Nonpharmacologic Treatment of Behavioral Disorders in … · Nonpharmacologic Treatment of...
21
Current Treatment Options in Neurology (2013) 15:765–785 DOI 10.1007/s11940-013-0257-2 DEMENTIA (E MCDADE, SECTION EDITOR) Nonpharmacologic Treatment of Behavioral Disorders in Dementia Jiska Cohen-Mansfield, PhD 1,2,3 Address 1 Department of Health Promotion, School of Public Health, Sackler Faculty of Medicine, Tel-Aviv University, Ramat Aviv, P.O.B. 39040, Tel-Aviv 69978, Israel 2 Herczeg Institute on Aging, Tel-Aviv University, Tel-Aviv, Israel 3 Minerva Center for the Interdisciplinary Study of End of Life, Tel-Aviv University, Tel-Aviv, Israel Email: [email protected] Published online: 18 October 2013 * Springer Science+Business Media New York 2013 Keywords Dementia I Behavior problems I Behavioral disorders I Agitation I Treatment I Nonpharmacologic treatment I Sensory interventions I Massage I Aromatherapy Opinion statement Dementia symptoms are often complicated by behavioral disorders such as repetitive verbalizations, aggressive behavior, and pacing. In clinical practice, the most common re- sponses to behavioral disorders are pharmacologic, mostly using antipsychotic medication, or ignoring the behavior. However, multiple research studies support the notion that these behav- ioral disorders in dementia are related to unmet needs that can be addressed by nonpharmacologic interventions. Persons with dementia present multiple unmet needs, most commonly pain and discomfort, need of social contact and support, and need of stimulation that alleviates boredom. A wide range of interventions that address these needs has been investigat- ed, though the rigor of the investigations varied greatly depending on factors related to the be- havioral disorder, setting, and resource limitations. In practice, the avenues to address the unmet needs should depend on the person’ s abilities and preferences. Thus, nonpharmacologic interventions that are individually tailored to the person with dementia comprise a superior re- sponse to behavioral disorders and should be at the frontline of treatment of these disorders. Introduction Conceptualization of behavioral disorders in dementia Behavioral disorders in dementia encompass a range of observable behaviors displayed by Persons With Dementia (PWDs) that are socially unusual or inap- propriate. These behaviors often manifest, express, or result from needs that are not readily identified and do not include behaviors that address clearly identifi- able bodily needs, such as running to the bathroom and wetting oneself.
Transcript of Nonpharmacologic Treatment of Behavioral Disorders in … · Nonpharmacologic Treatment of...

Current Treatment Options in Neurology (2013) 15:765–785DOI 10.1007/s11940-013-0257-2
DEMENTIA (E MCDADE, SECTION EDITOR)
Nonpharmacologic Treatmentof Behavioral Disordersin DementiaJiska Cohen-Mansfield, PhD1,2,3
Address1Department of Health Promotion, School of Public Health, Sackler Faculty ofMedicine, Tel-Aviv University, Ramat Aviv, P.O.B. 39040, Tel-Aviv 69978, Israel2Herczeg Institute on Aging, Tel-Aviv University, Tel-Aviv, Israel3Minerva Center for the Interdisciplinary Study of End of Life, Tel-Aviv University,Tel-Aviv, IsraelEmail: [email protected]
Published online: 18 October 2013* Springer Science+Business Media New York 2013
Keywords Dementia I Behavior problems I Behavioral disorders I Agitation I Treatment I Nonpharmacologictreatment I Sensory interventions I Massage I Aromatherapy
Opinion statement
Dementia symptoms are often complicated by behavioral disorders such as repetitiveverbalizations, aggressive behavior, and pacing. In clinical practice, the most common re-sponses to behavioral disorders are pharmacologic, mostly using antipsychotic medication, orignoring the behavior. However, multiple research studies support the notion that these behav-ioral disorders in dementia are related to unmet needs that can be addressed bynonpharmacologic interventions. Persons with dementia present multiple unmet needs, mostcommonly pain anddiscomfort, needof social contact and support, andneedof stimulation thatalleviates boredom. Awide range of interventions that address these needs has been investigat-ed, though the rigor of the investigations varied greatly depending on factors related to the be-havioral disorder, setting, and resource limitations. In practice, the avenues to address theunmet needs should depend on the person’s abilities and preferences. Thus, nonpharmacologicinterventions that are individually tailored to the person with dementia comprise a superior re-sponse to behavioral disorders and should be at the frontline of treatment of these disorders.
Introduction
Conceptualization of behavioral disordersin dementiaBehavioral disorders in dementia encompass a rangeof observable behaviors displayed by Persons WithDementia (PWDs) that are socially unusual or inap-
propriate. These behaviors often manifest, express, orresult from needs that are not readily identified anddo not include behaviors that address clearly identifi-able bodily needs, such as running to the bathroomand wetting oneself.

Multiple factor analyses [1] have shown that be-havioral disorders can be described along behavioraldimensions, namely: aggressive vs nonaggressive, ver-bal vs physical, and frequency of display (never toall the time). Subtypes of behavioral disorders aretherefore physically aggressive behaviors, such as hit-ting or kicking others; physical nonaggressive behav-iors, such as pacing back and forth or handlingthings inappropriately; verbally aggressive behaviors,such as cursing; and verbal nonaggressive behaviors,such as repetitious verbalizations. Both correlationaland longitudinal studies have shown that different sub-types of behavioral disorders are associated with differ-ent demographic and health variables. For example,verbal manifestations, but not physical nonaggressivebehaviors, have been associated with medical problemsor pain. Aggressive behaviors tend to occur in the verylast stages of dementia [2, 3].
Conceptually, it is important to determine whetherbehavioral disorders are symptoms of dementia andtherefore integral to the dementia syndrome, or alter-natively, represent disease symptoms that are not spe-cific to dementia but may stem from inappropriatetreatment of dementia and reflect symptoms of dis-content or other difficulties. As will be seen in the nextsection, different theoretical frameworks present differ-ent answers to this question.
Theories of behavioral disorders in dementiaFour theoretical frameworks have been proposed toexplain the etiology of behavioral disorders in demen-tia, including biological and genetic accounts [4], a be-havioral model of the behavior as triggered and
reinforced by the environment [5], a theory of reducedstress threshold in dementia [6], and an unmet needsmodel [7]. The biological theory postulates that be-havioral disorders stem from neurologic changes inthe brain or from severe organic brain deteriorationthat result in behavioral disinhibition. Therefore, thebehavioral disorder is a symptom of the disease. Thebehavioral theoretical framework asserts that problembehavior is controlled by its antecedents and conse-quences. Antecedents operate through stimulus controltriggering a behavior, and consequences involve its rein-forcement, for example, by caregivers who provide atten-tion when the problem behavior is displayed. The thirdtheory asserts that the dementia process results in greatervulnerability to the environment and a lower thresholdat which stimuli affect behavior. Therefore, normal stim-ulation engenders anover-reaction anddisturbances thataremanifested as behavioral disorders. The unmet needstheoreticalmodel explains the behavioral disorders as re-sponses to unmet needs. Given that the dementia in-volves a decreased ability to meet one’s needs becauseof communication difficulties and decreased ability toprovide for oneself and that the person’s environmentoften fails to detect or address the needs, personswith dementia often experience pain/health/physicaldiscomfort, mental discomfort (evident in affectivestates, eg,: depression, anxiety, frustration), loneliness,and boredom.
The above theoretical models are notmutually exclu-sive andmay pertain to different behaviors and differentpersons. Yet, my research and others’ observations pro-videmore support to the unmet needsmodel, as detailedelsewhere [8, 9].
TreatmentPharmacologic treatment
Drug therapy for behavioral disorders is based on the biological theoret-ical framework described above and therefore aims to decrease behavioraldisinhibition by changing the balance of neurotransmitters. The mostcommon class of drugs for pharmacologic treatment of persistent andpervasive behavioral disorders is antipsychotic medication [10–12], whichhas severe side effects including increased mortality rates [10, 13–15].Consensus statements and guidelines recommend limiting the use of an-tipsychotics in all settings [16–18]. Additional information on the use ofantipsychotics and the pharmacologic approach to treating behavioraldisorders in dementia is discussed in the accompanying topic of dementiawith Lewy bodies in this edition.
766 DEMENTIA (E MCDADE, SECTION EDITOR)

