New Parenteral Biologics Biosimilars—2015 - NHIA€¦ · Fairview Pharmacy Services Jesse...
39
3/14/2016 2016 NHIA Annual Conference & Exposition 1 New Parenteral Drugs, Biologics and Biosimilars—2015 Presented by: PGY1 Home Infusion Residents With an Introduction by: Pammi Farren, RPh, PhD
Transcript of New Parenteral Biologics Biosimilars—2015 - NHIA€¦ · Fairview Pharmacy Services Jesse...
3/14/2016
2016 NHIA Annual Conference & Exposition 1
New Parenteral Drugs, Biologics and
Biosimilars—2015 Presented by:
PGY1 Home Infusion ResidentsWith an Introduction by:
Pammi Farren, RPh, PhD

3/14/2016
2016 NHIA Annual Conference & Exposition 2
Option CareAmy Lee Alfred Olumba Elizabeth Lagasse Joshua
Jaussi Alexandre Ivanov Marlee Andis
CoramAshely Tran Noreen Chan Michael Anderson
Collin Chan
Fairview Pharmacy ServicesJesse PetersonVital CareRoss Woods
2
3/14/2016
2016 NHIA Annual Conference & Exposition 3
Speaker Disclosures
• The speaker(s) for this presentation have no conflicts of interest to disclose.
• Off‐label and/or investigational drug uses will not be discussed during this presentation.
3
3/14/2016
2016 NHIA Annual Conference & Exposition 4
New Drugs and Biologics Topic
• Thirteen year history of topic • Developed and presented by Anna Nowobilski Vasilios• New direction and format• Pharmacy residents with accredited PGY‐1 residency programs

3/14/2016
2016 NHIA Annual Conference & Exposition 5
Presentation Format
• Each resident to review assigned drug(s)• Additional handouts available
• Mobile conference app• NHIA website
• Pace and structure of presentation
3/14/2016
2016 NHIA Annual Conference & Exposition 6
THANK YOU!!
3/14/2016
2016 NHIA Annual Conference & Exposition 7
Carbidopa/Levodopa Ashley Tran
• Indication: Treatment of motor fluctuations in patients with advanced Parkinson’s disease (PD)
• Trials: In a 12‐week active controlled clinical trial, carbidopa/levodopa was compared to the oral immediate‐release carbidopa/levodopa. 416 patients with advanced Parkinson’s disease received this medication
• Dosing: Daily dose is determined by individualized patient titration and composed of a morning, continuous and extra doses (used to managed acute “Off” symptoms). Maximum recommended daily dose is 2000mg of the levodopa component
• Preparation: Single‐use cassettes containing 4.63 mg carbidopa (as 5 mg of the monohydrate) and 20 mg levodopa per mL of enteral suspension (approximately 100 mL)
• Administration: Into the jejunum through a percutaneous endoscopic gastrostomy with jejunal tube (PEG‐J) for long‐term (16 hrs) administration or through a naso‐jejunal tube for short term administration with the CADD®‐Legacy 1400 portable infusion pump.
7References:1) Duopa [package insert]. North Chicago, IL: AbbVie Inc. 2) Duopa [prescribing information]. North Chicago, IL: AbbVie Inc. 3) J.DiPiro et al. Pharmacotherapy: A Pathophysiologic Approach, 9e. New York, NY: McGraw‐Hill; 2014. 4) Carbidopa/Levodopa (Duopa). ©). 5) Lexicomp online, Lexicomp. Hudson, Ohio: Lexi‐Comp, Inc. December 2015.
Enteral ORPHAN(DUOPA)
3/14/2016
2016 NHIA Annual Conference & Exposition 8
Carbidopa/Levodopa Ashley Tran• Monitor: Electrocardiographic monitoring for arrhythmias and orthostatic hypotension, physical assessment for reduction of extrapyramidal movements, skin examinations
• A/Es: Complication of device insertion, nausea, depression, peripheral edema, hypertension, upper respiratory tract infection, oropharyngeal pain, atelectasis, and incision site erythema
• Patient education: No supplemental oral medication is needed if pump disconnection is anticipated, but an extra‐dose may be advised to be taken prior. Notify healthcare provider of gastrointestinal procedure‐related risks: bezoar, ileus, implant site erosion/ulcer, intestinal hemorrhage, intestinal ischemia, intestinal obstruction, intestinal perforation, pancreatitis, peritonitis, pneumoperitoneum, post‐operative wound infection
• Contraindications: Nonselective monoamine oxidase (MAO) inhibitors, (PEG‐J) with lack of transillumination/positive needle aspiration test; intestinal obstruction; sepsis; peritonitis; serious coagulation disorders; ascites; and neoplastic, inflammatory, and infiltrative diseases of the gastric and abdominal walls
• Drug Interactions: Selective MAO‐B inhibitors, antihypertensive drugs, Dopamine D2 receptor antagonists, isoniazid, iron salts, and high‐protein diet may reduce the effectiveness
1) Duopa [package insert]. North Chicago, IL: AbbVie Inc. 2) Duopa [prescribing information]. North Chicago, IL: AbbVie Inc. 3) J.DiPiro et al. Pharmacotherapy: A Pathophysiologic Approach, 9e. New York, NY: McGraw‐Hill; 2014. 4) Carbidopa/Levodopa (Duopa). ©). 5) Lexicomp online, Lexicomp. Hudson, Ohio: Lexi‐Comp, Inc. December 2015. 8
(DUOPA)

3/14/2016
2016 NHIA Annual Conference & Exposition 9
filgrastim‐sndz Amy Lee, Pharm.D.ZARXIO
• Description: Granulocyte colony‐stimulating factor
• Indications and Dosing: • Patients receiving myelosuppressive chemotherapy or acute myeloid leukemia (AML) receiving or consolidation chemotherapy: 5 mcg/kg/day SC or IV
• Bone marrow transplantation: 10 mcg/kg/day IV • Autologous peripheral blood progenitor cell collection and therapy: 10 mcg/kg SC daily• Cyclic or idiopathic neutropenia: 5 mcg/kg SC daily• Congenital neutropenia: 6 mcg/kg SC twice daily
• Clinical Trials• No head to head trials• Incidence and duration of febrile neutropenia, duration of antibiotic use, duration of hospitalization, remission rate, time to progression, overall survival, number of days of platelet transfusions, incidence of infection, fever, and oropharyngeal ulcers
9
References: 1. Zarxio [package insert]. Princeton, NJ: Sandoz Inc.; 2015 March.2. Lexi‐Comp, Inc. (Lexi‐Drugs® ). Lexi‐Comp, Inc.; December 4, 2015.3. Search results. ClinicalTrials.gov Web site. Available at: https://clinicaltrials.gov/ct2/results?term=zarxio&recr=Open. Accessed December 4, 2015.
SC, IV BIOLOGIC

3/14/2016
2016 NHIA Annual Conference & Exposition 10
filgrastim‐sndz Amy Lee, Pharm.D.ZARXIO
• Administration: Over 15 to 30 minutes or continuous IV infusion*• Direct administration of less than 0.3 mL is not recommended• May be diluted in D5W to concentrations between 5 mcg/mL and 15 mcg/mL• Diluted concentrations protected from adsorption to plastic materials• Compatible with glass, polyvinylchloride, polyolefin and polypropylene containers
• Warnings: Splenic rupture, acute respiratory distress syndrome, hypersensitivity, sickle cell crisis, alveolar hemorrhage, hemoptysis, capillary leak syndrome, severe chronic neutropenia, thrombocytopenia, leukocytosis, simultaneous chemotherapy and radiation
• Monitoring: CBC with differential and hypersensitivity
• ADRs: Pyrexia, pain, rash, cough, dyspnea, epistaxis, headache, bone pain, anemia, diarrhea, hypoesthesia, alopecia
• Drug Interactions: No known interactions
• Availability: 300mcg/ 0.5mL or 480 mcg/ 0.8 mL single‐use prefilled syringe References: 1. Zarxio [package insert]. Princeton, NJ: Sandoz Inc.; 2015 March.2. Lexi‐Comp, Inc. (Lexi‐Drugs® ). Lexi‐Comp, Inc.; December 4, 2015.3. Search results. ClinicalTrials.gov Web site. Available at: https://clinicaltrials.gov/ct2/results?term=zarxio&recr=Open. Accessed December 4, 2015.
10

