Nuclear Magnetic Resonance (NMR) Spectroscopy Part 1 Carbon 13 NMR.

NMR Spectroscopy of theHuman HeartPaul A. BottomleyJohns Hopkins University, Baltimore, MD, USA
1 Introduction 12 Methods 23 Results 94 Conclusions 165 Limitations 176 Related Articles 177 References 18
1 INTRODUCTION
The heart is the largest consumer of energy per gram oftissue, and disruptions in energy metabolism, including energysupply and demand, are thought to play a central role in manycommon diseases affecting the heart. Therefore, it is perhapsinevitable that the first human cardiac spectroscopy focusedon those energy metabolites that are NMR-detectable.1,2
Phosphorus (31P) NMR spectroscopy (MRS) can detect andmeasure adenosine triphosphate (ATP), the fundamental energycurrency of the body,1 – 3 phosphocreatine (PCr), a cellularenergy reserve, as well as the metabolic by-product, inorganicphosphate (Pi) in the heart. The chemical shift of Pi relativeto PCr is pH-dependent, permitting a measure of intracellularpH.4,5
Unfortunately, the signal-to-noise ratio (SNR) of thesemetabolites is about 2 × 10−6 to 20 × 10−6 that of the proton(1H) NMR signal from tissue water from the same volumeat the same magnetic field strength (B0),3 primarily due tothe low metabolite concentrations, which typically fall in therange 1–20 µmol g−1 wet weight of tissue (Table 1). PCrand ATP therefore cannot be imaged with the same spatialresolution, SNR and scan time as tissue water protons at thesame B0. Nevertheless, with compromises, primarily to spatialresolution and to a lesser extent scan time, PCr and ATP canbe measured in volume elements (voxels) as small as about8 ml in the anterior myocardium.6,7 This, with SNR levels thatare comparable to the SNR seen in the sub-microliter voxelsroutinely acquired by 1H MRI (Table 1).
1.1 Creatine Kinase Metabolism
PCr and ATP are linked via the reaction catalyzed by creatinekinase (CK), which serves as the prime energy reserve for theheart:
PCr + adenosine diphosphate (ADP) �k ATP + creatine (Cr)
(1)where k is the pseudo-first-order forward reaction rate constantmeasured in s−1. The product of k with the PCr concentration,
[PCr], is the forward CK flux rate, {k · [PCr]}, for generatingATP from adenosine diphosphate (ADP). Thus k can beinterpreted as the fraction of the PCr pool turning over persecond to generate ATP. Both k, and CK flux measurements arenow possible in the hearts of healthy volunteers and patientsvia new, four-angle saturation transfer (FAST ) 31P MRSsaturation transfer methods.9 The ATP pool is used to generateenergy to support cell function and muscular contraction:
ATP → ADP + Pi + energy (2)
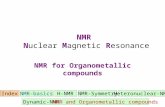
It is hypothesized that the CK reaction serves as an intra-cellular spatial energy shuttle and temporal buffer, facilitatingthe transfer of high-energy phosphate in the form of PCr fromthe mitochondria where ATP is produced via oxidative phos-phorylation, to the myofibrils where it is used.10,11 Cr is thenreturned to the mitochondria for rephosphorylation. Althoughsuch a shuttle may involve serial CK reactions distributedbetween the two sites, the upshot is a net transfer of high-energy phosphate, as shown in Figure 1. In this context, the31P MRS saturation transfer measurements9 would provide abulk-tissue average measurement of the flux through the shut-tle. For the shuttle to serve as a meaningful temporal buffer, itmust have sufficient capacity to deliver ATP to fuel contractilefunction over the entire range of normal cardiac function, andthe initial studies suggest that this is indeed the case.9
The penultimate participant in the CK reaction, Cr, isindirectly accessible to human cardiac MRS via its N-methylresonance at 3.0 parts per million (ppm) in the 1H spectrumrelative to tertramethyl silane (TMS). Unfortunately, thisresonance does not permit, at least at clinical MRI fields ofup to 3 T, differentiation of Cr from PCr. Thus the 3.0 ppmresonance measures the total creatine pool, [CR] = [Cr] +[PCr].13,14 [Cr] is , however, obtainable from joint 31P and1H MRS measurements of [PCr] and [CR].15 The spatialresolution of the [CR] measurements (Table 1) is presentlyabout 3–9 ml with scan times of less than 10 min for 1.5–3 T.With PCr, CR, ATP, Pi, pH, k, and CK flux measurements nowobtainable via a combination of 1H and 31P MRS methods, thelast ingredient, ADP can be estimated9 to complete the pictureof CK metabolism in human heart.
1.2 Other Moieties
While endogenous phosphorus energy metabolites dominatethe in vivo cardiac 31P spectrum, this is certainly not thecase for 1H MRS. The 1H spectrum is dominated by waterat 4.68 ppm, about a thousand times more intense than CR(Table 1). To view CR, the water must be suppressed (seeWater Suppression in Proton MRS of Humans and Animals),but in nonsuppressed spectra it can also serve as a convenientconcentration reference.13,14 In addition, the heart is typicallysurrounded by pericardial fat which generates intense lipidsignals from (–CH2 –)n and –CH3 moieties that fall inthe range 0–2.5 ppm, which can contaminate the typicallylarger voxels used in MRS studies. Nevertheless, myocardiallipids are discernible,16 and the pericardium can be avoidedentirely by positioning MRS voxels in the septum, whereuponintramyocardial triglyceride levels can be measured. Thesemay provide useful insights into the effects of obesity on the

2 NMR SPECTROSCOPY OF THE HUMAN HEART
Table 1 Relative sensitivity of cardiac metabolites detected by 1H and 31P MRS
Factor 100% H2O Tissue H2O (77%) 1H MRS of CR 31P MRS of PCr
Nuclear magnetic moment 2.79268 1.1305Relative magnetic moment 1.000 0.4048Sensitivity at constant B0/nucleusa 1 0.06634Relative SNR at constant B0/nucleusb 1 1 1 0.164In vivo concentration of substance (mol kg−1) 55.6 42.8 0.025 0.010In vivo concentration of nucleus in moiety (mol kg−1) 111.1 85.6 0.075 0.010Relative SNR of moiety 111.1 85.6 0.075 0.00164SNR relative to CR 1 0.02185SNR relative to PCr 45.8 1SNR relative to tissue water 1.30 1 8.77 × 10−4 1.92 × 10−5
Effect of voxel sizeTypical voxel size (ml) 0.00075 4 20Relative SNR, voxel size corrected 1 4.68 0.511Effect of relaxation and voxel sizeT2 decay factor 0.74 1T1 saturation factor at TR ∼ 1 s, 60◦ flip-angle 1.77 3.4SNR relative to PCr, T1, T2, & voxel-size corrected 6.6 1
B0, main field strength; SNR, signal-to-noise ratio; CR, total of phosphorylated and unphosphorylated creatine; TR, sequence repetition period; T1,cardiac longitudinal relaxational time; T2, cardiac transverse relaxation time.Mean T1 and T2 data are taken from Refs 13, 14, 49 at 1.5T; other values are assumed as stated. [ATP] ∼ [PCr]/2, so its sensitivity is about halfof PCr.aSensitivity is proportional to the magnetic moment cubed.bAssumes sample-dominant noise (SNR ∼ B0).
PCr
Cr
PCr
Cr
CK CKk
ATP
ADP + Pi
Myofibril
Energy sink
ATP
ADP + Pi
Mitochondria
Energy source
Figure 1 Illustration of the CK shuttle hypothesis in myocytes.10 ATPgenerated by oxidative phosphorylation in the mitochondria phospho-rylates Cr via CK to create PCr. The process may continue in theintracellular space until PCr arrives at the myofibrils, where PCr andADP are combined via CK to create ATP for muscular contraction.Unphosphorylated Cr eventually returns to the mitochondria. The pro-cess results in a transfer of biochemical energy from the mitochondriato the myofibrils. The CK pseudo-first-order reaction rate, k, measuredby 31P MRS saturation transfer9,12 would represent a tissue averagemeasure of the transfer rate
human heart17,18 (see also Body Fat Metabolism: Observationby MR Imaging and Spectroscopy).
MRS studies of the human heart with nuclei other than 31Pand 1H are few. Carbon (13C) potentially provides access toglycolytic and citric acid cycle metabolites such as lactate andglutamate, but has the disadvantage of low NMR sensitivityand a 1.1% natural isotopic abundance (see also ProtonDecoupling in Whole Body Carbon-13 MRS). This effectivelyprevents the detection of metabolites with concentrations in the1–10 µmol g−1 range at natural abundance using conventional
technology. Infusions of 13C-enriched metabolic substrateshave been exploited extensively in animal studies, but areexpensive for human trials owing to the amount of materialrequired and/or the need for targeted delivery. Otherwise,fatty acid resonances are the main contributors to the naturalabundance 13C human heart spectrum, of which pericardialfat is probably the dominant contaminant for studies of theventricular wall. Lipid (–CH2 –)n is at ∼30 ppm relative toTMS in natural abundance 13C spectra, glycerol and carboxyl(–CO) resonances are at 170 ppm, and glycogen may bediscernible at about 101 ppm with 1H-decoupling and nuclearOverhauser enhancement (nOe).19
Hyperpolarization, with mind-boggling potential SNR gainsof ∼105, is the technique of the future for 13C MRS studies ofglycolytic metabolism in the heart.20,21 There are no humanstudies to report yet, but hyperpolarized 13C metabolic imagesof lactate, alanine, bicarbonate, and pyruvate in a pig heartfollowing coronary occlusion are very exciting.
2 METHODS
2.1 Spatial Localization: 31P and 13C MRS
In 1980, small surface coils were introduced for performinglocalized in vivo MRS in animals22; these were placeddirectly against the rabbit heart to study high-energy phosphatemetabolism in regional ischemia and its response to therapy, in1981.23 Surface coils provide spectra whose contributions areheavily weighted toward signal sources lying closest to the coil(see also Surface Coil NMR: Detection with InhomogeneousRadiofrequency Field Antennas; Surface and Other LocalCoils for In Vivo Studies). This weighting is compoundedwhen the same coil is used for both detection and excitation,

NMR SPECTROSCOPY OF THE HUMAN HEART 3
as is often the case, due to the nonuniform transmit field.24
Thus, a 31P surface coil placed on the chest is not by itselfsuitable for providing unambiguous localization to the humanheart, because the detected MRS signals will be dominated bythe intense signals from superficial skeletal muscle.
Localized 31P NMR spectroscopy of the human heart wasfirst reported in 1985.1 That study, and all human cardiac 31PMRS performed since, employed surface detection coils placedon the chest close to the anterior myocardium. In the initialstudy,1 the myocardium was distinguished from chest wallusing the depth resolved surface coil spectroscopy (DRESS )technique. DRESS employs MRI slice selection wherein afrequency-selective pulse is applied in the presence of agradient directed along the surface coil axis, to select slicesparallel to the surface coil in a single excitation25 (see alsoSelective Excitation in MRI and MR Spectroscopy). The sliceis positioned relative to the heart under 1H MRI guidance.
While an unlocalized 31P MRS surface coil study ofthe chest of an infant with congenital cardiomegaly wasreported in 1985,2 the first localized human studies of heartpatients were not published until 1987. The latter were limitedto several patients with recent myocardial infarction (MI)4
and hypertrophic cardiomyopathy (HCM)26 with localizationafforded by DRESS or rotating frame zeugmatography (RFZ),respectively. RFZ uses the inherent nonuniformity of the RFexcitation field, B1, produced by surface coil excitation,27 inlieu of the MRI gradients employed by DRESS. Basically, inRFZ, the flip angle, θ , is stepped in many repeat applicationsof the sequence, whereupon the Fourier transform (FT) of theresulting acquisitions with respect to the flip-angle dimension,map the spectra to the B1 contours of the surface coil (see alsoRotating Frame Methods for Spectroscopic Localization).
Both DRESS and RFZ add localization essentially onlyin the dimension perpendicular to the surface coil. Thus,they rely on the intrinsic fade-off in sensitivity in the planeparallel to the coil axis to limit sensitivity in the two otherdimensions. Importantly, the relative fade-off decreases withboth increasing surface coil radius and depth from the coil,so that the effective size of the 31P MRS DRESS and RFZvoxel increases with surface coil size and with the depth ofthe tissue being examined. The first fully three-dimensional(3-D) localized 31P MRS spectra from the heart were obtainedby the image selected in vivo spectroscopy (ISIS) technique in1988.28 The ISIS method uses selective MRI inversion pulsesin all three dimensions (see also Single Voxel Whole BodyPhosphorus MRS). Each of these three pulses is either appliedor not applied in a cycle of eight excitations, followed bynonselective excitation. The resultant signals are added andsubtracted to obtain a spectrum from the single voxel that liesat the intersection of the three inverted planes.29
Multiple voxel 31P chemical shift imaging (CSI), studiesof the human heart using MRI phase-encoding gradients inone,30 two,24 and three31 dimensions were first published in1990 (see also Chemical Shift Imaging). CSI requires repeatapplication of a sufficient number of gradient pulses in eachdimension to span the field of view (FOV) at the desiredspatial resolution and avoid aliasing.8 These spectroscopylocalization techniques are also reviewed elsewhere (seeSpatial Localization Techniques for Human MRS), but aredepicted for reference in Figure 2. In practice, hybrids ofthese methods are commonly used, such as slice-selective 2-DCSI,24 or 1-D CSI combined with 2-D ISIS, to optimize the
RF
RF gradient
RF
RF
RF
RF
Acquire
Acquire
Acquire
Acquire
π π π a
a
± y t
t
t
t
nq x
Uniform RF
Acquire
t
a
a
a
Gy
Gy
GxGy
Gz
Gz
Gy
Gx
(a)
(b)
(c)
(d)
(e)
Figure 2 Timing diagrams for the DRESS (a), RFZ (b), 1-D CSI(c), ISIS (d), and (e) slice-selective 3-D CSI pulse sequences (left) forlocalizing MRS signals to various voxels in the heart (right; adaptedfrom Ref. 32). Gx, Gy , and Gz are imaging gradients in the threeCartesian directions, and MRS pulses with flip angles of α or π areapplied on the RF channel. With DRESS (a), a plane is selectivelyexcited in a single sequence application. In RFZ (b), the sequenceis repeated with different pulse flip-angle increments, θ , and the FTof the data set maps the spectra to the B1 contours of the surfacecoil. 1-D CSI, (c), requires repeat application of an imaging phase-encoding gradient, Gy , applied in the vertical direction, and the FT withrespect to Gy amplitude yields a set of spectra from all of the slicesencoded parallel to the detector. ISIS (d) selectively excites a singlevolume if the signals acquired serially from all eight combinations of thex-, y-, and z-selective excitation pulses being applied and not applied,are properly added. In (e), an axial slice through the chest is selectivelyexcited, and the remaining two dimensions encoded by the other twogradients. The sequence is repeated N = Nx · Ny times where Nx · Ny
is the array size. A 2-D FT with respect to gradient amplitude yieldsthe spatial information

