Nose, sinus, nasopharynx Dr K Outhoff. Contents Allergic Rhinitis Nasal furunculosis Epistaxis Local...
34
Nose, sinus, nasopharynx Dr K Outhoff
-
Upload
verity-james -
Category
Documents
-
view
269 -
download
1
Transcript of Nose, sinus, nasopharynx Dr K Outhoff. Contents Allergic Rhinitis Nasal furunculosis Epistaxis Local...
Nose, sinus, nasopharynxDr K Outhoff
Contents
• Allergic Rhinitis• Nasal furunculosis• Epistaxis• Local anaesthetic drugs• Rhinosinusitis– Viral– Bacterial– Fungal
• Iatrogenic conditions
A. Nasal Obstruction
• Viral URTI • Adults :– Deflected nasal septum– Polyps– Granulomatous disease -TB, Syph, Lep– Rhinitis– Chronic sinusitis– Iatrogenic – topical vasoconstrictors, reserpine,
TCA’s
A. Nasal obstruction
• Children: – large adenoids– choanal atresia– post nasal space tumours (angiofibromata)– foreign body– rhinitis

Allergic rhinitis
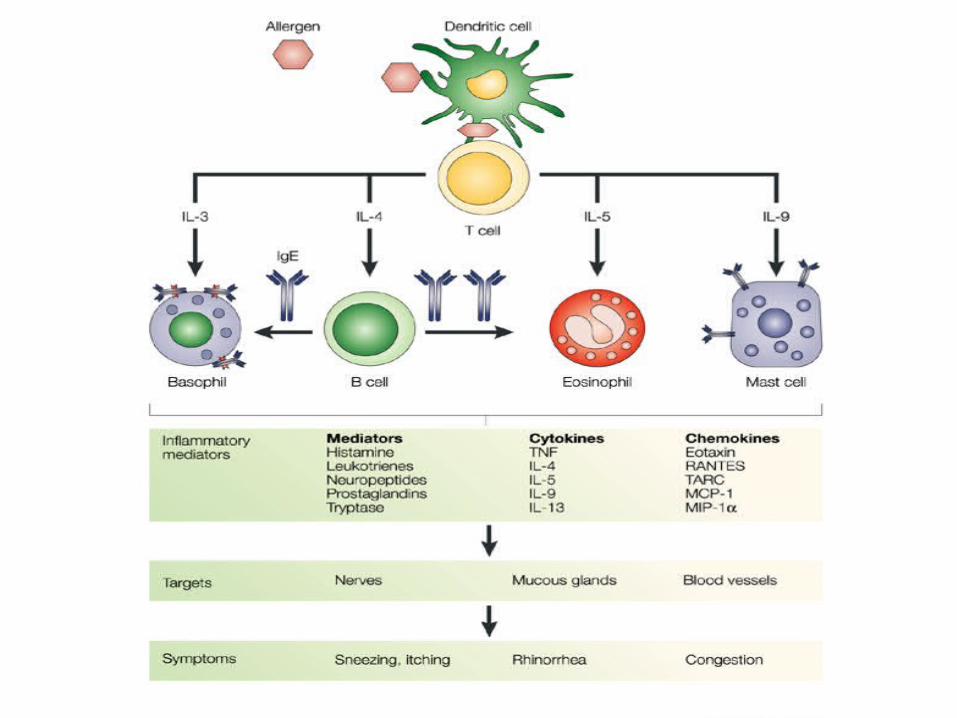
Allergic rhinitis
• Sneezing, pruritus, rhinorrhoea, swollen turbinates, nasal polyps
• Treatment options1. Topical nasal corticosteroids2. Topical antihistamines3. Systemic antihistamines
4. Topical sympathomimetics (pseudoephedrine)5. Prophylactic nasal sprays – Sodium cromoglycate6. Desensitizing injections ( anaphylaxis)
Topical corticosteroid nasal spraysmainstay of treatment
• Effective, fewer side effects than oral or parenteral routes, minimal absorption from nasal mucosa
• Reduce swelling and stuffiness• Take a few days to work at full potential
– Beclomethasone– Budesonide– Triamcinolone– Mometasone– Fluticasone
(may dry nasal mucosa; crusting, bleeding)
Histamine • Found largely in mast cell and basophil granules in skin, lungs,
GIT• and histaminergic neurones in brain• Mediator of hypersensitivity response• Acts on H-1 receptors:– Contracts smooth muscle (ileum, bronchioles, uterus)– Dilates blood vessels– Increased vascular permeability– Itching from sensory neuronal stimulation
