NEW WEAPONS IN THE WAR OF CANCER Lodovico Balducci M.D. H. Lee Moffitt Cancer Center Tampa, Florida.
43
NEW WEAPONS IN THE WAR OF CANCER Lodovico Balducci M.D. H. Lee Moffitt Cancer Center Tampa, Florida
-
Upload
liliana-burns -
Category
Documents
-
view
215 -
download
0
Transcript of NEW WEAPONS IN THE WAR OF CANCER Lodovico Balducci M.D. H. Lee Moffitt Cancer Center Tampa, Florida.

NEW WEAPONS IN THE WAR OF CANCER
Lodovico Balducci M.D.
H. Lee Moffitt Cancer Center
Tampa, Florida

OK! So Now Are We Ready to Select Drugs for Patients in a More Personalized Way?

The war onCancer startedWith weapons ofMass destruction

ContinuedWith conventionalweapons

And now has discovered Smart weapons

Personalized oncology
• Targets of treatment
• Predictive factors
• Individual rescue

Smart weapons in medical oncology
• Hormones• Monoclonal antibodies• Inhibitors of the signal transduction cascade• Drugs that reverse epigenetic changes• Others Thalidomide derivatives Proteosome inhibitors Antisense Prodrugs activated in neoplastic cells Drugs that reverse multidrug resistance


General issues related to the use of “smart drugs.”
• End-point of phase I trials: MTD vs target inhibition• End point of phase II trials: response rate vs stable
disease• Duration of treatment• Combinations vs single agents• Combination with chemotherapy• Single vs multiple inhibitors• Vertical and Horizontal inhibition of the signaling cascade• Mechanisms of resistance (the cancer guerrilla)• Enough patients for clinical trials

GROWTH FACTOR
RECEPTORTKI
PI3K
PDKI AKT
RAS NF1 (RAS-GAP)PTEN
TUBERINFOXOGsk3
BADMDM2
RHEB GTP RHEBGDP
mTOR
LKB1AMPK
HIF
DECREASEDTRANSCRIPTION
INCREASEDCELLPROLIFERATION
ACTIVATIONBcl2SUPPRESSION
p53

Issues of “smart drugs” in the older person
• Absorption
• Drug interactions
• Unexpected complications

A disease with multiple targetsIs an incurable disease
Checov

Combinations in Lung Cancer
IGF-1RInhibitor
Drug XDrug X
EGFREGFRInhibitorInhibitor
VEGF Inhibitor
mTORInhibitor
EGFR Inhibitor
But which ones?But which ones?
Designed for a Designed for a population, not an population, not an individual patient. individual patient.
But which ones?But which ones?
Designed for a Designed for a population, not an population, not an individual patient. individual patient.

STRATEGIES
• ANGIOGENESIS INHIBITORS + CHEMOTHERAPY
• ANGIOGENESIS INHIBITORS + TARGETED THERAPY
• CHEMOTHERAPY AND TARGETED THERAPY
• HORIZONTAL INHIBITION
• VERTICAL INHIBITION

Breast cancer: bevacizumab + paclitaxel

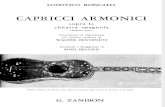
DTIC +/- Sorafenib Trial: PFS
1.00
0.75
0.50
0.25
0.00
1.00
0.75
0.50
0.25
0.0000 14 14 29 29 43 43 57 57 71 71
Weeks From RandomizationWeeks From Randomization
Pro
gre
ssio
n-f
ree
Su
rviv
al P
rob
abil
ity
Pro
gre
ssio
n-f
ree
Su
rviv
al P
rob
abil
ity
86 86
Sorafenib + DTIC (39 events)Sorafenib + DTIC (39 events)
Median: 21.1 weeks (95% CI: 16.0, 28.0) Median: 21.1 weeks (95% CI: 16.0, 28.0)
Placebo + DTIC (42 events)Placebo + DTIC (42 events) Median: 11.7 weeks (95% CI: 6.1, 17.9) Median: 11.7 weeks (95% CI: 6.1, 17.9)
Hazard Ratio = 0.665 (95%CI: 0.428, 1.034)p = 0.068
Hazard Ratio = 0.665 (95%CI: 0.428, 1.034)p = 0.068
McDermott et al. J Clin Oncol, in press.