3/14/2016
2016 NHIA Annual Conference & Exposition 11
Praluent (alirocumab)• Adjunct to diet and statins for adults with heterozygous familial hypercholesterolemia (HeFH) OR clinical atherosclerotic cardiovascular disease (ASCVD) in need of further LDL‐C lowering
• Dosing: • 75 mg/150 mg SC once every 2 weeks
• Clinical trials summary:• 5 double‐blind placebo‐controlled trials (n=3499), 36% with HeFH and 54% with ASCVD
• 3 studies with 75 mg Q2W, up‐titrated to 150 mg Q2W at week 12 if not at target LDL‐C• 2 studies with 150 mg Q2W dose only• 52 weeks long with primary efficacy endpoint (mean % change in LDL‐C) measured at week 24• All patients received a max tolerated dose of statin or other lipid lowering therapy• All studies met primary efficacy endpoint measured at week 24
• Limitations: effect on cardiovascular morbidity/mortality not determined
11References: ● Praluent (alirocumab) [prescribing information]. Bridgewater, NJ: Sanofi‐Aventis US LLC; July 2015.● Hobbs HH, Russell DW, Brown MS, Goldstein JL. The LDL receptor in familial hypercholesterolemia: mutational analysis of a membrane protein. Annu Rev Genet. 1990;24:133‐170.
Alexandre IvanovSC Human mAb

