NEXT GENERATION IMMUNOTHERAPIES - Neovacsneovacs.fr/wp-content/uploads/pi-10-03-15.pdf · NEXT...
32
NEXT GENERATION IMMUNOTHERAPIES NEOVACS MARCH 2015 INVESTOR PRESENTATION Miguel Sieler, CEO
Transcript of NEXT GENERATION IMMUNOTHERAPIES - Neovacsneovacs.fr/wp-content/uploads/pi-10-03-15.pdf · NEXT...

NEXT GENERATION IMMUNOTHERAPIES
NEOVACS
MARCH 2015
INVESTOR PRESENTATION Miguel Sieler, CEO

2
Disclaimer
This presentation and the information contained herein does not constitute or form part of, and should not be construed as, an offer or invitation to sell or subscribe for, or a solicitation of any offer or invitation to acquire, dispose of or subscribe for, shares in NEOVACS ("the Company") in any country. The decision to buy or sell shares of the Company should be based solely on the documents which have been reviewed by the "Autorité des Marchés Financiers"(AMF). The AMF has approved the Prospectus registered on February 14, 2013 under number 13-032 which includes an issuance memo, and an update to the "Document de Référence" registered with the AMF under number D.12-0109-A01 on February 14, 2013. The publication of this presentation in certain countries may violate applicable regulations. With respect to the member states of the European Economic Area whichhave implemented the Directive 2003/71/EC of the European Parliament and the Council of November 4, 2003 (the “Prospectus Directive”), other than France, no action has been undertaken or will be undertaken to make an offer to the public of the securities referred to herein requiring a publication of a prospectus in any relevant member state (other than France). As a result, the securities may not and will not be offered in any relevant member state (other than France) except in accordance with the exemptions set forth in Article 3(2) of the Prospectus Directive, if they have been implemented in that relevant member state, or under any other circumstances which do not require the publication by NEOVACS of a prospectus pursuant to Article 3 of the Prospectus Directive and/or to applicable regulations of that relevant member state. The information contained therein does not constitute an offer for securities in the United States, Canada, Australia or Japan or in any other jurisdiction. This presentation should not be published, transmitted or distributed, directly or indirectly, in the United States, Canada, Australia or Japan. This presentation is not an offer for sale or a solicitation of offers to purchase NEOVACS securities in the United States. The securities of NEOVACS may not be offered or sold in the United States absent registration or an exemption from registration under the U.S. Securities Act of 1933, as amended. NEOVACS does not intend to register any portion of the offering in the United States or to conduct a public offering of securities in the United States. This presentation does not constitute an invitation or inducement to engage in investment activity under section 21 of the Financial Services and Markets Act 2000 and is for distribution only to persons who (A) are outside the United Kingdom, or (B) are qualified investors as described in section 86(7) of the Financial Services and Markets Act 2000 (being persons falling within Article 2.1(e)(i), (ii) or (iii) of Directive 2003/71/EC) and (i) have professional experience in matters relating to investments falling within the definition of "investment professionals" in Article 19(5) of the Financial Services and Markets Act 2000 (Financial Promotion) Order 2005 (the "Order"), or (ii) are persons falling within Article 49(2)(a) to (d) ("high net worth companies, unincorporated associations etc") of the Order, or (iii) to whom it may otherwise be lawfully communicated (all such persons together being referred to as "relevant persons"). This presentation is directed only at relevant persons and must not be acted on or relied on by persons who are not relevant persons. Any investment or investment activity to which this presentation relates is available only to relevant persons. This presentation contains forward-looking statements. No guarantee can be given as to any of the events anticipated by the forward-looking statements, which are subject to inherent risks, including those described in the Document de Référence registered with the Autorité des Marchés Financiers under number R.12-008 on March 30, 2012 and the Note d’Opération that was approved by the Autorité des Marchés Financiers on February 14, 2013, changes in economic conditions, the financial markets or the markets in which NEOVACS operates.

