Non-invasive computed tomography and three-dimensional reconstruction of the dentition of a...
12
Non-Invasive Computed Tomography and Three-Dimensional Reconstruction of the Dentition of a 2,800-Year-Old Egyptian Mummy Exhibiting Extensive Dental Disease ANTONY H. MELCHER, 1 * STEPHANIE HOLOWKA, 2 MICHAEL PHAROAH, 3 AND PETER K. LEWIN 4 1 Faculty of Dentistry, University of Toronto, Toronto, Ontario, M5G 1G6, Canada 2 Department of Diagnostic Imaging, Hospital for Sick Children, Toronto, Ontario, Canada 3 Department of Radiology, Faculty of Dentistry, University of Toronto, Toronto, Ontario, M5G 1G6, Canada 4 Department of Pediatrics, Hospital for Sick Children, Toronto, Ontario, Canada KEY WORDS attrition; caries; periodontal disease; exposed pulp, secondarily infected cyst; death ABSTRACT A second CT scan of the mummy Djedmaatesankh, which is housed in the Royal Ontario Museum, Toronto, Ontario, has been undertaken after an interval of some 15 years. The image data set of her dentition and the associated tissues acquired from 3 mm thick 3 3 mm spacing slices was transferred to an ISG Allegro work station where two-dimensional reformats and three-dimensional reconstructions were produced. This non-invasive examination provided information on dental disease that is, in a number of respects, an advance on that which previously could be obtained from mummies by the traditional methods of visual inspection after unwrapping and by two-dimensional radiography. The two- and three-dimensional images reveal that: three molars are missing and the right maxillary canine is impacted; the rest of the dentition is afflicted by severe attrition, caries and periodontal disease; and, of the 28 teeth present in the mouth, 24 exhibit exposure of their dental pulps and 18 are afflicted by periapical lesions including five that could have contributed to a large secondarily infected radicular cyst. The cyst has displaced the maxillary antrum and enlarged the maxilla on its lateral aspect and the vault of the palate on its medial aspect. Pus from the cyst may have drained through five different sinuses. In life, Djedmaatesankh’s widespread dental infection probably caused her consider- able pain, personal distress and malaise, and possibly resulted in her death. Am J Phys Anthropol 103:329–340, 1997. r 1997 Wiley-Liss, Inc. X-ray computed tomography (CT) and three-dimensional reconstruction provides a valuable tool for examining mummies and fossils, and offers distinct advantages over the older methods of unwrapping mummies followed by autopsy, and of two-dimensional radiography (Lewin and Harwood-Nash, 1977; Lewin, 1978; Harwood-Nash, 1979; Vahey and Brown, 1984; Conroy and Van- nier, 1987; Lewin, 1991; Baldock et al., 1994). Although the state of the dentition can provide useful information regarding ancient peoples (Ruffer, 1920; Krogman, 1948; Puech et al., 1980; Skinner et al., *Correspondence to: A.H. Melcher, 708 Rosedale Glen, 278 Bloor St. East, Toronto, Ontario, M4W 3M4, Canada. E-mail: [email protected] Received 15 April 1996; revised 10 March 1997; accepted 26 March 1997. AMERICAN JOURNAL OF PHYSICAL ANTHROPOLOGY 103:329–340 (1997) r 1997 WILEY-LISS, INC.
Transcript of Non-invasive computed tomography and three-dimensional reconstruction of the dentition of a...

Non-Invasive Computed Tomography and Three-DimensionalReconstruction of the Dentition of a 2,800-Year-Old EgyptianMummy Exhibiting Extensive Dental Disease
ANTONY H. MELCHER,1* STEPHANIE HOLOWKA,2MICHAEL PHAROAH,3 AND PETER K. LEWIN4
1Faculty of Dentistry, University of Toronto, Toronto, Ontario, M5G 1G6,Canada2Department of Diagnostic Imaging, Hospital for Sick Children, Toronto,Ontario, Canada3Department of Radiology, Faculty of Dentistry, University of Toronto,Toronto, Ontario, M5G 1G6, Canada4Department of Pediatrics, Hospital for Sick Children, Toronto, Ontario,Canada
KEY WORDS attrition; caries; periodontal disease; exposed pulp,secondarily infected cyst; death
ABSTRACT A second CT scan of the mummy Djedmaatesankh, which ishoused in the Royal Ontario Museum, Toronto, Ontario, has been undertakenafter an interval of some 15 years. The image data set of her dentition and theassociated tissues acquired from 3 mm thick 3 3 mm spacing slices wastransferred to an ISG Allegro work station where two-dimensional reformatsand three-dimensional reconstructions were produced. This non-invasiveexamination provided information on dental disease that is, in a number ofrespects, an advance on that which previously could be obtained frommummies by the traditional methods of visual inspection after unwrappingand by two-dimensional radiography. The two- and three-dimensional imagesreveal that: three molars are missing and the right maxillary canine isimpacted; the rest of the dentition is afflicted by severe attrition, caries andperiodontal disease; and, of the 28 teeth present in the mouth, 24 exhibitexposure of their dental pulps and 18 are afflicted by periapical lesionsincluding five that could have contributed to a large secondarily infectedradicular cyst. The cyst has displaced the maxillary antrum and enlarged themaxilla on its lateral aspect and the vault of the palate on its medial aspect.Pus from the cyst may have drained through five different sinuses. In life,Djedmaatesankh’s widespread dental infection probably caused her consider-able pain, personal distress and malaise, and possibly resulted in her death.Am J PhysAnthropol 103:329–340, 1997. r 1997 Wiley-Liss, Inc.
