Nilotinib Demonstrates Superior Efficacy Compared With ... · *p-values are based on log-rank test...
30
Giuseppe Saglio, Dong-Wook Kim, Surapol Issaragrisil, Philipp le Coutre, Josy Reiffers, Clarisse Lobo, Ricardo Pasquini, Richard Clark, Timothy Hughes, Andreas Hochhaus, Neil Gallagher, Albert Hoenekopp, Mei Dong, Ariful Haque, Hagop Kantarjian, and Richard Larson on behalf of the ENESTnd Investigators Nilotinib Demonstrates Superior Efficacy Compared With Imatinib in Patients With Newly Diagnosed CML-CP: Results From the International Randomized Phase III ENESTnd Trial
Transcript of Nilotinib Demonstrates Superior Efficacy Compared With ... · *p-values are based on log-rank test...

Giuseppe Saglio, Dong-Wook Kim, Surapol Issaragrisil, Philipp le Coutre, Josy Reiffers, Clarisse Lobo, Ricardo
Pasquini, Richard Clark, Timothy Hughes, Andreas Hochhaus, Neil Gallagher, Albert Hoenekopp, Mei Dong,
Ariful Haque, Hagop Kantarjian, and Richard Larson
on behalf of the ENESTnd Investigators
Nilotinib Demonstrates Superior Efficacy Compared With Imatinib in
Patients With Newly Diagnosed CML-CP: Results From the
International Randomized Phase III ENESTnd Trial

Slid
e-
ResultsOverall survival (intent-to-treat):imatinib Arm
100
60
20
Alive, %
40
80
10
0 1080
90
50
30
70
96726048362412
Months since randomization
84
Overall survival
Survival: deaths associated with CML
Estimated overall survival
at 8 years was 85%(93%, considering only
CML-related deaths)
These results are not only due to imatinib!

% S
urv
ival
(all d
eath
s)
0
10
20
30
40
50
60
70
80
90
100
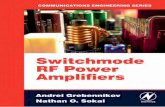
Months after stopping imatinib study therapy
0 12 24 36 48 60 72 84 96
Safety (n=30)
Efficacy (n=82)
Bone marrow transplant (n=16)
Other reason (n=80)
Survival 85% at 5 years after
discontinuing study
Survival approximately 50%
at 5 years after stopping
imatinib study drug
IRIS 7 year update
Survival of Patients Who
Discontinued Imatinib Study Therapy

Nilotinib
Held in place by lipophilic
interactions in place of hydrogen-
bonds, making it less susceptible to
point mutations
Specifically designed to
bind more efficiently to
the ATP binding site
Imatinib
ATP binding
site
Hydrogen bonds form with
specific amino acids lining
the binding site
• Differences in drug binding account for nilotinib’s activity in BCR-ABL mutations that are resistant to imatinib
Nilotinib designed for a better fit to inactivate
conformation of the ABL kinase domain
O'Hare T, Walters DK, Deininger MW, Druker BJ. AMN107: tightening the grip of imatinib. Cancer Cell. 2005;7:117.

Nilotinib:Increased potency and selectivity for Abl
Nilotinib
(Cell prolif. IC50)
Abl
(25 nM)
> PDGFR
(53 nM)
> KIT
(158 nM)
Imatinib
(cell prolif IC50)
PDGFR
(39 nM)
> KIT
(98 nM)
> Abl
(669 nM)
Nilotinib has no significant effect on other kinases evaluated
(including Src, FLT3, VEGFR, EGFR, InsR, RET, MET , IGFR, etc)
at concentration <3000 nM.
Mestan. Blood 2004;104(546a): Abstract 1978
Weisberg. Cancer Cell 2005;7(129)

0
500
1,000
1,500
IC50
Ce
ll P
rolife
rati
on
(n
M)
Nilotinib sensitive:
Range 19–791 nM
Nilotinib resistant:
>10,000 nM
Trough levels at 400 mg nilotinib BID (1,700 nM)
exceed IC50 for 32/33 mutations.
Hochhaus et al. Blood 2006;108(11):Abstract 749 Oral presentation
Nilotinib Against Imatinib-resistant
Bcr-Abl Mutants
T315I

