New Staging of Esophageal Caner - based on the 7 th edition of the AJCC Cancer Staging
52
New Staging of Esophageal Caner - based on the 7 th edition of the AJCC Cancer Staging Hyun-Sung Lee, MD, PhD Center for Lung Cancer Research Institute and Hospital National Cancer Center, Korea
description
New Staging of Esophageal Caner - based on the 7 th edition of the AJCC Cancer Staging. Hyun-Sung Lee, MD, PhD Center for Lung Cancer Research Institute and Hospital National Cancer Center, Korea. Disclosure. No financial disclosures - PowerPoint PPT Presentation
Transcript of New Staging of Esophageal Caner - based on the 7 th edition of the AJCC Cancer Staging

New Staging of Esophageal Caner
- based on the 7th edition of the AJCC Cancer
Staging
Hyun-Sung Lee, MD, PhD
Center for Lung CancerResearch Institute and HospitalNational Cancer Center, Korea

Disclosure
• No financial disclosures
• The presentation on a new AJCC staging is based on the AJCC Cancer Staging Manual 7th Edition
• Presentation slides were kindly provided by Dr. Young Tae Kim, Seoul National University in 2009 Esophageal Cancer Symposium(held in National Cancer Center)

과거 6 차 AJCC/UICC staging system
• 식도암의 병기는 단순히 T, N, M 병기 분류에 따른 해부학적 진행 정도에 따라 정하여 졌기 때문에 실제 임상에서의 생존율과 병기에 따른 생존율의 구분이 명확하지 않았다
• 병리조직학적 분류 , 암의 생물학적 양상 , 위치 등도 반영되지 않았다
• 식도 - 위 경계부암 (EGJ cancer) 과 관련되어 위암의 병기와 조화롭게 분류되지 않았다

새로운 병기 시스템
• AJCC Lung and Esophageal Task Force
• 임상자료들을 기반으로 하는 새로운 병기를 구상
• Worldwide Esophageal Cancer Collaboration (WECC)
• 3 개 대륙의 13 개 센터의 임상자료들을 근간
• 7 차 AJCC/UICC 식도암 병기를 제안

Worldwide EsophagealCancer Collaboration (WECC)
• USA(14)
Cleveland Clinic(T. W. Rice)
Fox Chase CC(W.J. Scott)
Indiana U(K. A. Kesler)
MD Anderson(W. Hofstetter, S.G. Swisher)
MGH(H. A. Gaissert, D. J. Mathisen)
Mayo Clinic(M. S. Allen)
Medical U South Carolina(C. E. Reed)
Memorial Sloan-Kettering(V. W. Rusch)
Oregon Health & Science U(J. G. Hunter)
U Alabama at Birmingham(R. Cerfolio)
U Michigan(M. B. Orringer)
U Pennsylvania(J. C. Kucharczuk)
U Pittsburgh Medical Center(J. D. Luketich)
U Rochester(T. J. Watson)
• Europe(2)
Helsinki U(J. A. Salo)
U Z Leuven, Belgium(T. E.M.R. Lerut)
• Orient(2)
Fourth Hospital of Hebei Medical U, China(Long-Qi Chen)
U Hong Kong(Simon Law, John Wong)
• Canada(2)
Toronto GH(G. Darling)
U Montreal(A. Duranceau)

제 7 차 AJCC/UICC staging system
• 식도암 또는 식도 - 위 경계부암 환자
• 수술만 시행 받고 수술 전 혹은 수술 후 보조치료를 받지 않은 환자
• 사망 여부 및 사망 원인이 확실히 밝혀진 4,627 명의 환자들의 임상데이터
• Risk-adjusted random-survival-forest analysis

Patient characteristics
T.W. Rice, Worldwide esophageal cancer collaboration, Diseases of the Esophagus 2009;22:1-8

Cancer characteristics (1)
‡ pT1a in 262 and pT1b in 244 among 506 in whom this distinction was made.§ pM1a in 104 and pM1b in 122 of 226 in whom this distinction was made.
T.W. Rice, Worldwide esophageal cancer collaboration, Diseases of the Esophagus 2009;22:1-8

Cancer characteristics (2)
T.W. Rice, Worldwide esophageal cancer collaboration, Diseases of the Esophagus 2009;22:1-8

Overall survival
T.W. Rice, Worldwide esophageal cancer collaboration, Diseases of the Esophagus 2009;22:1-8
30 days 98%1 year 78%5 year 42%10 year 31%

Slide from YT Kim

Survival stratified by pathologic classification
N M

Slide from YT Kim

새로운 식도암 병기 변경 요약• 종양의 위치를 단순화
• Esophagogastric junction(EGJ) 과 stomach 근위부 5cm 이내의 병변을 포함
• Tis 에 대한 재정의 ( 再定義 )
• T4 를 T4a/T4b 로 세분화
• Regional lymph node 의 재정의 ( 再定義 )
• N 병기를 전이된 regional lymph node 수에 따라 분류
• M 병기의 재정의 ( 再定義 ) : ( 기존 M1a/M1b 개념 소실 )
• Squamous cell carcinoma 와 adenocarcinoma 의 병기 설정을 구분하여 표기
• 초기 병기에서는 분화도 (Grade) 를 병기 설정 요소로 도입