X-ray computed tomography (CT) andthree-dimensional reconstruction provides avaluable tool for examining mummies andfossils, and offers distinct advantages overthe older methods of unwrapping mummiesfollowed by autopsy, and of two-dimensionalradiography (Lewin and Harwood-Nash,1977; Lewin, 1978; Harwood-Nash, 1979;Vahey and Brown, 1984; Conroy and Van-nier, 1987; Lewin, 1991; Baldock et al.,
1994). Although the state of the dentitioncan provide useful information regardingancient peoples (Ruffer, 1920; Krogman,1948; Puech et al., 1980; Skinner et al.,
*Correspondence to: A.H. Melcher, 708 Rosedale Glen, 278Bloor St. East, Toronto, Ontario, M4W 3M4, Canada. E-mail:[email protected] 15 April 1996; revised 10 March 1997; accepted 26
March 1997.
AMERICAN JOURNAL OF PHYSICAL ANTHROPOLOGY 103:329–340 (1997)
r 1997 WILEY-LISS, INC.

1982; Bennike, 1985), few observations havebeen made on their teeth using CT. Vaheyand Brown (1984) have commented on theabsence of a maxillary and a mandibularincisor in a mummy as part of a generaldescription of their CT findings. A specificCT study of amummy’s dentition was under-taken by Baldock et al. (1994) so that theycould use its stage of development to estab-lish the mummy’s age, and Conroy andVannier (1987) have used CT to determinethe state of development of the uneruptedpermanent dentition in the Taung fossilskull.Djedmaatesankh, a Theban woman from
the 22nd Dynasty (,9th Century BC), isknown from the inscription on her carton-nage to have been a lady musician in theTemple of Amun-Re at Karnak and to havebeen married to a doorkeeper in the sameTemple (Dr. Nicholas Millet, personal com-munication). Preliminary observations us-ing CT showed that her skeleton was free ofany evidence of abnormality or degenerativedisease and that she was a mature, nullipa-rous female.Harwood-Nash (1979) published the re-
sults of the first CT study of Djedmaate-sankh’s intact mummy. He described thebeautiful cartonnage in which the mummyis encased and reported on the structure ofthe mummy at various levels, but did notreport on the condition of her teeth. In thiscommunication, we report on the state of thedentition of Djedmaatesankh as revealed ina second non-destructive CT scan of themummy. This scan was carried out some 15years after the first using more advancedtechniques than those employed initially.The approach has revealed a dentition rav-aged by extensive attrition and disease, andthe presence of widespread dental infectionthat we consider to have been a possiblecause of her death.
MATERIALS AND METHODS
The mummy of Djedmaatesankh, which ishoused in the Royal Ontario Museum,Toronto, Ontario, was transported to theDepartment of Imaging, Hospital for SickChildren, Toronto, Ontario for CT imaging.Handling of the cartonnage was reduced to aminimum by supporting it on a specially
constructed board throughout the time thatit was out of the museum. This board did notinfluence the quality of the diagnostic im-ages.
The CT scan
A General Electric 9800 Quick scannerwith Hi Light Detectors (GE Medical Sys-tems-Americas, Milwaukee, WI) was used toproduce both image slices and three-dimen-sional images using the following param-eters: 1) 3mm thick3 3mm spacing throughthe head and neck using 120 kVp and 170mAs for 2 sec. Detailed analysis of thedentition was not an objective at the time ofimage acquisition, so image slices 1 mmthick 3 1 mm spacing that may have yieldedmore information regarding the oral andmaxillofacial tissues were not employed (seeDiscussion); 2) 5 mm thick 3 5 mm spacingthrough the thorax and abdomen, againusing 120 kVp, 170 mAs for 2 sec; 3) 1.5 mmthick 3 1.0 mm through the petrous bonesand orbits; 10 mm thick 3 10 mm spacingthrough the feet. The last two scans wereperformed using 120 kVp and 120 mAs for 2sec.All of the image data was archived onto
nine-track tapes. The original scan datawere also archived to allow for the possibil-ity of high resolution retrospective images.All of the image data were acquired in the
axial mode. These data were transferred toan ISG Allegro work station (ISG Technolo-gies, Mississauga, Ontario, Canada) wherethey were manipulated to produce two-dimensional reformats and three-dimen-sional image reconstructions of the head andneck. The two-dimensional reformats al-lowed the production of image slices in orien-tations different from the originally ac-quired axial mode.Two types of two-dimensional images were
produced. First, a panoramic type imagelayer: a curved slice that matched the con-tours of the maxillary and mandibular den-tal arches. This image is similar to thatproduced on the panoramic film used inmodern dental clinics for the diagnosis ofdental disease. Each of these image layersprovided an image through the long axes ofthe teeth from an anterior-posterior direc-tion. Using this technique, several image
