New Microsoft Office Word Document (2)
16
UAE Pharmacy license is granted in 2 stages: 1. Passing full Pharmacy examinations and 2. Granting Approval pharmacy license by Pharmacy Committee in UAE Ministry of Health for any licensed pharmaceutical establishment in UAE. 1.Full Pharmacy Examinations The UAE full Pharmacy examinations is consisted of 2 stages (for Arabic speaking candidates) or 3 stages (for non Arabic-speaking candidates): Arabic Exam (For Non Arabic speaking candidates Pharmacists and Technicians ) As Per Articles 2 and 3 of the of Pharmacy Federal Law No. (4) for (1983), fluency in Arabic is required for anyone receiving a license to practice pharmacy in UAE. The Arabic language exam is for non- Arabic speaking candidates, it ensures that licensed pharmacist or technician is fluent enough and having the basic communication skills to deal with Arabic customers in UAE. The first stage of full pharmacy licensure examinations is Arabic Exam which is a paper based written exam of 2 parts ; 1. First part : Translation Arabic- English medical terminology and counseling instructions sentences; 2. Second part : Translation English- Arabic of medical terminology and counseling instructions, sentences. Exam lasts for 1 hour only. Arabic Exam is mandatory for both pharmacists and technicians. Only 3 attempts of exams are allowed to pass. After passing the exam , then candidate may apply to pharmacy Exam. Documents to apply for Arabic Exam : 1. Detailed C.V or bio data in English. 2. Authenticated copy of Bachelor degree certificate for pharmacists (minimum 4 years) including mark sheet or authenticated copy of Diploma degree certificate for technicians (minimum 2 years ) including mark sheet. certificates of degree should be attested from the competent authority of country of graduation and UAE Ministry of foreign affairs. 3. Copy of testimonial and work experience letters, which should state date of starting of employment after graduation, date of leaving and post held.; Work experience should be attested from the competent authority of country of graduation and UAE Ministry of foreign affairs. and applicant should fulfill 2 years of experience duration after date of graduation. 4. Copy of valid registration for the degree or license to practice pharmacy from the respective syndicate of country of graduation or residency. 5. Copy of passport including visa page. 6. Passport size 3 photographs. Questions Second stage of pharmacy licensure examination is The Pharmacy exam which is a paper- computer adaptive examination that consists of 100 multiple-choice test questions (MCQ). Types of Questions will be on different pharmacy areas ; clinical , pharmacology , therapeutics , pharmaceutics , pharmacy –calculations; over the counter medicines , patient counseling , case studies,..etc. The language of exam will be in English only
-
Upload
afshan-rafeeq -
Category
Documents
-
view
26 -
download
0
Transcript of New Microsoft Office Word Document (2)