Figure 1. Hematologic and Cytogenetic Response in
Patients With a Minimum Follow-Up of 24 Months (N = 321)
• Median time to CHR was 1.0 month in patients without CHR at baseline
• Median time to MCyR was 2.8 months
• MCyR was achieved in 59% of patients, 74% of which were CCyR
n 321 155 55 321 226 95 321 226 95
* Patients who achieved (without baseline CHR) or maintained CHR (had CHR at study entry).
† Patients with no CHR at baseline.
‡ See definition of imatinib-intolerant with resistance in the Methods sections.
MCyR CCyRCHR
41%44%
56%59%
85%72%
66%
51%
0
10
20
30
40
50
60
70
80
90
100
% P
ati
en
ts
Overall* OverallImatinib
Resistant
Imatinib
Intolerant w/
Resistance ‡Overall
Imatinib
Resistant
Imatinib
Intolerant w/
Resistance ‡
CCyR, complete cytogenetic response; CHR, complete hematologic response; MCyR, major cytogenetic response.
RESULTS
Imatinib
Resistant †Imatinib
Intolerant w/
Resistance † ‡
90%
Kantarjian HM et al., ASH 2009

RESULTS
CCyR, complete cytogenetic response.
Figure 4. Duration of CCyR
Kantarjian HM et al., ASH 2009


2 Phase II clinical trials performed at MDAnderson and in Italy
testing nilotinib 400 mg BID as front line treatment of newly
diagnosed CML patients
showed very good results
Rosti G, et al. Blood. 2009 ; 114:4933.
Molecular responses (GIMEMA)

11
ENESTnd StudyStudy Design and Endpoints
• Primary endpoint: MMR at 12 months
• Secondary endpoint: CCyR by 12 months
• Other endpoints: time to and duration of MMR and
CCyR, EFS, PFS, time to AP/BC, OS
*Stratification by Sokal risk score
Imatinib 400 mg QD (n=283)
Nilotinib 300 mg BID (n=282)RANDOMIZED*
Nilotinib 400 mg BID (n=281)
• N = 846
• 217 centers
• 35 countries
Follow-up 5 years

1212
Definition of Endpoints
• MMR: BCR-ABL ≤ 0.1%IS
– Unavailable sample considered as lack of response
– Atypical transcripts at baseline considered as lack of response
• CCyR: No Ph+ metaphases out of 20
– Insufficient metaphases considered as lack of response
– Unavailable sample considered as lack of response
– FISH not allowed

13
Baseline Patient CharacteristicsNilotinib
300 mg BIDN = 282
Nilotinib400 mg BID
N = 281
Imatinib400 mg QD
N = 283
Age, median (range) 47 (18–85) 47 (18–81) 46 (18–80)
Time since Dx,
median (days)
31 31 28
Sokal risk, %
Low
Intermediate
High
37
36
28
37
36
28
37
36
28
Prior Rx, %
Hydroxyurea
Anagrelide
Imatinib (< 2 wks)
77
2
13
75
0
9
71
1
11

14
Patient DispositionNilotinib
300 mg BID
N = 282
Nilotinib400 mg BID
N = 281
Imatinib400 mg QD
N = 283
Still on treatment, % 84 82 79
Discontinued, % 16 18 21
Disease progression <1 <1 4
Treatment failure <1 2 4
Suboptimal response 3 0 2
Adverse events 5 9 7
Abnormal lab. values 2 2 1
Death <1 0 0
Protocol violation 1 2 1
Other reason 3 3 2

15
Suboptimal Response/Treatment Failure
5
1
5
2
13
8
0
5
10
15
20
25
Suboptimal response Treatment failure
Pe
rce
nta
ge
Nilotinib 300 mg BID
Nilotinib 400 mg BID
Imatinib 400 mg QD
% o
f p
ati
en
ts

16
K-M Estimate of EFS
Imatinib 400 mg QD
Nilotinib 300 mg BID
Nilotinib 400 mg BID
283
282
281
93
47
51
190
235
230
Pat Evt Cen
Censored observations
p < 0.0001p < 0.0001

17
MMR Rates Over Time (ITT)
9
33
43 44
5
30
3843
1
12
1822
0
10
20
30
40
50
60
Month 3 Month 6 Month 9 Month 12
Pe
rce
nta
ge
Nilotinib 300 mg BID Nilotinib 400 mg BID Imatinib 400 mg QD
% M
MR
p<0.0001
p<0.0001

18
Deeper Molecular Responses at Any Time (ITT)(4- and 4.5-log* Reduction)
24
13
21
1210
4
0
5
10
15
20
25
4-log reduction (< 0.01%) 4.5-log* reduction (< 0.0032%)
Pe
rce
nta
ge
Nilotinib 300 mg BID
Nilotinib 400 mg BID
Imatinib 400 mg QD
% r
esp
on
der
BCR-ABL Transcript Level Reduction
- -
*Most sensitive measure of leukemic burden available

19
CCyR Rates (ITT)
67
80
63
78
45
65
0
20
40
60
80
100
Month 6 Month 12
Nilotinib 300 mg BID Nilotinib 400 mg BID Imatinib 400 mg QD
p<0.0001
p=0.0005
% C
CyR