Topical antihistamines (H-1) for allergic rhinitis
• Azelastine:– Also inhibits release of inflammatory cytokines
• Levocabastine:– Long acting– For short term symptomatic treatment
Systemic Antihistamines (H-1)• ↓rhinorrhoea• sneezing, • eye symptoms• Not as effective as steroids for nasal congestion
Newer antihistamines: relatively free of sedation, alcohol, benzo potentiation as do not cross BBB
• Chlorpheneramine (Allergex – old generation)• Cetirizine (Zyrtec)• Levocetirizine• Loratidine• Desloratidine• Fexofenadine
Systemic antihistamines
• Well absorbed• Metabolised in liver• Excreted in urine• Older antihistamines:
Peripheral anti-muscarinic effects : dryness of mouth, blurred vision, constipation, urinary retention, and sedation
• Newer antihistamines: Less sedating, prolongation QT interval
Topical sympathomimetic decongestants
• Oxymetazoline (Iliadin N/Spray)• Xylometazoline• Ephedrine –containing preparations
– Vasoconstrictors, ↓oedema– Useful if severe congestion preventing topical
steroids, cromoglycate from working
– Limit use to 2-3 days – Beware rhinitis medicamentosa
Sodium Cromoglycate nasal spray / drops
• May be used for allergic conjunctivitis and rhinitis• Prevents release of mediators from mast cells• Mucous membranes less sensitive to allergens• Use long term, preventative• Well tolerated• Short lived sneezing, nasal irritation
• NO LONGER AVAILABLE IN RSA as nose drops. (eye drops still available)
Systemic corticosteroids
• Intractable, severe allergic rhinitis• Short course oral prednisolone• Anti-inflammatory• Prolonged use can suppress adrenal production of
corticosteroids• Abrupt discontinuation →nausea, vomiting, shock• Mask signs of infection• Impair natural immune response to infection• For specialist use only
