NOACs: Innovation in anticoagulation · Anticoagulants (NOACs), and the subsequent National...
24
NOACs: Innovation in anticoagulation – Optimising the prevention of AF-related stroke This report has been developed and funded by the Association of the British Pharmaceutical Industry (ABPI) Stroke in Atrial Fibrillation Initiative (SAFI). The SAFI member companies are: Bayer HealthCare, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo and Pfizer. The initiative has been supported by Anticoagulation Europe (ACE) and the Atrial Fibrillation Association (AF Association). Both organisations reviewed and provided comment on the report.
Transcript of NOACs: Innovation in anticoagulation · Anticoagulants (NOACs), and the subsequent National...

NOACs: Innovation in anticoagulation – Optimising the prevention of AF-related stroke
This report has been developed and funded by the Association of the British Pharmaceutical Industry (ABPI) Stroke in Atrial Fibrillation Initiative (SAFI). The SAFI member companies are: Bayer HealthCare, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo and Pfizer.
The initiative has been supported by Anticoagulation Europe (ACE) and the Atrial Fibrillation Association (AF Association). Both organisations reviewed and provided comment on the report.

Dr Keith RidgeChief Pharmaceutical OfficerNHS England
Prof Martin R CowieProfessor of CardiologyImperial College London (Royal Brompton Hospital)
Prof Huon GrayNational Clinical Director of Cardiac Care, NHS EnglandConsultant Cardiologist, University of Southampton
Prof Anthony RuddNational Clinical Director for Stroke, NHS EnglandProfessor of Stroke Medicine, Kings College, LondonConsultant Stroke Physician, Guy’s and St Thomas’, London
The publication of Innovation, Health and Wealth in 2011 highlighted the need for the NHS to embrace innovation in order to continue providing world class, high quality patient care in times of increased demand and financial challenge.
Medicines are the most commonly used therapeutic intervention in healthcare,1 and innovation in this field has transformed our health over the past century from prevention of disease through to treatment, cure and even eradication.
With our population now living longer, but not necessarily healthier lives, a range of long-term conditions are imposing an increasing burden on individuals, the NHS and the economy. Managing these conditions and improving the health of our nation is one of the greatest challenges to the NHS. There is a growing recognition that we need treatment to prevent disease and subsequent complications in order to reduce the need for hospital care and to enable people to live healthier lives in the community. It is in this situation where innovation is most required to revolutionise treatment and improve patient experience and outcomes.
Atrial Fibrillation (AF) is one of these long-term conditions. Affecting an increasing number of people in the UK, AF is a major risk factor for stroke – currently the third leading cause of death in England.2 Stroke has a devastating effect on patients, their families and carers and a significant financial impact on the UK economy. Costs are high, not just in terms of immediate care but also in providing long-term care for those living with the effects of stroke and the additional wider financial impact of lost productivity.
Medicines are available to prevent AF-related stroke but little has changed in the management of this condition for half a century. When used appropriately, warfarin, the most commonly prescribed anticoagulant, is an effective means of stroke prevention. However, warfarin has a number of recognised limitations and until recently a lack of effective alternatives meant that a significant proportion of patients at high risk of stroke remained untreated.3
The recent introduction of the Novel Oral Anticoagulants (NOACs), and the subsequent National Institute for Health and Care Excellence (NICE) guidance on their use, represents an opportunity to re-evaluate strategies for the prevention of AF-related stroke and address this unmet clinical need. Developed to overcome the limitations of warfarin, the NOACs provide an example of how innovation has been applied to the design of a medicine to meet the needs of a specific patient population. The introduction of any new technology presents a challenge to existing funding deployment and established treatment practices. Nonetheless, the NHS has an obligation to ensure that patients have access to clinically and cost effective medicines approved by NICE and these challenges must be addressed if we are to capitalise on innovative new medicines like the NOACs.
This report sets out the current situation in the prevention of AF-related stroke and identifies how stakeholders across the NHS can embrace innovation in stroke prevention, utilising the availability of these new therapies to evaluate and optimise existing anticoagulation services, improving outcomes and easing the emotional and financial burden of this condition in England.
Foreword

The Association of the British Pharmaceutical Industry (ABPI) Stroke in Atrial Fibrillation Initiative (SAFI) was created in 2012 to improve patient access to the Novel Oral Anticoagulants (NOACs) for the prevention of non-valvular AF-related stroke so that every appropriate patient who wants to take a NOAC and every clinician who wants to prescribe a NOAC should be able to do so.
The work of ABPI SAFI is collectively funded by its five members, all research-driven pharmaceutical companies that have developed and are marketing a NOAC or plan to launch one in the future. Our members are Bayer HealthCare, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo and Pfizer.
The current priorities of the group are to:
• Demonstrate to the NHS that investment in NOACs for stroke prevention in non-valvular AF can deliver improved patient outcomes cost effectively
• Support Government and NHS England endorsement of the importance of NOACs as a leading example of pharmaceutical innovation
• Highlight best practice in NOAC use in order to demonstrate solutions to prescribing barriers
2
About ABPI SAFI

3 Stroke is the third largest cause of death in England.2
5 Stroke afflicts more than one person every five minutes in the UK.6
900,000 The number of people in England living with the effects of stroke.7 Half of this number are dependent on other people for help with everyday activities.7
152,000 The number of strokes that occur each year in the UK.6
1,000,000 Approximately the number of people affected by AF in England and Wales.8 Data from the USA suggests that the incidence of AF will double by 2050.9
12,500The number of strokes estimated to be caused directly by AF in the UK each year.10 Patients with AF are 5-6 times more likely to suffer a stroke than patients who do not have AF.10
7,100 The number of AF-related strokes that could be prevented annually if everyone with AF was appropriately managed.11
2,100 The number of AF-related deaths that could be prevented annually if everyone with AF was appropriately managed.11
70% The higher risk of death in stroke patients with AF compared to those without AF.12
1:4
1:2
The lifetime risk of developing AF in everyone over 40.13
The proportion of people who will die within a year of having an AF-related stroke – around 32.5% will die within 30 days.14
AF-related stroke is a significant cause of death and disability in England with potentially devastating consequences for patients, their families and carers, and the NHS.
The impact of stroke and atrial fibrillation-related stroke
Atrial Fibrillation (AF) is the most common cardiac arrhythmia and is characterised by an irregular heart rhythm which may result in clots in the heart which can spread through the circulatory system. If the clots reach the brain they can cause a stroke. AF is a major risk factor for stroke and strokes suffered by people with AF are often more severe, leading to long-term disability and death.4 If preventative measures are not taken, patients with AF are left at risk of a stroke at any time. AF-related strokes are preventable5 but lives can only be saved if patients receive appropriate and well managed anticoagulation.