3/14/2016
2016 NHIA Annual Conference & Exposition 12
Praluent (alirocumab)
• MOA:• PCSK9 (protease) binds to LDL‐R on the surface of hepatocytes → LDL‐R breakdown• Praluent inhibits binding of PCSK9 to LDL‐R, thus ↑ LDL‐Rs available to clear LDL‐C
• Administration: • Self‐administration via SC injection into thigh, abdomen, or upper arm (site rotation)• NO co‐administration with other injectable drugs at the same injection site
• Monitoring: LDL‐C within 4 to 8 weeks of initiation or dose titration to assess response• Side effects: injection site reactions, nasopharyngitis and influenza in ≥ 5% of patients• Warnings/Precautions: hypersensitivity reactions (e.g. pruritus, rash), including anaphylaxis• Contraindications: serious hypersensitivity reactions to alirocumab• Drug interactions: sta ns ↓ alirocumab half‐life with no impact on dosing• Storage/Handling:
• Refrigerator at 2°C to 8°C (36°F to 46°F ) in outer carton to protect from light• Do NOT freeze or shake
• Cost/Assistance program: $672 per injector or prefilled pen/MyPRALUENT• Patient education: signs of allergic reaction, injection technique, and to use within 7 days of missed dose
12References: ● Praluent (alirocumab) [prescribing information]. Bridgewater, NJ: Sanofi‐Aventis US LLC; July 2015.● Hobbs HH, Russell DW, Brown MS, Goldstein JL. The LDL receptor in familial hypercholesterolemia: mutational analysis of a membrane protein. Annu Rev Genet. 1990;24:133‐170.
Alexandre IvanovSC Human mAb
3/14/2016
2016 NHIA Annual Conference & Exposition 13
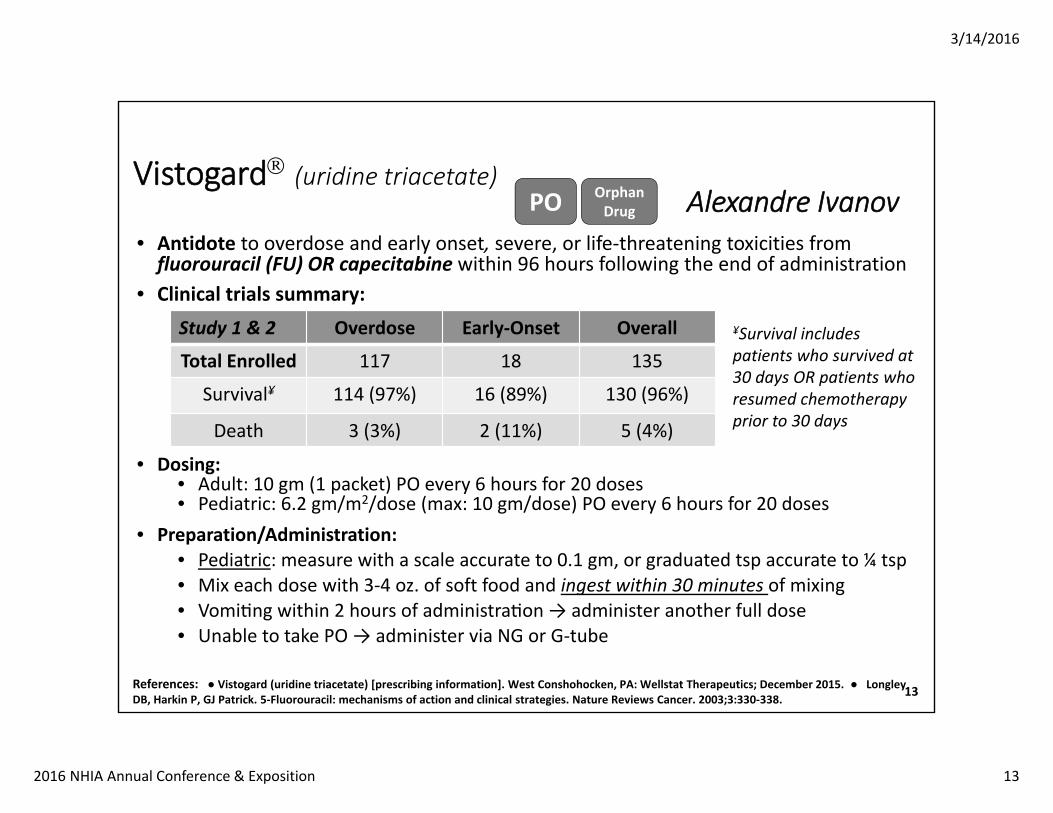
Vistogard (uridine triacetate)
• Antidote to overdose and early onset, severe, or life‐threatening toxicities from fluorouracil (FU) OR capecitabine within 96 hours following the end of administration
• Clinical trials summary:
• Dosing:• Adult: 10 gm (1 packet) PO every 6 hours for 20 doses• Pediatric: 6.2 gm/m2/dose (max: 10 gm/dose) PO every 6 hours for 20 doses
• Preparation/Administration:• Pediatric: measure with a scale accurate to 0.1 gm, or graduated tsp accurate to ¼ tsp• Mix each dose with 3‐4 oz. of soft food and ingest within 30 minutes of mixing• Vomi ng within 2 hours of administra on → administer another full dose• Unable to take PO → administer via NG or G‐tube
13References: ● Vistogard (uridine triacetate) [prescribing information]. West Conshohocken, PA: Wellstat Therapeutics; December 2015. ● Longley DB, Harkin P, GJ Patrick. 5‐Fluorouracil: mechanisms of action and clinical strategies. Nature Reviews Cancer. 2003;3:330‐338.
Alexandre IvanovPO
Study 1 & 2 Overdose Early‐Onset Overall
Total Enrolled 117 18 135
Survival¥ 114 (97%) 16 (89%) 130 (96%)
Death 3 (3%) 2 (11%) 5 (4%)
¥Survival includes patients who survived at 30 days OR patients who resumed chemotherapy prior to 30 days
Orphan Drug
3/14/2016
2016 NHIA Annual Conference & Exposition 14
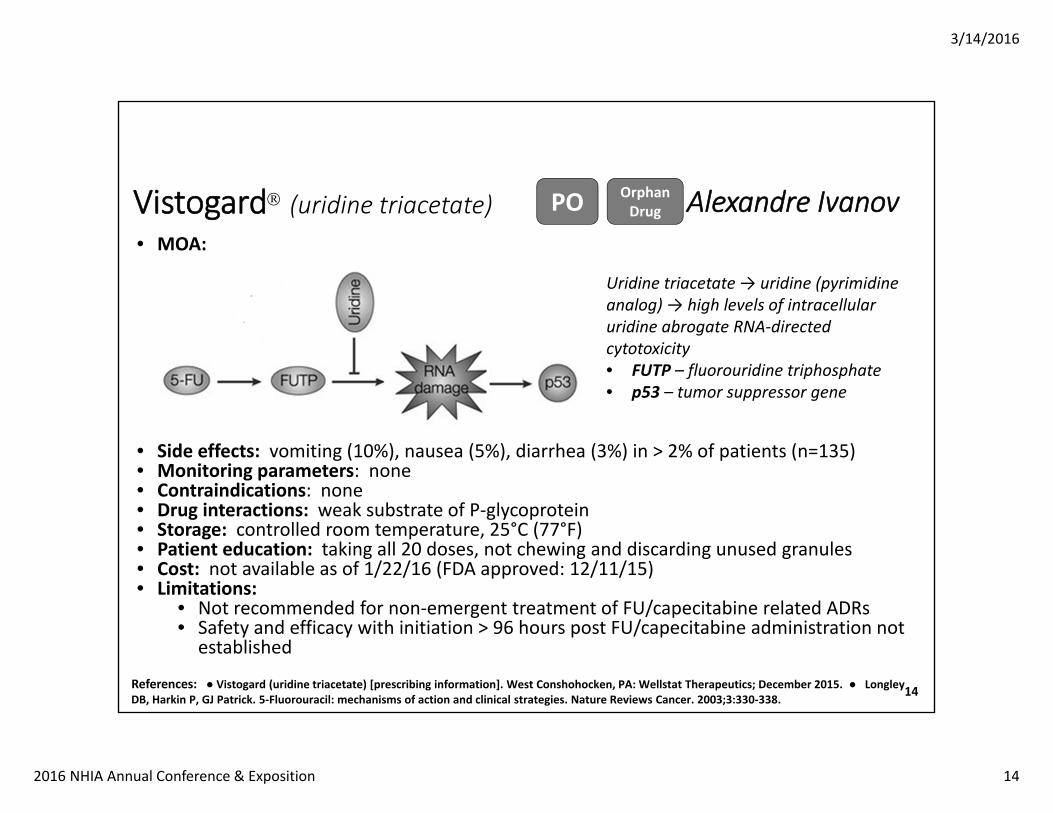
Vistogard (uridine triacetate) • MOA:
• Side effects: vomiting (10%), nausea (5%), diarrhea (3%) in > 2% of patients (n=135)• Monitoring parameters: none• Contraindications: none• Drug interactions: weak substrate of P‐glycoprotein • Storage: controlled room temperature, 25°C (77°F)• Patient education: taking all 20 doses, not chewing and discarding unused granules • Cost: not available as of 1/22/16 (FDA approved: 12/11/15)• Limitations:
• Not recommended for non‐emergent treatment of FU/capecitabine related ADRs• Safety and efficacy with initiation > 96 hours post FU/capecitabine administration not established
14
Alexandre IvanovPO
Uridine triacetate → uridine (pyrimidine analog) → high levels of intracellular uridine abrogate RNA‐directed cytotoxicity • FUTP – fluorouridine triphosphate• p53 – tumor suppressor gene
Orphan Drug
References: ● Vistogard (uridine triacetate) [prescribing information]. West Conshohocken, PA: Wellstat Therapeutics; December 2015. ● Longley DB, Harkin P, GJ Patrick. 5‐Fluorouracil: mechanisms of action and clinical strategies. Nature Reviews Cancer. 2003;3:330‐338.
3/14/2016
2016 NHIA Annual Conference & Exposition 15
Jadenu®(deferasirox) Ross Woods • Indications
• Chronic iron overload resulting from blood transfusion in patients ≥ 2 years• Chronic iron overload in patients with non‐transfusion‐dependent thalassemia (NTDT) syndromes with liver iron concentration (LIC) of ≥ 5 mg Fe/gram dry weight and serum ferritin > 300 mcg/L in patients ≥ 10 years old
• No clinical trials in patients with deferasirox. Approval was based off Exjade® trials
• Dose: • Transfusional Iron Overload: Initial dose 14 mg/kg (nearest whole tablet) once daily• NTDT syndromes: Initial dose 7 mg/kg (nearest whole tablet) once daily
• Storage: 25° C (77° F); protect from moisture
• Administration:• Once daily with water or other liquid on empty stomach or with light meal • Do not take with Al containing antacids; May be crushed and mixed with soft foods
15
References: (1) JADENU [package insert]. East Hanover, NJ: Novartis; October 2015. (2) JADENU. JADENU website. https://www.jadenu.com. Accessed December 21st, 2015. (3) Jadenu, Oral. In: Drug Facts and Comparisons (Facts and Comparisons eAnswers) [VCM Intranet]. St. Louis: Wolters Kluwer Health [updated September 2015 cited 2015 December]. [about 22 p.]. Available from http://online.factsandcomparisons.com (4) Red Book Online. In: Micromedex® System.Version 2.0 Greenwood Village, CO: Thomson Reuters (Healthcare) Inc. [updated 2015, cited 2015 Dec]. [about 4 p.]. Available from http://www.micromedexsolutions.com/ (5) Emedicine.medscape.com. Transfusion‐Induced Iron Overload: Background, Pathophysiology, Epidemiology. 2016. Available at: http://emedicine.medscape.com/article/1389732‐overview. Accessed January 15, 2016. (6)Taher A, Cappellini M. Management of Non‐Transfusion‐Dependent Thalassemia: A Practical Guide. Drugs. 2014;74(15):1719‐1729. doi:10.1007/s40265‐014‐0299‐0.
Oral
3/14/2016
2016 NHIA Annual Conference & Exposition 16
Jadenu® (deferasirox) Ross Woods• Warnings: Renal toxicity/impairment, hepatic toxicity/impairment, GI ulceration, bone marrow suppression, increased toxicity risk in Elderly, severe skin reactions, auditory and ocular disturbances, overchelation
• Monitoring:• Transfusional Iron Overload: weight, serum ferritin, CBC with differential, SCr and CrCl, urine protein, serum transaminases and bilirubin, auditory and ophthalmic examinations, GI hemorrhage, cumulative RBC units received
• NTDT: weight, serum ferritin, CBC with differential, SCr and CrCl, urine protein, serum transaminases and bilirubin, auditory and ophthalmic examinations, GI hemorrhage, LIC every 6 months
• ADRs: Skin rash, abdominal pain, diarrhea, nausea, vomiting, proteinuria, SCr increases• Cost: AWP $1000 to $4000 per 30 tablets; Assistance program through Novartis• Future Studies: No current studies with this formulation of deferasirox• Drug Interactions: Al containing antacids, CYP3A4, CYP2C8, and CYP1A2 metabolized agents; UDP‐glucuronosyltransferase (UGT) inducers; Bile acid sequestrants
• Education: hypersensitivity, infection, renal, hepatic, visual, and auditory changes, dyspepsia, skin reactions, hemorrhage, severe nausea and/or diarrhea
References: (1) JADENU [package insert]. East Hanover, NJ: Novartis; October 2015. (2) JADENU. JADENU website. https://www.jadenu.com. Accessed December 21st, 2015. (3) Jadenu, Oral. In: Drug Facts and Comparisons (Facts and Comparisons eAnswers) [VCM Intranet]. St. Louis: Wolters Kluwer Health [updated September 2015 cited 2015 December]. [about 22 p.]. Available from http://online.factsandcomparisons.com (4) Red Book Online. In: Micromedex® System.Version 2.0 Greenwood Village, CO: Thomson Reuters (Healthcare) Inc. [updated 2015, cited 2015 Dec]. [about 4 p.]. Available from http://www.micromedexsolutions.com/ (5) Emedicine.medscape.com. Transfusion‐Induced Iron Overload: Background, Pathophysiology, Epidemiology. 2016. Available at: http://emedicine.medscape.com/article/1389732‐overview. Accessed January 15, 2016. (6)Taher A, Cappellini M. Management of Non‐Transfusion‐Dependent Thalassemia: A Practical Guide. Drugs. 2014;74(15):1719‐1729. doi:10.1007/s40265‐014‐0299‐0.
16
Black Box WarningsRenal Failure, Hepatic
Failure, Gastrointestinal (GI)
Hemorrhage
3/14/2016
2016 NHIA Annual Conference & Exposition 17
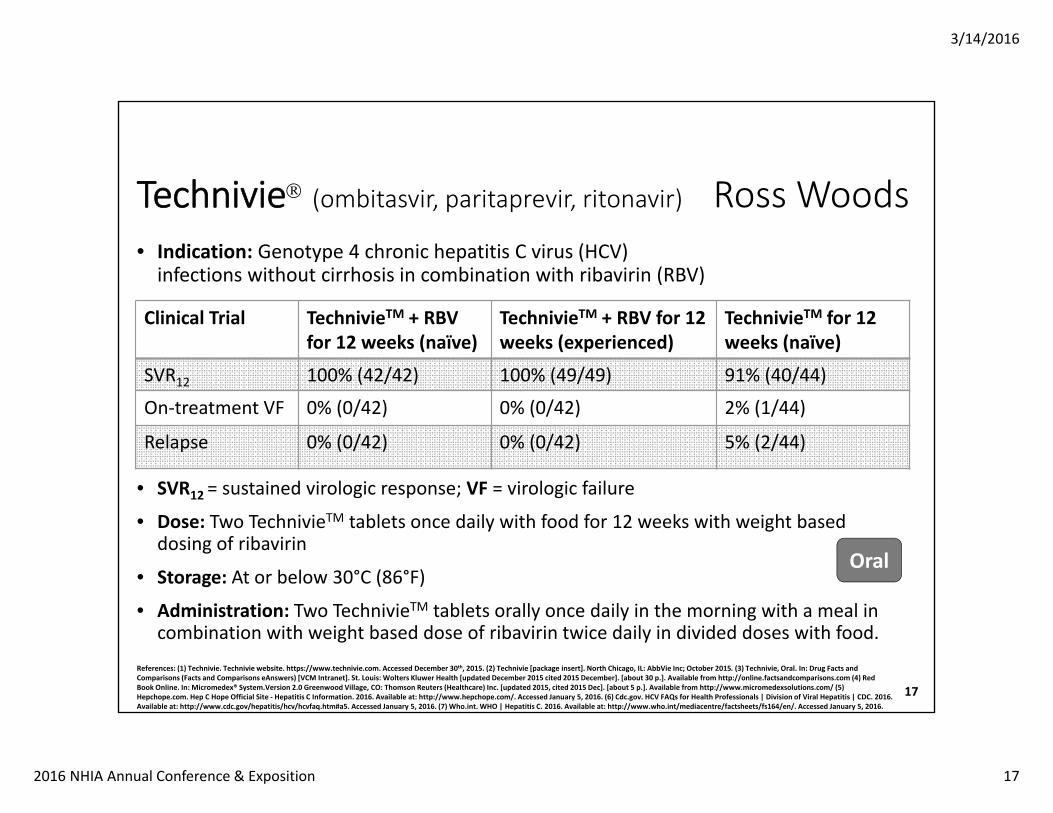
Technivie (ombitasvir, paritaprevir, ritonavir) Ross Woods • Indication: Genotype 4 chronic hepatitis C virus (HCV) infections without cirrhosis in combination with ribavirin (RBV)
• SVR12 = sustained virologic response; VF = virologic failure
• Dose: Two TechnivieTM tablets once daily with food for 12 weeks with weight based dosing of ribavirin
• Storage: At or below 30°C (86°F)
• Administration: Two TechnivieTM tablets orally once daily in the morning with a meal in combination with weight based dose of ribavirin twice daily in divided doses with food.
17
References: (1) Technivie. Technivie website. https://www.technivie.com. Accessed December 30th, 2015. (2) Technivie [package insert]. North Chicago, IL: AbbVie Inc; October 2015. (3) Technivie, Oral. In: Drug Facts and Comparisons (Facts and Comparisons eAnswers) [VCM Intranet]. St. Louis: Wolters Kluwer Health [updated December 2015 cited 2015 December]. [about 30 p.]. Available from http://online.factsandcomparisons.com (4) Red Book Online. In: Micromedex® System.Version 2.0 Greenwood Village, CO: Thomson Reuters (Healthcare) Inc. [updated 2015, cited 2015 Dec]. [about 5 p.]. Available from http://www.micromedexsolutions.com/ (5) Hepchope.com. Hep C Hope Official Site ‐ Hepatitis C Information. 2016. Available at: http://www.hepchope.com/. Accessed January 5, 2016. (6) Cdc.gov. HCV FAQs for Health Professionals | Division of Viral Hepatitis | CDC. 2016. Available at: http://www.cdc.gov/hepatitis/hcv/hcvfaq.htm#a5. Accessed January 5, 2016. (7) Who.int. WHO | Hepatitis C. 2016. Available at: http://www.who.int/mediacentre/factsheets/fs164/en/. Accessed January 5, 2016.
Oral
Clinical Trial TechnivieTM + RBV for 12 weeks (naïve)
TechnivieTM + RBV for 12 weeks (experienced)
TechnivieTM for 12 weeks (naïve)
SVR12 100% (42/42) 100% (49/49) 91% (40/44)
On‐treatment VF 0% (0/42) 0% (0/42) 2% (1/44)
Relapse 0% (0/42) 0% (0/42) 5% (2/44)
3/14/2016
2016 NHIA Annual Conference & Exposition 18
Technivie (ombitasvir, paritaprevir, ritonavir) Ross Woods • Warnings: hepatic decompensation, ALT elevation, risks associated with ribavirin, ADRs or reduced therapeutic effect due to drug interactions, risk of HIV‐1 protease inhibitor drug resistance in HCV/HIV‐1 co‐infections
• Monitoring: Baseline: Hepatic function tests, serum HCV‐RNA; During Therapy: Hepatic function tests within first 4 weeks then periodically; serum HCV‐RNA at the end of therapy, during follow up, then as clinically indicated.
• Studies: Recruiting for use in genotype 1 or 4 and treated early stage carcinoma with compensated cirrhosis; ongoing study in genotype 4 and decompensated cirrhosis
• ADRs: asthenia, fatigue, nausea, and insomnia
• Cost: AWP $1095.04 per 2 tablets; Assistance program through pparx.org
• Drug Interactions: Digoxin, antiarrhythmics, ketoconazole, voriconazole, quetiapine, amlodipine, fluticasone, furosemide, atazanavir, atazanavir/ritonavir, darunavir/ritonavir, lopinavir/ritonavir, rilpivirine, pravastatin, cyclosporine, tacrolimus, salmeterol, buprenorphine/naloxone, omeprazole, alprazolam
• Education: hypersensitivity reactions, liver impairment, severe asthenia, skin reactions, read medication guide, avoid during pregnancy, drug interactions, and missed dose info.
References: (1) Technivie. Technivie website. https://www.technivie.com. Accessed December 30th, 2015. (2) Technivie [package insert]. North Chicago, IL: AbbVie Inc; October 2015. (3) Technivie, Oral. In: Drug Facts and Comparisons (Facts and Comparisons eAnswers) [VCM ntranet]. St. Louis: Wolters Kluwer Health [updated December 2015 cited 2015 December]. [about 30 p.]. Available from http://online.factsandcomparisons.com (4) Red Book Online. In: Micromedex® System.Version 2.0 Greenwood Village, CO: Thomson Reuters (Healthcare) Inc. [updated 2015, cited 2015 Dec]. [about 5 p.]. Available from http://www.micromedexsolutions.com/ (5) Hepchope.com. Hep C Hope Official Site ‐ Hepatitis C Information. 2016. Available at: http://www.hepchope.com/. Accessed January 5, 2016. (6) Cdc.gov. HCV FAQs for Health Professionals | Division of Viral Hepatitis | CDC. 2016. Available at: http://www.cdc.gov/hepatitis/hcv/hcvfaq.htm#a5. Accessed January 5, 2016. (7) Who.int. WHO | Hepatitis C. 2016. Available at: http://www.who.int/mediacentre/factsheets/fs164/en/. Accessed January 5, 2016.
18
3/14/2016
2016 NHIA Annual Conference & Exposition 19
REPATHA (evolocumab) Noreen Chan Indication: Heterozygous familial hypercholesterolemia
• Along with diet and maximally tolerated statin therapy in adults • PCSK9 inhibitor
Clinical trials summary:• 8 placebo‐controlled trials that included 2651 patients, including 557 exposed for 6 months and 515 exposed for 1 year (median treatment duration of 12 weeks). Mean age was 57 years, 49% of the population were women, 85% white.
• The most common adverse reaction in a 52‐week controlled trial that led to treatment discontinuation and occurred at a rate greater than placebo was myalgia • (0.3% vs. 0% for evolocumab and placebo, respectively). • Adverse reactions led to discontinuation of treatment on 2.2% of evolocumab‐treated
patients and 1% of placebo patients• Amgen has completed enrollment in a study to clarify whether effects of evolocumab on LDL cholesterol levels translate into cardiovascular benefits
19References: Repatha package insert. http://pi.amgen.com/united_states/repatha/repatha_pi_hcp_english.pdfFamilial Hypercholesterolemia Foundation. https://thefhfoundation.org/about‐fh/what‐is‐fh/
Human mAb

