NGT journal.pdf
14
ORIGINAL ARTICLE Comparing methods of determining insertion length for placing gastric tubes in children 1 month to 17 years of ageMarsha L. Cirgin Ellett, Mervyn D. Cohen, Susan M. Perkins, Joseph M. B. Croffie, Kathleen A. Lane, and Joan K. Austin Marsha L. Ellett, PhD, RN, is Professor, Indiana University School of Nursing; Mervyn D. Cohen, MB, ChB, is Professor, Department of Radiology, Riley Hospital; Susan M. Perkins, PhD, is Associate Professor, Division of Biostatistics, Indiana University School of Medicine; Joseph M. B. Croffie, MD, is Clinical Associate Professor, Division of Gastroenterology, Hepatology and Nutrition, Department of Pediatrics, Indiana University School of Medicine, Riley Hospital; Kathleen A. Lane, MS, is a Biostatistician, Division of Biostatistics, Indiana University School of Medicine; and Joan K. Austin, PhD, RN, FAAN, is Distinguished Professor Emerita, Indiana University School of Nursing; Indianapolis, USA Search terms Children, enteral feeding, feeding tube. Author contact [email protected], with a copy to the Editor: [email protected] Acknowledgement This study was funded by the National Institute for Nursing Research, R01 NR08111, Marsha L. Ellett, PI. Disclosure: The authors report no actual or potential conflicts of interest. First received March 31, 2011; Revision received June 13, 2011; Accepted for publication July 5, 2011. doi: 10.1111/j.1744-6155.2011.00302.x Abstract Purpose. The purpose was to compare three methods of predicting the gastric tube insertion length in children 1 month to 17 years of age: age- related, height-based (ARHB); nose-ear-xiphoid (NEX); and nose-ear-mid- umbilicus (NEMU). Design and Methods. The design was a randomized controlled trial. Chil- dren were randomly assigned to the ARHB, NEX, or NEMU groups. Tubes placed high were considered to be misplaced. Results. There were significant differences in percentages of correctly placed tubes, with ARHB and NEMU being more accurate than NEX. Practice Implications. NEX should no longer be used as a gastric tube insertion-length predictor. Either ARHB or NEMU should be used. Feeding by a nasogastric/orogastric (NG/OG) tube is preferred when the gastrointestinal tract is intact and the need for assisted feeding is expected to be short term (< 30 days; Kirby, Delegge, & Fleming, 1995). When tubes are out of place, children can be seriously harmed, causing increased morbidity and occasionally death. Gastric tubes are improperly positioned if the feeding orifices are located in the respiratory tract or esophagus or past the pylorus (Khilnani, 2007). Preliminary studies in children by our research team show that between 21% and 44% of these tubes are placed incorrectly (Ellett & Beckstrand, 1999; Ellett, Maahs, & Forsee, 1998). With the current emphasis on safety of hospitalized patients, these error rates are unacceptably high (Institute of Medicine, 2001, 2003, 2010). REVIEW OF CURRENT EVIDENCE FOR PRACTICE Much of the previous research on predicting the length to insert NG/OG tubes has been done in infants (Tedeschi, Atimer, & Warner, 2004; Weibley, Adamson, Clinkscales, Curran, & Bramson, 1987; Ziemer & Carroll, 1978). In brief, these researchers found the NG/OG tube place- ment error rate varied from 5% to 55.6%. Two studies found that direct distance nose-ear-xiphoid (NEX) was too short in predicting the length to insert NG/OG tubes (Weibley et al., 1987; Ziemer & Carroll). One study showed direct distance nose- ear-mid-umbilicus (NEMU) to be too short (Weibley et al.), while another study showed NEMU to be reasonably accurate (Tedeschi et al., Journal for Specialists in Pediatric Nursing 19 Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.
-
Upload
ipul-bebek-adus-kali -
Category
Documents
-
view
108 -
download
4
description
Medikal
Transcript of NGT journal.pdf

O R I G I N A L A R T I C L E
Comparing methods of determining insertion length for placinggastric tubes in children 1 month to 17 years of agejspn_302 19..32
Marsha L. Cirgin Ellett, Mervyn D. Cohen, Susan M. Perkins, Joseph M. B. Croffie, Kathleen A. Lane,and Joan K. Austin
Marsha L. Ellett, PhD, RN, is Professor, Indiana University School of Nursing; Mervyn D. Cohen, MB, ChB, is Professor, Department of Radiology, Riley
Hospital; Susan M. Perkins, PhD, is Associate Professor, Division of Biostatistics, Indiana University School of Medicine; Joseph M. B. Croffie, MD, is Clinical
Associate Professor, Division of Gastroenterology, Hepatology and Nutrition, Department of Pediatrics, Indiana University School of Medicine, Riley
Hospital; Kathleen A. Lane, MS, is a Biostatistician, Division of Biostatistics, Indiana University School of Medicine; and Joan K. Austin, PhD, RN, FAAN, is
Distinguished Professor Emerita, Indiana University School of Nursing; Indianapolis, USA
Search termsChildren, enteral feeding, feeding tube.
