Nonpharmacologic Airway Clearance Techniques in...
27
Nonpharmacologic Airway Clearance Techniques in Hospitalized Patients: A Systematic Review Jeff Andrews MD, Nila A Sathe MA MLIS, Shanthi Krishnaswami MBBS MPH, and Melissa L McPheeters PhD MPH Introduction Methods Literature Search Strategy Inclusion and Exclusion Criteria Study Selection Data Extraction and Synthesis Quality (Risk of Bias) Assessment of Individual Studies Results Studies Evaluating CPT in Non-Postoperative Subjects Studies in Postoperative Subjects Discussion Sputum Weight or Volume Oxygenation and Gas Exchange Pulmonary Function Tests Need for and Progression to or Duration of Mechanical Ventilation Signs and Symptoms Exercise Tolerance Pulmonary Complications Stay Exacerbations/Hospital Readmissions Quality of Life Harms of Airway Clearance Techniques Methodologic Considerations and Limitations Future Research Summary Nonpharmacologic airway clearance techniques are used to reduce the sequelae of obstructive secretions. We systematically reviewed comparative studies of nonpharmacologic interventions that health professionals can employ to achieve mucus clearance in hospitalized or postoperative pa- tients without cystic fibrosis, over the age of 12 months. We searched MEDLINE and other data- bases from 1990 to 2012 to identify relevant literature. Two reviewers independently assessed each study against predetermined inclusion/exclusion criteria. Two reviewers also independently ex- tracted data regarding subject and intervention characteristics and outcomes, and assigned overall quality ratings. The 32 studies meeting the review criteria included 24 randomized controlled trials, 7 crossover randomized controlled trials, and one prospective cohort study. Studies were typically small and together included a total of 2,453 subjects (mean 76/study). Studies generally examined chest physical therapy/physiotherapy modalities in postoperative or critically ill subjects or those with COPD. Interventions, comparators, and populations varied considerably across studies, ham- pering our ability to draw firm conclusions. Interventions, including conventional chest physical 2160 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12
Transcript of Nonpharmacologic Airway Clearance Techniques in...

Nonpharmacologic Airway Clearance Techniquesin Hospitalized Patients: A Systematic Review
Jeff Andrews MD, Nila A Sathe MA MLIS, Shanthi Krishnaswami MBBS MPH,and Melissa L McPheeters PhD MPH
IntroductionMethods
Literature Search StrategyInclusion and Exclusion CriteriaStudy SelectionData Extraction and SynthesisQuality (Risk of Bias) Assessment of Individual Studies
ResultsStudies Evaluating CPT in Non-Postoperative SubjectsStudies in Postoperative Subjects
DiscussionSputum Weight or VolumeOxygenation and Gas ExchangePulmonary Function TestsNeed for and Progression to or Duration of Mechanical VentilationSigns and SymptomsExercise TolerancePulmonary ComplicationsStayExacerbations/Hospital ReadmissionsQuality of LifeHarms of Airway Clearance TechniquesMethodologic Considerations and LimitationsFuture Research
Summary
Nonpharmacologic airway clearance techniques are used to reduce the sequelae of obstructivesecretions. We systematically reviewed comparative studies of nonpharmacologic interventions thathealth professionals can employ to achieve mucus clearance in hospitalized or postoperative pa-tients without cystic fibrosis, over the age of 12 months. We searched MEDLINE and other data-bases from 1990 to 2012 to identify relevant literature. Two reviewers independently assessed eachstudy against predetermined inclusion/exclusion criteria. Two reviewers also independently ex-tracted data regarding subject and intervention characteristics and outcomes, and assigned overallquality ratings. The 32 studies meeting the review criteria included 24 randomized controlled trials,7 crossover randomized controlled trials, and one prospective cohort study. Studies were typicallysmall and together included a total of 2,453 subjects (mean 76/study). Studies generally examinedchest physical therapy/physiotherapy modalities in postoperative or critically ill subjects or thosewith COPD. Interventions, comparators, and populations varied considerably across studies, ham-pering our ability to draw firm conclusions. Interventions, including conventional chest physical
2160 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

therapy/physiotherapy, intrapulmonary percussive ventilation, and positive expiratory pressure,typically provided small benefits in pulmonary function, gas exchange, oxygenation, and needfor/duration of ventilation, among other outcomes, but differences between groups were generallysmall and not significant. Harms of the techniques were not consistently reported, though airwayclearance techniques were generally considered safe in studies that did comment on adverse effects.Further research with clearly characterized populations and interventions is needed to understandthe potential benefits and harms of these techniques. Key words: airway clearance techniques; chestphysical therapy; breathing exercises; airway obstruction/therapy; physical therapy modalities. [RespirCare 2013;58(12):2160–2186. © 2013 Daedalus Enterprises]
Introduction
Airway clearance techniques are intended to reduce thesequelae of obstructive secretions, which can include air-flow obstruction, wheeze, respiratory infection, dyspnea,fatigue, and reduced quality of life.1 Clearance techniquesinclude modalities such as active cycle of breathing tech-nique (ACBT), positive expiratory pressure (PEP) tech-niques such as the Flutter device, and intrapulmonary per-cussive ventilation (IPV). Conventional chest physicaltherapy or physiotherapy (CPT) approaches are frequentlyused as well, and include postural drainage, percussion,and vibration. Techniques may be categorized or groupedin multiple ways, and are often used in concert. Airwayclearance approaches may be used in individuals with im-paired cough or muscle weakness,2 impaired mucociliaryclearance,3-6 structural impairments such as bronchiecta-sis or asthma,7-9 and air-flow limitation, as seen inCOPD.7,10-12
The goal of the current project was to systematicallyreview comparative studies of nonpharmacologic interven-tions that respiratory therapists and other health profes-sionals can employ to achieve mucus clearance in hospi-talized or postoperative subjects over the age of 12 months.The American Association for Respiratory Care (AARC)
commissioned the review, and AARC committee membersparticipated in the review process. As a collaborative ef-fort, the AARC team and the Vanderbilt Evidence-BasedPractice Center developed the key questions and inclusionand exclusion criteria, and engaged in identification andreview of abstracts. The AARC members involved in thework were paired with Vanderbilt Evidence-Based Prac-tice Center staff in order to maintain rigor and protectagainst bias.
Methods
Literature Search Strategy
Detailed methods for this review and our search strate-gies can be found in the supplementary materials at http://www.rcjournal.com. Our primary literature search em-ployed the MEDLINE (via the PubMed interface) andCumulative Index of Nursing and Allied Health Literature(CINAHL) databases. Our search strategies used a com-bination of subject heading terms appropriate for each da-tabase and key words relevant to airway clearance (eg,sputum clearance, CPT). We limited searches to literaturepublished in English since 1990 to ensure that interven-tions used currently would be represented. Our searcheswere conducted in August 2012. We imported all citationsinto an electronic database and into the DistillerSR pro-gram for screening. We also manually searched the refer-ence lists of included studies and of recent narrative andsystematic reviews and meta-analyses addressing airwayclearance in adults to locate citations of potential rele-vance.
Inclusion and Exclusion Criteria
Studies needed to include subjects over 1 year of agewithout cystic fibrosis, who were receiving nonpharmaco-logic airway clearance therapies and who were either hos-pitalized (but not postoperative) or postoperative, had neu-romuscular disease or respiratory muscle weakness, or whohad impaired cough. We note that we excluded studies ofsubjects with cystic fibrosis, as the Cystic Fibrosis Foun-
The authors are affiliated with the Vanderbilt Evidence-Based PracticeCenter, Institute for Medicine and Public Health, Vanderbilt UniversityMedical Center, Nashville, Tennessee. Drs Andrews and McPheeters arealso affiliated with the Department of Obstetrics and Gynecology, Van-derbilt University Medical Center, Nashville, Tennessee.
This review was supported by the American Association for RespiratoryCare. The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
Correspondence: Melissa McPheeters PhD MPH, Vanderbilt Evidence-Based Practice Center, Institute for Medicine and Public Health, Van-derbilt University Medical Center, Suite 600, 2525 West End Avenue,Nashville TN 37203-1738. E-mail: [email protected].
DOI: 10.4187/respcare.02704
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2161

dation recently published guidelines specifically related toairway clearance.13 Studies had to report on interventionsexplicitly used for airway clearance and include a treat-ment group and an appropriate comparison group (Ta-ble 1). Comparators included other nonpharmacologicairway clearance approaches, no airway clearance inter-vention, or placebo. We also required that studies addressone of the outcomes related to the effects of the interven-tion on mucus clearance outlined in Table 1. We includedstudies with any length of follow-up and in the hospitalsetting (ie, not home- or out-patient-clinic-based).
Study Selection
Once we identified potential articles, we examined theabstracts to determine whether studies met our criteria.Two reviewers separately evaluated each abstract for in-clusion or exclusion, using an abstract review form (seethe supplementary materials at http://www.rcjournal.com).If one reviewer concluded that the article could be eligiblefor the review based on the abstract, we retained it for fulltext assessment. Two reviewers independently assessedthe full text of each included study, using a standardized
Table 1. Inclusion and Exclusion Criteria
Category Criteria
Study population Hospitalized or postoperative patients, over 1 year of age, without cystic fibrosis, and receiving nonpharmacologicairway clearance therapies
Patients with neuromuscular disease or respiratory muscle weakness, over 1 year of age, without cystic fibrosis,and receiving nonpharmacologic airway clearance therapies
Patients with impaired cough, over 1 year of age, without cystic fibrosis, and receiving nonpharmacologic airwayclearance therapies
Time period 1990–2012Publication languages English onlyAdmissible study designs Controlled trials, observational studies, including prospective cohort studiesOther criteria
Original research studies that provide sufficient detail regarding methods and results to enable use and adjustmentof the data and results
Patient population must include individuals as noted aboveMust address one or more of the following interventions:
Active cycle of breathingAutogenic drainageBronchoscopyChest physiotherapy (percussion, vibration, positioning, postural drainage)Cough assist (insufflation/exsufflation, forced expiratory technique, device)CuirassHigh-frequency chest compression vestIntrapulmonary percussive ventilationPositive expiratory pressure (PEP, oscillatory PEP, Flutter, Acapella)
Must provide baseline and outcome data for one or more of the following outcomes of interest:Time to exacerbation of disease/conditionNeed for ventilatory assistanceTime to re-admissionQuality of lifePulmonary function (FEV1, FVC, peak flow)Gas exchangeSymptoms and signs (dyspnea, cough, heart rate, breath sounds, retractions)Sputum clearance and expectoration (transport, weight, volume)Exercise toleranceOxygenation
or outcome data forAntibiotic use as affected by airway clearanceHarms (including mortality) related to airway clearance interventionsICU or hospital stayNumber of hospital admissions or hospital days
Must include extractable data on relevant outcomes, including data presented in text or tables (vs solely in figures)Must be hospital-based or in-patient-based
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2162 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

form (see the supplementary materials at http://www.rcjournal.com) that included questions stemming from ourinclusion/exclusion criteria. Disagreements between re-viewers were resolved by a third-party adjudicator. Thegroup of abstract and full text reviewers included expertclinicians and health services researchers, and we requiredthat studies be excluded by at least one clinician and onemethodologist. AARC members involved in screening werepaired with Vanderbilt Evidence-Based Practice Centerstaff in order to maintain rigor and protect against bias.
Data Extraction and Synthesis
We extracted data on study design, population charac-teristics (including age, underlying conditions, and needfor mechanical ventilation), intervention characteristics (in-cluding type and duration of intervention and concomitanttherapies), and key outcomes data into evidence tables (seethe supplementary materials at http://www.rcjournal.com).In addition to outcomes related to airway clearance inter-vention effectiveness, we extracted all data available onharms of airway clearance. Harms encompass the full rangeof specific negative effects, including the narrower defi-nition of adverse events. We determined that the differ-ences among populations, interventions, controls, and out-comemeasures renderedmeta-analysis inappropriate.Thus,our analysis was qualitative.
Quality (Risk of Bias) Assessment of IndividualStudies
We assessed quality using separate tools, as appropriateby study design. Tools included the Cochrane Risk of Biastool for randomized controlled trials (RCTs) and the New-castle-Ottawa scale for cohort studies. We rated the qualityfor key outcomes for which data were provided. If a studynoted, for example, that a given outcome was not signif-icantly different between groups but did not provide therelevant data, we did not rate quality for that outcome.Two reviewers independently assessed the quality of each
study, with final decisions made via discussion to reachconsensus or by third-party adjudication by a senior meth-odologist, as needed. We used the parameters outlined inTable 2 to translate quality ratings into final levels (good,fair, poor). We defined “good” studies as not having anyof the criteria that create a high risk of bias. For studieswith “unclear” ratings, we considered the likelihood that afactor would bias a given outcome and the importance ofthe limitation and down-graded the final level as appro-priate. Quality ratings for each outcome in the studiesreviewed can be found in the supplementary materials athttp://www.rcjournal.com.
Results
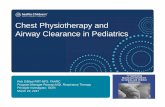
We reviewed 2,054 abstracts and 313 full-text papers,and 32 papers (representing 32 separate studies) met theinclusion criteria (Figure). The excluded studies can befound in the supplementary materials at http://www.rcjournal.com. The 32 studies that met the review criteriaincluded 24 RCTs, 7 crossover RCTs, and one prospectivecohort study (Table 3). The studies were mostly small, andtogether included a total of 2,453 subjects (mean 76 sub-jects/study). Studies typically examined CPT modalities inpostoperative or critically ill subjects or those with COPD.Subjects were typically assessed immediately following
Table 2. Quality Rating Algorithm
Low Risk ofBias Criteria
High Risk ofBias Criteria
Unclear Riskof Bias Criteria
Quality Level
7 0 0 Good6 0, 1 0, 1 Good or fair5 0, 1 1, 2 Good or fair5 2 0 Fair or poor4 0–2 0–3 Fair or poor0–3 0–7 0–7 Poor0–7 3–7 0–7 Poor0–7 0–7 4–7 Poor
Figure. Flow chart of study selection.
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2163

short-term interventions or upon hospital or ICU discharge.Five studies followed subjects for one to 6 months post-discharge.14-18
The following sections summarize the results of studiesthat met our criteria, and are categorized by interventionand comparison in those studies, including primarily hos-pitalized, non-postoperative subjects (Table 4) and thosefocused on postoperative subjects (Table 5). Several stud-ies of ICU populations included both postoperative sub-jects and subjects hospitalized for medical therapies. Wehave grouped these papers with studies of hospitalizedsubjects because their primary focus is not on the postop-erative period.
Studies Evaluating CPT in Non-PostoperativeSubjects
CPT Compared to Usual Care or Added to AnotherTreatment. Kodric and colleagues compared the “expi-ration with the glottis open in lateral posture” CPT tech-
nique (expiration group, n � 30) with standard medicaltreatment (n � 29) in subjects hospitalized with COPDexacerbation.16 Subjects in the expiration group also re-ceived standard medical therapy and were continued onmedical therapy alone after 7 days of the expiration treat-ment (two 30–40 min sessions/d). Investigators analyzedsubject respiratory data after 7 days of treatment, qualityof life (St George’s Respiratory Questionnaire [SGRQ])1 month post-discharge, and number of exacerbations andhospital admissions at 6 months post-discharge. The pri-mary outcome of sputum volume was not significantlydifferent between the groups after 7 days of treatment(mean 6.8 � 7.6 mL/d in the expiration group, 8.2 � 9.4in the medical treatment only group), though the volumechanges within each group differed significantly from base-line to follow-up (P � .001). Dyspnea (Borg scale) wassignificantly reduced in the expiration group at 7 days(3.0 � 1.8 vs 4.3 � 1.5, P � .004). Stay was similarbetween groups (mean 9.5 � 3.2 d in the expiration groupvs 10.0 � 2.4 d in the medical treatment only group). At1 month post-discharge, quality of life scores were notsignificantly different between the groups. Similarly, at 6months post-discharge, COPD exacerbations and hospital-izations did not differ significantly, though only roughly37% of subjects in each group were available at the 6-monthfollow-up. We rated the quality of all the outcome as-sessed (pulmonary function, oxygenation, dyspnea, qualityof life, sputum volume, stay, exacerbations) as poor.
In an RCT including mechanically ventilated ICU sub-jects, Templeton and Palazzo compared CPT (thoracic andpulmonary expansion; respiratory muscle exercise; and se-cretion removal via manual hyperinflation with vibration,positioning, and suctioning) with standard ICU care.21 Thefrequency and intensity of CPT could be varied at thetherapist’s discretion, and therapists were not blinded tosubjects’ group allocations. Control group subjects receivedsuctioning, mobilization, and decubitus care, though allsubjects could receive rescue CPT as needed (45 CPT and37 control group subjects required rescue CPT at any timewhile ventilated). The mean age of the 87 subjects in theCPT group was 57.7 years (median Acute Physiology andChronic Health Evaluation [APACHE] II score 49), whilethe corresponding values for the control group were58.2 years and median APACHE II score of 41. The groupswere not significantly different at baseline. Reasons forICU admission in both groups varied and included respi-ratory insufficiency (n � 21), intracerebral hemorrhage(n � 35), and gastrointestinal causes including bleedingand perforation (n � 18). The median number of days forhalf of subjects to become ventilator free was significantlylower in the control group than in the CPT group (11 d,range 3–76 d, vs 15 d, range 3–82 d, P � .045). Fourteenpercent (n � 12) of the control subjects and 12.6% (n � 11)of the CPT subjects required re-ventilation after becoming
Table 3. Overview of Included Studies
RCTCrossover
RCTProspective
CohortAll
Studies
Number of studies 24 7 1 32Population
Adult 18 7 1 26Pediatric 4 0 0 4Mixed 2 0 0 2
Underlying condition*Asthma 5 0 0 5Bronchiectasis 1 3 0 4COPD 8 2 1 11Pneumonia or other
pulmonary infection1 3 0 4
Post-surgical/criticalillness/trauma
13 3 1 17
Intervention category*Active cycle of breathing
technique0 1 0 1
Chest physical therapy 19 4 1 24High-frequency chest wall
compression1 0 0 1
Intrapulmonary percussiveventilation
3 1 0 4
Positive expiratory pressure 6 4 0 10Country
Asia 2 3 0 5Australia 4 1 1 6Europe 9 2 0 11South America 2 1 0 3United States or Canada 5 0 0 5Africa 2 0 0 2
* Numbers do not tally because studies may appear in more than one category.RCT � randomized controlled trial
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2164 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

