Noncommunicable Disease and Poverty - WPRO · Noncommunicable Disease and Poverty The Need for...
100
Noncommunicable Disease and Poverty The Need for Pro-poor Strategies in the Western Pacific Region World Health Organization Western Pacific Region A REVIEW
Transcript of Noncommunicable Disease and Poverty - WPRO · Noncommunicable Disease and Poverty The Need for...
Noncommunicable Disease and PovertyThe Need for Pro-poor Strategies in the Western Pacific Region
World HealthOrganization
Western Pacific Region
A REVIEW

Noncommunicable Disease and PovertyThe Need for Pro-poor Strategies in the Western Pacific Region
A REVIEW

Noncommunicable disease and poverty: the need for pro-poor strategies in the Western Pacific Region: a review.
1. Non-communicable diseases. 2. Poverty. 3. Developing countries.
ISBN 92 9061 234 7 (NLM Classification: WA 500)
© World Health Organization 2006All rights reserved.
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature
that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
The World Health Organization does not warrant that the information contained in this publication is complete and correct and shall not be liable for any damages incurred as a result of its use.
Publications of the World Health Organization can be obtained from Marketing and Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce WHO publications, in part or in whole, or to translate them whether for sale or for noncommercial distribution should be addressed to Publications, at the above address (fax: +41 22 791 4806; email: [email protected]). For WHO Western Pacific Regional Publications, request for permission to reproduce should be addressed to Publications Office, World Health Organization, Regional Office for the Western Pacific, P.O. Box 2932, 1000, Manila, Philippines, Fax. No. (632) 521-1036, email: [email protected].
WHO Library Cataloguing in Publication Data

Table of ContentsAcknowledgements .............................................................................................. ivAbbreviations ......................................................................................................... ivPreface ..................................................................................................................... vExecutive Summary .............................................................................................. viiIntroduction ............................................................................................................ 1 Methodology ................................................................................................... 2 Poverty ............................................................................................................ 3 NCD ............................................................................................................... 4 Comment on Poverty and NCD Literature ....................................................... 4Noncommunicable Disease in the Western Pacific ........................................ 7 The NCD Burden: is it a global or regional priority? ........................................ 10Prevention Programmes ..................................................................................... 17 Education and NCDs ..................................................................................... 20 Tobacco Controls .......................................................................................... 22Poverty and NCD Risk Factors ........................................................................ 25 Smoking and Polluted Air ................................................................................ 27 High Alcohol Consumption ............................................................................. 28 Weight and Diet ............................................................................................. 29 Physical Activity .............................................................................................. 32Selected NCDs in Poor Populations ............................................................... 35 Cardiovascular Disease and Hypertension ...................................................... 36 Diabetes ........................................................................................................ 37 Cancers ......................................................................................................... 38 Respiratory Diseases and COPD .................................................................... 39Seeking Treatment and Treatment Programmes ........................................... 41 The Emphasis on Personal Responsibility for Health ........................................ 43 The Cost of Care ........................................................................................... 44 Poverty and Inferior Treatment Services .......................................................... 46The Cycle of Poverty and Ill-health ................................................................. 49NCD outcomes for the poor ........................................................................... 53Justifying a Focus on the Poor .......................................................................... 57 Efficiency ....................................................................................................... 58 Equity ............................................................................................................ 59 Human Rights ................................................................................................ 60Conclusions .......................................................................................................... 61Bibliography .......................................................................................................... 66Endnotes ................................................................................................................ 77
FiguresFigure 1: Percentage of population in poverty in selected Western Pacific Region countries ........................................................................... 3
Tabl
e of
Con
tent
si
The Need for Pro-poor Strategies in the Western Pacific Region: A Review

Figure 2: Projected trends in causes of death in developing regions ........ 8Figure 3: Projected increase in NCDs in the Western Pacific Region 1975-2020 .................................................................................................... 9Figure 4: Disease impact projections in the Western Pacific Region ........ 9Figure 5: Disease profile in the Western Pacific Region 1995 ................... 10Figure 6: Disease profile projected to 2020 .................................................. 11Figure 7: Female adult mortality rates by cause of death and average community income, China 1987-1988 ................................................. 14Figure 8: Disease profile by country grouping in the Western Pacific 1995 ............................................................................................................ 15Figure 9: The pathway from exposure to disease outcome, the case of diabetes, using health benefit groups and health resource groups ......................................................................................................... 18Figure 10: Deaths in the United States of America (1995) by broad disease type and education .................................................................... 21Figure 11: Knowledge of smoking related diseases by education level in China, 1996 ................................................................................................ 22Figure 12: Prevalence of Obesity (BMI greater than 30) according to gender and socio-economic status, Valparaiso, Chile 1997 ............ 30Figure 13: Physical Activity by Level of Education (USA 2001) ................. 32Figure 14: Cancer as a % of causes of death 1960s to 1990s ................... 38Figure 15: No physician contact in the year 1994-1995 by adults age 25-64 with a health problem in the United States of America ...... 42Figure 16: Unmet need for health care by income, United States of America 1994-1995 ................................................................................. 44Figure 17: No health insurance coverage among persons age 25-64 in the United States of America 1994-1995 ........................................... 45Figure 18: Service utilization by income quintile in Viet Nam 1993 ........ 46Figure 19: The Cycle of Poverty and NCDs ................................................. 50
TablesTable 1: Key-words used in literature search ................................................ 2Table 2: Burden of disease in DALYs by cause and Regional mortality strata, estimates for 2001 ....................................................................... 12Table 3: Burden of disease in DALYs: Western Pacific Regional Office-B Nations as a % of global total for each broad cause group ........................................................................................................... 13Table 4: Attributable mortality by risk factor, sex and Regional mortality stratum (2000) ....................................................................... 26Table 5: Mortality from communicable diseases, NCDs and key NCD groups in the Western Pacific Region in 2002, comparisons between Western Pacific Regional Office-A and Western Pacific Regional Office-B nations ...................................................................... 54
Tabl
e of
Con
tent
sii
Noncommunicable Disease and Poverty

iii
Table 6: Causes of Death in Low and Middle Income Countries, 1998 ............................................................................................................ 54Table 7: Progression of NCDs: stages, barriers and outcomes for poor people .............................................................................................. 56Table 8: Evidence on relationships between poverty and NCDs .......... 64
BoxesBox 1: Modifying Diets in Chile ................................................................... 22Box 2: The North Karelia Project .............................................................. 23Box 3: NCD Management in Resource Poor Areas of South Africa ... 47
Tabl
e of
Con
tent
s
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
Ack
now
ledg
emen
tsiv
AbbreviationsAIDS Acquired immunodeficiency syndromeBMI Body-mass indexCINDI Countrywide Integrated Noncommunicable Disease InterventionCNPM Communicable diseases, nutrition, perinatal and maternal conditionsCOPD Chronic obstructive pulmonary diseaseCVD Cardiovascular diseaseDALY Disability-adjusted life yearGCSE General Certificate of Secondary EducationGNP Gross national productICCC Innovative Care for Chronic ConditionsNCD Noncommunicable diseaseNCI National Cancer InstituteNGO Non-governmental organizationOECD Organization for Economic Cooperation and DevelopmentSES Socioeconomic statusSTEPS STEPwise approach to surveillanceWHO World Health OrganizationWPRO Western Pacific Regional Office
AcknowledgementsThis review was prepared by Jude van Konkelenberg under the guidance of Gauden Galea, Regional Adviser, Noncommunicable Diseases, and Anjana Bhushan, Technical Officer, Poverty, Gender and Human Rights, at the World Health Organization Regional Office for the Western Pacific. The team gratefully acknowledges the thoughtful comments and input received from Carol Beaver, Robert Beaglehole, Amin Kebe, Bakuti Shengelia, Terrence Thompson, Ron van Konkelenberg and Nigel Unwin. James Hutchison edited the publication. Design and layout were handled by Zando Escultura.
Noncommunicable Disease and Poverty
Pref
ace
v
Preface
In October 2005, WHO proposed a global goal for noncommunicable disease (NCD) prevention and control of an additional 2% reduction in chronic disease death rates worldwide, per year, over the next 10 years. Work towards attaining this goal is essential,
especially in the Western Pacific Region, where around 25 000 people die every day from NCDs. Most of these NCD deaths occur in developing countries of the Region and at younger ages than in developed countries. The impact of early death and disability on the economies of the Region is immense. Between 2005 and 2015 China alone will lose an estimated US$ 550 billion from lost productivity due to death and disability associated with noncommunicable diseases.
Noncommunicable diseases are not, however, among the Millennium Development Goals (MDGs) because they tend to be erroneously characterized as diseases of affluence. Such beliefs obscure the need for urgent action to stem the growing tide of NCDs in low-income settings. Poor individuals who lack the resources to pursue healthy choices or access effective health care diagnosis and treatment for NCDs are particularly vulnerable. The knowledge and tools to reduce the burden of NCDs already exist and mobilizing support for prevention and control in developing countries will improve the health of millions, thereby contributing to poverty reduction.
This publication is an initial contribution towards a better understanding of the links between poverty and NCDs in the Western Pacific Region. It forms part of a family of resources being developed in this Region on the theme of poverty and NCD. This monograph is a review of available literature on this subject from within and outside the Region. Other initiatives include a forthcoming module on NCD under the series Integrating Poverty and Gender into Health Programmes: A Sourcebook for Health Professionals and a multi-country study on the associations between NCD risk factors and socioeconomic indicators.
Health and economic development are interlinked and must be simultaneously addressed. It is hoped that policy-makers in the Region
The Need for Pro-poor Strategies in the Western Pacific Region: A Review

Pref
ace
viNoncommunicable Disease and Poverty
recognise that any effective pro-poor policy must take into account the risk of NCD and that health promotion and NCD programmes should be designed and implemented to meet the needs of the poor.
Dr Shigeru Omi Regional Director
Exec
utiv
e Su
mm
ary
vii
Executive SummaryBased on a review of the available literature, this monograph explores the links between poverty and noncommunicable diseases (NCDs) with particular reference to the Western Pacific Region. The project was specifically designed to stimulate discussion on the relationship between poverty and NCDs, to contribute to the reduction of the impact of NCDs in developing countries, and to foster an understanding of how to improve health outcomes for the poor or socially marginalized groups with NCDs.
NCDs are not “diseases of affluence.” In wealthy nations, they have a disproportionate impact on the poor. Globally, the burden of NCDs is rising in developing countries, which also bear the greatest morbidity and mortality. NCDs, particularly cancer, cardiovascular disease (CVD) and diabetes are major public health issues in almost all countries and areas in the Western Pacific Region. Even in the Region’s developing nations, the NCD burden is greater than that of communicable disease and now causes the majority of deaths. Demographic and epidemiological transitions taking place in the developing countries of Asia and the Pacific are shifting the disease burden from communicable towards noncommunicable disease. As the burden of communicable diseases declined in developed countries it was replaced by a rising burden of noncommunicable disease. Developing nations, however, are experiencing a double burden, with communicable and noncommunicable diseases existing simultaneously.
The major NCDs, diabetes, cardiovascular diseases, cancers and chronic obstructive pulmonary disease (COPD), have common risk factors such as smoking, unhealthy diet, alcohol consumption and low levels of physical activity. These risk factors are high among poor people and poor nations. In the Western Pacific Region, all major risk factors for NCDs are increasing. Smoking is widespread in the Western Pacific, especially among the poor. As a result, NCDs are expected to rise sharply among vulnerable populations such as older people and those of low socioeconomic status. Due to common risk factors, the upward trend in NCDs can be mitigated by deploying effective prevention programmes which incorporate multi-level, multi-sectoral and community-based strategies. Interventions focused on risk factors and their environmental, economic, social and behavioural determinants are crucial. There is a strong link between low education levels and high rates of noncommunicable disease in both developed and developing nations. Improving social capacity in education has a significant positive impact on reducing NCDs.
The poor have the worst outcomes from NCDs. In developing nations,
The Need for Pro-poor Strategies in the Western Pacific Region: A Review

deaths from NCDs are highest among economically productive age groups. More severe outcomes for the poor from NCDs are not only caused by greater risk behaviours and increased incidence of disease, but also from their inability to access or afford preventative services and treatment. Late diagnoses due to a delay in seeking care means more chronic illness and complications. Poor people may also receive inferior services and be subject to discrimination from care providers. In developing countries, more accessible health care for the poor improves equity. Noncommunicable disease prevention, education programmes and affordable treatment initiatives are an appropriate priority for the World Health Organization (WHO), development agencies, and national and local health service providers.
The economic impact of ill-health on low-income households can be substantial, creating a vicious cycle which forces people deeper into poverty and more illness. Reducing reliance on out-of-pocket payments for health care can lessen the impact of these diseases on the poor. Targeting NCD interventions on the poor leads to a more efficient health sector by improving the well-being of the group with the greatest burden of disease and mortality. From an economic perspective, providing higher quality health care for the poor increases their productivity and income, thereby assisting national development. Successful prevention programmes for the poor also reduce costly hospital admissions and the demand for acute care.
The assumption that NCDs are diseases of affluence has inhibited effective planning for, and servicing of, the growing incidence of NCDs among the poor in the Western Pacific Region. The issues are clear: incidence and prevalence of NCDs are increasing rapidly and the poor bear a disproportionate burden. What is now urgently needed are policies, mechanisms and budget allocations to address this growing pandemic. Health services first require a focus on prevention and primary care, followed by secondary and tertiary prevention that is based on established NCD intervention protocols for specific conditions. Health information systems should be developed to monitor incidence, service activity and costs of NCD programmes and identify services by geographic area to help disaggregate information about the poor. This data can be used to manage effective NCD programmes and establish an evidence base in the Western Pacific Region, which currently does not exist. Effective pro-poor interventions for NCDs need to be multi-dimensional and involve local, national, global and public and private initiatives, including elements outside the health sector. Interventions must be targeted and sustained over long periods with regular monitoring to ensure objectives are met,. Pro-poor health systems combining formal and technical mechanisms as well as informal community or family-based structures should be in accessible locations and provide useful information. They should also be affordable, include
Exec
utiv
e Su
mm
ary
viii
Noncommunicable Disease and Poverty

equitable financing mechanisms and be sustained on a long-term basis. As the NCD burden among the poor and their needs vary substantially between and within countries of the Western Pacific Region, pro-poor NCD policies should be developed at a country level with local input. Given the high and increasing burden of disease from NCDs in the Western Pacific among the vulnerable poor, a strengthened focus on NCD interventions for the poor in the Region is justifiable. This is not to argue for a diversion of resources from communicable diseases to NCDs, but rather for an appropriate investment in primary and secondary prevention to ensure both are effectively and efficiently controlled.
Exec
utiv
e Su
mm
ary
ix
The Need for Pro-poor Strategies in the Western Pacific Region: A Review


The Need for Pro-poor Strategies in the Western Pacific Region: A Review
1
Introduction
Intr
oduc
tion

Noncommunicable Disease and Poverty
2
This paper analyses the links between poverty and noncommunicable diseases (NCDs). The analysis is based on a review of the current literature with particular reference to the Western Pacific Region. The paper was commissioned by the World Health Organization (WHO) Western Pacific Regional Office to stimulate discussion on the relationship between poverty and NCDs, to contribute to the reduction of their impact on poor people in developing countries, and to promote a better understanding of how health outcomes for poor people with NCDs can be improved.
Methodology
Literature on Poverty and NCD for the last 20 years was identified from Google, the National Library of Medicine Pubmed/Medline, the WHO website, the Asian Development Bank website, the World Trade Organization website and the World Bank website. Keywords used in searches are listed in Table 1. Keywords were progressively refined to ensure the relevance of literature to this review. Due to the immense volume of the literature on poverty and disease, this review is confined to a representative sample. Literature was extracted primarily from peer-reviewed journals, published texts and documents and reports from official WHO and related development agencies. The bibliographies and references in key articles identified additional literature sources.
The extent to which the links between poverty and health are the primary focus of the literature is highly variable. Thus, a large proportion
Intr
oduc
tion
Table 1: Key-words used in literature search
“Poverty and Disease”Poverty + Disease + PacificPoverty + “coping with disease”Poverty + “health outcomes”Poverty + “risk factors for disease”“Poor people” + “noncommunicable disease”Poverty + health + “best practice”“Noncommunicable disease” + Poverty + “Western Pacific”Poverty + NCDs + Pacific“noncommunicable disease” + gender“noncommunicable disease + “rural/urban dif-ferences”“noncommunicable disease” + “level of education”
Poverty + “noncommunicable disease”Poverty + “Burden of disease”Poverty + “access to health services”Poverty + “structural barriers” + healthPoverty + “cost of care”Poverty + “assistance programs” + health“Links between poverty and disease”Inequality + “Noncommunicable disease”“Socioeconomic status” + “noncommunicable disease” + Pacific“noncommunicable disease” + ethnicity“noncommunicable disease” + inequityDisease Specific searches (e.g., “Poverty and heart disease”; Poverty and Cancer) were also utilised.

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
3In
trod
uctio
n
of the literature reviewed deals with health or communicable diseases specifically without reference to poverty. Documents were selected based on the extent of their discussion of the links between poverty and/or low socioeconomic status and noncommunicable disease or of pro-poor interventions. The review aims primarily to focus on literature relating to the Western Pacific Region, but the limited availability of relevant information required the use of information from other regions. Where used, information from other regions is interpreted as indicative of the poverty-NCD relationships and it is not necessarily representative of the Western Pacific Region
Efforts were made to secure information from the broadest possible range of sources. However, WHO is a key source of information on the links between poverty and NCD and the dominance of this source is reflected in citations in the following sections.
Poverty
There are a number of different ways in which poverty can be defined and measured. Income measurements of poverty such as income below the nationally defined poverty line or living on less than one US dollar per day are the most widely used in the literature. The global definition of absolute poverty includes those living on less than one dollar per day.1 In nations with a higher average income, people can be earning more than a dollar a day and still be very poor compared with other
50
40
30
20
10
0
% in
Pove
rty
Cambod
iaChin
a Fiji
Republic
of Kore
a
Lao Pe
ople ‘s
Democr
atic Repu
blic Malaysia
Mongolia
Figure 1: Percentage of population in poverty in selected Western Pacific Region countries
Papua
New
GuineaPhi
lippine
s
Viet Nam
Samoa
Note: These figures are based on nationally defined income poverty lines. Source: Asian Development Bank Poverty and Inequality Indicators http://www.adb.org/Documents/EDRC/Statistics/rt_06.xls (last accessed 18th August 2005)
Total % in poverty Urban Rural

Noncommunicable Disease and Poverty
4In
trod
uctio
n
people in their society. This is termed relative poverty. Relative poverty is particularly important in discussing the Western Pacific Region, since most of the poor in this region would be classified as living in relative poverty as opposed to absolute poverty (see Figure 1).
Income-based definitions do not effectively describe the multi-dimensional nature of poverty. Families can be earning above the poverty line, but women and children in the family may be subsisting on far less. Disadvantaged ethnic groups or people living in rural areas may be considered to be in poverty due to their inability to access health care. Poor education can lead to social exclusion and disadvantage. Differences in health status and health inequities result not only from purely economic differences, but also from disparities in education, occupation, race, ethnicity and gender. Poverty also involves exclusion from the political process, leaving groups voiceless and disempowered.
Unless otherwise specified, this paper uses this broader conceptualization of poverty.
NCD
Noncommunicable diseases are defined as those diseases which are not transmissible or caused by injury. Many of the most common NCDs share common risk factors and can be reduced through common preventative strategies. Many NCDs take a chronic course and are therefore “amenable to common approaches to care or management.” 2 Due to space limitations, discussion on NCDs in this report is limited to major NCDs such as cardiovascular disease (CVD), cancers, respiratory disease and diabetes.
Psychological diseases and disorders are not specifically addressed, although it is noted that disorders such as depression represent a significant proportion of the global burden of disease. Similarly, there is variance in the literature as to whether injuries are included among NCDs. This paper, taking them as a separate category, excludes a discussion of injuries.
Noncommunicable diseases are also referred to in the literature as “chronic diseases”. However, for the purposes of this paper this terminology is not generally applied because chronic diseases now also include communicable diseases such as HIV and hepatitis.
Comment on Poverty and NCD Literature
A Google search using the term “links between poverty and disease” produces approximately 40 hits. Of these, more than 90% refer to communicable diseases. It was found that relatively little literature is
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
5In
trod
uctio
n
specifically devoted to the relationship between NCDs and poverty, reflecting the historical linkage and focus on the relationship between poverty and communicable diseases. Most available literature specific to the topic explores the relationship between poverty and specific NCD conditions (e.g., CVD) in developed countries. Links between NCD and poverty are clearly under-represented in the literature. Further, data on poverty and NCDs in Western Pacific Region nations are even more limited. Although some surveys have been conducted, especially in the more developed nations in the region, there is a lack of good national or regional databases on NCDs. Available methodologies for NCD surveillance tend to be research-oriented, and resource intensive and therefore generally unsuited for small, isolated or less developed countries. Baseline data on NCD risk factors and mortality and morbidity from NCDs are not available from many developing and/or small island countries.3
WHO has adopted and recommends the STEPwise approach to surveillance (STEPS) NCD surveillance tool as offering a common approach to “defining core variables for surveys with the goal of achieving data comparability over time within and between countries.” It provides an entry-point for low and middle income countries to begin NCD surveillance and control activities.4 The STEPS programme is useful for low-income nations as it focuses on increasing national capacity to obtain recent and valid statistical information on NCD and risk factor prevalence, and arranges the conduct of annual surveys.5 This tool is currently being implemented throughout the region. However, it is not specifically designed to assess the links between poverty and NCDs.
At the outset, it is noted that there are relatively few studies on the interrelationship between poverty and NCDs in the Western Pacific Region or elsewhere. Indeed, as stated above, regional data on NCDs are limited.
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
7N
onco
mm
unic
able
Dis
ease
in t
he W
este
rn P
acifi
cNoncommunicable Disease in the Western Pacific

