Noradrenalina en shock refractario
4
Acta Pædiatrica ISSN 0803–5253 REGULAR ARTICLE Noradrenaline for management of septic shock refractory to fluid loading and dopamine or dobutamine in full-term newborn infants Pierre Tourneux (tourneux.pierre@chu-amie ns.fr) 1,2,3,4 , Thameur Rakza 1,3 , Abdel Abazine 1,3 , G ´ erard Krim 2 , Laurent Storme 1,3 1.Cli nique de M ´ edeci ne N ´ eonat ale, H ˆ opital Jeanne de Flandre, CHRU de Lille, France 2.Se rvice de M ´ edec ine N ´ eonat ale et R ´ eanimation P´ ediatrique Polyvalente, Hˆ opital Nord, CHU d’Amiens, France 3.UPRES JE2490, Universit´ e Lille II, Lille, France 4.DMAG (BA 3901), Universit ´ e de Picardie Jules Verne, Amiens, France Keywords Blood pressure, Newborn infant, Noradrenaline, Septic shock Correspondence Tourneux Pierre, Service de M´ edeci ne N ´ eonatale et R´ eanimation P´ ediatrique Polyvalente, Centre Hospitalier et Universitaire—Hˆ opital Nord, 1 place Victor Pauchet 80054 Amiens cedex 1, France. Tel.: +33(0)3-22-66-82-86 | Fax.: +33(0)3-22-66-82-81 | Email: tourneux.pierre@chu -amiens.fr Received 22 June 2007; revised 31 August 2007; accepted 24 October 2007. DOI:10.1111/j.1651-2227.2007.00601.x Abstract Aim: To determine the effects of noradrenaline in full-term newborns with refractory septic shock. Methods: Newborns of >35 weeks’ gestation with persistent septic shock, despite adequate fluid resuscitation and high dose of dopamine/dobutamine were eligible. In this prospective observational study, we recorded respiratory and hemodynamic parameters prior to and 3 h after starting noradrenaline infusion. Results: Twenty-two newborns were included (gestational age [GA] 39 ± 1.7 weeks, birth weight (BW) 3110 ± 780 g). Before starting noradrenaline, the infants received a mean volume expansion of 31 ± 15 mL/kg and a mean infusion rate of dopamine of 14 ± 5 µg/kg/min or dobutamine of 12 ± 6 µg/kg/min. Three hours after starting noradrenaline (rate 0.5 ± 0.4 µg/kg/min), the mean arterial blood pressure rose from 36 ± 5 to 51 ± 7 mmHg (p < 0.001). Urine output increased from 1 ± 0.5 to 1.7 ± 0.4 mL/kg/h (p < 0.05). Blood lactate concentration decreased from 4.8 ± 2.3 to 3.3 ± 1.8 mmol/L (p < 0.01). Despite an initial correction of hypotension, four infants died later. Conclusion: Noradrenaline was effective in increasing systemic blood pressure. An increase in urine output and a decrease in blood lactate concentration suggest that noradrenaline may have improved cardiac function and tissue perfusion. INTRODUCTION Shock represents an important cause of morbidity and mor- tality in critically ill newborns (1). Early fluid and cardio- vascular resuscitation are essential to improve the outcome (2). In case of nonresponse to fluid resuscitation, initiation of inotropic and vasoactive agents are warranted to increase cardiac output, maintain adequate blood pressure and en- hance oxygen (O 2 ) delivery to the tissue (3). Dopamine is the sympathomimetic amine most frequently used for vas opl egi c sho ck in newborns (3) . The abi lit y of dop ami ne to rai se sys temic blo od pre ssu re (SBP) has been clearly documented (3). However, failure to sus- tain adequate blood press ure desp ite high dopamine doses has als o bee n rep ort ed (2,4,5). Dop ami ne fai led to rai se blood pressure in more than 30% preterm newborn in- fants with systemic hypotension (6). Thus, particular life- threatening conditions may require the use of other vasoac- tive drugs. In adul t pati ents with sept ic shock , norad renal ine was more effective than dopamine in reversing hypotension, and has rec ent ly bee n rec ommended as the fir st- choice vasopres- sor agent to correct hypotension (5–8). Such recommen- dation has also been proposed in children with vasoplegic shock (2,9). Noradrenaline was found to raise SBP and O 2 uptake without adverse effect on organ blood flow (5,10). Furthermore, noradrenaline may improve the outcome of septic shock