Non Traumatic Emergent Neuroradiology
17
AJR:191, September 2008 S1 AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY Nontraumatic Emergent Neuroradiology: Review and Self-Assessment Module Yoshimi Anzai 1 and Basavaraj Ghodke 2 Keywords: brain imaging, case-based learning, emergency, neuroradiology, self-assessment DOI:10.2214/AJR.07.7042 Received September 7, 2007; accepted after revision January 30, 2008. 1 Department of Radiology, Division of Neuroradiology, University of Washington, 1959 NE Pacific St., NW 011, Box 357115, Seattle, WA 98195-7115. Address correspondence to Y. Anzai ([email protected]). 2 Department of Radiology, Harborview Medical Center, Seattle, WA. AJR 2008;191:S1–S17 0361–803X/08/1913–S1 © American Roentgen Ray Society ABSTRACT Objective The educational objectives for this case-based self-assess- ment module on imaging of nontraumatic emergent neuro- radiology are to use case examples to teach the imaging features of CT and MRI of emergent neuroradiologic diag- noses and to improve the reader’s understanding of the pathophysiology and clinical management of each clinical scenario. Imaging plays a critical role in assessing patients with acute neurologic symptoms. CT is quick and easy to perform in an emergency setting and is often the technique of choice for any neurologic emergency situations. Clinical correlation is crucial for accurate diagnosis and triaging pa- tients for further evaluation. Persistent or progressive neu- rologic symptoms despite negative CT should prompt other imaging studies. Conclusion At the end of this self-assessment module, readers will be able to generate a concise list of differential diagnoses for imaging findings that often are encountered in patients with nontraumatic neurologic emergency. INTRODUCTION This self-assessment module on nontraumatic emergent neuroradiology diagnoses has an educational component and a self-assessment component. The educational compo- nent consists of six case scenarios that the participant should work through and four recommended articles that may provide additional information and perspective. The self-assessment component consists of 19 multiple-choice questions with solutions. All of these materials are avail- able on the ARRS Website (www.arrs.org). To claim CME and SAM credit, each participant must enter his or her re- sponses to the questions online. EDUCATIONAL OBJECTIVES By completing this educational activity, the participant will: A. Exercise, self-assess, and improve his or her understand- ing of the imaging features of nontraumatic emergent neuroradiology diagnoses. B. Exercise, self-assess, and improve his or her understand- ing of the clinical features of nontraumatic emergent neuroradiology diagnoses. RECOMMENDED READING 1. Provenzale JM. Centennial dissertation. Honoring Ar- thur W. Goodspeed, MD and James B. Bullitt, MD. CT and MR imaging and nontraumatic neurologic emergen- cies. AJR 2000; 174:289–299 2. Wintermark M, Albers GW, Alexandrov AV, et al. Acute stroke imaging research roadmap. Stroke 2008; 39: 1621–1628 3. Beauchamp NJ Jr, Bryan RN. Acute cerebral ishemic infarction: a pathophysiologic review and radiologic per- spective. AJR 1998; 171:73–84 4. Zuccoli G, Gallucci M, Capellades J, et al. Wernicke en- cephalopathy: MR findings at clinical presentation in twenty-six alcoholic and nonalcoholic patients. AJNR 2007; 28:1328–1331 INSTRUCTIONS 1. Complete the educational and self-assessment components. 2. Visit www.arrs.org and select Publications/Journals/ SAM Articles from the left-hand menu bar. 3. Using your member login, order the online SAM as di- rected. 4. Follow the online instructions for entering your respons- es to the self-assessment questions and complete the test by answering the questions online.
-
Upload
oralboards -
Category
Documents
-
view
110 -
download
1
description
Nontraumatic Emergent Neuroradiology
Transcript of Non Traumatic Emergent Neuroradiology

AJR:191, September 2008 S1
AJR Integrative Imaging
LIFELONG LEARNING FOR RADIOLOGY
Nontraumatic Emergent Neuroradiology: Review and Self-Assessment ModuleYoshimi Anzai1 and Basavaraj Ghodke2
Keywords: brain imaging, case-based learning, emergency, neuroradiology, self-assessment
DOI:10.2214/AJR.07.7042
Received September 7, 2007; accepted after revision January 30, 2008.1Department of Radiology, Division of Neuroradiology, University of Washington, 1959 NE Pacific St., NW 011, Box 357115, Seattle, WA 98195-7115. Address correspondence to Y. Anzai ([email protected]).2Department of Radiology, Harborview Medical Center, Seattle, WA.
AJR 2008;191:S1–S17 0361–803X/08/1913–S1 © American Roentgen Ray Society
AbstrAct
ObjectiveThe educational objectives for this case-based self-assess-
ment module on imaging of nontraumatic emergent neuro-radiology are to use case examples to teach the imaging features of CT and MRI of emergent neuroradiologic diag-noses and to improve the reader’s understanding of the pathophysiology and clinical management of each clinical scenario. Imaging plays a critical role in assessing patients with acute neurologic symptoms. CT is quick and easy to perform in an emergency setting and is often the technique of choice for any neurologic emergency situations. Clinical correlation is crucial for accurate diagnosis and triaging pa-tients for further evaluation. Persistent or progressive neu-rologic symptoms despite negative CT should prompt other imaging studies.
conclusionAt the end of this self-assessment module, readers will be
able to generate a concise list of differential diagnoses for imaging findings that often are encountered in patients with nontraumatic neurologic emergency.
INtrODUctIONThis self-assessment module on nontraumatic emergent
neuroradiology diagnoses has an educational component and a self-assessment component. The educational compo-nent consists of six case scenarios that the participant should work through and four recommended articles that may provide additional information and perspective. The self-assessment component consists of 19 multiple-choice questions with solutions. All of these materials are avail-able on the ARRS Website (www.arrs.org). To claim CME and SAM credit, each participant must enter his or her re-sponses to the questions online.
EDUcAtIONAL ObJEctIVEsBy completing this educational activity, the participant will:A. Exercise, self-assess, and improve his or her understand-
ing of the imaging features of nontraumatic emergent neuroradiology diagnoses.
B. Exercise, self-assess, and improve his or her understand-ing of the clinical features of nontraumatic emergent neuroradiology diagnoses.
rEcOMMENDED rEADING1. Provenzale JM. Centennial dissertation. Honoring Ar-
thur W. Goodspeed, MD and James B. Bullitt, MD. CT and MR imaging and nontraumatic neurologic emergen-cies. AJR 2000; 174:289–299
2. Wintermark M, Albers GW, Alexandrov AV, et al. Acute stroke imaging research roadmap. Stroke 2008; 39: 1621–1628
3. Beauchamp NJ Jr, Bryan RN. Acute cerebral ishemic infarction: a pathophysiologic review and radiologic per-spective. AJR 1998; 171:73–84
4. Zuccoli G, Gallucci M, Capellades J, et al. Wernicke en-cephalopathy: MR findings at clinical presentation in twenty-six alcoholic and nonalcoholic patients. AJNR 2007; 28:1328–1331
INstrUctIONs1. Complete the educational and self-assessment components.2. Visit www.arrs.org and select Publications/Journals/
SAM Articles from the left-hand menu bar.3. Using your member login, order the online SAM as di-
rected.4. Follow the online instructions for entering your respons-
es to the self-assessment questions and complete the test by answering the questions online.

