Avalanches III. Dry Flowing Avalanche Avalanche Impact Forces.

The Newsletter — www.gapna.org 1
Spring 2013 Volume 32, Number 1
President’sMessage
IN THIS ISSUEPreserving GAPNA’s History . . . . 2
How to Write an Abstract. . . . . . . 4
GAPNA Joins LACE APRNNetwork . . . . . . . . . . . . . . . . . . . . . 5
More Conference Photo Highlights . . . . . . . . . . . . . . . . . . 6-7
Chicago Welcomes GAPNA. . . . . 8
Clinical Research Corner . . . . . . . 9
New GNP Student Scholarship. . 11
NewsletterThe Official Newsletter of the Gerontological Advanced Practice Nurses Association — Founded in 1981
Call for Nominations,Excellence Awards,and Abstracts2013 GAPNA Election
The Call for Nominations for the2013 GAPNA Election is now avail-able. GAPNA is currently seeking nom-inations for President-Elect, Treasurer,Director-at-Large, and two NominatingCommittee members. Nominationforms can be found on the GAPNAweb site by clicking “About GAPNA,”then “Board of Directors,” then “Callfor Nominations.” Nomination packetsand consent statements are due byApril 1, 2013. See page 2 for moreinformation.
Excellence AwardsGAPNA strives to promote excel-
lence in gerontology practice and inthe care of the older adult. GAPNAmembers will be recognized for theiroutstanding contributions during theassociation’s 32nd Annual Conferencein Chicago. Individuals will be recog-nized for the following awards:
• Excellence in Clinical Practice• Excellence in Community
Service• Excellence in Leadership• Excellence in Education• Excellence in Research
Nominations are due by June 1,2013. For a more detailed descriptionof each award, see page 3.
Join the Conversation on GAPNA’s Facebook PageFacebook is the most visited web site both nationally and globally, second only to
Google, according to web data company Alexa’s annual list of the world’s 500 mostpopular sites. Second only to a search engine! That is one incredible statistic.
Facebook is a powerful tool for connecting with others, sharing information andopinions, and so much more. We encourage you to be a part of the growing numberof GAPNA members, nurses, and fans and join in on the conversation on the GAPNAFacebook page (facebook.com/GAPNA). continued on page 11
Share the Wealth of Knowledge
T raditionally at the beginning of a new year, one extendswishes for happiness as a common greeting, and on
behalf of the GAPNA Board of Directors, let me extendwishes for happiness in 2013 to you and those close to you.While we view the new year as a clean slate, a chance tostart over, we always seem to bring at least some of our bag-gage from the past year along with us – whether it is that fewextra pounds we want to lose, a commitment to be moreorganized, or a promise to take more time for ourselves. Thesame can be said of many of our country’s institutions. Withthe dropping of the ball at midnight on December 31, wewere tossed over a “fiscal cliff.” Congress continues to kickthe can on the debt ceiling and despite the fact that expertspredict an avalanche of older adults as baby boomers age,we still don’t have a health care system ready to handle the onslaught. As advancedpractice nurses who care for older adults, we are well aware that the perfect storm ofan inadequately prepared workforce, a dramatic increase of older patients in need ofcare, and a health care reimbursement system based on service provision instead ofprevention is likely to make us all the most fully employable group of our generation.
continued on page 5
Marianne Shaughnessy

2 The Newsletter — www.gapna.org • Spring 2013, Volume 32, Number 1
The Call for Nominations for the2013 GAPNA Election is now avail-
able. GAPNA is currently seeking nomi-nations for President-Elect, Treasurer,Director-at-Large, and two NominatingCommittee members. Nomination formscan be found on the GAPNA web site byclicking “About GAPNA,” then “Board ofDirectors,” then “Call for Nominations.”Nomination packets and consent state-ments are due by April 1, 2013.
Please consider volunteering yourleadership and talent for these importantroles!
President-ElectThe President-Elect serves as a mem-
ber of the Board of Directors and per-forms the following functions: performsduties as assigned by the President; auto-matically assumes the office of Presidentat the end of the President’s term or inthe event of a vacancy in the office ofPresident; develops a thorough under-standing of the bylaws and policies ofthe Society, and Robert’s Rules of Order,Newly Revised; works closely with thePresident; develops and prepares goalsfor upcoming term as President; estab-lishes contact with the National Officestaff for the operation of the Association;recognizes and advises of changing out-side influences which may affect the
decisions of the Board; participates inthe development and implementation ofthe strategic plan; contributes articles tonewsletter as required; and completesother duties as assigned. Travel isrequired and expenses are reimbursed asset by GAPNA policy. (Three-year com-mitment: first year as President-Elect,second year as President, and third yearas Immediate Past President)
TreasurerThe Treasurer serves as a member of
the Board of Directors and performs thefollowing functions: works with account-ant and National Office; works directlywith committee liaison for HistoricalCommittee; maintains and/or reviewsthe financial records of the organization;presents financial record to the Board ateach Board and Annual Meeting; pro-poses draft budget to the ExecutiveBoard at the Winter Meeting; and isresponsible for coordinating and assist-ing with resource development for theorganization. Travel is required andexpenses are reimbursed as set byGAPNA policy. (Two-year commitment)
Director-at-LargeThe GAPNA Director-at-Large serves
as a member of the Board of Directorsand performs the following functions:
assumes responsibilities delegated by thePresident and/or Board; participates inthe development and implementation ofthe strategic plan; contributes articles tonewsletter as required; assists to orientthe incoming Director-at-Large; andcompletes other duties as assigned. Travelis required and expenses are reimbursedas set by GAPNA policy. (Two-year com-mitment)
Nominating CommitteeMember (two positions)
The Nominating Committee over-sees the elections process, solicits andscreens applicants, and presents a slateof candidates to the membership for vot-ing. The business of the NominatingCommittee is conducted via conferencecalls; travel is not required. NominatingCommittee members may not run foroffice whilst serving on the NominatingCommittee. (The candidate receiving themost number of votes shall serve for twoyears, the second year of the term asChair of the Committee. The candidatereceiving the second most votes willserve a one-year term.)