Noncommunicable Disease and Poverty
8N
onco
mm
unic
able
Dis
ease
in t
he W
este
rn P
acifi
c NCDs are often regarded as “diseases of affluence.” However, in wealthier nations it is the poor who have higher risk factors and higher rates of NCDs.6 For example, in 1994 in the United States of America, 29.3% of children and adolescents in the lowest income bracket were classified as overweight, compared with 21.7% in the highest income bracket. From 1971, the percentage among the lowest income bracket had increased by 14.7%, compared with 8.6% in the highest income bracket.7 Mortality from CVD among people in the highest income brackets in the United States of America is believed to be one third of the mortality of those in the lowest income brackets. Similarly, mortality from CVD among those with university level education is approximately one third the mortality of those with only primary level education.8
Furthermore, developing countries now bear the major burden of NCDs and WHO notes that NCDs cannot continue to be regarded as diseases of affluence. Globally, low and middle income countries now account for 80% of all CVD related deaths and 87% of CVD related disabilities, mainly in working-age adults (see Figure 2).9 In the Western Pacific Region, 75% of diabetes and 90% of new cancer cases diagnosed each year are in developing countries.10
The Pan American Health Organization notes that erroneously identifying NCDs as diseases of affluence has led to misguided policy decisions and the growing awareness of how NCDs affect the poor as well as the rich requires greater attention be paid to NCDs in poverty reduction programmes.11 The assumption that NCDs, such as cardiovascular disease, mostly afflict the wealthy and elderly has resulted in the neglect of such diseases among the less well off and discounted their negative effect on the progress of developing nations. Besides, limited resources, low awareness of the risk factors and the low priority assigned to NCDs unfortunately “mean that many developing countries have been unable to respond effectively to rising levels of NCD.”12
In 2000, Gwatkin noted that “no analyses of the recent burden disease data have yet been undertaken for poor and rich population groups
Death
s (m
illion
s/yea
r)
Figure 2: Projected trends in causes of death in developing regions
Noncommunicable diseases
Communicable diseases
Injuries
1990 2000 2010 2020Source: Yach, D. et al. Noncommunicable Diseases with Special Focus on Cardiovascular disease and diabetes in the Developing World (Seminar Report 27 April 2001) ENRECA, Copenhagen 2001 http://enreca.pubhealth.ku.dk/2001_NonComDis.pdf (last accessed 25 August 2005)
40
30
20
10
0
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
9N
onco
mm
unic
able
Dis
ease
in t
he W
este
rn P
acifi
c
within countries.”13 The literature review conducted for the present paper has not identified recent data of this nature from the Western Pacific Region. Nevertheless, while the available information suggests that, globally, communicable diseases are still highly prevalent among the poor, NCDs are beginning to be recognised as the major cause of morbidity and mortality among this group.14
Other studies also demonstrate that developing nations are experiencing an epidemiological transition, which involves rapidly increasing burdens of NCDs, as well as continuing high rates of communicable disease. In 1998, 77% of all deaths attributable to NCD occurred in developing countries and 85% of the NCD disease burden occurred in low and middle income countries.15
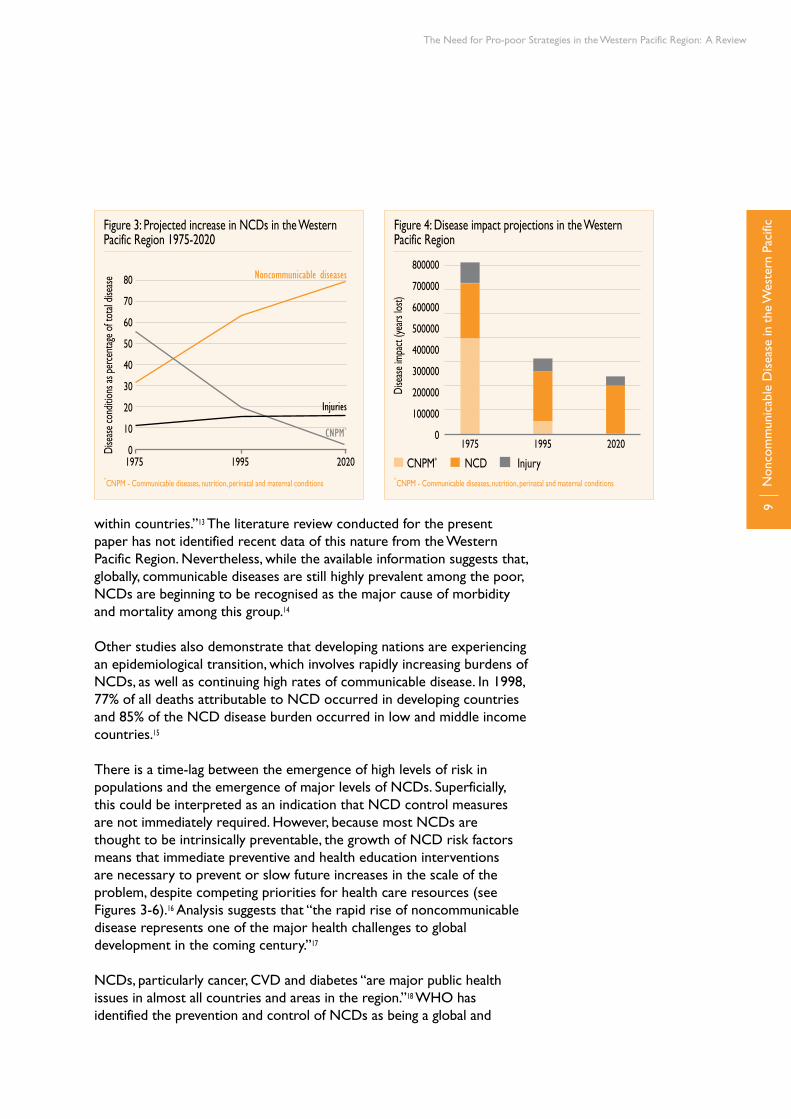
There is a time-lag between the emergence of high levels of risk in populations and the emergence of major levels of NCDs. Superficially, this could be interpreted as an indication that NCD control measures are not immediately required. However, because most NCDs are thought to be intrinsically preventable, the growth of NCD risk factors means that immediate preventive and health education interventions are necessary to prevent or slow future increases in the scale of the problem, despite competing priorities for health care resources (see Figures 3-6).16 Analysis suggests that “the rapid rise of noncommunicable disease represents one of the major health challenges to global development in the coming century.”17
NCDs, particularly cancer, CVD and diabetes “are major public health issues in almost all countries and areas in the region.”18 WHO has identified the prevention and control of NCDs as being a global and
Figure 4: Disease impact projections in the Western Pacific Region
Dise
ase i
mpa
ct (y
ears
lost)
1975 1995 2020
800000
700000
600000
500000
400000
300000
200000
100000
0
*CNPM - Communicable diseases, nutrition, perinatal and maternal conditions
CNPM* NCD Injury
80
70
60
50
40
30
20
10
0
Figure 3: Projected increase in NCDs in the Western Pacific Region 1975-2020
*CNPM - Communicable diseases, nutrition, perinatal and maternal conditions
Dise
ase c
ondit
ions
as p
erce
ntag
e of t
otal
disea
se
1975 1995 2020
Noncommunicable diseases
CNPM*
Injuries
Noncommunicable Disease and Poverty
10N
onco
mm
unic
able
Dis
ease
in t
he W
este
rn P
acifi
c
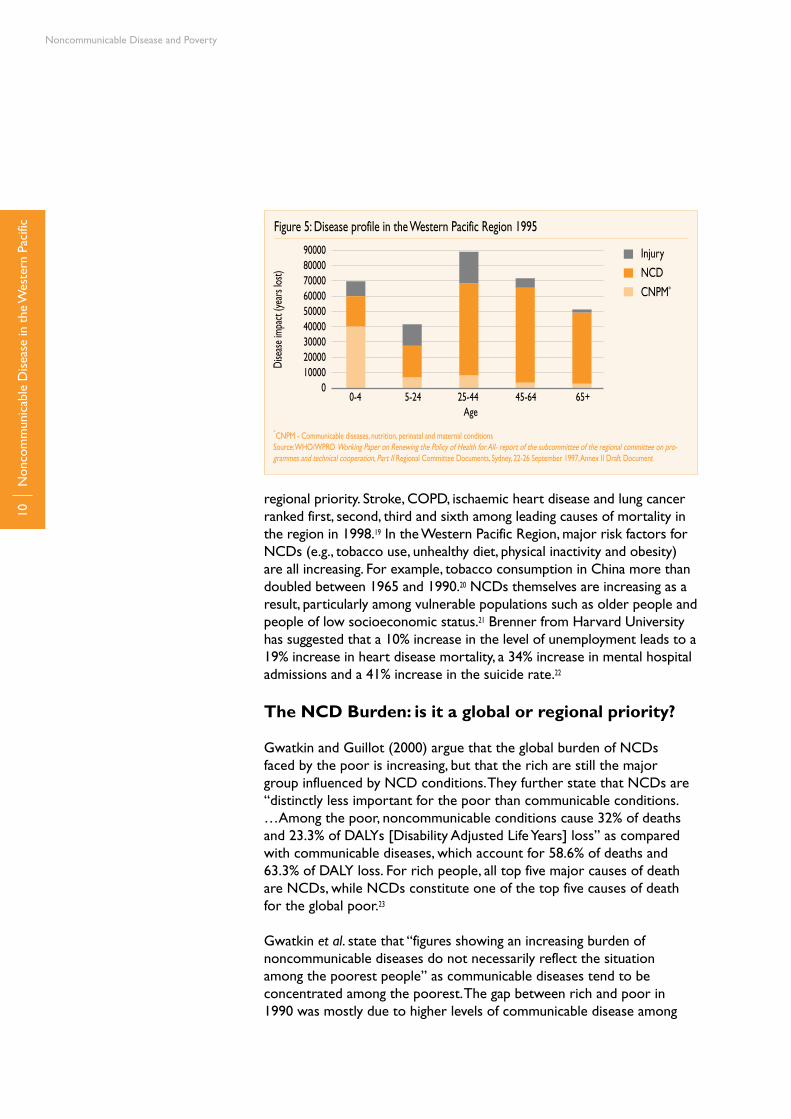
regional priority. Stroke, COPD, ischaemic heart disease and lung cancer ranked first, second, third and sixth among leading causes of mortality in the region in 1998.19 In the Western Pacific Region, major risk factors for NCDs (e.g., tobacco use, unhealthy diet, physical inactivity and obesity) are all increasing. For example, tobacco consumption in China more than doubled between 1965 and 1990.20 NCDs themselves are increasing as a result, particularly among vulnerable populations such as older people and people of low socioeconomic status.21 Brenner from Harvard University has suggested that a 10% increase in the level of unemployment leads to a 19% increase in heart disease mortality, a 34% increase in mental hospital admissions and a 41% increase in the suicide rate.22
The NCD Burden: is it a global or regional priority?
Gwatkin and Guillot (2000) argue that the global burden of NCDs faced by the poor is increasing, but that the rich are still the major group influenced by NCD conditions. They further state that NCDs are “distinctly less important for the poor than communicable conditions. …Among the poor, noncommunicable conditions cause 32% of deaths and 23.3% of DALYs [Disability Adjusted Life Years] loss” as compared with communicable diseases, which account for 58.6% of deaths and 63.3% of DALY loss. For rich people, all top five major causes of death are NCDs, while NCDs constitute one of the top five causes of death for the global poor.23
Gwatkin et al. state that “figures showing an increasing burden of noncommunicable diseases do not necessarily reflect the situation among the poorest people” as communicable diseases tend to be concentrated among the poorest. The gap between rich and poor in 1990 was mostly due to higher levels of communicable disease among
Dise
ase i
mpa
ct (y
ears
lost)
900008000070000600005000040000300002000010000
0
*CNPM - Communicable diseases, nutrition, perinatal and maternal conditionsSource: WHO/WPRO Working Paper on Renewing the Policy of Health for All- report of the subcommittee of the regional committee on pro-grammes and technical cooperation, Part II Regional Committee Documents, Sydney, 22-26 September 1997, Annex II Draft Document
Injury
NCD
CNPM*
0-4 5-24 25-44 45-64 65+Age
Figure 5: Disease profile in the Western Pacific Region 1995

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
11N
onco
mm
unic
able
Dis
ease
in t
he W
este
rn P
acifi
c
the poor “rather than to differences in their burden of noncommunicable disease”. However, these estimates are “necessarily crude” and are mainly of relevance to interventions on the global, rather than national, scale.24
The large difference between the effects of NCDs and communicable disease among the poor reflects the concentration of deaths and Disability Adjusted Life Years (DALYs) lost to communicable diseases among the global poor. Specifically, 60% of all ill-health for the poor results from communicable disease as opposed 8-11% among the richest quintile. The figures also reflect differences in age among distribution of deaths. For example, more than half of all deaths among the poor occur before the age of 15, compared with only 4% for the rich. This is also a result of communicable disease. However, “death and disability from [communicable disease] is projected to decline rapidly by 2020, roughly equalizing the health damage from communicable and noncommunicable diseases among the poor.”25 By 2020 it is expected that NCDs will be the largest cause of death in all regions apart from sub-Saharan Africa.26
Gwatkin et al. conclude that any shift in emphasis by health policies and programmes from communicable to noncommunicable disease “would have important distributional implications” and that a shift of this nature “would work to the detriment of the poor” and work primarily in favour of the rich.27
Sen and Bonita (2000) criticize Gwatkin’s conclusions as undermining the “developing momentum towards addressing the growing epidemic of noncommunicable diseases in less developed countries” with a “flawed interpretation of data of the global burden of disease study.”28 They argue that the focus on the poorest and richest quintiles of the global
Dise
ase i
mpa
ct (y
ears
lost)
100000900008000070000600005000040000300002000010000
0
*CNPM - Communicable diseases, nutrition, perinatal and maternal conditionsSource: WHO/WPRO Working Paper on Renewing the Policy of Health for All- report of the subcommittee of the regional committee on pro-grammes and technical cooperation, Part II Regional Committee Documents, Sydney, 22-26 September 1997, Annex II Draft Document
Injury
NCD
CNPM*
0-4 5-24 25-44 45-64 65+Age
Figure 6: Disease profile projected to 2020

Noncommunicable Disease and Poverty
12N
onco
mm
unic
able
Dis
ease
in t
he W
este
rn P
acifi
c population ignores the fact that “most of the remaining 60% live in less well-developed countries [and] the major burden of noncommunicable disease rests in this segment of the world’s population.”29 In other words, this 60% of the global population contains a significant share of poor people and there is considerable evidence that risk factors for NCDs are concentrated among low-income and disadvantaged groups within the global population. In 1998, of the total global mortality from NCDs, 77% occurred in low and middle income countries, and 85% of the global burden of disease attributed to NCDs was borne by low and middle income countries.30 Yach et al. (2001) comment that although NCDs are viewed as diseases of wealthy nations, it is the poor in these nations who are most affected. Furthermore, as the epidemiological transition progresses in developing nations, rising numbers of poor people in these nations are expected to be affected by NCDs.31
NCD mortality in developing countries is predicted to increase from 47% in 1990 to 69% in 2020.32 NCDs are now the leading cause of death and disability worldwide, accounting for 60% of all deaths and 43% of the global burden of disease in 1998.33 Factors driving the increase in chronic disease incidence and disability and death among the poor include social and demographic changes, shifts in patterns of consumption, under-nutrition, trauma and the structure and focus of health services. Material deprivation and low levels of education exacerbate the burden of disease.34
Age-specific death rates from all causes have a tendency to decline with development, but death rates from communicable diseases tend to decline more rapidly. Combined with demographic change this is a reason why NCDs tend to become the dominant diseases as countries develop.35 Age-specific mortality rates from NCDs, particularly before age 60, tend to be higher in developing countries than in developed countries.36 There are some exceptions, as age-specific incidence of type 2 diabetes, obesity and smoking related diseases tend to increase in many populations.
In the Western Pacific Region, the NCD burden is greater than that of communicable disease. For example, NCDs represent 92% of the burden of disease in DALYs in Western Pacific Regional Office-A nations (WPRO-A) and approximately 63% in Western Pacific Regional Office-B nations (WPRO-B) (see Table 2). Further, Western Pacific Regional Office-B nations have more than a quarter of the global total burden of disease in DALYs for malignant neoplasms and musculo-skeletal disorders, and close to a third
Cause WPRO-A WPRO-B (000) (000)All Communicable Disease 1 064 56 205All Noncommunicable Disease 13 720 150 556
Table 2: Burden of disease in DALYs by cause and Region-al mortality strata, estimates for 200137
Source: Derived from Murray, C. et al. World Health Report 2002 Geneva, WHO, 2002.
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
13N
onco
mm
unic
able
Dis
ease
in t
he W
este
rn P
acifi
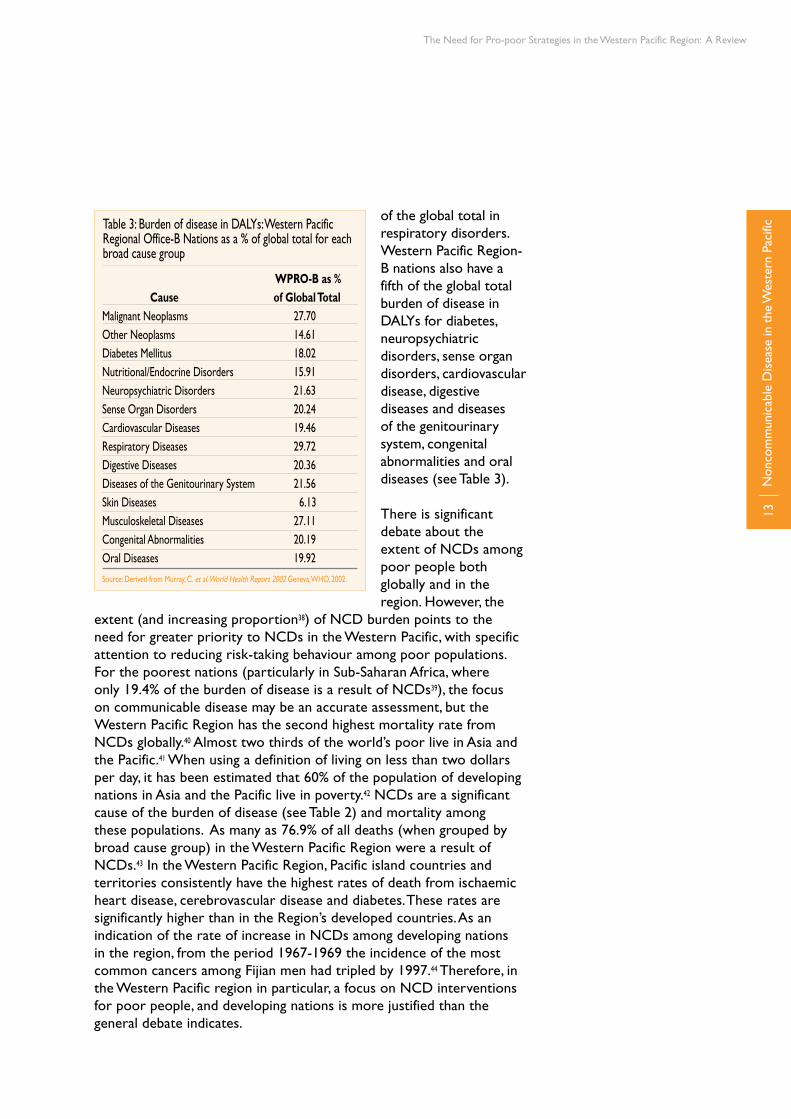
cof the global total in respiratory disorders. Western Pacific Region-B nations also have a fifth of the global total burden of disease in DALYs for diabetes, neuropsychiatric disorders, sense organ disorders, cardiovascular disease, digestive diseases and diseases of the genitourinary system, congenital abnormalities and oral diseases (see Table 3).
There is significant debate about the extent of NCDs among poor people both globally and in the region. However, the
extent (and increasing proportion38) of NCD burden points to the need for greater priority to NCDs in the Western Pacific, with specific attention to reducing risk-taking behaviour among poor populations. For the poorest nations (particularly in Sub-Saharan Africa, where only 19.4% of the burden of disease is a result of NCDs39), the focus on communicable disease may be an accurate assessment, but the Western Pacific Region has the second highest mortality rate from NCDs globally.40 Almost two thirds of the world’s poor live in Asia and the Pacific.41 When using a definition of living on less than two dollars per day, it has been estimated that 60% of the population of developing nations in Asia and the Pacific live in poverty.42 NCDs are a significant cause of the burden of disease (see Table 2) and mortality among these populations. As many as 76.9% of all deaths (when grouped by broad cause group) in the Western Pacific Region were a result of NCDs.43 In the Western Pacific Region, Pacific island countries and territories consistently have the highest rates of death from ischaemic heart disease, cerebrovascular disease and diabetes. These rates are significantly higher than in the Region’s developed countries. As an indication of the rate of increase in NCDs among developing nations in the region, from the period 1967-1969 the incidence of the most common cancers among Fijian men had tripled by 1997.44 Therefore, in the Western Pacific region in particular, a focus on NCD interventions for poor people, and developing nations is more justified than the general debate indicates.
WPRO-B as % Cause of Global TotalMalignant Neoplasms 27.70Other Neoplasms 14.61Diabetes Mellitus 18.02Nutritional/Endocrine Disorders 15.91Neuropsychiatric Disorders 21.63Sense Organ Disorders 20.24Cardiovascular Diseases 19.46Respiratory Diseases 29.72Digestive Diseases 20.36Diseases of the Genitourinary System 21.56Skin Diseases 6.13Musculoskeletal Diseases 27.11Congenital Abnormalities 20.19Oral Diseases 19.92
Table 3: Burden of disease in DALYs: Western Pacific Regional Office-B Nations as a % of global total for each broad cause group
Source: Derived from Murray, C. et al. World Health Report 2002 Geneva, WHO, 2002.

Noncommunicable Disease and Poverty
14N
onco
mm
unic
able
Dis
ease
in t
he W
este
rn P
acifi
c There is agreement in the literature that the demographic and epidemiological transitions in Asia and the Pacific are shifting the disease burden from communicable towards noncommunicable disease. The aging population in particular has trends away from diseases associated with poor nutrition and infection towards more degenerative diseases.45 However, there is a significant difference between the Asia Pacific region and the more classic epidemiological transition that occurred in Western countries where the burden of communicable disease declined and was replaced by a rising burden of noncommunicable disease. By contrast, developing nations in Asia and the Pacific are experiencing a double burden with noncommunicable and communicable diseases now existing simultaneously.
Over time, the overlap is expected to become more like the classic transition with a reduction of communicable disease and an increase of noncommunicable disease.46 In the meantime, the double burden of communicable and noncommunicable disease is likely to have the greatest impact on the Western Pacific Region’s poor. In China, the poor have greater mortality not only from communicable diseases, but also from NCDs which cause substantially more deaths (see Figure 7). The poor in China have higher rates of mortality than wealthier groups from both communicable diseases and NCDs, with NCDs causing the absolute greater amount of mortality.
In the Region, there are examples, such as the Pacific island nations, Cambodia and the Lao People’s Democratic Republic (see Figure 8), where communicable disease remains dominant. The phenomenon of overlap between communicable and NCD clearly varies not only
Poorest
II
III
Wealthiest
Communicable Diseases
Noncommunicable Diseases
Injuries
445Q
15 m
ortal
ity ra
te (D
eath
s per
1 0
00)
9
8
7
6
5
4
3
2
1
0
Figure 7: Female adult mortality rates by cause of death and average community income, China 1987-1988
Source: Peabody, J. W. et al. Policy and Health- implications for development in Asia, New York, Cambridge University Press, 1999. Note 45Q15 mortality rate is the probability of dying between the ages of 15 and 60.

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
15N
onco
mm
unic
able
Dis
ease
in t
he W
este
rn P
acifi
c
Dise
ase c
ondit
ions
as p
erce
ntag
e of t
otal
impa
ct 100%90%80%70%60%50%40%30%20%10%0%
Asia I Asia II Cam/Lao Aus/NZ Japan Pacific I Pacific II ChinaCountries
*CNPM - Communicable diseases, nutrition, perinatal and maternal conditionsAsia I: Brunei Darussalam, China; China, Hong Kong Special Administrative Region; China, Macao Special Administrative Region, Malaysia, Singapore, Republic of KoreaAsia II: Mongolia, Philippines, Viet NamCam/Lao: Cambodia and Lao People’s Democratic RepublicAus/NZ: Australia and New ZealandJapan: JapanPacific I: American Samoa, Cook Islands, Fiji, French Polynesia, Guam, Northern Mariana Islands, Nauru, New Caledonia, Niue, Palau, Samoa, Tokelau, Tonga, Tuvalu, Wallis and FortunaPacific II: Kiribati, Marshall Islands, Federated States of Micronesia, Papua New Guinea, Solomon Islands and VanuatuChina: ChinaSource: WHO/WPRO Working Paper on Renewing the Policy of Health for All- report of the subcommittee of the regional committee on programmes and technical cooperation, Part II Regional Committee Documents, Sydney, 22-26 September 1997, Annex II Draft Document.
Injury
NCD
CNPM*
Figure 8: Disease profile by country grouping in the Western Pacific 1995
between regions around the globe, but also between and within countries and regions. For example, all the Pacific island nations record both communicable and noncommunicable diseases as their leading causes of death. Communicable diseases remain major killers in nations such as Papua New Guinea, whereas Nauru has very high rates of diabetes (above 20% of the population) with diabetes, CVD and cancer now the leading causes of mortality. The decline in communicable diseases may stall in some groups within a population, while other groups within the same population may be primarily affected by NCDs.47

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
17
Prevention Programmes
Prev
entio
n Pr
ogra
mm
es
Noncommunicable Disease and Poverty
18Pr
even
tion
Prog
ram
mes
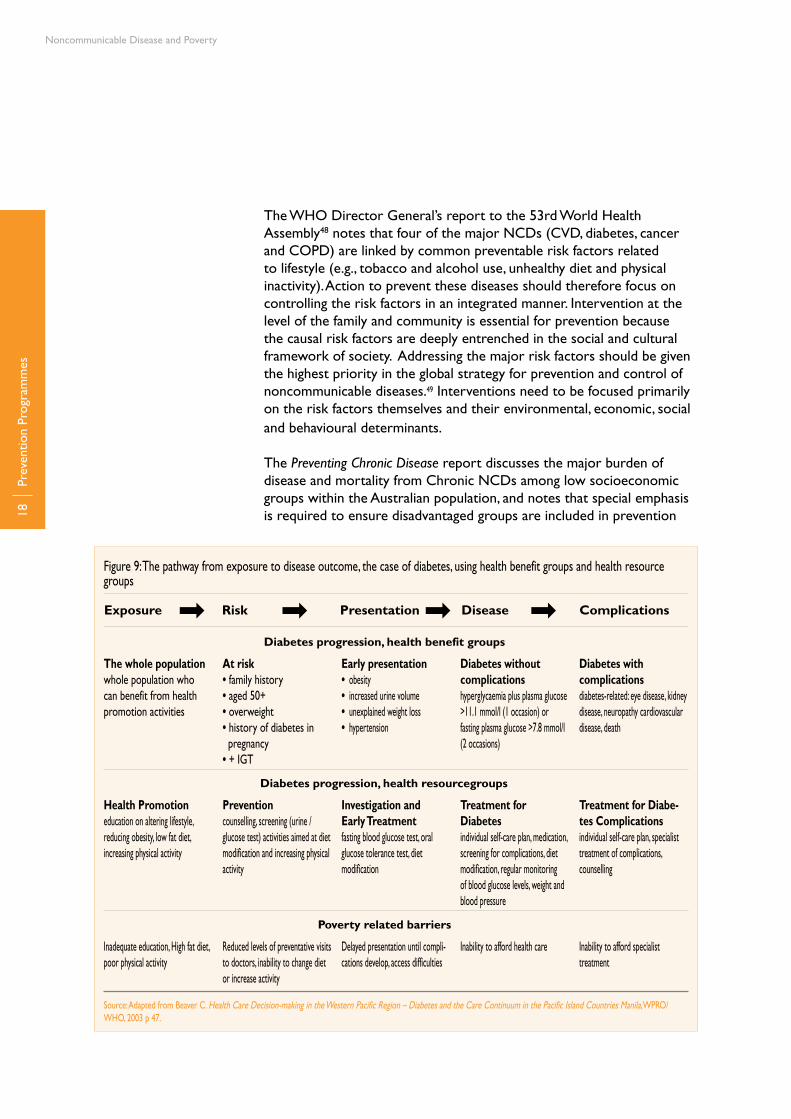
Figure 9: The pathway from exposure to disease outcome, the case of diabetes, using health benefit groups and health resource groups
The whole populationwhole population who can benefit from health promotion activities
At risk• family history• aged 50+• overweight• history of diabetes in pregnancy• + IGT
Early presentation• obesity• increased urine volume• unexplained weight loss• hypertension
Diabetes without complicationshyperglycaemia plus plasma glucose >11.1 mmol/l (1 occasion) or fasting plasma glucose >7.8 mmol/l (2 occasions)
Diabetes with complicationsdiabetes-related: eye disease, kidney disease, neuropathy cardiovascular disease, death
Exposure → Risk → Presentation → Disease → Complications
Diabetes progression, health benefit groups
Health Promotioneducation on altering lifestyle, reducing obesity, low fat diet, increasing physical activity
Preventioncounselling, screening (urine / glucose test) activities aimed at diet modification and increasing physical activity
Investigation and Early Treatmentfasting blood glucose test, oral glucose tolerance test, diet modification
Treatment for Diabetesindividual self-care plan, medication, screening for complications, diet modification, regular monitoring of blood glucose levels, weight and blood pressure
Treatment for Diabe-tes Complicationsindividual self-care plan, specialist treatment of complications, counselling
Diabetes progression, health resourcegroups
Inadequate education, High fat diet, poor physical activity
Reduced levels of preventative visits to doctors, inability to change diet or increase activity
Delayed presentation until compli-cations develop, access difficulties
Inability to afford health care Inability to afford specialist treatment
Poverty related barriers
Source: Adapted from Beaver C. Health Care Decision-making in the Western Pacific Region – Diabetes and the Care Continuum in the Pacific Island Countries Manila, WPRO/WHO, 2003 p 47.
The WHO Director General’s report to the 53rd World Health Assembly48 notes that four of the major NCDs (CVD, diabetes, cancer and COPD) are linked by common preventable risk factors related to lifestyle (e.g., tobacco and alcohol use, unhealthy diet and physical inactivity). Action to prevent these diseases should therefore focus on controlling the risk factors in an integrated manner. Intervention at the level of the family and community is essential for prevention because the causal risk factors are deeply entrenched in the social and cultural framework of society. Addressing the major risk factors should be given the highest priority in the global strategy for prevention and control of noncommunicable diseases.49 Interventions need to be focused primarily on the risk factors themselves and their environmental, economic, social and behavioural determinants.
The Preventing Chronic Disease report discusses the major burden of disease and mortality from Chronic NCDs among low socioeconomic groups within the Australian population, and notes that special emphasis is required to ensure disadvantaged groups are included in prevention

