
%
14
2.2
7
20
.00
%
0.0
0
0.00%
SH
IPJP
OS
TA
GE
-RE
AL
ES
TA
TE
1
6
o_oo 100.00%
o_oo
0.0
0%
o_oo
10D.00%
a_oo
0.00%
o_oo O
.UO
%
RE
GIS
TR
AT
ION
S
16
7
,25
2.4
7
100~00%
5,301_98 BO
.OD
%
1,450-49 20.00%
0.00
0.00%
Q_O
Q
0,DO
(o R
EG
IST
P.A
TlO
NS
AN
ES
/LA
TE
FE
ES
1
6
0,0
0
100_00%
o_oo 80_00%
0.00
20.00%
a_oo Q
_OO
%
Q_O
O
0_00%
SU
BT
OT
AL
(16
) 26,44,l-84
100.00'¼
15,728.21 5
9.4
6%
6,016.10
22.75%
4,705_53 17.7!3%
0.00
0.0
0%
CO
NT
RA
CT
S-
SP
EC
IAL
(1SA)
NU
MB
ER
T
OT
AL
%
P
RO
GR
AM
%
D
EV
EL
OP
ME
NT
%
M
GT
.GE
N.
%
DIF
F
DIF
F%
A
CC
OU
NT
ING
15A
i?,9
05
.00
1
00
.00
%
0.0
0
0.00%
0.00 0.0D
%
17,905.00 100,00%
0.00
0.00%
CO
NU
LTA
NT
S -
SP
EC
lAL
1
5A
0.00
100.00%
0,00 0
.00
%
o_oo 0
.00
%
o_ao 1
00
.00
%
0.00 0
.00
%
LE
GA
L-S
ER
VIC
E M
AR
KS
"l5A
500_00
100_00%
500.00 100.00%
0.00
0.00%
o_ao 0_00%
a.ca
0.0
0%
S
UB
TO
TA
L (16A
) 1
8.4
05
.00
100.00%
500.00
2-72%
0.00 0
.00
%
17,905.00 97-28%
0.00
0.0
0%
TO
TA
L 1
5 &
"fGA
,:1,4 ,S.-54J)4
10
0.0
0%
-g
,,22
a.2
•i 3~.131,%
610·16,10
'13.4·1%
22/J·l 0.5~
5D,:J.i%
O
_l}l} ::,.D
O%
SA
LA
RIE
S/P
AY
RO
LL
TA
XE
S
AN
D B
EN
EF
ITS
(17
) N
UM
BE
R
TO
TA
L
%
PR
OG
RA
M
%
DE
VE
LO
PM
EN
T
%
MG
T.G
EN
. %
D
IFF
D
lFF
%
EM
PL
ME
DID
ET
INS
. ',7
18,165.24 100.00%
',0,B
B9.14
60
.00
%
3,6
33
.05
2
0.0
0%
3
,63
3.0
5
20_00%
o_oo 0
.00
%
EM
PLO
YE
E-
L TC
1
7
405.01 1
00
.00
%
243.01 60_00%
81.0D
20.-00%
81.0D
2
0.0
0%
o_oo
0_00%
HA
S E
MP
LOY
EE
17
2,600_00 100.00%
1,560.00
60
.00
%
52
0.0
0
20.00%
52
0.0
0
20
.00
%
o_oo 0
.00
%
HE
ALT
H C
LU
B B
EN
EF
rr 1
7
278.38 100.00%
167.33
60
.00
%
55
.78
2
0.0
0%
55.78
20.00%
o_ao D
.00%
PE
NS
ION
PLA
N
17
2.546.00
10
0.0
0%
1,528.80
60
.00
%
50
9.6
0
20.00%
509.60 20_00%
0.00
0.00%
PE
NS
ION
PLA
N E
XP
EN
SE
i7
487-82
100.00%
292.89 6
0.0
0%
9
7.5
6
'40.00%
97
,56
2
0.0
~,t,
o_oo 0.00%
O
FF
ICE
R LIF
E IN
SU
RA
NC
E
17
1,005-00
100_00%
603.00 60_00%
2
01
.00
20.00%
201_00
20
.00
%
Q_OD 0
.00
%
TA
XE
S-P
AY
RO
LL
i7
10,821-98
·too.ooo/o 6.4%
.19 6
0.0
0%
2,164-4!)
20.00%
2.164.40 20.00%
0
.00
0.00%
T
AX
ES
-LA
TE
FE
ES
1
7
G.00
100_00%
0.00 6
0.0
0%
o_oo
20_00%
0.00 2Q
_OO
%
0.0
0
o_OQ
%
SA
LAR
IES
/WA
GE
S
17
1
48
.45
4.6
7
10
0.0
0%
89.•
72-80 6
0.0
0%
2
96
90
_9
3
20.00%
29,690.93 20_00%
0
,00
0
.00
%
iOtP
..L{1
7}
·t 34,7GG
. SO
i00.00%.
1·1U/i5!).90
EO.G
O~·Q
361953~
32 2-0,00%
26~.351-.31
2.D.iJD-0ib G
.jO
e).1)0%
PR
OD
UC
AT
ION
EX
PE
NS
§1
8
ED
UC
AT
ION
AN
VID
EO
S:
NUMBER
TO
TA
L
%
PR
OG
RA
M
%
DE
VE
LO
PM
EN
T
%
MG
T.G
EN
. ¾
D
JFF D
IFF¾
"AC
T" 1
8
0.00 100.00%
o_oo
10
0.0
0%
o_oo
0.00%
0,0
0
0_00%
o_oo 0.00%
"C
hoices" 18
o_oa 100.00%
.0.00
10
0.0
0%
o_oo
0_00%
0.00 0.00%
o_ao
0.00%
"Fillin
g In"
18
0
.00
100.00%
•-0
0
10
0.0
0%
D
,00 O
.OO
~'o 0
.00
0
.00
%
o_oo 0_0Q
%
"In A F
lash" English
18
0
,00
100_0()%
0.00
100_00%
o_oo 0.00%
, 0
.00
0_00%
o_oo
0.00"/4 "In A
Flash'' S
pa
nish
1
8
0.0
0
100.00%
0.00 i0
0,0
0%
0
,00
0.00%
0
.00
0
.00
%
o_oo 0.00%
"S
traight Fro
m the H
eart'' 1
6
a.co 100.00%
0.00
100,00';1, 0
.00
0.00%
0.00
0.00%
0.0
0
0.0
0%
IN
TE
RN
ET
ED
UC
. 1
6
12_00 100.00%
1
20
0
10
0.0
0%
0
,00
0
,00
%
0.00 0.00%
o_oo
0.00%
SU
BT
OT
AL
{18) (1) 12_00
10
0.0
0%
'12.00
10
0.0
0%
o_oo
0.00%
o_oo 0
.00
%
0,()0 0.00%
BO
OK
LE
TS
, BR
OC
HU
RE
S:
NU
MB
ER
T
OT
AL
%
P
RO
GR
AM
%
D
EV
EL
OP
ME
NT
%
M
GT
. GE
N.
01
D
IFF
D
lFF
%
,. ij rvnN G
UID
E-
HE
AR
T
18 0,00
100.00%
0.00 1
00
.00
%
0,00 0
.00
%
0.00 0.00%
D
.00 G
.00%
5 MIN
GU
IDE
-S
TR
OK
E
16
o_oo
100_00%
0.00 100.00o/v
o_oo 0.00%
G
.00 0.00%
0
.00
0.00%
A
TH
OU
GH
TF
UL
WIL
L
1& 0
.00
1(J(l()0%
0.00
10
0.0
0%
D
.00 0.00%
o_oo
0_00%
0.0D
D,00%
2o
!4
----------------------------------------------------------------------------------------------------

At\ach
men
t for question 2a
AC
TIV
ITY
BO
OK
LE
T
i8
0.00 100.00%
a.co
10
0.0
0%
0
.00
0.00%
0.00
0.0
0%
0.00
0.0C%
A
LZ
HE
IME
RS B
OO
KL
ET
ill
0,00 100.00%
0.00
10
0.0
0%
0,00
0.00'11/4 0,00
0.0
0%
0.00
0.0
0%
P
RE
SR
IPT
. DR
UG
-BO
OlQ
ET
i8
0.00
10
0.0
0¾
0.00
10
0.0
0%
0,00
0.00%
0.00 0
.00
%
0.00 0.00%
R
ET
IRE
ME
NT
BO
OK
LE
T
18
o.oo
100.00%
0.00 1
00
.00
%
0.0
0
0.00%
0,00 0
.00
%
0.00 o.00°1o
SA
FE
SE
NIO
RS
BO
OK
LE
T
16
a.ca
1G0.00%
0.00
10
0.0
0%
0.00
1).()0%
0.00 0_00%
0
00
0.00%
W
AT
ER
BO
OK
LE
T -
EN
G
16
0.00
10
0.0
0%
0.00
1-00.00%
0,0
0
0.00%
0,00 0
.00
%
0.00 0
.00
%
WA
TE
R B
OO
KL
ET
-S
PA
N
18
0.00
10
0.0
0%
0.00
10
0.0
0%
0
.00
0.00%
0.00
0.0
0%
0
,00
0.00%
W
AT
ER
BO
OK
LE
T -
PU
ER
1
8
0.00 100.00%
0.00
10
0.0
0%
0
.00
0.00%
0
,00
0.00%
0,00
0.00%
SP
EC
IAL
BO
OK
LE
TS
16
0.00 100.00%
0.00
10
0.0
0%
0
.00
0.00%
0
.00
0.00%
0.00
0.00%
TE
AC
HE
R G
UID
E
18 0
.00
100.00%
0.00
10
0.0
0%
0.00
0.00%
0.0
0
0.0
0%
0.00
0.0
0%
H
EA
RT
SUR
VIV
AL
MA
NU
AL
1
8
0.00 100.00%
0.00
10
0.0
0%
0
,00
0.00%
0
,00
0.00%
0.00
0.0
0%
S
TR
OK
E SU
RV
IVA
L M
AN
UA
L
18
0.00
100.00".,I, 0.00
10
0.0
0%
0.00
0.00%
0.0
0
0.00%
0.00 0.00%
H
EA
RT
LIN
ES N
EW
SL
ET
TE
R
18
0.00
100.00%
0.00 100_00%
o.oa
0.00%
0.00 0.00%
0.00
0.00%
ST
RO
KE
UN
ES
NE
WS
LE
TT
ER
1
8
0.00 100.00%
0.00
100.00%
0.0
0
0.00%t
0.0
0
O.O
D%
0.00
0.00%
AS
PR
IN PIL
L P
AC
K F
F
18
o.oo
100.00%
0.0
0
100.00%
0,0
0
0.00%
0.00 0.00%
0.00
0_00%
SU
BT
OT
AL
(18l (2) 0.00
100.00%
0.00 #D
lV/0!
0.0
0
#DIV
/01 o_oo
#DIV
/01 0.00
#DIV
/Ol
HE
AL
TH
CA
RD
S
NU
MB
ER
T
OT
AL
%
P
RO
GR
AM
%
D
EV
EL
OP
ME
NT
%
M
GT
.GE
N_
%
D
lFF
D
IFF
%
AlZ
ElM
ER
'S C
AR
DS
1
8
0,00 100.00%
0.00
10
0.0
0%
0
.00
0
.00
%
0.0
0
0.00%
0.00 '. 0.00%
H
EA
RT
CA
RD
S
18
o.oo
100.00%
o.oo 1
00
.00
%
0,0
0
o.o.o:i. 0
.00
0.00%
. 0.00
0.00%
ST
RO
KE
(STP.A
P) CA
RO
1
S
0.00 1
00
.0~
1)
0.00 1
00
.00
%
0.0
0
0.00%i-
0.0
0
0.0
0%
0.00
0.0
0%
S
TR
OK
E C
AR
DS
1
8
0.00 100.00%
0.00
100-00%
0.0
0
0.00%
0.0
0
0.0
0%
0.00
0.00%
EM
ER
. INFO
CA
RD
S
18
o.oo
100.00%
0.00 1
00
.00
%
0.00 0.00%
0
.00
0.00%
0.00
0.00%
SU
BT
OT
AL
(18l (3) 0.00
100.00%
0.00 #D
lV/01
0.0
0
#o
tV/0
l 0
.00
#D
IV/01
0.00 #D
lV/O
l
1st A
ID K
ITS
: N
UM
BE
R
TO
TA
L
%
PR
OG
RA
M
¾
DE
VE
LO
PM
EN
T
%
MG
T.G
EN
. %
D
!FF
D
IFF
¾
1st A
ID K
IT-H
EA
RT
1
6
0.00 100.00%
0
.00
1
00
.00
%
0.00 0.00%
o_oo
0.00%
0,00 0.00%
1stA
fD K
IT-S
TR
OK
E
18
0.00
100.00%
0.00 100.00%
0.00
0.0
0%
0
.00
0.00%
0.00
0.00%
1st A
ID K
IT-H
EA
RT
-S/H
1
6
0.00 1
00
.00
%
0.00 1
00
.00
%
0.00 0.00%
0
.00
0.00%
0.00
0.0
0%
istA
ID K
IT-S
TR
OK
E-
S/H
16.
0.00 100.00%
0.00
10
0.0
0%
0
.00
0
.00
%
0.0
0
0.00%
0.00 0.00%
S
UB
TO
TA
L(18) (4)
0.00 100.00%
0.00
#DlV
/0! 0
.00
#O
IV/0!
0.0
0
#DIV
/01 o.oo
#DIV
/Ol
PA
RE
NT
ING
BO
OK
LE
T:
NU
MB
ER
T
OT
AL
" "
PR
OG
RA
M
%
DE
VE
LO
PM
l=N
T
%
MG
T.G
EN
. %
D
IFF
D
IFF
%
BO
OK
OF
PA
RE
NT
ING
1
8
0.00 100.00%
0.00
10
0.0
0%
0.00
0.00%
0.0
0
0.00%
0.00 0.00%
B
OO
K O
F P
AR
EN
TIN
G-S
PA
NIS
H
16
0.00
100.00'lb 0.00
10
0.0
0%
0
.00
0.00%
0
.00
0.00%
0
.00
0
.00
%
BO
OK
OF
PA
RE
NT
ING
-S/H
1
8
0.01) 100.00%
0.00
10
0.0
0%
0.00
0.00%
0.0
0
0.00%
0.0
0
0.00%
BO
OK
PA
RE
NT
JNG
-SP
AN
ISH
-SIH
1
6
0.00 100.00%
0.00
10
0.0
0%
0.00
0.00%
0.0
0
0.00%
0.00 0.00%
S
UB
TO
TA
L (181 {51
0.00 100.00%
0.00
#DIV
/0! o.oo
#DIV
/0! 0
.00
#D
lVIO
l 0.00
#OIV
/01
RE
AD
ING
PR
OG
RA
M:
NU
MB
ER
T
OT
AL
%
P
RO
GR
AM
%
D
EV
EL
OP
ME
NT
%
M
GT
. GE
N.
%
D!F
F
DIF
F¾
C
HA
MPIO
N IN
AL
L-C
OM
IC
1B
0.00 100.00%
0.00
10
0.0
0%
0.00
0.0
0%
0
,00
0.00%
0.00
0.00%
C:H
A!v!PIO
N IN
AL
L-C
OM
IC-S
/H
1S
0.00
100.00%
0.00 1
00
.00
%
0.00 0.00%
0.00
0.00%
0.00 0.00%
S
UB
TO
TA
L (H
I) (6) 0.00
100.00%
0.00 #O
IV/0!
0.00 #D
IV/01
0.0
0
1/0lV/O
l 0.00
#DIV
/QI
OT
HE
R E
DU
PR
OG
RA
MS
: N
UM
BE
R
TO
TA
L
%
PR
OG
RA
M
%
DE
VE
LO
PM
EN
T
%
MG
T. G
EN
. %
D
IFF
D
IFF
%
AN
NU
AL
FUN
D (SPA
NISH
] 1
S
0.00 100.00%
0.00
100.00%
0.0
0
0.00%
0.0
0
0.00%
0.00 0.00%
PIL
L P
AC
K-H
EA
RT
1
8
o.oo 100.00%
0.00
10
0.0
0%
0.00
0.00%
o_oo 0.00%
0.00
0.00%
?OS
TE
R -
HE
AR
T
i8
0.00 100.00%
0.00
10
0.0
0%
0
.00
0
.00
%
0.0
0
0.0
0%
0,00
0.00%
PO
ST
ER
-S
TR
OK
E
18
0.00
100.000/o 0.00
100.00%
0.0
0
0.00°/o 0
.00
0
.00
%
0.0
0
0.00%
SU
BT
OT
AL
(18) (7) o.oo
100.00%
o.oo #P
IV/O
l 0
,00
#D
IV/O
l o.oo
#DIV
/Ol
0,0() #D
lV/O
l
SH
IPP
ING
/PO
ST
AG
E:
NU
MB
ER
T
OT
AL
%
P
RO
GR
AM
%
D
EV
EL
OP
ME
NT
%
M
GT
.GE
N.
%
OIF
F
DIF
F%
S
IP 1
sT A
ID H
RT
1
6
0.00 100.00%
0,00
100_00%
0.00 0.00%
0
.00
0.00%
0
.00
0.00%
S
IP 1
sT A
ID S
TR
1
8
o.oo 1
00
.00
%
o_oo 1
00
.00
%
0,00 0.00%
' 0
,00
0.00%
0.00
0.00%
S/P
5M
INH
RT
1
8
3S.24
10
0.0
0%
39.24
10
0.0
0%
0,00
0.00%
0.0
0
0.0
0%
0.00
0.00%
SIP
5M
IN S
TR
iS
39.24
100.00%
39.24 1
00
.00
%
0.0
0
0.00%
0.0
0
0.00%
0.00 0.00%
S
IP A
TH
OU
GH
TF
UL
WIL
L
16
3.61
10
0.0
0%
3
.8i
100.00%
0,00 0.00%
0
.00
0.00%
0.00
0.00%
SIP
AC
TJV
ITY
BK
1
8
0.00 100.00%
0.00
10
0.0
0%
0.00
0.00%
0.0
0
0.00%
0.00 0.00%
S
IP A
LZ
HE
!ME
R'S
BK
16
o.oo 100.00o/o
0.00 1
00
.00
%
Q.00
0.00%
0,0
0
0~00%
0.00 0.00%
S
IP P
AR
EN
TIN
G B
K
18
0,00
100.00%
0.00 1
00
.00
%
0.0
0
0.00%
o_oo 0_00%
0.00
0.00%
SJP
PR
ES
CP
BK
1ll
0.00 i0
0,0
0%
0.00
rno
.00
%
0.0
0
O.O
O'i'o
0.0
0
0.00%
0.00 0.00%
S
IP R
EA
D P
RO
G
18 0
00
100;00°/o
0.00 1
00
.00
%
0.00 0.00%
o_oo
C.00%
0
.00
. 0.00~'~
SiP
RE
TIR
EM
EN
T B
K
18 0.00
i00.0-0%
0.00 100.00%
0.00
0.00%
0.0
0
0.00%
0.00 0.00%
3o
f4
/
( t