330 A.H. MELCHER ET AL.

layers were constructed through the widthof the alveolar process and the containedteeth. Second, the image analysis softwareallowed for the reconstruction of images inany plane. This was done when diagnosticinformation additional to that provided bythe originally acquired axial images and thepanoramic reformats was required. This ca-pability of image manipulation is importantsince the position of the body of the mummycould not be altered within the gantry of theCT in order to produce acquired images inother than the axial plane.Three-dimensional reconstructed images
of the bandaged face, facial skeleton, jawsand dentitionwere also produced bymanipu-lating the pixels and the density algorithm.These images could be rotated and viewedfrom any perspective. Both soft and hardtissue anatomy could be highlighted by ma-nipulating the density algorithm.The attenuation of the resins and ban-
dageswas sometimes equal to adjacent struc-tures such as the skin and soft tissue. Diffi-culty could also be encountered in thedifferentiation between the image densitiesof the soft tissues and the mineralized bone,unlike in the living patient. This could haveresulted, at least in part, from the process ofmummification.
Examination of the images
To permit comprehensive examination,magnified images of the dentition were pro-duced following the initial examination ofthe original image data. The acquired axialimages, the two-dimensional panoramic re-formats and the three-dimensional recon-structions of each quadrant of the dentitionand the surrounding osseous structures werefirst examined. Then, each tooth and itssupporting structures were examined ingreater detail. This examination often in-volved additional manipulation of the im-ages. This included the isolation of compo-nents of the three-dimensional reconstructionsor the removal of the superficial layers of thelatter to expose components in situ (‘‘elec-tronic dissection’’). Isolation of individualteeth facilitated examination of their inter-proximal surfaces or wear of their crowns,and occasionally was used to provide particu-lar information about their root(s) and about
periapical lesions. ‘‘Electronic dissection’’wassometimes used to provide additional infor-mation about periapical lesions.
Classification of attrition
Attrition of Djedmaatesankh’s teeth wasexamined primarily in three-dimensionalreconstructions and exposure of the dentalpulp chamber in the two-dimensional pan-oramic reformats. The CT images did notprovide all of the detail that can be obtainedfrom visual examination. Consequently, al-though a number of approaches have beenused to record the extent and pattern ofattrition in human teeth (Broca, 1879; Mor-rees, 1957; Murphy, 1959; Molnar, 1971;Smith, 1984), a modified classification hasbeen devised to describe attrition seen in CTimages. The most advanced stage of wear ineach tooth is recorded: 0. No evidence ofwear of the masticatory surface; 1. Wear ofthe masticatory surface, but the cusps arestill evident on the posterior teeth; 2. Wearof the masticatory surface that has resultedin a tablelike surface; 3.Wear of themastica-tory surface that has resulted in a scallopedsurface; 4. Wear of the masticatory surfacethat has resulted in a scalloped surface in atooth where the pulp chamber is exposed; 5.Wear of the masticatory surface that hasresulted in a tablelike surface in a toothwhere the pulp chamber is exposed; ( ).Wear of the masticatory surface where thepattern of wear could have been complicatedby a carious lesion.
OBSERVATIONS
All of the teeth are present in the mouthexcept the right maxillary third molar andthe left mandibular second and third mo-lars, which are missing (Figs. 1 and 2), andthe right maxillary canine, which is im-pacted (Fig. 3). Practically all of the teethshow considerable attrition of their mastica-tory surfaces (Figs. 1, 2 and 4, and Table 1),and this has resulted in exposure of dentinewhich frequently has been worn in concavefashion (Figs. 1 and 2). There is evidence ofcaries (Figs. 5 and 6). The pulp chambers ofmany of the teeth are exposed (Figs. 3 and5). A large secondarily infected radicularcyst is located in the left maxilla (Figs. 3, 7and 8) and there are numerous other periapi-
331CT SCAN OF MUMMY WITH EXTENSIVE DENTAL DISEASE

cal lesions (Figs. 3 and 8). The individualteeth exhibiting evidence of attrition, inter-stitial caries that may have impinged uponthe worn masticatory surfaces, pulp expo-sure and periapical lesions are shown inTable 1. Destruction of alveolar bone conse-quent upon periodontal disease is also evi-dent (Fig. 4).
The secondarily infected radicular cyst
The secondarily infected radicular cyst(Fig. 7) has been measured by the computerto be 31.9 mm mesio-distal, 19 mm bucco-palatal and 22.6 mm superior-inferior in itsgreatest dimensions, and to have a volumemeasured at 6 cm3. It has encroached on anddisplaced the maxillary antrum superiorly(Fig. 3), and has expanded the maxilla later-ally (Fig. 8) and the palate medially (seebelow). The apices of the roots of five teeth,the lateral incisor, canine, first and secondpremolars and the first molar, are closelyassociated with the lesion (see below) andtheir pulp chambers are exposed. Conse-quently, it is possible that they all contrib-uted infection to the cyst.