patients (8). However, no published data are available about the clinical effects of noradrenaline in the newborn. In this prospective observational study, we evaluated the respiratory and the haemodynamic effects of noradrenaline in full-term newborn infants with septic shock refractory to fluid res usc ita tio n and to dob uta min e or dop ami ne infusion. MATERIAL AND METHODS The study was conducted in the neonatal intensive care unit (NICU) of Lille University Hospital, France. Newborns eli- gible for inclusion were: (i) newborn infants of >35 weeks’ gestation, and <1-month old; (ii) admitted in the NICU be- tween January 1, 2002 and December 31, 2004; (iii) with seps is (prov en infect ion or clini cal syndr omeassociated with a high probability of infection, and a systemic inflammatory response syndrome defined as an abnormal temperature or leucocyte count, or at least two of the following criteria: C- reactive protein [CRP] >50 mg/L, leucopenia <4000/mm 3 or thrombocyt openi a <80 000/ mm 3 (11) ); (i v) and wi th per- sist ent shock despite adequate fluid resus citat ion and high dose of dopamine/dobutamine or substitutive dose of hy- drocortisone and (v) mechanically ventilated and sedated. Shock was defined by systemic hypotension (mean blood pressure <10th per centil e of the norma l ran ge for birth weight [BW] and postnatal age) with at least three of the following criteria for decreased perfusion: (i) tachycardia C 2007 The Author(s)/Journal Compilation C 2007 Foundation Acta Pædiatrica/ Acta Pædiatrica 2008 97, pp. 177–180 177
-
Upload
williamsbarrios -
Category
Documents
-
view
217 -
download
0
Transcript of Noradrenalina en shock refractario

8/14/2019 Noradrenalina en shock refractario
http://slidepdf.com/reader/full/noradrenalina-en-shock-refractario 1/4
Acta Pædiatrica ISSN 0803–5253
R E G U L A R A R T I C L E
Noradrenaline for management of septic shock refractory to fluid loadingand dopamine or dobutamine in full-term newborn infantsPierre Tourneux ([email protected])1,2,3,4, Thameur Rakza1,3, Abdel Abazine1,3, Gerard Krim2, Laurent Storme1,3
1.Clinique de Medecine Neonatale, Hopital Jeanne de Flandre, CHRU de Lille, France
2.Service de Medecine Neonatale et Reanimation Pediatrique Polyvalente, Hopital Nord, CHU d’Amiens, France3.UPRES JE2490, Universite Lille II, Lille, France4.DMAG (BA 3901), Universite de Picardie Jules Verne, Amiens, France
Keywords
Blood pressure, Newborn infant, Noradrenaline,Septic shock
Correspondence
Tourneux Pierre, Service de Medecine Neonatale etReanimation Pediatrique Polyvalente, CentreHospitalier et Universitaire—Hopital Nord, 1 placeVictor Pauchet 80054 Amiens cedex 1, France.Tel.: +33(0)3-22-66-82-86 |Fax.: +33(0)3-22-66-82-81 |Email: [email protected]
Received22 June 2007; revised 31 August 2007;accepted 24 October 2007.
DOI:10.1111/j.1651-2227.2007.00601.x
Abstract
Aim: To determine the effects of noradrenaline in full-term newborns with refractory septic shock.
Methods: Newborns of >35 weeks’ gestation with persistent septic shock, despite adequate fluid
resuscitation and high dose of dopamine/dobutamine were eligible. In this prospective observational
study, we recorded respiratory and hemodynamic parameters prior to and 3 h after starting
noradrenaline infusion.
Results: Twenty-two newborns were included (gestational age [GA] 39 ± 1.7 weeks, birth weight
(BW) 3110 ± 780 g). Before starting noradrenaline, the infants received a mean volume expansion
of 31 ± 15 mL/kg and a mean infusion rate of dopamine of 14 ± 5 µg/kg/min or dobutamine of
12 ± 6 µg/kg/min. Three hours after starting noradrenaline (rate 0.5 ± 0.4 µg/kg/min), the meanarterial blood pressure rose from 36 ± 5 to 51 ± 7 mmHg (p < 0.001). Urine output increased from
1 ± 0.5 to 1.7 ± 0.4 mL/kg/h (p < 0.05). Blood lactate concentration decreased from 4.8 ± 2.3 to
3.3 ± 1.8 mmol/L (p < 0.01). Despite an initial correction of hypotension, four infants died later.