Author [email protected], with a copy to the Editor:
AcknowledgementThis study was funded by the National Institute
for Nursing Research, R01 NR08111, Marsha L.
Ellett, PI.
Disclosure: The authors report no actual or
potential conflicts of interest.
First received March 31, 2011; Revision received
June 13, 2011; Accepted for publication July 5,
2011.
doi: 10.1111/j.1744-6155.2011.00302.x
Abstract
Purpose. The purpose was to compare three methods of predicting thegastric tube insertion length in children 1 month to 17 years of age: age-related, height-based (ARHB); nose-ear-xiphoid (NEX); and nose-ear-mid-umbilicus (NEMU).Design and Methods. The design was a randomized controlled trial. Chil-dren were randomly assigned to the ARHB, NEX, or NEMU groups. Tubesplaced high were considered to be misplaced.Results. There were significant differences in percentages of correctlyplaced tubes, with ARHB and NEMU being more accurate than NEX.Practice Implications. NEX should no longer be used as a gastric tubeinsertion-length predictor. Either ARHB or NEMU should be used.
Feeding by a nasogastric/orogastric (NG/OG) tube ispreferred when the gastrointestinal tract is intactand the need for assisted feeding is expected to beshort term (< 30 days; Kirby, Delegge, & Fleming,1995). When tubes are out of place, children can beseriously harmed, causing increased morbidity andoccasionally death. Gastric tubes are improperlypositioned if the feeding orifices are located in therespiratory tract or esophagus or past the pylorus(Khilnani, 2007). Preliminary studies in children byour research team show that between 21% and44% of these tubes are placed incorrectly (Ellett &Beckstrand, 1999; Ellett, Maahs, & Forsee, 1998).With the current emphasis on safety of hospitalizedpatients, these error rates are unacceptably high(Institute of Medicine, 2001, 2003, 2010).
REVIEW OF CURRENT EVIDENCE FOR PRACTICE
Much of the previous research on predictingthe length to insert NG/OG tubes has beendone in infants (Tedeschi, Atimer, & Warner,2004; Weibley, Adamson, Clinkscales, Curran, &Bramson, 1987; Ziemer & Carroll, 1978). In brief,these researchers found the NG/OG tube place-ment error rate varied from 5% to 55.6%. Twostudies found that direct distance nose-ear-xiphoid(NEX) was too short in predicting the length toinsert NG/OG tubes (Weibley et al., 1987; Ziemer &Carroll). One study showed direct distance nose-ear-mid-umbilicus (NEMU) to be too short(Weibley et al.), while another study showedNEMU to be reasonably accurate (Tedeschi et al.,
Journal for Specialists in Pediatric Nursing
19Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

2004). See Ellett and colleagues (2011) for a morecomprehensive review of these studies.
Scalzo, Tominack, and Thompson (1992) reviewedthe radiographs of 14 of 36 children ranging in agefrom 8 months to 16 years needing a large-boregastric tube inserted in an emergency room for lavageas the initial treatment for toxic substance ingestion.The placement method was unspecified, and radio-graphs were not done in the other 22 children. Theystated that 7 of 14 (50%) of these tubes were malpo-sitioned with the most common problem (6 of 7)being “excess tube insertion, stretching the stomachinferiorly towards the pelvis” (Scalzo et al., 1992,p. 581). The other tube was malpositioned in theesophagus above the gastroesophageal junction(GEJ). The authors considered lavage tubes to beproperly placed when they were “well within thebody of the stomach with the distal end superimpos-ing the left upper abdominal quadrant on radiographand without the tip impinging on the wall of thestomach”(Scalzoet al., 1992,p.582).Theysuggestedusing an adaptation of Strobel, Byrne, Ament, andEuler’s (1979) previously published formula foresophageal pH probe placement: OG = 9.7 cm + (.226¥ length of child in cm) or NG = 8 cm + (.252 ¥ lengthof child in cm). Scalzo et al. tested these formulaeprospectively in only six randomly selected children(age range not provided) and found that five of sixtubes were well positioned in the stomach accordingto their criteria. One tube had the most proximalsuction port at the GEJ.