4
The financial impact of stroke and AF-related stroke
As well as saving lives that are unnecessarily being lost, preventing AF-related stroke could save the NHS money. On average, the healthcare costs associated with an AF-related stroke are £11,900 in the first year of care alone.10
Stroke in general has a significant impact on the UK economy. In England it is estimated to cost around £7 billion per year made up of: direct costs to the NHS of £2.8 billion, costs of informal care of £2.4 billion and costs due to lost productivity and disability of £1.8 billion.7
Emergency hospital admissions have increased by 47% over the last 15 years and are a major concern for the NHS.15 Improving the management of long-term conditions has been identified as an important factor in reducing avoidable hospital admissions.15
A considerable proportion of the costs incurred by the NHS in caring for and treating AF patients is related to hospital stays:
• One fifth of patients admitted to hospital with stroke have AF16
• Patients with AF-related stroke stay in hospital an average of 7.6 days longer than stroke patients without AF12
• Strokes in patients who have AF incur more costs than those who do not as they tend to experience more severe strokes17
“Growth in emergency admissions is a sign the rest of the health system may not be working properly. Making sure patients are treated in the most appropriate setting and in a timely manner is essential to taking the pressure off emergency hospital admissions.” Amyas Morse, Head of the National Audit Office, 31 Oct 2013.18
Hospital admissions
The cost of stroke care is a significant financial burden on the NHS. Optimising prevention of AF-related stroke is important in reducing the overall burden of stroke.

Unmet needs in the prevention of AF-related strokeAF-related stroke can be prevented. However, many patients at a high risk of stroke who would benefit from anticoagulation therapy are not receiving it, suggesting that there is substantial scope to improve the uptake of anticoagulants in the management of AF.19
“Despite there being incentives in the Quality and Outcomes Framework (QOF) and often clear evidence based guidelines (e.g. from NICE), people who have been diagnosed with or are at risk of CVD are not always optimally managed in primary care. For example, people who have atrial fibrillation are not always appropriately anti-coagulated.” Cardiovascular Disease Outcomes Strategy, March 201311
Results published in August 2013 in the first report of the new national stroke audit – the Sentinel Stroke National Audit Programme (SSNAP) – showed that only 36% of patients with known AF admitted to hospital with a stroke were taking anticoagulants and 38% were taking antiplatelet drugs such as aspirin, which have limited efficacy in patients with AF.16
If all appropriate, high-risk AF patients received anticoagulation therapy in preference to antiplatelet therapy, it is estimated that in excess of 3,000 strokes could be prevented annually.19
Anticoagulant AND antiplatelet
Anticoagulant ONLY
Antiplatelet ONLY
No medication
Aspirin, an antiplatelet, has historically been widely used in the prevention of AF-related stroke. Some physicians continue to use aspirin perceiving it to be safer than anticoagulants despite the fact that it has been shown to reduce the risk of AF-related stroke by only 19%20 vs warfarin at 64%,20 and it has the potential to cause significant bleeding into the brain
and gut.21 In 2012 the updated European Society of Cardiology (ESC) Guidelines for the Management of Atrial Fibrillation concluded that the evidence for effective stroke prevention with aspirin in AF is weak, with a potential for harm and, therefore, it has a limited role.22
Aspirin
Percentage of AF patients on stroke preventative medication by type on admission to hospital with a stroke16

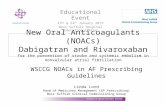
The increased risk of stroke and intracranial bleeding outside a narrow therapeutic range with warfarin.25
Warfarin is a vitamin K antagonist (VKA) and has been the established anticoagulant treatment option for the past 50 years. When used appropriately, warfarin is an effective means of stroke prevention, reducing the risk of AF-related stroke by 64%.20 However, while suitable for some patients, warfarin is associated with:
• A narrow therapeutic range – warfarin patients require close monitoring to ensure that their levels of anticoagulation remain between tight boundaries called INR levels - international normalised ratio (INR). The chart shows the narrow range for effective treatment with warfarin between an INR of 2-3. Below 2 and the risk of stroke increases. Above 3 and the risk of intracranial bleeding increases. As a result, patients must regularly attend an anticoagulation clinic to have their levels of anticoagulation monitored and their warfarin dose adjusted if required. This can be problematic for people in full-time employment who find it hard to take time off work, and the elderly who might find it hard to attend a clinic due to co-morbidities or mobility issues. Regularly changing the dose of
warfarin can be confusing leading to problems with adherence to treatment.
• Multiple food and drug interactions – warfarin is associated with a wide range of interactions that can necessitate more intensive anticoagulation monitoring and potential dose adjustment. Patients must take care with their diet and limit or avoid foods that may have an impact on their anticoagulation levels, for example, cranberry juice or broccoli.
• Prescribing errors and adverse events – warfarin is one of the most common causes of drug-related adverse events and is responsible for 5.6% of fatal and severe drug-related incidents, many of which will require hospital admission.23
As a result of the difficulties associated with warfarin management, many patients with AF at high risk of stroke who would otherwise be suitable for warfarin are either not treated at all or are treated with aspirin instead.24 This represents a huge unmet clinical need, and one which places a significant preventable burden (both clinically and financially) on patients, their families and carers and the NHS.
Warfarin
6
Evidence shows that many patients at high risk of AF-related stroke are not receiving appropriate anticoagulation.
Intracranial bleeding risk
1.0
1
5
10
15
20
2.0 3.0 4.0 5.0 6.0 7.0 8.0 INR
Odd
s R
atio
Ischaemic stroke risk