Tab
le4.
Sum
mar
yof
Key
Find
ings
ofSt
udie
sof
Air
way
Cle
aran
cein
Hos
pita
lized
,N
on-P
osto
pera
tive
Patie
nts
Firs
tA
utho
rY
ear
Stud
yD
esig
nPo
pula
tion
Gro
ups,
nE
nrol
lmen
t/nFi
nal
Key
Find
ings
CPT
com
pare
dw
ithus
ual
care
orC
PT�
addi
tiona
ltr
eatm
ent
DiD
ario
19
2009
RC
TC
hild
ren
with
stat
usas
thm
atic
usG
1:M
echa
nica
lpe
rcus
sion
�st
anda
rdm
edic
alth
erap
y20
/19
G2:
Stan
dard
med
ical
ther
apy
20/1
9
No
chan
gein
airw
ayre
sist
ance
inbo
thgr
oups
,an
dno
diff
eren
cebe
twee
ngr
oups
over
time
Nor
mal
oxyg
ensa
tura
tion
over
time
Phas
ean
gle
decr
ease
d(P
�.0
05)
inbo
thgr
oups
over
time
Peak
flow
impr
oved
(P�
.005
)in
both
grou
psan
dov
ertim
eA
llen
dpo
ints
impr
oved
inde
pend
ent
ofC
PTPa
ludo
20
2008
RC
TC
hild
ren
hosp
italiz
edw
ithpn
eum
onia
G1:
Post
ural
drai
nage
,th
orac
icsq
ueez
ing,
perc
ussi
on,
vibr
atio
n,co
ugh
stim
ulat
ion
�st
anda
rdpn
eum
onia
trea
tmen
t51
/47
G2:
Stan
dard
pneu
mon
iatr
eatm
ent
47/4
2
Lon
ger
med
ian
dura
tion
ofco
ughi
ngin
inte
rven
tion
grou
p(P
�.0
4)N
osi
gnif
ican
tdi
ffer
ence
sbe
twee
ngr
oups
intim
eto
reso
lutio
n,st
ay,
dura
tion
offe
ver,
whe
ezin
g,cr
ackl
es,
time
tono
rmal
brea
thin
gfr
eque
ncy,
orno
rmal
oxyg
enat
ion
satu
ratio
nT
empl
eton
21
2007
RC
TA
dult
ICU
patie
nts
with
vari
ous
diag
nose
s(C
OPD
,as
thm
a,ca
rdia
car
rest
,in
tra-
cere
bral
hem
orrh
age,
seps
is,
shoc
k,ca
ncer
),in
tuba
ted
and
vent
ilate
dfo
r48
h
G1:
Posi
tioni
ng,
man
ual
hype
rinf
latio
ndr
aina
ge91
/87
G2:
Stan
dard
ICU
care
89/8
5
Mar
gina
llysi
gnif
ican
tlylo
nger
med
ian
time
tove
ntila
tor-
free
inG
1(P
�.0
47):
time
tove
ntila
tor-
free
for
50%
ofpa
tient
s:15
din
G1,
11d
inG
2N
osi
gnif
ican
tdi
ffer
ence
sin
ICU
mor
talit
yor
time
tode
ath
(11
din
G1,
13d
inG
2),
med
ian
ICU
stay
(13
din
G1,
12d
inG
2),
ortim
eto
vent
ilato
r-fr
eeby
the
time
75%
ofpa
tient
sw
ere
wea
ned
Che
n22
2009
RC
TM
echa
nica
llyve
ntila
ted
adul
tIC
Upa
tient
sG
1:Po
sitio
ning
�ch
est
vibr
atio
n50
/50
G2:
Posi
tioni
ngon
ly45
/45
Gre
ater
dry
sput
umw
eigh
tan
dlo
wer
lung
colla
pse
inde
xin
vibr
atio
ngr
oup
Gre
ates
tsp
utum
expe
ctor
atio
nin
vibr
atio
ngr
oup
occu
rred
inth
efi
rst
24h
post
-vib
ratio
nK
odri
c16
2009
RC
TA
dults
with
CO
PDex
acer
batio
nG
1:E
xpir
atio
nw
ithgl
ottis
open
inla
tera
lpo
stur
e�
stan
dard
med
ical
trea
tmen
t30
/30
G2:
Stan
dard
med
ical
trea
tmen
ton
ly29
/29
No
sign
ific
ant
diff
eren
cein
sput
umvo
lum
ebe
twee
nth
e2
grou
ps;
sign
ific
ant
redu
ctio
nin
both
grou
psat
24h
(P�
.001
)Fe
wer
exac
erba
tions
and
hosp
italiz
atio
nsin
expi
ratio
ngr
oup,
but
nosi
gnif
ican
tgr
oup
diff
eren
ces
afte
r6
mon
ths
(11
inG
1,11
inG
2)Si
gnif
ican
tde
crea
sein
dysp
nea
scor
e(P
�.0
04)
inex
pira
tion
grou
pQ
ualit
yof
life
scor
esaf
ter
1m
onth
wer
esi
mila
rin
the
grou
psN
toum
enop
oulo
s23
2002
Pros
pect
ive
coho
rtC
ritic
ally
illad
ult
ICU
patie
nts,
intu
bate
dan
dm
echa
nica
llyve
ntila
ted
for
�48
h
G1:
Post
ural
drai
nage
,po
sitio
ning
,vi
brat
ion,
coug
hing
24/2
4G
2:C
ontr
ol/s
ham
CPT
36/3
6
CPT
sign
ific
antly
asso
ciat
edw
itha
redu
ctio
nin
vent
ilato
r-as
soci
ated
pneu
mon
ia:
adju
sted
odds
ratio
0.16
,95
%C
I0.
03–0
.94
No
grou
pdi
ffer
ence
sin
ICU
stay
orm
orta
lity
95%
deve
lope
dac
ute
lung
colla
pse/
cons
olid
atio
n,bu
tno
grou
pdi
ffer
ence
s(c
ontin
ued)
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2165

Tab
le4.
Con
tinue
d
Firs
tA
utho
rY
ear
Stud
yD
esig
nPo
pula
tion
Gro
ups,
nE
nrol
lmen
t/nFi
nal
Key
Find
ings
Ash
er24
1990
RC
TC
hild
ren
with
acut
ese
vere
asth
ma
G1:
CPT
(pos
ition
ing,
late
ral
cost
albr
eath
ing,
diap
hrag
mat
icbr
eath
ing,
shou
lder
rela
xatio
n,po
stur
aldr
aina
ge,
coug
hing
,FE
T,
vibr
atio
n,w
ing
flap
ping
,pe
rcus
sion
,th
orac
icm
obili
tyex
erci
ses,
post
ural
corr
ectio
nex
erci
ses)
�m
edic
alth
erap
y19
/16
G2:
“Pla
cebo
”�
med
ical
ther
apy
19/1
8
Lun
gfu
nctio
nan
dsp
utum
wei
ght
sim
ilar
inbo
thgr
oups
aten
dof
stud
yPl
aceb
ogr
oup
had
non-
sign
ific
antly
long
erho
spita
lst
ayth
anC
PTgr
oup
CPT
com
pare
dw
ithA
CB
TC
ross
15
2010
RC
TA
dults
with
CO
PDex
acer
batio
nG
1:M
anua
lC
PTw
ithpe
rcus
sion
,th
orac
icex
pans
ion
exer
cise
s,vi
brat
ion,
peri
ods
ofre
laxe
dab
dom
inal
brea
thin
g,an
dfo
rced
expi
ratio
nte
chni
que
acco
rdin
gto
AC
BT
tech
niqu
es,
advi
ceon
posi
tioni
ng26
1/18
6G
2:A
dvic
eon
posi
tioni
ng,
coug
h,an
dsp
utum
mob
iliza
tion
acco
rdin
gto
AC
BT
266/
186
No
sign
ific
ant
diff
eren
ces
inSt
Geo
rge’
sR
espi
rato
ryQ
uest
ionn
aire
scor
es(s
ympt
om,
impa
ct,
and
activ
itysc
ores
)at
6m
onth
sN
osi
gnif
ican
tdi
ffer
ence
inot
her
outc
ome
mea
sure
s,in
clud
ing
EQ
-VA
Squ
ality
-of-
life
scor
e,E
Q-5
Dsc
ore,
brea
thle
ssne
sssc
ale
scor
e,ho
spita
lst
ay(a
t6
wee
ksor
mon
ths)
G2
had
sign
ific
antly
long
erav
erag
e6-
min
-wal
kat
6m
onth
sSy
ed25
2009
RC
T,
cros
sove
rA
dults
with
prod
uctiv
ebr
onch
iect
asis
G1:
AC
BT
18G
2:Pe
rcus
sion
,vi
brat
ion,
coug
h,an
dbr
eath
ing
tech
niqu
es17
G1/
G2:
35/3
5
No
diff
eren
cebe
twee
ngr
oups
insp
utum
wei
ght
orvo
lum
e,or
abso
lute
pulm
onar
yfu
nctio
nte
stva
lues
Sign
ific
ant
diff
eren
cein
FEV
1/F
VC
betw
een
pre
and
post
ther
apy
inbo
thgr
oups
(P�
.03)
Subj
ects
mor
eco
mfo
rtab
lew
ithA
CB
Tth
anC
PT(V
AS
P�
.004
)C
PTco
mpa
red
with
IPV
Pane
roni
26
2011
RC
T,
cros
sove
rA
dults
with
bron
chie
ctas
isad
mitt
edto
resp
irat
ory
depa
rtm
ent
G1:
CPT
:fo
rced
expi
ratio
n,po
stur
aldr
aina
ge,
perc
ussi
on,
and
vibr
atio
nG
2:In
trap
ulm
onar
ype
rcus
sive
vent
ilatio
nG
1/G
2:22
/22
No
sign
ific
ant
betw
een-
grou
pdi
ffer
ence
sin
hear
tra
te,
S pO
2,vo
lum
eor
wet
ordr
yw
eigh
tof
sput
um,
dysp
nea,
sens
atio
nof
phle
gmen
cum
bran
ceSi
gnif
ican
tlygr
eate
rde
crea
sein
brea
thin
gfr
eque
ncy
with
IPV
Hea
rtra
tede
crea
sed
sign
ific
antly
inbo
thgr
oups
Sign
ific
antly
less
post
-tre
atm
ent
disc
omfo
rtin
IPV
grou
p,al
thou
ghth
ere
was
high
vari
abili
tyA
nton
aglia
27
2006
RC
TA
dult
ICU
patie
nts
with
CO
PDex
acer
batio
nG
1:St
anda
rdhe
lmet
NIV
�pe
rcus
sion
,po
stur
aldr
aina
ge,
expi
ratio
nw
ithgl
ottis
open
inla
tera
lpo
stur
e20
/20
G2:
Hel
met
NIV
�no
ninv
asiv
eIP
V20
/20
G3:
Face
mas
kN
IV�
perc
ussi
on,
post
ural
drai
nage
,ex
pira
tion
with
glot
tisop
enin
late
ral
post
ure
(his
tori
cal
cont
rols
)40
/40
At
disc
harg
e,IP
Vgr
oup
had
low
erP a
CO
2,hi
gher
P aO
2/F I
O2,
shor
ter
mec
hani
cal
vent
ilatio
n,an
dsh
orte
rIC
Ust
ayth
anth
eot
her
2gr
oups
Blo
odga
sex
chan
ge,
hear
tra
te,
and
brea
thin
gfr
eque
ncy
impr
oved
afte
rIP
V
Clin
i18
2006
RC
TA
dult
in-p
atie
nts
with
trac
heos
tom
yad
mitt
edfo
rve
ntila
tor
wea
ning
G1:
CPT
(pos
tura
ldr
aina
ge,
man
ual
drai
nage
)pl
usIP
V24
/23
G2:
CPT
22/2
1
Sign
ific
antly
mor
epa
tient
sw
ithno
soco
mia
lpn
eum
onia
inG
2N
osi
gnif
ican
tbe
twee
n-gr
oup
diff
eren
cein
acut
ehe
mor
rhag
e,at
elec
tasi
s,P a
O2,
P aC
O2,
orpH
Sign
ific
ant
impr
ovem
ent
inP a
O2/
F IO
2an
dm
axim
alex
pira
tory
pres
sure
inIP
Vgr
oup
(con
tinue
d)
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2166 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

