Noninvasive and Continuous Hemoglobin (SpHb). SpHb Overview Methods Accuracy Bleeding and...
49
Noninvasive and Continuous Hemoglobin (SpHb)
-
Upload
juliana-nicholson -
Category
Documents
-
view
224 -
download
2
Transcript of Noninvasive and Continuous Hemoglobin (SpHb). SpHb Overview Methods Accuracy Bleeding and...

Noninvasive and Continuous Hemoglobin (SpHb)

SpHb Overview
• Methods• Accuracy • Bleeding and Transfusion Challenges• Outcomes Study• Clinical Uses and Guidelines

Masimo SpHb:Continuous, Noninvasive, Immediate
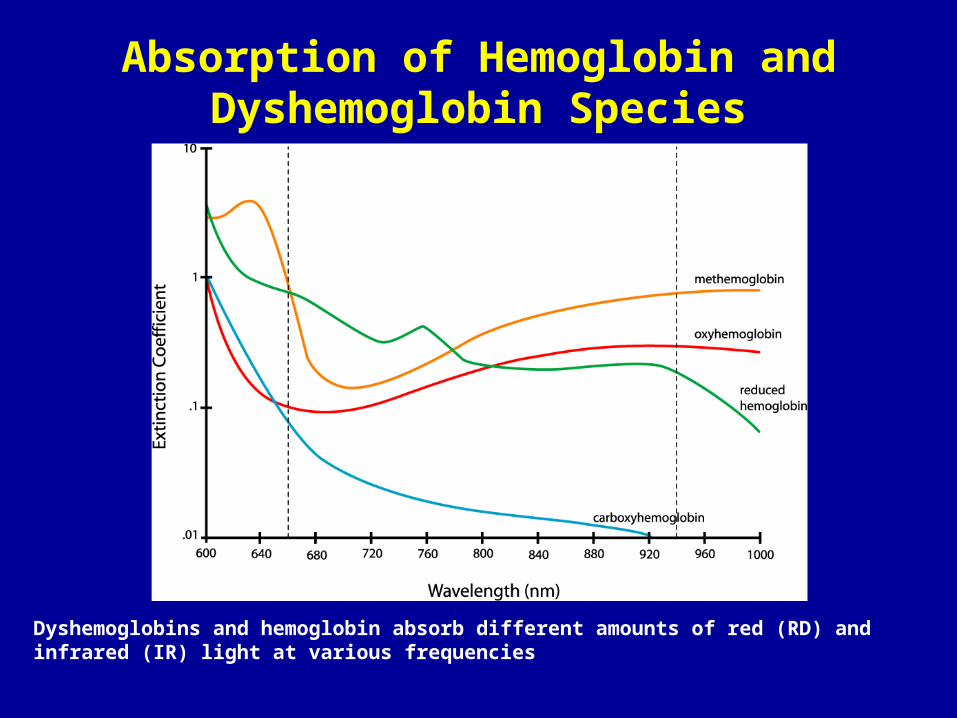
Absorption of Hemoglobin and Dyshemoglobin Species
Dyshemoglobins and hemoglobin absorb different amounts of red (RD) and infrared (IR) light at various frequencies

Digital Signal Processing Estimation
Detection, Signal Condition & Analog-to-Digital Conversion
Site
Noninvasive Pulse CO-Oximetry: Method
.
.
.Analog
Front End
ADConverter
Filtering,Decimation,Averaging
MultivariateEstimationAlgorithm
NoninvasiveHb
Emission
• Light is received by a photo detector• Generates electrical analog signals• Signals amplified, conditioned, and converted to digital signals
•Multiple visible and infrared lights applied to measurement site
• Advanced algorithms process digital signals• Analyzed by a multivariate estimation processor• Predicted hemoglobin density
Spectrophotometry-based

Hb Measurement Comparison
Device
Method
Characteristics
Substrate for Analysis
Sample Chamber
Needle Stick Hazard
Biohazard Waste Disposal
Special Training/Quality Control
Calibration
Patient Apprehension
CO-Oximeter, Hematology Analyzer, Point-of-Care Device
Pulse CO-OximetryTM
Spectrophotometry Multiple wavelengths of light
Invasive, Delayed, Intermittent Noninvasive, Immediate, Continuous
Blood Blood
Cuvette Finger
Yes No
Yes No
Yes No
Yes Internal
Moderate to High Low

