
New Oral Anticoagulants: A Review
26
New Oral Anticoagulants: A Review Babak Moini, MD Veterans Affairs Hospital Noon Lecture Series
-
Upload
hayes-fuentes -
Category
Documents
-
view
41 -
download
2
description
New Oral Anticoagulants: A Review. Babak Moini, MD Veterans Affairs Hospital Noon Lecture S eries. Acknowledgment:. Some of the slides were borrowed from Amanda Miller Phar.D. Case1. - PowerPoint PPT Presentation
Transcript of New Oral Anticoagulants: A Review

New Oral Anticoagulants: A Review
Babak Moini, MDVeterans Affairs Hospital
Noon Lecture Series
Acknowledgment:Some of the slides were borrowed from Amanda
Miller Phar.D.

Case168 male with hx of DM, CHF and prior ischemic
CVA admitted for new afib. He has a hx of non-compliance.
CHADs2: 4.
Which anticoagulant to send him home with?
Oral Anticoagulants Available in US
Coumadin
warfarin
1954
Pradaxa®
dabigatran
2010
Xarelto®rivaroxab
an
2011
Eliquis®apixaban
2012

Mechanism of ActionMedication Mechanism of Action
Coumadin (warfarin)
Vitamin K Antagonist
Pradaxa (dabigatran)
Direct Thrombin Inhibitor
Xarelto (rivaroxaban)
Factor Xa Inhibitor
Eliquis (apixaban)
Factor Xa Inhibitor
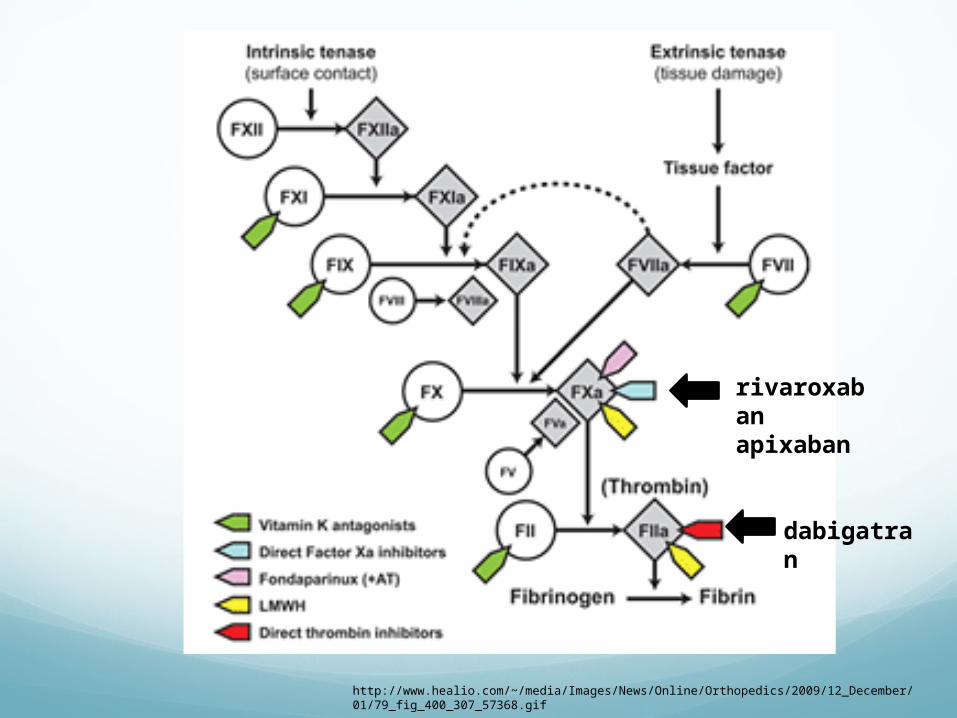
http://www.healio.com/~/media/Images/News/Online/Orthopedics/2009/12_December/01/79_fig_400_307_57368.gif
rivaroxabanapixaban
dabigatran

Pharmacology:Coumadin Dabigatran Rivaroxaba
nApixaban
Bioavailability
100% 3-7% 60-100% 50%
Protein bound
99% 30% 90-95% 80-85%
Metabolism CYP Conjugation CYP CYP
Half Life 40hrs 12-17hrs 5-9hrs 12hrs
Onset of action
72hrs 1-2hrs 2-4hrs 2-4hrs
Elimination Liver Renal Renal Renal