3/14/2016
2016 NHIA Annual Conference & Exposition 20
REPATHA (evolocumab)• Dosing: 420 mg SC once monthly, 140 mg SC every 2 weeks• Administration: single‐use (1 time) pre‐filled auto injector (SureClick auto injector), or as a single‐use pre‐filled syringe
• 140 mg/ml subcutaneous solution• Store in refrigerator• Prior to use, store at room temperature in the original carton for up to 30 days without refrigeration
• Monitoring: LDL‐C, in patients with homozygous familial hypercholesterolemia, 4 to 8 weeks after therapy initiation
• Precautions: Latex allergy• Needle cover contains dry natural rubber (a latex derivative) and may cause allergic reaction
• Possible side effects: allergic reactions, runny nose, sore throat, symptoms of the common cold, flu or flu‐like symptoms, back pain, redness, pain or bruising at the injection site
• Drug‐drug interactions: none known at this time• Cost: Lexicomp AWP –$ 650.77, Eligible patients can get help paying with the Repathacopay card
References: Repatha package insert. http://pi.amgen.com/united_states/repatha/repatha_pi_hcp_english.pdfFamilial Hypercholesterolemia Foundation. https://thefhfoundation.org/about‐fh/what‐is‐fh/ 20
SQ Noreen Chan