( (
Attach
men
t for q
uestio
i, _
.:i
SIP
SA
FE
SE
NIO
RS
BK
1
8
0.00 100-00%
o.oo
10
0.0
0%
0.0G
C
.00%
0.00 0
.00
%
0.00 0,00%
, S
IP W
AT
ER
BK
1
8
40
.66
100,00%
40.86
10
0.0
0%
0.00
0.00%
0.00 0
.00
%
0.00 0
.00
%
SIP
AL
ZC
AR
D
18
41.B
5 1
00
,00
%
41
.85
100.00%
0.00
0.0
0%
0.00
O.OOll.'o 0.00
0.0
0%
S
IP
HE
AR
T C
AR
D
18
4
1.7
9
100.00%
41
.79
'100.00%
0.00
0.0
0%
0.00
0.0
0%
0.00
0.00°/o S
/f ST
RO
KE
CA
RD
1
8
45
.92
100.00%
4
5.9
2
10
0.0
0%
0
.00
<J.00"/o-
0,00 0.00%
0.00
0.0
0%
S
IP E
ME
R. IN
FO
. CA
RD
1
8
51
.82
1()0.00%
51,82
'100.00%
0.0
0
0.0
0%
0.00
0.00%
0.00 0.00%
S
IP T
EA
CH
ER
S G
UID
E
18
0.00
100.00%
0.00 100.00%
0
.00
0.00%
D
.00 O.OO"la
0.00 0
.00
%
SIP
HO
M
18
0
.00
100.00%
0.00
100.-00%
0.0
0
0.00%
0.00 0
.00
%
0.00 0.00%
S
IP
HR
T M
AN
UA
LS
1
8
00
0
10
0.0
0%
0
.00
100.Q
QO
/ti. 0.00
0.0
0%
D
.00 0.00%
0.00
0,0
0%
S
IP S
TR
OK
E M
AN
UA
LS
1
8
0.0
0
100.00%
0.00 100.00%
0.00
0.0
0%
0.00
0.0
0%
0.00
0.00%
SIP
PIL
L P
AC
K
18
0
.00
1
00
.00
%
0.00 1
00
.00
%
0.00 0
.00
%
0.00 0
.00
%
0.00 0.00%
S
IPA
GT
1
8
0.00 100.0o<',l,
0.00 100.00%
0
.00
0.00%
D
.00 0
.00
%
0.00 0.00%
S
IP C
HO
ICE
S
18
0
.00
100.00%
0
.00
1
00
.00
%
0.0
0
0.0
0%
0.00
0.00%
0.01} O
.QO
P/c,
SIP
Flm
NG
lN
16
0.00
10
0.0
0%
o.oo
100.00%
0.0
0
0.00%
0.00 {),00%
0
.00
0
.00
%
SJP
IN A
FL
AS
H
18 0
.00
100.00%
0
.00
100.00%
0
.00
0.00%
•
.00 0.00%
0.00
0.00%
SIP
IN A
HE
AR
T
16 C
.00 1
00
.00
%
0.00 1
00
.00
%
0.0
0
0.00%
0.0
0
0.00%
0.00 0.00%
P
RO
GR
AM
EX
PE
NS
E
18
8
3.3
0
10
0.0
0%
llS
.30 100~00%
0
.00
0.00%
0
.00
0.00%
0.00
0,0
0%
S
UB
TO
TA
L l1B
) {8) 387.B
3 'IO
O.ll0%
387.83
10
0,0
0%
0
.00
0.00%
0.00
0.00%
0.00 0.00%
TO
TA
L P
RO
GR
t'..Pl~ C
OS
T (ig
) 3~:g_33
10\'tOO
o/.t -Z
B9.~3
1/JD.00'¼
. [LU
O
GJJ.il%
. o.oa
Q..(}Q
ll,'., (LO
O
~. C.OU':
1'.:;
SW
EE
PS
TA
KE
S P
RIZ
ES
{19) N
UM
BE
R
TO
TA
L
¼
PR
OG
RA
M
%
DE
VE
LO
PM
EN
T
%
MG
T.G
EN
. %
D
IFF
D
IFF
%
GIF
TS
-O
TH
ER
1
9
2,8
35
.84
1
00
.00
%
0.00 0.00%
0,00
0.00%
2,838.84 100.00%
0.00
0:00%
PR
JZE
S S
WE
EP
S C
ON
TE
ST
1
9
1,2
00
.00
1
00
.00
%
0.00 0
.00
%
1,2
00
.00
100,00%
0.00
0.00%
0.00 0,.00%
D
EV
EL
OP
ME
NT
EXP. 1
9
o.oo i0
0.0
0%
0.00
0.0
0%
0,00
0.0
0%
0.00
0.00%
0.00 1
00
.00
%
fOT
AL
{'lSJ
d.,.1 035.34 ·rno.oo¾
(,i.f/() l}.{H
J%,
·!,2fJG.O
::ll) 29.73%
2.33G
...~l 7t}.2T
;.l,) l1.DO
!LOG~;;,
GR
AN
TS
(20) N
UM
BE
R
TO
TA
L
%
PR
OG
RA
M
%
DE
VE
LO
PM
EN
T
%
MG
T.G
EN
. %
D
IFF
D
IFF
¾
GR
AN
1S
2
0
3,0
00
.00
100.00%
3.000.00
10
0.0
0%
0.00
0.0
0%
0.00
0.00%
0.00 0
.00
%
GR
AN
T &
AL
LO
CA
TIO
N
20
0
,00
100.00%
0.00
10
0.0
0%
0.00
0,0
0%
0.00
0.00%
0.0
0
0.0
0%
G
RA
NT
DE
VE
LO
PM
EN
T
20
1
,79
9.0
0
10
0.0
0%
1,799.00
10
0.0
0%
0.00
0.00%
0,00 0.00%
D
.00 0
.00
%
CH
AR
ITA
BL
E D
ON
AT
ION
S
20 3
00
.00
100.00%
300.00
10
0.0
0%
0,00
0.00%1
0,00 0.00%
0.00
0.0
0%
T
OT
AL
{2'J
} 5.,'099))(.t
·JGO.OfJ~J~ 5.099,iJG
·H
J0.00°;~ 0.D
O
l}_(t(j~d c~.Lm
(.1.00%
d.lHl
r;.no~·~
HE
AL
TH
CA
RE
PR
OD
(21
) N
UM
BE
R
TO
TA
L
%
PR
OG
RA
M
%
DE
VE
LO
PM
EN
T
%
MG
T.G
EN
. %
D
IFF
D
lfF%
C
OS
T O
F S
AL
ES
21
0.00 100.00%
0.00
10
0.0
0%
0.00
0.00%
0.0
0
0.0
0%
0.00
0.00%
INV
EN
TO
RY
AD
JUS
1M
EN
ST
S
21 0
.00
1
00
.00
%
0.00 1
00
.00
%
0.0
0
0.00%
0.00 0,00%
0
.00
0.00%
B
AN
K D
ISC
21
0.0
0
10
0.0
0%
0.00
10
0.0
0%
0.00
0.00%
0.0
0
0.00"/4 0
.00
0.00%
S
IP P
RO
DU
CT
S
21 o.oo
10
0.0
0%
0,00
10
0.0
0%
0.00
0.00%
0,0
0
O.O
O'}b
0.00 0.00%
P
UR
CH
AS
E D
1SC
. EX
P IT
EM
S
21 o.oo
100.00%
0.00 1
00
.00
%
0.0
0
0.00%
0.00 0
.00
%
0.00 0
.00
%
BA
NK
FE
ES
21
0.00 1
00
.00
%
0,00 1
00
.00
%
0.0
0
0.00%
0.0
0
0.00%
0,0
0
0.00%
TC
T~
IJ.O
!l -W
O.OD-0/o li.CKl
t1DJVfO'. G
.00 ,/01\//IH
!'..tOO
i;mv101
(UIO
i'::[H
Vifft
LA
ND
DE
AL
S (22}
NU
MB
ER
T
OT
AL
%
PR
OG
RA
M
%
DE
VE
LO
PM
EN
T
%
MG
T.G
EN
. ¾
D
lFF
D
!FF
%
LE
GA
L
22
0,00
100.00%
0.00 5
0.0
0%
0
.00
0,0D
%
0,00 5
0.0
0%
0.00
0.0
0%
C
OM
MIS
SIO
NS
2
2
0.0
0
100.00%
0.00 5
0.0
0%
0
.00
0.00%
0.00
50.00%
0.00 0
.00
%
OT
HE
R
22
0
.00
100.00%
0.00
50_00%
0.00 0.00%
0.00
50
.00
%
0.00 0
,00
%
RE
AL
ES
TA
TE
2
2
0.0
0
10
0.0
0%
0.00
50_00%
0.00 0.00%
0
.00
50.00%
0.00
0.00%
LA
ND
DE
AL
S
22
5
95
.06
1
00
.00
%
297.53 5
0.0
0%
0
.00
0
,00
¾
29
7.5
3
50
.00
%
0.00 0.00%
S
HlP
/PO
ST
AG
E -
LAN
O D
EA
LS
22
0.00
"100.00%
0.00 50.00%
0.00
0.00%
0,00 5
0.0
0%
0,00
O,O
Do/~ T
OT
J\L
(22
) 595.G
S
-rvauu:,;~ 2.~7.;J3
SG,G
u",S 0
.(\() {LGQ~.:,.
1.~7.53 .::;u_r,n;:;
f.U}ft
0.0
0%
GR
.f:~JD -roT/lj__
i,,-:-JtS,·J2E~}J9 .,iUOJDO'%
g-;:c~). ~1 ;.-:9 ._n0
05 .. ~'0~1!1
~-~B/3.BiJO, ~1 :; ~~~~•-·f91-::.,a,
·f?(£/]9G.t~:}
·g~3~~~:{. _G~0L'
(t{~{!);
4 of4
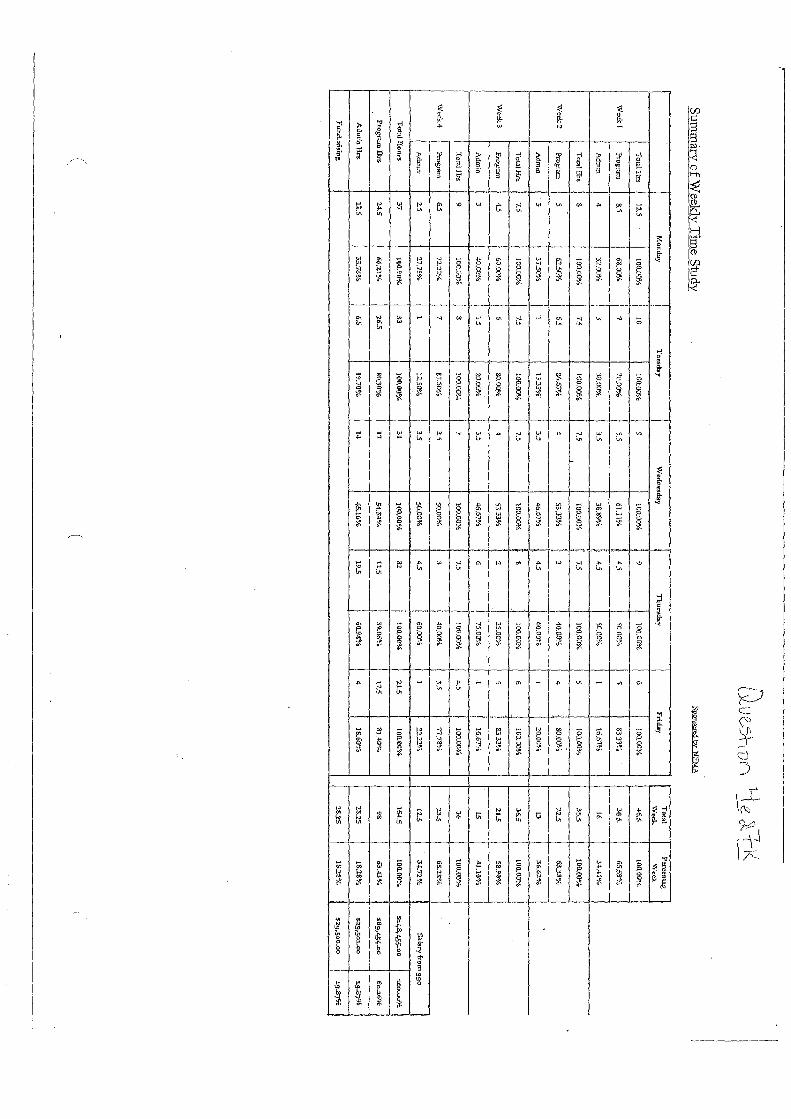
t\ . .
Ul V
l.S·h V
i'1 Y
e l +-1< -
-
Sum
mary o
f Weekly T1m
e Study
Spont:cred by: N
B.,rA
MoaW
ly iu
esc
by
W
ed'1esch!y T
hursd:i:ty F
rlw,y
Toe:al P
ercent.ng
Wool<
W~
k
Total H
o
12.5 100.C
IQ¼
10
100.00%
9 10Q
OO
%
9 100.00%
6
]00
.00
¾
~6.S [0
0;0
0%
We<:kl
Progcam
8.5 68.00%
7
10.0~/4
55
61.11¾
I l
45
so.o~-a
5 33.33%
3
(l5.
65.59'%,
Adm
tn 4
32.00%
J 3.<J.OCF/4
3.5 3S
.89¾
t 4.5
50.00%.
l 16.67%
. 16
34,41Uii,
I
ToC:11 Hrs
s 100.00¾
7:5
100.00%
7.5 ~00.00%
l
7.5 100.00%
s
100,00%
35
5
100.00%
I
'\\,'cek2
P
ro£.!am
5 62.51":%
6.5
81,.67%
4 53.33%
!
3 40.00%
.. 4
so.oo' ... o 2
25
63.3X
%
Ad
m,n
·3
37.50"/o.
l 1
33
3%
3
5
46.6-7"/4 l!
45
6
0.0
~C
, I
20
.00
%
n 3
6.6
2%
Total.H
n 7.5
100.C-©
f. 7.!
!00.00%
7.5 100.00%
8
100.00%
6 JO
O.D
O%
36.5
100.00%
Week
3
Pro-.fmm
4.5
60.0C%
6
30.00%
., 5
3.3
3%
0
25
.00
%
5 83-33%
2
1.5
5
8.9
0%
i A
dmin
3 40.0~
/o 1
5
20
.00
%
3.5 46.67%
6
j 75.00%
I
16.67%
15 4J.10b/iJ
' I T
ot:31Hrs
9 100.G
O¼
8
10
0.0
0%
7
100.00%
1.5 I
100..00%
4.5 100.00%
3
6
100.00a,./,, I
Wi:.::k4
Program
6
5
T'--2.2%
7
&1.50':','o 3.5
:50.00¾
3 f
-to.ore·i. 3.5
Tl.7
8%
2-3.5
6S
.28
%
i
Ad.m
in 2:5
27.?E¾
l
12,500'/o 3.5
50.00%
4.S ;
60.00%
1 12.22%
1
2.$
3
4.7
2%
S
alary fcom 9
90
! '
Totnl H
ours 3
7
100.80%
33
1-00.00%
3
1
]00
.00
%
32
f
10
0.0
0¾
2
1.5
lO
!LO
O¼
154.S
100-00%
s14S
, 455-00 1
00
..00
%
Pr<>gn::m.Ilrs.
24.S
66
.22
%
26.S
8'0.30-/,, 1
7
54.:1>4%.
ll.S
i 39.06'!·P
17..5 8
1-4
0%
9
8
63
. .0%
s89,454-oo
60
.16
%
Ai'.Jut~a H
rs 12.5
33
.. 73.%
6.5 g,p7{)'1,~
u 45.16¾
19.5
60-94%
4 18.60%
28..25
18.28%
S2
gr5
0l-O
O
19.$7'¾
Ftrncl..fflsing 2
0.2
5
1S:.:Z3%
$2
9,5
00
.00
19.87%

Exhibit F

Exhibit F.1

+
17
48
7 N
SC
Me
mb
ers
hip
Ren
OS
E_
31
08
NS
C M
em
be
r#3
OS
E 2
/9/1
6 3
:35
PM
P
age
1 --
$-
~
NA
TIO
NA
L
ST
RO
KE
>
CO
lJN
CIL
sM®
( a
pro
gram
of N
atio
nal
Em
erge
ncy
Med
icin
e A
ssoc
iati
on)
Mr.
Jo
hn
Sam
ple
per
son
N
ewp
ort
Cre
ativ
e C
om
mu
nic
atio
ns
33 R
ailr
oad
Av
enu
e D
uxbu
ry,
MA
023
32
111,,
,,, I, I
.. I I ..
. II ..
, I, I,
,11,1,
, I, I .
. I .. I
., I., I
I, .. I
I ... ,
I II
10216
7487
NS
C M
emb
ersh
ip R
enew
al
OS
E
Do
cum
en
t S
ize:
9.5
X 4
.12
5"
Co
lors
Use
d: P
MS
17
97
red
, 8
72
go
ld
--$
-
+
Dia
nn
e 7
.23.
151

17487 NSC Membership Ren FORM_Layou\ 1 2/16/16 1 :33 PM Page 1
NATIONAL STROKE
~~COUNCILs .. (a pr?gram of Natio~1al Eff!-e~-gen~y Medici~e Association)
P.O. Box 1039 Edgewood, MD 21040 www.nemahealth.org
Dear Mr. Sampleperson:
March 8, 2016
The Annual Fund Drive is our most important appeal of the year and your help is urgently needed now.
Over 100,000 Americans will die of stroke this year. Stroke (brain attack) is a leading cause of death and disability in adult Americans. We are winning the battles but have not yet won the war against stroke. Don't let stroke disable or kill you or someone in your family. Follow the guidelines provided on the back of this letter, And, make a small gift so that others may live.
Our plans are in place for the programs, educational materials and equipment grants that are so vital to so many people - people in your local area - perhaps even someone in your own family.
With your past support Mr. Sampleperson, we have been able to expand our grants for stroke education and develop stroke prevention materials for individuals at risk.
Your 2016 Amrnal Fund gift is vital to our success in fighting stroke and so much more needs to be done.
Please, won't you help us continue to give the gift of life by making your 2016 Annual Fund gift today? Thank you, you are a lifesaver!
~:!& President ~rzr/1 ()
P.S. Nothing is tougher than living with, dying from or losing a loved one to a stroke. Please give as generously to the Amrnal Fund as you can and send in your renewal gift today! Thank you!
___ •••• ___ •• _ ••• ____ • ___ 'I'. OETACHAT PERFORATION _'I' _______ • ___ • ________ • ____ •- ___ ._. __ ••••• ··- 'I' OETACHAT PERFORATION 'I' __ •• _____ ._ •• __ .?.~ ___ _ NATIONAL STROKE COUNCIL.,
1• _N'f'?'" ,,r Na!oo•~ .f:n..,;,ory ~''!'.'~~• ''=""'"'!"':/
D Yes! I will continue my membership in the National Stroke Council with my 2016 Annual Fund Gift,
John Sampleperson Newport Creative 21 Railroad Avenue Duxbury, J\l!A 02332
0 $XX D $XX
0 $XX 0$ __
Please make your check payable to: Nntlonnl Stroke Council or NSC, See reverse for credit card info.
~ Retum this portion with your membership g/{t.
Detach your Membership Card below at pe1:f'oratio11.
t
a program of the National Emergency A1edicine Association
This certifies that
is a member in good standing in the National Stroke Council
SIGNATURE
Document Size: 8.5 x 14" Colors: PMS 1797 Red, 872 Gold an~ and black lasers I 02167487 NSC Membership Renewal FORM

17487 NSC Membership Ren FORM_Layout 1 2/16/16 1:33 PM Page 2
STROKELINES
We all want to reduce our risk of stroke • that's for sure. A 1·ecent issue of Strokelines covered hemorrhagic stroke, the type of stroke that occurs when a blood vessel in the brain ruptures. One way to reduce your risk of this type of stroke is by con trolling high blood pressure.
Another type of stroke, in fact the most common type of stroke, is called ischemic stroke. Ischemia means a loss of blood supply to an organ, so an ischemic stroke means the blood supply is stopped to a ce1·tain area of the brain. This type of' stroke accounts for about 75% of' all st1·okes.
Ischemic strokes may occur when an artery becomes blocked by a clot that forms along the vessel wall. Such clots often form in an artery that is becoming blocked, as in the case of atherosclernsis. Atherosclerosis is the deposition of fatty material in the lining of a blood vessel, and over time, the vessel will become more and more occluded. Clots are more likely to form in these damaged vessels and completely shut off the blood supply. When this happens the type of ischemic stroke is called thrombotic.
If a clot that forms in a damaged vessel breaks loose and is carried away with the blood, it may travel until it reaches a vessel small enough to trap it. In this case, the type of ischemic stroke is called embolic, because a traveling clot is called an embolus.
In either case, one way to help reduce your risk of stroke is to have your blood cholesterol level checked. High blood cholesternl, that is, a total cholesterol over 200mg/dl, is considered too high. Some experts say that total cholesterol is not as important as two other measurements: high and low density lipoproteins, or HDL and LDL. These levels should be greater than 35 mg/dl and less than 130 mg/dl, respectively.
What can you do if your cholesterol level is too high? Many people respond well to dietary management. Limiting the amount of high cholesterol foods in your diet, such as red meat, eggs, butter, and other dairy products, may bring your cholesterol down to a more desirable level. Using cooking methods like steaming or baking instead of frying is also helpful.
Getting enough exercise has also been shown to reduce cholesterol levels. You can institute a simple walking program to help improve your overall health as well as lowering your cholesterol.
If your total cholesterol is very high, 240 mg/dl or higher, your physician may prescribe cholesterollowering dl'ltgs to bring it down. So it's important to see your physician and find out what your cholestcrnl number is. Let's all start today to reduce our risk of stroke!
The National Emergency Medicine Association wasfo11nded by Frederick C. Ruofin 1982
BEQUESTS Over the years many individuals have provided generously for National Stroke
Council in their wills. You may transfer cash, stock, real estate, furniture, art work or closely held stock to National Stroke Council under your will. In this way you will help secure the future of National Stroke Council, and your estate will benefit by saving taxes.
For more information about giving through your will call the National Stroke Council (a program of National Emergency Medicine Association) at (443) 922-7533.
CREDIT CARD GIVING INFORMATION I wish to charge a gift of $ _______ on my: • VISA I wsA I • MasterCard [,.J
CARD NO.
SIGNATURE (required)
NAME ON CARD (please print)
EXP. DATE (MONTH/YEAR)
-
NATIONAL STROKE COUNCJL®
la program of Na/Iona/ Emergency Medicine AMocwlionJ
My telephone number is: ___________ My email address is: ________ _
Please include this form with your credit card information or check payable to National Stroke Council In the enclosed reply envelope. Your gift is tax-deductible to the extent allowed by law, Thank you I

+
17
48
7 N
SC
Me
mb
ers
hip
Ren
RE
_N
EM
A L
ap
sed
Do
no
r B
RE
2/9
/16
4:51
PM
P
ag
e 1
----
-®-
THAN
K YO
U!
yoU
R G
ENER
OUS
GIFT
HEL
P SA
VE u
\/ES,
I
Nat
ion
al S
tro
ke C
ou
nci
l (a
pro
gram
of t
he
Nat
ion
al E
mer
gen
cy M
edic
ine
Ass
ocia
tion
)
PO
BO
X 1
03
9
ED
GE
WO
OD
, M
D 2
10
40
-03
39
C2
10216
7487
NS
C M
emb
ersh
ip R
enew
al
RE
~
Do
cum
en
t S
ize:
8.8
75 X
3.8
75"
Col
ors:
Bla
ck P
rint
s on
#2
4 lb
Wh
ite W
ove
1 11111
1111111
Ill I 11
I I I I I 1
1 I 1111
1111
1 111
1 h I 11I
111 111
11111
1 111 11
1 1 P
LEA
SE
P
LAC
E
PO
ST
AG
E
ST
AM
P
HE
RE
Dia
nn
e 2.9
.161
+

+
74
87
NS
C M
embe
rshi
p R
en R
E_N
EM
A L
apse
d D
on
or
BR
E
2/9/
16
4:51
PM
P
age
2--@
-
NSC
FACT
S So
licita
tion
For C
harit
able
Pur
pose
s Ca
rd
ABOU
T TH
E NA
TION
AL E
MERG
ENCY
MED
ICIN
E AS
SOCI
ATIO
N (in
corp
orat
ed in
Was
hingt
on, D
.C.)
WIT
H IT
S sp
ecial
pro
gram
NAT
IONA
L ST
ROKE
COU
NCIL
(NSC
). NE
MA
with
its
spec
ial p
rogr
am N
SC is
a
natio
nal h
ealth
org
aniza
tion
oper
ating
und
er n
on-p
rofit
tax
exem
pt In
tern
al Re
venu
e Co
de 5
01 (
c)(3)
. Th
roug
h ou
r m
ailin
gs w
e ra
ise th
e m
uch
need
ed fu
nds
for
the
prev
entio
n of
inju
ry a
nd il
lnes
s by
ad
dres
sing
heal
th a
nd s
ocia
l iss
ues
thro
ugh
educ
atio
n, a
pplie
d re
sear
ch, t
echn
olog
y, a
nd e
quip
men
t.
If yo
u wi
sh a
copy
of t
he s
umm
ary
of th
e lat
est f
inanc
ial s
tate
men
t, or
ann
ual r
epor
t, an
d re
gistra
tion
filed
by T
he N
ation
al Em
erge
ncy
Med
icine
Ass
ociat
ion, p
lease
write
to u
s at
P.O
. Box
103
9, E
dgew
ood,
MD
2104
0 (4
43)
922-
7533
. We
will
be p
lease
d to
resp
ond
prom
ptly.
Som
e sta
tes
requ
ire th
at s
pecia
l not
ices
be in
clude
d wi
th e
ach
solic
itatio
n. If
you
are
a re
siden
t of o
ne o
f the
se s
tate
s, yo
u m
ay o
btain
fina
ncial
inf
orm
ation
dire
ctly
from
the
state
age
ncy:
FLO
RID
A-A
COPY
OF
THE
OFFIC
IAL
REGI
STRA
TION
AND
FINA
NCIA
L IN
FORM
ATIO
N MA
Y BE
OBT
AINE
D FR
OM T
HE D
IVIS
ION
OF C
ONSU
MER
SERV
ICES
BY
CALL
ING
TOLL
FR
EE, 1
-800
-435
-735
2 (S
OD-H
ELP-
FLA)
WITH
IN T
HE S
TATE
. REG
ISTR
ATIO
N DO
ES N
OT IM
PLY
ENDO
RSEM
ENT,
APPR
OVAL
, OR
RECO
MMEN
DATI
ON B
YTHE
STA
TE. F
lorida
Reg
istra
tion
#CH3
13. M
ARYL
AND
-Fo
r th
e co
st of
cop
ies a
nd p
osta
ge, O
ffice
of th
e Se
cret
ary
of S
tate
, Stat
e Ho
use,
Anna
polis
, MD
2140
1 MI
SSIS
SIPP
I -Th
e of
ficial
regis
tratio
n an
d fin
ancia
l inf
orm
ation
of T
he N
ation
al Em
erge
ncy
Med
icine
Ass
ociat
ion
may
be
obta
ined
from
the
Miss
issipp
i Sec
reta
ry o
f Sta
te's
offic
e by
call
ing 1
-888
-236
-616
7. R
egist
ratio
n by
the
Secr
etar
y of
Sta
te d
oes
not i
mply
end
orse
men
t. NE
W J
ERSE
Y -
INFO
RMAT
ION
FILED
WITH
THE
AT
TORN
EY G
ENER
AL C
ONCE
RNIN
G TH
IS C
HARI
TABL
E SO
LICITA
TION
AND
THE
PERC
ENTA
GE O
F CO
NTRI
BUTIO
NS R
ECEIV
ED B
Y TH
E CH
ARITY
DUR
ING
THE
LAST
REP
ORTIN
G PE
RIOD
THA
T W
ERE
DEDI
CATE
D TO
TH
E CH
ARIT
ABLE
PU
RPOS
E M
AY
BE
OBTA
INED
FR
OM
THE
ATTO
RNEY
GE
NERA
L OF
THE
ST
ATE
OF
NEW
JER
SEY
BY C
ALLIN
G (9
73)
504-
6215
AN
D IS
AV
AILA
BLE
ON
THE
INTE
RNET
AT
www.
njcon
sum
eraf
fairs
.gov
/ocp
.htm
#cha
rity.
REGI
STRA
TION
WITH
THE
ATT
ORNE
Y GE
NERA
L DO
ES N
OT IM
PLY
ENDO
RSEM
ENT.
NEW
YOR
K -
Offic
e of
the
Atto
rney
Gen
eral,
Dep
artm
ent o
f Law
, Cha
rities
Bur
eau,
120
Broa
dway
, New
Yor
k, NY
102
71. N
ORTH
CAR
OLI
NA-F
INAN
CIAL
INFO
RMAT
ION
ABOU
T TH
IS O
RGAN
IZATIO
N AN
D A
COPY
OF
ITS L
ICEN
SE A
RE A
VAILA
BLE
FROM
THE
STA
TE S
OLIC
ITATIO
N LIC
ENSI
NG B
RANC
H AT
1-8
88-8
30-4
989.
THE
LIC
ENSE
IS N
OT A
N EN
DORS
EMEN
T BY
THE
STA
TE. P
ENNS
YLVA
NIA-
The
offic
ial re
gistra
tion
and
finan
cial i
nfor
mat
ion o
f The
Nat
ional
Emer
genc
y M
edici
ne A
ssoc
iation
may
be
obta
ined
from
the
Penn
sylva
nia D
epar
tmen
t of S
tate
by
callin
g to
ll-fre
e, w
ithin
Penn
sylva
nia, 1
-800
-732
-099
9. R
egist
ratio
n do
es n
ot im
ply e
ndor
sem
ent.
VIRG
INIA
-Vi
rgini
a St
ate
Divis
ion o
f Con
sum
er A
ffairs
, Dep
artm
ent
of A
gricu
ltura
l and
Con
sum
er S
ervic
es, P
O Bo
x 11
63, R
ichm
ond,
VA 2
3218
. WAS
HING
TON
-Ch
aritie
s Di
vision
, Offic
e of
the
Secr
etar
y of
Stat
e, St
ate
of W
ashin
gton
, Olym
pia, W
A 98
504-
0422
, 1-8
00-3
32-4
483.
W
EST
VIRG
INIA
-Re
siden
ts m
ay o
btain
a su
mm
ary
of th
e re
gistra
tion
and
finan
cial d
ocum
ents
from
the
Secr
etar
y of
Stat
e, St
ate
Capit
ol, C
harle
ston,
WV
2530
5. R
egist
ratio
n wi
th a
ny o
f the
se s
tate
age
ncies
doe
s no
t im
ply e
ndor
sem
ent,
appr
oval
or re
com
men
datio
n by
any
sta
te.
--@
-
+

Exhibit F.2
+
1757
8 N
SC
Ju
ne
20
16
OS
E_
31
08
NS
C M
em
be
r #3
OS
E 5
/5/1
6 4
:29
PM
P
age
1
ID N
AT
ION
AL
ST
RO
KE
CO
UN
CIL
®
P.O
. B
ox 1
039
Edg
ewoo
d, M
D 2
1040
w
ww
.nem
ahea
lth
.org
(A p
rogr
am o
f Nat
iona
l Em
erge
ncy
Med
icin
e A
ssoc
iati
on)
Ms.
Jan
e S
ampl
eper
son
New
port
Cre
ativ
e C
omm
unic
atio
ns
21 R
ailr
oad
Ave
nue
Dux
bury
, M
A 0
2332
-380
7 I Il
l 11111
1 '1111
I II I Ii
I •111
h111
111 h
h 111
In111
1 n In
I u tp
pl 11
I
1051
675
78 N
SC
Mem
ber
ship
Ren
ewal
O
SE
D
ocu
me
nt
Siz
e: 9
.5 X
4.1
25
" C
olor
s U
sed:
PM
S 1
79
7 r
ed,
87
2 g
old
~
+
~
Dia
nn
e 5
.4.1
61