Indications: USCoumadin Dabigatrn Rivaroxaba
nApixaban
Afib + + (RELY) + (ROCKET-AF)
+ (Aristotle)+ (AVERROES)
DVT/PE + Not yet. (RECOVER) +
(EINSTEIN)
Post TKA/THADVT prophylaxis
+ + + (RECORD 1-3)
+ (ADVANCE)
Not yet approved: Rivaroxaban for prophylaxis of DVT in medically ill patients (MAGELLAN). Rivaroxaban vs Enoxaparin. NI < 30 days, superior at 35 days.
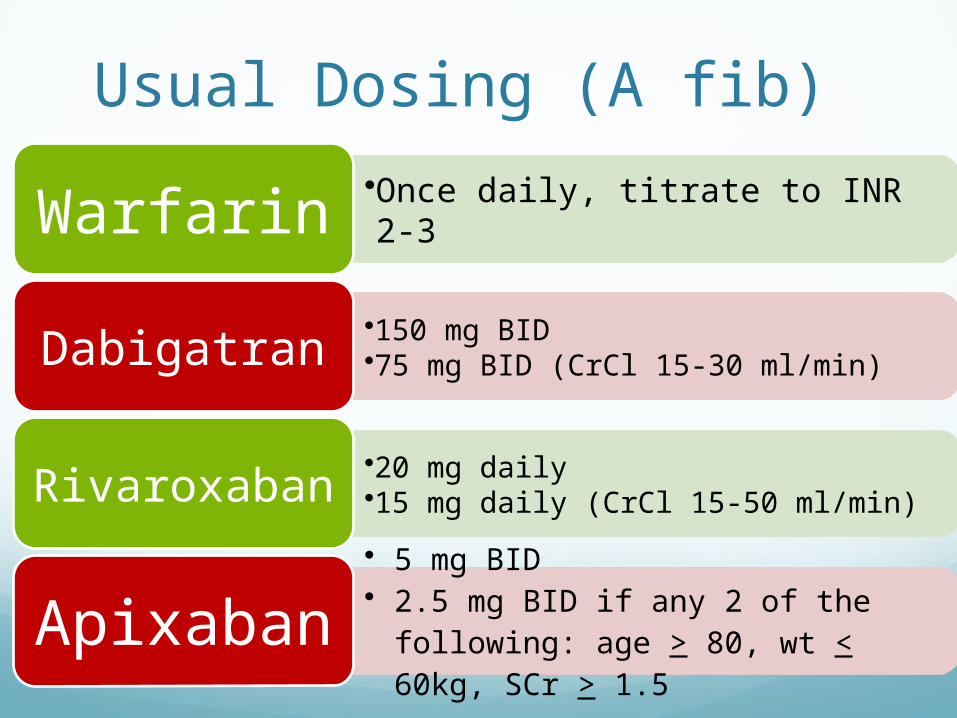
Usual Dosing (A fib)
•Once daily, titrate to INR 2-3Warfarin•150 mg BID •75 mg BID (CrCl 15-30 ml/min) Dabigatran
•20 mg daily•15 mg daily (CrCl 15-50 ml/min) Rivaroxaban
• 5 mg BID• 2.5 mg BID if any 2 of the
following: age > 80, wt < 60kg, SCr > 1.5
Apixaban

Usual Dosing (VTE)Only FDA-approved agent = rivaroxaban
VTE Prophylaxis (knee/hip surgery) 10mg once daily (up to 35 days) No renal dose (CrCl < 30 ml/min avoid)
VTE Treatment: 15 mg BID x 3 weeks then 20mg daily No renal dose (CrCl < 30 ml/min avoid)

Perioperative Recommendations
• Hold 1-2 days before procedure • CrCl < 50 hold 3-5 days
Dabigatran
• Low bleed risk hold 1 day• CrCl < 30/ low risk hold 2 days• High bleed risk hold 2 days• CrCl < 30/ high risk hold 4 days
Rivaroxaban
• Low bleed risk hold x 1 day • High bleed risk hold x 2 days
Apixaban
Dabigatran PI, Blood 2012;119:3016-23

Major Side Effects:Bleeding: varied definition in each study.
GI ICHMajor (drop in Hgb by 2, life threatening).
Dabigatran: Pills are made in acidic content, hence has 20%
rate of GI side effects. ? Observed increase risk of GI bleeding.