Conclusion: Noradrenaline was effective in increasing systemic blood pressure. An increase in urine output and a
decrease in blood lactate concentration suggest that noradrenaline may have improved cardiac function and
tissue perfusion.
INTRODUCTION
Shock represents an important cause of morbidity and mor-
tality in critically ill newborns (1). Early fluid and cardio-
vascular resuscitation are essential to improve the outcome(2). In case of nonresponse to fluid resuscitation, initiationof inotropic and vasoactive agents are warranted to increase
cardiac output, maintain adequate blood pressure and en-
hance oxygen (O2) delivery to the tissue (3).
Dopamine is the sympathomimetic amine most frequently
used for vasoplegic shock in newborns (3). The abilityof dopamine to raise systemic blood pressure (SBP) has
been clearly documented (3). However, failure to sus-
tain adequate blood pressure despite high dopamine doses
has also been reported (2,4,5). Dopamine failed to raise
blood pressure in more than 30% preterm newborn in-fants with systemic hypotension (6). Thus, particular life-
threatening conditions may require the use of other vasoac-tive drugs.
In adult patients with septic shock, noradrenaline was
more effective than dopamine in reversing hypotension, and
has recently been recommended as the first-choice vasopres-sor agent to correct hypotension (5–8). Such recommen-
dation has also been proposed in children with vasoplegic
shock (2,9). Noradrenaline was found to raise SBP and O 2
uptake without adverse effect on organ blood flow (5,10).Furthermore, noradrenaline may improve the outcome of
septic shock patients (8). However, no published data are
available about the clinical effects of noradrenaline in the
newborn.
In this prospective observational study, we evaluated the
respiratory and the haemodynamic effects of noradrenalinein full-term newborn infants with septic shock refractoryto fluid resuscitation and to dobutamine or dopamine
infusion.
MATERIAL AND METHODS
The study was conducted in the neonatal intensive care unit
(NICU) of Lille University Hospital, France. Newborns eli-gible for inclusion were: (i) newborn infants of >35 weeks’
gestation, and <1-month old; (ii) admitted in the NICU be-
tween January 1, 2002 and December 31, 2004; (iii) with
sepsis (proven infection or clinical syndrome associated with
a high probability of infection, and a systemic inflammatory
response syndrome defined as an abnormal temperature orleucocyte count, or at least two of the following criteria: C-
reactive protein [CRP] >50 mg/L, leucopenia <4000/mm3
or thrombocytopenia <80 000/mm3 (11)); (iv) and with per-
sistent shock despite adequate fluid resuscitation and highdose of dopamine/dobutamine or substitutive dose of hy-
drocortisone and (v) mechanically ventilated and sedated.
Shock was defined by systemic hypotension (mean blood
pressure <10th percentile of the normal range for birth
weight [BW] and postnatal age) with at least three of the
following criteria for decreased perfusion: (i) tachycardia
C2007 The Author(s)/Journal Compilation C2007 Foundation Acta Pædiatrica/ Acta Pædiatrica 2008 97, pp. 177–180 177

8/14/2019 Noradrenalina en shock refractario
http://slidepdf.com/reader/full/noradrenalina-en-shock-refractario 2/4
Noradrenaline for septic shock in the newborn Tourneux et al.
(heart rate>160 beats/min); (ii) abnormal peripheral pulses;
(iii) modified extremities colouration; (iv) prolonged capil-
lary refill time >3 sec and (v) urine output <1 mL/kg/h
(2,9). The following echocardiographic markers were usedto ensure that fluid resuscitation was adequate: inferior vena
cava diameter >5 mm in infants treated by conventional
mechanical ventilation and left ventricular end diastolic di-
mension between −2 and +2 standard deviation (SD) for
the body weight in infants treated by high-frequency oscil-latory ventilation (12). Exclusion criteria were: (i) congeni-
tal structural heart disease, except patent ductus arteriosus;
(ii) cardiac arrest or terminal disease (pulse oxygen satu-
ration value [SpO2] <60%, arterial pH <6.80, bradycardia
<90 beats/min and no measurable blood pressure) prior toinclusion in the study or (iii) start of noradrenaline before
inclusion in the study.