Nonpharmacologic interventionsThe goals of nonpharmacologic interventions depend on the theoretical modelused for the intervention. Most interventions aim to fulfill unmet needs,whereas some aim to decrease the level of stimulation (eg, by playing peacefulmusic) or tomodify behaviors by changing contingencies or by stimulus control(eg, by camouflaging a bothersome stimulus). Some interventions may be ap-propriate for multiple objectives. Regardless of the stated goal, the actualmechanism of action is often unclear. For example, music may be provided assensory stimulation to combat boredom, but, if the music is presented by amusician who provides participants with social contact, the social contact maybe the most important active ingredient of the intervention.
In a 2001 review [19] the following nomenclature for nonpharmacologicinterventions was set forth: sensory, structured activities, social contact - realor simulated, medical/nursing care interventions, environmental interven-tions, behavior therapy, staff training, and combination therapies. While thegoal and the theoretical formulation may vary among interventions, generalprinciples can be ascertained. The first four intervention categories are basedon the unmet needs model. Specifically, sensory interventions and activitiesare geared to ameliorate boredom and sensory deprivation (Fig. 1); socialcontact interventions aim to alleviate loneliness (Fig. 2); and medical andnursing interventions aim to address pain and discomfort (Fig. 3). In con-
Figure 1. Unmet needs of boredom, sensory deprivation or relaxation: examples of nonpharmacologic interventions.(Copyright 2013, Jiska Cohen-Mansfield, PhD).
Nonpharmacologic Treatment of Behavioral Disorders in Dementia Cohen-Mansfield 767

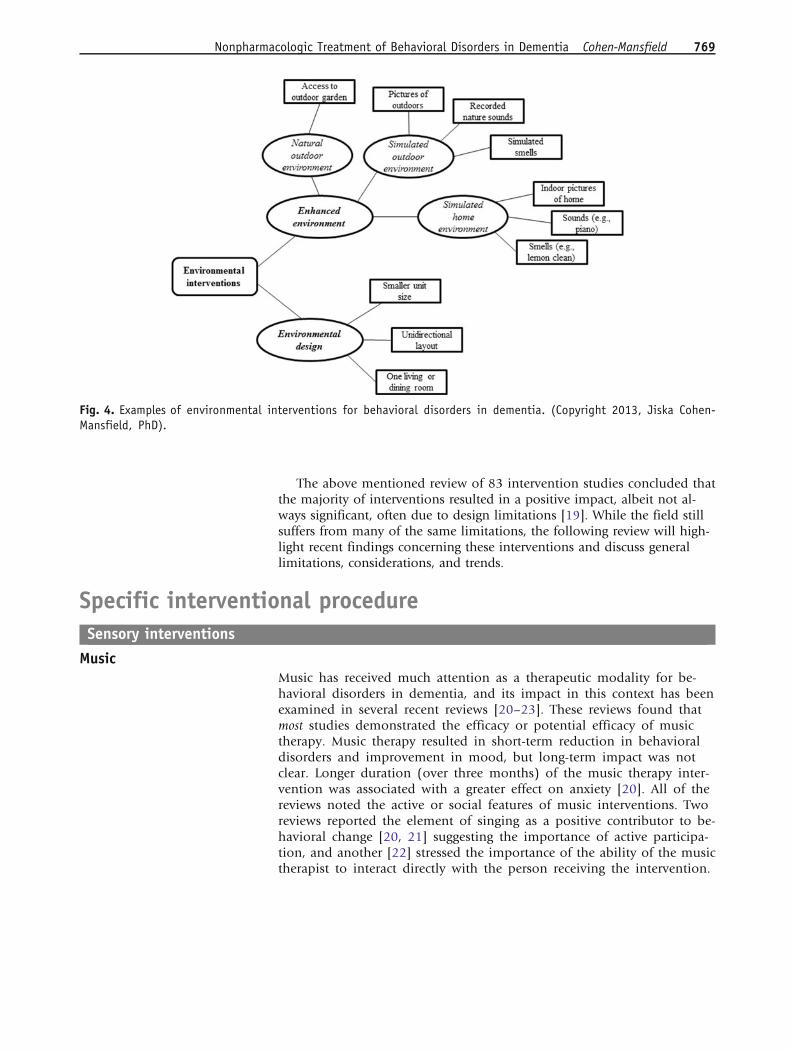
trast, behavior therapy interventions are based on a behavioral theoreticalmodel. Finally, environmental (Fig. 4) and combination therapies may relateto any of the above theoretical models. For example, an environmental in-tervention may aim to decrease stimulation, in accordance with the envi-ronmental vulnerability/lower stress threshold model, or it may increasestimulation based on an unmet need of boredom/need of stimulation.
Figure 2. Unmet need of loneliness: examples of nonpharmacologic interventions. (Copyright 2013, Jiska Cohen-Mansfield, PhD).
Figure 3. Unmet needs of pain or dis-comfort: Examples of nonpharmacologicand pharmacologic interventions. (Copy-right 2013, Jiska Cohen-Mansfield, PhD).
768 DEMENTIA (E MCDADE, SECTION EDITOR)
The above mentioned review of 83 intervention studies concluded thatthe majority of interventions resulted in a positive impact, albeit not al-ways significant, often due to design limitations [19]. While the field stillsuffers from many of the same limitations, the following review will high-light recent findings concerning these interventions and discuss generallimitations, considerations, and trends.
Specific interventional procedureSensory interventions
MusicMusic has received much attention as a therapeutic modality for be-havioral disorders in dementia, and its impact in this context has beenexamined in several recent reviews [20–23]. These reviews found thatmost studies demonstrated the efficacy or potential efficacy of musictherapy. Music therapy resulted in short-term reduction in behavioraldisorders and improvement in mood, but long-term impact was notclear. Longer duration (over three months) of the music therapy inter-vention was associated with a greater effect on anxiety [20]. All of thereviews noted the active or social features of music interventions. Tworeviews reported the element of singing as a positive contributor to be-havioral change [20, 21] suggesting the importance of active participa-tion, and another [22] stressed the importance of the ability of the musictherapist to interact directly with the person receiving the intervention.
Fig. 4. Examples of environmental interventions for behavioral disorders in dementia. (Copyright 2013, Jiska Cohen-Mansfield, PhD).
Nonpharmacologic Treatment of Behavioral Disorders in Dementia Cohen-Mansfield 769

The focus on active participation and on human contact within music ther-apy raises the question concerning the net effect ofmusic per se, ie, is listening tomusic without any additional activity or input of value by itself? A study of theuse of such passive music in comparison to no stimuli has shown its effect inreducing behavioral disorders [24] and increasing pleasure [25].
AromatherapyThere are relatively few studies of aromatherapy interventions. A review of11 randomized controlled trials [26] concluded that aromatherapy is po-tentially useful for treating behavioral disorders. A meta-analysis of twostudies [27, 28] in this review found a significant effect for aromatherapytreatment. Interestingly, a replication of one of these studies, which in-cluded an improved experimental design (ie, blinding of treatment arms)and a different assessment, did not find Melissa aromatherapy to be supe-rior to placebo [29]. Overall, despite some positive results, current evidenceis inconclusive due to the small number of studies and methodologicallimitations [26, 30].
MassageA review of massage interventions for behavioral disorders in persons withdementia [31] found only one study with adequate methodology [32] out of13 studies that met review criteria. This study demonstrated a significantreduction in behavioral disorders following massage in a sample of 52 per-sons with dementia. There was no comparison group. Several individualstudies support the impact of massage on behavioral disorders. Foot massagehas been associated with a significant decrease in behavioral disorders in 22persons with dementia [33]. Massage was also associated with a significantdecrease in aggressiveness, but not in other behavioral disorders, in a groupof 20 persons with dementia. No significant changes in behavioral disorderswere found in the control group (n=20) [34]. In a study of 65 nursing homeresidents with dementia, therapeutic touch significantly decreased restless-ness, but not other behavioral disorders, in comparison to a control groupreceiving routine care, and there was no significant reduction of behavioraldisorders in comparison with a placebo mimic treatment [35]. Taken to-gether, massage intervention studies all suffer from methodological short-comings or inconclusive results, often referring to a single behavioralsymptom. Nonetheless, they support the promise of massage and touch indecreasing behavioral disorders in persons with dementia.
Multisensory interventionsConflicting results have been found in studies of Snoezelen among personswith dementia, with some studies reporting some effect on behavior butothers finding no effect [30].
Structured activitiesThe positive impact of activities, such as arranging flowers or arts and crafts,has been demonstrated by several studies. In a comparison of different
770 DEMENTIA (E MCDADE, SECTION EDITOR)