NOACs: Innovation in the prevention of non-valvular, AF-related strokeThe NOACs: apixaban, dabigatran etexilate and rivaroxaban, are the first major innovation in the prevention of non-valvular AF-related stroke in 50 years. Appropriate use of the NOACs has the potential to prevent non-valvular AF-related strokes, save lives, remove the need for routine anticoagulation monitoring and reduce the financial burden of a costly, long-term condition on the NHS.
The 2012 European Society of Cardiology (ESC) guideline recommends NOACs as broadly preferable to warfarin in the vast majority of patients with non-valvular AF, when used as studied in the clinical trials performed so far.22
NOACs were specifically designed to overcome the limitations of warfarin. They provide predictable, stable and reliable levels of anticoagulation.
NOACs do not require routine anticoagulation monitoring, ongoing dose changes according to the level of anticoagulation or dietary restrictions26 and may be a preferable alternative to warfarin for many patients with non-valvular AF at increased risk of stroke.27
More than 50,000 patients with non-valvular AF have been studied in clinical trials of the NOACs (apixaban, dabigatran etexilate and rivaroxaban). These studies demonstrated that:28,29,30
• NOACs are comparable to or superior to warfarin in reducing the risk of stroke in patients with non-valvular AF
• NOACs are comparable to or superior to warfarin with regard to the incidence of major bleeding
• NOACs are associated with a lower risk of intracranial haemorrhage than warfarin
NICE has approved the NOACs as alternative treatment options to warfarin in the prevention of non-valvular, AF-related stroke and NICE assessments demonstrate that all three are cost effective compared with warfarin.31,32,33
Routine anticoagulation monitoring adds significantly to the cost of warfarin treatment. Treatment with NOAC therapies means that routine anticoagulation monitoring is not required, and therefore, NOACs may present a release of capacity opportunity for local health services.
Key facts
NOACs are an important advance in the prevention of AF-related stroke, providing a clinically effective and cost effective alternative to current treatment options.

Healthcare professionals in the Buckinghamshire area have applied an integrated, patient focused approach to implementing NICE guidance on the use of the NOACs throughout the area.
Before the publication of the first NICE guidance on the NOACs, a multi-disciplinary meeting involving consultants, GPs, pharmacists and medicines management was convened to develop appropriate patient pathways and manage the cost of an anticipated increase in prescribing of these therapies. The output was a pharmacist led, novel oral anticoagulants clinic with a remit to maximise investment in the NOACs to deliver excellent patient care.
Referrals to the clinic come from both GPs and consultants and patients are provided with information and support to enable them to fully participate in informed decision making about their treatment. All patients initiated on NOACs receive a follow-up telephone call within two weeks to monitor their progress. The service also helps to ensure consistency in prescribing habits across the area and monitor side effects and patient safety.
With permission from Satinder Bhandal, Consultant Anticoagulation Pharmacist
Buckinghamshire NOAC Service
8

Optimising anticoagulation in the prevention of AF-related strokeMedicines use in the prevention of AF-related stroke is currently suboptimal.11 Research has shown that aspirin has a limited effect and a potential to cause harm,22 and warfarin, though effective, requires regular anticoagulation monitoring and this can present significant challenges for patients, their families and carers and the NHS.
Medicines optimisation is a patient-focused approach to getting the best from investment in and use of medicines.1 The NOACs demonstrate how the pharmaceutical industry is responding to patients’ expectations for better care by developing innovative therapies that aim to improve the patient experience whilst simultaneously delivering value for the NHS.
The availability of the NOACs provides a significant opportunity to address some of the limitations of current anticoagulation management and respond to the individual needs of our patients. Patients who are able to express their needs and share in the decisions that are made about their treatment are more likely to engage in their healthcare and improve their outcomes because of this.
I was recently able to support a patient with AF that I encountered at a hypertension clinic. She had previously been prescribed warfarin for stroke prevention but was currently taking aspirin. The patient, a lady in her 70s, was unaware that anticoagulation would protect her against stroke much more effectively than aspirin, nor was she aware that aspirin was not necessarily a safer option. Following our discussion, we agreed that I would write to her GP to suggest a treatment review and referral to a haematologist if appropriate.
In his response, the GP explained that a stable level of anticoagulation could not be maintained for this patient using warfarin. Unfortunately, other options were not available for / not offered to the patient at that time and aspirin was thought to be a safer treatment option. As suggested, the lady was referred to a haematologist who initiated NOAC therapy. This demonstrates medicines optimisation in practice; the decision to prescribe was made, taking into consideration the patient’s previous experience, the evidence behind the NOACs, and the need to put patient safety and patient experience at the heart of the prescribing decision. Our patient’s stroke risk is now appropriately managed and she is doing well with good adherence to treatment.
With permission from Sotiris Antoniou Consultant Pharmacist Cardiovascular Medicine, Barts Health NHS Trust
Medicines optimisation case study in AF using NOACs to improve patient outcomes
NOACs support medicines optimisation principles, offering an opportunity to improve patient outcomes and experience whilst simultaneously delivering value for the NHS in the prevention of AF-related stroke.

