New Insights in Genetic Cholestasis: From Molecular...
13
Review Article New Insights in Genetic Cholestasis: From Molecular Mechanisms to Clinical Implications Eva Sticova , 1,2 Milan Jirsa, 3 and Joanna PawBowska 4 1 Clinical and Transplant Pathology Centre, Institute for Clinical and Experimental Medicine, Prague 4, 140 21, Czech Republic 2 Department of Pathology, ird Faculty of Medicine, Charles University, Prague 10, 100 00, Czech Republic 3 Laboratory of Experimental Hepatology, Experimental Medicine Centre, Institute for Clinical and Experimental Medicine, Prague 4, 140 21, Czech Republic 4 Department of Gastroenterology, Hepatology, Nutritional Disorders and Pediatrics, e Children’s Memorial Health Institute (CMHI), Warsaw 04-730, Poland Correspondence should be addressed to Eva Sticova; [email protected] Received 11 April 2018; Revised 10 July 2018; Accepted 17 July 2018; Published 26 July 2018 Academic Editor: Emmanuel Tsochatzis Copyright © 2018 Eva Sticova et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Cholestasis is characterised by impaired bile secretion and accumulation of bile salts in the organism. Hereditary cholestasis is a heterogeneous group of rare autosomal recessive liver disorders, which are characterised by intrahepatic cholestasis, pruritus, and jaundice and caused by defects in genes related to the secretion and transport of bile salts and lipids. Phenotypic manifestation is highly variable, ranging from progressive familial intrahepatic cholestasis (PFIC)—with onset in early infancy and progression to end-stage liver disease—to a milder intermittent mostly nonprogressive form known as benign recurrent intrahepatic cholestasis (BRIC). Cases have been reported of initially benign episodic cholestasis that subsequently transitions to a persistent progressive form of the disease. erefore, BRIC and PFIC seem to represent two extremes of a continuous spectrum of phenotypes that comprise one disease. us far, five representatives of PFIC (named PFIC1-5) caused by pathogenic mutations present in both alleles of ATP8B1, ABCB11, ABCB4, TJP2, and NR1H4 have been described. In addition to familial intrahepatic cholestasis, partial defects in ATP8B1, ABCB11, and ABCB4 predispose patients to drug-induced cholestasis and intrahepatic cholestasis in pregnancy. is review summarises the current knowledge of the clinical manifestations, genetics, and molecular mechanisms of these diseases and briefly outlines the therapeutic options, both conservative and invasive, with an outlook for future personalised therapeutic strategies. 1. Introduction Cholestasis is characterised by an impairment of bile secre- tion and transport, leading to the subsequent accumulation of toxic bile components in the organism. Bile salts (BS), the main organic solutes in bile, are physiological detergents that facilitate the absorption and transport of lipids, vitamins, and nutrients. BS also play an important role in cell signalling as part of key metabolic processes. 2. Bile Salt Synthesis BS are synthesised from cholesterol in the liver. e size of the total BS pool in human adults is 3-4 g [1, 2]. ere are two main pathways of BS synthesis. e classic (neutral) biosynthesis pathway, localised exclusively in the liver and accounting for at least 75% of the total BS pool, starts with modification of the sterol ring, followed by side chain cleav- age reactions to synthesise cholic and chenodeoxycholic acid, constituting the primary BS in humans. e first and rate- limiting enzyme in this pathway is microsomal cholesterol 7 alpha-hydroxylase (CYP7A1). In the alternative (acidic) pathway of BS synthesis, side chain oxidation precedes mod- ification of the sterol ring. e first enzyme in the alternative pathway is mitochondrial sterol-27 hydroxylase (encoded by CYP27A1). Primary BS are conjugated at the side chain either with taurine or glycine, while water soluble conjugates are excreted into bile where they are rapidly incorporated in mixed micelles containing phospholipids (predominantly phosphatidylcholine) and cholesterol. ereaſter, they are Hindawi Canadian Journal of Gastroenterology and Hepatology Volume 2018, Article ID 2313675, 12 pages https://doi.org/10.1155/2018/2313675
Transcript of New Insights in Genetic Cholestasis: From Molecular...

Review ArticleNew Insights in Genetic Cholestasis From MolecularMechanisms to Clinical Implications
Eva Sticova 12 Milan Jirsa3 and Joanna PawBowska4
1Clinical and Transplant Pathology Centre Institute for Clinical and Experimental Medicine Prague 4 140 21 Czech Republic2Department of Pathology Third Faculty of Medicine Charles University Prague 10 100 00 Czech Republic3Laboratory of Experimental Hepatology Experimental Medicine Centre Institute for Clinical and Experimental MedicinePrague 4 140 21 Czech Republic4Department of Gastroenterology Hepatology Nutritional Disorders and PediatricsThe Childrenrsquos Memorial Health Institute (CMHI) Warsaw 04-730 Poland
Correspondence should be addressed to Eva Sticova evasticovaikemcz
Received 11 April 2018 Revised 10 July 2018 Accepted 17 July 2018 Published 26 July 2018
Academic Editor Emmanuel Tsochatzis
Copyright copy 2018 Eva Sticova et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Cholestasis is characterised by impaired bile secretion and accumulation of bile salts in the organism Hereditary cholestasis is aheterogeneous group of rare autosomal recessive liver disorders which are characterised by intrahepatic cholestasis pruritus andjaundice and caused by defects in genes related to the secretion and transport of bile salts and lipids Phenotypic manifestation ishighly variable ranging from progressive familial intrahepatic cholestasis (PFIC)mdashwith onset in early infancy and progression toend-stage liver diseasemdashto a milder intermittent mostly nonprogressive form known as benign recurrent intrahepatic cholestasis(BRIC) Cases have been reported of initially benign episodic cholestasis that subsequently transitions to a persistent progressiveform of the disease Therefore BRIC and PFIC seem to represent two extremes of a continuous spectrum of phenotypes thatcomprise one disease Thus far five representatives of PFIC (named PFIC1-5) caused by pathogenic mutations present in bothalleles of ATP8B1 ABCB11 ABCB4 TJP2 and NR1H4 have been described In addition to familial intrahepatic cholestasis partialdefects in ATP8B1 ABCB11 and ABCB4 predispose patients to drug-induced cholestasis and intrahepatic cholestasis in pregnancyThis review summarises the current knowledge of the clinical manifestations genetics andmolecular mechanisms of these diseasesand briefly outlines the therapeutic options both conservative and invasive with an outlook for future personalised therapeuticstrategies
1 Introduction
Cholestasis is characterised by an impairment of bile secre-tion and transport leading to the subsequent accumulationof toxic bile components in the organism Bile salts (BS) themain organic solutes in bile are physiological detergents thatfacilitate the absorption and transport of lipids vitamins andnutrients BS also play an important role in cell signalling aspart of key metabolic processes
2 Bile Salt Synthesis
BS are synthesised from cholesterol in the liver The sizeof the total BS pool in human adults is 3-4 g [1 2] Thereare two main pathways of BS synthesis The classic (neutral)
biosynthesis pathway localised exclusively in the liver andaccounting for at least 75 of the total BS pool starts withmodification of the sterol ring followed by side chain cleav-age reactions to synthesise cholic and chenodeoxycholic acidconstituting the primary BS in humans The first and rate-limiting enzyme in this pathway is microsomal cholesterol7 alpha-hydroxylase (CYP7A1) In the alternative (acidic)pathway of BS synthesis side chain oxidation precedes mod-ification of the sterol ring The first enzyme in the alternativepathway is mitochondrial sterol-27 hydroxylase (encodedby CYP27A1) Primary BS are conjugated at the side chaineither with taurine or glycine while water soluble conjugatesare excreted into bile where they are rapidly incorporatedin mixed micelles containing phospholipids (predominantlyphosphatidylcholine) and cholesterol Thereafter they are
HindawiCanadian Journal of Gastroenterology and HepatologyVolume 2018 Article ID 2313675 12 pageshttpsdoiorg10115520182313675
2 Canadian Journal of Gastroenterology and Hepatology
Enterocyte
Cho
lang
iocyte
Hepatocyte
NTCP BSEP
FIC1
Aminophospholipids
MRP3
OST
BS
BSBSBS
BS
MDR3
Lecithin
MRP34
OST
OATP1B13
FXR-RXR
SHP
cholCYP7A1
FXR-RXR
SHP
MRP3
OST
ASBT
FXRBS
BS
ASBTIBABP
FGF19
FGF19
FGFR4
+
++
+
+
+
+
-
-
-
- -
BS
BS
SHP
Na+
Na+
Na+
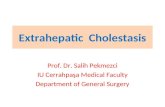
Figure 1 Bile salt and lipid transporters and their regulatory pathways
transported into the intestinal tract where they are decon-jugated oxidised and dehydroxylated to form 7-deoxycholicand lithocholic acid as part of a reaction catalysed by bacterial7 alpha-dehydroxylases Finally most intestinal BS (95)are reabsorbed in the distal part of the small intestine andtransported to the liver via the portal blood and to alesser extent via the hepatic artery in a process known asenterohepatic circulation The BS pool is recycled 4-12 timesa day BS lost in the faeces (02-06 gday) are replenished byde novo synthesis in the liver [1ndash3]
3 Bile Salt and Lipid Transporters
Bile acids form dissociated sodium or potassium salts inbody fluids with neutral pH Therefore BS transporters aredesigned as anion transporters Enterohepatic circulation ofBS is driven by several specific transport systems expressedpredominantly in hepatocytes and biliary and intestinalepithelia (Figure 1)
In hepatocytes Na+-dependent taurocholate cotrans-porting peptide (NTCP also known as the sodiumbile acidcotransporter) encoded by SLC10A1 (solute carrier family 10member 1) represents themajor conjugatedBS uptake systemfrom the blood contributing 80 of the transport capacity
NTCP is localised in the basolateral (sinusoidal) membraneand its driving force the Na+ concentration gradient ismaintained by Na+K+-ATPase [4 5] NTCP deficiency hasrecently been shown to cause severe familial predominantlyconjugated hypercholanemia with no cholestatic jaundicepruritus and liver disease [6]
Unconjugated BS are transported by the multispecificATP- and Na+-independent basolateral uptake transportersorganic anion-transporting polypeptide 1B1 (OATP1B1 alsotermed OATP-C OATP2 SLC21A6 or LST-1 encoded bySLCO1B1) and 1B3 (OATP1B3 synonyms OATP8 SLC21A8or LST3 encoded by SLCO1B3) [4 7 8] They play asecondary role in liver uptake of conjugated BS since thepresence of both OATP1Bs only partly compensates forNTCP deficiency [6]
The basolateral domain of hepatocytes also possessesseveral ATP-dependent efflux pumps which constitute themultidrug resistance protein (MRP) subfamily (ABCC)ABCC proteins transport organic anions including BS [9 10]
MRP3 (encoded by ABCC3) is a basolateral transporterof BS glucuronide and anionic conjugates including glu-tathione [11ndash13] In the liver MRP3 is expressed predomi-nantly in the centrilobular hepatocytes and its expression islow under physiological conditions MRP3 expression rate is
Canadian Journal of Gastroenterology and Hepatology 3
upregulated during cholestasis and independently of anycholestaticmanifestation in individuals withDubin-Johnsonsyndrome or after repeated administration of ethinylestradiol[11 14 15] As well as in hepatocytes Northern blotting ofvarious human tissues indicates the presence of MRP3 inthe bile duct epithelium gallbladder intestine pancreas andkidney [16]
MRP4 (gene ABCC4) is an inducible basolateral trans-porter that cotransports taurine and glycine conjugates ofcholic acid with glutathione It is also a high-affinity trans-porter of sulphated BS dehydroepiandrosterone sulphateeicosanoids and uric acid as well as signalling moleculessuch as cAMP and cGMP [17] Although MRP4 expressionin the liver is low it can be induced by BS in cholestasis [1819] Strong upregulation of human MRP4 has been demon-strated in patients with BS export pump (BSEP) deficiency[20]
The heterodimeric organic solute transporter OST120572-OST120573 initially identified as a basolateral BS efflux systemin enterocytes (see below) is also localised in the sinusoidalmembrane of hepatocytes [21] Hepatic OST120572-OST120573 expres-sion increases in patients with primary biliary cirrhosis andin bile duct-ligated rodents [22] Thus during cholestasisMRP3 MRP4 and OST120572-OST120573 may provide effective pro-tection against hepatocellular BS overload
