New Patient Introduction Packet & Intake Form III Aura Laser Program Reiki ... endocrine, and immune...
14
Fern Life Center 410 Newport Way NW, Suite B Issaquah, Washington 98027 Phone: 425-391-3376 www.FernLifeCenter.com FERN LIFE CENTER 410 Newport Way NW Suite B Issaquah, Washington 98207 Ph: 425-391-3376 Fax: 425-391-3378 www.FernLifeCenter.com Integrating modern medicine, Functional Medicine and the ancient practices of Ayurveda Medical Provider: Dr. Keesha Ewers Services: Ayurvedic Lifestyle Management Bioidentical Hormone Replacement Chronic Disease Management Colon Hydrotherapy Enneagram Consultations Far Infrared Sauna Healthy You Radio! Heart-Centered Clinical Hypnotherapy Heavy Metal Detoxification High-quality Herbs & Supplements Ideal Protein Weight Loss Program Just Stop Smoking! Massage Medically Guided Detoxification Meditation Nutrition Pancha Karma Primary Care PTL III Aura Laser Program Reiki Specialty Lab Testing Wellness & Personalized Health New Patient Introduction Packet & Intake Form Thank you for your interest and welcome to Fern Life Center! We are a full spectrum medical clinic and the first integrative medicine center on Seattle’s Eastside. Our mission is to support you to venture beyond mind/body/spirit medicine into transformative wellness. This packet provides the follow information and forms: 1. Demographics 2. Financial agreement 3. HIPAA (confidentiality) & Consent to Treat 4. Health history 5. Map & directions to our clinic, hours of operation and contacts Please read and complete all forms and bring them with you to your first visit. What is integrative medicine? Dr Keesha Ewers our medical provider brings modern medicine, progressive western medicine and traditional healing to every patient visit. Both are Family Nurse Practitioners licensed by the State of Washington to provide primary care, prescribe medications, order and interpret lab tests and refer to specialists. Both have also completed training in Ayurveda and are Functional Medicine providers. About Ayurveda: “Considered by many scholars to be the oldest healing science, Ayurveda is a holistic approach to health that is designed to help people live long, healthy, and well balanced lives. The basic principle of Ayurveda is to prevent and treat illness by maintaining balance in the body, mind, and consciousness through proper drinking, diet, and lifestyle, as well as herbal remedies.” - A.D.A.M. About Functional Medicine: “A newer approach to patient care which is said to assign a central role to gastrointestinal, endocrine, and immune system interactions with environmental factors, set at the level of the individual, to determine health.” Integration also exists between all the different specialty providers at Fern Life Center. Your treatment plan may include nutrition consultations, massage, Reiki, colon hydrotherapy, detoxification and other therapies. We are proud and happy to work in community as a team. Please see the sidebar at left for a full listing. Fern Life Center provides a space for community education, blissful rejuvenation and spiritual renewal. Wherever you are on your path, we encourage you to access your own wisdom...leading to greater self-awareness and lasting healing. Thank you for having us along on your journey, we look forward to serving you! Why the fern? This easily recognizable species is an abundant native of the Pacific Northwest. Like the fern, we grow and flourish as we unfurl toward light and that process is our natural way.
Transcript of New Patient Introduction Packet & Intake Form III Aura Laser Program Reiki ... endocrine, and immune...
Fern Life Center 410 Newport Way NW, Suite B Issaquah, Washington 98027 Phone: 425-391-3376 www.FernLifeCenter.com
FERN LIFE CENTER 410 Newport Way NW
Suite B Issaquah, Washington
98207
Ph: 425-391-3376 Fax: 425-391-3378
www.FernLifeCenter.com
Integrating modern medicine,
Functional Medicine and the ancient practices of Ayurveda
Medical Provider: Dr. Keesha Ewers
Services:
Ayurvedic Lifestyle Management Bioidentical Hormone Replacement
Chronic Disease Management Colon Hydrotherapy
Enneagram Consultations Far Infrared Sauna Healthy You Radio!
Heart-Centered Clinical Hypnotherapy Heavy Metal Detoxification
High-quality Herbs & Supplements Ideal Protein Weight Loss Program
Just Stop Smoking! Massage
Medically Guided Detoxification Meditation
Nutrition Pancha Karma
Primary Care PTL III Aura Laser Program
Reiki Specialty Lab Testing
Wellness & Personalized Health
New Patient Introduction Packet & Intake Form
Thank you for your interest and welcome to Fern Life Center! We are a full spectrum medical clinic and the first integrative medicine center on Seattle’s Eastside. Our mission is to support you to venture beyond mind/body/spirit medicine into transformative wellness. This packet provides the follow information and forms:
1. Demographics 2. Financial agreement 3. HIPAA (confidentiality) & Consent to Treat 4. Health history 5. Map & directions to our clinic, hours of operation and contacts
Please read and complete all forms and bring them with you to your first visit.
What is integrative medicine? Dr Keesha Ewers our medical provider brings modern medicine, progressive western medicine and traditional healing to every patient visit. Both are Family Nurse Practitioners licensed by the State of Washington to provide primary care, prescribe medications, order and interpret lab tests and refer to specialists. Both have also completed training in Ayurveda and are Functional Medicine providers. About Ayurveda:
“Considered by many scholars to be the oldest healing science, Ayurveda is a holistic approach to health that is designed to help people live long, healthy, and well balanced lives. The basic principle of Ayurveda is to prevent and treat illness by maintaining balance in the body, mind, and consciousness through proper drinking, diet, and lifestyle, as well as herbal remedies.” - A.D.A.M.
About Functional Medicine:
“A newer approach to patient care which is said to assign a central role to gastrointestinal, endocrine, and immune system interactions with environmental factors, set at the level of the individual, to determine health.”