17487 NSC Membership Ren FORM_Layoul 1 5/5/16 4:26 PM Page 1
D $XX D $XX
D $XX 0$ __
D Yes! I will continue my membership in the National Stroke Council with my 2016 Annual Fund Gift.
Please make your check payable to:
John Sampleperson Newport Creative 21 Railroad Avenue Duxbury, l\llA 02332
Natlonnl Stroke Council or NSC. See reverse for credit curd info.
11 NATIONAL STROKE COUNCIL P.O. Box 1039 Edgewood, MD 21040 www.nemahealth.org
(A program of National Emergency Medicine Assrx:iation)
Ms. Jane Sampleperson Newport Creative Communications 21 Railroad Avenue Duxbury, MA 02332-3807 lrulllll1l11l11111l•l•1••l1l11l11l1l1ll111111llll11llll11•1'IIII
Dear Mr. Sampleperson:
~ Return this portion with your membership g(ft.
Detach yo11r A1embership Card below at pe1foralio11.
•
a prugram of the National Emerge119 1 Medicine Assodation
This certifies cha L
is a member in good standing in the National Stroke Council
~H1Ni\TURI~
June 7, 2016
The Annual Fund Drive is our most imporfant appeal of the year and your help is urgently needed now.
Over 100,000 Americans will die of stroke this year. Stroke (brain attack) is a leading cause of death and disability in adult Americans. We are winning the battles but have not yet won the war against stroke, Don't let stroke disable or kill you or someone in your family. Follow the guidelines provided on the back of this letter. And, make a small gift so that others may live.
Our plans are in place for the programs, educational materials and equipment grants that are so vital to so many people - people in your local area - perhaps even someone in your own family.
With your past support Mr. Sampleperson, we have been able to expand our grants for stroke education and develop stroke prevention materials for individuals at risk.
Your 2016 Annual Fund gift is vital to our success in fighting stroke and so much more needs to be done.
Please, won't you help us continue to give the gift of life by making your 2016 Annual Fund gift today? Thank you, you are a lifesaver!
Sincerely,
Jffft~ President ,erz# {,)
P.S. Nothing is tougher than living with, dying from or losing a loved one to a stroke. Please give as generously to the Annual Fund as you can and send in your renewal gift today! Thank you!
I 05167578 NSC Membership Renewal FORM ~
Document Size: 8.5 x 15" Colors: PMS 1797 Red, 872 Gold and BIB'ck and black lasers
F2
17487 NSC Membership Ren FORM_Layout 1 5/5/16 4:26 PM Page 2
CREDIT CARD GIVING INFORMATION I wish to charge a gift of $ _______ on my: • VISA I VIM I • MasterCard f•J
CARD NO.
SIGNATURE (required)
NAME ON CARD (please print)
EXP, DATE (MONTH/YEAR)
ID NATIONAL STROKE COUNCIL®
ru µrogrum n( Notw11ul E111erg~11t:v Motd1w1~ As~u!'l1rt1u11)
My telephone number is: ___________ My email address is: ________ _
Please Include this form with your credit card Information or check payable to National Stroke Council In the enclosed reply envelope, Your gift is tax-deductible to the extent allowed by law, Thank you I
STROKELINES
We all want to t·educe our risk of st1·oke - that's for sure. A recent issue of Strokelines covered hemonhagic stroke, the type of stroke that occurs when a blood vessel in the brain ruptures. One way to reduce your risk of this type of strnke is by controlling high blood pressure.
Another type of stroke, in fact the most common type of stroke, is called ischemic stroke. Ischemia means a loss of blood supply to an organ, so an ischemic stroke means the blood supply is stopped to a certain area of the brain. This type of stroke accounts for about 75'¼, of all strokes.
Ischemic strokes may occur when an artery becomes blocked by a clot that forms along the vessel wall. Such clots often form in an artery that is becoming blocked, as in the case of atherosclerosis. Atherosclerosis is the deposition of fatty material in the lining of a blood vessel, and over time, the vessel will become more and more occluded, Clots are more likely to form in these damaged vessels and completely shut off the blood supply. When this happens the type of ischemic stroke is called thrombotic.
If a clot that forms in a damaged vessel breaks loose and is carried away with the blood, it may travel until it reaches a vessel small enough to trap it. In this case, the type of ischemic stroke is called embolic.\ bee a use a traveling clot is called an embolus.
In eithet· case, one way to help reduce your risk of stroke is to have your blood cholesterol level checked. High blood cholesterol, that is, a LoLal cholesternl over 200mg/dl, is considered Loo high. Some experts say that total cholesterol is not as important as two other measurements: high and low density lipoproteins, or HDL and LDL. These levels should be greater than 35 mg/dl and less than 130 mg/dl, rnspectively,
What can you do if yom cholesterol level is too high? Many people respond well to dietary management. Limiting the amount of high cholesterol foods in your diet, such as red meat, eggs, butter, and other dairy products, may bring your cholesterol down to a more desirable level. Using cooking methods like steaming or baking instead of frying is also helpful.
Getting enough exercise has also been shown to reduce cholesterol levels. You can institute a simple walking program to help improve your overall health as well as lowering your cholesterol.
If your total cholesterol is very high, 240 mg/di or higher, your physician may prescribe cholesterollowering drugs to bring it down. So it's important to see your physician and find out what your cholesterol numbet· is. Let's all start today to reduce out· l'isk of stroke!
The National Emergency Medicine Associalion was founded by Fredei°ick C. Ruof in I 982
BEQUESTS Over the years many individuals have provided generously for National Stroke
Council in their wills. You may transfer cash, stock, real estate, furniture, art work or closely held stock to National Stroke Council under your will. In this way you will help secure the future of National Stroke Council, and your estate will benefit by saving taxes.
For more information about giving through your will call the National Stroke Council (a program of National Emergency Medicine Association) at (443) 922-7533 .

+
1757
8 N
SC
Ju
ne
20
16
CR
E_
NE
MA
La
pse
d D
on
or
BR
E
5/4
/16
5:
20 P
M
Pa
ge
1
--@--
THAN
K YO
U!
yoU
fl GE
NERO
US G
IFT
HELP
SAV
E LIV
ES-
Nat
ion
al S
tro
ke C
ou
nci
l (a
pro
gram
of t
he
Nat
iona
l Em
erg
ency
Med
icin
e A
ssoc
iati
on)
PO
BO
X 1
03
9
ED
GE
WO
OD
, M
D 2
1040
-033
9
F2
10516
7578
NS
C M
emb
ersh
ip R
enew
al
RE
-@
D
ocu
me
nt
Siz
e: 8
.875
X 3
.875
" C
olor
s: B
lack
Pri
nts
on #
24
lb W
hite
Wo
ve
1 111' 1
111111
• 1111
1 111 1
•I II I 11
1 • 11
111 1
11 1ItI11
1111
It I• 11
111 11
1 111 I
PLEA
SE
PLA
CE
POST
AG
E ST
AM
P H
ERE
Dia
nn
e 5
.4.1
61
+

+
1757
8 N
SC
Ju
ne
20
16
CR
E_
NE
MA
Lap
sed
Do
no
r B
AE
5/
4/16
5
:20
PM
P
age
2
-+
NSC
FACT
S So
licita
tion
For C
harit
able
Pur
pose
s Ca
rd
ABOL
JT T
HE N
ATIO
NAL
EMER
GENC
Y M
EDIC
INE
ASSO
CIAT
ION
(inco
rpor
ated
in W
ashin
gton
, D.C
.) W
ITH
ITS
spec
ial p
rogr
am N
ATIO
NAL
STRO
KE C
OUNC
IL (N
SC).
NEM
A wi
th it
s sp
ecial
pro
gram
NSC
is a
na
tiona
l hea
lth o
rgan
izatio
n op
erat
ing u
nder
non
-pro
fit ta
x ex
empt
Inte
rnal
Reve
nue
Code
501
(c)(
3).
Thro
ugh
our m
ailin
gs w
e ra
ise th
e m
uch
need
ed fu
nds
for t
he p
reve
ntio
n of
inju
ry a
nd il
lnes
s by
ad
dres
sing
heal
th a
nd s
ocia
l iss
ues
thro
ugh
educ
atio
n, a
pplie
d re
sear
ch,
tech
nolo
gy,
and
equi
pmen
t.
If yo
u wi
sh a
copy
of t
he s
umm
ary
of th
e lat
est f
inanc
ial s
tate
men
t, or
ann
ual r
epor
t, an
d re
gistra
tion
filed
by T
he N
ation
al Em
erge
ncy
Med
icine
Ass
ociat
ion, p
lease
write
to u
s at
P.O
. Box
103
9, E
dgew
ood,
MD
2104
0 (4
43)
922-
7533
. We
will
be p
lease
d to
resp
ond
prom
ptly.
Som
e sta
tes
requ
ire th
at s
pecia
l not
ices
be in
clude
d wi
th e
ach
solic
itatio
n. If
you
are
a re
siden
t of o
ne o
f the
se s
tate
s, yo
u m
ay o
btain
fina
ncial
inf
orm
ation
dire
ctly f
rom
the
state
age
ncy:
FLO
RID
A-A
COPY
OF
THE
OFFI
CIAL
REG
ISTR
ATIO
N AN
D FI
NANC
IAL
INFO
RMAT
ION
MAY
BE O
BTAI
NED
FROM
THE
DIV
ISIO
N OF
CON
SUME
R SE
RVIC
ES B
Y CA
LLIN
G TO
LL
FREE
, 1-8
00-4
35-7
352
(800
-HEL
P-FL
A) W
ITHIN
THE
STA
TE. R
EGIS
TRAT
ION
DOES
NOT
IMPL
Y EN
DORS
EMEN
T, AP
PROV
AL, O
R RE
COMM
ENDA
TION
BY
THE
STAT
E. F
lorida
Reg
istra
tion
#CH3
13. M
ARYL
AND-
For
the
cost
of c
opies
and
pos
tage
, Offic
e of
the
Secr
etar
y of
Stat
e, St
ate
Hous
e, An
napo
lis, M
D 21
401
MISS
ISSI
PPI -
The
offic
ial re
gistra
tion
and
finan
cial i
nfor
mat
ion o
f The
Nat
ional
Emer
genc
y M
edici
ne A
ssoc
iation
m
ay b
e ob
taine
d fro
m th
e M
ississ
ippi S
ecre
tary
of S
tate
's of
fice
by c
alling
1-8
88-2
36-6
167.
Reg
istra
tion
by th
e Se
cret
ary
of S
tate
does
not
imply
end
orse
men
t. NE
W J
ERSE
Y -
INFO
RMAT
ION
FILED
WITH
THE
AT
TORN
EY G
ENER
AL C
ONCE
RNIN
G TH
IS C
HARI
TABL
E SO
LICITA
TION
AND
THE
PERC
ENTA
GE O
F CO
NTRI
BUTIO
NS R
ECEIV
ED B
Y TH
E CH
ARITY
DUR
ING
THE
LAST
REP
ORTIN
G PE
RIOD
THA
T W
ERE
DEDI
CATE
D TO
TH
E CH
ARIT
ABLE
PU
RPOS
E M
AY B
E OB
TAIN
ED
FROM
TH
E AT
TORN
EY
GENE
RAL
OF T
HE S
TATE
OF
NE
W J
ERSE
Y BY
CAL
LING
(973
) 50
4-62
15
AND
IS
AVAI
LABL
E ON
TH
E IN
TERN
ET A
T ww
w.njc
onsu
mer
affa
irs.g
ov/o
cp.h
tm#c
harit
y. RE
GIST
RATIO
N W
ITH T
HE A
TTOR
NEY
GENE
RAL
DOES
NOT
IMPL
Y EN
DORS
EMEN
T. NE
W Y
ORK
-Offic
e of
the
Atto
rney
Gen
eral,
Dep
artm
ent o
f Law
, Cha
rities
Bur
eau,
120
Broa
dway
, New
Yor
k, NY
102
71. N
ORTH
CAR
OLI
NA-F
INAN
CIAL
INFO
RMAT
ION
ABOU
T TH
IS O
RGAN
IZATIO
N AN
D A
COPY
OF
ITS L
ICEN
SE A
RE A
VAILA
BLE
FROM
THE
STA
TE S
OLIC
ITATIO
N LIC
ENSI
NG B
RANC
H AT
1-8
88-8
30-4
989.
THE
LIC
ENSE
IS N
OT A
N EN
DORS
EMEN
T BY
THE
STA
TE. P
ENNS
YLVA
NIA-
The
offic
ial re
gistra
tion
and
finan
cial i
nfor
mat
ion o
f The
Nat
ional
Emer
genc
y M
edici
ne A
ssoc
iation
may
be
obta
ined
from
the
Penn
sylva
nia D
epar
tmen
t of S
tate
by
callin
g to
ll-fre
e, w
ithin
Penn
sylva
nia, 1
-800
-732
-099
9. R
egist
ratio
n do
es n
ot im
ply e
ndor
sem
ent.
VIRG
INIA
-Virg
inia
Stat
e Di
vision
of C
onsu
mer
Affa
irs, D
epar
tmen
t of
Agr
icultu
ral a
nd C
onsu
mer
Ser
vices
, PO
Box
1163
, Rich
mon
d, VA
232
18. W
ASHI
NGTO
N -
Char
ities
Divis
ion, O
ffice
of th
e Se
cret
ary
of S
tate,
Stat
e of
Was
hingt
on, O
lympia
, WA
9850
4-04
22, 1
-800
-332
-448
3.
WES
T VI
RGIN
IA -
Resid
ents
may
obt
ain a
sum
mar
y of
the
regis
tratio
n an
d fin
ancia
l doc
umen
ts fro
m th
e Se
cret
ary
of S
tate,
State
Cap
itol,
Char
lesto
n, W
V 25
305.
Reg
istra
tion
with
any
of t
hese
sta
te a
genc
ies d
oes
not i
mply
end
orse
men
t, ap
prov
al or
reco
mm
enda
tion
by a
ny s
tate.
-+
+

Exhibit F.3
+
1741
1 N
HC
Win
ne
r A
nn O
SE
_W
inn
An
no
un
cem
en
t 1
1/2
5/1
5 2
:06
PM
P
age
1 ---
-$-
AWAR
D N
OTI
CE:
0
PRIZ
E •
111
\O,OO
O~OO
•••
SA
MP
LEP
ER
SO
N
SIG
NA
TU
RE
AN
D R
EP
LY
AR
E R
EQ
UIR
ED
FOR
PR
IZE
RE
LE
AS
E
1115
7411
NE
MA
NH
C W
inn
er
An
no
un
cem
ent
OSE
Doc
umen
t Siz
e: 9
.5 x
4.1
25
C
olor
s: p
ms
18
6 r
ed,
286
blue
and
(bl
ack
is l
aser
ed)
----$
-
----•,-,¢
-----
-·-
1 r-
-::.·.
~:.,;·
:.=·:..
:-.::;
;.::::
::-...:
:-:
r:'=~~ "'~
~~lrt
l\~os
1A&
f I
-r~'.'.-
': ,~
:;, "
¥,
:·
_,;"°"
.~
,,{]
#'
---
•.
~'.-;
,u-«o
lf',
\~"'
0
O ck
=
=
\ ~
4PI
1 ..
"-;:
::
i>3?
c':.
24Q
----·
'
J.
SA
MP
LE
PE
RS
ON
Y
OU
AR
E A
LR
EA
DY
A B
ON
US
P
RIZ
E W
INN
ER
! T
O T
HE
AT
TE
NT
ION
OF
:
JOH
N S
AM
PL
EP
ER
SO
N
NE
WP
OR
T C
RE
AT
IVE
CO
MM
UN
ICA
TIO
NS
21
R
AIL
RO
AD
AV
EN
UE
D
UX
BU
RY
, M
A 0
23
32
I• I 11
I I I I
I I 11 I
11111
I ii 11
1 I I
I I 11 I
11I11
1II11
1111
1111
, 1111
111•1
•'111
Dia
nne
11
.25
.15
+

17411 NHCWlnnerAnn FORM_Layout 1 11/25/15 2:05 PM Page 1 +
John Sampleperson 21 Railroad Avenue Duxbury, MA 02332
JOHN SAMPLEPERSON'S WINNER ANNOUNCEMENT
Attention Mr. Sampleperson;
Yes, this is GOOD NEWS for you, JOHN SAMPLEPERSON! You are in possession ofa WINNING Prize Authorization Number.
Provide me your approval and I will send your GUARANTEED PRIZE to 21 Railroad Avenue in Duxbury, Massachusetts.
To claim your guaranteed bonus prize, sign and detach the Reply Fann below and return it by March 15, 2016.
But, there's even more great news for the Sampleperson household. In a matter of weeks, you have the opportunity for another $10,000.00 and your name may already be on that $10,000.00 check. That's right:
Grand Prize Authorization Number XXX:XX is registered in your name. Should you return the reply fonn below, the number on the reply fonn be the winning Prize Authorization Number, and you return it before the deadline, you would almost immediately receive the $10,000.00 cash. The number one reason why winners lose thousands of dollars every month is that they simply don't reply. ·
By March 15th, provided you have met the qualifications, you'll be the newest member of our Grand Prize Winners' Club. You'll join the others who are enjoying their new found wealth and realizing their financial dreams. Imagine ... a $10,000.00 check made payable to John Sampleperson.
Remember, you are already a confirmed winner and guaranteed to receive any and all prizes to which you are entitled. So, don't wait another minute. Think about it. Don't let time run out on your opportunity for the $10,000.00 Grand Prize. A contribution is not required and will not increase chances to win.
When you send your reply and claim your prize, please send along a gift of $7, $10, or even $5 to join in our effort to fight and win the battle against heart disease. This is your chance to win a major prize ancI help us put an end to needless suffering. Please, your help is desperately needed.
We'll be watching for your reply and stand ready to send you your prize.
P.S. The Reply Fann is below. Return it today and please send alo the battle against heart disease.
small gift to help fight and win
'9' DETACH AT PERFORATION '9' '9' DETACH AT PERFORATION '9'
GRAND PRIZE $10,000.00 CASH SAMPLEPERSON REPLY REQUIRED
RETURN THIS ENTRY FORM BY MIDNIGHT, MARCH 15, 2016
I am enclosing $ ___ to help fight heart disease • $7 • $5 • $1 o • $25
Make check payable to: NATIONAL HEART COUNCIL OR NHC
SIGNATURE
JOHN SAMPLEPERSON
$10,000.00 GRAND PRIZE AUTHORIZATION NUMBER
xxxxx JOHN SAMPLEPERSON 21 RAILROAD AVENUE DUXBURY, MA 02332
xxxxxx 123456789•
A10/11/12
REPL y TOIJA y
1111111111111111111111
If for any reason you will not make a gift, please do not use this reply form. In that case. only, write your name, address and Grand Pnze Authonzat1on Number on a piece of paper, sign 11, and return 11 in the envelope provided. Giving is not required and will not improve chances to win.
1
11157411 NEMA NHC Winner Announcement FORM ~ Document Size: 8.5 x 14" Colors: PMS 100 Yellow, PMS 280 bluEif'\86 red and black lasers

17411 NHC Winner Ann FORM_Layout 1 11/25/15 2:05 PM Page 2
NHC FACTS Solicitation For Charitable Purposes Card:
Your gift is very much appreciated and fully deductible as a charitable contribution. A copy of the summary of the latest financial statement, or annual report, and registration filed by NATIONAL EMERGENCY MEDICINE ASSOCIATION (NEMA), Qncorporated in Washington, O.C.), WITH ITS special program NATIONAL HEART COUNCIL (NHC) may be obtained by contacting us at The National Emergency Medicine Association, P.O. Box 1039, Edgewood, MD 21040 (443) 922-7533. If you are a resident of one of these states, you may obtain financial information directly from the state agency: FLORIDA-A COPY OF THE OFFICIAL REGISTRATION AND FINANCIAL INFORMATION MAY BE OBTAINED FROM THE DIVISION OF CONSUMER SERVICES BY CALLING TOLL-FREE, 1-800-435-7352 (800-HELP-FLA) WITHIN THE STATE. REGISTRATION DOES NOT IMPLY ENDORSEMENT, APPROVAL, OR RECOMMENDATION BY THE STATE. Florida Registration //CH313. GEORGIA-A full and fair description of the programs of NEMA and our financial statement summary is available upon request at the office and phone number indicated above. Maryland - For the cost of copies and postage, Office of the Secretary of State, State House, Annapolis, MD 21401. MISSISSIPPI - The official registration and financial information of NEMA may be obtained from the Mississippi Secretary of State's office by calling 1-888-236-6167. Registration by the Secretary of State does not imply endorsement. NEW JERSEY - INFORMATION FILED WITH THE ATTORNEY GENERAL CONCERNING THIS CHARITABLE SOLICITATION AND THE PERCENTAGE OF CONTRIBUTIONS RECEIVED BY THE CHARITY DURING THE LAST REPORTING PERIOD THAT WERE DEDICATED TO THE CHARITABLE PURPOSE MAY BE OBTAINED FROM THE ATTORNEY GENERAL OF THE STATE OF NEW JERSEY BY CALLING (973) 504-6215 AND IS AVAILABLE ON THE INTERNET AT http://www.state.nj.us/lps/ca/charlrm.htm. REGISTRATION WITH THE ATTORNEY GENERAL DOES NOT IMPLY ENDORSEMENT. NEW YORK - Office of the Attorney General, Department of Law, Charities Bureau, 120 Broadway, New York, NY 10271. North Carolina - FINANCIAL INFORMATION ABOUT THIS ORGANIZATION AND A COPY OF ITS LICENSE ARE AVAILABLE FROM THE STATE SOLICITATION LICENSING BRANCH AT 1-888-830-4989. THE LICENSE IS NOT AN ENDORSEMENT BY THE STATE. PENNSYLVANIA- The official registration and financial information of NEMA may be obtained from the Pennsylvania Department of State by calling toll-free, within Pennsylvania, 1-800-732-0999. Registration does not imply endorsement. VIRGINIA-Virginia Slate Division of Consumer Affairs, Department of Agricultural and Consumer Services, PO Box 1163, Richmond, VA 23218. WASHINGTON - Charities Di~sion, Office of the Secretary of State, State of Washington, Olympia, WA 98504-0422, 1-800-332-4483. WEST VIRGINIA - Residents may obtain a summary of the registration and financial documents from the Secretary of State, State Capitol, Charleston, WV 25305. Registration with any of these state agencies does not imply endorsement, approval or recommendation by any state.
SWEEPSTAKES FOR $10,000.00 GRAND PRIZE OFFICIAL RULES
NO CONTRIBUTION IS REQUIRED * CONTRIBUTION WILL NOT 11\IPROVE CHANCES OF WINNING
! . Sponsor - this sweepstakes is sponsored by Nutionnl Hearl Council, (a program of the Nation<-1\ Emergency Medicine Associution.) Phone: 443-922-7533 Address: P.O. Box 1039, Edgewood, MD 21040.
2. Prizes- there are these three Prizes: 1) Grund Prize of $101000,001 2) Guar:u1tel•d Prize Is 11 Colorful 2016 Culendar 3) A Bonus Prize of $100,00. Prizes arc non-transfernble and there are no substitutes.
3. Entry Instructions: - to enter with n donation, return the reply form in the enclosed en\'elope postage pre-pnid postmarked before lhe entry deadline. To enter without a donation, follow directions on the reply form.
4, Prize Selection Process - I) Grand Prize: the winning entry wns randomly selected by an independent ngency whose decision was final and binding before the promotion letters were mailed and were randomly seeded among mailed letters. If your eligible entry matches the pre-selected number, you will be notified that you have won the Grnnd Prize, 2) Guaranteed Prize: all entries will receive the guaranteed merchandise prize, 3) Bonus Prize: The winning entry will be randomly selected from all eligible entries received by the deadline date. The agency's decisions arc linal and binding,
5. \Vho is eligible - the sweepstakes is open to residenls (18 years or older) of the United States and its possessions who receive the mailing. Employees, agents, vendors and staffol'the Sponsor, National Heart Council {a program of the National Emergency Medicine Association.) Address: P.O. Box 1039, Edgewood, MD 21040, its advertising and promotional agencies, and sweepstakes administrator (and their household members) are not eligible to win. The entry form will not be honored if not mailed in the enclosed envelope with sufficient postage by the e1ury deadline.
6, Entry Deadline: - the deadline for mailing your entry is March 15, 2016. Postmark determines date of entry,
7. General - Sweepstakes void where prohibited by law. All tederal, state and local regulations apply, Winners will be notified by mnil. By participating, entrants agree to be bound by these rules, Failure to comply with these or any other Official Rules will result in disqualification, Winner must sign and return un affiduvit of eligibility, a liability release, and except where prohibited by !aw, a publicity release within IO days of issuance of notilication. If winner docs not comply with the foregoing, or il'a prize or ptize notification is unde\ivernble, nnd/or ifa selected winner does not comply with any portion of these Onicial Rules, $Ucl1 winner will be disqualified und, in the case of the Bonus Prize only, an alternate winner will be selected. Entrants agree thut: I) Sponsor shal! have nght and permission to use (if a winner) entrant's name and city of residence for advertising, trade and/or other purposes in perpetuity without further compensation (unless prohibited by law); and 2) Sponsor, its advertising and promotion agencies tind each of their respective officers, directors, employees, representatives and agents sha11 have no liability and will be held harmless by entrants for ai,y liability, loss, injury or damage to entrants or any other person or entity relating to this sweepstakes. Taxes sole responsibility of winner. Sponsor and its agencies arc not responsible for lute, lost, or misdirected mail or any printing or technical errors or malfunctions of any kind, by any human error Lhat may occur in the processing of the entries in this Sweepstakes. ff for any reason that corrupts or affects the administration, security, fairness, integrity, or proper conduct of this Sweepstakes so that il is not capable of being conducted as described in these 111lcs. Sponsor shall have the 1'ight, at its so!e discretion, to cancel, terminate, modit)' or suspend the Sweepstakes. Any person who supplies false information, enters by fraudulent means, or is othenvise detcnnined to be in violation of these rules in an attempt to obtain any prize will forfeit any prize won. No gift or payment of any kind ncccssmy to enter or win. Entries become the prope1ty of the Sponsor and will not be retumed.
8. Winners - for the name of the Grand Prize winner, send a sclf~addresscd stamped envelope 10 National Heart Council. Address: P.O. Box 1039, Edgewood. MD 21040 on or within 60 days at\cr the entry deadline date,
9. Odds of Winning - l) Grand Prize: the number of entry limns mailed determines the odds of winning. Your odds of winning will be no greater than ! in X,XXX,XXX. 2) Guaranteed Prize: Odds that you will win the Guaranteed Prize arc I in 1. Your odds of winning the bonus prize arc dependent upon the number of qualifying entries received.
I 0, Creative Presentations - this sweepstakes may be mailed by NEMA with different creative presentations. The pre~se!ected winning Grand Prize number has been selected from all etttry numbers for a\1 creative presentations, and the winning Bonus Prize number has been selected from ull entries received for all creative presentations.
11. Malling List Suppressions Ir you do not wish to receive mailings of this type in the future please write to: National Heart Council. Addrem P.O. Box 1039, Edgewood1 MD 21040, Because winners are selected in advance and sweepstakes entries are printed In advance, It will take Six to Eight weeks before you stop receiving mail,
! 2. For additional information about this sweepstakes or sweepstakes in general, visit www.swccpstakcsconsumerguidc.net.
WINNER ANNOUNCEMENT AND GRAND PRIZE ENTRY ! J,
I $10,000.00 I