The transfer of BS from the liver to the bile canaliculus isdetermined by several transport proteins in the canalicular(apical) membrane of hepatocytes mainly ATP-dependentBSEP and MRPs
BSEP encoded by ABCB11 is responsible for the ATP-dependent transport of predominantly monovalent conju-gated BS across the hepatocyte canalicular membrane It isexclusively expressed in the liver and localised predominantlyin the canalicular microvillar (but not the intermicrovillar)membrane and to a lesser extent in subcanalicular (subapical)vesicles [23] Expression of BSEP is sensitive to the flux ofBS through hepatocytes The BSEP promoter contains aninverted repeat DNA element (IR-1) a binding site for thefarnesoid X receptor (FXR) which plays an important rolein maintaining BS homeostasis (see below)
Multidrug resistance protein 3 (MDR3 gene ABCB4) isunderstood to act as a floppase which translocates phospho-lipids from the inner to the outer leaflet of the lipid bilayer ofthe canalicular membrane [24] Mutations in ABCB4 causecholestasis which is characterised by the decreased biliarylecithin output impaired formation of mixed micelles andthe production ofmore hydrophilic bilewith potent detergentproperties resulting in membrane damage [25 26]
Familial intrahepatic cholestasis type 1 transporter (FIC1gene ATP8B1) a member of the type 4 subfamily of P-typeATPases (P4 ATPase) is a flippase that mediates the translo-cation of aminophospholipids from the outer (exoplasmic)to the inner (cytoplasmic) leaflet of the plasma membrane[27] In most eukaryotic cells phosphatidylcholine andsphingolipids are concentrated in the exoplasmic leafletwhereas the aminophospholipids (phosphatidylserine andphosphatidylethanolamine) are largely confined to the cyto-plasmic leaflet FIC1 thus helps in maintaining asymmetry
and fluidity characteristics of plasma membranes the essen-tial prerequisites for proper function of transmembraneembedded pumps [27]
Cholangiocytes are important modifiers of bile com-position Conjugated BS need to be actively transportedinto cholangiocytes via apical sodium-dependent bile acidtransporter (ASBT gene SLC10A2) and are exported into theperibiliary capillary plexus via the heterodimeric transporterOST120572-OST120573 and via MRP3 [28 29] Under physiologicalconditions BS transporters in cholangiocytes can play amajor role in the regulation of intracellular concentrationsof BS as signalling molecules In obstructive cholestasischolangiocellular BS receptors may facilitate the removal ofBS from stagnant bile [3 28 29]
An important step in maintaining BS homeostasis is thereabsorption of BS in the intestinal lumen predominantlyin the ileum Intestinal epithelial cells reabsorb the majorityof secreted BS through ASBT localised in the brush bordermembrane of enterocytes Human ASBT also called ileal bileacid transporter or ileal sodium-dependent bile acid trans-porter consists of 348 amino acids It transports conjugatedand unconjugated BS with a higher affinity for chenodeoxy-cholic and deoxycholic acid than for taurocholate [30] Afteruptake into the enterocyte the transcellular movement of BSis mediated by cytosolic ileal bile acid-binding protein alsoknown as fatty acid-binding protein 6 or gastrotropin (IBABPFABP6 gene FABP6) that is cytoplasmically attached toASBT [30]
The heterodimeric organic solute transporter OST120572-OST120573 (OST120572 gene SLC51A OST120573 gene SLC51B) is expressedin the basolateral membrane of enterocytes and effluxes BSto the portal blood In humans OST120572-OST120573 is expressed athigh levels in a variety of tissues and is the primary trans-porter of BS into the systemic circulation [21 22 30]
Furthermore MRP3 may also participate in the basolat-eral transport of BS in human enterocytes although its overallcontribution is small [10]
4 Regulation of Bile SaltSynthesis and Trafficking
The BS biosynthesis and enterohepatic circulation are tightlyregulated at many levels but particularly by transcriptionaland posttranscriptionalmechanisms [2 3] A key regulator ofBS synthesis and enterohepatic flow is the nuclear farnesoidX receptor (FXR) a major BS-responsive ligand-activatedtranscription factor with a high affinity for several majorendogenous BS [2 31 32] Expression levels of the FXRgene (also known as the NR1H4 genemdashnuclear receptorsubfamily 1 group H member 4) are highest in the intestinepredominantly in the ileal epithelium liver and kidneys [3132]
FXR acts as an agonist-dependent transcriptional acti-vator of its direct target genes The preferred DNA-bindingsequence for FXR within its target promoters is a variantof inverted repeat-1 motif (IR-1) to which FXR binds as aheterodimer with the retinoid X receptor (RXR) FXR canalso downregulate the transcription of specific target genesindirectly via another nuclear receptor the small heterodimer
4 Canadian Journal of Gastroenterology and Hepatology
partner (SHP the NR0B2 gene) SHP is an atypical orphannuclear receptor without a DNA-binding domain It acts asa repressor of nuclear receptors as well as of transcriptionfactors belonging to other protein families [2 31 33]
FXR plays a key role in controlling the enterohepaticcirculation of BS largely by directly regulating the expressionof several hepatobiliary transporters (Figure 1) In the liverthe heterodimer FXR-RXR induces the expression of BSEPby binding to an IR-1 element at the promoter [34 35]Likewise FXR can directly transactivate the ABCC2 ABCB4and SLCO1B3 genes [36 37]
The FXR-RXR complex directly induces the expressionof OST120572-OST120573 (in ileal enterocytes and in the basolateralmembrane of hepatocytes) as well as intestinal expression ofthe intestinal bile acid-binding protein (IBABP) [22 37]
In addition to directly activating the main BS effluxsystems under cholestatic conditions FXR concurrentlydownregulates the main BS uptake systems primarily NTCPin the basolateral membrane of hepatocytes and ASBT inthe ileal epithelium OATP1B1 is also suppressed by anFXR-dependent pathway during cholestasis FXR-mediatedrepression of target genes is indirect and mainly effected viaSHP [2 33 37]
As well as regulating transport systems involved in theenterohepatic flow of BS FXR represses the transcription ofgenes that encode regulatory enzymes in both classical andalternative BS biosynthetic pathways predominantlyCYP7A1and CYP27A1 [2 33]
There are two important FXR-dependent mechanismsfor BS-induced inhibition of CYP7A1 gene transcription theFXRSHP pathway in the liver and the FXRFGF19FGFR4pathway in the intestine [2 37]
In the liver the heterodimer FXRRXR after bindingretinoic acid andBS induces the expression of SHPThe inter-action of SHP with liver receptor homologue-1 (LRH-1 alsoNR5A2 gene NR5A2) and hepatocyte nuclear factor-4120572(HNF4120572 also NR2A1 gene HNF4A) inhibits CYP7A1 tran-scription [2 32 33] In the CYP27A1 gene the BS responseelement contains a DNA-binding site for HNF4120572 only notfor LRH-1 [2 31]
In the intestine FXR induces an intestinal hormonefibroblast growth factor 19 (FGF19 gene FGF19) whichactivates hepatic FGF receptor 4 (FGFR4 gene FGFR4) anddownregulates BS synthesis by inhibitingCYP71A expressionThe FXRFGF19FGFR4 pathway seems to be the physiolog-ical mechanism for feedback regulation of BS biosynthesisFurthermore the FGF19 autocrine pathway exists in thehuman liver [2 31 37 38]
Along with FXR-related regulation of BS biosynthesisthere are several FXR-independent mechanisms of CYP7A1inhibition mediated by pregnane X receptor (PXR) vitaminD receptor (VDR) the cytokines tumour necrosis factor120572 (TNF120572) and interleukin 1120573 (IL-1120573) transforming growthfactor 1205731 (TGF1205731) epidermal growth factor receptor (EGFR)and others These factors activate signalling pathways whichplay roles in protecting against BS toxicity during cholestaticliver injury [2 31 32 37]
Finally FXR also directly transactivates genes encod-ing enzymes that metabolise BS such as human uri-dine 5rsquo-diphosphate-glucuronosyltransferase 2B4 (UGT2B4encoded by UGT2B4) Interestingly FXR binds the UGT2B4promoter as amonomerwithout previous heterodimerisationwith RXR [32]
Several nuclear receptors such as FXR RXR LXR andSHP are also expressed in cholangiocytes but their role in bileduct biology remains to be elucidated [29]
5 Familial Intrahepatic Cholestasis
Up- and downregulation of transport systems involved inbile formation can explain the impaired liver uptake andexcretion of biliary constituents which result in cholestasisand jaundice in some hereditary andmany common acquiredliver disorders Hereditary diseases characterised by hepato-canalicular cholestasis which is caused by defects in hepato-biliary transporters their regulator FXR and in tightness ofthe liver epithelium include progressive familial intrahepaticcholestasis (PFIC) types 1 to 5 benign recurrent intrahepaticcholestasis (BRIC) 1 and 2 familial cholelithiasis caused by alack of biliary secretion of phospholipids (Low Phospholipid-AssociatedCholelithiasis orGallbladderDisease-1) intrahep-atic cholestasis of pregnancy (ICP) and several other raredisorders Hereditary predisposition also plays an impor-tant role in drug-induced intrahepatic cholestasis includingcholestasis induced by hormonal contraceptives [39 40]
51 Progressive Familial Intrahepatic Cholestasis PFIC firstdescribed in 1969 [41] is a genetically heterogeneous group ofautosomal recessive disorders caused by mutations in genesthat encode hepatocanalicular transporters of BS and phos-pholipids their regulator FXR andTJP2which is essential fortightness of cell junctions between the epithelial cells liningthe bile ducts The exact incidence of PFIC is not knownbut it is estimated to be in the region of 150000 to 1100000births Both genders are equally affected [42] Clinically PFICusuallymanifests in the first year of life and is characterised byjaundice severe pruritus hepatosplenomegaly steatorrhoeaand retardation of growth and mental development Furthersymptoms caused by a deficit of fat-soluble vitamins includecoagulopathy osteopaenia and neuromuscular disordersWithout adequate treatment the disease progresses to liverfibrosis and cirrhosis and usually ends in death due to liverfailure in the first or more rarely in the second decade of life[40 42]
The PFIC group consists of five representatives (PFIC 1-5) which are classified into two main categories according tolevels of serum rsaquo-glutamyl transferase (GGT) activity GGTis considered a cholestatic enzyme and when elevated isassociated with damage to the apical membranes of bile ductsand the disruption of intercellular connections due to highconcentrations of BS in bile However in some cholestaticdiseases synthesis or canalicular secretion of BS is virtuallyabsent and there are no conditions that predispose eitherto the release of membrane GGT from damaged cholan-giocytes or to leakage of bile into the extracellular spaceand subsequently the blood This explains why in hereditary
Canadian Journal of Gastroenterology and Hepatology 5
(a) (b)
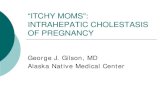
Figure 2 Histopathology of ABCB11 disease (a) Giant-cell hepatitis (arrows) with hepatocanalicular cholestasis and (b) complete absenceof ABCB11BSEP protein are typical findings in PFIC2 patients Inset immunohistochemical positivity of BSEP in the apical (canalicular)domain of hepatocytes in a healthy control (a) Hematoxylin and eosin original magnification x200 (b inset) Immunohistochemical stainingwith ABCB11 Rabbit Polyclonal Antibody (NBP1-89319 Novus Biologicals USA) original magnification x200 (b) x400 (inset)
cholestasis GGT activity is increased only in disorders ofphospholipid secretion (PFIC3)
511 Progressive Familial Intrahepatic Cholestasis Type 1(PFIC1) PFIC1 (ATP8B1 disease OMIM 211600) formerlyBylerrsquos disease [41] is the consequence of a severe defect in thegene encoding ATPase ATP8B1FIC1 (familial intrahepaticcholestasis 1) localised in the long arm of the 18th chro-mosome (18q21) [43 44] ATP8B1 deficiency which causesmembrane phospholipid asymmetry of the canalicular mem-brane reduces the capacity of the liver to secrete bile [45 46]In addition to the previously described common symptomsof PFIC clinical manifestation of PFIC1 also includes awide range of extrahepatic symptoms Extrahepatic mani-festations of ATP8B1 disease include elevated sweat chlorideconcentrations delayed pubescence and growth and waterydiarrhoea as well as impaired hearing andor pancreatitis[47] These symptoms often persist while diarrhoea eventends to worsen after liver transplantation (LTX) Liverallografts in PFIC1 patients may display diffuse steatosis witha variable necroinflammatory component with subsequentfibrosis [48] Both diarrhoea and steatosissteatohepatitismay improve after biliary diversion [49]