4 NMR SPECTROSCOPY OF THE HUMAN HEART
DPG
16
ATP
15
14
13
Depth
12
20ppm(a) (b)
0
9
PCr
PCr
PME
Pi
Ref.
PDE
DPG
LV
Stu: 08734Ser: 001/02Ima: 001/003
SE RV16
15
14
1312
109
Figure 3 (a) Typical axial 1H surface coil image of the chest and heart of a normal volunteer, annotated to show location of eight 1-cm thickcoronal slices localized in the spectroscopy examination. (b) Cardiac-gated 1-D CSI surface coil 31P spectra from the slices, show a reference peakfrom a vial embedded in the coil (slices 9, 10), chest muscle (slices 12, 13), and myocardium (slices 14–16). Scan time for the spectra was about12 min, in a clinical 1.5-T scanner (Ref. 33, Reproduced by permission of the Radiological Society of North America from Bottomley et al .)
various advantages and disadvantages of each approach for theparticular application at hand.
For example, a disadvantage of 3-D CSI is that it requires alarge number of phase-encoding steps at least equal to the 3-Darray size, in order to encode the entire sample volume. Thissets a minimum scan time, which may not be compatible withcertain clinical study protocols that require a limited duration,such as stress testing for myocardial ischemia,30 or repeatacquisitions with different variables, as is required for CK fluxmeasurements in the heart.9 In both these examples,9,30 1-DCSI was used for this very reason. An example of a 31P 1-DCSI data set and a corresponding annotated cardiac image isshown in Figure 3.33
On the other hand, use of single-voxel methods such asDRESS or ISIS requires accurate selection of a suspectedregion of abnormality a priori: incorrect voxel selection fora stress test,30 for example, could result in a missed findingfor reversible ischemia. A more subtle problem for all methodsemploying slice-selective excitation is that, because each MRSpeak is at a slightly different MRS frequency, the signalcomes from a slightly different location in space. This problemworsens as the chemical shift dispersion increases, as in thecase of 13C MRS, and as gradient strength or voxel sizedecrease.19
Except for RFZ, whose voxels follow the RF field profile,all of the approaches yield rectangular voxels that are arguablypoorly suited to the shape of the heart unless they canbe set much smaller than the myocardial wall. With the3-D (or 2-D) CSI approaches, this can be overcome bya postprocessing technique called spectral localization withoptimized point-spread function (SLOOP ).34 Basically, theheart is segmented on corresponding 1H images, and the CSIdata set is recombined using a special algorithm to createa single voxel or several predefined voxels, whose shapecorresponds to the segmented myocardium.
The shape of the rectangular voxels of the conventional CSIexperiment, as governed by the point-spread function, can alsobe improved by “acquisition weighting” (AW), which involvesaltering the distribution of the phase-encoding steps.35 Becausemore signals are acquired near the center of the spatial “k-space” where the gradients are less intense, a small gain in31P SNR is also realized in addition to an improved voxelprofile.
Single-voxel approaches, including SLOOP, are bettersuited to the study of global metabolism, such as that ofthe normal heart, and in cardiomyopathies or heart failure.On the other hand, multivoxel approaches can accommodateuncertainties in localization and regional metabolic changes

NMR SPECTROSCOPY OF THE HUMAN HEART 5
such as ischemia and MI. Note that, although the encoding maytake longer for CSI approaches, there is no penalty in SNR perunit time: basically, one obtains spectra from multiple voxelswith the same SNR that results from averaging acquisitionsfrom single voxels of the same size in the same time.
2.2 Spatial Localization: 1H MRS
Avoiding the use of spin echoes and consequent signal lossdue to J-coupling and spin–spin (T2) relaxation, has beena driving force for the localization strategies developed for31P and 13C MRS. While all of the localization techniquesused for MRS of those nuclei are also applicable to 1HMRS, 1H moieties are generally also blessed with longerT2s, rendering them more amenable to the use of spin-echolocalization sequences. Thus, 1H MRS studies of myocardialCR in patients to date have all been performed with thesingle-voxel stimulated-echo method (STEAM),13 or with thepoint-resolved surface coil spectroscopy method (PRESS),14
both with water suppression (see Water Suppression in ProtonMRS of Humans and Animals; Single Voxel LocalizedProton NMR Spectroscopy of Human Brain In Vivo; SpatialLocalization Techniques for Human MRS). The PRESSmethod uses a 90◦ –180◦ –180◦ pulse spin-echo experimentwith slice selection on each of the three pulses, to localize thesignal from the second echo to the single voxel that lies atthe intersection of the three slices.36 STEAM does the samething for the second echo of a 90◦ –90◦ –90◦ sequence.37 Theselocalization sequences are depicted in Figure 4. Because theFOV for 1H MRS is often large and the MRS spatial resolutionsmall, PRESS (and STEAM) are often used in conjunctionwith 2-D or 3-D CSI to reduce the number of phase encodes,and hence the minimum scan time, to a manageable size. ThisPRESS–CSI hybrid was first reported for human cardiac 1HMRS in 1994.16
2.3 Coils and Position
A typical experimental cardiac 31P surface coil probefor 1.5 T is pictured in Figure 5.38 When the sample isthe dominant source of noise detected by the surface coil,its diameter should be chosen roughly equal to the depthof the tissue of interest39 (see also Surface and OtherLocal Coils for In Vivo Studies). This leads to heart 31Pdetectors with typical diameters of 6–12 cm for the anteriorto midwall. Preferably, the signal is excited with a separate,larger RF coil to minimize spatial variations in flip anglethat arise from B1 inhomogeneity, in order to facilitatemetabolite quantification.38 In addition, the availability of aconventional 1H MRI capability with its associated 1H coils,is a standard requirement to ensure the correct positioning ofthe 31P detection coil, and voxel selection. This is critical formaximizing SNR at the heart, given the surface coil’s limitedrange of sensitivity, and minimizing potential contaminationfrom adjacent tissues, especially chest muscle, with thetypically large size of 31P MRS voxels (Table 1).
With the sensitivity of metabolite MRS in the human heartalso limited, any method of improving SNR is welcome. SNR
TE
TE
MRSsignal
MRSsignal
Gy
Gy
RF
Gx
Gz
4t13t1t1
RF
π/2
a° π π
π/2 π/2
Gx
Gz
Acquire
Acquire
t
t
t
t
t1
y
zx
t1TM
(a)
(b)
(c)
Figure 4 Spatial localization to a single voxel in the heart using thePRESS36 and STEAM methods.37 (a) In PRESS, a sequence composedof an α deg RF pulse followed by two π RF pulses at times t1 and 3t1later generate a spin-echo signal centered at time 4t1. The RF pulsesare slice selective, applied in the presence of Gx, Gy , and Gz imaginggradients, which are left on after the pulses to crush the directly excitedsignals. The echo signal at TE = 4t1 derives from the voxel at theintersection of the three slices (b). STEAM (c) is similar except thatthe selective pulses are all π/2 pulses. As a result, no T2 decay occursduring the period TM , and the effective echo time is shortened to 2t1,although this occurs at a cost of half the magnetization compared toPRESS

6 NMR SPECTROSCOPY OF THE HUMAN HEART
(a) (b)
Figure 5 The cardiac 31P MRS surface coil probe used to acquire the localized 31P spectra in Figure 3.38 (a) The padded coil set on whichthe patient lies, is positioned on the patient table in the center of the whole-body NMR magnet. This coil set consists of a square base with a0.40 m × 0.40 m 31P transmit coil, a smaller probe containing (b) a 0.065-m mean diameter spiral 31P detector coil and a 0.08 m × 0.13 m figure-of-eight 1H receiver coil, used for imaging and shimming. The black strips are of velcro, which permit the smaller probe to be positioned at will.Passive diode circuitry minimizes coil interactions38
gains of up to about 30%, as compared with the best-positionedsurface coil, can be realized with a phased-array of same-sized surface detection coils.40,41 Their use also relaxes theneed for careful coil positioning relative to the heart. Phased-array technology has long been used in MRI42 and now formsthe basis of parallel imaging wherein scan time is cut byreducing the number of phase-encoding steps. However, theimplementation of phased arrays for cardiac MRS has thus faronly been implemented in normal volunteers.40,41
2.4 Motion
Other factors that can improve sensitivity are the use ofa prone as opposed to a supine patient orientation, to bringthe heart closer to the detection coil(s) and to reduce chestmotion,38 and the synchronization of MRS acquisitions tothe cardiac and/or respiratory cycle, which also limits thedeleterious effects of motion.43 Cardiac motion affects spin-echo methods much more severely than nonecho methods,because the long time between initial excitation and echoformation provides ample time for phase cancellations toaccumulate, as nuclei move through different B0 fields.1H MRS studies of myocardial CR employing STEAMand PRESS are particularly prone to SNR loss from thismechanism. Its effects can be countered in part, by dualcardiac/respiratory double-triggering strategies,43 and/or by“constructive averaging”, wherein each individual acquisitionof a data set to be averaged is saved and phase-corrected, priorto averaging.44
2.5 Enhancing Polarization
For cardiac MRS of non-1H nuclei such as 13C and31P, proton nOe and 1H-decoupling can provide anotherpotentially valuable source of SNR19,45,46 (see also ProtonDecoupling During In Vivo Whole Body Phosphorus MRS;Proton Decoupling in Whole Body Carbon-13 MRS). This
technique requires (i) the addition of an RF channel that canprovide an essentially continuous 1H irradiation; (ii) associated1H excitation coils; and (iii) electronics to isolate the 1HnOe/decoupling power from the 31P or 13C receiver.19 At1.5 T, the combined effect of nOe and decoupling to collapsemultiplet peaks in the natural abundance 13C human heartspectrum, are improvements by factors of about two- tofivefold in SNR, depending on the particular resonance.19
This has to be viewed as worthwhile. For 31P MRS, lessernOe’s of η = 0.61 ± 0.25 SD (standard deviation) for PCr,η = 0.6 ± 0.3 for γ -ATP, and η = 0.3 ± 0.2 for β-ATP havebeen reported for the human heart, corresponding to SNR gainsof up to 1.6-fold.45 Because of the differences in η for the PCrand β-ATP metabolites, the nOe may distort the PCr/β-ATPratio by about 20%, necessitating a correction for quantitativemeasurements or comparisons.46
It is important to recognize that all corrections carry errorsthat add uncertainty to the final result. Thus, there is a trade-offbetween the SNR gain realized by applying a given techniqueto improve a spectrum, and the ultimate accuracy of theparameter being measured from the spectrum after all theappropriate corrections are applied.
As noted in the section “Other Moieties”, hyperpolarizationcould potentially reap enormous SNR gains for 13C MRS ofcardiac metabolites20,21 in future human studies. Hyperpolar-ization of a substrate of metabolic interest takes time, so thatthe substrate must be prepared separately and then deliveredto the site of interest. Once delivered, it has a limited life-time, analogous to a short-lived nuclear tracer, but withoutany radioactivity or heavy-nuclei toxicity. The lifetime in thiscase, depends on the in vivo spin-lattice relaxation time (T1)of the substrate, as delivered, and the rate at which the mag-netization is sampled by the MRS/MRI pulse sequence: youonly get one dose of hyperpolarization to use, per nucleus.
2.6 Quantifying PCr/ATP
Just obtaining a localized spectrum from the heart is oflittle use if it cannot be measured for comparison with data