Variability of Hb Measurement
• CO-Oximeter Devices• Comparison of 2 identical CO-Oximeters from each of 5 different
manufacturers• Average standard deviation of 0.5 g/dL1
• Point-of-Care Devices• Capillary blood sample comparison to reference lab
• Standard deviation ranged from 0.5 – 1.3 g/dL2,3,4,5
• Physiology • Standing vs. sitting position blood samples
• Standing measurements up to 1g/dL higher than sitting6
• Left hand vs. right hand blood samples• Up to 0.5 g/dL difference7
1 Gehring H et al. Anesthesia and Analgesia. 105(6);2007:524-530. 2 Gomez-Simon A et al. Transfusion and Apheresis Science. 2007;36:235-242; 3 Patel et al. JECT. 2007; 39:10-17. 4 van de Louw A et al. Intens Care Med. 2007; 33:355-358. 5 Argawal R et al. ASAIO J. 2001. 47(3):240-3. 6 Gore et al. Eur Jour Ap Phys and Occup Phys. 1992;65:302-310. 7 Morris SS, et al.. Am J Clin Nutr 1999 ;69 :1243-8

Variation in Hemoglobin Measurement by Lab Devices:CO-Oximeter vs. Coulter
• N=471 samples from 33 patients undergoing liver transplantation
• After 10 ml waste, 10 ml sample analyzed for tHb by the COULTER® Ac·T diff2™ analyzer (Beckman Coulter, Miami, FL, USA)
• Immediately after, 2 ml sample for tHb by the pHOx CO-Oximeter (Nova Biomedical, Waltham, MA, USA)
Torp KD et al. Anesthesiology 2009 (ASA abstract): A937. In press.

Accuracy of Point of Care Hemoglobin Devices Using Capillary Blood
Gomez-Simon et al. Transfusion & Apheresis Science 2007. Rippman et al. J Clin Monit 1997.
N=195 blood donors
Hemocue POC device
N=140 surgical samples
Hemocue POC device

Variation in Hb:Arterial vs. Venous
•N=107 healthy volunteers aged 18-30 years
•Four time-matched venous and arterial hemoglobin samples
•By 2 peripheral intravenous and 1 radial artery line
•Hemodilution with Isolyte® (40cc/kg) following phlebotomy of 1 unit whole blood
Rook JL et al. Anesthesiology 2009 (ASA abstract): A1294. In press.

2011 Radical 7

Noninvasive Hemoglobin:Study Methods for FDA Submission
• Data collected at three sites• Loma Linda Medical Center (Loma Linda, CA)• Mayo Clinic (Jacksonville, FL)• Masimo Corporation (Irvine, CA)
• Hb measurement• Noninvasive: Masimo Rainbow SET platform (SpHb)• Invasive: Radiometer ABL-820 CO-Oximeter (tHb)
• 492 data pairs collected from 59 total subjects• 35 (59%) healthy adults• 16 (27%) hemodilution subjects• 8 (14%) from surgical subjects
• Collected tHb values had a range of 6 to 18 g/dL• 220 (45%) <12 g/dL• 145 (29%) <11 g/dL• 74 (15%) <10 g/dL

Continuous & Noninvasive Hemoglobin (SpHb):Accuracy Study Results for FDA Submission
0
2
4
6
8
10
12
14
16
18
20
22
24
0 2 4 6 8 10 12 14 16 18 20 22 24
Reference tHb (g/dL) from Laboratory CO-Oximeter
Sp
Hb
(g
/dL
) fr
om
Pu
lse
CO
-Oxi
met
ry
S
Precision improves at lower Hb levels – when it matters most
Precision improves at lower Hb levels – when it matters most
> N=492 > 59% healthy subjects> 27% hemodilution subjects> 14% from surgical subjects
> N=492 > 59% healthy subjects> 27% hemodilution subjects> 14% from surgical subjects

Noninvasive Hemoglobin:Study Results for FDA Submission
tHb Range
Difference Between SpHb and tHbN (%)
<1.0 g/dL <1.5 g/dL <2.0 g/dL
<10 g/dL 80% 97% 100%
10 - 11.9 g/dL 68% 96% 99%
12 - 18 g/dL 67% 87% 94%
6 – 18 g/dL 69% 91% 97%
N=492

Accuracy of SpHb from Rainbow vs. tHb from CO-Oximeter
• N=20 healthy volunteers aged 18-30 years, 335 paired measurements
• Hemodilution with Isolyte® (40cc/kg) following phlebotomy of 1 unit whole blood
• Invasive tHb measurement by CO-oximeter (ABL-820)
• Noninvasive Hb measurement by Pulse CO-Oximetry (Masimo SpHb from Radical-7)
Macknet MR et al. Anesth Analg 2010;111:1424–6.