The included newborns received noradrenaline (diluted
in dextrose 5% to a concentration of 1 mL = 100 µg) in-
fused in a central catheter at an initial rate between 0.2 to0.5 µg/kg/min, at the discretion of the practitioner. The rate
of infusion was eventually increased every 30 min until the
mean blood pressure normalized (>10th percentile of thenormal range for BW and postnatal age). No change in the
dopamine/dobutamine infusion rate was performed during
the 3 h following the beginning of noradrenaline infusion.Haemodynamic and respiratory parameters were
recorded just before and 3 h after starting noradrenaline
infusion. Inspired oxygen concentration (FiO2) was set to
maintain SpO2 above 95%. The outcome was evaluated forextracorporeal membrane oxygenation (ECMO) require-
ment, cranial ultrasound and neurological examination
at the time of discharge from the unit. The protocol was
approved by the Regional Ethics Committee of Picardy.
Results were expressed as mean± SD. Use of median± in-
terquartile range (IQ) was mentioned in the text. Data wereanalysed using Wilcoxon signed rank test to compare paired
data before and during noradrenaline use. Significance was
set as p < 0.05.
RESULTS
Twenty-two newborns fulfilled the entry criteria. Mean ges-tational age (GA) and BW were, respectively, 39.1 ± 1.7
weeks’ gestation and 3110 ± 780 g. The mean Apgar score
was 7.4 ± 2.4 and 8.1 ± 1.9 at 1 and 5 min of life, respec-
tively. The postnatal age at the onset of the shock was 15 ±
37 h. Fifteen newborns required high-frequency oscillatory
ventilation and inhaled nitric oxide (iNO) for persistent pul-monary hypertension of the newborn (PPHN) assessed by
echocardiography. The mean FiO2 was 75 ± 20%. All the
newborns required vascular expansion with saline serum
or 10% albumin (mean volume expansion 31 ± 15 mL/kg).Mean dopamine (8 of 22 newborns) or dobutamine (12 of 22
newborns) infusion rate prior to noradrenaline infusion was,
respectively, 14± 5 µg/kg/min and 12± 6µg/kg/min. Three
received substitutive doses of hydrocortisone (0.5 mg/kg, 3
times a day). Just before starting noradrenaline, mean SBP
was 36 ± 5 mmHg. Mean arterial blood pH and lactate
0
10
20
30
40
50
60
70
80
Before
norepinephrine
3 hours after
norepinephrine start
M e a n a r t e r i a l p r e s s u r e ( m m H
g )
***************
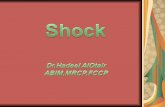
Figure 1 Mean (± SD, outer dots) and individual mean arterial blood pressure
measured just beforeand 3 h after starting noradrenaline infusion.Mean arterial
blood pressure increased in each newborn (∗∗∗p < 0.001).
concentration were, respectively, 7.25 ± 0.13 and 4.8 ±2.3 mmol/L. The mean urine output was 1 ± 0.5 mL/kg/h
during the 3 h preceding the noradrenaline infusion.
The initial noradrenaline infusion rate was 0.4 ±
0.15 µg/kg/min. Five newborns required an increase in no-radrenaline to normalize SBP. The mean noradrenaline in-
fusion rate to correct the systemic hypotension was 0.5 ±0.4 µg/kg/min (range 0.2–2.0 µg/kg/min). The median du-
ration of noradrenaline use was 61 ± 59 h (range 8–
116 h). The individual maximum noradrenaline infusion rateto sustain normal SBP ranged from 0.2 to 7.1 µg/kg/min.
SBP rose by 40% (from 36 ± 5 to 51 ± 7 mmHg, p <
0.001) within the first 3 h of noradrenaline infusion (Fig. 1).
The change in SBP was greater for diastolic pressure (from
29 ± 4 to 43 ± 8 mmHg) than for systolic pressure (from51 ± 8 to 66 ± 9 mmHg, p < 0.01). The heart rate increased
from 143 ± 26 to 154 ± 24 beats/min (p < 0.05).
The mean urine output increased by 70% after nora-drenaline infusion (from 1 ± 0.5 mL/kg/h during the 3 h
preceding the start of noradrenaline, to 1.7 ± 0.4 mL/kg/hduring the 3 h following the start of noradrenaline; p < 0.05).