approaches to selecting activities for participants (eg, based on functionallevel, personality style of interest, or both) it was found that all of the ac-tivities significantly decreased behavioral disorders, with no significant dif-ferences between those approaches [36]. In a study examining the efficacy ofvarious activities including tasks (eg, flower arrangement, coloring withmarkers), reading stimuli (eg, being presented with a large-print magazine),individualized activities matched to the individual’s past preferences oridentity, work like activities (eg, stamping envelopes, folding towels), andmanipulative stimuli (eg, a tetherball, building blocks), all types of stimuliand activities had a significant positive impact on behavioral disorders [37•].The greatest impact was found for task, reading, and self-identity stimuli (ie,matched to prior relationships, occupation, hobby, or other attribute thatwas important to the person), which significantly affected both physical andverbal agitation. In contrast, work activities and manipulative stimuli had asignificant impact only on physical agitation [37•].
A review of physical activity programs for persons with dementia [38]concluded that these programs are beneficial for behavioral disorders.Walking, however, did not appear to affect night-time restlessness [39]. Anexact specification of benefits by type of exercise, population, and behavioralsymptoms is needed. Dancing is a physical activity that also includes sensorystimulation (music) and a social component. While most of the research isdescriptive and exploratory, a review of ten studies, seven of which werequalitative, found that dance interventions decreased behavioral disorders[40]. Indoor gardening is another type of physical activity that was reportedto significantly reduce behavioral disorders in a pilot pre-post study [41].
Montessori activities are based on principles developed by Maria Montes-sori for teaching children. These principles include matching task demand tostudents’ abilities by breaking tasks into small components, using repetition,and starting with easier items and then increasing demands as competence isacquired. Typically, Montessori activities include a range of procedures thatmay include sensory stimulation, such as rhythmic music, task type activitiesbased on utilizing procedural memory, such as pouring (eg, through a fun-nel) or squeezing (eg, clay), and social interaction. Two crossover studiesfound that Montessori activities significantly decreased behavioral disorders[42•, 43], though in one of the studies [42•] the comparison condition ofnon-personalized activity was also effective, and both personalized and non-personalized activities included interaction , thereby potentially qualifying associal contact interventions.
Social contact— real or simulatedGiven the definite impact of social contact on behavioral disorders and itsrelative superiority to many other stimuli and activities [37•], it is not sur-prising that it is an integral part of many nonpharmacologic interventions.What is unexpected is the relative dearth of studies that address social contactas the main intervention.
An analysis of the dimensions of social contact and their relative impor-tance can be useful for devising interventions with a social contact compo-nent or focus. In a study that focused on engagement of nursing homeresidents with dementia with activities and stimuli rather than on the treat-
Nonpharmacologic Treatment of Behavioral Disorders in Dementia Cohen-Mansfield 771

ment of behavior disorders, Cohen-Mansfield et al [44] analyzed the fol-lowing dimensions: human vs nonhuman (ie, animal), realistic vs not real-istic (eg, a doll that looks like a baby vs one that looks like a doll), animated(eg, a robot with movement) vs not animated, and alive (eg, real baby or realdog) vs not alive (eg, video, doll, or robot). While any social stimuli werepreferable to nonsocial stimuli in promoting engagement, attention, and apositive attitude, there were advantages to human, animated, realistic, andlive stimuli. Nevertheless, there could be instances where engagement mightbe longer for a not alive stimulus like a robotic dog rather than a live dog.
The following discussion of social interventions is divided to those thatprovide human contact, animal-assisted social contact, and simulated socialcontact.
Human contactOne-on-one human contact with a PWD by a trained individual has beenrepeatedly found to be a highly potent intervention for behavioral disorders[37•, 45]. Humor therapy can serve as a source of social interaction, and itwas shown to significantly decrease agitation in a cluster randomized trial[46•] that utilized both trained staff and professional performers to deliver ahumor therapy intervention.
Animal-assisted interventionsA review of 18 studies of animal assisted interventions with persons withdementia [47] shows that these interventions may have the potential to re-duce behavioral disorders. Ten studies in this review examined the impact ofanimal assisted therapy on behavioral disorders in dementia, of which threereported statistically significant decreases in behavioral disorders [48, 49] oraggressiveness [50]. The remaining studies either did not report a statisticalanalysis or else reported nonsignificant results. While this review [47] sug-gested that robotic pets may be as effective as real live pets in terms of animalassisted therapy, the evidence for this is still lacking [47, 51].
Simulated social contactThese interventions include a range of techniques to simulate human andanimal contact. Human contact can be simulated by calling to mind mem-ories of past family relationships, such as through the use of family pictures.Simulated presence therapy includes video or audiotaped conversations byfamily members. Commercial respite videos, in which someone talks to orsings with the older person, are also available. A baby doll may elicit caringbehaviors. Simulated contact with animals includes robotic animals (usuallycats or dogs), stuffed animals, and videos of animals [24].
The impact of video family simulated presence therapy has been demon-strated in a study utilizing a single subject ABA design [52]. Specifically, re-sistance to basic care was decreased during the presentation of the familyvideo; when the video was not presented, the effect was reversed. A review ofboth audio and video simulated presence therapy [53] concluded, based onfour studies, that it has a significant positive effect on behavioral disorders,
772 DEMENTIA (E MCDADE, SECTION EDITOR)

though with limited support. For simulated presence therapy to be useful,several conditions need to be met: a positive relationship between the olderperson and the family member preparing the tape, a family member willingto prepare such a tape, cognitive impairment to a degree that will allow theperson to continue to enjoy the tape over repeated viewings, and hearing andvision abilities sufficiently intact to utilize audio or videotape. Both anec-dotal and research support has been documented regarding the beneficialeffect of using dolls with people with dementia, including the effect on be-havioral disorders [54•]. Dolls have been offered as an activity alternative inthis population or used in doll-therapy sessions. Dolls can offer comfort,security, companionship, and a role to persons with moderate to advanceddementia. Ethical concerns in using dolls involve scenarios in which thePWD thinks the doll is a baby or becomes over-involved with the doll, alongwith the need to protect the dignity of the PWD.
Medical/nursing care interventionsBehavioral disorders in general, and verbal agitation in particular, have beenshown to be associated with pain [3], and a large controlled study showedthat use of analgesics significantly decreased behavioral disorders in personswith dementia [55•]. Yet, the ability of both professional and family care-givers to detect pain in advanced dementia is questionable, and pain istherefore underdetected and undertreated [56]. Different assessments forpain have been compared for their efficacy to detect pain that responds toanalgesics. Informant ratings completed by primary direct-care caregiver werethe most useful in detecting pain in this population [57]. When analyzing thetype of behavior most likely to respond to pain medication, verbal agitation,which has been shown to be most highly related to pain [3], also emerged ashaving the largest response [58]. Despite the success of utilization of generalanalgesics protocols, it is important to also investigate specific sources ofpain. Dental pain, for example, is pervasive in this population and can bemanifested in behavioral disorders [59].
In addition to pain, discomfort represents unmet needs that contribute tobehavioral disorders. Providing a sweater to someone who is feeling cold andproviding food, drink, and timely help in going to the bathroom are all ex-amples of care activities that have been used to decrease behavioral disorders[60••]. A more comprehensive list of sources of discomfort is availableelsewhere [60••]. The use of physical restraints, especially, results in dis-comfort that has been associated with increased behavioral disorders [61].Conversely, the removal of such restraints has been associated with a de-crease in behavioral disorders [62]. Removal of restraints requires a systemicapproach; an educational program is likely to be insufficient [63].
Discomfort is often experienced during the bathing process of personswith dementia due to multiple sources, including poor understanding ofthe PWD, lack of knowledge of staff members on how to provide a pleasantbathing experience, a physical environment that does not meet the needs ofthe PWD or the caregivers, and regulations that do not offer the flexibilityneeded to provide tailored, person-centered bathing [64]. In a randomizedcontrolled trial [65], it was found that behavioral disorders and discomfortsignificantly decreased when PWDs were provided with either person-cen-
Nonpharmacologic Treatment of Behavioral Disorders in Dementia Cohen-Mansfield 773