Anzai and Ghodke
S2 AJR:191, September 2008
scenario 1Clinical History
A 32-year-old man presented to the emergency depart-ment complaining of headache and general fatigue. He was diagnosed with a viral syndrome and discharged with symp-tomatic treatment. Two weeks later he presented to the emergency department with severe headache and confusion. He was afebrile but his mental status had changed since his previous emergency department visit. A working diagnosis of bacterial meningitis was considered. The patient denied any focal weakness or sensory or visual changes.
Unenhanced CT (Fig. 1A) and CT angiography (Fig. 1B) of the head were performed. The patient also underwent cerebral angiography (Figs. 1C and 1D).
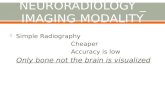
Description of ImagesUnenhanced CT of the head showed a large right frontal
intraparenchymal hematoma with surrounding edema, likely representing a subacute intracranial hematoma. CT
angiography did not reveal any cerebral aneurysms, arte-riovenous malformation, or enhancing focus as possible causes of a hematoma. Cerebral angiography showed ir-regularity of small- to medium-sized vessels and a beaded appearance, consistent with vasculitis. The patient admit-ted that he smoked marijuana almost daily and had a long history of amphetamine use.
QUEstION 2
Which one of the following is NOT associated with vasculitis?
A. Polyarteritis nodosa.B. Tuberculosis.C. Systemic lupus erythematosus.D. Drugs (amphetamine, cocaine).E. Marfan syndrome.
QUEstION 3
What is the most definitive test for diagnosing CNS vasculitis?
A. CT angiography with 3D volume rendering.B. Cerebral angiography.C. Biopsy.D. MR angiography.E. Transcranial Doppler sonography.
QUEstION 1
Which of the following is the preferred diagnosis?
A. Arteriovenous malformation.B. Hypertensive hemorrhage.C. Hemorrhagic tumor or metastasis.D. Vasculitis.E. Amyloid angiopathy.
A
Fig. 1—32-year-old man with headache and general fatigue who was diagnosed with viral syndrome and discharged but returned with severe headache and confusion.A and B, Unenhanced CT (A) and CT angiography (B) of head were performed. Unenhanced CT shows large right frontal intraparenchymal hematoma and surrounding edema (arrow, A), likely representing subacute intracranial hematoma. CT angiography does not reveal any cerebral aneurysms, arteriovenous malformation, or en-hancing focus as possible cause of hematoma.C and D, Cerebral angiography shows irregularity of small- to medium-sized vessels (arrows, D) and beaded appearance, consistent with vasculitis. Patient admitted that he smokes marijuana almost daily and has long history of amphetamine use.
D
c
b

AJR:191, September 2008 S3
Nontraumatic Emergent Neuroradiology
Solution to Question 1Arteriovenous malformation (AVM) is not an unusual cause
of intracranial hematoma for the young patient in this case. Patients with AVM often present with acute intracranial hem-orrhage or ischemic symptoms due to steal phenomenon. CT angiography often reveals a tangle of markedly dilated arter-ies and veins with a nidus of AVM. If the AVM is small, it may not be visualized or diagnosed correctly with CT angiography. In this setting, cerebral angio graphy is the most definitive test. However, cerebral angio graphy in this patient did not show early venous filling or an abnormal tangle of blood vessels to indicate AVM. Therefore, option A is not the best response.
Acute intracranial hematoma can have a number of causes. The most common cause is hypertensive hemorrhage. Hy-pertensive hemorrhages, which originate from terminal small vessels, are often centered at the basal ganglia, particularly the putamen and the external capsule; the thalamus; the pons; and occasionally, the cerebellum. Lobar hemorrhage can be seen in a setting of hypertension (≈ 1–2%), but it is rare. Hypertensive hemorrhage is much more common in older patients. Option B is not the correct response.
Certain types of brain tumors are often associated with intracranial hemorrhage. These are often aggressive tumors, such as glioblastoma multiforme, or vascular tumors, such as metastases from renal cell carcinoma or melanoma, but rare-ly papillary thyroid cancer and choriocarcinoma. Lung can-cer and breast cancer are not considered vascular; however, the incidence of brain metastasis from lung and breast can-cers is exceedingly higher than that of other vascular can-cers. Thus, when all hemorrhagic brain metastases are re-viewed, lung and breast remain the two top primary choices. Intracranial hemorrhage associated with brain tumor often has a focal area of enhancement and significant mass effect or vasogenic edema. Option C is not the best response.
Vasculitis is one of the causes of intracranial hemorrhage and is more frequently seen in young patients. Vasculitis can present with acute hemorrhage or ischemic symptoms. Many causes of vasculitis affect small- to medium-sized vessels; therefore, CT angiography may not show an irregularity of the blood vessels as definitively as cerebral angiography. Cere-bral angiography in Figures 1C and 1D shows a classic ap-pearance of segmental narrowing and poststenotic dilatation involving multiple small- to medium-sized blood vessels, con-sistent with vasculitis. Option D is the best response.
Amyloid angiopathy often causes a lobar intracranial hemorrhage centered at the deep white matter in the frontal or parietal lobes. Amyloid angiopathy is much more common in elderly patients and is rare in young patients. Cerebral an-giography may not show any irregularity or narrowing. Am-yloid angiopathy is often diagnosed after excluding other causes in elderly patients. Option E is not the best response.
Solution to Question 2The causes of vasculitis are often divided into infectious
and noninfectious. Infectious causes include tuberculosis, fun-
gal infection, bacterial vasculitis, and HIV vasculitis. The fre-quent causes of noninfectious vasculitis are immune-mediated vasculitis such as rheumatoid arthritis and systemic lupus er-ythematosus, and granulomatous disease, such as Wegener’s granulomatosis and sarcoid, as well as giant cell arteritis (also called temporal arteritis). Drugs, particularly amphetamines and cocaine, are frequent causes of noninfectious vasculitis. An amphetamine causes inflammatory vasculitis with vascu-lar wall necrosis and subsequent hemorrhage. The pathologic features of amphetamine-related vasculitis are similar to those of polyarteritis nodosa. This patient had taken amphet-amines for several years. Cocaine, on the other hand, induces cerebral infarction or ischemia as well as hemorrhage by vaso-constrictive effect and increased platelet aggregation, rather than a vasculitis-type inflammation of the vessels [1]. Options A, B, C, and D are not the best responses.
Marfan syndrome is an autosomal dominant disorder of the connective tissue characterized by disproportionally long limbs and tall stature. It affects the heart and aorta and causes aortic root dilatation, aortic regurgitation, and dissection. However, involvement of CNS vessels is unusual. Option E is the best response.
Solution to Question 3Because many cases of vasculitis affect small to medium-
sized blood vessels, MR angiography is relatively insensitive for the diagnosis of CNS vasculitis. CT angiography is less accurate than cerebral angiography. Cerebral angiography is used as the gold standard for diagnosis at many institutions. When characteristic angiographic findings such as alternat-ing areas of stenosis and dilatation or a beading appearance are observed in multiple vessels and multiple vascular beds, cerebral angiography is diagnostic. However, angiography can be normal in up to 40% of biopsy-proven cases. Thus, negative cerebral angiography does not completely exclude the diagnosis. Moreover, its specificity is not perfect. Intra-cranial atherosclerotic disease may show irregularity of mul-tiple vessels, mimicking CNS vasculitis.
Transcranial Doppler sonography is used to characterize the morphology of the superficial temporal artery as a screening tool for temporal arteritis. However, transcranial Doppler sonography is not suitable to evaluate arteries fully to diagnose CNS vasculitis. Options A, B, D, and E are not the best responses.
Biopsy of CNS tissue would logically be considered the ultimate gold standard of diagnosis, but clearly the proce-dure is limited by several factors. It is highly invasive and carries certain risks. Successful biopsy requires a willing and experienced neurosurgeon, who may not be readily available. Sampling error could result in limited sensitivity. The site of biopsy should be tailored to the individual pa-tient [2]. The biopsy of the superficial temporal artery is often performed in patients suspected of having giant cell vasculitis. The false-negative rate of biopsy for a diagnosis of vasculitis has been reported to be 16%, yielding a sensi-

