New York London - Amazon Web Services// 40 The Aging Intellect 50-year-old normals on MicroCog,...
27
Transcript of New York London - Amazon Web Services// 40 The Aging Intellect 50-year-old normals on MicroCog,...

New York London
The Aging Intellect
Douglas H. Powell
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853
Cover image: “Icarus”, plate VIII of the illustrated book “Jazz” by Henri Matisse. © 2011 Succession Henri Matisse/Artists Rights Society (ARS), New York. Photo: Archives Matisse.
RoutledgeTaylor & Francis Group711 Third AvenueNew York, NY 10017
RoutledgeTaylor & Francis Group27 Church RoadHove, East Sussex BN3 2FA
© 2011 by Douglas H. PowellRoutledge is an imprint of Taylor & Francis Group, an Informa business
Printed in the United States of America on acid-free paper10 9 8 7 6 5 4 3 2 1
International Standard Book Number: 978-0-415-99685-3 (Hardback)
For permission to photocopy or use material electronically from this work, please access www.copyright.com (http://www.copyright.com/) or contact the Copyright Clearance Center, Inc. (CCC), 222 Rosewood Drive, Danvers, MA 01923, 978-750-8400. CCC is a not-for-profit organiza-tion that provides licenses and registration for a variety of users. For organizations that have been granted a photocopy license by the CCC, a separate system of payment has been arranged.
Trademark Notice: Product or corporate names may be trademarks or registered trademarks, and are used only for identification and explanation without intent to infringe.
Library of Congress Cataloging‑in‑Publication Data
Powell, Douglas H.The aging intellect / Douglas H. Powell
p. cm.Includes bibliographical references and index.ISBN 978-0-415-99685-3 (hardback : acid-free paper)1. Cognition in old age. 2. Cognition--Age factors. 3. Aging. 4. Quality of life.
I. Title.
BF724.85.C64P677 2011155.67’13--dc22 2010043256
Visit the Taylor & Francis Web site athttp://www.taylorandfrancis.com
and the Routledge Web site athttp://www.routledgementalhealth.com
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853
v
Contents
Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . viiIntroduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xi
1 MaximizingIntellectualPowersintheThirdAgeofLife . . . . . . . . . . . . . . . . . 1
2 HowHealthAffectstheIntellect. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
3 HowtheMindAges . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
4 HealthyLifestyleHabitsBenefitingtheAgingBodyandMind. . . . . . . . . . . . 63
5 DirectActionsThatBenefittheIntellect. . . . . . . . . . . . . . . . . . . . . . . . . . . . 89
6 OptimalCognitiveAging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111
7 NormalCognitiveAging. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 133
8 High-RiskCognitiveAging. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 157
9 WritingandLearningAbouttheAgingIntellect. . . . . . . . . . . . . . . . . . . . . . 183
GlossaryofFrequentlyUsedTerms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203
Notes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 209
Index .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. .. . 283
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

39
3
How the Mind Ages
For most adults, mental ability slopes gently downward until age 60. As Figure 3.1 shows, the level of intellectual functioning of the average 60-year-old is only 6% less than that of a 30-year-old.1 At 70, the overall IQ is 11% less than the average of the young adults. In the next decade, the rate of cognitive decline accelerates, with the average octogenarian’s mental ability being about 20% lower than those at 30.
A limitation of these data is that they are cross sectional, not longitudi-nal. That is, each age group consists of different subjects who were tested at about the same time. It is possible that the differences between the age groups may be caused by factors known to be associated with lower IQ scores (such as health, education, or cohort differences) rather than age.2
A challenge when conducting cross-sectional research is matching all of the subjects on variables known to influence cognitive decline. For instance, education and income level influence the rate at which mental abilities diminish. It is not surprising that people with more education and financial resources show less intellectual deterioration in the 3rd Age than those less fortunate.3 So, when subjects for a cross-sectional study are selected, there is an advantage in their being comparable to one another with respect to education and income level. This makes it more likely that changes in men-tal ability from one decade to the next are caused by age rather than by other factors that also affect the power of the aging intellect.
We were able to match education and income level when we tested physi-cians during the development of MicroCog, a computerized test designed to identify professionals with mild cognitive impairment (MCI). We gave the test to 1,002 medical doctors aged 25 to 92. In the process of developing MicroCog, we also tested 581 nonphysician subjects whom we labeled “normals.”4
Figure 3.2 shows the total scores on MicroCog for the two groups. We can see the value of more education in slowing cognitive decline. In all age groups from 30 to 75+, the medical doctors slightly outscore the normals. However, the downward trajectory of the curves is parallel.
More education gives an edge on mental ability tests that lasts into the 3rd Age of life. The 60-year-old doctors performed at about the same level as
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

40 ❚ The Aging Intellect
50-year-old normals on MicroCog, while medical doctors aged 65–74 scored about as high as normals a decade younger.5
MentalAbilitiesThatDeclineLeastandMostWithAge:ResearchFindings
Not all mental skills decline at the same rate. Processing speed is the leading indicator of cognitive aging because it is the intellectual function that dimin-ishes most dramatically as we grow older. Our processing speed is how long it takes us to understand what the problem is, decide on the correct response, and give an answer. Tests of processing speed might involve solving analo-gies or assembling a puzzle under timed conditions. In real life, processing speed can be measured by the length of time it takes to check a credit card statement for errors or memorize the directions to a friend’s house.
Age
Perc
ent C
orre
ct
1009590858075706560
1002 MDs581 Normals
30 40 50 60 70 75+
Figure 3.2 Age-associated decline in total mental ability among physi-cians and nonphysician (normal) individuals.
Age
IQ105100
959085807570656035–44 35–54 55–64 65–74 75–79 80–84
Figure 3.1 Change in full-scale IQ from age 30.
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