3
Overview
1 2
3 4
CORPORATE HIGHLIGHTS CLINICAL AND PRECLINICAL PROGRAMS
APPENDIX FINANCIALS AND WRAP UP

4
Corporate Highlights
A CLINICAL-STAGE COMPANY DEVELOPING IMMUNOTHERAPIES FOR AUTO-IMMUNE AND CHRONIC DISEASES
Company University spin-off (Pierre and Marie Curie University) in 1993, Company formed in 2003. Seasoned leadership, 20-strong team including 6 Ph.D.s, headquartered in Paris.
Approach Active immunotherapy: using a patient’s own immune system to regulate inappropriate immune responses
Products Kinoids, new anti-cytokine therapeutic vaccines
Pipeline
4 products in immunology and inflammatory diseases and immuno-oncology:
1 clinical-phase product in Lupus and Dermatomyositis
2 pre-clinical phase products in 3 indications (Age-related Macular Degeneration, solid tumors, allergy)
Markets Inflammatory and autoimmune diseases, allergies and cancers: billion dollar markets
Financials Public Listing on NYSE Alternext Paris since April 2010 (ALNEV, ISIN: FR0004032746)

5
Treatment Resistance Creates Major Unmet Need
CDAI 70 (Week 30)
Accent I
MAJOR NEED FOR NEW TREATMENTS WHICH ARE NOT SUSCEPTIBLE TO REJECTION OR RESISTANCE
CDAI 70 (Week 26)
Charm
CDAI 100 and HBI* (Week 26)
Precise 2 – 3
Note: * CZP given open label after 6 months and HBI used
49% 57%
48% 59%
37% 53% 59%
Infliximab
Placebo
Adalimumab
Placebo
Certolizumab pegol
Placebo
100%
0%
100%
0%
100%
0% 6 12 18 6 12 6 12
Months Months Months
Loss of response to 3 monoclonal antibodies in Crohn’s Disease – Study by Professor M. Allez, M.D., Ph.D., Hôpital Saint-Louis, Paris

6
Biologic Penetration Limited by High Prices
A MARKET WITH CONTINUED HIGH GROWTH POTENTIAL, ESPECIALLY FOR LESS COSTLY THERAPEUTICS, ESPECIALLY IN LUPUS
Note: (1) source: Datamonitor, August 2011
/ yr USA France/Europe
Enbrel (Amgen/Pfizer) 14 300 $ 14 861 €
Humira (Abbvie) 17 700 $ 15 118 €
Remicade (J&J/Merck) 20 390 $ 11 567 €
Benlysta (HGS/GSK) 30 540 $ 19 067 €
Drug (molecule) Pharma Sales (M$) Growth
Humira (adalimumab) ABBVIE 10,659 15,0%
Remicade (infliximab) J&J / MERCK 8,944 8,90%
Enbrel (etanercept) PFIZER/AMGEN 8,325 4,50%
Benlysta (HGS/GSK) GSK 229 130%
48%
18%
30%
22%
33%
25%
20%
USA Japan France Germany Italy Spain U.K.
Proportion of diagnosed patients receiving a biologic in 2010
Cost of treatment of selected biologics
2013 sales of top 3 anti-TNF biologics
Source: Corporate data, 2011 and Datamonitor Report on Benlysta

7
Kinoid Technology: Vaccine-Like Approach to Treating Chronic Diseases
– Target multiple epitopes
– Blocking of overproduced cytokine, and its pro inflammatory effects
– Specific to cytokine: no cross-neutralization with other cytokines
– No blocking anti-antibodies (ADA)
– Broad and sustained efficacy
– T cell tolerance is NOT broken: no uncontrolled autoimmunity
The Kinoid is an immunogenic compound made of: T Cells generated by the carrier protein (KLH) bypass B cell tolerance to induce self polyclonal anti-cytokine antibodies:
Conjugation and
inactivation
Kinoid
Polyclonal antibodies to targeted cytokine
Targeted cytokine
Carrier protein
Components of active immunotherapy Immunization Stimulation of the body’s immune system