NMR SPECTROSCOPY OF THE HUMAN HEART 7
from other subjects or from normal values (see also QualityControl and Quantification in Whole Body MRI and MRS;Quantitation in In Vivo MRS). The most-measured parameterin human cardiac MRS is the PCr/ATP ratio from the 31Pspectrum. Published values from healthy volunteers range from0.9 ± 0.331 to 2.5 ± 0.5.47 This “normal” range is actuallylarger than most of the reported changes in PCr/ATP amongvarious patient populations. Why does this disagreement takeplace? There are three main causes.
First, the resonances are distorted to varying extents bypartial saturation effects that result from the use of pulsesequence repetition periods, TR, that are comparable or lessthan the T1s of PCr and ATP. Differences in the T1 values ofthe two moieties produce differential distortion of PCr/ATP.48
Literature average T1s for PCr and ATP at 1.5 T,49 andindividual studies at 2 T,49 3 T,50,51 and 4 T6 are tabulatedin Table 2. With a ratio of the T1 values of PCr and ATPof about 1.9, the distortion or saturation factor, F , by whichthe PCr/ATP ratio measured in the short TR experiment mustbe multiplied to yield the true myocardial PCr/ATP ratio, willvary between 1 and ∼2, depending on TR and the NMR pulseflip angle.48 Thus, measurements that are corrected for partialsaturation can differ from those that are not, by up to a factorof up to about 2.
Correction of experimental PCr/ATP values for partialsaturation can be done by two methods. F can be calculatedusing known myocardial T1 values and a measurement orknowledge of the experimental NMR pulse flip angle (e.g.,with equation (2) of Ref. 48). Owing to time constraints,T1 values usually must either be measured on a separategroup of individuals, or published values are adopted. Settinga known, precise, flip angle is a further requisite for thestudy protocol: a constant flip angle over the FOV can beensured with a combination of a separate larger excite coil38
and adiabatic excitation.49 An alternative to using known T1s,is to measure F directly from the ratio of spectra acquiredunder partially saturated conditions to signals acquired underfully relaxed conditions. Again, owing to constraints on theexamination time, this may only be feasible by adopting theexpedient of using the unlocalized signal from the surface
Table 2 31P NMR T1 values for some PCr and ATP in normalhuman myocardium
Parameter B0 (T) T1 (s) Reference
T1(PCr) 1.5 4.2 ± 0.2a 492.0 4.2 ± 1 493.0 3.8 ± 0.7 503.0 5.8 ± 0.5 514.0 5.3 ± 1.6 6
T1(γ -ATP) 1.5 2.61 ± 0.59b 492.0 2.24 ± 0.63 493.0 2.4 ± 1.1 503.0 3.1 ± 0.6 514.0 2.7 ± 0.6 6
T1(β-ATP) 1.5 2.24 ± 0.54a 492.0 2.48 ± 0.6 49
Means ± SD, as reported or calculated from reported standarderrors (SE). γ -ATP, β-ATP = γ - and β-phosphates of ATP.aLiterature average of four studies.bThe original source is a conference abstract.
coil on the chest,38,48 acquired with a relatively uniform flipangle over the FOV. Unlocalized 31P MRS saturation factorscan be obtained in about 6 min at 1.5 T, which is feasible forpatient protocols.30,38 The use of unlocalized saturation factorsrelies on an assumption that T1(PCr)/T1(ATP) is essentiallythe same in the chest and the heart muscle that contributeto the unlocalized spectrum.48 The assumption is consistentwith the available data at B0 ∼ 1.5 T,49 but is not necessarilyvalid at other fields because metabolite T1s may be B0-dependent (Table 2). Errors resulting from differences in theratio can also be minimized by using small excitation flipangles.
A second source of scatter in myocardial PCr/ATP ratiosis contamination from superficial muscle tissue, which has a[PCr] about 250% higher than that for the heart, but essentiallythe same [ATP].52 This increases the PCr/ATP in voxels thatintersect chest skeletal muscle, or where PCr signal frommuscle “bleeds” into the cardiac voxel. The difference in [PCr]is amplified by the higher sensitivity at the chest next to thesurface coil. The amount of muscle in the chest above the heartvaries significantly among subjects.48 In particular, becausethe amount of chest muscle likely varies systematicallywith age and gender, muscle contamination may be asource of differences mistakenly attributed to physiologicalor pathological changes in myocardial PCr/ATP. At present,the only solution to this problem lies with careful coil andvoxel placement and/or methods such as AW or SLOOP (seethe section “Spatial Localization: 31P and 13C MRS”) thatimprove the point-spread function and minimize bleed.
The third, albeit lesser, source of scatter in the reportedmyocardial PCr/ATP values, is that of contaminating blood inthe ventricular chamber, which contains ATP but no PCr. Thisreduces the apparent PCr/ATP ratio in voxels that intersect theventricles.53 The PCr/ATP ratio can be corrected for blood ATPcontamination by determining the amount of blood ATP, on thebasis of a measurement of the blood 2,3-diphosphoglycerate(DPG) signal present in the heart 31P spectrum. DPG has acharacteristic doublet at 5.4 and 6.3 ppm, near Pi at about5 ppm, and that of other phosphomonoesters (PM) are at6.5–6.9 ppm. The amount of ATP added by blood is estimatedfrom:
(corrected ATP signal) = (contaminated ATP signal)
− 0.5 Ab (DPG signal) (3)
where Ab = [ATP]/[DPG] ≈ 0.305,54 – 56, and the factor-of-half accounts for the two phosphates on DPG. Blood ATPcorrections typically increase PCr/ATP values by about 13 ±6%.5,33,53,56,57 Potential problems with this correction mayarise from differences between the T1 of ATP and DPG forshort TR protocols (possibly offset by the effects of inflowingunsaturated blood), variations in the blood [ATP]/[DPG] ratiowith localization method and among patients,58 and possiblecontamination of DPG by Pi or PM, which could result inblood contamination being overestimated.
2.7 PCr and ATP Concentrations
Myocardial [PCr] and [ATP] can be determined bycombining (i) the fully relaxed fully corrected PCr and ATP

8 NMR SPECTROSCOPY OF THE HUMAN HEART
signals measured in a voxel with (ii) a measurement ofthe volume of myocardium present in the voxel and (iii)a measurement of the NMR signal from a concentrationreference as calibration. If the reference lies outside of thesubject, corrections must be made for differences in B1 andthe sensitivity of the NMR coils at the heart voxel and at thereference location.24 Alternatively, a reference located at thesame position as the heart may be observed in a separateexperiment in which differences in coil loading are taken intoaccount.59 The tissue volumes sampled in each voxel mustagain be estimated, and weighting errors may need to beconsidered when the coil sensitivity varies across the voxel.The concentration of a metabolite P can thus be written24:
[P] = SPFPvRφPR[R]
SRFRvP(4)
where S, F, v, and φ, denote the signal per voxel, thesaturation correction factor, the filling fraction of tissue orreference sample in the voxel, and the ratio of the sensitivityin the metabolite voxel to the reference voxel, respectively. [R]is the reference concentration, and subscripts R and P denotereference and metabolite, respectively. Note that the percentroot mean square (rms) error in [P] is the root of the sum ofthe squares of the percent errors in each component factor ofequation (4).52 The SLOOP method also delivers known voxelvolumes, from which concentrations can be determined aftersuitable calibration and corrections are applied.60
A quantification method, not requiring tissue volumetryor sensitivity corrections, and hence avoiding some of theaccumulating errors in equation (4), employs measurements ofthe water 1H signal as a concentration reference, acquired withthe same localization sequence and coil.52 At 1.5 T, the watersignal is sufficiently intense (Table 1) that the 31P coil doesnot require retuning, and both the 31P and 1H spectra may beacquired with essentially the same B1 profile. The method doesrequire calibration with a phosphate reference to determinethe ratio of the 31P signal per phosphate to the 1H signalper proton, as well as knowledge of the myocardial tissuewater content, which appears to be relatively constant.13,15
The tissue water signal can, in principle, be corrected forcontamination from water in ventricular blood and water inpericardial fat, via a 31P DPG measurement and a measurementof the fat resonance in the 1H spectrum, respectively.52 Thecontaminating water signal from the ventricular chamber iscalculated from the known blood [DPG], and the watercontribution from the pericardial fat is calculated from theknown water content of fat.52
2.8 Quantifying Total Creatine (CR)
The detection of the N -methyl 1H resonance of CRat 3.0 ppm (see also Human Muscle Studies by MagneticResonance Spectroscopy) provides a means of quantifyingthe total (phosphorylated plus unphosphorylated) myocardialcreatine pool.13 – 15 Unlike PCr/ATP ratios, the CR in asingle 1H acquisition cannot be reliably measured as a ratiorelative to either water, which is normally suppressed, orto fat resonances, which may vary, for example, because ofcontamination from pericardial fat. A solution is to acquiretwo 1H spectra from the same voxel under the same conditions,but with and without water suppression. The CR peak in the
water-suppressed spectrum is measured relative to the waterpeak in the unsuppressed spectrum. Because 1H sensitivityis high and because the 1H T1 values are shorter than for31P, the experiment can essentially be done fully relaxed. TheCR/water ratios measured with the same STEAM- or PRESS-localized sequences (see the section “Spatial Localization:1H MRS”) can be used for patient comparative studies.13,14
The normal CR/water ratio is about 10−3 (Table 1), so a unitfor the ratio of the metabolite-to-(unsuppressed) water signal,the “milli-hoh”(mHOH ), with HOH representing water, mightbe instituted. Such ratios can be translated into absoluteconcentration measurements using the known myocardialtissue water content, after correcting for signal losses due toT2 during the STEAM/PRESS echo delay.13,14
2.9 Quantifying CK Reaction Kinetics
The flux of PCr through the CK reaction, equation (1) inthe human heart can be measured using the saturation transferNMR experiment61,62 (see also Phosphorus-31 MagnetizationTransfer Studies In Vivo). The experiment involves acquisi-tion of 31P spectra while the γ -phosphate resonance of ATPis being saturated, for example, by application of a long RFpulse tuned to its resonant frequency at −2.6 ppm relative toPCr. When ATP is saturated, the PCr signal declines as PCris converted to ATP via the forward reaction, in the absenceof any refreshment from unsaturated phosphates produced viathe reverse reaction. The ratio of the fully relaxed PCr sig-nals measured with γ -ATP saturated (M0
′) to that measuredwithout γ -ATP saturated (M0), is directly proportional to thepseudo-first-order rate constant, k, in units of the T1 of PCrmeasured in the presence of the saturating radiation applied toγ -ATP (T1
′):k T1
′ = 1 − M0′/M0 (5)
To obtain the forward flux, {k · [PCr]}, for generatingATP via the CK reaction, a measurement of myocardial[PCr] must be added to the protocol. To compensate for theeffects of spillover irradiation from γ -ATP on PCr, M0 isactually acquired with “control” irradiation applied on thesymmetrically opposite side of PCr to γ -ATP at +2.6 ppm.
The problem for measuring k, in vivo in human heart, isthe time required for the fully relaxed acquisitions needed todetermine M0
′/M0, given the long PCr T1s of 4–5 s (Table 2).This time must be added to the time required for a localizedmeasurement of T1
′ required for equation (5), and additionalacquisitions if [PCr] is to be determined to calculate flux.Once again, the practical constraint is the subject’s toleranceof the resulting exam time, which is typically about an hourfor real patients. The only solution that has enabled humanheart studies to date, involves basing the M0
′/M0 measurementon partially saturated data, to which a saturation correctionis subsequently applied. For this, knowledge of the T1 ofPCr with control irradiation is required, in addition to T1
′for equation (4). The T1 measurements were initially doneby omitting spatial localization, except for that provided bysurface coil detection.61 A better, practical solution employsthe “dual angle method” to obtain both the T1s of PCr(measured with control and γ -ATP saturated), in just fouracquisitions: two with γ -ATP saturated, and two with control