Laboratory findings with regard to PFIC1 have reportedcholestasis with low serum levels of GGT increased serumconcentrations of primary BS and normal levels of choles-terol Aminotransferases are initially within the referencerange but during disease progression they gradually increaseby up to tenfold [41] Histopathological changes predomi-nantly involve canalicular cholestasis accentuated around thecentral veins The interlobular ducts can be hypoplastic dueto subnormal bile flow Giant-cell changes of hepatocytes aregenerally not observed in biopsies Liver fibrosis progressioncorresponds with the respective stage of the disease and canterminate in cirrhosis A typical ultrastructural finding isthe presence of Byler-type coarsely granular bile in the bilecanaliculi [50] Molecular diagnosis is based on the detectionof pathogenic mutations in both alleles of the ATP8B1 gene
The milder intermittent nonprogressive form of ATP8B1deficiency is called BRIC1 (see below)
512 Progressive Familial Intrahepatic Cholestasis Type 2(PFIC2) PFIC2 (ABCB11 disease OMIM 601847) is causedby mutations in ABCB11 which is located on the longarm of the second chromosome (2q24) and encodes thecanalicular transport proteinABCB11BSEP [51] Clinical andlaboratory findings with regard to PFIC2 are similar to PFIC1but extrahepatic symptoms are not present Additionally inPFIC2 the formation of gallstones and the early elevation ofserum aminotransferase activity can occurThe developmentof hepatobiliarymalignancies both hepatocellular carcinomaand cholangiocarcinoma can be a serious complication ofPFIC2 which is not observed in PFIC1 [52 53] Screening forliver tumours is recommended from the first year of life inPFIC2 patients
Except for PFIC2 mutations in ABCB11 may result in amilder nonprogressive formof PFIC2 known asBRIC2 aswellas other forms of cholestasis such as ICP andor drug-inducedcholestasis (see below)
Histologically the typical findings in the liver biopsies ofPFIC2 patients are giant-cell (syncycial) hepatitis with hepa-tocanalicular cholestasis while extramedullary haemopoiesisis frequently discernible within lobules Interlobular bileducts can be hypoplastic and ductular proliferation at theperipheries of portal triads is commonly observed TheABCB11BSEP protein is usually undetectable immunohis-tochemically (Figure 2) Ultrastructurally canalicular bilecan be either amorphous or filamentous but is not coarselygranular [51]
Untreated PFIC2 usually leads to progressive liver fibrosisand cirrhosis the development of which ismore rapid than inPFIC1 One curative method for patients with PFIC2 is LTXUnlike in PFIC1 steatosis and steatohepatitis are not presentin liver allografts in the case of PFIC2 However in somepatients a recurrence of the PFIC2 phenotype accompaniedby elevated serum levels of BS and bilirubin with almost
6 Canadian Journal of Gastroenterology and Hepatology
normal GGT activity has been observed after LTX [54 55] Ithas been shown that canalicular immunostaining of the BSEPMDR3 and MRP2 proteins is preserved in the liver graftbiopsies and no discernible changes in BSEP immunoreactiv-ity distribution between the apical membrane and the cyto-plasm have been reported nonetheless de novo polyclonalinhibitory antibodies directed against the first extracellularloop of BSEP have been observed in the posttransplant serumof patients a condition known as Autoimmune BSEPDisease(AIBD) [56 57] The exact mechanism by which BS trans-port is inhibited by anti-BSEP antibodies is still unknownIt is supposed that the cross-linking of BSEP moleculeswhich in turn disrupts the structure and function ofcanalicular membranes andor the direct mechanical occlu-sion of the BSEP pore might explain the inhibitory effectsof the antibodies [56 57] It is estimated that up to 8 oftransplanted PFIC2 patients develop anti-BSEP antibodies[56] This may be explained by the insufficient autotoleranceagainst BSEP exhibited in some patients with severe ABCB11mutations resulting in the complete absence of the BSEPproteinThe causal relationship between recurrent cholestasisin the liver grafts of PFIC2 patients and the occurrence of denovo antibodies directed against BSEP is further supportedby observations that plasmapheresis and the administrationof anti-CD20 antibodies (rituximab) may alleviate symptomsof cholestasis [54ndash57]
Interestingly posttransplant development of inhibitoryautoantibodies directed against FIC1 andMDR3 transporterswith corresponding phenotypes has not yet been docu-mented in patients with PFIC1 and PFIC3 respectively[44]
513 Progressive Familial Intrahepatic Cholestasis Type 3(PFIC3) PFIC3 (ABCB4 disease OMIM 602347) is causedby mutations in both alleles of the ABCB4MDR3 gene thatencode phospholipid transporter MDR3 expressed in thecanalicular (apical) membrane of hepatocytes [26] As wellas PFIC3 there is evidence that either biallelic or monoal-lelic ABCB4 defects may cause or predispose patients to awide spectrum of human liver diseases such as LowPhospholipid-Associated Cholelithiasis Syndrome (LPACOMIM 600803) Intrahepatic Cholestasis of Pregnancy(ICP OMIM 147480) drug-induced liver injury transientneonatal cholestasis small duct sclerosing cholangitis andadult biliary fibrosis or cirrhosis [58ndash61] Moreover hepa-tocellular carcinoma and intrahepatic cholangiocarcinomahave been documented in patients withABCB4MDR3muta-tions [61]
Clinical and laboratory findings associated with PFIC3correspond to the other two forms of PFIC but are charac-terised by the absence of extrahepatic symptoms (except forcholelithiasis) Unlike PFIC1 and PFIC2 elevated serumGGTactivity and normal cholesterol levels are typically observedas exhibited by the MDR3 deficit [26 62]
Histopathological findings in connection with ABCB4disease are variable Syncytial (giant-cell) changes cholesta-sis portal inflammatory infiltrate and periportal ductularproliferation accompanied by various stages of fibrosis have
been observed in liver tissue Lipid crystals within bile ductsand fibroobliterative bile duct lesions can be seen Immuno-histochemistry has indicated the absence of the canalicularMDR3 protein predominantly in early onset forms howeverits use is limited compared to PFIC2 Ultrastructurally bile isdense and amorphous in PFIC3 [26 61]
Prolonged cholestasis in PFIC3 is associated with signifi-cant accumulation of copper in liver tissue andwith increasedurine copper excretion ie findings that overlap with thediagnostic criteria for Wilsonrsquos disease [63 64]
514 Progressive Familial Intrahepatic Cholestasis Type 4(PFIC4) The fourth form of PFIC (PFIC4 TJP2 deficiencyOMIM 615878) first described in 2014 [65] is clinicallysimilar to PFIC2 and caused by homozygous or compoundheterozygous mutations in the TJP2 gene located in the9q12 chromosome Tight junction protein 2 (TJP2 also zonaoccludens-2) is a cytoplasmic component of cell-cell junc-tional complexes expressed in most epithelia and creates alink between transmembrane tight junction proteins and theactin cytoskeleton Complete TJP2 deficiency is associatedwith a significant reduction in an integral tight junction pro-tein claudin-1 predominantly in the canalicular membranesof liver cells which subsequently leads to the disruption ofintercellular connections and the leakage of bile through theparacellular space into the liver parenchyma [65 66]
Patients with TJP2 deficiency display severe progressivecholestatic liver disease in early childhood which puts themat increased risk of developing hepatocellular carcinoma [67]Serum GGT activity is normal or at most slightly increasedwhile expression of the canalicular proteins BSEP andMDR3is maintained In addition to liver impairment extrahepaticfeatures have been identified in PFIC4 patients includ-ing neurological and respiratory disorders [66] A singlehomozygous missense mutation in TJP2 has been previouslydescribed as causing benign familial hypercholanemia a raredisorder of oligogenic inheritance which usually manifestsin elevated serum BS concentrations pruritus and fat mal-absorption but which does not lead to the development ofliver disease [68]
515 Progressive Familial Intrahepatic Cholestasis Type 5(PFIC5) PFIC5 (OMIM 617049) first described in 2016[69] is a cholestatic disorder caused by mutations in NR1H4a gene located at 12q231 which encodes FXR the keyregulator of BS metabolism (see above) Homozygous loss ofFXR function is associated with severe neonatal cholestasisand early onset vitamin K-independent coagulopathy whichrapidly progresses to end-stage liver disease The nonrespon-siveness of coagulopathy to vitamin K treatment is likelya direct consequence of the loss of FXR function repre-senting an important distinguishing diagnostic feature ofNR1H4-related cholestasis In addition to low (or normal)GGT activity serum levels of alpha-fetoprotein are typicallyelevated [69]
Liver biopsies have shown diffuse giant-cell transforma-tion of hepatocytes with hepatocellular cholestasis and ductu-lar proliferation Progressive fibrosis and even micronodularcirrhosis are evident at later stages BSEP is undetectable in
Canadian Journal of Gastroenterology and Hepatology 7
the apical domains of hepatocytes which is consistent withlow activity of GGT MDR3 expression on the other hand ismaintained [69]
Since FXR affects several metabolic pathways someNR1H4 variations may be associated with susceptibility tovarious human diseases NR1H4 single-nucleotide polymor-phisms seem to be correlated with differences in glucosehomeostasis gallstone formation ICP inflammatory boweldisease and several other disorders [70 71]
52 Benign Recurrent Intrahepatic Cholestasis (BRIC) BRICis a group of genetically heterogeneous autosomal recessivediseases characterised by intermittent episodes of cholesta-sis They are caused by mutations in the ATP8B1 and ABCB11genes (the same as in PFIC1 and PFIC2) and probably inat least one other as yet unidentified gene [72] Thereare two genetically characterised forms of BRIC BRIC1(Summerskill-Walshe-Tygstrup syndrome OMIM 243300)and BRIC2 (OMIM 605479) caused by partial deficiency inATP8B1 [39 73] and ABCB11 [74] respectively The diseasetypically manifests before the second decade of life but theage of the first manifestation can vary greatly The samevariability has been documented in the duration of cholestaticepisodes (several days to several months) and their intensityInfection or pregnancy may act as a triggering factor Theclinical manifestations include jaundice pruritus fatigueanorexia and steatorrhoea Increase of bilirubin and BS levelsin serum has been observed during cholestatic attacks butGGT activity and serum cholesterol levels tend to be normalAminotransferase activity is usually normal or only slightlyelevated while biochemical parameters fall within normalranges Liver biopsies performed during cholestatic attackshave demonstrated hepatocanalicular cholestasis withoutfibrosis During the asymptomatic period the histologicalpicture is completely normal Since canalicular expression ofBSEP protein in hepatocytes is mostly maintained immuno-histology is of limited significance in these cases Diagnosisof BRIC1 and BRIC2 is based on demonstrating evidence ofmutations in both alleles of the corresponding genesATP8B1and ABCB11
While mutations causing PFIC are often located in theconserved regions of the genes that encode conserved func-tional domains of the corresponding proteins mutations inBRIC only partially impact protein function and expressionHowever several cases of initially benign episodic cholestasisthat have subsequently transitioned to a persistent progres-sive form of the disease have been reported [75] Thus BRICand PFIC seem to represent two extremes of a continuousspectrum of phenotypes of the one disease
