NICHE Nurses Improving Care of Health System Elders The SPICES Tool NICHE Nurses Improving Care of...
44
NICHE Nurses Improving Care of Health System Elders The SPICES Tool February, 2011 Rita LaReau MSN GNP BC Geriatric Clinical Nurse Specialist Bronson Methodist Hospital [email protected]
-
Upload
shanon-holmes -
Category
Documents
-
view
221 -
download
0
Transcript of NICHE Nurses Improving Care of Health System Elders The SPICES Tool NICHE Nurses Improving Care of...

NICHENurses Improving Care of
Health System Elders
The SPICES Tool
NICHENurses Improving Care of
Health System Elders
The SPICES Tool
February, 2011February, 2011
Rita LaReau MSN GNP BCGeriatric Clinical Nurse SpecialistBronson Methodist [email protected]
Rita LaReau MSN GNP BCGeriatric Clinical Nurse SpecialistBronson Methodist [email protected]

Learning ObjectivesUpon completion of this program the
learner will be able to:
• Describe a basic assessment tool for assessment of the geriatric patient.
• State demographics related to falls in older adults.
• State interventions to prevent a fall.

Older Adult Patients
Older Adult Patients > age 65 Challenge to health care providers Numerous & complex diagnoses Shorter hospital stays Navigation through hospital process Potential for cascade of poor outcomes

Hartford Institute Nurses Improving Care for Health System
Elders (NICHE) 1992 Sponsored by John A. Hartford Foundation
Institute for Geriatric Nursing@ New York University
National nursing led initiative: Nationally Recognized Nursing Leaders
Currently over 200 NICHE sites Geriatric Resource Nurse (GRN) Model

NICHE Outcomes Enhance Nursing Knowledge and Skills
Regarding the Treatment of Common Geriatric Syndromes
Increase Patient Satisfaction Decrease Length of Stay Reduce Readmission Rates Reduce Costs Associated with Elder Care.

Evidenced Based Practice
Research based protocols that focus specifically on common geriatric care syndromes
Reflect current research and standards including those developed by The Agency For Health Care Policy Research (AHCPR)
Accessible and usable by bedside nurses

Evidenced Based Resources http://nicheprogram.org http://www.consultgerirn.org Hartford Institute Protocols Book
Evidenced Based NICHE Tools: Handout

Geriatric Syndromes Physical Restraints Pressure Ulcers Sleep Disturbances Advance Directives Pain Management Assessing Cognitive
Function Functional
Assessment
Depression Incontinence Eating/Feeding Acute Confusion/
Delirium Medication Management Falls Discharge Planning

Bronson NICHE ProgramNICHE Program Geriatric Independent Study Modules NICHE AGEducation Day (8 hours) Support for Gerontological Nurse Certification

Geriatric Resource Nurse (GRN) Program Geriatric Clinical Nurse Specialist (GCNS) Certified GRNs GCNS supports GRNs in their new roles
– Instruction– Nurse-to-Nurse Consultation– Resource Development– Geriatric Clinical Excellence
Assesses selected geriatric patients in context of geriatric syndromes
NICHE Clinical Support

GRN Rounding/Consult
Assist staff in assessing, planning, implementing, and evaluating geriatric care according to SPICES Tool
Evaluate and provide feedback to staff regarding SPICES Tool assessments and interventions
Augment staff knowledge and attitudes as they relate to geriatric care.
GRN Rounding/Consult
Disseminate information about geriatric care management through a variety of ways including– Documentation
• Progress Notes • CareGraph
Collaborate with NICHE Council and other resource people as necessary.
SPICES Tool
GRN Core Screening Tool– Raises awareness and triggers
further evaluation & documentationSkin ImpairmentPoor NutritionIncontinenceConfusionEvidence of FallsSleep Disturbances

Geriatric Assessment RoundingGRNs Use SPICES Tool for assessing patients > age 70
– Problems with• Skin
– Skin Integrity Score < 18 (Braden Tool)• Problems with Eating
– Less than 80% ideal Body Weight– % food eaten < 25% > 6 days (25% > $
days (80+ Yrs)• Incontinence
– Stress/Urge/Functional/Diarrhea/Foley