NMR SPECTROSCOPY OF THE HUMAN HEART 9
saturation.62 The two sets of acquisitions with saturation oneach side of the PCr are each performed with 60◦ and 15◦adiabatic excitation. The two T1s are used to correct thepartially saturated signals for saturation, and thereby obtainM0
′/M0. Then, T1′ is reused in equation (5) to obtain k.62
This FAST experiment can be done in under 40 min at 1.5 Tin heart patients, leaving a little time for the concentrationmeasurement needed to compute the CK flux.9 A completespatially localized FAST data set from the normal human heartis presented in Figure 6.
3 RESULTS
3.1 Normal Values
Table 3 presents literature average values for humancardiac metabolite parameters determined by 31P and 1HMRS published through 2008.1 – 106 Source references arelisted. While it is hoped to include all publications (excludingabstracts), inevitably some will have been missed. Papers thatuse measurements from other papers where expressly stated,are excluded from the average to avoid duplication. Even so,while the total numbers of subjects being reported are noted,there will inevitably be some duplication of subjects who wereused as controls for different patient studies performed by thesame research groups, in addition to instances of duplicatepublication. Accordingly, the averages are not weighted by thenumber of subjects or the SDs listed in the source publications:the SDs in Table 3 reflect the variation in the means ofall the reports, not the SDs of the individual papers. Thisbeing said, the mean value for PCr/ATP is robust to theinclusion or exclusion of duplicated normal values in 17 ofthe studies where multiple comparisons of the normal datawere performed. The overall mean value of 1.72 ± 0.26 shouldrepresent the best current estimate for the true PCr/ATP ratio inthe normal human heart. Indeed, despite the numerous reportsthat have appeared in the interim, this value has not changedappreciably from the literature average of 1.83 ± 0.12 notedin 1994.32 Tissue ATP and PCr appear to be 100% NMRvisible.107,108
Intracellular pH can be measured from the chemical shift ofthe Pi resonance (see also pH Measurement In Vivo in WholeBody Systems), which varies from 3.7 to 5.2 ppm relative to
PCr over a pH range of 6.0 to 7.3.110 In the normal heart, Piis small, difficult to unambiguously resolve from blood DPGand PM, and is probably better expressed as an inequality.41H decoupling can reduce the linewidths of the DPG andPM signals and permit a less ambiguous determination ofany neighboring Pi, but Pi still appears undetectable in abouthalf of the normal subjects studied.5 It is indeed possible thatPi is only partially NMR visible in normal subjects.107,108
However, it is unlikely that the Pi and pH measurements thathave been reported are contaminated by Pi in blood,111 sincePi is imperceptible in 31P spectra from human blood56,58 andthe [Pi] in whole human blood is listed as about 0.08 mM.111
Thus, the normal average myocardial pH of about 7.13 beingreported for normal subjects in Table 3 comes with the caveatthat it is actually not measurable in half or more normalsubjects.
The concentration measurements for normal human myocar-dial [PCr] and [ATP] in Table 3 are supported by 9 stud-ies totaling over 100 subjects, from about four independentresearch groups, and can probably be considered robust. Onthe other hand, CR estimates, while in agreement and consis-tent with canine and human necropsy studies,13,15 are frombut two groups,13,14 and the CK measurements to date are allfrom one research group.9,12
While those who have studied PCr/ATP ratios during thecardiac cycle in normal subjects at rest have not notedsignificant changes during the cardiac cycle, several studieshave reported some variation of PCr/ATP ratios and/or [PCr]and [ATP] concentrations with age71,76,77 and gender.77 Thesefindings are summarized in Table 4, and suggest a trend ofreduced metabolite concentrations with age above 40 years,and in women vs men of similar age. Yet these results requirecautious interpretation because (i) they may be confounded bychest muscle composition, a known possible contaminant (seethe section “Quantifying PCr/ATP”) that is likely affectedby age and gender; and (ii) values for which significantdifferences are being reported do not agree with many otherstudies of individuals of comparable age, or indeed, each other.Thus, the values from younger individuals are higher than theoverall average PCr/ATP of ∼1.7 (Table 3), but these subjectsare also likely to have a higher skeletal muscle mass withhigher [PCr]. No significant variations in PCr/ATP have yetbeen reported with location in the normal heart.6,75
Table 3 Literature average metabolic parameters measured in normal human by 31P MRS
Variable Mean SD na Source References
PCr/ATPb 1.72 0.26 847 1, 2, 4–7, 12, 24, 26, 28, 30, 31, 33–35, 46–48, 5052, 53, 56, 57, 59, 60, 63–72, 74–77,79–83, 85–95, 99–101, 104–106, 109
[PCr] (µmol g−1) wet 9.97 1.46 174 9, 12, 24, 52, 59, 60, 71, 77, 88[ATP] (µmol g−1) wet 5.96 1.07 174 9, 12, 24, 52, 59, 60, 71, 77, 88pH 7.13 0.03 31 4, 5, 47, 67k (s−1) 0.38 0.09 49 9, 12, 61, 78CK flux (µmol g−1 s−1) 3.15 0.85c 31 9, 12[CR] (µmol g−1) wet 28.4 5c 32 13, 14
aNumber of measurements may include the same subjects reported in repeat publications, and data from same subjectsgrouped differently (e.g., via age and sex).bExcludes data reported as “uncorrected for saturation.”cAverage SD of the only two studies reporting so far.

10 NMR SPECTROSCOPY OF THE HUMAN HEART
15°NEX = 24
1
2
3
4
5
6
7
12
3
4
5
6
7
60°
NEX =12
g -ATP
g -ATP
Control
Control
(b)
(d) (e)
(c)
7531
(a)
Figure 6 Cardiac axial spin-echo scout MRI of a normal subject acquired at rest (a) with horizontal lines (yellow) showing the seven locationsof the four 31P 1-D CSI data sets of a FAST experiment, which are plotted as a function of depth through the chest (b–e). Vertical arrows onthe spectra identify the frequency of the saturating irradiation, which is tuned to the γ -ATP resonance (red; c and e), and to a symmetric controllocation relative to PCr in (green; b, d). With γ -ATP saturated, the PCr resonances decrease (blue lines) in direct proportion to the forward CKflux. Each of the 31P data sets in (b) and (c) were acquired in 6 min using 60◦ adiabatic excitation (number of excitations, NEX = 12, T R = 1 s):the other two (d, e) were acquired in 12 min each, with a 15◦ excitation (NEX = 24)
Myocardial phosphate metabolism has also been measuredin normal subjects during stress designed to increase cardiacoutput while lying in the scanner. Three types of stress wereintroduced in the early 1990s: (i) an isometric exercise, per-formed, for example, with a hand-grip dynamometer30; (ii)an aerobic exercise involving the lifting of weights with thelegs65; and (iii) stress induced by pharmaceutical agents suchas dobutamine.92 The increase in cardiac workload as indexedby the heart-rate blood-pressure product (HR × BP) in theseprotocols, is limited to about 30–40% with the isometrichand-grip exercise at 30% of the subject’s maximum force.A HR × BP increase of about 70% is achievable with an aer-obic leg exercise lifting 5-kg weights, while the increase canbe up to threefold with dobutamine infusion.70,72 While elic-iting a lesser increase in cardiac work, the isometric exercisedoes minimize motion problems during acquisition, as com-pared with aerobic exercise. Studies using isometric30,81,96
and aerobic61,65 exercises did not show significant changesin normal volunteers. Dobutamine stress eliciting a 200%
HR × BP increase did not produce significant changes in[PCr], [ATP], k, or CK flux.9 On the other hand signifi-cant myocardial PCr/ATP reductions of 14–21% (p < 0.001)are reported at higher stress levels of 300% HR × BPincrease,70,74 even in athletes.72
Finally, chronic exposure to hypobaric hypoxia may repre-sent another “normal” variant for human myocardial PCr/ATP.Six 20- to 30-year-old professional Sherpa trekker guidesnative to a region of altitude of ∼3400m in Nepal, exhibitedsignificant reductions in myocardial PCr/ATP to 1.0 ± 0.15vs control “lowlanders” with PCr/ATP = 1.76 ± 0.06.69 Theseresults suggested that the heart may adapt its energy sourcesand delivery over time, in response to chronic environmentalstress.69
3.2 Myocardial Infarction
Published 31P MRS studies are divided on whether restingmyocardial PCr/ATP ratios are altered in MI. These data

NMR SPECTROSCOPY OF THE HUMAN HEART 11
Table 4 Reported age and gender variations in PCr and ATP in normal subjects
n Age (years) or gender (M/F) PCr/ATP [PCr] (µmol g−1) wet [ATP] (µmol g−1) wet Reference
15 32 ± 3 1.7 ± 0.3 13.5 ± 1.9 8.2 ± 1.4 Okada71
15 60 ± 13 1.6 ± 0.4 9.7 ± 2.5a 6.4 ± 1.8 Okada71
37 30 ± 6 2.16 ± 0.36 — — Schocke76
39 53 ± 7 1.83 ± 0.37b — — Schocke76
16 <40 1.9 ± 0.5 9.7 ± 2.4 5.1 ± 1.0 Kostler77
14 >40 1.9 ± 0.4 7.7 ± 2.5a 4.1 ± 0.8c Kostler77
18 M 1.9 ± 0.4 9.2 ± 2.4 4.9 ± 1.0 Kostler77
12 F 1.9 ± 0.6 8.0 ± 2.8 4.2 ± 0.9 Kostler77
Mean ± SD, as reported or calculated from reported standard errors (SE). n = number of subjects.aProbability that difference is not significant, P < 0.01 vs younger group.bP < 0.001 vs younger group.cP < 0.05 vs younger group.
Table 5 Resting myocardial PCr/ATP in patients with myocardial infarction (MI) and/or ischemic disease (ISCH)
MI/ISCH PCr/ATP of controls PCr/ATP of patients
mean SD n mean SD n P vs controls Ref.
MI 1.6 0.4 7 1.7 0.40 4 ns 4MI + ISCH. 1.72 0.15 11 1.45 0.31 16a 0.052 30MI 1.95 0.45 19 no change in patients 57MI 1.85 0.25 11 1.24 0.3 15 <0.01 81MI 1.8 1.03 11 0.94 0.41 12 ns 59ISCH — — — 1.37 0.57 29 ns 59MI 1.61 0.18 8 1.51 0.17 29 0.17 82MI 1.72 0.31 10 1.47 0.38 5 ns 83MI — — — 1.03 0.39 8 <0.05b 84
Mean ± SD, as reported or calculated from reported standard errors (SE).n, number of subjects; P , probability that difference is not significant; ns, not statistically significant vs normal controls.aPatients with ischemia including six with MI.bMI vs uninvolved tissue.
are summarized in Table 5. It is conceivable that otherconditions such as congestive heart failure (CHF) and/orcardiomyopathy associated with post-MI remodeling may beconfounding factors in these cases (see the sections “DilatedCardiomyopathy and Heart Failure” and “Hypertrophy, ValveDisease, and Heart Failure”), while these would be expectedto play lesser roles in more acute cases.4,82 Thus, in recentanterior MI, significant elevations in Pi might be visible aweek or so after onset at a normal pH ∼7.15,4 consistentwith canine studies showing persistent Pi elevations in thefirst week post-MI after an initial acute decline in PCr andATP.112 Biochemical analyses of animal hearts also show thatessentially all ATP and PCr are depleted within the first fewhours of ischemic injury that results in cell death.113 Thus,as dead cells can contribute no high-energy phosphates, it islikely that the normal resting PCr/ATP ratios reported in recentMI derive from a mixture of tissue that appears “metabolicallynormal”, and possibly, jeopardized myocardium adjacent to orinterspersed with, the infarction. The infarction and scar tissuemay best be characterized by a relative absence of significanthigh-energy phosphate contributions to the spectrum. Note that“metabolically normal” does not necessarily mean functionallynormal. A study of 29 reperfused patients with “myocardialstunning” found no significant changes in PCr/ATP fromnormal at 4 ± 2 days post-onset, nor changes a month or
so later after the patients showed functional improvement.82
Nevertheless, a preserved PCr/ATP is at least an indicator ofviable surviving tissue, post-MI.
While PCr/ATP can be normal in the weeks followingMI, there is indeed 31P MRS evidence that [PCr] and [ATP]are reduced in the infarction itself.59,80,83 This includesthe observation of a significant negative correlation betweenATP levels and the size of perfusion deficits in the heart,as quantified by thallium 201Tl radionuclide imaging,80 andreductions in [PCr] and [ATP] in patients with fixed 201Tldefects, as compared to those with reversible defects.59
Concentration measurements made by 31P NMR must betreated cautiously, however, since the tissue volume presentin the voxel may be reduced by wall-thinning followinginfarction. This may partially offset the signal loss due toinfarction, depending on how well tissue volume is accountedfor in the concentration measurements. Nevertheless, theseresults59,80 are consistent with a model for MI wherein thebulk-tissue myocardial PCr and ATP levels are reduced inthe heart113 in proportion to the volume of infarcted tissue inthe voxel.
Reductions of about 60% in myocardial [CR] can alsobe detected with the water-referenced 1H MRS method (seethe section “PCr and ATP Concentrations”) in patients withMI (Figure 7).13 These results are consistent with animal