tered showering or a towel bath with no-rinse soap in comparison with usualcare.
Other medical/nursing interventions involve aids for vision and hearingloss. While hearing loss is prevalent in dementia, the use of hearing aids isrelatively scarce [66]. A review of the limited reports on the impact of hearingaids in dementia concluded that they do benefit the behavior of PWDs(available in French; [67]).
Environmental interventionsA previous review on nonpharmacologic interventions [19] includedstudies showing some support for the impact of enhanced environments,such as those simulating natural conditions (eg, pictures of outdoors,bird sounds) or a home environment in decreasing behavioral disorders.Access to an outdoor garden, access to refreshments, and a quiet unithave all been reported to decrease behavioral disorders [19]. Much of themore recent literature on the impact of environmental change on PWDshas not focused directly on behavioral disorders, but rather on constructsthat may either trigger behavioral symptoms or be incompatible withthem. For example, specific environmental features, such as small num-ber of residents per unit, no change in direction within the unit layout,and provision of only one living or dining room were related to betterway finding by residents [68]. Better way finding is likely to result inmore autonomy and less frustration and thereby the manifestation offewer behavioral symptoms. Similarly, design features, such as small unitsize, that are related to improved quality of life have been identified[69]. Improved quality of life is generally incongruent with behavioraldisorders [70]. The same review [69] reported that decreasing the insti-tutional characteristics of residential facilities was associated with fewerbehavioral disorders and that a wall mural over an exit door decreasedexit attempts. Finally, bright light therapy, used in a study of 66 olderPWDs in two residential care settings, showed no benefit and a potentialexacerbating effect and remains a controversial modality for behavioraldisorders in dementia [71].
Behavior therapyPrevious studies have showed the efficacy of differential reinforcement andstimulus control in treating behavior disorders yet the evidence is limitedbecause most used a single subject design or very small samples [19]. Inrecent years there seems to be a dearth of studies using behavior therapycompared with those investigating other approaches. Yet, the few studiesconducted have generally supported behavior therapy for treating behaviordisorders. For example, a single subject design demonstrated the impact ofboth stimulus control and differential reinforcement on wandering behavior[72], and a pilot study using a pre-post design reported significant im-provement in behavioral disorders [73].
Culture change, system change, and staff trainingStaff training is undertaken in order to affect behavior change in staffthat will then result in reduction in behavioral disorders in PWDs under
774 DEMENTIA (E MCDADE, SECTION EDITOR)

their care. These complex interventions can target various groups ororganizational levels and may include person-centered care or specificinterventions.
The results of staff training interventions thus far have been mixed. In aCochrane review, four studies that successfully decreased antipsychoticmedication use in care home residents were identified. The outcome wasachieved using a variety of educational methods, including education andtraining of physicians, pharmacists, and nursing staff, as well as consultationswith the home administrator, information meeting for family members,multidisciplinary team meetings, and additional education for all staff whocome in contact with residents [74]. An exploratory trial with no controlgroup found that a staff training intervention [75] significantly reduced be-havioral disorders in 32 assisted-living residents with dementia. In a ran-domized controlled trial [76•], an education and supervision interventionsignificantly reduced behavioral disorders at 6- and 12-month follow-up in145 nursing home residents with dementia when compared with controls.The program included lectures, written materials, provision of resources toimplement the new skills, feedback and peer support. Another controlledstudy that significantly reduced behavioral disorders [77] utilized a combi-nation of lectures, instruction cards, and individual and iterative sessionsproviding instruction and feedback as to how to handle behavioral prob-lems. The trainers were also available to staff members at designated times toprovide training and advice.
Other staff interventions did not appear to be successful in reducing be-havioral disorders. A review of case conferences for handling behavioraldisorders [78] reported that four of the seven identified studies showed areduction in behavioral disorders and concluded that there is little evidencefor the utility of case conferences. Other interventions included the use of amulti-component education toolkit utilizing an assessment to trigger careplanning of persons with behavioral disorders [79], as well as an attempt toimprove staff interaction with residents with severe dementia by trainingthem to observe and identify awareness in residents [80]. Adherence is oftena problem in staff training programs [81].
Culture change implies a greater institutional change than staff training.In a longitudinal study examining culture change that focused on provid-ing person-centered care, a significant benefit on behavioral disorders wasreported; however, the benefit was accounted for by significant increases inbehavior disorders in the control communities while the intervention com-munities maintained pre-intervention levels [82••]. This equivocal resultsuggests that future research of culture change interventions may need toexamine the impact of specific aspects of such programs or of specific com-binations of elements in order to ascertain the necessary ingredients to affectchange.
One example of successful system change is provided in the experience ofthe Kansas Bridge Program, a dementia crisis intervention program utilizingsupport to family caregivers of persons with behavioral disorders by a trainedsocial worker and improving education and coordination among profes-sionals working with PWDs. The program resulted in multiple significantbenefits for PWDs and their caregivers, including a reduction in PWDs' be-havioral disorders [83•].
Nonpharmacologic Treatment of Behavioral Disorders in Dementia Cohen-Mansfield 775

Combination therapies / complex algorithmsThe rationale behind the use of algorithms that utilize a combination ofinterventions is that both the type and specifics of an intervention need to bematched to the person, setting, situation, and resources. The particulars of theindividualization process differ across studies. The “Treatment Routes forExploring Agitation – TREA” approach first assesses the unmet needs of theindividual. Each type of unmet need can be addressed by a range of inter-ventions, so that the specific intervention is selected to meet the person’ssensory (eg, vision and hearing) and mobility abilities, as well as past andpresent preferences. Understanding past and present preferences can be fa-cilitated by the use of assessments such as the Self-Identity in Dementiaquestionnaire [84] or the SHAPE – Self Maintenance Habits and Preferencesin Elderly [85]. The efficacy of this TREA algorithm approach has been re-ported in two studies [60••, 86]. A similar approach was taken in a programtitled “Behavior-based ergonomics therapy - BBET”, which provided indi-vidualized relaxing and stimulating activities and stimuli on a preventivebasis, ie, on an ongoing basis rather than after a disruptive behavior. Thisdecreased behavioral disorders and use of psychotropic medication [87].Similarly, an individualized intervention addressing needs for comfort, socialinteraction, and sensory stimulation significantly decreased verbal agitation[88]. Another intervention with caregivers of home-residing PWDs that suc-cessfully reduced behavior disorders utilized home and telephone contactsbetween an occupational therapist and the caregiver that addressed com-munication, environmental problems, and medical issues while also brain-storming concerning problems reported by the caregiver [89]. Finally, areview of 18 functional analysis-based interventions drawing on varioustheoretical orientations to individualize interventions within a wide range ofsettings, including family care and care homes, found that the frequency ofbehavioral disorders decreased after the interventions [90].
General issues in research and implementationof nonpharmacologic interventionsThe level of evidence, and does it make a difference?
There is an abundance of reviews of the impact of nonpharmacologic interven-tions on behavior problems, and several reviews of reviews [91]. Many of thereviews exclude much evidence by insisting on randomized controlled trialsas an inclusion criterion [Cohen-Mansfield et al., Expanded review criteria:the case of nonpharmacological interventions in dementia, unpublished man-uscript]. One review of reviews concluded that three types of interventions areeffective:music,massage, and physical activity [91], while another found behav-ior therapy, cognitive stimulation, and physical activities to be effective [92].Such discrepancies raise the question of whether it is helpful to focus on proofof efficacy rather than proof of promise. I would like to argue that an efficacy-based approach to clarifying the level of evidence is not useful. This conclusionis based on practical, methodological, and theoretical considerations.
From a theoretical point of view, given that the bulk of the evidencepoints to unmet needs as an appropriate framework for understandingmost behavioral disorders, it can be expected that different PWDs have dif-
776 DEMENTIA (E MCDADE, SECTION EDITOR)