The administration of statins corticosteroids cholestyra-mine or ursodeoxycholic acid (UDCA) is usually not veryeffective in BRIC patients Improvement of pruritus andshortening of symptomatic phase has been described inBRIC patients treated with the antibiotic rifampicin a potenthuman activator of PXR [76 77] However severe hepa-totoxicity after long-term administration of rifampicin hasbeen reported in patients with cholestatic disorders [77 78]Nasobiliary drainage seems to have a prompt effect during
cholestatic episodes but the mechanism of action remainsunclear [79]
53 Intrahepatic Cholestasis of Pregnancy (ICP) ICP (OMIM147480) also known as obstetric cholestasis is characterisedby cholestasis and prurituswith onset in pregnancy usually inthe third trimester It is associated with abnormal liverfunction in the absence of other liver diseases and resolvescompletely after delivery [80 81]The incidence of ICP varieswith geographical location and ethnicity Seasonal variationsindicate higher incidence in winter months as reported insome countries and it more commonly occurs in associationwith multiple pregnancies and following in vitro fertilisationIn Europe ICP affects about 1 of all pregnancies [81] Atypical symptom is intense pruritus commonly localised inthe palms and the soles which progresses during pregnancyElevated levels of serum BS and increased liver aminotrans-ferase activity are typical laboratory findings in such casesIncreased serum bilirubin levels have been observed in asmall proportion of cases while jaundice only rarely occursin affected women [81]
ICP usually resolves soon after delivery Although thedisease is considered relatively benign for themother there isan increased rate of adverse foetal outcomes including foetaldistress foetal asphyxia stillbirth or even intrauterine deathall known complications of ICP [81 82] ICPmay also be asso-ciated with an abnormalmetabolic profile in afflictedwomenespecially higher prevalence of dyslipidaemia impaired glu-cose tolerance and maternal comorbidities eg gestationaldiabetes and preeclampsia [82 83] Administration of UDCAimproves clinical symptoms predominantly pruritus andmay even reduce the risk of premature birth [84ndash86]
Mutations in ABCB4 ABCB11 and ATP8B1 have beenidentified in some patients suffering from ICP [87ndash90]Additionally variations in NR1H4 may be implicated in ICPpossibly via downregulation of BSEP expression [71]
6 Conclusions and Perspectives
Identification of the genes involved in hereditary cholestasishas advanced our understanding of the molecular mecha-nisms behind bile formation and transport
Recently mutations in TJP2 and NR1H4 have been foundin patients with apparent BSEP deficiency normal serumGGT activity and no mutations in ABCB11 However thereare rare cases of genetic cholestasis causes of which haveyet to be identified Therefore it seems likely that other yetunidentified genes involved in secretion andor transport ofcholephiles may be responsible for FIC-like phenotypes
Current therapeutic regimens in FIC patients compriseboth nonsurgical and surgical approaches Nonsurgical ther-apy includes drugs predominantly UDCA and rifampicinand nasobiliary drainage the latter being predominantly usedin BRIC patients with intractable pruritus during long-lastingcholestatic episodes [76 77 79] However the mechanismresponsible for the instant and complete relief from pruritusis still unclear
In addition to cholestyramine phenobarbital S-adeno-sylmethionine opiate antagonists UDCA rifampicin and
8 Canadian Journal of Gastroenterology and Hepatology
serotonin antagonists and its reuptake inhibitors seem to bebeneficial in managing refractory pruritus in patients withPFIC [77 91 92] Furthermore clinical and biochemicalimprovements have been observed in BRIC patients withintractable pruritus after using the molecular adsorbentrecirculating system (MARS) and the Prometheus system anextracorporeal liver support therapy based on fractionatedplasma separation and adsorption [93]
Surgical therapies include partial biliary diversion iemechanical interruption of BS enterohepatic circulation inorder to prevent reabsorption of pruritogens (unidentifiedthus far) and their precursors which is primarily usefulin noncirrhotic children with low-GGT PFIC permanentcholestasis andor intense refractory pruritus and orthotopicLTX which is still the ultimate treatment modality for manyPFIC patients [91] However as well as the risks associatedwith these invasive procedures other serious postoperative-related complications have been reported particularly inPFIC1 patients with extradigestive symptoms which canpersist or even worsen most likely due to extrahepaticexpression of FIC1 [47]Moreover the development of steato-sis and steatohepatitis leading to progressive liver allograftfibrosis in PFIC1 patients [48] and recurrence of the PFIC2phenotype in ABCB11 deficiency may represent other seriouscomplications after LTX and for some patients may evennecessitate retransplantation [54ndash57]
Importantly because of the shortage of cadaveric donorsparental living-related LTX is often considered in PFICpatients As heterozygous conditions can cause mild-to-moderate disease expression under certain circumstancesthe use of blood relatives as donors is seen as controversial Insuch cases it is likely that the heterozygous status of the donorallograft could pose a risk of complications during the lateposttransplant period such as lithiasis or cholestasis whichcan be precipitated by infections or by drugs administeredto the patient However the results of a recent study indicatethat the PFIC heterozygote status of the organ donor does notincrease the risk of liver dysfunction [94]
The limited effectiveness of current conservative proce-dures along with the complications of invasive methods par-ticularly LTX stress the need for the development and intro-duction of new treatment options Total biliary diversionpharmacological diversion of BS and hepatocyte transplanta-tion as well as gene- and mutation-targeted pharmacothera-pies represent promising future therapeutic approaches Thelatter two methods provide the basis for personalised treat-ment strategies in FIC patients Pharmacological chaperones(eg 4-phenylbutyrate) agonists of nuclear receptors (egstatins fibrates 6-ethyl chenodeoxycholic acid) endoplasmicreticulum-associated degradation inhibitors (MG132) andseveral other mutation-specific drugs can be used to increasethe expression of functional proteins and mitigate or eveneliminate deficient phenotypes [95ndash97]
Nevertheless despite the indisputable progress in thetherapy of FIC patients the increased risks of hepatobiliarymalignancies particularly in relation to ABCB11 deficiencystill remain serious life-threatening complications Furtherstudies are required in order to elucidate the complex patho-genesis of cholestasis unlock the mechanism of cholestatic
pruritus and improve the clinical management of bothhereditary and acquired cholestatic liver diseases
Abbreviations
ABC ATP-binding cassette subfamilyABCB4 ATP-binding cassette subfamily B
member 4ABCB11 ATP-binding cassette subfamily B
member 11AIBD Autoimmune BSEP DiseaseASBT Apical sodium-dependent bile acid
transporterATP8B1 ATPase aminophospholipid transporter
class I type 8B member 1BRIC Benign Recurrent Intrahepatic CholestasisBS Bile saltsBSEP Bile salt export pumpCYP7A1 Cholesterol 7 alpha-hydroxylaseCYP27A1 Sterol-27 hydroxylaseFGF19 Fibroblast growth factor 19FGFR4 Fibroblast growth factor receptor 4FIC Familial intrahepatic cholestasisFXR Farnesoid X-activated receptorGGT rsaquo-Glutamyl transferaseHNF4120572 Hepatocyte nuclear factor 4120572IBABP Intestinal bile acid-binding proteinICP Intrahepatic cholestasis of pregnancyIR-1 Inverted repeat DNA element with 1
nucleotide spacingLPAC Low Phospholipid-Associated
Cholelithiasis SyndromeLTX Liver allograft transplantationLXR Liver X receptorMDR3 Multidrug resistance protein 3MRP Multidrug resistance-associated proteinNR1H4 Nuclear receptor subfamily 1 group H
member 4NTCP Na+-taurocholate cotransporting
polypeptidesolute carrier family 10member 1
OATP Organic anion-transporting polypeptideOMIM Electronic database Online Mendelian
Inheritance in ManTMOST Organic solute transporterPFIC Progressive Familial Intrahepatic
CholestasisPXR Pregnane X receptorRXR Retinoid X receptorSHP Small heterodimer partnerSLC22A Solute carrier family 22 (organic cation
transporter) member 1SLCO Solute carrier organic anion transporter
familyTJP2 Tight junction protein 2 zona occludens-2UDCA Ursodeoxycholic acidUGT2B4 Uridine
51015840-diphosphate-glucuronosyltransferase2B4
Canadian Journal of Gastroenterology and Hepatology 9
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
Milan Jirsa was supported by Ministry of Health CzechRepublicmdashConceptual Development of Research Organiza-tion (ldquoInstitute for Clinical and Experimental MedicinendashIKEM IN 00023001rdquo)
References
[1] N B Javitt ldquoBile acid synthesis from cholesterol regulatory andauxiliary pathwaysrdquoThe FASEB Journal vol 8 no 15 pp 1308ndash1311 1994
[2] J Y L Chiang ldquoBile acids regulation of synthesisrdquo Journal ofLipid Research vol 50 no 10 pp 1955ndash1966 2009
[3] J L Boyer ldquoBile formation and secretionrdquo ComprehensivePhysiology vol 3 no 3 pp 1035ndash1078 2013
[4] B Hagenbuch and P J Meier ldquoSinusoidal (basolateral) bile saltuptake systems of hepatocytesrdquo Seminars in Liver Disease vol16 no 2 pp 129ndash136 1996
[5] B Hagenbuch B Stieger M Foguet H Lubbert and P JMeier ldquoFunctional expression cloning and characterization ofthe hepatocyte Na+bile acid cotransport systemrdquo Proceedingsof the National Acadamy of Sciences of the United States ofAmerica vol 88 no 23 pp 10629ndash10633 1991
[6] F M Vaz C C Paulusma H Huidekoper et al ldquoSodiumtaurocholate cotransporting polypeptide (SLC10A1) deficiencyConjugated hypercholanemia without a clear clinical pheno-typerdquo Hepatology vol 61 no 1 pp 260ndash267 2015
[7] B Hagenbuch and P J Meier ldquoOrganic anion transportingpolypeptides of the OATPSLC21 family Phylogenetic classi-fication as OATPSLCO super-family new nomenclature andmolecularfunctional propertiesrdquo Pflugers Archiv - EuropeanJournal of Physiology vol 447 no 5 pp 653ndash665 2004
[8] B Hagenbuch and B Stieger ldquoThe SLCO (former SLC21)superfamily of transportersrdquoMolecular Aspects of Medicine vol34 no 2-3 pp 396ndash412 2013
[9] M Muller and P L M Jansen ldquoThe secretory function ofthe liver New aspects of hepatobiliary transportrdquo Journal ofHepatology vol 28 no 2 pp 344ndash354 1998
[10] G J E J Hooiveld J E Van Montfoort D K F Meijerand M Muller ldquoFunction and regulation of ATP-bindingcassette transport proteins involved in hepatobiliary transportrdquoEuropean Journal of Pharmaceutical Sciences vol 12 no 4 pp525ndash543 2001
[11] J Konig D Rost Y Cui and D Keppler ldquoCharacterizationof the human multidrug resistance protein isoform MRP3localized to the basolateral hepatocyte membranerdquoHepatologyvol 29 no 4 pp 1156ndash1163 1999
[12] H Zeng G Liu P A Rea and G D Kruh ldquoTransport ofamphipathic anions by human multidrug resistance protein 3rdquoCancer Research vol 60 pp 4779ndash4784 2000
[13] Y-M A Lee Y Cui J Konig et al ldquoIdentification and func-tional characterization of the natural variantMRP3-Arg1297Hisof human multidrug resistance protein 3 (MRP3ABCC3)rdquoPharmacogenetics vol 14 no 4 pp 213ndash223 2004
[14] M Donner ldquoUp-regulation of basolateral multidrug resistanceprotein 3 (Mrp3) in cholestatic rat liverrdquoHepatology vol 34 no2 pp 351ndash359 2001
[15] M L Ruiz J P Rigalli A Arias et al ldquoInduction of hepaticmultidrug resistance-associated protein 3 by ethynylestradiol isindependent of cholestasis and mediated by estrogen receptorrdquoDrug Metabolism and Disposition vol 41 no 2 pp 275ndash2802013
[16] N J Cherrington D P Hartley N Li D R Johnson and C DKlaassen ldquoOrgan distribution of multidrug resistance proteins1 2 and 3 (Mrp1 2 and 3) mRNA and hepatic induction ofMrp3 by constitutive androstane receptor activators in ratsrdquoTheJournal of Pharmacology and Experimental Therapeutics vol300 no 1 pp 97ndash104 2002
[17] C A Ritter G Jedlitschky H Meyer Zu Schwabedissen MGrube K Kock and H K Kroemer ldquoCellular export ofdrugs and signaling molecules by the ATP-binding cassettetransporters MRP4 (ABCC4) and MRP5 (ABCC5)rdquo DrugMetabolism Reviews vol 37 no 1 pp 253ndash278 2005
[18] F G M Russel J B Koenderink and R Masereeuw ldquoMul-tidrug resistance protein 4 (MRP4ABCC4) a versatile effluxtransporter for drugs and signalling moleculesrdquo Trends inPharmacological Sciences vol 29 no 4 pp 200ndash207 2008