• SAMF 2008: ‘systemic steroids have no role in the routine management of allergic rhinitis’
Systemic corticosteroids cont...
• Impair calcium absorption, new bone formation
• Short course prednisolone well tolerated• Prolonged use: fluid retention, weight gain,
potassium loss, headache, muscle weakness, peptic ulceration, easy bruising, convulsions, psychiatric symptoms, etc!
Nasal furunculosis
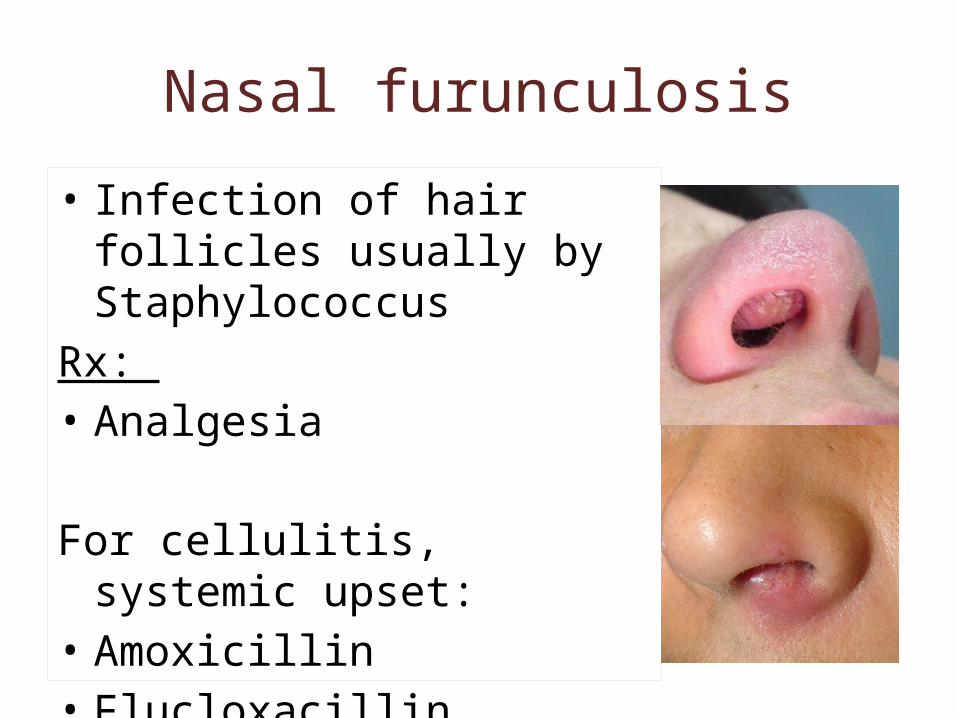
• Infection of hair follicles usually by Staphylococcus
Rx: • Analgesia
For cellulitis, systemic upset: • Amoxicillin• Flucloxacillin
Drug treatment of Epistaxis
• First aid, ice, transfusion• 2.5-10% Cocaine solution
nasal spray: anaesthetises and constricts vessels
• Anterior ribbon gauze pack with paraffin, iodoform paste
• Posterior pack
Local Anaesthetic Drugs I: Cocaine
surface local anaestheticreuptake inhibitor of sympathomimetic amines:• intense vasoconstriction• mydriasis of pupil• anxiety• tremor• euphoria
Local Anaesthetic Drugs II: Lignocaine: • IV regional anaesthesia• Infiltration anaesthesia (with or without vasoconstrictor, adrenaline)• Epidural anaesthesia• Topical anaesthesia
– Spray– Gel
Rapid diffusion through tissues (2-3min)Duration of action: 1-3 hours
• Side effects: dose related: – Dizziness, agitation– Drowsiness, respiratory depression, convulsions– Heart block: direct effect– Nausea, vomiting, transient tinnitus
• amide-type local anaesthetic
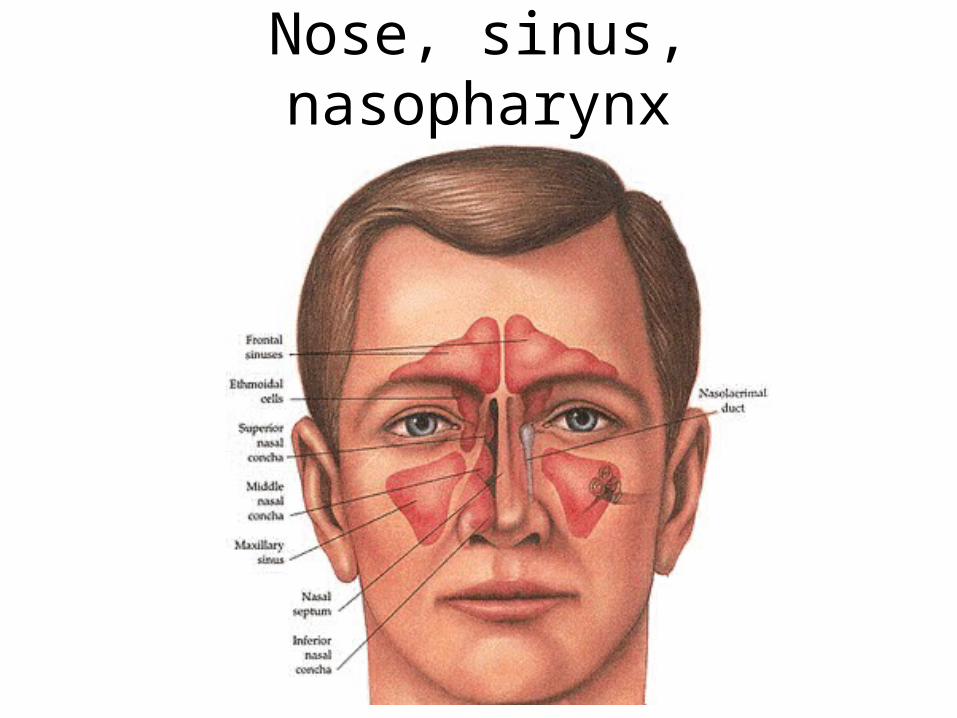
Paranasal sinuses
• Ciliated cells sweep mucous into nose• Viral infections depress cilia activity• Cause oedema around sinus ostia to nose• Collection of stagnating mucous• May become secondarily infected by bacteria
• Polyps, deflected septum, nasal mucosal swelling, tooth roots, also predispose.