8
Polyclonal antibodies
Kinoid Technology: Superiority of the Polyclonal Approach
INDUCING A SAFE AND EFFECTIVE POLYCLONAL RESPONSE FROM THE BODY’S OWN IMMUNE SYSTEM
Monoclonal antibodies:
– Injection of non-self Abs
– Abs bind to one specific epitope of the cytokine
– Risk of monoclonal antibody rejection and loss of efficacy (Anti-drug antibodies)
Current treatments
Monoclonal antibodies
Polyclonal antibodies:
– Self Abs generated by the patient’s immune system
– Abs bind to multiple epitopes of the targeted cytokine
– Better and sustained antibody efficacy
– Excellent tolerance
Neovacs treatment

9
Kinoid Technology: Competitive Positioning vs. Monoclonal Antibodies
KINOIDS: A MAJOR BREAKTHROUGH WITH THE POTENTIAL TO SUPERSEDE MONOCLONAL ANTIBODIES
Fully human response: no risk of rejection
3 to 5 injections per year vs. once every 2 – 4 weeks
~ 1mg of protein/year vs. > 1g /year with mAbs
Binding to multiple epitopes vs. single epitopes

10
Scientific Advisory Board New York, NY 12 February 2015
Pr. JACQUES BANCHEREAU, PhD
Président du SAB
• Director of immunological sciences The Jackson Laboratory for Genomics Medicine, At the UConn Health Center
• Baylor Institute for Immunology Research, Dallas, Texas, USA
Dr. VIRGINIA PASCUAL
• Director, Center for Inflammation and Autoimmune Diseases
• Director, Center for Personalized Medicine
• Adjunct Professor of Pediatrics, University of Texas Southwestern Medical Center, Dallas, Texas
• Adjunct Professor of Pediatrics, Mount Sinai School of Medicine, New York, New York
• Adjunct Associate Professor of Biomedical Studies, Baylor University
Pr. MIRIAM MERAD, MD, PhD
• Professor Oncological Sciences and Medicine, Tisch Cancer Institute, New York
Pr. STEVE A GREENBERG, MD • Department of Neurology, Brigham and Women's
Hospital and Children's Hospital Informatics Program, • Harvard Medical School and Harvard-MIT Division of
Health Sciences and Technology, Boston, Massachusetts
Pr. BETTY DIAMOND, MD • Investigator & Head, Center for Autoimmune and
Musculoskeletal Diseases, The Feinstein Institute for Medical Research
• Professor of Molecular Medicine and Medicine, Hofstra North Shore-LIJ School of Medicine, Manhasset, NY
Pr. NAPOLEONE FERRARA, MD • Professor of Ophthalmology and Pathology Senior
Deputy • Director for Basic Sciences, UC San Diego Health System
- La Jolla, CA
Pr. LAURENCE ZITVOGEL, MD • Research Director at INSERM U1015, Gustave
Roussy Cancer Campus • Center of Clinical Investigations in Biotherapies of
Cancer (CICBT) 507, Villejuif, France
Pr. BERNARD LAUWERYS, MD, PhD
• Service de Rhumatologie, SSS/IREC/RUMA, Cliniques Universitaires Saint Luc & Université Catholique de Louvain