How the Mind Ages ❚ 41
Advancing years slow processing speed. One investigation, summarized in Figure 3.3, shows the effects of aging on the time required to complete the digit symbol substitution test.6 This test requires that the subject learn symbols associated with numbers 1–9 (e.g., n goes with 1, Ω = 2) and then fill in the correct symbols as possible within the short time allowed when the numbers are presented in random order. Age group differences show up early. The 40-year-olds were 20% slower than those in their 30s. By age 60, it took twice as long to complete the test than for the young adults. The 70-year-olds were nearly three times slower. No other single mental ability declines as rapidly during the adult years as processing speed.7
Time pressure is not the only factor that influences how well older people perform. The difficulty level of the problem to be solved also contributes to processing time. Psychologists gave a test of reasoning (analogies test) under strict time limits to adults aged 25 to 75+.8 The analogies were rated as easy, medium difficulty, or hard. Little difference occurred between the youngest and oldest volunteers on the easy analogies (“Green is to grass as _____ is to sky”). On analogies of medium difficulty, the scores of those aged 75 and older were only 6.5% lower than those a half century younger. The performance of older test-takers fell off noticeably compared to the young adults on the hardest of the analogies (e.g., “Fission is to splitting as fusion is to ____ ?”). Here, the combination of difficulty and time pressure took its toll even on midlifers at the threshold of the 3rd Age. Those in the 55- to 64-year-old group scored nearly 18% below the 25-year-olds on the hardest analogies.
Of particular interest to 3rd Agers is what happens when the time pres-sure is removed and younger and older subjects are compared only on the number of correct responses. A body of research by University of Virginia professor Timothy Salthouse has demonstrated that when speed is removed
Age
Proc
essi
ng S
peed
in S
econ
ds
2.5
2
1.5
1
0.5
030 40 50 60 70 80
Figure 3.3 Processing speed and aging.
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

42 ❚ The Aging Intellect
as a variable performance on complex tasks, by scoring the percentage of correct answers to the analogies questions instead of the number of right responses, the decline from age 30 to 75 is reduced by about two-thirds.9
As we might anticipate, not all mental abilities decline at the same rate. Some aptitudes, called crystallized abilities, decline gradually with age because they are less dependent on processing speed.10 Crystallized abilities do not usually involve time pressure and are largely dependent on acquired knowledge and formal education. General information, vocabulary, and cal-culation are examples.
In contrast, fluid abilities are less dependent on acquired knowledge and education and are more influenced by how quickly the mind works. Commonly used tests to measure fluid aptitudes include visuospatial tasks (assembling puzzles or blocks to match a design), learning and applying a number-symbol code, and reasoning. Most tests of fluid abilities involve working memory and processing speed, which, as we have seen, decline more rapidly with advancing age than other mental skills.
Our own research with both doctors and normal subjects supported the theory that crystallized and fluid aptitudes decline at different rates.11 Figure 3.4. graphs the average age group scores of physicians aged 30 to 75+ on two crystallized abilities (short-term verbal memory and calculation) and two fluid aptitudes (reasoning and visuospatial abilities) from the MicroCog test battery.
In Figure 3.4, notice that the crystallized abilities slope gently down-ward from age 30, while the two fluid aptitudes diminish rapidly with each passing decade. At age 70, the average calculation and short-term memory scores were only 8% and 9% lower than at age 30. During that same 40-year interval, fluid abilities-related visuospatial and reasoning scores fell 44% and 28%, respectively.
Comparable findings occur with other tests. The individually adminis-tered Wechsler Adult Intelligence Scale consists of two halves: the Verbal
Age
Crystallized
Fluid
Perc
ent C
orre
ct
9585756555453525
Verbal MemoryCalculationReasoningVisuospatial
30 40 50 60 70 75+
Figure 3.4 Decline in crystallized and fluid abilities: 1,002 physicians.
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853
How the Mind Ages ❚ 43
and Performance IQs. The Verbal IQ is comprised largely of subtests mea-suring crystallized abilities, whereas the Performance IQ consists mainly of tests of fluid aptitudes. The pattern of the test score differences of subjects from 30 to 70 years of age resembled the MicroCog physician data, although the absolute differences were smaller. The differences in average Verbal or crystallized IQ between the younger and older volunteers was only 3%; however, the mean Performance/fluid IQ for the septuagenarians was 20% lower than those 30 years of age.12
EffectsofAgingonWorkingMemoryandMultitasking
Advancing age degrades working memory and the capacity for multitask-ing. Working memory is the ability to store important information while working on a related task.13 Tests that scientists employ to assess working memory include repeating a series of digits backward. An everyday example is multiplying 78 × 78 without a calculator. Decades of research have found that working memory follows the same downward slope as fluid abilities. The effect is more apparent with mental challenges of greater difficulty.14
Working memory is required when complex decisions need to be made. Imagine that you are a 3rd Ager who has to choose among three different health plans. Each has slightly different costs, coverage, copays, breadth of health care providers to choose from, and levels of consumer satisfaction. Making a decision about which plan is best for you requires that you care-fully read the prospectus of all three plans and then compare each with the others on the factors that are important to you. For instance, are you willing to settle for generic rather than the more expensive brand name drugs in order pay less for your health insurance?
Studies of complex decision-making competence in selecting health care coverage find that compared to midlifers, older adults work more slowly. In addition, they make more errors in comprehending the differences between key elements in the health plans (such as what is and what is not covered) and make nonoptimal decisions more frequently.15 The older adults who are better at complex decision making tend to have more education, have greater emotional stability, are more open to advice from others, and are willing to delegate responsibility to those helping them make the decision.
Multitasking is doing two things at one time—the intellectual equivalent of rubbing your tummy and patting your head simultaneously. Other terms for this process, which have slightly different meanings but encompass the same general idea, are dual-task attention and divided attention. You are multitasking when you read your e-mail while talking on the phone or make out a grocery list while sitting in a meeting. People at all age levels have more difficulty when they try to do two things at once compared to
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

44 ❚ The Aging Intellect
working on a single problem. Multitasking also can be dangerous. Consider cell phone use while driving. Whether hands free or not, talking to someone on the cell phone while behind the wheel increases the probability of an accident fourfold for all age groups. This is the same risk as driving drunk.16
As people grow older, their multitasking capability wanes.17 On average, people in their 60s and 70s take about twice as long as younger adults to carry out two tasks at a time. In addition, one of the two is usually not done well. Do experienced older people reduce the differences between them and midlife adults on familiar tasks such as routine household chores?18 Might their years of doing these chores enable the seniors to compensate for their slower machine speed?
The short answer is “no.” Here are two cases in point, both involving cooking: Occupational therapists in Colorado videotaped women in their late 20s and those in their early 70s while they carried out a variety of household chores, including cooking eggs and making toast and coffee.19 Based on the tapes, the older women were less efficient in carrying out these tasks. In Toronto, psychologists compared the efficiency of younger and older subjects matched for education and IQ in preparing a breakfast consisting of coffee, toast, sausage, eggs, and pancakes. The aim was to cook the foods so that they would all be ready to eat simultaneously. This was a challenge because each had a slightly different cooking time. They found that 3rd Agers worked more slowly, made twice as many overcook-ing or undercooking errors as the younger chefs, and had more difficulty shifting their attention from one task to the other to monitor the progress of the cooking.20
MentalSkillsThatDeclineWithAge:InterviewFindings
As someone who holds dual citizenship as a clinician and a researcher, I find that the therapist in me is always a little skeptical about whether older people interviewed by students would exhibit the same patterns of cogni-tive decline as the hundreds of subjects in my own investigations and the research of others. For instance, would the interview subjects notice the same differences in the relative decline of their crystallized and fluid apti-tudes that are pictured in Figure 3.4? And, might these clinical interviews turn up unexpected findings about how the mind ages?
I excerpted short descriptions of declining mental skills from some of the student interviews of volunteers who were all classified as optimal cogni-tive agers. These optimal agers rated their mental abilities as the same or better than 5 years earlier and stronger than those of their age mates. Yet, three of four acknowledged some decline in intellectual functioning. Their comments about the cognitive decline they noticed can be clustered into
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

