Non-alcoholic steatohepatitis Wen-Ying, Chen 2006, 10 Chapter 11.
35
Non-alcoholic steato Non-alcoholic steato hepatitis hepatitis Wen-Ying, Chen Wen-Ying, Chen 2006, 10 2006, 10 Chapter 11
-
Upload
agnes-watson -
Category
Documents
-
view
223 -
download
0
Transcript of Non-alcoholic steatohepatitis Wen-Ying, Chen 2006, 10 Chapter 11.
Non-alcoholic steatohepatitisNon-alcoholic steatohepatitis
Wen-Ying, ChenWen-Ying, Chen
2006, 102006, 10
Chapter 11
Definition of nonalcoholic fatty liver Definition of nonalcoholic fatty liver diseasedisease
Nonalcoholic Fatty Liver Disease (NAFLD) or Nonalcoholic Fatty Liver Disease (NAFLD) or Non-alcoholic steatohepatitis (NASH) is fatty infNon-alcoholic steatohepatitis (NASH) is fatty inflammation of the liver when this is not due to exlammation of the liver when this is not due to excessive alcohol use. It is a major cause of cryptocessive alcohol use. It is a major cause of cryptogenic cirrhosis of the liver. genic cirrhosis of the liver.
It differs from the simple accumulation of fat in tIt differs from the simple accumulation of fat in the liver (fatty liver, or hepatic steatosis) in that the liver (fatty liver, or hepatic steatosis) in that the inflammation of NASH causes damage to the he inflammation of NASH causes damage to the liver cells while simple fatty liver probably does liver cells while simple fatty liver probably does not. not.
Chronic liver diseaseChronic liver disease prevalence in the U.S.prevalence in the U.S.
Nonalcoholic fatty liver disease 20 %Nonalcoholic fatty liver disease 20 %
Nonalcoholic steatohepatitis 3 %Nonalcoholic steatohepatitis 3 %
Chronic hepatitis C 2 %Chronic hepatitis C 2 %
Alcoholic liver disease 0.7 %Alcoholic liver disease 0.7 %
Chronic hepatitis B 0.4 %Chronic hepatitis B 0.4 %
NASH is one of the commonest liver diseases in Western countries.
IntroductionIntroduction
NASH is the most prevalent from of progressive NASH is the most prevalent from of progressive liver disease and it is suggested that it affects betliver disease and it is suggested that it affects between ween 10-39%10-39% of the global population, with an a of the global population, with an average incidence of verage incidence of 20%.20%.
Diabetes, obesity and hypertriacylglycerolaemia Diabetes, obesity and hypertriacylglycerolaemia are all well-known risk factors for NASH.are all well-known risk factors for NASH.
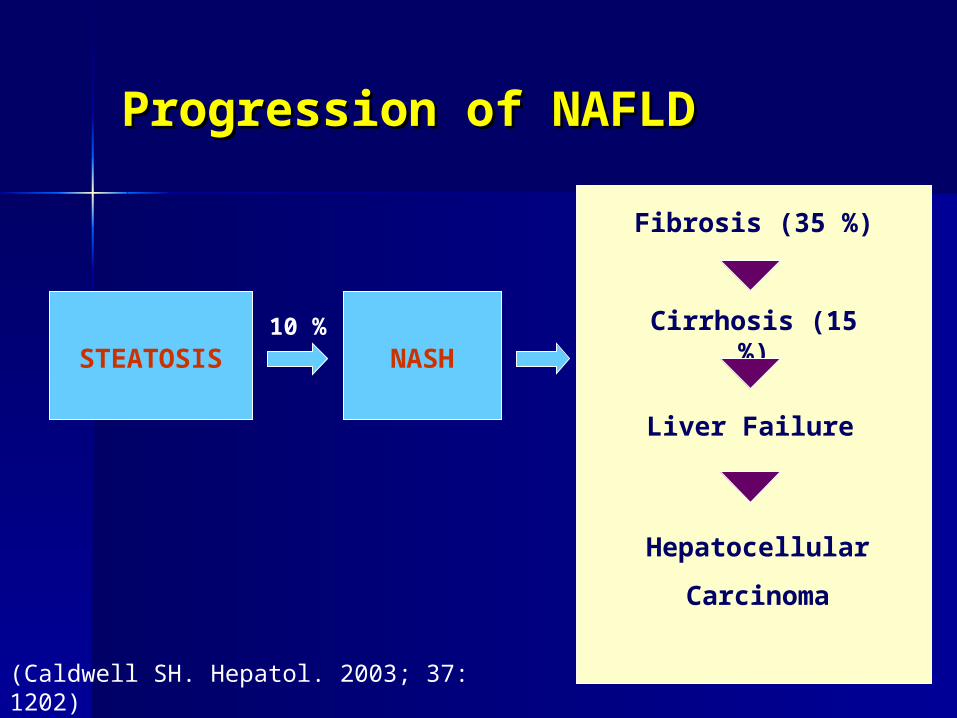
Progression of NAFLDProgression of NAFLD
STEATOSIS NASH
Fibrosis (35 %)
Cirrhosis (15 %)
Liver Failure
Hepatocellular
Carcinoma
(Caldwell SH. Hepatol. 2003; 37: 1202)
10 %
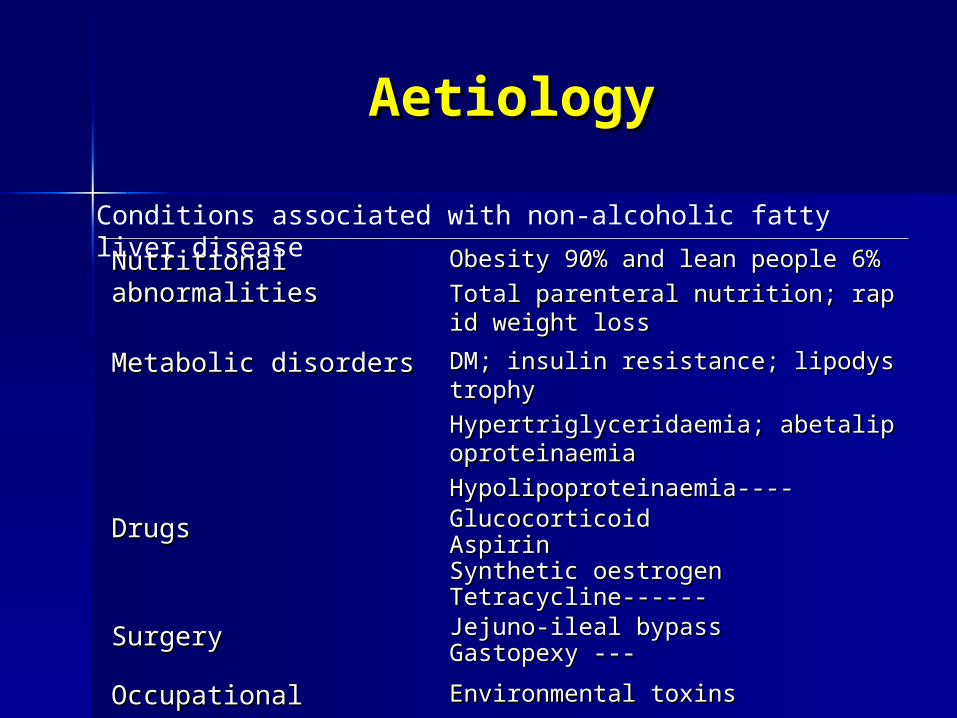
AetiologyAetiology
