North West London Trauma Network Spinal Pathway and ... fileNorth West London Trauma Network 4 Acute...
12
North West London Trauma Network 1 Acute Spinal Injury Pathway v1.0 December 2014 North West London Trauma Network Spinal Pathway and Protocols 1. Spinal Clearance in the Trauma Patient Inclusions: All trauma patients who are not alert and orientated, unable to cooperate (including intoxication) or who have distracting injuries precluding reliable clinical assessment. Exclusions: Children under the age of 16. 1.1. Protection and immobilisation of entire spine From arrival of patient until appropriate clinical or radiological clearance of spinal injury. Immobilisation using all of the following: Semi-rigid collar (Miami J collar) (Stif-Nek collar to be replaced within 2 hours of arrival); 1 litre fluid bags (as blocks) and tape; firm mattress; entire bed may be tilted head up to 30 degrees, but no “break” in the bed at the patient’s waist. 1.2. Documentation In all at risk patients, documentation of the neurological status and a clinical examination of the entire spine. The ASIA score should be documented within 24 hours of admission. 1.3. Radiological spinal clearance imaging If any symptom or sign of spinal cord injury, or anticipated that a patient will remain unconscious, unassessable or unreliable for clinical examination for more than 48 hours. Cervical spine: 2-3mm (thin slice) helical CT scan from the base of the skull to T4/5 with both sagittal and coronal reconstructions. This should be undertaken with the first CT brain in all head injured patients with an altered level of consciousness. Thoracic and lumbar spine: Either sagittal and coronal reformatting of <5mm slice helical CT scans of chest, abdomen and pelvis, or AP and lateral plain radiographs. A senior radiologist must report spinal clearance images prior to withdrawal of spinal protection precautions. Ideally completed within 12 hours, but within a maximum of 48 hours. 2. Detection of spinal cord injury If a spinal cord injury is detected, a neurological assessment must be repeated 2 hourly, and a telephone referral made to the Spinal Cord Injury Centre within 4 hours of arrival (0844 89291915). Consider urgent MRI if the neurological deficits are secondary to spinal cord injury. All must be admitted to HDU for invasive BP monitoring aiming for normotension and good oxygenation.
Transcript of North West London Trauma Network Spinal Pathway and ... fileNorth West London Trauma Network 4 Acute...