Anzai and Ghodke
S4 AJR:191, September 2008
scenario 2Clinical History
A 19-year-old woman presented to an outside hospital with severe headache, nausea, vomiting, and photophobia. She had no significant medical history. Laboratory examinations were unremarkable. Her initial head CT scans (unenhanced and contrast-enhanced) are shown in Figures 2A and 2B.
Description of ImagesUnenhanced CT of the head showed a focal area of low
attenuation in the left temporal lobe and mild regional mass effect. The ventricles were normal in size with no shift of midline structures. No parenchymal hemorrhage was evi-dent. The contrast-enhanced image showed the empty delta
sign (Fig. 2B). Brain MRI, including sagittal T1-weighted imaging (Fig. 2C), diffusion-weighted imaging (Fig. 2D), and apparent diffusion coefficient (ADC) mapping (Fig. 2E) were also performed at the outside hospital. The sagittal T1-weighted image showed an isointense clot along the su-perior sagittal sinus that was of concern for superior sagit-tal sinus thrombosis. The diffusion-weighted image showed no areas of restricted diffusion or ADC map abnormality. The patient’s mental status deteriorated at the outside hos-pital and she was transferred to the emergency department of our hospital, at which time she was unresponsive and obtunded, and her pupils were dilated. CT of the head was
tivity of 84% [2]. Therefore, the most definitive test is bi-opsy of the blood vessels. Option C is the best response.
ConclusionVasculitis involving the CNS presents diagnostic chal-
lenges to clinicians as well as radiologists. There are many causes, including infection, autoimmune disease, drug ex-
posure, radiation, and malignancies. Cerebral angiography is more sensitive than noninvasive vascular imaging (CT an-giography or MR angiography), but it is invasive and has limited sensitivity and specificity. Treatment of noninfec-tious vasculitis is long-term, high-dose immunosuppression, which causes profound morbidity as a result of opportunis-tic infection or organ failures.
QUEstION 4
What is your preferred diagnosis after the initial CT scans (Figs. 2A and 2B)?
A. Acute infarction of the left middle cerebral artery (MCA).
B. Herpes encephalitis.C. Underlying tumor.D. Sinus thrombosis.
QUEstION 5
Which one of the following techniques is LEAST appropriate to confirm a diagnosis of venous sinus thrombosis?
A. Rapid contrast-enhanced gradient-echo MRI with contrast-enhanced multiplanar imaging.
B. MDCT angiography or venography.C. Brain MRI and phase-contrast MR venography.D. Cerebral angiography.E. BrainMRIwithtime-of-flightMRvenography.
A
Fig. 2—19-year-old woman who presented to an-other hospital with severe headache, nausea, vomit-ing, and photophobia.A, Unenhanced CT scan of head obtained at outside hospital shows focal area of low attenuation in left temporal lobe and mild regional mass effect. Ventri-cles are normal in size with no shift of midline struc-tures. No parenchymal hemorrhage is evident.B, Contrast-enhanced image from other hospital shows empty delta sign (arrows).(Fig. 2 continues on next page)
b

AJR:191, September 2008 S5
Nontraumatic Emergent Neuroradiology
obtained immediately after her admission (Figs. 2F and 2G) and showed marked worsening of the cerebral edema and diffuse effacement of the cortical sulci and basilar cistern. In addition, a new focus of venous infarction and parenchy-mal hemorrhage was present in the left frontal lobe.
Solution to Question 4In the inferior aspect of the superior sagittal sinus on ini-
tial head CT was an area of high attenuation with a convex border that was of concern for superior sagittal sinus throm-bosis. Contrast-enhanced head CT showed lack of contrast enhancement in the superior sagittal sinus, the empty delta sign. Findings were consistent with venous sinus thrombo-sis and venous infarction involving the left temporal lobe. The patient had been taking oral contraceptives for the pre-vious 3 months.
CT findings of middle cerebral artery (MCA) infarction are loss of gray and white matter differentiation or presence
of an acute clot in the expected location of the proximal MCA (dense MCA sign). In this case, an area of low attenu-ation predominantly involved the white matter and spared the gray matter. In addition, diffusion-weighted imaging and the ADC map showed no area of restricted diffusion. Option A is not the best response.
QUEstION 6
Which one of the following is NOT associated with venous sinus thrombosis?
A. Sickle cell disease.B. Oral contraceptives.C. Cancer.D. Disseminated intravascular coagulation.E. Dehydration.
c
F
Fig. 2 (continued)—19-year-old woman who pre-sented to another hospital with severe headache, nausea, vomiting, and photophobia.C–E, Brain MR images, including sagittal T1-weight-ed (C), diffusion-weighted (D), and apparent diffu-sion coefficient (ADC) map (E) images obtained at outside hospital. T1-weighted image shows hyperin-tense clot along superior sagittal sinus (arrows), causing concern for superior sagittal sinus thrombo-sis. Diffusion-weighted images show no areas of restricted diffusion or ADC map abnormality.F and G, CT scans of head obtained immediately af-ter admission to our hospital show marked worsen-ing of cerebral edema and diffuse effacement of cortical sulci and basilar cistern. In addition, new focus of venous infarction and parenchymal hemor-rhage (arrow, F) is present in left frontal lobe.
ED
G

Anzai and Ghodke
S6 AJR:191, September 2008
Herpes encephalitis typically involves the medial tempo-ral lobe and is often associated with parenchymal hemor-rhage. This was the diagnosis made at the outside hospital, and the patient was treated with acyclovir. However, herpes encephalitis does not explain the presence of a clot in the superior sagittal sinus. Option B is not the best response.
The presence of tumor with vasogenic edema is also a possibility based on the area of low attenuation in the left temporal lobe. However, this does not explain the presence of a clot in the superior sagittal sinus. Option C is not the best response.
The correct diagnosis is venous sinus thrombosis and ve-nous infarction involving the left temporal lobe. Option D is the best response. The venous sinus can show slightly high attenuation, particularly among athletes, smokers, or neo-nates. The lateral border of the venous sinus, in these normal settings, should be concave, not convex toward the brain pa-renchyma. After the administration of contrast material, the dura may enhance but the venous sinus does not, giving the empty delta sign. Venous sinus thrombosis can be a challeng-ing diagnosis to make unless one has a high clinical suspicion. Patients present with nonspecific headache or confusion, and a clinical history of oral contraceptive use is often not avail-able to radiologists at the time of interpretation.
Sagittal T1-weighted MR images at the outside hospital showed lack of flow void along the superior sagittal sinus, highly suggestive of the diagnosis. Please note that diffu-sion-weighted images and the ADC map did not necessar-ily show an area of restrictive diffusion in the setting of venous infarction because increased venous pressure ini-tially causes vasogenic edema. This is distinctly different from arterial infarction, when the arterial supply to an area of the brain is abruptly terminated, resulting in cyto-toxic edema. Lack of diffusion signal change should not exclude venous infarction. However, venous infarction does progress to cytotoxic edema with restricted diffusion if the disease remains untreated.
Solution to Question 5The next diagnostic test to confirm venous sinus throm-
bosis is brain MRI with MR venography. On conventional MRI, venous sinus thrombosis may be suspected from lack of a flow void or high-signal thrombus in the dural sinuses. Lack of flow void is best appreciated on FLAIR or T2-weighted spin-echo images. Parenchymal changes, such as venous infarction or hemorrhage, along with lack of a flow void on conventional MRI raises the suspicion of venous sinus thrombosis. Superacute thrombus is relatively iso-intense on T1- and hypointense on T2-weighted images be-cause of deoxyhemoglobin potentially mimicking slow ve-nous flow on conventional MR images and thus requiring MR venography to confirm the diagnosis of venous sinus
thrombosis [3]. A subacute blood clot in the venous sinus is often seen as hyperintense on T1-weighted images as a re-sult of methemoglobin mimicking flowing blood on time-of-flight (TOF) MR venography. Phase-contrast MR venogra-phy is a fairly reliable test for the diagnosis of subacute venous sinus thrombosis.
Recently, rapid contrast-enhanced gradient-echo imag-ing has been reported to yield a higher diagnostic accuracy than 2D TOF MR venography [4, 5]. With advances in MDCT technology, CT angiography and venography have been increasingly used to diagnose venous sinus thrombo-sis and are considered a quick and reliable alternative to MR venography. Options A, B, C, and E, the appropriate next tests to confirm venous sinus thrombosis, are not the best responses.
Cerebral angiography also shows lack of flow in the dural venous sinuses. However, cerebral angiography is an inva-sive test that is associated with complication rates of 1–2%. Noninvasive imaging should be considered first to confirm the diagnosis of venous sinus thrombosis. Option D, which is the least appropriate technique, is the best response.
Solution to Question 6Common medical conditions associated with venous si-
nus thrombosis are pregnancy, a postpartum state, and hypercoagulable states such as sickle cell disease, oral con-traceptives use, and cancer. Dehydration often seen in neo-nates and elderly patients is associated with venous sinus thrombosis as a result of low-flow circulatory states. Ex-trinsic compression (tumor) or adjacent infection (mas-toiditis) is also a risk factor. Options A, B, C, and E are not the best responses.
Disseminated intravascular coagulation, however, is a hypocoagulable state and is not associated with venous si-nus thrombosis. Option D is the best response.
Venous sinus thrombosis is an underdiagnosed condition and can be a life-threatening disease if left untreated. Delay in diagnosis often leads to rapid deterioration and poor clin-ical outcomes. Intracranial hemorrhage is associated with 20–50% of cases of venous sinus thrombosis. Treatment for venous sinus thrombosis is immediate IV anticoagulation with low-molecular-weight heparin, despite the risk of hemorrhagic complications [6].
ConclusionVenous sinus thrombosis is an underdiagnosed condition
that can potentially lead to adverse clinical sequelae. Find-ings on contrast-enhanced CT or conventional T1-weighted sagittal images should make one suspicious in the appropri-ate clinical setting. Understanding the risk factors and med-ical history of patients will help to guide further diagnostic testing and immediate treatment.