Klasner, Luke, and Scalzo (2002) conducted a ran-domized double-blind, controlled trial involving 89children ranging in age from 6 months to 18 yearsneeding gastric intubation in the emergency room.Children were stratified (tall, medium, and short)according to percentile height using standard growthcurves and were block randomized. Of the children,45 were assigned to the height-based graphic methodusing regression equations of Scalzo et al. (1992),and 44 were assigned to what is standardly called theNEMU method in which insertion length “was esti-mated by measuring the distance from the nose ormouth to the earlobe, to a point midway between thexiphoid process and the umbilicus” (Klasner et al.,2002, p. 269). Note that the authors referred to thismethod as the NEX method in their 2002 publication;however, to be consistent with standard terminology(which is what is being utilized in the current article),it will be referred to as the NEMU method. Theresearchers reported that three of the tubes, whichwereall in theNEMUgroup,were found tobeoutsidethe confines of the stomach; the exact position of
these three tubes was not reported. They reportedthat tubes inserted using a nomogram based onheight (graphic method) had a smaller mean distancefrom the center of the stomach compared to theNEMU method and showed less variability. Theradiographs were reviewed by two blinded pediatricemergency room physicians. A definition of thecenter of the stomach was “the midpoint between thelower esophageal sphincter or diaphragm andpylorus” (Klasner et al., 2002, p. 270).
Beckstrand, Ellett, and McDaniel (2007) con-ducted a prospective descriptive study in which thepotential of 20 external measures including NEX,NEMU, age, height, and weight were examined aspossible insertion length predictors in 494 children,2 weeks to 19 years of age, undergoing upper gas-trointestinal endoscopy, or esophageal manometricstudies. Regression equations using height in agegroups (age-related height-based [ARHB]), derivedindependently of the Klasner and colleagues (2002)graphic method discussed above, were found to bethe best predictors of optimal placement of the endo-scope or manometric probe in the stomach. Theresearchers concluded that age-specific regressionequations using the child’s height/length have thepotential to predict accurately the distances to thebody of the stomach in 98.8% of children youngerthan 100 months and in 96.5% of children olderthan 100 months. The next best choice was theNEMU length. The Beckstrand et al. study did notclinically validate their proposed ARHB equations ina new cohort.
Although NEX has been shown to be too short inprevious studies, a telephone survey of 113 Level IIand III nurseries in five Midwestern states publishedin 1996 by Shiao and DiFiore (1996) found that 98%of nurses continued to use the direct NEX distance tocalculate tube insertion distance. Because of thecontinued use of NEX as an insertion-length predic-tor, the mixed results from the three studies testingNEMU, and the need to test the ARHB equationsclinically, the current study was undertaken.
PURPOSE
The results being presented herein were part of alarger study examining gastric tube placement in276 children including neonates. The purpose of thestudy reported here was to compare the error ratesof three existing methods of predicting the correctgastric tube insertion length in 103 children 1 monthto 17 years of age: ARHB, NEX, and NEMU.
Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age M. L. Cirgin Ellett et al.
20 Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

METHODS
Design
A single-blind, randomized controlled trial was con-ducted. The children were randomly assigned tohave their NG/OG tube inserted using one of thethree insertion-length predictors: ARHB, NEX, orNEMU. The statisticians (third and sixth authors)used a computer-generated stratified block random-ization strategy in which stratification was by use ofacid-inhibiting medication (needed for a differentaim of this trial) and age group (1–28 months,29–100 months, and 101–204 months). The randomassignments were delivered to the research nurses insequentially numbered opaque sealed envelopes.Envelopes were opened just prior to inserting theNG/OG tube to determine which method to use.
Recruitment
Children were recruited from three Midwesternhospitals. All children hospitalized on one of the par-ticipating units requiring an NG/OG tube to beinserted were eligible unless: (a) their staff physi-cians refused consent, (b) their medical conditioncould drastically affect their gastric acid-secretingability (e.g., Zollinger-Ellison Syndrome or congeni-tal achlorhydria), (c) they had had previous gastricsurgery resulting in removal of part of the stomach,or (d) the NG/OG tube ordered by the physician hadorifices further than 3 cm from the tip of the tube.Exclusion criterion (b) was needed for another aimof this study; a manuscript reporting these results isin preparation.