The lateral incisor is the most mesial ofthe teeth that appear to have contributed tothe lesion. It is labioverted (Fig. 1) andconsequently shows less incisal wear thanthe adjacent teeth (Fig. 4), but there isattrition of its lingual surface, and the pulpchamber is exposed (Fig. 3). The root canal isof large diameter (Fig. 3) and there is de-struction of bone around the root. Axialimages show the lesion to reach mid-root,and three-dimensional images depict a coro-nal extention of the cyst along the mesio-labial, mesial and palatal aspects of the root(Fig. 7).The cyst surrounds the apex of the root of
the canine (Figs. 3 and 7). Although the firstpremolar is broken down and the apex of theroot has been resorbed (Figs. 3 and 4), thecyst involves the end of the remaining rootfragment, as well as the apex of the secondpremolar and the roots of the first molar(Figs. 3 and 7). While neither the second northird molars appear to have contributed tothe lesion, the cyst lies close to the palatalaspects of the roots of these teeth (Fig. 7).There appear to be a number of pathways
through which pus from the infected cystcould have drained: 1) through the exten-sion of the cyst mesio-labial to the lateralincisor (Figs. 4, 7 and 8); 2) through a sinuspalatal to the lateral incisor (Fig. 1); 3) through
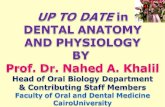
Fig. 1. Postero-inferior view of a three-dimensionalreconstruction of the maxilla and contained teeth. Notethe absence of the right third molar and of the alveolarridge where the molar would have been located; theattrition of the masticatory surfaces; the labioversion ofthe left maxillary lateral incisor; the rugae and incisalpapilla, the sinus in the palatal mucosa adjacent to theleft lateral incisor and canine and the perforation adja-cent to the right central incisor (long arrows); and theasymmetry of the palatal vault. L, left; R, right; 2, leftmaxillary lateral incisor.
Fig. 2. Postero-superior view of a three-dimensionalreconstruction of part of the mandible and the containedteeth. Note the attrition, the absence of the left secondand third molars, and the atrophied alveolar ridgewhere the molars would have been located.
332 A.H. MELCHER ET AL.

a sinus in the alveolar process that is locateddisto-superior to the apex of the canine(Fig. 8). Three-dimensional reconstructionof the alveolar process, the teeth and second-arily infected radicular cyst, and ‘‘electronicdissection’’ from the external surface of thebone, revealed the sinus to be slitlike intransverse section. The lumen of the sinuswas measured by the computer to be 6.4mm 3 1.8 mm, with the greater dimensionorientated approximately parallel to the longaxis of the canine. An image correspondingto the external aspect of the bony sinus (Fig.8) suggests that the sinus could have drainedinto the tissues of the face. We have soughtevidence for a tract in three-dimensionalreconstructions of the soft tissues but havenot been able to confirm the possibilitydespite there being evidence for swelling ofthe face (Fig. 9); 4) through a sinus apical to
the fragment of the first premolar. The gingi-val margin and alveolar bone on the labialaspect of the premolar had been resorbed(Fig. 4); 5) through a sinus into the nasalcavity (not shown).
The impacted right maxillary canine
The right maxillary canine is impacted inthe palate and is orientated disto-superiorto mesio-inferior. The palatal aspect of thecrown of the canine has penetrated both thepalatal mucous membrane adjacent tothe central incisor (Fig. 1) and the socket ofthe incisor, leaving the palatal gingival mar-gin intact. The labial aspect of the crown isin contact with the palatal aspect of the rootof the central incisor and the former hascaused erosion of the latter (not shown).Isolation of the right maxillary central andlateral incisors, the first premolar and their
Fig. 3. Two-dimensional panoramic reformat of thedentition showing primarily the maxillary teeth. Notethe impacted right canine; the secondarily infected cystin the left maxilla (*), the related teeth and the dis-placed left maxillary antrum; teeth exhibiting exposedpulp chambers; periapical lesions (arrowheads); the
large root canal in the left maxillary lateral incisor(arrow); and the broken-down left maxillary first premo-lar. A, teeth exhibiting exposed pulp chambers; AL, leftmaxillary antrum; AR, right maxillary antrum; P, leftmaxillary first premolar; 3, impacted right maxillarycanine.
333CT SCAN OF MUMMY WITH EXTENSIVE DENTAL DISEASE

associated periapical lesions from three-dimensional reconstructions revealed thatthe periapical lesions extend over the im-pacted canine (not shown).
The palate
An image consistent with rugae and anincisal papilla indicates the presence of pala-tal mucosa and gingiva (Fig. 1). Expansionof the left maxilla by the cyst has deformedthe palatal vault (Figs. 1 and 8). There aretwo perforations in the mucosa, one causedby a sinus from the cyst and the other by theimpacted canine (see above).