17411 NHC Win+INSERT_Layoui 1 11/25/15 1 :2
ODDS THAT YOU WILL WIN THE GUARANTEED PRIZE ARE 1 IN 1
FOR ELIGIBLE ENTRIES RECEIVED. YOU HAVE NOT YET WON THE GRAND PRIZE. ENTRY IS FREE.
DONATING WILL NOT INCREASE YOUR CHANCES OF WINNING. YOU MAY OR MAY NOT HAVE A NUMBER THAT IS THE WINNING NUMBER. ODDS THAT YOU WILL
WIN THE GRAND PRIZE OF $10,000.00 WILL BE NO GREATER THAN ONE IN X,XXX,XXX. ODDS
THAT YOU WILL WIN THE CONSOLATION PRIZE OF $100
ARE BASED UPON THE NUMBER OF ELIGIBLE ENTRIES RECEIVED.
NHC01/16
1
11157411 NEM.,A NHC Winner l Announce~ 2x3 Insert Dianne 6.6.14 Colors: bl ck

17411 NHC Win+INSERT_Layoui 1 11/25/15 1 :2
..J
0 z ::)
0 0 r-
~ + ..J <( z 0
~ z
+
1741
1 N
HC
Win
ner
Ann
RE
_Lay
out1
11
/25/
15
1:25
PM
P
age
1
FROM
__
__
__
__
_
Att
n:
Sw
ee
psta
ke
s
Ad
min
istr
ati
on
A 1
0/11
/12
1
1115
7411
NE
MA
NH
C W
inn
er A
nn
ou
nce
men
t R
E
Do
cum
en
t S
ize:
3.
875
x 8.
875
Col
ors:
bla
ck
--@
-
GU
AR
AN
TE
ED
AN
D $
10
,00
0.0
0
WIN
NE
R P
RO
CE
SS
ING
A
ND
GR
AN
D P
RIZ
E E
NT
RY
N
atio
nal
He
art
Co
un
cil
(a p
rogr
am o
f the
Nat
iona
l E
mer
genc
y M
edic
ine
Ass
ocia
tion
)
PO
BO
X 2
0626
S
T.
LOU
IS,
MO
6
31
39
-06
26
I 1111n
h1I11
h111 1
1 •11111 1
1 11111 1
h III I
h1•11
III11
11111 '1•1
111' 1
--@
-
PLEA
SE
PLAC
E PO
STAG
E HE
RE
Dia
nn
e 1
1.25
.1 I +

Exhibit F.4
NA
C A
WA
RD
NO
TIF
ICA
TIO
N
$10,
425.
76 T
RA
NS
FE
R A
UT
HO
RIZ
AT
ION
EN
CL
OS
ED
*
**
R
ESP
ON
SE
RE
QU
IRE
D*
**
D
EA
DL
INE
S
TR
ICT
LY
E
NF
OR
CE
D**
*
FOR:
JO
HN
Q.
SAM
PLEP
ERSO
N
AD
DR
ESS
AD
DR
ESS
AD
DR
ESS
AD
DR
ESS
6~
){.)
{.){
.){.
){.)
{.)L
){. I
.W
~ V
L ~
c{J i:
k
i2 {;
IO14
Z57
G, .w
~~
0~
cdi-~~
r----------------------------------------------
--,
I : M
OVE
TH
IS L
ABEL
TO
T
rans
ier
Pro
cess
Aut
hori
zatio
n T
o:
-:
: EN
CLOS
ED T
RANS
FER
J.
SA
MP
LEP
ER
SO
N
: :
E!\iT
RYAU
THO
RIZA
TiO
N C
ITY
XX
XX
XX
XX
XX
,~
~ :
I I
: RE
PLY
BEFO
RE
DEA
DLI
NE:
•
' ;
: I
D-,,
, .. ~
I
: 17
/1.,5
/1,,o
l&
·· ·
: ~
----
----
----
----
----
----
----
----
----
----
----
----
----
-~
1111
5741
8 N
AC
No
tific
atio
n O
SE
F
lat siz
e=
11
x 4
.75
" C
olo
rs=
Bla
ck,
PM
S 1
805U
, La
ser
Var
iabl
e

Tra
nsfe
r P
roce
ss A
utho
riza
tion
To:
· ·
--
""""""
' - -=
(c)J
r<
11
15
7 41
8 N
AG
No
tifi
cati
on
I
Fla
t siz
e=
2 x
1"
Co
lors
= B
lack
, P
MS
29
9C

G'" il!IR0.,
J. SAMPLEPERSON
$10,425.76 & "'• D "• We could soon transfer $ 1 0 , 4 2 5 • 7 6 in Grand Prize cash to:
xxxxxxxxxxxx JOHN Q, SAMPLEPERSON
1111111111111111 m 1~ 11111111111111111111 However. we MUST receive your Transfer Entry Authorization before the deadline.
John Q. Sampleperson
THE WINNER HAS BEEN IDENTIFIJRD/ ,, ,-•.•--
GUARANTEED RECIPIENT OF TRANSFER ENTRY AUTHORIZATION FOR GRAND PRIZE IN THE TOTAi. Ai:10UNT OF:
CONFIRMATION We are thrilled to advise you that we have identified the Grand Prize winner. Most OF PRIZE importantly, the eligibility of Prize ID XXXXXXXXXXXX -- SOLELY OWNED BY JOHN
TRANSFER AMOUNT: Q. SAMPLEPERSON -- is 100% CONFIRMED for the maximum Grand Prize in the amount of ****$10.425.76 ****.
Not only are we ready to transfer the full $10,425.76 Grand Prize to the winner ... but should you complete and return the form below as directed by the March 25, 2016 deadline, and Prize ID XXXXXXXXXXXX matches the pre-selected winning number ... a courier would deliver the $10,425.76 check directly to [Addressxxxxxxxxxxxxxxxxxxxxxxx],
And it gets even better Mr. Sampleperson! We are scheduled to award this $10,425.76 prize in just a couple weeks! In fact, you could have an extra $10,425.76 in your [Cityxxxxxxxxxxx] area bank by April 15th! Imagine how great that would be!
PRIZE TRANSFER Take action now by transferring your Transfer Process Label from the envelope to the form ENTRY PR09l;:PllREs.\,,,::•;,. below. Complete the entire form and mail in the enclosed envelope by 3/25/2016.
Remove Transfer label from outer envelope and affix below. Mall in reply envelope provided.
' Mr. Sampleperson, we also request your formal participation by enclosing a tax-deductible gift to help end the tragedy of Alzheimer's Disease. A donation is not required and will 1101 increase your chances ofwi1111i11g. But your gift of just MRCI, or MRC2 will bring hope and happiness to many families struggling with this disease ... even right there in <ST>.
Mr. Sampleperson, we cannot even begin to process your $10,425.76 Transfer Entry Authorization unless we receive your completed form by March 25th. I've seen thousands of dollars slip away from people like you simply because they failed to respond. Don't be one of them. Reply now.
ti#~. ____ ~;t~~\ ~~7
~}]rnw,s __ _ GRAND PRizi1f~XXXXXXXXX -/::t:1
] JOHN Q, SAMPLEPERSON r-------------------1 } TRANSFER ENTRY AUTHORIZATION I I I I I AFFIX YOUR LABEL I I I
HERE : DEADLINE: 17/1-? /?.-olw I I
Issued Exclusively To:
JOHN Q. SAMPLEPERSON
Confirmed Delivery Address:
ADDRESS ADDRESS ADDRESS ADDRESS
J,
PLEASE COMPLETE THIS ENTIRE SECTION
0 YES •· By affixing my Label at left and signing below, I hereby confirm my eligibility to accept and authorize the $10,425.76 Prize Transfer per regulations.
0 YES, I want to help people in [ST] fight Alzheimer's. I have enclosed my one-time donation (pa able to NAC or National Alzheimer's Council):
0 $X.XX
A gift is not required and will not Increase your chances of winning.
0 Other$____ \
w·Jl 4 <;o, ~-
xxxxxxxxxx xxxxx
111157418 NAG Notification Form Flat size= 8.5 x 14"
Letter colors= Black, PMS 1805U, Laser Variable

17418 NAC Notification BackerOnly_Layout 1 12/1/15 5:56 PM Page 1
SWEEPSTAKES FOR $10,425.76 GRAND PRIZE OFFICIAL RULES
NO CONTRIBUTION IS REQUIRED* CONTRIBUTION WILL NOT IMPROVE CHANCES OF WINNING I. ~ - !his sweepstakes is sponsored by National Alzheimer's Council (a program of the National Emergency Medicine Association,) Phone: 443-922-7533
Address: P.O. Box 1039, Edgewood, MD 21040.
2. Prizes - there are these two Prizes: I) Grund Prize of $10,425.761 2) A Bonus Prize of S 100.00, Prizes al'e non-transferable and there are no substitutes.
3, Entry Instructions: - to enter with or without donating, return the n!ply rorm in the enclosed cn\'clopc postage prc-p<1id postmarkl!d before !he entry deadline.
4. Prize Selection Process I) Grand Prize: the winning entry was randomly selected by an 111dependent agency whose decision wns final and binding before the promotion letters were mailed and were randomly seeded among mailed letters, If your eligible entry matches the pre•selected number, you will be notified that you have won the Grand Prize. 2) Bonus Prize; The winning entry will be randomly selected from all eligible entries received by the deadline date, The agency's decisions are final and binding.
5, Who is eligible the sweepstakes is open to residents (18 years or older) of the United States and its possessions who receive the maili11g. Employi.!es, agents, vendors and staff of the Sponsor, National Alzheimer's Council (a program of the National Emergency Medicine Association.) Address: P.O. Box I 039, Edgewood, MD 21040, its advertising and promotional agencies, and sweepstakes administrator (and their household members) are not eligible to win. The entry fonn will no! be honored if not mailed in the enclosed envelope with sufficient postage by the entry deadline.
6. Entry Deadline: - the deadline for muiling your entry is Murch 25, 2016, Postmark determines date or entry,
7. General - Sweepstakes void where prohibited by law. All federal. state and local regulations apply. Winners will be notified by mail. By participating, entrants agree to be bound by these rules. Failure to comply with these or any other Official Rules will result in disqualification. Winner must sign and return un aftidavit of eligibility, a liability release, and except where prohibited by law, a publicity release within 10 days of issuance ofnotifieation. If winner does not comply with the fon:going, or if u prize or prize notification is u11dclivcrub!e, and/or if a selected winner does not comply with any portion of these Official Ru!es, such winner wi!! be disqualified and, in the case of the Bonus Prize only, an alternate witmer will be selected. Entrants agree that: I) Sponsor shall have right am! permission to use (ifa winner) entrant's name and city of residence for advertising, trade and/or other purposes in perpetuity without further compensation (unless prohibited by law); and 2) Sponsor, its advertising and promotion agencies and each of their respective ofiicers, directors, employees, representatives and agents shall have no liability and will be held harmless by entrants for u11y liubility, loss, injury or damage to entrants or any other person or entity relating to this sweepstakes. Tuxes sole responsibility of winner. Sponsor and its age11cies are not responsible for late, lost, or misdirected mail or any printing or technical crnm or nrnlfu11ctim1s of any kind, by any human error that may occur in the processing of the entries in this Sweepstakes, If for any reason that corrupts or affects the udmi11istrat1011, security, fairness, integrity, or proper conduct of this Sweepstakes so that it is not capable of being conducted us described in these rules, Sponsor shall have the right, at its sole discretion, to cuncel, tem1inute, modify or suspend the Sweepstakes. Any person who supplies fnlse information, enters by fraudulent means, or is otherwise determined to be in viQlation of these rn!es in an attempt to obt.1i11 any prize will forfeit nny prize won, Entries become the property of the Sponsor and will nol be returned.
8. Winners- for the name of the Grand Prize winner, send a self-addressed stamped envelope to National Alzheimer's Council. Address: P.O. Box 1039, Edgewood, MD 21040 on or within 60 days a(\er the entry deadline date.
9, Odds of Winning ! ) Grund Prize: the number of entry forms mailed determines the odds of winning. Your odds of winning will be no greater than I in X,XXX,XXX. 2) Your odds of winning the Bonus Prize are dependent upon the number of qualifying entries received.
10. Creative Presentations- this sweepstakes may be mailed by NEMA with different creative presentations. The pre-selected winning Grand Prize number has been selected from all entry numbers for all creative presentations, and the winning Bonus Prize number has been selected from al! entries received for all creative presentations.
11. !Vlolliru• List Suppressions - if you do not wish to receive mailings of this type in the future please write to: National Alzhcimcr)s Council. Address: P.O. Box 1039, Edgewood, ~•ID 21040. Because winners arc selected in advance and sweepstakes entries arc printed In advnnce, it will tnk(.' Six to Eight weeks before you stop 1·ccciving mall.
12. For additional information about this sweepstakes or sweepstakes ln general, visit www.sweepstakesconsumerguidc.net
What is Alzheimer disease? Alzheimer disease, or Alzheimer's as it is also referred to, is the leading cause of dementia. Named after the person who first described it, Alzheimer disease may be defined as a set of symptoms that include loss of memory, judgement, reasoning ability, and often changes in behavior. With the aging of the "baby boomers" the incidence of Alzheimer's is expected to more than triple by the middle of the 21st century. At the present time, Alzheimer's cannot be stopped or cured. Research, however, is resulting in greater understanding of the disease and identification of steps that may reduce your risk of experiencing Alzheimer's.
How is Alzheimer disease dfrtgnosed? There are several warning signs that you can look for that may indicate Alzheimer disease. These include memory losses that affect someone's ability to function, such as forgetting where you are or how to get to a familiar place, difficulty performing familiar tasks, problems with language, disorientation of time and place, poor or decreased judgement, problems with abstract thinking, misplacing or losing things, changes in mood or behavior, changes in personality, or loss of initiative.
Just one of these signs doesn't mean someone has the disease; usually several of them are present and changes are progressive.
If you or someone you know suspects Alzheimer disease, tests to make the diagnosis may include a complete medical history, a mental status exam, a physical exam, laboratory tests and psychological or psychiatric evaluations. Getting a diagnosis and getting it early will help the affected person and their family make plans for the future.
There are other conditions and diseases that can produce dementia. These include thyroid disease, depression, infections, drug interactions, alcohol abuse, or simply not enough to eat or drink. That's why it is very important to see your doctor if you suspect Alzheimer disease. Many of the other conditions can be treated and the dementia cleared up before pennanent damage is done.
How Your Support of NAC Could Help Someone You Love ... The National Alzheimer's Council is an outreach of the National Emergency Medicine Association, a 50l(c)(3) nonprofit organization founded in 1982. Our Mission is the prevention of injury and illness by addressing health and social issues through education, applied research, technology, and equipment. "Prevention through Education" is the overall theme of our efforts, and we have become known for our educational health-related materials, which are free to schools, hospitals, health centers, and a wide array of social service programs.
For example, the information above was taken from the pocket book, "Alzheimer's - Hope Through Education" which was written and produced by the National Alzheimer's Council. It explains Alzheimer's, what we know today and what steps research suggests that we might take today to reduce the risk of Alzheimer's. If you or someone you love is concerned about Alzheimer's, we encourage you to contact the National Alzheimer's Council today.
11157418 NAC Notification Backer Only 8.5 x 14" Colors: Black

17418 NAC Notif+NSERT_Layoutl1 12/1/15 5:56
CONSUMER DISCLOSURES YOU HAVE NOT YET WON THE GRAND PRIZE. ENTRY IS FREE. DONATING WILL NOT INCREASE YOUR CHANCES OF WINNING. YOU MAY OR MAY NOT HAVE A
+ NUMBER THAT IS THE WINNING
+ NUMBER. ODDS THAT YOU WILL WIN THE GRAND PRIZE OF $10,425.76 WILL BE NO GREATER THAN x,xxx,xxx. ODDS THAT YOU WILL WIN THE BONUS PRIZE DEPEND ON THE NUMBER OF ELIGIBLE REPLIES RECEIVED.
A13/14/15
INSERT SIZE: 2 X · ORS- Black 111157418 NAC ~ation

17418 NAG Notif~NSERT_Layoutl1 12/1/15 5:56
_.J
0 z ::)
0 0 Cf)
a: w ~ w I ~ <t: _.J
<t: z 0
~ z
FIR
ST
, L
AS
T N
AM
E
AD
DR
ES
S
CIT
Y,
ST
AT
E,
ZIP
$1
0,4
25
.76
TR
AN
SF
ER
EN
TR
Y
AU
TH
OR
IZA
TIO
N E
NC
LO
SE
D
ID
PR
-5
$1
0,4
25
.76
-
AM
OU
NT
CO
NFI
RM
ED
T
RA
NSF
ER
TO
W
INN
ER
-
APP
RO
VE
D
Pro
cess
ing
Req
uir
emen
ts:
~--'----------1
1-.L
-l---L
)
A13
/14/
15
3/25
}~
11
15
7 4
18
NA
C N
otif
ica
tion
RE
Fla
t si
ze =
8.8
75
x 3
.87
5"
Co
lors
= B
lack
, P
MS
18
05
U
1111
1111
1111
1111
1!111
1111
1111
1111
1111
1111
1111
1111
1111
111
10
K0
32
52
01
6
TRA
CK
ED
MA
TTE
R.
DO
NO
T TA
MP
ER
.
TR
AN
SF
ER
EN
TR
Y P
RO
CE
SS
ING
N
AG
P
O B
OX
18
18
M
ER
RIF
IELD
VA
22
11
6-8
01
8
1lll•
l••l1
l11l
11l•l
1l•ll
ll•ll1
1l11
1llll
11lll
l1•1
•l••ll
l11l
ll11l
ll
PLA
CE
ST
AM
P
HE
RE

+
1741
8 N
AC
Not
ifica
tion
RE
Bac
ker_
Layo
ut 1
12
/1/1
5 5:
57 P
M
Pag
e 1
---+-
NA
C F
AC
TS
Solic
itatio
n F
or C
hari
tabl
e P
urpo
ses
Car
d:
You
r gi
ft i
s ve
ry m
uch
appr
ecia
ted
and
fully
ded
ucti
ble
as a
cha
rita
ble
cont
ribu
tion
. A
cop
y o
f the
sum
mar
y o
f the
lat
est
fina
ncia
l st
atem
ent,
or a
nnua
l re
port
, an
d re
gist
rati
on f
iled
by N
AT
ION
AL
E
ME
RG
EN
CY
ME
DIC
INE
AS
SO
CIA
TIO
N (
NE
MA
), (
inco
rpor
ated
in
Was
hing
ton,
D.C
.),
wit
h its
spe
cial
pro
gram
Nat
iona
l Alz
heim
er's
Cou
ncil
(N
AC
) m
ay b
e ob
tain
ed b
y co
ntac
ting
us
at T
he
Nat
iona
l E
mer
genc
y M
edic
ine
Ass
ocia
tion
, P.
O.
Box
I 0
39,
Edg
ewoo
d, M
D 2
1040
(44
3) 9
22-7
533.
If
you
are
a re
side
nt o
f on
e o
f the
se s
tate
s, y
ou m
ay o
btai
n fi
nanc
ial
info
rmat
ion
dire
ctly
fro
m
the
stat
e ag
ency
: F
LO
RID
A-A
CO
PY
OF
TH
E O
FF
ICIA
L R
EG
IST
RA
TIO
N A
ND
FIN
AN
CIA
L I
NFO
RM
AT
ION
MA
Y B
E O
BT
AIN
ED
FR
OM
TH
E D
IVIS
ION
OF
CO
NS
UM
ER
SE
RV
ICE
S B
Y C
AL
LIN
G T
OL
L-F
RE
E,
1-80
0-43
5-73
52 (
800-
HE
LP
-FL
A)
WIT
HIN
TH
E S
TA
TE
. R
EG
IST
RA
TIO
N D
OE
S N
OT
IM
PLY
EN
DO
RS
EM
EN
T, A
PPR
OV
AL
, O
R R
EC
OM
ME
ND
AT
ION
BY
T
HE
ST
AT
E. F
lori
da R
egis
trat
ion
#CH
3 l 3
. G
EO
RG
IA-A
full
and
fair
des
crip
tion
of t
he p
rogr
ams
ofN
EM
A a
nd o
ur fi
nanc
ial
stat
emen
t sum
mar
y is
ava
ilab
le u
pon
requ
est
at th
e of
fice
and
pho
ne
num
ber
indi
cate
d ab
ove.
Mar
yla
nd
-F
or th
e co
st o
f cop
ies
and
post
age,
Off
ice
of t
he S
ecre
tary
of S
tate
, Sta
te H
ouse
, Ann
apol
is,
MD
214
01.
MIS
SIS
SIP
PI
-T
he o
ffic
ial
regi
stra
tion
and
fin
anci
al
info
m1a
tion
ofN
EM
A m
ay b
e ob
tain
ed fr
om t
he M
issi
ssip
pi S
ecre
tary
of S
tate
's o
ffic
e by
cal
ling
1-8
88-2
36-6
167.
Reg
istr
atio
n by
the
Sec
reta
ry o
f Sta
te d
oes
not i
mpl
y en
dors
emen
t. N
EW
JE
RS
EY
-
INFO
RM
AT
ION
FIL
ED
WIT
H T
HE
AT
TO
RN
EY
GE
NE
RA
L C
ON
CE
RN
ING
TH
IS C
HA
RIT
AB
LE
SO
LIC
ITA
TIO
N A
ND
TH
E P
ER
CE
NT
AG
E O
F C
ON
TR
IBU
TIO
NS
RE
CE
IVE
D B
Y T
HE
C
HA
RIT
Y D
UR
ING
TH
E L
AS
T R
EP
OR
TIN
G P
ER
IOD
TH
AT
WE
RE
DE
DIC
AT
ED
TO
TH
E C
HA
RIT
AB
LE
PU
RP
OS
E M
AY
BE
OB
TA
INE
D F
RO
M T
HE
AT
TO
RN
EY
GE
NE
RA
L O
F T
HE
ST
AT
E O
F N
EW
JE
RS
EY
BY
CA
LL
ING
(97
3) 5
04-6
215
AN
D I
S A
VA
ILA
BL
E O
N T
HE
IN
TE
RN
ET
AT
http
://w
ww
.sta
te.n
j.us/
lps/
ca/c
harf
rm.h
trn.
R
EG
IST
RA
TIO
N W
ITH
TH
E A
TT
OR
NE
Y
GE
NE
RA
L D
OE
S N
OT
IMPL
Y E
ND
OR
SEM
EN
T.
NE
W Y
OR
K-
Off
ice
of t
he A
ttor
ney
Gen
eral
, D
epar
tmen
t o
f Law
, C
hari
ties
Bur
eau,
120
Bro
adw
ay,
New
Yor
k, N
Y 1
0271
. N
orth
Car
oli
na
FIN
AN
CIA
L IN
FOR
MA
TIO
N A
BO
UT
TH
IS O
RG
AN
IZA
TIO
N A
ND
A C
OP
Y O
F IT
S L
ICE
NS
E A
RE
AV
AIL
AB
LE
FR
OM
TH
E S
TA
TE
SO
LIC
ITA
TIO
N L
ICE
NS
ING
BR
AN
CH
AT
l-88
8-83
0-49
89.
TH
E L
ICE
NS
E I
S N
OT
AN
EN
DO
RS
EM
EN
T B
Y T
HE
ST
AT
E.
PE
NN
SY
LV
AN
IA-
The
off
icia
l re
gist
rati
on a
nd f
inan
cial
inf
orm
atio
n o
fNE
MA
may
be
obta
ined
fro
m t
he P
enns
ylva
nia
Dep
artm
ent
of S
tate
by
call
ing
toll
-fre
e, w
ithi
n P
enns
ylva
nia,
1-8
00-7
32-0
999.
Reg
istr
atio
n do
es n
ot i
mpl
y en
dors
emen
t. V
IRG
INIA
-Vir
gini
a S
tate
Div
isio
n o
f Con
sum
er A
ffai
rs,
Dep
artm
ent
of
Agr
icul
tura
l an
d C
onsu
mer
Ser
vice
s, P
O B
ox l
I 63
, R
ichm
ond,
VA
232
18.
WA
SHIN
GT
ON
-C
hari
ties
Div
isio
n, O
ffic
e o
f the
Sec
reta
ry o
f Sta
te,
Sta
te o
f Was
hing
ton,
Oly
mpi
a, W
A 9
8504
-042
2,
l-80
0-33
2-44
83.
WE
ST
VIR
GIN
IA-R
esid
ents
may
obt
ain
a su
mm
ary
of t
he r
egis
trat
ion
and
fina
ncia
l do
cum
ents
fro
m t
he S
ecre
tary
of
Stat
e, S
tate
Cap
itol
, C
harl
esto
n, W
V 2
5305
. R
egis
trat
ion
wit
h an
y o
f the
se s
tate
age
ncie
s do
es n
ot i
mpl
y en
dors
emen
t, ap
prov
al o
r re
com
men
dati
on b
y an
y st
ate.
1115
7418
NA
C N
oti
fica
tio
n
RE
bac
ker
OS
E
Do
cum
en
t S
ize:
8.8
75
x 3
.875
C
olor
s: b
lack
---
+-D
ian
ne
12.
1.15
+