[19] D Keppler ldquoProgress in the molecular characterization ofhepatobiliary transportersrdquoDigestive Diseases vol 35 no 3 pp197ndash202 2017
[20] V Keitel M Burdelski U Warskulat et al ldquoExpression andlocalization of hepatobiliary transport proteins in progressivefamilial intrahepatic cholestasisrdquo Hepatology vol 41 no 5 pp1160ndash1172 2005
[21] N Ballatori F FangWV Christian N Li andC LHammondldquoOst120572-Ost120573 is required for bile acid and conjugated steroiddisposition in the intestine kidney and liverrdquoAmerican Journalof Physiology-Gastrointestinal and Liver Physiology vol 295 no1 pp G179ndashG186 2008
[22] J L Boyer M Trauner A Mennone et al ldquoUpregulationof a basolateral FXR-dependent bile acid efflux transporterOSTalpha-OSTbeta in cholestasis in humans and rodentsrdquoAmerican Journal of Physiology-Gastrointestinal and Liver Phys-iology vol 290 no 6 pp G1124ndashG1130 2006
[23] T Gerloff B Stieger B Hagenbuch et al ldquoThe sister of P-glycoprotein represents the canalicular bile salt export pump ofmammalian liverrdquoThe Journal of Biological Chemistry vol 273no 16 pp 10046ndash10050 1998
[24] A M van der Bliek F Baas T Ten Houte de Lange P MKooiman T van der Velde-Koerts and P Borst ldquoThe humanmdr3 gene encodes a novel P-glycoprotein homologue and givesrise to alternatively splicedmRNAs in liverrdquo EMBO Journal vol6 no 11 pp 3325ndash3331 1987
[25] A J Smith J L Timmermans-Hereijgers and B RoelofsenldquoThe human MDR3 P-glycoprotein promotes translocation ofphosphatidylcholine through the plasma membrane of fibrob-lasts from transgenic micerdquo FEBS Letters vol 354 no 3 pp263ndash266 1994
[26] J M L de Vree E Jacquemin E Sturm et al ldquoMutations in theMDR3 gene cause progressive familial intrahepatic cholestasisrdquoProceedings of the National Acadamy of Sciences of the UnitedStates of America vol 95 no 1 pp 282ndash287 1998
[27] A Groen M R Romero C Kunne et al ldquoComplementaryfunctions of the flippase ATP8B1 and the floppase ABCB4 inmaintaining canalicular membrane integrityrdquoGastroenterologyvol 141 no 5 pp 1927ndash1937 2011
10 Canadian Journal of Gastroenterology and Hepatology
[28] P A Dawson T Lan and A Rao ldquoThematic review series Bileacids Bile acid transportersrdquo Journal of Lipid Research vol 50no 12 pp 2340ndash2357 2009
[29] E Halilbasic T Claudel andM Trauner ldquoBile acid transportersand regulatory nuclear receptors in the liver and beyondrdquoJournal of Hepatology vol 58 no 1 pp 155ndash168 2013
[30] B L Shneider ldquoIntestinal bile acid transport Biology physiol-ogy and pathophysiologyrdquo Journal of Pediatric Gastroenterologyand Nutrition vol 32 no 4 pp 407ndash417 2001
[31] T Claudel G Zollner M Wagner and M Trauner ldquoRoleof nuclear receptors for bile acid metabolism bile secretioncholestasis and gallstone diseaserdquoBiochimica et Biophysica Acta(BBA) - Molecular Basis of Disease vol 1812 no 8 pp 867ndash8782011
[32] J J Eloranta and G A Kullak-Ublick ldquoThe role of FXR indisorders of bile acid homeostasisrdquo Physiology Journal vol 23no 5 pp 286ndash295 2008
[33] B Goodwin S A Jones R R Price et al ldquoA regulatory cascadeof the nuclear receptors FXR SHP-1 and LRH-1 represses bileacid biosynthesisrdquo Molecular Cell vol 6 no 3 pp 517ndash5262000
[34] M Muller P L M Jansen K N Faber et al ldquoFarnesoid Xreceptor and bile salts are involved in transcriptional regulationof the gene encoding the human bile salt export pumprdquoHepatology vol 35 no 3 pp 589ndash596 2002
[35] M Ananthanarayanan N BalasubramanianMMakishima DJ Mangelsdorf and F J Suchy ldquoHuman bile salt export pumppromoter is transactivated by the farnesoid X receptorbile acidreceptorrdquo The Journal of Biological Chemistry vol 276 no 31pp 28857ndash28865 2001
[36] L Huang A Zhao J L Lew et al ldquoFarnesoid X receptoractivates transcription of the phospholipid pump MDR3rdquo TheJournal of Biological Chemistry vol 278 no 51 pp 51085ndash510902003
[37] M Wagner G Zollner and M Trauner ldquoNuclear receptorregulation of the adaptive response of bile acid transporters incholestasisrdquo Seminars in Liver Disease vol 30 no 2 pp 160ndash1772010
[38] Y Zhang H R Kast-Woelbern and P A Edwards ldquoNaturalstructural variants of the nuclear receptor farnesoid X recep-tor affect transcriptional activationrdquo The Journal of BiologicalChemistry vol 278 no 1 pp 104ndash110 2003
[39] SW C VanMil R H J Houwen and LW J Klomp ldquoGeneticsof familial intrahepatic cholestasis syndromesrdquo Journal of Med-ical Genetics vol 42 no 6 pp 449ndash463 2005
[40] V E H Carlton L Pawlikowska and L N Bull ldquoMolecularbasis of intrahepatic cholestasisrdquoAnnals ofMedicine vol 36 no8 pp 606ndash617 2004
[41] R J Clayton F L Iber B H Ruebner and V A MckusickldquoByler Disease Fatal Familial Intrahepatic Cholestasis in anAmish Kindredrdquo American Journal of Diseases of Children vol117 no 1 pp 112ndash124 1969
[42] E Jacquemin ldquoProgressive familial intrahepatic cholestasisrdquoClinics andResearch inHepatology andGastroenterology vol 36supplement 1 pp S26ndashS35 2012
[43] L N Bull M J T Van Eijk L Pawlikowska et al ldquoA geneencoding a P-type ATPase mutated in two forms of hereditarycholestasisrdquo Nature Genetics vol 18 no 3 pp 219ndash224 1998
[44] L W J Klomp J C Vargas S W C Van Mil et al ldquoCharac-terization of mutations in ATP8B1 associated with hereditarycholestasisrdquo Hepatology vol 40 no 1 pp 27ndash38 2004
[45] P Ujhazy D Ortiz S Misra et al ldquoFamilial intrahepaticcholestasis 1 Studies of localization and functionrdquo Hepatologyvol 34 no 4 I pp 768ndash775 2001
[46] C C Paulusma A Groen C Kunne et al ldquoAtp8b1 deficiencyin mice reduces resistance of the canalicular membrane tohydrophobic bile salts and impairs bile salt transportrdquo Hepatol-ogy vol 44 no 1 pp 195ndash204 2006
[47] SW C VanMil LW J Klomp L N Bull and RH J HouwenldquoFIC1 disease A spectrumof intrahepatic cholestatic disordersrdquoSeminars in Liver Disease vol 21 no 4 pp 535ndash544 2001
[48] A Miyahawa-Hayashino H Egawa T Yorifuji et al ldquoAllograftsteatohepatitis in progressive familial intrahepatic cholestasistype 1 after living donor liver transplantationrdquo Liver Transplan-tation vol 15 no 6 pp 610ndash618 2009
[49] E Nicastro X Stephenne F Smets et al ldquoRecovery of graftsteatosis and protein-losing enteropathy after biliary diversionin a PFIC 1 liver transplanted childrdquo Pediatric Transplantationvol 16 no 5 pp E177ndashE182 2012
[50] K Evason K E Bove M J Finegold et al ldquoMorphologic find-ings in progressive familial intrahepatic cholestasis 2 (PFIC2)Correlation with genetic and immunohistochemical studiesrdquoThe American Journal of Surgical Pathology vol 35 no 5 pp687ndash696 2011
[51] S S Strautnieks L N Bull A S Knisely et al ldquoA gene encodinga liver-specific ABC transporter is mutated in progressivefamilial intrahepatic cholestasisrdquo Nature Genetics vol 20 no3 pp 233ndash238 1998
[52] A S Knisely S S Strautnieks Y Meier et al ldquoHepatocellularcarcinoma in ten children under five years of age with bile saltexport pumpdeficiencyrdquoHepatology vol 44 no 2 pp 478ndash4862006
[53] A O Scheimann S S Strautnieks A S Knisely J A Byrne RJ Thompson andM J Finegold ldquoMutations in Bile Salt ExportPump (ABCB11) in Two Children with Progressive FamilialIntrahepatic Cholestasis and Cholangiocarcinomardquo Journal ofPediatrics vol 150 no 5 pp 556ndash559 2007
[54] V Keitel M Burdelski Z Vojnisek L Schmitt D HaussingerandRKubitz ldquoDe novo bile salt transporter antibodies as a pos-sible cause of recurrent graft failure after liver transplantationA novel mechanism of cholestasisrdquo Hepatology vol 50 no 2pp 510ndash517 2009
[55] P Jara L Hierro P Martınez-Fernandez et al ldquoRecurrence ofbile salt export pump deficiency after liver transplantationrdquoTheNew England Journal of Medicine vol 361 no 14 pp 1359ndash13672009
[56] R Kubitz C Droge S Kluge et al ldquoAutoimmune BSEPDiseaseDisease Recurrence After Liver Transplantation for ProgressiveFamilial Intrahepatic Cholestasisrdquo Clinical Reviews in Allergy ampImmunology vol 48 no 2-3 pp 273ndash284 2015
[57] J Stindt S Kluge C Droge et al ldquoBile salt export pump-reactive antibodies form a polyclonal multi-inhibitoryresponse in antibody-induced bile salt export pump deficiencyrdquoHepatology vol 63 no 2 pp 524ndash537 2016
[58] E Jacquemin J M DeVree D Cresteil et al ldquoThe widespectrum of multidrug resistance 3 deficiency from neonatalcholestasis to cirrhosis of adulthoodrdquoGastroenterology vol 120no 6 pp 1448ndash1458 2001
[59] O Rosmorduc and R Poupon ldquoLow phospholipid associatedcholelithiasis association with mutation in the MDR3ABCB4generdquo Orphanet Journal of Rare Diseases vol 2 article 29 2007
Canadian Journal of Gastroenterology and Hepatology 11
[60] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoThe spectrum of liver diseases related to ABCB4 gene muta-tions Pathophysiology and clinical aspectsrdquo Seminars in LiverDisease vol 30 no 2 pp 134ndash146 2010
[61] DWendumV BarbuO Rosmorduc L Arrive J-F Flejou andR Poupon ldquoAspects of liver pathology in adult patients withMDR3ABCB4 gene mutationsrdquo Virchows Archiv vol 460 no3 pp 291ndash298 2012
[62] R P J Oude Elferink andC C Paulusma ldquoFunction and patho-physiological importance of ABCB4 (MDR3 P-glycoprotein)rdquoPflugers Archiv - European Journal of Physiology vol 453 no 5pp 601ndash610 2007
[63] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoProgressive familial intrahepatic cholestasisrdquo Clinical Pedi-atrics vol 51 pp 689ndash691 2012
[64] S Boga D Jain andM L Schilsky ldquoPresentation of progressivefamilial intrahepatic cholestasis type 3 mimicking wilson dis-ease molecular genetic diagnosis and response to treatmentrdquoPediatric Gastroenterology Hepatology amp Nutrition vol 18 no3 p 202 2015
[65] M Sambrotta S Strautnieks E Papouli et al ldquoMutationsin TJP2 cause progressive cholestatic liver diseaserdquo NatureGenetics vol 46 no 4 pp 326ndash328 2014
[66] M Sambrotta and R J Thompson ldquoMutations in TJP2 encod-ing zona occludens 2 and liver diseaserdquo Tissue Barriers vol 3no 3 Article ID e1026537 2015
[67] S Zhou P M Hertel M J Finegold et al ldquoHepatocellularcarcinoma associated with tight-junction protein 2 deficiencyrdquoHepatology vol 62 no 6 pp 1914ndash1916 2015
[68] V EH Carlton B ZHarris E G Puffenberger et al ldquoComplexinheritance of familial hypercholanemia with associated muta-tions in TJP2 and BAATrdquo Nature Genetics vol 34 no 1 pp 91ndash96 2003
[69] N Gomez-Ospina C J Potter R Xiao et al ldquoMutations inthe nuclear bile acid receptor FXR cause progressive familialintrahepatic cholestasisrdquoNature Communications vol 7 ArticleID 10713 2016
[70] I Koutsounas S Theocharis I Delladetsima E Patsouris andC Giaginis ldquoFarnesoid x receptor in human metabolism anddisease the interplay between gene polymorphisms clinicalphenotypes and disease susceptibilityrdquo Expert Opinion on DrugMetabolism amp Toxicology vol 11 no 4 pp 523ndash532 2015
[71] S W C van Mil A Milona P H Dixon et al ldquoFunctionalVariants of the Central Bile Acid Sensor FXR Identified inIntrahepatic Cholestasis of Pregnancyrdquo Gastroenterology vol133 no 2 pp 507ndash516 2007
[72] C Droge M Bonus U Baumann et al ldquoSequencing of FIC1BSEP and MDR3 in a large cohort of patients with cholestasisrevealed a high number of different genetic variantsrdquo Journal ofHepatology vol 67 no 6 pp 1253ndash1264 2017
[73] L N Bull V E H Carlton N L Stricker et al ldquoGeneticand morphological findings in progressive familial intrahepaticcholestasis (Byler disease [PFIC-1] and Byler syndrome) Evi-dence for heterogeneityrdquo Hepatology vol 26 no 1 pp 155ndash1641997
[74] S W C Van Mil W L Van Der Woerd G Van Der Brugge etal ldquoBenign recurrent intrahepatic cholestasis type 2 is causedby mutations in ABCB11rdquo Gastroenterology vol 127 no 2 pp379ndash384 2004
[75] N A M Van Ooteghem L W J Klomp G P Van Berge-Henegouwen andRH JHouwen ldquoBenign recurrent intrahep-atic cholestasis progressing to progressive familial intrahepatic
cholestasis Low GGT cholestasis is a clinical continuumrdquoJournal of Hepatology vol 36 no 3 pp 439ndash443 2002
[76] F Balsells R Wyllie R Steffen and M Kay ldquoBenign recurrentintrahepatic cholestasis Improvement of pruritus and shorten-ing of the symptomatic phase with rifampin therapy A casereportrdquo Clinical Pediatrics vol 36 no 8 pp 483ndash485 1997