Procedures
This study was approved by the appropriate institu-tional review board and the hospitals/units in whichthe study was conducted. Two research associateswere trained in all aspects of data collection by theprincipal investigator (PI, first author) using awritten protocol. They collected approximately 83%of the data. Other research nurses were trained bythe two research associates using the same protocoland collected the other 17% of the data. The PIevaluated each research nurse prior to giving him/her permission to collect data independently. Inter-rater reliability was collected between each traineddata collector and the PI with approximately every15th child per nurse. A research associate orresearch nurse obtained anthropometric data from
the child. In children younger than 2 years of age,length was obtained by marking with a washablemarker on the underlying sheet the length from themost distal border of the head to the most distalborder of the heel held perpendicular to the leg withthe child lying supine and flat, and then measuringthe marked length with a paper tape measure afterthe child had been moved to the side of the sheet toallow accurate measurement. In children youngerthan or equal to 2 years of age, a standing height wasobtained using a stadiometer with the child’s headhorizontal. NEX and NEMU were measured bystretching the tube to be inserted from the tip of thenose to the bottom of the earlobe and next to thexiphoid process (NEX) and then to the observedmidpoint between the xiphoid process and theumbilicus (NEMU). In addition, birth date, term/preterm status, gestational age, weight, and acid-inhibiting medication use were obtained from themedical records of all children. For children youngerthan 3 years of age, corrected age was calculated bysubtracting the number of weeks/days prematurefrom the chronological age in weeks/days (March ofDimes Foundation, 2010) and used for the stratifica-tion and in the ARHB equations.
The nurse caring for the child was consulted todetermine the standard method for inserting tubes(nasally or orally) in children in the specific unit.Enrolled children were then randomly assigned tohave their tubes inserted using one of the threeexisting insertion-length predictors: NEX, NEMU, orARHB. The following ARHB equations were used(Beckstrand, 2005):
OG tube insertion distancecm HT if to months ocm= + ( )13 3 19 1 28. . ff agecm HT if to months of agecm HT
cm= + ( )= +
16 8 19 29 10015 1 22
. .
. . ccm if months of age( ) > 100
NG tube insertion distancecm HT if to months ocm= + ( )14 8 19 1 28. . ff agecm HT if to months of agecm HT
cm= + ( )= +
18 3 19 29 10016 6 22
. .
. . ccm if months of age( ) > 100
Measurements from all three insertion lengthmethods were obtained on all children. The tubewas then inserted using the randomly assignedinsertion-length predictor distance by the researchnurse. The nurse temporarily taped the tube inplace.
Shortly after placement of the tube, an abdominalradiograph was obtained to show the internal loca-tion of the tube. Once the radiograph was read by a
M. L. Cirgin Ellett et al. Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age
21Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

pediatric radiologist, physician, or pediatric nursepractitioner (based on unit policy) using theirnormal criteria, the tube length was adjusted as nec-essary prior to use based on the healthcare provid-er’s recommendation.
Radiographs
Currently, an abdominal radiograph provides theonly consistently valid and reliable evidence of theinternal location of NG/OG tubes, and it was consid-ered the “gold standard” for initial placement in thisstudy. All radiographs taken after initial placementof the tube were reviewed at a later time by a singleboard-certified pediatric radiologist (second author)who was blinded as to the method used to estimatethe required length of the tube. For each radiographthe location of the tip of the tube was classified intoone of four locations:
1. Tube tip in the esophagus (if the tube tip was inthe esophagus, then it was noted if the lower endof the tube was straight or curled back on itselfwith the tip pointing towards the head),
2. Tube tip in the region of the GEJ,3. Tube tip in the stomach, or4. Tube tip in the pylorus or the duodenum.
In addition, the length of tube below the dia-phragm was measured when the tip was clearlyvisible. This was measured from the junction of thediaphragm with the left side of the adjacent vertebralbody to the tip of the tube.
Definition of correct placement
For the primary analysis, only tubes that were placedtoo high with the tube tip in the esophagus or GEJwere considered to be placed incorrectly, and tubesplaced in the stomach, pylorus, or duodenum wereconsidered correctly placed. This decision was madebecause, based on prior experience of the researchteam, it was known that tubes placed the same dis-tance below the GEJ tended to either curve to theleft along the greater curvature of the stomach or tothe right into or through the pylorus into the duode-num by chance. As a secondary analysis, a morestrict definition of correctness was used whereby thetube tip was required to actually be in the stomach.
Data analysis
Descriptive statistics were calculated, includingmeans and standard deviations for continuous vari-
ables and number and percent in each category forcategorical variables. One-way analysis of variance(ANOVA) models were used to compare child char-acteristics such as ethnicity/race, gender, age, andheight across the three insertion methods. Chi-square tests or Fisher’s exact tests as appropriate forsmall sample sizes were used to compare the cat-egorical child characteristics (see Table 1). All analy-ses were performed on an intention-to-treat basis.For the primary objective, chi-square tests wereused to compare the correct placement ratesbetween the insertion methods. Following a signifi-cant overall comparison of the three methods, pair-wise comparisons were made using chi-square testsor Fisher’s exact tests. Logistic regression was used tomodel misplacement to obtain confidence intervalestimates for odds ratios (both crude and adjustedfor the two stratification factors) comparing thethree methods. A t-test was used to compare themeasurement lengths between stomach and intesti-nal placements for tubes deemed long enough toenter the intestine.