Monitoring Levels:Coumadin: INR
New Oral anticoagulants: no standardized studies. No accurate quantitative measures.
Dabigatran: ECT, Thrombin clotting timeRivaroxaban: special anti-Xa activityAbixaban special anti-Xa activity

Drug-Drug Interactions:No where as severe as with Warfarin.
Dabigatran: P-glycoprotein, pro-drug.Needs acidic environment, avoid co-administration
with PPI.
Rivaroxaban: CYP-450 and P-glycoprotein. Caution with dual inhibitors (Ketoconazole,
Itroconazole, Clarithromycin). No dose adjustments needed.
Abixaban: CYP3A4 and P-glycoprotein.Decrease dose to 2.5mg bid in dual inhibitors.

Switching To/From Warfarin
Medication Recommendations for Conversion
DabigatranStop warfarin, initiate dabigatran when INR < 2
Initiate warfarin 3 days before D/C dabigatran
Rivaroxaban
Stop warfarin, initiate rivaroxaban when INR < 2-3
Initiate warfarin with bridging 24 hours after D/C rivaroxaban
Apixaban
Stop warfarin, initiate apixaban when INR < 2
Initiate warfarin with bridging when next apixaban dose is due.
Gonsalves Et al. Mayo Clinic Proc. 5-2013
Treatment of Bleeding:No evidence based guidelines.
Remember that unlike Coumadin, the new OAC will continuously bind to factor Xa or thrombin, hence making FFP less useful.
Current available Rx for life threatening active bleeding: based on case reports. Factor VII PCC: 3 and 4 factor concentrates. HD: only for Dabigatran. Large volume of distribution. Charcoal

Trials vs Warfarin for A Fib RE-LY
DAB vs WARROCKET-AFRIV vs WAR
ARISTOTLEAPIX vs WAR
Comparator Dabigatran Rivaroxaban Apixaban
Design Open-label, blind outcomes, noninferiority
Double-blind, noninferiority
Double-blind, noninferiority
Sample size n = 18,113 n = 14,264 n = 18,201
Randomization D 150mg BIDD 110mg BID
W (INR 2-3)
R 20mg daily* W (INR 2-3)
A 5mg BID* W (INR 2-3)
InclusionCriteria Nonvalvular AF
with increased stroke risk
Nonvalvular AF with prior
stroke or >2 risk factors
Nonvalvular AF with >1 risk
factor for stroke
Exclusion CrCl < 30 CrCl < 30 CrCl < 25
* Dose reductions for renal impairment

Trials vs Warfarin for A fibRE-LY
DAB vs WARROCKET-AFRIV vs WAR
ARISTOTLE APIX vs WAR
Average age (yrs) 71 73 70
Mean CHADS2 2.1 3.5 2.1
0-1 32% 0% 34%
2 36% 13% 36%
3-6 32% 87% 30%
Prior TIA/stroke 20% 55% 19%
TTR (INR @ goal) 64% 55% 62%
Median follow-up 2 yrs 1.9 yrs 1.8 yrs
Primary endpoint Stroke (ischemic, hemorrhagic) + systemic embolism

Major Findings:RELY
Dabigatran 110mg NI to Warfarin (1.53% vs 1.69%). Dabigatran 150mg superior to Warfarin ONLY if
compared with sub-optimal INR subgroup (1.11 % vs 1.69%).
Major bleeding less with 110mg (2.71 vs 3.11%).
ROCKET-AFRivaroxaban NI to Warfarin (2.1% vs 2.4%)Less ICH or fatal bleeding (0.4% vs 0.8% )
ARISTOTLE:Abixaban Superior to Warfarin (1.27% vs 1.6% )Less Major bleeding (1.4% vs 2.1% )

Key Safety Endpoints (% per year) RE-LY ROCKET AF ARISTOTLE
D110 D150 WAR RIV WAR APIX WAR
1o bleeding endpoint* 2.71 3.11 3.36 14.9 14.5 2.13 3.09
Major bleed 2.71 3.11 3.36 5.55 5.42 2.13 3.09
GI bleeding 1.12 1.51 1.02 3.2 2.2 0.76 0.86
Intracranial hemorrhage
0.23 0.3 0.74 0.5 0.7 0.33 0.8
*: Primary safety endpoint:o RE-LY major hemorrhage o ROCKET-AF major + non-major clinically relevant bleeding o ARISTOTLE ISTH (Int Soc Thromosis & Hemostasis) major bleeding

Figure 3 Forest plot for (A) major bleeding, (B) intracranial bleeding, and (C) gastrointestinal bleeding, new oral anticoagulants (NOA) versus warfarin in patients with AF.
http://dx.doi.org/10.1016/j.amjcard.2012.03.049