Rhinosinusitis
• Viral– Acute: no antibiotics
• Bacterial– Acute: see next– Chronic: culture for anaerobes (Bacteroides) and
Staphylococcus• Fungal– Invasive– Non-invasive
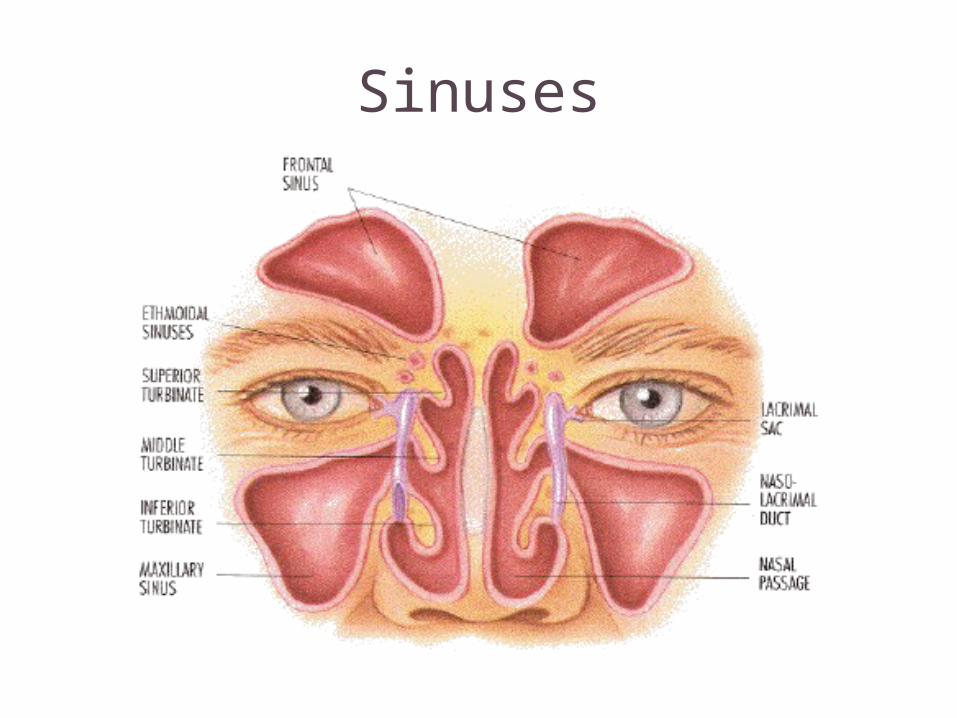
Sinuses
Acute bacterial sinusitis (ABS)• Fever, pain, tenderness, discoloured nasal discharge• Aetiology:
– S. pneumoniae – H. Influenzae – Moraxella catarrhalis (consider if no rapid clinical response)
Rx: • Analgesia• Antibiotics:
– Amoxicillin 10 days (first choice) or – Co-amoxiclav 10 days if failed therapy
– Penicillin allergy: erythromycin / clarithromycin/ moxifloxacin
• (decongestant nasal drops – eg pseudoephedrine)
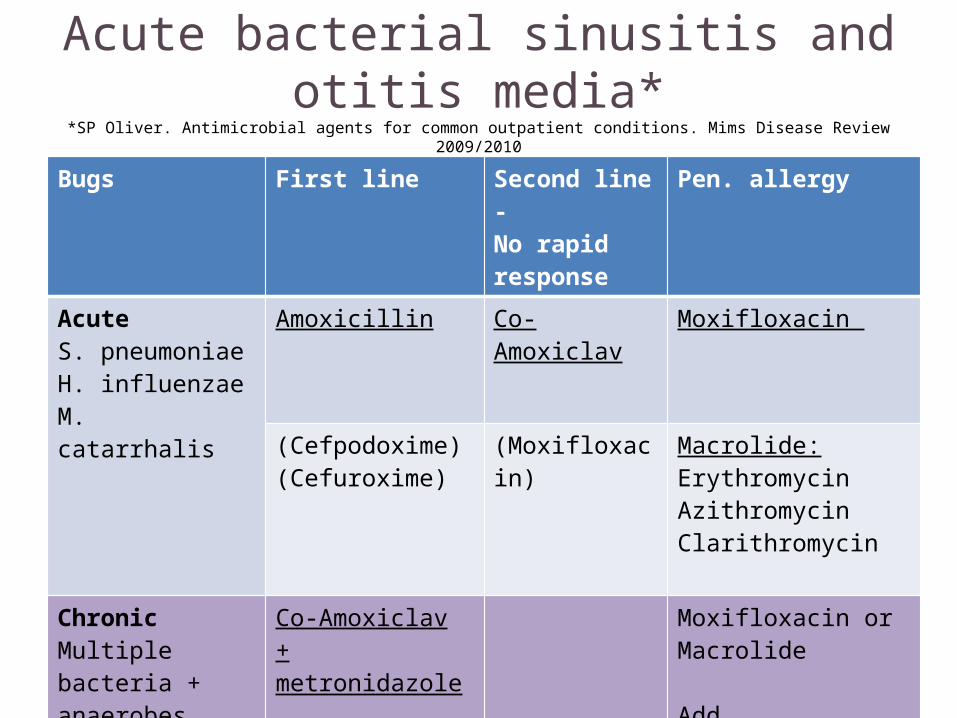
Acute bacterial sinusitis and otitis media**SP Oliver. Antimicrobial agents for common outpatient conditions. Mims Disease Review 2009/2010
Updated guidelines for the management of URTI in SA 2008 SA Fam Prac 2009
Bugs First line Second line -No rapid response
Pen. allergy
AcuteS. pneumoniaeH. influenzaeM. catarrhalis
Amoxicillin Co-Amoxiclav Moxifloxacin
(Cefpodoxime)(Cefuroxime)
(Moxifloxacin) Macrolide:ErythromycinAzithromycinClarithromycin
ChronicMultiple bacteria +anaerobes
Co-Amoxiclav+ metronidazole