AJR:191, September 2008 S7
Nontraumatic Emergent Neuroradiology
scenario 3Clinical History
A 48-year-old woman presented to the emergency de-partment with “the worst headache of my life” and a de-clining level of consciousness. No known medical history or medication use was noted. Unenhanced CT of head was first performed.
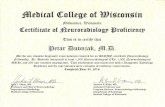
Description of ImagesUnenhanced head CT (Figs. 3A and 3B) showed diffuse
subarachnoid hemorrhage in the basilar cistern and sylvian fissures bilaterally and along the anterior falx, associated with intraventricular hemorrhage. The temporal horns of the lateral ventricle were mildly dilated, suggestive of de-
veloping hydrocephalus. Focal hematoma in the medial frontal region was also evident. The patient underwent CT angiography of head for further evaluation. Thin-slice maximum-intensity-projection (Fig. 3C) and 3D volume-rendering (Fig. 3D) images showed a lobulated saccular an-eurysm arising from the anterior communicating artery and measuring approximately 5 mm.
The proximal A2 segments of the anterior cerebral arter-ies were displaced laterally, likely due to the presence of he-matoma surrounding the aneurysm. Three-dimensional ro-tational angiography (Fig. 3E) showed detailed anatomy and morphology of the anterior communicating aneurysm and the adjacent ophthalmic artery and perforating arter-ies, which are not easily visualized on CT angiography.
A
D
Fig. 3—48-year-old woman with “the worst head-ache of my life” and declining level of consciousness.A and B, Unenhanced CT scans show diffuse sub-arachnoid hemorrhage in basilar cistern and sylvian fissures bilaterally and along anterior falx, associ-ated with intraventricular hemorrhage. Temporal horns of lateral ventricle are mildly dilated, sugges-tive of developing hydrocephalus. Focal hematoma (arrow) in medial frontal region is also evident.C and D, Thin-slice maximum-intensity-projection (C) and 3D volume-rendering (D) images show lobu-lated saccular aneurysm (arrow) arising from ante-rior communicating artery and measuring approxi-mately 5 mm. Proximal A2 segments (arrowhead, D) of anterior cerebral arteries are displaced laterally, likely due to surrounding aneurysm.E, Three-dimensional rotational angiography shows detailed anatomy and morphology of anterior com-municating aneurysm, adjacent ophthalmic artery, and perforating arteries (arrow), which are not eas-ily visualized on CT angiography.
cb
E

Anzai and Ghodke
S8 AJR:191, September 2008
Solution to Question 7Arteriovenous malformation (AVM) is a congenital anom-
aly of blood vessels with one or more large feeding arteries and drainage veins. AVM often presents not only with sub-arachnoid hemorrhage but also with parenchymal hemor-rhage or symptoms of ischemia due to steal phenomenon. Blood flow preferentially goes to AVMs with low resistance, leaving the adjacent normal brain relatively hypoperfused. CT may show a hyperdense mass or curvilinear or speckled calcification adjacent to a parenchymal hematoma. MRI may show numerous foci of flow voids and venous aneurys-mal dilatation. Option A is not the best response.
Venous sinus thrombosis could present with subarachnoid hemorrhage; however, it tends to be focal to the area of ve-nous infarction or hypertension. Venous sinus thrombosis does not normally present diffuse subarachnoid hemor-rhage. Option B is not the best response.
Unenhanced CT of the head shows diffuse subarachnoid hemorrhage as well as a focal hematoma along the anterior falx, a typical location for a ruptured anterior communicating artery aneurysm. Option C is the best response. Approximately 50–70% of subarachnoid hemorrhages are due to aneurysm rupture. Of patients with subarachnoid hemorrhage, 10–15% have no aneurysm found even on cerebral angiography.
Amyloid angiopathy commonly affects elderly patients and presents with a lobar rather than a subarachnoid hemor-rhage. Option D is not the best response. Hypertensive hem-orrhage often affects the small perforating vessels along the lenticulostriate or thalamoperforating vessels and thus is of-ten present with parenchymal hemorrhage in the basal gan-glia, thalamus, and pons. Option E is not the best response.
Solution to Question 8Aneurysmal subarachnoid hemorrhage (SAH) has a
30-day mortality rate of 45%, with approximately half of the survivors sustaining irreversible brain damage [7]. Option C is the best response. The annual incidence of aneurysmal SAH is six per 100,000 in the United States. Approximately 5–10% of stroke cases are secondary to ruptured saccular aneurysms [8]. Recurrent hemorrhage remains a serious con-sequence, with a 70% fatality rate in patients who rebleed.
Solution to Question 9Treatment options for a ruptured aneurysm are surgical
resection or endovascular coil embolization. Endovascular oc-clusion of aneurysms using electrolytically detachable Gug-lielmi detachable coil system (GDC, Target Therapeutics [now Boston Scientific]) has been used to treat ruptured or unrup-tured aneurysms in a large number of patients worldwide. Published reports suggest that the endovascular technique is associated with fewer treatment-related complications than open surgery [7]. However, the long-term efficacy in the pre-vention of rupture or recurrence of aneurysm remains in-determinate. The recent International Subarachnoid Aneu-
QUEstION 7
What is the most likely cause of the findings on unenhanced CT?
A. Arteriovenous malformation rupture.B. Venous sinus thrombosis.C. Cerebral aneurysm rupture.D. Amyloid angiopathy.E. Hypertensive hemorrhage.
QUEstION 8
What is the 30-day mortality rate of subarachnoid hemorrhage secondary to aneurysm?
A. 15%.B. 30%.C. 45%.D. 65%.E. 80%.
QUEstION 9
Which of the following factors does NOT influence management decisions for a ruptured aneurysm?
A. Age.B. Sex.C. Aneurysm size.D. Aneurysm location.E. History of hypertension.
QUEstION 10
Despite CT angiography showing an aneurysm causing subarachnoid hemorrhage, cerebral angiography is still performed at some institutions. Which one of the following is NOT a rationale for performing cerebral angiography in this setting?
A. Searching for an additional incidental aneurysm that could be treated at the same time.
B. Better assessing the degree of incorporation of the aneurysm wall into the parent vessel.
C. Assessingflowdynamics—thatis,thesideoftheinternal carotid artery feeding anterior communicating aneurysm.
D. Measuring the aneurysm neck–dome ratio.E. Suspecting mycotic aneurysm in patients with IV
drug use.