UAE Pharmacy license is granted in 2 stages:1. Passing full Pharmacy examinations and2. Granting Approval pharmacy license by Pharmacy Committee in UAE Ministry of Health for any licensed pharmaceutical establishment in UAE.
1.Full Pharmacy ExaminationsThe UAE full Pharmacy examinations is consisted of 2 stages (for Arabic speaking candidates) or 3 stages (for non Arabic-speaking candidates):
Arabic Exam (For Non Arabic speaking candidates Pharmacists and Technicians )As Per Articles 2 and 3 of the of Pharmacy Federal Law No. (4) for (1983), fluency in Arabic is required for anyone receiving a license to practice pharmacy in UAE. The Arabic language exam is for non- Arabic speaking candidates, it ensures that licensed pharmacist or technician is fluent enough and having the basic communication skills to deal with Arabic customers in UAE.
The first stage of full pharmacy licensure examinations is Arabic Exam which is a paper based written exam of 2 parts ;1. First part : Translation Arabic- English medical terminology and counseling instructions sentences;2. Second part : Translation English- Arabic of medical terminology and counseling instructions, sentences.
Exam lasts for 1 hour only.Arabic Exam is mandatory for both pharmacists and technicians.Only 3 attempts of exams are allowed to pass.After passing the exam , then candidate may apply to pharmacy Exam.
Documents to apply for Arabic Exam :1. Detailed C.V or bio data in English.2. Authenticated copy of Bachelor degree certificate for pharmacists (minimum 4 years) including mark sheet or authenticated copy of Diploma degree certificate for technicians (minimum 2 years ) including mark sheet.certificates of degree should be attested from the competent authority of country of graduation and UAE Ministry of foreign affairs.3. Copy of testimonial and work experience letters, which should state date of starting of employment after graduation, date of leaving and post held.; Work experience should be attested from the competent authority of country of graduation and UAE Ministry of foreign affairs. and applicant should fulfill 2 years of experience duration after date of graduation.4. Copy of valid registration for the degree or license to practice pharmacy from the respective syndicate of country of graduation or residency.5. Copy of passport including visa page.6. Passport size 3 photographs.
QuestionsSecond stage of pharmacy licensure examination is The Pharmacy exam which is a paper- computer adaptive examination that consists of 100 multiple-choice test questions (MCQ).
Types of Questions will be on different pharmacy areas ; clinical , pharmacology , therapeutics , pharmaceutics , pharmacy –calculations; over the counter medicines , patient counseling , case studies,..etc.The language of exam will be in English onlyExam lasts for 2 hour onlyOnly 3 attempts of exams are allowed to pass.Pharmacy exam is of 2 types for pharmacists and for pharmacists- technicians
Documents to apply for Pharmacy exam for pharmacists :1. Detailed C.V or bio data in English or Arabic2. Copy or list of candidates passed Arabic exam for non-Arabic applicants only.3. Copy of Bachelor degree certificate (minimum 4 years) including mark sheet.certificates of degree should be attested from the competent authority of country of graduation and UAE Ministry of foreign affairs.4. Copy of testimonial and work experience letters, which should state date of starting of employment after graduation, date of leaving and post held.; Work experience should be attested from the competent authority of country of graduation and UAE Ministry of foreign affairs. And applicant should fulfill 2 years of

experience duration after date of graduation.5. Copy of valid registration for the degree or license to practice pharmacy from the respective syndicate of country of graduation or residency.6. Copy of passport including visa page7. 3 passport size photographs8. Receipt for Dh 100 via e- dirham from the cashier's office (3rd floor MOH building).
Documents to apply for Pharmacy exam for Technicians1. Detailed C.V or bio data in English or Arabic2. Copy or list of candidates passed Arabic exam for non-Arabic applicants only.3. Copy of Diploma degree certificate ( minimum 2 years ) including mark sheet.certificates of degree should be attested from the competent authority of country of graduation and UAE Ministry of foreign affairs.4. Copy of testimonial and work experience letters, which should state date of starting of employment after graduation, date of leaving and post held.; Work experience should be attested from the competent authority of country of graduation and UAE Ministry of foreign affairs. And applicant should fulfill 2 years of experience duration after date of graduation.5. Copy of Secondary / High school Certificate6. Copy of Passport including visa page7. 3 passport size photographs8. Receipt for Dh 50 via e- dirham from the cashier's office (3rd floor MOH building).
UAE Pharmacy regulation ExamAfter passing the Pharmacy exam , the candidate may apply to final exam of Pharmacy Law , Code of Conduct and Good Pharmacy Practice for UAE which is the last stage of Pharmacy licensure examination . UAE Pharmacy regulation Exam which is paper- computer adaptive examination consist of 40 multiple-choice test questions (MCQ) On :a. UAE Federal Pharmacy Law No 4 for 1983;b. UAE code of conduct for professional pharmacists and assistants;c. Guidelines and minimum standards for Good Pharmacy Practice (GPP) in UAE Pharmacies and General regulations to practice pharmacy in UAE.Materials of article 3a ,3b and 3c are available on website of Drug Control Department http://www.moh.gov.ae/moh_site/phar_med/moh_p_m.htm
Exam lasts for 1 hour only.Only 3 attempts of exams to pass.Language of exam will be in Arabic for Arabic speaking candidates and English for non- Arabic speaking candidates.This exam is compulsory for both Pharmacists and Pharmacist technicians.
Licensed Establishment requirements:1. List of employees working in the establishment with their professions), a license numbers shall be stated if they wereany pharmacists or assistant- pharmacists working in the establishment).2. Copy of establishment license from chamber of commerce and economic.3. Copy of establishment license from Municipality of city.
N.B: If the establishment is not licensed in MOH, then the manager or agent are requested to proceed for the license procedures along or prior license the pharmacists and technicians.
Pharmacy Guidelineshttp://www.moh.gov.ae/en/Page_773.aspx
Evaluation Procedures of Pharmacists & Their Assistants http://www.moh.gov.ae/en/Page_921.aspx
Platelet activation