How the Mind Ages ❚ 45
four groups: slower processing speed; occasional trouble recalling names, numbers, and things; intermittent tip-of-the-tongue (TOT) blockage; and periodic difficulties maintaining attention.
Nancy (age 78) notices that it takes her quite a bit longer to knit sweaters for her great-grandchildren than it did her grandchil-dren. In addition to her hands moving a little slower, she thinks it takes her longer to figure out the patterns.
According to Gary (78), larger, more difficult projects like mak-ing furniture take quite a bit more time to complete than a few years ago. He also admits that he now works mostly on pieces he is familiar with rather than taking on something new.
Sarah (78) reads both fiction and nonfiction, does crossword puzzles, watches the news, and even takes video college courses. However, she sometimes feels a decline of her verbal memory for people’s names, including occasionally those of her grandchildren.
Melina (70) has not lost any of her mental abilities, except she notices the occasional temporary blocking of the name of some-thing or a zip code. This frustrates her because it is right on the tip of her tongue.
Nick (74) says that sometimes when he is talking to his friends he loses track of what he is talking about. He starts telling the story, but about halfway through he loses his way and cannot remember the point of the story. The last time this happened, Nick had to ask, “What were we talking about?” As soon as someone reminded him, Nick recalled how the story should go. His buddies told him this happens to them all the time.
Gabriela (69) says she is as sharp as ever, with one exception: Names and numbers are an issue. Sometimes, she calls one grandchild by another one’s name.
Peter (79) says he does a lot to stay mentally active. He reads four newspapers a day. The only problems he has are occasional attention problems. An example was getting lost when follow-ing a detour off the interstate highway. When he stopped at a gas station to ask for help, Peter could not focus his attention sharply enough to memorize the new direction the first time. “It doesn’t always happen but sometimes things don’t lock in right away like they used to,” he says.
Overall, these clinical interviews partially confirmed the predicted order in which fluid or crystallized aptitudes decline. The research finding that was solidly confirmed was slower processing speed. Among these optimal agers, this was the most frequently mentioned declining aptitude. Most
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

46 ❚ The Aging Intellect
often, this is noticed when carrying out complex tasks (knitting sweaters or building furniture) that demand both working memory and psychomo-tor speed. Declining visuospatial ability made its presence known in Peter’s example of getting lost while driving.
After slower processing speed, working memory, and visuospatial prob-lems, the next most frequently mentioned cognitive difficulty involved moments of inability to remember a name, a number, or what something is called, such as “that covering on the outside of houses that looks like cement” (stucco). These were often experienced as a TOT problem. A TOT memory blockage is the sensation of being on the verge of remembering but being unable to produce a word you are certain you know. Here is a description of the TOT experience written by Harvard psychology professor and physician William James more than a century ago:
Suppose we try to recall a forgotten name. The state of our consciousness is peculiar. There is a gap therein; but no mere gap. It is a gap that is intensely active. A sort of wraith of the name is in it, beckoning us in a given direction, making us at moments tingle with a sense of our closeness, and then letting us sink back without the longed-for term.21
Though less dramatically experienced, TOT memory blockages occur among all adults, and their frequency increases with age. Investigators in California asked groups of subjects in their 20s, 60s, and early 80s to keep a diary of such moments during a 4-week period.22 Predictably, the oldest subjects recorded the most TOT experiences, averaging one every 3 days, compared to the younger volunteers, who had a memory blockage every 4 or 5 days. However, octogenarians outperformed the younger subjects in the spontaneous recall of the lost word, which was remembered 98% of the time.23
An interesting finding from the student interviews was the number of optimal agers who mentioned minor difficulties with maintaining attention: getting sidetracked while telling a story, momentary inability to recall a familiar name or phone number, and at times not being able to instantly assimilate information to be memorized, such as the directions back to the interstate highway when one is lost. The subjects who commented on their difficulties with concentration attributed their problems to “senior moments,” by which they meant a lapse in memory.
Neuroscientists in Europe and North America might disagree, arguing instead that the memories of well-functioning seniors are usually relatively strong. Their problem is weakened concentration due to interference cre-ated by the growing inability to inhibit or block out previously learned but no longer relevant knowledge. When 3rd Agers were instructed to memorize
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

How the Mind Ages ❚ 47
a list of words, and forget half of them after being learned, they were both slower and less accurate than young adults with similar IQs and memory skills. Since previous testing demonstrated that all of the subjects had simi-lar scores on memory tests, it seems that problems older adults have with remembering are because of the inability to suppress distractions rather than a weakened memory.24
For nearly two decades, research psychologist Lynn Hasher and her coworkers25 have reported the adverse effects of diminished cognitive inhibi-tion among older adults on memory, reading, and solving more complicated problems. They have identified three components of cognitive inhibition that affect learning and problem solving: the access function, which denies admission of irrelevant information during new learning; the restraint func-tion, which operates when automatic responses are triggered by a familiar cue but are no longer correct; and the delete function, which suppresses information that is no longer relevant.26 Hasher’s research helps us under-stand the examples above: Gabriela’s lapse in remembering the name of a granddaughter who walks into her house unexpectedly is because of the momentary difficulty of suppressing the names of her other female grand-children; lost driver Peter’s problem focusing on the instructions back to the interstate is because he has trouble deleting the wrong directions from his mind so that he can memorize the correct ones.
Neuroplasticity
Aging is linked to diminished blood flow to the brain, reduced sensory capability, gray and white matter atrophy, reduced neurotransmitter activ-ity, synaptic shrinkage and dendritic regression, as well as less activation of the hippocampal and occipital areas and the loss of overall brain volume.27 These changes in the brain are largely responsible for age-related decline in intellectual ability. Using brain-scanning technology, cognitive neuroscien-tists in the United States, Canada, and Sweden studied the brain activity of older and younger volunteers as they were trying to recall the answers to a series of memory tests.28 As expected, the younger subjects outperformed their elders. While attempting to recall the correct answer, the older subjects showed weaker activation of portions of the brain associated with memory, especially in the hippocampal and occipital regions. Reduced hippocampal activation during mental tasks causes less-effective encoding of information to be remembered as well as less-efficient recollection at retrieval.
This explains the cognitive decline among most of the aging seniors. But, how do we account for those optimal agers whose intellectual powers remain on a par with men and women in midlife? One explanation is a
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