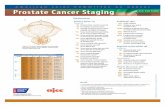
Primary site of esophageal cancer based on proximal edge
of tumor
Anatomic Name
EsophagealLocation
Anatomic Boundaries
Typical esophagectomy
Cervical Upper Hypopharynx-sternal notch
15 to <20cm
Thoracic UpperMiddleLower
Sternal notch-azygos veinLower border of AV-IPVLower border of IPV to EGJ
20 to <25cm25 to <30cm30 to <40cm
Abdominal LowerEGJ/cardia
EGJ to 5cm below EGJEGJ to 5cm below EGJ
40-45cm40-45cm

SurvivalUpper extent of cancer in the
esophagus

Esophageal wall• Mucosal layer
Epithelium(m1)
Lamina propria(m2)
Muscularis mucosae(m3)
• Submucosal layer
Inner(sm1), middle(sm2), outer thirds(sm3)
• Muscularis propria layer
Inner circular & outer longitudinal muscle layer
• No serosa

T4 lesion
• T4a; 식도암이 직접 침범한 경우에도 절제가 가능한 구조물
pleura, peritoneum, pericardium, diaphragm
• T4b; 완전 절제가 불가능한 구조물
aorta, carotid vessels, azygos vein, trachea, left main bronchus, vertebral body

Lymphatics
• Intramural network
• longitudinal 하게 전파되는 특징
• 림프계가 submucosa 에 집중되어 있기는 하지만 , lymphatic channel 은 mucosal layer 의 lamina propria에도 존재하기 때문에 mucosa 에만 국한된 암이라도 하더라도 림프절 전이가 일어날 수 있다

N descriptor

LN mappingNode number Node name Location
1 Supraclavicular nodes above suprasternal notch and clavicles
2R Right upper paratracheal nodes between intersection of caudal margin of innominate artery with trachea and the apex of the lung
2L Left upper paratracheal nodes between the top of aortic arch and apex of the lung
3P Posterior mediastinal nodes upper paraesophageal nodes, above tracheal bifurcation
4R Right lower paratracheal nodes between intersection of caudal margin of innominate artery with trachea and cephalic border of azygos vein
4L Left lower paratracheal nodes between top of aortic arch and carina
5 Aortopulmonary nodes subaortic and para-aortic nodes lateral to the ligamentum arteriosum
6 Anterior mediastinal nodes anterior to ascending aorta or innominate artery
7 Subcarinal node caudal to the carina of the trachea
8M Middle paraesophageal lymph nodes from the tracheal bifurcation to the caudal margin of the inferior pulmonary vein
8L Lower paraesophageal lymph node from the caudal margin of the inferior pulmonary vein to the EGJ
8R, 9 Pulmonary ligament nodes within the inferior pulmonary ligament
10R Right tracheobronchial nodes from cephalic border of azygos vein to origin of RUL bronchus
10L Left tracheobronchial nodes between carina and LUL bronchus
15 Diaphragmatic nodes lying on the dome of the diaphragm and adjacent to or behind its crura
16 Paracardial nodes immediately adjacent to the gastroesophageal junction
17 Left gastric nodes along the course of the left gastric artery
18 Common hepatic nodes along the course of the common hepatic artery
19 Splenic nodes along the course of the splenic artery
20 celiac nodes at the base of the celiac artery

Supraclavicular Highest mediastinal
Upper paratracheal
Lower paratracheal
Posterior mediastinal
Upper periesophageal

Tracheal bifurcation
Subcarinal
LowerPeri-
esophageal
Caudal margin of
Inferior pulmonary vein

Left cardial
Right cardial
Lesser curvature
Left gastric
Celiac
Common hepatic

Recurrent laryngeal lymph node chain
Right upper paratracheal LNs Left upper paratracheal LNs
Trachea retraction
Innoinate a.

Common hepatic & celiac LNs

Left gastric LNs

Optimum lymphadectomy for esophageal cancer
• 7 차 AJCC/UICC staging system 에서는 각각의 T 병기에 따라
• pT1 의 경우 10 개
• pT2 의 경우 20 개
• pT3, pT4 에서는 30 개 이상의 림프절 절제가 최대 생존율을 보장할 수 있음을 제안
• 이러한 림프절 절제술은 결국 환자의 morbidity 와 근치적 절제술 여부 등을 고려하여 그 범위가 결정되어야 할 것이다
Rizk NP, et al. Annals of Surgery 2010;251:46-50

Distant metastatic sites
• 이전의 pM1a 및 pM1b 분류가 없어지고
• 원격 장기에 전이가 있는 경우 pM1 으로 분류

Survival according to histopathologic cell type

Slide from YT Kim

Staging system; Squamous cell carcinoma
AnyAny0N3AnyAnyAny0Any4b
AnyAny023IIIBAnyAny004aAnyAny013AnyAny021-2IIIAAnyAny011-2
Lower1002-3Any2-3001IBAny1001IAAny100is (HGD)0
Upper, middle2-3002-3IIBLower2-3002-3
Upper, middle1002-3IIA
Any
Any
G
Any1AnyAnyIV
Any01-24aIIIC
LocationMNTStage