Nutritional abnormalitiesNutritional abnormalities Obesity 90% and lean people 6%Obesity 90% and lean people 6%
Total parenteral nutrition; rapid weight loss Total parenteral nutrition; rapid weight loss
Metabolic disordersMetabolic disorders DM; insulin resistance; lipodystrophyDM; insulin resistance; lipodystrophy
Hypertriglyceridaemia; abetalipoproteinaemiaHypertriglyceridaemia; abetalipoproteinaemia
Hypolipoproteinaemia----Hypolipoproteinaemia----
DrugsDrugs GlucocorticoidGlucocorticoidAspirinAspirinSynthetic oestrogenSynthetic oestrogenTetracycline------Tetracycline------
Surgery Surgery Jejuno-ileal bypassJejuno-ileal bypassGastopexy ---Gastopexy ---
Occupational exposureOccupational exposure Environmental toxinsEnvironmental toxins
Conditions associated with non-alcoholic fatty liver disease
DiagnosisDiagnosis
Clinical featuresClinical features Biochemistry testsBiochemistry tests Imaging Imaging Histopathological featuresHistopathological features
Clinical featuresClinical features
often asymptomatic----delays early diagnosisoften asymptomatic----delays early diagnosis Discomfort in the upper right quadrant, fatigue----Discomfort in the upper right quadrant, fatigue----
NASH is another feature of the metabolic syndromeNASH is another feature of the metabolic syndrome In one study of 66 patients: 98% insulin resistance and In one study of 66 patients: 98% insulin resistance and
39% diabetic39% diabetic Obesity and insulin resistance are linked with NASH Obesity and insulin resistance are linked with NASH
Biochemistry testsBiochemistry tests
Liver dysfunction in NASHLiver dysfunction in NASH serum alkaline phosphatase (ALP) and γ-glutamyltransfeserum alkaline phosphatase (ALP) and γ-glutamyltransfe
rase (γ-GT) are increasedrase (γ-GT) are increased
Increased serum ferritin----- 50%Increased serum ferritin----- 50%
ImagingImaging
UltrasoundUltrasound
87% sensitivity and 77% specificity87% sensitivity and 77% specificity
Computed tomography scanningComputed tomography scanning
Magnetic resonance imagingMagnetic resonance imaging
quantitative assessment of fatty infiltration is best quantitative assessment of fatty infiltration is best achievedachieved
Histopathological featuresHistopathological features
SteatosisSteatosis Inflammatory cell infiltrationInflammatory cell infiltration Hepatocyte ballonning and necrosisHepatocyte ballonning and necrosis Glycogen nucleiGlycogen nuclei Mallory’s hyalineMallory’s hyaline FibrosisFibrosis liver biopsy is recommended for : 1. increased liver enzyliver biopsy is recommended for : 1. increased liver enzy
mes 2. metabolic syndrome: type 2 diabetes, hyperlipidames 2. metabolic syndrome: type 2 diabetes, hyperlipidaemia and obesity.emia and obesity.