Exhibit F.5

CH
EC
K A
UT
HO
RIZ
AT
ION
EN
CL
OS
ED
A
UT
HO
RIZ
AT
ION
IS
SU
ED
ON
RE
CO
RD
AS
BE
ING
SE
NT
TO
YO
U
PLE
AS
E C
ON
FIR
M A
LL
INF
OR
MA
TIO
N E
NC
LOS
ED
IS
CU
RR
EN
T A
ND
CO
RR
EC
T
OP
EN
AT
ON
CE
PE
RS
ON
AL
AN
D C
ON
FID
EN
TIA
L
1101
6777
1 NA
G C
heck
Aut
horiz
atio
n Si
ze =
#10
9.5
X 4
.125
PR
INT
colo
rs =
BLA
CK, P
MS
485
non
prin
t WIN
DO
W D
IE C
UT :
mag
enta
Rec
orde
d "
~ {°
'-11
Dci
'.J O
L
J;t 9
,),;g
~ lB
y f-!:'1
1'..!-'-
t1U

NATIONAL ALZHEIMER'S COUNCIL AUTHORIZATION NOTE OFFICIAL CHECK AUTHORIZATION ENTRY VOUCHER
41-0108 ~
w •31718
DATE- Dec, 1 4 , 2 D 16 NAME:
NUMBER
SampleName
#123 45A
PRIZEAMOUNT: $9,&73.97 ~•1111\rWm= ~,8731~ OATEOF ISSUE: 12 / 1 4 / 17
TOTAL AMOUNT TO BE AWARDED
NINE THOUSAND EIGHT HUNDRED SEVENTY THREE AND 97/100 DOLLARS TO SELECTED WINNER***
AUTHORIZED TO ACCOUNT:
John Q, Sampleperson Address
PENDING YS VOID AFTER 60 DA
TO SELECTED WINNER Address
Bar Code
AlffHORIZED SIGNATURE
Exciting News Mr. Samplenamel
A check has been authorized for payment of 9 873.97 for rize award. The winning lv~)/'number has been selected and I'm appy to tell you your name came up as a match during
/if< our winning number selection process as owner of Check Authorization Number 12345AI
Mr. Samplename, you have been selected for a Check Authorization Number ~that may very well have been selected as the winner. We would be fuify committed to overnighting the authorized check of $9,873.97 for delivery to 123 Anystreet provided you have been issued the winning number and reply by the February 25, 2017 deadline.
frvthoi,-;ud Urgent To Act Now Mr. Samplename To Confirm Your Check Authorization Number 12345A
Your possession of Check Authorization Number 12345A could win you this Grand Prize. In fact, you made it past thousands who were eliminated and never issued a number. But we could not disburse this check to you unless your Check Authorization Number is returned on time. Don't miss out or risk being late returning your Check Authorization Number as follows - a lot of money is on the line.
A Complete the Check Authorization Number Form below for the $9,873.97 Grand Prize Check. This check has been authorized for payment to the winner.
2) Thank you for your previous donation to NAC. Mr. Samplename, we hope you will continue to support our fight to end the tragedy of Alzheimer's Disease. A gift is not required and won't increase your
),/,1,J,/,J.f--~chances of winning, but your donation will bring hope to families lJ2i;11' If struggling with the disease and help fund vital research to find a
J,;J.5;rJ, cure.
L13/14/15
RISK OF FORFEITURE WARNING: If you have the winning Authorization Number and fail to return it on time, you will forfeit any and all prize monies due you. Don't let that happen -- if you return the winning form today, the $9,873.97 check will be on its way to you right away! So return your Check Authorization Form before the 2/25/17 deadline.
'f DETACH AMO RETURl'I UEFOlff DEADLINE 'f
Detach and return before deadline
Issued lo:
Mr. John Sampleperson Date of Issue
12/14/15 Check authorization number:
12345A Return before:
2/25/17
© (s\\]J
AUTHORIZED Mr. John Sampleperson ADDRESS: Sample Name, 12 3 Anystreet,
NY 12345-0000
MEMO:
A $9,873.97 check would be authorized and delivered to John Samplename immediately upon having met requirements for winning and replying by the 2/25/17 deadline.
MAIL IMMEDIATELY RETURN THIS~ TO ARRIVE BY~
1234567890 123456
A GIFT IS NOT REQUIRED ANO WILL NOT INCREASE OIJOS OF WINNING
10167771 NAG Check Authorization Form Size= 8.5 x 14 Letter colors= Black, PMS 485 RED, PMS 2935, Laser Variable-non-print personalization color: magenta
PRIZE CHECK AMT AUTHORIZED:
I wish to support the fight against Alzheimer's disease.
Enclosed is my tax-deductible gift of:
• $7 • $10 • $25 D $5 D $50 D Other ____ _
n~~e,7,~~[,~~:;~ fo~X.ad~1~0\~;,~~~1~[0~:.ti~1~i;o~)Z,~~ie~,~~~s~~uncil Check Authorization# and print "NAG Dec. 16" on a 3 x 5 card and mail it In the enclosed envelope.
5
8 <

SWEEPSTAKES FOR $9,873.97 GRAND PRIZE OFFICIAL RULES
NO CONTRIBUTION IS REQUIRED* CONffilBUTION Will NOT IMPROVE CHANCES OF WINNING
1. Sponsor-this sweepstakes Is sponsored by National Alzheimer's Council {a program of the National Emergency Medicine Association.) Phone: 443-922-7533 Address: P.O. Box 1039, Edgewood, MD 21040.
2. Prizes-there arc these two Prizes: 1) Grand Prize of $9,873,971 2) A Bonus Prize of $100,00, Prizes are non~transforable and there are no substitutes. 3. Entry Instructions: - to enter With a gift, return the entry form In the enclosed envelope. To enter without a gift, print your name, address, Authorization# and "NAG Dec. 16" on a 3 x 5 card
and mall It In the enclosed envelope, Failure to comply will result In disqualificallon. 4. Prize Select!on Process -1) Grand Prize: the winning entry was randomly selected by an Independent agency whose decision was flnal and b!ndlng belore ttle promotion letters were mailed
and were randomly seeded among mailed letters. If your ellgible entry matches the pre-selected number, you will be notified that you have wan the Grand Prize. 2) Bonus Prize: The winning entry will be randomly selected from an eligible entries received by the deadline date. The agency's decisions are flnal and binding.
5. Who ls ehglble - the sweepstakes ls open to residents (18 years or alder) of the United States and Its possessions who receive the mailing. Employees, agents, vendors and staff of the Sponsor, National Alzheimer's Council (a program of the National Emergency Medicine Association.) Address: P.O. Box 1039, Edgewood, MD 21040, Its advertising and promotional agencies, and sweepstakes administrator {and their household members) are not eligible to win, The entry form will not be honored if not mailed In the enclosed envelope with sufficient postage by the entry deadline.
6. Entry Deadline: -the deadline for malling your entry is February 25, 2017. Postmark determines date of entry. 7. General-Sweepstakes void where prohlblled by law. All federal, state and local regulations apply, Winners will be notified by mail. By participating, entrants agree to be bound by these rules.
Failure to comply with these or any other Official Rules will result in disqualification. Winner must sign and return an affidavit of eligibility, a liability release, and except where prohibited by law, a publicity release within 10 days of issuance of notification. If winner does not comply with the foregoing, or If a pr!ze or prize notification Is undeliverable, and/or if a selected winner does not comply with any portion of these Offlclal Rules, such winner will be d!squalif!ed and, !n the case of the Bonus Prize only, an alternate winner will be selected. Entrants agree that: 1) Sponsor shall have right and permission to use {if a winner) entrant's name and city of residence for advertising, trade and/or other purposes In perpetuity without lurther compensation {unless prohibited by law); and 2) Sponsor, Its advertising and promotion agencies and each of their respective officers, directors, employees, representatives and agents shall have no liabl!ity and wlll be held harmless by entrants for any liability, loss, injury or damage to entrants or any other person or entity relating to this sweepstakes. Taxes sole responslbllity of winner. Sponsor and lts agencies are not responsible for late, lost, or mlsdlrected mail or any printing or technical errors or malfunctions of any kind, by any human error that may occur in the processing of the entries ln this Sweepstakes. If for any reason that corrupts or affects the administration, security, fairness, Integrity, or proper conduct of this Sweepstakes so that it Is not capable of being conducted as described In these rules, Sponsor shall have the right, at Its sole discretion, to cancel, terminate, modify or suspend the Sweepstakes, Any person who supplles fa!se information, enters by fraudulent means, or is otherwise determined to be In vlolatlon of these rules in an attempt to obtain any prlze wlll forfeit any prize won. No gift or payment of any klnd Is necessary to enter or w!n. Entries become the property of the Sponsor and will not be returned ..
8, Winners -for the name of the Grand Prize winner, send a self~addressed stamped envelope to National Alzhe!mer's Council. Address: P.O. Box 1039, Edgewood, MO 21040 on or within 60 daysaftertheentrydeadllnedate.
9. Odds of Winning -1) Grand Prize: the number of entry forms mailed determines the odds of winning. Your odds of winning will be no greater than i in X,XXX,XXX. Your odds of winning the Bonus Prize are dependent upon the number of qualifying entries received.
10. Creative Presentations - this sweepstakes may be mailed by NEMA with different creative presentations. The pre-selected winning Grand Prize number has been selected from au entry numbers for a!I creative presentations, and the winning Bonus Prize number has been selected from all entries received for all creative presentations.
11. Malling List Suppressions-if you do not wish to receive mailings of this type in the future please write to: National Alzheimer's Councll. Address: P.O. Box 1039, Edgewood, MD 21040. Because winners are selected in advance and sweepstakes entrles are printed In advance, It wlll take Six to Eight weeks before you stop receiving mail.
12. For additional information about this sweepstakes or sweepstakes In general, visit www.sweepstakesconsumerguide.net.
NAG FACTS Solicitation For Charitable Purposes Card:
Your gift is very much appreciated and fully deductible as a char!table contribution. A copy of the summary of the latest financial statement, or annual report, and registration filed by NATIONAL EMERGENCY MEDICINE ASSOCIATION {NEMA), {Incorporated In Washington, D.C.), with Its spacial program National Alzheimer's Council {NAG) may be obtained by contacting us at The National Emergency Medicine Association, P.O. Box 1039, Edgewood, MD 21040 {443) 922-7533, If you are a resident of one of these states, you may obtain financial information directly from the state agency: FLORIDA-A COPY Of THE OFFICIAL REGISTRATION AND FINANCIAL INFORMATION MAY BE OBTAINED FROM THE DIVISION OF CONSUMER SERVICES BY CALLING TOLL-FREE, 1-800-435-7352 {800-HELP-FLA) WITHIN THE STATE. REGISTRATION DOES NOT IMPLY ENDORSEMENT, APPROVAL, OR RECOMMENDATION BY THE STATE, Florida Registration #CH313, GEORGIA -A full and fair description of Iha programs of NEMA and our financial statement summary is available upon request at the office and phone number Indicated above. Maryland - for the cost of copies and postage, Office of the Secretary of State, State House, Annapolis, MD 21401. MISSISSIPPI - The official registration and financial information of NEMA may be obtained from the Mississippi Secretary of State's office by calling 1-888-236-6167, Registration by the Secretary of State does not Imply endorsement. NEW JERSEY -INFORMATION FILED WITH THE ATTORNEY GENERAL CONCERNING THIS CHARITABLE SOLICITATION AND THE PERCENTAGE OF CONTRIBUTIONS RECEIVED BYTHE CHARITY DURING THE LAST REPORTING PERIOD THAT WERE DEDIGATEO TO THE CHARITABLE PURPOSE MAY BE OBTAINED FROM THE ATTORNEY GENERAL Of THE STATE Of NEW JERSEY BY GALLING {973) 504-6215 AND IS AVAILABLE ON THE INTERNET AT http:// www.state.nj.us/lps/ca/charfrm.htm, REGISTRATION WITH THE ATTORNEY GENERAL DOES NOT IMPLY ENDORSEMENT. NEW YORK - Office of the Attorney General, Department of Law, Charities Bureau, 120 Broadway, New York, NY 10271, North Carolina - FINANCIAL INFORMATION ABOUTTHIS ORGANIZATION AND A COPY OF ITS LICENSE ARE AVAilABLE FROM THE STATE SOLICITATION LICENSING BRANCH AT 1-888-830- 4989, THE LICENSE IS NOT AN ENDORSEMENT BY THE STATE. PENNSYLVANLI\ - The official registration and financial information of NEMA may be obtained from the Pennsylvania Department of State by calling toll-free, within Pennsylvania, 1-800-732-0999. Registration does not Imply endorsement. VIRGINIA -Virginia State Division of Consumer Affairs, Department of Agricultural and Consumer Services, PO Box 1163, Richmond, VA 23218. WASHINGTON - Charities Division, Office of the Secretary of State, State of Washington, Olympia, WA 9B504-0422, 1-800-332-4483, WEST VIRGINIA- Residents may obtain a summary of the registration and financial documents from the Secretary of State, State Capitol, Charleston, WV 25305. Registration with any of these state agencies does not Imply endorsement, approval or recommendation by any state.
What is Alzheimer disease? Alzheimer disease, or Alzheimer's as it is also refe1Ted to, is the leading cause of dementia. Named after the person who first described it, Alzheimer disease may be defined as a set of symptoms that include loss ofmemmy,judgement, reasoning ability, and often changes in behavior. With the aging of the "baby boomers" the incidence of Alzheimer's is expected to more than triple by the middle of the 21st century. At the present time, Alzheimer's cannot be stopped or cured. Research, however, is resulting in greater understanding of the disease and identification of steps that may reduce your risk of experiencing Alzheimer's
How is Ahlteimer disease diagnosed? There are several warning signs that you can look for that may indicate Alzheimer disease. These include memory losses that affect someone's abillty to function, such as forgetting where you are or how to get to a familiar place, difficulty performing familiar tasks, problems with language, disorientation of time and place, poor or decreased judgement, problems with abstract thinking, misplacing or losing things, changes in mood or behavior, changes in personality, or loss of initiative. Just one of these signs doesn't mean someone has the disease; usually several of them are present and changes are progressive.
If you or someone you know suspects Alzheimer disease, tests to make the diagnosis may include a complete medical history, a mental status exam, a physical exam, laboratory tests and psychological or psychiatric evaluations, Getting a diagnosis and getting it early will help the affected person and their family make plans for the future.
There are other conditions and diseases that can produce dementia. These include thyroid disease, depression, infections, drug interactions, alcohol abuse, or simply not enough to eat or drink. That's why It is very important to see your doctor If you suspect Alzheimer disease, Many of the other conditions can be treated and the dementia cleared up before permanent damage is done,
How is Ahlteimer disease diagnosed? The National Alzheimer's Council is an outreach of the National Emergency Medicine Association, a 50l(c)(3) nonprofit organization founded in 1982. Our Mission is the prevention of injury and illness by addressing health and social Issues through education, applied research, technology, and equipment. "Prevention through Education" is the overall theme of our efforts, and we have become known for our educational health-related materials, which are free to schools, hospitals, health centers, and a wide array of social service programs, For example, the information above was taken from the pocket book, ''.Alzheimer's - Hope Through Education" which was written and produced by the National Alzheimer's Council, It explains Alzheimer's, what we know today and what steps research suggests that we might take today to reduce the risk of Alzheimer's, If you or someone you love is concerned about Alzheimer's, we encourage you to contact the National Alzheimer's Council today,
10167771 NAG Check Authorization Size= 8.5 x 14

17656 NAC Che+INSERT_Layout\i 10/27/16 3:i
CONSUMER DISCLOSURES YOU HAVE NOT YET WON THE GRAND PRIZE. ENTRY IS FREE. DONATING WILL NOT INCREASE YOUR CHANCES OF WINNING. YOU MAY OR MAY NOT HAVE A NUMBER THAT IS THE WINNING NUMBER. ODDS THAT YOU WILL WIN THE GRAND PRIZE OF $9,873.97 WILL BE NO GREATER THAN X,XXX,XXX. ODDS THAT YOU WILL WIN THE BONUS PRIZE DEPEND ON THE NUMBER OF ELIGIBLE REPLIES RECEIVED.
L13/14/15
1
10167771 NAC C~k Authorization INSERT SIZE: 2 X~ORS- Black

17656 NAC Che+INSERT_Layoutl 1 10/27/16 3:1
_J
0 z ::)
0 0 Cf)
0:: w ~ w I ~ <C _J
<C z 0
~ z

NA
ME
AD
DR
ES
S
CIT
Y
ST
AT
E
AU
TH
OR
IZE
D
AM
OU
NT
:
ZIP
i, 9
,&7
3.9
7
9 ,
0 0
0.
0 0
80
0.0
0
7 0
. 0
0
- - - - -
-----3~
$ ~
FU
LL
EL
IGIB
ILIT
YT
OW
IN
)(°A
UT
HO
RIZ
ED
D
EN
IED
RE
TU
RN
TO
AR
RIV
E O
N O
R B
EF
OR
E
FE
B.
25
/
20
1 7
D
EA
DLI
NE
[ 101
6777
1 NA
C C
heck
Aut
horiz
atio
n CR
E S
ize=
8.8
75 X
3.87
5 co
lors
= B
LACK
, PM
S 29
35
FIR
ST
11 I I
I A
FF
IX
MAI
L P
RO
PE
R
PO
ST
AG
E
PR
IOR
TO
MA
ILIN
G
NA
C
PO
BO
X 1
818
ME
RR
IFIE
LD
VA
221
16-8
018
1lll1
l11 l1 l
11 l11
l1 lil1
llll1
ll11l1
111111
1 1111 111
11 l11 l
1111111
1•111

Exhibit F.6

111
11 *S
ELEC
TIO
N AL
ERT*
&)
X{[p
ffJ&~
~ ml
&IP!
L W
$ 1
0 0
0 0
• 0
0
~~
~~
~~
.._
..,_
_.,
,.,.
, :
-~~JA.
o,. --
~f
i Af
f 11 th
',,;
,;e-al
~-
--=,
to t
he-
e-V1u
-lo,;e
-d _.
.If
• • ~•~
itci-----=
=-::_
:_
-=
~~
~~
A& f,v
a-MoV
I f'o
vrVI
Rso
N
Joh
n
Q_
Sarn
ple
pers
on
A
dd
ress
C
ity
, ST
1
23
45
B
AR
CO
DE
1121
4704
1 N
EM
A S
elec
tion
Ale
rt #
10 O
SE
4.1
25
" x
9.5
" co
lors
:
. .,11
.. l· 11,
-m "\
•,it
:,~
,\:
f ll
.-'i'
J ,....
.,,,,
-
ll\•
''"' ·
tll
V''
-~-.. ,~,
._ ,_
.. -"'

·~l\'(
*SELECTION ALERT* &JZffaOO&©© OO&ffeJ!L W
Immediate Dispatch To: John Q, Sampleperson Address1xxxxxxxxxx Cityxxxxxxxxxx, ST 12345
Re: Prize ID 999999
For Prize Amount:
**$10,000.00**
Dear Mr, Sampleperson,
This is an urgent, PERSONAL ALERT about your Prize I,D, XXXXXX which entitles only you the opportunity to win $10,000,00, That's right, only you were selected for Prize I,D, XXXXXX, Only you have the ability to use this unique alpha/numeric code to win the $10,000,00,
In fact, Mr. Sampleperson, the $10,000,00 could be available to deliver to your address as early as April 1st - - -
The address we have in our records is [address], [city], [state] [zip code], If our records are incorrect, please inform us immediately, We absolutely must know by March 15th, That's the deadline, If I have not heard from you by then, you will forfeit your eligibility for the money,
All of the above is true and accurate, So, by all means, don't delay, The $10,000,00 check will be sent as quickly as possible after the winning Prize I,D, is received by this office, A contribution is not required and will not increase your chances to win,
Here's what you need to do to maintain your eligibility and join in the fight against heart disease:
• Transfer your Selection Alert Seal from the outer envelope to the Prize Activation Form below,
• Check the .Y.e.s. box to indicate that you would like to win and would accept the $10,000,00 Prize,
• Check the .Y.e.s. box indicating that you are making a contribution to fight heart disease, Be sure to designate the gift you would like to make, Most people give $7 or $5, Simply choose a gift level you can afford and that represents your interest in stopping heart disease,
• Mail the Prize Activation Form by March 15th,
Thank You, I'm looking forward to receiving the winning reply,
~ o ·1 erz J. ., Heart Counc1 . t Nat'f o,,a,. Pres1den ,
A10/A11/A12 ._!, REPLY BY MARCH 15TH. THE DEADLINE CANNOT BE EXTENDED . ._!,
~·10'99ie"g·g,ACrivA"r·mi .. UFDRM·~~~:;!;:~~:~::~J ~~_, ................ ,, .... .,...,.,,.. ... ~.,--.,,~~.....,_ ... .._.._,..,...,.,.,,...,.,, ... ,....~- SELECTION ALERT w..l
D YES I want to win the $10,000.00.
D YES I have affixed my Selection Alert Seal at right and am mailing this form by 03/15/2015.
• YES I have enclosed a gift to help in the fight to stop heart disease: ] $7 .00 [ ] $5.00
1hOJ1k You 1.
[ ]$ __ ] $10.00
Make check payable to NEMA or National Heart Council.
Gift not required and will not increase winning chances.
11]111111111111111111111111111111111111 i iV~~~i~;~i~~u;~~ 6
For Delivery To: John a. Sampleperson Address City, ST 12345
Signature: ___________ _ John a. Sampleperson
xxxxxxxxxx xxxxx
12147041 NEMA NHC Selection Alert Form 8.5 x 14" colors: Black, Orange PMS 021, blue