Integration also exists between all the different specialty providers at Fern Life Center. Your treatment plan may include nutrition consultations, massage, Reiki, colon hydrotherapy, detoxification and other therapies. We are proud and happy to work in community as a team. Please see the sidebar at left for a full listing. Fern Life Center provides a space for community education, blissful rejuvenation and spiritual renewal. Wherever you are on your path, we encourage you to access your own wisdom...leading to greater self-awareness and lasting healing. Thank you for having us along on your journey, we look forward to serving you! Why the fern? This easily recognizable species is an abundant native of the Pacific Northwest. Like the fern, we grow and flourish as we unfurl
toward light and that process is our natural way.
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
DEMOGRAPHIC PATIENT INFORMATION Patient Name: ________________________________________________________ Date: ________________
Address: ____________________________________________ City: _________________________ State: ________ Zip: ___________
Age: _______ Birth date: ____________ Gender: female male trans Social Security #: ______________
City/State of birth: _______________________ Occupation/Employer: ___________________________________
Employer phone: _______________________________________
Employer address:
Please fill all & check primary contact choice:
Phone (home) ________________________
Phone (work) ________________________
Phone (cell) _________________________
Email _______________________________
May we leave personal/medical information at this place of contact? yes no
Partner status: Single Partnered Married
Widowed Divorced Separated
Spouse Name: __________________________________________
Spouse birth date: _____________ Spouse SS#: ______________
Spouse Employer: ______________________________________
If patient is a student, name of school/college: _________________________________________________________
Whom may we thank for referring you? Friend- name: ______________________________________ Internet
Radio Saw while driving by Referred by my insurance company Referred by provider: ______________
Emergency contact name: ___________________________________________ Relationship: _________________
Phone: ___________________________ Cell: __________________________ Pager: _______________________
EMAIL COMMUNICATION: I would like the ability to discuss my personal health matters via email communication. I give my permission for Fern Life Center providers and staff to discuss personal health matters, understanding that email may not be a confidential mode of communication.
Preferred email account:
Insurance Information
Insured through: Self Spouse Parent Other:____________ Subscriber name: ___________________________
If not listed above, please list Subscriber birth date: ___________ SS#: _______________ Phone: _______________
Insurance company: __________________________ ID#: ___________________ Group#: ____________________
If insurance is through employment, please indicate employer name: _______________________________________
Secondary insurance name: __________________________ ID#: ________________ Group#: _________________
Please list other medical providers currently caring for you:
Name: ____________________________________________ Specialty: _____________________________ Contact info: _____________________
Name: ____________________________________________ Specialty: _____________________________ Contact info: _____________________
Name: ____________________________________________ Specialty: _____________________________ Contact info: _____________________
Rights and Responsibilities: Our promise to you: Our mission is to empower you to learn the patterns of behavior that inform your wellness choices. We promise to listen carefully, think deeply and kindle insight into directions (therapies, treatments, services) that will nourish sustainable health. We promise to be considerate about your time and thoughtful regarding your finances. We thank you for allowing us to journey with you on this path to transformation and look forward to growing with you!
We ask in return for your authenticity and courage to step outside of usual thinking and behavioral patterns. A key component of success is the willingness to incorporate diet, lifestyle and relationship changes. We ask you to be honest with what are realistic changes to begin with, and to wholeheartedly embrace the possibility that your health and life can look and feel exactly how you want it to, although this requires both effort and time and there are no guarantees from our clinic or providers that this will happen.
(Signature) ________________________________________________________________ Date ____________________ (Name of minor if above is parent/guardian) ____________________________________ Relationship: _____________
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
PATIENT FINANCIAL AGREEMENT
Medical visit consultations and fees: • The first office consult, which includes a comprehensive intake, review of medical records, physical exam and
initial treatment plan, generally lasts 60 minutes and costs $240.00 without insurance. • Follow-up visits last 20-60 minutes depending on need $90.00 - 140.00 without insurance. • Lab work and nutritional supplements are not included in these fees. • Fees for all other services are available from the Fern Life Center front desk. Please call for details.
Insurance billing and payment:
• As a courtesy to our patients we do bill insurance on their behalf for specific services; however, it is the patient’s responsibility to verify your benefits plan and coverage of providers and /or services. We cannot quote specific insurance plan details.
• Payment for visit co-pays and/or medications and supplies are to be rendered at time of service and can be made by cash, check, money order, or credit card.
• There is a $35 NSF fee on all returned checks. • Patients will be held responsible for non-payment by their insurance company. Accounts unpaid by the
insurance company greater than 90 days will be billed to the patient. • Outstanding balances greater than 120 days will be turned over to a collection agency unless prior arrangements
have been made in writing. • Requests for medical necessity letters will be charged $25.00 per patient.
Phone consultations will be charged at the rate of $ 5.00 per minute.
• Telephone consults are time guaranteed only when pre-scheduled. • Consults are billable directly to patient, phone consultations are not a billable under most insurance
carriers. Email communication:
• Patient emails are accepted by providers no more than twice a week. Please be courteous as provider time is limited. If a question requires more than a few lines of response, it is probably better served by a visit.
• Please allow 24-48 business hours to receive a response.
Appointment cancellation/No show/Late arrival charge: • You may cancel an appointment at no charge if you notify our office at least 48 hours in advance. Failure to do
so will result in the full charge of your scheduled appointment. Scheduled phone consultation appointments will be charged a minimum cancellation fee of $100.00 (20 minutes at $5.00 per minute). Late arrivals to scheduled appointments of 15 minutes or more may result in a full charge fee if the provider is not able to keep the appointment due to time constraints.