[77] U Beuers M Trauner P Jansen and R Poupon ldquoNewparadigms in the treatment of hepatic cholestasis FromUDCAto FXR PXR and beyondrdquo Journal of Hepatology vol 62 no 1pp S25ndashS37 2015
[78] L Bachs A Pares M Elena C Piera and J Rodes ldquoEffectsof long-term rifampicin administration in primary biliarycirrhosisrdquoGastroenterology vol 102 no 6 pp 2077ndash2080 1992
[79] J M Stapelbroek K J Van Erpecum L W J Klomp et alldquoNasobiliary drainage induces long-lasting remission in benignrecurrent intrahepatic cholestasisrdquoHepatology vol 43 no 1 pp51ndash53 2006
[80] F Lammert H-U Marschall A Glantz and S MaternldquoIntrahepatic cholestasis of pregnancymolecular pathogenesisdiagnosis and managementrdquo Journal of Hepatology vol 33 no6 pp 1012ndash1021 2000
[81] P H Dixon and C Williamson ldquoThe pathophysiology ofintrahepatic cholestasis of pregnancyrdquo Clinics and Research inHepatology and Gastroenterology vol 40 no 2 pp 141ndash1532016
[82] M G Martineau C Raker P H Dixon et al ldquoThe metabolicprofile of intrahepatic cholestasis of pregnancy is associatedwith impaired glucose tolerance dyslipidemia and increasedfetal growthrdquo Diabetes Care vol 38 no 2 pp 243ndash248 2015
[83] D G Goulis I A LWalkerMDe Swiet CWG Redman andC Williamson ldquoPreeclampsia with Abnormal Liver FunctionTests Is Associated with Cholestasis in a Subgroup of CasesrdquoHypertension in Pregnancy vol 23 no 1 pp 19ndash27 2004
[84] A Glantz H-U Marschall F Lammert and L-A MattssonldquoIntrahepatic cholestasis of pregnancy A randomized con-trolled trial comparing dexamethasone and ursodeoxycholicacidrdquo Hepatology vol 42 no 6 pp 1399ndash1405 2005
[85] R Zapata L Sandoval J Palma et al ldquoUrsodeoxycholic acidin the treatment of intrahepatic cholestasis of pregnancy A 12-year experiencerdquo Liver International vol 25 no 3 pp 548ndash5542005
[86] T Binder P Salaj T Zima and L Vıtek ldquoRandomized prospec-tive comparative study of ursodeoxycholic acid and S-adenosyl-L-methionine in the treatment of intrahepatic cholestasis ofpregnancyrdquo Journal of PerinatalMedicine vol 34 no 5 pp 383ndash391 2006
[87] P H Dixon N Weerasekera K J Linton et al ldquoHeterozy-gous MDR3 missense mutation associated with intrahepaticcholestasis of pregnancy Evidence for a defect in proteintraffickingrdquo Human Molecular Genetics vol 9 no 8 pp 1209ndash1217 2000
[88] C Gendrot Y Bacq M-C Brechot J Lansac and C AndresldquoA second heterozygous MDR3 nonsense mutation associatedwith intrahepatic cholestasis of pregnancyrdquo Journal of MedicalGenetics vol 40 no 3 article e32 2003
[89] A Floreani I Carderi D Paternoster et al ldquoIntrahepaticcholestasis of pregnancy Three novel MDR3 gene mutationsrdquoAlimentary Pharmacology amp Therapeutics vol 23 no 11 pp1649ndash1653 2006
[90] J N Painter M Savander A Ropponen et al ldquoSequencevariation in the ATP8B1 gene and intrahepatic cholestasis of
12 Canadian Journal of Gastroenterology and Hepatology
pregnancyrdquo European Journal of Human Genetics vol 13 no 4pp 435ndash439 2005
[91] W L Van Der Woerd R H J Houwen and S F J Van DeGraaf ldquoCurrent and future therapies for inherited cholestaticliver diseasesrdquoWorld Journal of Gastroenterology vol 23 no 5pp 763ndash775 2017
[92] A Thebaut D Habes F Gottrand et al ldquoSertraline as an addi-tional treatment for cholestatic pruritus in childrenrdquo Journal ofPediatric Gastroenterology and Nutrition vol 64 no 3 pp 431ndash435 2017
[93] U Ołdakowska-Jedynak I JankowskaM Hartleb et al ldquoTreat-ment of pruritus with Prometheus dialysis and absorption sys-tem in a patient with benign recurrent intrahepatic cholestasisrdquoHepatology Research vol 44 no 10 pp E304ndashE308 2014
[94] L Cutillo M Najimi F Smets et al ldquoSafety of living-related liver transplantation for progressive familial intrahep-atic cholestasisrdquo Pediatric Transplantation vol 10 no 5 pp570ndash574 2006
[95] E Gonzales B Grosse B Schuller et al ldquoTargeted phar-macotherapy in progressive familial intrahepatic cholestasistype 2 Evidence for improvement of cholestasis with 4-phenylbutyraterdquo Hepatology vol 62 no 2 pp 558ndash566 2015
[96] E Gonzales and E Jacquemin ldquoMutation specific drug ther-apy for progressive familial or benign recurrent intrahepaticcholestasis A new tool in a near futurerdquo Journal of Hepatologyvol 53 no 2 pp 385ndash387 2010
[97] M Trauner C D Fuchs E Halilbasic and G PaumgartnerldquoNew therapeutic concepts in bile acid transport and signalingfor management of cholestasisrdquo Hepatology vol 65 no 4 pp1393ndash1404 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

2 Canadian Journal of Gastroenterology and Hepatology
Enterocyte
Cho
lang
iocyte
Hepatocyte
NTCP BSEP
FIC1
Aminophospholipids
MRP3
OST
BS
BSBSBS
BS
MDR3
Lecithin
MRP34
OST
OATP1B13
FXR-RXR
SHP
cholCYP7A1
FXR-RXR
SHP
MRP3
OST
ASBT
FXRBS
BS
ASBTIBABP
FGF19
FGF19
FGFR4
+
++
+
+
+
+
-
-
-
- -
BS
BS
SHP
Na+
Na+
Na+
Figure 1 Bile salt and lipid transporters and their regulatory pathways
transported into the intestinal tract where they are decon-jugated oxidised and dehydroxylated to form 7-deoxycholicand lithocholic acid as part of a reaction catalysed by bacterial7 alpha-dehydroxylases Finally most intestinal BS (95)are reabsorbed in the distal part of the small intestine andtransported to the liver via the portal blood and to alesser extent via the hepatic artery in a process known asenterohepatic circulation The BS pool is recycled 4-12 timesa day BS lost in the faeces (02-06 gday) are replenished byde novo synthesis in the liver [1ndash3]
3 Bile Salt and Lipid Transporters
Bile acids form dissociated sodium or potassium salts inbody fluids with neutral pH Therefore BS transporters aredesigned as anion transporters Enterohepatic circulation ofBS is driven by several specific transport systems expressedpredominantly in hepatocytes and biliary and intestinalepithelia (Figure 1)
In hepatocytes Na+-dependent taurocholate cotrans-porting peptide (NTCP also known as the sodiumbile acidcotransporter) encoded by SLC10A1 (solute carrier family 10member 1) represents themajor conjugatedBS uptake systemfrom the blood contributing 80 of the transport capacity
NTCP is localised in the basolateral (sinusoidal) membraneand its driving force the Na+ concentration gradient ismaintained by Na+K+-ATPase [4 5] NTCP deficiency hasrecently been shown to cause severe familial predominantlyconjugated hypercholanemia with no cholestatic jaundicepruritus and liver disease [6]
Unconjugated BS are transported by the multispecificATP- and Na+-independent basolateral uptake transportersorganic anion-transporting polypeptide 1B1 (OATP1B1 alsotermed OATP-C OATP2 SLC21A6 or LST-1 encoded bySLCO1B1) and 1B3 (OATP1B3 synonyms OATP8 SLC21A8or LST3 encoded by SLCO1B3) [4 7 8] They play asecondary role in liver uptake of conjugated BS since thepresence of both OATP1Bs only partly compensates forNTCP deficiency [6]
The basolateral domain of hepatocytes also possessesseveral ATP-dependent efflux pumps which constitute themultidrug resistance protein (MRP) subfamily (ABCC)ABCC proteins transport organic anions including BS [9 10]
MRP3 (encoded by ABCC3) is a basolateral transporterof BS glucuronide and anionic conjugates including glu-tathione [11ndash13] In the liver MRP3 is expressed predomi-nantly in the centrilobular hepatocytes and its expression islow under physiological conditions MRP3 expression rate is
Canadian Journal of Gastroenterology and Hepatology 3
upregulated during cholestasis and independently of anycholestaticmanifestation in individuals withDubin-Johnsonsyndrome or after repeated administration of ethinylestradiol[11 14 15] As well as in hepatocytes Northern blotting ofvarious human tissues indicates the presence of MRP3 inthe bile duct epithelium gallbladder intestine pancreas andkidney [16]
MRP4 (gene ABCC4) is an inducible basolateral trans-porter that cotransports taurine and glycine conjugates ofcholic acid with glutathione It is also a high-affinity trans-porter of sulphated BS dehydroepiandrosterone sulphateeicosanoids and uric acid as well as signalling moleculessuch as cAMP and cGMP [17] Although MRP4 expressionin the liver is low it can be induced by BS in cholestasis [1819] Strong upregulation of human MRP4 has been demon-strated in patients with BS export pump (BSEP) deficiency[20]
The heterodimeric organic solute transporter OST120572-OST120573 initially identified as a basolateral BS efflux systemin enterocytes (see below) is also localised in the sinusoidalmembrane of hepatocytes [21] Hepatic OST120572-OST120573 expres-sion increases in patients with primary biliary cirrhosis andin bile duct-ligated rodents [22] Thus during cholestasisMRP3 MRP4 and OST120572-OST120573 may provide effective pro-tection against hepatocellular BS overload
The transfer of BS from the liver to the bile canaliculus isdetermined by several transport proteins in the canalicular(apical) membrane of hepatocytes mainly ATP-dependentBSEP and MRPs
BSEP encoded by ABCB11 is responsible for the ATP-dependent transport of predominantly monovalent conju-gated BS across the hepatocyte canalicular membrane It isexclusively expressed in the liver and localised predominantlyin the canalicular microvillar (but not the intermicrovillar)membrane and to a lesser extent in subcanalicular (subapical)vesicles [23] Expression of BSEP is sensitive to the flux ofBS through hepatocytes The BSEP promoter contains aninverted repeat DNA element (IR-1) a binding site for thefarnesoid X receptor (FXR) which plays an important rolein maintaining BS homeostasis (see below)
Multidrug resistance protein 3 (MDR3 gene ABCB4) isunderstood to act as a floppase which translocates phospho-lipids from the inner to the outer leaflet of the lipid bilayer ofthe canalicular membrane [24] Mutations in ABCB4 causecholestasis which is characterised by the decreased biliarylecithin output impaired formation of mixed micelles andthe production ofmore hydrophilic bilewith potent detergentproperties resulting in membrane damage [25 26]
Familial intrahepatic cholestasis type 1 transporter (FIC1gene ATP8B1) a member of the type 4 subfamily of P-typeATPases (P4 ATPase) is a flippase that mediates the translo-cation of aminophospholipids from the outer (exoplasmic)to the inner (cytoplasmic) leaflet of the plasma membrane[27] In most eukaryotic cells phosphatidylcholine andsphingolipids are concentrated in the exoplasmic leafletwhereas the aminophospholipids (phosphatidylserine andphosphatidylethanolamine) are largely confined to the cyto-plasmic leaflet FIC1 thus helps in maintaining asymmetry
and fluidity characteristics of plasma membranes the essen-tial prerequisites for proper function of transmembraneembedded pumps [27]
Cholangiocytes are important modifiers of bile com-position Conjugated BS need to be actively transportedinto cholangiocytes via apical sodium-dependent bile acidtransporter (ASBT gene SLC10A2) and are exported into theperibiliary capillary plexus via the heterodimeric transporterOST120572-OST120573 and via MRP3 [28 29] Under physiologicalconditions BS transporters in cholangiocytes can play amajor role in the regulation of intracellular concentrationsof BS as signalling molecules In obstructive cholestasischolangiocellular BS receptors may facilitate the removal ofBS from stagnant bile [3 28 29]
An important step in maintaining BS homeostasis is thereabsorption of BS in the intestinal lumen predominantlyin the ileum Intestinal epithelial cells reabsorb the majorityof secreted BS through ASBT localised in the brush bordermembrane of enterocytes Human ASBT also called ileal bileacid transporter or ileal sodium-dependent bile acid trans-porter consists of 348 amino acids It transports conjugatedand unconjugated BS with a higher affinity for chenodeoxy-cholic and deoxycholic acid than for taurocholate [30] Afteruptake into the enterocyte the transcellular movement of BSis mediated by cytosolic ileal bile acid-binding protein alsoknown as fatty acid-binding protein 6 or gastrotropin (IBABPFABP6 gene FABP6) that is cytoplasmically attached toASBT [30]
The heterodimeric organic solute transporter OST120572-OST120573 (OST120572 gene SLC51A OST120573 gene SLC51B) is expressedin the basolateral membrane of enterocytes and effluxes BSto the portal blood In humans OST120572-OST120573 is expressed athigh levels in a variety of tissues and is the primary trans-porter of BS into the systemic circulation [21 22 30]