PathogenesisPathogenesis
Insulin resistanceInsulin resistance ObesityObesity Oxidative stressOxidative stress Nuclear receptor regulation of gene Nuclear receptor regulation of gene
expressionexpression
PathogenesisPathogenesis insulin resistance insulin resistance
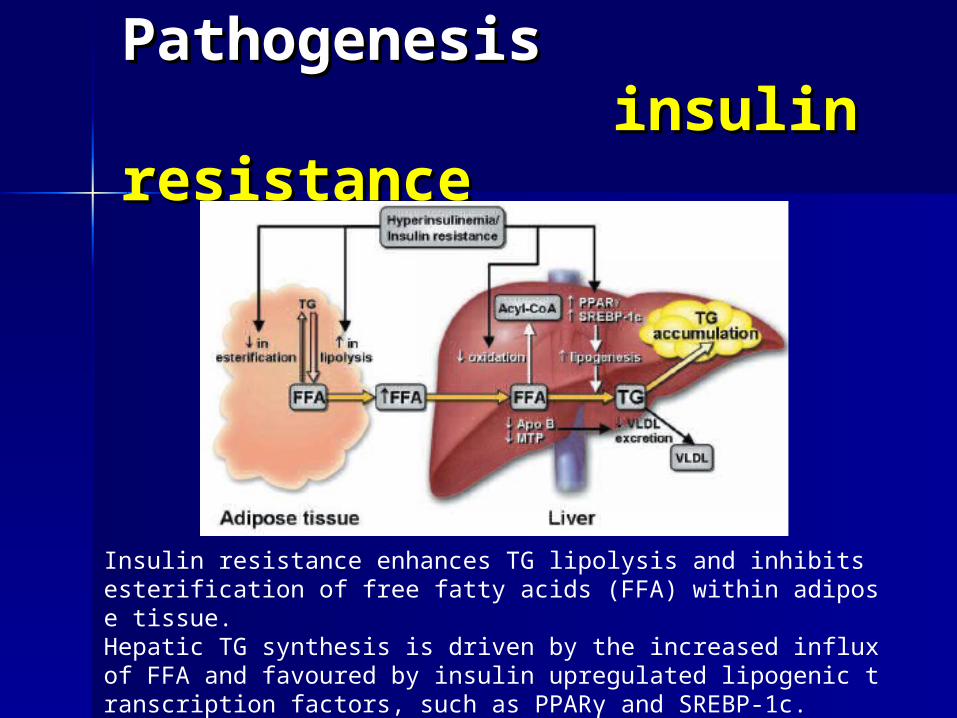
Insulin resistance enhances TG lipolysis and inhibits esterification of free fatty acids (FFA) within adipose tissue.Hepatic TG synthesis is driven by the increased influx of FFA and favoured by insulin upregulated lipogenic transcription factors, such as PPARγ and SREBP-1c.TG export via VLDL may be inhibited by decreased synthesis of apo B.
PathogenesisPathogenesis insulin resistance insulin resistance
Rad Rad (ras associated with(ras associated with DM),which interferes with essential cell functiDM),which interferes with essential cell functionsons (growth, differentiation, vesicular transport, and signal transduction).(growth, differentiation, vesicular transport, and signal transduction).
PC-1PC-1 (a membrane glycoprotein that has a role in I.R.), (a membrane glycoprotein that has a role in I.R.), which reduces inwhich reduces insulin-stimulated tyrosine kinase activity. sulin-stimulated tyrosine kinase activity.
leptinleptin, which induces dephosphorylation of insulin-receptor substrate-1, which induces dephosphorylation of insulin-receptor substrate-1
fatty acidsfatty acids, which inhibit insulin-stimulated peripheral glucose, which inhibit insulin-stimulated peripheral glucose uptake. uptake. TNF- TNF- ,which down-regulates insulin-induced ,which down-regulates insulin-induced phosphorylation of insuphosphorylation of insu
lin-receptor substrate-1 and reduceslin-receptor substrate-1 and reduces the expression of the insulin-dependthe expression of the insulin-dependent glucose-transport moleculeent glucose-transport molecule Glut4Glut4..
Adiponectin, which suppress Adiponectin, which suppress TNF- TNF- . .
Several molecular targets have now been identified linked to the actions of insulin that contribute to the dyslipidaemia that may inform the pathogenesis of NASH.