AJR:191, September 2008 S9
Nontraumatic Emergent Neuroradiology
rysm Trial (ISAT) showed that retreatment was performed in 17.4% of patients treated with endovascular coiling and in 3.8% of patients after surgical clipping [9]. Younger age and larger aneurysm size were risk factors for retreatment. A higher rate of recurrence is seen in posterior communicat-ing artery aneurysms after endovascular coiling and anterior communicating artery aneurysms after surgical clipping, which might reflect the technical difficulty. Hyper tension is also associated with an increasing rate of rupture in patients with an unruptured aneurysm. Thus age, medical history such as hypertension, aneurysm location, and size are all rel-evant factors in treatment decisions and, therefore, options A, C, D, and E, all relevant factors in treatment decisions, are not the best responses. Although aneurysms are more common in women than in men, sex is not a factor affecting management decisions or predicting outcomes. Option B is the best response.
Solution to Question 10CT angiography is a noninvasive vascular imaging tech-
nique that has replaced catheter angiography in some insti-tutions. CT angiography may show aneurysms larger than 3 mm with a sensitivity of 77–97% and specificity of 87–100% [10]. CT angiography also has been used as a screening tool in populations at high risk for cerebral aneurysms. Cerebral an-giography, however, still remains the gold standard in the di-agnostic evaluation of cerebral aneurysms. In particular, 3D rotational angiography shows the most information about
small perforating vessels, the relationship of the aneurysm to the parent vessels (how much of the aneurysm wall is incor-porated into the parent vessel), and the flow dynamics of an-eurysms that affect surgical planning. Multiple aneurysms can be seen in patients with subarachnoid hemorrhage. These incidental aneurysms are often smaller than 3 mm, which CT angiography has a limited ability to detect. Small unrup-tured aneurysms are associated with a risk of future SAHs. If they are in a surgically or endovascularly accessible loca-tion, these incidental aneurysms can be treated at the same time as the ruptured primary aneurysm. Mycotic aneurysms often involve peripheral vessels and may present with sub-arachnoid or parenchymal hemorrhage or septic emboli. Be-cause mycotic aneurysms involve distal vessels, cerebral angi-ography is a more definitive test than CT angiography. Options A, B, C, and E are not the best responses. The aneu-rysm neck–dome ratio can be calculated on the basis of CT angiography. Option D is the best response.
ConclusionSAH associated with aneurysm rupture has high rates of
mortality and morbidity. Accurate detection and assess-ment of cerebral aneurysm lead to proper treatment deci-sions by either surgical clipping or endovascular coiling. Although CT angiography has rapidly replaced cerebral an-giography in some institutions, 3D rotational angiography provides the most information regarding characterization of aneurysms in relation to parent or adjacent vessels.
QUEstION 11
Assuming the patient does not have any medical conditions, what would be the most appropriate urgent therapy at this point?
A. IV recombinant tissue plasminogen activator (tPA).B. IV streptokinase.C. IV heparin.D. Antiplatelet therapy and aspirin.E. Intraarterial tPA and mechanical clot removal.
QUEstION 12
What percentage of patients with acute ischemic stroke are treated with IV tPA?
A. Less than 6%.B. 8–15%.C. 20–25%.D. 25–50%.E. 50–60%.
scenario 4Clinical History
A 65-year-old woman presented to the emergency de-partment 4 hours after the onset of right-sided weakness and dysarthria. Unenhanced CT of the head was obtained.
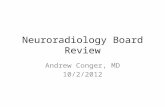
Description of ImagesUnenhanced CT of the head (Figs. 4A and 4B) showed
loss of gray–white matter differentiation in the left insular cortex and the temporal lobe. The left middle cerebral ar-tery was hyperdense compared with the basilar artery.
The patient underwent cerebral angiography for poten-tial endovascular intervention. A left internal carotid artery injection image (Fig. 4C) showed the presence of a clot in the right internal carotid bifurcation and no flow visible in the anterior and middle cerebral arteries. The microcathe-ter was placed proximal to the clot before advancing the Merci retrieval device (Merci Retrieval System, Concentric Medical, Inc.) (Fig. 4D). Subsequent angiography showed persistent occlusion of the MCA branches (Fig. 4E). In-traarterial tissue plasminogen activator (tPA) was infused through the left MCA; after tPA infusion, angiography (Fig. 4F) showed opening of the anterior division of the left MCA and occlusion of the posterior division of the left MCA.

Anzai and Ghodke
S10 AJR:191, September 2008
Solution to Question 11Current therapy for acute stroke is limited to IV recombi-
nant tPA administered within 3 hours of symptom onset. The results of the National Institute of Neurologic Disorders and Stroke (NINDS) tPA trial showed that the use of tPA within 3 hours of ischemic stroke onset substantially improved func-tional outcomes compared with a placebo group at 3 months [11]. Based on this trial, for every 100 patients given tPA, 12 more experienced complete neurologic recovery than patients given a placebo. The European Corporative Acute Stroke (ECASS) randomized trial of tPA using a 6-hour therapeutic window did not show an overall benefit, primarily because of a high rate of cerebral hemorrhage [12]. The current strict
QUEstION 13
Which of the following is NOT associated with poor neurologic outcomes in patients with acute ischemic infarction?
A. Hypoventilation.B. Extensive area of low attenuation and mass effect
on initial head CT.C. Hyperglycemia.D. Hypothermia.E. Arrhythmia.
A
D
Fig. 4—65-year-old woman 4 hours after onset of right-sided weakness and dysarthria who underwent cerebral angiography for potential endovascular intervention.A and B, Unenhanced CT scans show loss of gray matter–white matter differentiation (arrowheads) in left insular cortex and temporal lobe. Left middle cerebral ar-tery (MCA) is hyperdense compared with basilar artery (arrow, A).C, Left internal carotid artery injection image shows presence of clot (arrow) in internal carotid bifurcation and no flow visible in anterior and middle cerebral arteries.D, Unsubtracted angiography shows microcatheter placed proximal to clot (arrow) before retrieval device was advanced.E, Subsequent angiography shows persistent occlusion of MCA branches (arrow). Intraarterial tissue plasminogen activator (tPA) was infused through left MCA.F, After infusion, tPA angiography shows opening of anterior division of left MCA and occlusion (arrow) of posterior division of left MCA.
c
F
b
E