Candace Harrington, DNP, ANP-BC,GNP-BC
Nominating Committee [email protected]
Call for Nominations: Share Your Talents and Leadership
Don’t Let GAPNA’s History Get Swept Away!GAPNA’s Historical Committee is committed to preserving the history of our
organization. Send us your stories so they may be saved for years to come. Manyplaces in our country get hit with storms and we often don’t think about our mem-ories and pictures getting lost. Help the Historical Committee collect your mem-ories in a story format to be documented and protected.
Here are a few questions to think about for your submission. • How did you get involved in GAPNA? When did you attend your first chapter
meeting or national convention? Describe your experiences.• How has GAPNA helped you professionally/socially?• What has been your level of involvement in GAPNA, either direct or indirect?• What has being a member meant to you?• Do you have any amusing or inspiring stories related to our membership?• What frustrations or controversies have you experienced? • What keeps you involved in GAPNA?
We will be reviewing the stories and deciding how to compile them, somefor the archives and some for newsletter, etc. We will ask for permission to reprintif we use your story.
Please send all submissions to Pat Hess at [email protected]
Stacey O’Brien Eadie, CRNPHistorical Committee
Looking for PharmacologyHours? Check Out OurOnline Library!
GAPNA has developed “Pharmaco -therapeutics: Lipid Lowering Agents inthe Gerontology Population,” a new, two-part series available in GAPNA’s OnlineLibrary. Part I reviews the current researchand the guidelines on cholesterol man-agement while Part II covers medicationsand implications for the gerontologicadvanced practice nurse. This series offersover 2 hours of pharmacology credit! Visitwww.prolibraries.com/gapna to purchasethese sessions.

The Newsletter — www.gapna.org • Spring 2013, Volume 32, Number 1 3
GAPNA strives to promote excel-lence in gerontology practice and in thecare of the older adult. This excellence isachieved by members who excel indi-vidually and collectively in improvingpractice through education, research,leadership, and community service.Each year, GAPNA recognizes our mem-bers who have gone above and beyondsupporting the mission and vision of theorganization. GAPNA invites you to sub-mit a nomination for one of the follow-ing awards by June 1, 2013. For nomina-tion forms, visit the “About GAPNA” sec-tion at www.gapna.org
Nominations are peer reviewed andselected based on established criteria inachieving excellence. GAPNA will hostan Awards Dinner Friday, September 20,2013 at the Sheraton Chicago Hotel andTowers in Chicago, IL, during the 32ndAnnual Conference to recognize the out-standing contributions of GAPNA mem-bers. Individuals will be recognized forthe following awards:
Excellence in Clinical PracticeThis award for outstanding clinical
practice is presented to an individualwho demonstrates a commitment togeriatric clinical practice. This award rec-ognizes an individual who demonstrates,through the use of geriatric principles,outstanding geriatric care that goes wellbeyond the traditional service role of theprofession. The award highlights clinicalpractice as an important element of themission of nursing professionals and sin-gles out individuals who serve as exam-ples of geriatric expertise.
Excellence in CommunityService
This award for outstanding communi-ty service acknowledges an individualwho demonstrates a commitment to serv-ice to the community. This commitment isdemonstrated through the developmentor participation in programs that go wellbeyond the traditional service role of theprofession. The award highlights commu-nity service as an important element ofthe mission of nursing professionals andsingles out individuals who serve asexamples of social responsiveness on thepart of the nursing community.
Excellence LeadershipThis award for outstanding leader-
ship identifies an individual who demon-strates a commitment to geriatrics;
through direct care, education, and/orresearch. This award recognizes an indi-vidual who demonstrates the tenacity toadvocate, through a variety of means, forgeriatric education and care in a varietyof settings that goes well beyond the tra-ditional service role of the profession.The award highlights leadership as animportant element of the mission ofnursing professionals and singles outindividuals who serve as examples ofgeriatric expertise.
Excellence in EducationThe Award for Excellence in
Education recognizes an individualinvolved in the teaching and/or design ofgerontological nurse practitioner cur-riculum or course content. The facultymember demonstrates knowledge of thecare of older adults and the ability totranslate that knowledge to enhance stu-dents’ understanding in innovative ways.The faculty member encourages andinspires advanced practice students todevelop their excellence in gerontology.In addition to excellence in teaching, thefaculty member exhibits excellence inpractice and service to the community.
Excellence in ResearchThis award for research identifies an
individual who demonstrates a commit-ment to research in nursing that benefitsthe geriatric community. This commit-ment is demonstrated through the devel-opment or participation in research proj-ects that emphasize or go beyond the tra-ditional service role of the profession. The
award highlights research as an importantelement of the mission of nursing profes-sionals and singles out individuals whoserve as examples of nursing scientistswithin the nursing community.
Chapter Excellence AwardThe Chapter Excellence Award hon-
ors a chapter that best promotes thegoals of the Gerontological AdvancedPractice Nurses Association through itsmember relationships, professionalactivities, and promotion of advancedpractice gerontological nursing through-out the local, regional, and/or state dur-ing the past year. The winning chapterwill be awarded $250.