+
17041 NHC Selection Alert Backer Only_Layoul1 12/8/14 3:58 PM Page 1 + SWEEPSTAKES FOR $10,000.00 GRAND PRIZE
OFFICIAL RULES NO CONTIUBUTION IS REQUIRED* CONTRIBUTION WILL NOT IMPROVE CHANCES OF WINNING
1. i%a~~~%:P.~~sa5~~cf8j~~k~a~~\t~~d~OMB ~ro~~~ional Heart Council (a program of the National Emergency Medicine Association) Telephone (443) 922-7533
2. Prizes - there are two Prizes: I) Grand Prize of SI0,000.00, and 2) Bonus Prize of S 100.00, Prizes arc non-transferable and there arc no substitutes. 3. J~~&Ti~~~truclions: to enter with or without a donation, return the reply form in the enclosed envelope postage pre-paid postmarked before the entry
4. Prize Selection Process - I) Grand Prize: the winning entry was randomly selected by an independent agency whose decision was linal and binding before the ~romotton letters were mailed and were randomly seeded among mailed letters. If your eligible ent~ matches the pre-selected m.unbcr, you will be ~g:~i~~dr~~~fJe~u~~a~hc 'd~~dW~cGJri~~ ~~~eaJJn~;~uJe~i~f~i1 tf!efiri~7n1
1~cf bTT~~
11~_ill be randomly selecte by an independent agency from among all eligible
5. Who is eli ible the sweeP.stakes is open to residents (18 years or older) of the United States and its possessions who receive the mail in~ Employees, ~cnts, vcn ors and staff or the SJrnnsor, National I lcarl Council (a program of the National Emergency Medicine Association) Address: P.O. Box 1039, Eclgcwood, MD 21040, its advertising and promotional agencies, and sweepstakes administrator l!_uu.l thcir household members) arc not eligible to win. The entry fom1 will not be honored if not mailed in the enclosed envelope with suflicient postage by the entry deadline.
6. Entry Deadline: the deadline for mailing your entry is March 15, 2015. Postmark determines date of entry 7. General - Sweepstakes void where prohibited by law, All federal, state and local rcg_ulations aP.ply. Winners will be notified by mail. By participating,
entrants agree to be bound by these rules. Failure lo comply with these or any other Official Rules will result in dis!=jualification. Winner must sign and return an affidavit of eligibi!1t{J, a liability release, and except where prohibited by law, a publicitY. release within 10 days of issuance of notificatton, If
~vJ~t1:!ed8ffi~\~\ ~i11s1:'sii~hh w?rin~f~~11i~· gi~i~!1ffi~d ~~1,rl~~6~
0~1f~~n~?ih~s ~~~~;ip~~~~
1~nr~~~raife~i:t
1;~~i~~~:1~~f1) t~e;cre~\gg_mRlrtr~~l~ !~feg~,~lfn I) Sponsor shall have right and permission to use (if a winner~ entrant's name and city of residence for advertising, trade and/or other purposes in perpetuity
di~~~~~ist~!i~~rocy0e~?,er~~~~~n\~ti~e:; fi~.d~i~!~~t~ ~fia\ft~l~:~~o 11atWi~~itjt~r1Ybe:~!
11~1;~!Fers~
1i~ti~~r~¥1~~t~e/ a~;d1i:~i7i~ \~~~
1: i~jt'iryt~~ed~~;~c~~st'o
entrants or any other person or entity relating to this sweepstakes. Taxes sole responsibility of winner. Sponsor and its agencies arc not rcsponsifile for late, los\; or misdirected mail or any printini or technical errors or malfunctions of any kind, bf: any human error that may occur in the processing of the entries
i~ Ao\s c~;ibfes~}k~!i~! ~~1~~t~~a~~nd~s~~i1'C:d~ht~h~~:f::1~t;j ig;o~~~~~~!wi~~e st1~tl:·t~11t! ~t~t~s:of~tjfsr~~~\i~i,;~i~~1~~r~~~~y~·~re\s 1~~"Jify5~~~~ss;~1{~~h~t
~t\~i~~iltok~btiii~~if/~sr~~e '~tif l sf~~Pc1if ~£~1 ~~i~~r~s~~~ tii~11trig;e~~~6t1f ~aili~u~~g~~1e;~Y th
1~ is;~~~~~~,~~i~\lf~~ieb~ \?e~~~~liolation of
these rules in an
8. Winners - for the names of the Grand Prize and Bonus Prize winner(s), send a self-addressed stamP.ed envelope to National Heart Council (a program of the National Emergency Medicine Association) Address: P.O. Box 1039, Edgewood, MD 21040 on or within 60 days after the entry deadline dale.
9· £~8<.~x~.n~ir~~n~11 ~f.r:1c~ t{Ja~: th~~ ~~~~\~~1°,(,fi~~lfu f861~l~s
11b~\~ecd o~e$1l(IBi~i~ a~~e~~~~gJb~i~nj~~o~~~~ ~~~ib~~ ~i~Yl~&1~i~~1?r1e
1i0nf[~i~~~-
than l in
10. ~:i~~\~VJ t~~~~c~{1a~igt~~ ~l~;~~b:;~tb~s~llk~:e~~~re ~~~s1i~1t~~i~~i~~l a~Sf ~~~l~~f ~~f ~~i~~~u~~w~~~~~imb~~ g~~-~~~cri~ee~e\~f ~
1SiR-g1~~,r~tt~!!~ t~el~~~~~ htt~ ~f{n creative presentations.
11. Mailinfi List ~uppressions - if you do not wish to receive mailings of this type in the future please write to: National Heart Council (a program of the Na tonal qncrgcncy Medicine Association) Address: P.O. Box 1039, Edgewood, MD 21040.
12. If you would like additional lnfonnation about this sweepstakes or sweepstakes in general, visit www.sweepstakesconsumeq,uide net.
1.
2.
Don't smoke. Ten Steps To A Healthy Heart
There's no question that smokers suffer more heart disease than people who don't smoke. Smoking increases the risk of heart attacks and makes them more severe when they occur. So if you smoke, quit. Many programs and medicines are available to help you do it. If you live with a smoker, encourage them to quil. Exercise regularly. Regular exercise helps yom hearl stay healthy. Just like any other muscle in your body, your heart needs exercise to keep in shape. Your exercise goals can be modest. You will see heart~healthy benefits. So get moving.
3. \Vatch what you eat. Anything that you eat has an impact on your body's health, Ifs important to choose a diet that includes lots of whole grains, and fresh fruits and vegetables.
4. Limit your fat Intake, You should try to limit fat consumption to no more than 30% of your calories per day. For most people, that means between 50 and 70 grams of fat per day. With the new nutrition labels on foods, it is fairly easy to make sure you stay below that limit. Read the labels of foods before you buy them.
5, \Vatch your weight. People who arc overweight, even just a little bit, are at increased risk of heart disease. Try not to let your weight creep up, which it tends to do as we get older.
6. See your physician regularly. Regular examinations help insure that problems will be recognized before they become severe,
7. Know your family history. It's important to know if anyone in your family has suffered a heart attack, and how old they were when it occutTed. Sometimes this indicates that you are at increased risk of heart disease and may need a very thorough evaluation,
8. Know your medications, Keep accurate records of the medications you take and take them as they are prescribed. Your pharmacist can help you with this. Especially with heart medicines, it's important to know what else you may be taking, and never stop taking the medicine without the advice of your doctor.
9. Stay connected. Social supports arc very important for people, We know that those who have the support of family and friends suffer fewer and less severe heart attacks. So stay connected.
10. Stop to smell the roses. Don't let ordinary irritations like traffic jams or aggressive drivers get to you. Do things at your own pace and take time to enjoy life.
You Can Help Fight Heart Disease Through A Bequest In Your Will Sitnply add this language to your will:
"I bequeath to NlfC (a program of National Emergency Medicine Association, a not-for-profit organization incoq>0ratc<l in Washington, D.C.) the Slltll of$_ to be used in sllppor! of its efforts including education, applied research, technology nnd equipment."
If you already have a will, it generally is possible to udd a bequest lo fight heart disensc without preparing a new will, Through 11 short scpuratc document (known as u 0 codicil"), you can include NHC as your beneficiary, Be sure and check with your attorney to make sure thnt any change in your wm or codicil complie.~ with the law of the state where you live. For more information about the fonn of a hequest or other estate gift to fight heart disease ju$t call the Estate Planning Department at (443) 922-7533.
Please remember the National Heart Council in your will.
+
+

+
17041 NHC Sele~ert lnsert_Layou11 12/8/14 3:41
CONSUMER DISCLOSURES YOU HAVE NOT YET WON THE GRAND PRIZE. ENTRY IS FREE. DONATING WILL NOT INCREASE YOUR CHANCES OF WINNING. YOU MAY OR MAY NOT HAVE A NUMBER THAT IS THE WINNING NUMBER. ODDS THAT YOU WILL WIN THE GRAND PRIZE OF $10,000.00 WILL BE NO GREATER THAN XXX,XXX. ODDS THAT YOU WILL WIN THE BONUS PRIZE OF $100 DEPEND ON THE NUMBER OF ELIGIBLE ENTRIES RECEIVED.
AIO/All/Al2
-$-
+

+
17041 NHC Sele+ert lnsert_Layou11 12/8/14 3:41
-®-
....J
0 z ::)
0 0 la: <( w I ....J <( z 0
~ z
+

PR
INT
Le
ga
l De
live
ry A
dd
ress
-~~~~
• Y
ES
-I a
m m
ailin
g by
dea
dlin
e
*SEL
ECTI
ON
ALE
RT*
g;:
{ffe/K
i&@
@ !K
i&!Pl
b W
$1
0,0
00
RE
PL
Y P
RO
CE
SS
ING
N
atio
nal
He
art
Co
un
cil
I
(a p
rog
ram
of t
he
Nat
iona
l E
mer
genc
y M
ed
icin
e A
sso
cia
tion
)
PO
Bo
x 20
626
St.
Lo
uis
, M
A 6
31
39
-06
26
I 11 •III
I 111 •
111111 1
1 • I 11
11 11 h
111 1 h 11
1 I I 11 •
11 1•1111
11111
11111
111
1214
7041
NE
MA
NH
C S
ele
ctio
n A
lert
#9
RE
" B
lack
, o
ran
ge
pm
s 02
1
PLAC
E ST
AMP
HERE

IMP
OR
TA
NT
--
MA
IL W
ITH
GIF
T B
EF
OR
E 0
3/1
5/2
01
5 D
EA
DL
INE
NHC
FACT
S So
licita
tion
For C
harit
able
Pur
pose
s Ca
rd:
Your
gift
is v
ery
muc
h ap
prec
iate
d an
d fu
lly d
educ
tible
as
a ch
arita
ble
cont
ribut
ion.
A co
py o
f the
sum
mar
y of
the
late
st fin
anci
al s
tate
men
t, or
ann
ual r
epor
t, an
d re
gist
ratio
n file
d by
Nat
iona
l Em
erge
ncy
Med
icin
e As
socia
tion
(inco
rpor
ated
in W
ashi
ngto
n, D
C) m
ay b
e ob
tain
ed b
y co
ntac
ting
us a
t Nat
iona
l Em
erge
ncy
Med
icin
e As
socia
tion,
P.O
. Box
103
9, E
dgew
ood,
MD
2104
0 (4
43) 9
22-7
533.
If y
ou a
re a
resi
dent
of o
ne
of th
ese
stat
es, y
ou m
ay o
btai
n fin
anci
al in
form
atio
n di
rect
ly fr
om th
e st
ate
agen
cy:
FLO
RIDA
-A
COP
Y OF
THE
OFF
ICIA
L RE
GIST
RATI
ON A
ND F
INAN
CIAL
INFO
RMAT
ION
MAY
BE
OBTA
INED
FRO
M T
HE D
IVIS
ION
OF C
ONSU
MER
SER
VICE
S BY
CAL
LING
TO
LL-F
REE,
1-8
00-4
35-7
352
(800
-HEL
P-FL
A) W
ITHI
N TH
E ST
ATE.
REG
ISTR
ATIO
N DO
ES N
OT IM
PLY
ENDO
RSEM
ENT,
APP
ROVA
L, O
R RE
COM
MEN
DATI
ON
BY T
HE S
TATE
. Fl
orid
a R
egis
tratio
n #C
H31
3.
GEOR
GIA
-A
full
and
fair
desc
riptio
n of
the
prog
ram
s of
NEM
A an
d ou
r fin
anci
al s
tate
men
t sum
mar
y is
avai
labl
e up
on r
eque
st a
t the
offi
ce a
nd p
hone
num
ber
indi
cate
d ab
ove.
M
aryla
nd -
For t
he c
ost o
f cop
ies
and
post
age,
Offic
e of
the
Secr
etar
y of
Sta
te, S
tate
Hou
se, A
nnap
olis,
MD
2140
1.
MIS
SISS
IPPI
-Th
e of
ficia
l reg
istra
tion
and
finan
cial
info
rmat
ion
of N
EMA
may
be
obta
ined
fro
m th
e M
issi
ssip
pi S
ecre
tary
of S
tate
's of
fice
by c
allin
g 1-
888-
236-
6167
. Reg
istra
tion
by th
e Se
cret
ary
of S
tate
doe
s no
t im
ply
endo
rsem
ent.
NEW
JERS
EY -
INFO
RMAT
ION
FILE
D W
ITH
THE
ATTO
RNEY
GEN
ERAL
CO
NCER
NING
THI
S CH
ARIT
ABLE
SOL
ICIT
ATIO
N AN
D TH
E PE
RCEN
TAGE
OF
CONT
RIBU
TION
S RE
CEIV
ED B
Y TH
E CH
ARIT
Y DU
RING
THE
LAS
T RE
PORT
ING
PERI
OD T
HAT
WER
E DE
DICA
TED
TO T
HE C
HARI
TABL
E PU
RPOS
E M
AY B
E OB
TAIN
ED F
ROM
THE
ATT
ORNE
Y GE
NERA
L OF
THE
STA
TE O
F NE
W J
ERSE
Y BY
CAL
LING
(97
3) 5
04-6
215
AND
IS A
VAIL
ABLE
ON
THE
INTE
RNET
AT
http
://w
ww
.sta
te.n
j.us/
lps/
ca/c
harfr
m.h
tm.
REGI
STRA
TION
WIT
H TH
E AT
TORN
EY G
ENER
AL D
OES
NOT
IMPL
Y EN
DORS
EMEN
T.
NEW
YOR
K -
Offi
ce o
f the
Atto
rney
Gen
eral
, Dep
artm
ent o
f Law
, Cha
ritie
s Bu
reau
, 120
Bro
adw
ay, N
ew Y
ork,
NY 1
0271
. Nor
th
Car
olin
a -
FINA
NCIA
L IN
FORM
ATIO
N AB
OUT
THI
S OR
GANI
ZATI
ON A
ND A
COP
Y OF
ITS
LICE
NSE
ARE
AVAI
LABL
E FR
OM T
HE S
TATE
SOL
ICIT
ATIO
N LI
CENS
ING
BRAN
CH A
T 1-
888-
830-
4989
. THE
LIC
ENSE
IS N
OT
AN
ENDO
RSEM
ENT
BY T
HE S
TATE
. PE
NNSY
LVAN
IA -
The
offic
ial r
egis
tratio
n an
d fin
anci
al in
form
atio
n of
NEM
A m
ay b
e ob
tain
ed fr
om th
e Pe
nnsy
lvani
a D
epar
tmen
t of S
tate
by
callin
g to
ll-fre
e, w
ithin
Pen
nsylv
ania
, 1-
800-
732-
0999
. Reg
istra
tion
does
not
impl
y en
dors
emen
t. V
IRG
INIA
-Virg
inia
Sta
te D
ivisio
n of
Con
sum
er A
ffairs
, D
epar
tmen
t of A
gric
ultu
ral
and
Con
sum
er S
ervic
es,
PO B
ox 1
163,
Rich
mon
d, V
A 23
218.
W
ASHI
NGTO
N -
Cha
ritie
s D
ivisio
n, O
ffice
of t
he S
ecre
tary
of S
tate
, Sta
te o
f Was
hing
ton,
Olym
pia,
WA
9850
4-04
22, 1
-800
-332
-448
3. W
EST
VIR
GIN
IA-
Res
iden
ts m
ay o
btai
n a
sum
mar
y of
the
regi
stra
tion
and
finan
cial
doc
umen
ts fr
om th
e Se
cret
ary
of S
tate
, Sta
te C
apito
l, C
harle
ston
, WV
2530
5.
Reg
istra
tion
with
any
of t
hese
sta
te a
genc
ies
does
not
impl
y en
dors
emen
t, ap
prov
al o
r rec
omm
enda
tion
by a
ny s
tate
.
Exhibit F.7

NA
C EN
TR
Y ID
LA
BE
L E
NC
LO
SE
D -
RE
PL
Y R
EQ
UIR
ED
NO
TIC
E O
F C
ASH
PR
IZE
EN
TR
Y O
PPO
RTU
NIT
Y
JOH
N Q
. SA
MPL
EPER
SON
1S
I.O
. EN
TRY
NUM
BER
ENCL
OSE
D
PR
IZE
AM
OU
NT
1Sl
800
900
00
PR·~~
-~·
.. '
"··
·.. '..
L
"" ~ _<
. ~
\ l L
..
1214
7064
NAC
Inst
allm
ent O
SE F
lat s
ize =
4.1
25 x
9.5
"
Col
ors=
Bla
ck, P
MS
1797
, Las
er V
aria
ble
SE
CU
RIT
Y
CO
NF
IRM
ED
m
1u11
n111
um 111
11 nu
t 111
11 11
1n nu
111~
RE
CIP
IEN
T
JOH
N
Q.
SAM
PLE
PER
SON
A
DD
RE
SS
1 A
DD
RE
SS
2 C
ITY
, ST
1
23
45
B
AR
CO
DE

I IH
';i,7
i•ci:-O'•
o·PRr
ztErh
iv111
UI
'••
~•
•••••~
-,•
>
--
• ""'" 0
"
• "'
>
C ~
<
om
•
>
§
112
14
70
61
NA
G I
nsta
llmen
t La
bel
1.7
5"
x .7
5"
Bla
ck &
PM
S 4
52

SECURITY VERIFIED FOR OFFICE USE ONLY
VOID AFTER DEADLINE _JJ2_;:i"l{Jl~l~5~-MIL [O] • [2] [3] [4] [5] [6] [7] [8] [9] WIRE j [N]
-11is is vo.r Olfi:i,1 $' Millon ~ Pr~e Enlry Label Transfer
To form Below lvla1I Al Once PRIZE ID 999999999999 JOHN Q, SAMPLEPERSON
CONFIRMATION OF CASH PRIZE ENTRY OPPORTUNITY JOHN Q, SAMPLEPEl!SON HAS BEEN APPROVED
To ENTEi! SUPER PRIZE ID # 999999999999 Fol! THE AMOUNT OF
$1,000,000~00 PRIZE *** ONE MILLION and 00/100 DOLLARS PAID IN 30 ANNUAL PAYMENTS OF $33,333,34 ***
JOHN Q. SAMPLEPERSON Address! Address2 City, ST Zip
IDENTITY CONFIRMED - REPLY REQUIRED
CONFIRMED RECIPIENT 1111111 lllll lllll lllll lllll lllll lllli 1111111111111
Dear Johnxxxxxx,
Have you ever considered what you might do with an extra $33,333.34 every single year for the next 30 years?
Because you, JOHN Q, SAMPLEPERSON have been assigned Super Prize ID #999999999999 for entry in the Super $1,000,000,00 Prize sweepstakes, with Grand Prize available to be paid in 30 annual installments of $33,333.34 to the Winner.
That means when you reply for receipt by the deadline and if your Super Prize ID #99999999999 matches the pre-selected winning number ... your Grand Prize winnings could total $1,000,000.
Johnxxxxx, the National Alzheimer's Council (NAC) is thrilled to bring you this Million Dollar prize opportunity to raise awareness for our mission to end the tragedy of Alzheimer's Disease.
Johnxxxxxx, please help by enclosing just [$MRCI], [MRC2], or even [$MRC2]. A contribution is not required and will not increase your chances of winning, but any amount you can spare will help bring hope and happiness to many families struggling with this disease.
Johnxxxxxx, if you fail to complete and mail the form below for receipt by the 3/25/2015 deadline, the judges will not be able to send any prize to your [Cityxxxxxxxxxxx] residence that you may win, including the first of 30 installments toward the $1,000,000.00 prize if you have the super prize winning number, or even $2,500 in cold hard cash if you win the Early Bird Prize Drawing.
Please reply today so you don't miss out on this entry opportunity for the $ ! ,000,000.00 or $2,500.00 Early Bird prize.
.Johnxxxxxx1 P/e0v.5e ,e+urn +hi.s fo'fT'l OJld, JOU, d.ona.., +ion b.3 Ma..,,ch zS+h(
Attention John Q. Sampleperson: Please respond for receipt by 3/25/2015 to activate your $1,000,000 Prize entry for potential win of Prize paymenls as detailed below.
POTENTIAL PRIZE/ENTRY SCHEDULE
FOR POTENTIAL SCHEDULE FOR PAYMENT WINNER
PAYMENT #1 $33,333.34 PAYMENT #2 $33,333.34 PAYMENT #3 $33,333.34 PAYMENT #4 $33,333.34 PAYMENT #5 $33,333.34 PAYMENT #6 $33,333.34 PAYMENT #7 $33,333.34 PAYMENT #8 $33,333.34 PAYMENT #9 $33,333.34 PAYMENT #10 $33,333.34 PAYMENT #11 $33,333.34 PAYMENT #12 $33,333.34 PAYMENT #13 $33,333.34 PAYMENT #14 $33,333.34 PAYMENT #15 $33,333.34 PAYMENT #16 $33,333.34 PAYMENT #17 $33,333.34 PAYMENT #18 $33,333.34 PAYMENT #19 $33,333.34 PAYMENT #20 $33,333.34 PAYMENT #21 $33,333.34 PAYMENT #22 $33,333.34 PAYMENT #23 $33,333.34 PAYMENT #24 $33,333.34 PAYMENT #25 $33,333.34 PAYMENT #26 $33,333.34 PAYMENT #27 $33,333.34 PAYMENT #28 $33,333.34 PAYMENT #29 $33,333.34 PAYMENT #30 $33,333.34
iiiii PRIZE IDENTIFICATION VOIDAFTER ~: Plac~O$~NN~l;o~~::~~~:~a~~1~,ere ;
~--'~TRY/REGISTRATION FORM DEADLINE '.J (;/20'15 :. _______ ~la~A~o~c~ .• ___ :
;;;;. ENTER SUPER P1t1zE ID 999999999999 FoR THE • YES I am John Q. Sampleperson residing at the address shown. Enter
: / 11:l 0f;.f'A ee· f'i, 0('), PRI"EI melnthe$1,000,000SuperPrizesweepstakes. 'f ' . Cl Cl ' . · Cl ~ . . t;J · l · 1 • YES I have enclosed the following tax-deductible gift:
!!!!!I! - *** ONE MILLION and 00/100 DOLLARS PAID l [ ] $X.OO [ ] $XX.OO [ ] $XXX.OO [ ] $ ___ ', l:iii IN 30 ANNUAL PAYMENTS OF $33,333,34 *** r I - Make check payable to NAO or NATIONAL ALZHEIMER COUNCIL uY{f1 1 \
:
1
:o~!~s;~~;i;LEPERSON .Johnxxxxxxtgn x ,;;~~(~;)
= ~~dy:e;~\ip +hOJlt jOU to, jOU, i+1• - xxxxxxxxxx xxxxx = A contribution is not required and will not increase your chances of winning.
I 12147061 NAC Installment 8.5 x 11" Black, PMS 1797, Laser Variable