10
Aim to understand the patient’s experience: NOACs aim to improve the patient experience, simplifying anticoagulation therapy by reducing the need for dietary restrictions and routine anticoagulation monitoring. NOACs may be preferable to warfarin for many patients with non-valvular AF at increased risk of stroke.27
Evidence based choice of medicines: Studies in more than 50,000 patients with non-
valvular AF have shown the NOACs to be comparable to or superior to warfarin
in the prevention of AF-related stroke.28,29,30 All three available
therapies have been approved by NICE as a cost effective
use of NHS resources in the prevention of AF-
related stroke.31,32,33
Make medicines optimisation part of routine practice: The availability of the NOACs provides an opportunity to simplify anticoagulation therapy and treatment pathways. They should be included as a choice of therapy for those patients, as outlined in the appropriate NICE technology appraisals, requiring anticoagulation for the prevention of non-valvular AF-related stroke. Providing patients with information about anticoagulation therapy and enabling them to make informed choices about the appropriate medicine for them and their lifestyle may improve the proportion of patients effectively anticoagulated, thereby reducing the incidence of AF-related stroke and the associated burden on the NHS.
Ensure medicines use is as safe as possible: Warfarin is the third
most common cause of severe and fatal incidents
related to medicines, some of which will result in
hospital admissions.23 NOACs are associated with a lower
risk of intracranial haemorrhage than warfarin and are comparable or
superior to warfarin with regard to the incidence of major bleeding.28,29,30
NOACs fit into the four principles1 of medicines optimisation
Improved patient outcomes
Aligned measurement & monitoring
of medicines optimisation
Principle 1Aim to understand the patient’s experience
Principle 4Make medicines optimisation part of routine practice
Patientcentred
approach
Principle 2Evidence based
choice of medicines
Principle 3Ensure medicines
use is as safe as possible

NOACs: Supporting the delivery of national policyOptimising anticoagulation with the NOACs supports the delivery of NHS policy and is aligned with improvement areas defined in the outcomes frameworks to which the NHS is accountable.11,31,32,33,34,35,36,37,38,39,40,41,42,43
Achieving Outcomes
The NHS Outcomes FrameworkDomain 1 – Preventing people from dying prematurelyDomain 2 – Enhancing quality of life for people with long-term conditionsDomain 3 – Helping people recover from episodes of ill health or following injuryDomain 4 – Ensuring that people have a positive experience of care
CCG Outcomes Indicator SetDomain 1 – Reducing premature mortality from the major causes of death• Under 75 mortality from cardiovascular disease• Mortality within 30 days of hospital admissions
for strokeDomain 2• Health related quality of life for people with
LTCs• Ensuring people feel supported to manage their
condition• Reducing time spent in hospital by people with
LTCsDomain 3 – Emergency re-admissions within 30 days of discharge from hospitalDomain 4 • Patient experience of primary and hospital care
Quality and Outcomes Framework• The percentage of patients with atrial
fibrillation in whom stroke risk has been assessed using the CHADS2 risk stratification scoring system in the preceding 15 months (excluding those whose previous CHADS2 score is greater than 1)
• In patients with atrial fibrillation, in whom there is a record of a CHADS2 score of 1 (latest in the preceding 15 months), the percentage of patients who are currently treated with anticoagulation drug therapy or anti-platelet therapy
• In patients with atrial fibrillation, whose latest record of a CHADS2 score is greater than 1, the percentage of patients who are currently treated with anticoagulation therapy
The Public Health Outcomes Framework Domain 4 – Healthcare, public health and preventing premature mortality
CVD Outcomes StrategyThis outcomes strategy identifies for commissioners and providers the main areas where there is scope to deliver improvement. It notes that more could be done to identify and manage cardiovascular risk in primary care. The management of hypertension and conditions which contribute to cardiovascular problems (especially atrial fibrillation and diabetes) is often inadequate.
NICE Approval
NICE Technology Appraisals (TAs)NICE has approved all currently available NOACs as a cost-effective use of NHS resources• NICE TA 249 – dabigatran etexilate• NICE TA 256 – rivaroxaban• NICE TA 275 – apixaban
NICE – Support for Commissioning Anticoagulation TherapySupports commissioners, clinicians and managers in commissioning high-quality, evidence based care for adults across England.
Comply or Explain RegimeNHS England, Everyone Counts: Planning for Patients 2013/14 states that: NHS organisations should demonstrate their commitment to implement each of the four elements of the Comply or Explain regime:• Automatic inclusion of positive NICE
Technology Appraisals on local formularies in a planned way that supports safe and clinically appropriate practice
• Publication of local formularies• Tracking of adoption of NICE Technology
Appraisals through the Innovation Scorecard• Support to overcome the system barriers
to implementation of NICE Technology Appraisals.
NHS ConstitutionStates that: ‘You have the right to drugs and treatments that have been recommended by NICE for use in the NHS, if your doctor says they are clinically appropriate for you.’
Innovation
Innovation, Health and Wealth (IHW)NOACs are a leading example of the innovative treatments described in the IHW report. The report describes innovation as central to the NHS for three main reasons:• Innovation transforms patient outcomes• Innovation can simultaneously improve quality
and productivity• Innovation is good for economic growth‘Formulary processes should proactively consider the impact of new NICE technology appraisals, and all NICE technology appraisal recommendations should – where clinically appropriate – be automatically incorporated into local formularies.’
NICE Implementation Collaborative (NIC)The NIC has already begun pilot work on NOACs in order to better understand the barriers to their adoption within the system, and develop solutions that promote better and more consistent access to NICE recommended treatments.
High Impact Innovation NOACs are listed in the Catalogue of Potential Innovations – the document developed to provide a means by which the NHS can explore innovative ideas and, where appropriate, adopt them and adapt them to deliver high impact improvements in a sustainable way.