48 ❚ The Aging Intellect
phenomenon called neuroplasticity. Neuroplasticity is the capacity of the human brain to change in response to environmental stimulation. The effects of the external experience may be on the structure, connectivity, and functioning of the brain.29
Here is an example of neuroplasticity. In Durham, North Carolina, brain researchers at Duke University tested the theory that older subjects with good memories use more of their brains, specifically both halves of the pre-frontal cortex, when taking memory tests than do their peers with weaker recall abilities.30 In this experiment, the volunteers were asked to memo-rize several lists, including 24 unrelated word pairs (lawyer-window). Then, while they were being asked to recall this material (e.g., “lawyer-?”), PET (positron emission tomography) scans of the prefrontal cortex were carried out. The PET scans showed that mentally vigorous aging adults used more areas of their brains during memory tasks or other cognitive challenges. Specifically, older subjects with good memories used both hemispheres of the prefrontal cortex, while those with weaker recall relied on just one side. This is viewed as compensation for the age-related diminished functioning in other regions of the cerebral cortex.31
What is it that influences one 3rd Ager’s ability to activate both halves of his or her prefrontal cortex when trying to recall the word paired with “lawyer,” while another cannot mobilize more than one hemisphere? What external behavioral patterns might influence 3rd Agers to use more of their brain to pay attention, to encode and retrieve information, to visualize where in the mall lot the car is parked? The baker’s half dozen of healthy lifestyle habits described in Chapter 1 is a good start for such a list: Not smoking, exercising regularly and fighting obesity, eating healthfully, taking prescribed medication, repopulating social networks, and managing stress all link to higher intellectual functioning. To that list of activities, others have added cognitive training, meditation, treatment of mental disorders, and engaging in stimulating activities.32
An example is physical exercise. For more than a decade, psychologist Arthur Kramer and his colleagues from the University of Illinois have spear-headed research efforts to demonstrate the power of exercise to improve cognition, enhance neural activity, and increase brain volume. In two recent articles,33 they reported that 6 months of moderate levels of aerobic activity were sufficient to produce significant improvements in cognitive function—with the most dramatic effects occurring in executive control (in this case, planning, goal maintenance, working memory, and task switching). These improvements are accompanied by altered brain activity and increases in prefrontal and temporal gray matter volume that translate into a more effi-cient and effective neural system.
Might those seniors who learn a new physical and mental skill also influ-ence the structure of their brains? German neuroscientists taught a group
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

How the Mind Ages ❚ 49
of 3rd Age volunteers to juggle three balls.34 The subjects were given mag-netic resonance imaging (MRI) scans three times: prior to learning to juggle, when they had learned to juggle for at least 60 seconds, and 3 months after the study ended. The MRI scans of the trained group of elders showed an increase in gray matter in the hippocampus, the temporal area, and other regions of the cortex while they were in the process of acquiring this skill. At the 3-month follow-up, when the 3rd Agers were no longer learning a new skill, the gains in gray matter disappeared. With respect to this par-ticular skill, the increase in gray matter throughout the brain occurred only during the initial training and receded when exercise stopped. These cases suggest that neuroplasticity is activity dependent, and the apparent change in brain structure is likely to disappear when the skill is learned.
But, something had changed within these individuals. Even with their reduced gray matter volume, they could still juggle.35
Neuroplasticity is one of the exciting new ideas in the field of cognitive aging. The notion that regions of our brain may grow or become more active in response to external activities is encouraging for those aspiring to age optimally. As with most new ideas, however, much remains to be learned about the nature of neuroplasticity before its basic principles can be applied to older adults with confidence.
Here are four questions, drawn from a larger list, that need to be addressed to help us understand how learning about neuroplasticity will improve the lives of older people.36 Will the proposed linkages be confirmed in longi-tudinal studies with larger numbers of ordinary community-dwelling older adults? To what extent do changes in brain structure and activation patterns affect cognitive performance on objective measures of intellectual function-ing? To what extent are changes in the brain activity dependent on external stimulus, and if the apparent changes in neurobiological structure vanish when the external stimulus ceases (e.g., no more juggling), are the cognitive gains retained? Finally, what is the role of the intricate neural mechanisms that underlie brain plasticity? Regional activations or reductions are unlikely to be the whole story. So, in spite of the wealth of information that has accu-mulated in the past two decades, a long journey lies ahead to understand the full potential and limitations of neuroplasticity.
TheLowerEndoftheBellCurve:Age-RelatedCognitiveDecline,MildCognitiveImpairment,andDementia
Apparent in a growing number of older adults are signs of compromised intellectual functioning. These lapses are more severe than intermittent dif-
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