I, the undersigned, understand that I am financially responsible for all charges accrued by myself and/or my dependent(s) and agree to pay for services. I hereby authorize the provider to release all information necessary to secure the payment of benefits and authorize the use of this signature on all insurance submissions. I further authorize that payments be made directly to Fern Life Center. I understand that if I do not have insurance, or fail to provide complete and accurate billing information at the time of service, I will be billed and held responsible for all charges. I understand that it is my responsibility to find out if my insurance covers any services that I engage in through Fern Life Center. If services are not covered, full payment is due at time of service. I, ________________________________________, agree to the above defined financial policies of Fern Life Center. In the case of default of payment, I am responsible for full payment of the balance, interest accrued, and any collection costs and legal fees incurred to collect on this account. I, the undersigned, have read, understand, and accept the information and conditions specified in this document. ________________________________________ __________________________________________ ______________ Client signature Print Name Date
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
HIPAA ACKNOWLEDGEMENT: SEE ATTACHED STATEMENT OF PRIVACY Our practice is dedicated to maintaining the privacy of your individually identifiable health information (also called protected
health information, or PHI). In conducting our business, we will create records regarding you and the treatment and services we
provide to you. We are required by law to maintain the confidentiality of health information that identifies you. We also are
required by law to provide you with this notice of our legal duties and the privacy practices that we maintain in our practice
concerning your PHI. By federal and state law, we must follow the terms of the Notice of Privacy Practices that we have in effect.
I acknowledge that I have been provided a copy of and have read and understand Fern Life Center’s HIPAA Privacy Notice containing a complete description of my rights, and the permitted uses and disclosures, under HIPAA. While Fern Life Center has reserved the right to change the terms of its Privacy Notice, copies of the Privacy Notice as amended are available from Fern Life Center or by sending a written request with return address to _______________ initial _____ date _______ You have the right to revoke this authorization, in writing, at any time, except to the extent that Fern Life Center has taken action in reliance on it. A revocation is effective upon receipt by Fern Life Center of a written request to revoke and a copy of the executed authorization form to be revoked. _______ _______
ADDITIONAL HIPAA DISCLOSURE AUTHORITY In addition to the allowable disclosures described in the Statement of Privacy Practices, I hereby specifically authorize disclosure of my protected health care information to the person indicated below: (circle) Any member of my immediate family YES NO Spouse only YES NO Other (please specify): YES NO
_______________________________________________ ___________________________________________________ _________________ Client signature Print name Date
CONSENT TO TREAT: Having come to Fern Life Center for evaluation or treatment, I (or my authorized representative on my behalf) hereby consent to
and authorize Fern Life Center medical providers and other staff members involved in my care to administer such diagnostic
procedures, treatment or both as they may consider advisable to maintain my health and to assess and to evaluate and treat my
injury or illness. I understand that the provider responsible for my care has the responsibility to explain to me the purpose, the
benefits and the most common risks involved in the diagnosis and treatment of my illness or injury, as well as alternative available
courses of treatment, and I understand that I have the right to refuse any suggested examination, test or treatment.
Right to Refuse Treatment: In giving my general consent to treatment, I understand that I retain the right to refuse any particular
examination, test, procedure, treatment, therapy or medication recommended or deemed medically necessary by my individual
treating health care providers. I also understand that the practice of medicine is not an exact science and that no guarantees have
been made to me as to the results of my evaluation and/or treatment.
_______________________________________________ ___________________________________________________ _________________ Client signature Print name Date
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
HEALTH HISTORY & CURRENT STATUS
What are your main health concerns at this time? Order by importance to you: 1. 2. 3. 4. What would you like to get out of this consultation today? 1. 2. 3. What do you think you need to heal? Please rate your overall level of health: (Poor) 1 2 3 4 5 6 7 8 9 10 (Excellent) Please rate your overall level of stress: (Low) 1 2 3 4 5 6 7 8 9 10 (High) Please assign a number value to your satisfaction with the following areas of your life; 1 is low & 10 is the highest: Physical environment ________ Health ________ Fun & recreation ________ Romance/significant other ________ Career ________ Friends/family ________ Personal growth ________ Money ________
Personal Medical History Allergies: list all known allergies to medications, environment and food AND reaction. 1. 2. 3. Birth History: Premature Breathing problems Breech C-section Vaginal birth Time of day: _____________ Childhood health: (Poor) 1 2 3 4 5 6 7 8 9 10 (Excellent) Place lived: _____________________________________ Breastfed Formula Colic Illnesses: _________________________________ Received antibiotics? Yes No Height: __________ Weight: _________ Weight 1 year ago: _________ Maximum weight: _________ Age at that time: _____ Is there any possibility that you are pregnant? Yes No List all previous surgeries & year:
1.
2.
3.
4.
Describe all serious illnesses & year diagnosed:
1.
2.
3.
4.
List all accidents and injuries (if not listed above):
1.
2.
3.
4.
List all hospitalizations:
1.
2.
3.
4.
Have you been under the care of a licensed heath care professional in the past year? Yes No If so, for what reasons? ____________________________________________________________________ Indicate dates for the most recent (if ever) of the following preventative exams. Write “never” if you’ve never had this test. Physical exam: _______________ Full blood work: ______________ Colonoscopy: ________________
Eye exam: _______________ Dental exam: _____________ Fecal Occult Blood test: ____
Prostate/Gyn exam: _____________ Mammogram: __________________ Bone density: __________________
List immunizations: ________________________________________________________________________________________ Any reaction ever? No Yes: what happened? _______________________________________________________________
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
Medication/Supplement/Herbal/Vitamin History Preferred pharmacy name/city: __________________________________________ Phone: _____________ Name Dosage/Frequency How long taken? What for? Who prescribed?