11
Overview
1 2
3 4
CORPORATE HIGHLIGHTS CLINICAL AND PRECLINICAL PROGRAMS
APPENDIX FINANCIALS AND WRAP UP

12
2015 2016 2017 2018
IFNα-Kinoid : Planned clinical studies
IFNα-Kinoid Phase IIb in lupus: EU, Asia and Latin America • Objectives: biomarkers and clinical efficacy • N = ~160; IFNα-Kinoid versus Placebo; Double-blind, Randomized • FPI: Q2/3 2015 – Results 1Q-2017
STRONG CLINICAL PORTFOLIO WITH IFNα-KINOID
IFNα-Kinoid program in Dermatomyositis ODD EU-USA: Request 2Q-2015, Designation 4Q-2015
1. Phase IIa – Adults - EU: FPI 4Q-2015, Results 1Q-2017, N = 15 pts
2. Phase IIb – Adults – EU-USA-Asia: FPI 2Q-2017, Results 1Q-2019, N = 60-80 pts
3. Phase IIa/b – Pediatrics – EU-USA: FPI 3Q-2016, Results 3Q-2018, N = 40-50 pts
IFNα-Kinoid Phase IIa in lupus: USA • Objectives: Safety, Dose, Immunogenicity • N = 60; IFNα-Kinoid 60-240 µcg • FPI: Q1 2016 ; Results: 3Q-2017
Note : estimated development plan pending regulatory approvals

13
Preclinical pipeline
ONE CLINICAL STUDIES TO BEGIN IN 2015/2016, OTHER TRIALS UNDER EVALUATION FOR MID-TERM LAUNCH
Preclinical Phase I Phase II Phase III
VEGF-Kinoid in AMD
VEGF-Kinoid in solid tumors
IL-4 / IL-13 Kinoid in allergies
Study design under evaluation
TNF-Kinoid in RA and Crohn’s Disease
Most advanced program to launch in 2015/2016

14
Systemic Lupus Erythematosus (SLE) or Lupus
A chronic auto-immune disease:
– Auto-antibodies
– Fluctuating disease course: relapses-remissions
– Can affect all organs (skin, kidneys, liver, heart)
– Accumulations of manifestations over time
– Increased mortality
Population:
– Young women: 15-40 Y, F:M ratio: 6-10:1
– Blacks>Asians/Hispanics>Caucasians
No curative therapy
– Largely undiagnosed
Prevalence:
– 0.05% of the general population
– USA: 500,000 (CDC) to 1.5 million (Lupus Foundation of America)
– Europe: 500,000
Source: adapted from Houssiau F 2008
Arthritis 84%
Serositis 36%
Nephritis 39%
Immune thrombocytopenia 5%
CNS inflammation 10%
Malar rash 58 % Photosensitivity 45%

15
IFNα-Kinoid And The Market For SLE
MARKET THAT HAS LITTLE COMPETITION AND SIZEABLE GROWTH PROSPECTS
Source: 1 FDA / 2 Datamonitor Report on Benlysta 2014
Million dollars
Significant market
– US$ 3.5 billion estimate (2010)
– 18% CAGR potential by 2019
– GSK $3.6 bn takeover of HGS (Benlysta)
An unmet medical need
– Benlysta (HGS/GSK), first new drug in 50 years
– FDA: “marginal efficacy”1
– cost: 30 540 US$ per patient per year2
Market for lupus therapies 2010 vs. 2019
0
500
1 000
1 500
2 000
2 500
3 000
3 500
2010 2019
Generic & Offlabel Novel
Source: Datamonitor 2011

16
Clinical Advisory Board November 2014 Boston, MA
Pr. BERNARD LAUWERYS, MD, PhD
• Service de Rhumatologie, SSS/IREC/RUMA, Cliniques Universitaires Saint Luc & Université Catholique de Louvain, Brussels
Pr. FRÉDÉRIC HOUSSIAU, MD
• Chief of Rheumatology Unit, SSS/IREC/RUMA, Cliniques Universitaires Saint Luc & Université Catholique de Louvain, Brussels
Pr. ERIC HACHULLA, MD
• Professor and clinical expert Centre Hospitalier
Universitaire de Lille; Centre de Référence des
Maladies Auto-immunes et Systémiques rares,
France
Pr. KIRYAKOS KIROU, MD, DSc, FACP
• Mary Kirkland Center for Lupus Research, New-York
• Director, Lupus Nephritis Program, Hospital for Special Surgery, New-York
Pr. JOAN MERRILL, MD
• , Professor of Medicine, Adjunct Professor, Oklahoma Medical Research Foundation; School of Pharmacy University of Oklahoma Health Sciences Center
• Medical Director of the Lupus Foundation of America, and member of the Systemic Lupus International Collaborating Clinics
Pr. VIBEKE STRAND, MD, FACP, FACR
• Clinical Professor, Adjunct, Division of Immunology
and Rheumatology of the clinical faculty at Stanford
University,
• Consultant in clinical research and regulatory affairs
Pr. RONALD VAN VOLLENHOVEN, MD
• Chief of the Unit for Clinical Therapy Research,
Inflammatory Diseases (ClinTRID) at the Karolinska
Institute, and of the Clinical Trials Unit Rheumatology
at the Karolinska University Hospital, Stockholm