12 NMR SPECTROSCOPY OF THE HUMAN HEART
Anterior MI
Lateralnon-MI
CR
CR
(ppm)(a)
(b)
(c)
8.0 6.0 4.0 2.0
Water Lipids
Figure 7 (a) Cardiac-gated axial spin-echo scout MRI of a patient withanterior MI, annotated to show the locations of 8-ml STEAM voxelswith corresponding water-suppressed 1H spectra from the noninfarctedlateral LV wall (b), and from an infarcted area (c). The spectra wereacquired in about 6 min. The CR resonance is evident at 3.0 ppm, whileintense residual water at ∼ 5 ppm is shaded. (Reproduced from Ref.13. Elsevier, 1998)
studies and the concept of metabolic depletion in infarction.113
Because the resolution and sensitivity are intrinsically betterwith 1H than 31P MRS (Table 1), 1H MRS could providea useful metabolic means for distinguishing healthy frominfarcted nonviable myocardium. The practical question in thecontext of the MRI/MRS scanner in which such studies areperformed, is whether 1H MRS offers advantages in MI ascompared to state-of-the-art contrast-enhanced MRI.
3.3 Myocardial Ischemia
In patients with ischemia and coronary artery disease (CAD)involving severe stenosis of the anterior vessels, the restinganterior myocardial PCr/ATP is normal, or nearly so (Table 5).However, under the anaerobic conditions that may occur inischemic heart disease in regions of the heart supplied byconstricted arteries, limited oxygen supply during periodsof stress may cause excess PCr consumption to maintainthe supply of ATP30 that is essential for fueling muscularcontraction. Thus, stress-induced reductions in the PCr/ATPratio may occur, and/or elevations in Pi, as indexed by Pi/PCror Pi/ATP as a by-product of the reaction given by equation (2).As noted above (in the section “Normal Values”), exercise ordobutamine-induced stress in healthy subjects that are free ofsignificant coronary disease does not alter anterior myocardialPCr/ATP ratios for stresses up to about 200% of the restingHR × BP,9,30,61,65,81,96 but may cause reductions of 14–21%at higher stress levels.70,72,74
Yet in the first application of stress 31P MRS employingisometric hand-grip exercise with just a 30–40% HR × BPincrease, myocardial PCr/ATP decreased 37% in 16 patientswith severe anterior coronary stenoses, as compared to restingvalues (Figure 8).30 After exercise, metabolite ratios recoveredto near-normal, pre-exercise values. As in normal controls,nine patients with nonischemic heart disease (cardiomyopathyor valve disease) exhibited no PCr/ATP changes during thesame exercise, suggesting that the stress-induced changesin PCr/ATP are specific to ischemic disease. Five patients
2.5
2.0
PC
r/A
TP
1.5
1.0
0.5Rest(a)
(b)
Exercise Recovery
2.5
2.0
PC
r/A
TP
1.5
1.0
0.5Rest Exercise Recovery
Figure 8 Transient changes in anterior myocardial PCr/ATP in controlsubjects free of CAD (a), and in patients with CAD involving theanterior wall (b), in response to continuous isometric hand-grip exerciseat 30% of the subjects maximum force.30 Error bars show mean ± SD(Reprinted by permission of the New England Journal of Medicine Vol.323, p 1593, 1990)
with ischemia underwent repeat 31P MRS stress testing aftersuccessful revascularization therapy. Prior to therapy, stressprovoked a 33% decrease in PCr/ATP in these patients, as inthe larger group. Post-therapy, exercise stress testing producedno change, so that the metabolic abnormality resolved withsuccessful clinical outcome.30
In a second report employing isometric hand-grip exercise, asimilar 40% decrease in PCr/ATP was observed in 15 patientswith reversible anterior wall ischemia that was confirmed byexercise 201Tl radionuclide imaging.81 Twelve patients withfixed 201Tl defects indicative of MI, as well as normal controls,exhibited no exercise-induced PCr/ATP changes. This, andthe observation that dobutamine stress testing induced nosignificant reduction in myocardial PCr/ATP in patients withdilated cardiomyopathy (DCM) and CHF, except in one ofeight cases,92 further suggests that the stress-induced changesmay be specific to myocardial ischemia.
Two additional studies have utilized isometric hand-grip exercise to measure myocardial ischemia. One studied“women’s ischemic syndrome” involving chest pain but nosignificant coronary vessel disease.96 It reported that 7 of 35women with the condition had cardiac PCr/ATP ratios duringstress that were two SDs below the mean of control subjects,which was interpreted as evidence of ischemia.96 However,the overall variation of PCr/ATP changes in the patient study

NMR SPECTROSCOPY OF THE HUMAN HEART 13
group as a whole, was higher than for normal controls, withboth decreases as well as increases in PCr/ATP during stress.The other study was a double-blinded application of stress31P MRS to test the efficacy of an experimental anti-ischemictherapy involving a pharmaceutical agent that reduces thebinding affinity of oxygen to hemoglobin, thereby potentiallyincreasing oxygen availability.97 The stress produced a 31%PCr/ATP reduction during control studies, a 24% reductionwith a placebo, and a 20% decline with the anti-ischemic agentin the same subjects, but the differences were not significantand the outcome was inconclusive.97
Thus, exercise testing with 31P MRS appears to be a specificmethod for detecting ischemic changes in cardiac high-energyphosphate metabolism. While it is unfortunate that present 31PMRS studies remain essentially limited to the anterior wallbeacuse of sensitivity issues (Table 1) and the time constraintsof stress testing, it may well find a role in evaluating the effectof experimental and existing therapies.
3.4 Dilated Cardiomyopathy and Heart Failure
The first 31P MRS studies of DCM appeared in 199031 fol-lowed by two studies in 1991.53,91 One showed a highly signif-icant PCr/ATP reduction,53 while the other two did not; insteadthey reported higher phosphodiesters (PD) in DCM.31,91 Sub-sequent work in 1992 noted that the PD in DCM patients wascorrelated with blood DPG, suggesting contamination fromblood, exacerbated by the thinner ventricular wall typical ofthese subjects (see the section “Quantifying PCr/ATP”).5 Anelevated Pi/PCr was also suggested in three subjects in whomPi was detectable, although pH was normal.5 The literaturePCr/ATP ratios for DCM then and since are summarized inTable 6. The preponderance of studies suggest a reduction of∼20% in myocardial PCr/ATP in DCM. PCr/ATP ratios havegenerally correlated weakly with etiology and with functionaland dimensional indices of disease severity such as the leftventricular (LV) ejection fraction (EF) or fractional shorten-ing. Importantly, virtually all studies report the coexistence of
symptoms of CHF from which the findings for DCM cannottherefore be resolved.
Moreover, one group reported a highly significant correla-tion between increasing severity of CHF as indexed by theNew York Heart Association (NYHA) classifications I–IV,and decreasing myocardial PCr/ATP57 (Table 6). In addition,myocardial PCr/ATP recovered in patients whose NYHA clas-sification was improved by drug therapy.57 Except for NYHAclassification, PCr/ATP ratios have generally correlated weaklywith etiology and functional and dimensional indices of diseaseseverity such as the LV EF or fractional shortening. Because arelative reduction in PCr would represent a drop in the reserveof myocardial high-energy phosphate, these findings providesupport for an old hypothesis that the failing heart is energystarved.114 This is consistent with data suggesting that abnor-mal myocardial PCr/ATP may first become detectable betweenNYHA classes II and III,57 which is the point at which physicalactivity is limited by fatigue, and symptoms such as palpita-tion, dyspnea, or angina. It is also consistent with studies thatconclude that the cell’s ability to sustain adequate levels ofATP is compromised only in the more advanced stages offailure.115
Thus, a reduced energy reserve as indexed by a lowermyocardial PCr/ATP (Table 6), mirrored in separate studiesshowing decreased myocardial [Cr] and CK activity in surgicalbiopsies,116 may limit the heart’s ability to do work andlead to contractile dysfunction. Indeed, myocardial PCr/ATPhas been proposed as a possible predictor of mortality.94
This is supported by data showing that values of myocardialPCr/ATP < 1.6 (n = 20) are associated with a significantlyhigher risk of mortality in 2.5 years (mortality = 40%), ascompared to those with PCr/ATP > 1.6 (n = 19; mortality =11%).94
Three more recent in vivo studies of myocardial [PCr]and [ATP] in patients with DCM and CHF are essentiallyconsistent with this picture, and the overall measurements inTable 6. One 31P MRS study reported 50 and 25% reductionsin [PCr] and [ATP] in 10 patients with NYHA class II (n = 1)and III (n = 9) CHF.88 The second studied 17 DCM patients
Table 6 Myocardial PCr/ATP in patients with dilated cardiomyopathy (DCM) and heart failure (CHF)
PCr/ATP of normal controls PCr/ATP in DCM
CHF? Mean SD n Mean SD n p Ref.a ns 31
NYHA I III 1.51 0.08 8 1.54 0.04 13 ns 91CHF 1.8 0.21 12 1.46 0.31 20 <0.001 53NYHA II III 1.65 0.26 9 1.52 0.58 9 ns 5
a 2.09 0.44 15 1.88 0.4 6 ns 86NYHA II IV 1.95 0.45 19 1.78 0.51 19 ns 57NYHA < III ns 57NYHA ≥
≥
III <0.05 57NYHA I III 1.86 0.17 7 1.63 0.24 8 0.5 92NYHA II 2.02 0.41 14 1.54 0.48 23 <0.05 93NYHA I III 1.94 0.60 30 1.3 0.22 20 0.02 94
a 1.75 0.25 9 1.26 0.29 5 951.84 0.18 123 1.55 0.20 123 Literature averageb
a
−
−
−
−
−
0.89 0.30 14 0.70 0.29 6
1.95 0.45 19 1.94 0.43 111.95 0.45 19 1.44 0.52 8
Mean ± SD, as reported or calculated from reported standard errors (SE).n, number of subjects; P, probability that difference is not significant; NYHA, New York Heart Classification for CHF; ns, not statistically significantvs normal controls.aNot specified.bUnweighted, excludes repeat entries,57 data uncorrected for saturation31 (shaded).

14 NMR SPECTROSCOPY OF THE HUMAN HEART
with NYHA class I–IV CHF.9 Reductions in [ATP] were notsignificant but an 18% reduction in [PCr] was.9 The thirdused 1H MRS to measure total myocardial creatine, [CR],noninvasively in patients with DCM and NYHA class II andIII CHF.14 A 40% reduction in [CR] was reported.
The second study of [PCr] and [ATP] in 17 patients withDCM noted above,9 also included the first measurementsof the CK pseudo-first-order forward rate constant k, andthe forward CK flux for generating ATP. While [PCr] wasonly reduced 18%, k was reduced 35% from 0.32 ± 0.07to 0.21 ± 0.07, so that the net flux was only half that innormal subjects (1.6 ± 0.6 vs 3.2 ± 0.9 µmol g−1 s−1, P <
0.005). In the context of the role of CK as a putativespatial buffer for delivering ATP from the mitochondria tothe myofibrils (see the section “Creatine Kinase Metabolism”),and a temporal buffer during periods of varying demand evenduring the cardiac cycle, it was argued that these reductions inATP supply might be of sufficient magnitude to limit ATPsupply during periods of peak demand, and contribute todysfunction.9
3.5 Hypertrophy, Valve Disease, and Heart Failure
The first localized 31P MRS study of (HCM) in 198726
reported on two patients: one subject had normal myocardialPCr/ATP, while in the other it was reduced by 40%. Publishedmyocardial PCr/ATP values for hypertrophic disease to dateare summarized in Table 7. Common underlying causes arehypertension (HT) and valve disease. As in DCM, patientswith hypertrophy often develop symptoms or are treated forCHF. Such associated causes and conditions are confoundingfactors that may contribute to the different findings seen in theinitial study,26 as well as those evidenced in Table 7.
Overall, the published data suggest that myocardial PCr/ATPis reduced by about 20% in hypertrophy, a similar level to thatseen in DCM (Table 6). Also like DCM, two studies suggestthat the magnitude of the PCr/ATP reduction increases withthe more severe symptoms of CHF, as in NYHA class IIIfailure.89,90 However, other studies report PCr/ATP reductionsthat are not explicitly linked to CHF (Table 7). In addition,a recent study of hypertrophic patients in whom functionaland morphologic measures of the disease were comparable,found that those with CHF had the same PCr/ATP as thosewithout symptoms of CHF, with both groups exhibiting a∼30% PCr/ATP reduction.12 Two other studies associate theextent that PCr/ATP is reduced with the degree of severity ofunderlying valve disease.31,90 Taken together, these studiessuggest that the magnitude of the PCr/ATP reductions inhypertrophic disease may reflect the severity of disease inmeasures that are not limited to the presence or severity ofCHF.
Moving beyond PCr/ATP ratios, the PCr and ATP con-centrations measured by SLOOP in 10 patients with HCMand CHF with NYHA class II–III severity showed a ∼30%reduction in [PCr] from 8.8 ± 1.3 µmol g−1 in controls to6.3 ± 1.5 µmol g−1 wet weight in patients (P < 0.05), while[ATP] reductions were not significant.88 Similar 25–35%reductions in [PCr] are reported using quantitative 1-D CSI:6.1 ± 2 µmol g−1 in 10 patients with left ventricular hypertro-phy (LVH) without CHF, as compared to 9.4 ± 1.1 µmol g−1
in 10 controls (P < 0.006).12 Curiously, in the same study 10
LVH patients who had comparable etiology and morphologicmeasures of disease, and who did have CHF, actually had ahigher mean [PCr] of 7.2 ± 3.7 µmol g−1 that was not signif-icantly different from the controls.12 This suggests that CHFmay not be the central factor in the [PCr] reduction in patientswith LVH, or is at least a nonspecific indicator. As in the otherstudy,88 [ATP] changes were not significant.12 1H MRS mea-surements in seven patients with HCM have also demonstratedsignificant reductions in total myocardial [CR] (22.6 ± 8.1 inHCM vs 27.6 ± 4.1 µmol g−1 in controls; P < 0.05).14 Thereduction in [CR] in HCM was less than that seen in DCMin the same study (16.1 ± 4.5 µmol g−1 in DCM; P < 0.05vs HCM).14 However, only two of the seven HCM patientsstudied were in failure, whereas all of the DCM patients hada history of severe CHF,14 so disease severity could againbe a factor affecting the magnitude of the [CR] reduction. Acouple of studies have reported elevated Pi in hypertrophicdisease.5,86
CK reaction kinetics, k and CK flux, were also reportedin the study of comparably matched LVH patients with andwithout CHF, along with controls. In the non-CHF LVHgroup, k was actually the same as in healthy controls (k =0.36 ± 0.04 s−1 vs 0.32 ± 0.06 s−1 in controls). Because theCK flux is given by the product, {k[PCr]}, in these non-CHF LVH patients, the combined effect of a normal k butreduced [PCr] was a significant 35% reduction in CK flux(2.2 ± 0.7 vs 3.1 ± 0.8 µmol g−1s−1 in controls; P = 0.01).Unlike the non-CHF LVH group, LVH patients with CHF,exhibited a dramatic reduction in k by almost 50% (to k =0.17 ± 0.06, P < 0.001). In these subjects, with both k and[PCr] down significantly, CK flux fell by an even larger 65%from 3.1 ± 0.8 g−1 s−1 in normals to 1.1 ± 0.4 µmol g−1 s−1
(P < 0.001).These findings suggest that it is not PCr/ATP, [PCr] or [ATP]
that distinguish failing from nonfailing hypertrophic heart, buta deficit in ATP kinetics, mostly notably, k. Note that k alsoshowed the largest reductions in DCM patients who had CHF,9
suggesting that perhaps reduced k may be specific indicator ofheart failure. In any case, in LVH patients with failure, theconsequences of a nearly 70% reduction in the ATP suppliedby CK is expected to have significant consequences to energysupply if CK does play a central role as a spatial/temporalATP buffer (Figure 1). Indeed calculations suggest that theCK energy supply may be so compromised that it would beunable to meet peak energy demands during the cardiac cycleand/or periods of stress.12
3.6 Other Specific Disorders
Human cardiac 31P MRS studies have been reported ina number of other specific diseases. An infant with con-genital cardiomyopathy and massive cardiomegaly exhibitedPCr/ATP = 1.3 ± 0.1 as compared to 2.0 ± 0.1 in a controlinfant, observed by unlocalized surface coil MRS.2 Localized31P MRS studies of patients with muscular dystrophy (n = 11),cardiac beriberi (n = 2), and amyloidosis (n = 1) showed a∼40% reduction in myocardial PCr/ATP when pooled as agroup, as compared to controls (1.3 ± 0.27 vs 2.09 ± 0.44in controls P < 0.01).86 Myocardial PCr/ATP and pH is alsoreported in a study of five patients with progressive systemicsclerosis.67 In obese subjects, 1H MRS shows elevations in