Tab
le4.
Con
tinue
d
Firs
tA
utho
rY
ear
Stud
yD
esig
nPo
pula
tion
Gro
ups,
nE
nrol
lmen
t/nFi
nal
Key
Find
ings
Stud
ies
eval
uatin
gPE
Pm
odal
ities
Chi
cayb
an28
2011
RC
T,
cros
sove
rM
echa
nica
llyve
ntila
ted
adul
tpa
tient
sw
ithpu
lmon
ary
infe
ctio
n
G1:
Flut
ter
G2:
Nor
mal
pres
sure
-con
trol
led
vent
ilatio
nG
1/G
2:20
/20
Flut
ter
impr
oved
sput
umpr
oduc
tion
(P�
.001
),ex
pira
tory
flow
at75
%of
tidal
volu
me
(P�
.005
),an
dP a
O2/
F IO
2
(P�
.001
)N
osi
gnif
ican
tch
ange
inre
spir
ator
yre
sist
ance
,he
art
rate
,or
mea
nar
teri
alpr
essu
reT
sang
29
2003
RC
TA
dults
with
exac
erba
tion
ofbr
onch
iect
asis
G1:
Post
ural
drai
nage
�br
eath
ing
and
coug
hing
G2:
Flut
ter
�br
eath
ing
and
coug
hing
G3:
Bre
athi
ngan
dco
ughi
ngal
one
G1/
G2/
G3:
26/1
5(5
inea
chgr
oup)
No
sign
ific
ant
diff
eren
ces
insp
utum
prod
uctio
n(w
etw
eigh
t)or
lung
func
tion
para
met
ers
amon
gth
e3
grou
ps
Sam
rans
amru
ajki
t30
2003
RC
TC
hild
ren
with
acut
e,un
com
plic
ated
asth
ma
G1:
Flut
ter
�st
anda
rdth
erap
y20
/20
G2:
Stan
dard
ther
apy
20/2
0G
1ha
dm
ore
seve
reas
thm
aat
base
line
Bot
hgr
oups
had
sign
ific
ant
incr
ease
inFV
Can
dFE
V1
onth
e1s
tan
d2n
dho
spita
lda
ysG
1ha
dhi
gher
FEV
(P�
.08)
No
betw
een-
grou
pdi
ffer
ence
inho
spita
lst
ay(P
�.3
)N
ose
riou
sad
vers
eef
fect
sin
G1
Bel
lone
31
2002
RC
TA
dults
with
CO
PDex
acer
batio
nre
quir
ing
NIV
inre
spir
ator
yIC
U
G1:
PEP
�as
sist
edco
ugh
13/1
3G
2:A
ssis
ted
coug
hon
ly14
/14
Sput
umpr
oduc
tion
atth
een
dof
trea
tmen
tw
ashi
gher
inG
1:9.
6�
3.9
gvs
4.7
�2.
5g
(P�
.01)
Mor
talit
yno
tsi
gnif
ican
tlydi
ffer
ent
betw
een
the
grou
psN
osi
gnif
ican
tch
ange
inox
ygen
satu
ratio
nin
eith
ergr
oup
Sens
atio
nof
disc
omfo
rtre
port
edw
ithPE
Pby
2pa
tient
s(1
5.3%
)A
mbr
osin
o32
1995
RC
T,
cros
sove
rA
dult
in-p
atie
nts
with
high
sput
um(�
25m
L/d
)du
eto
dise
ases
othe
rth
ancy
stic
fibr
osis
G1:
Osc
illat
ory
PEP
G2:
Post
ural
drai
nage
�pe
rcus
sion
G1/
G2:
14/1
4
No
chan
gein
expi
rato
ryfl
owor
oxyg
ensa
tura
tion
Sim
ilar
amou
ntof
sput
umpr
oduc
ed60
min
afte
rtr
eatm
ent
No
adve
rse
effe
cts
duri
ngei
ther
trea
tmen
t
Uno
ki33
2005
RC
T,
cros
sove
rA
dult
mec
hani
cally
vent
ilate
dIC
Upa
tient
sG
1:R
ibca
geco
mpr
essi
on/s
uctio
ning
G2:
Suct
ioni
ng/r
ibca
geco
mpr
essi
onG
1/G
2:14
4/31
No
impr
ovem
ent
inox
ygen
atio
n,ve
ntila
tion,
orse
cret
ion
clea
ranc
ew
ithri
bca
geco
mpr
essi
onN
osi
gnif
ican
tP a
O2/
F IO
2or
P aC
O2
diff
eren
ces
betw
een
the
2po
st-i
nter
vent
ion
peri
ods
No
sign
ific
ant
diff
eren
ces
inw
eigh
tof
colle
cted
sput
umin
the
2pe
riod
sSt
udie
sev
alua
ting
post
ural
drai
nage
Ber
ney3
420
02R
CT
,do
uble
cros
sove
rIn
tuba
ted,
vent
ilate
dan
dca
rdio
vasc
ular
lyst
able
adul
tpa
tient
s
G1:
Post
ural
drai
nage
plus
man
ual
hype
rinf
latio
n,fo
llow
edby
vent
ilato
rhy
peri
nfla
tion
G2:
Post
ural
drai
nage
plus
vent
ilato
rhy
peri
nfla
tion,
follo
wed
bym
anua
lhy
peri
nfla
tion
G1/
G2:
20
No
sign
ific
ant
diff
eren
cein
sput
umw
etw
eigh
tbe
twee
ngr
oups
(P�
.11)
Pulm
onar
yco
mpl
ianc
eim
prov
edw
ithbo
thhy
peri
nfla
tion
tech
niqu
es(P
�.0
01)
No
adve
rse
chan
ges
inhe
art
rate
,m
ean
arte
rial
pres
sure
,or
oxyg
ensa
tura
tion
(con
tinue
d)
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2167

Tab
le4.
Con
tinue
d
Firs
tA
utho
rY
ear
Stud
yD
esig
nPo
pula
tion
Gro
ups,
nE
nrol
lmen
t/nFi
nal
Key
Find
ings
Nto
umen
opou
los3
519
98R
CT
Mec
hani
cally
vent
ilate
dad
ult
trau
ma
patie
nts
G1:
Man
ual
hype
rinf
latio
n�
post
ural
drai
nage
22/1
8G
2:St
anda
rdca
re24
/16
No
betw
een-
grou
pdi
ffer
ence
inpu
lmon
ary
dysf
unct
ion
(wor
stda
ilyP a
O2/
F IO
2)N
oIC
Ude
aths
No
betw
een-
grou
pdi
ffer
ence
inIC
Ust
ay:
G1
7.4
�5.
7d,
G2
6.8
�4.
6d
Mor
eno
soco
mia
lpn
eum
onia
inG
2(P
�.0
2)K
raus
e36
2000
RC
TIn
tuba
ted
teen
/adu
ltIC
Upa
tient
sw
ithat
elec
tasi
s(a
cute
loba
r)
G1:
Post
ural
drai
nage
�pe
rcus
sion
�su
ctio
ning
9/9
G2:
Mod
ifie
dpo
stur
aldr
aina
ge�
perc
ussi
on�
suct
ioni
ng8/
8
Oxy
gena
tion
impr
oved
mor
ein
G1
than
G2
G1
requ
ired
3tr
eatm
ents
whi
leG
2re
quir
ed4.
5tr
eatm
ents
tore
solv
elu
ngco
llaps
eB
ette
rlu
ngga
sex
chan
gein
G1,
and
min
imal
chan
ges
inG
2N
osi
gnif
ican
tdi
ffer
ence
sB
arke
r37
2002
RC
TM
echa
nica
llyve
ntila
ted
adul
tIC
Upa
tient
sw
ithac
ute
lung
inju
ry
G1:
Suct
ioni
ng5/
5G
2:Su
ctio
ning
�po
sitio
ning
5/5
G3:
Suct
ioni
ng�
posi
tioni
ng�
man
ual
hype
rinf
latio
n7/
7
Sign
ific
ant
P aC
O2
chan
ge(P
�.0
3)ov
ertim
ein
all
3gr
oups
,bu
tno
diff
eren
cebe
twee
ngr
oups
(P�
.56)
P aO
2/F I
O2
did
not
alte
rin
any
grou
pSi
gnif
ican
tbe
twee
n-gr
oups
diff
eren
cein
mix
edve
nous
oxyg
ensa
tura
tion
(P�
.03)
Hea
rtra
tean
dbl
ood
pres
sure
sign
ific
antly
diff
eren
t(P
�.0
4)be
twee
ngr
oups
over
time,
but
diff
eren
ceno
tcl
inic
ally
impo
rtan
tSt
udie
sev
alua
ting
IPV
Var
gas3
820
05R
CT
Adu
ltIC
Upa
tient
sw
ithC
OPD
exac
erba
tion
G1:
IPV
2se
ssio
nspe
rda
y�
stan
dard
med
ical
ther
apy
17/1
7G
2:St
anda
rdm
edic
alth
erap
y(o
xyge
nvi
ana
sal
cann
ula
with
nebu
lized
salb
utam
olor
terb
utal
ine,
nebu
lized
ipra
trop
ium
brom
ide,
subc
utan
eous
hepa
rin,
cort
icos
tero
ids,
and
antib
iotic
)16
/16
Sign
ific
antly
less
wor
seni
ngof
exac
erba
tion
inG
1(0
%)
than
inG
2(3
5.3%
)N
oho
spita
lde
aths
inei
ther
grou
pSi
gnif
ican
tlylo
nger
stay
inG
2:6.
8�
1.0
dvs
7.9
�1.
3d,
P�
.05
Stud
ies
eval
uatin
gch
est
wal
lco
mpr
essi
onM
ahaj
an14
2011
RC
TA
dult
in-p
atie
nts
with
acut
eas
thm
aor
CO
PDG
1:H
igh-
freq
uenc
ych
est
wal
lco
mpr
essi
on25
/25
G2:
Sham
devi
ce27
/27
No
betw
een-
grou
psi
gnif
ican
tdi
ffer
ence
inad
here
nce
orsa
tisfa
ctio
nSi
gnif
ican
tlygr
eate
rim
prov
emen
tin
Bor
gsc
ore
inG
1:71
%vs
42%
,P
�.0
48N
obe
twee
n-gr
oup
sign
ific
ant
diff
eren
ces
inex
pect
orat
edsp
utum
,ch
ange
inpo
st-b
ronc
hodi
lato
rFE
V1%
,st
ay,
syst
emic
cort
icos
tero
ids
use,
orac
ute
care
visi
ts
CPT
�ch
est
phys
ioth
erap
yR
CT
�ra
ndom
ized
cont
rolle
dtr
ial
FET
�fo
rced
expi
rato
ryte
chni
que
AC
BT
�ac
tive
cycl
eof
brea
thin
gIP
V�
intr
apul
mon
ary
perc
ussi
veve
ntila
tion
NIV
�no
ninv
asiv
eve
ntila
tion
PEP
�po
sitiv
eex
pira
tory
pres
sure
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2168 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

Tab
le5.
Sum
mar
yof
Key
Find
ings
ofSt
udie
sof
Air
way
Cle
aran
ceT
echn
ique
sin
Post
oper
ativ
ePa
tient
s
Firs
tA
utho
rY
ear
Stud
yD
esig
nPo
pula
tion
Gro
ups,
nE
nrol
lmen
t/nFi
nal
Key
Find
ings
Stud
ies
ofC
PTM
acka
y39
2005
RC
TA
dults
unde
rgoi
ngab
dom
inal
surg
ery
G1:
Dee
pbr
eath
ing,
coug
hing
,hu
ffin
g,FE
T�
mob
iliza
tion
29/2
9G
2:M
obili
zatio
non
ly27
/21
No
sign
ific
ant
diff
eren
cein
inci
denc
eof
pulm
onar
yco
mpl
icat
ions
:G
117
%,
G2
15%
Sign
ific
ant
diff
eren
cein
stay
:G
110
.4�
3d,
G2
13.3
�4.
5d
(P�
.008
)D
eneh
y40
2001
RC
TA
dults
adm
itted
for
uppe
rab
dom
inal
surg
ery
G1:
CPT
(dee
pbr
eath
ing
exer
cise
s,su
stai
ned
max
imal
insp
irat
ion,
FET
,co
ughi
ng)
�C
PAP
for
15m
inG
2:C
PT�
CPA
Pfo
r30
min
G3:
CPT
only
G1,
G2,
G3:
57/5
0
Cha
nge
inox
ygen
satu
ratio
nac
ross
time
was
sign
ific
ant
(P�
.001
)N
osi
gnif
ican
tbe
twee
n-gr
oup
diff
eren
ces
infu
nctio
nal
resi
dual
capa
city
,vi
tal
capa
city
,or
S pO
2
Post
oper
ativ
eco
mpl
icat
ions
occu
rred
inal
lgr
oups
:G
111
%,
G2
6%,
G3
22%
,di
ffer
ence
not
sign
ific
ant
Lon
ger
hosp
ital
stay
inth
ose
with
com
plic
atio
ns(P
�.0
2),
but
nobe
twee
n-gr
oup
diff
eren
cein
hosp
ital
stay
deC
harm
oy41
2000
RC
TU
ncom
plic
ated
card
iac
valv
ular
surg
ery
patie
nts,
11–6
3y
old
G1:
Cou
ghas
sist
�br
eath
ing
exer
cise
16/1
6G
2:In
stru
ctio
nsfo
rco
ughi
ng14
/14
No
subj
ects
deve
lope
dpu
lmon
ary
com
plic
atio
nsN
obe
twee
n-gr
oup
diff
eren
ces
inho
spita
lst
ayor
P aO
2
Ate
lect
asis
pres
ent
onpo
stop
erat
ive
day
4,in
depe
nden
tof
trea
tmen
tFa
gevi
kO
lsen
42
1997
RC
TA
dults
unde
rgoi
ngel
ectiv
eop
enab
dom
inal
surg
ery
G1:
CPT
(ear
lym
obili
zatio
n,br
eath
ing
exer
cise
,hu
ffin
g,co
ughi
ng,
and
PEP
for
high
risk
patie
nts)
174/
172
G2:
Con
trol
(no
info
/trea
tmen
tex
cept
for
thos
ew
ithpu
lmon
ary
com
plic
atio
ns)
194/
192
Post
oper
ativ
epu
lmon
ary
com
plic
atio
nsm
ore
freq
uent
inG
2:27
%vs
6%,
P�
.001
Bet
ter
oxyg
ensa
tura
tion
inG
1N
ogr
oup
diff
eren
cein
peak
expi
rato
ryfl
ow,
FVC
,or
hosp
ital
stay
John
son4
319
96R
CT
Adu
ltsun
derg
oing
elec
tive
card
iac
valv
esu
rger
yG
1:Su
stai
ned
max
imal
insp
irat
ion
41/4
1G
2:Su
stai
ned
max
imal
insp
irat
ion
�m
anua
lpe
rcus
sion
34/3
4
Bot
hgr
oups
also
rece
ived
earl
yam
bula
tion
and
deep
brea
thin
gN
obe
twee
n-gr
oup
diff
eren
ces
inat
elec
tasi
s,re
duct
ion
inFV
C,
FEV
1,
hosp
ital
stay
,an
dIC
Ust
ayA
tdi
scha
rge,
abso
lute
valu
esof
carb
onm
onox
ide
diff
usio
nan
dne
gativ
ein
spir
ator
ypr
essu
res
wer
elo
wer
inG
2(P
�.0
2),
but
decr
ease
from
base
line
todi
scha
rge
was
sim
ilar
betw
een
the
grou
ps4
subj
ects
(2in
each
grou
p)de
velo
ped
pneu
mon
ia(o
vera
llin
cide
nce
5%)
The
rapy
cost
shi
gher
for
G2
John
son4
419
95R
CT
Adu
ltsun
derg
oing
coro
nary
arte
ryby
pass
G1
Min
imal
atel
ecta
sis:
earl
yam
bula
tion
�de
epbr
eath
ing
48G
2M
inim
alat
elec
tasi
s:ea
rly
ambu
latio
n�
deep
brea
thin
g�
sust
aine
dm
axim
alin
spir
atio
n49
G3
Ext
ensi
veat
elec
tasi
s:ea
rly
ambu
latio
n�
deep
brea
thin
g�
sust
aine
dm
axim
alin
spir
atio
n64
G4
Ext
ensi
veat
elec
tasi
s:ea
rly
ambu
latio
n�
deep
brea
thin
g�
sust
aine
dm
axim
alin
spir
atio
n�
man
ual
perc
ussi
on63
Pulm
onar
yfu
nctio
nde
teri
orat
edfr
omba
selin
eto
follo
w-u
pac
ross
all
grou
ps(P
�.0
01),
but
valu
esat
follo
w-u
pdi
dno
tdi
ffer
sign
ific
antly
Stay
was
long
erin
the
exte
nsiv
eat
elec
tasi
sgr
oups
No
betw
een-
grou
pdi
ffer
ence
inin
cide
nce
ofpn
eum
onia
:ov
eral
lin
cide
nce
12%
Hig
her
inci
denc
eof
min
orco
mpl
icat
ions
inG
4
(con
tinue
d)
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2169