PathogenesisPathogenesis
Obesity Obesity 70-100 % of NASH patients are obese70-100 % of NASH patients are obese.. Steatosis is a common observation in obesity and may be aSteatosis is a common observation in obesity and may be a
ssociated with inflammatory signs of non-specific hepatitis.ssociated with inflammatory signs of non-specific hepatitis. The TNF-α gene is overexpressed in adipose tissue in the oThe TNF-α gene is overexpressed in adipose tissue in the o
bese and in overweight or obese patients with type 2 diabetbese and in overweight or obese patients with type 2 diabetes, resulting in higher plasma TNF-α concentations that maes, resulting in higher plasma TNF-α concentations that may contribute NASH. y contribute NASH.
PathogenesisPathogenesis
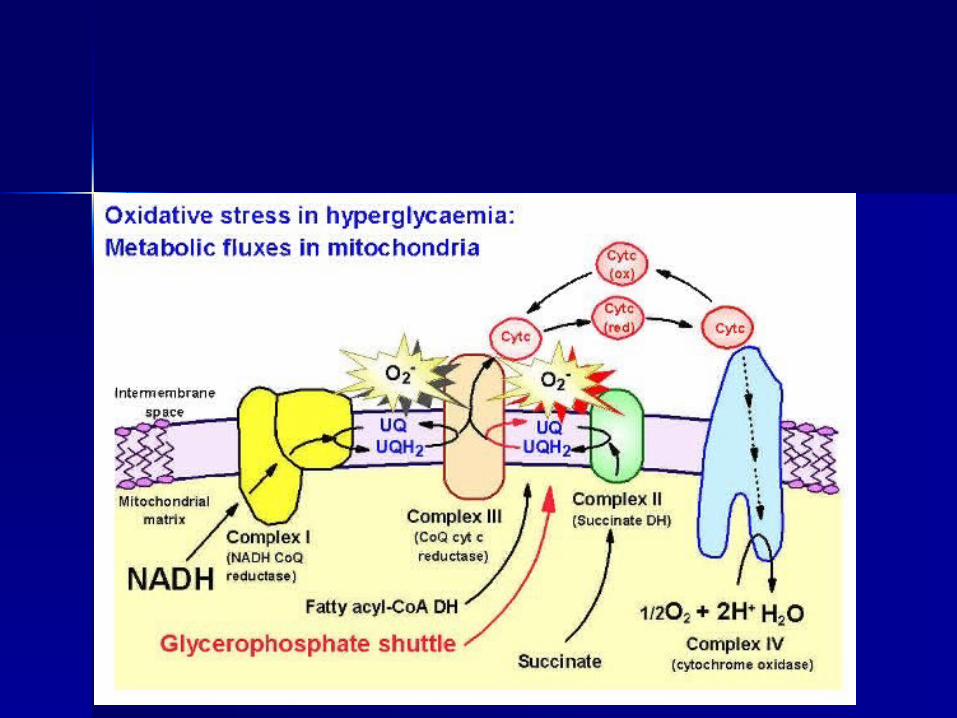
Oxidative stress Oxidative stress Mitochondria are the main cellular source of reactive oxMitochondria are the main cellular source of reactive ox
ygen species, which may trigger the inflammatory compygen species, which may trigger the inflammatory component of NASH.onent of NASH.
Numberous studies have emphasized the critical importaNumberous studies have emphasized the critical importance of oxidative stress as a crucial pathophysiological mnce of oxidative stress as a crucial pathophysiological mechanism of NASH.echanism of NASH.
PathogenesisPathogenesis
Oxidative stress Oxidative stress Nitric oxideNitric oxide: : iNOS may facilitate regeneration by inhibiting cell iNOS may facilitate regeneration by inhibiting cell
death in NASHdeath in NASH..
In iNOS knockout mice: unscavenged superoxide production may caIn iNOS knockout mice: unscavenged superoxide production may cause toxic lipid peroxidation and ultimately microvesicular steatosis ause toxic lipid peroxidation and ultimately microvesicular steatosis and NASH.nd NASH.
AdiponectinAdiponectin: : have hepatoprotective effectshave hepatoprotective effects..
1). Increased lipid clearance through β-oxidation possibly mediated 1). Increased lipid clearance through β-oxidation possibly mediated via activation of CPT-1.via activation of CPT-1.
2). Direct anti-inflammatory effects through inhibition of TNF-α2). Direct anti-inflammatory effects through inhibition of TNF-α
3). Reduce hepatomegaly, steatosis and serum ALT3). Reduce hepatomegaly, steatosis and serum ALT
Adiponectin may play a role in directly or indirectly regulating factors iAdiponectin may play a role in directly or indirectly regulating factors involved in the development of NASH.nvolved in the development of NASH.
PathogenesisPathogenesis
Oxidative stress Oxidative stress Cytochrome P450 enzymesCytochrome P450 enzymes: : CYP2E1 & CYP4ACYP2E1 & CYP4A
are capable of generating free radicals to increase oxidatiare capable of generating free radicals to increase oxidative stress.ve stress.
CYP2E1CYP2E1: :
1). to be up-regulated persistently in type 2 diabetes, insu1). to be up-regulated persistently in type 2 diabetes, insulin resistance, central obesity and NASH; lin resistance, central obesity and NASH;
2). also is up-regulated by a high-fat/low-carbohydrate di2). also is up-regulated by a high-fat/low-carbohydrate diet.et.