Furthermore MRP3 may also participate in the basolat-eral transport of BS in human enterocytes although its overallcontribution is small [10]
4 Regulation of Bile SaltSynthesis and Trafficking
The BS biosynthesis and enterohepatic circulation are tightlyregulated at many levels but particularly by transcriptionaland posttranscriptionalmechanisms [2 3] A key regulator ofBS synthesis and enterohepatic flow is the nuclear farnesoidX receptor (FXR) a major BS-responsive ligand-activatedtranscription factor with a high affinity for several majorendogenous BS [2 31 32] Expression levels of the FXRgene (also known as the NR1H4 genemdashnuclear receptorsubfamily 1 group H member 4) are highest in the intestinepredominantly in the ileal epithelium liver and kidneys [3132]
FXR acts as an agonist-dependent transcriptional acti-vator of its direct target genes The preferred DNA-bindingsequence for FXR within its target promoters is a variantof inverted repeat-1 motif (IR-1) to which FXR binds as aheterodimer with the retinoid X receptor (RXR) FXR canalso downregulate the transcription of specific target genesindirectly via another nuclear receptor the small heterodimer
4 Canadian Journal of Gastroenterology and Hepatology
partner (SHP the NR0B2 gene) SHP is an atypical orphannuclear receptor without a DNA-binding domain It acts asa repressor of nuclear receptors as well as of transcriptionfactors belonging to other protein families [2 31 33]
FXR plays a key role in controlling the enterohepaticcirculation of BS largely by directly regulating the expressionof several hepatobiliary transporters (Figure 1) In the liverthe heterodimer FXR-RXR induces the expression of BSEPby binding to an IR-1 element at the promoter [34 35]Likewise FXR can directly transactivate the ABCC2 ABCB4and SLCO1B3 genes [36 37]
The FXR-RXR complex directly induces the expressionof OST120572-OST120573 (in ileal enterocytes and in the basolateralmembrane of hepatocytes) as well as intestinal expression ofthe intestinal bile acid-binding protein (IBABP) [22 37]
In addition to directly activating the main BS effluxsystems under cholestatic conditions FXR concurrentlydownregulates the main BS uptake systems primarily NTCPin the basolateral membrane of hepatocytes and ASBT inthe ileal epithelium OATP1B1 is also suppressed by anFXR-dependent pathway during cholestasis FXR-mediatedrepression of target genes is indirect and mainly effected viaSHP [2 33 37]
As well as regulating transport systems involved in theenterohepatic flow of BS FXR represses the transcription ofgenes that encode regulatory enzymes in both classical andalternative BS biosynthetic pathways predominantlyCYP7A1and CYP27A1 [2 33]
There are two important FXR-dependent mechanismsfor BS-induced inhibition of CYP7A1 gene transcription theFXRSHP pathway in the liver and the FXRFGF19FGFR4pathway in the intestine [2 37]
In the liver the heterodimer FXRRXR after bindingretinoic acid andBS induces the expression of SHPThe inter-action of SHP with liver receptor homologue-1 (LRH-1 alsoNR5A2 gene NR5A2) and hepatocyte nuclear factor-4120572(HNF4120572 also NR2A1 gene HNF4A) inhibits CYP7A1 tran-scription [2 32 33] In the CYP27A1 gene the BS responseelement contains a DNA-binding site for HNF4120572 only notfor LRH-1 [2 31]
In the intestine FXR induces an intestinal hormonefibroblast growth factor 19 (FGF19 gene FGF19) whichactivates hepatic FGF receptor 4 (FGFR4 gene FGFR4) anddownregulates BS synthesis by inhibitingCYP71A expressionThe FXRFGF19FGFR4 pathway seems to be the physiolog-ical mechanism for feedback regulation of BS biosynthesisFurthermore the FGF19 autocrine pathway exists in thehuman liver [2 31 37 38]
Along with FXR-related regulation of BS biosynthesisthere are several FXR-independent mechanisms of CYP7A1inhibition mediated by pregnane X receptor (PXR) vitaminD receptor (VDR) the cytokines tumour necrosis factor120572 (TNF120572) and interleukin 1120573 (IL-1120573) transforming growthfactor 1205731 (TGF1205731) epidermal growth factor receptor (EGFR)and others These factors activate signalling pathways whichplay roles in protecting against BS toxicity during cholestaticliver injury [2 31 32 37]
Finally FXR also directly transactivates genes encod-ing enzymes that metabolise BS such as human uri-dine 5rsquo-diphosphate-glucuronosyltransferase 2B4 (UGT2B4encoded by UGT2B4) Interestingly FXR binds the UGT2B4promoter as amonomerwithout previous heterodimerisationwith RXR [32]
Several nuclear receptors such as FXR RXR LXR andSHP are also expressed in cholangiocytes but their role in bileduct biology remains to be elucidated [29]
5 Familial Intrahepatic Cholestasis
Up- and downregulation of transport systems involved inbile formation can explain the impaired liver uptake andexcretion of biliary constituents which result in cholestasisand jaundice in some hereditary andmany common acquiredliver disorders Hereditary diseases characterised by hepato-canalicular cholestasis which is caused by defects in hepato-biliary transporters their regulator FXR and in tightness ofthe liver epithelium include progressive familial intrahepaticcholestasis (PFIC) types 1 to 5 benign recurrent intrahepaticcholestasis (BRIC) 1 and 2 familial cholelithiasis caused by alack of biliary secretion of phospholipids (Low Phospholipid-AssociatedCholelithiasis orGallbladderDisease-1) intrahep-atic cholestasis of pregnancy (ICP) and several other raredisorders Hereditary predisposition also plays an impor-tant role in drug-induced intrahepatic cholestasis includingcholestasis induced by hormonal contraceptives [39 40]
51 Progressive Familial Intrahepatic Cholestasis PFIC firstdescribed in 1969 [41] is a genetically heterogeneous group ofautosomal recessive disorders caused by mutations in genesthat encode hepatocanalicular transporters of BS and phos-pholipids their regulator FXR andTJP2which is essential fortightness of cell junctions between the epithelial cells liningthe bile ducts The exact incidence of PFIC is not knownbut it is estimated to be in the region of 150000 to 1100000births Both genders are equally affected [42] Clinically PFICusuallymanifests in the first year of life and is characterised byjaundice severe pruritus hepatosplenomegaly steatorrhoeaand retardation of growth and mental development Furthersymptoms caused by a deficit of fat-soluble vitamins includecoagulopathy osteopaenia and neuromuscular disordersWithout adequate treatment the disease progresses to liverfibrosis and cirrhosis and usually ends in death due to liverfailure in the first or more rarely in the second decade of life[40 42]
The PFIC group consists of five representatives (PFIC 1-5) which are classified into two main categories according tolevels of serum rsaquo-glutamyl transferase (GGT) activity GGTis considered a cholestatic enzyme and when elevated isassociated with damage to the apical membranes of bile ductsand the disruption of intercellular connections due to highconcentrations of BS in bile However in some cholestaticdiseases synthesis or canalicular secretion of BS is virtuallyabsent and there are no conditions that predispose eitherto the release of membrane GGT from damaged cholan-giocytes or to leakage of bile into the extracellular spaceand subsequently the blood This explains why in hereditary
Canadian Journal of Gastroenterology and Hepatology 5
(a) (b)
Figure 2 Histopathology of ABCB11 disease (a) Giant-cell hepatitis (arrows) with hepatocanalicular cholestasis and (b) complete absenceof ABCB11BSEP protein are typical findings in PFIC2 patients Inset immunohistochemical positivity of BSEP in the apical (canalicular)domain of hepatocytes in a healthy control (a) Hematoxylin and eosin original magnification x200 (b inset) Immunohistochemical stainingwith ABCB11 Rabbit Polyclonal Antibody (NBP1-89319 Novus Biologicals USA) original magnification x200 (b) x400 (inset)
cholestasis GGT activity is increased only in disorders ofphospholipid secretion (PFIC3)
511 Progressive Familial Intrahepatic Cholestasis Type 1(PFIC1) PFIC1 (ATP8B1 disease OMIM 211600) formerlyBylerrsquos disease [41] is the consequence of a severe defect in thegene encoding ATPase ATP8B1FIC1 (familial intrahepaticcholestasis 1) localised in the long arm of the 18th chro-mosome (18q21) [43 44] ATP8B1 deficiency which causesmembrane phospholipid asymmetry of the canalicular mem-brane reduces the capacity of the liver to secrete bile [45 46]In addition to the previously described common symptomsof PFIC clinical manifestation of PFIC1 also includes awide range of extrahepatic symptoms Extrahepatic mani-festations of ATP8B1 disease include elevated sweat chlorideconcentrations delayed pubescence and growth and waterydiarrhoea as well as impaired hearing andor pancreatitis[47] These symptoms often persist while diarrhoea eventends to worsen after liver transplantation (LTX) Liverallografts in PFIC1 patients may display diffuse steatosis witha variable necroinflammatory component with subsequentfibrosis [48] Both diarrhoea and steatosissteatohepatitismay improve after biliary diversion [49]
Laboratory findings with regard to PFIC1 have reportedcholestasis with low serum levels of GGT increased serumconcentrations of primary BS and normal levels of choles-terol Aminotransferases are initially within the referencerange but during disease progression they gradually increaseby up to tenfold [41] Histopathological changes predomi-nantly involve canalicular cholestasis accentuated around thecentral veins The interlobular ducts can be hypoplastic dueto subnormal bile flow Giant-cell changes of hepatocytes aregenerally not observed in biopsies Liver fibrosis progressioncorresponds with the respective stage of the disease and canterminate in cirrhosis A typical ultrastructural finding isthe presence of Byler-type coarsely granular bile in the bilecanaliculi [50] Molecular diagnosis is based on the detectionof pathogenic mutations in both alleles of the ATP8B1 gene
The milder intermittent nonprogressive form of ATP8B1deficiency is called BRIC1 (see below)
512 Progressive Familial Intrahepatic Cholestasis Type 2(PFIC2) PFIC2 (ABCB11 disease OMIM 601847) is causedby mutations in ABCB11 which is located on the longarm of the second chromosome (2q24) and encodes thecanalicular transport proteinABCB11BSEP [51] Clinical andlaboratory findings with regard to PFIC2 are similar to PFIC1but extrahepatic symptoms are not present Additionally inPFIC2 the formation of gallstones and the early elevation ofserum aminotransferase activity can occurThe developmentof hepatobiliarymalignancies both hepatocellular carcinomaand cholangiocarcinoma can be a serious complication ofPFIC2 which is not observed in PFIC1 [52 53] Screening forliver tumours is recommended from the first year of life inPFIC2 patients
Except for PFIC2 mutations in ABCB11 may result in amilder nonprogressive formof PFIC2 known asBRIC2 aswellas other forms of cholestasis such as ICP andor drug-inducedcholestasis (see below)
Histologically the typical findings in the liver biopsies ofPFIC2 patients are giant-cell (syncycial) hepatitis with hepa-tocanalicular cholestasis while extramedullary haemopoiesisis frequently discernible within lobules Interlobular bileducts can be hypoplastic and ductular proliferation at theperipheries of portal triads is commonly observed TheABCB11BSEP protein is usually undetectable immunohis-tochemically (Figure 2) Ultrastructurally canalicular bilecan be either amorphous or filamentous but is not coarselygranular [51]
Untreated PFIC2 usually leads to progressive liver fibrosisand cirrhosis the development of which ismore rapid than inPFIC1 One curative method for patients with PFIC2 is LTXUnlike in PFIC1 steatosis and steatohepatitis are not presentin liver allografts in the case of PFIC2 However in somepatients a recurrence of the PFIC2 phenotype accompaniedby elevated serum levels of BS and bilirubin with almost
6 Canadian Journal of Gastroenterology and Hepatology