Slide from YT Kim

GMNTStage
Any0N3Any
Any0Any4b
Any023IIIB
Any004a
Any013
Any021-2IIIA
1-2002
3001IB
1-2001IA
100is (HGD)0
Any011-2
Any003IIB
3002IIA
Any
Any
1AnyAnyIV
01-24aIIIC
Staging system; Adenocarcinoma

Slide from YT Kim

Stage T N M Histology Grade Location
0 is(HGD) 0 0 Any Any Any
I A 1
1
0
0
0
0
SqCC
Adenoca
G1
G1-2
Any
Any
B 1
1
2-3
2
0
0
0
0
0
0
0
0
SqCC
Adenoca
SqCC
Adeno
G2-3
G3
G1
G1-2
Any
Any
Lower
Any
II A 2-3
2-3
2
0
0
0
0
0
0
SqCC
SqCC
Adenoca
G1
G2-3
G3
Upper, middle
Lower
Any
B 2-3
1~2
3
0
1
0
0
0
0
SqCC
Any
Adenoca
G2-3
Any
Any
Upper, middle
Any
Any
III A 1~2
3
4a
2
1
0
0
0
0
Any
Any
Any
Any
Any
Any
Any
Any
Any
B 3 2 0 Any Any Any
C 4a
4b
Any
1-2
Any
3
0
0
0
Any
Any
Any
Any
Any
Any
Any
Any
Any
IV Any Any 1 Any Any Any
New Staging Grouping

Application of newly proposed staging system for Esophageal Squamous Cell
Carcinoma
National Cancer Center, Korea

Patients• March 2001 ~ April 2010
• 592 esophagectomy for esophageal cancer
• Exclusion criteria
- neoadjuvant treatment
- cervical esophageal cancer
• Cohort of 492 patients in this study

Patient characteristics(1)Median age (range) 65.0 yrs (range 41-93 yr)
Gender (%)
Male 469 (95.3)
Differentiation (%)
Well 58 (11.8)
Moderate 353 (71.7)
Poor 73 (14.8)
CIS 8 (1.6)
Location (%)
Upper 125 (25.4)
Middle 148 (30.1)
Lower 216 (44.5)
T status (%)
Tis 8 (1.6)
T1 162 (32.9)
T2 51 (10.4)
T3 227 (46.1)
T4a 8 (1.6)
T4b 36 (7.3)

Patient characteristics(2)
N status (%)
N0 200 (40.7)
N1 123 (25)
N2 112 (22.8)
N3 57 (11.8)
No. of LNs 45 ± 18 (3-129)
TNM stage (%)
0 8 (1.6)
IA 16 (3.3)
IB 104 (21.1)
IIA 25 (5.1)
IIB 83 (16.9)
IIIA 91 (18.5)
IIIB 74 (15.0)
IIIC 90 (18.3)
IV 1 (0.2)

Overall survival30 days 97.3%1 year 93.2%5 year 50.8%

Overall survival (T factor)
Tis
T1
T2
T3
T4b
T4a

Overall survival (N factor)
N0
N1
N2
N3

Overall survival (Location)
N3
Lower
Mid
Upper
p=0.124

Overall survival (Grade)
N3
p=0.085
WDMD
PD

Stage groupingStage 0
Stage IBStage IIA
Stage IIB
Stage IIIA
Stage IIIB
Stage IIICStage IV
Stage IA

Conclusion 1• New staging system in which the number
of lymph node metastasis is the important prognostic factor revealed the discrete survival curves among stage III esophageal cancer
• Stage IA and IIA had the low proportions in the new staging system. Also, there was no significant differences between IB and IIA/B, which lead the overlay of the survival curves

Conclusion 2• However, subgroup analysis of the survival
according to the grade or location in early esophageal squamous cell carcinoma did not show the significant differences
• New staging system has the merit to discriminate the stage III system in esophageal squamous cell carcinoma. However, system is too complex d/t five characteristics. It seems that new staging system is not yet perfect

Limitation of the new staging system
• 수술 전후 항암이나 방사선치료가 없이 식도절제술을 시행한 식도암의 pT, pN, pM 병기를 근간으로 하였기 때문에 , 수술을 시행하지 않은 환자나 수술에 따른 위험도가 높아 수술이 불가능하였던 환자 , 근치적 수술 없이 개흉술만 시행한 환자들은 이 자료에서는 제외
• 특히 pT4 또는 pM1 병기를 보이는 환자에서 다른 치료 없이 수술만 시행 받은 환자는 굉장히 선택된 경우
• T1a/T1b data; incomplete
• Uncertain if celiac nodes included
• Cervical esophageal cancers: Not represented

Future perspectives
• 8th edition AJCC/UICC: 2016
• Stage grouping
• Prospective data collection
• Add new centers including Japan and Korea
• Advanced stages (inoperable cases)
• Further refined data-driven staging
• Individual patients based approach
• Patient-specific (personalized) prognostication and strategic decision tool; molecular markers

Thank you for your attention!