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
19Pr
even
tion
Prog
ram
mes
and treatment programmes, including targeting the social and life-course determinants of disadvantage. However the proposed measures do not describe specifically how the interventions can be targeted to meet the needs of poor people.50
WHO has initiated the CINDI (Countrywide Integrated Noncommunicable Disease Intervention) programme, which has provided successful examples of comprehensive long-term NCD prevention programmes. The approach of the programme has been to address behavioural risk factors “through multi-level prevention strategies, while aiming to control biological risk factors and conditions through early detection and effective management to prevent progression to chronic disease and complications.” These programmes have “achieved a certain level of success in European countries”, but there is a further challenge posed by the “disproportionate impact of the rapid increase of NCDs on poor and disadvantaged populations.”51
The lack of a specific pro-poor focus within NCD programmes may undermine their long-term success. Providing health for poor people is not only a matter of providing appropriate services and quality care but is also integrally linked with the provision of an enabling environment for the poor to protect health as an asset for their livelihoods. Health for the poor should be approached from a rights and security perspective which requires strengthening the capacity, skills and knowledge of poor people.52
In South Africa, awareness of disease and risk factors (as well as treatment and use of medication) has been found to increase significantly with increased wealth.53 Dissemination of information on NCD risk factors through the mass media, health campaigns, public information systems and schools can thus be crucial. Effective information, education and communications can facilitate personal behavioural change.54
RAND Corporation studies on poverty and health links in developing countries in Asia show that interventions which are focused on individual case management in high level facilities are often too costly to be effective for the majority of the population and have little impact on reducing societal health burdens. However, the wealthy elites often use political leverage to ensure governments allocate resources to expensive medical/surgical treatment of [increasing rates] of NCDs. This disadvantages poorer segments of the population and eats into scarce public health resources.
The implication is that for the good of society as a whole, interventions on NCDs should concentrate on health education, promotion and prevention activities and screening, as well as low cost interventions in order to reduce long-term and high-cost complications. Specific

Noncommunicable Disease and Poverty
20Pr
even
tion
Prog
ram
mes
interventions with efficient cost-effectiveness values include reducing smoking and alcohol consumption (cost per DALY averted $25) and cancer pain palliation (cost per DALY averted $150). As national incomes increase, other programmes such as cancer screening for easily treatable and preventable cancers (cost per DALY averted $50-100), health education on cardiovascular risk factors (cost per DALY averted of $75-$250) and the medical management of diabetes (cost per DALY averted $25-$250) should be prioritized.55
WHO is adopting a broad range approach to NCD prevention and has formulated a global strategy on Diet, Physical Activity and Health. The guiding principles of this strategy are: • providingstrongerevidenceforpolicy(synthesizingexisting
knowledge, science and interventions on the relationship between diet, physical activity and chronic disease);
• advocacyforpolicychange(informingdecisionmakersandstakeholders of the problem, determinants, interventions and policy needs);
• stakeholderinvolvement(agreeontherolesofstakeholdersinimplementing the global strategy); and
• astrategicframeworkforaction(toproposeappropriatelytailored policies and interventions for countries).56
Education and NCDs
Socioeconomic status, literacy and access to health services have a strong impact on the development of NCD and the delivery of health care.57 The benefits of good educational attainment in childhood are consistent across the life-course (see Figure 10). According to Hayward et al. (2001), populations that undergo a major increase in social capacity (defined as the linkage between individual life-course and institutional conditions favourable to health such as increasing the level of education among a population) are likely to experience a substantial decline in the burden of disease.58
Poor children are at much greater risk of low educational achievement and, hence, poor health in their adult years. For example, children of families experiencing financial difficulties are almost nine times more likely to have no educational qualifications and more than 3.5 times more likely to have a limiting illness (such as diabetes or asthma) than children who grow up in a financially secure environment. In developed nations, it has been shown that material and environmental disadvantage tends to increase over the life-course for poorer, older people. Thus if a person is poor, and suffers ill-health as a child, their chances of ill-health throughout life, and experiencing a health disadvantage as they grow older, are significantly higher than for their wealthy and healthier counterparts.59

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
21Pr
even
tion
Prog
ram
mes
Disease in adulthood (e.g., cancer or CVD) is often brought about by a cumulative effect of pathogens, incidents and behaviours which may develop in infancy or in childhood. Studies in the United Kingdom of Great Britain and Northern Ireland have shown that low socioeconomic status throughout the life course is perceived to be a major contributor to the likelihood of the early onset of many types of disease, including NCDs, and reduced chance of survival.60 Men and women aged between 26 and 54 who have experienced low socioeconomic position in childhood are twice as likely to die as people in the highest socioeconomic brackets. Those whose socioeconomic disadvantage continued into early adulthood are between three and five times more likely to die of diseases such cancers and circulatory diseases.61
Low education reduces the ability of poor people to ask questions or read preventive information.62 Poor people may be less “acculturated” to using health care due to low levels of education.63 According to the World Bank, “participatory health education for schoolchildren … is one of the most timely and effective ways of promoting healthier lifestyles and averting the emerging pandemic of noncommunicable diseases among the next generation of the poor”64 (see Figure 11). Crucially, poverty-related interventions should not only address the specific health needs of the poor, they should also create an environment which addresses the broader determinants of health such as education, opportunities for work and income, adequate food and social and political integration of the poor. 65
Less than 12 years
12 years
13 or more years
Death
per
100
000
pop
ulatio
n
Chroni Injuries Communicablediseases diseases
Men
1 000
500
100
50
10
5
1
Women
Education
Figure 10: Deaths in the United States of America (1995) by broad disease type and education
Chroni Injuries Communicablediseases diseases
Source: Pamuk, E. et al. Socioeconomic status and health chartbook, Hyattsville, National Centre for Health Statistics, 1998.

Noncommunicable Disease and Poverty
22Pr
even
tion
Prog
ram
mes
Tobacco Controls
Tobacco taxes can have a significant effect on reducing rates of smoking and providing revenue for other health activities.66 Studies in a number of countries show that for every 10% increase in tobacco prices via taxation, tobacco consumption declines by 5%-8%, with the most marked impact among poor people.67
The short-run price responsiveness of cigarette demand in low- and middle-income countries is twice that of developed nations. It has been estimated that increasing the price of cigarettes by 10% globally through taxation would reduce premature deaths from smoking by 10 million in the current cohort of smokers. Almost 90% of the improved life expectancy would be for people in low and middle income countries.68
Young people are particularly responsive to price increases in tobacco, and price increases would reduce the number of young smokers leading to a significant long-term health gain. Studies from the United States of
Figure 11: Awareness of Diseases Caused by Smoking by Education Level, China 1996
Source: Chinese Academy of Preventive Medicine, Smoking and Health in China: 1996 National Prevalence Survey of Smoking Pattern, China Science and Technology Press 1997.
No schooling Primary Secondary High middle College school school school and above
80%
60%
40%
20%
0%
Injury
NCD
CNPM*
Box 1: Modifying Diets in Chile
In Chile, prevention interventions have focused on enhancing the capability of women of low socio-economic status to purchase healthy and inexpensive food, instead of cheap but unhealthy alternatives. Classes have been conducted which emphasise such alternatives as home-made granola instead of sugared cornflakes. The classes provide a venue for sharing of ideas and recipes, and information on the comparative nutritional value of low-cost foods.
Source: Shaw, J. Chronic Disease: The New Face of Poverty in Chile, American Dietetic Association Foundation http://www.eatright.org/Public/7772_17341.cfm (last accessed 18 August 2005).

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
23Pr
even
tion
Prog
ram
mes
America have shown that the price-elasticity of cigarette demand by people at or below the median income was 70% larger than the rates for people with family incomes above median levels.69
Box 2: The North Karelia Project
The North Karelia Project was launched in 1972 to reduce very high levels of Coronary Heart Disease in North Karelia in Finland, a low-income area with scarce medical resources and many socio-economic problems. The original objective was to reduce the incidence of NCDs through programs involving health services, schools, NGOs, innovative media campaigns, local media, food industry, supermarkets, agriculture and other stakeholders.
In North Karelia, the project was extremely successful. Over 25 years, smoking rates among middle-aged men have been reduced by over 20%, vegetable intake has increased markedly and use of butter on bread has been reduced by around 83%. Changes in behaviour have led to a reduction of 17% in the mean serum cholesterol level of the population. Blood pressure levels “have been brought well under control”. The annual mortality rate from CHD in the middle aged male population has been reduced by 73%. Lung cancer mortality has been reduced more than 70%. This has led to greater life expectancy, an increase of approximately 7 years for men and 6 years for women. However, smoking has increased among women.
Over its lifetime, the scope of the North Karelia project was enlarged to include the broader objectives of integrated prevention and control of major NCDs, health promotion and the prevention of risk related lifestyles in childhood and youth. It was also expanded to cover the entire nation.
Success of the North Karelia project has been attributed to a number of factors. It was sustained over the long-term, with strong leadership and “appropriate institutional basis.” At the time of commencement, there was widespread public concern over the scale of the problem of Coronary Heart Disease, so there was existing public support for the project. Theoretical frameworks were carefully developed in consultation with WHO and leading experts, both in terms of underlying risk factors and with social and behavioural frameworks. Community organisation was a key factor. A wide variety of community groups and stakeholders were directly consulted and there was strong involvement from the community itself. The interventions were flexible, based on ongoing monitoring and feedback, and advantage was taken of opportunities as they arose. Multiple strategies were pursued, including innovative media and communications activities, systematic involvement of primary health care (especially from GPs and public health nurses), collaboration with the food industry and policy changes. The project also worked in close collaboration with national health authorities.
Although this approach can be seen as a general intervention to reduce NCDs overall, regardless of income profile, the success of the North Karelia project in a low income region demonstrates that multi-dimensional and multi-level prevention initiatives can be successful in reducing NCD rates in poor areas. However, it has not yet been determined if the approach can be generalised to control NCDs in poor populations in the Western Pacific Region.
Source: Puska, P. Successful prevention of noncommunicable diseases: 25 year experiences with North Karelia Project in Finland. Public Health Medicine, 2002; 4(1):5-7.
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
25
Poverty and NCD Risk Factors
Pove
rty
and
NC
D R
isk
Fact
ors

Noncommunicable Disease and Poverty
26Po
vert
y an
d N
CD
Ris
k Fa
ctor
s
There is agreement in the literature that there are relatively few major risk factors for the major NCDs. The literature also agrees that these risk factors can be minimised relatively cheaply through health promotion and other community-based interventions.70 High levels of risk and lifestyle factors for NCDs have been shown to exist across socioeconomic strata. Many lifestyle factors such as smoking, alcohol dependence, poor diet and exposure to polluted air have been associated with poverty.71
In Asia and the Pacific, changing lifestyle patterns, including an increased reliance on imported food rich in fat and sugar, changing physical activity patterns resulting in an increasingly sedentary lifestyle and increasing alcohol and tobacco use, have resulted in the growth of the incidence and prevalence of circulatory disorders, coronary artery disease, stroke, diabetes, dental decay and cancer(s). As a result, chronic NCDs have replaced infections and parasitic disease as the principle cause of morbidity and mortality. In Fiji, for example, NCDs now account for more than 50% of deaths among the entire population.72 Availability of unhealthy consumer goods is increasing and public sector health services are often already overstretched, which makes expansion of their programmes into specifically pro-poor interventions increasingly difficult.73
In Western Pacific Regional Office-A nations, risk factor attributable mortality in 2000 was greater among men than women, however, with some exceptions, in Western Pacific Regional Office-B nations the reverse is generally true (see Table 4). Women in Western Pacific Regional Office-B nations have moderately greater mortality from most NCD risk factors, and significantly greater mortality than men from indoor smoke from solid fuels (2.6 times greater). However, men in Western Pacific Regional Office-B nations have significantly greater mortality than women from exposure to carcinogens
Source: Murray, C. et al. World Health Report 2002 Geneva, WHO, 2002.
Risk Factor
Blood pressureCholesterolOverweightLow fruit and veg intakePhysical InactivityTobaccoAlcoholUrban air pollutionIndoor smoke from solid fuelsCarcinogens
Men85 00039 00021 00026 00023 000
128 00023 00010 000
04 000
Women76 00039 00020 00019 00019 00049 000
-28 0008 000
01 000
Men711 000222 000163 000269 000132 000661 000465 000176 000137 00034 000
Women758 000265 000184 000232 000134 000137 00066 000
179 000366 00012 000
WPRO-A WPRO-B
Table 4: Attributable mortality by risk factor, sex and Regional mortality stratum (2000)

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
27Po
vert
y an
d N
CD
Ris
k Fa
ctor
s
(2.8% greater), airborne particles (7.6 times greater), alcohol use (7 times greater) and tobacco use (4.8 times greater).
Smoking and Polluted Air
In the Western Pacific Region, the prevalence of smoking among adult men is around 60%, which is the highest of all WHO regions.74 However, smoking prevalence among Asian women is also rising rapidly.75 There remains a significant gap in smoking prevalence between men and women in the Western Pacific. Of those age 15 years or older in 1998, 62.3% of men smoked as compared with 5.8% of women. Smoking “is generally more prevalent among lower-income populations.”76 World Bank studies show that tobacco consumption is most common among the poor within both wealthy and poor nations and is rising rapidly in low-income countries. 77 Analysis of the impact of smoking on men of low socioeconomic status in Poland in 1996 showed that smoking is responsible for two thirds of the excess risk of mortality for men with only primary education. Studies from other countries (Canada, the United Kingdom and the United States of America) indicate that smoking is responsible for approximately half the difference in adult male mortality between those of highest and lowest socioeconomic status.78
In China, the 1996 National Prevalence Survey of Smoking Patterns showed that people with no education were 6.9 times more likely to smoke than people with university education.79 In Japan, men with junior high school education are more than three times as likely to smoke as men with university education. Japanese women with junior high school education are more than five times as likely to smoke as women with a university education.80 The World Bank notes that, “Smoking prevalence in most developing countries is already highest among the poor, and that if these countries experience a similar pattern to the high income countries, the gap in smoking between rich and poor will widen over time.”81
Smoking prevalence is generally higher in rural than in urban areas in the Pacific. In 1995, it was reported that 70% of men age 46-65 smoked in rural Fijian villages compared with the 60% overall smoking rate in the Western Pacific Region cited above. However, young urban women are increasingly taking up smoking.82 In 1993, in the Lao People’s Democratic Republic, smoking prevalence was three times higher among rural men than urban men and 30 times higher among rural women than urban women.83 Studies in the United States of America have shown that the gender gap in adult smoking prevalence tends to narrow over time, eventually stabilising at a difference of 5%. Smoking among women in the United States of America is nearly three times higher among women with 9 to 11 years of education than among those with more than 16 years of education.84 The educational

Noncommunicable Disease and Poverty
28Po
vert
y an
d N
CD
Ris
k Fa
ctor
s
divide among women who smoke has also been noted in India. Among women in Mumbai, the smoking prevalence among illiterate women is 72%, among those with only primary education 52% and among college graduates 10%.85 In Bangladesh, more than 50% of men in the poorest income groups smoked in 1997, as opposed to 31.7% in the highest income group. Similarly, 59.5% of Bangladeshi men with no education smoke as opposed to 31.6% among men who had completed secondary education.86 Smoking cessation rates are higher for women than men, particularly in the Pacific islands.87 Religious factors and pregnancy influence higher cessation rates among women.88
In South Africa, the poor are at high risk of exposure to passive cigarette smoking and smoky fuels, especially in rural areas. There was approximately 15% greater exposure to environmental tobacco smoke in the home for the poorest men as opposed to the wealthiest men, and more than 50% less exposure for men with more than 12 years of education as opposed to those with no education. In contrast, increases in education and wealth in women did not improve their chances of avoiding this risk. Exposure to polluted air climbed with increasing wealth among women, exposure being around 80% higher in the poorest quintile than in the richest quintile, but among men of the highest income quintile the risk of exposure was 25% less than that among the poorest.89
Those who cook on stoves using wood or other organic matter fuel, mostly women, inhale the equivalent of two packets of cigarettes per day in toxic chemicals. Cooking smoke is estimated to cause 1.6 million deaths per year, mostly among women and children. In households using traditional stoves, women are up to four times as likely to suffer from a long-term obstructive pulmonary disease such as chronic bronchitis.90 The risk of exposure was also more than four times greater in rural areas.91 Mortality among women in Western Pacific Regional Office-B nations attributable to indoor smoke from fuels is more than twice as high as for men.92
High Alcohol Consumption
Excessive alcohol use has been associated with poverty in numerous studies. This risk factor contributes to high levels of hypertension among poor people and produces a range of physical and psycho-social pathologies as well as injury.93 In Malaysia, heavy alcohol consumption is reported among rural Indian labourers, particularly those working on rubber and palm oil plantations. The cost of regular heavy drinking also contributes to the exacerbation of poverty.94
In China, 26.3% of men with less than six years of education and 1.3% of women with less than six years of education reported drinking more than once a day. By comparison, only 7.4% of men and 0.2% of women
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
29Po
vert
y an
d N
CD
Ris
k Fa
ctor
s
with more than 13 years of education reported drinking more than once per day.95
In some Asian and Pacific countries, alcohol use is “a masculine activity, and while heavy drinking is tolerated in males, it is usually disapproved in women.”96 Anthropological studies have shown a trend among some working women to emulate male drinking patterns, though there is the suggestion that this behaviour is concentrated among women with greater earning capacity.97
In many Asian countries, alcohol advertising is specifically targeted to poorer sections of the community. The “Guinness Stout is Good for You” campaign in Asia during the 1980s appealed to the poorer working class, through the tag line that the drink would “put back what the day takes out.”98 The drink also contained a higher alcohol content than beer for the same price. In Malaysia, special offers and redemption schemes entice the poor to purchase more of the product, such as a free promotional plate being offered with a carton of stout. Alcohol companies target poorer ethnic minorities, such as the Indians in Malaysia, by offering special concerts or scholarship programmes for their children.99
High levels of alcohol consumption are strongly associated with difficulties in finding and gaining employment, or acquiring the necessary educational qualifications for employment. Family and social support networks are adversely affected by alcohol dependency. Alienation from these networks can exacerbate existing health problems. High levels of alcohol consumption (and other forms of substance abuse including smoking) can be seen as “a means of coping with social isolation and other effects of poverty.”100 Alcohol abuse and dependence can lead to scarce financial resources being diverted from essentials such as food and health care. Children raised in families of low socioeconomic status may be at increased risk of early onset drug and alcohol abuse.101
Weight and Diet
Obesity in the Pacific “is a serious epidemic”102 which is correlated with diseases such as diabetes and heart disease. Obesity is also increasing in Asian nations. Obesity affects all ages and social classes and in poorer populations it co-exists with under-nutrition.103 In some cultures there is resistance to perceiving obesity as a health issue due to the link between beauty, social status and large size.104 Higher education and socioeconomic status has been associated with lower risk of obesity (see Figure 12).105
In China, changing patterns of food consumption are leading to a rapid increase in the number of overweight people. According to Barry Popkin,

Noncommunicable Disease and Poverty
30Po
vert
y an
d N
CD
Ris
k Fa
ctor
s
“what took a century to happen in the West has taken a decade in China.” The increase in people obtaining 30% or more of their energy from fat is higher among lower income groups.106 Historically, obesity has been associated with wealth. However, while rates of obesity remain generally higher among more wealthy segments of the population, data from China shows that the rate of increase is greatest among the poorest. For example, in 1991, 51.4% of high income earners and 14.3% of those on a low income received 30% or more of their energy intake from fat. By 1997, the rates had increased to 54.6% of high income people (an increase of 3.2%) receiving 30% or more of their energy intake from fat, compared with 21.4% of low income people (an increase of 7.4%). In a six year period, the increase in prevalence of poor people receiving 30% or more of their energy intake from fat was more than double the increase of those on a high income. 107
Undernutrition is a double burden for poor people, as the poorest groups in society have high rates of both undernutrition and obesity.108 In Asian countries, between 3% and 15% of households have both an overweight and underweight person, usually an underweight child and an overweight adult. These households are most often among the urban poor.109
Obesity is traditionally associated more with urban than rural areas.110 This distribution is observed in both Asia and the Pacific, where obesity and consumption of imported foods seems to be “an urban phenomenon.”111 Obesity also appears to be correlated with ethnicity. “Populations differ in the level of risk associated with a particular waist circumference.”112 South Asians, for example, have high levels of abdominal obesity although they may not be considered obese by conventional BMI criteria. While Asian populations may be predisposed to abdominal obesity, Pacific Islander populations have lower levels of body fat than Europeans for the same BMI.113 The cause of these correlations between ethnicity and obesity may be genetic factors, diet, lifestyle, acculturation and body image.114 Increasing obesity rates in the region is expected to increase a number of obesity related NCDs, including CVD, cancer and Type 2 Diabetes.115
Figure 12: Prevalence of Obesity (BMI greater than 30) according to gender and socio-economic status, Valparaiso, Chile 1997
Source: Kain, J., Vio, F., Albal, C. Obesity Trends and Determinant Factors in Latin America. Cadernos de Saúde Pública, 2003, 19(suppl.1): 77-86.
30
25
20
15
10
5
0
% O
bese
Low Medium HighSocio-economic Status
Men
Women

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
31Po
vert
y an
d N
CD
Ris
k Fa
ctor
s
In the last fifty years, fat consumption has dramatically increased in many parts of Asia and the Pacific. With the trend of supplementing traditional foods with foreign foods that is associated with increased urbanisation, cooking methods have changed from “fat-free to fat assisted”. Imported and store-bought foods are convenient and low in cost. Cheap, high-fat foreign food is readily available in stores and is a major dietary component of the poor.116 For example, in Hong Kong SAR, 50% of Chinese with higher education reported buying western hot dogs at least once compared with 39% of those with lower education. However, 22% of people with lower education reported consuming hot dogs three to four times per week, while people with higher education usually only ate them once or twice a month.117 Imported foods are often consumed in addition to, and not instead of, local foods. According to Hughes, most Pacific people prefer locally produced food. However, social and economic barriers to access, especially among poorer people, force reliance on nutritionally inferior foreign foods. In Vanuatu, rural populations consume more calories, but they have a lower incidence of obesity. The proportion of total fat consumed from imported foods was 44.8% for urban populations, compared with 8.4% for rural populations. People are 2.2 times more likely to be obese and 2.4 times more likely to be diabetic if they consumed fat from imported foods rather than from traditional sources.118
Poorer people are often constrained in their food choices, because high-fat, low fibre foods are usually cheaper. As a result, people from low income groups are less likely to consume the healthy diets recommended by nutritionists.119 For example, a British National Food Survey shows that the diets of those from lower socioeconomic groups consisted primarily of “cheap energy” from meat products, full cream milks, fats, sugars, preserves, potatoes and cereals. This type of diet contained less essential nutrients than the diets of those from upper socioeconomic groups.120
In Australian studies, children with low socioeconomic status have been found to have approximately 20% higher skin-fold thickness than children from higher socioeconomic groups. Children with fathers having completed tertiary education also have a body mass index (BMI) of 16.6 compared with a BMI of 17.4 for those whose fathers had only primary education. Children whose mothers had only primary level education recorded higher diastolic and systolic blood pressure than children whose mother’s had university level education, and the level of mothers’ education had the greatest impact on the likelihood of children having risk factors for heart disease.121 The proportion of overweight children has been found to be 19.0% among households with low socioeconomic status, compared with 16.8% among households from other groups. Similarly, the proportion of obesity among children is 8.9% among households with low socioeconomic status, compared with 5.8% among households with higher socioeconomic status.122 Working-age adults

Noncommunicable Disease and Poverty
32Po
vert
y an
d N
CD
Ris
k Fa
ctor
s
with only primary education were around twice as likely as working-age adults with tertiary education to be obese. This relationship also holds for income. Adults on a weekly income of more than $1500 were 30-40% less likely to be obese than people on a weekly income of $0-$199.123
In developing nations, recent studies have shown that the probability of obesity for groups of low socioeconomic status exceeds the probability of obesity in groups of higher economic status once a nation’s per-capita income reaches US$ 2500. This study shows that obesity can no longer be considered solely a disease of higher SES groups in developing nations and that as Gross National Product (GNP) increases the burden of obesity tends to shift to groups of lower SES. The shift towards obesity among the poor appears to occur earlier among women than among men.124
Physical Activity
There is some general information regarding overall levels of physical fitness in China125 but information on this topic in the Western Pacific Region for poor populations is hard to find.
People living in poor, unsafe neighbourhoods who work long hours often find it extremely difficult to increase their levels of physical activity.126 “The aggressive and insecure environment that often characterises life in peri-urban areas prevents the poor population from engaging in systematic physical exercise [and people living in those areas] usually receive less information on the health and quality of life benefits of exercise.”127
Reduced physical activity and habitual inactivity accompany nutritional transition in people of all ages. Furthermore, modernization and industrialization lead to reduced physical activity in the work place and at home for both men and women. In the United States of America, less than 20% of adults now engage in regular exercise (see Figure 13). This trend is due to the shift from agriculture and manual labour to service industries and manufacturing and “office based” physically sedentary work. In developing nations, the reduction of physical activity occurs most prominently in areas where urbanization has been rapid.128
Figure 13: Physical Activity by Level of Education (USA 2001)
Source: Drewnowski, A. Poverty and Obesity presented at the Obesity and the Built Environment: Improving Public Health Through Community Design Conference, Washington DC, May 24-26 2004 http://www.niehs.nih.gov/drcpt/beoconf/postconf/drewnowski.pdf (last accessed 29th August 2005).
50403020100%
with
no
leisu
re
time a
ctivi
ty
Less than 12 years 12-16 16 years 12 years years
Education (years)

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
33Po
vert
y an
d N
CD
Ris
k Fa
ctor
s
In the United Kingdom, 60.9% of people with an annual income of below £33 480 were likely to be classified as sedentary as opposed to 39.5% of people with higher income. It is worth noting that while there is no standardized definition of poverty in the United Kingdom, the national income poverty line is most commonly considered to be household income of £6000 annually, approximately 60% of median income.129 Therefore, these levels of sedentary lifestyle by income relate not only to people in poverty, but also to those with a much higher income. People in the highest income bracket are much less likely to be sedentary). The findings were also related to education with 55% of people above certificate for higher secondary education (GCSE) level education sedentary, as opposed to 70% of people without GCSE level education. Sedentary lifestyles are also more prevalent with increasing age.130