ferent needs and even the needs of a single PWD will vary by time. Moreover,the proper response to a need is unique and is a function of the person’sabilities, habits, and preferences. Therefore, any study that uses the samespecific intervention for all participants is likely to have a moderate impact atbest. An effort, instead, is needed to provide a proof of concept or feasibilityfor a wide range of potential solutions. Efficacy should be examined for re-search of algorithms utilizing these solutions or for research of change ofculture of practice style, which also likely would utilize these solutions.
From a methodological point of view, the determination of whether a trialshows a significant effect often seems to depend as much on the proceduresused as on the results. The label of a nonpharmacologic intervention doesnot itself indicate the active ingredient(s) in that intervention. Clarifying the re-sult of an intervention is therefore confounded by several factors. The qualityand frequency of interactions with the person administering the interventionmay have a major effect on its outcome. The impact of the intervention onthe caregiver is also important, as the intervention may require extra effort fromthe caregiver, it may have a direct impact on the caregiver (eg, music) or, alter-nately, provide tools to care for the PWD or result in the PWD becoming moreamenable to care. Prior attitudes toward the intervention modality (music, pet,manipulative object, game) can also affect the response to the intervention. Thesetting of the intervention and dosage (eg, duration, timing, and frequency) canall affect the response. It is extrinsic factors such as these that can lead differentstudies and different reviews to reach different conclusions for ostensibly thesame intervention. Further clouding the issue are inadequate reviews that repeatthe results of other inadequate reviews to provide either a thoroughly vague andambiguous picture or to recite the need for additional research and reiterate theknown limitations of studies in this field. This approach is neither informativenor useful for practice or research in this area.
A practical point of viewwould indicate that, as can be seen in Figs. 1, 2, and3, nonpharmacologic approaches encompass a multitude of techniques andprocedures and, therefore, it is unlikely that sufficient resources will be availableto perform properly powered randomized controlled studies on all of these in-terventions. Moreover, each intervention encompasses many particular exem-plars, such that a doll may be small or baby size, soft or plastic, baby-like ornot, of the same race as the PWD or a different one, etc, or a physical exercisemay differ by type of activity, by person providing it and the amount and typeof communication and support provided, by the number of PWDs included inthe activity, and other attributes. It is definitely impossible to study each of the-se variants in a large study. Studies comparing attributes of interventions to clar-ify the crucial dimensions, which impact efficacy may ultimately be moreuseful. However, those studies are often not considered for inclusion in reviewsbecause they do not fit the current devotion to the RCT design [Cohen-Mans-field et al., unpublished manuscript].
Contraindications, complications, adverse events, and negative resultsBecause of the nature of nonpharmacologic interventions, they have very fewadverse events or contraindications, and reports of these are rare. One ex-ample of an adverse event involved a family video that resulted in an exac-erbation of problem behaviors. Upon further inquiry, the researchers found
Nonpharmacologic Treatment of Behavioral Disorders in Dementia Cohen-Mansfield 777

out that the relationship between the PWD and the family member who hadproduced the video had been strained for years [93]. This incident exem-plifies the importance of fitting the intervention to the personal character-istics of the PWD, not just in terms of cognitive and physical abilities andsensory deficits, but also in terms of the particular meaning of the inter-vention to the person. Accordingly, animal-assisted therapy is more likely tohelp persons who liked pets. Because not all background information can begained prior to an intervention, some studies have used an initial trial periodto assess and refine the particulars of the intervention prior to providing it ona more prolonged basis [25]. Such a trial period is a good opportunity todocument both refusals and nonresponse, which have been understudied inpast research.
Reports of negative results, ie, of interventions that did not produce theanticipated effect on problem behaviors, can still be insightful, particularlygiven the multiple limitations of studies in this area. Indeed, despite publi-cation bias, there are nevertheless many reports of negative results [94, 95].Such studies demonstrate the difficulty of affecting change in a population ofpersons with advanced dementia, who are often cared for in conditions thatmay be difficult for them and/or their caregivers. This situation needs to bekept in mind in reviewing the results of the imperfect research that consti-tutes most of the knowledge currently available, and potentially much ofwhat will be available in the foreseeable future.
Cost/cost-effectivenessThe dearth of information concerning cost-effectiveness ofnonpharmacologic interventions in dementia is due to the complexity of thecalculations and to the underdeveloped nature of the interventions them-selves. Calculating the cost effectiveness of the interventions would need totake into account any system changes (eg, training and mentoring caregivers,providing necessary materials, etc) required to make nonpharmacologic in-terventions a part of daily life in the care of the PWD. Necessary funds couldpotentially be achieved through savings in costs associated with pharmaco-logic care, currently the common practice in the clinical management ofbehavioral disorders, such as medicine aids, physician calls, handling ofadverse events, etc. One study that did examine the cost-effectiveness [96] ofhome visits by occupational therapists to develop customized activities andtrain families in their use concluded that the program was cost-effective.
Comparing treatments to each otherGiven the large range of nonpharmacologic interventions, the practitionerwould benefit from information about their relative efficacy. Yet, thatknowledge is currently limited.
A few studies have reported an equivalent efficacy of different interven-tions in reducing behavior disorders. These included comparisons of musictherapy and recreational activities [97], Snoezelen and reminiscence therapy[98], and Person Centered Showering and Towel Bath, which were both su-perior to usual care [65].
Other studies have reported both equivalent and differential efficacy in re-ducing behavior disorders when comparing different interventions. For ex-
778 DEMENTIA (E MCDADE, SECTION EDITOR)
ample, one-on-one social contact, videotapes of family members, and musicwere all more effective than usual care in reducing verbal agitation, but one-on-one social contact was the most effective [45]. Another study reportedthat, while both simulated family presence and preferred music reducedphysical agitation, only simulated family presence significantly reduced ver-bal agitation [99]. Comparison of eight stimulus categories revealed a hier-archy among stimuli with regard to their ability to decrease agitation. Humansocial interaction was the most effective intervention, while manipulativestimuli were the least effective. The other categories of stimuli, such as thosebased on the person’s self-identity had an intermediate level of impact [37•].The ultimate goal of such comparisons is to clarify which intervention is bestfor whom.
Long-term vs short-term impactOne of the common criticisms of nonpharmacologic interventions is thattheir effects are of short duration, only being seen while the intervention isactually taking place but not at post-trial follow-up [45, 49]. It is to beexpected that interventions addressing unmet needs would satisfy thoseneeds while the intervention is ongoing (eg, providing an activity to a personwho is bored and unable to engage herself or elimination of pain and dis-comfort), but the need still remains after the intervention is stopped. Forproviding nonpharmacologic interventions that meet continuing needs, en-vironmental, technological, system, and care changes would need to beeffected, often providing continuous intervention.
Requirements for translation/barriersA successful implementation of nonpharmacologic interventions requirescaregivers to effectively communicate with PWDs at the highest level possi-ble; to observe the PWD’s behaviors and their antecedents and consequences;to know the past habits, preferences, and identities of the PWD; to empathizewith the predicament of the PWD, who often confronts an environment thatis inexplicable to him/her with limited sensory, communicative, and cogni-tive tools; and to effectively problem solve how to best utilize the widetoolkit of interventions to address the needs of the PWD. Insight into what isneeded to achieve this level of care can be obtained from the description of aculture change initiative within a nursing-home setting. Some steps taken toprovide person-centered care include the creation of a staff coordinator andmentor position, staff and family education, organizational changes, focus-ing on tailored activities, and environmental changes [82••].
Several barriers to the implementation of nonpharmacologic interven-tions have been identified. These include staff-related barriers, such as de-nial of unmet need, refusal to provide for a need, or lack of access to aphysician; family-related barriers, such as unavailability or lack of coopera-tion in providing information about the person’s past or memorabilia tohelp devise appropriate interventions; and environmental barriers, such asuncomfortable surroundings [100]. Strategies to address barriers tononpharmacologic interventions have also been proposed. For example,within the context of bathing PWDs at home [101], it was concluded that toimprove the process of care there is a need to conduct in vivo observations to
Nonpharmacologic Treatment of Behavioral Disorders in Dementia Cohen-Mansfield 779