Family Medical History List illnesses that have occurred in your blood relatives including: cancer, high blood pressure, heart disease, renal disease (kidneys), TB, bleeding tendencies, diabetes, stroke, mental disease, drug or alcohol addiction, glaucoma, psychiatric illness Family Member Current Age Diagnosis Age at diagnosis? Current health or age at
death Father Mother Paternal g’father Paternal g’father Maternal g’father Maternal g’mother Sibling Sibling Sibling Sibling Children Children Children Dietary Habits Please list typical foods consumed on a regular basis Do you have any routines around eating? Yes No Sometimes
Breakfast: ______________________________________________________________________________________________
Lunch: _________________________________________________________________________________________________
Dinner: ________________________________________________________________________________________________
Snacks: ________________________________________________________________________________________________
Fluids: _________________________________________________________________________________________________
Any food cravings? Please list: ______________________________________________________________________________ Check which foods/substances you use & describe what kind, how much & how many times a week: Caffeine Alcohol Candy/sweets Carbonated beverages Tobacco (with history & quit date) Margarine Milk/ ice cream Fast food Cheese Fried foods Luncheon meats If you use alcohol: Have you ever felt you should cut down? Yes No Have people ever been annoyed with you or nagged you about your drinking? Yes No Have you ever felt guilty about your drinking? Yes no Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hangover? Yes No
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
For the following questions, check all that apply to you: How Is Your Appetite? None Weak Normal Strong Irregular How Does Food Affect You? Satisfied, Energized Unsatisfied, Still Hungry Fatigued, Sleepy How Do You Eat? Sitting On The Go Snacking Throughout The Day Temperature Preferences: Hot Food Cold Food Hot Drinks Cold Drinks Varies Is Your Thirst: Extreme Changeable No Thirst Dry Mouth Which Tastes Do You Prefer? Sweet Sour Salty Pungent Bitter Astringent Do you follow a special diet? Please describe &/or check all that apply: ___________________________________________ Non-
Vegetarian Vegetarian Vegan Raw Foods Low Fat Diet Low carb No carb Paleo APOE gene diet Elimination diet GAPS/SCD
Eating disorders or other issues with eating?
Current Past Please describe:
Any food reactions or intolerances?
Please describe:
How many glasses of water do you consume each week?_____
On average, how often do you eat breakfast in a week? ____
How many meals do you eat out per week? ___________ How often do you choose organic foods? Always Sometimes Never
When I eat meat, fish or poultry: I almost always have it fried or cooked with oil or another
fat, or with gravy I almost always have it broiled, baked or stewe and without
any gravy or fat I do both I don’t eat meat, fish or poultry
When I eat cooked vegetables: I almost always have them with butter, margarine or sauce;
or cooked with butter, magarine oil or another fat. I almost always have them without any of the fats listed
above. I do both. I don’t eat cooked vegetables
Please circle any digestive symptoms that you experience: Abdominal Pain Bloating Heartburn Overweight
Acid Reflux Candida Hiccups Sudden Weight Loss
Aggravated By Spices Eating Disorder Hypoglycemia Ulcers
Bad Breath Food Allergies Nausea Underweight
Belching Gas Nutritional Deficiencies Vomiting
Please circle any elimination symptoms that you experience:
Anal Fissures Crohn’s Disease Incomplete Evacuation Oily Stools
Anal Itching/Burning Diarrhea Intestinal Pain/Cramping Parasites
Blood In Stools Difficulty Passing Stools Irritable Bowel Syndrome Rectal Prolapse
Colitis Gallstones Laxative Use Smelly Stools
Constipation Hemorrhoids Mucus In Stools Undigested Food In Stools
Daily Schedule Time Routine Activity Variation Spritual
Practices Exercise
Morning
Mid-morning
Lunch
Mid-Afternoon
Evening
Late-evening
Middle of the night Sleep patterns: Rate ease of falling asleep: (Easy) 1 2 3 4 5 6 7 8 9 10 (Difficult)