North West London Trauma Network 1 Acute Spinal Injury Pathway v1.0 December 2014
North West London Trauma Network
Spinal Pathway and Protocols
1. Spinal Clearance in the Trauma Patient
Inclusions: All trauma patients who are not alert and orientated, unable to cooperate (including
intoxication) or who have distracting injuries precluding reliable clinical assessment.
Exclusions: Children under the age of 16.
1.1. Protection and immobilisation of entire spine
From arrival of patient until appropriate clinical or radiological clearance of spinal injury.
Immobilisation using all of the following: Semi-rigid collar (Miami J collar) (Stif-Nek collar to be
replaced within 2 hours of arrival); 1 litre fluid bags (as blocks) and tape; firm mattress; entire bed
may be tilted head up to 30 degrees, but no “break” in the bed at the patient’s waist.
1.2. Documentation
In all at risk patients, documentation of the neurological status and a clinical examination of the
entire spine. The ASIA score should be documented within 24 hours of admission.
1.3. Radiological spinal clearance imaging
If any symptom or sign of spinal cord injury, or anticipated that a patient will remain unconscious,
unassessable or unreliable for clinical examination for more than 48 hours.
Cervical spine: 2-3mm (thin slice) helical CT scan from the base of the skull to T4/5 with both
sagittal and coronal reconstructions. This should be undertaken with the first CT brain in all head
injured patients with an altered level of consciousness.
Thoracic and lumbar spine: Either sagittal and coronal reformatting of <5mm slice helical CT
scans of chest, abdomen and pelvis, or AP and lateral plain radiographs.
A senior radiologist must report spinal clearance images prior to withdrawal of spinal protection
precautions. Ideally completed within 12 hours, but within a maximum of 48 hours.
2. Detection of spinal cord injury
If a spinal cord injury is detected, a neurological assessment must be repeated 2 hourly, and a
telephone referral made to the Spinal Cord Injury Centre within 4 hours of arrival (0844 89291915).
Consider urgent MRI if the neurological deficits are secondary to spinal cord injury. All must be
admitted to HDU for invasive BP monitoring aiming for normotension and good oxygenation.
North West London Trauma Network 2 Acute Spinal Injury Pathway v1.0 December 2014
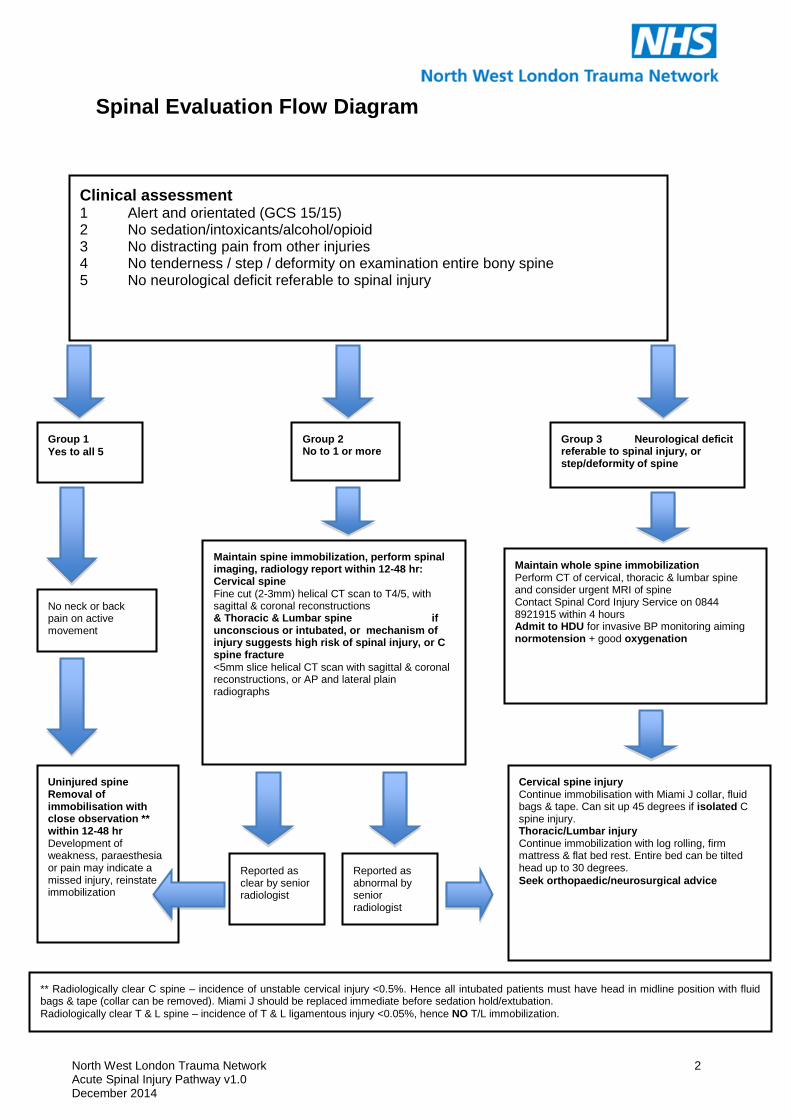
Spinal Evaluation Flow Diagram
Clinical assessment
1 Alert and orientated (GCS 15/15) 2 No sedation/intoxicants/alcohol/opioid 3 No distracting pain from other injuries 4 No tenderness / step / deformity on examination entire bony spine 5 No neurological deficit referable to spinal injury
Group 1
Yes to all 5
Maintain spine immobilization, perform spinal imaging, radiology report within 12-48 hr: Cervical spine Fine cut (2-3mm) helical CT scan to T4/5, with sagittal & coronal reconstructions & Thoracic & Lumbar spine if unconscious or intubated, or mechanism of injury suggests high risk of spinal injury, or C spine fracture <5mm slice helical CT scan with sagittal & coronal reconstructions, or AP and lateral plain radiographs
Reported as clear by senior radiologist
No neck or back pain on active movement
Uninjured spine Removal of immobilisation with close observation ** within 12-48 hr Development of weakness, paraesthesia or pain may indicate a missed injury, reinstate immobilization
Cervical spine injury Continue immobilisation with Miami J collar, fluid bags & tape. Can sit up 45 degrees if isolated C spine injury. Thoracic/Lumbar injury Continue immobilization with log rolling, firm mattress & flat bed rest. Entire bed can be tilted head up to 30 degrees.
Seek orthopaedic/neurosurgical advice
Group 2 No to 1 or more
Reported as abnormal by senior radiologist
Group 3 Neurological deficit referable to spinal injury, or step/deformity of spine
Maintain whole spine immobilization Perform CT of cervical, thoracic & lumbar spine and consider urgent MRI of spine Contact Spinal Cord Injury Service on 0844 8921915 within 4 hours Admit to HDU for invasive BP monitoring aiming normotension + good oxygenation
** Radiologically clear C spine – incidence of unstable cervical injury <0.5%. Hence all intubated patients must have head in midline position with fluid bags & tape (collar can be removed). Miami J should be replaced immediate before sedation hold/extubation.
Radiologically clear T & L spine – incidence of T & L ligamentous injury <0.05%, hence NO T/L immobilization.