The Need for Pro-poor Strategies in the Western Pacific Region: A Review
35
Selected NCDs in Poor Populations
Sele
cted
NC
Ds
in P
oor
Popu
latio
ns

Noncommunicable Disease and Poverty
36Se
lect
ed N
CD
s in
Poo
r Po
pula
tions
With a higher incidence of risk factors, the poor are also more likely to develop noncommunicable diseases. The following illustrates this for a selection of NCDs.
Cardiovascular Disease and Hypertension
In the United States of America, minority groups in poor neighbourhoods have significantly higher rates of mortality from CVD.131 CVD mortality rates for people earning more than $50 000 per year are less than one third of those in the lowest income groups. Similarly, CVD mortality rates among those with the lowest educational attainment are three times higher than rates among those with the highest educational attainment.132 In Canada, poverty contributes 3% to variation in mortality from cardiovascular disease and additional community characteristics such as high population density, immigrant and minority population status add a further 5%.133
Two thirds of CVD-related deaths globally occur in developing nations.134 Almost half of these deaths in developing countries in 1990 occurred among those below the age of 70 years, compared with just 22.8% of CVD deaths among those below that age in high-income industrial countries.135 For example, in Tatarstan (a republic of the Russian Federation), CVD mortality rates increased by more than 70% among men aged 35-39 between 1984 and 2002. Projections for developing nations expect an increase in ischemic heart disease mortality of 120% for women and 137% for men between 1990 and 2020, while in developed nations the increase is expected to be between 30% and 60%.136
In Singapore, the share of CVD as a cause of death has increased from 8.2% to 37.8% and in Fiji, it increased from 20.6% in 1970 to 36% in 1988. However, in the Republic of Korea, CVD declined by 0.9% between 1987 and 1996. Studies from China, India and Malaysia indicate that higher levels of education reduce the risk of developing NCDs. Benefits of higher education include reduced rates of smoking, healthier diets and healthier diets among children.137
Studies in African developing nations (Cameroon, Dar es Salaam and the United Republic of Tanzania) show elevated levels of high blood pressure among those living in urban as opposed to rural areas. Studies have shown similar results in the South-East Asia Region.138 Illiterate people in urban areas of Cameroon had a mean systolic blood pressure of 121 as opposed to 110 for university educated people.139 In the United States of America, a study of an urban and low income population showed that hypertension is related to age, education, income, race and church attendance.140 Adherence with medication treatment regimes for hypertension over 12 months is approximately 20% higher in skilled compared with

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
37
unskilled workers.141 In Japan, manual workers have 71% higher rates of hypertension than higher level professionals, and men with junior high school education have 68% higher rates of hypertension than men with a university education.142
Studies in Australia show that adults of low socioeconomic status have higher mortality rates from cardiovascular disease, higher rates of suspected heart attack, higher mortality from strokes and are more likely to have high blood pressure.143 For example, in 1983, the proportion of hypertensive men in manual occupations was 25%, as opposed to 15.6% for men in professional occupations.144 Men in manual occupations were at least 35% more likely to die from coronary heart disease and 60% more likely to die from strokes than men in professional occupations.
Diabetes
Studies in the United States of America have shown a link between poverty and diabetes. In 2003, prevalence of diabetes in the Hispanic population of Los Angeles was highest (17.2%) for those with annual incomes below the federally defined poverty line. This prevalence was higher than that for those from all socioeconomic groups who reported obesity (15.5%). The precise cause for this correlation was unclear, but it was presumed that living below the poverty line indicated greater risk of diabetes, or that a diagnosis of diabetes caused a decline in income.145
Risk of diabetes also increases with age, especially for people over age 40.146 Studies from Trinidad and Tobago show that diabetes is associated with indicators of low socioeconomic status and especially affects elderly people and women.147
Globally, there are more women than men with diabetes, particularly in developed countries.148 In the United States of America, women account for approximately 52% of all persons over age 20 with diabetes. In 2002, the socioeconomic status of women with diabetes was shown to be markedly lower than that of women without diabetes. Women with diabetes were more likely than women without diabetes to be more than 45 years old, non-white, divorced, separated or widowed, living alone, retired or unable to work. Women with diabetes are also more likely to have lower levels of education and twice as likely to have an annual household income under $25 000. Higher levels of education equate to better decision-making, and higher levels of income improve access to health care and better living standards, both of which translate into health benefits. Low socioeconomic status compromise the ability of women to benefit from treatments that reduce complications and risk of death.149
Sele
cted
NC
Ds
in P
oor
Popu
latio
ns
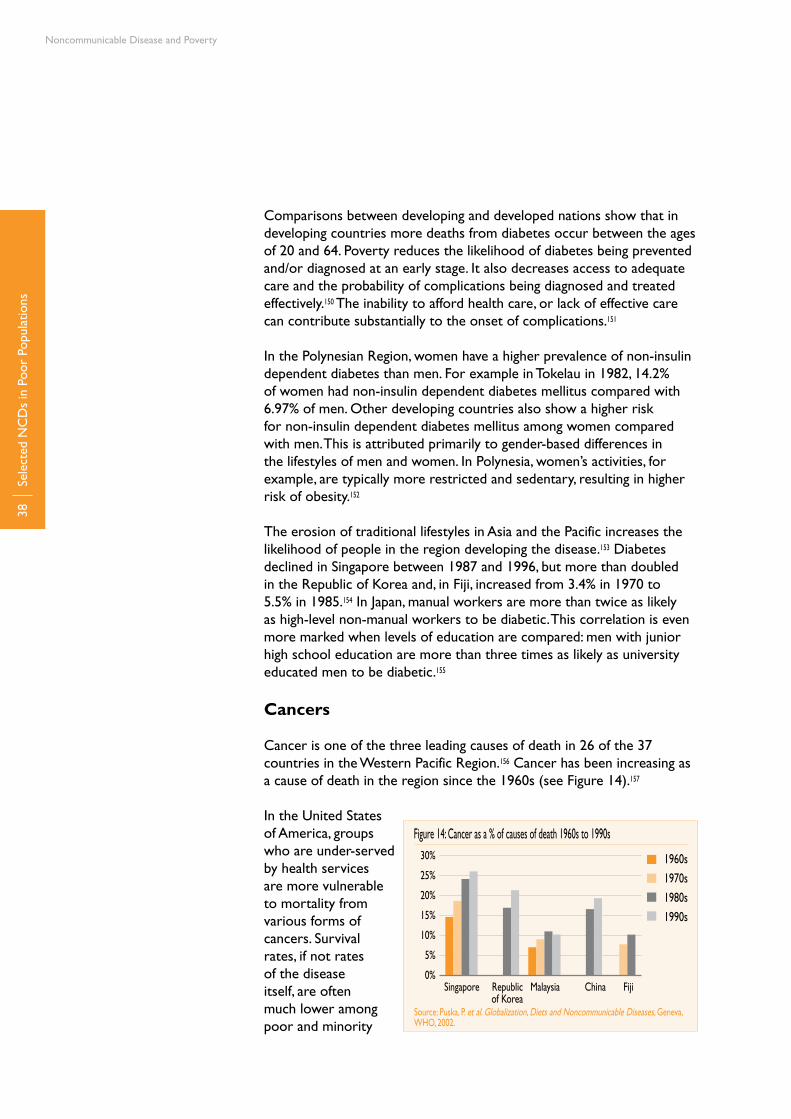
Noncommunicable Disease and Poverty
38
Comparisons between developing and developed nations show that in developing countries more deaths from diabetes occur between the ages of 20 and 64. Poverty reduces the likelihood of diabetes being prevented and/or diagnosed at an early stage. It also decreases access to adequate care and the probability of complications being diagnosed and treated effectively.150 The inability to afford health care, or lack of effective care can contribute substantially to the onset of complications.151
In the Polynesian Region, women have a higher prevalence of non-insulin dependent diabetes than men. For example in Tokelau in 1982, 14.2% of women had non-insulin dependent diabetes mellitus compared with 6.97% of men. Other developing countries also show a higher risk for non-insulin dependent diabetes mellitus among women compared with men. This is attributed primarily to gender-based differences in the lifestyles of men and women. In Polynesia, women’s activities, for example, are typically more restricted and sedentary, resulting in higher risk of obesity.152
The erosion of traditional lifestyles in Asia and the Pacific increases the likelihood of people in the region developing the disease.153 Diabetes declined in Singapore between 1987 and 1996, but more than doubled in the Republic of Korea and, in Fiji, increased from 3.4% in 1970 to 5.5% in 1985.154 In Japan, manual workers are more than twice as likely as high-level non-manual workers to be diabetic. This correlation is even more marked when levels of education are compared: men with junior high school education are more than three times as likely as university educated men to be diabetic.155
Cancers
Cancer is one of the three leading causes of death in 26 of the 37 countries in the Western Pacific Region.156 Cancer has been increasing as a cause of death in the region since the 1960s (see Figure 14).157
In the United States of America, groups who are under-served by health services are more vulnerable to mortality from various forms of cancers. Survival rates, if not rates of the disease itself, are often much lower among poor and minority
Sele
cted
NC
Ds
in P
oor
Popu
latio
ns
Figure 14: Cancer as a % of causes of death 1960s to 1990s
Source: Puska, P. et al. Globalization, Diets and Noncommunicable Diseases, Geneva, WHO, 2002.
30%
25%
20%
15%
10%
5%
0%Singapore Republic Malaysia China Fiji of Korea
1960s
1970s
1980s
1990s
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
39
groups. These findings are explained by such factors as low rates of health insurance among the poor, limited access to high quality care, geographical and/or cultural isolation, limited education and linguistic differences limiting the ability to read and/or understand preventive information.158 The director of the United States of America National Cancer Institute (NCI) declared in 1991, “poverty is a carcinogen.” The total cancer incidence attributable to poverty among the white American population in the United States of America (as measured in terms of a family income of less than $15 000) is 16.5%.159
In Australia, analyses of tracheal, bronchus and lung cancers show that manual labourers have almost twice the mortality rate of professionals.160 After taking into account age differences, professionals have 5% lower, and tradesmen and labourers 19% higher, than average rates of mortality from respiratory cancer.161
As rates of tobacco smoking increase in developing nations in the Region, there is potential for dramatic increases in smoking-related cancer. Projections suggest that 70% of the estimated 10 million smoking-attributable deaths expected in 2030 will take place in low-income nations.162
Poverty can reduce the probability of early diagnosis of cancer. In developed nations, 80% of patients with breast, cervix or mouth cancer are diagnosed at an early stage compared to only 20% in developing nations. As a result, most cancer patients in developing nations come to seek care only when they are already incurable. This tendency is due to factors such as inability to afford primary care, low levels of education reducing awareness of symptoms, poor access to health services and inappropriate balance between primary and prevention and acute treatment services.163
Respiratory Diseases and COPD
The burden of COPD in the Western Pacific Region is three times higher than the global average. Lung disorders have been linked with low socioeconomic status in numerous studies. COPD accounted for 12% of total deaths in the Western Pacific Region in 1998. Most of these deaths occurred in rural areas with poor living conditions and inadequate health services.164
Studies on COPD by the US Centers for Disease Control and Prevention show that adults living below the poverty line are about 75% more likely to report COPD than those with incomes 200% or more above the national poverty line. While women were 60% more likely to self-report COPD, when obstructive lung disease is objectively measured by lung capacity, men have higher prevalence.165 Australian studies show that working-age men of low socioeconomic status have 203% higher death
Sele
cted
NC
Ds
in P
oor
Popu
latio
ns

Noncommunicable Disease and Poverty
40
rates from bronchitis, emphysema and asthma than working-age men in the higher income quintile. In other words, working-age men in Australia in the lowest income prestige group are 2.03 times as likely to die from these conditions as men in the highest occupational prestige group.166
Sele
cted
NC
Ds
in P
oor
Popu
latio
ns
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
41
Seeking Treatment and Treatment Programmes
Seek
ing
Trea
tmen
t an
d Tr
eatm
ent
Prog
ram
mes
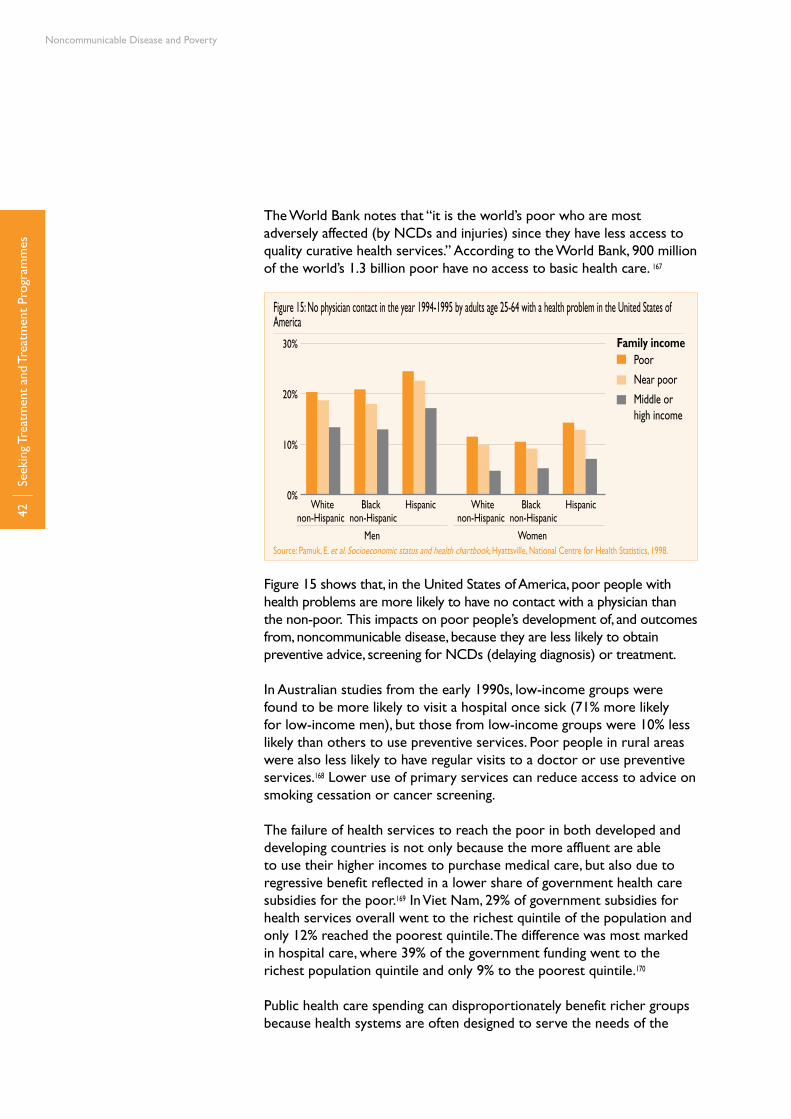
Noncommunicable Disease and Poverty
42Se
ekin
g Tr
eatm
ent
and
Trea
tmen
t Pr
ogra
mm
es
The World Bank notes that “it is the world’s poor who are most adversely affected (by NCDs and injuries) since they have less access to quality curative health services.” According to the World Bank, 900 million of the world’s 1.3 billion poor have no access to basic health care. 167
Figure 15 shows that, in the United States of America, poor people with health problems are more likely to have no contact with a physician than the non-poor. This impacts on poor people’s development of, and outcomes from, noncommunicable disease, because they are less likely to obtain preventive advice, screening for NCDs (delaying diagnosis) or treatment.
In Australian studies from the early 1990s, low-income groups were found to be more likely to visit a hospital once sick (71% more likely for low-income men), but those from low-income groups were 10% less likely than others to use preventive services. Poor people in rural areas were also less likely to have regular visits to a doctor or use preventive services.168 Lower use of primary services can reduce access to advice on smoking cessation or cancer screening.
The failure of health services to reach the poor in both developed and developing countries is not only because the more affluent are able to use their higher incomes to purchase medical care, but also due to regressive benefit reflected in a lower share of government health care subsidies for the poor.169 In Viet Nam, 29% of government subsidies for health services overall went to the richest quintile of the population and only 12% reached the poorest quintile. The difference was most marked in hospital care, where 39% of the government funding went to the richest population quintile and only 9% to the poorest quintile.170
Public health care spending can disproportionately benefit richer groups because health systems are often designed to serve the needs of the
Poor
Near poor
Middle or high income
White Black Hispanicnon-Hispanic non-Hispanic
Men
30%
20%
10%
0%
Women
Family income
Figure 15: No physician contact in the year 1994-1995 by adults age 25-64 with a health problem in the United States of America
Source: Pamuk, E. et al. Socioeconomic status and health chartbook, Hyattsville, National Centre for Health Statistics, 1998.
White Black Hispanicnon-Hispanic non-Hispanic
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
43Se
ekin
g Tr
eatm
ent
and
Trea
tmen
t Pr
ogra
mm
es
wealthy rather than the poor.171 Health services themselves are often located in more affluent areas.172 Since services are usually scarcer in areas where poor people live, the poor may be forced to travel relatively long distances in order to obtain care. Poor roads and high transport costs make this expensive, time-consuming and difficult. Particularly for people living in rural areas, difficulties in accessing health services are a cause of stress due to the lack of local facilities.173 In Indonesia, the poor must travel 50% further than the non-poor to obtain access to a modern medical care provider.174 Health “visitors” (health professionals who volunteer to service areas with low availability of health services) devote a large proportion of their time to poorer patients, but are still unable to compensate for the large differences in demand between poor and non-poor patient caseloads.175
Reaching the extremely poor may require a disproportionately high level of resources. This is a key resource mobilization and allocation challenge, which is difficult to resolve in the absence of adequate resources and competing demands.176
The traditional focus on acute treatment for NCD conditions is a reactive response and is ineffective in minimising the growth of NCD conditions, particularly for the poor who are often unable to afford or obtain preventative medical care and have limited ability to afford acute care at later stages of disease progression (see below). The Innovative Care for Chronic Conditions (ICCC) framework demonstrates a multi-faceted, multi-level approach to improving outcomes for people with chronic conditions and provides a focus on prevention as well as treatment. The ICCC aims to improve health care at the macro, policy level, the meso level of the health care organisation and the community, and the micro level of patient interaction.177
The Emphasis on Personal Responsibility for Health
Studies of heart disease in Canada show that the disadvantaged are often blamed for smoking, physical inactivity or poor diet as contributing to their morbidities. However, this attitude does not adequately recognize that income differences can contribute to cardiovascular disease independently of risk behaviours.178 Unhealthy lifestyle choices related to NCDs such as smoking and high alcohol consumption are often a response and/or a coping mechanism for the stresses and challenges poor people face in their everyday lives.179 There may also be structural reasons for poor people being at greater risk for NCDs. For example, in Australia, people of the lowest socioeconomic status have 2.5 times the exposure to fast food restaurants than their wealthiest counterparts. In Melbourne, in the lowest income area, there was one fast food outlet per 5641 people, as opposed to one per 14 256 people in the highest income area.180
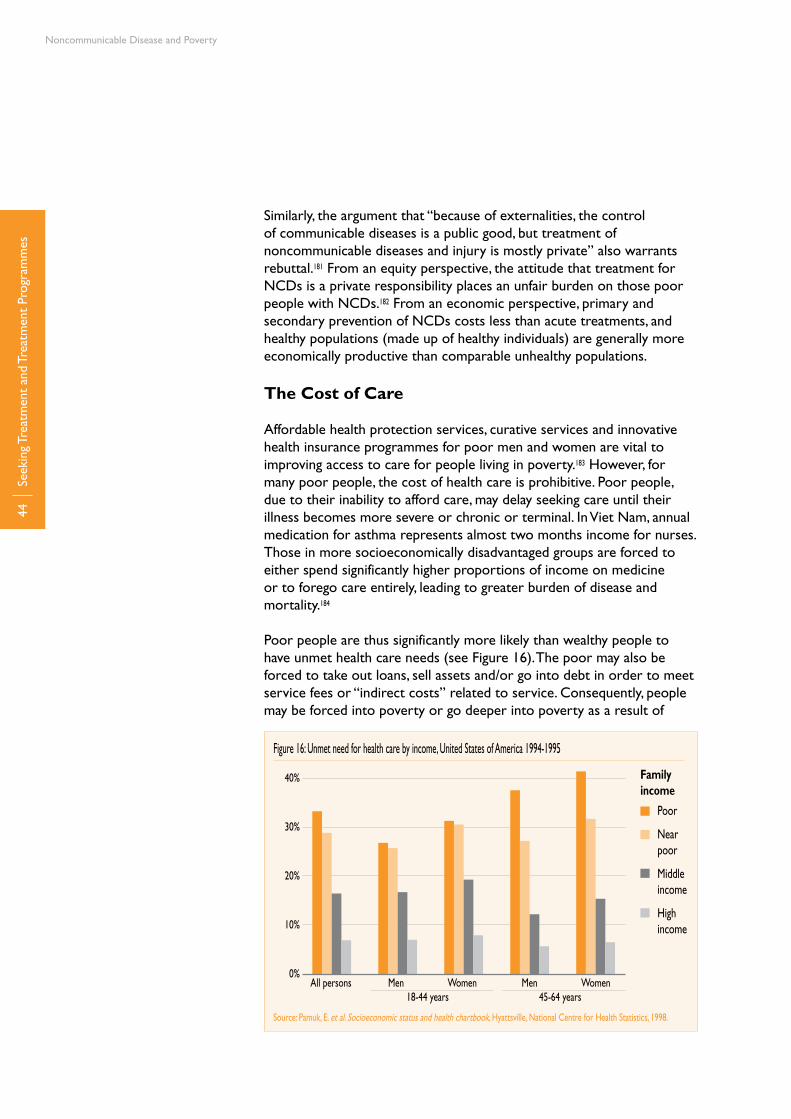
Noncommunicable Disease and Poverty
44Se
ekin
g Tr
eatm
ent
and
Trea
tmen
t Pr
ogra
mm
es
Similarly, the argument that “because of externalities, the control of communicable diseases is a public good, but treatment of noncommunicable diseases and injury is mostly private” also warrants rebuttal.181 From an equity perspective, the attitude that treatment for NCDs is a private responsibility places an unfair burden on those poor people with NCDs.182 From an economic perspective, primary and secondary prevention of NCDs costs less than acute treatments, and healthy populations (made up of healthy individuals) are generally more economically productive than comparable unhealthy populations.
The Cost of Care
Affordable health protection services, curative services and innovative health insurance programmes for poor men and women are vital to improving access to care for people living in poverty.183 However, for many poor people, the cost of health care is prohibitive. Poor people, due to their inability to afford care, may delay seeking care until their illness becomes more severe or chronic or terminal. In Viet Nam, annual medication for asthma represents almost two months income for nurses. Those in more socioeconomically disadvantaged groups are forced to either spend significantly higher proportions of income on medicine or to forego care entirely, leading to greater burden of disease and mortality.184
Poor people are thus significantly more likely than wealthy people to have unmet health care needs (see Figure 16). The poor may also be forced to take out loans, sell assets and/or go into debt in order to meet service fees or “indirect costs” related to service. Consequently, people may be forced into poverty or go deeper into poverty as a result of
Figure 16: Unmet need for health care by income, United States of America 1994-1995
Source: Pamuk, E. et al. Socioeconomic status and health chartbook, Hyattsville, National Centre for Health Statistics, 1998.
40%
30%
20%
10%
0%All persons Men Women Men Women
Poor
Near poor
Middle income
High income
18-44 years 45-64 years
Family income

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
45Se
ekin
g Tr
eatm
ent
and
Trea
tmen
t Pr
ogra
mm
es
becoming ill.185 Studies of the effects of health care costs in rural areas in China have shown that the average cost of a one-time hospital visit can be well over the annual income of a poor peasant, that other health care expenses consumed 10%-15% of household income and that 80% of poor people needing hospitalisation did not obtain it because of the expense.186
Studies from Latin America show that potentially effective interventions for existing NCDs are not producing adequate results, due to the high cost of care. For example effective anti-hypertensive treatments, which can cost US$ 100 per month, are out of reach for people on an average monthly income in the range of US$ 50-200. More than half of Jamaicans with cancer and diabetes became medically indigent187 given the high proportion of costs that required direct payment from patients. Up to 50% forego treatment due to the inability to pay.188 This study also showed that 70% of care foregone was because of inability to afford treatment and medication.189 Poor people often lack health insurance, which dramatically reduces their ability to afford care, particularly high cost treatments for NCDs. In the United States of America, health insurance coverage is significantly greater among the wealthiest income quintile than among the poorest (see Figure 17).
In Viet Nam, approximately 70% of those in the poorest income quintile self-medicate as opposed to 55% in the wealthiest quintile (see Figure 18). Those in the poorest quintile bypass professional diagnosis and treatment in favour of self-diagnosis and treatment. This may have an impact on the use of preventive services and accurate diagnosis and treatment. Data from Indonesia (and there are similar patterns in studies from Viet Nam) shows that the poorest income group make 0.14 health care visits per month, compared with 0.31 visits per month
Figure 17: No health insurance coverage among persons age 25-64 in the United States of America 1994-1995
Source: Pamuk, E. et al. Socioeconomic status and health chartbook, Hyattsville, National Centre for Health Statistics, 1998.
60%
50%
40%
30%
20%
10%
0%
Poor
Near poor
Middle income
High income
Family income
White Black Hispanicnon-Hispanic non-Hispanic
Men Women
White Black Hispanicnon-Hispanic non-Hispanic

