No ducking. Facial fractures in the AFL.
2
INSIDE FOOTBALL WEDNESDAY, OCTOBER 31, 2012 34 Inside features 34 X H ORRIFIC. That’s the only word fit to describe the facial fractures suffered by some of AFL’s greatest players including James Hird and Jonathan Brown. So severe were Hird’s and Brown’s injuries that they were likened to those of high-speed car crash victims. These injuries rank among some of the worst the AFL has seen and have repercussions extending beyond the footy field. Such is the severity of some facial fractures that they have the potential to cause “the temporary or permanent loss of function thereby threatening a player’s earning potential and length of playing career” according to a recent research paper published in the ANZ Journal of Surgery. Thankfully, the research shows a trend towards fewer incidences of facial fractures in the AFL. Researchers, including sports physician and AFL Injury Report co-author Dr John Orchard, reviewed facial fractures from the injury records collected by the AFL over 17 seasons between 1992 and 2008. They investigated facial fractures by frequency, location, time of season, player recovery, fracture incidence per season and geographical location of the injury. Over the 17 years of the study, AFL players were reported to have sustained a total of 175 facial fractures, accounting for fewer than 2 per cent of total injuries to AFL players in that time. Players missed 517 games as a result of their injuries, averaging three games per injury. The facial skeleton is composed of 14 bones; eight bones form the nasal cavity as well as contributing to other parts of the face. The most common facial fracture sustained in the AFL over the period of the research was to the zygomaticomaxillary complex (41 per cent), also known as a tripod fracture. Fractures of this kind damage the bone around the eye, under the eye and the cheekbone. The next most common type of fracture was to the lower jawbone (37 per cent). A long-standing definition for an injury to be included in the stats is that the player must miss a game as a result. Consequently, many broken noses and minor facial fractures are not recorded in any survey. Chris Judd’s broken nose in Round 12, 2009 was such an injury. Judd’s nose was broken just minutes into the second half of the game against the Saints when he collided with teammate Stephen Browne. He returned to play but left the field multiple times under the blood rule as the doctors found it hard to stop the bleeding. If you’ve ever had a hard knock to the nose, you’ll know the experience is painful. Judd’s nose was badly broken and he just kept going back on to play. After plugging his nose with gauze was unsuccessful, doctors inserted a bladder into his nose and inflated it in an attempt to compress the blood vessels to stem the bleeding. Judd had surgery the day after the injury, was lucky to have the bye the next week, and returned for Carlton’s next game. Dr Jason Savage, trainee max- illofacial surgeon and author The AFL has put its head over the ball in trying to reduce serious facial injuries, writes DR JODI RICHARDSON. NO DUCKING! of the research paper on facial fractures in the AFL, explains that the surgical management of these injuries can be influenced by what the player wants to do. “Football is a profession and players want to get back to playing,” Dr Savage said. “There are several cases where players have significant facial fractures, consult a surgeon, undergo surgery and then play the following week.” The report’s authors have recommended that the AFL change the injury definition and extend the scope of injury reporting to include other forms of maxillofacial trauma to get a true picture of these injuries so that prevention measures can be implemented accordingly. Facial fractures can have serious short-term and lifelong consequences. They can result in permanent eye damage, blindness, facial deformity, scarring, poor healing (non-union of the fracture site), infection and the loss of sensation. For example if the lower jaw is fractured, teeth may be damaged, the dental occlusion may change affecting the bite and sensory nerves can be damaged affecting speech. Of course given that facial fractures are the result of a severe blow to the head, concussion is a consideration. At times surgeons cannot reconnect the facial bones exactly the same way they were positioned prior to the injury. “Warnings for patients include bleeding, bruising, pain, swelling and the possibility of infection,” Dr Savage explained. “For the two most common AFL facial fractures, players are warned of a change in their occlusion, where