The missing molars
The left second and third mandibularmolars are missing (Fig. 2). The opposingleft second and third maxillary molars arehypererupted (Figs. 4 and 5); the crown ofthe former exhibits signs of attrition, as doesthat of the latter, but to a lesser degree (Fig.1). The right third maxillary molar is miss-ing (Fig. 1). The crowns of the opposing rightsecond and third mandibular molars alsoexhibit signs of attrition (Fig. 2). There is noevidence of healing sockets or retained root
fragments (Fig. 5), or of well-formed alveolarridges (Figs. 1 and 2) in the bony sites thatwould have been occupied by the three miss-ing molars.
DISCUSSIONExamination of the dentition using CT
We believe this to be the first report of acomprehensive examination of a mummy’sdentition using CT and three-dimensionalreconstruction. While two-dimensional radi-ography provides far more information onthe dentition than does examination of anunwrapped mummy (Leek, 1979), themethod used here is much more informativestill. The power of CT for this type of exami-nation is formidable and, in some respects, itprovides more information than can be ob-tained from a routine clinical and radiologi-cal dental examination. It can provide theinvestigator with both two- and three-dimensional images of the soft and mineral-ized tissues in complex structures that canbe viewed from any angle. It permits compo-nents of the three-dimensional structures tobe isolated so that they also can be viewedfrom all aspects. ‘‘Electronic dissection’’ al-lows components to be viewed in situ. Theremoval of components can also be used tofacilitate elucidation of spatial relation-ships. It provides for simultaneous viewingof correlated two- and three-dimensionalimages so that observations can be con-firmed and anatomically elucidated. And,finally, it offers the means to measure thestructures that it reveals.The technology has allowed us to identify
a number of pathological changes in thedentition of Djedmaatesankh. These includethe lesions affecting each individual tooth,including the pattern of attrition affecting agiven tooth, and the lesions affecting therelated bone and soft tissues; the probablesite of origin and the extent of the second-arily infected radicular cyst and some of itsdimensions, the effect of the cyst on theanatomy of the maxilla and overlying softtissue, and the sinuses through which con-tained pus may have drained; the orienta-tion of the impacted maxillary canine, itsrelationship to, and effect on, the root of theadjacent central incisor and palatal mucosa,and the relationship between it and periapi-
Fig. 4. Three-dimensional reconstruction of the jawsviewed from the left. Note the marked attrition affectingmost of the teeth, but not the incisal edge of the leftmaxillary lateral incisor; the effect of periodontal dis-ease on the height of the alveolar process, particularly inrelation to the mandiblar anterior teeth; the breakdownof the left maxillary first premolar; the sinuses associ-ated with the lateral incisor and the first premolar; and,the hyperuption of the second and third maxillarymolars. S, sinus; 2, left maxillary lateral incisor; 7, leftmaxillary second molar.
334 A.H. MELCHER ET AL.

cal lesions affecting adjacent teeth; and, thelikelihood of missing teeth having been con-genitally absent.However, the technology used here does
have limitations. It has not been possible to
obtain all of the information that a CT scanundertaken in conjunction with a clinicalexamination in vivo could provide. For ex-ample, it is unlikely that small carious le-sions that may have been present on the
TABLE 1. Lesions affecting individual teeth
Maxilla Mandible
Tooth Attrition1 Periapical lesion Tooth Atrition1 Periapical lesion
LeftIncisor 1 (4) 1 Incisor 1 3Incisor 2 4 1 Incisor 2 5Canine (4) 1 Canine 4Premolar 1 (4) 1 Premolar 1 4 1Premolar 2 4 1 Premolar 2 4 1Molar 1 4 1 Molar 1 4 1Molar 2 3 Molar 23Molar 3 1 Molar 33RightIncisor 1 (4) 1 Incisor 1 3Incisor 2 (5) 1 Incisor 2 4Canine2 Canine 4Premolar 1 (4) 1 Premolar 1 (4)Premolar 2 (4) 1 Premolar 2 4 1Molar 1 4 1 Molar 1 4 1Molar 2 4 Molar 2 (4) 1Molar 33 Molar 3 (4) 1
1 Six levels of attrition are recorded. See Materials and Methods. Parentheses indicate that pattern of wear could have beencomplicated by a carious lesion.2 Impacted tooth.3 Missing teeth.
Fig. 5. Two-dimensional panoramic reformat primarily showing the mandibular teeth. Note the teeththat exhibit loss of interproximal tooth substance indicative of caries and those that exhibit exposure oftheir pulp chambers. The left maxillary second molar is hypererupted. A, teeth exhibiting exposed pulpchambers; C, teeth exhibiting interproximal caries.