Noncommunicable Disease and Poverty
46Se
ekin
g Tr
eatm
ent
and
Trea
tmen
t Pr
ogra
mm
es
by the richest group.190 It has been estimated that only 2% of people with disabilities in developing countries have access to rehabilitation and appropriate basic services.191
When poor people delay diagnosis or seeking treatment of a condition such as cancer, they may find it impossible to obtain health insurance because people with high medical care costs may be denied coverage directly or effectively by being charged premiums which are equal to the actual cost of care and administrative costs. These charges “may be prohibitively expensive, leaving these individuals effectively uninsured.”192
Poverty and Inferior Treatment Services
Poor patients, in both developed and developing countries generally receive poorer quality care. Studies from the United States of America on the relationship between poverty and breast cancer show that women receiving Medicaid assistance, which is available only to people living below the poverty line, are 41% more likely to be diagnosed with late-stage breast cancer, 44% less likely to receive radiation after breast-conserving surgery, and more than three times more likely to die than women not insured by Medicaid (i.e., those over the poverty line).193 Similarly, studies in the United Kingdom show that people in the lowest socioeconomic groups have about three week longer waiting times for cardiac surgery than those in the highest socioeconomic groups. Disadvantaged patients are also about half as likely to have their surgery classified as urgent. Despite poor patients being more likely to develop cardiovascular disease (see chapter Poverty and NCD Risk Factors), they are less likely to be investigated or offered surgery once it has developed.194 In Scotland, socioeconomically disadvantaged patients were found to be 44% more likely to develop heart failure, but 23% less likely to see their general practitioner on an ongoing basis than the most affluent group.195 In a study of health among poor people in Yemen, half of the focus groups reported discrimination by health care workers according to ability to pay for services and social status.196
Language difficulties can also create barriers for people from different ethnic groups, and people may also be subjected to institutionalised racism, which can lead to limited access to information and services.197 Lack of interpreters and stereotypical views about ethnic groups
Figure 18: Service utilization by income quintile in Viet Nam 1993
Source: Peabody, J. W. et al. Policy and Health- implications for development in Asia, Cambridge University Press, New York 1999.
100%
80%
60%
40%
20%
0%
% us
e of f
ciliti
es
Poorest II III IV Wealthiest
Household income per capita income quintile
Private pharmacy
Private providers
Public providers

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
47Se
ekin
g Tr
eatm
ent
and
Trea
tmen
t Pr
ogra
mm
es
may affect people’s access to preventive and treatment services.198 For example, a study from the United Kingdom showed that 46% of white patients visiting their doctor for routine examinations received mammography as opposed to only 20% of other ethnic groups. Vietnamese and Chinese patients in the study were half as likely as Caucasian patients to have regular blood pressure checks.199
Doctors and health service providers often tend to be less effective at communicating with people with low levels of education. A study of diabetes care and treatment in the United States of America showed less effective dissemination on symptoms, test results, treatments and prognosis to people of poor education. Furthermore, health service providers are more likely to adopt a “directive approach” with less educated patients, who are therefore less likely to have their expectations met. This factor has been shown to influence poor outcomes from diabetes among people with low levels of education.200
Demands for unofficial “fees” or “gifts” in return for ordinary services from health staff are commonly reported experiences by poor people seeking care.201 Explicit co-payment systems can reduce “under the table” patient payments while increasing the transparency of the system can address indirect costs.202 NGOs are often appreciated where they exist, but poor people may not always perceive NGOs as empowering or accountable to them. As a result, poor people may primarily rely on their own informal networks of family, kin and friends for financial support.203
Changes in the timing and staffing of services, including training or employing staff with language and cultural-anthropological skills, can enable them to fit in with culturally acceptable practices and overcome communication barriers.204
Box 3: NCD Management in Resource Poor Areas of South Africa
In South Africa, an NCD disease management program designed for resource-poor areas focused on enabling nurses to provisionally diagnose patients with NCDs, decide on the initial management, to alter treatment in non-complex cases and to identify patients requiring referral to hospital. Each patient was seen by a doctor at a primary care clinic for confirmation of diagnosis and detection of complications. Treatment focused on the use of essential drugs, health education on the importance of long term management of the condition, simplifying the treatment and involving the patient in agreeing to an acceptable drug regimen. A hospital clinic, mobile clinics and village clinics were utilised as the base contact point for people seeking treatment. A focus on providing management in local clinics was of particular benefit to the rural poor. Adherence of patients to treatment regimes increased by almost 10% over a two year period. Control of Hypertension, NIDDM and Asthma was achieved in between 80 and 95% of cases.
Source: Coleman, R., Gill, G., Wilkinson, D. Noncommunicable disease management in resource-poor settings: A primary care model from rural South Africa. Bulletin of the World Health Organization 1998, 76(6):633-640.
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
49
The Cycle of Poverty and Ill-health
The
Cyc
le o
f Pov
erty
and
Ill-h
ealth

Noncommunicable Disease and Poverty
50T
he C
ycle
of P
over
ty a
nd Il
l-hea
lth
In the case of both communicable and NCDs poverty and ill-health form a vicious cycle. Poverty leads to ill-health which in turn creates greater poverty. By mutually reinforcing each other, poverty and disability can lead to increased vulnerability and exclusion (see Figure 19).
High levels of expenditure on health can have major impacts on households. The coping mechanisms of poor households faced with increasing health costs are varied. They may divert expenditure away from other vital areas such as food and education, which in turn reduces the level of the health of a population.205 Families may go without adequate food when money is required to buy medicine or obtain treatment. Increased household borrowing and higher debt shift spending from expenses such as education and cause delay, reduction or avoidance in seeking health care.206 In addition, “distress sales” are made to meet the costs of health care. In some rural areas of Viet Nam, families sell their buffalo to meet health costs.207 Sales such as this have a major negative impact of future livelihoods and earning capacity.208
The poor often dread sickness the most, as it can result in loss of income and increased debt.209 Sickness of primary income earners may be especially difficult for poor people. Food and income ceases, and payment for treatment brings further impoverishment. This downward spiral of poverty and ill-health results in malnutrition from scarce food and children being withdrawn from school and sent to work. Surveys of poor
POVERTYEconomic deprivationLow educationUnemployment
NCDsHigher prevalenceLack of careMore severe disease
ECONOMIC IMPACTIncreased health expenditureLoss of jobReduced productivity
Figure 19: The Cycle of Poverty and NCDs
Source: Adapted from Srinivasa Murthy, R. et al. World Health Report 2001 WHO; Geneva 2001.

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
51T
he C
ycle
of P
over
ty a
nd Il
l-hea
lth
people have shown that illness ranks highly as a cause of destitution, being the most frequently mentioned of 15 causes of a downward slide into poverty. Ill-health was mentioned even more frequently than loss of employment as a cause of poverty.210
There are also indications that the increasing reliance by Western Pacific Region nations on user fees and out-of-pocket payments for health care may increase poverty and decrease the equitable distribution of health care, especially if national health funding is reduced. Although health insurance can provide some protection for the poor in terms of their ability to meet health costs, this protection is “sometimes marginal and rarely more than modest,”211 since families must still pay the insurance premiums as well as co-payments for services covered and full payments for services not covered.212

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
53N
CD
Out
com
es fo
r th
e Po
or
NCD Outcomes for the Poor
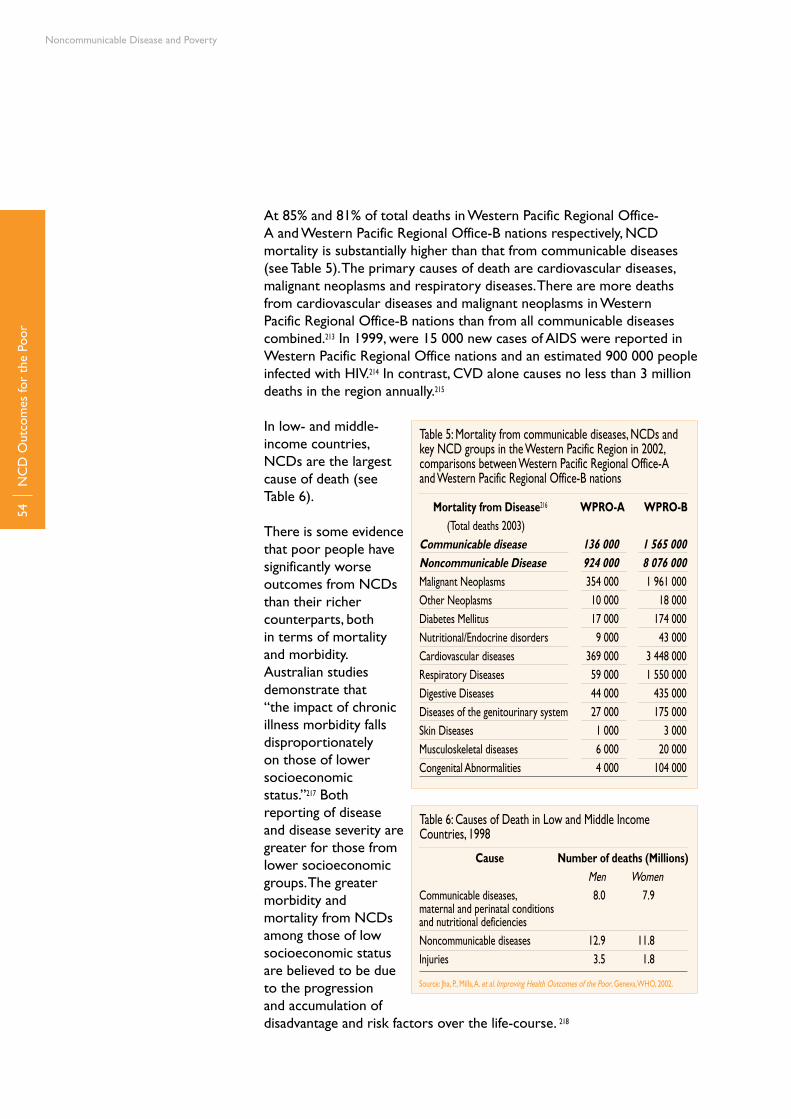
Noncommunicable Disease and Poverty
54N
CD
Out
com
es fo
r th
e Po
or
At 85% and 81% of total deaths in Western Pacific Regional Office-A and Western Pacific Regional Office-B nations respectively, NCD mortality is substantially higher than that from communicable diseases (see Table 5). The primary causes of death are cardiovascular diseases, malignant neoplasms and respiratory diseases. There are more deaths from cardiovascular diseases and malignant neoplasms in Western Pacific Regional Office-B nations than from all communicable diseases combined.213 In 1999, were 15 000 new cases of AIDS were reported in Western Pacific Regional Office nations and an estimated 900 000 people infected with HIV.214 In contrast, CVD alone causes no less than 3 million deaths in the region annually.215
In low- and middle-income countries, NCDs are the largest cause of death (see Table 6).
There is some evidence that poor people have significantly worse outcomes from NCDs than their richer counterparts, both in terms of mortality and morbidity. Australian studies demonstrate that “the impact of chronic illness morbidity falls disproportionately on those of lower socioeconomic status.”217 Both reporting of disease and disease severity are greater for those from lower socioeconomic groups. The greater morbidity and mortality from NCDs among those of low socioeconomic status are believed to be due to the progression and accumulation of disadvantage and risk factors over the life-course. 218
Table 5: Mortality from communicable diseases, NCDs and key NCD groups in the Western Pacific Region in 2002, comparisons between Western Pacific Regional Office-A and Western Pacific Regional Office-B nations
Mortality from Disease216 WPRO-A WPRO-B (Total deaths 2003) Communicable disease 136 000 1 565 000Noncommunicable Disease 924 000 8 076 000Malignant Neoplasms 354 000 1 961 000Other Neoplasms 10 000 18 000Diabetes Mellitus 17 000 174 000Nutritional/Endocrine disorders 9 000 43 000Cardiovascular diseases 369 000 3 448 000Respiratory Diseases 59 000 1 550 000Digestive Diseases 44 000 435 000Diseases of the genitourinary system 27 000 175 000Skin Diseases 1 000 3 000Musculoskeletal diseases 6 000 20 000Congenital Abnormalities 4 000 104 000
Table 6: Causes of Death in Low and Middle Income Countries, 1998
Cause Number of deaths (Millions) Men WomenCommunicable diseases, 8.0 7.9 maternal and perinatal conditions and nutritional deficienciesNoncommunicable diseases 12.9 11.8Injuries 3.5 1.8
Source: Jha, P., Mills, A. et al. Improving Health Outcomes of the Poor, Geneva, WHO, 2002.
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
55
People from low socioeconomic groups in Australia were found to be significantly more likely than their richer counterparts to die from respiratory illness, lung cancer, ischaemic heart disease and diabetes. Specifically, compared to the highest income group, men from low-income groups were 55% more likely to die from lung cancer, 102% more likely to die from cerebrovascular disease and 74% more likely to die from diabetes. Women from low-income groups were 211% more likely to die from diabetes and 53% more likely to die from lung cancer. Men from low income groups were 54% and women 124% more likely to die from ischaemic heart disease.219
The Australian Burden of Disease and Injury study found that “the excess mortality burden associated with socioeconomic disadvantage is particularly high for diabetes, chronic respiratory diseases, [injuries] and acute respiratory conditions (in males).”220 Death rates from heart disease are nearly twice as high in people living in the most disadvantaged areas of Australia as compared with those who live in areas of least disadvantage. Between 1985 and 1995, the differential in death rates between most well-off and most disadvantaged areas increased for respiratory system diseases, circulatory system diseases and lung cancer. In Australia, coronary heart disease in 1996 was 30% higher for men and 21% higher for women who live outside capital cities. This gap had widened significantly since 1986. Indigenous people in Australia are particularly vulnerable to CVD, diabetes and end-stage renal disease, with rates very significantly higher than averages for the population.221
Later diagnosis and/or poor diagnosis means chronic conditions and complications are more likely to develop. For example, greater rates of deaths from cancer among poor peoples and minority groups in the United States of America can at least partially be explained by late diagnosis and poor access to health care.222 Lack of treatment/medicine means that the poor are more likely to die from, or suffer, long-term from chronic illness.223
Studies in the United States of America have found that:• Heartdiseasemortalityis2.5to3timesgreateramongpeopleon
annual incomes of less than $10 000 compared with those on an income of more than $15 000.
• Menage25-64onanincomeof$10000orlessperyearsuffera mortality rate from lung cancer 2.4 greater than those on an income of more than $25 000.
• Womenonafamilyincomeoflessthan$15000suffera40%-60%greater mortality rate from lung cancer than those earning more than $15 000.
• Womenonanincomeoflessthan$10000annuallyarethreetimes more likely to die from diabetes than women with an
NC
D O
utco
mes
for
the
Poor

Noncommunicable Disease and Poverty
56
income of more than $25 000.• Formenthelowestincomegroupwas2.6timesmorelikelytodie
from diabetes than the highest income group.224
In the words of Ghaffar, et al., “as the rich are likely to recognize their risk earlier and seek medical attention, they will develop chronic but manageable disease; as the poor are likely to be less aware of their risk and less able to access medical care, they will develop rapidly progressive disease with early and sudden fatal outcomes.”225 In summary, the poor tend to be more disadvantaged, carry a heavier burden and have greater barriers and poorer outcomes than those who are more advantaged. Table 7 summarizes this progression among the poor.
NC
D O
utco
mes
for
the
Poor
Table 7: Progression of NCDs: stages, barriers and outcomes for poor people
Table developed by the author as a summary of the findings from the literature.
Progression of NCD
Stage
Prevention
Risk
Develop NCD
Seek Health Care
Treatment
Final Outcome
Barrier for Poor People
Low education, low access to health care and therefore less ability to be informed of preventive information
Greater risk taking activity, e.g., higher smoking rates, greater consumption of alcohol, unhealthy diet
Greater likelihood of developing disease
Delayed care seeking due to inability to afford treatment, geographical barriers, inability to recognise symptoms
High cost medicines, high cost tertiary care, discrimination, poor quality of care
Early mortality or chronic illness affect-ing livelihood
Outcome
Increased likelihood of risk taking activity
Increased likelihood of developing NCD
Pain and suffering, reduced income
Diagnosis comes when disease is incurable
Inadequate treatment, income diverted to treatment, food supply reduced, edu-cation reduced, other family members become ill
Loss of wage earner, productive years reduced, increased pain and suffering
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
57Ju
stify
ing
a Fo
cus
on t
he P
oor
Justifying a Focus on the Poor

Noncommunicable Disease and Poverty
58Ju
stify
ing
a Fo
cus
on t
he P
oor
Efficiency
It has been argued in relation to communicable diseases that “It is not possible to make an impact on the health status of the population… without addressing the areas and the populace where most of the disease burden exists. Also, addressing the major causes of morbidity and mortality among the poor… is the most cost effective solution giving the maximum and the most rapid return on health investments.”226 This argument also holds true for addressing NCDs.
Since the poor face a higher NCD burden than the rich and more severe barriers to access, the success of NCD-control programmes may be jeopardized if the situation of the poor and their needs are not taken into account. Moreover, NCD programmes that are better tailored to the needs of the poor are more likely to be successful for NCD control than those that are “neutral” or focus on the better off.
In the Organization for Economic Co-operation and Development (OECD) nations people of lower SES often use health services more than the wealthy, particularly acute care facilities when disease conditions have progressed. In developing countries the inability and/or failure of health services to reach the poor is the major cause of inequalities in health outcomes. Thus, improvements in health outcomes for people in poverty in developing nations is a matter of improving access to health knowledge and services.227
Specifically targeting interventions to the poor improves the health of the whole population, due to high disease burden and mortality among these groups. It can also constitute more efficient use of limited available resources and result in a greater health impact for the same expenditure. Studies of pro-poor targeted programmes relating to provision of health care clinics and food subsidies in Latin America show that the share of programme benefits accruing to the lowest two income groups range from 59%-83%.228 An initiative in Lodz, Poland designed to improve primary health care for homeless men presenting at shelters, typically with conditions including alcoholism, coronary disease and high blood pressure, provided considerable savings in terms of avoiding hospital admissions. This initiative was shown to not only improve the health of the homeless directly, but also improve general public health “reducing one of the factors that make people poor.”229
From an economic development perspective, improving the health status of the poor increases their productivity and income thereby benefiting all society. Assets which would be diverted by the poor to medical care can be saved and invested in the welfare of the household. The human and social capital of the nation can be increased by preventing NCDs and expenditure on prevention will
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
59
off-set the alternative need for treatment in the acute care and hospital sector.230
Equity
As discussed above, there is evidence of significant poor-rich gaps in NCD risk, prevalence and outcomes. Age-specific death rates for almost all causes, whether communicable or noncommunicable diseases, are higher for the poor than for the rich.231 The rich-poor differences in NCD risk, prevalence and outcomes may be due to structural factors more than to personal decisions, and are thus unfair. Equity requires that NCD policies should address this poor-rich gap and be tailored to the needs of the poor as well as the non-poor.
In the case of developing countries it has been argued that the causes of health inequalities are different from those of developed countries. In high income countries, where there is commonly universal access to health care, inequalities tend to be directly related to income and other socioeconomic factors. In developing countries, improved health among the wealthier groups, particularly in urban areas, tends to be related to better access for these groups to improved health care knowledge and services rather than income level per se.232
Out-of pocket payments account for more than a third of total health expenditure in most developing countries in the region. Low income families spend a higher percentage of their income on health than richer households. This is exacerbated when access to health services is diminished and there is no social protection mechanism against increasing health care costs. User fees thereby affect the livelihood of low income people, and can lead them to total exclusion and poverty. In addition, a lack of appropriate policy and regulation to guide health care financing has led to erosions in the equity, quality and efficiency of health care systems.233
The fact that the high costs of health care contribute to keeping people in poverty is increasingly seen as an issue of social justice. Income losses due to poor health “are involuntary and simply the consequence of unwanted health ‘shocks’.”234 Health costs are categorized differently from other items of household expenditure, and the community as a whole, especially those more able to afford and absorb the impact of such shocks, has a responsibility to share this financial burden, rather than allowing it to disproportionately fall on those least able to afford them. Equitable health expenditure mechanisms avoid placing additional burdens on poor households in the form of catastrophic out of pocket expenses. Payment for health care should not only be proportionate to levels of household income, but a fair proportion should be applied to those on low incomes.235
Just
ifyin
g a
Focu
s on
the
Poo
r

Noncommunicable Disease and Poverty
60
Human Rights
In the World Health Organization’s constitution, health is defined as a fundamental human right, regardless of race, religion, political belief or economic and social condition. This right is also, though less forcefully, proclaimed by the Universal Declaration of Human Rights. These binding international human rights instruments236 require that health outcomes for all sections of society are not unduly influenced by conditions beyond the control of individuals.
Just
ifyin
g a
Focu
s on
the
Poo
r

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
61C
oncl
usio
ns
Conclusions

Noncommunicable Disease and Poverty
62C
oncl
usio
ns
There is a limited literature specifically on poverty and NCDs in the Western Pacific Region and very little disaggregated data on the prevalence of NCD risk factors and the incidence of NCDs among the poor in the Region. The literature available on links between poverty and disease is primarily related to communicable disease. Most information on the topic of NCDs and poverty relate to areas other than the Western Pacific, and primarily come from developed nations such as the United States of America and Western Europe, although the Pan American Health Organization is currently developing a significant body of literature on the topic.
The literature that is available shows that the burden of NCDs in the region is high and increasing. Furthermore, all the major risk factors for NCDs have established links with poverty. Despite limited actual data, there is agreement in the literature that poverty and NCDs are strongly correlated. The literature also indicates that risk factors for NCDs are significantly greater among the poor than among the wealthy. As a result, the poor are particularly susceptible to CVD, respiratory illness, diabetes and cancers.
The extent to which the literature cited supports hypotheses concerning the relationship between poverty and NCDs is summarised below (see Table 8). The summary is based on sources cited for the conduct of this review, which represents a partial sample of literature available on poverty and noncommunicable disease. Gaps in the literature are also identified.
Initiatives such as the North Karelia Project in Finland have proven effective in reducing rates of NCDs across socioeconomic lines. Effective pro-poor interventions for NCDs need to be multi-dimensional and involve global, national, local, public and private initiatives including elements outside the health sector. Interventions must be targeted, monitored regularly to ensure that objectives are met, and sustained over long periods. Pro-poor health systems should combine both formal, technical mechanisms and informal community or family based structures; be accessible in terms of both location and information, be affordable (with equitable financing mechanisms); and be sustained over the long term.237 The literature favours prevention rather than treatment as the focus for interventions both from a social equity perspective and as a cost-effective measure.
People living in relative poverty in the Western Pacific Region have limited ability to afford and access care. Poor people are more likely to use high level tertiary care rather than primary and preventive measures such as regular medical check-ups, but are least able to afford such care. Costs often lead to delays in seeking care and people with diseases such as cancer and diabetes may forgo treatment due to the inability to
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
63C
oncl
usio
ns
pay. The poor are more likely to self-medicate, bypassing professional diagnosis and treatment. Measures to strengthen poor people’s access to appropriate NCD prevention and education programmes and affordable treatment initiatives should be a priority focus of WHO, development agencies, and national and local health service providers.
The traditional focus of the health system on acute care for people in the latter stages of disease progression can be detrimental to the poor who are unable to afford such care which does little to prevent the growth of NCDs among the poor and in developing nations. An increased focus on prevention and a multi-faceted, multi-level approach such as the WHO Global Strategy on Diet, Physical Activity and Health and the ICCC framework can be useful in making the system more responsive to prevention, and improve outcomes once diseases have developed.
Costs of accessing health care contribute to maintaining the cycle of poverty. Though data specifically related to NCDs is scanty on this issue, the high cost of tertiary treatment and medication for NCDs combined with the high and/or increasing proportion of health costs borne by individuals in the region is likely to contribute to the effect of ill-health on poverty.
Outcomes for poor people with NCDs are consistently worse than for their richer counterparts. Poor people are more likely to die an early death and have significantly higher mortality rates from NCDs. Australian studies have indicated that people of low socioeconomic status suffer between 50% and 200% higher mortality rates than people of the highest socioeconomic status for conditions such as ischaemic heart disease, diabetes mellitus and respiratory illness.
The assumption that NCDs are diseases of affluence has inhibited effective planning for, and servicing of, the growing incidence of NCDs among the poor in the Region. Globally, and particularly in Sub-Saharan Africa, communicable diseases are still the major cause of mortality and morbidity among the poor. However, in the Western Pacific Region, communicable diseases form a minority of the causes of burden of disease and mortality. Given the high and increasing proportion of burden of disease from NCDs in the Western Pacific, and that poor people are highly vulnerable to these diseases, a strengthened focus on NCD interventions for the poor in the Region is justifiable. Here, we do not argue for a substitution of resources diverted from communicable diseases to NCDs, but for an appropriate investment in primary and secondary prevention to ensure both are effectively and efficiently controlled.
Protecting and improving the health of the poor can have significant, positive national economic impact. Improving social equity leads to better
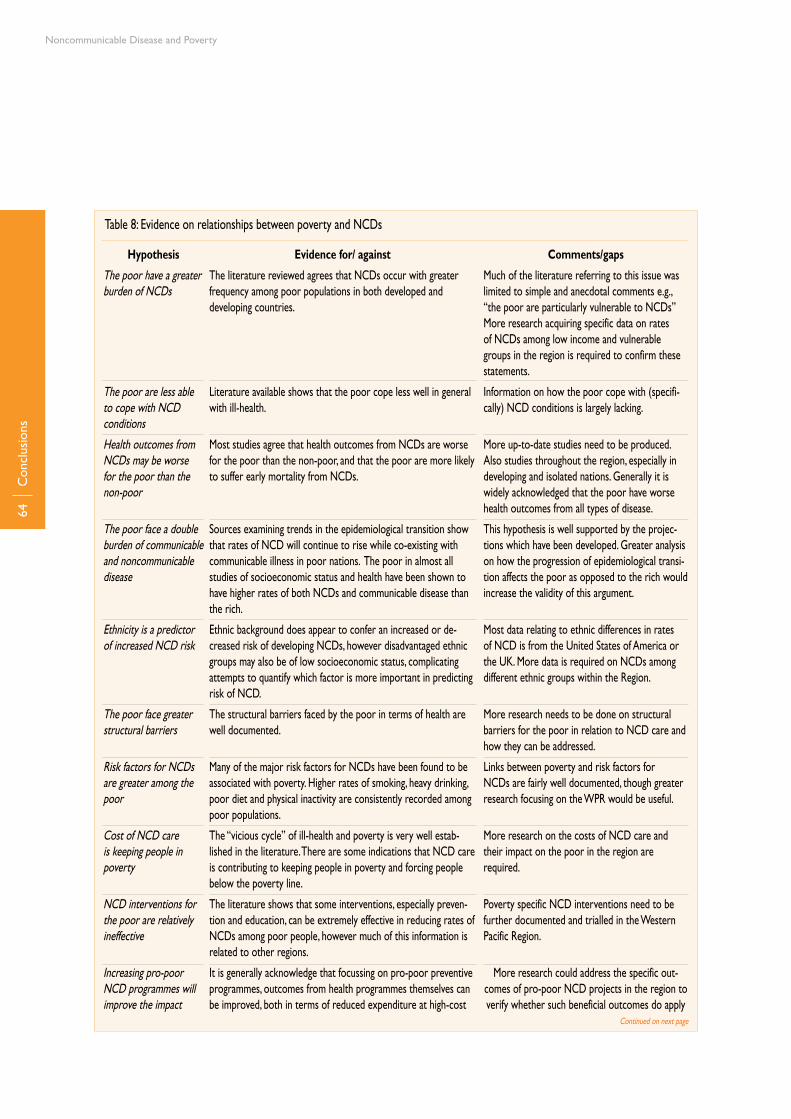
Noncommunicable Disease and Poverty
64C
oncl
usio
ns
Table 8: Evidence on relationships between poverty and NCDs
Continued on next page
Hypothesis
The poor have a greater burden of NCDs
The poor are less able to cope with NCD conditions
Health outcomes from NCDs may be worse for the poor than the non-poor
The poor face a double burden of communicable and noncommunicable disease
Ethnicity is a predictor of increased NCD risk
The poor face greater structural barriers
Risk factors for NCDs are greater among the poor
Cost of NCD care is keeping people in poverty
NCD interventions for the poor are relatively ineffective
Increasing pro-poor NCD programmes will improve the impact
Evidence for/ against
The literature reviewed agrees that NCDs occur with greater frequency among poor populations in both developed and developing countries.
Literature available shows that the poor cope less well in general with ill-health.
Most studies agree that health outcomes from NCDs are worse for the poor than the non-poor, and that the poor are more likely to suffer early mortality from NCDs.
Sources examining trends in the epidemiological transition show that rates of NCD will continue to rise while co-existing with communicable illness in poor nations. The poor in almost all studies of socioeconomic status and health have been shown to have higher rates of both NCDs and communicable disease than the rich.
Ethnic background does appear to confer an increased or de-creased risk of developing NCDs, however disadvantaged ethnic groups may also be of low socioeconomic status, complicating attempts to quantify which factor is more important in predicting risk of NCD.
The structural barriers faced by the poor in terms of health are well documented.
Many of the major risk factors for NCDs have been found to be associated with poverty. Higher rates of smoking, heavy drinking, poor diet and physical inactivity are consistently recorded among poor populations.
The “vicious cycle” of ill-health and poverty is very well estab-lished in the literature. There are some indications that NCD care is contributing to keeping people in poverty and forcing people below the poverty line.
The literature shows that some interventions, especially preven-tion and education, can be extremely effective in reducing rates of NCDs among poor people, however much of this information is related to other regions.
It is generally acknowledge that focussing on pro-poor preventive programmes, outcomes from health programmes themselves can be improved, both in terms of reduced expenditure at high-cost
Comments/gaps
Much of the literature referring to this issue was limited to simple and anecdotal comments e.g., “the poor are particularly vulnerable to NCDs”More research acquiring specific data on rates of NCDs among low income and vulnerable groups in the region is required to confirm these statements.
Information on how the poor cope with (specifi-cally) NCD conditions is largely lacking.
More up-to-date studies need to be produced. Also studies throughout the region, especially in developing and isolated nations. Generally it is widely acknowledged that the poor have worse health outcomes from all types of disease.
This hypothesis is well supported by the projec-tions which have been developed. Greater analysis on how the progression of epidemiological transi-tion affects the poor as opposed to the rich would increase the validity of this argument.
Most data relating to ethnic differences in rates of NCD is from the United States of America or the UK. More data is required on NCDs among different ethnic groups within the Region.
More research needs to be done on structural barriers for the poor in relation to NCD care and how they can be addressed.
Links between poverty and risk factors for NCDs are fairly well documented, though greater research focusing on the WPR would be useful.
More research on the costs of NCD care and their impact on the poor in the region are required.
Poverty specific NCD interventions need to be further documented and trialled in the Western Pacific Region.
More research could address the specific out-comes of pro-poor NCD projects in the region to verify whether such beneficial outcomes do apply
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
65C
oncl
usio
ns
human capital in society. Binding international agreements focus on health as a human right for all people. Health for all requires addressing the barriers to care for poor people and meeting the growing rates of NCDs among the poor, rather than considering the treatment of NCDs to be a private issue. A focus on poor people in NCD programmes can reduce national mortality rates, and the efficiency of NCD programmes themselves requires that the needs of the poor are addressed.
The literature suggests that both NCDs and the needs of the poor vary substantially between and within countries of the Western Pacific Region. Pro-poor NCD policies should, therefore, be developed at country level with local inputs. There are many interesting questions that can be further examined to strengthen arguments that NCDs and poverty are related in the Western Pacific Region. However, many of these questions are of academic interest and have no immediate practical relevance to reducing the NCD burden for the poor.
The issues are clear: incidence and prevalence of NCDs are increasing rapidly and the poor bear a disproportionate burden. What is required now are policies, mechanisms and budget allocations to address these needs. Specifically, health services require a focus on prevention and primary care and then secondary and tertiary prevention, based on established NCD intervention protocols for specific conditions. Investments in such services would generate health gains and savings. Health information systems should be developed to monitor incidence, service activity and costs of NCD programmes and identify services by geographic area to help disaggregate information about the poor. This information can be used to manage effective NCD programmes and establish an evidence base in the Western Pacific Region, which currently does not exist.
Hypothesis
of NCD programmes themselves
Human rights, equity and social justice require a reconfiguring of health funding in favour of pro-poor NCD programmes
Evidence for/ against
tertiary institutions and in reducing burden of disease and mortal-ity rates.
It is recognised widely by all health and development agencies that health is a human right for all. The literature suggests that health services are somewhat biased towards richer segments of the community. Equity and social justice argue in favour of increasing the provision of pro-poor health projects. Whether health funding should be reconfigured towards NCDs will depend on the outcome of further research, diagnostics, assessment and comparative analysis
Comments/gaps
in this area.
Does the burden of NCDs among the poor in the Western Pacific justify reconfiguring funding for pro-poor NCD programmes?
Table 8 continued