17
IFNα-Kinoid: Development Strategy
Preclinical studies of IFNα-Kinoid in lupus
Establish POC in mouse model
Toxicology in rabbits & monkeys up to 400mcg x5: no safety issue
No T cell response to IFNα
No cross-reactivity to IFNβ,γ, ω: preserved anti viral defences
2005 – 2009
Phase I/II study of IFNα-Kinoid in lupus: established POC in SLE patients
N = 28 SLE patients
Completed
2010 – 2011
Phase IIb study of IFNα-Kinoid in lupus in Europe, Latin-America and Asia
Preparation ongoing
Study expected to launch mid 2015
2015 – 2016
2016 – 2017 Phase IIa study of IFNα-Kinoid in lupus in the US
Preparation ongoing
Study expected to launch early 2016

18
IFNα-Kinoid Phase I/II Study Systemic Lupus Erythematosus (Lupus)
4 doses tested: Kinoid 30/60/120/240 mcg by intramuscular injection
3 injections, days 0-7-28
4th dose at week 12 for 50% of patients
Multicenter, Double blind, placebo controlled clinical trial, randomized 3:1
28 patients with moderate disease
Safety and tolerability
Immunogenicity
Evolution of biomarkers
Clinical Response
Evaluation criteria
The IFNα-Kinoid induces an immune response against IFNα in 100% of patients, with strong dose impact
Dose related and potent neutralisation of IFNα gene signature
Excellent safety profile
Results presented in November 2011 at the Conference of the American College for Rheumatology and published in Arthritis & Rheumatism 2013

19
IFNα-Kinoid in Systemic Lupus Erythematosus (Lupus)
IFN-Kinoid Induction of high
levels of anti-IFNα
antibodies: dose dependent
AND Neutralizing Antibodies
Anti-IFNα antibodies
Neutralizing antibodies
An
ti-I
FN
an
tib
od
y G
MT
100
1000
10000
100000
0 50 100 150 200 250 300 350
35000 Dil-1
1000
10000
NC
50
(ge
om
etr
ic m
ean
)
60 mcg IFN-K 120 mcg IFN-K 240 mcg IFN-K Placebo

20
IFNα-Kinoid in Systemic Lupus Erythematosus (Lupus)
THE POLYCLONAL ANTIBODY RESPONSE STRONGLY
NEUTRALISES ALL IFNα SUBTYPES
Neutralizing polyclonal anti-IFNα antibodies
IFNα
IFNα
IFNα
NEUTRALISATION STRONG
NEUTRALISATION WEAK
NO NEUTRALISATION
IFNα subtypes (10 U/mL)
Polyclonal antibodies from IFN-K vaccinated lupus patient (Dilution)
Monoclonal antibody anti-IFNa (concentration ng/mL)
A 2a 1/22475 <7.8
B2 1/8936 98
C 1/8857 >1000
D 1/9648 >1000
F 1/2493 329
G 1/10693 78
H2 1/9147 57
I 1/13354 >1000
J1 1/5270 >1000
K 1/16878 >1000
4b 1/10154 >1000
WA 1/10148 945
A 2b 1/22326 <7.8
Neutralized subtypes 13/13
+++
2/13: +++
5/13: +/-

