
Northern England Strategic Clinical Network Conference 15 th May 2015 Update - Head and Neck Site...
19
Northern England Strategic Clinical Network Conference 15 th May 2015 Update - Head and Neck Site Specific Group Eleanor Aynsley Clinical Oncologist
-
Upload
vernon-knight -
Category
Documents
-
view
214 -
download
1
Transcript of Northern England Strategic Clinical Network Conference 15 th May 2015 Update - Head and Neck Site...

Northern England Strategic Clinical Network Conference
15th May 2015
Update - Head and Neck Site Specific Group
Eleanor AynsleyClinical Oncologist
Robotic surgery (TORS)
• Currently being used in Newcastle by Mr Vin Paleri for selected cases for selected oropharynx cases, approx 50 cases operated on
• Presented findings at 1 international and 2 national meetings
• Quicker operation time, shorter inpatient stay• Can operate on cases may not otherwise be able to• Hope to be operational in James Cook and Sunderland
in near future


Intensity Modulated RadiotherapyIMRT
• Standard for complex head and neck cases in Newcastle and Middlesbrough
• Still not in Carlisle, although offered to go to Newcastle
• Rolling out IMRT for all head and neck cases

CF 71 year old lady
• Presented with lump in left neck• PMH of hypertension and OA• Smoked 10 a day, occasional alcohol• PS 2• Histology squamous cell ca


• Had 3 cycles of neoadjuvant chemotherapy (cisplatin and 5FU) with a partial response
• 65 Gy in 30 fractions to PTV1 which was the larynx and left levels Ib to V and 54 Gy in 30 fractions to PTV2 which was right levels II to IV plus 3/6 weekly Cisplatin chemotherapy cycles.
• Was dizzy during treatment and required peg feeding
• Following treatment managing soft diet





Survivorship• Recognition important due to long term side effects of
radiotherapy such as dysphagia and after effects of surgery eg laryngectomy affecting speech and body image
• National Cancer Survivorship Initiative (collaborative between NHS England and Macmillan) has 4 main aims:1. Holistic needs assessment (HNA) to be done on all patients
at diagnosis and any other time appropriate (key times-post treatment and again 6 months after treatment ) All
2. Treatment summary Sunderland3. Cancer care review-by GP4. Health and wellbeing clinics/educational events /signposting
patients
Holistic needs assessment
Should cover the following: • Addressing any physical or practical concerns• Signposting to either local or national support groups• Information about local Health and Wellbeing Clinics, Education Events or
self management courses as available in your area.• Referral to Allied Healthcare Professionals for support if required• Advice related to lifestyle i.e. Stop smoking services• Information or referral to an appropriate physical activity programme• Information or referral for advice on diet and nutrition• Referral for counselling or psychological support• Support related to work and finance concerns• Support for spiritual needs

Clinical trials
• Head and neck 5000 recruited very well across network
• Other trials helping quality assurance of radiotherapy and surgery

SEND The role of selective neck dissection used electively in patients with early oral squamous cell carcinoma (tumour stage T1 and
T2) and no clinical evidence of lymph node metastases in the neck
. T1/T2 N0 SqCC oral cavity
Randomisation1:1
Resection of primary with simultaneousneck dissection at
presentation
Resection of primary tumour alone and
salvage treatment of neck if neck metastases develop
CI: Prof Ian Hutchison
→ plan for merged data analysis with similar RCT Tata Memorial Hospital, Mumbai – 330 patients/460 in total (of 650)

ART-DECO A Multicentre Randomised Study of Dose Intensity Modulated Radiotherapy Versus Standard Dose Radiotherapy in
Patients with Locally Advanced Laryngeal and Hypopharyngeal Cancers.
Induction chemotherapy [Optional by centre]
Diagnosis oflocallyadvancedsquamous cellcancer of thelarynx orhypopharynxrequiringdefinitiveTreatment WithRT or chemoradiotherapy
Dose escalated IMRT
67.2Gy in 28 fractions to the involved site and nodal groups56Gy in 28 fractions to nodal areas at risk of harbouring microscopic disease.
Standard dose IMRT
65Gy in 30 fractions to involved site and nodal groups54 Gy in 30 fractions to nodal areas at risk of harbouring microscopic disease.
Patients may receive a maximum of 3 (21 day) cycles of platinum based induction chemotherapy prior to radiotherapy
Concomitant cisplatin(Day 1 and Day 29)[All patients]
R
CI: Prof Chris Nutting RMH