20
CCyR Rates by 12 Months by Sokal Score
8678
74
8780
63
77
65
49
0
10
20
30
40
50
60
70
80
90
100
Low Intermediate High
Pe
rce
nta
ge
Nilotinib 300 mg BID Nilotinib 400 mg BID Imatinib 400 mg QD
% C
CyR

21
Overall Progression to AP/BC (ITT)
21
11
0
5
10
15Nilotinib 300 mg BID
Nilotinib 400 mg BID
Imatinib 400 mg QD
nu
mb
er
of
pa
tie
nts
• No patients who achieved MMR progressed to AP/BC
• 3 patients who achieved CCyR on imatinib progressed to AP/BC
p=0.0095* p=0.0037*
*p-values are based on log-rank test stratified by Sokal risk group vs imatinib for time to AP/BC
0.7% 0.4%
3.9%

22
Grade 3/4 Myelosuppression
3
1210
3
1012
5
20
9
0
10
20
30
Anemia Neutropenia Thrombocytopenia
Nilotinib 300 mg BID Nilotinib 400 mg BID Imatinib 400 mg QD
% o
f p
ati
en
ts

2323
Study Drug-Related Adverse Events (≥ 10% in Any Group)
% of patients treated
Nilotinib300 mg BID
N = 279
Nilotinib400 mg BID
N = 277
Imatinib400 mg QD
N = 280
All Grades
Grade 3/4
All Grades
Grade 3/4
AllGrades
Grade 3/4
Nausea 12 <1 20 1 31 0
Muscle spasms 7 0 6 <1 24 <1
Diarrhea 8 <1 7 0 21 1
Vomiting 5 0 9 1 14 0
Rash 31 <1 36 3 11 1
Myalgia 10 <1 10 0 10 0
Headache 14 1 21 1 8 0
Fatigue 11 0 9 <1 8 <1
Pruritus 15 <1 13 <1 5 0
Alopecia 8 0 13 0 4 0

24
Study Drug-Related Fluid Retention (All Grades)
% of patients treatedNilotinib
300 mg BID
N = 279
Nilotinib400 mg BID
N = 277
Imatinib400 mg QD
N = 280
Peripheral edema 5 5 14
Eyelid edema <1 2 13
Periorbital edema <1 <1 12
Facial edema <1 2 8
Weight Gain 3 <1 6
Pericardial effusion <1 0 <1
Pleural effusion <1 0 0
•Grade 3/4 AEs were rarely observed in any treatment arm (<1%)

25
Laboratory Abnormalities (Grade 3/4)
% of pts treated Nilotinib300 mg BID
N = 279
Nilotinib 400 mg BID
N = 277
Imatinib400 mg QD
N = 280
Lipase ↑ 6 6 3
Amylase ↑ <1 1 1
ALT ↑ 4 9 3
AST ↑ 1 3 1
Total bilirubin ↑ 4 8 <1
Glucose ↑ 6 4 0
Albumin ↓ 0 0 0
Cholesterol ↑ 0 <1 0
Phosphorous ↓ 5 5 8
Alkaline phos. ↑ 0 0 <1
Cholesterol ↑ 0 <1 0
Creatinine ↑ 0 0 <1
Calcium ↓ <1 <1 0
• One patient in the imatinib arm and one in the nilotinib 400 mg BID arm
discontinued the study due to acute pancreatitis

2626
QTcF Prolongation
% of patients treatedNilotinib
300 mg BIDN = 279
Nilotinib400 mg BID
N = 277
Imatinib400 mg QD
N = 280
Absolute QTcF >480 ms 0 <1 0
Absolute QTcF >500 ms 0 0 0
QTcF increase >30 ms 26 26 18
QTcF increase >60 ms <1 <1 0
•There was no decrease from baseline in mean LVEF
anytime during treatment in any arm

27
Conclusions• Nilotinib is superior to imatinib with significantly higher
rates of MMR and CCyR, at both 300 mg BID and 400 mg BID
• Significantly fewer patients on nilotinib progressed compared with imatinib
• Nilotinib is superior to imatinib across all Sokal risk groups
• Nilotinib is generally well-tolerated
• Incidence of AEs leading to discontinuation was lowest in the nilotinib 300 mg BID arm
• Based on these results nilotinib may become the new standard of care in newly diagnosed CML

The available data with nilotinib used as first-
line therapy for CP-CML show:
1) A high percentage of responses (CCyR, MMR) (less primary resistance)
2) A lower rate of progression (less secondary resistance)
Why?