Lapatinib pazopanib superior to lapatinib alone

Combinations that do not work
• Bevacizumab erlotinib in RCC
• Bevacizumab+ cetuximab (CAIRO2)
• Erlotinib + platinum chemotherapy


Gemzar and erlotinib vs Gemzar erlotinib and bevacizumab

COMBINATION OF AGENTS TARGETING THE SIGNAL TRANSDUCTION CASCADE
• VERTICAL BLOCKADE
• HORIZONTAL BLOCKADE
• OVERCOMING RESISTANCE

HIFHIF
KDRKDR
? TOR Inhibitor (temsirolimus or RAD 001)? TOR Inhibitor (temsirolimus or RAD 001)
BevacizumabBevacizumab
Sorafenib Sunitinib Sorafenib Sunitinib
Vertical Combinations- Targeting of VEGF at multiple levels
HIF
VEGF

Temsirolimus plus BevacizumabMerchan et al., ASCO 2007
-80
-60
-40
-20
0
20
40
* = PD (Clinical progression)
**
Dose Level 1Dose Level 1Dose Level 2Dose Level 2
Pe
rce
nt
Re
du
cti
on
Pe
rce
nt
Re
du
cti
on
Maximum Percent Reduction of Target Lesions by Patient
Maximum Percent Reduction of Target Lesions by Patient

Combination Targeted TherapyFor Advanced NSCLC
Herbst RS et al. J Clin Oncol. 2005;23:2544-2555.
Inhibitor Erlotinib BevacizumabBevacizumab
Mechanism
Inhibits tumor cell growth and blocks synthesis of angiogenic proteins (e.g., bFGF, VEGF, TGF-a) by tumor cells
Inhibits endothelial cells from responding to the angiogenic protein VEGF
bFGFVEGFTGF-a
bFGFVEGFTGF-a
Endothelial cellsEndothelial cellsTumorTumor

Median PFS(months) 6 month PFS
rate (%)
12 month OS rate
(%)
4.4 33.6 57.1
4.8 30.5 53.6
3.0 21.5 31.8
Bevacizumab + Erlotinib (n=39)Bevacizumab + Erlotinib (n=39)
Chemotherapy(n=41)
Chemotherapy(n=41)
Chemotherapy+ Bevacizumab
(n=40)
Chemotherapy+ Bevacizumab
(n=40)
Previously treated
advanced non-squamous
NSCLC (n=120)
Previously treated
advanced non-squamous
NSCLC (n=120)
Herbst RS et al. J Clin Oncol. 2007;25:4743-4750.
• Randomized, Multicenter Study • Primary endpoint : safety and preliminary efficacy (PFS)• Secondary endpoints: ORR (+ duration); duration of survival
Phase 2: Bevacizumab With Chemotherapy Or Erlotinib in
Advanced NSCLC

Example of vertical inhibition: lapatinib + trastuzumab

Continue
CR treatment for
Week 1 2 3 4 5 6 7 8 9 PR 12 months or until
Stable tumor progression
A A A A Reevaluate
S Progression
Off treatment
Doses:Bevacizumab 3mg/kg, 5 mg/kg, 10mg/kg, IV infusion, q 2 weeksSorafenib- 200mg, 200mg BID, 400mg BID daily PO
Continue
CR treatment for
Week 1 2 3 4 5 6 7 8 9 PR 12 months or until
Stable tumor progression
A A A A Reevaluate
S Progression
Off treatment
Doses:Bevacizumab 3mg/kg, 5 mg/kg, 10mg/kg, IV infusion, q 2 weeksSorafenib- 200mg, 200mg BID, 400mg BID daily PO
Enhanced sorafenib-type toxicity
Enhanced sorafenib-type toxicity
Phase I / II Sorafenib + Bevacizumab Trial: Treatment
Regimen
Sosman et al