ventilator-free. The median ICU stay also differed signif-icantly between the groups (13 d in CPT group, 12 d incontrol group). We rated the quality of the outcomes ofstay and need for and duration of ventilation as fair.
In a cohort study including mechanically ventilated ICUpatients, Ntoumenopoulos et al evaluated CPT comparedwith standard care for the prevention of ventilator-associ-ated pneumonia (VAP).23 CPT (n � 24 subjects, meanAPACHE II score 20.7 � 6.9) included postural drainageor positioning for at least 20 min, expiratory chest wallvibration (4 sets of 6 cycles, with coughing added forsubjects weaned from ventilator), and suctioning (� 3times). The control group (n � 36, mean APACHE IIscore 18.8 � 5.4) received sham CPT, consisting of car-diopulmonary assessment and occasional musculoskeletalphysical therapy plus re-positioning and suctioning asneeded. Both groups received standard medical and nurs-ing care, which included hemodynamic support, infectioncare, enteral nutrition, antibiotic therapy, and bronchos-copy, as needed. The subjects’ underlying conditions in-cluded COPD (6 in the CPT group, 11 in the controlgroup), cardiomyopathy (1 in the CPT group, 3 in thecontrol group), and cardiac arrest (3 in the CPT group, 5 inthe control group). Groups were similar at baseline interms of risk factors for VAP; however, among the surgi-cal subjects the American Society of Anesthesiologistsscore was higher in the control arm (P � .04). Signifi-cantly more subjects in the control arm developed VAP(14 vs 2, P � .01). The duration of ventilation, ICU stay,and number with lung collapse or consolidation were non-significantly lower in the CPT group: median ventilationdays 4.4 vs 5.2, median ICU days 5.6 vs 5.8, number withlung collapse/consolidation 23 vs 34. We rated this cohortstudy as good quality.
In an RCT that included mechanically ventilated ICUsubjects, 20–85 years old, Chen and colleagues comparedmechanical chest vibration (via vibration pad used in su-pine position, 60 min/session, 6 times/d over 72 h) plusroutine positioning in 50 subjects, to routine positioningalone in 45 subjects.22 Underlying conditions in both groupsincluded sepsis (38%), respiratory failure (37%), and sur-gery (31%). Sixteen percent of subjects had COPD, and27% had had cerebrovascular accident. The subjects werenot significantly different at baseline: mean APACHE IIscore 25.4 � 6.6 in the positioning-only group versus23.1 � 7.2 in the vibration group. Mean dry sputum weightat baseline was 5.74 � 6.23 mg/24 h in the vibration groupand 5.42 � 3.98 mg/24 h in the positioning-only group.After 72 hours, sputum weight was 4.04 � 3.43 mg/24 hin the vibration group versus 3.56 � 3.10 mg/24 h in thepositioning-only group. However, when the investigatorsused generalized estimating equations to address the lon-gitudinal nature of the data and account for correlation, thedifferences in sputum weight were significant betweenT
able
5.C
ontin
ued
Firs
tA
utho
rY
ear
Stud
yD
esig
nPo
pula
tion
Gro
ups,
nE
nrol
lmen
t/nFi
nal
Key
Find
ings
Stud
ies
ofPE
PH
aeff
ener
17
2008
RC
TA
dults
with
isch
emic
hear
tdi
seas
eun
derg
oing
coro
nary
arte
ryby
pass
graf
tsu
rger
y
G1:
Ince
ntiv
esp
irom
etry
�ex
pira
tory
PEP
21/1
7G
2:U
sual
care
22/1
7G
1ha
dbe
tter
FVC
(P�
.05)
,FE
V(P
�.0
5),
insp
irat
ory
capa
city
(P�
.01)
,an
d6-
min
wal
kdi
stan
ce(P
�.0
1),
and
few
erpo
stop
erat
ive
pulm
onar
yco
mpl
icat
ions
(P�
.004
)D
eneh
y40
2001
RC
TA
dults
adm
itted
for
uppe
rab
dom
inal
surg
ery
G2:
CPT
�C
PAP
for
30m
inG
3:C
PTon
lyG
1,G
2,G
3:57
/50
Cha
nge
inox
ygen
satu
ratio
nac
ross
time
was
sign
ific
ant
(P�
.001
)N
osi
gnif
ican
tbe
twee
n-gr
oup
diff
eren
ces
inpu
lmon
ary
func
tion
test
sor
S pO
2
Post
oper
ativ
eco
mpl
icat
ions
occu
rred
inal
lgr
oups
:G
111
%,
G2
6%,
G3
22%
,di
ffer
ence
not
sign
ific
ant
Lon
ger
hosp
ital
stay
inth
ose
with
com
plic
atio
ns(P
�.0
2),
but
nobe
twee
n-gr
oup
diff
eren
cein
stay
CPT
�ch
est
phys
ioth
erap
yR
CT
�ra
ndom
ized
cont
rolle
dtr
ial
FET
�fo
rced
expi
rato
ryte
chni
que
PEP
�po
sitiv
eex
pira
tory
pres
sure
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2170 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

groups, with sputum greater in the intervention group(P � .001). The lung collapse index of the vibration groupwas significantly improved, compared with the positioninggroup at 72 hours (mean 0.96 � 0.73 vs 1.60 � 0.91,P � .001). We rated the quality of the outcome of sputumvolume findings as poor.
Paludo et al conducted an RCT with children (29 d to12 y old) hospitalized with acute pneumonia, and com-pared twice-daily CPT and standard pneumonia therapy(n � 51) to standard treatment alone (n � 47).20 CPTsessions were 30 min in duration and included posturaldrainage, thoracic squeezing, chest percussion, vibration,cough stimulation, and suctioning as needed. Standard med-ical therapy included antibiotics, fluids, and oxygen ther-apy as needed. The subjects were similar at baseline. Therewere no significant differences at follow-up in stay, timeto normal breathing frequency, time to normal oxygensaturation, time to normal auscultation, or duration ofwheezing, crackles, or chest in-drawing. The CPT grouphad a longer median duration of coughing (5.0 d vs 4.0 d,P � .04) and longer duration of rhonchi (median 2.0 d vs0.5 d, P � .03) than the medical treatment only group. Werated the quality of the outcomes of stay and time to nor-mal breathing frequency and oxygenation as fair.
In an RCT assessing CPT as an adjunct to medicaltherapy in children with asthma, Asher and colleaguesrandomized subjects hospitalized with acute asthma to pla-cebo (n � 19) or CPT with modalities selected at thediscretion of the therapist (n � 19).24 CPT included relax-ation techniques (positioning, lateral costal or diaphrag-matic breathing, shoulder relaxation), secretion clearancetechniques (postural drainage, coughing, forced expiratorytechnique, vibration, wing flapping), thoracic mobility ex-ercises, and postural correction exercises.
Each subject received a total of 4 treatment or placebosessions. The placebo was a 20-min visit from a hospitalvolunteer who provided emotional support. CPT sessionswere 20–30 min long and included the modalities de-scribed above, selected by the therapist for each child.Relaxation techniques were most frequently used at thefirst and fourth treatment sessions (used in 95% and 84%of sessions, respectively). Secretion clearance techniqueswere used in 79% of the first treatment sessions and 74%of the fourth. The medical therapy included nebulized sal-butamol, theophylline, and steroids, and the use of medicaltherapies were similar at baseline. The subjects’ mean agewas approximately 10 years, the mean onset of asthma wasat roughly age 2, and the mean asthma severity score wasapproximately 2.3 on a scale of 1 (mild) to 3 (severe).Three children (1 in the placebo group, 2 in the CPTgroup) completed the study twice, due to readmissions.Lung function did not differ significantly between thegroups at baseline or follow-up. Sputum production wasmeasured in 26% of the CPT sessions, and the weight
range was 0.7–10.8 g. Stay was non-significantly longer inthe placebo group. We rated the quality of the outcomes ofstay and pulmonary function tests as fair.
An RCT that included children with asthma (ages 4–18 y)admitted with status asthmaticus randomized the subjectsto either CPT plus standard medical therapy (n � 20) orstandard medical therapy alone (n � 20).19 CPT included6 sessions (one each hour over 24 h) of percussion with apneumatic chest percussor for 20 min, after nebulized al-buterol administration. Medical therapy included inhaled�2 agonists and systemic steroids. The investigators mea-sured airway resistance at baseline and follow-up, withimpulse oscillometry, and the initial measurement occurreda mean 12 � 6 hours after admission; thus, the subjectshad some degree of improvement before the baseline mea-surement. Oxygen saturation did not differ from baselineto follow-up in either group, whereas peak flow improvedin both groups from baseline to follow-up (P � .005). Thedifferences in peak flow between the groups were notsignificant. Airway resistance did not change significantlyin either group from baseline to follow-up. The differencesin airway resistance between the groups as a function oftime or steroid use were not significant. We rated thequality of the outcome of oxygenation as poor.
CPT Compared With ACBT. The Management of Ex-acerbations of COPD (MATREX) RCT allocated subjectshospitalized with COPD to either CPT plus ACBT or ACBTalone.15 CPT included manual positioning, percussion dur-ing thoracic expansion, and vibration upon expiration, andACBT techniques included forced expiration. The numberand duration of CPT treatments was up to the discretion ofthe therapist, although the CPT treatments themselves werestandardized. Subjects randomized to ACBT alone receivedadvice on positioning and ACBT to mobilize sputum. Sub-jects in both groups also received standard medical ther-apy. Subjects were followed for 6 months after random-ization, and primary outcomes were scores on the SGRQand European Quality of Life-5 Dimensions (EQ-5D) andvisual analog scales (EQ-VAS). The mean age of the258 subjects randomized to the CPT group was69.08 � 9.85 years, the mean baseline SGRQ total scorewas 68.94 � 14.66, and the mean baseline EQ-VAS was44.95 � 21.03. The ACBT-only arm included 264 subjects(mean age 69.58 � 9.51 y, mean baseline SGRQ totalscore 69.13 � 14.76, mean EQ-VAS 46.64 � 21.42).Differences between the groups at baseline were not sig-nificant.
The CPT subjects received a median of 2 CPT sessions(median duration 11 min, median 2 positions/session). At6 months the between-group differences in COPD-specificquality of life were not significant in the adjusted (forbaseline value and hospital site) or unadjusted intention-to-treat analyses (mean SGRQ symptoms score effect size
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2171

in the adjusted analysis 0.04, 95% CI �0.15 to 0.23; meanSGRQ activity score effect size in the adjusted analy-sis �0.02, 95% CI �0.20 to 0.16; mean SGRQ impactscore effect size in the adjusted analysis 0.02, 95% CI�0.15 to 0.18). All of the 95% confidence intervals werewithin the study’s predefined limits for equivalence. Sim-ilarly, quality of life ratings on the EQ-VAS (effect size2.65, 95% CI �2.37 to 7.65) and EQ-5D (effect size �0.01,95% CI �0.07 to 0.06) were not significantly different inthe adjusted or the unadjusted intention-to-treat analyses.Mean stay was not significantly different between thegroups (CPT 16.02 � 16.57 d, ACBT 16.85 � 18.11 d).The mean number of hospital admissions during the6-month follow-up period was 3.47 for the CPT group and3.89 for the ACBT group (significance not reported). At6 months the control group performed significantly betteron the 6-min walk test (mean difference 83.23, 95% CI13.09–153.37). The CPT subjects reported 15 adverse,events, including increased shortness of breath (n � 5),pain (n � 5), arrhythmia (n � 3), bronchospasm (n � 1),and thoracic hematoma (n � 1). The investigators did notconsider these harms that compromised patient safety. Werated the quality of the outcomes of stay, exacerbations/readmissions, and harms of airway clearance techniques asfair, and the quality of the outcomes of dyspnea, exercisetolerance, and quality of life as poor.15
Syed et al included 35 adults with bronchiectasis in acrossover RCT that compared short-term CPT to ACBT.25
They used a convenience sample of subjects undergoingmedical therapy for bronchiectasis, allocating them to ei-ther CPT (percussion and vibration in various posturaldrainage positions, cough, and deep breathing techniquesin 20–30 min sessions every 3 h) or ACBT (huffing, deepbreathing, and relaxed breathing cycles for a maximum of30 min in various postural drainage positions). Interven-tion sequences were separated by 12 hours over 2 days.The mean age of the 35 subjects was 45.8 � 11.2 years,25 were smokers, and 17 had a history of tuberculosis. Thewet weight or volume of expectorated sputum did notdiffer significantly between treatments at follow-up (meanweight difference 0.96 � 17.7 mg, mean volume differ-ence �1.68 � 20.50 mL, P � .05). FVC, FEV1, andFEV1/FVC also did not differ between treatment sequences.The subjects rated ACBT as more comfortable on a 10 cmvisual analog scale (median 8 vs 5 for CPT, P � .004). Werated the quality of the outcomes of pulmonary functionand sputum volume as poor.
CPT Compared With IPV. Paneroni et al evaluated IPVand CPT in a crossover RCT that included 22 subjectswith bronchiectasis.26 The mean age of the subjects was64.4 � 8.9 years, and the mean percent-of-predicted FEV1
was 53 � 30%. The IPV arm included 3 active cyclesalternating high and low pressure for 30 min. CPT in-
cluded forced expiration, postural drainage, percussion,and vibration in 3 positions, for a total of 30 min. Atfollow-up there was no significant difference in mean spu-tum volume or wet or dry sputum weight between thegroups. SpO2
also did not differ between the groups. Heartrate fell significantly from baseline to follow-up in bothgroups, but did not differ between the groups. Breathingfrequency decreased significantly in the IPV group frombaseline, but not for CPT, and the difference between groupsat the final follow-up was also significant (P � .047).Dyspnea improved significantly from baseline (P � .004)in the IPV group also, but the between-group differenceswere not significant. Harms were reported by both groups,and included dry throat, nausea, and/or fatigue (27% ofboth groups). Post-treatment discomfort was lower withIPV than with CPT (P � .03). We rated the quality of theoutcomes as: oxygenation good, sputum volume fair, andheart rate, breathing frequency, dyspnea, and harms poor.
Antonaglia et al randomized subjects with COPD un-dergoing helmet noninvasive ventilation (NIV) to eitherCPT (n � 20) or IPV (n � 20).27 CPT included 25–30 minof chest percussion, mobilization, postural drainage, andexpiration with the glottis open in lateral posture. IPVconsisted of 25–30 min sessions of mouthpiece IPV de-livering high-flow mini-bursts at 225 cycles/min. The sub-jects also received medical treatments as required. Thegroups were similar at baseline: mean age 69 � 7 years inthe CPT group versus 72 � 7 years in the IPV group;median APACHE II score 22 in both groups. Twenty-seven subjects in both groups were hypersecretive (� 30 mLsecretions/d). The investigators assessed differences withan overall analysis of variance, and included data from ahistorical control group in the analysis. Differences be-tween the groups at discharge were not significant formedian breathing frequency, heart rate, or mean arterialpressure. PaCO2
and PaO2/FIO2
differed significantly betweenthe groups at discharge: mean PaCO2
: 64 � 5.2 mm Hg inthe CPT group, 58 � 5.4 in the IPV group, 67 � 4,P � .01; mean PaO2
/FIO2218 � 34.2 mm Hg in the CPT
group, 274 � 14.8 mm Hg in the IPV group,237 � 20 mm Hg in the historical control group, P � .01.The IPV group had higher PaO2
/FIO2and lower PaCO2
. Inboth groups 7 subjects required intubation and mechanicalventilation (vs NIV), but the IPV group required a lowermedian number of hours of ventilatory assistance (61 h vs89 h, P value not reported). Median ICU stay was alsolower for the IPV group (7 d vs 9 d for CPT, P value notreported). Four subjects in the CPT group and 2 in the IPVdeveloped sepsis or pneumonia (P value not reported). Werated the quality of the outcomes of gas exchange, stay,mean arterial pressure, and need for and duration of ven-tilation as fair. We rated the quality of the outcomes ofheart rate and breathing frequency as poor.
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2172 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