50 ❚ The Aging Intellect
ficulties recalling names, numbers, or things or TOT blockages. They are persistent, debilitating, and worrisome. The following are four illustrations:
Clara (73) always prided herself on her memory. For decades, she did her grocery shopping without a list. Recently, she has noticed that she is beginning to have trouble remembering. Last week, she made a quick trip to the grocery store to pick up four items for dinner and could not think of one of them when she started shopping. This is the third time this has happened in the past month. She wonders if these memory problems might be the first signs of Alzheimer’s dis-ease. Both her mother and aunt had Alzheimer’s in their 70s. Clara wonders whether she should bring her memory problem up with her doctor at her next checkup. But, he never asks her about how she is doing mentally, so maybe she does not need to worry.
At 83, Bernie still plays a good game of tennis. In fact, he still plays doubles once a week with friends 10 to 15 years his junior. In the past couple of years, however, Bernie has started to have difficul-ties remembering the score and then whether he was playing in the forehand or backhand court when they changed sides. In the past 6 months, during a break between games, the other players noticed that Bernie was uncertain who his partner was when they resumed the game. After they finished playing, the other players talked among themselves about Bernie’s memory problems and whether they should let his wife know about their concerns.
During the past year, Maurice’s three children have started to worry that their 76-year-old widower father is starting to lose his driving abil-ity, especially his navigational skills. This has never been his strength, but things are getting worse. Last summer, while visiting his son in New Jersey, Maurice volunteered to do the grocery shopping and became so lost that he had to call 911 to help him find his way back to his son’s house. Recently, Maurice admitted to his daughter that he misread a map on the way to visit a friend in Maine and “drove half-way to Canada” before he recognized the mistake and found his way back to the friend’s house. When his children bring up their worries about his driving, Maurice ignores them, saying that he is no worse now than he has always been.
Anna’s bout with H1N1 flu kept her in the hospital for more than a week before she was well enough to return home. At 84, Anna loved
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853
How the Mind Ages ❚ 51
living independently in her cozy two-bedroom condo. When an old friend came to visit Anna about a month after she returned from the hospital, the friend smelled traces of gas when she opened the door. Asked about the odor, Anna admitted that she had forgotten to light one of the gas burners the night before and only noticed the smell when she got up in the middle of the night to go to the bathroom. She immediately shut the burner off and opened the windows. Later, Anna admitted to her friend that she had forgotten to turn the oven off after cooking dinner a week earlier, and several times has left the light on over the stove. Anna tells herself that this will pass when she is fully recovered from the flu. Her friend, a retired nurse, is not so sure.
The 3rd Agers experiencing these mental lapses, and those caring for them, often wonder if they are merely examples of normally decreasing mental acuity or if they are the first stages of Alzheimer’s disease (AD). Or, are they symptoms of an “in-between condition,” called mild cognitive impairment (MCI), in which cognitive deficiencies are greater than would be expected based on age and educational background but fall short of the standards for dementia.
Before discussing MCI, we should define what is meant by the mental conditions on either side of it: age-related cognitive decline and dementia. Age-related cognitive decline is a term used by professionals to describe an intermittent pattern of problems with memory, orientation, or reasoning that are essentially benign.37 These are greater than average for the person’s age but are still considered within normal limits. This noticeable age-related weakening of mental skills may be greater in one area such as memory or involve other aptitudes such as visuospatial ability. Age-related cognitive decline is not seen as an early stage of dementia but rather as a nonpatho-logical extreme of normal cognitive aging.38
Dementia refers to the loss of mental abilities because of death or dam-age to brain cells. The most common form of dementia is AD, a devastating condition that takes away the very essence of an individual’s identity—their memory of themselves.39 In addition to memory impairment that gradu-ally increases in severity over at least a 6-month period, five other primary features distinguish AD: (a) a loss of at least one other mental ability, such as attention, calculation, motor skills, orientation, judgment, and problem solving; (b) inability to function normally in self-care, hobbies, and occu-pational, community, and social activities; (c) noticeable, gradual decline from a previous level of intellectual functioning over a period of 6 months or more; (d) exclusionary criteria, which involves ruling out other causes for the cognitive impairment, such as disease (cancer metastasizing to the
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

52 ❚ The Aging Intellect
brain), other systemic conditions (hypothyroidism), psychiatric disorder (depression), or behavioral problems (alcohol abuse); and (e) lower mental ability confirmed by history and testing.40
About one in eight Americans aged 65 or older have moderate-to-severe AD.41 As we might imagine, the proportion of 3rd Agers with AD increases with age. One estimate of the frequency of moderate and severe cases is that the frequency of AD roughly doubles every half decade after 65, for example, 65–69 (1.4%), 70–74 (2.8%), 75–79 (5.6%), 80–84 (10.5%).42
Not everyone with dementia suffers from AD. Other conditions also cause memory problems, inattentiveness, disorientation, and impaired psychomo-tor skills. Two of the most common are Lewy body dementia and vascular dementia. In their early stages, both of these conditions are difficult to dif-ferentiate from one another and from AD. Patients with Lewy body dementia are found among people with Parkinson’s disease. This condition shares with AD the gradual unremitting cognitive decline and impaired social and occu-pational functioning. Among the clinical symptoms that distinguish Lewy body dementia from AD are a relatively intact memory but with episodes of difficulty sustaining attention and handling visuospatial tasks. Other clinical symptoms may include sleep disruptions and visual hallucinations.43
Vascular dementia (formerly called multi-infarct dementia) is caused by multiple tiny strokes (or infarcts) in the brain due to transient interruption of blood flow from clogged or burst blood vessels. These accumulated infarcts cause diffuse damage throughout the brain that can lead to vascular demen-tia. Significant comorbidity with AD is found, including impairment in at least two cognitive domains. Clinical characteristics that may differentiate vascular dementia from AD are spared memory but impaired processing speed and executive functions, as well as emotional lability.44
Generations of geriatric clinicians and neuroscientists have agreed that an intermediate stage of cognitive decline exists. This stage is below normal age-based expectations but above the threshold for AD. What these experts have disagreed most about is how likely this in-between stage will lead to AD. Two examples that already have been mentioned are age-associated cognitive decline (AACD) and MCI. AACD is considered to be more likely to remain stable, whereas MCI is viewed as a transitional phase leading to dementia.45
Closer inspection of the criteria for AACD and MCI, however, finds a great deal of overlap. For example, the major identifying characteristics of both are symptoms of memory impairment or other weakened mental skills in otherwise healthy normal older adults. Both also stipulate that mental ability tests verify that someone has these conditions by scoring in the lower ranges of normal IQ but above the threshold for dementia.
Longitudinal studies of 3rd Age subjects diagnosed with either AACD or MCI confirmed the impression that there is much overlap between them.46
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853
How the Mind Ages ❚ 53
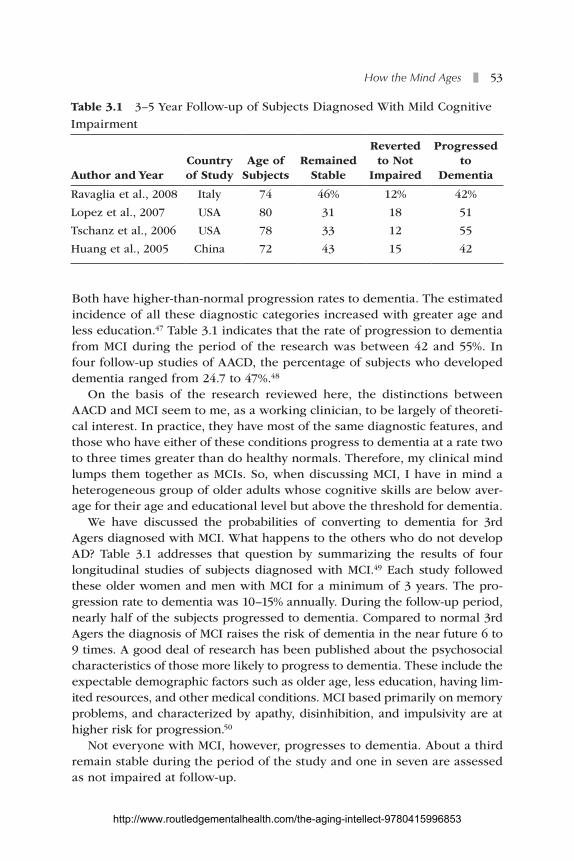
Both have higher-than-normal progression rates to dementia. The estimated incidence of all these diagnostic categories increased with greater age and less education.47 Table 3.1 indicates that the rate of progression to dementia from MCI during the period of the research was between 42 and 55%. In four follow-up studies of AACD, the percentage of subjects who developed dementia ranged from 24.7 to 47%.48
On the basis of the research reviewed here, the distinctions between AACD and MCI seem to me, as a working clinician, to be largely of theoreti-cal interest. In practice, they have most of the same diagnostic features, and those who have either of these conditions progress to dementia at a rate two to three times greater than do healthy normals. Therefore, my clinical mind lumps them together as MCIs. So, when discussing MCI, I have in mind a heterogeneous group of older adults whose cognitive skills are below aver-age for their age and educational level but above the threshold for dementia.
We have discussed the probabilities of converting to dementia for 3rd Agers diagnosed with MCI. What happens to the others who do not develop AD? Table 3.1 addresses that question by summarizing the results of four longitudinal studies of subjects diagnosed with MCI.49 Each study followed these older women and men with MCI for a minimum of 3 years. The pro-gression rate to dementia was 10–15% annually. During the follow-up period, nearly half of the subjects progressed to dementia. Compared to normal 3rd Agers the diagnosis of MCI raises the risk of dementia in the near future 6 to 9 times. A good deal of research has been published about the psychosocial characteristics of those more likely to progress to dementia. These include the expectable demographic factors such as older age, less education, having lim-ited resources, and other medical conditions. MCI based primarily on memory problems, and characterized by apathy, disinhibition, and impulsivity are at higher risk for progression.50
Not everyone with MCI, however, progresses to dementia. About a third remain stable during the period of the study and one in seven are assessed as not impaired at follow-up.
Table 3.1 3–5 Year Follow-up of Subjects Diagnosed With Mild Cognitive Impairment
Author and YearCountry of Study
Age of Subjects
Remained Stable
Reverted to Not
Impaired
Progressed to
Dementia
Ravaglia et al., 2008 Italy 74 46% 12% 42%
Lopez et al., 2007 USA 80 31 18 51
Tschanz et al., 2006 USA 78 33 12 55
Huang et al., 2005 China 72 43 15 42
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