21
IFNα-Kinoid in Systemic Lupus Erythematosus (Lupus)
HIGH IFNα SIGNATURE
LOW IFNα SIGNATURE
Healthy
Monoclonal Ab (ROSE)
Polyclonal Ab (Phase I-II IFN-Kinoid)
MAb: Clinical Efficacy
MAb: No clinical efficacy
IFNα-Kinoid: complete neutralisation of IFNα signature
POLYCLONAL ANTIBODIES NEUTRALIZE BETTER THE IFNα GENE SIGNATURE THAN MONOCLONAL ANTIBODIES, EVEN FOR SEVERE FORMS OF LUPUS

22
IFNα-Kinoid in Systemic Lupus Erythematosus (SLE)
Polyclonal neutralizing anti-IFNα antibodies
IFNα
IFNα
IFNα
IN CONCLUSION: • Very strong antibody response (40x>TNF-Kinoid)
• Strong response neutralizing antibodies
• Those antibodies neutralize all 13 subtypes of IFNα, in contrast with monoclonal anti-IFNα antibodies (2 subtypes only are completely neutralized) • Higher production of binding and neutralizing antibodies in patients with more severe lupus • Improvement of disease biomarkers is correlated with the intensity and duration of the neutralizing response

23
Comparison between TNF-Kinoid and IFNα-Kinoid: two different products
100
5100
10100
15100
20100
25100
30100
35100
40100
0 20 40 60 80 100 120 140 160 180
Mo
yen
ne
gé
om
étr
iqu
e d
es
titr
es
(Dil
-1)
Study Day
TNF-K-006540µg; 5 inj.
TNF-K-003360µg; 3 inj.
TNF-K-003360µg; 2 inj.
TNF-K-003180µg; 3 inj.
IFN-K-001240µg
Comparison of antibody levels induced by TNF-Kinoid in RA And by IFNα-Kinoid in Lupus
SIGNIFICANT SUPERIORITY OF IFNα-KINOID IN TERMS OF ANTIBODY RESPONSE AND NEUTRALIZING ACTIVITY
IFN-K
TNF-K

24
Lessons Learned from TNF-Kinoid Studies for IFNα-Kinoid Program
- IFNα animal model relevant - Much higher anti-IFNα antibody response: 20x higher than TNF-K - Neutralizing antibodies, dose dependent, in human - Neutralization of 13 subtypes of IFNα vs 2-7 with Mabs - Neutralization of IFN gene signature - Correlation between antibody levels and neutralization of IFN gene signature
TNF-KINOID STUDY RESULTS DO NOT PREDICT OUTCOME FOR IFNα-KINOID STUDY
Learning curve on active immunotherapy
- Good safety and tolerability of the product (5 clinical trials to date) - Highest antibody response obtained at highest dose + boost (TNF-K-003, 005 and IFN-K-001) - Possible interference of Kinoid with residual antibodies (TNF-K-005) - Neutralizing antibodies necessary to obtain clinical response ; simple presence of binding
antibodies not sufficient (TNF-K-006)

25
Programs of Preclinical Development
VEGF-Kinoid in Age-related Macular Degeneration (AMD)
– Very encouraging results had been obtained with a preliminary VEGF Kinoid
– Prevention of laser induced neo vascularization in mice
– Results presented at EVER conference in 20093
VEGF-Kinoid in solid tumors
– Very encouraging results had been obtained with a preliminary VEGF Kinoid
IL-4 / IL-13 -Kinoid in allergies
– Preliminary studies indicate the potential to control allergic reactions thanks to a Kinoid targeting IL-44.
Note : 1Gringeri, 1999 2Teijaro et al. 2013 ; Wilson et al. 2013, 3 European Association for Vision and Eye Research (EVER) 2009, September 30-October 3, Portoroz, Slovenia. Abstract 4352 4 Le Buanec, 2007