Noncommunicable Disease and Poverty
66Bi
blio
grap
hy
Bibliography
Abdul-Rahim, H. F. et al. The Metabolic Syndrome in the West Bank Population- an urban-rural comparison. Diabetes Care, 2001, 24:275-279
Adhikari, R., Gertler, P., Lagman, A. Economic Analysis of Health Sector Projects- a review of issues, methods and approaches, Manila, Asian Development Bank, 1999
Ait-Khaled, N., Enarson, D., Bousquet, J. Chronic Respiratory Diseases in Devel-oping Countries: The Burden and Strategies for Prevention and Management. Bulletin of the World Health Organization, 2001, 79:971-979
Ali, Z., Rahman, A., Rahman, T. Appetite for Nicotine- An economic analysis of tobacco control in Bangladesh, Washington DC, The World Bank, 2003
Al Serouri, A. W., Balabanova, D., Al-Hibshi, S., Cost Sharing for Primary Health Care, London, Oxfam (undated) http://www.oxfam.org.uk/what_we_do/resources/downloads/wp_yemen/wp_yemen_4discuss.pdf (last accessed 18 August 2005)
Asian Development Bank Poverty and Inequality Indicators http://www.adb.org/Documents/EDRC/Statistics/rt_06.xls (last accessed 18 August 2005)
Assunta, M. Impact of Alcohol Consumption on Asia. The Globe (2001) 3:4 http://www.ias.org.uk/publications/theglobe/01issue3,4/globe0103_04_p4.html (last accessed 18 August 2005)
Assunta, M. Marketing Alcohol in Asia. American Journal of Health Promotion Vol 4 No 5 (Dec 2001/Jan 2002) http://www.healthpromotionjournal.com/publica-tions/global/2002-01/ (last accessed 22 August 2005)
Atri, J. et al. Fair Shares in Health Care? Ethnic and Socioeconomic influences on recording of preventive care in selected inner London general practices. British Medical Journal, 1996 312:614-617
Australian Health Ministers’ Advisory Council Preventing Chronic Disease: A strate-gic framework Melbourne, National Public Health Partnership, 2001
Baile, S. et al. DAC Guidelines and Reference Series: Poverty and Health, Paris, OECD/WHO, 2003
Bakker, B. Consumer Preferences in Hong Kong on Western Foods, Hong Kong, United States Department of Agriculture/Asian Commercial Research Ltd, 2000
BeaverC.HealthCareDecision-makingintheWesternPacificRegion–Dia-betes and the Care Continuum in the Pacific Island Countries Manila, WPRO/WHO, 2003
Bennett, S. Socioeconomic Inequalities in Coronary Heart Disease and Stroke Mortality Among Australian Men 1979-1993. International Journal of Epidemiology, 1996, 25:266-275

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
67Bi
blio
grap
hy
Boulton, T. et al. Profile of heart disease risk factors and their relation to par-ents’ education, fathers’ occupation and family history of heart disease in 843 South Australian Families: The Adelaide Children’s WHO Collaborative Study. Journal of Paediatrics and Child Health, 1995, 31:200-206
Boutayeb, A. and Boutayeb, S. The Burden of Noncommunicable Diseases in Developing Countries. International Journal for Equity in Health, 2005, 4:2
Bovet, P. et al. Monitoring one-year compliance to antihypertension medica-tion in the Seychelles. Bulletin of the World Health Organization, 2002, 80:33-39
Bradley, C., Given, C., Roberts, C. Race, Socioeconomic Status, and Breast Cancer Treatment and Survival. Journal of the National Cancer Institute, 2002, 94(7):490-96
Bradshaw, D., Steyn, K. (eds.) Poverty and Chronic Diseases in South Africa- tech-nical report 2001 WHO/MRC, 2001 (ISBN 1-919809-17-1)
Brands, A., Yach D. Women and the Rapid Rise of Noncommunicable Diseases, Geneva, WHO, 2002
Brewis, A. et al. Gender and Noncommunicable Disease in the Pacific. Pacific Health Dialog, March 1996, 3(1):107-113
Brown, A. et al. Socioeconomic position and health among persons with Diabetes Mellitus: a conceptual framework and a review of the literature. Epidemiological Review, 2004, 26:63-77
Burnley, I.H. Disadvantage and Male Cancer Incidence and Mortality in NSW 1985-1993. Social Science and Medicine, 1997, 45:465-476
Burnley, I.H. Mortality from Respiratory System Cancer in NSW and Sydney. Australian Journal of Public Health, 1992, 16:251-261
Cameron, A. et al. Overweight and obesity in Australia: the 1999-2000 Aus-tralian diabetes, obesity and lifestyle study. Medical Journal of Australia, 2003, 178(9):427-432
Centers for Disease Control and Prevention. NCHS Data on Chronic Obstruc-tive Pulmonary Disease (undated) http://www.cdc.gov/nchs/data/factsheets/copd.pdf (last accessed 18 August 2005)
Centers for Disease Control and Prevention, Diabetes among Hispanics, Los Angeles County, California, 2002-2003. Morbidity and Mortality Weekly Review, November 28, 2003, 52(47):1152-1155
Centers for Disease Control and Prevention, Socioeconomic status of Women with Diabetes- United States 2000. Morbidity and Mortality Weekly Report, 22 February 2002; 51(7):107-108 and 159
Centers for Disease Control and Prevention, Women and Smoking: a report

Noncommunicable Disease and Poverty
68
of the Surgeon General- Executive Summary. Morbidity and Mortality Weekly Report, 30 August 2002; 51/RR12:1-30
Chaloupka, F. et al. The Evidence Base for Reducing Mortality from Smoking in Low and Middle Income Countries CMH Working Paper Series Paper No: WG5:7 (2001) http://www3.who.int/whosis/cmh/cmh_papers/e/pdf/wg5_paper07.pdf (last accessed 29th August 2005)
Chinese Academy of Preventive Medicine, Smoking and Health in China: 1996 National Prevalence Survey of Smoking Pattern. China Science and Technology Press 1997
Coleman, R., Gill, G., Wilkinson, D. Noncommunicable disease management in resource-poor settings: A primary care model from rural South Africa. Bulletin of the World Health Organization, 1998, 76(6):633-640
Davis, J. et al. The Relationship between Ethnicity and Obesity in Asian and Pacific Islander Populations: A literature review. Ethnicity and Disease, 2004, 14(1):111-118
Demers, A., Room, R., Bourgault, C. Surveys of Drinking Patterns and Problems in Seven Developing Countries, Geneva, WHO, 2000
Department for International Development, Disability, poverty and development ID21 Highlights, January 2002 http://www.soziologie.ch/users/markus/health/docs/5%20Other%20documents/5.16_Disability_Poverty_and_Development.pdf (last accessed 18 August 2005)
Devereux, S. Conceptualising Destitution, Brighton, Institute of Development Stud-ies, 2003
Drewnowski, A. Poverty and Obesity presented at the Obesity and the Built Environment: Improving Public Health Through Community Design Conference, Washington DC, 24-26 May 2004 http://www.niehs.nih.gov/drcpt/beoconf/post-conf/drewnowski.pdf (last accessed 29 August 2005)
Economics and Development Resource Centre. Handbook for the Economic Analy-sis of Health Sector Projects, Manila, Asian Development Bank, 2000
Evans, T. et al. Summary of the book: Challenging Inequalities in Health, New York, Oxford University Press, 2001 http://www.rockfound.org/Documents/435/sum-mary_challenging.pdf (last accessed 29 August 2005)
Evans, T. et al. World Health Report 2003, WHO, Geneva 2003
Fahey, S. Development Labour Relations and Gender in Papua New Guinea. Mankind, 1986, 16(2):118-31
Fiji Ministry of Information. Poverty Contributes to NCDs, Fiji Government Press Release, 5 February 2002
Garcia, M., Mason, J. Second Report on the World Nutrition Situation- Volume 1 Global
Bibl
iogr
aphy
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
69
and Regional Results, Geneva, United Nations Administrative Committee on Co-ordination Subcommittee on Nutrition, 1992 (Reprinted 1993)
Ghaffar, A., Srinath Reddy, K., Singhi, M. Burden of Noncommunicable Diseases in South Asia. British Medical Journal, 2004, 328: 807-810
Graham, H. (ed.) Understanding Health Inequalities, Buckingham, Open University Press 2001
Grosh, M. Administering Targeted Social programs in Latin America: From platitudes to practice, Aldershot, Ashgate Publishing Ltd, 1996
Gulliford, M., Mahabir, D. Social inequalities in morbidity from Diabetes Mellitus in public primary care clinics in Trinidad and Tobago. Social Science and Medicine, 46(1):137-144
Gwatkin, D. Inequalities in Access to Health Care in Developing Countries: What Should Be Done? HNP and Poverty Seminar Report, World Bank, 21 March 2001 http://www1.worldbank.org/prem/poverty/health/library/gwatkin4.pdf (last ac-cessed 25 August 2005)
Gwatkin, D. Reducing Health Inequalities in Developing Countries, Washington DC, The World Bank 2002
Gwatkin, D. The Current State of Knowledge about Targeting Health Programs to Reach the Poor, Washington DC, World Bank, 2000 http://siteresources.world-bank.org/INTPAH/Resources/Publications/Recent-Papers/targeting.pdf (last accessed 18th August 2005)
Gwatkin, D., Guillot, M. The Burden of Disease among the global poor, Washington D.C., The World Bank, 2000
Gwatkin, D., Guillot, M., Heuveline, P. The Burden of Disease among the Global Poor. The Lancet, 1999, 354: 586-589
Harvard Center for Cancer Prevention, Socioeconomic Status. in Harvard Reports on Cancer Prevention Volume 1: Human Causes of Cancer, Rapid Science Publishers 1996 http://www.hsph.harvard.edu/cancer/publications/reports/vol1_full_text/print_ready/socio.html (last accessed 18 August 2005)
Hayward, M., Crimmins, E., Zhang, Z. Consequences of Educational Change for the Burden of Chronic Health Problems in the Population, Population Research Institute, Pennsylvania State University (Working Paper) December 2001 http://www.pop.psu.edu/general/pubs/working_papers/psu-pri/wp0202.pdf (last accessed 25 August 2005)
Henry-Lee, A., Yearwood, A. Protecting the poor and the medically indigent under health insurance: A case study of Jamaica, Bethesda, Partnerships for Health Re-form, 1999
Herman, W.H., Smith, P.J., Thompson, T.J., Engelgau, M.M., and Aubert R.E. A new
Bibl
iogr
aphy

Noncommunicable Disease and Poverty
70
and simple questionnaire to identify people at increased risk for undiagnosed diabetes. Diabetes Care, 1995, 18:382-387
Hodgkins, B.J., Manring, E,. Meyers, M. Demographic, Social and Stress Correlates of Hypertension among the Urban Poor. Family Practice, 1990, 7(4):261-6
Hughes, R. Diet, Food Supply and Obesity in the Pacific, Geneva, WHO 2003
Inoue, S., Zimmet, P., Bassett, J. The Asia Pacific Perspective: redefining obesity and its treatment, Sydney, Health Communications Australia Pty Ltd 2000
James, W. et al. Socioeconomic Determinants of Health: The Contribution of Nu-trition to Inequalities in Health. British Medical Journal (24 May 1997) 314:1545-1550
Jha Prabhat, Chaloupka, F. et al. Curbing the Epidemic: governments and the econom-ics of tobacco control, Washington DC, The World Bank, 1999
Jha, P., Chaloupka, F. (eds.) Tobacco Control in Developing Countries, New York, Ox-ford University Press, 2000
Jha, P., Mills, A. et al. Improving Health Outcomes of the Poor, Geneva, WHO, 2002
Johnson, K. W. et al. Macrosocial and Environmental Influences on Minority Health. Health Psychology, 1995, 14(7):601-612
Jones-Webb, R. et al. 2002. The Effects of Socioeconomic Position on Black-White Crossover Effects in CVD Mortality, Presentation at the 2002 University of Min-nesota Maternal and Child Health Program’s Summer Institute: “Strategies for Addressing Health Disparities.” http://www.epi.umn.edu/mch/summer/Summer-Institute/presentations/rhonda.ppt#2 (last accessed 23 August 2005)
Kain, J., Vio, F., Albal, C. Obesity Trends and Determinant Factors in Latin America. Cadernos de Saúde Pública, 2003, 19(suppl.1): 77-86
Kern, A., Ritzen, J. Dying for Change- Poor People’s Experience of Health and Ill-health, Washington DC, WHO/World Bank, 2001
Kuh, D. et al. Mortality in Adults aged 26-54 Years Related To Socio-Economic Conditions In Childhood And Adulthood: Post War Birth Cohort Study. British Medical Journal, November 2002, 325(7372):1076-1080
Leeder, S. et al. A Race Against Time: The Challenge of Cardiovascular Disease in Devel-oping Economies, New York, Trustees of Columbia University, 2004
Leon, D., Walt, G. (eds.) Poverty, Inequality and Health- an international perspective, New York, Oxford University Press, 2000
Lie RK. Human rights, equity and health sector reform (Final Report). May, 2000 (unpublished document), http://www.hf.uib.no/i/filosofisk/ethica/rights22.pdf (last accessed 22 August 2005)
Bibl
iogr
aphy

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
71
Low, A., Ithindi, T., Low, A. A Step Too Far? Making Health Equity Interventions in Namibia More Sufficient. International Journal for Equity in Health, 2003, 2:5
Mathers, C. Health Differentials among Adult Australians aged 25-64 Years, Canberra, Commonwealth Government Publishing Service, 1994
Mathers, C., Vos, S. Stevenson, C. The Burden of Disease and Injury in Australia, Canberra, Australian Institute of Health and Welfare, 1999
Mbanya, J. C. Class Divide: Education and NCD Risk Factors in Cameroon http://www.id21.org/insights/insights-h01/insights-issh01-art04.html Insights Health 2001 (last accessed 18 August 2005)
McAlister, F et al. Influence of socio-economic deprivation on the primary care burden and treatment of patients with a diagnosis of heart failure in Gen-eral Practice in Scotland: Population based Study. British Medical Journal, 2004, 328:1110
McCawley, P. Economic Security and Regional Integration in South East Asia, Malay-sian National Economic Outlook Conference, Kuala Lumpur, 7 December 2004 http://www.adbi.org/speeches/2004/12/07/852.seasian.economic.security/mass.poverty.in.the.region/ (last accessed 18 August 2005)
McClelland, A., Pirkis, J., Willcox, S. Enough to Make You Sick- how income and envi-ronment affect health, Melbourne, National Health Strategy Research Paper No. 1 September 1992
Misra, R. Pro-poor Health Reforms, Why, What and How? Geneva, WHO, 2003
Monteiro, C. et al. Socioeconomic Status and Obesity in Adults of Developing Countries: a review. Bulletin of the World Health Organization, 2004, 82:940-946
Murray, C. et al. World Health Report 2002, Geneva, WHO, 2002
Murray, C., Feachem, R. Adult Mortality in Developing Countries, Transactions of the Royal Society of Tropical Medicine and Hygiene, 1990, 84:1-2
Musgrove, P. et al. World Health Report 2000, Geneva, WHO, 2000
National Aboriginal Community Controlled Health Organisation Australia. Estimation of Requirements for and Supply of the Health Workforce for Aboriginal and Torres Strait Islander Peoples, Canberra, Office of Aboriginal and Torres Strait Islander Health, 2000
National Clearinghouse on Tobacco and Health Program, Canada. Smoking Prevalence in the Western Pacific Region. http://www.ncth.ca/NCTH_new.nsf/Docs/Taxation~Smoking-WesternPacificRegion?OpenDocument (last accessed 18 August 2005)
National Heart, Lung and Blood Institute (US) & National Institutes of Health. Report on the Conference on Socioeconomic Status and Cardiovascular Health and
Bibl
iogr
aphy

Noncommunicable Disease and Poverty
72
Disease, November 6-7 1995 http://www.nhlbi.nih.gov/resources/docs/ses.txt (last accessed 18 August 2005)
New Policy Institute/Joseph Rowntree Foundation http://www.poverty.org.uk/summary/key_facts.htm (last accessed 18 August 2005)
Nishi, N. et al. Effects of socioeconomic indicators on coronary risk factors, self-rated health and psychological well-being among urban Japanese civil servants. Social Science and Medicine, 2004, 58:1159-1170
Nissinen, A., Berrios, X., Puska, P. Community based noncommunicable disease interventions: lessons from developed countries for developing ones. Bulletin of the World Health Organization, 2001, 79(10):963-970
(No author listed) “Filling the World’s Belly” The Economist 11 December 2003 http://www.economist.com/printerfriendly.cfm?Story_ID=2261775 (last accessed 18 August 2005)
O’Dea, J. Differences in overweight and obesity among Australian school chil-dren of low and middle/high socioeconomic status. Medical Journal of Australia, 2003, 179(1):63
Oxfam, Cut the Cost- Patent Injustice: how world trade rules threaten the health of poor people 2001 http://www.oxfam.org.uk/what_we_do/issues/health/down-loads/patentinjustice.pdf (last accessed 25 August 2005)
Pamuk, E. et al. Socioeconomic status and health chartbook, Hyattsville, National Centre for Health Statistics, 1998
Pan American Health Organization/WHO. Public Health response to Chronic Diseases (130th Session of the Executive Committee) [CE130/17] Washington DC, 24-28 June 2002 http://www.paho.org/english/gov/ce/ce130-17-e.pdf (last accessed 25 August 2005)
Peabody, J. W. et al. Policy and Health- implications for development in Asia, New York, Cambridge University Press, 1999
Pell, J. et al. Effect of Socioeconomic deprivation on waiting time for cardiac sur-gery: respective cohort study. British Medical Journal, 2000, 320:15-19
Peña, M. & Bacallo, J. Obesity and Poverty- a new public health challenge, Wash-ington DC, Pan American Health Organisation, 2000 (Scientific Publication 576)
Popkin, B., Horton, S., Kim, S. The Nutritional Transition and Diet Related Chronic Dis-eases in Asia, Food Consumption and Nutrition Division Discussion paper 105, Washington DC, International Food Policy Research Institute, 2001
Popkin, B., Liu, B., Zhai, F. Understanding the Nutrition Transition: Measuring rapid dietary changes in transitional countries. Public Health Nutrition, 2002, 5(6A):947-953
Bibl
iogr
aphy
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
73
Preker, A.S. et al. Sector Strategy: Health, Nutrition and Population, Washington DC, World Bank, 1997
Pruitt, S. et al. Innovative Care for Chronic Conditions- building blocks for action, Ge-neva, WHO, 2002
Purdy, M., Banks, D (eds.) Health and Exclusion, London, Routledge, 1999
Puska, P. et al. Globalization, Diets and Noncommunicable Diseases, Geneva, WHO, 2002
Puska, P. Successful prevention of noncommunicable diseases: 25 year experi-ences with North Karelia Project in Finland. Public Health Medicine, 2002
Raphael, D. Inequality is Bad for Our Hearts: why low income and social exclusion are major causes of heart disease in Canada, Toronto, North York Heart Health Network, 2001
Reidpath, D. et al. An ecological study of the relationship between social and environmental determinants of obesity. Health and Place, 2002, 8(2):141-145
Ross, H. Lifting the Unequal Burden of Cancer on Minorities and the Unders-erved. Closing the Gap- newsletter of the Office of Minority health, US Department of Health and Human Services August 2000 p1-16
Secretariat of the Pacific Community. Public Health Programme http://www.spc.org.nc/health/hpa/public_health_programme.htm (last accessed 18 August 2005)
Sen, K., Bonita, R. Global Health Status: two steps forward, one step back. The Lancet, 2000; 356:577-82
Seniloli, K. They are Digging Their Graves with their Teeth: Mortality, Poverty and Malnutrition in the Pacific, CICRED Seminar on Mortality as Both a Determinant and a Consequence of Poverty and Hunger, Thiruvananthapuram, India, 23-25 February 2005, pp. 1-27. http://www.cicred.org/Eng/Seminars/Trivandrum2005/Trivandrum-SENILOLI.pdf (last accessed 6 September 2005)
Shariif, I. The Socioeconomic Implications of AIDS in Developing Countries in General and Africa in Particular (undated) http://www.uwmc.uwc.edu/csepa/mhall/IGS/Plagues/TextPages/globalimplications.htm (last accessed 18 August 2005)
Shaw, J. Chronic Disease: The New Face of Poverty in Chile, American Dietetic Associ-ation Foundation http://www.eatright.org/Public/7772_17341.cfm (last accessed 18 August 2005)
Smith, G., Hart, C. Life-course Socioeconomic and Behavioural Influences on Cardiovascular Disease Mortality: The Collaborative Study. American Journal of Public Health, August 2002, 92(8):1295-1298
Sorlie, P., Johnson, M., Backlund, E. “Socioeconomic Status and Cardiovascular Disease Mortality: National Longitudinal Mortality Study” in Report of the Confer-
Bibl
iogr
aphy