OFFICIAL RULES NO PURCHASE, PAYMENT, SALES PRESENTATION, OR CONTRIBUTION NECESSARY TO ENTER OR WIN.
A PURCHASE, PAYMENT, SALES PRESENTATION OR CONTRIBUTION WILL NOT IMPROVE YOUR CHANCES OF WINNING, Entry must bo received by date spaclflod elsewhere in otter or by prize doadllno(s) below, whlcheverlssooner, Fol!owallentrytnstructlonspubUshedelsewhorelnthisoffer,
SUPER MILLION DOLLAR XXII SWEEPSTAKES (REFERRED TO HEREIN AS "SWEEPSTAKES")
Prior to the Sweepstakes start date, the grand prize winning number was selected using a specfally designed computer program to randomly pick six lndlvldua( two digit numbers from 00 through 99 and output them In ascending numer1cal order with no spaces In between to form one 12·dlg!t wlrmlng number. The selection of the winning number was conducted under the supervision of Ventura Associates International LLC ("Ventura Assoclates" or ''Judges"), an Independent judging organization whose decisions are final. That winning number was placed In a sealed envelope and !s being held In a secure locked safe under the supervision of an independent auditor until the end of the Sweepstakes. !f you received an entry form with a Sweepstakes entry number appearing on H, the same type of computer program was used to randomly generate your entry number. If your entry form (whether on paper or on line or through other e!ectronlc means) Invites you to select your own entry number, you may do so by selecting six. lndlvldual two digit numbers from 00 to 99 without repeating any one such number and Inputting them on your entry form 1n ascending numerical order with no spaces !n between to form one 12 digit Sweepstakes entry number,
A winner will be determined by comparing Sweepstakes entry numbers on all elfglble entries received wllh the pre-selected winning grand prize number held In the aforementioned safe, If a Sweepstakes entry number e~acUy matching the preselected grand prize winning number is returned or submitted by an eligible entrant, winner notification wllf be made on or before 5/31/16. IF NO SWEEPSTAKES ENTRY NUMBER EXACTLY MATCH· !NG THE PRESELECTED GRANO PRIZE WINNING NUMBER IS RETURNED, THE PRIZE Will NOT BE AWARDED. Sweepstakes open only to leg a! residents of the 50 United States and the District or Columbia, and to residents of other countr1es and U.S. territories and possessions only where offered and perm!tted by law. Vold where prohibited by law. This Sweepstakes wm NOT BE MAILED Into Texas,
!I, due to a prlntrng, production, technical, human or other error of any nature, or by mere random chance, more than one vaUd entry with the pre-selected grand prize winning number Is returned, the prize wm be awarded In a random drawing conducted by Ventura Associates, whose declslons are final, from among all eligible, validated and non-suspect entries received with the pre-selected grand prize winning number to determine one prize winner only.
SWEEPSTAKES CONSUMER DISCLOSURES: You have not yet won. No purchase necessary. One prize of $1,000,000, if claimed, will be awarded as an annuity of 30 annual installments of $33,333.34 (current value of annuity as of 9/25/14 was $588,000), OR winner may choose $500,000 lump sum cash as the sole maximum cash alternative to the annuity payment option. Odds of winning are 1 :1, 192,052,400. Sweepstakes registered by Ventura Associates International LLC, 60 E 42nd Street, NY, NY 10165 ("Ventura Associates" or "Judges") & may be presented in different creative presentations by different organizations (the "Presenting Promoter(s)"). Begins 12/1 /14 at 12:01 AM EST and ends 1 /30/16 at 11 :59 PM EST. For the name of the Sweepstakes winner (!I prize Is claimed), available after 07/31/16, send self-addressed, stamped envelope by 1/30/16 to: Super Million XXH Winner, P.O. Box 9322, Medford NY 11763-9322.
DREAM OF A LIFETIME ("PROMOTION")
W!nner(s) of prizes below will be selected rrom among an ellglbte entries received !n random drawings conducted on or before 6/30/16 by Ventura Associates lnternatlonal LLC (uventura Associates" or" Judges"), whose decisions are final. Potential winr,ers will be notified wi!hin 2 weeks of selection. All prizes guaranteed to be awarded. Open only to legal rnsidents of the fifty United States and the District of Columbia and Canada and to residents of other countries and U.S. territories and possessions only where offered & permitted by law. Vold where prohlbl\ed by !aw.
ff due to a printing, production technical, human or other error of any nature, more prize claims are received for any prize level than the slated number of prize(s) Intended to be awarded per these Official Rules. the prizes at that level will be awarded in a random drawing conducted by Ventura Associates, whose decisions are final, from among all eligible, validated and non-suspect entries received.
DREAM OF A LIFETIME BONUS/EARLY BIRO GIVEAWAY CONSUMER DISCLOSURES: You have not yet won. No purchase necessary. Bonus/Early Bird winner will receive check for $2,500.00. ARV: $2,500.00. Estimated odds of winning: 1 :12,000,000. Promotion registered by Ventura Associates, 60 E. 42nd St., NY, NY 10165 & may be presented In different creative presentations by different organizations (the "Presenting Promoter(s)"). Begins 12/1/14 at 12:01 AM EST and ends 1/30/16 at 11 :59 PM EST. THE FOLLOWING APPLIES TO ALL OF THE ABOVE (Collect!vely, "the promotions")
All entries become property of their respective Presenting Promoter & will not be returned or acknowledged. Participating entrants agree to these rules and the decisions of Judges end the Presenting Promoters, which ara final and binding and release Ventura Associates and the Presenting Promoters and their respective parents, subsidiaries and affiliated companies, and all other businesses involved in these promotions, as well as the employees, officers, directors and agents of each, from all clalms and liability relating to their participation, acceptance, use, and or redemp!lon of prize. Winners assume all liab!!ity for any injury or damage caused or claimed tobecaused,bypartlclpatlonlnthesepromo\lonsoracceptance,useorredemptlonofanyprize.
Presenting Promoters and Ventura Associates are not responsible for any printing, production, typographlcal, human or other error of any nature In printing of any promotional notice, promotion number, entry form or prize nollce, or In the admlnlstrallon of the promotions or announcement of the prizes. Any notice, prize number, entry form or prize notice containing a printing, production, typographical, human or other error of any nature shell be deemed null and void. No responslbllity assumed for lost, late, misdirected, llleg!b!e, Incomplete, muUlated/postage due or mecl1anlcally reproduced entry forms, or entry forms that have been tampered w!lh or not ob· talned thtough legitlmate channels, all of which will be disqualified. l.labll!ty for an irregular entry form, pri2e number, prize notice or promotional nollce shall be limited !o replacemer,t with another. Ventura Associates shall always have the right to take such other measures as It deems necessary or appropriate, in !ts sole discretion, to preserve the Integrity of the promoUons. In no event shall Ventura Associates and/or PresenUng Promoters have any Uab!llty or obllgaUon to award more than the stated pr!ze(s) offered !n conjunction with these promotlons. Reference to third parties !n connection with prizes and/or third party websites or services are for refer· enceand!dentiflcationpurposeson!yandnotintendedtosuggestendorsement.sponsorshiporafflliatlonwlthPresentlngPromoter{s)orthepromotlons.
Ventura Associates and any of the Presenting Ptomoters are not l!able for payment of any prize to entrants who have violated these official rules. Winners acknowledge thatVenturaAssociales, Presenting Promoters and aU other businesses concerned with these promotions and their agents do not make, nor are In any manner respons!b!e for any warranty or representations, ex.pressed or Implied, In fact or In law, relative to the quallty, condl· tions,fitnessormerchan!abllityofanyaspectofanymerchandiseprlzeex.ceptthatsuchprlzeshal!besubjecttomanulacturer'sstandardwarranty.
In order to win a prize, a winner may be required (at Judges' discretion) to sign & return anAffidaviVDeclaration of Eligibilily/Uability Release, & where legally permissible, a Publicity Release within 10 days of date on notification and may be reQulred to provide proof of identity, Winners of prizes valued at S600 or more will be required to furnish their taxpayer identificatfon number Information before the awarding of any prize to comply with IRS tax. reporting requirements, Failure to execute and return any required documentation within the !!me period specified and/or return of any prize notificatlon or prize as undeliverable may result in disquallfication and selecUon of an alternate winner. Acceptance of a prize by a minor (eighteen (18) In most states, nineteen (19) In Alabama and Nebraska and twenty-one (21) In Mississippi) wltl require ex.ecutlon by parent or legal guardian of re Quired documentallon. Costs lot goods or services not specified are winner's responsibility. No subst!tution of prizes ex.cept by Presenting Promoter or Ventura Associates due to unavailability. Except where prohibited by law, wlnner(s) consent to use of their names, vo!ces, hometowns, prizes won & likenesses for advertising, promotional and/or publlclty purposes on behalf of all Prasentlng Promoters and Ventura Associates and Its deslgnee(s), In all forms of media and by all manners (now and hereafter known), worldwide, In perpetuity, without any ob!lgatlon, noUce or additional compensation. Vold where prohibited by law, All federal, state, provincial & local laws & regulations apply. Prize values awarded In U.S. currency. No transferor assignment of pr1ze permltled except to a surviving spouse. Winners responsible for all taxes on prizes. U.S.laws govern all aspects of these promotions, AU disputes and claims arising out of or relating to these promotions sha!I be determined according to the laws of the State of New York without regard toils conflict of law principles, rules or provisions that would cause the application of any other state's laws and all participating entrants consent to the personal ]ur1sdlctlon of the federal and state courts located !n New York County and agree that such courts have exclusive jurlsd!cllon over all such disputes. All causes of action arising out of or In connection with these promotions shall be resolved lndlv!dually without resort to any form of class action l!Ugatlon and any and all clalms, judgments and awards shall be llmlted to actual, third-party, out of pocket costs and expenses Incurred but In no event wi!l attorneys' fees be awarded or recoverable. UNDER NO CIRCUMSTANCES Will ANY ENTRANT BE PERMITTED TO OBTAIN ANY AWARD FOR, ANO ENTRANT HEREBY KNOWINGLY ANO EXPRESSLY WAIVES All RIGHTS TO SEEK, PUNITIVE. INCIDENTAL, CONSEQUENTIAL OR SPECIAL DAMAGES, LOST PROFITS ANO/OR ANY OTHER DAMAGES, OTHER THAN ACTUAL OUT OF POCKET EXPENSES , ANO/OR ANY RIGHTS TO HAVE DAMAGES MULTIPLIED OR OTHERWISE INCREASED; ANO ENTRANTS' REMEDIES ARE LIMITED TO A CLAIM FOR MONEY DAMAGES jF ANY) AND ENTRANT IRREVOCABLY WAIVES ANY RIGHTTO SEEK INJUNCTWE OR EQUITABLE RELIEF. SOME JURISDICTIONS 00 NOT ALLOW THE LIMITATIONS OR EXCLUSION OF LIABILITY, SO THE ABOVE MAY NOT APPLY TO YOU.
Winner selection ex.ecuted at 60 E. 42nd St., NY, NY 10165. Ventura Associates, the Independent judging organization, has provided an prizes at no charge, Ventura Associates and/or Presenting Promoters reserve the right to modlly, cancel, suspend, or terminate these promotions If they become technlcally corrupted. In the event of termination, prizes wlll be awarded (If applicable) from eligible entries received prior to thls date of termination. Employees or Presenting Promoters, Ventura Associates, their respective advertising & promotion agencies & any other person or organlzat!on directly Involved with the promotions & their respective lmmedlete ramllles (spouse, parents, children, slbllngs and their spouses) and/or household members {whether related or not) of such employees are !ne11glble. The name, address, telephone number and email address, If available, provided by entrant to the Presenting Promoter will be forwarded to judging agency solely for Its use ln administering these promot!ons, and will be destroyed thereafter.
Thelnva!ldityorunenforceabllityofanyprovisicnoftheseofficlalruleswillnotaffecttheval!dityorenforceabllityofanyotherprov!slon. lntheeventthatanyprovisionoftheofficialrulesisdeterminedtobelnvalidorotherwlse unenforceable or Illegal, the other provisions will remain In eflect and will be construed In accordance with their terms as If the Invalid or Illegal provision were not contained herein. Any failure by Ventura Associates or any Presenting Promoter to enforce any term of these offlcial rules will not constitute a waiver of that provision. Entrants agree to waive any rights lo claim ambiguity of these ofl!cial rules,
MAIL PREFERENCE SERVICE: IF YOU WOULD PREFER NOT TO RECEIVE FUTURE SWEEPSTAKES MAILINGS FROM THIS PRESENTING PROMOTER, PLEASE WRITE TO NATIONAL ALZHEIMER'S COUNCIL (A PROGRAM OF THE EMERGENCY MEDICINE ASSOCIATION), P.O. BOX 1039, EDGEWOOD, MO 21040.
How Your Smwort ofNAC Could Help Someone You Love ... The National Alzheimer's Council is an outreach of the National Emergency Medicine Association, a 50 I (c)(3) nonprofit organization founded in 1982. Our Mission is the prevention of injury and illness by addressing health and social issues through education, applied research, technology, and equipment. "Prevention through Education" is the overall theme of our efforts, and we have become known for our educational health-related materials, which are free to schools, hospitals, health centers, and a wide array of social service programs.
For example, the information above was taken from the pocket book, "Alzheimer's - Hope Through Education" which was written and produced by the National Alzheimer's Council. Tl explains Alzheimer's, what we know today and what steps research suggests that we might lake today lo reduce the risk of Alzheimer's. If you or someone you love is concerned about Alzheimer's, we encourage you lo contact the National Alzheimer's Council today.
What is Alzheimer disease? Alzheimer disease, or Alzheimer's as it is also referred to, is the leading cause of dementia. Named after the person who first described it, Alzheimer disease may be defined as a set of symptoms that include loss of memory, judgement, reasoning ability, and often changes in behavior. With the aging of the "baby boomers" the incidence of Alzheimer's is expected to more than triple by the middle of the 21 sl century. Al the present time, Alzheimer's cannot be slopped or cured. Research however, is resulting in greater understanding of the disease and identification of steps that may reduce your risk of experiencing Alzheimer's.

17061 NAC lnst~nsert_Layout 1 112/19/14 3:29 P
CONSUMER DISCLOSURES YOU HAVE NOT YET WON THE GRAND PRIZE. ENTRY IS FREE. DONATING WILL NOT INCREASE YOUR CHANCES OF WINNING. YOU MAY OR MAY NOT HAVE A NUMBER THAT IS THE WINNING
1 NUMBER. ODDS THAT YOU ~ I WILL WIN THE GRAND PRIZE I
OF $9,467.38 WILL BE NO GREATER THAN XXX,XXX. ODDS THAT YOU WILL WIN THE ADDITIONAL PRIZE OF $100 DEPEND ON THE NUMBER OF ELIGIBLE ENTRIES RECEIVED.
NAC01/15
1
12147061 NAC BiJLWindow
1
2x3 Insert ~ne 12.19.20 Document Size: 2x3 Colors: black

17061 NAC lnsta~nsert_Layout 1 112/19/14 3:29 P
·u C: ::::J 0 u ti)
~i...
Cl)
E Cl) .c N
<t ca C: 0
~ z

I
IDE
NT
IFIC
AT
ION
CO
NF
IRM
ED
111111
111111
UIH I
IIH II
III III
H lltl
f HIU
1111 l
llt
NAM
E
ADD
RES
S
CITY
, ST.
ZIP
GIF
T E
NC
LOS
ED
D
YE
S
D N
O
REPL
Y BY
DEA
DLIN
E 1
J t
t, i'
7J fl
1 t.,
--,,
,,f-
v-l
:;:r
•JJ-f
::
'-"'
.'-'
-" =
•·----
FO
R P
RIZ
E E
NT
RY
1 $l
,000
,000.0
0PRI
2E
NA
TIO
NA
L A
LZ
HE
IME
R'S
CO
UN
CIL
PO
BO
X 2
1606
ST
. L
OU
IS,
MO
631
39-0
606
111 • 1•
11 I •ii 11
1' hi'
J n Ill
1hl•l
111 h I• 11 111 11
1I•I1
111111
11 • 11
•11
1214
7064
NAC
Inst
allm
ent
CR
E F
lat
siz
e=
8.8
75 x
3.8
75
" C
olo
rs=
Bla
ck,
PM
S 1
79
7
PLA
CE
STA
MP
HE
RE

TIM
E S
EN
SIT
IVE
-R
EP
LY
RE
QU
IRE
o··
Be
Sur
e To
... •
Pla
ce I
D L
abel
on
For
m •
Sig
n F
orm
•
Enc
lose
Gift
(O
ptio
nal)

Exhibit F.8
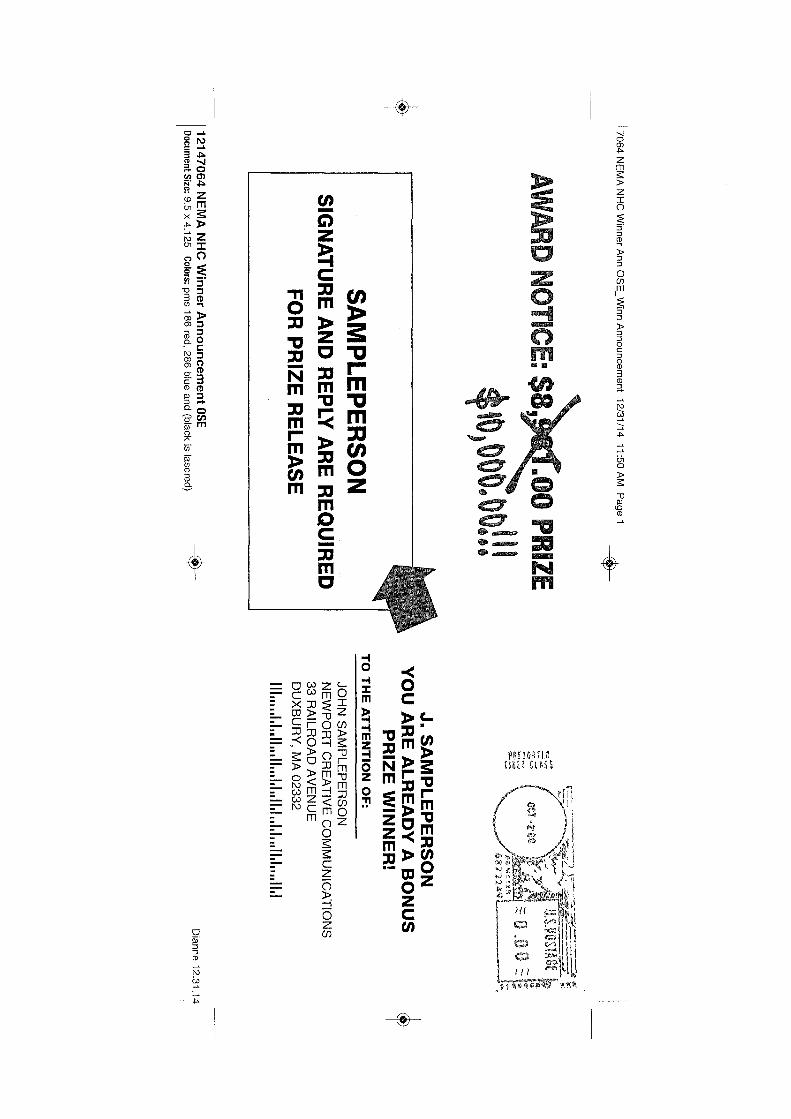
+ 70
64
NE
MA
NH
C W
inn
er A
nn OS
E_
Win
n A
nn
ou
nce
me
nt
12
/31
/14
11:50 AM
P
ag
e 1
~
AW
AR
D N
OTIC
E: $8
~ PRIZE
,o,ooo.oorn
SA
MP
LE P
ER
SO
N
SIG
NA
TU
RE
AN
D R
EP
LY A
RE
RE
QU
IRE
D
FO
R P
RIZ
E R
EL
EA
SE
1 12
14
70
64
NE
MA
NH
C W
inn
er An
no
un
ce
me
nt O
SE D
ocument Size: 9.5 x 4
.12
5
Colors: p
ms 1
86
red, 28
6 blue and (black is lasered)
~
- ~ ... ,,.,,. ~ ... ;,,,A•-
~<
..A1
>
«-''>
.......
~~
,,___
J. SA
MP
LE
PE
RS
ON
Y
OU
AR
E A
LR
EA
DY
A B
ON
US
P
RIZ
E W
INN
ER
! T
O T
HE
AT
TE
NT
ION
OF
:
JOH
N S
AM
PL
EP
ER
SO
N
NE
WP
OR
T C
RE
AT
IVE
CO
MM
UN
ICA
TIO
NS
33 R
AIL
RO
AD
AV
EN
UE
D
UX
BU
RY
, MA
02
33
2
11 Im I ,I, 1 .. II11111111I,I1111,1 .. I, I, .. II ,I, I
ll 11, I
Dianne 12.31.1 t +

+
17064 NEMA NHC Winner Ann FORM_Layout 1 1 /5/15 2:03 PM Page 1 +
John Sampleperson 33 Railroad Avenue Duxbury, MA 02332
JOHN SAMPLEPERSON'S WINNER ANNOUNCEMENT
Attention Mr. Sampleperson;
Yes, this is GOOD NEWS for you, JOHN SAMPLEPERSON ! You are in possession of a WINNING Prize Authorization Number.
Provide me your approval and I will send your GUARANTEED PRIZE to 33 Railroad Avenue in Duxbury, Massachusetts.
To claim your guaranteed bonus prize, sign and detach the Reply Form below and return it by April 15, 2015.
But, there's even more great news for the Sampleperson household. In a matter of weeks, you have the opportunity for another $10,000.00 and your name may already be on that $10,000.00 check. That's right:
Grand Prize Authorization Number XXXXX is registered in your name. Should you return the reply form below, the number on the reply form be the winning Prize Authorization Number, and you return it before the deadline, you would almost immediately receive the $10,000.00 cash. The number one reason why winners lose thousands of dollars every month is that they simply don't~ -
By April 15th, provided you have met the qualifications, you'll be the newest member of our Grand Prize Winners' Club. You'll join the others who are enjoying their new found wealth and realizing their financial dreams. Imagine ... a $10,000.00 check made payable to John Sampleperson.
Remember, you are already a confirmed winner and guaranteed to receive any and all prizes to which you are entitled. So, don't wait another minute. Think about it. Don't let time run out on your opportunity for the $10,000.00 Grand Prize. A contribution is not required and will not increase chances to win.
When you send your reply and claim your prize, please send along a gift of $7, $10, or even $5 to join in our effort to fight and win the battle against heart disease. This is your chance to win a major prize and help us put an end to needless suffering. Please, your help is desperately needed.
We'll be watching for your reply and stand ready to send you your prize.
P.S. The Reply Form is below. Return it today and please send alo the battle against heart disease.
small gift to help fight and win
V DETACH AT PERFDMTIDN 1' 1' DETACH AT PERFOMTIDN 1'
GRAND PRIZ~CH SAMPLEPERSON REPLY REQUIRED $10 000.00 c~
' RETURN THIS ENTRY FORM BY MIDNIGHT, APRIL 15, 2015
I am enclosing $ ___ to help fight heart disease D $7 D $5 D $10 D $25
Make check payable to: NATIONAL HEART COUNCIL OR NHC
SIGNATURE
11:+r SAMPLEPERSON J.~ JOHN
$10,000.00 GRAND PRIZE AUTHORIZATION NUMBER
xxxxx JOHN SAMPLEPERSON 33 RAILROAD AVENUE DUXBURY, MA 02332
xxxxxx 1234567890
B10/11/12
REPLY TODAY
1111111111111111111111
If for any reason you will not make a gift, please do not use this reply form. In that case. ~nly, write your name, address and Grand Pnze Authonzat1on Number on a piece of paper, sign 1t, and return 1t in the envelope provided. Giving is not required and will not improve chances to win.
1
12147064 NEMA NHC Winner Announcement FORM _{k___
Document Size: 8.5 x 14" Colors: PMS 100 Yellow, PMS 280 blue;t'-186 red and black lasers
+

+
17064 NEMA NHC Winner Ann FORM_Layoul 1 1/5/15 2:03 PM Page 2 +
NHC FACTS Solicitation For Charitable Purposes Card:
Your gift is very much appreciated and fully deductible as a charttable contribution. A copy of the summary of the latest financial statement, or annual report, and registration filed by NATIONAL EMERGENCY MEDICINE ASSOCIATION (NEMA), Qncorporated in Washington, D.C.), WITH ITS special program NATIONAL HEART COUNCIL (NHC) may be obtained by contacting us at The National Emergency Medicine Association, P.O. Box 1039, Edgewood, MD 21040 (443) 922-7533, If you are a resident of one of these states, you may obtain financial information directly from the state agency: FLORIDA-A COPY OF THE OFFICIAL REGISTRATION AND FINANCIAL INFORMATION MAY BE OBTAINED FROM THE DIVISION OF CONSUMER SERVICES BY CALLING TOLL-FREE, 1-800-435-7352 (800-HELP-FLA) WITHIN THE STATE. REGISTRATION DOES NOT IMPLY ENDORSEMENT, APPROVAL, OR RECOMMENDATION BY THE STATE. Florida Registration #CH313. GEORGIA-A full and fair description of the programs of NEMA and our financial statement summary is available upon request at the office and phone number indicated above. Maryland - For the cost of copies and postage, Oftlce of the Secretary of State, State House, Annapolis, MD 21401, MISSISSIPPI - The official registration and financial information of NEMA may be obtained from the Mississippi Secretary of State's office by calling 1-888-236-6167. Registration by the Secretary of State does not imply endorsement. NEW JERSEY - INFORMATION FILED WITH THE ATTORNEY GENERAL CONCERNING THIS CHARITABLE SOLICITATION AND THE PERCENTAGE OF CONTRIBUTIONS RECEIVED BY THE CHARITY DURING THE LAST REPORTING PERIOD THAT WERE DEDICATED TO THE CHARITABLE PURPOSE MAY BE OBTAINED FROM THE ATTORNEY GENERAL OF THE STATE OF NEW JERSEY BY CALLING (973) 504-6215 AND IS AVAILABLE ON THE INTERNET AT http://www.state,nj.us/lps/ca'chartrm.htm. REGISTRATION WITH THE ATTORNEY GENERAL DOES NOT IMPLY ENDORSEMENT. NEW YORK - Office of the Attorney General, Department of Law, Charities Bureau, 120 Broadway, New York, NY 10271, North Carolina - FINANCIAL INFORMATION ABOUT THIS ORGANIZATION AND A COPY OF ITS LICENSE ARE AVAILABLE FROM THE STATE SOLICITATION LICENSING BRANCH AT 1-888-830-4989. THE LICENSE IS NOT AN ENDORSEMENT BY THE STATE. PENNSYLVANIA- The official registration and financial information of NEMA may be obtained lrom the Pennsylvania Department ol State by calling toll-free, within Pennsylvania, 1-800-732-0999. Registration does not imply endorsement. VIRGINIA-Virginia Stale Division of Consumer Affairs, Department of Agricultural and Consumer Services, PO Box 1163, Richmond, VA 23218. WASHINGTON - Charities Division, Office of the Secretary of State, State of Washington, Olympia, WA 98504-0422, 1 ·800-332-4483. WEST VIRGINIA - Residents may obtain a summary of the registration and financial documents from the Secretary of State, State Capitol, Charleston, WV 25305. Registration with any ol these state agencies does not imply endorsement, approval or recommendation by any state.
I.
2,
),
4,
5,
6,
7,
SWEEPSTAKES FOR $8,981.00 GRAND PRIZE OFFICIAL RULES
rn,I\IT1>11u i,rrn,l\l IS REQUIRED * CONTRIBUTION WILL NOT IMPR,OVE {'.H)1N<:ES
Sponsor- this sweepstakes is sponsored by National Hcnrt Council, (a program of the Nutiomli Emergency Medicine Associution.) Phone: 443-922-7533 Address: P.O. Box I 039, Edgewood, MO 21040.
Prizes- there arc these three Prizes: I) Grand Prize of $10,000.00, 2) Guaranteed Prize Is a Colorful Calendar, Bookmark and Ruler 3) A Bonus Prize of $100,U0, Prizes are non-transfernble and there are no substitutes.
Entry lnslructions: - to enter with a donalion, return the reply form in the enclosed envelope postage pre-paid postmarked before the et\lry dendlme. To enter without a donation, follow directions on the reply form.
Prize Selection Procei;s I) Grand Prize: the winning entry wns randomly selected by nn independent ngency whose decision wns flnn! and binding before lhe promotion letters were mailed and were randomly seeded among mailed letters. lfyour eligible entry matche::: the pre-selected number, you will be notified that you have won 1he Grand Prize. 2) Guaranteed Prize: all entries will receive the guaranteed merchandise prize, 3) Bonus Prize: The winning entry will be randomly selected from all eligible entries received by the deadline dntc, The agency's decisions arc linal and binding.
Who is eligible - the sweepstakes is open to residenls ( 18 years or older) of the United States and its possessions who receive the mailing. Employees, agents, vendors and stnff or the Sponsol', National Heart Council (a program or the Nationn! Emergency Medicine Association.) Address: P.O. Box I 039, Edgewood, MD 21040, its advertising and promotional agencies, and sweepstakes administrator (and their household members) are not eligible to win. The entry form will not be honored if not mailed in the enclosed envelope with sufficient postage by the entry deadline.
Entry Deadline: - the deadline for mailing your entry is April 15, 2015. Postmark determines date of entry.
General - Sweepstakes void where prohibited by law. All federal, state and local regulations apply. Winners will be notified by mail. By participating, entrants agree to be bound by these rules. Failure to comply with these or any other Official Rules will result in disqualification. Winner must sign and return un affidavit + or eligibility, a liability release, and except where prohibited by law1 a publicity release within IO days of issuance of notification. If winner does not comply with the foregoing, or if a prize or prize notification is undeliverable, and/or if a selected winner does not comply with any portion of these Otncial Rules, such winner will be disqualified and, in the cuse of the Bonus Prize only, an alternate winner will be selected. Entrants agree that: I) Sponsor shall have right und permission to use (if a winner) entrant's name and city of residence for advertising, trade and/or other purposes in perpetuity without further compensation (unless prohibited by law); and 2) Sponsor, its advertising and promotion agencies and each of thelr respective officers, directors, employees, reprcscnt.itives and agents shall have no liability and will be held harmless by entrants for any linbility, loss, injury or damage to entrants or any other person or entity relating to this sweepstakes. Taxes sole responsibility of winner. Sponsor and its agencies arc not responsible for lute, !ost, or misdirected m11il or any printing or tcclmieul errors or mu I functions of any kind, by any human error that may occur in the processing of the entries in this Sweepstakes. [f for any reason \hat corrupts or affects the administration, security, fairness, integrity, or proper conduct of this Sweepstakes so that it is not capable ot' being conducted as described in these rules, Sponsor shall have lhe right, at its sole discretion, to cancel, terminate, modify or suspend the Sweepstakes. Any person who supplies false information, enters by fraudulent meons, or 1s
otherwise detcnnined to be in violation of these rules in an attempt to obtain any prize wi!! forfeit any prize won. No gift or p.iyment of any kind necessary to enter or win, Entries become the prope1ty of the Sponsor and will not be returned.
Winners - for the name of the Grand Prize winner, send a self-addressed stamped envelope to National Heart Council. Address: P.O. Box I 039, Edgewood. l'vlD 21040 on or within 60 days aner the entry deadline date.
9. Odds of Winning - I) Grand Prize: the number of entry fonns mailed determines the odds of winning. Your odds of winning will be no greater than 1 in XX,XXX. 2) Guaranteed Prize: Odds that you wil! win the Guaranteed Prize arc l in I. Your odds of winning the bonus prize arc dependent upon the number of qualifying entries received.
! 0. CrealiYe Presentations this sweepstakes may be mailed by NEMA with different creative presentations. The pre-selected winning Grand Prize number hos been selected from all entry numbers for all creative presentations, and the winning Bonus Prize number has been selected from all entries received for all creative presentations.
11. MaUlng List Suppressions- if you do not wish to receive mailings of this type In the future please write to: National Heart Council. Address: P.O. Box 1039, Edgewood, !HD 21040.
12. For additional information about this sweepstakes or sweepstakes in general, visit www.sweepstakesconsurncrguide.net.
WINNER ANNOUNCEMENT AND GRAND PRIZE ENTRY
I s10,ooo.oo I
+