12
There is a wealth of policy to support the use of NOACs in the prevention of AF-related stroke.

NOAC use: The NHS experience
Some NHS organisations are early adopters of new technologies and use these successfully in redesigning services to deliver best practice care. However, this good practice is far from universal, and in some areas situations exist that make it difficult to ensure that patients receive the newest and most innovative medicines designed to improve poor patient outcomes and reduce ill health, and exert a wider positive impact on economic productivity.44 The NOACs are a case in point. Despite having been launched in the UK in advance of several other European countries, NOAC uptake in the UK lags significantly behind its European contemporaries45 and is considerably less than the anticipated uptake calculated by NICE in the costing templates for the NOACs of approximately 20% within the first year post guidance.46,47,48
Dudley Group of Hospitals NHS Foundation Trust instituted the use of NOACs for appropriate patients with AF in November 2012. An informative campaign was conducted across the anticoagulation service and to those involved in the anticoagulation care pathway to ensure that the changes and new protocols were communicated to all teams to enable adoption of NOACs at pace. Posters, screensavers and educational talks at induction/audit meetings helped in ensuring a safer introduction of the NOACs for all levels of staff. In addition, a database of patients using NOACs was created to ensure their experience was captured and monitored.
At the heart of the change was an emphasis on ensuring that patients were engaged and supported in their anticoagulation. Bespoke materials for patients were developed to help them understand their condition, enabling a detailed discussion with healthcare professionals about the risk/benefit of
appropriate treatments for them. Particular attention was placed on helping patients understand and be aware of the need to adhere to their anticoagulation medicine.
Observed outcomes of the changes for patients using NOACs have included:
• A simplification of the treatment regimen, which benefits both patients and NHS staff
• Freeing up of capacity within the anticoagulation service
Particular areas of success have been around the simplicity of dosing in the elderly and the logistical and lifestyle benefits for the younger working generation.
With permission from Sarah Hughes, Clinical Nurse Specialist Anticoagulation and Thrombosis
Best Practice in Dudley

14
In the table above, NOACs include Dabigatran, Rivaroxaban and Apixaban. All anticoagulants include Vitamin K Antagonists (e.g. Warfarin), Heparin (fractionated and unfractionated), NOACs and Fondaparinux
Budget concerns Cost is often cited as a concern in NOAC use. However, the full cost of strokes and the provision of anticoagulation monitoring is not completely understood and considered when assessing the cost impact of NOAC implementation. Costs incurred by patients in attending anticoagulation monitoring clinics, and the cost of hospital admissions and other factors involved in managing the adverse effects of warfarin, are not always taken into account.
Slow implementation of NICE guidanceAccess to the NOACs is also being restricted by the development of local formulary guidance or protocols that state that NOACs should be initiated after warfarin despite no restriction to a particular line of therapy in their licence or in the NICE Technology Appraisals. There is evidence in some areas that financial incentives are being offered through the Commissioning for Quality and Improvement (CQUIN) programme to adhere to these locally imposed guidelines.49
In the recently published metrics report from the Health and Social Care information Centre, which reviewed the use of NICE appraised medicines in the NHS in England, statistics revealed a 29-fold difference in NOAC prescribing across the UK.50 The significant variation in prescribing is recognised as a problem in the prevention of AF-related stroke and prompted NICE to comment in its recent commissioning guide, ‘Support for Commissioning Anticoagulation Therapy’, that ‘Commissioners should note their obligations in meeting the recommendations made in the relevant NICE technology appraisals.’40
Even when NOAC therapy is initiated in secondary care, patients can find that their GP refuses to continue the prescription.
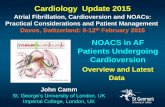
NOAC Uptake as of August 2013 (IMS Health, Retail and Hospital Sales, Standard Unit % of Anticoagulants, MAT August 2013)45
Despite being placed on NOAC therapy by his consultant, Mr G in London now pays for a private prescription because his GP refused to issue a repeat prescription as the local CCG does not support NOAC use. Case study supplied by Anticoagulation Europe
Germany
Belgium
Denmark
Switzerla
nd
Norway
Poland
Ireland
Czech RepublicSpain
Sweden
Finland
United Kingdom
Netherlands
Italy
Average
28.20%30.00%
25.00%
20.00%
15.00%
10.00%
5.00%
0.00%
25.60%
21.80%
18.30%
15.90% 15.20%13.50%
11.70% 11.60%
5.10% 5.10%3.40% 2.70% 2.70%
12.90%

The above ratio ‘Units/AF pt per locality’ is defined as: (NOAC sales/AF patients) per quarter in a given CCG or Health Board. The maximum that the ratio can be is three. That is, three prescriptions equating to a three month supply of a NOAC to all of the AF patients. In Q3 2013 the maximum ratio was 0.87.
The map shows the impact of local barriers, resulting in poor uptake and wide regional variation in NOAC use across the UK. The average uptake is generally low (in comparison to other countries in Europe and the uptake anticipated by NICE). The lighter shading indicates those areas with the lowest uptake.51
NICE technology appraisal guidance recommends NOACs as an option for the prevention of non-valvular AF-related stroke. However, there are many examples from across the UK where this guidance is not being put into practice.
In some areas, physicians are encouraged to follow particular treatment pathways that state that patients are eligible for NOACs only if warfarin treatment has been unsuccessful or if treatment with warfarin puts them at unacceptable risk of harm.52
In another location, the Area Prescribing Guidelines indicate that warfarin remains a suitable first line oral anticoagulant for the majority of patients, with only one of the NOACs indicated as a suitable option if any of the following apply:
• Patients require blood tests at home
• Patients known to have excess and unpredictable alcohol consumption
• Patients unable to comply with ongoing dose changes53,54
All of these examples result in restricting the numbers of patients in a locality who can access NOACs. These restrictions go beyond the NICE guidance and mean that patients in some areas of the country may not be offered NOACs as a treatment option, whereas their neighbours may be offered the choice.
IMS RSA Retail Sales Units per AF Patients (All NOACs) 2013 Q3
Units/AF Pt per locality
10
2
3