Geriatric Assessment Rounding• Cognition
– Mini-Cog, Geriatric Depression Scale (GDS)
– Positive Confusion Assessment Method (CAM), Anxiety
– Sensory Impairment
– Evidence of Dementia, Depression
• Evidence of Falls
– Confusion, Depression, Elimination, Dizziness, Gender, Antiepileptics, BZD, Mobility/Get Up and Go
• Sleep
– Difficulty falling/ staying asleep
– Sleep promotion interventions

Reasons for Geriatric Resource Nurse ConsultSome potential reasons for consult:
Delirium
Dementia
Sitter
Falls
Sleep Problems
Problems with eating
Use of Diversional Activities

Evidence of Falls/Function

What Do These People Have in Common? Laura Ashley (Fashion Designer) Robert Atkins (Doctor) George Washington Carver (Inventor) Genghis Khan (Royalty) Robert Peel (Head of State) Kurt Vonnegut (Author) William the Conqueror (Royalty) Malcolm Baldrige (Politician)

Cause of Death:Accidental Fall

Why Do We Need to Be Concerned?
Injuries Deaths Associated complications Costs

Demographics Community-dwelling persons > 65 years:
– 30% - 40% fall each year Hip fractures:
– 90% result from a fall– 20% die within one year
Leading cause of death from injury in those > 65 years old: A fall
Source: Auerhahn C, Capezuti, E., Flaherty, E., and Resnick, b., eds. Geriatric Nursing Review Syllabus; A Core Curriculum in Advanced Practice Geriatric nursing, 2nd edition. New York: American Geriatric Society; 2007.
American Academy of Orthopedic Surgeons: Don’t Let a Fall Be Your last Trip: Prevention Facts. Available at http://orthoinfo.aaos.org/brochure/thr_report.cfm?Thread_ID=21 , Accessed, May 25, 2007.

Demographics
Falls are associated with:• Decline in functional
status• Development of “fear of
falling”• Greater likelihood of
nursing home placement

Cost of a Fall
Costs associated with fall-related injuries in persons > 65 years old:• Mean hospital cost: $15,938• Lifetime costs: $12.6 billion
Source: Auerhahn C, capezuti, E., Flaherty, E., and resnick, b., eds. Geriatric Nursing Review Syllabus; A Core Curriculum in Advanced Practice Geriatric nursing, 2nd edition. New York: American Geriatric Society; 2007.
Nurse Assist – Improving senior Care<[email protected], A Weekly Q & A from Nurse Assist - The Clinical Experts in Fall Management. Available at file://C:\Documents and Settings\lareaur\localSettings\Temp\Xpgrpwise\45F5FEE3DOM

Fall - Defined Fall: A fall is an unplanned
descent to the floor ( or extension of the floor, e.g., trash can or other equipment) with or without injury to the patient.
All types of falls are to be included whether they result from physiological reasons (fainting) or environmental reasons (slippery floor).

Fall - Defined
Include assisted falls – when a staff member attempts to minimize the impact of the fall.
Included in this definition are patients found lying on the floor unable to account for their situation.
Fall Prevention: All Patients
Orient patient to environmentEducate patient/family using:
– The Fall Prevention Scripting• Use TeachBack
– Prevent Falls in the Hospital handout– Both located on the Nurses and Clinician’s page
under Fall Prevention Resource ToolsOrient to ‘Call to Stop a Fall’ signMaintain call light in reach and assess/ensure
ability to use.
Fall Prevention: All Patients (1)
Place bed in low position and lock Utilize non-slip well-fitted
footwear Leave bathroom or night light on Wipe up spills immediately Arrange furniture/objects safely Place patient items in reach

Fall Prevention: All Patients (2)
Teach transfer techniques prn Assist in meeting elimination needs Evaluate potential medication side
effects Assure ambulation as ordered Encourage use of handrails in
bathroom and hall

Fall Prevention: All Patients (3)
ROM BID by nursing staff if not out of bed
Keep assistive devices (glasses, canes walkers etc.) at bedside within reach
Evaluate patient’s ability to interpret information (Can they hear, feel and interpret? Need hearing amplifier or hearing aides?)
Utilize upper 2 of 4 side rails in raised position, to maintain freedom of movement