their teeth may not bite together in the way they did prior to the injury. “We try to reposition their occlusion exactly the way it was, but if you have ever had a filling and it’s even half a millimetre too high, it doesn’t feel quite right. “Sometimes a patient will have a 1-2cm gap where they used to touch as a result of the way they fractured their maxilla (upper) or mandible (lower jawbone).” Ten years ago James Hird suffered shocking facial injuries after colliding with the knee of teammate Mark McVeigh. Dr Peter Larkins reported on Channel Nine at the time that Hird suffered a compound or open fracture, meaning that parts of bone were visible after the injury. He explained that Hird’s injury was a five-part fracture incorporating most of the left eye socket, and parts of the forehead, nose and upper teeth. “His whole middle third of his face got shifted to the right side when he got hit on the left side,” Dr Larkins said. “This is an injury we normally see in motor-car accidents where the middle third of the face gets caved in. It’s a common trauma injury in high-velocity accidents. Players undergo general anaesthetic for facial fracture surgery. To avoid scarring, surgeons make their incisions inside the mouth to repair facial fractures wherever possible. Often, surgeons use malleable titanium plates called mini plates to fix fractures. These plates remain within the patient. “Occasionally, if you have a fracture with a lot of displacement, such as a mandibular fracture (of the lower jawbone) or if a player wants to return to play straight away, surgeons can attach larger ‘reconstruction plates’ which are a lot thicker and bulkier and can be taken out after a period IMPACT: James Hird. JUDD: Nose rearranged, 2009. ‘His whole middle third of his face got shifted to the right side when he got hit on the left side.’ – DR PETER LARKINS ON JAMES HIRD BROWN OUT: The Brisbane skipper hits the deck.
-
Upload
jodi-richardson -
Category
Documents
-
view
231 -
download
0
description
HORRIFIC. That’s the only word fit to describe the facial fractures suffered by some of AFL’s greatest players including James Hird and Jonathan Brown. So severe were Hird’s and Brown’s injuries that they were likened to those of high-speed car crash victims. These injuries rank among some of the worst the AFL has seen and have repercussions beyond the footy field.
Transcript of No ducking. Facial fractures in the AFL.

InsIde Football Wednesday, OctOber 31, 2012
34 Inside features34
X
HORRIFIC. That’s the only word fit to describe the facial
fractures suffered by some of AFL’s greatest players including James Hird and Jonathan Brown.
So severe were Hird’s and Brown’s injuries that they were likened to those of high-speed car crash victims.
These injuries rank among some of the worst the AFL has seen and have repercussions extending beyond the footy field.
Such is the severity of some facial fractures that they have the potential to cause “the temporary or permanent loss of function thereby threatening a player’s earning potential and length of playing career” according to a recent research paper published in the ANZ Journal of Surgery.
Thankfully, the research shows a trend towards fewer incidences of facial fractures in the AFL.
Researchers, including sports physician and AFL Injury Report co-author Dr John Orchard, reviewed facial fractures from the injury records collected by the AFL over 17 seasons between 1992 and 2008.
They investigated facial fractures by frequency, location, time of season, player recovery, fracture incidence per season and geographical location of the injury.
Over the 17 years of the study, AFL players were reported to have sustained a total of 175 facial fractures, accounting for fewer than 2 per cent of total injuries to AFL players in that time. Players missed 517 games as a result of their injuries, averaging three games per injury.
The facial skeleton is composed of 14 bones; eight bones form the nasal cavity as well as contributing to other parts of the face.
The most common facial fracture sustained in the AFL over the period of the research was to the zygomaticomaxillary
complex (41 per cent), also known as a tripod fracture. Fractures of this kind damage the bone around the eye, under the eye and the cheekbone.
The next most common type of fracture was to the lower jawbone (37 per cent).
A long-standing definition for an injury to be included in the stats is that the player must miss a game as a result. Consequently, many broken noses and minor facial fractures are not recorded in any survey.
Chris Judd’s broken nose in Round 12, 2009 was such an injury.