RESULTS
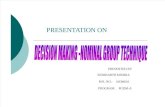
Children were recruited from three Midwesternhospitals. A total of 1,087 children, ages 1 monthto 17 years, met inclusion criteria. Only in 55.2%of the children (n = 600) did physicians agree toallow the family to be approached regarding studyparticipation. Reasons given for physician’s refusalincluded that the child was too ill and/or had acomplicated social situation. Also, in few cases, thestaff physician was not available to give permission.In 22.0% (132/600) of children in which physicianpermission was received to approach the family,parent(s) provided written informed consent;reasons given for refusal included radiation expo-sure of radiograph for research purposes and thatthe child had already been through too much. Inaddition, children 7 years of age and older alsoneeded to give written assent to participate. A fewchildren refused. The final overall recruitment ratewas 17.2% (representing 78.0% of children whoseparents provided informed consent) because insome cases, the child’s condition improved allow-ing progression to oral feeding, the unit was toobusy for nurses to allow study participation, chil-dren were discharged home with the tube in placeafter parental consent was received but beforethe child could participate in the study, or thechild refused. Figure 1 shows the Consolidated
Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age M. L. Cirgin Ellett et al.
22 Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

Standards of Reporting Trials (CONSORT) flowdiagram of the study. Because of the limited infor-mation allowed to be collected prior to writtenparental consent and a signed Health InsurancePortability and Accountability Act (HIPAA) form, itwas not possible to test whether children partici-pating in this study differed significantly from thosewho did not.
The sample consisted of 103 hospitalized children(1 month to 17 years of age) requiring placement ofan NG/OG tube. There were 101 NG tubes and 2 OGtubes placed in children. Because only two OG tubeswere inserted during this study, the OG regressionequations could not be separately tested. There were36 tubes placed by the ARHB method, 35 by theNEMU method, and 32 by the NEX method. Therewere no significant differences among the threeinsertion methods on child characteristics, includingethnicity/race, gender, and age (see Table 1).
Of the tubes inserted, 97.1% using NEMU, 88.9%using ARHB, and 59.4% using NEX were correctlyplaced in the stomach, duodenum, or pylorus
regions (see Table 2). During insertion, three tubescurled back on themselves in the esophagus, leavingthe tip of the tube near the entrance to the respira-tory tract. These placement errors would not havebeen known prior to feeding the children throughthese tubes without the abdominal radiographrequired as part of this study. Based on theintention-to-treat principle, these cases were treatedas tube placement errors when calculating the errorrate. The differences in percentages of correctlyplaced tubes among the three methods was signifi-cant (chi-square = 18.09 p = .0001), with bothNEMU and ARHB being more accurate than NEX(NEMU chi-square = 14.43, p = .0001, phi coefficient= -.46 [large effect]; ARHB chi-square = 7.87, p =.005, phi coefficient = -.34 [large effect]). There wasno statistically significant difference between ARHBand NEMU (Fisher’s exact p = .357). Assumingthe true percentages of correct placements in thestomach/duodenum/pylorus were as observed inthis study, there was 97% power to detect an asso-ciation between placement method and correct
Table 1. Comparison of PatientCharacteristics by Three PlacementMethods
ARHB (n = 36) NEMU (n = 35) NEX (n = 32) p-value
Gender, n (%)
.5726Male 20 (55.6) 19 (54.3) 14 (43.8)
Female 16 (44.4) 16 (45.7) 18 (56.3)
Agea (mo), n (%)
.96671–28 months 16 (44.4) 15 (42.9) 15 (46.9)
29–100 months 15 (41.7) 14 (40.0) 11 (34.4)
101–215 months 5 (13.9) 6 (17.1) 6 (18.8)
Term, n (%)
.6403Preterm 28 (77.8) 27 (77.1) 22 (68.8)
Full term 8 (22.2) 8 (22.9) 10 (31.3)
Length (cm), mean � SD 92.5 � 30.3 94.9 � 31.4 95.2 � 33.1 .9251
Race, n (%)
.7418bCaucasian 29 (80.6) 28 (80.0) 29 (90.6)
African American 3 (8.3) 4 (11.4) 2 (6.3)
Other 4 (11.1) 3 (8.6) 1 (3.1)
Ethnicity, n (%)
.7749bHispanic 2 (5.6) 3 (8.6) 1 (3.1)
Non-Hispanic 34 (94.4) 32 (91.4) 31 (96.9)
Acid-inhibiting medication
use, n (%).8794
On 10 (27.8) 9 (25.7) 10 (31.3)
Not on 26 (72.2) 26 (74.3) 22 (68.8)
Tube type, n (%)
.7601bNG 35 (97.2) 35 (100.0) 31 (96.9)
OG 1 (2.8) 0 (.0) 1(3.1)
aAge is corrected if < 36 months; bp-value is from the Fisher’s exact test.