GPs in South Devon and Torbay have benefitted from a NOAC e-learning toolkit. The toolkit, which has been used by nearly all GPs in the South Devon and Torbay area, was specifically developed to provide heightened awareness of this novel drug class to reduce the risk of prescribing errors and support safe implementation of the NICE guidance covering the
NOACs. GPs were asked to return their responses to a set of multiple-choice questions on completion of the educational module.
With permission from Larissa Sullivan, Interface Pharmacist
Developing clinical confidence in Devon
16
Low clinical awareness and lack of confidence in using the NOACsAlthough a relatively new intervention in the prevention of non-valvular AF-related stroke, NOACs have been used in the UK for over two years in stroke prevention in AF and five years in VTE prevention after hip and knee replacement surgery. However, despite this and extensive supportive literature and guidance, GPs appear to lack confidence in their use to prevent AF-related stroke; with research showing that only 34% are willing to initiate NOAC therapy.34
In June 2013, the All Party Parliamentary Group on Atrial Fibrillation (APGAF) reported that: ‘The GRASP-AF initiative is beginning to demonstrate that GPs’ detailed knowledge of their under-treated patients is insufficient motivation to make the required changes to reduce stroke risk.’55
There is also a perception by some clinicians that warfarin is safer than the NOACs even though it is one of the most frequent causes of fatal and severe drug-related incidents.23 Clinical trials have shown that the NOACs are associated with a lower risk of intracranial haemorrhage than warfarin and are comparable or superior to warfarin with regard to the incidence of major bleeding.28,29,30
There should be no local barriers to accessing technologies recommended in NICE appraisals, beyond a clinical decision relating to an individual patient.Innovation, Health and Wealth Report, Department of Health, 2011.35
The patient voice is not being heard In many areas, patients are not being offered sufficient information about treatment options in the prevention of AF-related stroke and, as a result, are unable to make an informed choice about their care. They lack awareness of the NOACs and the advantages these novel therapies have to offer in simplifying their treatment regimens. Many patients are also unaware of their rights to treatment as set out in the NHS Constitution. As such, the majority lack the confidence to challenge decisions made about their healthcare and do not voice their opinions.
*GRASP-AF is a free, audit tool managed by NHS Improving Quality and used in primary care to assist in the identification and effective management of AF patients, in order to reduce the risk of stroke. Voluntary submission of data to a central server enables analysis of the initiative and provides users with the ability to benchmark their data against other practices.
Some NHS organisations have successfully adopted the NOACs but there are significant obstacles preventing the further spread of good practice.
Every appropriate patient who wants to take a NOAC and every clinician who wants to prescribe a NOAC should be able to.

Conclusions• The incidence of AF is increasing and needs to be addressed now in order to prevent future strokes and their
consequences for patients, their families and the NHS
• AF-related stroke has a potentially devastating impact on the patient and their families and carers, and is a significant contributor to UK death and disability
• AF-related stroke is preventable but current anticoagulation management is suboptimal and requires immediate attention
• Stroke care is costly – preventing AF-related stroke will save the NHS millions of pounds and have a positive impact on the UK economy
• NOACs are innovative medicines designed specifically to address the suboptimal management of anticoagulation in the prevention of non-valvular AF-related stroke: improving the patient experience and reducing the financial burden on the NHS
• The NOACs have been found to be a cost effective use of NHS resources by NICE31,32,33
• The 2012 European Society of Cardiology (ESC) guideline recommends NOACs as ‘broadly preferable to warfarin in the vast majority of patients with non-valvular AF, when used as studied in the clinical trials performed so far’22
• There is a wealth of evidence and NHS policy to support use of the NOACs in non-valvular AF-stroke prevention
• Patients are being denied timely access to NOACs because of barriers put up by local NHS organisations, even though the NOACs are approved by NICE as cost effective treatments for stroke prevention in non-valvular AF31,32,33

18
RecommendationsClinicians should:• Recognise that the rigorous
assessments of the EMA and NICE have evaluated the safety profile and clinical effectiveness of the NOACs
• Adopt and implement good practice in NOAC use according to NICE guidance and professional guidelines
• Review patients who are prescribed aspirin for stroke prevention in AF to ensure that the use of appropriate anticoagulation is optimised
• Address individual patient needs, and empower and enable patients to make fully informed decisions about anti-coagulation therapy
• Use the GRASP-AF tool as a matter of routine to identify people needing treatment for AF, to benchmark local performance and encourage the spread of best practice
• Ensure they are informed about the existing body of evidence supporting the NOACs
• Ensure prompt reporting of any adverse effects with NOACs to support a wider understanding of the NOACs and their efficacy and safety in different patient populations
Commissioners should:• Work with local stakeholders,
including primary healthcare professionals, clinical senates and strategic clinical networks to adopt NICE guidance on the NOACs
• Ensure that providers follow good practice according to the NICE Commissioning Guide
• Recognise the valuable impact of effective anticoagulation on indicators across a number of domains within the National Outcomes Framework
• Ensure that there is clear ownership and leadership for improving the management of AF in their localities
• Require that medicines optimisation principles are adopted in anticoagulation clinics
• Recognise the limitations of warfarin and address these, when appropriate, through the use of NOACs
• Take a whole-system approach to management of AF-related stroke that puts the cost of NOAC treatment in the context of the savings made by preventing strokes and reducing hospital admissions
• Provide an opportunity to deliver holistic care for patients via anticoagulation clinics and consider redistribution or decommissioning of excess clinic capacity freed up by NOAC use
Pharmacists should:• Work with clinicians to embed
medicines optimisation in anticoagulation clinics to prevent AF-related stroke
• Support patients to understand and optimise their anticoagulation therapy through Medicines Use Reviews (MURs) and the New Medicines Service (NMS)
• Ensure prompt reporting of any adverse effects with NOACs to support a wider understanding of the NOACs and their efficacy and safety in different patient populations
Patients should:• Understand their rights to NICE
approved medicines in the NHS Constitution
• Discuss their preferences and experiences with their healthcare professional to ensure that they are aware of all available treatment options and that they receive anticoagulation therapy that meets their needs
• Challenge NHS organisations denying patients NOAC therapy as a treatment option in accordance with NICE guidance
NHS England should:• Embed incentives to ensure a
whole-system approach to the prevention of AF-related stroke and ensure accountability at all levels of the system for the delivery of best practice
• Make anticoagulation a focus for medicines optimisation
• Include stroke prevention in the NHS Mandate, NHS Outcomes Framework and CCG Outcomes Indicator Set
• Work closely with the Operations Directorate to put measures in place to ensure that the NICE ‘Comply and Explain’ regime is implemented in practice
• Improve the usability of the Innovation Scorecard for local NHS organisations
• Include NOACs in future reports that make international comparisons on adoption of new medicines
• Ensure that NOACs as potential NHS High Impact Innovations are effectively promoted and incentivised to encourage service development and improved outcomes in localities
• Prioritise non-valvular AF-related stroke for a national CQUIN
• Ensure AHSNs support defined best practice on the use of NOACs in their areas
* GRASP-AF is a free, audit tool managed by NHS Improving Quality and used in primary care to assist in the identification and effective management of AF patients, in order to reduce the risk of stroke. Voluntary submission of data to a central server enables analysis of the initiative and provides users with the ability to benchmark their data against other practices.