3). may play a role in initiating hepatic fibrosis.3). may play a role in initiating hepatic fibrosis.
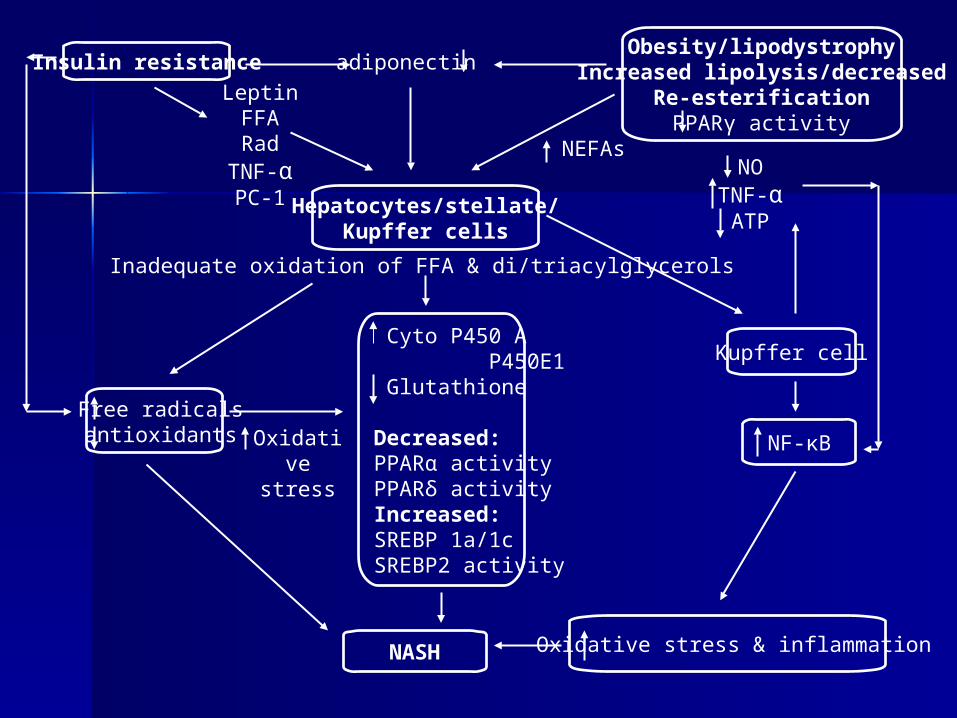
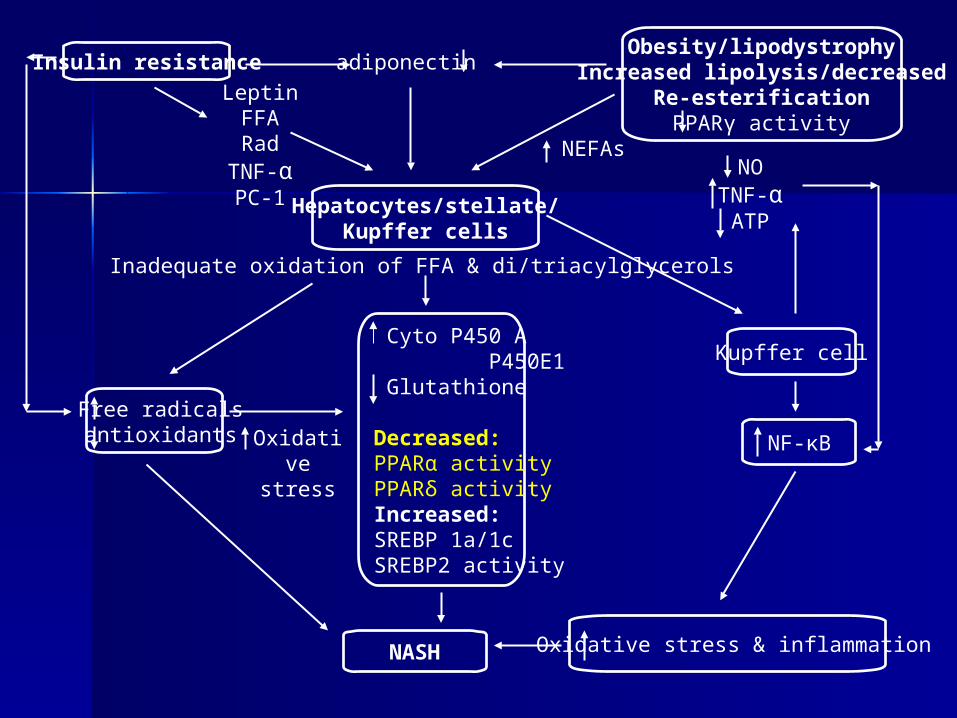
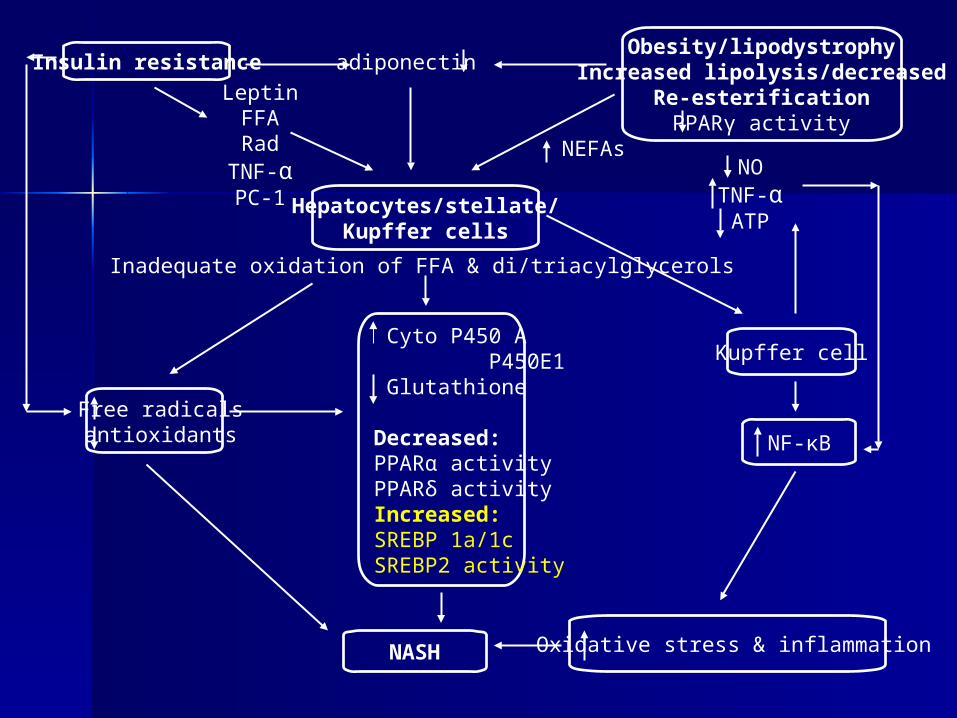
Insulin resistanceObesity/lipodystrophy
Increased lipolysis/decreasedRe-esterificationPPARγ activity
Hepatocytes/stellate/Kupffer cells
Cyto P450 A P450E1 Glutathione
Decreased:PPARα activityPPARδ activityIncreased:SREBP 1a/1cSREBP2 activity
Free radicals antioxidants
NASH Oxidative stress & inflammation
Kupffer cell
NF-κB
LeptinFFARad
TNF-αPC-1