North West London Trauma Network 3 Acute Spinal Injury Pathway v1.0 December 2014

North West London Trauma Network 4 Acute Spinal Injury Pathway v1.0 December 2014
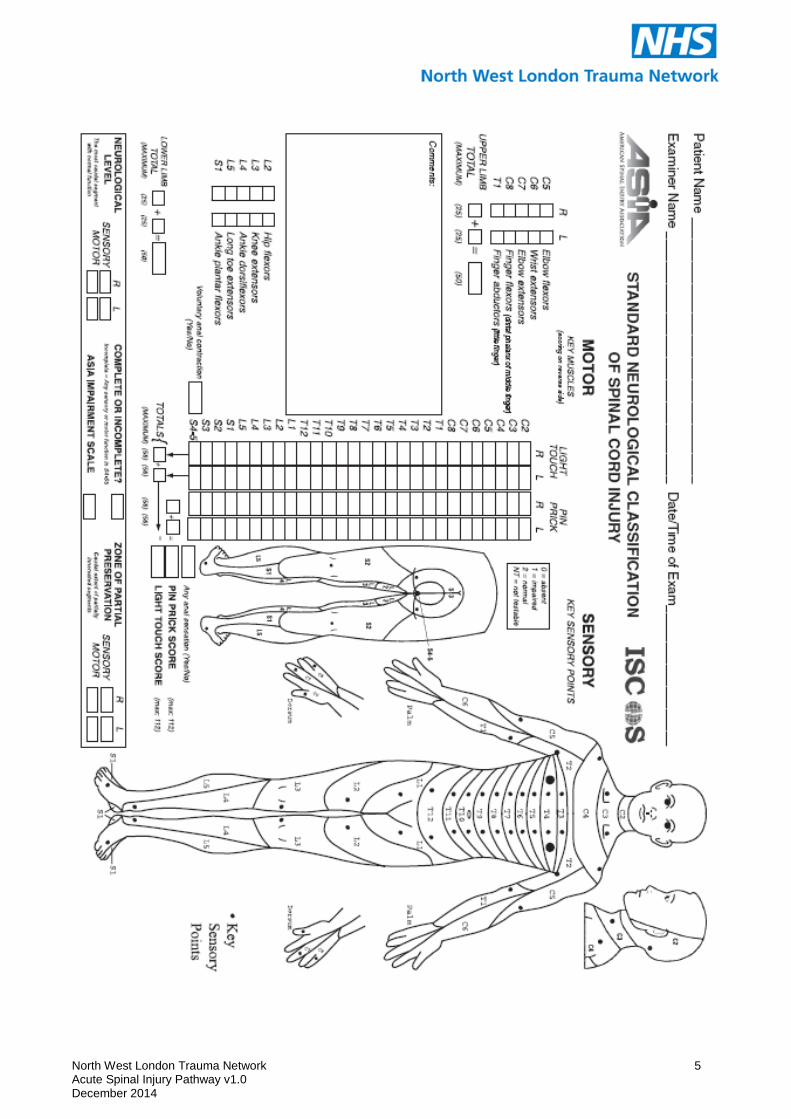
SPINAL CORD INJURY Spinal cord injury may be recorded using the American Spinal Injury Association (ASIA) chart. This is how all spinal-injured patients are assessed at St. Mary’s MTC. It has a number of benefits:
- It provides a quick reference guide to dermatomes and myotomes when performing a neurological examination for suspected spinal cord injury;
- The patient’s neurological status can be given motor and sensory scores (ASIA score) which helps describe a breakdown of the severity of injury;
- Scoring on the ASIA Impairment Scale (A – E, see below), can be done to present a broader picture of the spinal cord lesion;
- These scores can be repeated to track any changes in the spinal cord lesion; - Using the ASIA chart and the standardised terminology therein facilitates discussions with
the Neurotrauma team when referring patients, as this is the ‘language’ used for the assessment of spinal cord trauma patients at the MTC.
North West London Trauma Network 5 Acute Spinal Injury Pathway v1.0 December 2014