AJR:191, September 2008 S11
Nontraumatic Emergent Neuroradiology
guideline is that IV tPA must be given within 3 hours of stroke onset. Option A is not the best response. Although administra-tion of tPA after the 3-hour window may benefit some pa-tients, the interval between onset of symptoms and initiation of thrombolysis remains the most critical factor in treatment, because therapeutic efficacy decreases even within the 3-hour window [12]. Clearly, “time is brain.” Whether diffusion–per-fusion mismatch can be used to better triage patients who ben-efit from endovascular treatment beyond the 6-hour window is yet to be determined in a large clinical trial.
Streptokinase, used to treat acute ischemic stroke, is no lon-ger used because of unacceptably high rates of hemorrhage. It should not be used. Option B is not the best response. Another thrombolytic agent, urokinase, has been occasionally used intraarterially to treat vertebral and basilar thrombosis in some institutions up to 24 hours after symptom onset.
A randomized controlled trial from the International Stroke Trial showed that fewer recurrent ischemic strokes occur in patients given heparin, but this improvement was offset by an increase in hemorrhagic stroke [13]. Recent evidence does not support the routine use of heparin in pa-tients with acute stroke. Option C is not the best response.
The study evaluating the value of aspirin enrolled a large number of subjects. Aspirin was started between 12 and 24 hours after stroke onset. The results showed that aspirin sig-nificantly improved outcomes at 6 months, but the magnitude of the reduction was small. The early use of aspirin offers only modest benefit [14]. Option D is not the best response.
Intraarterial tPA and mechanical clot removal can be per-formed up to 6 hours after the onset of symptoms to an area of blood clot via a microcatheter to an area of blood clot. The presence of intracranial hemorrhage, severely elevated blood pressure, low platelet count, anticoagulation therapy, and end-stage liver or kidney disease excludes the use of tPA. Op-tion E is the best response.
Solution to Question 12Neurons die within a few minutes of oxygen deprivation.
Neuronal death occurs in areas of no blood flow within a few minutes of stroke onset. Adjacent to such areas of neuronal death is a region of hypoperfused, electronically silent tissues that receive barely enough blood flow to keep neurons alive. This tissue is called the “ischemic penumbra.” A major goal of acute stroke management is resuscitation of the ischemic penumbra. Because neuronal death is time-dependent, it is critical to intervene as early as possible.
Treatment of acute ischemic stroke with IV tPA has prov-en to be efficacious in clinical trials by reducing functional disability. However, only a fraction of patients with ischemic stroke receive IV tPA. In a community-based observational study of 13,440 patients, approximately 3% of all ischemic stroke patients, and 10.4% of patients admitted within 3 hours of stroke onset were treated with tPA [15]. Multicenter studies also report the rate of tPA use outside clinical trials ranges from 1.6% to 6%. Option A is the best response.
Solution to Question 13Maintaining adequate tissue oxygenation is critical in the
setting of acute stroke to prevent hypoxia and potential worsening of brain damage. Patients with decreased con-sciousness or brain stem dysfunction have the greatest risk of airway compromise. The prognosis of a patient who requires endotracheal intubation is generally poor; approximately 50% of these patients die within 30 days of their stroke. Op-tion A is not best response.
An extensive area of low attenuation on initial head CT indicates widespread damage to the brain tissue. An “ear-ly infarct sign” on unenhanced CT involving more than one third of the territory of the middle cerebral infarction indicates a poor outcome. The presence of mass effect or edema is also associated with an eightfold increase in the risk of symptomatic hemorrhage [11]. Option B is not the best response.
Hyperglycemia is associated with poor clinical outcomes, presumably due to increased tissue acidosis secondary to an-aerobic glycolysis and lactic acidosis. Hyperglycemia may af-fect the blood–brain barrier and lead to brain edema. Hypo-glycemia may cause focal neurologic signs and symptoms that mimic acute ischemic stroke. Hypoglycemia itself may aggravate neuronal ischemia. The prompt assessment of the serum glucose level and correction of the glucose level are important. Option C is not the best response.
Fever in the setting of acute ischemic stroke is associated with a poor neurologic outcome secondary to increased metabolic de-mands and enhanced release of neurotransmitters. Hypo-thermia is not associated with poor clinical outcomes. In fact, hypothermia has been reported to be neuroprotective in experi-mental models and small clinical trials. Hypothermia may delay depletion of the energy reserve, slow tissue acidosis, and slow calcium iron influx into cells. Option D is the best response.
Patients with acute ischemic stroke have an increased risk of developing myocardial infarction and cardiac arrhythmia. Patients with infarctions of the right hemisphere, particu-larly those involving the insula, may have an increased risk of cardiac complications, presumably secondary to distur-bances in autonomic nervous system function. The most common arrhythmia associated with acute stroke is atrial fi-brillation, which may be either the cause of stroke or a com-plication. Life-threatening arrhythmia is relatively uncom-mon, but sudden death may occur. Cardiac monitoring is often required for at least first 24 hours after the onset of stroke symptoms. Option E is not the best response.
ConclusionStroke continues to have a devastating impact on public
health and is the third leading cause of death in the United States. At least 700,000 new stroke cases occur every year. Approximately 85% of all strokes are ischemic in nature. Be-cause of the narrow therapeutic windows for treatment of acute ischemic stroke, timely evaluation, diagnosis, and treatment are of paramount importance.

Anzai and Ghodke
S12 AJR:191, September 2008
scenario 5Clinical History
A 38-year-old woman presented to the emergency de-partment with severe headache, nausea, and vomiting. Un-enhanced CT of the head was ordered. The patient had a declining level of consciousness and was admitted on that day. MRI of the brain was performed 2 days later. The pa-tient also had a history of a heart transplantation.
Description of ImagesUnenhanced CT of the head showed a vague area of low
attenuation in the right cerebellar hemisphere and mild mass effect on the right aspect of the fourth ventricle (Figs. 5A and 5B). Otherwise, no hemorrhage, hydrocephalus, or midline shift was present. Contrast-enhanced MRI was rec-ommended for further imaging workup.
FLAIR images (Figs. 5C and 5D) showed numerous foci of hyperintensity throughout the cerebral and cerebellar hemi-spheres, predominantly at the corticomedullary junction. Some lesions were seen in the basal ganglia as well as the thal-amus. The extent of disease on MRI was much more than expected from head CT performed 2 days earlier, indicating rapid progression of the disease process. These numerous foci were markedly hyperintense on diffusion-weighted images (Figs. 5E and 5F). Contrast-enhanced images showed no area of abnormal enhancement on any of the lesions (Fig. 5G).
Solution to Question 14In this patient, the combination of rapid progression of
disease, numerous small foci of restricted diffusion, and lack of enhancement makes septic emboli the most likely diagnosis. Option D is the best response.
Brain metastasis and CNS lymphoma usually do en-hance, making options A and E incorrect responses. Tuber-culosis can have numerous small foci of parenchymal le-sions, or could be miliary tuberculosis less than 2 mm in size. However, CNS tuberculous lesions are typically associ-ated with a rim of enhancement or the target sign on gado-linium-enhanced images. Restricted diffusion is not typical for CNS tuberculosis. Option C is not the best response. The lesions involve both gray matter and white matter, and the rapid progression of disease is highly unusual for multiple sclerosis. Option B is not the best response.
Solution to Question 15Septic emboli are often seen in immunocompromised pa-
tients such as those who have undergone organ transplanta-tion, those who have AIDS, and patients who have under-gone chemotherapy. In these cases, organisms may include tuberculosis or fungal infections. Among immunocompe-tent patients, infection with Staphylococcus organisms is most often seen in IV drug abusers or in patients with endo-carditis. Options A, B, C, and E are not the best responses. A history of recent travel to Southeast Asia can be seen in other infections such as tuberculosis, brucellosis, West Nile virus, hepatitis, and malaria. This is not the expected his-tory in this patient. Option D is the best response.
This patient had a history of heart transplantation and pulmonary aspergillosis. Pulmonary aspergillosis in severe-ly immunocompromised patients is highly invasive and has a dismal prognosis (near 100% mortality). It quickly gains access to the systemic circulation and is disseminated throughout the body, including the brain. This patient died 4 days after MRI was performed.
Solution to Question 16Disseminated cerebral aspergillosis infection in immuno-
compromised patients is most often caused by hemato-genous spread from pulmonary infection. Hematogenous, or angioinvasive, Aspergillus organisms characteristically
QUEstION 14
What is your preferred diagnosis in this patient?
A. Brain metastases.B. Multiple sclerosis.C. Tuberculosis.D. Septic emboli.E. CNS lymphoma.
QUEstION 15
Which of the following in a patient’s medical history is LEAST likely to be associated with septic emboli in the brain?
A. Organ transplantation with pulmonary infection.B. Cancer and presently receiving systemic chemo-
therapy.C. IV drug abuse.D. Recent travel to Southeast Asia.E. Aortic valve replacement and endocarditis.
QUEstION 16
What are the characteristic MRI findings of disseminated cerebral aspergillosis in immunocompromised patients?
A. Numerous foci of restricted diffusion in the cor-ticomedullary junction, basal ganglia, and thalami, with minimum or no enhancement.
B. Markedly bright signal on diffusion-weighted images.C. Involvement of the middle cerebellar peduncle.D. Leptomeningeal invasion.E. Infection in the paranasal sinuses.