Accuracy of SpHb from Rainbow vs. tHb from CO-Oximeter
Macknet MR et al. Anesth Analg 2010;111:1424–6.

Validation of a New Non-Invasive Hemoglobin Algorithm in Patients Undergoing Liver Transplantation
Torp et al. Anesthesiology 2009 (ASA abstract): A184.

Comparison of New Non-Invasive Continuous Spectrophotometry vs. RBC Count for Hemoglobin During Surgery
• N=20 patients subjected to an urologic surgery with hemorrhagic risk
• Spectrophotometric hemoglobin measurement (Radical-7 Rainbow) and RBC count (laboratory)
• Measurements performed at beginning and end of each intervention and before and after each transfusion (54)
• Correlation between laboratory and noninvasive values of 0.88, bias of 0.26 g/dL with a standard deviation of 1.11 g/dL
Lamhaut L, et al. European Journal of Anesthesiology. 2010; 27(suppl 47):3AP7-1.

SpHb Compared to tHb in Pediatric Patients
• Method• 15 patients from a variety of surgery cases enrolled; mean age 9.3 +/- 5.9 years• Average of 2.7 arterial blood samples per patient taken during surgery• 49 CO-Oximeter tHb measurements, 46 POC tHb and 92 SpHb measurements compared
• Results
• Conclusion• All significant directional changes in tHb form the CO-Oximeter were indicated by changes in
SpHb.
Jou C, et al. Anesthesia and Analgesia. 2010; S401.
SpHb – Lab Hb
N = 92
POC –Lab Hb
N = 45
Bias (g/dL) 0.18 -0.26
Standard Deviation (g/dL) 1.10 0.46
ARMS (g/dL) 1.12 0.53

Continuous Hemoglobin Monitoring
• Real time view of changes in total hemoglobin• Rising • Falling • Stable →
SpH
b
Time
SpH
bSp
Hb
SpH
b

Noninvasive Hemoglobin:Accuracy Trend
MackNet MR et al. Anesthesia and Analgesia. 2007;104;S-31 (abstract).
0
2
4
6
8
10
12
0 10000 20000 30000 40000 50000 60000
Time (secs)
Hem
oglo
bin
(g/d
L)
SpHb
Invasive Hb
Co-Oximeter

Target hemoglobin
range
tHb outside target range
SpHbContinuousHemoglobin
Trend
Continuous and Noninvasive Hemoglobin Monitoring:Potential for Earlier and Better Clinical Decision-Making
SpHb data blinded during caseSpHb data blinded during case

Undetected Bleeding Challenges
• Significant bleeding is common in surgical and critical care patients• Up to 35% of patients1
• Bleeding is a significant risk factor for surgical, critical care, and OB patients• Late detection further increases the risk2
• Bleeding significantly increases the cost of treatment2
• Low hemoglobin identifies almost 90% of patients with bleeding• However, traditional laboratory measurements are infrequent and
delayed3
1 Hebert PC. Crit Care. 1999: 3(2):57-63. 2 Herwaldt LA. Infect Control Hosp Epidemiol. 2003; 24(1):44-50.3 Bruns B et al. J Trauma. 2007; 63(2):312-5.1 Hebert PC. Crit Care. 1999: 3(2):57-63. 2 Herwaldt LA. Infect Control Hosp Epidemiol. 2003; 24(1):44-50.3 Bruns B et al. J Trauma. 2007; 63(2):312-5.

Impact of Continuous and Noninvasive Hemoglobin Monitoring on
Intraoperative Blood Transfusions
Jesse M. Ehrenfeld MD, MPHJustin P. Henneman MS
Warren S. Sandberg, MD, PhD
Department of Anesthesia, Critical Care and Pain Medicine
Massachusetts General HospitalHarvard Medical School
Ehrenfeld JM et al. ASA. 2010. LB05.