Noncommunicable Disease and Poverty
74
ence on Socioeconomic Status and Cardiovascular Health and Disease, National In-stitutes of Health/National Heart, Lung and Blood Institute, November 6-7 1995 http://www.nhlbi.nih.gov/resources/docs/ses.txt (last accessed 18 August 2005)
Srinivasa Murthy, R. et al. World Health Report 2001, WHO; Geneva 2001
Stanton, H. J. Chapman was Right After All! Pacific Health Dialog, March 1996, 3(1):6-7
Sturgis, P., Jackson, J. Examining Participation in Sporting and Cultural Activities: Analy-sis of the UK 2000 Time Use Survey Phase 2, London, United Kingdom Depart-ment for Culture, Media and Sport, November 2003
The Jobs Letter No 16, 3rd May 1995 http://www.jobsletter.org.nz/jbl01600.htm (last accessed 18 August 2005)
Turrell, G. et al. Socioeconomic Determinants of Health: towards a national research program and a policy and intervention agenda, Canberra, Queensland University of Technology, School of Public Health, Ausinfo, 1999
Unwin, N. Taking Poverty to Heart. Noncommunicable diseases and the poor http://www.id21.org/zinter/id21zinter.exe?a=0&i=InsightsHealth%231Editorial&u=43095b04 Insights Health 2003 (last accessed 22 August 2005)
Victorian Alcohol and Drug Association. The Links between Alcohol and Drug Use and Poverty, Submission to the Senate Community Affairs Reference Commit-tee’s Inquiry into Poverty in Australia March 2003 http://www.vaada.org.au/Poverty%20Inquiry%20Submission%20FINAL.doc (last accessed 29 August 2005)
Wagstaff, A. Poverty and Health Sector Inequalities. Bulletin of the World Health Organisation, 2002, 80(2):97-105
Wagstaff, A. The Contribution of High Health Care Costs to Impoverishment, HNP and Poverty Seminar Report, The World Bank, 6 September 2000 http://www1.worldbank.org/prem/poverty/health/library/wagstaf3.pdf (last accessed 25 August 2005)
Waldron, I et al. Gender Differences in Tobacco Use in Africa, Asia, the Pacific and Latin America. Social Science and Medicine, 1988, 27(11):1269-1275
Wang, Y., Monteiro, C., Popkin, B. Trends of Obesity and Underweight in Older Children and Adolescents in the United States, Brazil, China and Russia. American Journal of Clinical Nutrition, 2002, 75(6):971-7
Wardle, J., Waller, J., Jarvis, M. Sex Differences in the Association of Socio-economic status with Obesity. American Journal of Public Health, August 2002, 92(8):1299-1304
Warwick, H. For want of a dollar a year. New Scientist, 6 December 2003, 2424:22
WHO Department of Gender and Women’s Health. Gender, Health and Tobacco,
Bibl
iogr
aphy

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
75
World Health Organization, Geneva, November 2003
WHO Department of Health in Sustainable Development. Partnership in Health and Poverty: Towards a Common Agenda- report of an international meeting WHO HQ Geneva 12-14 June 2000, Geneva, WHO, 2001
WHO Department of Noncommunicable Disease Prevention and Health Promotion. Global Forum on integrated NCD prevention and control, Geneva, WHO, 2001
WHO European Regional Office. Poverty and Health- Evidence and Action in WHO’s European Region (Regional Committee for Europe 52nd Session, Copenhagen 16-19 September 2002) [EUR/RC52/8] http://www.euro.who.int/Document/RC52/edoc8.pdf (last accessed 29 August 2005)
WHO Global Strategy on Diet, Physical Activity and Health- overall goal and guid-ing principles http://www.who.int/dietphysicalactivity/goals/en/ (last accessed 18 August 2005)
WHO Health and Sustainable Development Department. Health and Poverty Reduction- an informal consultation with selected development partners, Geneva 7-8 September 1999 Summary Report, Geneva, WHO, 1999 http://www.cct-freiburg.de/who/pro_poor/documents/informalcons.pdf (last accessed 5 September 2005)
WHO, Obesity, Preventing and Managing a Global Epidemic, WHO Technical Report Series 894, Geneva, WHO, 2000
WHO Regional Office for Europe. Noncommunicable Diseases in the European Region: the Challenge Fact Sheet EURO 06/04, Copenhagen, WHO, 2004
WHO, Surveillance of Noncommunicable Disease Risk Factors Fact Sheet No. 273, March 2003 http://www.who.int/mediacentre/factsheets/2003/fs273/en/ (last ac-cessed 1 September 2005)
WHO, Tobacco and Health in the Developing World, Brussels, European Commis-sion/WHO/World Bank, 2003 http://europa.eu.int/comm/development/body/theme/human_social/docs/health/03-03_tobacco_background_WHO.pdf (last accessed 9 September 2005)
WHO, Tobacco or Health: A Global Status Report, Geneva, WHO, 1997
WHO, Noncommunicable Diseases and Mental Health. Surveillance in Brief, 4th Quarter 2002, 1(1):1-4 http://www.who.int/ncd_surveillance/media/en/605.pdf (last accessed 29 August 2005)
WHO/WPRO, Fiji Islands http://www.wpro.who.int/countries/fij/health_situation.htm (last accessed 19 August 2005)
WHO/WPRO Prevention and Control of Noncommunicable Diseases (Regional Commit-tee 51st Session, Manila 18-22 September 2000) [WPR/RC51/8], Manila, WHO, 2000
Bibl
iogr
aphy

Noncommunicable Disease and Poverty
76
WHO/WPRO The Work of the WHO in the Western Pacific Region- Report of the Regional Director 1 July 1999- 30 June 2000, Manila, WPRO, 2000
WHO/WPRO The Work of the WHO in the Western Pacific Region- Report of the Regional Director 30 June 2002- 1 July 2003, Manila, WPRO, 2003
WHO/WPRO Working Paper on Renewing the Policy of Health for All- report of the subcommittee of the regional committee on programmes and technical cooperation, Part II Regional Committee Documents, Sydney, 22-26 September 1997, Annex II Draft Document
WHO/WPRO, Report- Workshop on Obesity Prevention and Control Strategies in the Pacific, Manila, WPRO, July 2002
Wielgosz, A. Surveillance at work: Zeroing in on cardiovascular diseases in regional health units across Canada. Canadian Journal of Cardiology, October 2003, 19(11):1239-1240
World Bank World Development Report 2004: Making services work for poor people, London, Oxford University Press, 2003
WPRO Health Financing and Social Protection: Current Issues http://www.wpro.who.int/sites/hcf/issues.htm (last accessed 18 August 2005)
WPRO STI HIV/AIDS Surveillance Report, August 2000, 15:1-8
Wu Fan. Situation and Strategy of Noncommunicable Disease Control and Prevention in China, Beijing , National Center for Chronic and Noncommunicable Disease Control and Prevention, China Center for Disease Control and Prevention, 2003
Yach, D. et al. Noncommunicable Diseases with Special Focus on Cardiovascular disease and diabetes in the Developing World (Seminar Report 27 April 2001) EN-RECA, Copenhagen 2001 http://enreca.pubhealth.ku.dk/2001_NonComDis.pdf (last accessed 25 August 2005)
Yach, D. et al. Noncommunicable diseases, prevention and control of a global epidemic- report of a WHO consultation, Geneva, 27-30 September 1999 (Draft 5), 9 August 2001 http://www.hpclearinghouse.ca/downloads/MACLEAN2.doc (last accessed 25 August 2005)
Ziglio, E. et al. (eds.) Health Systems Confront Poverty, Copenhagen, World Health Organization European Office, 2003
Bibl
iogr
aphy

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
77En
dnot
es
Endnotes1 Devereux, S. Conceptualising Destitution, Brighton, Institute of Develop-
ment Studies, 2003.2 WHO Regional Office for Europe Noncommunicable Diseases in the European
Region: the Challenge Fact Sheet EURO 06/04, Copenhagen, WHO, 2004.3 WHO/WPRO The Work of the WHO in the Western Pacific Region- Report of the
Regional Director 1 July 1999- 30 June 2000, Manila, WPRO, 2000.4 WHO, Noncommunicable Diseases and Mental Health. Surveillance in
Brief, 4th Quarter 2002, 1(1):1-4 http://www.who.int/ncd_surveil-lance/media/en/605.pdf (last accessed 29 August 2005).
5 WHO/WPRO The Work of the WHO in the Western Pacific Region- Report of the Regional Director 30 June 2002- 1 July 2003, Manila, WPRO, 2003 and WHO, Surveillance of Noncommunicable Disease Risk Factors Fact Sheet No. 273, March 2003 http://www.who.int/mediacentre/factsheets/2003/fs273/en/ (last accessed 1 September 2005).
6 World Bank World Development Report 2004: Making services work for poor people, London, Oxford University Press, 2003.
7 Wang, Y., Monteiro, C., Popkin, B. Trends of Obesity and Underweight in Older Children and Adolescents in the United States of America, Brazil, China and Russia. American Journal of Clinical Nutrition, 2002, 75(6):971-7.
8 Sorlie, P., Johnson, M., Backlund, E. “Socioeconomic Status and Car-diovascular Disease Mortality: National Longitudinal Mortality Study” in Report of the Conference on Socioeconomic Status and Cardiovascular Health and Disease National Institutes of Health/National Heart, Lung and Blood Institute, 6-7 November 1995 http://www.nhlbi.nih.gov/resources/docs/ses.txt (last accessed 18 August 2005).
9 Leeder, S. et al. A Race Against Time: The Challenge of Cardiovascular Disease in Developing Economies, New York, Trustees of Columbia University, 2004
10 WHO/WPRO Prevention and Control of Noncommunicable Diseases (Regional Com-mittee 51st Session, Manila 18-22 September 2000) [WPR/RC51/8], Manila, WHO, 2000.
11 Pan American Health Organization/WHO Public Health response to Chronic Diseases (130th Session of the Executive Committee) [CE130/17] Washington DC, 24-28 June 2002 http://www.paho.org/english/gov/ce/ce130-17-e.pdf (last accessed 25 August 2005).
12 WHO/WPRO Prevention and Control of Noncommunicable Diseases (Regional Committee 51st Session, Manila 18-22 September 2000) [WPR/RC51/8], Manila, WHO, 2000.
13 Gwatkin, D. The Current State of Knowledge about Targeting Health Programs to Reach the Poor, Washington DC, World Bank, 2000 http://siteresources.worldbank.org/INTPAH/Resources/Publications/Recent-Papers/tar-geting.pdf (last accessed 18 August 2005).
14 Leeder, S. et al. A Race Against Time: The Challenge of Cardiovascular Disease in Developing Economies, New York, Trustees of Columbia University, 2004.
15 Puska, P. et al. Globalization, Diets and Noncommunicable Diseases, Geneva, WHO, 2002.
16 Sen, K., Bonita, R. Global Health Status: two steps forward, one step back, The Lancet 2000; 356:577-82.
17 Australian Health Ministers’ Advisory Council Preventing Chronic Disease: A
strategic framework Melbourne, National Public Health Partnership, 200118 WHO/WPRO Prevention and Control of Noncommunicable Diseases (Regional Com-
mittee 51st Session, Manila 18-22 September 2000) [WPR/RC51/8], Manila, WHO, 2000.
19 WHO/WPRO Prevention and Control of Noncommunicable Diseases (Regional Com-mittee 51st Session, Manila 18-22 September 2000) [WPR/RC51/8], Manila, WHO, 2000.
20 WHO Tobacco or Health: A Global Status Report, Geneva, WHO, 1997.21 Yach, D. et al. Noncommunicable diseases, prevention and control of a global epidemic-
report of a WHO consultation, Geneva, September 27-30 1999 (Draft 5) 9 August 2001 http://www.hpclearinghouse.ca/downloads/MACLEAN2.doc (last accessed 25 August 2005).
22 The Jobs Letter No 16, 3 May 1995 http://www.jobsletter.org.nz/jbl01600.htm (last accessed 18 August 2005).
23 Gwatkin, D., Guillot, M. The Burden of Disease among the global poor, Washing-ton D.C., The World Bank, 2000.
24 Gwatkin, D., Guillot, M., Heuveline, P. The Burden of Disease among the Global Poor. The Lancet, 1999, 354: 586-589.
25 Musgrove, P. et al. World Health Report 2000 Geneva, WHO, 200026 Unwin, N. Taking Poverty to Heart. Noncommunicable diseases and the poor http://
www.id21.org/zinter/id21zinter.exe?a=0&i=InsightsHealth%231Editorial&u=43095b04 Insights Health 2003 (last accessed 22 August 2005).
27 Gwatkin, D., Guillot, M. The Burden of Disease among the global poor, Washing-ton D.C., The World Bank, 2000.
28 The global burden of disease study is a project of the World Bank, WHO and the Harvard School of Public Health which is to provide an epidemiological data-set to identify priorities for health services and research. Projections are made to the year 2020 to enable forward planning and to identify trends.
29 Sen, K., Bonita, R. “Global Health Status: two steps forward, one step back” The Lancet 2000; 356:577-82.
30 Nissinen, A., Berrios, X., Puska, P. Community based noncommuni-cable disease interventions: lessons from developed countries for developing ones. Bulletin of the World Health Organization, 2001, 79(10):963-970 and Yach, D. et al. Noncommunicable diseases, prevention and control of a global epidemic- report of a WHO consultation, Geneva, 27-30 September 1999 (Draft 5) 9 Au-gust 2001 http://www.hpclearinghouse.ca/downloads/MACLEAN2.doc (last accessed 25 August 2005).
31 Yach, D. et al. Noncommunicable diseases, prevention and control of a global epidemic- report of a WHO consultation, Geneva, 27-30 September 1999 (Draft 5) 9 August 2001 http://www.hpclearinghouse.ca/downloads/MACLEAN2.doc (last accessed 25 August 2005).
32 Boutayeb, A. and Boutayeb, S. The Burden of Noncommunicable Diseases in Developing Countries International Journal for Equity in Health 2005, 4:2.
33 Yach, D. et al. Noncommunicable diseases, prevention and control of a global epidemic- report of a WHO consultation, Geneva, 27-30 September 1999 (Draft 5) 9 August 2001 http://www.hpclearinghouse.ca/downloads/MACLEAN2.doc (last accessed 25 August 2005).

Noncommunicable Disease and Poverty
78En
dnot
es
34 WHO Department of Health in Sustainable Development Partnership in Health and Poverty: Towards a Common Agenda- report of an international meeting WHO HQ Geneva 12-14 June 2000, Geneva, WHO, 2001.
35 Murray, C., Feachem, R. Adult Mortality in Developing Countries Transactions of the Royal Society of Tropical Medicine and Hygiene, 1990, 84:1-2 and Garcia, M., Mason, J. Second Report on the World Nutrition Situation- Volume 1 Global and Regional Results, Geneva, United Nations Administrative Committee on Coordination Subcommittee on Nutrition, 1992 (Reprinted 1993).
36 See, for example, Leeder, S. et al. A Race Against Time: The Challenge of Cardio-vascular Disease in Developing Economies, New York, Trustees of Columbia University, 2004.
37 WPRO-A: Australia, Brunei Darussalam, Japan, New Zealand, Singapore. WPRO-B : Cambodia, China, Cook Islands, Fiji, Kiribati, The Lao People’s Democratic Republic, Malaysia, Marshall Islands, Micronesia, Mongolia, Nauru, Niue, Palau, Papua New Guinea, Philippines, Republic of Korea, Samoa, Solomon Islands, Tonga, Tuvalu, Vanuatu, Viet Nam.
38 As described in Yach, D. et al. Noncommunicable diseases, prevention and control of a global epidemic- report of a WHO consultation, Geneva, 27-30 September 1999 (Draft 5) 9 August 2001 http://www.hpclearinghouse.ca/downloads/MA-CLEAN2.doc (last accessed 25 August 2005).
39 Peabody, J. W. et al. Policy and Health- implications for development in Asia, New York, Cambridge University Press, 1999.
40 WHO Department of Noncommunicable Disease Prevention and Health Promotion Global Forum on integrated NCD prevention and control, Geneva, WHO, 2001.
41 Sen, K., Bonita, R. “Global Health Status: two steps forward, one step back” The Lancet 2000; 356:577-82.
42 McCawley, P. Economic Security and Regional Integration in South East Asia Malaysian National Economic Outlook Conference, Kuala Lumpur, 7 December 2004 http://www.adbi.org/speeches/2004/12/07/852.seasian.economic.security/mass.poverty.in.the.region/ (last accessed 18 August 2005).
43 WHO Department of Noncommunicable Disease Prevention and Health Promotion Global Forum on integrated NCD prevention and control, Geneva, WHO, 2001.
44 Secretariat of the Pacific Community Public Health Programme http://www.spc.org.nc/health/hpa/public_health_programme.htm (last accessed 18 August 2005).
45 Peabody, J. W. et al. Policy and Health- implications for development in Asia, New York, Cambridge University Press, 1999.
46 Peabody, J. W. et al. Policy and Health- implications for development in Asia, New York, Cambridge University Press, 1999
47 Seniloli, K. They are Digging Their Graves with their Teeth: Mortality, Poverty and Malnutrition in the Pacific CICRED Seminar on Mortality as Both a Determinant and a Consequence of Poverty and Hunger, Thiruvananthapuram, India, 23-25 February 2005, pp. 1-27. http://www.cicred.org/Eng/Semi-nars/Trivandrum2005/TrivandrumSENILOLI.pdf (last accessed 6 September 2005).
48 As quoted in the Australian Health Ministers’ Advisory Council
Preventing Chronic Disease: A strategic framework (2001).49 Australian Health Ministers’ Advisory Council Preventing Chronic Disease: A
strategic framework Melbourne, National Public Health Partnership, 2001.50 Australian Health Ministers’ Advisory Council Preventing Chronic Disease: A
strategic framework Melbourne, National Public Health Partnership, 2001.51 Australian Health Ministers’ Advisory Council Preventing Chronic Disease: A
strategic framework Melbourne, National Public Health Partnership, 2001.52 WHO Department of Health in Sustainable Development Partnership in
health and Poverty: Towards a Common Agenda- report of an international meeting WHO HQ Geneva 12-14 June 2000, Geneva, WHO, 2001.
53 Bradshaw, D., Steyn, K. (eds) Poverty and Chronic Diseases in South Africa- techni-cal report 2001 WHO/MRC, 2001 (ISBN 1-919809-17-1).
54 WHO/WPRO Prevention and Control of Noncommunicable Diseases (Regional Com-mittee 51st Session, Manila 18-22 September 2000) [WPR/RC51/8], Manila, WHO, 2000.
55 Peabody, J. W. et al. Policy and Health- implications for development in Asia, New York, Cambridge University Press, 1999.
56 WHO Global Strategy on Diet, Physical Activity and Health- overall goal and guiding prin-ciples http://www.who.int/dietphysicalactivity/goals/en/ (last accessed 18 August 2005).
57 WHO/WPRO Prevention and Control of Noncommunicable Diseases (Regional Com-mittee 51st Session, Manila 18-22 September 2000) [WPR/RC51/8], Manila, WHO, 2000.
58 Hayward, M., Crimmins, E., Zhang, Z. Consequences of Educational Change for the Burden of Chronic Health Problems in the Population Population Research Institute, Pennsylvania State University (Working Paper) December 2001 http://www.pop.psu.edu/general/pubs/working_papers/psu-pri/wp0202.pdf (last accessed 25 August 2005).
59 Graham, H. (ed.) Understanding Health Inequalities, Buckingham, Open University Press 2001.
60 Smith, G., Hart, C. Life-course Socioeconomic and Behavioural Influ-ences on Cardiovascular Disease Mortality: The Collaborative Study. American Journal of Public Health, August 2002, 92(8):1295-1298.
61 Kuh, D. et al. Mortality in Adults aged 26-54 Years Related To Socio-Economic Conditions In Childhood And Adulthood: Post War Birth Cohort Study. British Medical Journal, November 2002, 325(7372):1076-1080.
62 Ross, H. Lifting the Unequal Burden of Cancer on Minorities and the Underserved. Closing the Gap- newsletter of the Office of Minority health, US Department of Health and Human Services August 2000 p1-16.
63 Peabody, J. W. et al. Policy and Health- implications for development in Asia, New York, Cambridge University Press, 1999.
64 Preker, A.S. et al. Sector Strategy: Health, Nutrition and Population, Washington DC, The World Bank, 1997.
65 WHO Health and Sustainable Development Department Health and Poverty Reduction- an informal consultation with selected development partners, Geneva 7-8 September 1999 Summary Report, Geneva, WHO, 1999 http://www.cct-freiburg.de/who/pro_poor/documents/informalcons.pdf (last accessed 5 September 2005).
66 Peabody, J. W. et al. Policy and Health- implications for development in Asia, New York, Cambridge University Press, 1999

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
79
67 Baile, S. et al. DAC Guidelines and Reference Series: Poverty and Health, Paris, OECD/WHO, 2003 and Jha, P., Mills, A. et al. Improving Health Outcomes of the Poor Geneva, WHO, 2002.
68 Jha, P., Chaloupka, F. (eds.) Tobacco Control in Developing Countries, New York, Oxford University Press, 2000.
69 Jha, P., Chaloupka, F. (eds.) Tobacco Control in Developing Countries, New York, Oxford University Press, 2000.
70 See (for example) Nissinen, A., Berrios, X., Puska, P. Community based noncommunicable disease interventions: lessons from devel-oped countries for developing ones. Bulletin of the World Health Organization, 2001, 79(10):963-970.
71 Bradshaw, D., Steyn, K. (eds.) Poverty and Chronic Diseases in South Africa- technical report 2001 WHO/MRC, 2001 (ISBN 1-919809-17-1).
72 WHO/WPRO Fiji Islands http://www.wpro.who.int/countries/fij/health_situation.htm (last accessed 19 August 2005) and Fiji Ministry of Information Poverty Contributes to NCDs Fiji Government Press Release, February 5 2002.
73 WHO Department of Health in Sustainable Development Partnership in health and Poverty: Towards a Common Agenda- report of an international meeting WHO HQ Geneva 12-14 June 2000, Geneva, WHO, 2001.
74 WHO/WPRO Prevention and Control of Noncommunicable Diseases (Regional Committee 51st Session, Manila 18-22 September 2000) [WPR/RC51/8], Manila, WHO, 2000.
75 Peabody, J. W. et al. Policy and Health- implications for development in Asia, New York, Cambridge University Press, 1999.
76 WHO Department of Gender and Women’s Health Gender, Health and Tobacco, World Health Organization, Geneva, November 2003.
77 Preker, A.S. et al. Sector Strategy: Health, Nutrition and Population, Washington DC, World Bank, 1997.
78 Jha Prabhat, Chaloupka, F. et al. Curbing the Epidemic: governments and the economics of tobacco control, Washington DC, The World Bank, 1999 and Jha, P., Chaloupka, F. (eds.) Tobacco Control in Developing Countries, New York, Oxford University Press, 2000.
79 WHO Tobacco and Health in the Developing World European Commission/WHO/World Bank, Brussels 2003 http://europa.eu.int/comm/devel-opment/body/theme/human_social/docs/health/03-03_tobacco_back-ground_WHO.pdf (last accessed 9 September 2005).
80 Nishi, N. et al. Effects of socioeconomic indicators on coronary risk factors, self-rated health and psychological well-being among urban Japanese civil servants. Social Science and Medicine, 2004, 58:1159-1170.
81 Jha, P., Chaloupka, F. (eds.) Tobacco Control in Developing Countries, New York, Oxford University Press, 2000.
82 Stanton, H. J. Chapman was Right After All! Pacific Health Dialog, March 1996, 3(1):6-7.
83 National Clearinghouse on Tobacco and Health Program, Canada Smoking Prevalence in the Western Pacific Region. http://www.ncth.ca/NCTH_new.nsf/Docs/Taxation~Smoking-WesternPacificRegion?OpenDocument (last accessed 18 August 2005).
84 Centers for Disease Control and Prevention, Women and Smoking: a report of the Surgeon General- Executive Summary. Morbidity and Mortality Weekly Report, August 30 2002; 51/RR12:1-30.
85 Brands, A., Yachs D. Women and the Rapid Rise of Noncommunicable Diseases, Geneva, WHO, 2002.
86 Ali, Z., Rahman, A., Rahman, T. Appetite for Nicotine- An economic analysis of tobacco control in Bangladesh, Washington DC, The World Bank, 2003.
87 Waldron, I et al. Gender Differences in Tobacco Use in Africa, Asia, the Pacific and Latin America. Social Science and Medicine, 1988, 27(11):1269-1275.
88 Waldron, I et al. Gender Differences in Tobacco Use in Africa, Asia, the Pacific and Latin America. Social Science and Medicine, 1988, 27(11):1269-1275.
89 Bradshaw, D., Steyn, K. (eds.) Poverty and Chronic Diseases in South Africa- technical report 2001 WHO/MRC, 2001 (ISBN 1-919809-17-1).
90 Warwick, H. For want of a dollar a year. New Scientist, 6th Dec 2003, 2424:22.
91 Bradshaw, D., Steyn, K. (eds.) Poverty and Chronic Diseases in South Africa- technical report 2001 WHO/MRC, 2001 (ISBN 1-919809-17-1).
92 Murray, C. et al. World Health Report 2002 Geneva, WHO, 2002.93 Bradshaw, D., Steyn, K. (eds.) Poverty and Chronic Diseases in South Africa-
technical report 2001 WHO/MRC, 2001 (ISBN 1-919809-17-1).94 Assunta, M. Impact of Alcohol Consumption on Asia. The Globe
(2001) 3:4 http://www.ias.org.uk/publications/theglobe/01issue3,4/globe0103_04_p4.html (last accessed 18 August 2005).
95 Demers, A., Room, R., Bourgault, C. Surveys of Drinking Patterns and Problems in Seven Developing Countries, Geneva, WHO, 2000.
96 Brewis, A. et al. Gender and Noncommunicable Disease in the Pacific. Pacific Health Dialog, March 1996, 3(1):107-113.
97 Fahey, S. Development Labour Relations and Gender in Papua New Guinea. Mankind, 1986, 16(2):118-31.
98 Assunta, M. Marketing Alcohol in Asia. American Journal of Health Promotion Vol 4 No 5 (December 2001/January 2002) http://www.healthpro-motionjournal.com/publications/global/2002-01/ (last accessed 22 August 2005).
99 Assunta, M. Marketing Alcohol in Asia. American Journal of Health Promotion Vol 4 No 5 (December 2001/January 2002) http://www.healthpro-motionjournal.com/publications/global/2002-01/ (last accessed 22 August 2005).
100 Victorian Alcohol and Drug Association The Links between Alcohol and Drug Use and Poverty Submission to the Senate Community Affairs Reference Committee’s Inquiry into Poverty in Australia March 2003 http://www.vaada.org.au/Poverty%20Inquiry%20Submission%20FINAL.doc (last accessed 29 August 2005).
101 Victorian Alcohol and Drug Association The Links between Alcohol and Drug Use and Poverty Submission to the Senate Community Affairs Reference Committee’s Inquiry into Poverty in Australia March 2003 http://www.vaada.org.au/Poverty%20Inquiry%20Submission%20FINAL.doc (last accessed 29 August 2005).
102 WHO/WPRO, Report- Workshop on Obesity Prevention and Control Strategies in the Pacific, Manila, WPRO, July 2002.
103 WHO Obesity, Preventing and Managing a Global Epidemic WHO Technical Report Series 894, Geneva, WHO, 2000 and WHO/WPRO, Report- Workshop on Obesity Prevention and Control Strategies in the Pacific, Manila, WPRO,
Endn
otes