Special Interest GroupExcellence Award
The Special Interest Group Excel lenceAward honors a SIG that best promotes thegoals of GAPNA through its memberinvolvement, professional activities, andpromotion of advanced practice geronto-logical nursing during the past year. Theaward recognizes a SIG that promotesengagement of members in the area ofspecial interest and in the advancement ofgerontological nursing practice.
GAPNA invites you to submit a nom-ination by June 1, 2013. Nominationforms are available at www.gapna.org
George Byron Smith, DNP, ARNP,GNP-BC, NP-C, CNE
Awards Committee [email protected]
Help for LGBT EldersDo you need help working with
your LGBT elders? Are there issuesthey have that you do not understand?Do you know that when one partnerof a LGBT couple dies, the other is notentitled to the social security and ben-efits of a married couple, and thesurving partner may be at risk offinancial difficulties, including losinghis/her home as a result?
Please send your questions andconcerns to GAPNA’s LGBT FocusGroup. We would love to be of help.
Trudy Keltz, RN, [email protected]
Colleen Wojciechowski, MSN, [email protected]
GAPNA Recognizes Excellence: Award Nominations Sought
Call for Abstractscontinued from page 1
Research and Clinical ProjectAbstracts
The GAPNA Research Committee isaccepting research project and clinicalproject abstracts for presentation at the2013 GAPNA Annual Conference.Projects should enrich the advancedpractice nurse’s knowledge and/orenhance the care of the older adult.Abstracts must be received by May 15,2013. Visit www.gapna.org for detailsand online submission form.

4 The Newsletter — www.gapna.org • Spring 2013, Volume 32, Number 1
Advanced practice nurses (APNs) working with older adultshave the potential to significantly impact care and become
innovators of the future. They bring novel and fresh ideas to existingpractice, devise different ways to approach problems, and pioneernew models of care. APNs can improve patient care and the quali-ty of this care while in certain situations reducing health care costs(Lopez-Bushnell, 2002). APNs contribute to the development ofnew knowledge and the science of nursing. And, APNs have theobligation to share their knowledge and expertise to advance careby sharing with others who may benefit from this expertise.
Particular areas where APNs can impact care include evaluatingthe association between treatment of symptoms and outcomes;increasing the evidence base for treatment of health issues; under-standing psychological well-being, spiritual well-being, and quality oflife of patients; re-evaluating service delivery; and creating innovativemodels of care. There are special needs, particularly in geriatrics, inthe areas of caregiver burden, the adaptation for palliative care of theolder adult, and health disparities in minority elders as well as a vari-ety of other issues related to the older population. However, practic-ing APNs rarely share their expertise by presenting, publishing, or par-ticipating in research due to a number of reasons from a hectic workschedule to lack of knowledge on presenting or publishing as well asfear or intimidation. It is imperative APNs assist in increasing nursingknowledge and sharing their expertise.
Creating an AbstractCreating an abstract is the first step toward sharing nursing
expertise. Attention should be paid to developing an abstract thatconveys your knowledge and passion while being concise. Keyinformation should be included in the abstract:
• Who the problem affects or what is the issue. Briefly explainthe problem, the rationale for a different way of treating, or theimportance of a different model of care.
• Why it is important. Familiarize the reader with the back-ground and set up the problem or issue.
• Where and when. Where the solution will take place (type ofsetting), and when this will occur.
• How. The solution, different method of care, or new model ofcare; essentially the project or idea.
• Findings or results. Share what was learned.• Finally, So what. This is the best part. Share how this idea will
impact and/or improve care. Bring it home. This is your timeto say your thoughts. Speak passionately to convey your mes-sage, and deliver the punch.
Writing an abstract is an easy and efficient way of sharing ideas,solutions to problems, research findings, or models of care. Whenwriting an abstract, decide the intent or audience of reviewer/editorand speak in the language usually accepted by that party. Optionsto share knowledge or expertise include publishing or presenting,either verbally/orally or as a poster. Remember to submit accordingto the guidelines provided. Remember to submit in a timely manneraccording to the prescribed deadline and be ready to answer ques-tions from the reviewers by providing contact information. The onlyway to add to the body of nursing science and improve care is bysharing your expertise. So get out there! Publish, present, and shareyour expertise.
Hints for SuccessRead and follow the directions. Know what the
reviewers want you to submit and how, including style forreferences (American Psychiatric Association vs.American Medical Association). Pay attention to maxi-mum word count (use word count feature to check).
• Spell and grammar check. Read before submitting.Avoid run-on sentences and do not assume the read-er knows what you mean. Avoid the use of jargon.
• Avoid abbreviations and acronyms or provide thefull name first then put abbreviations in parenthesis,e.g., advanced practice nurse (APN).
• Begin with an idea or problem statement which getsthe reviewer’s attention and draws interest for theperson to continue reading.
• Keep focused on the main message and avoid ram-bling.
• Have someone else read it and listen to any criti-cisms to improve the abstract.
• Review well-written abstracts or abstracts acceptedfrom the previous call for abstracts.
• Avoid tables, charts, and citations unless crucial(Marimaldi, Berkman, Coleman, & Strumpf, 2008;Shaugh nessy, 2009).
Remember, your first abstract may not be accepted,but learn from any criticisms to improve your submissions.Persistence will pay off. Good luck and just do it!