Background• Blood transfusions increase patient risk for adverse outcomes1-3
• Up to 40% increase in 30-day morbidity• Up to 38% increase in 30-day mortality & 67% increase in 6-month mortality
• Blood transfusions are costly4
• $522 to $1,183 per unit, without short- or long-term morbidity included• Annual estimates for surgical blood costs at $1.6 to $6.0 million per hospital
• Laboratory hemoglobin (Hb) values used to determine need for blood transfusion,5 but testing is intermittent and delayed
• Lack of Hb values is associated with inappropriate transfusions6
• Noninvasive and continuous (SpHb) monitoring is now possible• Pulse CO-Oximetry and a multi-wavelength adhesive sensor
• Hypothesis• SpHb monitoring could reduce intraoperative blood transfusions
Ehrenfeld JM et al. ASA. 2010. LB05. 1 Taylor RW et al. Crit Care Med. 2006; 34(9):2302-8. 2 Bernard AC et al. Journal of the American College of Surgeons. 2009;208:931-937. 3 Surgenor SD et al, for the Northern New England Cardiovascular Disease Study Group. Anesthesia & Analgesia 2009;108:1741-1746. 4 Shander A et al. Transfusion. 2010;50(4):753-65 5 ASA Task Force on Perioperative Blood Transfusion. Anesthesiology. 2006 Jul;105(1):198-208. 6 Tartter PI et al. Transfusion. 1985;25:113-115.
Ehrenfeld JM et al. ASA. 2010. LB05. 1 Taylor RW et al. Crit Care Med. 2006; 34(9):2302-8. 2 Bernard AC et al. Journal of the American College of Surgeons. 2009;208:931-937. 3 Surgenor SD et al, for the Northern New England Cardiovascular Disease Study Group. Anesthesia & Analgesia 2009;108:1741-1746. 4 Shander A et al. Transfusion. 2010;50(4):753-65 5 ASA Task Force on Perioperative Blood Transfusion. Anesthesiology. 2006 Jul;105(1):198-208. 6 Tartter PI et al. Transfusion. 1985;25:113-115.
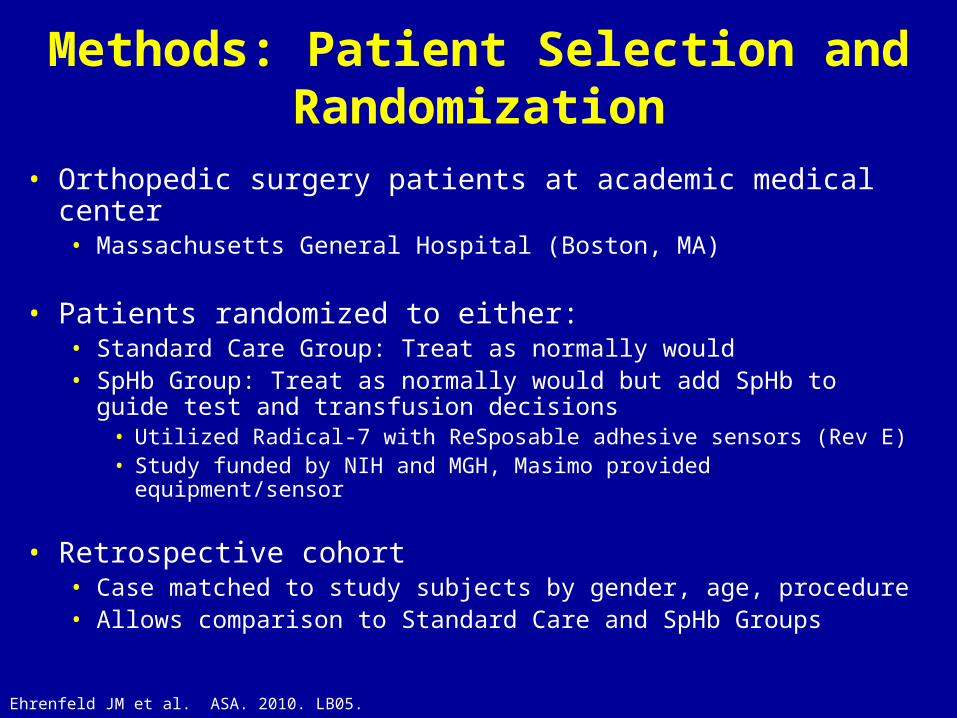
Methods: Patient Selection and Randomization
• Orthopedic surgery patients at academic medical center• Massachusetts General Hospital (Boston, MA)
• Patients randomized to either:• Standard Care Group: Treat as normally would• SpHb Group: Treat as normally would but add SpHb to guide test and
transfusion decisions• Utilized Radical-7 with ReSposable adhesive sensors (Rev E)• Study funded by NIH and MGH, Masimo provided equipment/sensor
• Retrospective cohort • Case matched to study subjects by gender, age, procedure• Allows comparison to Standard Care and SpHb Groups
Ehrenfeld JM et al. ASA. 2010. LB05.

Methods: Outcome Variables
• Primary outcome variables• Frequency of intraoperative blood transfusions• Mean number of blood transfusions per patient
• Secondary outcome variables• Frequency of laboratory Hb testing
• Safety Variables• Post-operative transfusion frequency• 28 day complication rates
Ehrenfeld JM et al. ASA. 2010. LB05.