AJR:191, September 2008 S13
Nontraumatic Emergent Neuroradiology
A
D
G
Fig. 5—38-year-old woman with severe headache, nausea, and vomiting. Patient had history of heart trans-plantation.A and B, Unenhanced CT scans of head shows vague area of low attenuation in right cerebellar hemisphere and mild mass effect on right aspect of fourth ventricle (arrow, A). No hemorrhage, hydrocephalus, or midline shift is present.C–G, MR images of brain obtained 2 days after A and B. FLAIR images (C and D) show numerous foci of hy-perintensity throughout cerebral and cerebellar hemispheres, predominantly at corticomedullary junction. Some lesions are seen in basal ganglia as well as thalamus. Extent of disease is more than expected from CT, indicating rapid progression of disease process. These numerous foci are markedly hyperintense on diffu-sion-weighted images (E and F). Contrast-enhanced T1-weighted image (G) shows no area of abnormal en-hancement on any lesions.
c
F
b
E

Anzai and Ghodke
S14 AJR:191, September 2008
lodge inside medium-sized blood vessels, resulting in multi-focal infarction, and then invade through the vascular walls, causing hemorrhagic transformation or direct extension into the parenchyma. This vasculopathy-mediated septic infarction has regional vulnerability to basal ganglia or thalami, in addition to the corticomedullary junction. The predilection to basal ganglia and thalami indicates involve-ment of the lenticulostriate and thalamoperforating arter-ies. Aspergillosis often destroys the internal elastic lamina of the cerebral arteries. Perforating vessels are the first ones to lose their patency because of their narrow diameter.
MRI characteristics of disseminated aspergillosis in-volvement of the brain in 18 patients was reported by De-Lone et al. [16] and others [17, 18]. Those authors reported that the typical MRI appearance is a predilection to basal ganglia or thalami. Enhancement was minimal or absent.
Lack of enhancement is most likely related to the host’s immune capacity. Severely immunocompromised patients have no or little immune capacity to react to an infectious organism to form capsule or inflammatory response; thus, lack of enhancement may indicate poor prognosis and rapid dissemination of angioinvasive aspergillosis. Option A is the best response.
Marked bright signal on diffusion-weighted images in this patient likely reflects infarction and cytotoxic edema. Numer-
ous foci of restricted diffusion can be seen in patients with embolic infarction, brain abscesses, and metastases from high-ly cellular tumors [19]. Option B is not the best response.
Neither involvement of the middle cerebellar peduncle nor leptomeningeal involvement is a typical finding for dis-seminated aspergillosis. Options C and D are not the best responses.
Involvement of the paranasal sinuses is often seen in dia-betic patients who have angioinvasive mucormycosis. Mu-cormycosis is a rare opportunistic infection caused by ubi-quitous fungi typically found in soil or dust. The route of infection is usually rhinocerebral and is commonly seen in patients with uncontrolled diabetes, which is often associ-ated with metabolic acidosis or ketoacidosis [20]. Mucormy-cosis can spread from the paranasal sinuses to the brain in a few days. Treatment should include aggressive débridement and IV amphotericin B. Option E is not the best response.
ConclusionRapid progression, early ischemic manifestation, and
predilection for the perforating arteries are characteristic features of disseminated aspergillosis infection in severely immunocompromised patients. Diagnosis should be made when clinical suspicion is high so that aggressive IV anti-fungal therapy can be initiated.
scenario 6Clinical History
A 27-year-old woman with a 2-week history of nausea and vomiting after a recent cholecystectomy presented to the emergency department with abdominal pain and nau-sea. Abdominal CT and pelvic sonography were negative. The patient later developed slurred speech and confusion. Brain MRI was performed (Figs. 6A–6D).
Description of ImagesFLAIR images showed bilateral symmetric hyperinten-
sity involving the mamillary bodies, the medial thalami along the third ventricle, and the periaqueductal gray mat-
ter. Diffusion-weighted images also showed an area of hy-perintensity in the medial thalami.
QUEstION 18
Which of the followings is LEAST likely to be a risk factor for Wernicke’s encephalopathy?
A. Chronic alcoholism.B. Prolonged parenteral nutrition without a vitamin
supplement.C. Hyperemesis gravidarum.D. Gastrectomy.E. Anorexia nervosa.
QUEstION 19
Which one of the following is a characteristic clinical feature of Wernicke’s encephalopathy?
A. Learning disability.B. Rigidity and tremor.C. Visual hallucination.D. Nystagmus and bilateral lateral rectus paralysis.E. Global ataxia.
QUEstION 17
What is the diagnosis given the imaging abnormality and clinical presentations?
A. Creutzfeldt-Jakob disease.B. Leigh disease.C. Wernicke’s encephalopathy.D. Maple syrup urine disease.E. Wilson’s disease.

AJR:191, September 2008 S15
Nontraumatic Emergent Neuroradiology
Solution to Question 17Brain MRI shows T2 hyperintensity predominantly in-
volving the medial thalami, periaqueductal gray matter, and mamillary bodies. The distribution of signal abnormalities on MRI and a history of prolonged emesis make Wernicke’s encephalopathy the most likely diagnosis. Wernicke’s en-cephalopathy is a severe neurologic disorder caused by thia-mine (vitamin B1) deficiency. It is a disabling and potentially lethal condition that can be prevented or reversed if treated early. It is often unrecognized and is likely more prevalent than reported. Wernicke’s encephalopathy can progress to a state of chronic amnesia called “Korsakoff ’s syndrome.” Pa-tients suffering from Wernicke’s encephalopathy show de-generation of the diencephalic regions, specifically the ma-millary bodies and the medial thalamic nuclei along the mammillothalamic tract. Option C is the best response.
Creutzfeldt-Jakob disease (CJD) is a rare neurodegenera-tive disorder that is currently thought to be caused by an abnormal protein called “prion.” Pathologically, CJD leads to spongiform encephalopathy. Patients with CJD often present with progressive dementia. CJD is divided into three types: sporadic CJD, with no known risk factors, the most common type in the United States; hereditary CJD, associated with genetic mutation; and acquired CJD, which is acquired by medical procedures such as corneal trans-plantation, human growth hormone injection, and so forth. Bovine spongiform encephalopathy (BSE) or mad cow dis-ease, is called “variant CJD,” and is believed to be due to the ingestion of infected beef. The signal abnormality on FLAIR and diffusion images is seen in the cerebral cortex, striatum, and posterior thalami. Mamillary bodies are not usually involved in CJD. Option A is not the best response.
A
c
Fig. 6—27-year-old woman with 2-week history of nausea and vomiting after recent cholecystectomy. Patient presented with abdominal pain and nausea.A–D, FLAIR images show bilateral symmetric hyper-intensity involving mamillary bodies, medial thalami along third ventricle, and periaqueductal gray mat-ter (arrows, A–C). Diffusion-weighted image (D) also shows area of hyperintensity in medial thalami.
b
D