+
17064 NEMA NH+er Ann INSRT_iayout 1 12/31/1
ODDS THAT YOU WILL WIN THE GUARANTEED PRIZE ARE 1 IN 1
FOR ELIGIBLE ENTRIES RECEIVED. YOU HAVE NOT YET WON THE GRAND PRIZE. ENTRY IS FREE.
DONATING WILL NOT INCREASE YOUR CHANCES OF WINNING.
YOU MAY OR MAY NOT HAVE A NUMBER THAT IS THE WINNING NUMBER. ODDS THAT YOU WILL
WIN THE GRANO PRIZE OF $10,000.00 WILL BE NO
GREATER THAN ONE IN YY,YXX. ODDS THAT YOU WILL WIN THE CONSOLATION PRIZE OF $100
ARE BASED UPON THE NUMBER OF ELIGIBLE ENTRIES RECEIVED.
NHC02/15
+
1
12147064 NEMA.:tW.C-Winner Annouj1cement 2x3 Insert Diannef'6,6.14 Colors: blrck

z ~ 0 z )> r I m )> JJ -I 0 0 C z 0 r























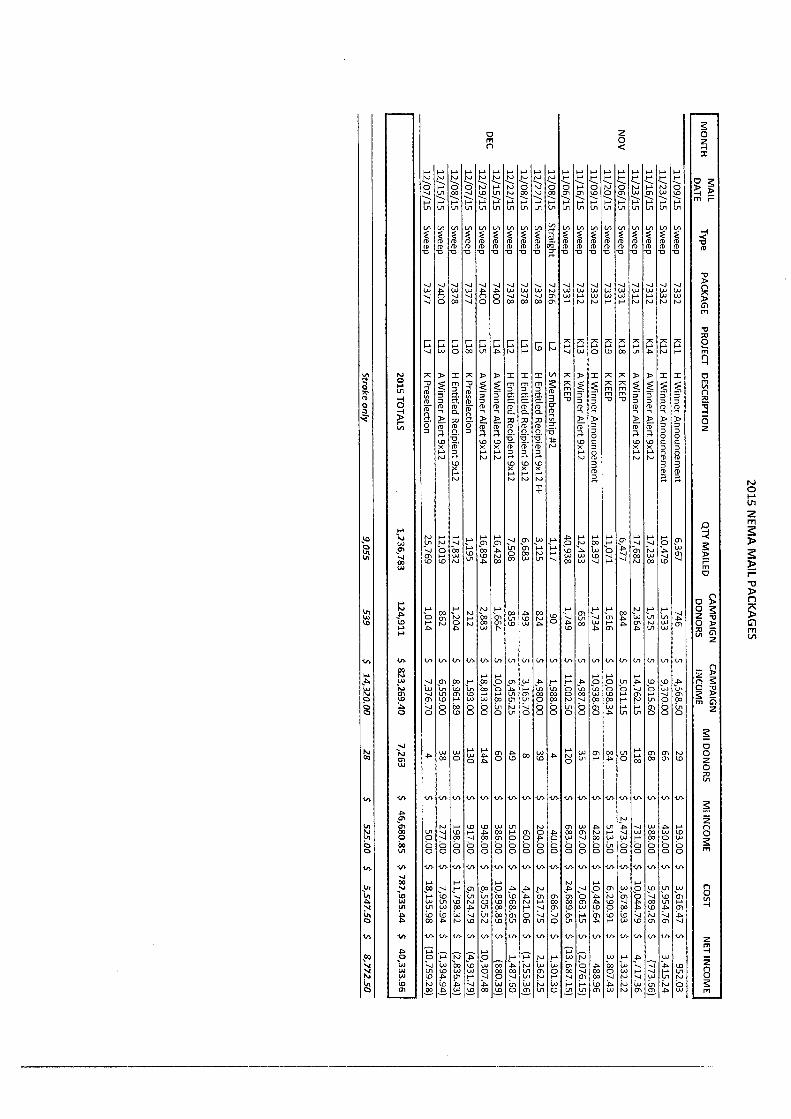

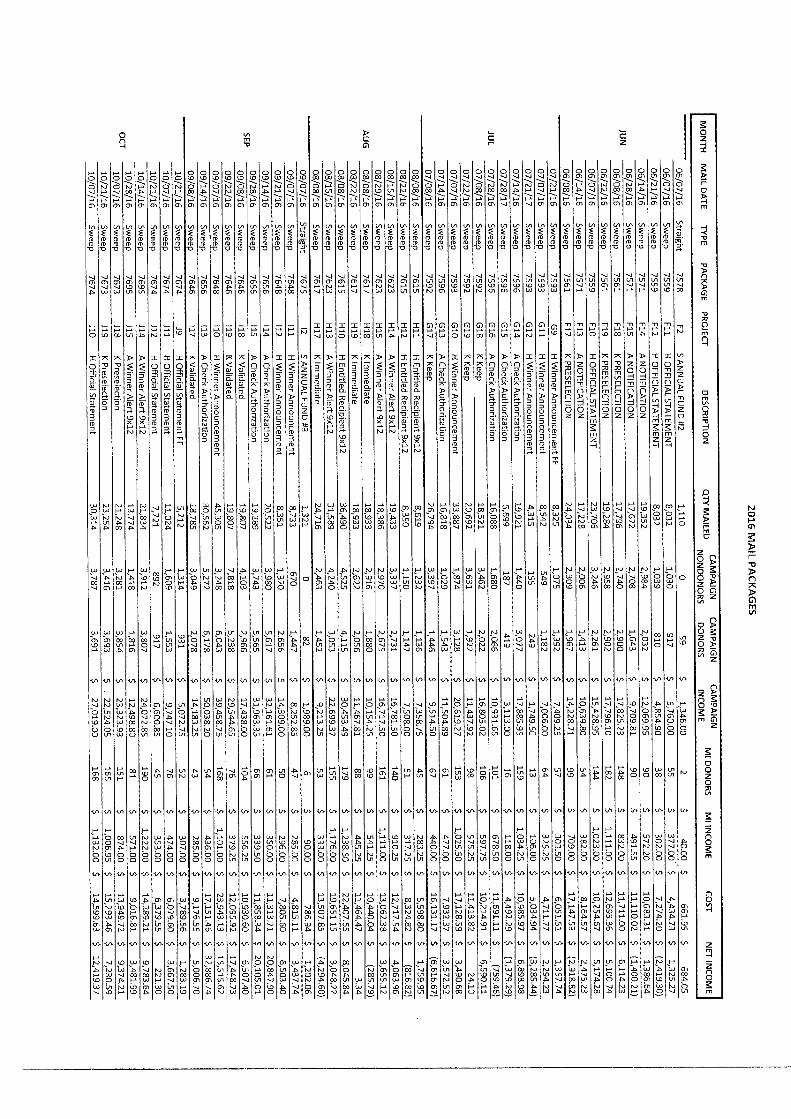

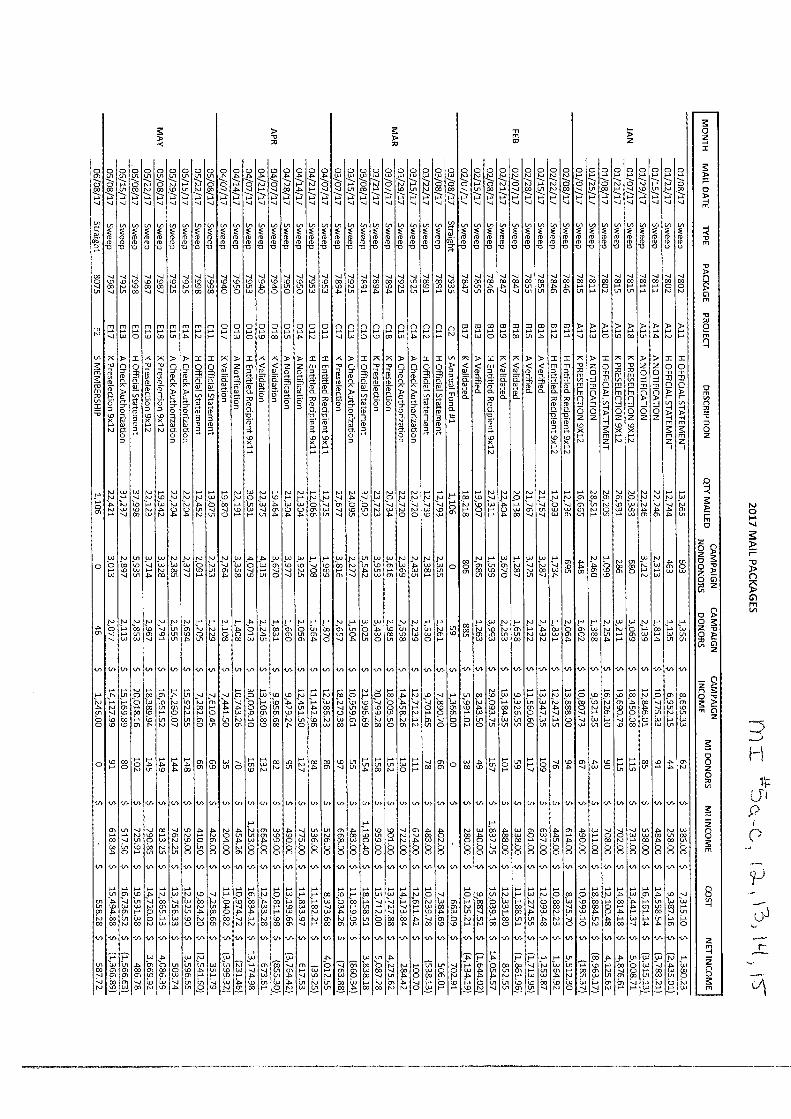





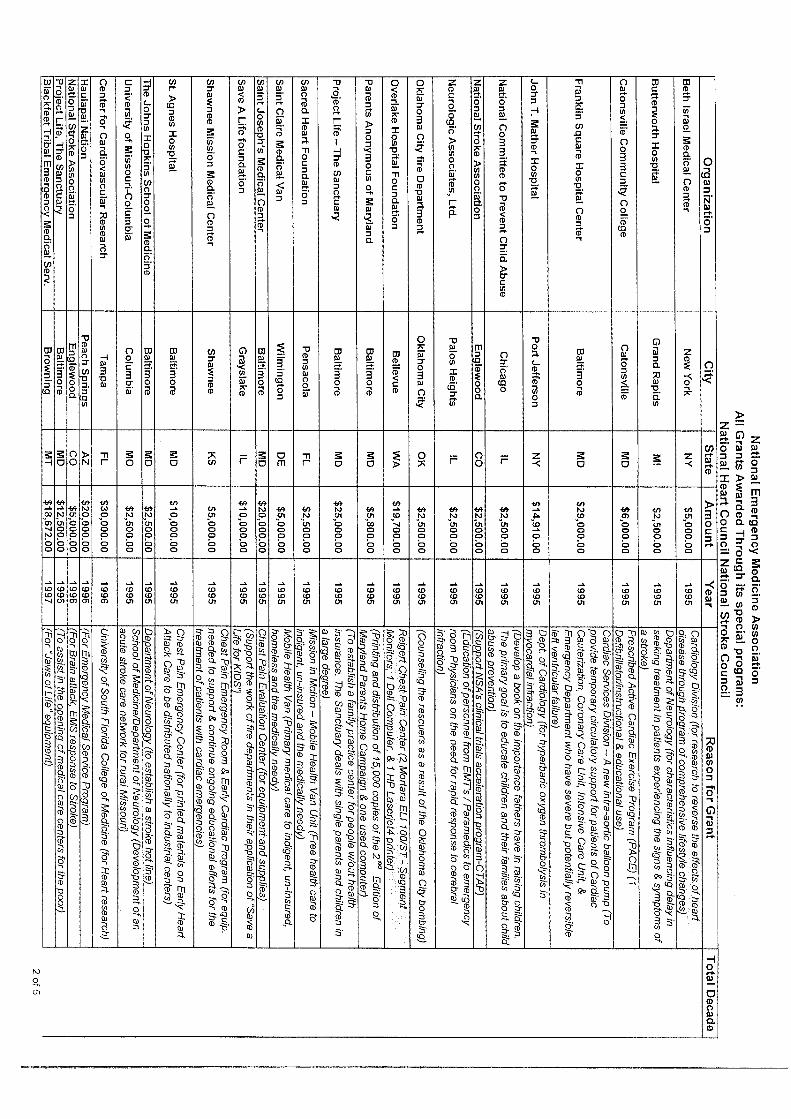

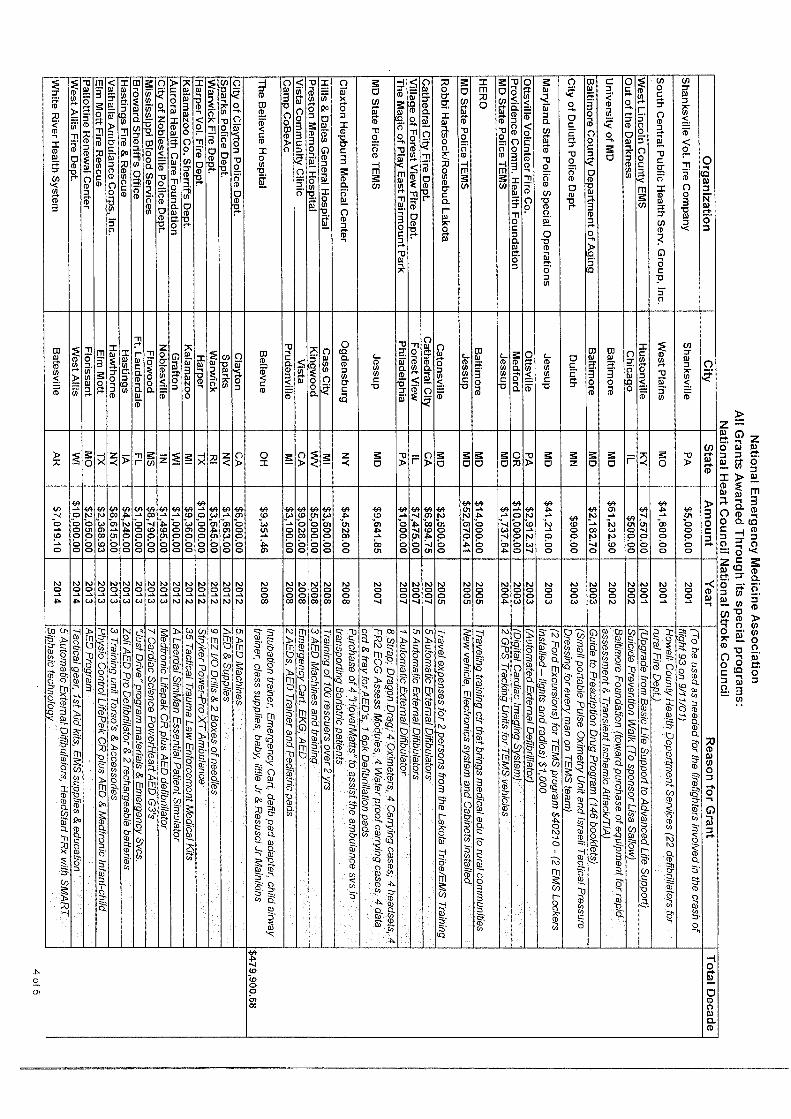



Exhibit I
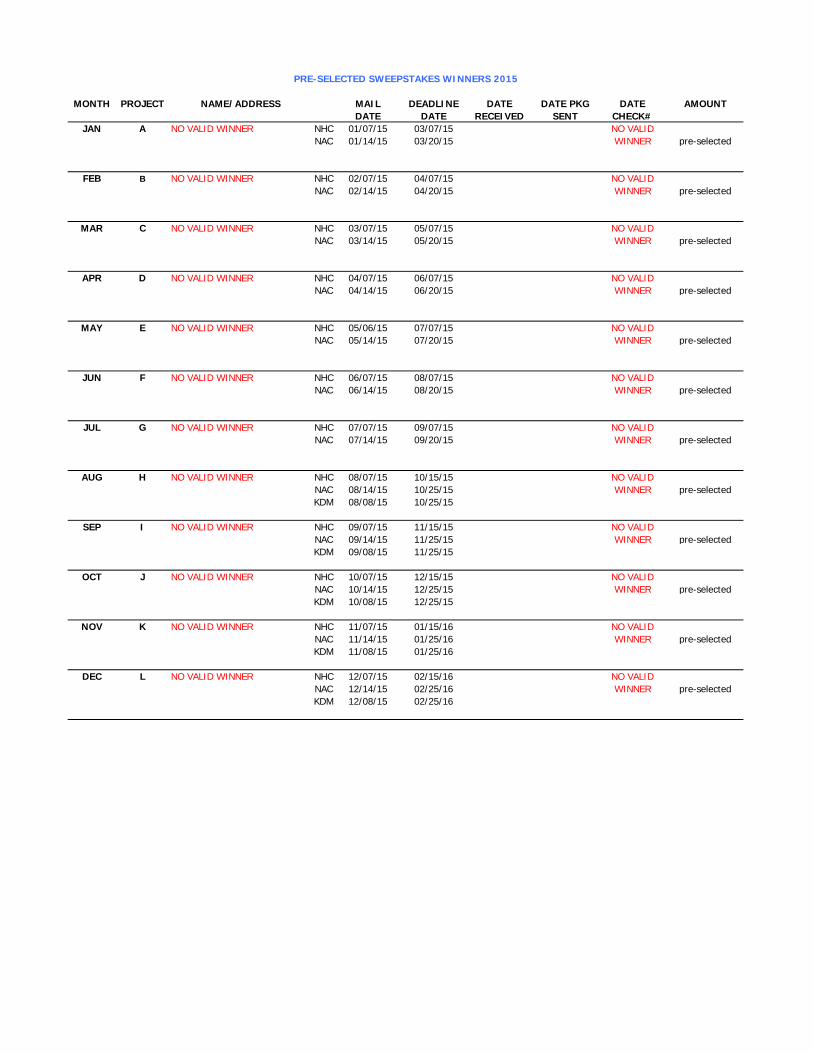
MONTH PROJECT NAME/ADDRESS MAIL DEADLINE DATE DATE PKG DATE AMOUNT
DATE DATE RECEIVED SENT CHECK#
JAN A NO VALID WINNER NHC 01/07/15 03/07/15 NO VALID
NAC 01/14/15 03/20/15 WINNER pre-selected
FEB B NO VALID WINNER NHC 02/07/15 04/07/15 NO VALID
NAC 02/14/15 04/20/15 WINNER pre-selected
MAR C NO VALID WINNER NHC 03/07/15 05/07/15 NO VALID
NAC 03/14/15 05/20/15 WINNER pre-selected
APR D NO VALID WINNER NHC 04/07/15 06/07/15 NO VALID
NAC 04/14/15 06/20/15 WINNER pre-selected
MAY E NO VALID WINNER NHC 05/06/15 07/07/15 NO VALID
NAC 05/14/15 07/20/15 WINNER pre-selected
JUN F NO VALID WINNER NHC 06/07/15 08/07/15 NO VALID
NAC 06/14/15 08/20/15 WINNER pre-selected
JUL G NO VALID WINNER NHC 07/07/15 09/07/15 NO VALID
NAC 07/14/15 09/20/15 WINNER pre-selected
AUG H NO VALID WINNER NHC 08/07/15 10/15/15 NO VALID
NAC 08/14/15 10/25/15 WINNER pre-selected
KDM 08/08/15 10/25/15
SEP I NO VALID WINNER NHC 09/07/15 11/15/15 NO VALID
NAC 09/14/15 11/25/15 WINNER pre-selected
KDM 09/08/15 11/25/15
OCT J NO VALID WINNER NHC 10/07/15 12/15/15 NO VALID
NAC 10/14/15 12/25/15 WINNER pre-selected
KDM 10/08/15 12/25/15
NOV K NO VALID WINNER NHC 11/07/15 01/15/16 NO VALID
NAC 11/14/15 01/25/16 WINNER pre-selected
KDM 11/08/15 01/25/16
DEC L NO VALID WINNER NHC 12/07/15 02/15/16 NO VALID
NAC 12/14/15 02/25/16 WINNER pre-selected
KDM 12/08/15 02/25/16
PRE-SELECTED SWEEPSTAKES WINNERS 2015

MONTH PROJECT NAME/ADDRESS MAIL DEADLINE DATE DATE PKG DATE AMOUNT
DATE DATE RECEIVED SENT CHECK#
JAN A NO VALID WINNER NHC 01/07/16 03/15/16 NO VALID
NAC 01/14/16 03/25/16 WINNER pre-selected
KDM 01/08/16 03/25/16
FEB B NO VALID WINNER NHC 02/07/16 04/15/16 NO VALID
NAC 02/14/16 04/25/16 WINNER pre-selected
KDM 02/08/16 04/25/16
MAR C NO VALID WINNER NHC 03/07/16 05/15/16 NO VALID
NAC 03/14/16 05/25/16 WINNER pre-selected
KDM 03/08/16 05/25/16
APR D NO VALID WINNER NHC 04/07/16 06/15/16 NO VALID
NAC 04/14/16 06/25/16 WINNER pre-selected
KDM 04/08/16 06/25/16
MAY E NO VALID WINNER NHC 05/06/16 07/15/16 NO VALID
NAC 05/14/16 07/25/16 WINNER pre-selected
KDM 05/08/16 07/25/16
JUN F NO VALID WINNER NHC 06/07/16 08/15/16 NO VALID
NAC 06/14/16 08/25/16 WINNER pre-selected
KDM 06/08/16 08/25/16
JUL G NO VALID WINNER NHC 07/07/16 09/15/16 NO VALID
NAC 07/14/16 09/25/16 WINNER pre-selected
KDM 07/08/16 09/25/16
AUG H NO VALID WINNER NHC 08/07/16 10/15/16 NO VALID
NAC 08/14/16 10/25/16 WINNER pre-selected
KDM 08/08/16 10/25/16
SEP I NO VALID WINNER NHC 09/07/16 11/15/16 NO VALID
NAC 09/14/16 11/25/16 WINNER pre-selected
KDM 09/08/16 11/25/16
OCT J NO VALID WINNER NHC 10/07/16 12/15/16 NO VALID
NAC 10/14/16 12/25/16 WINNER pre-selected
KDM 10/08/16 12/25/16
NOV K NO VALID WINNER NHC 11/07/16 01/15/17 NO VALID
NAC 11/14/16 01/25/17 WINNER pre-selected
KDM 11/08/16 01/25/17
DEC L NO VALID WINNER NHC 12/07/16 02/15/17 NO VALID
NAC 12/14/16 02/25/17 WINNER pre-selected
KDM 12/08/16 02/25/17
PRE-SELECTED SWEEPSTAKES WINNERS 2016

MONTH PROJECT NAME/ADDRESS MAIL DEADLINE DATE DATE PKG DATE AMOUNT
DATE DATE RECEIVED SENT CHECK#
JAN A NO VALID WINNER NHC 01/07/17 03/15/17 NO VALID
NAC 01/14/17 03/25/17 WINNER pre-selected
KDM 01/08/17 03/25/17
FEB B NO VALID WINNER NHC 02/07/17 04/15/17 NO VALID
NAC 02/14/17 04/25/17 WINNER pre-selected
KDM 02/08/17 04/25/17
MAR C NO VALID WINNER NHC 03/07/17 05/15/17 NO VALID
NAC 03/14/17 05/25/17 WINNER pre-selected
KDM 03/08/17 05/25/17
APR D NO VALID WINNER NHC 04/07/17 06/15/17 NO VALID
NAC 04/14/17 06/25/17 WINNER pre-selected
KDM 04/08/17 06/25/17
MAY E NO VALID WINNER NHC 05/06/17 07/15/17 NO VALID
NAC 05/14/17 07/25/17 WINNER pre-selected
KDM 05/08/17 07/25/17
JUN F NO VALID WINNER NHC 06/07/17 08/15/17 NO VALID
NAC 06/14/17 08/25/17 WINNER pre-selected
KDM 06/08/17 08/25/17
JUL G NO VALID WINNER NHC 07/07/17 09/15/17 NO VALID
NAC 07/14/17 09/25/17 WINNER pre-selected
KDM 07/08/17 09/25/17
AUG H NO VALID WINNER NHC 08/07/17 10/15/17 NO VALID
NAC 08/14/17 10/25/17 WINNER pre-selected
KDM 08/08/17 10/25/17
SEP I NO VALID WINNER NHC 09/07/17 11/15/17 NO VALID
NAC 09/14/17 11/25/17 WINNER pre-selected
KDM 09/08/17 11/25/17
OCT J NO VALID WINNER NHC 10/07/17 12/15/17 NO VALID
NAC 10/14/17 12/25/17 WINNER pre-selected
KDM 10/08/17 12/25/17
NOV K NO VALID WINNER NHC 11/07/17 01/15/18 NO VALID
NAC 11/14/17 01/25/18 WINNER pre-selected
KDM 11/08/17 01/25/18
DEC L NO VALID WINNER NHC 12/07/17 02/15/18 NO VALID
NAC 12/14/17 02/25/18 WINNER pre-selected
KDM 12/08/17 02/25/18
PRE-SELECTED SWEEPSTAKES WINNERS 2017


