335CT SCAN OF MUMMY WITH EXTENSIVE DENTAL DISEASE

surfaces of the teeth, such as those that arerevealed clinically using a sharp dentalprobe, were resolved in the CT images.Furthermore, neither occlusal carious le-sions that may have been established priorto the elimination of the occlusal fissures byattrition nor carious lesions that had beeninitiated on interproximal surfaces, but thathad extended to involve the masticatorysurface, could be identified with confidenceon worn masticatory surfaces. Small expo-sures of the dental pulp, such as those thatalso can be identified with a sharp dentalprobe, and small facets on the occlusal sur-faces of teeth, such as those that can beidentified visually in clinical examinationand that could provide evidence of the earlyeffects of attrition, may not have been re-solved. Except for sites where parapets ofenamel were left surrounding areas fromwhere dentine had been worn away by attri-tion, it was not possible to differentiateenamel from dentine, particularly when en-deavouring to visualize the effects of attri-tion in three-dimensional reconstructions.Some of these shortcomings are inherent inthe technology; for example, the inability todifferentiate enamel from dentine in a three-
dimensional image of a worn masticatorysurface. Others arose out of the lack of finedetail in some images consequent upon thevolume averaging that resulted from employ-ing 3 mm scan widths. Use of 1 mm scanwidths (Baldock et al., 1994) would haveimproved resolution and could be expectedto have provided more detailed informationabout the dental tissues and their support-ing structures.Notwithstanding the limitations described
above, it is evident that a wealth of informa-tion about the dentition can be obtainedfrom CT as used here. Consequently, wesuggest that CT scans of mummies shouldalways include imaging of the jaws employ-ing the narrowest scan widths possible andthat, because of its advantages, CT shouldbe used in preference to all of the othermethods presently available for examiningmummies.
Destruction of Djedmaatesankh’s dentition
Djedmaatesankh suffered from extensivedental disease. Of the 28 teeth present in themouth, the pulp chambers of 24 are exposed,13 exhibit periapical lesions, and five couldhave been involved with the secondarilyinfected radicular cyst. She also sufferedfrom extensive periodontal disease as re-vealed by the appreciable loss of bone sup-porting her teeth. It is probable that attri-tion and caries, as well as the infection thatresulted from their destruction of the teethand possibly from periodontal disease,caused her immense pain, suffering, per-sonal distress andmalaise. It is also possiblethat spread of the infection beyond the con-fines of her jaws was the cause of her death.Dental attrition appears to have been a
major cause of Djedmaatesankh’s problems.In this condition, the masticatory surfaces ofthe teeth are worn down as coarse, fibrous orabrasive food is chewed between them. Thehard, insensitive enamel is worn away ini-tially, eventually exposing the underlyingsofter and sensitive dentinewhich is abradedmore quickly, the surface often becomingscalloped as a result. If the destruction ofthe dentine progresses at a rate that isfaster than is reactive dentinogenesis bypulp odontoblasts, the roof of the pulp cham-ber may be penetrated. This exposes the
Fig. 6. Three-dimensional reconstruction of righthalf of the mandible and its contained teeth. Note thecarious cavities involving the mesial aspect of the firstbicuspid and the buccal aspect of the third molar(arrowheads) and the occlusal attrition of the secondand third molars.
336 A.H. MELCHER ET AL.

underlying pulp and, ultimately, by exten-sion, the alveolar bone at the apex of thetooth, to bacterial infection from the oralcavity (Ruffer, 1920; Smith and Dawson,1924; Leek, 1979). This could result in theformation of a periapical lesion, an apicalgranuloma, dental abscess or radicular cyst.Dental attrition was widespread among
the ancient Egyptians (Ruffer, 1920; Smithand Dawson, 1924; Leek, 1979; Harris et al.,1980) and was the predominant destructivelesion of tooth substance (Leek, 1979; Harriset al., 1980). While many of the foods eatenby the Egyptians could have contributed tothe condition, the milling of the flour used tomake bread may have played a particularlysignificant role. The flourwas coarselymilled(Smith andDawson, 1924) and was contami-nated by fine debris from the millstonesused to grind it as well as by fine sandparticles (Ruffer, 1920; Brothwell and Broth-well, 1969; Leek, 1979). As bread formed animportant part of the Egyptian diet, thesethree components, when chewed frequently,would effectively haveworn away the enameland dentine of the teeth (Ruffer, 1920).
Djedmaatesankh, like other ancient Egyp-tians, also suffered from caries (Ruffer, 1920;Bucaille, 1990), periodontal disease (Ruffer,1920; Harris et al., 1980) and apical dentallesions (Ruffer, 1920; Harris et al., 1980). Wediagnosed dental caries in our CT imageswith confidence only when there was sub-stantial destruction of the interproximal,facial or oral surfaces of a tooth. However, itwas frequently evident that destruction oftooth substance by an interproximal lesioncould have extended to the occlusal surface.Our observations on Djedmaatesankh’s cari-ous teeth are consistent with those madedirectly on the teeth of the much moreancient Kabwe fossil (Puech et al., 1980); hiscaries also appears to have developed inter-dentally.