ARHB is the age-related, height-based regression equation; NEMU is the distance from the nose
to the ear to the mid-umbilicus; NEX is the distance from the nose to the ear to the xiphoid; NG
is a nasogastric tube; OG is an orogastric tube.
M. L. Cirgin Ellett et al. Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age
23Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

placement using a chi-square test (two-sided, levelof significance .05). Conservatively using FisherExact tests (two-sided, level of significance .017) toestimate power for all pair-wise differences, therewas 93% power when comparing NEX to NEMU,but only 57% power when comparing NEX toARHB, and 4% power when comparing NEMU toARHB.
From a logistic regression model, the estimatedodds ratios (unadjusted) for NEX compared toNEMU and ARHB were 23.26 (95% CI 2.82-191.88) and 5.47 (95% CI 1.56-19.22), respec-tively, indicating that if NEX rather than NEMU orARHB was used as the insertion-length predictor,the odds were 23.26 or 5.47 times greater that the
tube would be misplaced on insertion, leaving thetip and/or pores in the esophagus or GEJ. Adjust-ing for the two stratification factors, use of acid-inhibiting medications (p = .2935) and age group(p = .3270), did not substantially change theresults. In addition, use of the stricter definition oftreating only tubes actually placed in the stomachas correctly placed was explored. Using the stricterdefinition, the percentage of correctly placed tubesdecreased from 97.1% to 85.7% using the NEMUmethod (see Table 2). This change did not result insignificant differences in the results between thetwo definitions.
To demonstrate in this sample that tubes placedthe same distance below the GEJ tend to either curve
Figure 1 Consolidated Standards of Reporting Trials (CONSORT) Flow Diagram.
Note: ARHB is the age-related height-based regression equation.
NEMU is the distance from the nose to the ear to the mid-umbilicus.
NEX is the distance from the nose to the ear to the xiphoid.
Table 2. Radiographic Location of NG/OG Tube by Insertion-Length Predictors
ARHB (n = 36)(%)
NEMU (n = 35)(%)
NEX (n = 32)(%) p-value
Placement in stomach/duodenum/pylorus 32 (88.9) 34 (97.1) 19 (59.4) .0001a,b
Placement in stomach 32 (88.9) 30 (85.7) 19 (59.4) .0056a,b
ap-value comparing NEX and NEMU < .05; bp-value comparing NEX and ARHB < .05.
ARHB is the age-related, height-based regression equation; NEMU is the distance from the nose to the ear to the mid-umbilicus; NEX is the dis-
tance from the nose to the ear to the xiphoid; NG is a nasogastric tube; OG is an orogastric tube.
Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age M. L. Cirgin Ellett et al.
24 Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

to the left along the greater curvature of the stomachor to the right into or through the pylorus into theduodenum by chance, we first determined theminimal distance a tube could be inserted intothe stomach before it could possibly reach thepylorus/duodenum region. In a separate study, thepediatric radiologist measured the distance betweenthe GEJ and the pylorus of 200 children ages 1–204months chronological age undergoing upper gas-trointestinal barium (UGI) studies for medicalreasons in 2009 (Cohen, Perkins, Lane, & Ellett, inpress). This sample was utilized because both theGEJ and pylorus are visible on UGI radiographsusing contrast but are not visible on the abdominalradiographs without contrast that are routinelydone for determining the location of NG/OG tubes.In the 77 children in the youngest age group (1–28months), the mean distance was 6.0 cm, the medianwas 5.5 cm, and the standard deviation was 2.8 cm,and, although there was a large standard deviationdue to the differences in the shape of the stomach,the 11.6 cm distance (mean + 2 standard deviations)between the GEJ and pylorus was supported as inthe complete sample of 200, 89% of the distancesmeasured less than or equal to 11.6 cm. The 11.6 cmvalue represented the mean + 2 standard deviationsin the youngest age group, which is a conservativeestimate as the older age categories have largervalues. In a post hoc analysis in the current study,there were 14 children who had measurementsfrom the diaphragm to the tip along the curvature ofthe tube over 11.6 cm that would indicate the tubewas potentially long enough to enter the pylorus/duodenum regions. No difference (p = .7246) in thiscurved length was seen on average between the 13tubes that stayed in the stomach (mean � SD; 14.8 �3.0) and the 1 that entered the pylorus/duodenumregion (mean = 14.8).