Anzai and Ghodke
S16 AJR:191, September 2008
Leigh disease is a mitochondrial disorder caused by pyru-vate carboxylase deficiencies. It leads to necrotizing en-cephalomyelopathy. Leigh disease often affects the putami-na bilaterally, other deep gray matter structures, and the brain stem [21]. Option B is not the best response.
Maple syrup urine disease results from severe inherited defects in branched-chain amino acids. Patients are unable to catabolize branched-chain amino acids (leucine, isoleu-cine, and valine), which are increased in the blood and urine. The primary therapy is a protein-restricted diet. MRI find-ings are white matter involvement in the cerebellum, the periaqueductal gray matter along the dorsal midbrain, the cerebral peduncle, and the basal ganglia and thalami. Ma-millary bodies are not involved. Patients with maple syrup urine disease present as newborns or in infancy. Option D is not the best response.
Wilson’s disease is an autosomal recessive disorder. The Wil-son’s disease gene is mapped to chromosome 13. The main fea-ture is accumulation of copper in the tissues, predominantly in the cornea, brain, and liver. A suppressed level of cerulo-plasmin is observed in more than 80% of patients. Clinical symptoms include dysarthria, dystonia, rigidity, and ataxia. MRI findings in Wilson’s disease are signal abnormality in the lentiform nucleus and the thalami as well as tegmentum of the midbrain, red nuclei, and substantia nigra. Periaqueduc-tal gray matter involvement has been reported in Wilson’s disease. Mamillary bodies are not normally abnormal in Wil-son’s disease. Option E is not the best response.
Solution to Question 18Wernicke’s encephalopathy is a neurologic disorder with
acute onset. It is caused by a thiamine deficiency due to poor oral intake in chronic alcoholics, food refusal in an-orexia nervosa, or recurrent vomiting in pregnant patients. Approximately 50% of patients with Wernicke’s encepha-lopathy are not alcoholic. This patient presented with 2 weeks of nausea and vomiting. Other causes include chron-ic infection and a febrile status, pancreatitis, cancer, chron-ic dialysis, and prolonged parenteral hyperalimentation without a vitamin supplement [22]. Options A, B, C, and E are not the best responses.
Gastrectomy is often associated with vitamin B12 deficien-cies. In order for vitamin B12 to be absorbed from the small bowel, it needs to be chemically linked to an intrinsic factor that is produced in the stomach. Gastrectomy leads to mal-absorption of vitamin B12, which results in pernicious ane-mia. Gastrectomy is least likely to be associated with Wer-nicke’s encephalopathy. Option D is the best response.
Solution to Question 19The triad of encephalopathy, ataxic gait, and oculomotor
dysfunction is seen in only one third of patients with Wer-nicke’s encephalopathy. Ocular abnormalities are the hall-marks of Wernicke’s encephalopathy. The oculomotor signs
are nystagmus, bilateral lateral rectus palsies, and conjugate gaze palsies reflecting involvement of the oculomotor and ab-ducens nerves. Option D is the best response. Gait ataxia is believed to be due to focal midline degeneration of the supe-rior vermis, as opposed to global ataxia, a sign of cerebellar dysfunction. Option E is not the best response. Cerebellar testing with the finger-to-nose or heel-to-shin test may not elicit any notable deficit. Vestibular dysfunction without hearing loss is also a common finding.
Rigidity and tremor as well as bradykinesia and postur-al instability are common symptoms seen in patients with Parkinson’s disease, not in patients with Wernicke’s enceph-alopathy. Visual hallucination is associated with psychiat-ric disorders and drugs, particularly alcohol. Patients with schizo phrenia often have visual and, more often, auditory hallucinations. Learning disability refers to a group of dis-orders affecting academic and functional skills, including the abilities to listen, speak, write, read, and organize informa-tion. It is not specific for Wernicke’s encephalopathy. Thus, options A, B, and C are not the correct responses.
ConclusionWernicke’s encephalopathy is a severe medical emergency
that is often associated with malnutrition states. It is an un-derdiagnosed disease that can be reversed or treated with IV thiamin. Wernicke’s encephalopathy should be considered in patients with chronic alcohol abuse and malnutrition or pro-longed vomiting along with acute confusion, ataxia, oculo-motor abnormalities, and memory disturbance. Brain MRI should be ordered to assess changes in the patient’s mental status. It is important for radiologists to recognize this dis-ease so that appropriate treatment is initiated immediately.
references 1. Brown E, Prager J, Lee HY, Ramsey RG. CNS complications of cocaine abuse:
prevalence, pathophysiology, and neuroradiology. AJR 1992; 159:137–147 2. Chu CT, Gray L, Goldstein LB, Hulette CM. Diagnosis of intracranial vasculi-
tis: a multi-disciplinary approach. J Neuropathol Exp Neurol 1998; 57:30–38 3. Grossman RI, Yousem DM. Vascular disease of the brain. In: Grossman RI,
Yosem DM. Neuroradiology: the requisites, 2nd ed. St. Louis, MO: Mosby, 2003: P173–P241
4. Liang L, Korogi Y, Sugahara T, et al. Evaluation of the intracranial dural si-nuses with a 3D contrast-enhanced MR-RAGE sequence: prospective evalua-tion with 2D-TOF MR venography and digital subtraction angiography. AJNR 2001; 22:481–492
5. Klingebiel R, Bauknecht HC, Bohner G, Kirsch R, Berger J, Masuhr F. Com-parative evaluation of 2D-TOF and 3D elliptic centric contrast-enhanced MR venography in patients with presumptive cerebral venous and sinus thrombo-sis. Eur J Neurol 2007; 14:139–143
6. de Bruijn SF, Stam J, for the Cerebral Venous Sinus Thrombosis Study Group. Randomized, placebo-controlled trial of anticoagulant treatment with low-molecular-weight heparin for cerebral sinus thrombosis. Stroke 1999; 30:484–488
7. Mayberg MR, Batjer HB, Decey R, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage. Circulation 1994; 90:2592–2605
8. Bederson JB, Awad IA, Wiebers DO, et al. Recommendations for the manage-ment of patients with unruptured intracranial aneurysms: a statement for healthcare professionals from the Stroke Council of the American Heart As-sociation. Stroke 2000; 31:2742–2750

AJR:191, September 2008 S17
Nontraumatic Emergent Neuroradiology
9. Campi A, Ramzi N, Molyneux AJ, et al. Retreatment of ruptured cerebral an-eurysms in patients randomized by coiling or clipping in the international sub-arachnoid aneurysm trial (ISAT). Stroke 2007; 38:1538–1544
10. Hope JK, Wilson JL, Thomson FJ. Three-dimensional CT angiography in the detection and characterization of intracranial berry aneurysms. AJNR 1996; 17:439–445
11. [No authors listed]. Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurologic Disorders and Stroke rt–PA Stroke Study Group. N Eng J Med 1995; 333:1581–1587
12. Hacke W, Kaste M, Fieschi C, et al. Intravenous thrombolysis with recombi-nant tissue plasminogen activator for acute hemispheric stroke. The European Corporative Acute Stroke Study (ECASS). JAMA 1995; 274:1017–1025
13. International Stroke Trial Collaborative Group. The International Stroke Trial (IST): a randomized trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischemic stroke. Lancet 1997; 349:1569–1581
14. [No authors listed]. CAST: randomised trial of early aspirin use in 20,000 pa-tients with acute ischemic stroke. CAST (Chinese Acute Stroke Trial) Collab-orative Group. Lancet 1997; 349:1641–1649
15. Heuschmann PU, Berger K, Misslwitz B, et al. Frequency of thrombolytic therapy
in patients with acute ischemic stroke and the risk of in-patients hospital mortality: the German Stroke Registers Study Group. Stroke 2003; 34:1106–1113
16. DeLone DR, Goldstein RA, Petermann G, et al. Disseminated aspergillosis involving the brain: distribution and imaging characteristics. AJNR 1999; 20:1597–1604
17. Gabelmann A, Klein S, Kern W, et al. Relevant imaging findings of cerebral aspergillosis on MRI: a retrospective case-based study in immunocompro-mised patients. Eur J Neurol 2007; 14:548–555
18. Tempkin AD, Sobonya RE, Seeger JF, Oh ES. Cerebral aspergillosis: radio-logic and pathologic findings. RadioGraphics 2006; 26:1239–1242
19. Hayashida Y, Hirai T, Morishita S, et al. Diffusion-weighted imaging of meta-static brain tumors: comparison with histologic type and tumor cellularity. AJNR 2006; 27:1419–1425
20. Hopkins MA, Treloar DM. Mucormycosis in diabetes. Am J Crit Care 1997; 6:363–367
21. Ho VC, Fitz CR, Chuang SH, Geyer CA. Bilateral basal ganglia lesions: pedi-atric differential considerations. RadioGraphics 1993; 13:269–292
22. Bae SJ, Lee HK, Lee JH, Choi CG, Suh DC. Wernicke’s encephalopathy: atypical manifestation at MR imaging. AJNR 2001; 22:1480–1482