Lisa Byrd, PhD, FNP-BC, GNP-BCGerontologist
ReferencesLopez-Bushnell, K. (2002). Get research-ready. Nursing Management,
33(11), 41-44.Marimaldi, P., Berkman, B., Coleman, E., & Strumpf, N. (2008). How do
I write a strong abstract? Retrieved from http://bandwidthonline.org/howdoi/write_strong_abstract.asp
Shaughnessy, M. (2009). Abstracts that score. Geriatric Nursing, 30(2),140-143.
Publish, Present, and Share Expertise asan Advanced Practice Nurse Expert: How to Write an Abstract

The Newsletter — www.gapna.org • Spring 2013, Volume 32, Number 1 5
GAPNA Joins LACE APRN Network
The Consensus Model forAdvanced Practice Regis -
tered Nursing (APRN) Regula -tion: Licensure, Accreditation,Certification, and Education(LACE) has changed the waynurse practitioners caring forolder adults are educated and certified and soon it will changethe way we are licensed. Schools of nursing need to meet thenew adult-gerontology competencies for accreditation. Thesefour aspects of regulation of APRN practice are referred to asLACE. The LACE APRN Network was formed to facilitate imple-mentation of the Consensus Model and is not the same as theConsensus Model. LACE provides a mechanism for communi-cating about APRN regulatory issues, facilitating implementa-tion of the APRN Consensus Model, and involving all stake-holders in advancing APRN regulation. While many groups par-ticipated in developing the model, not all have continued asmembers of the LACE Network. GAPNA was not at the tablewhen the Consensus Model was created, but the leadership haslobbied hard to be included in the LACE APRN Network. InAugust 2012, the Network voted to add GAPNA to the mem-bership. Nikki Davis, Evelyn Duffy, and Laurie Kennedy-Malone were appointed by GAPNA as representatives to LACE.The inclusion of GAPNA in LACE couldn’t have come at a bet-ter time as the Network is discussing the development of guide-lines for grandfathering. (For the most part, family nurse practi-tioners will not be affected.)
The Network meets each month via conference call, and aspecial face-to-face meeting was held to discuss grandfatheringof APRNs. The meeting in Chicago was called by the NationalCouncil State Boards of Nursing. Grandfathering is especiallyimportant to the GAPNA membership because many are certi-fied as ANPs or GNPs, populations that are to be replaced bythe new A-GNP group. Relicensure in a state in which an NP iscurrently practicing is a concern, but the greatest concern is theNP who relocates to a state in which she/he has not beenlicensed, when endorsement is necessary. The documentaddressed at the face-to-face meeting encouraged boards ofnursing to follow the consensus guidelines for all new APRNsfor licensure and for those being licensed by endorsement toaccept any APRN who held a current license that was unen-cumbered. Additional guidance was also included regardingendorsement for those who did not fit a population under theConsensus Document.
The GAPNA LACE representatives who attended the meet-ing, Evelyn and Nikki, where grateful for the opportunity topresent data collected from our membership regarding prob-lems experienced with licensure in the clinical and/or facultysetting. GAPNA’s representatives contributed that informationand helped edit portions of the document that had the potentialto be problematic especially to our GNP membership. Ourattendance at the meeting increased awareness of the knowl-edge and experience GAPNA brings to the discussion going for-ward. The document is not complete. When approved by theNetwork, it will be published on the public side of the LACEAPRN Network web page.
Evelyn Duffy, DNP, GNP/ANP-BC, [email protected]
President’s Messagecontinued from page 1
The implementation of the Consensus Model that mergesadult and gerontologic nursing into one population focusaddresses, in part, the workforce component of the problem,but is by no means a total fix. Sharing the unique body ofknowledge and experience developed from years of studyingand caring for older adults is the only way we can prepare ourcolleagues for the challenges that await us down the road as anation. This responsibility belongs to all of us. GAPNA’sCommittees and Special Interest Groups have been hard atwork this year developing informational and educational prod-ucts to enhance clinical practice, guiding us as teachers to thenext generation, keeping us informed about legislation likely toimpact our practices and our patients, preserving our past, andmapping our future. Every educational product, service, orevent we produce has the potential to be useful to the adultgerontology NP student or faculty member, who may be on a“gerontology learning curve” of his or her own.
As we move forward into this year of changes we know arecoming and those yet to surprise us, it is clear we now have aunique opportunity to step up and “share the wealth” – ourknowledge on how to provide the best care for older adultsacross settings. I urge you all to consider getting involved onone (or more) of our committees or special interest groups. Youmay find your own practice enhanced by what you learn fromnetworking with colleagues from across the nation with a vari-ety of experiences and wisdom to share. If participating in agroup is not an option for you right now, please get involved byresponding to periodic surveys that come from GAPNA. Thesesurveys are usually targeted to gathering specific informationfrom membership, so that we can represent your concerns andopinions adequately in other forums where our participation isinvited, or support the scholarly work of our members. GAPNAis our organization and your opinion does count. So let us knowwhat you think. And Happy New Year!
Marianne Shaughnessy, PhD, ANP-BC, GNP-BCPresident
Special Thanks to
for their continued support as a Plantinum Corporate Member
Special Thanks to
as GAPNA’s Corporate Partners

GAPNA’s Annual ConferenceMORE PHOTO HIGHLIGHTS
September 19-22, 2012 in Las Vegas, NVPhotos by Cashman Productions – Las Vegas, NV
GAPNA’s 32nd Annual Conference
September 18-21, 2013 • Chicago, IL
Make plansnow to
attend

D id you know that Chicago’s nick-names include The Windy City, the
City of Big Shoulders, the Second City,Hog Butcher of the World, and The CityThat Works? And, from September 18-21, 2013, Chicago will also be known asthe host of GAPNA’s 32nd AnnualConference.