Judd’s nose was broken just minutes into the second half of the game against the Saints when he collided with teammate Stephen Browne. He returned to play but left the field multiple times under the blood rule as the doctors found it hard to stop the bleeding.
If you’ve ever had a hard knock to the nose, you’ll know the experience is painful. Judd’s nose was badly broken and he just kept going back on to play.
After plugging his nose with gauze was unsuccessful, doctors inserted a bladder into his nose and inflated it in an attempt to compress the blood vessels to stem the bleeding.
Judd had surgery the day after the injury, was lucky to have the bye the next week, and returned for Carlton’s next game.
Dr Jason Savage, trainee max-illo facial surgeon and author
The AFL has put its head over the ball in trying to reduce serious facial injuries, writes DR JODI RICHARDSON.
NO DUCKING!
of the research paper on facial fractures in the AFL, explains that the surgical management of these injuries can be influenced by what the player wants to do.
“Football is a profession and players want to get back to playing,” Dr Savage said.
“There are several cases where players have significant facial fractures, consult a surgeon, undergo surgery and then play the following week.”
The report’s authors have recommended that the AFL change the injury definition and extend the scope of injury reporting to include other forms of maxillofacial trauma to get a true picture of these injuries so that prevention measures can be implemented accordingly.
Facial fractures can have serious short-term and lifelong consequences.
They can result in permanent eye damage, blindness, facial deformity, scarring, poor healing (non-union of the fracture site), infection and the loss of sensation.
For example if the lower jaw is fractured, teeth may be damaged, the dental occlusion may change affecting the bite and sensory nerves can be damaged affecting speech.
Of course given that facial fractures are the result of
a severe blow to the head, concussion is a consideration.
At times surgeons cannot reconnect the facial bones exactly the same way they were positioned prior to the injury.
“Warnings for patients include bleeding, bruising, pain, swelling and the possibility of infection,” Dr Savage explained.
“For the two most common AFL facial fractures, players are warned of a change in their occlusion, where their teeth may not bite together in the way they did prior to the injury.
“We try to reposition their occlusion exactly the way it was, but if you have ever had a filling
and it’s even half a millimetre too high, it doesn’t feel quite right.
“Sometimes a patient will have a 1-2cm gap where they used to touch as a result of the way they fractured their maxilla (upper) or mandible (lower jawbone).”
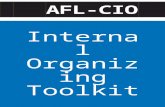
Ten years ago James Hird
suffered shocking facial injuries after colliding with the knee of teammate Mark McVeigh.
Dr Peter Larkins reported on Channel Nine at the time that Hird suffered a compound or open fracture, meaning that parts of bone were visible after the injury.
He explained that Hird’s injury was a five-part fracture incorporating most of the left eye socket, and parts of the forehead, nose and upper teeth.
“His whole middle third of his face got shifted to the right side when he got hit on the left side,” Dr Larkins said.
“This is an injury we normally see in motor-car accidents where the middle third of the face gets caved in. It’s a common trauma injury in high-velocity accidents.
Players undergo general anaesthetic for facial fracture surgery. To avoid scarring, surgeons make their incisions inside the mouth to repair facial fractures wherever possible.
Often, surgeons use malleable titanium plates called mini plates to fix fractures. These plates remain within the patient.
“Occasionally, if you have a fracture with a lot of displacement, such as a mandibular fracture (of the lower jawbone) or if a player wants to return to play straight away, surgeons can attach larger ‘reconstruction plates’ which are a lot thicker and bulkier and can be taken out after a period
IMPACT: James Hird.
JUDD: Nose rearranged, 2009.
‘His whole middle third of his face got shifted to the right side when he got hit on the left side.’ – DR PETER LARKINS ON JAMES HIRD
BROWN OUT: The Brisbane skipper hits the deck.