54 ❚ The Aging Intellect
How do we understand those that do not progress to dementia during this longitudinal research? When discussing the results of these longitudinal studies of MCI patients the investigators spent little time discussing why some of their mildly impaired subjects did not progress.
Four explanations come to mind. First, making the differential diagnosis between the lower range normal intellectual functioning and MCI is diffi-cult, and experienced experts can disagree about a diagnosis while looking at the same clinical evidence.
A second explanation is that the person diagnosed with MCI may have sought and received successful treatment for his or her condition that restored or stabilized intellectual functioning.
A third possibility is normal intra-individual variation. We do not know how variable or stable MCI is within most patients. The diagnosis could have been made in some subjects when they were having a downward swing in their cognitive variability, and a not impaired evaluation could have been made when the fluctuation in their mental skills moved into posi-tive territory.
Finally, it is possible that being diagnosed with MCI mobilized some patients or loved ones to begin activities associated with not impaired cog-nitive functioning such as exercise, mental stimulation, and greater social interaction.
CognitiveAging:HowMuchIsHereditary?
How much of our mental ability is determined by heredity and how much by environmental influences? And, to what extent is our intelligence affected by the interaction between our genetic makeup and external fac-tors? For those of us interested in optimal cognitive aging, these are not trivial questions. To make the case that there are things that we can do to affect the quality of the older age we are growing into, we first have to demonstrate that environmental forces play a significant role in shaping our intellect.
Research evidence has been accumulating from studies of identical twins raised apart that provides more precise answers to the contributions of nature and nurture to our mental ability.51 Of these, the OctoTwin Study is the most interesting. Investigators in Sweden, the United Kingdom, and the United States gave mental aptitude tests to twins aged 80 and older who were adopted by different families as youngsters. Since these twins had lived apart for most of their lives, the thinking here was that the correla-tion between their IQs would be caused by genetic factors. The research-ers found that about 60% of the similarity in their IQs was attributable to heredity and the rest to environmental causes. Reports from the Swedish
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

How the Mind Ages ❚ 55
Adoption Twin Study, the Minnesota Twin Study, and other investigations found that between 50 and 60% of the factors associated with IQ are related to heredity and the rest to environmental influences.52
Among a growing number of neuroscientists today, the debate about the relative contributions to intelligence of nature and nurture is largely moot. This is because genes do not act independently. They are interactive. Every gene needs an environment in which to act.53 The environment can be external, as when stimuli from the outside world modify the structure of the brain. An illustration is research by Colcombe and his colleagues, who found that adults who exercised regularly lost less brain tissue than less-fit subjects in areas of the cortex related to memory, reasoning, and spatial ability.54
It is increasingly apparent that the heredity-environment discussion has moved from nature versus nurture to the integration of nature and nurture. Today, neuroscientists are hard at work studying neuroplasticity, seeking those specific environmental influences that affect particular gene expres-sions and alter the structure and functions of the brain.
ReflectionsandApplications
How does this knowledge help those caring for older adults? Begin by taking seriously the findings that certain mental skills will probably diminish with age, even among those aging optimally. This information provides a good starting point when asking 3rd Agers about the quality of their intellectual functions. Even optimal cognitive agers are likely to have some declining skills that concern them, and it may be comforting to know that people who are looking after them appreciate how the mind ages and wouldn’t mind hearing their concerns. The likelihood of aging optimally increases when 3rd Agers anticipate these age-related cognitive weaknesses and find ways to compensate for them.
For instance, an argument can be made that people’s worst abilities are likely to worsen with age. That is, the weakest aptitudes in midlife (e.g., visuospatial ability or reasoning) are candidates to decline more rapidly than other skills. Looking at Figure 3.4 again, we see that fluid abilities, which are slightly lower at the beginning, trend downward more rapidly than crystallized competencies.55
Consider the case of Maurice, described in the vignettes above. His visuo-spatial abilities were not strong in midlife, and his navigational skills have since worsened, especially in the last 5 years. Although he is reluctant to admit it, he knows that he is easily disoriented, has trouble finding his way to unfamiliar places, and is often relieved to arrive at his destination without getting lost. As it turned out, his children confronted him about his
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