Results: Patients• Patient recruitment occurred over a six-month period
• February 2010 through July 2010
• 350 patients screened, 327 patients enrolled• 157 Standard Care, 170 SpHb
• Procedures included:• Hip replacement 31%
• Knee replacement 29%
• Spinal surgery 14%
• 327 subjects in matched retrospective cohort• From six-month period prior to study commencement
• Received no intervention
Ehrenfeld JM et al. ASA. 2010. LB05.
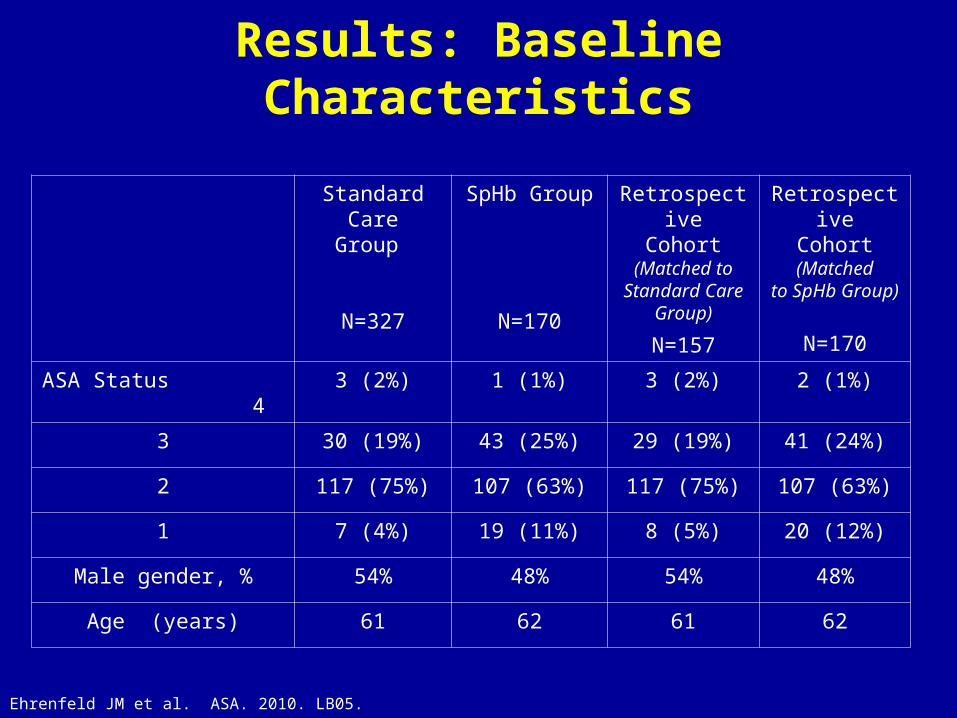
Results: Baseline Characteristics
Standard CareGroup
N=327
SpHb Group
N=170
RetrospectiveCohort
(Matched to Standard Care
Group)
N=157
RetrospectiveCohort
(Matchedto SpHb Group)
N=170
ASA Status 4
3 (2%) 1 (1%) 3 (2%) 2 (1%)
3 30 (19%) 43 (25%) 29 (19%) 41 (24%)
2 117 (75%) 107 (63%) 117 (75%) 107 (63%)
1 7 (4%) 19 (11%) 8 (5%) 20 (12%)
Male gender, % 54% 48% 54% 48%
Age (years) 61 62 61 62
Ehrenfeld JM et al. ASA. 2010. LB05.