Damage to blood vessel walls exposes subendothelium proteins, most notably von Willebrand factor (vWF), present under the endothelium. vWF is a protein secreted by healthy endothelium, forming a layer between the endothelium and underlying basement membrane. When the endothelium is damaged, the normally-isolated, underlying vWF is exposed to white blood cells and recruits Factor VIII, collagen, and other clotting factors. Circulating platelets bind to collagen with surface collagen-specific glycoprotein Ia/IIa receptors. This adhesion is strengthened further by additional circulating proteins vWF, which forms additional links between the platelets glycoprotein Ib/IX/V and the collagen fibrils. These adhesions activate the platelets.
Activated platelets release the contents of stored granules into the blood plasma. The granules include ADP, serotonin, platelet-activating factor (PAF), vWF, platelet factor 4, and thromboxane A2 (TXA2), which, in turn, activate additional platelets. The granules' contents activate a Gq-linked protein receptor cascade, resulting in increased calcium concentration in the platelets' cytosol. The calcium activates protein kinase C, which, in turn, activates phospholipase A2 (PLA2). PLA2 then modifies the integrin membrane glycoprotein IIb/IIIa, increasing its affinity to bind fibrinogen. The activated platelets change shape from spherical to stellate, and the fibrinogen cross-links with glycoprotein IIb/IIIa aid in aggregation of adjacent platelets (completing primary hemostasis).
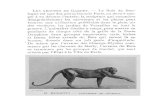
[edit] The coagulation cascade
The coagulation cascade of secondary hemostasis.
The coagulation cascade of secondary hemostasis has two pathways which lead to fibrin formation. These are the contact activation pathway (also known as the intrinsic pathway), and

the tissue factor pathway (also known as the extrinsic pathway). It was previously thought that the coagulation cascade consisted of two pathways of equal importance joined to a common pathway. It is now known that the primary pathway for the initiation of blood coagulation is the tissue factor pathway. The pathways are a series of reactions, in which a zymogen (inactive enzyme precursor) of a serine protease and its glycoprotein co-factor are activated to become active components that then catalyze the next reaction in the cascade, ultimately resulting in cross-linked fibrin. Coagulation factors are generally indicated by Roman numerals, with a lowercase a appended to indicate an active form.
The coagulation factors are generally serine proteases (enzymes). There are some exceptions. For example, FVIII and FV are glycoproteins, and Factor XIII is a transglutaminase. Serine proteases act by cleaving other proteins at specific sites. The coagulation factors circulate as inactive zymogens. The coagulation cascade is classically divided into three pathways. The tissue factor and contact activation pathways both activate the "final common pathway" of factor X, thrombin and fibrin.
[edit] Tissue factor pathway (extrinsic)
The main role of the tissue factor pathway is to generate a "thrombin burst," a process by which thrombin, the most important constituent of the coagulation cascade in terms of its feedback activation roles, is released instantaneously. FVIIa circulates in a higher amount than any other activated coagulation factor.
Following damage to the blood vessel, FVII leaves the circulation and comes into contact with tissue factor (TF) expressed on tissue-factor-bearing cells (stromal fibroblasts and leukocytes), forming an activated complex (TF-FVIIa).
TF-FVIIa activates FIX and FX. FVII is itself activated by thrombin, FXIa, FXII and FXa. The activation of FX (to form FXa) by TF-FVIIa is almost immediately inhibited by tissue factor
pathway inhibitor (TFPI). FXa and its co-factor FVa form the prothrombinase complex, which activates prothrombin to
thrombin. Thrombin then activates other components of the coagulation cascade, including FV and FVIII
(which activates FXI, which, in turn, activates FIX), and activates and releases FVIII from being bound to vWF.
FVIIIa is the co-factor of FIXa, and together they form the "tenase" complex, which activates FX; and so the cycle continues. ("Tenase" is a contraction of "ten" and the suffix "-ase" used for enzymes.)
[edit] Contact activation pathway (intrinsic)
The contact activation pathway begins with formation of the primary complex on collagen by high-molecular-weight kininogen (HMWK), prekallikrein, and FXII (Hageman factor). Prekallikrein is converted to kallikrein and FXII becomes FXIIa. FXIIa converts FXI into FXIa. Factor XIa activates FIX, which with its co-factor FVIIIa form the tenase complex, which activates FX to FXa. The minor role that the contact activation pathway has in initiating clot formation can be illustrated by the fact that patients with severe deficiencies of FXII, HMWK, and prekallikrein do not have a bleeding disorder. Instead, contact activation system seems to be