Possible explanations
• Higher potency in inhibiting BCR-ABL1 TK
• Lower dependence of intra/extracellular mechanisms of drug influx/efflux
• Higher capability in suppressing “permissive situations” for the development of resistance
– Mutations of BCR-ABL1
– Activation of alternative TK activities

30
ENESTnd Contributing InvestigatorsArgentina: B Moiraghi, M Perez; Austria: R Greil, P Valent; Belgium: L Noens, A Bosly, G Verhoef, M André,
P Martiat; Brazil: MA Zanichelli, C Souza, M Mello, V Hungria, V Colturato, A Nonino; Canada:
J Lipton, D Forrest, M Lalancette, R Delage, M-L Savoie; Colombia: G Quintero, M Gomez; Czech Republic:
H Klamova, E Faber; Denmark: H Frederiksen, H Vestergaard, C Marcher, O Weis Bjerrum, C Marcher; Egypt:
H Kamel, H Elzawam; Finland: K Porkka, K Remes; France: J-L Harousseau, A-P Guerci-Bresler, F Rigal-
Huguet, M Tulliez, D Guyotat, M Gardembas, M Escoffre, L Legros, F Guilhot, D Rea, FE Nicolini, T Facon, J-Y Cahn,
A Johnson-Ansah, A Charbonnier; Germany: N Gatterman, C Scheid, D Niederwieser, O Ottmann,
K Blumenstengel, J Duyster, T Bruemmendorf, M Kneba, F Stegelmann, P Schathausen; Hong Kong:
Y-I Kwong; Hungary: T Masszi; Italy: G Fioritoni, G Alimena, F Nobile, E Pungolino, G Rosti, M Gobbi, E Abruzzese,
M Petrini, A Bosi, AM Carella, EM Orlandi, F Ferrara, F Lauria, S Amadori, F Di Raimondo, A Levis, M Tiribelli, P Leoni,
A Rambaldi, M Martelli, B Rotoli, F Pane; Japan: M Hino, I Matsumura, M Kurokawa, Y Kanda, C Nakaseko, O Miura,
I Jinnai, Y Maeda, K Ohnishi, T Nagai, S Miyawaki, K Imai, K Ohishi, K Usuki, M Okada, Y Miyazaki, A Kimura,
K Miyamura, S Nakao, K Toba, S Okamoto, S Chiba, N Tsukamoto, N Takahashi, Y Kobayashi, K Ohyashiki,
T Kawaguchi, M Hino, M Imamura, I Jinnai, A Matsuda, I Matsumura, J Ishikawa; Malaysia: TC Ong; Mexico:
J Kassack, D Gómez Almaguer; Netherlands: GJ Ossenkoppele; Norway: T Gedde-Dahl, H Hjorth-Hansen;
Poland: K Kuliczkowski, S Kyrcz-Krzemieñ, W Jedrzejczak, A Dmoszynska, J Starzak-Gwozdz; Russia: A Turkina,
T Pospelova, A Zaritsky; Singapore: LP Koh, YT Goh; Slovakia: L Demitrovicova, M Mistrik; South Africa: G Cohen,
LM Dreosti, V Louw, P Ruff, N Novitzky; South Korea: S-K Sohn, H-J Kim, C-W Jung, K-H Lee, S-Y Park;
Spain: F Cervantes, F Marin, J Hernandez Boluda, C Boque, R De paz, J Batlle, RF Rodriguez, E Conde, J Odriozola,
M Perez Encinas, C Cañizo, A Julia Font, B Heredia, P Giraldo, P Lopez, JL Steegman, MA Echeveste, M Sanz Alonso,
S del Castillo, F Martin, R Perez, P Herrera, R Rogriguez, MJ Rodriguez; Sweden: L Stenke, S Lehmann,
B Simonsson, H Wadenvik, B Markevarn, K Myhr Eriksson, M Bjoreman, J Richter, ASjälander; Switzerland:
Y Chalandon; Taiwan: M-C Wang, M Yao, L-Y Shih; Thailand: S Jootar, U Bunworasate; United Kingdom: D Marin,
Holyoake, J Byrne, G Smith; United States: I Flinn, S Goldberg, M Kalaycio, R Gingrich, J Burke, T Ervin, T Shea,
B Powell, C Alemany, K Kolibaba, G Guzley, M Guerra, L Fehrenbacher, WG Harker, J Davis, W Edenfield, E
Arrowsmith, H Koh, L Fehrenbacher, R Paquette, A Al-Janadi, L Akard, G Robbins, M Savin, D Schlossman, D
Richards, W Berry, M Woodson, C Siegrist, J Glass, M Heaney, H Wallach; Venezuela: J Lopez