After starting the noradrenaline infusion, a lower mean FiO2
was required to achieve a postductal SpO2 of 95% (74 ±27% vs. 66 ± 28%, p < 0.05). Mean airway pressure (16 ±5 cm H2O vs. 16 ± 5 cm H2O, p = 0.38) and both preduc-tal SpO2 (96 ± 5% vs. 94 ± 4%, p = 0.47) and postductal
SpO2 (92 ± 14% vs. 92 ± 14%, p = 0.09) were unchanged.
Arterial pH (7.25 ± 0.13 vs. 7.28 ± 0.09, p = 0.90), arte-
rial carbon dioxide pressure (paCO2) (47 ± 17 torr vs. 43 ±10 torr, p = 0.78), BE (−6 ± 7 mmol/L vs. −7 ± 5 mmol/L,
p = 0.48) and bicarbonates concentrations (19 ± 4 mmol/Lvs. 18 ± 6 mmol/L, p = 0.78) did not change significantly
over the first 3 h of noradrenaline infusion. Plasma lac-
tate concentration decreased significantly from 4.8 ± 2.3 to
3.3 ± 1.8 mmol/L (p < 0.05).No newborn presented ischaemic distal lesions during no-
radrenaline infusion. Four newborns died despite an ini-
tial correction of systemic hypotension was obtained. The
cause of death was refractory hypoxaemia and shock. Three
infants required ECMO for PPHN. Eighteen infants were
alive at the discharge home. Two newborn infants had a
178 C2007 The Author(s)/Journal Compilation C2007 Foundation Acta Pædiatrica/ Acta Pædiatrica 2008 97, pp. 177–180

8/14/2019 Noradrenalina en shock refractario
http://slidepdf.com/reader/full/noradrenalina-en-shock-refractario 3/4
Tourneux et al. Noradrenaline for septic shock in the newborn
hyperechogenicity of the white mater at 7 days after birth.
At 1 month after birth, despite the electroencephalogram
was normal, magnetic resonance imaging (MRI) confirmed
temporo-occipital ischaemic lesions in one of the two chil-dren. Cranial ultrasound and clinical examination were
considered as normal in the other infant at the discharge
home.
DISCUSSION
In this observational study, we found that noradrenaline
was effective in increasing the SBP at a mean infusion rateof 0.5 ± 0.4 µg/kg/min. No impairment of the respiratory
function was observed after starting the noradrenaline in-
fusion. In contrast, an increase in urine output and a de-
crease in O2 need and in blood lactate concentration suggest
that noradrenaline may improve cardiac function and tissueperfusion.
There are many controversial and unresolved issues re-
garding the most effective vasopressor agent to manage sep-
tic shock. While dopamine is preferred worldwide for the
initial management of hypotension in sepsis, several reportsmentioned a failure to sustain adequate tissue perfusion
pressure with dopamine, even at high doses (2,4–6). Other
studies highlighted the potential side effect of dopamine to
raise pulmonary vascular resistance and pulmonary artery
pressure in newborns (13,14). In contrast, growing evidencesuggests that noradrenaline may represent an optimal vaso-
pressor drug to manage septic shock. Both experimental and
clinical studies showed that noradrenaline raises systemic
arterial blood pressure, cardiac output, oxygen delivery and
consumption and regional blood flow, including mesentericand renal blood flows, and improves survival (15,16). More-
over, whereas dopamine may elevate pulmonary artery re-
sistance (13,14), noradrenaline could exhibit a pulmonaryvasodilator effect, especially at elevated basal pulmonary
vascular tone (17–20). We found that similar benefi-cial effects of noradrenaline can be obtained in full-term
newborn infants with life-threatening septic shock unre-
sponsive to fluid resuscitation and high doses of dopamine
or dobutamine. Our data show that noradrenaline not only
raises perfusion pressure, but may also help to improve or-
gan blood flow and functions in newborns with refractoryseptic shock. Supporting this hypothesis are the decrease in
blood lactate concentrations and the elevation of urine out-
put shortly after starting noradrenaline infusion. Although
lactate concentration requires careful interpretation, a high
lactate level is generally considered as a marker of hypoxiaand a reliable indicator of poor outcome. Thus, a drop in
lactate concentration strongly suggests that noradrenaline
can decrease tissue hypoxia in septic neonates.