Screen 910 biopsies from T3-T4NO, T1-4,N1-2 oropharynx SCC
HPV+ on PCR AND
p16+ on immunohistochemistry
(Central MHRA-approved Laboratory)
Randomise 330 patients 1:1Control
Concomitant Cisplatin
+ Radiotherapy (70 Gy in 30 F)
Study
Concomitant Cetuximab
+ Radiotherapy (70 Gy in 30 F)Stratified by Centre,
Tumour site, T & N stage, Smoking status
10% Lost to follow up (n=17) 10% Lost to follow-up (n=17)
Analysed (n= 148) Analysed (n= 148)
Follow-up: 2 years
Primary outcomes: Overall survival
Severe Acute and Late Toxicity: using CTCAE grading, including skin rashes, mucositis
Secondary outcomes:
Health economics using EQ-5D, Early toxicity, Quality of life: using EORTC general and head neck specific modules, Swallowing: using MDADI questionnaire and gastrostomy - dependency rates, Mortality (cause of death), disease free survival, recurrence, metastases.
Key: HPV – Human Papilloma Virus PCR – polymerase chain reaction
CTCAE – Common Terminology Criteria for Adverse Events version 3.0
MDADI – MD Anderson Dysphagia Inventory
De-escalate
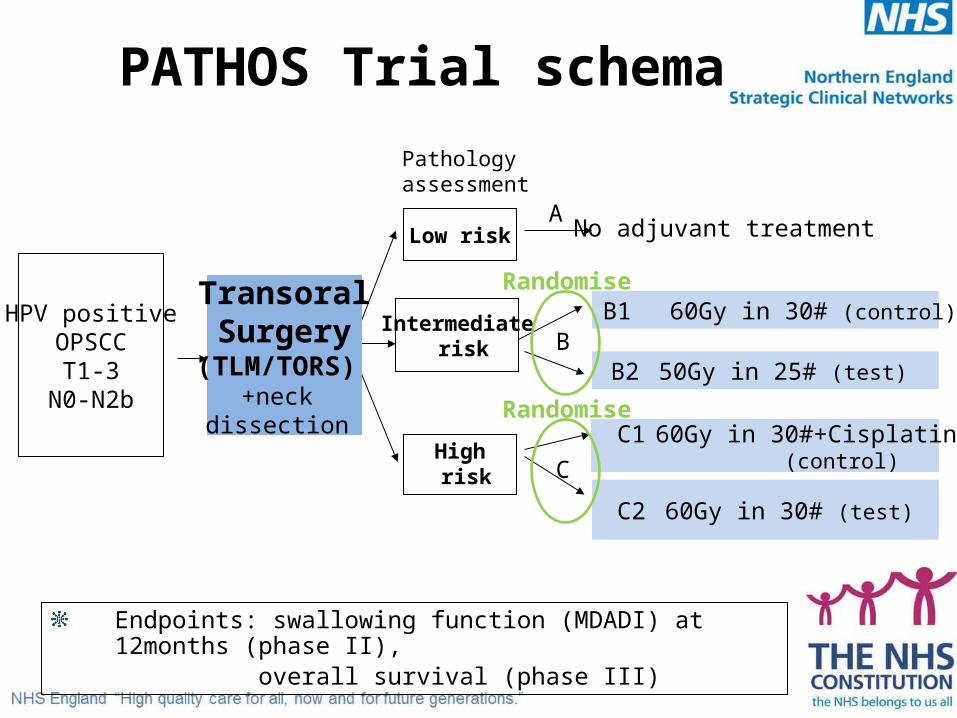
PATHOS Trial schema
No adjuvant treatment
HPV positiveOPSCCT1-3
N0-N2b
Low risk
Pathology assessment
Intermediate risk
High risk
B1 60Gy in 30# (control)
B2 50Gy in 25# (test)
C1 60Gy in 30#+Cisplatin (control)
C2 60Gy in 30# (test)
TransoralSurgery
(TLM/TORS) +neck
dissection
Endpoints: swallowing function (MDADI) at 12months (phase II), overall survival (phase III)
A
B
C
Randomise
Randomise

Any questions?


