3/14/2016
2016 NHIA Annual Conference & Exposition 21
Cresemba (isavuconazonium sulfate) Noreen Chan
Indication: Anti‐fungal used for invasive aspergillosis and mucomycosis
Dosing• Oral/IV – Loading dose of 372 mg PO/IV every 8 hours for 6 doses. Maintenance dose of 372 mg PO/IV every 8 hours 12‐24 hours after the last loading dose. No renal/hepatic dosing adjustments
IV Preparation ‐ Reconstitute with 5 mL of sterile water. Dissolve contents by gentle mixing or swirling. Avoid shaking vials. Further dilute using 250 mL NS or D5W and infuse over a minimum of 1 hour using a 0.2‐1.2 micron filter. Complete infusion within 6 hours of dilution if kept at room temperature or within 24 hours if kept under refrigeration
21References: (1) Cresemba [Isocunavonium Sulfate) [package insert]. Astellas Pharma US, INC. Northbrook, IL. June 2015
Oral/IV
Trial Endpoint Cresemba Voriconazole
SECURE(N=516)
Proven or probable invasive aspergillosis at EOT
43% 42%

3/14/2016
2016 NHIA Annual Conference & Exposition 22
Cresemba (isavuconazonium sulfate) Noreen Chan
Monitoring • Liver function tests, resolution of infection
Side effects, ADRs• Common – Peripheral edema (15.2%), hypokalemia (19.1%), constipation (14%), diarrhea (23.7%), nausea (27.6%), vomiting (25%), backache (10.1%), headache (16.7%), cough (12%), dyspnea (17.1%),
• Serious – Cholestasis, hepatitis (up to 5%), Increased LFT (17.1%), liver failure (up to 5%), hypersensitivity reaction (up to 5%), renal failure (10.1%), acute respiratory failure (10.1%), and infusion reaction (6.2%)
Care Plan: Advise patients to report signs of hepatitis, cholestasis, or hepatic failure. Advise patients to consult their physician before starting any new medications as this drug has many serious drug‐drug interactions.Pricing (AWP and/or AAWP)
• Capsule – 186 mg (14) ‐ $1176.00• IV solution – 372 mg (1) ‐ $286.00
References: (1) Cresemba [Isocunavonium Sulfate) [package insert]. Astellas Pharma US, INC. Northbrook, IL. June 2015 22
Oral/IV
3/14/2016
2016 NHIA Annual Conference & Exposition 23
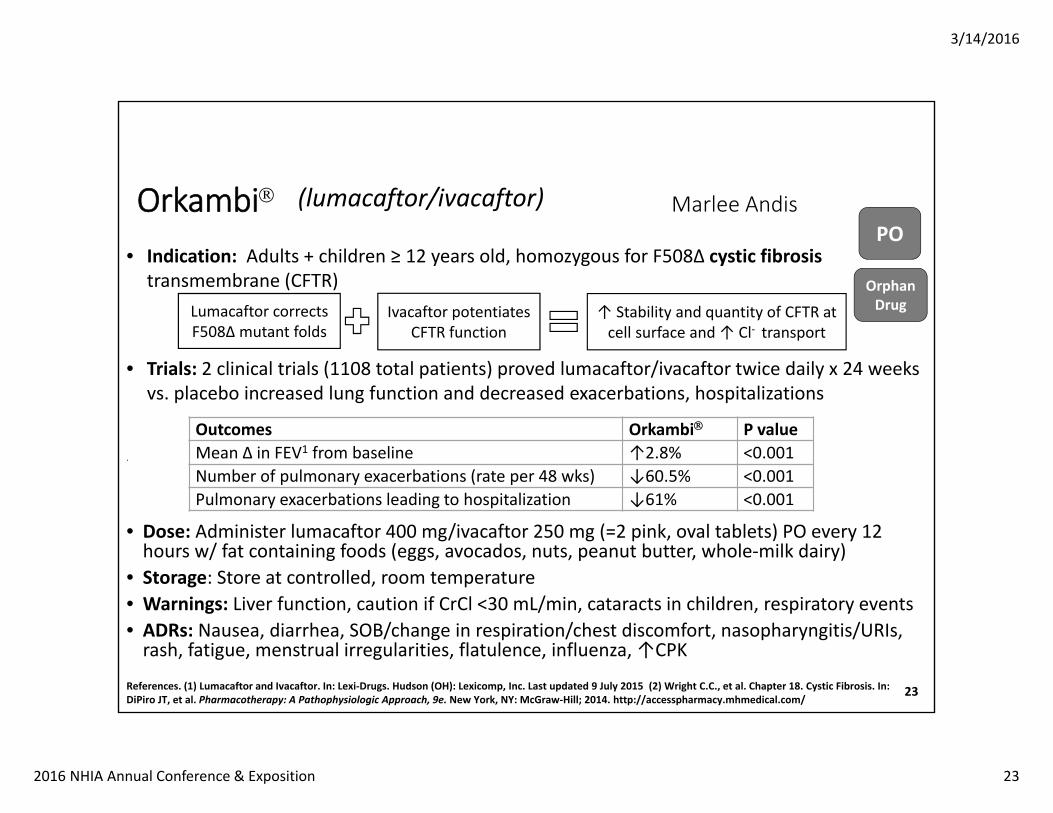
Orkambi Marlee Andis
• Indication: Adults + children ≥ 12 years old, homozygous for F508∆ cystic fibrosis transmembrane (CFTR)
• Trials: 2 clinical trials (1108 total patients) proved lumacaftor/ivacaftor twice daily x 24 weeks vs. placebo increased lung function and decreased exacerbations, hospitalizations
.
• Dose: Administer lumacaftor 400 mg/ivacaftor 250 mg (=2 pink, oval tablets) PO every 12 hours w/ fat containing foods (eggs, avocados, nuts, peanut butter, whole‐milk dairy)
• Storage: Store at controlled, room temperature• Warnings: Liver function, caution if CrCl <30 mL/min, cataracts in children, respiratory events• ADRs: Nausea, diarrhea, SOB/change in respiration/chest discomfort, nasopharyngitis/URIs, rash, fatigue, menstrual irregularities, flatulence, influenza, ↑CPK
23References. (1) Lumacaftor and Ivacaftor. In: Lexi‐Drugs. Hudson (OH): Lexicomp, Inc. Last updated 9 July 2015 (2) Wright C.C., et al. Chapter 18. Cystic Fibrosis. In: DiPiro JT, et al. Pharmacotherapy: A Pathophysiologic Approach, 9e. New York, NY: McGraw‐Hill; 2014. http://accesspharmacy.mhmedical.com/
PO
Orphan Drug
(lumacaftor/ivacaftor)
Outcomes Orkambi P valueMean ∆ in FEV1 from baseline ↑2.8% <0.001Number of pulmonary exacerbations (rate per 48 wks) ↓60.5% <0.001Pulmonary exacerbations leading to hospitalization ↓61% <0.001
Lumacaftor corrects F508∆ mutant folds
Ivacaftor potentiates CFTR function
↑ Stability and quantity of CFTR at cell surface and ↑ Cl‐ transport
3/14/2016
2016 NHIA Annual Conference & Exposition 24
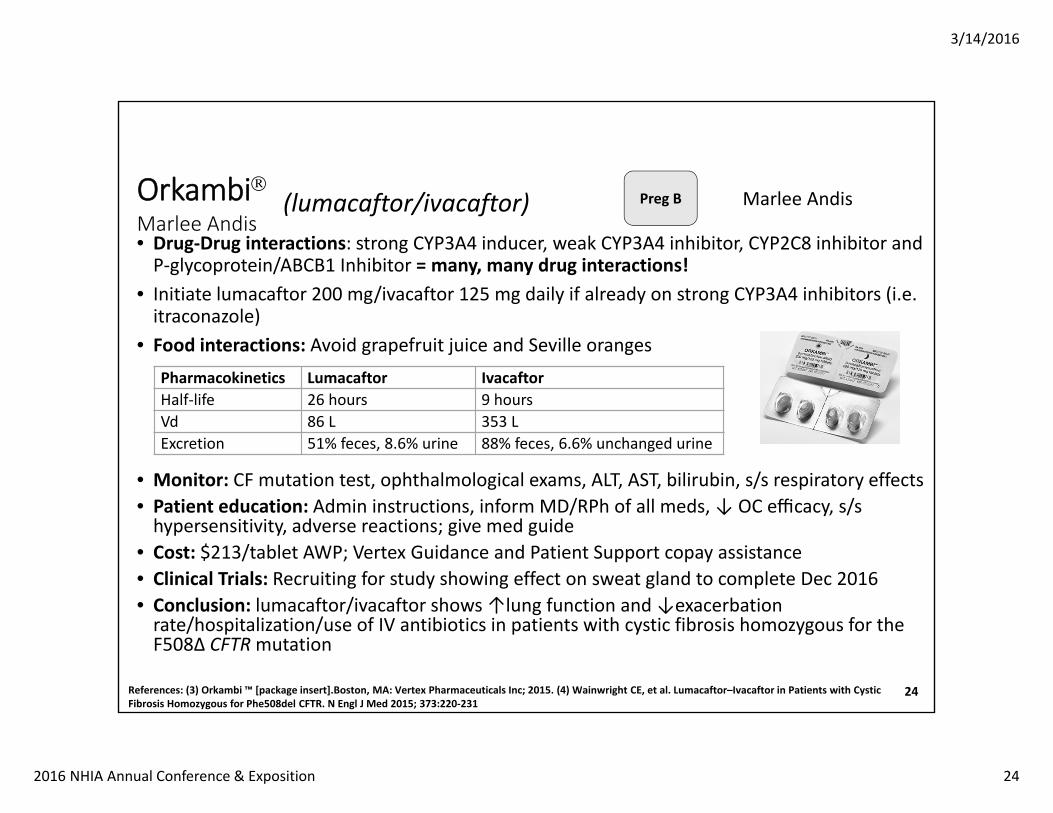
OrkambiMarlee Andis • Drug‐Drug interactions: strong CYP3A4 inducer, weak CYP3A4 inhibitor, CYP2C8 inhibitor and P‐glycoprotein/ABCB1 Inhibitor = many, many drug interactions!
• Initiate lumacaftor 200 mg/ivacaftor 125 mg daily if already on strong CYP3A4 inhibitors (i.e. itraconazole)
• Food interactions: Avoid grapefruit juice and Seville oranges
• Monitor: CF mutation test, ophthalmological exams, ALT, AST, bilirubin, s/s respiratory effects• Patient education: Admin instructions, inform MD/RPh of all meds,↓ OC efficacy, s/s hypersensitivity, adverse reactions; give med guide
• Cost: $213/tablet AWP; Vertex Guidance and Patient Support copay assistance• Clinical Trials: Recruiting for study showing effect on sweat gland to complete Dec 2016• Conclusion: lumacaftor/ivacaftor shows ↑lung function and ↓exacerbation rate/hospitalization/use of IV antibiotics in patients with cystic fibrosis homozygous for the F508∆ CFTRmutation
References: (3) Orkambi ™ [package insert].Boston, MA: Vertex Pharmaceuticals Inc; 2015. (4) Wainwright CE, et al. Lumacaftor–Ivacaftor in Patients with Cystic Fibrosis Homozygous for Phe508del CFTR. N Engl J Med 2015; 373:220‐231
24
(lumacaftor/ivacaftor)
Pharmacokinetics Lumacaftor IvacaftorHalf‐life 26 hours 9 hoursVd 86 L 353 LExcretion 51% feces, 8.6% urine 88% feces, 6.6% unchanged urine
Preg B Marlee Andis