more involved in inflammation. Patients without FXII (Hageman factor) suffer from constant infections.[citation needed]
[edit] Final common pathway
Thrombin has a large array of functions. Its primary role is the conversion of fibrinogen to fibrin, the building block of a hemostatic plug. In addition, it activates Factors VIII and V and their inhibitor protein C (in the presence of thrombomodulin), and it activates Factor XIII, which forms covalent bonds that crosslink the fibrin polymers that form from activated monomers.
Following activation by the contact factor or tissue factor pathways, the coagulation cascade is maintained in a prothrombotic state by the continued activation of FVIII and FIX to form the tenase complex, until it is down-regulated by the anticoagulant pathways.
[edit] Cofactors
Various substances are required for the proper functioning of the coagulation cascade:
Calcium and phospholipid (a platelet membrane constituent) are required for the tenase and prothrombinase complexes to function. Calcium mediates the binding of the complexes via the terminal gamma-carboxy residues on FXa and FIXa to the phospholipid surfaces expressed by platelets, as well as procoagulant microparticles or microvesicles shed from them. Calcium is also required at other points in the coagulation cascade.
Vitamin K is an essential factor to a hepatic gamma-glutamyl carboxylase that adds a carboxyl group to glutamic acid residues on factors II, VII, IX and X, as well as Protein S, Protein C and Protein Z. In adding the gamma-carboxyl group to glutamate residues on the immature clotting factors Vitamin K is itself oxidized. Another enzyme, Vitamin K epoxide reductase, (VKORC) reduces vitamin K back to its active form. Vitamin K epoxide reductase is pharmacologically important as a target for anticoagulant drugs warfarin and related coumarins such as acenocoumarol, phenprocoumon, and dicumarol. These drugs create a deficiency of reduced vitamin K by blocking VKORC, thereby inhibiting maturation of clotting factors. Other deficiencies of vitamin K (e.g., in malabsorption), or disease (hepatocellular carcinoma) impairs the function of the enzyme and leads to the formation of PIVKAs (proteins formed in vitamin K absence); this causes partial or non-gamma carboxylation, and affects the coagulation factors' ability to bind to expressed phospholipid.
[edit] Regulators
Five mechanisms keep platelet activation and the coagulation cascade in check. Abnormalities can lead to an increased tendency toward thrombosis:
Protein C is a major physiological anticoagulant. It is a vitamin K-dependent serine protease enzyme that is activated by thrombin into activated protein C (APC). Protein C is activated in a sequence that starts with Protein C and thrombin binding to a cell surface protein thrombomodulin. Thrombomodulin binds these proteins in such a way that it activates Protein C. The activated form, along with protein S and a phospholipid as cofactors, degrades FVa and FVIIIa. Quantitative or qualitative deficiency of either may lead to thrombophilia (a tendency to develop thrombosis).

Impaired action of Protein C (activated Protein C resistance), for example by having the "Leiden" variant of Factor V or high levels of FVIII also may lead to a thrombotic tendency.
Antithrombin is a serine protease inhibitor (serpin) that degrades the serine proteases: thrombin, FIXa, FXa, FXIa, and FXIIa. It is constantly active, but its adhesion to these factors is increased by the presence of heparan sulfate (a glycosaminoglycan) or the administration of heparins (different heparinoids increase affinity to FXa, thrombin, or both). Quantitative or qualitative deficiency of antithrombin (inborn or acquired, e.g., in proteinuria) leads to thrombophilia.
Tissue factor pathway inhibitor (TFPI) limits the action of tissue factor (TF). It also inhibits excessive TF-mediated activation of FIX and FX.
Plasmin is generated by proteolytic cleavage of plasminogen, a plasma protein synthesized in the liver. This cleavage is catalyzed by tissue plasminogen activator (t-PA), which is synthesized and secreted by endothelium. Plasmin proteolytically cleaves fibrin into fibrin degradation products that inhibit excessive fibrin formation.
Prostacyclin (PGI2) is released by endothelium and activates platelet Gs protein-linked receptors. This, in turn, activates adenylyl cyclase, which synthesizes cAMP. cAMP inhibits platelet activation by decreasing cytosolic levels of calcium and, by doing so, inhibits the release of granules that would lead to activation of additional platelets and the coagulation cascade.
[edit] Fibrinolysis
Main article: Fibrinolysis
Eventually, blood clots are reorganised and resorbed by a process termed fibrinolysis. The main enzyme responsible for this process (plasmin) is regulated by various activators and inhibitors.