examine behavioral triggers and caregiver skills; to clearly identify the iden-tity of the caregiver responsible for care; to develop a trusting relationshipbetween the mentor and the caregiver; and to provide ongoing coaching,modeling and support to the caregivers.
Another practical barrier to implementation of nonpharmacologic inter-vention is the lack of clear professional expertise in this topic. While thereare nurses, social workers, psychologists, occupational therapists, and otherswho do have such expertise through their clinical or research work, this ex-pertise is unique to those individuals and not yet generally provided as partof a specific training program or certification. This is a direction for futuredevelopment.
In summation, this review indicates that the study and practice of a widerange of nonpharmacologic interventions for behavioral disorders in de-mentia is increasing. Some interventions, particularly those that are based onthe unmet needs model and utilize individually-tailored interventions, showmore promise than others. However, the existing level of evidence is limiteddue to various theoretical, methodological, and practical concerns that needto be taken into consideration in order to promote the successful investiga-tion of nonpharmacologic interventions for behavioral disorders and thedelivery of efficacious person-centered care.
AcknowledgmentThis work was supported in part by the Minerva-Stiftung Foundation grant no. 31583295000.
Compliance with Ethics Guidelines
Conflict of InterestJiska Cohen-Mansfield declares that she has no conflict of interest.
Human and Animal Rights and Informed ConsentThis article does not contain any studies with animal subjects performed by the author. With regard to theauthor’s research cited in this paper, all procedures were followed in accordance with the ethical standardsof the responsible committee on human experimentation and with the Helsinki Declaration of 1975, asrevised in 2000 and 2008.
References and Recommended ReadingPapers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. Rabinowitz J, Davidson M, De Deyn PP, Katz I,Brodaty H, Cohen-Mansfield J. Factor analysis of theCohen-Mansfield Agitation Inventory in three large
samples of nursing home patients with dementia andbehavioral disturbance. Am J Geriatr Psychiatry.2005;13:991–8.
780 DEMENTIA (E MCDADE, SECTION EDITOR)
2. Cohen-Mansfield J, Culpepper WJ, Werner P. Therelationship between cognitive function and agita-tion in senior day care participants. Int J GeriatrPsychiatry. 1995;10:585–95.
3. Cohen-Mansfield J, Werner P. Longitudinal predic-tors of non‐aggressive agitated behaviors in the el-derly. Int J Geriatr Psychiatry. 1999;14:831–44.
4. Craig D, Hart DJ, Carson R, McIlroy SP, Passmore AP.Allelic variation at the A218C tryptophan hydroxy-lase polymorphism influences agitation and aggres-sion in Alzheimer's disease. Neurosci Lett.2004;363:199–202.
5. Fisher JE, Drossel C, Yury C, Cherup S. A contextualmodel of restraint–free care for persons with de-mentia. In: Sturmey P, editor. Functional analysis inclinical treatment. London: Elsevier; 2007. p. 211–238.
6. Hall GR, Buckwalter KC. Progressively lowered stressthreshold: a conceptual model for care of adults withAlzheimer's disease. Arch Psychiatry Nurs.1987;1:399–406.
7. Cohen-Mansfield J. Theoretical frameworks for be-havioral problems in dementia. Alzheimer's CareQuarterly. 2000;1:8–21.
8. Algase D, Beck C, Kolanowski A, Whall A, Berent S,Richards K, et al. Need-driven dementia-compromised behavior: an alternative view of dis-ruptive behavior. Am J Alzheim Dis Other Dement.1996;11:10–9.
9. Cohen-Mansfield J, Deutsch LH. Agitation: subtypesand their mechanisms. Semin Clin Neuropsychiatry.1996;1:325–39.
10. Schneider LS, Dagerman K, Insel PS. Efficacy andadverse effects of atypical antipsychotics for demen-tia: meta-analysis of randomized, placebo-controlledtrials. Am J Geriat Psychiatry. 2006;14:191–210.
11. Olsson J, Bergman Å, Carlsten A, Oké T, Bernsten C,Schmidt IK, et al. Quality of drug prescribing in el-derly people in nursing homes and special care unitsfor dementia. Clin Drug Invest. 2010;30:289–300.
12. Cohen-Mansfield J, Juravel-Jaffe A, Cohen A, RasoolyI, Golander H. Physicians’ practice and familiaritywith treatment for agitation associated with demen-tia in Israeli nursing homes. Int Psychogeriatr.2013;25:236–44.
13. Ballard C, Waite J, Birks J. Atypical antipsychotics foraggression and psychosis in Alzheimer’s disease: re-view. The Cochrane Library. 2008:1–47.
14. Huybrechts K, Gerhard T, Crystal S, Olfson M, AvornJ, Levin R, et al. Differential risk of death in olderresidents in nursing homes prescribed specific anti-psychotic drugs: population based cohort study. BMJ.2012;344:977–89.
15. Kales HC, Kim HM, Zivin K, Valenstein M, SeyfriedLS, Chiang C, et al. Risk of mortality among indi-vidual antipsychotics in patients with dementia. Am JPsychiatry. 2012;169:71–9.
16. Ouslander J, Bartels S, Beck C, Beecham N, Burger S,Clark T. Consensus statement on improving thequality of mental health care in US nursing homes:management of depression and behavioral symp-toms associated with dementia. J Am Geriatr Soc.2003;51:1287–98.
17. American Psychiatric Association. Practice guidelinefor the treatment of patients with Alzheimer's diseaseand other dementias. 2nd ed. USA: American Psy-chiatric Association; 2007.
18. Salzman C, Jeste D, Meyer RE, Cohen-Mansfield J,Cummings J, Grossberg G, et al. Elderly patients withdementia-related symptoms of severe agitation andaggression: consensus statement on treatment op-tions, clinical trials methodology, and policy. J ClinPsychiatry. 2008;69:889–98.
19. Cohen-Mansfield J. Nonpharmacologic interventionsfor inappropriate behaviors in dementia: a review,summary, and critique. Am J Geriatr Psychiatry.2001;9:361–81.
20. Ueda T, Suzukamo Y, Sato M, Izumi S. Effects ofmusic therapy on behavioral and psychologicalsymptoms of dementia: a systematic review andmeta-analysis. Ageing Res Rev. 2013;12:628–41.
21. McDermott O, Crellin N, Ridder HM, Orrell M.Music therapy in dementia: a narrative synthesissystematic review. Int J Geriatr Psychiatry.2012;28:781–794.
22. Raglio A, Bellelli G, Mazzola P, Bellandi D,Giovagnoli A, Farina E, et al. Music, music therapyand dementia: a review of literature and the recom-mendations of the Italian Psychogeriatric Associa-tion. Maturitas. 2012;72:305–10.
23. Tang HJ, Vezeau T. The use of music intervention inhealthcare research: a narrative review of the litera-ture. J Nurs Res. 2010;18:174–90.
24. Marx MS, Cohen-Mansfield J, Regier NG, Dakheel-AliM, Srihari A, Thein K. The impact of different dog-related stimuli on engagement of persons with de-mentia. Am J Alzheim Dis Other Demen.2010;25:37–45.
25. Cohen-Mansfield J, Marx MS, Freedman LS, MuradH, Thein K, Dakheel-Ali M. What affects pleasure inpersons with advanced stage dementia? J PsychiatryRes. 2012;46:402–6.
26. Fung JKK, Tsang HW, Chung RC. A systematic reviewof the use of aromatherapy in treatment of behav-ioral problems in dementia. Gerontol Geriatr Int.2012;12:372–82.
27. Ballard C, O Brien J, Reichelt K, Perry E. Aromather-apy as a safe and effective treatment for the man-agement of agitation in severe dementia: the resultsof a double-blind, placebo-controlled trial withMelissa. J Clin Psychiatry. 2002;63:553–8.
28. Lin PW, Chan W, Ng BF, Lam LC. Efficacy of aro-matherapy (Lavandula angustifolia) as an interven-tion for agitated behaviours in Chinese older persons
Nonpharmacologic Treatment of Behavioral Disorders in Dementia Cohen-Mansfield 781