56 ❚ The Aging Intellect
difficulty navigating. Before his trip south for the winter, they encouraged him to plan his route carefully using computer-assisted map services. For his birthday in December, they gave him a GPS (global positioning system). Maurice was able to accept his children’s help, which solved his navigational problems for now.
For me, the information about the hazards of multitasking was preaching to an already true believer. I learned this lesson the hard way. Just before my 62nd birthday, while I was talking on the telephone with a colleague, a staff assistant brought me a letter to sign. The letter was to Dan Ramsey, then the president of the Harvard Risk Management Foundation, the group that funded our research on aging doctors. I remember scanning the letter and signing it. About a week later, the letter was returned from Dan with the address circled in red with a large exclamation mark. The address of the letter, which I thought I proofed while talking on the phone, read:
Mr. Daniel M. RamseyPresidentThe Harvard Risky Management Association
Since then, it has been one thing at a time for me.Figure 3.3 contains useful clinical information for those caring for elders.
Slower processing speed affects nearly everyone, including optimal agers. Those optimally aging women and men who continue to function com-petently in their occupations and families usually know that their mental machine speed is slower than it was a decade or two earlier, and they work around this limitation by allocating more time to checking their credit card charges. When slower processing speed becomes problematic for 3rd Agers is when they have a complex decision to make.
Imagine that a 72-year-old client wants your opinion. Earlier this month, she received a form for renewing her license as a social worker and has put off deciding whether to keep working or retire. She still enjoys part-time clinical practice with developmentally disabled adults, and her coworkers want her to stay. But it has been a long winter, and she is feeling worn out and has been thinking about giving up her job. This is partly because she has been dealing with breast cancer for the last year. Although the disease is now in remission, the chemotherapy and radiation have taken a lot out of her. And, renewing her license requires a hefty payment, along with com-pleting several dozen hours of continuing education. On top of that is the malpractice insurance. The decision has to be made by the end of the week. She wants your opinion. What should she do?
Should you find yourself working with someone who wants to discuss major life issues like this, the research described in this chapter is a place to start. For instance, older adults should not be hurried when decisions are
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

How the Mind Ages ❚ 57
complicated. Making sound judgments about complex matters requiring the consideration of many factors takes longer than in middle age. The likeli-hood of a high-quality decision improves when a 3rd Ager is encouraged to set aside enough concentrated time to think about the problem, gather the relevant information, talk with confidantes, look objectively at the pluses and minuses of each option, and assess gut feelings.
The student interviews gave examples of optimal agers who experi-enced other periodic mental difficulties, including name, number, or word retrieval difficulties. In a 3rd Age population, these TOT lapses may occur two to three times a week. How can clinicians help people with TOT blockages? One option is to tell them that nine times out of ten the for-gotten word pops up spontaneously within a minute or two. Otherwise, like cures for hiccups, people have their own homemade remedies. Mine is to put the forgotten word in the back of my mind and move on to thinking about something else. The word nearly always returns within a short time. Experts on such occurrences make these recommendations: (a) Try guessing the first or last letter of the TOT word; (b) estimate the number of syllables in it; (c) think of synonyms or homonyms; and (d) if appropriate, reduce stress/preoccupation level so you can concentrate on word retrieval.56
The negative effect of distractions on memory was emphasized by the research reviewed in this chapter. Even when elders were as competent on memory tests as younger adults, they had more difficulty with the recall of material they had previously memorized because they were less effective in blocking out incorrect information. Being unable to recall a grandchild’s name or a familiar phone number, not being able to focus on information to be memorized such as the names of new neighbors, or getting lost when telling a story is not unusual among adults aging well.
What advice is there for elders who ask what they can do to maintain their concentration skills? Most of the evidence-based recommendations come from the research on age-related decline in the ability to inhibit dis-tractions. After discussing the role of suppressing distractions in memory, here are four simple strategies that 3rd Agers in our study used to retain focus: First, get right to the point. If you are telling a story, keep it short and ignore distracting side roads, no matter how attractive they are. Next, one thing at a time. If you are going to the basement freezer for ice cream, keep your mind on that task and try to block out other interesting thoughts on the way to the freezer. Third, when you cannot recall the name of a granddaughter, silently “call the roll” of grandchildren until her name comes to you. Finally, suppress other competing preoccupations when meeting new people or hearing directions so that you can concentrate on this new information.
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

58 ❚ The Aging Intellect
For the professional with clinical research interests, this chapter sug-gests a number of intriguing possibilities. Among them are these: (a) What is the frequency of mental mistakes during a 7-day period among optimally aging groups of 3rd Agers? (b) What contributes to recovery of lost names, numbers, or words? (c) To what extent might healthy lifestyle habits con-tribute to changes in brain function or structure? (d) What external factors are associated with stability or reversion to normal of individuals diagnosed with MCI?
And, of course, neuroplasticity is one of the exciting new ideas in cogni-tive aging and will be a major research area for years to come. Today, the application of imaging techniques such as PET and functional MRI scans enables neuroscientists to observe the brain in action as people solve prob-lems, as well as study the changes in brain structure that occur because of healthy lifestyle habits such as exercise.
These accolades given, it is also true that the field is in its infancy. The majority of the research has been with laboratory rodents. Studies of humans have been with small numbers. Longitudinal research with adults is just beginning. Much remains to be discovered and understood.57 A prob-lem for health care providers is that the enthusiasm for the concept of neu-roplasticity has gotten ahead of the science. Extravagant promises about reversing the aging process or remodeling our brains that come from the Internet, 60-second sound bites, and 200-word newspaper stories rarely can do justice to the complexities and to the limitations of promising sci-entific findings.
After these media reports appear, you can expect to be approached by elders in your care with questions about whether these new mental games, physical exercises, diets, or other endeavors might be helpful to their intel-lect. Here are several thoughts to keep in mind: Information that activates the “doctor within” is not a bad thing, even if the promising new activity or idea has a limited scientific basis. As long as the activity is safe, I see no harm in encouraging older clients to pay attention to things that may help them sustain their intellectual powers. Moreover, most cognitive skills can be improved through training. Although these enhanced aptitudes may not generalize to other tasks, and they tend to diminish rapidly with disuse, engaging in new challenges is good for our clients if only to prove that they can still do it. And, it does not matter either if the benefits are not long last-ing. Life is lived in the short run.
An important application of these findings is making a decision about when a referral to a medical professional should be made to evaluate the mental status of someone in your care who is exhibiting signs of cognitive impairment. Recognizing weakened mental abilities in older adults is not difficult, but it can be extremely difficult to judge accurately how impaired a person is likely to be on the basis of a single symptom such as declining
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