Clini and colleagues evaluated the effectiveness of IPVin ICU subjects with tracheostomy recently weaned frommechanical ventilation.18 The 46 subjects included 6 post-cardiac surgery subjects, 8 neuromuscular disease/impair-ment subjects, and 22 COPD or chronic respiratory insuf-ficiency subjects. The groups were similar at baseline, andall the subjects were hypersecretive (� 40 mL secretions/d). The investigators allocated the subjects to either 15 daysof IPV (2 sessions/d) plus CPT (n � 24), or CPT alone(n � 22). CPT in both groups comprised 2 one-hour ses-sions per day of postural and manual drainage, followedby nebulized saline and repeat of the drainage maneuverswith suctioning. In the IPV group PaO2
increased signifi-cantly from baseline (69 � 8 mm Hg to 76 � 9 mm Hg,P � .05), as did PaO2
/FIO2(238 � 51 mm Hg to
289 � 52 mm Hg, P � .005). Maximal expiratory pressurealso significantly increased from baseline to day 15 in theIPV group (34 cm H2O [12%] to 47 cm H2O [1%], P � .005)and as compared with the CPT-only group (P � .05). Themean differences in PaO2
/FIO2and maximal expiratory pres-
sure between the groups were, respectively, 21.65 mm Hg(95% CI �11.75 to 55.05 mm Hg, P � .04) and 9.26 mm Hg(95% CI 1.98–16.54 mm Hg, P � .01). At day 15, 2subjects in the CPT arm and one in the IPV arm had anypulmonary complications. At the 1-month follow-up, noIPV subjects had any complications, whereas 2 in the CPTgroup had pneumonia (P � .05 for comparison of pneu-monia between groups at all time points). We rated thequality of pulmonary function and gas exchange as poor.
PEP Modalities With and Without CPT. In an RCTthat included 30 subjects with bronchiectasis (mean age50.7 � 6.4 y, mean FEV1 21% of predicted), the subjectsreceived Acapella or inspiratory muscle training, in a cross-over study design.45 Acapella treatment included 10 breathsat near maximum capacity followed by breath-hold, activeexhalation, and coughing or huffing after every 5 breaths.Use of the inspiratory muscle trainer similarly included10breaths atmaximal inspiratory effort, followedbybreath-hold, active exhalation, and coughing/huffing after every 5breaths. Treatment occurred at the same time over 3 con-secutive days, with medications administered � 1 hourprior to treatment. The medications included inhaled �-ago-nists (n � 17), inhaled corticosteroids (n � 2), oral anti-biotics (n � 15), and oral corticosteroids (n � 2). Expec-torated sputum was significantly greater in the Acapellagroup: mean � SD 7.16 � 1.12 mL vs 6.46 � 1.08 mL,P � .02, mean difference 0.70 mL, 95% CI 0.13–1.27).The subjects rated Acapella as more useful in clearingsecretions, but ratings of convenience, comfort, and over-all performance did not differ significantly between themodalities. We rated the quality of the outcome of sputumvolume as poor.
In an RCT that included ICU subjects with COPD ex-acerbation, Bellone et al evaluated 3 daily, 30–40 minsessions of PEP plus assisted cough compared with as-sisted cough alone.31 All the subjects received NIV untilthey met the weaning criteria or the criteria for intubation,and all received medical therapy (nebulized salbutamol,nebulized ipratropium bromide, intravenous methylpred-nisolone, antibiotics). The subjects were similar at base-line: PEP group: n � 13, mean age 65 � 7.8 y, meanAPACHE II score 16.6 � 1.1; assisted-cough-only group:n � 14, mean age 64 � 7.7 y, mean APACHE IIscore 17 � 1.2). Sputum production was higher in the PEPgroup at the end of treatment (9.6 � 3.9 g vs 4.7 � 2.5 g,P � .01), and continued to increase in the 60 min follow-ing treatment in the PEP subjects, but not in the assisted-cough-only group. The PEP group also required fewerdays to wean from NIV (4.9 � 0.8 d vs 7.0 � 0.7 d,P � .01). No subjects in the PEP group, and one in theassisted-cough-only group progressed to intubation. PEP-related harms included discomfort from the PEP mask,reported by 2 subjects (15.3%), neither of whom stoppedtreatment during the study. We rated the quality of theoutcomes of duration of ventilation as fair, and that forsputum volume as poor.
In a crossover RCT including mechanically ventilatedICU subjects, Unoki and colleagues compared rib cagecompression (one 5-min session) plus endotracheal suc-tioning to suctioning alone.33 Intervention sequences wereseparated by 3 hours. The subjects (mean age 56.7 � 17.6 y,mean Simplified Acute Physiology score 59.4 � 10.7)were hospitalized for various causes, including intracere-bral hemorrhage (19%), cardiac arrest (19%), pneumonia(12%), and cerebral infarction (12%). Forty-two percent ofthe subjects had radiographic evidence of atelectasis. Spu-tum weight, PaO2
/FIO2, and PaCO2
did not differ signifi-cantly between the intervention periods. The quality of theoutcome of gas exchange was poor.
Studies Assessing the Flutter Valve. Ambrosino andcolleagues compared the effects of the Flutter device topostural drainage plus percussion in 14 subjects hospital-ized with COPD, bronchiectasis, bronchitis, or silicosis,on sputum production and patient discomfort in a cross-over RCT.32 Each subject underwent 2 sessions of posturaldrainage and manual chest percussion or breathing throughthe Flutter device. Each session could be conducted for upto 30 min, at the discretion of the subject, and the subjectcould cough and perform deep breathing as desired duringeach treatment. Treatments were separated by a 24-hourwash-out period, so the study extended over 8 days. Thesubjects continued their standard medical therapiesthroughout the study. At baseline the subjects produced amean of 51 � 27 mL of sputum/d and had a mean FEV1
of 49 � 26% of predicted. Sputum production increased
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2173

significantly, by roughly 10 mL, during both treatmentsequences (P � .001, compared with baseline for eachtreatment) and was non-significantly increased over base-line at 60 min post-treatment. The subjects’ self-rated feel-ings of “chest unpleasantness due to sputum” improvedsignificantly from baseline to 60 min post-treatment withboth treatment sequences (P � .001). FEV1, FVC, peakflow, and oxygen saturation remained stable and did notdiffer significantly across the time points. We rated thequality of the outcomes of pulmonary function, oxygen-ation, and sputum volume as poor.
In a single-blind RCT that included 15 subjects hospi-talized with bronchiectasis exacerbation, Tsang and Jonescompared 3 airway clearance modalities (each deliveredonce a day for 15 min until discharge): postural drainageplus breathing and coughing exercises, Flutter and breath-ing/coughing, and breathing/coughing alone.29 Each groupincluded 5 subjects with the mean age/group ranging from66.8 to 64.2 years. Mean percent-of-predicted FEV1 atbaseline ranged from 36.10% to 48.47%. The groups weresimilar at baseline, though there were more smokers in thebreathing/coughing-only group (4/5 vs 1/5 in the postural-drainage-plus-breathing/coughing group, and 3/5 in theFlutter group, P value not reported). Mean stay was sim-ilar among the groups: 7.2 � 3.3 d in the postural-drain-age-plus-breathing/coughing group, 6.2 � 3.83 d in theFlutter group, and 5.2 � 0.84 d in the breathing/coughing-only group. Similarly, the wet weight of sputum expecto-rated did not differ significantly among the groups at anytime point. FVC, FEV1, and peak expiratory flow also didnot differ significantly from baseline to follow-up withinthe groups or between the groups. The subject-rated scoresof effectiveness were higher in the Flutter group than inthe breathing/coughing-only group at all time points(P � .05). The effectiveness scores did not differ signif-icantly between the Flutter and postural-drainage-plus-breathing/coughing group. We rated the quality of the out-come of stay as fair. We rated the quality of the outcomesof pulmonary function and sputum weight as poor.
In a crossover RCT that included 20 mechanically ven-tilated subjects with pulmonary infection and hypersecre-tion in an adult ICU, Chicayban et al compared Flutter tonormal pressure controlled ventilation.28 The subjects weremechanically ventilated for a mean 21.6 days, had a meanAPACHE II score of 21.7, and 75% had VAP. The sub-jects received normal ventilation or two 15-min sessionsof Flutter, separated by a 6-hour wash-out period. At fol-low-up immediately after the intervention, secretion pro-duction was greater in the Flutter group: 5.1 � 0.5 mL vs3.3 � 0.3 mL (P � .001). In the Flutter group staticcompliance increased significantly from baseline(P � .001), as did peak flow (P � .008) and expiratoryflow at 75% of tidal volume (P � .005). Respiratory me-chanics did not change significantly in the control sub-
jects. In the Flutter group mean airway pressure increasedsignificantly from baseline (P � .05), and compared withthe control group (P � .05). The end-tidal partial pressureof CO2 increased significantly from baseline in the controlgroup (P � .05) and in the Flutter subjects as comparedwith the control group (P � .05). Oxygen saturation alsoincreased significantly in the Flutter group, compared withcontrol (P � .05). We rated as good the quality of theoutcomes of oxygenation and arterial pressure. We ratedas fair the quality of the outcomes of pulmonary function,gas exchange, heart rate, and sputum volume.
Samransamruajkit and colleagues randomized children(6–16 y old) hospitalized for acute asthma to either Flutter(15–20 min session) plus medical therapy, or medical ther-apy alone.30 Subjects in the medical therapy group alsohad instructions to cough. The baseline age and pulmonarycharacteristics were similar between the groups, except forinitial asthma score (mean 5.9 in Flutter group vs 4.45 inthe medical treatment group, P � .01) and oxygen require-ment (mean 30 in the Flutter group vs 25 in the medicaltreatment group, P � .05). At day 3 of the study thebetween-group differences in oxygen saturation, FIO2
, andasthma score were not significant; however, only 5 sub-jects in each group remained at that point. The mean post-treatment asthma score had decreased significantly in theFlutter group, compared with the medical-treatment groupon day 2 (1.3 � 0.3 vs 2.5 � 0.3, P � .01). Stay was notsignificantly different between the groups, and no seriousadverse events were reported in the Flutter group (harmsnot specified). We rated the quality of the outcomes ofoxygenation and stay as fair. We rated the quality forpulmonary function as poor.
Studies Evaluating Postural Drainage. Berney andDenehy included 20 mechanically ventilated ICU subjectsin a crossover RCT that compared postural drainage plusmanual hyperinflation followed by ventilatory hyperinfla-tion to postural drainage plus ventilator hyperinflation fol-lowed by manual hyperinflation.34 In both groups the footof the bed was elevated and the subjects were placed in aside-lying position before undergoing 6 sets of 6 manualor ventilator hyperinflation breaths and suctioning. Thesubjects received both treatments, separated by 2 hours, oneach of 2 days. The subjects (mean age 45.2 y, APACHE IIscore range 10–22) had spinal injury (n � 12, 10 withquadriplegia), multiple trauma (n � 4), respiratory failure(n � 1), and other indications. After the 2-day study themean sputum production in the manual hyperinflation groupwas 6.53 g (95% CI 5.86–7.20) and 6.01 g in the ventilatorhyperinflation group (95% CI 4.83–7.19 g); those weightsdid not differ significantly: mean difference 2.65 g, 95% CI1.79–3.54 g). Both treatments significantly improved(P � .001) static pulmonary compliance from baseline,with a mean percentage improvement of 9.7% with man-
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2174 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

ual hyperinflation (95% CI 46.5–54.9) and 11.6% withventilator hyperinflation (95% CI 45.5–54.7). Mean arte-rial pressure, heart rate, and arterial oxygen saturation didnot change adversely with either treatment. We rated thequality of the outcome of sputum weight as poor.
Ntoumenopoulos and colleagues assessed the effects ofmanual hyperinflation plus postural drainage, comparedwith usual care, on pulmonary complications in mechan-ically ventilated trauma subjects in an RCT.35 The subjectsin the manual hyperinflation group (n � 22) received 6hyperinflation breaths, repeated 4 times, in postural drain-age positions, for 20 min, plus suctioning as needed be-tween sets and routine turning. The control subjects (n � 24)received routine nursing care (suctioning as needed andturning twice an hour). The groups were similar at baseline(treatment group: mean age 38.85 � 16.62 y, meanAPACHE II score 12.3 � 3.8; control group: meanage 41.20 � 20.15 y, mean APACHE II score 14.1 � 7.4).Days on mechanical ventilation, ICU days, and level ofpulmonary dysfunction (worst daily PaO2
/FIO2) were simi-
lar between the groups at follow-up. Four subjects in thetreatment group and 8 in the control were withdrawn fromthe study per protocol, because of suspected pneumonia; 3subjects in the treatment and 4 in the control group werediagnosed with pneumonia. We rated the quality of theoutcomes of pulmonary function, stay, and duration ofventilation as good.
An RCT by Krause et al included mechanically venti-lated ICU subjects with atelectasis of the lower lobes, andcompared standard postural drainage to modified posturaldrainage.36 Subjects were 13–85 years old and had con-ditions that included bronchial obstruction (n � 2), ribfracture or surgery (n � 5), pleural effusion (n � 3),pneumonia (n � 3), Guillain-Barre syndrome (n � 1), andpneumothorax/hemothorax (n � 3). The subjects received15 min of either standard postural drainage (one of 4 po-sitions, depending on the location of lung collapse, eachincluding elevation of the foot of the bed,) following in-halation of mucolytics (n � 9), or modified postural drain-age (supine, side-lying, or 1/4 prone positioning, depend-ing on location of lung collapse) following mucolytics(n � 8). Both groups received percussion for 5 min, andsuctioning following positioning. The study did not reportwhether or not the subjects were statistically similar atbaseline. The standard drainage group required a mean of3 treatments to resolve the collapse, compared with 4.5 inthe modified-postural-drainage group (P value not re-ported). Arterial blood gas values (PaO2
, oxygen saturation,diffusion capacity, alveolar/arterial oxygen difference, re-spiratory index, and venous shunt value) improved morefrom baseline to final treatment in the standard-postural-drainage group, though the differences were not signifi-cant. We rated the quality of the outcome of gas exchangeas fair.
Barker and Adams conducted an RCT to assess theeffects of a single session of commonly used CPT modal-ities on pulmonary function and oxygenation in mechan-ically ventilated subjects with acute lung injury.37 Thesubjects were randomly allocated to either supine position-ing plus suctioning (n � 5, mean age 73 � 2.6 y), lateraldecubitus positioning plus suctioning (n � 5, mean age70 � 7.4 y), or lateral decubitus positioning plus 6 manualhyperinflation breaths plus suctioning (n � 7, mean age70 � 16.3 y). The subjects were hospitalized with sepsis(n � 7), aspiration pneumonia (n � 5), community-ac-quired pneumonia (n � 4), and pancreatitis (n � 1). Thestudy does not indicate if the baseline differences amongthe groups were significant. Venous oxygenation satura-tion did not change significantly over time within or amongthe groups, though it was lower in the lateral-decubitus-positioning-plus-suctioning group at all time points(P � .03). PaCO2
and PaO2/FIO2
also did not differ withingroups or among groups at the 60-min follow-up. Dy-namic compliance and mean arterial pressure did not differamong the groups at follow-up. Heart rate varied signifi-cantly within and among groups over time (P � .05). Werated the quality of the outcome of gas exchange as fair.We rated the quality of the outcomes of heart rate andmean arterial pressure as poor.
Studies Evaluating Intrapulmonary Percussive Venti-lation. Vargas et al conducted an RCT comparing stan-dard medical and oxygen therapy to standard therapy plusIPV via face mask in ICU subjects with COPD.38 The 16subjects in the IPV group had a mean age of 69.2 years anda mean FEV1 of 39% of predicted. Those values in thestandard therapy group were 70.2 years and 38%. Thegroups were not significantly different at baseline. IPVsubjects received the same medical treatment as the con-trol group (supplemental oxygen, nebulized salbutamol orterbutaline, nebulized ipratropium bromide, subcutaneousheparin, corticosteroids, oral methylprednisolone, antibi-otic, correction of electrolyte abnormalities) plus 2 daily30-min IPV sessions (mean duration of therapy 3 � 1 d).No subject in either group received any additional airwayclearance modalities. Six subjects in the standard treat-ment group had a worsening of exacerbation and requiredNIV, compared with 0 subjects in the IPV group (P � .05).Stay was also significantly longer in the standard therapygroup (7.9 � 1.3 d vs 6.8 � 1 d, P � .05). Breathingfrequency and PaCO2
decreased significantly from baselineto the end of the first IPV session in the IPV group, whereasPaO2
increased (P � .05); these values were not reportedfor the standard therapy group. We rated the quality of theoutcomes of pulmonary function, need for ventilation, ox-ygenation, and stay as fair. We rated the quality of theoutcome of breathing frequency as poor.
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2175