References1. Royal Pharmaceutical Society. Medicines
Optimisation: Helping patients to make the most of medicines. Good practice guide for healthcare professionals in England. May 2013.
2. Public Health England. Act FAST. Available at: http://campaigns.dh.gov.uk/category/act-fast/
3. Ogilvie IM, Newton N, Welner SA, Cowell W, Lip GY. Underuse of oral anticoagulants in atrial fibrillation: a systematic review. Am J Med 2010;123638-645.e4.
4. Gladstone DJ, Bui E, Fang J, et al. Potentially preventable strokes in high-risk patients with atrial fibrillation who are not adequately anticoagulated. Stroke 2009;40:235-40.
5. National Institute for Health and Clinical Excellence. Atrial fibrillation: the management of atrial fibrillation. NICE Clinical Guideline 36. June 2006.
6. Stroke Association. What is a stroke: who is at risk? Available at: http://www.stroke.org.uk/about/who-risk
7. National Audit Office. Reducing brain damage: faster access to better stroke care. (HC 452 Session 2005–2006). London: The Stationery Office, 2005.
8. Brown V. Using the GRASP-AF audit tool to help prevent strokes in patients with AF. Presentation to NHS Alliance, 2012. Available at: http://nhsalliance2012.co.uk/Th9NHSImpAF.pdf
9. Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention; the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001;285:2370-5.
10. NHS Improvement. Commissioning for Stroke Prevention in Primary Care – The Role of Atrial Fibrillation. 2009. Available at: http://www.atrialfibrillation.org.uk/files/file/AF_Commissioning_Guide.pdf
11. Department of Health. Cardiovascular Disease Outcomes Strategy: Improving outcomes for people with or at risk of cardiovascular disease 2013. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/214895/9387-2900853-CVD-Outcomes_web1.pdf
12. Jorgensen HS, Nakayama H, Reith J, et al. Acute stroke with atrial fibrillation. The Copenhagen Stroke Study. Stroke 1996;27:1765–9.
13. Lloyd-Jones DM, Wang TJ, Leip EP, et al. Lifetime risk for development of atrial fibrillation: The Framingham Heart Study. Circulation 2004:110:1042-6.
14. Marini C, de Santis F, Sacco S, et al. Contribution of atrial fibrillation to incidence and outcome of ischemic stroke: results from a population-based study. Stroke 2005;36:1115-9.
15. National Audit Office Emergency admissions to hospital: managing the demand. (HC 739 Session 2013-14) London: The Stationery Office, 2013.
16. Royal College of Physicians Clinical Effectiveness and Evaluation Unit on behalf of the Intercollegiate Stroke Working Party. Sentinel Stroke National Audit Programme. Clinical Audit First Public Report. August 2013. Available at: http://www.rcplondon.ac.uk/sites/default/files/ssnap_first_pilot_national_report_january_-_march_2013_admissions_with_appendices_.pdf
17. Fernandez RL, Gray AM, Rothwell PM. Population-based study of determinants of initial secondary care costs of acute stroke in the United Kingdom. Stroke 2006;37:2579-87;
18. National Audit Office. Emergency admissions to hospital: managing the demand. http://www.nao.org.uk/report/emergency-admissions-hospitals-managing-demand/
19. Cowan C, Healicon R, Robson I, et al. The use of anticoagulants in the management of atrial fibrillation among general practice in England. Heart 2013;99:1166-72.
20. Hart RG, Pearce LA, Aguilar MI. Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: a meta analysis. Ann Intern Med 2007;146:857-67.
21. Cleland JG. Is aspirin useful in primary prevention? Eur Heart J 2013;34:3412-8.
22. Camm AJ, Lip GY, de Caterina R, et al. 2012 Focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J 2012;33:2719-47.
23. Cousins D, Gerrett D, Warner B. A review of medication incidents reported to the National Reporting and Learning System in England and Wales over 6 years (2005 – 2010). Br J Clin Pharmacol 2012;74:597-604.
24. National Institute for Health and Clinical Excellence. Atrial fibrillation: the management of atrial fibrillation. Costing Report Implementing NICE guidance in England. NICE Clinical Guideline 36. July 2006. Available at: http://www.nice.org.uk/nicemedia/live/10982/30061/30061.pdf