Rate ease of staying asleep: (Easy) 1 2 3 4 5 6 7 8 9 10 (Difficult) Are you sexually active? Yes No Frequency? __________________ Current method of birth control? __________________ Have you ever contracted a sexually transmitted disease? Yes No If so, what & when? ______________________________ Do you exercise regularly? Yes No Length of time? __________ Times per week? ______ Types ___________________ Body temperature: Do you generally run hot or cold? Please explain: _________________________________________________
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
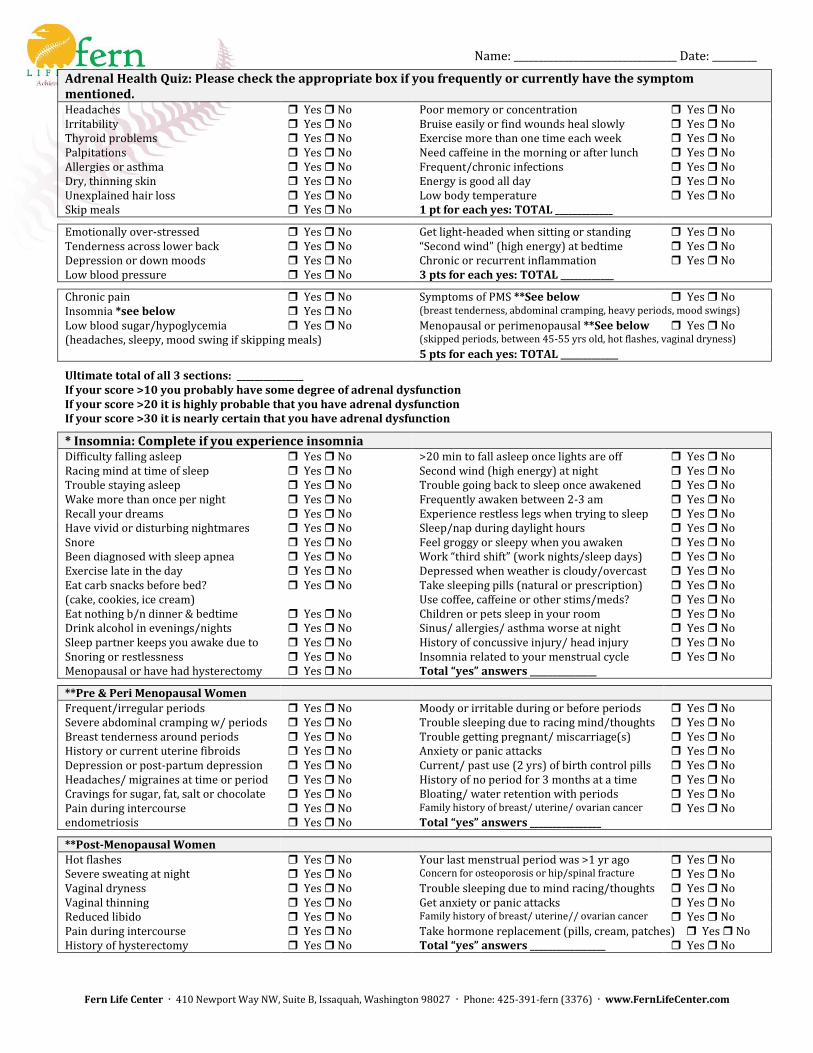
Adrenal Health Quiz: Please check the appropriate box if you frequently or currently have the symptom mentioned. Headaches Yes No Poor memory or concentration Yes No Irritability Yes No Bruise easily or find wounds heal slowly Yes No Thyroid problems Yes No Exercise more than one time each week Yes No Palpitations Yes No Need caffeine in the morning or after lunch Yes No Allergies or asthma Yes No Frequent/chronic infections Yes No Dry, thinning skin Yes No Energy is good all day Yes No Unexplained hair loss Yes No Low body temperature Yes No Skip meals Yes No 1 pt for each yes: TOTAL _____________
Emotionally over-stressed Yes No Get light-headed when sitting or standing Yes No Tenderness across lower back Yes No “Second wind” (high energy) at bedtime Yes No Depression or down moods Yes No Chronic or recurrent inflammation Yes No Low blood pressure Yes No 3 pts for each yes: TOTAL ____________
Chronic pain Yes No Symptoms of PMS **See below Yes No Insomnia *see below Yes No (breast tenderness, abdominal cramping, heavy periods, mood swings)
Low blood sugar/hypoglycemia Yes No Menopausal or perimenopausal **See below Yes No (headaches, sleepy, mood swing if skipping meals) (skipped periods, between 45-55 yrs old, hot flashes, vaginal dryness)
5 pts for each yes: TOTAL _____________
Ultimate total of all 3 sections: _______________ If your score >10 you probably have some degree of adrenal dysfunction If your score >20 it is highly probable that you have adrenal dysfunction If your score >30 it is nearly certain that you have adrenal dysfunction
* Insomnia: Complete if you experience insomnia Difficulty falling asleep Yes No >20 min to fall asleep once lights are off Yes No Racing mind at time of sleep Yes No Second wind (high energy) at night Yes No Trouble staying asleep Yes No Trouble going back to sleep once awakened Yes No Wake more than once per night Yes No Frequently awaken between 2-3 am Yes No Recall your dreams Yes No Experience restless legs when trying to sleep Yes No Have vivid or disturbing nightmares Yes No Sleep/nap during daylight hours Yes No Snore Yes No Feel groggy or sleepy when you awaken Yes No Been diagnosed with sleep apnea Yes No Work “third shift” (work nights/sleep days) Yes No Exercise late in the day Yes No Depressed when weather is cloudy/overcast Yes No Eat carb snacks before bed? Yes No Take sleeping pills (natural or prescription) Yes No (cake, cookies, ice cream) Use coffee, caffeine or other stims/meds? Yes No Eat nothing b/n dinner & bedtime Yes No Children or pets sleep in your room Yes No Drink alcohol in evenings/nights Yes No Sinus/ allergies/ asthma worse at night Yes No Sleep partner keeps you awake due to Yes No History of concussive injury/ head injury Yes No Snoring or restlessness Yes No Insomnia related to your menstrual cycle Yes No Menopausal or have had hysterectomy Yes No Total “yes” answers _______________
**Pre & Peri Menopausal Women
Frequent/irregular periods Yes No Moody or irritable during or before periods Yes No Severe abdominal cramping w/ periods Yes No Trouble sleeping due to racing mind/thoughts Yes No Breast tenderness around periods Yes No Trouble getting pregnant/ miscarriage(s) Yes No History or current uterine fibroids Yes No Anxiety or panic attacks Yes No Depression or post-partum depression Yes No Current/ past use (2 yrs) of birth control pills Yes No Headaches/ migraines at time or period Yes No History of no period for 3 months at a time Yes No Cravings for sugar, fat, salt or chocolate Yes No Bloating/ water retention with periods Yes No Pain during intercourse Yes No Family history of breast/ uterine/ ovarian cancer Yes No endometriosis Yes No Total “yes” answers ________________