Chicago is America’s third largestcity and its scenic lakeside location,world-class cultural offerings, andunique architecture are just some of thereasons why it is a great place to visit.The city grew from a small trading post atthe mouth of the Chicago River into aglobal city, a thriving center of interna-tional trade and commerce, and a placewhere people of every nationality cometo pursue the American dream.
There’s no better way to exploreChicago than by taking advantage of themultitude of attractions, events, tours,and recreational activities happeningthroughout the city, every single day.Whether you’re here for business orvacation travel, you’ll never be boredwith so many things to do in Chicago!
When you’re not attending one ofthe fantastic educational sessions orsocial events during the GAPNAConference, stop by one of the officialVisitor Centers, located at Chicago WaterWorks, 163 E. Pearson St., or theChicago Cultural Center, 77 E. RandolphSt. Pick up helpful brochures and travelmaps, or talk with one of the friendly,knowledgeable visitor services represen-tatives to make the most of your visit!And prepare for your visit by exploringwww.choosechicago.com
What’s your passion? Ballet? Base -ball? Brontosaurus? Classical music?Political satire? Modern architecture? InChicago, you’re sure to find attractionsthat match your interests, and you’llprobably develop some new ones whileyou’re here.
With more than 7,300 restaurants inChicago, there’s sure to be one to suitevery taste, budget, and mood. Whetheryou’re looking for Chicago-style hot dogsor French haute cuisine, steaks orseafood, pierogies or pizza, you will findthem in Chicago. And they’ll be good.
In addition to being a top travel des-tination, Chicago has long been a pre-mier shopping and fashion capital.Major department stores and chicdesigner boutiques are all part of avibrant retail scene that caters to anyshopper’s needs. Today, the city is hometo more than 250 Chicago-based fashiondesigners and 400 independently ownedboutiques.
So make plans now to join yourfriends and colleagues in ChicagoSeptember 18-21, 2013 for GAPNA’s32nd Annual Conference. The city hasmany nicknames, but you’re likely to callit fun, exciting, and stimulating!
8 The Newsletter — www.gapna.org • Spring 2013, Volume 32, Number 1
Your Kind of Town: Chicago Welcomes GAPNA Convention Attendees
GAPNA’s Career Center: Your Opportunity Awaits
Perhaps you know of a friend who is looking to change careers? Maybe you arecontemplating changing positions or employers? Do you have to move to a new
area and can’t transfer within your current company? Maybe your company has anopening and wants to find a qualified individual to fill the vacancy?
If any of the above questions apply to you, it may be time for you to visitGAPNA’s Career Center. Simply log onto the GAPNA web site and click the“Resources” then “Career” tab to view current employment opportunities. If youwould like to post an opportunity, please contact the National Office at 856-355-1392 or send your advertisement to [email protected] for a quick pricequote!

The Newsletter — www.gapna.org • Spring 2013, Volume 32, Number 1 9
Nurse Practitioners Have Potential to ImproveAccess to Primary Care
One way states could increase access to primary care for theirresidents is to consider easing their scope of practice restrictionsand modifying their reimbursement policies to increase the role ofnurse practitioners in providing primary care, according to a newpaper released by the National Governors Association (NGA).
With the demand for primary care services already strainingcapacity in most states, more than 16 million individuals projectedto gain health insurance coverage by 2016 and a rapidly aging pop-ulation, many states are considering options to increase the numberand role of primary care providers.
“The Role of Nurse Practitioners in Meeting IncreasingDemand for Primary Care” reviews academic and policy-orientedliterature and state rules governing nurse practitioners’ scope ofpractice to examine the extent to which:
• Scope of practice rules, licensure, and other conditionalrequirements vary across states.
• States’ rules and requirements deviate from evidence-basedresearch of appropriate activities for nurse practitioners.
• Changes to state scope of practice laws and regulations onaccess to health care and its quality.
To learn more about the NGA Center for Best Practices HealthDivision, please visit www.nga.org/cms/center/health. For NGA’svirtual resource center on potential solutions to health policy prob-lems, visit statepolicyoptions.nga.org
Certain Medications Are Associated withFunctional Decline in the Elderly
Functional status is the hallmark by which geriatric care ismeasured. Medication use is a known risk factor for functional sta-tus decline, but a recent review of studies on the topic revealed thatsome drug classes are associated with greater functional declinethan others. A recent literature review included 19 studies thatlooked at the relationship between medication use and type andfunctional decline among older adults. In general, as the number ofprescriptions increased, so did functional decline.
Specifically, three of four studies found a negative associationbetween functional decline and the use of benzodiazepines. Therewas also a relationship found between worse functional status andincreasing exposure to anticholinergic medications. Other studiesproduced mixed results for other drug classes, such as antidepres-sants and antihypertensives.
See results in Perone, E.P. et al. (2011). Medication use andfunctional status decline in older adults: A narrative review. TheAmerican Journal of Geriatric Pharmacotherapy, 9(6), 378-391.
Bowel Incontinence and Other Clinical FactorsPredict the Development of Pressure Ulcers
The elderly are vulnerable to pressure ulcers, particularly whenthey have limited mobility and cannot ambulate. Identifying whichpatients are most at risk for pressure ulcers is an important part ofprevention. In this study, researchers determined a set of factors thatraise the risk of developing pressure ulcers in older home carepatients.