3/14/2016
2016 NHIA Annual Conference & Exposition 25
Nucala Marlee Andis
• Description: Monoclonal antibody; IL‐5 antagonist• Indication: Add‐on maintenance for severe asthma in adults + children ≥12 years old w/eosinophilic phenotype
• MOA: Blocks growth, differentiation, recruitment, activation, and survival of eosinophils • Trials‐ ranging (Trial 1) and 2 confirmatory trials (Trial 2 and 3); no head to head trials
• Dosing: 100 mg SC (upper arm, thigh, abdomen) every 4 weeks; no dosage adjustment in renal or hepatic impairment
• Warnings: Hypersensitivity, herpes zoster, do not administer if active helminth infection, gradually taper down corticosteroids
• ADRs: Hypersensitivity, injection site reaction, HA, fatigue, back pain, muscle spasm, eczema/pruritus, abdominal pain, UTI, influenza and immunogenicity
• DDI: no known significant interactions
25References: (1) Mepolizumab. In: Lexi‐Drugs. Hudson (OH): Lexicomp, Inc. Last updated 5 Nov 2015. (2)Nucala® [package insert]. GlaxoSmithKline LLC, Philadelphia, PA; 2015 (3) Kelly H, et al. Chapter 15. Asthma. In: DiPiro JT, et al. Pharmacotherapy: A Pathophysiologic Approach, 9e. New York, NY: McGraw‐Hill; 2014. (4) Ortega HG, et al. Mepolizumab Treatment in Patients with Severe Eosinophilic Asthma. N Engl J Med 2014;371:1198‐207.
SQ Biologic(mepolizumab)
Trial Primary Outcome ResultDREAM (Trial 1; n=621) Rate of clinically significant
exacerbations↓48% in 75 mg IV mepolizumab vs. placebo (p<0.001)
SIRIUS (Trial 2; n=135) Degree of ↓ in glucocorticoid dose
2.39 odds ratio for reduction in dose category with mepolizumab (p=0.008)
MENSA (Trial 3; n=576) Frequency of clinically significant exacerbations
↓47% in SQ mepolizumab (p<0.001)

3/14/2016
2016 NHIA Annual Conference & Exposition 26
Nucala Marlee Andis• Pharmacokinetics: Vd = ~3.6 L; T ½ = 16‐22 days; excretion non‐renal• Prep/Storage: Unused vials below 25°C (77°F); do not freeze; protect from light
• Reconstitute with 1.2 mL SWFI for 100mg/mL and administer immediately• May take up to 5 minutes to dissolve completely• Do not shake vial• Solution should be clear to opalescent, colorless to pale yellow or pale brown• Discard within 8 hours of reconstitution (no extended stability)
• Patient education: Hypersensitivity, reconstitution technique, not for acute symptoms, shingles vaccine, s/s hypersensitivity, adverse reactions; give med guide
• Monitor: FEV1, peak flow, PFT, increased SABA use• Cost: 100 mg vial = $3000 AWP; $0 Copay Program for those with private, non‐government‐funded, commercial insurance
• Clinical Trials: Recruiting for: SQ use in children aged 6‐11, cessation vs. continuation, compassionate use in Hypereosinophilic Syndrome (HES), Use in Bullous Pemphigoid (BP)
• Conclusion: Nucala® (mepolizumab) can help decrease asthma exacerbations and glucocorticoid use in those with severe asthma and an eosinophilic phenotype.
References: (5) Pavord ID, et al. Mepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double‐blind, placebo‐controlled trial. Lancet 2012; 380: 651–59. (6) Bel EH, et al. Oral Glucocorticoid‐Sparing Effect of Mepolizumab in Eosinophilic Asthma. N Engl J Med 2014;371:1189‐97. (7) FDA approves Nucalato treat severe asthma. FDA News Release. Last updated Nov 6, 2015.
26
(mepolizumab)Preg:Not rated