Preclinical POC with VEGF-Kinoid: In Vivo Qualitatives Analyses of CNV
D 6
140 ‘’
40 ‘’ 150 ‘’
50 ‘’
D 13
Placebo VEGF-Kinoid
IMMUNIZATION WITH VEGF-KINOID REDUCES LASER INDUCED CHOROID NEOVASCULARISATONS
European Association for Vision and Eye Research (EVER) 2009, September 30-October 3, Po

27
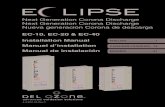
VEGF-Kinoid in Tumor Growth Inhibition
Tu
mo
r vo
lum
e (c
m3)
0
0,5
1
1,5
2
D 21 D28 D 35 D42
bevacizumab + Paclitaxel
PBS
Anti-VEGF IgGs + Paclitaxel
Ab-induced inhibition of tumor growth in xenografted immunodeficient mice. Effect of anti-VEGF IgGs (8 mg/kg) combined with paclitaxel (10 mg/kg) on HT29 tumor growth in NOD/SCID mice (2 × 105 cells; 10 mice per group, compared with effect of bevacizumab (5 mg/kg) combined with paclitaxel (10 mg/kg).
Proc Natl Acad Sci U S A. 2007 Feb 20;104(8):2837-42. Epub 2007 Feb 14. VEGF kinoid vaccine, a therapeutic approach against tumor angiogenesis and metastases. Rad FH, Le Buanec H, Paturance S, Larcier P, Genne P, Ryffel B, Bensussan A, Bizzini B, Gallo RC, Zagury D, Uzan G.
Abstract Tumor growth depends on blood supply, requiring the development of new vessels, and vascular endothelial growth factor (VEGF) plays a central role in neoangiogenic processes. For this reason, VEGF represents a target for the development of new therapeutic antiangiogenic molecules. Clinical trials using anti-VEGF mAbs such as bevacizumab have validated the efficacy of this therapeutic approach but have also revealed adverse effects. Here we report that a VEGF-derived immunogen, consisting of a heterocomplex of a murine (m)VEGF and keyhole limpet hemocyanin, called "mVEGF kinoid," triggered a strong Ab immune response in mice. The anti-VEGF Abs inhibited both the proliferation of human umbilical vein endothelial cells cultured in the presence of mVEGF and the binding of mVEGF to its receptor-2 Flk-1. In mVEGF kinoid-immunized BALB/c mice challenged with syngeneic CT26 colorectal tumor cells, the number and size of lung metastases were significantly decreased. In human (h)VEGF kinoid-immunized BALB/c mice, high levels of serum Abs to hVEGF were present, and purified IgG from these mice decreased by > or =50% the tumor growth of human A673 rhabdomyosarcoma cells and HT29 colon carcinoma xenografted in Swiss nude and NOD/SCID mice, respectively. Tumor cell growth inhibition was similar to that observed in mice receiving therapeutic doses of bevacizumab. These experiments suggest that a therapeutic vaccine containing VEGF kinoid may represent a strategy for safely combating VEGF-dependent neovascularization and metastases occurring in malignant tumors.

28
Overview
1 2
3 4
CORPORATE HIGHLIGHTS CLINICAL AND PRECLINICAL PROGRAMS
APPENDIX FINANCIALS AND WRAP UP

29
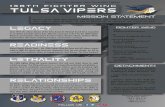
Shareholding structure and Stock information
NYSE Alternext Paris
ISIN code: FR0004032746
1.20 € (Closing January 30, 2015)
– Market cap: 28 M€
– Average Vol.: 748K shares / per day
– Number of shares outstanding: 23,006,310
7%
5%
77%
5% 3% 2%
Truffle Capital
Novartis Venture Fund
Free Float
OTC AM
Other historical investors
Founders
SHAREHOLDERS December 2014
Date Reco. Target price Upside
Kepler L. Labourdette 12/16/14 Reduce 1,80 € 55%
Invest Sec. M. Descoutures 01/05/15 Reduce 1,80 € 55%
CIC A Guekam 12/16/14 Sell 2,10 € 81%
Portzamparc A Guerin 27/02/15 Reduce 1,00 € -14%
Alpha Value A Moulin 01/11/15 Buy 1,71 € 47%
Edison J. Savin 07/11/14 - 1,70 € 47%
Consensus 01/23/15 1,69 € 45%