NMR SPECTROSCOPY OF THE HUMAN HEART 15
Table 7 Literature myocardial PCr/ATP ratios for patients with hypertrophy (LVH, HCM), including associated valve disease and heart failure(CHF)
CHF? PCr/ATP in controls PCr/ATP in patients
NYHA class Mean SD n Mean SD n P ∗ Ref
1.55 0.2 6 0.9 0.2 1
26LVH-mild ns 31LVH-severe a ns 31VALVE CHF 1.5 0.2 13 1.1 0.32 6 <.001 85VALVE non-CHF 1.56 0.15 8 ns 85VALVE 1.76 0.22 19 1.34 0.25 3 48HT, VALVE 2.09 0.44 15 1.43 0.36 12 <0.001 86HCM 1.89 0.2 12 ns 86
1.65 0.26 9 1.32 0.29 8 <0.05 51.71 0.32 6 1.07 0.44 19 <0.01 56
VALVE NYHA III 0.001 89VALVE NYHA I−
−
−
−
−
−
II ns 89AS CHF 0.008 89AI CHF 0.15 89VALVE NYHA I III 2.02 0.41 14 1.64 0.42 22 0.01 89
2.46 0.53 11 1.98 0.37 14 <.02 471.6 0.4 15 1.6 0.6 10 ns 71
MR-severe NYHA I III 1.61 0.3 13 1.29 0.3 11 <.02 90MR-dyspnea <.003 90MR NYHA I III <.01 90MR-mild NYHA I 1.73 0.17 6 <0.01∗∗ 90MR-moderate NYHA I II 1.49 0.18 5 <0.05∗∗∗ 90HT 1.39 0.17 13 1.2 0.18 11 <0.05 74VALVE 1.65 0.21 10 0.8 0.25 10 0.0002 87HT non-CHF ns 88AS NYHA II III 1.59 0.33 10 1.3 0.2 10 ns 88HCM, AS or DCM NYHA II ns 88HCM, AS, or DCM NYHA III <0.05 88HT CHF 1.9 0.3 14 1.3 0.5 10 <0.003 12HT non-CHF 1.3 0.3 10 <0.003 12
1.75 0.28 168 1.38 0.31 188 Literature averageb
0.89 0.30 14 0.78 0.16 50.89 0.30 14 0.8 0.29 6
1.5 0.2 13
2.09 0.44 15
2.02 0.41 14 1.51 0.09 SE a
2.02 0.41 14 1.86 0.18 SE a
2.02 0.41 14 1.55 0.43 132.02 0.41 14 1.77 0.36 9
1.61 0.3 13 1.21 0.24 101.61 0.3 13 1.29 0.29 131.61 0.3 131.61 0.3 13
1.59 0.33 10 no change 10
1.59 0.33 10 1.36 0.22 81.59 0.33 10 1.21 0.3 12
1.9 0.3 14
Mean ± SD, as reported or calculated from standard errors (SE) where possible.n, number of subjects; NYHA, New York Heart Association Classification for CHF; ns, not statistically significant; VALVE, valve disease; HCM,hypertrophic cardiomyopathy; HT, hypertension; AS, aortic stenosis; AI, aortic incompetence; MR, mitral regurgitation; mod., moderate.∗Probability that difference is not significant vs controls.∗∗Probability that difference is not significant vs severe MR.∗∗∗Probability that difference is not significant vs mild MR.aNot specified.bUnweighted, excludes repeat entries or data uncorrected for saturation31 (shaded).
triglycerides in the septum that correlate with both body massindex and LV mass17 (see also Body Fat Metabolism: Obser-vation by MR Imaging and Spectroscopy).
Three 31P MRS reports have investigated patients withdiabetes mellitus (DM). The first, published in 2002, examined34 men with Type I DM using slice-selective 2-D CSI(Figure 2(e) and reported a modest decrease in myocardialPCr/ATP from 2.15 ± 0.3 to 1.9 ± 0.4 as compared to 35healthy volunteers (P < 0.05).104 These patients had no othersymptoms of cardiac disease. Both of the other studies areof Type II DM, appeared in 2003, and also found significant,albeit larger, reductions in myocardial PCr/ATP. The earlierof these reported a decrease in diastolic function and reducedPCr/ATP of 1.47 ± 0.28 vs 1.88 ± 0.34 in 12 subjects (P <
0.01).105 The third study of 21 patients found a PCr/ATP of1.5 ± 0.11, as compared to 2.3 ± 0.12 in 15 controls. Diastolicfunction was not significantly depressed, although the meantrended lower.106
These studies suggest that cardiac energy reserve as indexedby the PCrATP ratios may be altered in a number of conditions.However, high values for normal subjects reported in severalof the studies, as compared with much of the prior publishedwork (for example, as summarized in Table 3), suggestthat factors affecting quantification are not fully controlled,warranting some caution in interpretation.
3.7 Heart Transplant Patients
The idea that changes in myocardial metabolite ratios mightpredict histological rejection in human heart transplants stemsfrom animal 31P studies of non-immunosuppressed allografts,which showed metabolic changes prior to the occurrence ofhistological evidence for acute rejection in the first weekor so posttransplantation.117 – 121 In the management of hearttransplant patients, the standard criterion for assessing theexistence of significant allograft rejection of severity sufficient

16 NMR SPECTROSCOPY OF THE HUMAN HEART
to warrant augmentation of immunosuppressive therapy, ishistological evidence of myocyte necrosis in endomyocardialbiopsies acquired at regularly scheduled cardiac catheterizationprocedures. Clearly, a noninvasive method of assessingrejection would be welcomed.
The first published paper applying 31P MRS to patientswith heart transplants examined 19 subjects up to 5.5 yearspost-transplantation, and did find significantly lower restinganterior myocardial PCr/ATP ratios relative to normal controls(1.57 ± 0.5 vs 1.93 ± 0.21; P < 0.01), consistent with theanimal studies.33 However, the 31P MRS abnormalities agreedwith histological evidence for necrosis in distinguishing mildfrom moderate rejection in only about 60–70% of thoseexamined. The paper concluded that 31P MRS was not aprecise predictor of significant histological rejection in manytransplant patients.33
The finding that PCr/ATP does not correlate well withthe histological score for rejection was confirmed in asecond study of 13 patients studied serially 13–294 daysposttransplantation.99 Importantly, this study did, however,demonstrate a correlation between PCr/ATP and time aftertransplantation, with PCr/ATP values increasing from 0.95 ±0.17 before day 50, to 1.17 ± 0.17 (P < 0.01) after day 50.The latter value was the same as the value of 1.23 ± 0.17reported by these authors in healthy volunteers. This worksupports the view that high-energy phosphate metabolism maybe temporarily altered early after transplantation, independentof rejection.99 A third group also reported no correlationbetween PCr/ATP and biopsy score for rejection or betweenPCr/ATP and the future biopsy score.100 Some transplantpatients from a group of 25 had lower PCr/ATP duringisometric hand-grip exercise, although again, the overallchange in PCr/ATP—both high and low—was apparentlygreater for the patient group, as compared to controls.101
The observation that PCr/ATP ratios may not preciselypredict histological rejection likely reflects fundamental dif-ferences between histological and metabolic indices. In partic-ular, myocyte necrosis may not cause altered PCr/ATP ratiosbecause dead cells can contribute no high-energy phosphates,whereas necrosis is important for histological evaluation. This,and evidence for a correlation with time after transplantationin the acute phase,99 suggests that PCr/ATP changes, at leastin part, reflect other processes associated with the transplantprocedure, including graft harvesting and storage methods, aswell as the duration of hypoxia, and that these require anextended period for complete metabolic recovery. Even so,the recovery period is inevitably punctuated by episodes ofacute rejection.
A number of studies have also examined whether themetabolic information provided by 31P MRS might aid inthe assessment of excised donor hearts being prepared fortransplantation98,102,103 (see also Tissue Behavior Measure-ments Using Phosphorus-31 NMR). Such studies can be donewithout spatial localization other than that which results fromusing a surface coil. They show that increased PCr/ATP,PCr/Pi, and pH are associated with an uneventful (positive)outcome for the procedure.98,102,103 An MRS score equal to{PCr/Pi + pH − 7}, based on these parameters, has been pro-posed to aid in the decision to transplant grafts into selectedrecipients.103
4 CONCLUSIONS
For over two decades, the application of MRS to thehuman heart has focused on the detection of metabolism andmetabolic substrates, for which the 31P nucleus’s attachmentto the molecules responsible for fueling muscular contractionhave landed it center stage. Indeed 31P MRS remains theonly method capable of providing noninvasive measures ofendogenous ATP, PCr, and CK reaction kinetics in humanheart today. As such, it has contributed unique quantitativeinformation—inaccessible by any other technique—to thebody of knowledge on human cardiac energetics in normaland diseased states.
The quantitative metabolite concentrations, ratios, intracel-lular pH, CK’s pseudo-first-order forward reaction rate andforward flux are summarized here in Tables 2–7 and the text.More recent developments with 1H for detecting myocardialcreatine remain promising, while the potential for acquiringaccess to oxidative phosphorylation using hyperpolarized 13Cin human heart is certainly something to look forward to.20,21
A qualitative summary of the changes seen by MRS in dif-ferent patient groups is presented in Table 8. The blanksshow potential areas for future research studies, and differ-ences among the metabolic responses may offer opportunitiesfor tailoring the 1H/31P MRS protocols to identify specificdiseases or conditions.
The question is whether 31P MRS studies of patients offerclinical value. Reduced cardiac PCr/ATP measurements doprovide an indicator of disease severity in cardiomyopathies,CHF and valve disease, for example. A reduced PCr/ATPmay help identify patients in heart failure where physicalactivity or diagnosis is complicated by other conditions,including age and lung disease. PCr/ATP may also holdvalue as a prognostic indicator of mortality,94 to identifythose at most risk who might best benefit from augmentedtherapy. In patients with valve disease, the detection ofmetabolic abnormalities might find a use in surgical planningto minimize permanent injury and maximize benefit.122 Onthe other hand, measurements of metabolite concentrationsand CK reaction kinetics involve more complicated protocols,pulse sequences, and analyses, which have undoubtedlylimited the number of studies reporting them. Nevertheless,all of the techniques are demonstrably feasible in humancardiac research studies, so their application for understandingthe physiology of the normal heart and disease processes,or for evaluating the metabolic response to experimentaltherapies,97 is certainly a practical pathway to providingclinical value.
The central problem for human cardiac metabolic MRS isthe low sensitivity, mainly due to the metabolite concentra-tions. This places real limits on what can be accomplished ina tolerable exam time, necessitating compromises on voxelsize and localization technique that depend on the type ofinformation being sought. As a result, one spatial localizationtechnique does not suit all applications, and spatial resolu-tion generally must be sacrificed for studies requiring repeatapplications, for example, to measure T1, k, or to do stresstesting.
Unlike MRI where a picture alone will nearly always suffice,the poor spatial resolution of MRS means that MRS has littleto offer unless the spectra can be quantified. It is clear fromTables 2–7 that obtaining quantitative measurements from