adiponectin
NEFAsNO
TNF-αATP
Inadequate oxidation of FFA & di/triacylglycerols
Oxidative stress
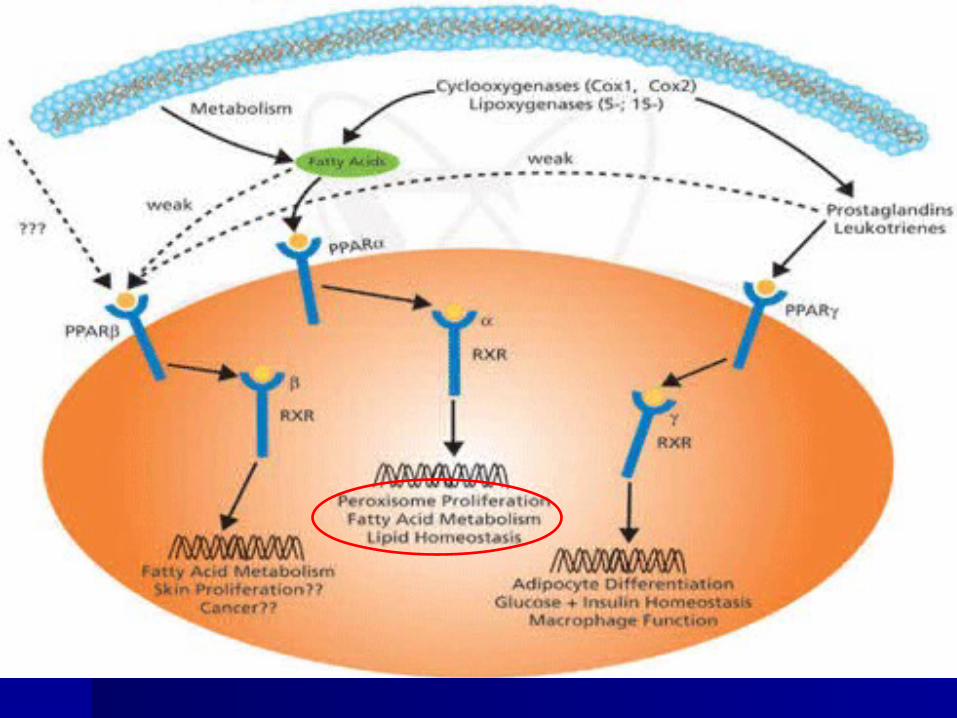
PathogenesisPathogenesisNuclear receptor regulation of gene Nuclear receptor regulation of gene expressionexpression
Peroxisome proliferator-activated receptors (PPAPeroxisome proliferator-activated receptors (PPAR)R)
membersmembers a nuclaer receptor superfamily and key regulators a nuclaer receptor superfamily and key regulators of adipogenesis----involved in the pathogenesis of NASH.of adipogenesis----involved in the pathogenesis of NASH.