Clindamycin?
Moxifloxacin orMacrolide
Add Metronidazole
Amoxicillin
• Beta-lactam penicillin• Inhibits bacterial cell wall synthesis• Stomach upset• Allergic reactions
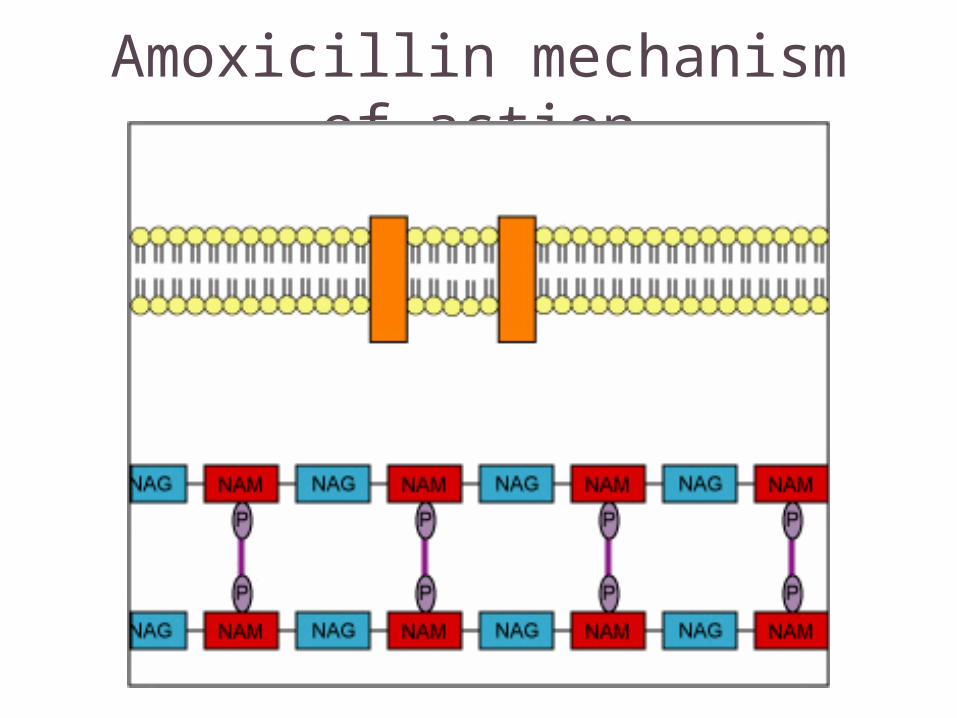
Amoxicillin mechanism of action
Fungal sinusitis
• Recently been blamed for causing most cases of chronic rhinosinusitis
• Most are benign except when occur in immuno-compromised patients where they become invasive (acute and chronic)
• Prognosis is different for each• Pathogens:
– Aspergillus and– Mucor species
Rx: Surgical debridement for all.Adjuvant medical
Ramadan HH. Fungal sinusitis 2009. emedicine. medscape.com
Fungal sinusitis:adjuvant drug therapy
Allergic fungal sinusitis and sinus mycetoma:• Surgical treatment only
Acute and Chronic invasive fungal sinusitis:• Initiate systemic antifungals
– Amphotericin B ivi– Replace with oral ketaconazole or itraconazole once disease
under control
Chronic granulomatous fungal sinusitis:• Surgical debridement followed by systemic antifungal
medication
Iatrogenic / drug induced conditions I• Blocked nose: (↑NA): TCA’s, reserpine,
vasoconstrictors
• Rhinorrhoea: ↑Ach with physostigmine (acetylcholine esterase inhibitor, glaucoma Rx)