Eicosanoids are a class of compounds that mediate a variety of cellular responses. One group of eicosanoids is called prostaglandins. These compounds are produced by all cells and they cause the inflamatory reponse to injury and the production of pain and fever. They act like hormones and are often called hormones. They differ from true hormones in that they are produced by all cells and act locally.
Prosaglandins are made by cyclizing a 20 carbon polyunsaturated fatty acid called arachidonate. Recall that arachidonate is made from lineolate and we need to absorb linealoate from food because we can't make it ourselves. The most important reaction is the first one in the pathway. It is catalyzed by prostaglandin H synthase (PGHS) a key target for pain relief.
PGHS is a bifunctional enzyme, which means it carries out two separate reactions. The first reaction is a cyclization reaction converting arachidonate to a hydroperoxide called prostaglandin G2. This activity is often called a cyclooxygenase (COX) activity. The second reaction is catalyzed at a different site, the hydroperoxidase site, and the final product is prostaglandin H2.

Although having low triglycerides or LDL cholesterol can have a positive effect on your heart health, having low levels of HDL cholesterol could actually count against you. Your HDL, or “good," cholesterol removes excess cholesterol in the blood and can help to protect you against heart disease. Having low levels of HDL may place you at risk of getting coronary heart disease -- especially if other lipids in your blood are high, such as LDL cholesterol and triglycerides.
There are some things, however, that could cause your HDL levels to be too low, such as:
Uncontrolled diabetes (high blood glucose levels) Smoking Being overweight High triglyceride levels Lack of physical activity Genes Certain medications (anabolic steroids, progestins) Poor diet, especially if high in carbohydrates
When your HDL cholesterol levels fall below 40 mg/dL, you may need to take some measures to help raise them. Fortunately, many of these measures require just a few changes to your lifestyle. Some things you could do to boost your HDL cholesterol include:
Adding exercise to your daily routine Losing weight, if you are overweight or obese Smoking cessation Getting your blood sugar levels under control, if you have diabetes Modifying your diet to a healthier one, especially if you are consuming foods that are high in
carbohydrates and saturated fat
If these measures do not help raise your HDL levels, your healthcare provider may decide to put you on medications that can help you, including niacin and fibrates. There are currently no medications on the market that can solely raise your HDL cholesterol levels. These medications, however, can also improve other aspects of your lipid panel, including lowering your LDL and triglyceride levels.
Normal: Less than 150 mg/dL Borderline High: 150 - 199 mg/dL

High: 200 - 499 mg/dL Very High: 500 mg/dL or above
What Abnormal Results Mean
High triglyceride levels may be due to:
Cirrhosis Diet low in protein and high in carbohydrates Familial hyperlipoproteinemia (rare) Hypothyroidism Nephrotic syndrome Pancreatitis Poorly controlled diabetes
Low triglyceride levels may be due to:
Low fat diet Hyperthyroidism Malabsorption syndrome Malnutrition
Additional conditions under which the test may be performed:
Chylomicronemia syndrome Hyperlipidemia; acquired Familial combined hyperlipidemia Familial dysbetalipoproteinemia Familial hypertriglyceridemia Familial lipoprotein lipase deficiency Noninsulin-dependent diabetes (NIDD)
What causes high triglycerides?