Insulin resistanceObesity/lipodystrophy
Increased lipolysis/decreasedRe-esterificationPPARγ activity
Hepatocytes/stellate/Kupffer cells
Cyto P450 A P450E1 Glutathione
Decreased:PPARα activityPPARδ activityIncreased:SREBP 1a/1cSREBP2 activity
Free radicals antioxidants
NASH Oxidative stress & inflammation
Kupffer cell
NF-κB
LeptinFFARad
TNF-αPC-1
adiponectin
NEFAsNO
TNF-αATP
Inadequate oxidation of FFA & di/triacylglycerols
Oxidative stress
PathogenesisPathogenesisNuclear receptor regulation of gene Nuclear receptor regulation of gene expressionexpression
Sterol regulatory element-binding proteins (SREBPs): Sterol regulatory element-binding proteins (SREBPs): iimportant members of transcription factors that regulate hepatocyte mportant members of transcription factors that regulate hepatocyte cholesterol homeostasis.cholesterol homeostasis.
In the liver, three SREBP isoforms, SREBP-1a, SREBP-1c and SRIn the liver, three SREBP isoforms, SREBP-1a, SREBP-1c and SREBP-2, regulate the production of lipid for export into the plasma aEBP-2, regulate the production of lipid for export into the plasma as lipoproteins and into the bile as micelles.s lipoproteins and into the bile as micelles.
Expression of SREBP-1c in the liver is regulated by LXR, which iExpression of SREBP-1c in the liver is regulated by LXR, which increases fatty acid synthesis. ncreases fatty acid synthesis.
PathogenesisPathogenesisNuclear receptor regulation of gene Nuclear receptor regulation of gene expressionexpression
Sterol regulatory element-binding proteins (SREBSterol regulatory element-binding proteins (SREBPs)Ps)
1). SREBP-1c levels are increased in the fatty livers of obese (ob/ob) mice 1). SREBP-1c levels are increased in the fatty livers of obese (ob/ob) mice with insulin resistance and hyperinsulinaemia caused by leptin deficiency,with insulin resistance and hyperinsulinaemia caused by leptin deficiency, and SREBP-1c increases lipogenic gene expression, enhances fatty acid and SREBP-1c increases lipogenic gene expression, enhances fatty acid synthesis and accelerates triacyglycerol accumulation.synthesis and accelerates triacyglycerol accumulation.
2). Overexpression of SREBP-1a in rats resulted in a 26-fold increase in fa2). Overexpression of SREBP-1a in rats resulted in a 26-fold increase in fatty acid synthesis and a 5-fold increase in cholesterol synthesis.tty acid synthesis and a 5-fold increase in cholesterol synthesis.
3). SREBP-2 overexpression in transgenic mice resulted in a 28-fold increa3). SREBP-2 overexpression in transgenic mice resulted in a 28-fold increase in cholesterol synthesis and a 4-fold increase in fatty acid synthesis.se in cholesterol synthesis and a 4-fold increase in fatty acid synthesis.
Insulin resistanceObesity/lipodystrophy
Increased lipolysis/decreasedRe-esterificationPPARγ activity
Hepatocytes/stellate/Kupffer cells
Cyto P450 A P450E1 Glutathione
Decreased:PPARα activityPPARδ activityIncreased:SREBP 1a/1cSREBP2 activity
Free radicals antioxidants
NASH Oxidative stress & inflammation
Kupffer cell
NF-κB
LeptinFFARad
TNF-αPC-1
adiponectin
NEFAsNO
TNF-αATP
Inadequate oxidation of FFA & di/triacylglycerols
TreatmentTreatment
Peroxisome proliferator-activated recepPeroxisome proliferator-activated receptor gamma agoniststor gamma agonists
BiguanidesBiguanides Peroxisome proliferator-activated recepPeroxisome proliferator-activated recep
tor alpha agoniststor alpha agonists AntioxidantsAntioxidants Weight lossWeight loss
TreatmentTreatment PPARPPARγγ agonists agonists Rosiglitazone (24 weeks) in 30 NASH: improved insulin Rosiglitazone (24 weeks) in 30 NASH: improved insulin
sensitivity, reduced liver fat content and improved ALT lsensitivity, reduced liver fat content and improved ALT level. (may be due in part to the anti-inflammatory effects evel. (may be due in part to the anti-inflammatory effects of of PPARγ ligants.PPARγ ligants.
Troglitazone (400 mg for 6 months) in 10 NASH women:Troglitazone (400 mg for 6 months) in 10 NASH women: normal ALT level and mild histological improvement.normal ALT level and mild histological improvement. for 48 weeks: improved insulin sensitivity, reduced liver for 48 weeks: improved insulin sensitivity, reduced liver
fat content and improved the biochemical and histologicafat content and improved the biochemical and histological features of NASH.l features of NASH.