Studies Evaluating Chest Wall Compression. Mahajanand colleagues assessed hospitalized adults (� 18 y old)with physician-diagnosed acute asthma and/or COPD inan RCT sponsored by the manufacturer of the pneumaticvest evaluated.14 The investigators randomly allocated25 subjects (median age 46.5 y) to high-frequency chestwall compression (the Vest, Hill-Rom, St Paul, Minne-sota) and 27 subjects (median age 50.4 y) to sham chestwall compression, which provided a sensation of vibrationbut without air flow oscillation. The subjects also receivedstandardized medical treatment (albuterol, systemic or in-haled corticosteroids, supplemental oxygen, other medica-tions as needed). Roughly 60% of subjects in each grouphad asthma, and 40% had COPD. Baseline characteristicsdid not differ significantly between groups; subjects inboth groups had a median of one hospitalization in theyear preceding the current admission.
After 60 total minutes of treatment or sham treatmentadministered over 2 days, dyspnea was significantly im-proved in the treatment group, compared with the shamgroup (median change in Borg dyspnea score �1.5 vs 0,P � .048). The differences in spontaneously expectoratedsputum, FEV1%, and hospital stay were not significant.Four subjects in each group reported an acute care visit(hospitalization or emergency department visit) in the 30-day follow-up period. Subject satisfaction and adherenceto both the treatment and the sham treatment were high.We rated the quality of all the outcomes (pulmonary func-tion, dyspnea, sputum, stay, and time to readmission) asgood.14
Studies in Postoperative Subjects
Studies Evaluating CPT. Johnson and colleagues strat-ified subjects by degree of atelectasis in an RCT that com-pared CPT modalities of graduated intensity (combina-tions of early ambulation plus deep breathing, sustainedmaximal inspirations, and percussion) in post-coronary-artery-bypass subjects.44 The investigators randomly allo-cated subjects with minimal atelectasis on chest x-ray toeither early mobilization plus deep breathing (group 1,n � 48) or early mobilization plus deep breathing plussustained maximal inspirations (group 2, n � 49). Subjectswith marked atelectasis were allocated to either early mo-bilization plus deep breathing plus sustained maximal in-spirations (group 3, n � 64) or all of those modalities pluspercussion (group 4, n � 63). Mobilization included grad-uated increases in activity. Deep breathing instructionswere for 5 deep breaths/hour daily, recorded by the subjectin a log. Sustained maximal inspiration comprised stackedinhalations to total lung capacity, with a 5-second breath-hold, for 5 repetitions, conducted once each waking hour,with position changes as tolerated. Percussion sessions(3/d) consisted of 1 or 2 cupped hand percussions/s to the
chest wall during the total lung capacity phase of a sus-tained maximal inspiration.
The subjects were similar at baseline in all preoperativeand pulmonary function parameters except, as per proto-col, degree of atelectasis. All the pulmonary function val-ues (vital capacity, FEV1, functional residual capacity, max-imum expiratory pressure, negative inspiratory pressure,carbon monoxide diffusion) deteriorated significantly inall groups from baseline to discharge (P � .001), thoughthe discharge values did not differ significantly among thegroups. ICU stay was significantly greater (P � .05) ingroup 3 (2.3 � 0.8 d) and group 4 (2.3 � 0.6 d) than ingroups 1 or 2 (both groups stay 2.0 � 0.5 d). Hospital staywas significantly longer (P � .05) in group 3 (9 � 2.7 d)and group 4 (10 � 8.5 d) than in the other groups (8 � 1.5 dor 1.6 d). Eight subjects in group 1, 10 in group 2, 14 ingroup 3, and 13 in group 4 met the criteria for pneumonia,with an overall incidence of 12%. No subjects developedrespiratory failure, and none required repeat ICU admis-sion because of respiratory complications. Percussion wasassociated with minor complications; however, only datafor falling oxygen saturation (below 90% in 7/295 treat-ments) and tachycardia (12/295 treatments) were reported.None of those episodes was associated with important bloodpressure changes. We rated the quality of the outcomes ofpulmonary function, stay, and pulmonary complications aspoor.44
In a related study, Johnson et al randomized subjectsundergoing cardiac valve surgery to the same regimen ofeither early mobilization and deep breathing exercises plussustained maximal inspirations (group 1) or early mobili-zation, deep breathing exercises, sustained maximal inspi-rations, and 2 sessions of percussion/day (group 2).43 Thisstudy most likely involved some of the same subjects asJohnson’s earlier study in bypass subjects,44 though theprecise extent of overlap is unclear. The 41 subjects ingroup 1 and 34 in group 2 were similar in most charac-teristics at baseline; however, the subjects in group 2 wereolder, by approximately 5 years (63 � 12 years vs68 � 10 years, P � .004). Pulmonary function valuesdecreased in both groups from baseline to discharge, withchanges in FVC, functional residual capacity, FEV1%, andcarbon monoxide diffusion reaching statistical significancein both groups (P � .001). Carbon monoxide diffusionwas significantly lower in group 2 than in group 1 atdischarge (15 � 5 mL/min/mm Hg vs 10 � 2.4 mL/min/mm Hg, P � .05), as was negative inspiratory pressure(39 � 19 cm H2O vs 33 � 14 cm H2O, P � .05). Atel-ectasis scores at discharge and ICU stay and hospital staywere similar between the groups. Two subjects in eachgroup developed pneumonia, for an overall incidence of5%. No subject progressed to respiratory failure, and nonerequired ICU readmission for respiratory complications.
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2176 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

We rated the quality of all the outcomes (pulmonary func-tion, heart rate, stay, pulmonary complications) as poor.
In an RCT on CPT following cardiac valve surgery,de Charmoy and Eales allocated surgical subjects to re-ceive either coughing and mobilization instructions (n �14) or CPT (n � 16), including positioning and breathingand coughing exercises, with sessions twice a day on post-operative days 1 and 2 and once a day on days 3 and 4.41
The CPT subjects also received assisted walking at eachtreatment session. The subjects were similar at baseline,with an overall mean age of 29.72 years (range 11–63 y).PaO2
declined significantly in both groups from baseline,but the values at follow-up did not differ significantlybetween the groups. Stay did not differ between the groups.No subjects in either group developed pulmonary compli-cations, including pneumonia. We rated the quality of theoutcomes gas exchange and pulmonary complications aspoor.
In an RCT on the effectiveness of deep breathing andsputum clearance techniques in reducing post-abdominal-surgery pulmonary complications, Mackay et al random-ized 56 subjects to either early post-surgical mobilization(n � 21) or early mobilization plus deep breathing(“coached lateral basal expansion”) exercises and airwayclearance maneuvers (coughing huffing, forced expiratorytechnique).39 The deep breathing group (n � 29) receivedtherapy 3 times a day on postoperative day 1, twice a dayon days 3 and 4, and then daily until the subject wasmobile and had a clear chest assessment for 3 consecutivedays. The subjects were also encouraged to practice thedeep breathing techniques independently during each wak-ing hour. Early mobilization included graduated assistedand independent walking, as tolerated, plus leg flexionexercises, performed independently. One early-mobiliza-tion-only subject (who was later withdrawn from the study)was mistakenly given deep breathing exercises; the inves-tigators analyzed data for that subject by intention-to-treatand with the deep breathing group.
The mean age of the 50 study completers was 66 years,and the groups were similar at baseline: 14 treatment sub-jects and 11 early-mobilization-only subjects had a historyof chronic airway limitation or pulmonary disease. Sur-gery types in both groups included colectomy/hemicolec-tomy (n � 26), bowel resection (n � 4), gastrectomy/esophagectomy (n � 6), and abdominoperineal resection(n � 3). The incidence of postoperative pulmonary com-plications (defined as � 3 respiratory signs, including aus-cultation changes, fever, chest x-ray changes, and increaseor change in sputum), did not differ between the groups(17% in the treatment group vs 14% in the mobilization-only group). The absolute risk reduction was �3.0%(95% CI �0.22 to 0.19%). Stay was longer in the mobi-lization-only group (mean 13 � 4.5 d vs 10.4 � 3.0 d,P � .008, difference in means 2.9, 95% CI 0.77–5.03 d).
Mean ICU stay was similar between the groups, as was theneed for mechanical ventilation: 2 subjects in each grouprequired mechanical ventilation, for 2 d in the controlgroup, and 0.75 d in the treatment group. We rated thequality of the outcomes stay, pulmonary complications,and need for and duration of ventilation as good.39
In another RCT in post-abdominal surgery subjects, Fa-gevik Olsen et al compared preoperative and postoperativeCPT to no CPT on the incidence of pulmonary complica-tions.42 The CPT group (n � 174) underwent preoperativeCPT (10–15 min of breathing exercises, huffing and cough-ing, education about positioning and mobilization) on theday before surgery, and postoperative CPT (15–20 minsessions conducted hourly by the subject, and includingdeep breathing plus huffing and coughing) thereafter foran unspecified duration. The investigators also preopera-tively classified the subjects in each group as low or highrisk, based on age � 50 years plus one of: smoker orrecent ex-smoker, body mass index � 30 kg/m2, pulmo-nary disease with need for daily medication, or history ofother condition causing reduced ventilatory function. Highrisk subjects in the CPT group also received PEP mask forrespiratory resistance training during breathing exercises.The control subjects received no preoperative training andno postoperative CPT unless a pulmonary complicationwas diagnosed, at which point they received CPT plus PEPmask. The groups did not differ significantly at baseline.Postoperative pulmonary complications (defined as oxy-gen saturation � 92% or 2 of: fever, negative auscultation,or radiologic evidence of pneumonia or atelectasis) werediagnosed in 10 (6%) CPT subjects, 6 of whom wereconsidered high risk, and 52 (27%, 20 considered highrisk) in the control arm (P � .001). Among the obesesubjects, 3 CPT subjects and 27 control subjects developedcomplications (P � .001). One CPT subject and 13 controlsubjects were diagnosed with pneumonia, for an overallincidence rate of 4%. Vital capacity and peak expiratoryflow declined significantly in all subjects from baseline tofollow-up, but differences between groups were not sig-nificant. Hospital stay was also not significantly different(mean 8.8 � 4.5 d in the CPT group, 9.0 � 5.1 in thecontrol group). The study did not indicate the duration ormodalities of CPT provided to the 52 control subjects withpulmonary complications, who presumably received post-operative CPT per protocol. We rated the quality of theoutcomes of pulmonary function and complications, heartrate, and stay as poor.
Studies Evaluating PEP Modalities With and WithoutCPT. Denehy and colleagues compared twice-daily stan-dard CPT (coughing and deep breathing, including sus-tained maximal inspirations and forced expiratory tech-nique for a minimum of 10 min) to CPT plus either 15 or30 min sessions of CPAP, 4 times per 24 hours, in an RCT
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2177

that included post-abdominal surgery subjects.40 The in-vestigators encouraged the subjects in each group to walkearly and to perform deep breathing exercises indepen-dently each hour, though adherence to the protocol was nottracked. Among the 50 study completers, 18 were random-ized to CPT only (mean age 73.3 � 5.8 y, mean preoper-ative FEV1 2.3 � 0.6 L), 17 to 15 min of CPAP (meanage 72.5 � 6.5 y, mean FEV1 2.3 � 0.8 L), and 15 to30 min of CPAP (mean age 70.5 � 6.3 y, meanFEV1 2.4 � 0.6 L). The subjects did not differ signifi-cantly at baseline. Pulmonary function measurements (re-ported for 40/50 subjects) included vital capacity and func-tional residual capacity. Pulmonary function measurementstypically varied across the time points in each group butdid not differ significantly among groups at follow-up onpostoperative day 5. Mean oxygen saturation and stay werealso not significantly different among the groups. Nearly70% of all the subjects had some radiographic evidence oflung collapse or consolidation on the third postoperativeday. Fourteen percent of the subjects across groups (4 inthe CPT-only group, 5 in the 15-min-CPAP group, and 1in the 30-min-CPAP group) had pulmonary complications(defined as fever � 24 h, chest radiograph score of � 2,elevated white cell count, altered sputum, isolation of patho-gen in sputum, or need for additional antibiotics). Werated the quality of the outcomes of oxygenation, pulmo-nary complications, and stay as fair. We rated the qualityof the outcome of pulmonary function as poor.
Haeffener et al conducted an RCT assessing the effectsof incentive spirometry plus expiratory positive airwaypressure, compared with control techniques (coughing in-structions, deep breathing exercises, early mobilization)on pulmonary function and complications in post-coro-nary-artery-bypass-graft subjects.17 The intervention groupperformed the incentive-spirometry protocol twice a dayfor 15–20 min; therapists gradually increased expiratorypressure to a maximum of 15 cm H2O. The incentive-spirometry subjects continued the protocol at home post-discharge, with weekly telephone check-ins by study staff.Lung alterations on chest x-ray (at 1 week post-surgery)were significantly lower among the incentive-spirometrysubjects (P � .001). At the 1-month follow-up, pulmonaryfunction improved from baseline in the incentive-spirom-etry group, whereas in the control group pulmonary func-tion remained 10–26% lower than baseline. Six-min-walkdistance was higher in the incentive-spirometry group (datain figure only, P � .001). We rated the quality of theoutcomes of pulmonary function, exercise tolerance, andstay as poor.
Discussion
The 32 studies that met our review criteria typicallyreported a small magnitude of treatment effect across a
spectrum of interventions. The patient populations variedacross the studies, and included subjects with COPD, bron-chiectasis, and asthma, as well as ICU and trauma patients.The comparators used across studies also varied. While thestudies often measured the same outcomes (eg, stay, ox-ygen saturation), they varied in reporting of outcomes andhow the outcomes were measured (eg, sputum weight vssputum volume). This heterogeneity meant that meta-anal-ysis was not appropriate or feasible.
Variations of CPT were the most frequently studiedintervention, but there is no standardized method for de-livering CPT (Table 6), and inter-therapist variation andstudy technique variation may be important co-factors.Moreover, the subjects were often receiving critical carefor more than one diagnosis, and the airway clearanceoutcomes and care modalities were likely not the primarydeterminant of the subject’s condition or course of illnessor recovery. Therefore, it is difficult to ascribe importantclinical outcomes to the airway clearance intervention un-der study; and often surrogate or intermediate measureswere utilized for comparison data.
We considered most studies of poor quality for the out-comes assessed (Table 7, and see the supplementary ma-terials at http://www.rcjournal.com). Frequently used out-come measures for airway clearance techniques are limitedin their accuracy and reliability, and most are difficult totie to the effects of airway clearance specifically.12,46,47
Some measures, such as sputum weight or volume, havelimited repeatability and specificity. Similarly, pulmonaryfunction test results depend on the subject’s effort andmotivation, may be variably interpreted, and may not ac-curately reflect the effectiveness of a given clearance mo-dality.46-48 We summarize study results by key outcomesbelow.
Sputum Weight or Volume
The studies measured sputum using both weight andvolume. The measurement techniques differed: some stud-ies assessed dry weight, others wet weight, and some useddedicated collection pots or other techniques. Two studiesof poor quality for the outcome of sputum expectoratedcompared CPT and standard care and found no differencesbetween the groups.16,22 For adults with bronchiectasis, acomparison of CPT versus ACBT, rated as poor quality,reported no significant difference in sputum volume orweight.25 Similarly, for adults with bronchiectasis, a com-parison of CPT versus IPV, rated as fair quality, reportedno significant difference in sputum volume or weight.26
Three different studies (all poor quality) of subjects with 3different conditions assessed the effects of PEP versusCPT on sputum weight or in volume. Two studies reportedno significant difference between PEP and the compari-
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2178 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

son.33,45 One small study of adult ICU subjects with COPDreported more sputum in the intervention group.31
Three studies compared the Flutter device to a controlintervention: 2 poor quality studies reported no significantdifference.29,32 The third small study of ventilated adultICU subjects reported more sputum in the interventiongroup.31 One poor quality study of postural drainage re-ported no significant difference in sputum measurements,33
whereas one good quality study of chest wall compressionwith a vest in patients with asthma and COPD reported nosignificant difference in sputum between the interventiongroup and the sham vest group.14
Oxygenation and Gas Exchange
Seven studies of CPT in various populations, includingchildren with asthma,19,20,30 adults with COPD16 or bron-chiectasis,26 and mechanically ventilated or postoperativesubjects40,42 reported no significant between-group differ-ences in oxygenation. Those studies were of good,26
fair,16,19,20,42 and poor30,40 quality for this outcome. Onegood study of Flutter in mechanically ventilated subjects,
and one fair study of IPV in subjects with COPD reportedimproved oxygenation in the intervention arms.28,38
Measurement of arterial blood gases, an indirect andinvasive measure of the effectiveness of airway clear-ance interventions, was evaluated in 9 studies, all ofwhich reported no significant difference in values be-tween the groups: 2 were fair quality, and 4 were poorquality.18,32,33,36-38,41 A fair quality study of the Flutterdevice reported better values for adult ventilated subjectsin the intervention group.28 Finally, a fair quality studyreported worse values for subjects with COPD treated withCPT, compared with those treated with IPV.27
Pulmonary Function Tests
Thirteen studies, most of poor quality for pulmonarytest outcomes, reported no significant difference in valuesbetween the groups.14,17,19,24,25,29,32,34,37,40,42,43,44 Threestudies reported improved results: a poor quality study ofIPV � CPT versus CPT in ICU subjects, with COPDreported better pulmonary function tests in the interven-tion group18; and a poor quality study of spirometry plus
Table 6. Components of CPT in Studies Using CPT as a Treatment or Comparator
First Author Year CPT Components*
Paneroni26 2011 FET, postural drainage, percussion, vibration, coughingCross15 2010 Chest percussion, vibration, assisted coughing, positioningChen22 2009 Positioning, mechanical vibrationDiDario19 2009 Mechanical percussionKodric16 2009 Expiration with glottis open in lateral postureSyed25 2009 Postural drainage, manual percussion, vibration, coughing, diaphragmatic breathingPaludo20 2008 Postural drainage, thoracic squeezing, percussion, vibration, cough stimulationTempleton21 2007 Thoracic and pulmonary expansion, respiratory muscle exercise, manual hyperinflation, positioning, vibrationAntonaglia27 2006 Percussion, postural drainage, expiration with glottis open in lateral postureClini18 2006 Postural drainage, manual drainageMackay39 2005 Deep breathing, coughing, huffing, FETTsang29 2003 Postural drainage, deep breathing, coughingBarker37 2002 Positioning, manual hyperinflationBerney34 2002 Postural drainage, manual hyperinflation, ventilator hyperinflationNtoumenopoulos23 2002 Postural drainage, positioning, vibration, coughingDenehy40 2001 Deep breathing exercises, sustained maximal inspiration, FET, coughingde Charmoy41 2000 Positioning, breathing exercises, coughingKrause36 2000 Postural drainage, percussionNtoumenopoulos35 1998 Postural drainage, manual hyperinflationFagevik Olsen42 1997 Breathing exercises, coughing, huffingJohnson43 1996 Deep breathing exercises, sustained maximal inspiration, postural drainage, manual percussionAmbrosino32 1995 Postural drainage, manual chest percussionJohnson44 1995 Deep breathing exercises, sustained maximal inspiration, postural drainage, manual percussionAsher24 1990 Positioning, lateral costal breathing, diaphragmatic breathing, shoulder relaxation, postural drainage, coughing,
FET, vibration, wing flapping, percussion, thoracic mobility exercises, postural correction exercises
* Patients typically also received suctioning, early mobilization, medical therapy, and standard turning per ICU protocols.CPT � chest physiotherapyFET � forced expiratory technique
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2179