Results: Patient Characteristics
• No differences in pre-operative laboratory Hb value• 13.5 +/- 1.6 vs. 13.6 +/- 1.5, p=ns
• No differences in intraoperative estimated blood loss• 157 +/- 212 vs. 210 +/- 280 mL, p=ns
• No differences in procedure type
Ehrenfeld JM et al. ASA. 2010. LB05.
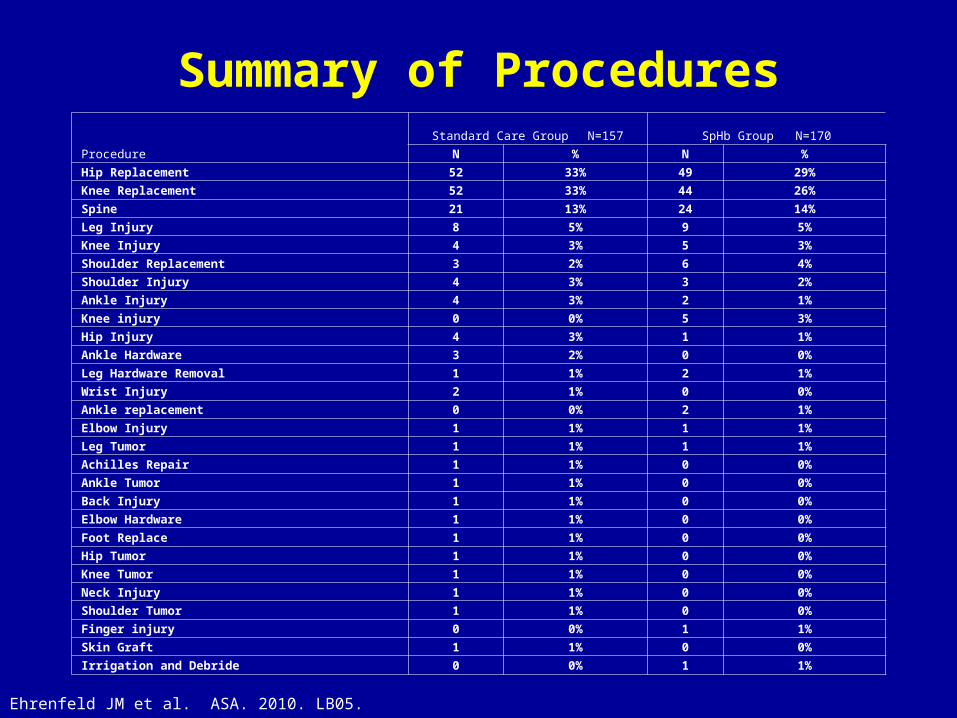
Summary of Procedures
Procedure
Standard Care Group N=157 SpHb Group N=170
N % N %
Hip Replacement 52 33% 49 29%
Knee Replacement 52 33% 44 26%
Spine 21 13% 24 14%
Leg Injury 8 5% 9 5%
Knee Injury 4 3% 5 3%
Shoulder Replacement 3 2% 6 4%
Shoulder Injury 4 3% 3 2%
Ankle Injury 4 3% 2 1%
Knee injury 0 0% 5 3%
Hip Injury 4 3% 1 1%
Ankle Hardware 3 2% 0 0%
Leg Hardware Removal 1 1% 2 1%
Wrist Injury 2 1% 0 0%
Ankle replacement 0 0% 2 1%
Elbow Injury 1 1% 1 1%
Leg Tumor 1 1% 1 1%
Achilles Repair 1 1% 0 0%
Ankle Tumor 1 1% 0 0%
Back Injury 1 1% 0 0%
Elbow Hardware 1 1% 0 0%
Foot Replace 1 1% 0 0%
Hip Tumor 1 1% 0 0%
Knee Tumor 1 1% 0 0%
Neck Injury 1 1% 0 0%
Shoulder Tumor 1 1% 0 0%
Finger injury 0 0% 1 1%
Skin Graft 1 1% 0 0%
Irrigation and Debride 0 0% 1 1%
Ehrenfeld JM et al. ASA. 2010. LB05.

Results: Primary Outcome Variables
* p=0.03 vs. Standard Care Group; † p=0.02 vs. Matched Retrospective Cohort; **p<0.0001 vs. Standard Care Group; †† p<0.0001 vs. Matched Retrospective Cohort
Matched Retrospective
Cohort N=327
Standard Care Group N=157
SpHb GroupN=170
Patients receiving RBC transfusion, N (%)
15 (4.6%) 7 (4.5%) 1 (0.6%)* †
Total RBC units transfused, N (mean) 26 (0.08) 15 (0.10) 2 (0.01)** ††
Ehrenfeld JM et al. ASA. 2010. LB05.

Frequency of Patients Receiving RBC Transfusion (%)
* p=0.03 vs. Standard Care Group; † p=0.02 vs. Matched Retrospective Cohort
Ehrenfeld JM et al. ASA. 2010. LB05.
4.6% 4.5%
0.6%
0%
1%
2%
3%
4%
5%
Retrospective Cohort Standard Care Group SpHb Group
Fre
qu
ency
of
In
tro
op
erat
ive
Blo
od
Tra
nsf
usi
on
s
* †

Results: Other Outcome Variables• Secondary Variables
• Frequency of patients receiving intraoperative Hb testing similar in the SpHb and Standard Care Groups
• 11.8% vs. 16.3%, p=ns
• Mean number of Hb tests performed were similar in the SpHb and Standard Care Groups
• 0.24 vs. 0.21 tests per case, p=ns
• Safety Variables• No patient from either group received a transfusion during the
immediate twelve-hour postoperative period• No differences at 28 days in the rate of post-operative complications
between the SpHb and Standard Care Groups• 1.9% vs. 3.0%, p=ns
Ehrenfeld JM et al. ASA. 2010. LB05.