**Post-Menopausal Women
Hot flashes Yes No Your last menstrual period was >1 yr ago Yes No Severe sweating at night Yes No Concern for osteoporosis or hip/spinal fracture Yes No Vaginal dryness Yes No Trouble sleeping due to mind racing/thoughts Yes No Vaginal thinning Yes No Get anxiety or panic attacks Yes No Reduced libido Yes No Family history of breast/ uterine// ovarian cancer Yes No Pain during intercourse Yes No Take hormone replacement (pills, cream, patches) Yes No History of hysterectomy Yes No Total “yes” answers _________________ Yes No
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
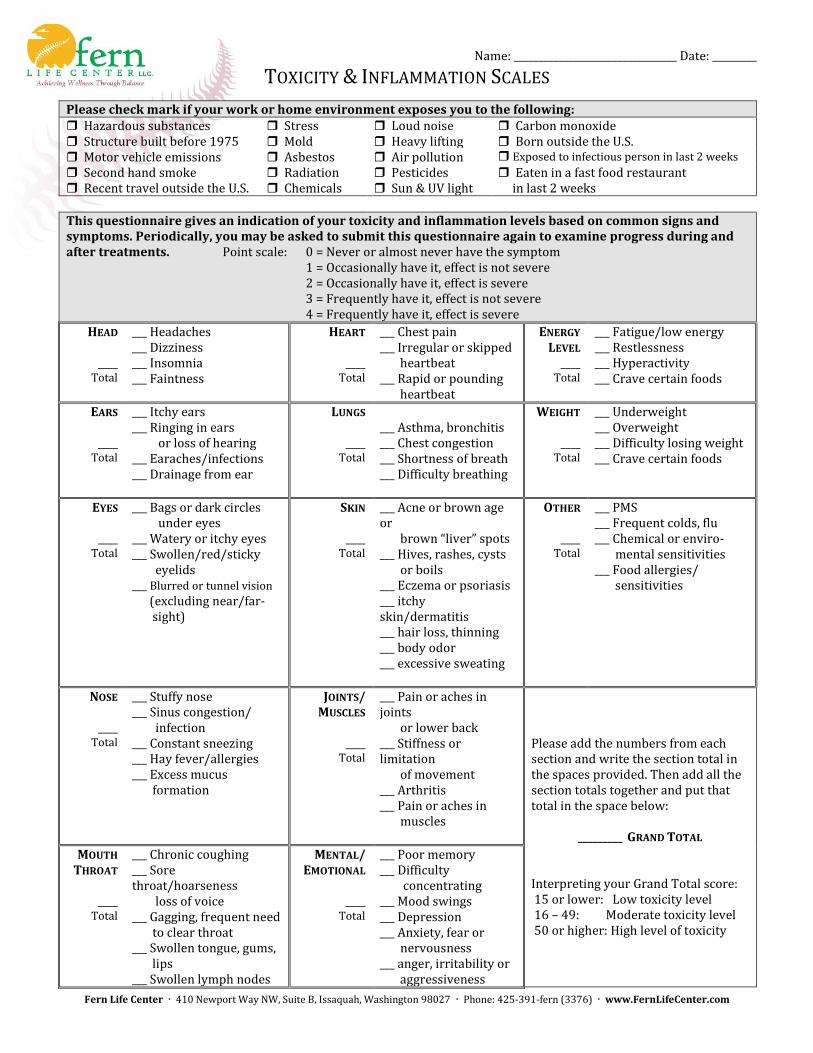
TOXICITY & INFLAMMATION SCALES
Please check mark if your work or home environment exposes you to the following: Hazardous substances Stress Loud noise Carbon monoxide Structure built before 1975 Mold Heavy lifting Born outside the U.S. Motor vehicle emissions Asbestos Air pollution Exposed to infectious person in last 2 weeks Second hand smoke Radiation Pesticides Eaten in a fast food restaurant Recent travel outside the U.S. Chemicals Sun & UV light in last 2 weeks This questionnaire gives an indication of your toxicity and inflammation levels based on common signs and symptoms. Periodically, you may be asked to submit this questionnaire again to examine progress during and after treatments. Point scale: 0 = Never or almost never have the symptom
1 = Occasionally have it, effect is not severe 2 = Occasionally have it, effect is severe 3 = Frequently have it, effect is not severe 4 = Frequently have it, effect is severe
HEAD
____ Total
___ Headaches ___ Dizziness ___ Insomnia ___ Faintness
HEART
____ Total
___ Chest pain ___ Irregular or skipped heartbeat ___ Rapid or pounding heartbeat
ENERGY LEVEL
____ Total
___ Fatigue/low energy ___ Restlessness ___ Hyperactivity ___ Crave certain foods
EARS
____ Total
___ Itchy ears ___ Ringing in ears or loss of hearing ___ Earaches/infections ___ Drainage from ear
LUNGS
____ Total
___ Asthma, bronchitis ___ Chest congestion ___ Shortness of breath ___ Difficulty breathing
WEIGHT
____ Total
___ Underweight ___ Overweight ___ Difficulty losing weight ___ Crave certain foods
EYES
____ Total
___ Bags or dark circles under eyes ___ Watery or itchy eyes ___ Swollen/red/sticky eyelids ___ Blurred or tunnel vision
(excluding near/far- sight)
SKIN
____ Total
___ Acne or brown age or brown “liver” spots ___ Hives, rashes, cysts or boils ___ Eczema or psoriasis ___ itchy skin/dermatitis ___ hair loss, thinning ___ body odor ___ excessive sweating
OTHER
____ Total
___ PMS ___ Frequent colds, flu ___ Chemical or enviro- mental sensitivities ___ Food allergies/ sensitivities
NOSE
____ Total
___ Stuffy nose ___ Sinus congestion/ infection ___ Constant sneezing ___ Hay fever/allergies ___ Excess mucus formation
JOINTS/ MUSCLES
____
Total
___ Pain or aches in joints or lower back ___ Stiffness or limitation of movement ___ Arthritis ___ Pain or aches in muscles
Please add the numbers from each section and write the section total in the spaces provided. Then add all the section totals together and put that total in the space below:
_________ GRAND TOTAL Interpreting your Grand Total score: 15 or lower: Low toxicity level 16 – 49: Moderate toxicity level 50 or higher: High level of toxicity
MOUTH THROAT
____
Total
___ Chronic coughing ___ Sore throat/hoarseness loss of voice ___ Gagging, frequent need to clear throat ___ Swollen tongue, gums, lips ___ Swollen lymph nodes
MENTAL/ EMOTIONAL
____
Total
___ Poor memory ___ Difficulty concentrating ___ Mood swings ___ Depression ___ Anxiety, fear or nervousness ___ anger, irritability or aggressiveness
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
___ Canker sores, mouth ulcers
___ Insomnia
REVIEW OF SYSTEMS
Check all the symptoms that are of concern to you at this time that you want to discuss with the practitioner. On the
comments line, please indicate if any checked symptoms are current or past and describe any area in which you have
experienced a severe episode and indicate if that episode was in previous 6 months or prior to 6 months ago.