PEP compared with standard care in postoperative CABGsubjects reported better pulmonary function in the inter-vention group.17 A fair quality study reported that subjectsin the Flutter arm had better pulmonary function, com-pared with those receiving standard care.28
Need for and Progression to or Duration ofMechanical Ventilation
For CPT compared to standard care in ventilated adultICU subjects, 2 studies of fair quality reported ventilationdays. One reported no significant difference in the dura-tion,23 and the other reported a longer duration on theventilator for the CPT (intervention) group.21 A fair qual-ity study in COPD subjects receiving CPT or IPV reportedno group difference in progression to ventilation, but ashorter duration of ventilation in the IPV group.27 Anotherfair quality study of IPV in COPD subjects reported thatfewer IPV subjects progressed to ventilation,38 while in astudy of CPT in postoperative subjects, progression toventilation did not differ between the groups.39 In 2 fairquality studies of NIV31 versus routine ventilation,35 sub-jects receiving PEP31 required fewer ventilator days, butthe duration did not differ in the study of postural drain-age.35
Signs and Symptoms
Four studies rated poor quality for the outcome of heartrate included subjects with COPD,27 bronchiectasis,26 and
postoperative43 or mechanically ventilated ICU subjects.37
Differences in heart rate were not significant between thegroups in any of these studies. Similarly, 3 studies thatassessed mean arterial pressure (one good quality study ofFlutter vs usual care in mechanically ventilated ICU sub-jects, one fair quality study of IPV vs CPT in COPDsubjects, and one poor quality study comparing CPT reg-imens in mechanically ventilated subjects) reported no sig-nificant group differences.
In studies that assessed breathing frequency, one fairquality study reported no differences in time to normalbreathing frequency in children with pneumonia receivingeither CPT or CPT plus usual care.20 One study of IPV insubjects with COPD reported no significant differences.27
Subjects with COPD or bronchiectasis receiving IPV im-proved significantly, compared with those who receivedusual care in 2 poor quality studies.26,38
Two studies, one poor quality study that compared CPTto usual care in COPD patients,16 and one good qualitystudy that compared high-frequency chest wall compres-sion to placebo,14 reported significant improvements indyspnea in the intervention arms. Two poor quality studiesthat compared either IPV to CPT26 or CPT to ACBT15
reported no significant group differences.
Exercise Tolerance
Two studies were considered poor quality for the out-come of exercise tolerance.15,17 One compared CPT plusACBT to ACBT alone, and reported significantly bettertolerance among CPT subjects.15 Similarly, a small studyof PEP versus usual care in postoperative subjects foundimproved walk distance in the PEP group.17
Pulmonary Complications
For adult ventilated ICU subjects, one good quality studyof CPT found reduced risk of VAP, compared to the con-trol intervention,23 and a fair quality study of IPV andstandard care found reduced risk of VAP, compared tostandard care alone.27 In a poor quality study of chestvibration in mechanically ventilated ICU subjects, vibra-tion resulted in less atelectasis, compared to positioning.22
While studies have reported improved outcomes with in-tervention, the literature base is currently small, and theresults are imprecise. Future studies may confirm or changecurrent estimates.
For surgical patients, preoperative training reduced therisk of hospital-acquired pneumonia, compared to no pre-operative training, in a poor quality study.42 Four otherstudies of airway clearance interventions in postoperativesubjects reported no significant difference in complicationrates: one good, one fair, and 2 poor quality studies.39-41,43
Table 7. Numbers of Studies Reporting Key Outcomes, by QualityRating
Outcome
Number of Studies
GoodStudies
FairStudies
PoorStudies
Stay 2 9 5Pulmonary function 1 3 11Sputum weight/volume 1 2 8Oxygenation 2 4 4Gas exchange 0 5 3Pulmonary complications 1 2 4Duration of ventilation 1 4 0Heart rate 0 1 4Dyspnea 1 0 3Harms of airway clearance techniques 0 1 2Mean arterial pressure 1 1 1Breathing frequency 0 1 3Exercise tolerance 0 0 2Quality of life 0 0 2Need for ventilation 1 3 0Hospital readmission (time to
exacerbation)1 1 1
Total 12 37 53
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2180 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

Stay
Stay, another indirect measure of CPT effectiveness,was reported in nearly half of the studies. For CPT com-pared to standard care, 5 studies (3 of poor quality, and 2of fair quality) reported no significant difference.16,20,21,23,24
A fair quality study reported longer stay in COPD subjectstreated with CPT, compared to those treated with IPV.27
Two studies of the Flutter device reported no significantdifference in stay, compared to other standard treat-ments.29,30 A fair quality study of postural drainage andmanual inflation versus standard care reported no signifi-cant difference in stay.35
A good quality study of a chest wall compression vest insubjects with asthma or COPD reported no significant dif-ference in stay, compared to a sham vest.14 Two studies ofIPV versus standard care in ICU subjects reported shorterstay in the subjects who received IPV.18,38
Three studies of airway clearance modalities in postop-erative subjects reported shorter stay in the treatmentgroups.39,40,44 The studies reporting stay were in differentpatient populations, and used different interventions andcomparators, and stay is an indirect outcome measure, sothe studies could not be combined meaningfully.
Exacerbations/Hospital Readmissions
Three studies (one good,14 one fair,15 one poor16 qual-ity) that assessed different interventions (high-frequencychest wall compression or variations of CPT) in subjectswith COPD reported no significant group differences inthe number of admissions or exacerbations.
Quality of Life
Two poor quality studies of subjects with COPD, onethat compared CPT to ACBT,15 and one that comparedCPT with usual care,16 reported no significant group dif-ferences in quality of life as assessed on the SGRQ andother measures.
Harms of Airway Clearance Techniques
Three studies reported harms specific to the airway clear-ance modalities.15,26,34 One poor quality study noted a sig-nificantly lower incidence of harms in the IPV arm, whereasthe others did not report the significance.
Methodologic Considerations and Limitations
The small magnitude of treatment effects, the uncertainand high risks of bias of the included studies, and the smallnumber of studies that used clinically meaningful outcomessignificantly limits the potential impact of the present re-
view’s findings for individuals, guideline panels, andhealthcare policy-makers. More than half of the studieswere rated as having high risk of bias, on the basis ofallocation concealment, but this is in the face of the factthat concealment would be a major challenge in this typeof research. Prior surgical sham studies, however, wouldsuggest that it is possible. The complexity of care, and thefact that many other factors were more powerful drivers ofimportant clinical outcomes, render it difficult to tease outthe specific effect of the interventions on important clin-ical outcomes (Table 8). Indeed, the comparison is fre-quently poorly described or not described, and with “usualcare” lacking standardization, it is challenging to assessthe impact of airway clearance interventions. As shown inthe tables throughout this report, neither the interventionsnor the comparators were consistent across any subset ofstudies. There were few controls for variation in tech-nique, for example among therapists, and the interventionswere typically poorly characterized in terms of durationand quantity. In addition, the studies routinely failed toidentify or capture harms of the intervention.
Nonetheless, although the differences in effect were typ-ically not significant, it is possible that the effects aremeaningful in patients’ experience and perception. It isunclear whether small changes in pulmonary function mea-sured by sputum weight, sputum volume, and blood gasestranslate to subjective changes in patient comfort. Few ofthe studies included any assessment of comfort or qualityof life, and we suggest that comfort and quality of life areimportant areas for further exploration. Important outcomesto consider include exacerbations and health-related qual-ity of life.
Future Research
In building the body of evidence, initial studies shouldestablish the effectiveness of individual interventionsagainst placebo, and then proceed to head to head com-parisons among interventions. Without the placebo-ver-sus-intervention studies, head to head comparisons yield-ing nonsignificant results cannot establish the effectivenessof either intervention. Researchers in this field should beencouraged to use standard RCT methodology, with ran-dom sequence generation, and to develop approaches forgood allocation concealment. In this way, even small stud-ies would be more useful for providing a basis for guid-ance. However, ultimately, because of the complexity ofthe patient condition and the numerous modalities of care,large studies with the ability to match patient and carecharacteristics are essential.
The promising studies in the review should be repeatedwith rigorous methods, and with similar populations, in-terventions, comparators, and outcomes, thus enabling fu-ture meta-analysis to generate adequately powered esti-
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2181

Tab
le8.
Sign
ific
ant
Dif
fere
nces
inK
eyFi
nal
Out
com
es*
Firs
tA
utho
rA
rms
FEV
1FV
CFR
CPe
akFl
ow
Lun
g/R
espi
rato
ryC
ompl
ianc
eor
Cap
acity
Max
imal
Exp
irat
ory
Pres
sure
Sput
umW
eigh
t/V
olum
eD
yspn
eaH
eart
Rat
eB
reat
hing
Freq
uenc
y
6-M
inW
alk
Tes
t
Oxy
gen
Satu
ratio
nP a
O2
P aC
O2
P aO
2/F I
O2
Post
oper
ativ
ePu
lmon
ary
Com
plic
atio
ns†
Pneu
mon
ia/
VA
P
Hos
pita
lor IC
USt
ay
Nee
dfo
r/Pr
ogre
ssio
nto
Mec
hani
cal
Ven
tilat
ion
Dur
atio
nof
Mec
hani
cal
Ven
tilat
ion
Re-
adm
issi
ons
Qua
lity
of Lif
e
Mah
ajan
1420
11H
FCW
C0
0�
00
Sham
HFC
WC
00
–0
0
Chi
cayb
an28
2011
Flut
ter
��
�0
��
Stan
dard
vent
ilatio
n–
––
0–
–
Pane
roni
2620
11IP
V0
00
�0
CPT
00
0–
0
Nar
apar
aju45
2010
Aca
pella
�
Insp
irat
ory
mus
cle
trai
ning
–
Cro
ss15
‡20
10C
PT�
AC
BT
0�
00
AC
BT
0–
00
Che
n2220
09C
PT�
Usu
alca
re–
Kod
ric16
2009
Exp
irat
ion
with
glot
tisop
enin
late
ral
post
ure
00
�0
00
0
Usu
alca
re0
0–
00
00
DiD
ario
1920
09C
PT0
0
Usu
alca
re0
0
Syed
2520
09A
CB
T0
00
CPT
00
0
Hae
ffen
er17
2008
Spir
omet
ry�
PEP
00
00
��
��
Usu
alca
re0
00
0–
––
–
Palu
do20
2008
CPT
00
0
Usu
alca
re0
00
Tem
plet
on21
2007
CPT
00
–
Usu
alca
re0
0�
Ant
onag
lia27
§20
06IP
V0
00
00
00
0
CPT
00
00
00
00
Clin
i1820
06C
PT�
IPV
�0
0�
�
CPT
–0
0–
–
Uno
ki33
2005
Rib
cage
com
pres
sion
�su
ctio
ning
00
0
Suct
ioni
ngal
one
00
0
Var
gas38
2005
IPV
0�
��
Usu
alca
re0
––
–
Mac
kay39
2005
Bre
athi
ngan
dco
ughi
ng0
�0
0
Mob
iliza
tion
only
0–
00
Sam
rans
amru
ajki
t3020
03Fl
utte
r�
�0
0
Usu
alca
re–
–0
0
Tsa
ng29
2003
Post
ural
drai
nage
�br
eath
ing/
coug
hing
00
00
0
Flut
ter
�br
eath
ing/
coug
hing
00
00
0
(con
tinue
d)
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2182 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

Tab
le8.
Con
tinue
d
Firs
tA
utho
rA
rms
FEV
1FV
CFR
CPe
akFl
ow
Lun
g/R
espi
rato
ryC
ompl
ianc
eor
Cap
acity
Max
imal
Exp
irat
ory
Pres
sure
Sput
umW
eigh
t/V
olum
eD
yspn
eaH
eart
Rat
eB
reat
hing
Freq
uenc
y
6-M
inW
alk
Tes
t
Oxy
gen
Satu
ratio
nP a
O2
P aC
O2
P aO
2/F I
O2
Post
oper
ativ
ePu
lmon
ary
Com
plic
atio
ns†
Pneu
mon
ia/
VA
P
Hos
pita
lor IC
USt
ay
Nee
dfo
r/Pr
ogre
ssio
nto
Mec
hani
cal
Ven
tilat
ion
Dur
atio
nof
Mec
hani
cal
Ven
tilat
ion
Re-
adm
issi
ons
Qua
lity
of Lif
e
Bre
athi
ng/
coug
hing
alon
e
00
00
0
Bar
ker37
2002
Posi
tioni
ng�
man
ual
hype
rinf
latio
n�
suct
ioni
ng
00
0
Lat
eral
posi
tioni
ng�
suct
ioni
ng
00
0
Supi
nepo
sitio
ning
�su
ctio
ning
00
0
Nto
umen
opou
los23
2002
CPT
�0
0
Sham
CPT
–0
0
Ber
ney34
2002
Man
ual
hype
rinf
latio
n/ve
ntila
tor
hype
rinf
latio
n
00
Ven
tilat
orhy
peri
nfla
tion/
man
ual
hype
rinf
latio
n
00
Bel
lone
3120
02PE
P�
assi
sted
coug
h�
�
Ass
iste
dco
ugh
––
Den
ehy40
2001
CPT
00
00
0
CPT
�C
PAP
15m
in0
00
00
CPT
�C
PAP
30m
in0
00
00
deC
harm
oy41
2000
CPT
00
0
Usu
alca
re0
00
Kra
use36
2000
Post
ural
drai
nage
�pe
rcus
sion
00
0
Mod
ifie
dpo
stur
aldr
aina
ge�
perc
ussi
on
00
0
Nto
umen
opou
los35
1998
CPT
00
0
Usu
alca
re0
00
Fage
vik
Ols
en42
1997
CPT
00
0�
�0
Usu
alca
re0
00
––
0
John
son43
1996
Ear
ly mob
iliza
tion
�SM
I
00
00
00
Ear
ly mob
iliza
tion
�SM
I�
perc
ussi
on
00
00
00
(con
tinue
d)
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2183