• Epistaxis: beclomethasone, ipratroprium bromide (antimuscarinic), ASPIRIN, warfarin
• Immunosuppression: prolonged systemic corticosteroids, chemotherapy
Iatrogenic / drug induced conditions II
• Septum perforation: steroids post Ø, cocaine
• Drying of nasal mucosa: ipratropium bromide, beclomethasone inhaler
• Nasal polyps: chronic drug allergy, aspirin
• Rhinitis medicamentosa: sympathomimetic vasoconstricting decongestants
Rhinitis medicamentosa
• Iatrogenic obstruction• Decongestant vasoconstrictive sprays or drops• Damage mucosa (anoxia)• Rebound engorgement• Mucosal oedema• Further drug use• Vicious cycle
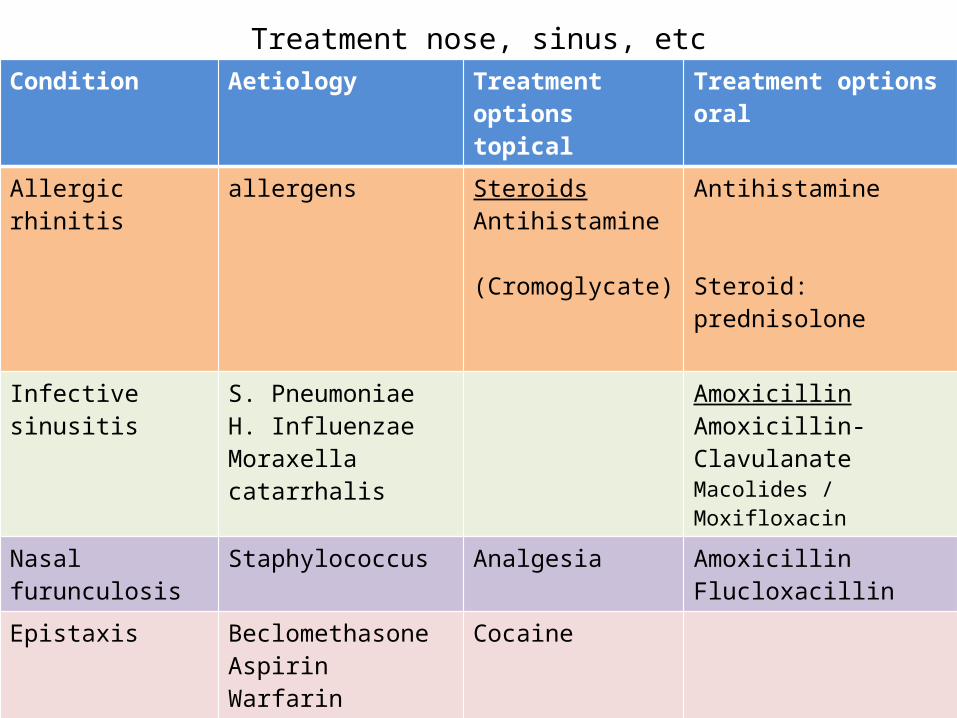
Treatment nose, sinus, etcCondition Aetiology Treatment options
topicalTreatment options oral
Allergic rhinitis allergens SteroidsAntihistamine
(Cromoglycate)
Antihistamine
Steroid: prednisolone
Infective sinusitis S. PneumoniaeH. InfluenzaeMoraxella catarrhalis
AmoxicillinAmoxicillin-ClavulanateMacolides / Moxifloxacin
Nasal furunculosis Staphylococcus Analgesia AmoxicillinFlucloxacillin
Epistaxis BeclomethasoneAspirinWarfarinAntimuscarinics
Cocaine
Rhinitis medicamentosa
Sympathomimetic vasoconstricting decongestants
Stop drugs