Quick Review of Evidence- Based Medicine:
I A: Systemic review of multiple RCTs / multiple RTCs B: High quality single RTC
II: A: Systemic review of cohort studies B: High quality cohort studie(s)
III: Systemic review of Case/Control studies / Case Control studies
IV Case reports
IV Expert opinion
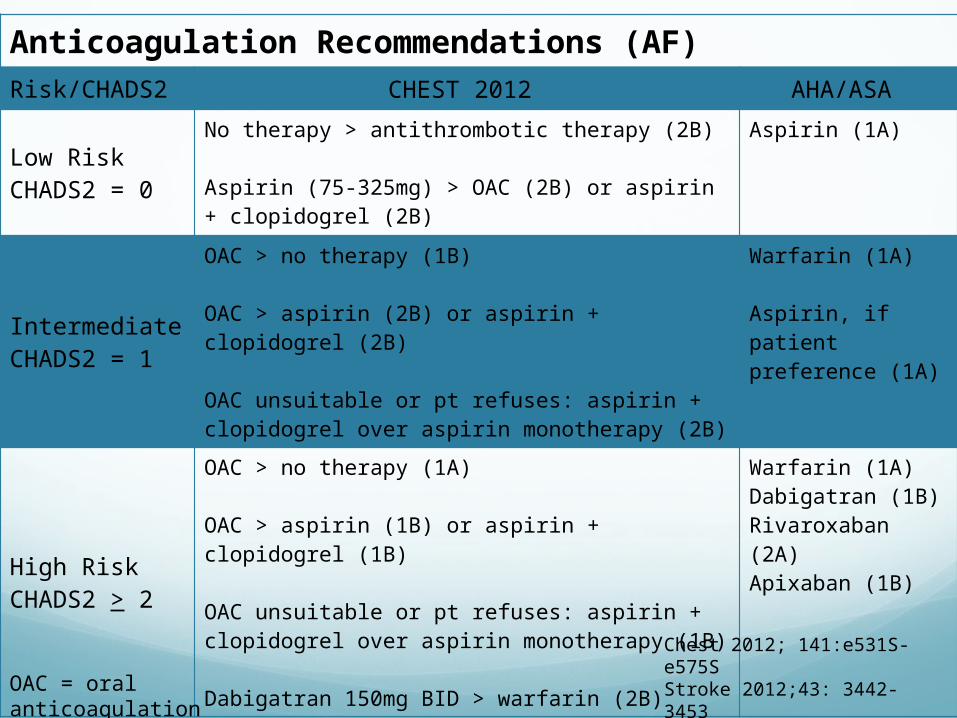
Anticoagulation Recommendations (AF) Risk/CHADS2 CHEST 2012 AHA/ASA
Low RiskCHADS2 = 0
No therapy > antithrombotic therapy (2B)
Aspirin (75-325mg) > OAC (2B) or aspirin + clopidogrel (2B)
Aspirin (1A)
Intermediate CHADS2 = 1
OAC > no therapy (1B)
OAC > aspirin (2B) or aspirin + clopidogrel (2B)
OAC unsuitable or pt refuses: aspirin + clopidogrel over aspirin monotherapy (2B)
Warfarin (1A)
Aspirin, if patient preference (1A)
High RiskCHADS2 > 2
OAC > no therapy (1A)
OAC > aspirin (1B) or aspirin + clopidogrel (1B)
OAC unsuitable or pt refuses: aspirin + clopidogrel over aspirin monotherapy (1B)
Dabigatran 150mg BID > warfarin (2B)
Warfarin (1A)Dabigatran (1B)Rivaroxaban (2A)Apixaban (1B)
OAC = oral anticoagulation
Chest 2012; 141:e531S-e575SStroke 2012;43: 3442-3453

New OAC: Pros:
Easy administration Immediate effect Much less food and drug
interactions One dose fits all The names sound so
much cooler than WARFARIN.
Cons: Expensive Inability to monitor
compliance Short duration: loss of
effect with a single missed dose
No safe/reliable antidotes ? Bleeding. Observational
bias vs real difference. Renal dosing

Take home message:Coumadin still remains the drug of choice for many
patients due to cost, past experience and known side effects.
Many new OAC are in the pipeline, expect a barrage of pharma bombardments, must remain objective as many of the studies have different inclusion/exclusion criteria, definition of end points and side effects.
Each patient may benefit from a different type of OAC based on comorbidities and drug side effect profile.
Watch out for recall bias with the new OAC among your own colleagues.
Patient compliance is a major factor: remember with the new OAC one missed dose means a lot!

The End!


