HEAD
Headaches Dizziness Fainting spells Loss of balance Difficulty remembering
Difficulty thinking clearly Thinning or loss of hair
Comments:
EYES
Blurry Dry Tic/twitch Itchy Red Watery Cataracts Color blindness Burning
Contacts/ glasses For ___ Years Farsighted Nearsighted Glaucoma Eye strain Mucus
Night blindness Pain/soreness in eyes Poor/loss of vision Sensitive to light Floaters
Comments:
EARS
Earaches/pain Excess Earwax Hearing loss Ringing Sensitivity To Sound Discharge
Comments:
NOSE
Loss of smell Bleeding Pain Discharge Post-nasal drip Sinus congestion
Frequent Colds Nasal Polyps Deviated Septum
Comments:
MOUTH
Excessive thirst Loss of taste Strange taste Bad breath Lip ulcers or lesions Dry/cracking lips Tongue pain Bleeding gums Receding gums Tooth pain Cavities Tooth sensitivity TMJ Dry mouth Excess saliva Comments:
THROAT/ NECK
Pain Swollen glands Stiffness Lumps Difficulty Swallowing Comments:
HAIR & NAILS
Dandruff Dry Hair Loss Oily
Brittle, Break Easily Dry, Rough Ridged Oily Pale Pink Smooth
Comments:
SKIN
Acne Boils Bruises Easily Clammy Dry Eczema Fungal Infections Itching
Psoriasis Rashes/Hives Scars Sensitive Skin Eruptions Changing or bleeding moles
Comments:
PERSPIRATION
Spontaneous Or Without Exertion Excessive Rarely Nighttime Cold Sweats Unusual Odor Comments:
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
CIRCULATION
Blood Clots Calf pain Swollen ankles Varicose veins Cold hands/feet Puffy eyes Comments:
CARDIOVASCULAR
Arteriosclerosis Chest Pain Coronary Disease Heart Murmur Hypertension Heaviness Or Tightness In Chest High Blood Pressure High Cholesterol Low Blood Pressure Hypotension Palpitations Irregular Heart Beat Bradycardia Tachycardia Pacemaker Congenital Heart Defect(s): __________________________ Comments:
DIGESTION
Pain Burning indigestion Belching Regurgitation Vomiting Excessive gas Heavy bloating after meals Hemorrhoids Constipation (<1 BM/day) Diarrhea Both constipation & diarrhea Bloody stool Comments:
GENITO/ URINATION
Frequency: ______/ Day Color: __________ # Of Times At Night ________ Burning/ Painful Loss of urinary control Dribbling Blood in urine Foamy Frequent Profuse Retention Scanty Urgent Bedwetting Kidney/Bladder Infections Kidney/Bladder Stones Congenital Kidney Problems Frequent Urinary Tract Infections (UTI) Pain in kidney/groin area Comment:
MUSCLES & JOINTS
Swelling in joints Pain/ache in joints Stiff joints Persistant muscle/bone pains Tremors/tics in muscles Muscle weakness/atrophy Numbness Comments:
NERVES
Loss of taste, smell or touch Tingling sensations Tremors in limbs Uncoordinated muscle/limbs Neuropathic pain Comments:
MALE SYSTEM
Prostate gland swollen/painful low sperm count Low motility Genital sores or lesions Genital discharge Erectile function difficulty Change in libido Comments:
FEMALE SYSTEM
Irregular cycle Heavy/prolonged bleeding Vaginal discharge Painful menses Fibroids Missed menses or spotting discharge PMS or menopausal symptoms Ovarian cyst Pregnancies #: ______ Miscarriages/abortions #: _____ Unsatisfactory sex/change in libido Genital sores Last menstrual period date _________ Last menstrual period date: __________ Comments:
BREASTS Swelling Redness Lumps Nipple discharge Tenderness/pain Comments:
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
ENVISIONING YOUR OWN HEALTH
Please take a few minutes to go inside of yourself to answer these last questions so that we may better design a program to fit your unique needs. Thank you for your careful consideration. It is very much appreciated. 1. What are you doing in your life that brings you peace and harmony? 2. What do you want your spiritual life to look like?