with dementia: a cross‐over randomized trial. Int JGeriatr Psychiatry. 2007;22:405–10.
29. Burns A, Perry E, Holmes C, Francis P, Morris J,Howes M, et al. A double-blind placebo-controlledrandomized trial of Melissa officinalis oil anddonepezil for the treatment of agitation inAlzheimer’s disease. Dement Geriatr Cogn Disord.2011;31:158–64.
30. Padilla R. Effectiveness of environment-based inter-ventions for people with Alzheimer’s disease andrelated dementias. Am J Occup Ther. 2011;65:514–22.
31. Moyle W, Murfield JE, O’Dwyer S, Van Wyk S. Theeffect of massage on agitated behaviours in olderpeople with dementia: a literature review. J ClinNurs. 2013;22:601–10.
32. Holliday-Welsh DM, Gessert CE, Renier CM. Massagein the management of agitation in nursing homeresidents with cognitive impairment. Geriatr Nurs.2009;30:108–17.
33. Moyle W, Johnston ANB, O'Dwyer ST. Exploring theeffect of foot massage on agitated behaviours in olderpeople with dementia: a pilot study. Australas JAgeing. 2011;30:159–61.
34. Suzuki M, Tatsumi A, Otsuka T, Kikuchi K, Mizuta A,Makino K, et al. Physical and psychological effects of6-week tactile massage on elderly patients with severedementia. Am J Alzheim Dis Other Demen.2010;25:680–6.
35. Weiser M, Gegenheimer H, Klein P. The effect oftherapeutic touch on behavioral symptoms and cor-tisol in persons with dementia. ForschendeKomplementärmedizin/Research in ComplementaryMedicine. 2009;16:181–9.
36. Kolanowski A, Litaker M, Buettner L, Moeller J, CostaJr PT. A randomized clinical trial of theory-basedactivities for the behavioral symptoms of dementiain nursing home residents. J Am Geriatr Soc.2011;59:1032–41.
37.• Cohen-Mansfield J, Marx MS, Dakheel-Ali M, RegierNG, Thein K, Freedman L. Can agitated behavior ofnursing home residents with dementia be preventedwith the use of standardized stimuli? J Am GeriatrSoc. 2010;58:1459–64.
This paper is important because; (1) it is one of very fewpreventive studies for behavior problems, (2) It systemati-cally compares the preventive impact of different types ofstimuli. This paper should pave the way to systematic pre-vention using more complex interventions.38. Thuné-Boyle I, Iliffe S, Cerga-Pashoja A, Lowery D,
Warner J. The effect of exercise on behavioral andpsychological symptoms of dementia: towards a re-search agenda. Int Psychogeriat. 2012;24:1046.
39. Eggermont LH, Blankevoort CG, Scherder EJ. Walk-ing and night-time restlessness in mild-to-moderatedementia: a randomized controlled trial. Age Ageing.2010;39:746–9.
40. Guzmán-García A, Hughes J, James I, Rochester L.Dancing as a psychosocial intervention in carehomes: a systematic review of the literature. Int JGeriatr Psychiatry. 2012;28:914–924.
41. Lee Y, Kim S. Effects of indoor gardening on sleep,agitation, and cognition in dementia patients: a pilotstudy. Int J Geriatr Psychiatry. 2008;23:485–9.
42.• van der Ploeg ES, Eppingstall B, Camp CJ, Runci SJ,Taffe J, et al. A randomized crossover trial to studythe effect of personalized, one-to-one interactionusing Montessori-based activities on agitation, affect,and engagement in nursing home residents with de-mentia. Int Psychogeriatr. 2013;25:565–75.
This paper demonstrates the decisive role of social contact inaffecting behavior problems and the importance of person-alized contact especially for those with language difficulties.43. Lin L, Yang M, Kao C, Wu S, Tang S, Lin J. Using
acupressure and Montessori‐based activities to de-crease agitation for residents with dementia: a cross‐over trial. J Am Geriatr Soc. 2009;57:1022–9.
44. Cohen-Mansfield J, Thein K, Dakheel-Ali M, RegierNG, Marx MS. The value of social attributes ofstimuli for promoting engagement in persons withdementia. J Nerv Ment Dis. 2010;198:586–92.
45. Cohen-Mansfield J, Werner P. Management of ver-bally disruptive behaviors in nursing home residents.J Gerontol A Biol Sci Med Sci. 1997;52A:369–77.
46.• Low L, Brodaty H, Goodenough B, Spitzer P, Bell J,Fleming R, et al. The Sydney Multisite Intervention ofLaughterBosses and ElderClowns (SMILE) study:cluster randomized trial of humor therapy in nursinghomes. BMJ Open. 2013;3.
This paper provides a novel approach to providing socialcontact by using humor therapy. It raises many questions,such as how much of the impact is attributable to the at-tention, the energy conveyed, and the caring, and how muchto actual humor. What kinds of humor are appropriate forpersons who are at different stages of dementia?47. Bernabei V, De Ronchi D, La Ferla T, Moretti F,
Tonelli L, Ferrari B, et al. Animal-assisted interven-tions for elderly patients affected by dementia orpsychiatric disorders: a review. J Psychiatry Res.2013;47:762–73.
48. McCabe BW, Baun MM, Speich D, Agrawal S. Resi-dent dog in the Alzheimer’s special care unit. West JNurs Res. 2002;24:684–96.
49. Richeson NE. Effects of animal-assisted therapy onagitated behaviors and social interactions of olderadults with dementia. Am J Alzheimers Dis OtherDemen. 2003;18:353–8.
50. Kanamori M, Suzuki M, Yamamoto K, Kanda M,Matsui Y, Kojima E, et al. A day care program andevaluation of animal-assisted therapy (AAT) for theelderly with senile dementia. Am J Alzheimers DisOther Demen. 2001;16:234–9.
51. Libin A, Cohen-Mansfield J. Therapeutic robocat fornursing home residents with dementia: preliminary
782 DEMENTIA (E MCDADE, SECTION EDITOR)

inquiry. Am J Alzheimers Dis Other Demen.2004;19:111–6.
52. O'Connor C, Smith R, Nott M, Lorang C, Mathews R.Using video simulated presence to reduce resistanceto care and increase participation of adults with de-mentia. Am J Alzheimers Dis Other Demen.2011;26:317–25.
53. Zetteler J. Effectiveness of simulated presence therapyfor individuals with dementia: a systematic reviewand meta-analysis. Aging Mental Health.2008;12:779–85.
54.• Higgins P. Using dolls to enhance the wellbeing ofpeople with dementia in residential care. Nurs Times.2010;106:18–20.
This is a thoughtful review of the potential impact of dolls asstimuli for PWD as well as the ethical and practical problemsinvolved with their use.55.• Husebo BS, Ballard C, Sandvik R, Nilsen OB,
Aarsland D. Efficacy of treating pain to reduce be-havioural disturbances in residents of nursing homeswith dementia: cluster randomised clinical trial. BMJ.2011;343.
This paper is important in that it establishes the importanceof pain treatment in order to address behavioral disorders indementia.56. Cohen-Mansfield J, Lipson S. Pain in cognitively
impaired nursing home residents: how well arephysicians diagnosing it? J Am Geriatr Soc.2002;50:1039–44.
57. Cohen-Mansfield J. Pain assessment innoncommunicative elderly persons-PAINE. Clin JPain. 2006;22:569.
58. Corbett A, Husebo B, Malcangio M, Staniland A,Cohen-Mansfield J, Aarsland D, et al. Assessment andtreatment of pain in people with dementia. Nat RevNeurol. 2012;8:264–74.
59. Inaba A, Young C, Shields D. Biting for attention: acase of dental discomfort manifesting in behaviouralproblems. Psychogeriatrics. 2011;11:242–3.
60.•• Cohen-Mansfield J, Thein K, Marx MS, Dakheel-AliM, Freedman L. Efficacy of nonpharmacologic inter-ventions for agitation in advanced dementia: a ran-domized, placebo-controlled trial. J Clin Psychiatry.2012;73:1255–61.
This paper shows the efficacy of an algorithm to addressbehavioral disorders. The algorithm is based on personaliz-ing the intervention to address the specific unmet needswithin the understanding of the person's abilities, prefer-ences, and habits. The paper also clarifies the specific inter-ventions used within the algorithm.61. Werner P, Cohen-Mansfield J, Braun J, Marx MS.
Physical restraints and agitation in nursing homeresidents. J Am Geriatr Soc. 1989;37:1122.
62. Werner P, Cohen-Mansfield J, Koroknay V, BraunJ. The impact of a restraint-reduction program onnursing home residents. Geriatr Nurs.1994;15:142–6.
63. Möhler R, Richter T, Köpke S, Meyer G. Interventionsfor preventing and reducing the use of physical re-straints in long-term geriatric care. Cochrane Data-base Syst Rev. 2011;2.
64. Cohen-Mansfield J, Parpura-Gill A. Bathing: aframework for intervention focusing on psychoso-cial, architectural and human factors considerations.Arch Gerontol Geriatr. 2007;45:121–35.
65. Sloane PD, Hoeffer B, Mitchell CM, McKenzie DA,Barrick AL, Rader J, et al. Effect of person‐centeredshowering and the towel bath on bathing-associ-ated aggression, agitation, and discomfort innursing home residents with dementia: a ran-domized, controlled trial. J Am Geriatr Soc.2004;52:1795–804.
66. Cohen-Mansfield J, Taylor JW. Hearing aid use innursing homes, Part 1: prevalence rates of hearingimpairment and hearing aid use. J Am Med Dir Assn.2004;5:283–8.
67. Petitot C, Perrot X, Collet L, Bonnefoy M.Alzheimer's disease, hearing impairment andhearing-aids: a review. Psychol NeuropsychiatryVieil. 2007;5:121–5.
68. Marquardt G, Schmieg P. Dementia-friendly archi-tecture: environments that facilitate wayfinding innursing homes. Am J Alzheimers Dis Other Demen.2009;24:333–40.
69. Calkins M. Evidence-based design for dementia.Long-Term Living. 2011;60:42–6.
70. Cohen-Mansfield J, Dakheel-Ali M, Jensen B, MarxMS, Thein K. An analysis of the relationships amongengagement, agitated behavior, and affect in nursinghome residents with dementia. Int Psychogeriatr.2012;24:742.
71. Barrick AL, Sloane P, Williams C, Mitchell M,Connell B, Wood W, et al. Impact of ambient brightlight on agitation in dementia. Int J Geriatr Psychia-try. 2010;25:1013–21.
72. Padilla DV, González MTD, Agis IF, Strizzi J,Rodríguez RA. The effectiveness of control strate-gies for dementia-driven wandering, preventingescape attempts: a case report. Int Psychogeriatr.2012;1:1–5.
73. Sato J, Nakaaki S, Torii K, Oka M, Negi A, TatsumiH, et al. Behavior management approach for agi-tated behavior in Japanese patients with dementia:a pilot study. Neuropsychiatry Dis Treat. 2013;9:9–14.
74. Richter T, Meyer G, Möhler R, Köpke S. Psychosocialinterventions for reducing antipsychotic medicationin care home residents. Cochrane Database of SystRev. 2012:1–31.
75. Teri L, Huda P, Gibbons L, Young H, van Leynseele J.STAR: a Dementia-Specific Training Program for Staffin Assisted Living Residences. Nancy Morrow-Howell, MSW, PhD, editor. Gerontologist.2005;45:686–93.
Nonpharmacologic Treatment of Behavioral Disorders in Dementia Cohen-Mansfield 783