The main side-effects reported in these studies were weight The main side-effects reported in these studies were weight gain and in total body fatgain and in total body fat..
TreatmentTreatment BiguanidesBiguanides Metformin is the only biguanide FDA-approved for use in tMetformin is the only biguanide FDA-approved for use in t
he United Stated. It regulates AMP-activated protein kinase he United Stated. It regulates AMP-activated protein kinase
in hepatocytes, which is a major cellular regulator of lipid ain hepatocytes, which is a major cellular regulator of lipid a
nd glucose metabolism.nd glucose metabolism.
Improvement in liver biochemical test, insulin sensitivity anImprovement in liver biochemical test, insulin sensitivity an
d decreasing hepatic volume and body weight.d decreasing hepatic volume and body weight.
Thus, metformin may be beneficial in the treatment of NASH bThus, metformin may be beneficial in the treatment of NASH b
ut some of the benefit may be a direct benefit of weight loss.ut some of the benefit may be a direct benefit of weight loss.
TreatmentTreatment PPARα agonistsPPARα agonistsa). Clofibrate (2g/day): no significant benefit in liver tests oa). Clofibrate (2g/day): no significant benefit in liver tests o
r hepatic histologyr hepatic histology
b). Gemfibrozil (600 mg/day) in 46 NAFLD patients: a signb). Gemfibrozil (600 mg/day) in 46 NAFLD patients: a significant improvement in aminotransferase levlesificant improvement in aminotransferase levles
More evidence is needed from long-term studies with the neMore evidence is needed from long-term studies with the newer PPARα agonists.wer PPARα agonists.
TreatmentTreatment AntioxidantsAntioxidants It is uncertain at present whether antioxidant therapy is It is uncertain at present whether antioxidant therapy is
beneficial in the treatment of NASH.beneficial in the treatment of NASH.
1. 1. Ursodeoxycholic acid (UDCA)Ursodeoxycholic acid (UDCA) (a epimer of chenodeoxy (a epimer of chenodeoxycholic acid and non-hepatotoxic)cholic acid and non-hepatotoxic)
a). 4 open-label pilot studies: have evaluated the therapea). 4 open-label pilot studies: have evaluated the therapeutic benefit of UDCA in patients with NAFLD.utic benefit of UDCA in patients with NAFLD.
b). 2 years randomized trials concluded that no significab). 2 years randomized trials concluded that no significant differences in the degree of stestosis, inflammation or nt differences in the degree of stestosis, inflammation or fibrosis occurred between the UDCA and placebo groups.fibrosis occurred between the UDCA and placebo groups.
TreatmentTreatment AntioxidantsAntioxidants
2. Betaine2. Betaine is a normal component of the is a normal component of the metabolism of methionmetabolism of methionine and increases the S-adenosylmethionine (SAM)ine and increases the S-adenosylmethionine (SAM)
level, which has been shown to protect against triacyglycerlevel, which has been shown to protect against triacyglycerol deposition and liver injury in ethanol-fed rats.ol deposition and liver injury in ethanol-fed rats.
a). In a recent study: betaine (20g/day for 12 months)---7 NAFLa). In a recent study: betaine (20g/day for 12 months)---7 NAFLD patients ------decrease hepatic steatosisD patients ------decrease hepatic steatosis
TreatmentTreatment AntioxidantsAntioxidants3. 3. N-AcetylcysteineN-Acetylcysteine is an antioxidant that increases glutathione levels in is an antioxidant that increases glutathione levels in
hepatocytes.hepatocytes.
a). 11 NAFLD patients: N-acetylcysteine (1g/day for 3 m)----well toleraa). 11 NAFLD patients: N-acetylcysteine (1g/day for 3 m)----well tolerated and with a significant improvement in aminotransferase levles.ted and with a significant improvement in aminotransferase levles.
4. 4. Vit EVit E
5. 5. α-tocopherolα-tocopherol
Thus, it is still uncertain whether there is benefit from treatThus, it is still uncertain whether there is benefit from treatment with antioxidants.ment with antioxidants.
TreatmentTreatment Weight lossWeight loss Obesity is the condition most commonly associated with Obesity is the condition most commonly associated with
NASH and therefore weight loss is frequently advocated. NASH and therefore weight loss is frequently advocated.
However, the benefit of weight loss is difficult to evaluate However, the benefit of weight loss is difficult to evaluate because obese patients with NASH rarely achieve or because obese patients with NASH rarely achieve or maintain sustained reductions in body weight.maintain sustained reductions in body weight.
Moreover, the effect of weight loss on NASH is not Moreover, the effect of weight loss on NASH is not consistent.consistent.
TreatmentTreatment Weight lossWeight loss For the future, weight loss combined with PPARα or perFor the future, weight loss combined with PPARα or per
haps PPARγ agonists will most likely be the treatments ohaps PPARγ agonists will most likely be the treatments of choice but before this recommendation can be advocatef choice but before this recommendation can be advocated more evidence of efficacy and safety is required.d more evidence of efficacy and safety is required.