Post-hoc Analysis: Potential Cost Savings• RBC transfusion reduction per patient with SpHb (0.09 units per case)• Applied over range of RBC cost estimates
Range of Total Cost Estimates per RBC Unit Transfused
Potential Cost Savings per Patient with SpHb Monitoring
$ 250 $ 23
$ 500 $ 45
$ 750 $ 68
$ 1,000 $ 90
$ 1,250 $ 113
$ 1,500 $ 135
Note: Estimates of RBC cost vary due to consideration of direct, indirect, and RBC-related complications.
Ehrenfeld JM et al. ASA. 2010. LB05.

Study Conclusions
• The use of SpHb monitoring resulted in a lower frequency of intraoperative RBC transfusions and a lower number of RBC units transfused during elective orthopedic surgery
• SpHb monitoring may reduce unnecessary transfusions, reduce patient risk, and reduce costs
• Future studies will help determine the role of SpHb monitoring in other settings and populations
Ehrenfeld JM et al. ASA. 2010. LB05.

Blood Transfusions and Nosocomial Infections
• Post-transfusion nosocomial infection rate
• Number of red blood cell transfusions• Independently associated with nosocomial infection rates
• Mortality, LOS in both the ICU and hospital• Significantly higher in transfused patients, even when corrected for illness severity
Taylor RW, et.al. Crit Care Med. 2006; 34(9): 2302-2308.

Effect of Blood Transfusion on 30 Day Outcomes
• 125,177 general surgery patients from 121 hospitals • 4,788 received RBC transfusion
• 30 day risk-adjusted odds ratio for receiving 1U and 2U of blood
Bernard AC et al. Journal of the American College of Surgeons. 2009; 208:931-937.
• = Mortality ■ = Morbidity
1 Unit 2 Units
Mortality 1.32 1.38
All-cause Morbidity 1.23 1.40
Pneumonia 1.24 1.25
Sepsis 1.29 1.53

Effect of Blood Transfusion on 6-Month Outcomes
• N= 9,079 cardiac surgery patients at eight hospitals• 3,254 (36%) pts received transfusion of one or two units of blood• Risk-adjusted 67% increase in 6-month mortality for transfused patients
Surgenor SD et al. Anesthesia & Analgesia 2009; 108:1741-1746.

TRICC RCT in Adult Critical Care:Liberal vs. restrictive transfusion strategy
Hebert, et al. N Engl J Med 1999;340:409-17.
• N=838 total• N=418 to Restrictive group
• Received 54% fewer red cell units
• Overall - at least as effective as the liberal strategy
Pilot Blood Measures
• New pilot blood measures• Patients with pre-transfusion hemoglobin or hematocrit
completed AND documentation of clinical indication for each RBC unit administered
• Documentation that the patient was screened for anemia 14 - 30 days prior to surgery
• Blood measures are being finalized by end of 2010• Will be optional for hospitals to report • Pilot measures often become core measures
http://www.jointcommission.org/PerformanceMeasurement/PerformanceMeasurement/Blood+Management.htm

Clinical Practice Guidelines: ASA Guidelines for Perioperative Blood
Transfusion
1. Monitoring for blood loss. Visual assessment of the surgical field should be periodically conducted to assess the presence of bleeding
2. Monitoring for inadequate perfusion and oxygenation of vital organs. Conventional monitoring systems (e.g., blood pressure, heart rate, oxygen saturation, urine output, electrocardiography) should be used to assess the adequacy of perfusion and oxygenation of vital organs. Special monitoring systems should be used when appropriate (e.g., echocardiography, mixed venous oxygen saturation, blood gasses).
3. Monitoring for transfusion indications. Measure hemoglobin or hematocrit when substantial blood loss or any indication of organ ischemia occurs. Red blood cells should usually be administered when the hemoglobin concentration is low (e.g., less than 6 g/dl in a young, healthy patient), especially when the anemia is acute. Red blood cells are usually unnecessary when the hemoglobin concentration is more than 10 g/dl. These conclusions may be altered in the presence of anticipated blood loss. The determination of whether intermediate hemoglobin concentrations (i.e., 6–10 g/dl) justify or require red blood cell transfusion should be based on any ongoing indication of organ ischemia, potential or actual ongoing bleeding (rate and magnitude), the patient’s intravascular volume status, and the patient’s risk factors for complications of inadequate oxygenation.These risk factors include a low cardiopulmonary reserve and high oxygen consumption.
4. Transfusion of allogeneic red blood cells or autologous blood. Maintain adequate intravascular volume and blood pressure with crystalloids or colloids until the criteria for red blood cell transfusion listed above are met. Adequate quantities of red blood cells should be transfused to maintain organ perfusion. When appropriate, intraoperative or postoperative blood recovery and other means to decrease blood loss (e.g., deliberate hypotension) may be beneficial. Acute normovolemic hemodilution, although rarely used, may also be considered.
ASA Practice Guidelines: 2006ASA Practice Guidelines: 2006