High triglycerides are usually caused by other conditions, such as:
Obesity . Poorly controlled diabetes. An underactive thyroid (hypothyroidism). Kidney disease. Regularly eating more calories than you burn. Drinking a lot of alcohol.
Certain medicines may also raise triglycerides. These medicines include:
Tamoxifen . Steroids. Beta-blockers . Diuretics . Estrogen . Birth control pills .
In a few cases, high triglycerides also can run in families
Pattern of the SGOT/SGPT test pattern or the degree of SGOT/SGPT enzyme
elevation in the blood is a good way of diagnosing different liver diseases. Different
types of liver diseases give rise to different level of SGOT/SGPT enzyme test value.
But these enzyme changes are not diagnostic but help in the process of diagnosis.
In most acute hepatocellular disorders, the SGPT is higher than or equal to the SGOT. An SGOT:SGPT
ratio>2:1 is suggestive while a ratio >3:1 is highly suggestive of alcoholic liver disease. The AST in
alcoholic liver disease is rarely >300 U/L and the SGPT is often normal. A low level of SGPT in the serum
is due to an alcohol-induced deficiency of pyridoxal phosphate. The aminotransferases are usually not
greatly elevated in obstructive jaundice. One notable exception occurs during the acute phase of biliary
obstruction caused by the passage of a gallstone into the common bile duct. In this setting, the
aminotransferases can briefly be in the 1000 to 2000 U/L range. However, aminotransferase levels
decrease quickly, and the liver function tests rapidly evolve into one typical of cholestasis.
Liver disease SGOT/SGPT test patternGilbert’s syndrome normalLiver diseases with hemolysis Normal (usually)Viral hepatitis >500 IU
SGPT>SGOTDrug hepatitis >500 IU

SGPT>SGOTAcute hepatocellular
Necrosis (heart failure)
>500 IU
SGPT>SGOTChronic hepatocellular
disorders
Elevated, but usually
>300 IUAlcoholic hepatitis AST:ALT >2Cirrhosis AST:ALT >2Obstructive
jaundice
Normal to moderate
elevation
Rarely >500 IUInfiltrative diseases
(tumor,
granulomata)
Normal to slight
elevation
Intra- and extra hepatic
cholestasis
Normal to moderate
elevation
Rarely >500 IU
POSTED BY SAMEERA DASANAYAKE AT 5:21 AM

Values below 25 seconds or over 39 s (depending on local normal ranges) are generally abnormal. Shortening of the PTT has little clinical relevance. Normal PTT times require the presence of the following coagulation factors: I, II, V, VIII, IX, X, XI, & XII. Notably, deficiencies in factors VII or XIII will not be detected with the PTT test. Prolonged APTT may indicate:
use of heparin (or contamination of the sample) antiphospholipid antibody (especially lupus anticoagulant, which paradoxically increases propensity
to thrombosis) coagulation factor deficiency (e.g. hemophilia)
To distinguish the above causes, mixing tests are performed, in which the patient's plasma is mixed (initially at a 50:50 dilution) with normal plasma. If the abnormality does not disappear, the sample is said to contain an "inhibitor" (either heparin, antiphospholipid antibodies or coagulation factor specific inhibitors), while if it does correct a factor deficiency is more likely. Deficiencies of factors VIII, IX, XI and XII and rarely von Willebrand factor (if causing a low factor VIII level) may lead to a prolonged aPTT correcting on mixing studies.
ConditionProthrombin
timePartial thromboplastin
timeBleeding time Platelet count
Vitamin K deficiency or warfarin prolonged prolonged unaffected unaffected
Disseminated intravascular coagulation
prolonged prolonged prolonged decreased
Von Willebrand disease unaffected prolonged prolonged unaffected
Haemophilia unaffected prolonged unaffected unaffected
Aspirin unaffected unaffected prolonged unaffected
Thrombocytopenia unaffected unaffected prolonged decreased
Early Liver failure prolonged unaffected unaffected unaffected
End-stage Liver failure prolonged prolonged prolonged decreased
Uremia unaffected unaffected prolonged unaffected
Congenital afibrinogenemia prolonged prolonged prolonged unaffected
Factor V deficiency prolonged prolonged unaffected unaffected
Factor X deficiency as seen in amyloid purpura
prolonged prolonged unaffected unaffected

Glanzmann's thrombasthenia unaffected unaffected prolonged unaffected
Bernard-Soulier syndrome unaffected unaffected prolonged decreased




![[MS-OFFDI]: Microsoft Office File Format Documentation … · 2017-09-19 · Microsoft Word 97 Microsoft Word 2000 Microsoft Word 2002 Microsoft Office Word 2003 Microsoft Office](https://static.fdocuments.in/doc/165x107/5edde022ad6a402d66691993/ms-offdi-microsoft-office-file-format-documentation-2017-09-19-microsoft-word.jpg)