Several potential mechanisms may explain the beneficial
effect of noradrenaline in newborns with refractory septicshock: (i) In most infants included in the present study,
PPHN was associated with septic shock. PPHN is usually
associated with low systemic pressure and low cardiac out-
put because of an increased right ventricular afterload and
myocardial dysfunction (21). Noradrenaline improved cir-
culatory adaptation at birth in a newborn lamb with per-
sistent pulmonary hypertension (20). Other data suggest
that noradrenaline can improve cardiac performance in pul-
monary hypertension (22,23). Our results are consistent
with these studies as the O2 need decreased during the no-
radrenaline infusion, suggesting that noradrenaline-induced
increase in aortic pressure may be associated with improve-
ment of PPHN-induced cardiac dysfunction. (ii) In shock,
a decrease in blood pressure may result in decreased re-gional blood flow, which in turn may contribute to tissue
hypoxia and to organ failure (7). Beneficial effect of nora-
drenaline in shock may be explained at least, in part, by
its striking effectiveness in raising arterial blood pressure.
In our study, noradrenaline increased SBP in each treatedinfant.
As mentioned earlier, in this study, four infants died (18%)
despite an initial correction of hypotension. The mortal-
ity rate ranges from 7 to 40% in the population of paedi-
atric and neonatal shocks (2,11). In adult patients with sep-tic shock, noradrenaline could improve survival (8). How-
ever, whether or not noradrenaline may improve outcome in
the newborn with refractory septic shock remains an openquestion.
This study has some limitations. The population of our
study was highly selected. Despite shock, the circulating blood volume was normal. Special care was taken to ensure
an appropriate fluid therapy before using noradrenaline.
Present recommendations clearly stated that adequate fluid
resuscitation is a prerequisite for using vasopressor ther-
apy (7). When these recommendations were applied, noadverse effect on tissue perfusion was mentioned during no-
radrenaline infusion (24,25). In the present study, the shock
was unresponsive to dopamine or dobutamine infusion. Al-
though systemic vascular resistances were not measured in
the present study, the haemodynamic profile of the shockwas probably mainly hyperdynamic, as indicated by the low
values of diastolic blood pressure. Whether or not nora-
drenaline may be beneficial in other conditions is still un-
known.
CONCLUSION
Severe septic shock in the newborn may not respond to fluid
resuscitation and to dopamine or dobutamine infusion. We
found that noradrenaline could be beneficial in raising the
perfusion pressure. In contrast, noradrenaline may have im-
proved tissue oxygenation, as indicated by an increase in
urine output and by a decrease in blood lactate concentra-tion. We suggest that noradrenaline may be used in septic
full-term newborn infants with life-threatening hypotension
after correction of possible hypovolaemia. Adequate titra-
tion of noradrenaline infusion is required to prevent exces-sive vasoconstriction.
References
1. Meadow W, Rudinsky B. Inflammatory mediators andneonatal sepsis. Rarely has so little been known by so manyabout so much. Clin Perinatol 1995; 22: 519–36.
C2007 The Author(s)/Journal Compilation C2007 Foundation Acta Pædiatrica/ Acta Pædiatrica 2008 97, pp. 177–180 179

8/14/2019 Noradrenalina en shock refractario
http://slidepdf.com/reader/full/noradrenalina-en-shock-refractario 4/4
Noradrenaline for septic shock in the newborn Tourneux et al.
2. Han YY, Carcillo JA, Dragotta MA, Bills DM, Watson RS,Westerman ME, et al. Early reversal of pediatric-neonatalseptic shock by community physicians is associated withimproved outcome. Pediatrics 2003; 112: 793–9.
3. Seri I. Circulatory support of the sick preterm infant. Semin
Neonatol 2001; 6: 85–95.4. Meadows D, Edwards JD, Wilkins RG, Nightingale P.
Reversal of intractable septic shock with norepinephrinetherapy. Crit Care Med 1988; 16: 663–6.
5. Martin C, Papazian L, Perrin G, Saux P, Gouin F.Norepinephrine or dopamine for the treatment of hyperdynamic septic shock? Chest 1993; 103: 1826–31.
6. Pellicer A, Valverde E, Elorza MD, Madero R, Gaya F, Quero J, et al. Cardiovascular support for low birth weight infantsand cerebral hemodynamics: a randomized, blinded, clinicaltrial. Pediatrics 2005; 115: 1501–12.