Anemia Challenges in Critical Care• Anemia has high prevalence in the ICU
• 95% of ICU patients have a below-normal Hb level by ICU day 3• 35% experience acute bleeding
• Repeated blood draws induce anemia• Ranges from 40 to 70 mL/day• 601 to 2,156 mL over entire hospital stay
• Blood transfusion prevalence• Undetected bleeding a major cause of blood transfusions • 75% of ICU patients with >1 week LOS receive a transfusion• 29% have no indication for blood transfusion
• Morbidity and mortality rate lower for restrictive vs. liberal transfusion strategy
Gould S et al. AJCC. 2007;16:39-47. Corwin HL et al. Chest. 1995. 108;767-771. Von Ahsehn N et al. Crit Care Med. 99;12;2630-2639. Hebert, et al. N Engl J Med 1999;340:409-17. Zimmerman JE et al, Crit Care Med 1997;25:737-48. Smoller BR et al, NEIM 1986;314:1233-35

Clinical Practice Guidelines: RBC Transfusion in Adult Trauma and Critical Care
Napolitano et al. Critical Care Medicine 2009Napolitano et al. Critical Care Medicine 2009
• Strategies to reduce RBC transfusion• Intraoperative/postoperative blood salvage, reduction in diagnostic laboratory testing is associated
with a reduction in phlebotomy volumes and a reduction in blood transfusion• A “restrictive” strategy of RBC transfusion (Hb transfusion trigger @ 7 g/dL) is as effective as a
“liberal” transfusion strategy (Hb transfusion trigger @ 10 g/dL) • Use of Hb level only as “trigger” for transfusion should be avoided
• Decision for RBC transfusion should be based on an individual patient’s:• Intravascular volume status, evidence of shock, duration and extent of anemia, cardiopulmonary
physiologic parameters
• All efforts should be initiated to avoid RBC transfusion in patients at risk for acute
lung injury and acute respiratory distress syndrome

Anemia Challenges in the ED
• Challenges in anemia diagnosis• May be masked by other conditions• Common during occult bleeding and hemorrhage during trauma• Associated with higher in-hospital morbidity and mortality
• Laboratory tests delay treatment and disposition• 34% of all ED visits result in a Complete Blood Count (CBC)• Long waits fuel ED overcrowding problem
• Increase number patients who leave without being seen
• Decreasing turnaround time for diagnostic tests• Identified as major solution to increasing ED efficiency
Weiss SJ et al. Am J Emerg Med. 2005; 23:288-294. ACEP Task Force on Boarding, 2008.

Postpartum Hemorrhage
• 2.9% of deliveries had PPH• Accounting for 19.1% of postpartum hospital deaths
Bateman BT et al. A&A 2010

2010 Sentinel Event Alert: Preventing Maternal Death
#2 Recommendation Action:
Identify specific triggers for responding to changes in the mother’s vital signs and clinical condition and develop and use protocols and drills for responding to changes, such as hemorrhage and pre-eclampsia.
http://www.jointcommission.org/sentinelevents/sentineleventalert/sea_44.htm
The Problem: PPH is a Leading Cause of Pregnancy-Related Mortality
• No single definition exists, various definitions include:• > 500 mL EBL after completion of the third stage• 900 mL EBL, which typically corresponds to 15%
volume deficit• Any blood loss from the genital tract > 500 mL• 10% change in hematocrit or need for blood
transfusion
• Accurate measurement of blood loss can be difficult
Gregory, K, et al. OB Hemorrhage Definitions and Triggers. CMQCC Hemorrhage Task Force. 03/06/2009

CMQCC Recommendations
• Management of all women with cumulative blood loss
• > 500 ml• At > 500 ml blood loss: notify MD and proceed
with administration of Methergine 0.2 mg IM, Fundal Massage
• Clinical Triggers: surveillance and intervention:• 1. HR > 110• 2. BP < 85/45• 3. SpO2 <95%
Gregory, K, et al. OB Hemorrhage Definitions and Triggers. CMQCC Hemorrhage Task Force. 03/06/2009