20
25. Fuster V, Ryden LE, Cannom DS, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 Guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2011;123:e269-e367.
26. Galanis T, Thomson L, Palladino M, Merli GJ. New oral anticoagulants. J Thromb Thrombolysis 2011;31:310–20.
27. de Caterina R, Husted S, Wallentin L, et al. New oral anticoagulants in atrial fibrillation and acute coronary syndromes: ESC Working Group on Thrombosis – Task Force on Anticoagulants in Heart Disease position paper. J Am Coll Cardiol 2012;59:1413–25.
28. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139-51.
29. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation N Engl J Med 2011;365:883-91.
30. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation N Engl J Med 2011;365:981-92.
31. National Institute for Health and Clinical Excellence. Dabigatran etexilate for the prevention of stroke and systemic embolism in atrial fibrillation. (NICE technology appraisal guidance 249). March 2012.
32. National Institute for Health and Clinical Excellence. Rivaroxaban for the prevention of stroke and systemic embolism in people with atrial fibrillation. (NICE technology appraisal guidance 256). May 2012.
33. National Institute for Health and Clinical Excellence. Apixaban for preventing stroke and systemic embolism in people with non-valvular atrial fibrillation. (NICE technology appraisal guidance 275). February 2013.
34. NICE Implementation Collaborative Pilot 2 Update – Novel Oral Anticoagulants. Available at: http://www.aomrc.org.uk/publications/reports-a-guidance/doc_details/9676-pilot-2-noac.html
35. Innovation Health and Wealth. Accelerating adoption and diffusion in the NHS. Department of Health, NHS Improvement & Efficiency Directorate, Innovation and Service Improvement. 5th December 2011.http://www.networks.nhs.uk/nhs-networks/life-sciences/documents/InnovationHealth-Wealth.pdf/view
36. The NHS Outcomes Framework 2013-14. Department of Health. 13 November 2012. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/256456/NHS_outcomes.pdf
37. Improving outcomes and supporting transparency. A Public Health Outcomes Framework for England Parts 1A and 1B 2013-16. Department of Health. January 2012. Available at: https://www.gov.uk/government/publications/healthy-lives-healthy-people-improving-outcomes-and-supporting-transparency
38. NHS England. CCG Outcomes Indicator Set 2014/15 – at a glance. December 2013. Available at: http://www.england.nhs.uk/wp-content/uploads/2013/12/ccg-ois-1415-at-a-glance.pdf December 2012.
39. Quality and Outcomes Framework guidance for GMS Contract 2013/14. NHS Employers. March 2013. Available at: http://www.nhsemployers.org/Aboutus/Publications/Documents/qof-2013-14.pdf
40. NICE Commissioning Guides. Support for commissioning anticoagulation therapy. May 2013. Available at: http://www.nice.org.uk/guidance/cmg49
41. Department of Health. The NHS Constitution for England: The NHS belongs to us all. 26 March 2013. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/170656/NHS_Constitution.pdf
42. NHS Commissioning Board. Everyone Counts: Planning for Patients 2013/14. Available at: http://www.england.nhs.uk/wp-content/uploads/2012/12/everyonecounts-planning.pdf
43. Innovation Health and Wealth. Catalogue of Potential Innovations. March 2013. Available at: http://innovault.innovation.nhs.uk/pg/dashboard
44. Association of the British Pharmaceutical Industry (ABPI). Delivering Value to the UK. The contribution of the pharmaceutical industry to patients, the NHS and the economy. January 2014. Available at: http://www.abpi.org.uk/our-work/library/industry/Pages/310114.aspx
45. IMS Health, MIDAS, August 2013. NOACs include Dabigatran, Rivaroxaban and Apixaban. All anticoagulants include Vitamin K Antagonists (e.g. Warfarin), Heparin (fractionated and unfractionated), NOACs and Fondaparinux.

46. National Institute for Health and Clinical Excellence. Dabigatran etexilate for the prevention of stroke and systemic embolism in people with atrial fibrillation. Costing template. Implementing NICE guidance. NICE 2012. Available at: http://guidance.nice.org.uk/TA249/CostingTemplate/xls/English
47. National Institute for Health and Clinical Excellence. Rivaroxaban for the prevention of stroke and systemic embolism in people with atrial fibrillation. Costing template. Implementing NICE guidance. NICE 2012. Available at: http://guidance.nice.org.uk/TA256/CostingTemplate/xls/English
48. National Institute for Health and Care Excellence. Apixaban for preventing stroke and systemic embolism in people with nonvalvular atrial fibrillation. Costing Statement. NICE 2013. Available at: http://www.nice.org.uk/nicemedia/live/14086/62922/62922.pdf
49. All-Party Parliamentary Group on Atrial Fibrillation. Access to treatments: what are the barriers to patients accessing the most appropriate treatments? Meeting summary, 4th December 2012. Available at: http://www.atrialfibrillation.org.uk/files/file/APGAF%20Report,%20December%202012.pdf
50. Health and Social Care Information Centre. Use of NICE appraised medicines in the NHS in England – 2012, experimental statistics. 21 January 2014. Available at: http://www.hscic.gov.uk/catalogue/PUB13413/use-nice-app-med-nhs-exp-stat-eng-12-rep.pdf
51. IMS RSA Retail Sales Units per AF Patients (All NOACs) 2013 Q3.
52. Prescribing Points. Oxfordshire CCG Statement on the use of Dabigatran (▼Pradaxa®) in the Prevention of Stroke and Systemic Embolism in Adult Patients with Non-valvular Atrial Fibrillation (AF). Available at: http://www.oxfordshireccg.nhs.uk/wp-content/uploads/2013/08/Prescribing-Points-Vol-21-04-Dabigatran-and-rivaroxaban-in-AF-v2-updated-apr-13.pdf. Last accessed 18/03/14.
53. Nottinghamshire Area Prescribing Committee. Position statement for the prescribing of the Novel Oral Anticoagulants (NOACs) - dabigatran (Pradaxa), rivaroxaban (Xarelto) and apixaban (Eliquis). July 2013. Available at: http://www.nottsapc.nhs.uk/attachments/article/3/novel%20oral%20anticoagulants%20position%20statement.pdf. Last accessed 18/03/14.
54. Nottinghamshire Area Prescribing Committee. Rivaroxaban for prevention of Stroke in patients with non-valvular atrial fibrillation. November
2012. Available at: http://www.nottsapc.nhs.uk/attachments/article/3/rivaroxaban%20in%20af.pdf. Last accessed 18/03/14.
55. All-Party Parliamentary Group on Atrial Fibrillation. Commissioning for Change: AF within the new NHS. Meeting Summary 24 June 2013.

22

Association of the British Pharmaceutical Industry7th Floor, Southside, 105 Victoria Street, London SW1E 6QTt +44 (0)870 890 4333 [email protected]
abpi.org.uk
SAFI/14/02 Date of preparation: March 2014