The cumulative incidence of new pressure ulcers was 1.3%.Among the 71 patients who developed an ulcer, there was a high-er prevalence of a cancer diagnosis, diabetes, and longer time in
home health care. The two top predictors of developing a new ulcerwere bowel incontinence and patient inability to transfer self. Otherfactors included needing assistance with grooming and dressing,dependence in toileting, being bedfast or chairfast, and already hav-ing a pressure ulcer at the start of home health care.
For more info, see Bergquist-Beringer, S., & Gajewski, B.J.(2011). Outcome and assessment information set data that predictpressure ulcer development in older adult home health patients.Advances in Skin & Wound Care, 24(9), 404-414.
Adverse Drug Reactions a Major Cause ofUnplanned Hospitalizations of Elderly Veterans
Veterans who are age 65 and older and taking multiple med-ications for various conditions are at risk of adverse drug reactions(ADRs) that can lead to unplanned hospitalizations. In fact, a newstudy reveals 10% of unplanned hospitalizations among this groupwere related to ADRs. The study included a group of 678 veteranshospitalized directly from an ambulatory care setting for anunplanned admission. There were 70 ADRs involving 113 drugs in68 hospitalizations. More than one-third (36.8%) of these hospital-izations were considered to be preventable. The researchers estimat-ed that if they applied these findings to the population of more than2.4 million veterans receiving care during the study period (2003-2006), as many as 8,000 hospitalizations would have been prevent-able.
For details, see Marcum, Z.A. et al. (2012). Prevalence ofunplanned hospitalizations caused by adverse drug reactions inolder veterans. Journal of the American Geriatric Society, 60, 34-41.
Introduction of Hospice Services by NursingHomes Does Not Significantly Affect NursingAssistant Staffing
More and more nursing homes are providing hospice care totheir residents. End-of-life care is managed by hospice organiza-tions, which can also provide routine hands-on care normally pro-vided by certified nursing assistants (CNAs). As a result, nursinghomes could reduce staffing, thereby serving as an incentive forhospice referrals. However, a new study finds that the introductionof hospice services in nursing homes does not result in significantCNA staffing changes. Rather, as hospice patient volume increased,small increases in CNA staffing were observed.
For details, see Tyler, D.A. (2011). Effect of increased nursinghome hospice use on nursing assistant staffing. Journal of PalliativeMedicine, 14(11), 1236-1239.
Studies Link Adverse Drug Interactions toElevated Risk for Hospitalization Among theElderly
A review of 17 studies that assessed specific drug interactionsin elderly patients found that 16 of the studies reported an elevatedrisk for hospitalization in older adults associated with drug interac-tions. These interactions included angiotensin-converting enzyme(ACE) inhibitors and potassium-sparing diuretics; ACE inhibitors orangiotensin receptor blockers and sulfamethoxazole/trimethoprim(SMX/TMP); benzodiapines or zolpidem and other medications;calcium channel blockers and macrolide antibiotics; digoxin andmacrolide antibiotics; lithium and loop diuretics or ACE inhibitors;
Published an Article Recently?We are looking for GAPNA members who have recently published clinical or research arti-
cles. Let us know the title, publication, volume, and issue number of your article, along with abrief abstract/summary, and we’ll share it with your fellow members in the GAPNA Newsletter.Keep us updated at [email protected]
Clinical ResearchCorner

10 The Newsletter — www.gapna.org • Spring 2013, Volume 32, Number 1
phenytoin and SMX/TMP; sulfonylureas and antimicrobial agents;theophylline and ciprofloxacin; and warfarin and antimicrobialagents or non-steroidal anti-inflammatory drugs.
The researchers concluded that when the elderly receive drugtherapy, it should be absolutely necessary for the achievement ofwell-defined goals. They also recommend that an evidence-based,high-priority list of drug interactions in the elderly be developed andmaintained.
For more info, see Hines, L.E. et al. (2011). Potentially harmfuldrug-drug interactions in the elderly: A review. American Journal ofGeriatric Pharmacotherapy, 9, 364-377.
Elderly Blacks Less Likely than Elderly Whitesto Receive a Depression Diagnosis orTreatment
Researchers examining racial and ethnic disparities in the diag-nosis and treatment of depression among the elderly found that4.2% of Blacks received a diagnosis of depression compared to6.4% of Whites, 7.2% of Hispanics, and 3.8% of other groups.Blacks who were diagnosed were also less likely to be treated fordepression than non-Hispanic Whites. For example, among Blacksdiagnosed with depression, 39.6% did not receive treatment com-pared with 27% of Whites.
The authors point out that differences in depression diagnosisrates among racial/ethnic groups may be the result of both differ-ences in underlying rates of pathology and underdiagnosis ofdepression in certain groups. They also suggest a need to look atother factors, including racial/ethnic differences in depression help-seeking behaviors, stigma, knowledge, and attitudes.
For details, see Akincigil, A. (2012). Racial and ethnic dispari-ties in depression care in community-dwelling elderly in the UnitedStates. American Journal of Public Health, 102(2), 319-328.
Alcohol May Be Misused by Residents inAssisted Living Places
A new study suggests that alcohol use is rather widespread andmay be abused in assisted living (AL) facilities.
Nurse aides who had worked in AL facilities believed themajority of AL residents (69%) drank alcohol. Of these, a third(34%) of residents were considered by the nurse aides to drink on adaily basis. Also, 44% of the nurse aides suspected that some resi-dents under their care made poor choices about alcohol, with 40%saying such use had a negative impact on residents’ health.