Hendrich II Fall Risk Model
Fall Risk Assessment Tool used at Bronson
Identifies patient risk factors that contribute to fall potential.
Hendrich, A., Bender, P., Nyhuis A., Validation of the Hendrich II Fall Risk Model: A Large Concurrent Case/Control Study of Hospitalized Patients. 2003. Applied Nursing Research (16) 1, pp 9-21
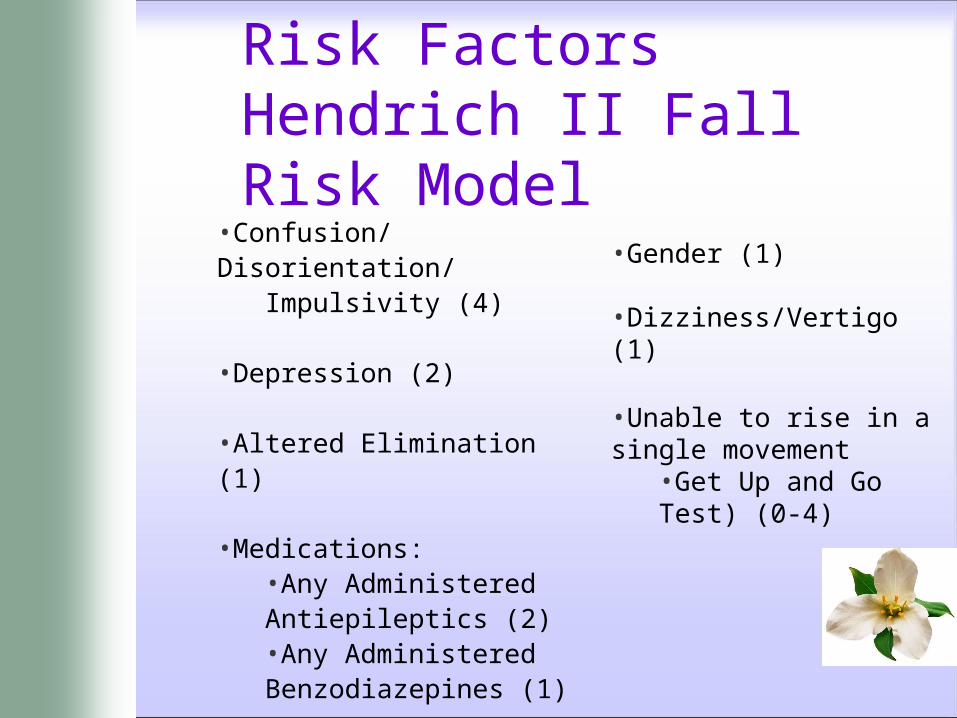
Risk Factors Hendrich II Fall Risk Model
•Confusion/Disorientation/Impulsivity (4)
•Depression (2)
•Altered Elimination (1)
•Medications:•Any Administered Antiepileptics (2) •Any Administered Benzodiazepines (1)
•Gender (1)
•Dizziness/Vertigo (1)
•Unable to rise in a single movement
•Get Up and Go Test) (0-4)



Fall Risk Interventions

Fall Watch Option
‘Fall Watch’ Option: Reserved for patients who require intensive surveillance.
‘Fall Watch’ Criteria: • Non-compliance of fall precautions• Impulsive or lack of safety
awareness• Discretion of nurse

Fall Watch Option
A magnetic Fall Watch sign is placed on the door frame of any patient identified as high risk.
When passing by that patient room, all hospital employees are to look into the room to observe if the patient is safe.

Fall Watch Option
If safe, employees continue on their way.
If patient is at risk, the employee is to maintain patient safety and put on the call light for assistance.
‘Fall Watch’ is the responsibility of everyone on the unit to ensure patient safety.
Keep room doors and curtains open.

Community:Interventions to Consider Cardiac evaluation Vision improvement Home safety modifications Medication reduction Physical Therapy Exercise
Tinetti ME, Kumar C. The patient who falls: “It’s always a trade-off. JAMA 2010 Jan 20;303(3):258-66

Bronson Intranet Handouts



Questions?
NICHENurses Improving Care of Health
System Elders
The SPICES Tool
Questions?
NICHENurses Improving Care of Health
System Elders
The SPICES Tool