NMR SPECTROSCOPY OF THE HUMAN HEART 17
Table 8 Summary of MRS findings in heart disease through 2008
Disorder PCr/ATP Pi [PCr] [ATP] k CK flux [CR]
MI acute — ↑ ↓ ↓MI chronic ↓ ↓ ↓ — ↓ ↓Isch. rest —Isch. exercise ↓ ↑LVH/HCM ↓ ↑ ↓ — or ↓ — ↓ ↓DCM ↓ — or ↑ ↓ — or ↓ ↓ ↓CHF + (DCM or LVH) ↓ ↓ — or ↓ ↓ ↓ ↓Valve disease ↓ ↓ —XPLANT ↓Diabetes I ↓Diabetes II ↓
Isch.; ischemia; XPLANT, transplanted heart (post-operation); ↓, decrease vs normal; ↑, increase vs normal; —, unchanged vs normal; — or ↓(↑), unchanged or reduced (increased) vs normal.
spectra remains an ongoing challenge. The validation andreproducibility of measurements performed at the same site,and between different sites, is the key to progress as well asestablishing the credibility of new studies (see also QualityControl and Quantification in Whole Body MRI and MRS).Put more bluntly, if numbers are to be the central output ofthe cardiac MRS exam, then it is incumbent on investigatorsto validate their numbers and ensure reproducibility. If, forexample, the PCr/ATP decreases from a value of say, 2.2 inhealthy subjects, to perhaps 1.8 in another group as part of thesame study (Table 4), the question of why the PCr/ATP wentup in the first group as compared to the literature value of1.7–1.8 (Table 3), is arguably just as valid as the question ofwhy it is lower in the second group. Similarly, any reductionsin PCr/ATP observed at stress testing,96 must be weighed inthe context of any stress-induced increases observed in thesame group, if no other independent factors distinguishing thegroup are present.
The vast majority of cardiac MRS studies to date havebeen performed in clinical MRI/MRS systems at fields of1.5 T. Experimental systems operating at 4 T have beenaround since 1992.6,61 However, apart from the Sherpastudy,69 higher field whole-body MRI/MRS systems havethus far made relatively limited MRS contributions tothe body of cardiac MRS knowledge in humans, reflect-ing the real experimental challenges that are essential tothe production of quantitative results at any field strength.This adds a cautionary note to the hope that the SNRand spectral resolution improvements promised by the lat-est commercial clinical 3-T and experimental 7-T systemswill significantly change the landscape for human cardiacMRS.
5 LIMITATIONS
This chapter has focused on human cardiac MRS, and exceptfor the occasional relapse, reference to the vast amount ofrelevant work on animal models is omitted to keep the reviewto a reasonable size. Except for one footnote, all referencesto human studies reported in abstracts are also excluded. Thediscussion on MRS methods is limited to those that have beenapplied to human heart. It was hoped to include all of thepublished human work through 2008: apologies to those whose
work was inadvertently missed. It is, nevertheless, gratifying tonote that pooling the patient studies (Tables 5–7) strengthensthe case for the existence of metabolic abnormalities in manydisorders, while the anomalies serve as a caution for futureresearch in other cases.
6 RELATED ARTICLES
6.1 Spatial localization methods
Spatial Localization Techniques for Human MRS; ChemicalShift Imaging; Rotating Frame Methods for SpectroscopicLocalization; Single Voxel Whole Body Phosphorus MRS;Selective Excitation in MRI and MR Spectroscopy; SingleVoxel Localized Proton NMR Spectroscopy of Human BrainIn Vivo.
6.2 Surface coils
Surface Coil NMR: Detection with Inhomogeneous Radiofre-quency Field Antennas; Surface and Other Local Coils for InVivo Studies.
6.3 Other in vivo MRS methods
Water Suppression in Proton MRS of Humans and Animals;Proton Decoupling During In Vivo Whole Body PhosphorusMRS; Proton Decoupling in Whole Body Carbon-13 MRS; pHMeasurement In Vivo in Whole Body Systems; Phosphorus-31 Magnetization Transfer Studies In Vivo; Human MuscleStudies by Magnetic Resonance Spectroscopy; Body FatMetabolism: Observation by MR Imaging and Spectroscopy;Tissue Behavior Measurements Using Phosphorus-31 NMR.
6.4 MRS quantification
Quality Control and Quantification in Whole Body MRI andMRS; Quantitation in In Vivo MRS.

18 NMR SPECTROSCOPY OF THE HUMAN HEART
7 REFERENCES
1. P. A. Bottomley, Science, 1985, 229, 769.
2. J. R. Whitman, B. Chance, H. Bode, J. Maris, J. Haselgrove,R. Kelley, B. J. Clark, and A. H. Harken, J. Am. Coll. Cardiol.,1985, 5, 745.
3. P. A. Bottomley, Radiology , 1989, 170, 1.
4. P. A. Bottomley, R. J. Herfkens, L. S. Smith, and T. M. Bashore,Radiology , 1987, 165, 703.
5. A. de Roos, J. Doornbos, P. R. Luyten, L. J. M. P. Oosterwaal,E. E. van der Wall, and J. A. den Hollander, J. Magn. Reson.Imaging , 1992, 2, 711.
6. R. S. Menon, K. Hendrich, X. Hu, and K. Ugurbil, Magn. Reson.Med., 1992, 26, 368.
7. H. P. Hetherington, D. J. E. Luney, J. T. Vaughan, J. W. Pan, S.L. Ponder, O. Tschendel, D. B. Twieg, and G. M. Pohost, Magn.Reson. Med., 1995, 33, 427.
8. T. R. Brown, B. M. Kincaid, and K. Ugurbil, Proc. Natl. Acad.Sci. USA, 1982, 79, 3523.
9. R. G. Weiss, G. Gerstenblith, and P. A. Bottomley, Proc. Natl.Acad Sci. USA, 2005, 102, 808.
10. T. Wallimann, Curr. Biol., 1994, 4, 42.
11. P. P. Dzeja and A. Terzic, J. Exp. Biol., 2003, 206, 2039.
12. C. S. Smith, P. A. Bottomley, S. P. Schulman, G. G. Gerstenblith,and R. G. Weiss, Circulation , 2006, 114, 1151.
13. P. A. Bottomley and R. G. Weiss, Lancet , 1998, 351, 714.
14. I. Nakae, K. Mitsunami, T. Omura, T. Yabe, T. Tsutamoto, S.Matsuo, M. Takahashi, S. Morikawa, T. Inubushi, Y. Nakamura,M. Kinoshita, and M. Horie, J. Am. Coll. Cardiol., 2003, 42,1587.
15. P. A. Bottomley and R. G. Weiss, Radiology , 2001, 219, 411.
16. J. A. Den Hollander, W. T. Evanochko, and G. M. Pohost, Magn.Reson. Med., 1994, 32, 175.
17. L. S. Szczepaniak, R. L. Dobbins, G. J. Metzger, G. Sartoni-D’Ambrosia, D. Arbique, W. Vongpatanasin, R. Unger, and R.G. Victor, Magn. Reson. Med., 2003, 49, 417.
18. S. Jason, J. S. Reingold, J. M. McGavock, S. Kaka, T. Tillery,R. G. Victor, and L. S. Szczepaniak, Am. J. Physiol., 2005, 289,E935.
19. P. A. Bottomley, C. J. Hardy, P. B. Roemer, and O. M. Mueller,Magn. Reson. Med., 1989, 12, 348.
20. K. Golman, R. I. Zandt, and M. Thaning, Proc. Natl. Acad. Sci.USA, 2006, 103, 11270.
21. K. Golman, J. S. Petersson, P. Magnusson, E. Johansson, P.Akeson, C.-M. Chai, G. Hansson, and S. Mansson, Magn. Reson.Med., 2008, 59, 1005.
22. J. J. H. Ackerman, T. H. Grove, G. G. Wong, G. D. Gadian, andG. K. Radda, Nature, 1980, 283, 167.
23. R. L. Nunnally and P. A. Bottomley, Science, 1981, 211, 177.
24. P. A. Bottomley, C. J. Hardy, and P. B. Roemer, Magn. Reson.Med., 1990, 14, 425.
25. P. A. Bottomley, T. H. Foster, and R. D. Darrow, J. Magn. Reson.,1984, 59, 338.
26. B. Rajagopalan, M. J. Blackledge, W. J. McKenna, N. Bolas, andG. K. Radda, Ann. NY Acad. Sci., 1987, 508, 321.
27. M. J. Blackledge, B. Rajagopalan, R. D. Oberhaensli, N. M.Bolas, P. Styles, and G. K. Radda, Proc. Natl. Acad. Sci. USA,1987, 84, 4283.
28. S. Schaefer, J. Gober, M. Valenza, G. S. Karczmar, G. B. Matson,S. A. Camacho, E. H. Botvinick, B. Massie, and M. W. Weiner,J. Am. Coll. Cardiol., 1988, 12, 1449.
29. R. J. Ordidge, A. Connelly, and J. A. B. Lohman, J. Magn.Reson., 1986, 66, 283.
30. R. G. Weiss, P. A. Bottomley, C. J. Hardy, and G. Gerstenblith,N. Engl. J. Med., 1990, 323, 1593.
31. S. Schaefer, J. R. Gober, G. G. Schwartz, D. B. Twieg, M. W.Weiner, and B. Massie, Am. J. Cardiol., 1990, 65, 1154.
32. P. A. Bottomley, Radiology , 1994, 191, 593.
33. P. A. Bottomley, R. G. Weiss, C. J. Hardy, and W. A.Baumgartner, Radiology , 1991, 181, 67.
34. R. Loffler, R. Sauter, H. Kolem, A. Haase, and M. von Kienlin,J. Magn. Reson., 1998, 134, 287.
35. R. Pohmann and M. von Kienlin, Magn. Reson. Med., 2001,45, 817.
36. P. A. Bottomley, Ann. N.Y. Acad. Sci., 1987, 508, 333.
37. J. Frahm, K. D. Merboldt, and W. Hanicke, J. Magn. Reson.,1987, 72, 502.
38. P. A. Bottomley and C. J. Hardy, Phil. Trans. Roy. Soc. Lond. A,1990, 333, 531.
39. P. A. Bottomley, C. H. Lugo-Olivieri, and R. Giaquinto, Magn.Reson. Med., 1997, 37, 591.
40. C. J. Hardy, P. A. Bottomley, K. W. Rohling, and P. B. Roemer,Magn. Reson. Med., 1992, 28, 54.
41. R. F. Lee, R. Giaquinto, C. D. Constantinides, S. Souza, R. G.Weiss, and P. A. Bottomley, Magn. Reson. Med., 2000, 43, 269.
42. P. B. Roemer, W. A. Edelstein, C. E. Hayes, S. P. Souza, and O.M. Mueller, Magn. Reson. Med., 1990, 16, 192.
43. J. Felblinger, B. Jung, J. Slotboom, C. Boesch, and R. Kreis,Magn. Reson. Med., 1999, 42, 903.
44. R. E. Gabr, S. Sathyanarayana, M. Schar, R. G. Weiss, and P. A.Bottomley, Magn. Reson. Med., 2006, 56, 754.
45. P. R. Luyten, G. Bruntink, F. M. Sloff, J. I. Vermeulen, J. I.van der Heijden, J. A. den Hollander, and A. Heerschap, NMRBiomed., 1989, 1, 177.
46. P. A. Bottomley and C. J. Hardy, Magn. Reson. Med., 1992, 24,384.
47. W. I. Jung, L. Sieverding, J. Breuer, T. Hoess, S. Widmaier, O.Schmidt, M. Bunse, F. van Erckelens, J. Apitz, O. Lutz, and G.J. Dietze, Circulation , 1998, 97, 2536.
48. P. A. Bottomley, C. J. Hardy, and R. G. Weiss, J. Magn. Reson.,1991, 95, 341.
49. P. A. Bottomley and R. Ouwerkerk, Magn. Reson. Med., 1994,32, 137.
50. D. J. Tyler, L. E. Hudsmith, K. Clarke, S. Neubauer, and M. D.Robson, NMR Biomed., 2008, 21, 793.
51. A. E. M. El-Sharkawy, M. Schar, R. Ouwerkerk, R. G. Weiss,and P. A. Bottomley, Magn. Reson. Med., 2009, 61, 785.
52. P. A. Bottomley, E. A. Atalar, and R. G. Weiss, Magn. Reson.Med., 1996, 35, 664.
53. C. J. Hardy, R. G. Weiss, P. A. Bottomley, and G. Gerstenblith,Am. Heart J., 1991, 122, 795.
54. S. Minakami, C. Suzuki, T. Saito, and H. Yoshikawa, J. Biochem.,1965, 58, 543.
55. E. Beutler, in Hematology , 3rd edn., eds W. J. Williams, E.Beutler, A. J. Erslev, and M. A. Lichtman, McGraw-Hill: NewYork, 1983, p 283.
56. H. Sakuma, K. Takeda, T. Tagami, T. Nakagawa, S. Okamoto,T. Konishi, and T. Nakano, Am. Heart J., 1993, 125, 1323.
57. S. Neubauer, T. Krahe, R. Schindler, M. Horn, H. Hillenbrand, C.Entzeroth, H. Mader, E. P. Kromer, G. A. J. Riegger, K. Lackner,and G. Ertl, Circulation , 1992, 86, 1810.
58. M. Horn, S. Neubauer, M. Bomhard, M. Kadgien, K. Schnackerz,and G. Ertl, Magn. Reson. Mater. Phy., 1993, 1, 55.
59. T. Yabe, K. Mitsunami, T. Inubushi, and M. Kinoshita, Circula-tion , 1995, 92, 15.