The secondarily infected radicular cyst
Diagnosis of the large radiolucent area inthe left maxilla as a commonly occurringsecondarily infected radicular cyst was basedon the curved shape of the lesion, and on thefact that it occupied a space by displacing
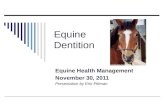
Fig. 7. Three-dimensional reconstruction showingthe relationship between the left maxillary teeth andthe associated secondarily infected cyst (*), viewed fromthe buccal (left) and from the palatal (right). Note theapparent involvement with the cyst of the lateral inci-sor, canine, both premolars and first molar; the exten-sion of the cyst along the mesio-labial, mesial andpalatal aspects of the root of the lateral incisor (arrows);
the extension of the cyst beside the palatal aspect of thesecond and third molars (arrowheads). Although theperiapical lesion associated with the central incisor mayappear to be continuous with the cyst, analysis of thecomputer images shows them to be separate. 1 through6, left maxillary central incisor through first molarrespectively.
337CT SCAN OF MUMMY WITH EXTENSIVE DENTAL DISEASE

the floor of the antrum, the lateral aspect ofthe maxilla and the palate.The contour of the area of rarefaction
related to the apex of the lateral incisorsuggests that this tooth could have been theepicentre of the lesion. This belief is sup-ported by the following. First, the tooth,which was labioverted and hypererupted,exhibits considerable attrition on its lingualaspect. The mineralized tissue covering thepulp is thinner here than that found inci-sally, so it could have been abraded rela-tively quickly. Mastication on the thin den-tine that was exposed following attrition ofthe enamel could have led to repetitivenoxious stimuli being transmitted to thepulp, development of an acute pulpitis andnecrosis of the pulp relatively early in itslife. A clue to the early death of the pulp isprovided by the comparatively large diam-
eter of the root canal, an indication of earlynecrosis of the odontoblasts. Second, thelateral incisor would have erupted at least 5years earlier than any of the other teethwhich may have contributed to the lesion,with the exception of the first molar. Whileboth of these teeth would have been sub-jected to attrition from the time that theyreached occlusion, it is evident that, becauseof its anatomy, the destruction of the incisorwould have occurred the more quickly of thetwo. It is also worth noting that, in modernpopulations, the most common teeth in-volved with radicular cysts are believed tobe maxillary incisors (Shear, 1983).There may be another explanation for the
early necrosis of the pulp, and that is trauma.A sharp blow to the tooth could have dis-rupted the blood supply to the dental pulp,and this would have been followed by itsdeath.The infected pulps of the canine, the two
premolars and the first molar may havecontributed bacteria to the enlarging cyst.
Loss of teeth
There is no evidence to suggest that den-tal extraction was used as a therapeutic
Fig. 8. An originally acquired axial image viewedfrom below (top) and a frontal view of a three-dimensional reconstruction of the facial skeleton (bot-tom). The expansion of the left maxillary alveolarprocess and the orifice of the sinus at its surface(arrowhead, bottom) correlates with the cyst (*, top) andits sinus (small arrow, top). Note the notch indicating asinus in the alveolar margin of the maxillary left lateralincisor (small arrow, bottom) in the three-dimensionalreconstruction. Radiolucent areas (arrowheads, top) thatindicate periapical lesions are associated with apices ofthe right maxillary teeth and the palate is deformed(branched arrow, top). 3, impacted right maxillary ca-nine.
Fig. 9. Three-dimensional reconstruction of the faceseen from the front and below. Note the swelling of theleft cheek (arrow).
338 A.H. MELCHER ET AL.

procedure to treat toothache in ancient Egypt(Ruffer, 1920; Breasted, 1930; Ghalioungui,1983; Weeks, 1980). It is consequently diffi-cult to explain the absence of Djedmaate-sankh’s three molars. The two third molarscould have been congenitally absent (Regeziand Sciubba, 1993). However, three-dimen-sional reconstruction of the crowns of theteeth that would have opposed them exhibitsigns of attrition. Consequently, it is reason-able to conclude that both third molars haderupted into function prior to being lost.Attrition of the opposing teeth confirms thatthe left mandibular second molar had alsoerupted into occlusion.A common cause of tooth loss among an-
cient Egyptians was periodontal disease(Harris et al., 1980). Djedmaatesankh’s den-tition shows clear evidence of generalisedperiodontal disease. This could explain theconsiderable resorption of the alveolus re-lated to the absent second and third molarsthat was seen in the three-dimensional re-constructions. It is therefore possible thatthe teeth were lost as a result of periodontaldisease. Another possibility is that the teethwere destroyed by caries but, unless theywere extracted, one could expect the CT scanto have revealed fragments of their rootslying in the bone from where the teeth werelost. The only conclusion relating to theabsence of the three teeth that can be drawnwith confidence is that they were lost sometime before death: there is no radiologicalevidence of healing sockets in the sites wherethe teeth were once located.
ACKNOWLEDGMENTS
We are grateful for the valuable assis-tance and advice that we have received fromDr. Nicholas Millet, Curator, Egyptian De-partment, Royal Ontario Museum, Toronto,Ontario, who made possible this examina-tion of Djedmaatesankh; and for that re-ceived from Mr. Allan Hollett of the samedepartment, fromMr.Michael Starr, Depart-ment of Pathology, and the late Dr. DerekHarwood-Nash and Dr. Derek Armstrong,Department of Imaging, Hospital for SickChildren, Toronto, Ontario. Dr. ChristopherMcCulloch of the MRC Group in PeriodontalPhysiology, Faculty of Dentistry, University
of Toronto, arranged for the printing of theillustrations.