InsIde Football Wednesday, OctOber 31, 2012
‘ ’
Cit
yVis
taC
ourt
LockwoodCourt
Osprey Drive
Sp
ringla
nds
Cre
scent
Bra
mle
yP
lace
Jard
ine
Drive
Hume Drive
Als
ace
Way
SpringlandsCrescent
LockwoodCourt
Medium Density
Future
Neighbourhood
Convenience
Centre
HollydeneW
ay
25.18
7.07
7.07
7.07
7.08
7.07
27
27
9.29
9.29
27.0726.39
4.5
12
27
10
5.8
585
467
445
461
358
467
150
579
22.66
31.83
10
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLDSOLDSOLD
SOLD
SOLD
’• Talented player group• Dedicated and well resourced back office support• UQ coaching qualifications available
The UQAFC is looking to appoint a Senior Coach for our elite playing group. The Club has grown from two to four senior teams culminating in 2012 being the most successful year on field for the club in its history with two Premierships. Backed by a well resourced and professional off-field structure and a wealth of talented athletes, the Senior Coach will play a key role in establishing the club and delivering success at higher levels of competition.
This unique opportunity has significant benefits including:• Developing a talented playing group backed by a scholarship program • Professional committee structure and enthusiastic Old Boys support• The opportunity to receive University qualifications in coaching• Access to coaching conferences, sports science and medical resources• Preferred access to campus sports infrastructure and all-weather off-campus
training facilities • Assistant coaches, confirmed lower grade appointments and salary.
The UQAFC is keen to progress on and off the field such that the Senior Coach will be provided the resources to help take the club to new levels of operating excellence. The club seeks an experienced coach with a track record of success where a professional culture and player development are paramount. Applicants from interstate are welcome to apply.
Please send applications to [email protected] with a CV including referees’ details. Thank you in advance for your application.
SENIOR COACH – UQAFCof time requiring a second operation,” Dr Savage said.
“However, this does not happen very often.
“Patients are then put on pain relief medication and antibiotics, and are normally advised to go on a soft food diet for six weeks so as not to put too much pressure on the plates as the bone heals.”
Six weeks of rest is recommended after surgery to allow enough time for the bones to heal well, however, three weeks is the ave r age number of games missed.
Players undoubtedly have concerns over re-injury when they return to the field so soon after surgery but statistically there is not a high rate of recurrence.
“There is increased risk of more damage when players return to play before the bone is repaired but they are prepared to take the risk,” Dr Orchard said.
“Players roll the dice with facial fractures and factors such as finals contention come into play when they are making these decisions.”
Dr Orchard said that for the general community a facial fracture was a significant injury psychologically and many would struggle to get back to playing hard football after the event but AFL players were
usually different.“The majority of players
would prefer a facial fracture to an injury that will affect their ability to run,” Orchard said.
The good news is that the past three years of the facial fractures study between 2006 and 2008 showed a trend of decreased incidence in the AFL.
Much of this reduction is likely due to the introduction of the Match Review Panel in 2005 as the report shows marked differences in facial fracture incidence after this change.
“In the 13 seasons prior to the rule change, a mean of 11.2 fractures per season were recorded. This was reduced to a mean of 7.5 in the four seasons from 2005 to 2008,” Dr Savage and colleagues reported.
“The introduction in 2007
of a free kick for any front-on contact to a player with his head over the ball or for high contact to a player may have also encouraged safer play, but with few seasons since its introduction this is difficult to assess on facial fracture results.”
In the 2011 AFL season there was an increase in the number of games missed as a result of concussion.
There is more publicity around concussion than ever before and it is possible that club doctors, players and coaches are taking a more conservative approach, which will influence this injury statistic.
This apparent increase in concussion means it is being taken more seriously. The AFL is trying to decrease the incidence of head contact and the results from the facial fractures article suggest that related rule changes are in fact effective.
“The documented recent fall in facial fractures shows that head high contact is actually dropping in AFL,” Dr Orchard said.
“Because concussion is so hard to measure, we can’t really rely on comparison of past and current concussion rates as the reporting threshold is changing as much as the actual incidence.
“However, missed games due to facial fractures are a much more objective measure.”
HIRD: Returned with protection.