To learn more, see Castle, N.G. (2012). Alcohol misuse andabuse reported by nurse aides in assisted living. Research on Aging,34(3), 321-326.
Complications Affect QOL in Older Adults withDiabetes
Older adults with diabetes are at increased risk for geriatric syn-dromes, such as depression and falls, as well as hypoglycemiaresulting from drugs they are taking.
A new study reveals that geriatric syndromes and hypo-glycemia are associated with lower health-related quality of life(HRQL) as much as diabetes complications. No association wasfound between significantly lower mental HRQL and having a geri-atric syndrome or diabetes complication in general. However, someconditions, such as depression and being underweight, resulted inlower mental HRQL. Amputation, coronary heart failure, falls,chronic pain, heart attack, depression, underweight, and hypo-glycemia were more strongly associated with lower HRQL than dia-betes-related factors, such as duration of diabetes and insulin use.
For more info, see Laiteerapong, N. (2011). Correlates of qual-ity of life in older adults with diabetes: The diabetes & aging study.Diabetes Care, 34(8), 1749-1753.
Washington
Oregon
California
NorthernCalifornia
Nevada
Idaho
Wyoming
Montana
Nebraska
Kansas
Oklahoma
New Mexico
Utah
Colorado
Minnesota
Iowa
Missouri
Arkansas
Louisiana
MississippiAlabama
Georgia
South Carolina
Florida
North Carolina
Tennessee
Kentucky
Illinois
IndianaOhio
Michigan
New York
Vermont
New Hampshire
Massachussetts
Maine
Pennsylvania
Virginia
Arizona
Maryland
Washington, DC
Wisconsin
WestVirginia
Texas
Delaware
Rhode Island
New Jersey
Connecticut
Puerto Rico
North Dakota
South Dakota
Michigan
Alaska
Hawaii
NortheastRegion
SoutheastRegion
WesternRegion
North CentralRegion
402
401
207
209
205 204
201
203
101 102
103
303
302
304
202
206208
301
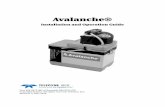
ChaptersLooking for a CHAPTER NEAR YOU?
ARIZONA (SONORAN)Jean [email protected]
CHICAGOLANDJill [email protected]
NORTHERN CALIFORNIAJulie [email protected]
DELAWARE/PENNSYLVANIAStacy [email protected]
FLORIDA GAPNAJo Ann [email protected]@oslermedical.com
FLORIDA GULF COASTPeggy [email protected]
GEORGIA (ATLANTA)Carolyne [email protected]
LOUISIANATanya [email protected]
MISSISSIPPI & ALABAMADr. Lisa [email protected]
MARYLANDSusan [email protected]
NEW ENGLANDSusan [email protected]
MICHIGAN (GREAT LAKES)Debra [email protected]
NORTH CAROLINA (TRIAD)Marigold (Margo) [email protected]@aol.com
OHIOBeth [email protected]
TENNESSEE (MIDDLE)Amber [email protected]
TENNESSEE (MIDSOUTH)Regina [email protected]
TEXAS (GULF COAST) - HOUSTONRhonda [email protected]
WISCONSIN (SOUTHEAST)Nancy [email protected]
Interested in Starting a Chapter?
Contact the GAPNA National Office — [email protected] • (866) 355-1392 • Fax (856) 589-7463

The Newsletter — www.gapna.org • Spring 2013, Volume 32, Number 1 11
MinuteClinic is partnering with Johnson & Johnson Familyof Consumer Companies to sponsor the “Together We Care™”Nurse Practitioner Scholarship Program.
The scholarships will be awarded this spring through TheFoundation of the International Scholarship and TuitionServices, Inc. There will be up to 30 scholarships worth $2,500apiece awarded to nurse practitioners and up to five scholar-ships worth $5,000 each awarded to doctor of nursing practicestudents. The funds will be eligible to cover tuition, books, andacademic fees for the 2013-2014 academic year.
Scholarship applications will be accepted unitil May 1,2013 at www.minuteclinic.com/scholarship. Applicants mustbe legal U.S. residents enrolled in nationally accredited nursepractitioner master’s or doctor’s programs. To be eligible, stu-dents must be in programs leading to licensure as an APRN witha family nurse practitioner specialty or other special interest incommunity or public health. High academic performance andstrong community involvement will be taken into account.
Code of Ethics for Nurses RevisedThe International Council of Nurses (ICN) Code of Ethics
for Nurses, most recently revised in 2012, is a guide for actionbased on social values and needs. The Code has served as thestandard for nurses worldwide since it was first adopted in1953.
The Code is regularly reviewed and revised in response tothe realities of nursing and health care in a changing society.The Code makes it clear that inherent in nursing is respect forhuman rights, including the right to life, to dignity, and to betreated with respect.
The ICN Code of Ethics guides nurses in everyday choicesand it supports their refusal to participate in activities that con-flict with caring and healing. To obtain a hard copy of the ICNCode of Ethics, please visit www.icn.ch
Nurses Ranked #1 Again in Honestyand Ethics
Nurses once again scored the highest in the latest 2012Gallop Poll ratings of professional honesty and ethics. Nurseshave scored tops in this category every year since 1999 whenthey were first included in the list of professions, except for2001 when firefighters were included in the survey followingthe September 11 terrorist attacks.
Americans rate the top five professions for honesty and eth-ical standards as nurses (85% very high/high), pharmacists(75%), medical doctors (70%), engineers (70%), and dentists(62%). At the bottom are car salespeople (8%), members ofCongress (10%), advertising practitioners (11%), stockbrokers(11%), and HMO managers (12%).