How the Mind Ages ❚ 59
memory or disorientation. In these cases, a referral is necessary to a pri-mary health care provider, who can send the patient for a consultation to a neurologist or neuropsychologist trained to differentiate normal cognitive decline from MCI and dementia. Making these distinctions requires a com-plete evaluation that usually includes a detailed history, physical examina-tion, cognitive testing, and sometimes brain scans.
For those caring for older adults with worrisome symptoms, the challenge is deciding how to proceed. It is a good bet that many 3rd Agers exhibiting visible signs of mental decline will be unenthusiastic about a referral to a specialist in diagnosing dementia. At the heart of their resistance may be a version of this fear: “Why do I want to know whether I have Alzheimer’s dis-ease? It’s incurable. Since nothing can help me, why do I want to know?”
Here are two answers to this question: First, the symptoms exhibited by the four subjects described in this chapter do not inevitably result in the diagnosis of dementia. Sometimes, the results are comforting and can be easily resolved. While she has experienced normal cognitive decline, Clara’s evaluation and test scores showed her to be above average compared to other septuagenarians. The only recommendation for her is to make a list before she shops. Maurice’s diagnosis was age-related cognitive decline, but his navigational problems can be mitigated by more thorough planning and using a GPS.
The second reason a referral to a specialist can be helpful is that early diagnosis leads to a higher probability of a positive outcome. The neurologi-cal evaluation of both Bernie and Anna resulted in the diagnoses of MCI. Even with this diagnosis, there is reason for hope. Table 3.1 reminds us that a high percentage of adults diagnosed with MCI did not progress to demen-tia during a 3- to 5-year follow-up period. And, a small number, about one in seven, return to normal. Also, new psychoeducational and pharmaceuti-cal treatments with the potential for stabilizing or reversing MCI are coming to the market as these words are written. For instance, a 2009 report from a large multicenter study demonstrated that MCI subjects who received 10 sessions of cognitive training gained as much as normal participants in reasoning and processing speed and maintained this improvement for 2 years.58 So, there is justification for a cautiously positive attitude even when the diagnosis is MCI. Art’s story59 is an example.
Art
I am a retired physician and an emeritus professor of medicine. Also, I have Alzheimer’s disease. My diagnosis was suspected by my wife and confirmed by my internist. All the while, I was in total denial (a com-mon failing when doctors are patients). After doing a few tests of my
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

60 ❚ The Aging Intellect
memory in the office, the doctor ordered other tests and a brain scan. The diagnosis was mild Alzheimer’s disease.
I was started on a medicine that has been used for many years and has many side effects. I had a few Alzheimer’s patients in my practice who had taken this medicine with no benefit. My doctor had me con-tinue it, though I was kicking and screaming, and the side effects even-tually disappeared. This drug was continued, and another was added later on, which turned out to be helpful.
In 2 months, I was much better, and I am now close to normal. At my worst, I have difficulty speaking, do not know the names of my grandchildren or my doctor, can neither add nor subtract or find my way home. I am considered one of the rare lucky ones.
Looking back, I now recognize my memory problems arose 10 years ago when I was 76. I chaired a monthly program about medical ethics. I knew most of the speakers and found it easy and enjoyable to introduce them. That year, I began to be more forgetful. I had to read the prepared material to make the introductions. My memory for names started to slip, never faces. “Senior moments,” I concluded.
Over the last decade, I had two transitory ischemic attacks or small strokes, and my mental difficulties worsened. The final blow was the occasion 1 year ago when I was receiving a citation for service in my hospital. I stood up to thank them and found that I could not say a word. “Aging brain,” I said and sat down. That is when I saw my doctor, and the diagnosis of Alzheimer’s disease was made.
For some reason—no one knows why—my condition has improved. I am still not back to normal, and I have bad days, but I can continue to live at home with the help of my wife and the care of my doctor.
I am learning many things since being improved that have helped me. I would like to share with you: When you want to recall things, carry a little note pad and write it down. When you cannot remember a name, make a little joke and ask them to repeat it—then write it down. Read books. Take walks. If you cannot walk, exercise in bed. Draw and paint. Garden, if you can. Do puzzles and games. Try new things. Organize your day. Learn to prepare food, eat, dress, wash, and go to bed in an efficient way. Eat a healthy diet that includes fish twice a week, fruits and vegetables, and omega 3 fatty acids.
Finally, do not be ashamed to talk to your friends and your family. People want to help you.
To my knowledge, no one has compared cases like Art’s that do not convert to dementia to those individuals diagnosed with MCI who do prog-ress as expected. What a research project this would be. Certainly, in Art’s case the medications played a central role. But, what about some of the
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853

How the Mind Ages ❚ 61
suggestions Art has made, as well as other healthy lifestyle habits practiced by people aging optimally that could be examined along with dozens of others? Art was fortunate in having a doctor who was willing to continue working with him when he had to be convinced to take medication he did not believe would help him and who must have encouraged him to come up with ideas of his own to help himself.
Knowing that dementia is not a certainty for everyone with MCI can inspire hope among those in your care. Having a health care provider who has some ideas about activities that might retard the progression to demen-tia can also stimulate them to come up with ideas of their own that will make a difference in their well-being.
Still, the majority of those diagnosed with MCI or mild AD will progress toward more severe impairment. What you do then depends on your role, your other responsibilities, and your relationship with these clients. Overall, you want to be sure that those with cognitive impairment have someone to care for them. Sometimes, these are professionals with experience working with such cases. Often, however, no one is available. There will be some people newly diagnosed with cognitive impairment who may feel aban-doned if you suddenly terminate your relationship with them because you are not an expert. You can provide them a great deal of comfort if you accompany them as they cope with the challenges in this next phase of their lives.
http://www.routledgementalhealth.com/the-aging-intellect-9780415996853