DISCUSSION
A major finding from this randomized clinical trialinvolving 103 children was that 97% of NG/OGtubes using NEMU, 89% using ARHB, and only 59%using NEX were correctly placed in the stomach,duodenum, or pylorus regions, and 86% of NG/OGtubes using NEMU, 89% using ARHB, and 59%using NEX were correctly placed in the stomachonly. This means that 41% of tubes inserted usingNEX were placed with the tube tip ending either inthe esophagus or GEJ. Both NEMU and ARHB werestatistically superior to NEX as an NG/OG tube
insertion-length predictor in children regardless ofwhich definition of tube placement error (less ormore restrictive) was used. These results are similarto those of Beckstrand and colleagues (2007), who,in a descriptive study involving a large sample ofchildren, also found ARHB and NEMU to be thesuperior NG/OG tube insertion-length predictorswhen compared to NEX. Klasner and colleagues(2002) found the graphic method using height to besuperior to NEMU.
Based on the results of four studies in children(Beckstrand et al., 2007; Klasner et al., 2002;Weibley et al., 1987; Ziemer & Carroll, 1978), NEXshould no longer be used as an insertion-lengthpredictor for placing NG/OG tubes in childrenbecause of the significant risk of the tube tip andorifices ending in the esophagus or the GEJ,increasing the likelihood of the child aspiratingfeeding formula.
Figure 2 allows the healthcare provider a way toimplement the ARHB method. To use, first choosethe appropriate part of the table based on whetheran NG or OG tube is to be inserted and the child’sage. Next, find the child’s length in column 1 andthen determine the recommended length to insertthe tube in the same row horizontally in column 2.Alternatively, the regression equations can beentered into the hospital’s computer system or inpersonal digital assistants allowing healthcare pro-viders the ability to insert the child’s height/lengthand obtain the desired NG or OG tube insertionlength.
Clearly tubes with a length in the stomach lessthan the distance from the GEJ to the pylorus couldnot pass through the pylorus. In this study, the factthat only 1 of 14 tubes that were long enough toenter the pylorus/duodenum region actually didpass through the pylorus suggested that errors inestimating desired total tube length were extremelyimportant if the length was too short (tube tip wouldbe in the esophagus or GEJ) but probably not ofgreat importance if the estimated tube length wastoo long.
Limitations
One limitation of this study was the low recruitmentrate of 17.2%. The vulnerability of the populationand the multiple layers of protective gatekeepersmade recruitment difficult. A second limitation wasthat there was lack of power to detect differencesbetween ARHB and NEMU.
M. L. Cirgin Ellett et al. Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age
25Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

Figure 2 Length to Insert Nasogastric/Orogastric (NG/OG) Tubes Based on Child’s Height/Length.
Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age M. L. Cirgin Ellett et al.
26 Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

Figure 2 Continued
M. L. Cirgin Ellett et al. Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age
27Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

Figure 2 Continued
Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age M. L. Cirgin Ellett et al.
28 Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

Figure 2 Continued
M. L. Cirgin Ellett et al. Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age
29Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

Figure 2 Continued
Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age M. L. Cirgin Ellett et al.
30 Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

References
Beckstrand, J. (2005). Predicting the insertion length for gastricgavage tubes. (NIH R01NR1922 Final Grant Report.)Unpublished report.
Beckstrand, J., Ellett, M. L. C., & McDaniel, A. (2007).Predicting the internal distance to the stomach forpositioning nasogastric and orogastric feeding tubes inchildren. Journal of Advanced Nursing, 59, 274–289.doi:10.1111/j.1365-2648.2007.04296.x
Cohen, M. D., Perkins, S. M., Lane, K. L., & Ellett, M. L. (inpress). Accurate localization of the position of the tip of anaso/orogastric tube in children. Pediatric Radiology.
Ellett, M. L. C., & Beckstrand, J. (1999). Examination ofgavage tube placement in children. Journal of the Societyof Pediatric Nurses, 4(2), 51–60. doi: 10:1111/j.1744-6155.1999.tb00035.x
Ellett, M. L. C., Cohen, M. D., Perkins, S. M., Smith, C. E.,Lane, K. L., & Austin, J. K. (2011). Predicting theinsertion length for gastric tube placement in neonates.Journal of Obstetric, Gynecologic, and Neonatal Nursing, 40,412–421. doi:10.1111/j.1552-6909.2011.01255.x
Ellett, M. L., Maahs, J., & Forsee, S. (1998). Prevalence offeeding tube placement errors and associated risk factorsin children. American Journal of Maternal Child Nursing,23(5), 234–239. doi: 10.1097/00005721-199809000-00004
Gharib, A. M., Stern, E. J., Sherbin, V. L., & Rohrmann,C. A. (1996). Nasogastric and feeding tubes. PostgraduateMedicine, 99(5), 165–168, 174–176.