GAPNA’s Facebook Pagecontinued from page 1
On the GAPNA Facebook page youwill experience news and promotionalopportunities, changes and trends ingerontological nursing, and inspiringquotes and fun facts that fans “like.” Thinkof the Facebook page as an extension ofthe GAPNA web site, where people canengage and interact with both the associ-ation and colleagues in real-time.
Share your comments, pictures, sto-ries, and advice with the GAPNAFacebook community by liking us today!www.facebook.com/GAPNA
MinuteClinic, Johnson & Johnson Family of Consumer Companies Announce up to $100,000 in Scholarships for Nurse Practitioners
GNP Student Scholarship Available! GAPNA is excited to announce the availability of a new GNP Scholarship for
2013-2014. Scholarship amounts are at least $2,500, and may be awarded up to$5,000. Submission deadline is June 15, 2013.
Among other things, candidates must:1. Be matriculated or matriculating into one of the following programs:
Adult/Gerontological Primary Care Nurse Practitioner; Adult/GerontologicalAcute Care Nurse Practitioner; or Adult/Gerontological Clinical NurseSpecialist for the 2013-2014 school year at a school of nursing in the UnitedStates.
2. Plan to continue in the field of nursing with a career interest in working witholder adults upon completion of degree program.
3. Be a registered nurse and a United States citizen.
4. Agree that any Scholarship award monies will be used to defer the cost oftuition and other school-related fees (excluding: room, board, social, healthinsurance or athletic fees) in the degree-granting program and further under-stands that GAPNA will pay the awarded Scholarship jointly to the individualand the indicated school.
5. Be a member of GAPNA and in good standing.
Visit the GAPNA web site for full requirements/eligibility for candidates and toobtain the scholarship application form.

12 The Newsletter — www.gapna.org • Spring 2013, Volume 32, Number 1
NewsletterThe Official Newsletter of the Gerontological Advanced Practice Nurses Association — Founded in 1981
PRESIDENTMarianne Shaughnessy, PhD, ANP-BC, GNP-BCUniversity of Maryland, BaltimoreSchool of NursingBaltimore, [email protected]
PRESIDENT-ELECTLisa Byrd, PhD, RN, FNP-BCLisa Byrd Healthcare Inc.Bolton Family ClinicMadison, [email protected]
IMMEDIATE PAST PRESIDENTElizabeth Galik, PhD, CRNPUniversity of MarylandSchool of NursingBaltimore, [email protected]
SECRETARYJennifer Serafin, MSN, BSN, RN, GNPJewish Home for the AgedSan Francisco, [email protected]
TREASURERKathyrne Barnoski, MN, FNP, GNP-BCEvercare PhoenixPhoenix, [email protected]
DIRECTOR-AT-LARGELaurie Kennedy-Malone, PhD, GNP, FAANPSchool of NursingUNC GreensboroJamestown, [email protected]
DIRECTOR-AT-LARGEPatty Kang, MSN, RN, GNPPermanente Medical Group/Kaiser South SacramentoFairfield, [email protected]
NATIONAL OFFICEMichael Brennan, CMPExecutive [email protected]
Sherry DzurkoAssociation Services [email protected]
East Holly Avenue/Box 56Pitman, NJ 08071Phone: 856-355-1392Fax: [email protected]
Spring 2013 • Volume 32, Number 1
Please send mail and email address changes to [email protected] Newsletter Deadline: April 4, 2013
Send articles to: [email protected]
2012-2013 Committee ChairsAwardsSusan Mullaney, MS, APN, [email protected]
Chapter LeadershipJo Ann Fisher, MSN, [email protected]
Conference PlanningDawn Marie Baylis, [email protected]
EducationBarbara Harrison, PhD, [email protected]
Health AffairsEvelyn Duffy, DNP, GNP/ANP-BC, [email protected]
HistoricalKathleen Fletcher, MSN, RN, CS, GNP,[email protected]
Trudy Keltz, RN, [email protected]
Chapter LeadershipJo Ann Fisher, MSN, [email protected]
NominatingCandance Harrington, DNP, ANP-BC, [email protected]
PracticeMeghan Routt, MSN, ANP/GNP-BC, [email protected]
ResearchValerie Sabol, ACNP-BC, [email protected]
Journal Section EditorDeb Bakerjian, PhD, MSN, RN, [email protected]
Newsletter EditorCandace Harrington, DNP, ANP-BC, [email protected]
Web Site EditorsCarolyn Clevenger, DNP, [email protected]
SPECIAL INTEREST GROUPSHospice/Palliative CareCaroline [email protected]
House CallsDeb Wolff-Baker, MSN, FNP-BC, [email protected]
LeadershipPat Kappas-Larson, MPH, APN-C, [email protected]
LGBT Focus GroupTrudy Keltz, RN, [email protected]
Colleen Wojceichowski, MSN, [email protected]
LTC/Nursing HomeSuzanne Ransehousen, [email protected]
Transitional CareLauren Van Saders, GCNS-BC, [email protected]
Volunteers Needed: Interested in serving on a GAPNA Com mittee? Learn more bycontacting the GAPNA National Office at [email protected] or call 856-355-1392 andrequest a Call for Volunteers form.
Notice Regarding SubmissionsGAPNA encourages the submission of news items and photos of interest toGAPNA members. By virtue of your submission, you agree to the usage andediting of your submission for possible publication in GAPNA’s newsletter,web site, social media, and other promotional and educational materials.