3/14/2016
2016 NHIA Annual Conference & Exposition 27
• Description: Human IgG1 monoclonal antibody that binds interleukin‐17A • MOA: Blocks the interaction of IL‐17A with the receptor, IL‐17 that occurs during normal inflammatory and immune responses.
• Indication: Moderate to severe plaque psoriasis • Dose: 300mg SC at weeks 0, 1, 2, 3, and 4 followed by 300mg SC every 4 weeks.• Supplied: Sensoready pen, pre‐filled syringes, vials
27References:
SecukinumabCosentyx
Elizabeth Lagasse, PharmDPGY‐1 Pharmacy Resident
Trial Endpoint Secukinumab 300mg Secukinumab 150mg Placebo
1 Reduction in PASI score of ≥ 75% at week 12
N=245200 (82%)
N=245174 (71%)
N=24811 (4%)
2 Reduction in PASI score of ≥ 75% at week 12
N=327249 (76%)
N=327219 (67%)
N=32616 (5%)
3 Reduction in PASI score of ≥ 75% at week 12
N=5944 (75%)
N=5941 (69%)
N=590 (0%)
4 Reduction in PASI score of ≥ 75% at week 12
N=6052 (87%)
N=6143 (70%)
N=612 (3%)
Human mAb SC

3/14/2016
2016 NHIA Annual Conference & Exposition 28
• Warnings‐ hypersensitivity, Crohn’s disease exacerbations, risk of serious infections
• ADRs‐ Nasopharyngitis, diarrhea, and upper respiratory tract infection
• DDI – Live vaccines• CI – serious hypersensitivity reactions to secukinumab• Patient Education – s/s of infection or hypersensitivity• Monitoring – s/s of TB, infection, exacerbation of Crohn’s Dx• Studies – other forms of psoriasis, alopecia areata, atopic dermatitis, psoriatic arthritis, ankylosing spondylitis, rheumatoid arthritis
• Cosentyx Connect program provide co‐pay assistance
28
SecukinumabCosentyx
Elizabeth Lagasse, PharmDPGY‐1 Pharmacy ResidentSCHuman
mAb

3/14/2016
2016 NHIA Annual Conference & Exposition 29
Kanuma® (Sebelipase alfa) Collin ChanIndication: Lysosomal Acid Lipase Deficiency
Clinical Trials Summary:1) 6 of 9 patients who received sebelipase alfa survived beyond 12 months, with
1 patient surviving past 15 months vs. 0 of 21 patients who did not receive sebelipase alfa survived past 8 months in a historical cohort
2) ALT was normalized in 31% of patients (66 children and adults) who had LAL Deficiency. Patients received 1 mg/kg every other week x 20 weeks
Dosing: Newborn: 1 mg/kg IV qWeekly, which may increase to 3 mg/kg qWeekly
• Pediatric and Adults with LAL Deficiency: 1 mg/kg IV every other week
29References: Sebelipase alfa for injection [package insert]. Alexion Pharmaceuticals Inc. Dec 2015.
IV Orphan Drug
Weight (kg)1 mg/kg 3 mg/kg
Total Volume (mL) Total Volume (mL)1 ‐ 10.9 10 2511 ‐ 24.9 25 5025 ‐ 49.9 50 10050 ‐ 99.9 100 250
100 ‐ 120.9 250 500

3/14/2016
2016 NHIA Annual Conference & Exposition 30
Preparation: (Refer to the package insert’s table for the required dilution volume)• Withdraw the total calculated dose from the required vials and dilute with NS
Administration:• Using a 0.2 micron filter, infuse over 2 hours, with longer infusion times for patients with
hypersensitivity reactions and for those receiving a 3 mg/kg dose. A 1 hour infusion may be considered for patients receiving 1 mg/kg if tolerated prior infusions
Monitoring: Hypersensitivity reactions, lipid panel, ALT, antibody assessmentsPrecautions and Warnings: Hypersensitivity Reactions, allergy to eggs Adverse Reactions: • Newborns: Diarrhea, vomiting, fever, rhinitis, anemia, cough, nasopharyngitis, urticaria. • For pediatric and adult patients: Headache, fever, oropharyngleal pain, nasopharyngitis,
asthenia, constipation, nausea
Care Plan: Educate patients of the above precautions, warnings, and adverse reactionsCosts: AWP and/or AAWP: 20 mg / 10 mL vial ‐ $12,000
30References: Burton BK, et al. A Phase 3 Trial of Sebelipase Alfa in Lysosomal Acid Lipase Deficiency. N Engl J Med. 2015 Sep 10;373(11):1010‐20.
Kanuma® (Sebelipase alfa) Collin Chan