Institute of Medicine. (2001). Crossing the quality chasm.Washington, DC: National Academy Press.
Institute of Medicine. (2003). Keeping patients safe:Transforming the environment for nurses. Washington, DC:The National Academies.
Institute of Medicine. (2010). The future of nursing: Leadingchange, advancing health. Washington, DC: The NationalAcademies.
How might this information affectnursing practice?
Abdominal radiographs have been recommendedby several research groups to determine tube place-ment in adults and children (Ellett et al., 2011;Gharib, Stern, Sherbin, & Rohrmann, 1996; Walsh& Banks, 1990). The authors agreed that radio-graphic verification at the time of initial NG/OGtube placement or tube change is necessary in chil-dren to ensure that the tube has not been mis-placed by curling in the esophagus or ending in theesophagus, pylorus, or duodenum. This radiographshould be read by an appropriately trained health-care provider prior to using the tube for feeding ormedication instillation. Institution-specific policieswill need to be evaluated based on the best avail-able evidence from this and other studies, keepingin mind the goal of keeping children who haveNG/OG tubes safe.
NEX with an error rate of 41% should no longerbe used as an NG/OG tube insertion-length predic-tor in children. Either NEMU or ARHB for NG tubesshould be used. NEMU should be measured fromthe tip of the nose to the ear lobe to the observedmidpoint between the xiphoid and the umbilicus.A chart to facilitate use of the ARHB equations isprovided in Figure 2. Although use of either theNEMU or ARHB insertion-length predictor is morelikely to place the NG/OG tube in the stomach,there is still an 11.1–14.3% error rate if the morerestrictive definition of correct tube placement (inthe stomach) is used.
Figure 2 Continued
M. L. Cirgin Ellett et al. Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age
31Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.

Khilnani, P. (2007). Errors in placement of enteral tube incritically ill children: Are we foolproof yet. PediatricCritical Care Medicine, 8, 193–194. doi:10.1097/01.PCC.0000257106.94293.F2
Kirby, D. F., Delegge, M. H., & Fleming, C. R. (1995).American Gastroenterological Association technicalreview on tube feeding for enteral nutrition.Gastroenterology, 108, 1282–1301. doi:10.1016/0016-5085(95)90231-7
Klasner, A. E., Luke, D. A., & Scalzo, A. J. (2002). Pediatricorogastric and nasogastric tubes: A new formulaevaluated. Annals of Emergency Medicine, 39, 268–272.doi:10.1067/mem.2002.120124
March of Dimes Foundation. (2010). Your premature baby.Retrieved from http://www.marchofdimes.com/pnhec/24043_24065.asp
Scalzo, A. J., Tominack, R. L., & Thompson, M. W. (1992).Malposition of pediatric gastric lavage tubesdemonstrated radiographically. Journal of EmergencyMedicine, 10, 581–586. doi:10.1016/0736-4679(92)90142-G
Shiao, S. Y., & DiFiore, T. E. (1996). A survey of gastrictube practices in level II and level III nurseries. Issues
in Comprehensive Pediatric Nursing, 19, 209–220.doi:10.3109/01460869609026862
Strobel, C. T., Byrne, W. J., Ament, M. E., & Euler, A. R.(1979). Correlation of esophageal lengths in childrenwith height: Application to the Tuttle test withoutprior esophageal manometry. Journal ofPediatrics, 94(1), 81–84. doi:10.1016/S0022-3476(79)80361-3
Tedeschi, L., Atimer, L., & Warner, B. (2004). Improvingthe accuracy of indwelling gastric feeding tubeplacement in the neonatal population. Neonatal IntensiveCare : The Journal of Perinatology-Neonatology, 17(1),16–18.
Walsh, S. M., & Banks, L. A. (1990). How to insert asmall-bore feeding tube safely. Nursing, 20(3), 55–59.
Weibley, T. T., Adamson, M., Clinkscales, N., Curran, J., &Bramson, R. (1987). Gavage tube insertion in thepremature infant. American Journal of Maternal ChildNursing, 12(1), 24–27. doi:10.1097/00005721-198701000-00009
Ziemer, M., & Carroll, J. S. (1978). Infant gavagereconsidered. American Journal of Nursing, 78,1543–1544. doi:10.2307/3461959
Comparing Methods of Determining Insertion Length for Placing Gastric Tubes in Children 1 Month to 17 years of Age M. L. Cirgin Ellett et al.
32 Journal for Specialists in Pediatric Nursing 17 (2012) 19–32 © 2011, Wiley Periodicals, Inc.