30
Financing
Cash and cash equivalents as of 12/31/2014: €5.6 million
Equity line arranged with Kepler Cheuvreux: up to €20 million in financing available
– 1st tranche : up to €7 million over the next 12 months (~9.9% of capital)
– 2nd and 3rd tranches : 2* €6.5 million from November 2015 onwards and over 18 months – to be drawn down only if needed
Other resources
– French Research Tax Credit – Q2 2015
– Possible Grants and subsidies (BPI submission April)
COMPANY FINANCING INSURED FOR 2015

31
An experienced management team
MIGUEL SIELER Chief Executive Officer
• 32 years of an international career for Bayer, in 1998 he became Chairman and C.E.O of the Bayer Group in France until his retirement in 2008.
• Member of the board of Nexity S.A, Stratoz, Plasmaprime and Abivax, a biotech company focused on the development of innovative vaccines and antivirals.
• Master of Law from the University of Tubingen, Germany and graduated from the Institut d’Etudes Politiques de Paris, France.
BERNARD FANGET Vice President Pharmaceutical Development
• Bernard joined Neovacs in 2005, he was previously Senior Vice President, Pharmaceutical Development, of Flamel Technologies and Prior to Flamel was Corporate Vice President, Global Industrialization, at Sanofi Pasteur.
• Degree in biological chemistry from the University of Lyon, France.
OLIVIER DHELLIN Director of Pharmaceutical Development
• Olivier joined Neovacs in 2005. He previously held positions at Anosys (a US/French cell therapy biotech company), and research activities for 7 years at Gustave Roussy Institute (molecular biology and genomics) and Pasteur Institute where he was a post-doctorate fellow in molecular pharmacology. He had previously spent 4 years as a resident in several hospital departments (pediatrics, pharmacology and biochemistry).
• Degree in Pharmacy (Paris XI University, France) and a PhD in Virology (Pierre et Marie Curie University, France).
PIERRE VANDEPAPELIÈRE Chief Medical Officer
• Pierre joined Neovacs in June 2008 after 18 years as Head of Clinical Research and Early Development at GlaxoSmithKline Biologicals in charge of the clinical evaluation of early phase project. Prior to GSK Biologicals, Pierre was at ICI Pharmaceuticals from 1987 to 1990, working on cardiovascular products.
• Medical Doctorate from the Universities of Namur and Louvain-Brussels, a Postgraduate Diploma in Tropical Medicine from the Institute of Tropical Medicine of Antwerp and a PhD in Biomedical Medicine from the University of Ghent.
GERALDINE GROUARD-VOGEL Head of Research and Preclinical Development
• Géraldine joined Neovacs in 2005. She previously worked at Sanofi-Pasteur USA in bacterial vaccine development and as a researcher at the Walter Reed Army Institute of Research at the Seattle University.
• Degree in Pharmacy from Angers University (France) and did her PhD in Immunology with Dr Jacques Banchereau at Schering-Plough Lyon (France).
• She has authored several scientific publications in peer-reviewed journals.
NATHALIE THOMAS-PUJOL Head of Regulatory Affairs
• Nathalie joins Neovacs in 2014 after more than 20 years in the pharmaceutical industry in regulatory affairs and clinical research, such as head of Regulatory Affairs EMEA at Cephalon/Teva. Previously, she worked for 15 years at Sanofi-Aventis R&D.
• Pharmacist Doctorate from the University of Rouen in France and a PhD in toxicology from the University of Paris VII in France.

32
Thank you & Contact
Nathalie TREPO IR manager 3/5 impasse Reille 75014 Paris Tel: +33-153-109-314 [email protected]
Do not hesitate to contact us
Press - IR – U.S. - The Ruth Group Melanie Sollid-Penton Tel.: +1.646.536.7023 [email protected]