Noncommunicable Disease and Poverty
80
July 2002.104 WHO/WPRO, Report- Workshop on Obesity Prevention and Control Strategies in
the Pacific, Manila, WPRO, July 2002.105 Wardle, J., Waller, J., Jarvis, M. Sex Differences in the Association
of Socio-economic status with Obesity. American Journal of Public Health, August 2002, 92(8):1299-1304.
106 (No Author listed) “Filling the World’s Belly” The Economist 11 December 2003 http://www.economist.com/printerfriendly.cfm?Story_ID=2261775 (last accessed 18 August 2005) and Popkin, B., Liu, B., Zhai, F. Understanding the Nutrition Transition: Measuring rapid dietary changes in transitional countries. Public Health Nutrition, 2002, 5(6A):947-953
107 Popkin, B., Liu, B., Zhai, F. Understanding the Nutrition Transition: Measuring rapid dietary changes in transitional countries. Public Health Nutrition, 2002, 5(6A):947-953.
108 World Bank World Development Report 2004: Making services work for poor people, London, Oxford University Press, 2003.
109 Popkin, B., Horton, S., Kim, S. The Nutritional Transition and Diet Related Chronic Diseases in Asia Food Consumption and Nutrition Division Discussion paper 105, Washington DC, International Food Policy Research Institute, 2001.
110 Abdul-Rahim, H. F. et al. The Metabolic Syndrome in the West Bank Population- an urban-rural comparison. Diabetes Care, 2001, 24:275-279.
111 Inoue, S., Zimmet, P., Bassett, J. The Asia Pacific Perspective: redefining obesity and its treatment, Sydney, Health Communications Australia Pty Ltd 2000 and Hughes, R. Diet, Food Supply and Obesity in the Pacific, Geneva, WHO 2003.
112 Inoue, S., Zimmet, P., Bassett, J. The Asia Pacific Perspective: redefining obesity and its treatment, Sydney, Health Communications Australia Pty Ltd 2000.
113 Inoue, S., Zimmet, P., Bassett, J. The Asia Pacific Perspective: redefining obesity and its treatment, Sydney, Health Communications Australia Pty Ltd 2000.
114 Davis, J. et al. The Relationship between Ethnicity and Obesity in Asian and Pacific Islander Populations: A literature review. Ethnicity and Disease, 2004, 14(1):111-118.
115 (No Author listed) “Filling the World’s Belly” The Economist 11 De-cember 2003 http://www.economist.com/printerfriendly.cfm?Story_ID=2261775 (last accessed 18 August 2005).
116 Hughes, R. Diet, Food Supply and Obesity in the Pacific, Geneva, WHO 2003.117 Bakker, B. Consumer Preferences in Hong Kong on Western Foods, Hong Kong,
United States of America Department of Agriculture/Asian Commer-cial Research Ltd, 2000.
118 Hughes, R. Diet, Food Supply and Obesity in the Pacific, Geneva, WHO 2003.119 Purdy, M., Banks, D (eds.) Health and Exclusion, London, Routledge, 1999.120 James, W. et al. Socioeconomic Determinants of Health: The Contribu-
tion of Nutrition to Inequalities in Health. British Medical Journal (24 May 1997) 314:1545-1550.
121 Boulton, T. et al. Profile of heart disease risk factors and their relation to parents’ education, fathers’ occupation and family history of heart disease in 843 South Australian Families: The Adelaide Children’s WHO Collaborative Study. Journal of Paediatrics and Child Health, 1995,
31:200-206.122 O’Dea, J. Differences in overweight and obesity among Australian
school children of low and middle/high socioeconomic status. Medical Journal of Australia, 2003, 179(1):63.
123 Cameron, A. et al. Overweight and obesity in Australia: the 1999-2000 Australian diabetes, obesity and lifestyle study. Medical Journal of Australia, 2003, 178(9):427-432
124 Monteiro, C. et al. Socioeconomic Status and Obesity in Adults of Developing Countries: a review. Bulletin of the World Health Organization, 2004, 82:940-946.
125 See, for example, Wu Fan, Situation and Strategy of Noncommunicable Disease Control and Prevention in China Beijing , National Center for Chronic and Noncommunicable Disease Control and Prevention, China Center for Disease Control and Prevention, 2003.
126 Pan American Health Organization/WHO Public Health response to Chronic Diseases (130th Session of the Executive Committee) [CE130/17] Washington DC, 24-28 June 2002 http://www.paho.org/english/gov/ce/ce130-17-e.pdf (last accessed 25 August 2005).
127 Peña, M. and Bacallo, J. Obesity and Poverty- a new public health challenge, Washington DC, Pan American Health Organisation, 2000 (Scientific Publication 576).
128 Puska, P. et al. Globalization, Diets and Noncommunicable Diseases, Geneva, WHO, 2002.
129 New Policy Institute/Joseph Rowntree Foundation http://www.poverty.org.uk/summary/key_facts.htm (last accessed 18th August 2005).
130 Sturgis, P., Jackson, J. Examining Participation in Sporting and Cultural Activities: Analysis of the UK 2000 Time Use Survey Phase 2 London, United Kingdom Department for Culture, Media and Sport, November 2003.
131 Jones-Webb, R. et al. 2002 The Effects of Socioeconomic Position on Black-White Crossover Effects in CVD Mortality, Presentation at the 2002 University of Minnesota Maternal and Child Health Program’s Summer Institute: “Strategies for Addressing Health Disparities.” http://www.epi.umn.edu/mch/summer/SummerInstitute/presentations/rhonda.ppt#2 (last accessed 23rd August 2005).
132 National Heart, Lung and Blood Institute (US) & National Institutes of Health Report on the Conference on Socioeconomic Status and Cardiovascular Health and Disease 6-7 November 1995 http://www.nhlbi.nih.gov/re-sources/docs/ses.txt (last accessed 18 August 2005).
133 Wielgosz, A. Surveillance at work: Zeroing in on cardiovascular dis-eases in regional health units across Canada. Canadian Journal of Cardiology, October 2003, 19(11):1239-1240.
134 Puska, P. et al. Globalization, Diets and Noncommunicable Diseases, Geneva, WHO, 2002 and Brands, A., Yach D. Women and the Rapid Rise of Noncommunicable Diseases, Geneva, WHO, 2002.
135 Yach, D. et al. Noncommunicable diseases, prevention and control of a global epidemic- report of a WHO consultation, Geneva, September 27-30 1999 (Draft 5) 9 August 2001 http://www.hpclearinghouse.ca/downloads/MACLEAN2.doc (last accessed 25 August 2005).
136 Leeder, S. et al. A Race Against Time: The Challenge of Cardiovascular Disease in Devel-oping Economies, New York, Trustees of Columbia University, 2004.
Endn
otes
The Need for Pro-poor Strategies in the Western Pacific Region: A Review
81
137 Puska, P. et al. Globalization, Diets and Noncommunicable Diseases, Geneva, WHO, 2002.
138 Unwin, N. Taking Poverty to Heart. Noncommunicable diseases and the poor http://www.id21.org/zinter/id21zinter.exe?a=0&i=InsightsHealth%231Editorial&u=43095b04 Insights Health 2003 (last accessed 22 August 2005).
139 Mbanya, J. C. Class Divide: Education and NCD Risk Factors in Cameroon http://www.id21.org/insights/insights-h01/insights-issh01-art04.html Insights Health 2001 (last accessed 18 August 2005).
140 Hodgkins, B.J., Manring, E,. Meyers, M. Demographic, Social and Stress Correlates of Hypertension among the Urban Poor. Family Practice, 1990, 7(4):261-6.
141 Bovet, P. et al. Monitoring one-year compliance to antihypertension medication in the Seychelles. Bulletin of the World Health Organization, 2002, 80:33-39.
142 Nishi, N. et al. Effects of socioeconomic indicators on coronary risk factors, self-rated health and psychological well-being among urban Japanese civil servants. Social Science and Medicine, 2004, 58:1159-1170.
143 Turrell, G. et al. Socioeconomic Determinants of Health: towards a national research program and a policy and intervention agenda, Canberra, Queensland University of Technology, School of Public Health, Ausinfo, 1999.
144 Bennett, S. Socioeconomic Inequalities in Coronary Heart Disease and Stroke Mortality Among Australian Men 1979-1993. International Journal of Epidemiology, 1996, 25:266-275.
145 Centers for Disease Control and Prevention, Diabetes among His-panics, Los Angeles County, California, 2002-2003. Morbidity and Mortality Weekly Review, November 28, 2003, 52(47):1152-1155.
146 Herman, W.H., Smith, P.J., Thompson, T.J., Engelgau, M.M., and Aubert R.E.. A new and simple questionnaire to identify people at increased risk for undiagnosed diabetes. Diabetes Care, 1995, 18:382-387.
147 Gulliford, M., Mahabir, D. Social inequalities in morbidity from Diabe-tes Mellitus in public primary care clinics in Trinidad and Tobago. Social Science and Medicine, 46(1):137-144.
148 Puska, P. et al. Globalization, Diets and Noncommunicable Diseases, Geneva, WHO, 2002.
149 Centers for Disease Control and Prevention, Socioeconomic status of Women with Diabetes - United States of America 2000. Morbidity and Mortality Weekly Report, Feb 22 2002; 51(7):107-108 & 159.
150 WHO/WPRO Prevention and Control of Noncommunicable Diseases (Regional Committee 51st Session, Manila, 18-22 September 2000) [WPR/RC51/8], Manila, WHO, 2000.
151 Johnson, K. W. et al. Macrosocial and Environmental Influences on Minority Health. Health Psychology, 1995, 14(7):601-612.
152 Brewis, A. et al. Gender and Noncommunicable Disease in the Pacific. Pacific Health Dialog, March 1996, 3(1):107-113.
153 Puska, P. et al. Globalization, Diets and Noncommunicable Diseases, Geneva, WHO, 2002.
154 Puska, P. et al. Globalization, Diets and Noncommunicable Diseases, Geneva, WHO, 2002.
155 Nishi, N. et al. Effects of socioeconomic indicators on coronary risk factors, self-rated health and psychological well-being among urban Japanese civil servants. Social Science and Medicine, 2004, 58:1159-1170.
156 WHO/WPRO The Work of the WHO in the Western Pacific Region- Report of the Regional Director 1 July 1999- 30 June 2000, Manila, WPRO, 2000.
157 Puska, P. et al. Globalization, Diets and Noncommunicable Diseases, Geneva, WHO, 2002.
158 Ross, H. Lifting the Unequal Burden of Cancer on Minorities and the Underserved. Closing the Gap- newsletter of the Office of Minority health, US Department of Health and Human Services, August 2000 p1-16.
159 Harvard Center for Cancer Prevention, Socioeconomic Status. in Harvard Reports on Cancer Prevention Volume 1: Human Causes of Cancer Rapid Science Publishers 1996 http://www.hsph.harvard.edu/cancer/publi-cations/reports/vol1_full_text/print_ready/socio.html (last accessed 18 August 2005).
160 Burnley, I.H. Disadvantage and Male Cancer Incidence and Mortality in NSW 1985-1993. Social Science and Medicine, 1997, 45:465-476.
161 Burnley, I.H. Mortality from Respiratory System Cancer in NSW and Sydney. Australian Journal of Public Health, 1992, 16:251-261.
162 Chaloupka, F. et al. The Evidence Base for Reducing Mortality from Smoking in Low and Middle Income Countries CMH Working Paper Series Paper No: WG5:7 (2001) http://www3.who.int/whosis/cmh/cmh_papers/e/pdf/wg5_pa-per07.pdf (last accessed 29 August 2005).
163 WHO/WPRO Prevention and Control of Noncommunicable Diseases (Regional Com-mittee 51st Session, Manila 18-22 September 2000) [WPR/RC51/8], Manila, WHO, 2000.
164 WHO/WPRO Prevention and Control of Noncommunicable Diseases (Regional Com-mittee 51st Session, Manila 18-22 September 2000) [WPR/RC51/8], Manila, WHO, 2000.
165 Centers for Disease Control and Prevention NCHS Data on Chronic Obstructive Pulmonary Disease (undated) http://www.cdc.gov/nchs/data/factsheets/copd.pdf (last accessed 18 August 2005).
166 Mathers, C. Health Differentials among Adult Australians aged 25-64 Years, Canberra, Commonwealth Government Publishing Service, 1994.
167 Preker, A.S. et al. Sector Strategy: Health, Nutrition and Population, Washington DC, World Bank, 1997.
168 McClelland, A., Pirkis, J., Willcox, S. Enough to Make You Sick- how income and environment affect health, Melbourne, National Health Strategy Research Paper No. 1 September 1992.
169 Wagstaff, A. Poverty and Health Sector Inequalities. Bulletin of the World Health Organisation, 2002, 80(2):97-105
170 Leon, D., Walt, G.(eds) Poverty, Inequality and Health- an international perspective, New York, Oxford University Press, 2000.
171 Evans, T. et al. Summary of the book: Challenging Inequalities in Health, New York, Oxford University Press, 2001 http://www.rockfound.org/Docu-ments/435/summary_challenging.pdf (last accessed 29 August 2005).
172 Purdy, M., Banks, D (eds.) Health and Exclusion, London, Routledge, 1999.173 Kern, A., Ritzen, J. Dying for Change- Poor People’s Experience of Health and Ill-health,
Washington DC, WHO/World Bank, 2001.174 Peabody, J. W. et al. Policy and Health- implications for development in Asia, New
York, Cambridge University Press, 1999.175 Purdy, M., Banks, D (eds.) Health and Exclusion, London, Routledge, 1999.176 Gwatkin, D. Inequalities in Access to Health Care in Developing Countries: What Should
Be Done? HNP and Poverty Seminar Report, World Bank, 21 March
Endn
otes

Noncommunicable Disease and Poverty
82
2001 http://www1.worldbank.org/prem/poverty/health/library/gwat-kin4.pdf (last accessed 25 August 2005).
177 Pruitt, S. et al. Innovative Care for Chronic Conditions- building blocks for action, Geneva, WHO, 2002.
178 Raphael, D. Inequality is Bad for Our Hearts: why low income and social exclusion are major causes of heart disease in Canada, Toronto, North York Heart Health Network, 2001.
179 Purdy, M., Banks, D (eds.) Health and Exclusion, London, Routledge, 1999.180 Reidpath, D. et al. An ecological study of the relationship between
social and environmental determinants of obesity. Health and Place, 2002, 8(2):141-145.
181 Shariif, I. The Socioeconomic Implications of AIDS in Developing Countries in General and Africa in Particular (undated) http://www.uwmc.uwc.edu/csepa/mhall/IGS/Plagues/TextPages/globalimplications.htm (last accessed 18 August 2005).
182 Economics and Development Resource Centre Handbook for the Economic Analysis of Health Sector Projects, Manila, Asian Development Bank, 2000.
183 WHO Department of Health in Sustainable Development Partnership in health and Poverty: Towards a Common Agenda- report of an international meeting WHO HQ Geneva 12-14 June 2000, Geneva, WHO, 2001.
184 Ait-Khaled, N., Enarson, D., Bousquet, J. Chronic Respiratory Diseases in Developing Countries: The Burden and Strategies for Prevention and Management. Bulletin of the World Health Organization, 2001, 79:971-979.
185 WHO European Regional Office Poverty and Health- Evidence and Action in WHO’s European Region (Regional Committee for Europe 52nd Session, Copenhagen 16-19 September 2002) [EUR/RC52/8] http://www.euro.who.int/Document/RC52/edoc8.pdf (last accessed 29 August 2005).
186 Gwatkin, D. Reducing Health Inequalities in Developing Countries, Washington DC, The World Bank 2002.
187 Medically indigent is a person who is unable to meet their medical bills. This may either be a result of poverty or a person with gener-ally adequate income who is suddenly facing catastrophically high medical bills.
188 Pan American Health Organization/WHO Public Health response to Chronic Diseases (130th Session of the Executive Committee) [CE130/17] Washington DC, 24-28 June 2002 http://www.paho.org/english/gov/ce/ce130-17-e.pdf (last accessed 25 August 2005).
189 Henry-Lee, A., Yearwood, A. Protecting the poor and the medically indigent under health insurance: A case study of Jamaica, Bethesda , Partnerships for Health Reform, 1999.
190 Peabody, J. W. et al. Policy and Health- implications for development in Asia, New York, Cambridge University Press, 1999.
191 Department for International Development Disability, poverty and develop-ment ID21 Highlights, January 2002 http://www.soziologie.ch/users/markus/health/docs/5%20Other%20documents/5.16_Disability_Pov-erty_and_Development.pdf (last accessed 18 August 2005).
192 Adhikari, R., Gertler, P., Lagman, A. Economic Analysis of Health Sector Projects- a review of issues, methods and approaches, Manila, Asian Development Bank,
1999.193 Bradley, C., Given, C., Roberts, C. Race, Socioeconomic Status, and
Breast Cancer Treatment and Survival. Journal of the National Cancer Institute, 2002, 94(7):490-96.
194 Pell, J. et al. Effect of Socioeconomic deprivation on waiting time for cardiac surgery: respective cohort study. British Medical Journal, 2000, 320:15-19.
195 McAlister, F et al. Influence of socio-economic deprivation on the primary care burden and treatment of patients with a diagnosis of heart failure in General Practice in Scotland: Population based Study. British Medical Journal, 2004, 328:1110.
196 Al Serouri, A. W., Balabanova, D., Al-Hibshi, S., Cost Sharing for Primary Health Care London, Oxfam (undated) http://www.oxfam.org.uk/what_we_do/resources/downloads/wp_yemen/wp_yemen_4discuss.pdf (last accessed 18 August 2005).
197 National Aboriginal Community Controlled Health Organisation Australia Estimation of Requirements for and Supply of The Health Workforce for Aboriginal and Torres Strait Islander Peoples, Canberra, Office of Aboriginal and Torres Strait Islander Health, 2000.
198 Purdy, M., Banks, D (eds.) Health and Exclusion, London, Routledge, 1999.199 Atri, J. et al. Fair Shares in Health Care? Ethnic and Socioeconomic
influences on recording of preventive care in selected inner London general practices. British Medical Journal, 1996 312:614-617
200 Brown, A. et al. Socioeconomic position and health among persons with Diabetes Mellitus: a conceptual framework and a review of the literature. Epidemiological Review, 2004, 26:63-77.
201 Kern, A., Ritzen, J. Dying for Change- Poor People’s Experience of Health and Ill-health, Washington DC, WHO/World Bank, 2001.
202 WHO European Regional Office Poverty and Health- Evidence and Action in WHO’s European Region (Regional Committee for Europe 52nd Session, Copenhagen 16-19 September 2002) [EUR/RC52/8] http://www.euro.who.int/Document/RC52/edoc8.pdf (last accessed 29 August 2005).
203 WHO Department of Health in Sustainable Development Partnership in health and Poverty: Towards a Common Agenda- report of an international meeting WHO HQ Geneva 12-14 June 2000, Geneva, WHO, 2001.
204 WHO European Regional Office Poverty and Health- Evidence and Action in WHO’s European Region (Regional Committee for Europe 52nd Session, Copenhagen 16-19 September 2002) [EUR/RC52/8] http://www.euro.who.int/Document/RC52/edoc8.pdf (last accessed 29 August 2005).
205 Oxfam, Cut the Cost- Patent Injustice: how world trade rules threaten the health of poor people 2001 http://www.oxfam.org.uk/what_we_do/issues/health/downloads/patentinjustice.pdf (last accessed 25 August 2005).
206 Oxfam, Cut the Cost- Patent Injustice: how world trade rules threaten the health of poor people 2001 http://www.oxfam.org.uk/what_we_do/issues/health/downloads/patentinjustice.pdf (last accessed 25 August 2005).
207 Oxfam, Cut the Cost- Patent Injustice: how world trade rules threaten the health of poor people 2001 http://www.oxfam.org.uk/what_we_do/issues/health/downloads/patentinjustice.pdf (last accessed 25 August 2005).
208 Oxfam, Cut the Cost- Patent Injustice: how world trade rules threaten the health of
Endn
otes

The Need for Pro-poor Strategies in the Western Pacific Region: A Review
83
poor people 2001 http://www.oxfam.org.uk/what_we_do/issues/health/downloads/patentinjustice.pdf (last accessed 25 August 2005).
209 Kern, A., Ritzen, J. Dying for Change- Poor People’s Experience of Health and Ill-health, Washington DC, WHO/World Bank, 2001.
210 Kern, A., Ritzen, J. Dying for Change- Poor People’s Experience of Health and Ill-health, Washington DC, WHO/World Bank, 2001.
211 Wagstaff, A. The Contribution of High Health Care Costs to Impoverishment HNP and Poverty Seminar Report, World Bank, 6 September 2000 http://www1.worldbank.org/prem/poverty/health/library/wagstaf3.pdf (last accessed 25 August 2005).
212 Wagstaff, A. The Contribution of High Health Care Costs to Impoverishment HNP and Poverty Seminar Report, World Bank, 6 September 2000 http://www1.worldbank.org/prem/poverty/health/library/wagstaf3.pdf (last accessed 25 August 2005).
213 Derived from Evans, T. et al. World Health Report 2003 WHO, Geneva 2003.214 WPRO STI HIV/AIDS Surveillance Report, August 2000, 15:1-8.215 WHO/WPRO Prevention and Control of Noncommunicable Diseases (Regional Com-
mittee 51st Session, Manila 18-22 September 2000) [WPR/RC51/8], Manila, WHO, 2000.
216 Derived from Evans, T. et al. World Health Report 2003 WHO, Geneva 2003.217 Australian Health Ministers’ Advisory Council Preventing Chronic Disease: A
strategic framework Melbourne, National Public Health Partnership, 2001.218 Australian Health Ministers’ Advisory Council Preventing Chronic Disease: A
strategic framework Melbourne, National Public Health Partnership, 2001.219 McClelland, A., Pirkis, J., Willcox, S. Enough to Make You Sick- how income and
environment affect health, Melbourne, National Health Strategy Research Paper No. 1 September 1992.
220 Mathers, C., Vos, S. Stevenson, C. The Burden of Disease and Injury in Australia Canberra, Australian Institute of Health and Welfare, 1999.
221 Australian Health Ministers’ Advisory Council Preventing Chronic Disease: A strategic framework Melbourne, National Public Health Partnership, 2001.
222 Ross, H. Lifting the Unequal Burden of Cancer on Minorities and the Underserved. Closing the Gap- newsletter of the Office of Minority health, US Department of Health and Human Services August 2000 p1-16.
223 Yach, D. et al. Noncommunicable diseases, prevention and control of a global epidemic- report of a WHO consultation, Geneva, September 27-30 1999 (Draft 5) 9 August 2001 http://www.hpclearinghouse.ca/downloads/MACLEAN2.doc
(last accessed 25 August 2005).224 Pamuk, E. et al. Socioeconomic status and health chartbook, Hyattsville, National
Centre for Health Statistics, 1998.225 Ghaffar, A., Srinath Reddy, K., Singhi, M. Burden of Noncommunicable
Diseases in South Asia. British Medical Journal, 2004, 328: 807-810.226 Misra, R. Pro-poor Health Reforms, Why, What and How? Geneva, WHO, 2003.227 Low, A., Ithindi, T., Low, A. A Step Too Far: Making Health Equity
Interventions in Namibia More Sufficient. International Journal for Equity in Health, 2003, 2:5
228 Grosh, M. Administering Targeted Social programs in Latin America: From platitudes to practice, Aldershot, Ashgate Publishing Ltd, 1996.
229 Ziglio, E. et al. (eds.) Health Systems Confront Poverty, Copenhagen, World Health Organization European Office, 2003.
230 WHO Health and Sustainable Development Department Health and Poverty Reduction- an informal consultation with selected development partners, Geneva 7-8 September 1999 Summary Report, Geneva , WHO, 1999 http://www.cct-freiburg.de/who/pro_poor/documents/informalcons.pdf (last accessed 5 September 2005).
231 Leon, D., Walt, G. (eds.) Poverty, Inequality and Health- an international perspective, New York, Oxford University Press, 2001.
232 Low, A., Ithindi, T., Low, A. A Step Too Far: Making Health Equity Interventions in Namibia More Sufficient. International Journal for Equity in Health, 2003, 2:5 and Wagstaff, A. Poverty and Health Sector Inequali-ties. Bulletin of the World Health Organisation, 2002, 80(2):97-105.
232 WPRO Health Financing and Social Protection: Current Issues http://www.wpro.who.int/sites/hcf/issues.htm (last accessed 18 August 2005).
234 Wagstaff, A. Poverty and Health Sector Inequalities. Bulletin of the World Health Organisation, 2002, 80(2):97-105.
235 Wagstaff, A. Poverty and Health Sector Inequalities. Bulletin of the World Health Organisation, 2002, 80(2):97-105.
236 Lie RK. Human rights, equity and health sector reform (Final Report). May, 2000 (un-published document), http://www.hf.uib.no/i/filosofisk/ethica/rights22.pdf (last accessed 22 August 2005).
237 WHO Department of Health in Sustainable Development Partnership in health and Poverty: Towards a Common Agenda- report of an international meeting WHO HQ Geneva 12-14 June 2000, Geneva, WHO, 2001.
Endn
otes
www.wpro.who.int