3/14/2016
2016 NHIA Annual Conference & Exposition 31
Coagadex® (Coagulation Factor X) Collin Chan• Indication:
1) On‐demand treatment and control of bleeding episodes2) Perioperative management of bleeding in major surgery in patients with mild hereditary
Factor X deficiency
• Clinical Trials Summary:1) Control of Bleeding Episodes – 16 patients with 98 major and 88 minor bleeding
episodes saw hemostasis in 98% of cases after 1‐4 infusions (83% with 1 infusion)2) Perioperative Management – 5 patients with 7 procedures saw hemostasis in major
surgeries after a median of 13 infusions and in minor surgeries after 2.5 infusions.
• Dosing:• Bleeding episodes:
• 25 IU / kg / dose. May repeat q24 hrs until bleeding stops• Perioperative Management of Bleeding
• Dose = Body weight (kg) x Desired Factor X Increase (IU/dL) x 0.5• Pre‐surgery goal: 70‐90 IU/dL• Post‐surgery goal: ≥ 50 IU/dL• Repeat dose as necessary to maintain plasma levels at goal
• Max of 60 IU / kg / day
31References: Coagadex® (Coagulation Factor X[Human]) [package insert]. Durham, NC 27701: Bio Products Laboratory; 2015.
IV
Orphan Drug
3/14/2016
2016 NHIA Annual Conference & Exposition 32
Coagadex® (Coagulation Factor X) Collin Chan
• Preparation: Reconstitute with the SWFI and transfer device that comes with the medication for a final concentration of 100 IU/mL. Withdraw into a syringe. If using more than one vial, draw up all the solutions into a single syringe. Use the product immediately after reconstitution.
• Administration: Attach a suitable needle to the syringe, administer intravenously at a rate of 10 mL/min, but no more than 20 mL/min
• Monitoring: Factor X activity and levels; Development of Factor X inhibitors• Precautions and Warnings: Hypersensitivity Reactions, neutralizing Antibodies (inhibitors), transmissible Infectious Agents (made from human blood)
• Adverse Reactions: Infusion site reactions, fatigue, back pain• Care Plan: Educate patients of the above precautions and warnings• Drug Interactions: Use with caution in patients receiving other medications that may contain Factor X or medications that may inhibit Factor Xa
• Costs:• AWP and/or AAWP: 250 Units ‐ $9.29; 500 Units ‐ $9.29
32References: Coagadex® (Coagulation Factor X[Human]) [package insert]. Durham, NC 27701: Bio Products Laboratory; 2015.
3/14/2016
2016 NHIA Annual Conference & Exposition 33
Unituxin (dinutuximab) Jesse S. Peterson• Indication
• GD2‐binding monoclonal antibody approved March 2015• Pediatric patients with high‐risk neuroblastoma who achieved partial response to 1st line multivalent, multimodality therapy
• Approved in combination with granulocyte‐macrophage colony‐stimulating factor (GM‐CSF), interleukin‐2 (IL‐2), and 13‐cis‐retinoic acid (isotretinoin)
• Dosing• Recommended: 17.5 mg/m2/day administered as an IV infusion over 10 to 20 hours for 4 consecutive days for a maximum of 5 cycles
• Initiate at an infusion rate of 0.875 mg/m2/hour for 30 minutes. May increase as tolerated to a maximum rate of 1.75 mg/m2/hour
• Preparation • Single‐use vial containing 17.5mg/5mL solution to be refrigerated at 2°C to 8°C• Protect from light | Do not shake | Do not freeze
• Administration• Pretreatment with antihistamines, analgesics, antipyretics, and IV hydration is required prior to each dose of dinutuximab
33References: Unituxin® [package insert]. Silver Spring, MD: United Therapeutics Corp.; 2015
IV
Orphan Drug
Biologic
3/14/2016
2016 NHIA Annual Conference & Exposition 34
• Clinical Trial Summary • Randomized (1:1) cohort of a single, open‐label, multicenter trial including 226 patients randomized to dinutuximab, isotretinoin, GM‐CSF, and IL‐2 or isotretinoin
• Three years after treatment assignment 63% of dinutuximab group was alive and free of tumor growth or recurrence compared to 46% with isotretinoin alone
• No drug‐drug interaction studies have been conducted • Phase II: Recurrent osteosarcoma (dinutuximab + GM‐CSF)
• Warnings and Precautions Serious infusion reactions | Pain and peripheral neuropathy Capillary leak syndrome (CLS) | Systemic infection | Neurological disorders of the eye Atypical hemolytic uremic syndrome | Bone marrow suppression| Serum electrolytes
• Most Common Adverse Drug Reactions (≥ 25%) Pain/Fever| Thrombocytopenia | Lymphopenia | Infusion reactions | Hypotension Na+ | Ca++ | ALT/AST | Anemia | Vomiting | Urticaria | Hypoalbuminemia
• Most Common Serious Adverse Drug Reactions (≥ 5%) Infection | Infusion reaction | Hypokalemia | Hypotension | Pain/Fever | CLS
References: Unituxin® [package insert]. Silver Spring, MD: United Therapeutics Corp.; 2015 34
Black Box
Warning
Unituxin (dinutuximab) Jesse S. Peterson
3/14/2016
2016 NHIA Annual Conference & Exposition 35
Natpara Joshua Jaussi
• Indication: Hypocalcaemia secondary to hypoparathyroidism.
• Clinical Trial: Evaluated in a 24‐week, randomized, double‐blind, placebo‐controlled, multicenter trial. Patients with established hypoparathyroidism receiving calcium and active forms of vitamin D (vitamin D metabolite or analogs) were randomized (2:1) to NATPARA (n=84) or placebo (n=40).
• Dosing: Recommended initial dose is 50 mcg once daily administered subcutaneously in the thigh (alternating thighs daily). For dose titration, the following is recommended: for serum calcium less than 8 mg/dL, increase the dose in increments of 25 mcg subcutaneously every 4 weeks. Maximum dose: 100 mcg subcutaneously once daily.
• Preparation: Unmixed medicine cartridges: Refrigerate between 36°F to 46°F (2°C to 8°C). Mixed medicine cartridges: Refrigerate between 36°F to 46°F (2°C to 8°C). You can use the Q‐Cliq pen for up to 14 days after mixing the medicine cartridge. Discard mixed medicine cartridges 14 days after mixing. Do not freeze.
• Administration: Patient can self‐administer via SC injection.
References: Parathyroid hormone (Natpara) for injection package insert. Bedminster, NJ: NPS Pharmaceuticals, Inc.; 2015 Jan. Parathyroid hormone therapy for hypoparathyroidism Cusano, Natalie E. et al. Best Practice & Research Clinical Endocrinology & Metabolism , Volume 29 , Issue 1 , 47 ‐ 55 Clinical Pharmacology [Internet]. Tampa, (FL): Elsevier/Gold Standard, Inc. c2015. Natpara [updated 2015 Oct 23; cited 2015 Nov 15].
35
SQ Orphan Drugparathyroid hormone
3/14/2016
2016 NHIA Annual Conference & Exposition 36
Natpara Joshua Jaussiparathyroid hormone
• Recommended monitoring: serum 25(OH)D concentrations serum albumin and calcium, serum intact parathyroid hormone concentrations (iPTH). Safety and efficacy of parathyroid hormone have not been established in pediatric patients.
• ADRs: nausea, vomiting, diarrhea, upper abdominal pain, paresthesia, headache, hypoesthesia, facial hypoesthesia, arthralgia, extremity musculoskeletal pain, and neck pain.
• Care plan: Available only through a restricted program called the NATPARAREMS Program, because of the potential risk of osteosarcoma.
• Drug interactions: Alendronate and digoxin.
• Cost: $4987.50 per cartridge ‐ Discount drug card available.
Parathyroid hormone (Natpara) for injection package insert. Bedminster, NJ: NPS Pharmaceuticals, Inc.; 2015 Jan. Parathyroid hormone therapy for hypoparathyroidism Cusano, Natalie E. et al. Best Practice & Research Clinical Endocrinology & Metabolism , Volume 29 , Issue 1 , 47 ‐ 55 Clinical Pharmacology [Internet]. Tampa, (FL): Elsevier/Gold Standard, Inc. c2015. Natpara [updated 2015 Oct 23; cited 2015 Nov 15].
36
There is a potential risk of osteosarcoma (osteogenic sarcoma) with the use of parathyroid hormone.
SQ Orphan Drug
3/14/2016
2016 NHIA Annual Conference & Exposition 37
Avycaz
Ceftazidime & Avibactam• Description: 3rd Generation Cephalosporin/Non‐Beta Lactam Beta Lactamase Inhibitor Combination• Indication: Complicated Intra‐Abdominal Infections (cIAI) & Urinary Tract Infections (cUTI)• MOA: Binds to penicillin‐binding proteins inhibit cell wall synthesis causing cell lysis while beta
lactamase inhibitor prevents beta‐lactamases deactivating cephalosporin• Dosing: cIAI: 2.5g IV every 8 hrs in combination with metronidazole x 5‐14 days; cUTI: 2.5g IV every 8
hrs x 7‐14 days• Renally Adjust: CrCl 31‐50=1.25g q 8 hrs; CrCl 16‐30=0.94 g q 12 hrs; CrCl 6‐15=0.94 g q 24 hrs; CrCl <5=0.94 g q
48 hrs
• Admin: Intermittent IV infusion over 2 hours• Reconstitute w/ 10mL of SWI, NS, D%W, or LR• Dilute further in 50‐250 mL; BUD 12hrs (room), 24hrs (refrigerate)
• Warnings: Hypersensitivity, C. difficile associated Diarrhea, decreased clinical response with baseline CrCl 30 to ≤50 mL/min, bacterial resistance, neurological rxns
• ADRs: Anxiety, constipation, nausea, & vomiting• DDI: Probenecid & false‐positives for glucose in urine• Contraindications: Hypersensitivity to ceftazidime, avibactam, other Cephalosporins
371) Adult UTI: American Urological Association." Adult UTI: American Urological Association. American Urological Association, n.d. Web. 22 Jan. 2016. 2) Avycaz ceftazidime/avibactam [prescribing information]. Cincinnati, OH: Forest Pharmaceuticals; September 2015. 3) Ceftazidime and Avibactam." LexiComp. N.d. Lexicomp. Web. 05 Jan. 2016. 4) Safety and Tolerability of Ceftazidime‐Avibactam for Pediatric Patients With Suspected or Confirmed Infections." Safety and Tolerability of Ceftazidime‐Avibactam for Pediatric Patients With Suspected or Confirmed Infections. AstraZeneca & Forest Laboratories, 11 June 2015. Web. 22 Jan. 2016.
IV
Alfred Olumba

3/14/2016
2016 NHIA Annual Conference & Exposition 38
AvycazCeftazidime & Avibactam
• Pharmacokinetics: Ceft/Avi Vd: 18L/23L; Ceft/Avi T½: 3hr/2.5hr• How supplied: 2.5 gram single dose vial• Cost: $342 per vial, No Co‐pay assistance program available • Monitor: Hypersensitivity, infection symptoms, renal function particularly in renal impairment
• Patient Education: Hypersensitivity, possibility of serious diarrhea, neurological, antibiotic resistance
• Clinical Trials:• Phase 2 trials showed similar ADR with other treatments in cIAI & cUTI• No head‐to‐head trials/ ADR comparison of treatments only!• 2 Trials underway: Safety trial in pediatric patients & Pharmacokinetic study in cystic fibrosis• Phase 3 Trial: cIAI in 2.5% of Ceft/Avi + metronidazole vs. 1.5% meropenem
• 25.8% of Death in Ceft/Avi + metronidazole with CrCl 30‐50 mL/min
5) Steady‐state Pharmacokinetics of Ceftazidime/Avibactam in Cystic Fibrosis." Steady‐state Pharmacokinetics of Ceftazidime/Avibactam in Cystic Fibrosis. ClinicalTrials.gov/University of Southern California, 20 July 2015. Web. 05 Jan. 2016. https://clinicaltrials.gov/ct2/show/NCT02504827?term=avycaz&rank=3 6) UTI and CAUTI." UTI and CAUTI. Virgina Department Of Health, 2016. Web. 22 Jan. 2016http://www.vdh.virginia.gov/epidemiology/surveillance/hai/uti.htm 7) Clinical Updates in Infectious Diseases: Intraabdominal Infections‐A Surgical Perspective." Clinical Updates in Infectious Diseases. National Foundation for Infectious Diseases, 1996. Web. 22 Jan. 2016. http://www.nfid.org/content‐conversion/idarchive/intraabdominal.html
38
Alfred Olumba

3/14/2016
2016 NHIA Annual Conference & Exposition 39
Questions?
Download the Complete Drug Information Sheet and Learning Assessment Questions/Answers from www.nhia.org/ac16/handouts
39