Tab
le8.
Con
tinue
d
Firs
tA
utho
rA
rms
FEV
1FV
CFR
CPe
akFl
ow
Lun
g/R
espi
rato
ryC
ompl
ianc
eor
Cap
acity
Max
imal
Exp
irat
ory
Pres
sure
Sput
umW
eigh
t/V
olum
eD
yspn
eaH
eart
Rat
eB
reat
hing
Freq
uenc
y
6-M
inW
alk
Tes
t
Oxy
gen
Satu
ratio
nP a
O2
P aC
O2
P aO
2/F I
O2
Post
oper
ativ
ePu
lmon
ary
Com
plic
atio
ns†
Pneu
mon
ia/
VA
P
Hos
pita
lor IC
USt
ay
Nee
dfo
r/Pr
ogre
ssio
nto
Mec
hani
cal
Ven
tilat
ion
Dur
atio
nof
Mec
hani
cal
Ven
tilat
ion
Re-
adm
issi
ons
Qua
lity
of Lif
e
John
son44
1995
Ear
ly mob
iliza
tion
�de
epbr
eath
ing
(min
imal
atel
ecta
sis)
00
0�
Ear
ly mob
iliza
tion
�de
epbr
eath
ing
�SM
I(m
inim
alat
elec
tasi
s)
00
0�
Ear
ly mob
iliza
tion
�de
epbr
eath
ing
�SM
I(m
arke
dat
elec
tasi
s)
00
0–
Ear
ly mob
iliza
tion
�de
epbr
eath
ing
�SM
I�
perc
ussi
on(m
arke
dat
elec
tasi
s)
00
0–
Am
bros
ino32
1995
CPT
00
00
0
Flut
ter
00
00
0
Ash
er24
1990
CPT
00
00
0
Plac
ebo
00
00
0
*T
his
tabl
ere
port
sva
lues
/cha
nge
betw
een
grou
psat
fina
lfo
llow
-up
only
.V
alue
sty
pica
llych
ange
dfr
omba
selin
eto
follo
w-u
pw
ithin
each
grou
p.H
arm
sof
airw
aycl
eara
nce
tech
niqu
esw
ere
also
asse
ssed
in3
stud
ies,
14,2
5,30
but
sign
ific
ance
was
not
typi
cally
asse
ssed
.O
nest
udy25
repo
rted
asi
gnif
ican
tlylo
wer
inci
denc
eof
harm
sin
the
IPV
arm
.E
mpt
yce
ll�
outc
omes
not
asse
ssed
inst
udy.
†Pu
lmon
ary
com
plic
atio
nsas
defi
ned
inst
udy
‡N
umbe
rof
exac
erba
tions
requ
irin
gho
spita
lizat
ions
give
n,bu
tsi
gnif
ican
ceno
tre
port
ed.
§Si
gnif
ican
cere
port
edin
clud
esda
tafo
rhi
stor
ical
cont
rol
grou
p;di
ffer
ence
sbe
twee
nac
tive
inte
rven
tion
grou
psno
tcl
ear.
��
valu
e/ch
ange
sign
ific
antly
bette
rfo
rgr
oup
indi
cate
dth
anfo
rot
her
grou
p.–
�va
lue/
chan
gesi
gnif
ican
tlyw
orse
for
grou
pin
dica
ted
than
for
othe
rgr
oup.
0�
nosi
gnif
ican
tdi
ffer
ence
betw
een
grou
ps.
CPT
�ch
est
phys
ioth
erap
yH
FCW
C�
high
-fre
quen
cych
est
wal
lco
mpr
essi
onIP
V�
intr
apul
mon
ary
perc
ussi
veve
ntila
tion
PEP
�po
sitiv
eex
pira
tory
pres
sure
SMI
�su
stai
ned
max
imal
insp
irat
ion
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2184 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12

mates of effect. The elements of the intervention should bestandardized, and the characteristics of the comparator welldescribed. As a field, respiratory care should consider as-sessing the degree to which study outcomes are clinicallymeaningful, and agreeing on a set of core outcomes forfuture work.
Summary
In summary, the 32 studies included in this review pro-vide limited evidence for the effectiveness of nonpharma-cologic airway clearance techniques. The evidence we re-viewed indicates that airway clearance techniques areprobably safe for ventilated ICU patients, and confer zeroto small benefit to some clinical outcomes.18,21-23,28,33–37
Consideration may be given to the use of airway clearancetechniques for ventilated ICU patients, to reduce the riskof acquiring pneumonia, based upon 2 studies, which in-cluded 76 subjects.23,27 Based on the current limitedevidence, airway clearance modalities might not be rec-ommended as routine prophylaxis to prevent postopera-tive pulmonary complications in adults.39-43 Similarly,in people with COPD, data from 6 single studies thatspecifically targeted COPD did not provide evidence ofsignificant short-term benefit from airway clearancemodalities.14-16,27,31,38
Our finding of limited evidence is in line with similar,recent reviews of airway clearance in patients with COPDand pneumonia, which have generally found small bene-fits.11,12,49,50 The interventions, comparators, and popula-tions varied considerably across the studies, hamperingour ability to draw firm conclusions. The interventions,including conventional CPT, IPV, and PEP, typically pro-vided small benefits to pulmonary function, gas exchange,oxygenation, and the need for or duration of ventilation,among other outcomes, but the between-group differenceswere generally small and not significant. The harms ofairway clearance techniques were not consistently reported,though airway clearance techniques were generally con-sidered safe in studies that did comment on adverse ef-fects. Further research with clearly characterized popula-tions and interventions is needed to understand the potentialbenefits and harms of these techniques.
ACKNOWLEDGMENTS
We gratefully acknowledge the contributions of the American Associa-tion for Respiratory Care (AARC) Airway Clearance Clinical PracticeGuidelines Committee, whose insights on scoping the literature and re-viewing the studies were invaluable. The committee includes RichardBranson MSc RRT FAARC, Gail Drescher MA RRT, Carl Haas MLSRRT FAARC, Dean Hess PhD RRT FAARC, Ray Masferrer RRTFAARC, Catherine O’Malley RRT-NPS, Bruce Rubin MD MEngr MBAFAARC, Shawna Strickland PhD RRT-NPS AE-C FAARC, Teresa Vol-sko MHHS RRT FAARC.
REFERENCES
1. Laurent GJ, Shapiro SD. Encyclopedia of respiratory medicine. Am-sterdam: Elsevier 2006:332-343.
2. Reid WD, Brown JA, Konnyu KJ, Rurak JM, Sakakibara BM. Phys-iotherapy secretion removal techniques in people with spinal cordinjury: a systematic review. J Spinal Cord Med 2010;33(4):353-370.
3. McCool FD, Rosen MJ. Nonpharmacologic airway clearance thera-pies: ACCP evidence-based clinical practice guidelines. Chest 2006;129(1 Suppl):250S-259S.
4. Main E. What is the best airway clearance technique in cystic fibro-sis? Paediatr Respir Rev 2013;14(Suppl 1):10-12.
5. Pisi G, Chetta A. Airway clearance therapy in cystic fibrosis patients.Acta Biomed 2009;80(2):102-106.
6. Bradley JM, Moran FM, Elborn JS. Evidence for physical therapies(airway clearance and physical training) in cystic fibrosis: an over-view of five Cochrane systematic reviews. Respir Med 2006;100(2):191-201.
7. Jones AP, Rowe BH. Bronchopulmonary hygiene physical therapyfor chronic obstructive pulmonary disease and bronchiectasis. Co-chrane Database Syst Rev 2000;(2):CD000045.
8. Schechter MS. Airway clearance applications in infants and children.Respir Care 2007;52(10):1382-1390, discussion 1390-1391.
9. Bruurs ML, van der Giessen LJ, Moed H. The effectiveness ofphysiotherapy in patients with asthma: a systematic review of theliterature. Respir Med 2013;107(4):483-494.
10. Jones A, Rowe BH. Bronchopulmonary hygiene physical therapy inbronchiectasis and chronic obstructive pulmonary disease: a system-atic review. Heart Lung 2000;29(2):125-135.
11. Hill K, Patman S, Brooks D. Effect of airway clearance techniquesin patients experiencing an acute exacerbation of chronic obstructivepulmonary disease: a systematic review. Chron Respir Dis 2010;7(1):9-17.
12. Osadnik CR, McDonald CF, Jones AP, Holland AE. Airway clear-ance techniques for chronic obstructive pulmonary disease. CochraneDatabase Syst Rev 2012;3:3.
13. Flume PA, Robinson KA, O’Sullivan BP, Finder JD, Vender RL,Willey-Courand DB, et al. Cystic fibrosis pulmonary guidelines:airway clearance therapies. Respir Care 2009;54(4):522-537.
14. Mahajan AK, Diette GB, Hatipoglu U, Bilderback A, Ridge A, Har-ris VW, et al. High frequency chest wall oscillation for asthma andchronic obstructive pulmonary disease exacerbations: a randomizedsham-controlled clinical trial. Respir Res 2011;12:120.
15. Cross J, Elender F, Barton G, Clark A, Shepstone L, Blyth A, et al.A randomised controlled equivalence trial to determine the effec-tiveness and cost-utility of manual chest physiotherapy techniques inthe management of exacerbations of chronic obstructive pulmonarydisease (MATREX). Health Technol Assess 2010;14(23):1-147, iii-iv.
16. Kodric M, Garuti G, Colomban M, Russi B, Porta RD, Lusuardi M,et al. The effectiveness of a bronchial drainage technique (ELTGOL)in COPD exacerbations. Respirology 2009;14(3):424-428.
17. Haeffener MP, Ferreira GM, Barreto SS, Arena R, Dall’Ago P.Incentive spirometry with expiratory positive airway pressure re-duces pulmonary complications, improves pulmonary function and6-minute walk distance in patients undergoing coronary artery by-pass graft surgery. Am Heart J 2008;156(5):900, e901-e908.
18. Clini EM, Antoni FD, Vitacca M, Crisafulli E, Paneroni M, Chezzi-Silva S, et al. Intrapulmonary percussive ventilation in tracheos-tomized patients: a randomized controlled trial. Intensive Care Med2006;32(12):1994-2001.
19. DiDario AG, Whelan MA, Hwan WH, Yousef E, Cox TJ, OldhamHM, et al. Efficacy of chest physiotherapy in pediatric patients withacute asthma exacerbations. Pediatr Asthma Allergy Immunol 2009;22(2):69-74.
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12 2185

20. Paludo C, Zhang L, Lincho CS, Lemos DV, Real GG, Bergamin JA.Chest physical therapy for children hospitalised with acute pneumo-nia: a randomised controlled trial. Thorax 2008;63(9):791-794.
21. Templeton M, Palazzo MG. Chest physiotherapy prolongs durationof ventilation in the critically ill ventilated for more than 48 hours.Intensive Care Med 2007;33(11):1938-1945.
22. Chen YC, Wu LF, Mu PF, Lin LH, Chou SS, Shie HG. Using chestvibration nursing intervention to improve expectoration of airwaysecretions and prevent lung collapse in ventilated ICU patients: arandomized controlled trial. J Chin Med Assoc 2009;72(6):316-322.
23. Ntoumenopoulos G, Presneill JJ, McElholum M, Cade JF. Chestphysiotherapy for the prevention of ventilator-associated pneumonia.Intensive Care Med 2002;28(7):850-856.
24. Asher MI, Douglas C, Airy M, Andrews D, Trenholme A. Effects ofchest physical therapy on lung function in children recovering fromacute severe asthma. Pediatr Pulmonol 1990;9(3):146-151.
25. Syed N, Maiya AG, Siva Kumar T. Active Cycles of BreathingTechnique (ACBT) versus conventional chest physical therapy onairway clearance in bronchiectasis: a crossover trial. Adv Physiother2009;11(4):193-198.
26. Paneroni M, Clini E, Simonelli C, Bianchi L, Degli Antoni F, Vi-tacca M. Safety and efficacy of short-term intrapulmonary percus-sive ventilation in patients with bronchiectasis. Respir Care 2011;56(7):984-988.
27. Antonaglia V, Lucangelo U, Zin WA, Peratoner A, De Simoni L,Capitanio G, et al. Intrapulmonary percussive ventilation improvesthe outcome of patients with acute exacerbation of chronic obstruc-tive pulmonary disease using a helmet. Crit Care Med 2006;34(12):2940-2945.
28. Chicayban LM, Zin WA, Guimaraes FS. Can the Flutter valve im-prove respiratory mechanics and sputum production in mechanicallyventilated patients? A randomized crossover trial. Heart Lung 2011;40(6):545-553.
29. Tsang SM, Jones AY. Postural drainage or Flutter device in con-junction with breathing and coughing compared to breathing andcoughing alone in improving secretion removal and lung function inpatients with acute exacerbation of bronchiectasis: a pilot study. H KPhysiother J 2003;21:29-36.
30. Samransamruajkit R, Chin TW, Yuengsrigul A, Newton T, Nuss-baum E. Possible beneficial effect of chest physical therapy in hos-pitalized asthmatic children. Pediatr Asthma Allergy Immunol 2003;16(4):295-303.
31. Bellone A, Spagnolatti L, Massobrio M, Bellei E, Vinciguerra R,Barbieri A, et al. Short-term effects of expiration under positivepressure in patients with acute exacerbation of chronic obstructivepulmonary disease and mild acidosis requiring non-invasive positivepressure ventilation. Intensive Care Med 2002;28(5):581-585.
32. Ambrosino N, Callegari G, Galloni C, Brega S, Pinna G. Clinicalevaluation of oscillating positive expiratory pressure for enhancingexpectoration in diseases other than cystic fibrosis. Monaldi ArchChest Dis 1995;50(4):269-275.
33. Unoki T, Kawasaki Y, Mizutani T, Fujino Y, Yanagisawa Y, Ishi-matsu S, et al. Effects of expiratory rib-cage compression on oxy-genation, ventilation, and airway-secretion removal in patients re-ceiving mechanical ventilation. Respir Care 2005;50(11):1430-1437.
34. Berney S, Denehy L. A comparison of the effects of manual andventilator hyperinflation on static lung compliance and sputum pro-duction in intubated and ventilated intensive care patients. Phys-iother Res Int 2002;7(2):100-108.
35. Ntoumenopoulos G, Gild A, Cooper DJ. The effect of manual lunghyperinflation and postural drainage on pulmonary complications inmechanically ventilated trauma patients. Anaesth Intensive Care 1998;26(5):492-496.
36. Krause MW, Van Aswegen H, De Wet EH, Joubert G. Posturaldrainage in intubated patients with acute lobar atelectasis: a pilotstudy. S African J Physiother 2000;56(3):29-32.
37. Barker M, Adams S. An evaluation of a single chest physiotherapytreatment on mechanically ventilated patients with acute lung injury.Physiother Res Int 2002;7(3):157-169.
38. Vargas F, Bui HN, Boyer A, Salmi LR, Gbikpi-Benissan G, GuenardH, et al. Intrapulmonary percussive ventilation in acute exacerba-tions of COPD patients with mild respiratory acidosis: a randomizedcontrolled trial. Crit Care 2005;9(4):R382-R389.
39. Mackay MR, Ellis E, Johnston C. Randomised clinical trial of phys-iotherapy after open abdominal surgery in high risk patients. Aust JPhysiother 2005;51(3):151-159.
40. Denehy L, Carroll S, Ntoumenopoulos G, Jenkins S. A randomizedcontrolled trial comparing periodic mask CPAP with physiotherapyafter abdominal surgery. Physiother Res Int 2001;6(4):236-250.
41. de Charmoy SB, Eales CJ. The role of prophylactic chest physio-therapy after cardiac valvular surgery: is there one? S African JPhysiother 2000;56(3):24-28.
42. Fagevik Olsen M, Hahn I, Nordgren S, Lonroth H, Lundholm K.Randomized controlled trial of prophylactic chest physiotherapy inmajor abdominal surgery. Br J Surg 1997;84(11):1535-1538.
43. Johnson D, Kelm C, Thomson D, Burbridge B, Mayers I. The effectof physical therapy on respiratory complications following cardiacvalve surgery. Chest 1996;109(3):638-644.
44. Johnson D, Kelm C, To T, Hurst T, Naik C, Gulka I, et al. Postop-erative physical therapy after coronary artery bypass surgery. Am JRespir Crit Care Med 1995;152(3):953-958.
45. Naraparaju S, Vaishali K, Venkatesan P, Acharya V. A comparisonof the Acapella and a threshold inspiratory muscle trainer for sputumclearance in bronchiectasis: a pilot study. Physiother Theory Pract2010;26(6):353-357.
46. Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, CasaburiR, et al. Interpretative strategies for lung function tests. Eur Respir J2005;26(5):948-968.
47. Marques A, Bruton A, Barney A. Clinically useful outcome mea-sures for physiotherapy airway clearance techniques: a review. PhysTher Rev 2006;11(4):299-307.
48. Hyatt RE, Scanlon PD, Nakamura M. Interpretation of pulmonaryfunction tests: a practical guide. Philadelphia: Lippincott Williams &Wilkins; 2009.
49. Yang M, Yan Y, Yin X, Wang BY, Wu T, Liu GJ, et al. Chestphysiotherapy for pneumonia in adults. Cochrane Database Syst Rev2010;(2):2.
50. Ides K, Vissers D, De Backer L, Leemans G, De Backer W. Airwayclearance in COPD: need for a breath of fresh air? A systematicreview. COPD 2011;8(3):196-205.
NONPHARMACOLOGIC AIRWAY CLEARANCE TECHNIQUES IN HOSPITALIZED PATIENTS
2186 RESPIRATORY CARE • DECEMBER 2013 VOL 58 NO 12