76.• Testad I, Ballard C, Bronnick K, Aarsland D. The ef-fect of staff training on agitation and use of restraintin nursing home residents with dementia: a single-blind, randomized controlled trial. J Clin Psychiatry.2010;71:80–6.
This study describes the components of a successful stafftraining program.77. Deudon A, Maubourguet N, Gervais X, Leone E,
Brocker P, Carcaillon L, et al. Nonpharmacologicalmanagement of behavioural symptoms in nursinghomes. Int J Geriatr Psychiatry. 2009;24:1386–95.
78. Reuther S, Dichter MN, Buscher I, Vollmar HC, HolleD, Bartholomeyczik S, et al. Case conferences as in-terventions dealing with the challenging behavior ofpeople with dementia in nursing homes: a systematicreview. Cambridge J. 2011.
79. Jeon Y, Govett J, Low L, Chenoweth L, McNeill G,Hoolahan A, et al. Care planning practices for be-havioural and psychological symptoms of dementia(BPSD) in residential aged care: a pilot of an educa-tion tool kit informed by the Aged Care FundingInstrument (ACFI). Contemp Nurs. 2013:3209–49.
80. Clare L, Whitaker R, Woods RT, Quinn C, Jelley H,Hoare Z, et al. AwareCare: a pilot randomized con-trolled trial of an awareness-based staff training in-tervention to improve quality of life for residentswith severe dementia in long-term care settings. IntPsychogeriatr. 2012:128–39.
81. Beer C, Horner B, Flicker L, Scherer S, LautenschlagerNT, Bretland N, et al. A cluster-randomised trial ofstaff education to improve the quality of life ofpeople with dementia living in residential care: theDIRECT study. PloS one. 2011;6:e28155.
82.•• Burack OR, Weiner AS, Reinhardt JP. The impact ofculture change on elders’ behavioral symptoms: alongitudinal study. J Am Med Dir Assoc.2012;13:522–528.
Although the results of this study are not clear cut, the paperprovides a useful overview of the components of the culturechange undertaking.83.• Johnson DK, Niedens M, Wilson JR, Swartzendruber
L, Yeager A, Jones K. Treatment outcomes of a crisisintervention program for dementia with severe psy-chiatric complications: the Kansas Bridge Project.Gerontologist. 2013;53:102–12.
This paper describes a successful system change to addresscrises in the care of PWD in the community.84. Cohen-Mansfield J, Parpura-Gill A, Golander H.
Utilization of self-identity roles for designing inter-ventions for persons with dementia. J Gerontol BPsychol Sci Soc Sci. 2006;61:202–12.
85. Cohen-Mansfield J, Jensen B. Self-maintenanceHabits and Preferences in Elderly (SHAPE): reliabilityof reports of self-care preferences in older persons.Aging Clin Exp Res. 2007;19:61–8.
86. Cohen-Mansfield J, Libin A, Marx MS.Nonpharmacological treatment of agitation: a con-trolled trial of systematic individualized intervention.J Gerontol A Biol Sci Med Sci. 2007;62:908–16.
87. Mowrey C, Parikh PJ, Bharwani G, Bharwani M. Ap-plication of behavior-based ergonomics therapies toimprove quality of life and reduce medication usagefor Alzheimer’s/Dementia Residents. Am JAlzheimers Dis Other Demen. 2013;28:35–41.
88. Bédard A, Landreville P, Voyer P, Verreault R, VézinaJ. Reducing verbal agitation in people with dementia:evaluation of an intervention based on the satisfac-tion of basic needs. Aging Ment Health.2011;15:855–65.
89. Gitlin LN, Hauck WW, Dennis MP, Winter L. Main-tenance of effects of the home environmental skill-building program for family caregivers and individ-uals with Alzheimer's disease and related disorders. JGerontol A Biol Sci Med Sci. 2005;60:368–74.
90. Moniz Cook ED, Swift K, James I, Malouf R, De VugtM, Verhey F. Functional analysis-based interventionsfor challenging behaviour in dementia. CochraneDatabase Syst Rev. 2012;2.
91. Hulme C, Wright J, Crocker T, Oluboyede Y,House A. Non‐pharmacological approaches fordementia that informal carers might try or access:a systematic review. Int J Geriatr Psychiatry.2010;25:756–63.
92. Vernooij-Dassen M, Vasse E, Zuidema S, Cohen-Mansfield J, Moyle W. Psychosocial interventions fordementia patients in long-term care. RCT. 2010;4:19.
93. Werner P, Cohen-Mansfield J, Fischer J, Segal G.Characterization of family-generated videotapes forthe management of verbally disruptive behaviors. JAppl Gerontol. 2000;19:42–57.
94. Cooke ML, Moyle W, Shum DH, Harrison SD,Murfield JE. A randomized controlled trial exploringthe effect of music on agitated behaviours and anxi-ety in older people with dementia. Aging MentalHealth. 2010;14:905–16.
95. Beck CK, Vogelpohl TS, Rasin JH, Uriri JT, O'SullivanP, Walls R, et al. Effects of behavioral interventionson disruptive behavior and affect in dementednursing home residents. Nurs Res. 2002;51:219–28.
96. Gitlin LN, Hodgson N, Jutkowitz E, Pizzi L. The cost-effectiveness of a nonpharmacologic intervention forindividuals with dementia and family caregivers: thetailored activity program. Am J Geriat Psychiatry.2010;18:510.
97. Vink A, Zuidersma M, Boersma F, Jonge P, ZuidemaS, Slaets J. The effect of music therapy compared withgeneral recreational activities in reducing agitation inpeople with dementia: a randomised controlled trial.Int J Geriatr Psychiatry. 2012;28:1031–1038.
784 DEMENTIA (E MCDADE, SECTION EDITOR)
98. Baillon S, Van D, Prettyman R, Redman J, Rooke N,Campbell R. A comparison of the effects ofSnoezelen and reminiscence therapy on the agitatedbehaviour of patients with dementia. Int J GeriatrPsychiatry. 2004;19:1047–52.
99. Garland K, Beer E, Eppingstall B, O'Connor DW. Acomparison of two treatments of agitated behavior innursing home residents with dementia: simulatedfamily presence and preferred music. Am J GeriatrPsychiatry. 2007;15:514–21.
100. Cohen-Mansfield J, Thein K, Marx MS, Dakheel-AliM. What are the barriers to performingnonpharmacological interventions for behavioralsymptoms in the nursing home? JAMA.2012;13:400–5.
101. Mahoney EK, Trudeau SA, Penyack SE, MacLeodCE. Challenges to intervention implementation:lessons learned in the bathing persons withAlzheimer's disease at home study. Nurs Res.2006;55:S10–6.
Nonpharmacologic Treatment of Behavioral Disorders in Dementia Cohen-Mansfield 785