7. Dellinger RP, Carlet JM, Masur H, G erlach H, Calandra T,Cohen J, et al. Surviving Sepsis Campaign guidelines formanagement of severe sepsis and septic shock. Crit Care Med
2004; 32: 858–73.8. Martin C, Viviand X, Leone M, Thirion X. Effect of
norepinephrine on the outcome of septic shock. Crit Care
Med 2000; 28: 2758–65.9. Ceneviva G, Paschall JA, Maffei F, Carcillo JA. Hemodynamic
support in fluid-refractory pediatric septic shock. Pediatrics1998; 102: E19.
10. Redl-Wenzl EM, Armbruster C, Edelmann G, Fischl E,Kolacny M, Wechsler-Fordos A, et al. The effects of norepinephrine on hemodynamics and renal function insevere septic shock states. Intensive Care Med 1993; 19:151–4.
11. Goldstein B, Giroir B, Randolph A. International pediatricsepsis consensus conference: definitions for sepsis and organdysfunction in pediatrics. Pediatr Crit Care Med 2005; 6: 2–8.
12. Kampmann C, Wiethoff CM, Wenzel A, Stolz G, Betancor M,Wippermann CF, et al. Normal values of M modeechocardiographic measurements of more than 2000 healthyinfants and children in central Europe. Heart 2000; 83:667–72.
13. Liet JM, Boscher C, Gras-Leguen C, Gournay V, Debillon T,Roze JC. Dopamine effects on pulmonary artery pressure inhypotensive preterm infants with patent ductus arteriosus. J
Pediatr 2002; 140: 373–5.14. Jaillard S, Houfflin-Debarge V, Riou Y, Rakza T, Klosowski S,
Lequien P, et al. Effects of catecholamines on the pulmonary
circulation in the ovine fetus. Am J Physiol Regul Integr Comp
Physiol 2001; 281: R607–14.15. Di Giantomasso D, Morimatsu H, May CN, Bellomo R.
Intrarenal blood flow distribution in hyperdynamic septicshock: effect of norepinephrine. Crit Care Med 2003; 31:2509–13.
16. Minneci PC, Deans KJ, Banks SM, Costello R, Csako G,Eichacker PQ, et al. Differing effects of epinephrine,norepinephrine, and vasopressin on survival in a canine
model of septic shock. Am J Physiol Heart Circ Physiol 2004;287: H2545–54.
17. Hirsch LJ, Rooney MW, Wat SS, Kleinmann B, Mathru M.Norepinephrine and phenylephrine effects on right ventricularfunction in experimental canine pulmonary embolism. Chest
1991; 100: 796–801.18. Cutaia M, Friedrich P. Hypoxia-induced alterations of
norepinephrine vascular reactivity in isolated perfused catlung. J Appl Physiol 1987; 63: 982–7.
19. Tulloh RM, Dyamenahalli U, Stuart-Smith K, Haworth SG.Adrenoceptor-stimulated endothelium-dependent relaxationin porcine intrapulmonary arteries. Pulm Pharmacol 1994; 7:299–303.
20. Jaillard S, Elbaz F, Bresson-Just S, Riou Y, Houfflin-DebargeV, Rakza T, et al. Pulmonary vasodilator effects of
norepinephrine during the development of chronic pulmonaryhypertension in neonatal lambs. Br J Anaesth 2004; 93:818–24.
21. Belik J, Light RB. Effect of increased afterload on rightventricular function in newborn pigs. J Appl Physiol 1989; 66:863–9.
22. Vlahakes GJ, Turley K, Hoffman JI. The pathophysiology of failure in acute right ventricular hypertension: hemodynamicand biochemical correlations. Circulation 1981; 63: 87–95.
23. Tritapepe L, Voci P, Cogliati AA, Pasotti E, Papalia U,Menichetti A. Successful weaning from cardiopulmonary bypass with central venous prostaglandin E1 and left atrialnorepinephrine infusion in patients with acute pulmonaryhypertension. Crit Care Med 1999; 27: 2180–3.
24. LeDoux D, Astiz ME, Carpati CM, Rackow EC. Effects of
perfusion pressure on tissue perfusion in septic shock. CritCare Med 2000; 28: 2729–32.
25. Martin C, Viviand X, Arnaud S, Vialet R, Rougnon T. Effectsof norepinephrine plus dobutamine or norepinephrine aloneon left ventricular performance of septic shock patients. Crit
Care Med 1999; 27: 1708–13.
180 C2007 The Author(s)/Journal Compilation C2007 Foundation Acta Pædiatrica/ Acta Pædiatrica 2008 97, pp. 177–180