3. What does your spiritual life currently look like? 4. If you could design your perfect state of wellness and balance, what would your life look like? 5. What would you have to give up to achieve this life? 6. How can we best support you to meet your dreams? 7. What does it look like when you are spiraling down emotionally? 8. How do you bring yourself back out? 9. Have you noticed patterns that repeat themselves in your life (only the names, places & occurrences have changed
names)? 10. Do you know your purpose in life? 11. Do you have vivid dreams? 12. Please assign a number value to your satisfaction with the following areas of your life; 1 is low and 10 is the highest: Physical environment ______ Career ______Fun and Recreation ______Health ______Money ______Romance/Significant other______ Personal Growth______Friends/Family______
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
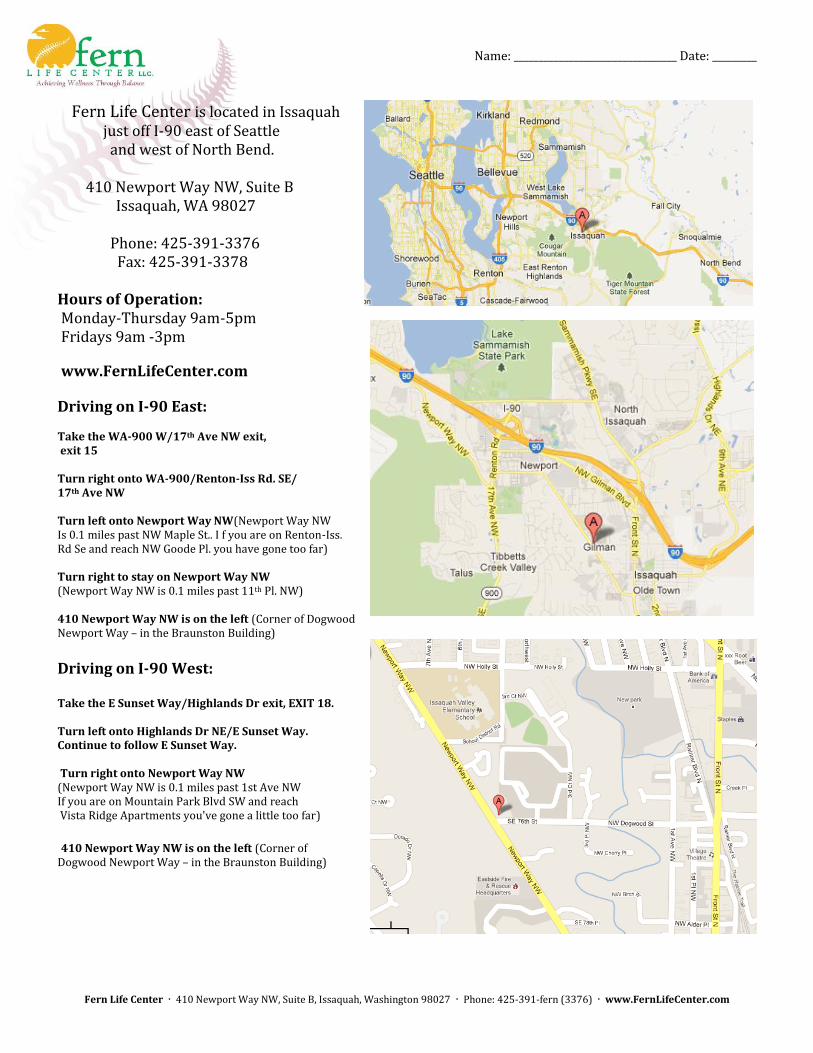
Fern Life Center is located in Issaquah just off I-90 east of Seattle and west of North Bend. 410 Newport Way NW, Suite B Issaquah, WA 98027 Phone: 425-391-3376 Fax: 425-391-3378 Hours of Operation: Monday-Thursday 9am-5pm Fridays 9am -3pm
www.FernLifeCenter.com
Driving on I-90 East: Take the WA-900 W/17th Ave NW exit, exit 15 Turn right onto WA-900/Renton-Iss Rd. SE/ 17th Ave NW Turn left onto Newport Way NW(Newport Way NW Is 0.1 miles past NW Maple St.. I f you are on Renton-Iss. Rd Se and reach NW Goode Pl. you have gone too far) Turn right to stay on Newport Way NW (Newport Way NW is 0.1 miles past 11th Pl. NW) 410 Newport Way NW is on the left (Corner of Dogwood Newport Way – in the Braunston Building)
Driving on I-90 West: Take the E Sunset Way/Highlands Dr exit, EXIT 18. Turn left onto Highlands Dr NE/E Sunset Way. Continue to follow E Sunset Way. Turn right onto Newport Way NW (Newport Way NW is 0.1 miles past 1st Ave NW If you are on Mountain Park Blvd SW and reach Vista Ridge Apartments you've gone a little too far)
410 Newport Way NW is on the left (Corner of Dogwood Newport Way – in the Braunston Building)
Name: _________________________________ Date: _________
Fern Life Center 410 Newport Way NW, Suite B, Issaquah, Washington 98027 Phone: 425-391-fern (3376) www.FernLifeCenter.com
STATEMENT OF PRIVACY PRACTICES
Our office is dedicated to protect the privacy rights of our patients and the confidential information entrusted to us. The commitment of each employee to ensure that your health information is never compromised is a principal concept of our practice. We may, from time to time, amend our privacy policies and practices but will always inform you of any changes that might affect your rights.
Protecting Your Personal Healthcare Information We use and disclose the information we collect from you only as allowed by the Health Insurance Portability and Accountability Act and the state of Washington (HIPAA). This includes issues relating to your treatment, payment and our medical operations. Your personal health information will never be otherwise given to anyone-even family members- without your written consent. You, of course, may give written authorization for us to disclose your information to anyone you choose, for any purpose. Our office and electronic systems are secure from unauthorized access and our employees are trained to make certain that the confidentiality of your records is always protected. Our privacy policy and practices apply to all former, current and future patients, so you can be confident that your protected health information will never be improperly disclosed or released.
Collection Protected Health Information We will only request personal information needed to provide our standard of quality integrative medical care, implement payment activities, conduct normal medical practice operations and comply with the law. This may include your name, address, telephone numbers, social security number, employment data, medical history, health records, etc. While most of the information will be collected from you, we may obtain information from third parties if it is deemed necessary. Regardless of the source, your personal information will always be protected to the full extent of the law.
Disclosure of our protected Health Information As stated above, we may disclose information as required by law. We are obligated to provide information to law enforcement and governmental officials under certain circumstances. We will not use your information for marketing purposes without your written consent. We may use and/or disclose your health information to communicate reminders about your appointments including voicemail messages, answering machines and emails.
Patient Rights You have a right to request copies of your healthcare information; to request copies in a variety of formats; and to request a list of instances in which we, or our business associates have disclosed your protected information for uses other than stated above. All such requests must be in writing. We may charge for your copies in an amount allowed by law. If you believe your rights have been violated, we urge you to notify us immediately. You can also notify the U.S. Department of Health and Human Services.
We value you for being a patient at Fern Life Center. Please let us know if you have any questions concerning your privacy rights and the protection of your personal health information.