NMR SPECTROSCOPY OF THE HUMAN HEART 19
60. M. Meininger, W. Landschutz, M. Beer, T. Seyfarth, M. Horn,T. Pabst, A. Haase, D. Hahn, S. Neubauer, and M. von Kienlin,Magn. Reson. Med., 1999, 41, 657.
61. P. A. Bottomley and C. J. Hardy, J. Magn. Reson., 1992,99, 443.
62. P. A. Bottomley, R. Ouwerkerk, R. F. Lee, and R. G. Weiss,Magn. Reson. Med., 2002, 47, 850.
63. M. A. Conway, J. D. Bristow, M. J. Blackledge, B. Rajagopalan,and G. K. Radda, Lancet , 1988, ii, 692.
64. T. M. Grist, J. B. Kneeland, W. R. Rilling, A. Jesmanowicz, W.Froncisz, and J. S. Hyde, Radiology , 1989, 170, 357.
65. M. A. Conway, J. D. Bristow, M. J. Blackledge, B. Rajagopalan,and G. K. Radda, Br. Heart J., 1991, 65, 25.
66. H. Sakuma, S. J. Nelson, D. B. Vigneron, J. Hartiala, and C. B.Higgins, Magn. Reson. Med., 1993, 29, 688.
67. J. Doornbos, P. R. Luyten, M. Janssen, M. Wasser, and A. DeRoos, J. Magn. Reson. Imag., 1994, 4, 165.
68. J. O. Van Dobbenburgh, C. Lekkerkerk, R. de Beer, and C. J. A.Van Echteld, NMR Biomed., 1994, 7, 218.
69. P. W. Hochachka, C. M. Clark, J. E. Holden, C. Stanley, K.Ugurbil, and R. S. Menon, Proc. Natl. Acad. Sci. USA, 1996, 93,1215.
70. H. J. Lamb, H. P. Beyerbacht, R. Ouwerkerk, J. Doornbos, B. M.Pluim, E. E. van der Wall, A. van der Laarse, and A. de Roos,Circulation , 1997, 96, 2969.
71. M. Okada, K. Mitsunami, T. Inubushi, and M. Kinoshita, Magn.Reson. Med., 1998, 39, 772.
72. B. M. Pluim, H. J. Lamb, H. W. M. Kayser, F. Leujes, H.P. Beyerbacht, A. H. Zwinderman, A. van der Laarse, H. W.Vliegen, A. de Roos, and E. E. van der Wall, Circulation , 1998,97, 666.
73. M. Beer, W. Landschutz, M. Meininger, T. Seyfarth, M. Viehrig,J. Sandstede, T. Pabst, W. Kenn, M. Horn, K. Harre, M. vonKienlin, S. Neubauer, and D. Hahn, ROFO , 1999, 171, 65.
74. H. J. Lamb, H. P. Beyerbacht, A. van der Laarse, B. C. Stoel,J. Doornbos, E. E. van der Wall, and A. de Roos, Circulation ,1999, 99, 2261.
75. H. Kostler, M. Beer, W. Landschutz, S. Buchner, J. Sandstede,T. Pabst, W. Kenn, S. Neubauer, M. von Kienlin, and D. Hahn,ROFO , 2001, 173, 1093.
76. M. F. H. Schocke, B. Metzler, C. Wolf, P. Steinboeck, C.Kremser, O. Pachinger, W. Jaschke, and P. Lukas, Magn. Reson.Imag., 2003, 21, 553.
77. H. Kostler, W. Landschutz, S. Koeppe, T. Seyfarth, C. Lipke, J.Sandstede, M. Spindler, M. von Kienlin, D. Hahn, and M. Beer,Magn. Reson. Med., 2006, 56, 907.
78. R. E. Gabr, R. G. Weiss, and P. A. Bottomley, J. Magn. Reson.,2008, 191, 248.
79. D. J. Tyler, Y. Emmanuel, L. E. Cochlin, L. E. Hudsmith, C.J. Holloway, S. Neubauer, K. Clarke, and M. D. Robson, NMRBiomed., 2009 DOI: 10.1002/nbm.1350
80. K. Mitsunami, M. Okada, T. Inoue, M. Hachisuka, M. Kinoshita,and T. Inubushi, Jpn. Circ. J., 1992, 56, 614.
81. T. Yabe, K. Mitsunami, M. Okada, S. Morikawa, T. Inubushi,and M. Kinoshita, Circulation , 1994, 89, 1709.
82. R. Kalil-Filho, C. P. de Albuquerque, R. G. Weiss, A. Mocelim,G. Bellotti, G. Cerri, and F. Pileggi, J. Am. Coll. Cardiol., 1997,30, 1228.
83. M. Beer, J. Sandstede, W. Landschutz, M. Viehrig, K. Harre,M. Horn, M. Meininger, T. Pabst, W. Kenn, A. Haase, M.von Kienlin, S. Neubauer, and D. Hahn, Eur. Radiol., 2000,10, 1323.
84. M. Beer, M. Spindler, J. J. W. Sandstede, H. Remmert, S. Beer,H. Kostler, and D. Hahn, J. Magn. Reson. Imag., 2004, 20, 798.
85. M. A. Conway, J. Allis, R. Ouwerkerk, T. Niioka, B.Rajagopalan, and G. K. Radda, Lancet , 1991, 338, 973.
86. Y. Masuda, Y. Tateno, H. Ikehira, T. Hashimoto, F. Shishido, M.Sekiya, Y. Imazeki, H. Imai, S. Watanabe, and Y. Inagaki, Jpn.Circ. J., 1992, 56, 620.
87. M. Beer, M. Viehrig, T. Seyfarth, J. Sandstede, C. Lipke, T. Pabst,W. Kenn, K. Harre, M. Horn, W. Landschutz, M. von Kienlin,S. Neubauer, and D. Hahn, Radiologie, 2000, 40, 162.
88. M. Beer, T. Seyfarth, J. Sandstede, W. Landschutz, C. Lipke, H.Kostler, M. von Kienlin, K. Harre, D. Hahn, and S. Neubauer, J.Am. Coll. Cardiol., 2002, 40, 1267.
89. S. Neubauer, M. Horn, T. Pabst, K. Harre, H. Stromer, G. Bertsch,J. Sandstede, G. Ertl, D. Hahn, and K. Kochsiek, J. Invest. Med.,1997, 45, 453.
90. M. A. Conway, P. A. Bottomley, R. Ouwerkerk, G. K. Radda,and B. Rajagopalan, Circulation , 1998, 97, 1716.
91. W. Auffermann, W. M. Chew, C. L. Wolfe, N. J. Tavares, W.W. Parmley, R. C. Semelka, T. Donnelly, K. Chatterjee, and C.B. Higgins, Radiology , 1991, 179, 253.
92. S. Schaefer, G. G. Schwartz, S. K. Steinman, D. J. Meyerhoff,B. M. Massie, and W. M. Weiner, Magn. Reson. Med., 1992, 25,260.
93. S. Neubauer, M. Horn, T. Pabst, M. Godde, D. Lubke, B. Jilling,D. Hahn, and G. Ertl, Eur. Hrt. J., 1995, 16, 115.
94. S. Neubauer, M. Horn, M. Cramer, K. Harre, J. B. Newell, W.Peters, T. Pabst, G. Ertl, D. Hahn, J. S. Ingwall, and K. Kochsiek,Circulation , 1997, 96, 2190.
95. M. von Kienlin, M. Beer, A. Greiser, D. Hahn, K. Harre, H.Kostler, W. Landschutz, T. Pabst, J. Sandstede, and S. Neubauer,J. Magn. Reson. Imag., 2001, 13, 521.
96. S. D. Buchthal, J. A. Den Hollander, C. N. B. Merz, W. J. Rogers,C. J. Pepine, N. Reichek, B. L. Sharaf, S. Reis, S. F. Kelsey, andG. M. Pohost, N. Engl. J. Med., 2000, 342, 829.
97. S. S. Najjar, P. A. Bottomley, S. P. Schulman, M. M. Waldron,R. P. Steffen, G. Gerstenblith, and R. G. Weiss, J. Cardiovasc.Magn. Reson., 2005, 7, 1.
98. J. O. Van Dobbenburgh, J. R. Lahpor, S. R. Woolley, N. deJonge, C. Klopping, and C. J. Van Echteld, Circulation , 1996,94, 2831.
99. J. O. Van Dobbenburgh, M. C. H. De Groot, N. De Jonge, C.Klopping, J. R. Lahpor, S. R. Woolley, E. O. R. de Medina, andC. J. A. Van Echteld, NMR Biomed., 1999, 12, 515.
100. S. D. Buchthal, T. O. Noureuil, J. A. den Hollander, R. C. Bourge,J. K. Kirklin, C. R. Katholi, J. B. Caulfield, G. M. Pohost, andW. T. Evanochko, J. Cardiovasc. Magn. Reson., 2000, 2, 51.
101. W. T. Evanochko, S. D. Buchthal, J. A. den Hollander, C. R.Katholi, R. C. Bourge, R. L. Benza, J. K. Kirklin, and G. M.Pohost, J. Hrt. Lung Transplant., 2002, 21, 522.
102. F. Kober, T. Caus, A. Riberi, S. Confort-Gouny, Y. LeFur, M.Izquierdo, J. P. Ranjeva, P. Viout, T. Mesana, D. Metras, P. J.Cozzone, and M. Bernard, Transplantation , 2002, 74, 1752.
103. T. Caus, F. Kober, A. Mouly-Bandini, A. Riberi, D. R. Metras,P. J. Cozzone, and M. Bernard, Eur. J. Card. Surg., 2005,28, 576.
104. B. Metzler, M. F. H. Schocke, P. Steinboeck, C. Wolf, W.Judmaier, M. Lechleitner, P. Lukas, and O. Pachinger, J.Cardiovasc. Magn. Reson., 2002, 4, 493.
105. M. Diamant, H. J. Lamb, Y. Groeneveld, E. L. Endert, J. W. A.Smit, J. J. Bax, J. A. Romijn, A. de Roos, and J. K. Radder, J.Am. Coll. Cardiol., 2003, 42, 328.

20 NMR SPECTROSCOPY OF THE HUMAN HEART
106. M. Scheuermann-Freestone, P. L. Madsen, D. Manners, A. M.Blamire, R. E. Buckingham, P. Styles, G. K. Radda, S. Neubauer,and K. Clarke, Circulation , 2003, 107, 3040.
107. S. M. Humphrey and P. B. Garlick, Am. J. Physiol., 1991,260, H6.
108. P. B. Garlick and R. M. Townsend, Am. J. Physiol., 1992, 263,H497.
109. H. J. Lamb, J. Doornbos, J. A. den Hollander, P. R. Luyten, H. P.Beyerbacht, E. E. van der Wall, and A. de Roos, NMR Biomed.,1996, 9, 217.
110. D. G. Gadian, Nuclear Magnetic Resonance and its Applicationsto Living Systems , Oxford University Press: Oxford, 1982, p 30.
111. K. M. Brindle, B. Rajagopalan, N. M. Bolas, and G. K. Radda,J. Magn. Reson., 1987, 74, 356.
112. P. A. Bottomley, L. S. Smith, S. Brazzamano, L. W. Hedlund,R. W. Redington, and R. J. Herfkens, Magn. Reson. Med., 1987,5, 129.
113. R. B. Jennings and K. A. Reimer, Am. J. Pathol., 1981,102, 241.
114. S. Neubauer, N. Engl. J. Med., 2007, 356, 1140.
115. S. M. Krause, Heart Fail., 1988, 267.
116. J. S. Ingwall, Circulation , 1993, 87 (Suppl VII), VII-58.
117. R. C. Canby, W. T. Evanochko, L. V. Barrett, J. K. Kirklin, D. C.McGiffen, T. T. Sakai, M. E. Brown, R. E. Foster, R. C. Reeves,and G. M. Pohost, J. Am. Coll. Cardiol., 1987, 9, 1067.
118. C. E. Haug, J. L. Shapiro, L. Chan, and R. Weil, Transplantation ,1987, 44, 175.
119. C. D. Fraser, V. P. Chacko, W. E. Jacobus, R. L. Soulen, G. M.Hutchins, B. A. Reitz, and W. A. Baumgartner, Transplantation ,1988, 46, 346.
120. C. D. Fraser, V. P. Chacko, W. E. Jacobus, P. Mueller, R. L.Soulen, G. M. Hutchins, B. A. Reitz, and W. A. Baumgartner, J.Heart Transplant., 1990, 9, 197.
121. C. D. Fraser, V. P. Chacko, W. E. Jacobus, G. M. Hutchins, J.Glickson, B. A. Reitz, and W. A. Baumgartner, Transplantation ,1989, 48, 1068.
122. Editorial, Lancet , 1991, 338, 981.
Acknowledgments
I thank RG Weiss for many years of fruitful collaboration and helpfuldiscussions. This work is supported in part by National Institutes ofHealth grant R01 HL5688.
Biographical Sketches
Paul A. Bottomley. BSc (Hon.), 1975, PhD in Physics, 1978, Univer-sity of Nottingham, UK. Research Associate, Johns Hopkins University,Baltimore, 1978–1980. Physicist, GE Research and Development Cen-ter, 1980–1994. Currently Russell H Morgan Professor and Director ofthe Division of MR Research, of the Russell H Morgan Department ofRadiology and Radiological Sciences, Johns Hopkins University. Recip-ient, gold medal of the Society of Magnetic Resonance in Medicine,1989; Coolidge Fellowship and medal, GE Company, 1990; gold, sil-ver, and bronze patent medals, GE Company; 34 patents, about 160papers, and 190 published conference reports. Research specialties: invivo NMR, MRI, tissue relaxation times, localized NMR spectroscopy,human cardiac NMR spectroscopy, interventional MRI, MRI safety.