Targeted therapy in the elderly
• Effectiveness
• Toxicity

Copyright © American Society of Clinical Oncology
Ramalingam, S. S. et al. J Clin Oncol; 26:60-65 2008
Fig 1. Kaplan-Meier curves for (A) overall survival for elderly (PC v PCB), (B) PFS for elderly (PC v PCB), (C) combined overall survival by age groups (PC + PCB), and (D) combined PFS by age groups (PC +
PCB)

TOXICITY OF PC AND PCB IN PATIENTS 70+Ramalingam et al, JCO, 2008, 26, 60-65
TOXICITY PC PCB P
HEMATO NEUTROPENIA
FEVER
THROMBOCYTO
22
0.9
0
34
6.2
3.5
.06
0.03
.06
NON-HEMATOHYPERTENSION
PROTEINURIA
HEMORRHAGE
NAUSEA
ANOREXIA
.9
0
1.7
0
0.9
6.2
7.9
7.9
4.4
7.9
.03
.002
.03
.03
.01

TOXICITY PC ABD PCB IN PEOPLE 70+ AND YOUNGER PATIENTS
RAMALINGAM ET AL, JCO, 2008, 26, 60-65
TOXICITY PCB PC
>70 <70 >70 <70
NEUTROPENIA
MELENA
PROTEINURIA
WEAKNESS
NEUROPATHY
DIZZINESS
WORST GRADE TOXICITY
TRD
34 22
3.5 0
7.9 1.3
7.8 2.2
3.5 0.6
7.9 1.6
87 71
6.3 2.6
.02
.005
.001
.02
.05
.003
.001
.08
22 15
1.8 0
0 0
4.3 3.1
2.6 1.5
2.6 1.5
65 61
1.8 0
.08
.07
.07

Toxicity of cetuximab in the elderlyBouchachada et al, Crit Rev oncol
Hematol, 2008
• Skin Rash 75% (11% grade 3)
• Diarrhea 80% (20% grade 3 and 4)

Copyright © American Society of Clinical Oncology
Lin, W.-L. et al. J Clin Oncol; 26:2779-2780 2008
Fig 1.

Copyright ©2008 American Association for Cancer Research
Murgo, A. J. et al. Clin Cancer Res 2008;14:3675-3682
Figure 1">

Copyright ©2008 American Association for Cancer Research
Murgo, A. J. et al. Clin Cancer Res 2008;14:3675-3682
Figure 2">

Copyright ©2008 American Association for Cancer Research
Hoering, A. et al. Clin Cancer Res 2008;14:4358-4367
Figure 1">

Copyright ©2008 American Association for Cancer Research
Hoering, A. et al. Clin Cancer Res 2008;14:4358-4367
Figure 2">

Conclusions
• Targeted therapy involves:Agents directed to a specific targetTargets predictive of response to treatmentOvercoming resistance• Targeted therapy has been very
successful in situations where a single or few targets are responsible to maintain the disease (CML, HER2 positive breast cancer; some B cell malignancies)

Conclusions
• The combination of antiangiogenesis agents with cytotoxic chemotherapy has increased the activity of chemotherapy in breast, colon, and lung cancer and in melanoma

Conclusions
• The combination of 2 or more targeting agents seems to be more effective and safer when the inhibition is vertical, at least in the case of inhibition of the signal transduction cascade.

Conclusions
• The plethora of new agents require more diversified clinical studies: this include phase 0 studies to test the doses providing full inhibition of the target and randomized phase II studies to establish the value of stable disease
• Scarcity of patients will make the need of including older patients in clinical trials more compelling

Conclusions
• Data on toxicity of targeted agents in older individuals are limited: the risk of thrombosis with avastin and of serious cutaneous reactions with cetuximab appears to increase with age

A CASE FOR GERIATRIC ONCOLOGY
• A WORLD GOVERNED BY TECHNOLOGY IS A
WORLD OF SLAVES.
G. Bernanos: La France contre les robots