LITERATURE CITED
Baldock C, Hughes SW, Whittaker DK, Taylor J, DavisR, Spencer AJ, Tonge K, and Sofat A (1994) 3-DReconstruction of an ancient Egyptian mummy usingX-ray computer tomography. J. R. Soc. Med. 87:806–808.
Bennike P (1985) Palaeopathology of Danish Skeletons.A Comparative Study of Demography, Disease andInjury. Copenhagen: Adademisk Forlag.
Breasted JH (1930) The Edwin Smith Surgical Papyrus,vol 1. Chicago: University of Chicago Press.
Broca P (1879) Instructions relatives a l’etude anthro-pologique du systeme dentaire. Bull. Soc. Anthropol.(Paris) 2:128–165.
Brothwell D and Brothwell P (1969) Food inAntiquity. ASurvey of the Diet of Early Peoples. London: Thamesand Hudson.
Bucaille M (1990) Mummies of the Pharaohs. Trans-lated by Alastair D. Pannell and Maurice Bucaille.NewYork: St. Martin’s Press.
Conroy GC and Vannier MW (1987) Dental developmentof the Taung skull from computerized tomography.Nature 329:625–627.
Ghalioungui P (1983) The Physicians of Pharaonic Egypt.Cairo: Al Ahram Center for Scientific Translations.
Harris JE, Storey AT, and Ponitz PV (1980) Dentaldisease in the royal mummies. In JE Harris and EFWente (eds.): An X-ray Atlas of the Royal Mummies.Chicago: University of Chicago Press, pp. 328–345.
Harwood-Nash DCF (1979) Computed tomography ofancient Egyptian mummies. J. Comput. Assist. To-mogr. 3:768–773.
Krogman WM (1948) The skeletal and dental pathologyof an early Iranian site. Bull. Hist. Med. 8:28–48.
Krogman WM and Baer MJ (1980) Age at death ofpharaohs of the New Kingdon, determined from x-rayfilms. In JE Harris and EF Wente (eds.): An X-rayAtlas of the Royal Mummies. Chicago: University ofChicago Press, pp. 188–285.
Leek FF (1979) The dental history of the Manchestermummies. In RA David (ed.): Manchester MuseumMummy Project. Multidisciplinary Research on An-cient Egyptian Mummififed Remains. Manchester:Manchester Museum, pp. 65–77.
Lewin PK (1978) Whole body scan of an Egyptianmummy using x-ray computed axial tomography. Pa-leopathol. Newslett. 22:T7–8.
Lewin PK (1991) Technological innovations and discov-eries in the investigation of ancient preserved man. InDJOrtner andACAufderheide (eds.): HumanPaleopa-thology: Current Syntheses andFutureOptions.Wash-ington, D.C.: Smithsonian Institution Press, pp. 90–91.
Lewin PK and Harwood-Nash DCF (1977) X-ray com-puted axial tomography of an Egyptian brain. IRCSMed. Sci. 5:78.
Molnar S (1971) Human tooth wear, tooth function andcultural variability. Am. J. Phys. Anthropol. 34:175–190.
Moorrees CFA (1957) The Aleut Dentition. Cambridge,Mass.: Harvard University Press.
Murphy T (1959) The changing pattern of dentineexposure in human tooth attrition. Am. J. Phys.Anthropol. 17:167–178.
Puech P-F, Albertini H, and Mills NTW (1980) Dentaldestruction in Broken-Hill Man. J. Hum. Evol. 9:33–39.
339CT SCAN OF MUMMY WITH EXTENSIVE DENTAL DISEASE

Regezi JA and Sciubba J (1993) Oral Pathology, 2nd ed.Philadelphia: W.B. Saunders.
Ruffer A (1920) Study of abnormalities and pathology ofancient Egyptian teeth.Am. J. Phys.Anthropol. 3:335–382.
Shear M (1983) Cysts of the Oral Regions. London:Wright PSG.
Skinner MF, Sperber GH, and Tobias PV (1982) Atlas ofRadiographs of Early Man NewYork: Alan R. Liss.
Smith BH (1984) Patterns of molar wear in hunter-
gatherers and agriculturalists. Am. J. Phys. Anthro-pol. 63:39–56.
Smith GE and Dawson WR (1924) Egyptian Mummies.London: GeorgeAllen and Unwin.
Vahey T and Brown D (1984) Comely Wenuhotep: Com-puted tomography of an Egyptianmummy. J. Comput.Assist. Tomogr. 8:992–997.
Weeks KR (1980) Ancient Egyptian dentistry. In JEHarris and EF Wente (eds.): An X-ray Atlas of theRoyalMummies. Chicago: University of Chicago Press.
340 A.H. MELCHER ET AL.