North West London Trauma Network 6 Acute Spinal Injury Pathway v1.0 December 2014
Spinal clearance checklist
Complete at admission and amend over time.
1) History Given the mechanism of injury, is there risk
of spinal injury? Yes / No
1 High energy mechanism (e.g. fall >2m, pedestrian or any road traffic accident, polytrauma) Yes / No
2 Admission GCS <15/15 or abnormal brain CT scan Yes / No
3 Associated distracting injures Yes / No
2) Examination Is there risk of spinal injury? Yes / No
1 Neck or back pain Yes / No
2 Spinal tenderness, deformity or steps on log roll Yes / No
3 neurological signs referrable to spinal injury Yes / No
(systolic bp <90, loss perianal sensation or anal tone, priapism, abnormal upper or lower limb power & reflexes)
3) Radiological clearance Reported by senior radiologist within 12-48 hours
C spine: Fine cut (2-3mm) helical CT scan to T4/5, with coronal & sagittal reconstructions
T&L spine: <5mm slice helical CT scan with coronal & sagittal reconstructions, or AP & lateral Xrays
Required Radiological clearance Date By whom
Yes No Yes No, unstable / stable Injuries are:
C spine
T&L spine
4) Spinal Immobilisation This will progress to no precautions over time.
C spine Full: Miami J collar, fluid bags & tape, midline position, logroll, sit up 45 degrees if isolated C spine injury Limited: either none, or midline position, fluid bags & tape; replace Miami J collar just prior to extubation Limited: mobilise with Miami J collar
T&L spine Full: log roll, supine flat bed rest, tilt entire bed head up 30 degrees, scoop stretcher, firm mattress Limited: mobilise with brace, ambulatory X ray
Updates / changes
1. Name Date of birth
Hospital no.
Required Immobilisation: full / limited / none Date By whom
Yes No

North West London Trauma Network 7 Acute Spinal Injury Pathway v1.0 December 2014
Further management
Neurological assessment
Document every ______ hours Contact bleep ________ if neurological deterioration ASIA score ____
If neurological deficit MRI of spine Contact Spinal Cord Injury Service (0844 8921915)
Follow Spinal Cord Injury protocol Oxygen mask; Aim systolic blood pressure > ______
Anti thrombosis prophylaxis
TEDS plus Flowtrons or TEDS plus tinzaparin (stop tinzaparin 24 hours prior to spinal surgery, restart 48 hours postop, use TEDS plus Flowtrons periop)
If surgery, post operative instructions & imaging
Clinic follow up ([email protected])
Complications associated with spinal precautions
Pressure sore Respiratory Raised ICP
Halo, Miami J or TL brace management Application Lying with spinal
immobilisation Lying Sitting
Size
Fitted by
Duration of use 24 hours / day Only when mobilising / sitting
Night time only
Time period of use ____ weeks Until clinic review
Washing Supine with spinal precautions
Sitting with neck still, +/- assistance
Remove, no restrictions
Name Date of birth
Hospital no.
Date By whom

North West London Trauma Network 8 Acute Spinal Injury Pathway v1.0 December 2014
2. MIAMI J Collar Management Patient Name: Hospital Number: DOB:
STABILITY Level of fracture/ Injury:
Unstable: Spinal Precautions Required = Head Hold Y / N
= Flat Bed Y / N
= Log Roll Y / N
Stable
Application
Lying with Spinal Precautions
Lying
Sitting
Duration of Use
24 hours a Day
Only when Sitting/ Mobilising
At night time only
Time Period of Use
____ weeks
Until next Outpatient Consultant Review
Indefinitely
Washing/ Bathing
With assistance Supine with Spinal Precautions
Sitting with Neck Still
Without assistance Sitting with Neck Still
Remove with no restrictions
Neurosurgical Consultant:
Signed (Consultant or SpR):
Date:
Collar fitted by:
Collar Size:

North West London Trauma Network 9 Acute Spinal Injury Pathway v1.0 December 2014
3. MIAMI TLSO – Request form Patient Name: Date:
DOB:
Hospital Number:
STABILITY Level of Fracture / Injury: Type of Fracture/ Injury:
Stable
Unstable Spinal Precautions Required
- Flat Bed Rest Y / N
- Log Roll Y / N
Is pain relief optimal prior to measurement and fitment. Y / N
Reason for requesting Bracing:
Pain relief
Stability post surgery
Support Conservative management
Mobilisation
Application
Lying with Spinal Precautions
Lying
Sitting
Standing
Duration of Use
24 hours a Day
Only when Sitting/ Mobilising
At night only
Can be removed for washing.
Time Period of Use
____ weeks
Until next Outpatient Consultant Review
Indefinitely
Neurosurgical Consultant:
Consultant or SpR Signature:
Orthotist:
Orthotist Signature:
Physiotherapist:
Physiotherapist Signature:
Lumbar/TLSO brace fitted by:
Signature: Type and Size:

North West London Trauma Network 10 Acute Spinal Injury Pathway v1.0 December 2014
4. SPINAL INJURY / CORD COMPRESSION
Use Spinal Management Pathway pack to initiate assessment. Ascertain whether stable or
unstable. (Unstable would be log rolling)
Consider level of injury & involvement of respiratory / abdominal muscles – initiate use of FVC 4
hourly monitoring if <1.5, consider prophyactic IPPB +/- incentive spirometer to ventilate bases
If A&E or extrication collar in place change to Miami J within 24 hours.
Ensure nursing staff are documenting Bowels closely
Ensure nursing staff have ordered pressure mattress
Consider use of abdominal binder if level cervical or thoracic to help maintain intra-abdominal
pressures
Consider teaching manual assisted cough if weak, ineffective cough
Discuss referral to Stoke / Stanmore spinal injury unit with team
Ensure ASIA completed within 72 hours

North West London Trauma Network 11 Acute Spinal Injury Pathway v1.0 December 2014
5. Acute Spinal Cord Injury Physiotherapy Management Pathway Name DOB Hospital # Physiotherapist Signature Initial Acute Assessment (See SCI Management Sheet)
Criteria Tick or N/A
Variance Date & Initial
Document date of injury
Document spinal injury level
Document stability status
Document manual handling guidelines
Document any additional injury
Apply collars / jackets as ordered by medical staff
Assess muscle groups on ASIA chart
Acute Respiratory Management
Criteria Tick N/A
Variance Date & Initial
Standard Respiratory Assessment
Consider SCI level and respiratory muscle innervation to identify risks
Ensure regular FVC measurement
Instigate treatment & / or prophylactic treatment.
Caution with manual / prophylactic techniques with primary lung Ca / bony mets
Daily reassessment / liaison with MDT
Acute Physical Management (See database forms)
Criteria Tick N/A
Variance Date & Initial
ASIA form
Appropriate databases completed: Proprioceptive defecit Full muscle strength chart Range of movement chart Tone Other limiting factors
Assess for and supply any necessary splints and record relevant advice given to MDT. Consider Abdominal Binder.
Specific positioning requirements & advice to nursing staff are documented
Instigate active assisted ROM programme in line with spinal protocol (limb guidelines for unstable)
Consider medical management e.g. baclofen

North West London Trauma Network 12 Acute Spinal Injury Pathway v1.0 December 2014
Spinal Cord Compression Physiotherapy Management Sheet Name DOB Hospital # ------------------------------------- --------------------- --------------------- SCI Level (Bony / Motor / Sensory) Date of Injury; Stable / Unstable (To be documented by Medical Staff); Surgery and Date; Movement Restrictions (eg Log Rolling); Associated Injury; Other Limiting Factor (eg Bony mets); Chest Status; Ensure regular Bowel Monitoring by Nursing Staff Recommendations; Physiotherapist Signature Date ------------------------- ----------------------------- -----------------