normal GGT activity has been observed after LTX [54 55] Ithas been shown that canalicular immunostaining of the BSEPMDR3 and MRP2 proteins is preserved in the liver graftbiopsies and no discernible changes in BSEP immunoreactiv-ity distribution between the apical membrane and the cyto-plasm have been reported nonetheless de novo polyclonalinhibitory antibodies directed against the first extracellularloop of BSEP have been observed in the posttransplant serumof patients a condition known as Autoimmune BSEPDisease(AIBD) [56 57] The exact mechanism by which BS trans-port is inhibited by anti-BSEP antibodies is still unknownIt is supposed that the cross-linking of BSEP moleculeswhich in turn disrupts the structure and function ofcanalicular membranes andor the direct mechanical occlu-sion of the BSEP pore might explain the inhibitory effectsof the antibodies [56 57] It is estimated that up to 8 oftransplanted PFIC2 patients develop anti-BSEP antibodies[56] This may be explained by the insufficient autotoleranceagainst BSEP exhibited in some patients with severe ABCB11mutations resulting in the complete absence of the BSEPproteinThe causal relationship between recurrent cholestasisin the liver grafts of PFIC2 patients and the occurrence of denovo antibodies directed against BSEP is further supportedby observations that plasmapheresis and the administrationof anti-CD20 antibodies (rituximab) may alleviate symptomsof cholestasis [54ndash57]
Interestingly posttransplant development of inhibitoryautoantibodies directed against FIC1 andMDR3 transporterswith corresponding phenotypes has not yet been docu-mented in patients with PFIC1 and PFIC3 respectively[44]
513 Progressive Familial Intrahepatic Cholestasis Type 3(PFIC3) PFIC3 (ABCB4 disease OMIM 602347) is causedby mutations in both alleles of the ABCB4MDR3 gene thatencode phospholipid transporter MDR3 expressed in thecanalicular (apical) membrane of hepatocytes [26] As wellas PFIC3 there is evidence that either biallelic or monoal-lelic ABCB4 defects may cause or predispose patients to awide spectrum of human liver diseases such as LowPhospholipid-Associated Cholelithiasis Syndrome (LPACOMIM 600803) Intrahepatic Cholestasis of Pregnancy(ICP OMIM 147480) drug-induced liver injury transientneonatal cholestasis small duct sclerosing cholangitis andadult biliary fibrosis or cirrhosis [58ndash61] Moreover hepa-tocellular carcinoma and intrahepatic cholangiocarcinomahave been documented in patients withABCB4MDR3muta-tions [61]
Clinical and laboratory findings associated with PFIC3correspond to the other two forms of PFIC but are charac-terised by the absence of extrahepatic symptoms (except forcholelithiasis) Unlike PFIC1 and PFIC2 elevated serumGGTactivity and normal cholesterol levels are typically observedas exhibited by the MDR3 deficit [26 62]
Histopathological findings in connection with ABCB4disease are variable Syncytial (giant-cell) changes cholesta-sis portal inflammatory infiltrate and periportal ductularproliferation accompanied by various stages of fibrosis have
been observed in liver tissue Lipid crystals within bile ductsand fibroobliterative bile duct lesions can be seen Immuno-histochemistry has indicated the absence of the canalicularMDR3 protein predominantly in early onset forms howeverits use is limited compared to PFIC2 Ultrastructurally bile isdense and amorphous in PFIC3 [26 61]
Prolonged cholestasis in PFIC3 is associated with signifi-cant accumulation of copper in liver tissue andwith increasedurine copper excretion ie findings that overlap with thediagnostic criteria for Wilsonrsquos disease [63 64]
514 Progressive Familial Intrahepatic Cholestasis Type 4(PFIC4) The fourth form of PFIC (PFIC4 TJP2 deficiencyOMIM 615878) first described in 2014 [65] is clinicallysimilar to PFIC2 and caused by homozygous or compoundheterozygous mutations in the TJP2 gene located in the9q12 chromosome Tight junction protein 2 (TJP2 also zonaoccludens-2) is a cytoplasmic component of cell-cell junc-tional complexes expressed in most epithelia and creates alink between transmembrane tight junction proteins and theactin cytoskeleton Complete TJP2 deficiency is associatedwith a significant reduction in an integral tight junction pro-tein claudin-1 predominantly in the canalicular membranesof liver cells which subsequently leads to the disruption ofintercellular connections and the leakage of bile through theparacellular space into the liver parenchyma [65 66]
Patients with TJP2 deficiency display severe progressivecholestatic liver disease in early childhood which puts themat increased risk of developing hepatocellular carcinoma [67]Serum GGT activity is normal or at most slightly increasedwhile expression of the canalicular proteins BSEP andMDR3is maintained In addition to liver impairment extrahepaticfeatures have been identified in PFIC4 patients includ-ing neurological and respiratory disorders [66] A singlehomozygous missense mutation in TJP2 has been previouslydescribed as causing benign familial hypercholanemia a raredisorder of oligogenic inheritance which usually manifestsin elevated serum BS concentrations pruritus and fat mal-absorption but which does not lead to the development ofliver disease [68]
515 Progressive Familial Intrahepatic Cholestasis Type 5(PFIC5) PFIC5 (OMIM 617049) first described in 2016[69] is a cholestatic disorder caused by mutations in NR1H4a gene located at 12q231 which encodes FXR the keyregulator of BS metabolism (see above) Homozygous loss ofFXR function is associated with severe neonatal cholestasisand early onset vitamin K-independent coagulopathy whichrapidly progresses to end-stage liver disease The nonrespon-siveness of coagulopathy to vitamin K treatment is likelya direct consequence of the loss of FXR function repre-senting an important distinguishing diagnostic feature ofNR1H4-related cholestasis In addition to low (or normal)GGT activity serum levels of alpha-fetoprotein are typicallyelevated [69]
Liver biopsies have shown diffuse giant-cell transforma-tion of hepatocytes with hepatocellular cholestasis and ductu-lar proliferation Progressive fibrosis and even micronodularcirrhosis are evident at later stages BSEP is undetectable in
Canadian Journal of Gastroenterology and Hepatology 7
the apical domains of hepatocytes which is consistent withlow activity of GGT MDR3 expression on the other hand ismaintained [69]
Since FXR affects several metabolic pathways someNR1H4 variations may be associated with susceptibility tovarious human diseases NR1H4 single-nucleotide polymor-phisms seem to be correlated with differences in glucosehomeostasis gallstone formation ICP inflammatory boweldisease and several other disorders [70 71]
52 Benign Recurrent Intrahepatic Cholestasis (BRIC) BRICis a group of genetically heterogeneous autosomal recessivediseases characterised by intermittent episodes of cholesta-sis They are caused by mutations in the ATP8B1 and ABCB11genes (the same as in PFIC1 and PFIC2) and probably inat least one other as yet unidentified gene [72] Thereare two genetically characterised forms of BRIC BRIC1(Summerskill-Walshe-Tygstrup syndrome OMIM 243300)and BRIC2 (OMIM 605479) caused by partial deficiency inATP8B1 [39 73] and ABCB11 [74] respectively The diseasetypically manifests before the second decade of life but theage of the first manifestation can vary greatly The samevariability has been documented in the duration of cholestaticepisodes (several days to several months) and their intensityInfection or pregnancy may act as a triggering factor Theclinical manifestations include jaundice pruritus fatigueanorexia and steatorrhoea Increase of bilirubin and BS levelsin serum has been observed during cholestatic attacks butGGT activity and serum cholesterol levels tend to be normalAminotransferase activity is usually normal or only slightlyelevated while biochemical parameters fall within normalranges Liver biopsies performed during cholestatic attackshave demonstrated hepatocanalicular cholestasis withoutfibrosis During the asymptomatic period the histologicalpicture is completely normal Since canalicular expression ofBSEP protein in hepatocytes is mostly maintained immuno-histology is of limited significance in these cases Diagnosisof BRIC1 and BRIC2 is based on demonstrating evidence ofmutations in both alleles of the corresponding genesATP8B1and ABCB11
While mutations causing PFIC are often located in theconserved regions of the genes that encode conserved func-tional domains of the corresponding proteins mutations inBRIC only partially impact protein function and expressionHowever several cases of initially benign episodic cholestasisthat have subsequently transitioned to a persistent progres-sive form of the disease have been reported [75] Thus BRICand PFIC seem to represent two extremes of a continuousspectrum of phenotypes of the one disease
The administration of statins corticosteroids cholestyra-mine or ursodeoxycholic acid (UDCA) is usually not veryeffective in BRIC patients Improvement of pruritus andshortening of symptomatic phase has been described inBRIC patients treated with the antibiotic rifampicin a potenthuman activator of PXR [76 77] However severe hepa-totoxicity after long-term administration of rifampicin hasbeen reported in patients with cholestatic disorders [77 78]Nasobiliary drainage seems to have a prompt effect during
cholestatic episodes but the mechanism of action remainsunclear [79]
53 Intrahepatic Cholestasis of Pregnancy (ICP) ICP (OMIM147480) also known as obstetric cholestasis is characterisedby cholestasis and prurituswith onset in pregnancy usually inthe third trimester It is associated with abnormal liverfunction in the absence of other liver diseases and resolvescompletely after delivery [80 81]The incidence of ICP varieswith geographical location and ethnicity Seasonal variationsindicate higher incidence in winter months as reported insome countries and it more commonly occurs in associationwith multiple pregnancies and following in vitro fertilisationIn Europe ICP affects about 1 of all pregnancies [81] Atypical symptom is intense pruritus commonly localised inthe palms and the soles which progresses during pregnancyElevated levels of serum BS and increased liver aminotrans-ferase activity are typical laboratory findings in such casesIncreased serum bilirubin levels have been observed in asmall proportion of cases while jaundice only rarely occursin affected women [81]
ICP usually resolves soon after delivery Although thedisease is considered relatively benign for themother there isan increased rate of adverse foetal outcomes including foetaldistress foetal asphyxia stillbirth or even intrauterine deathall known complications of ICP [81 82] ICPmay also be asso-ciated with an abnormalmetabolic profile in afflictedwomenespecially higher prevalence of dyslipidaemia impaired glu-cose tolerance and maternal comorbidities eg gestationaldiabetes and preeclampsia [82 83] Administration of UDCAimproves clinical symptoms predominantly pruritus andmay even reduce the risk of premature birth [84ndash86]
Mutations in ABCB4 ABCB11 and ATP8B1 have beenidentified in some patients suffering from ICP [87ndash90]Additionally variations in NR1H4 may be implicated in ICPpossibly via downregulation of BSEP expression [71]
6 Conclusions and Perspectives
Identification of the genes involved in hereditary cholestasishas advanced our understanding of the molecular mecha-nisms behind bile formation and transport
Recently mutations in TJP2 and NR1H4 have been foundin patients with apparent BSEP deficiency normal serumGGT activity and no mutations in ABCB11 However thereare rare cases of genetic cholestasis causes of which haveyet to be identified Therefore it seems likely that other yetunidentified genes involved in secretion andor transport ofcholephiles may be responsible for FIC-like phenotypes
Current therapeutic regimens in FIC patients compriseboth nonsurgical and surgical approaches Nonsurgical ther-apy includes drugs predominantly UDCA and rifampicinand nasobiliary drainage the latter being predominantly usedin BRIC patients with intractable pruritus during long-lastingcholestatic episodes [76 77 79] However the mechanismresponsible for the instant and complete relief from pruritusis still unclear
In addition to cholestyramine phenobarbital S-adeno-sylmethionine opiate antagonists UDCA rifampicin and
8 Canadian Journal of Gastroenterology and Hepatology
serotonin antagonists and its reuptake inhibitors seem to bebeneficial in managing refractory pruritus in patients withPFIC [77 91 92] Furthermore clinical and biochemicalimprovements have been observed in BRIC patients withintractable pruritus after using the molecular adsorbentrecirculating system (MARS) and the Prometheus system anextracorporeal liver support therapy based on fractionatedplasma separation and adsorption [93]
Surgical therapies include partial biliary diversion iemechanical interruption of BS enterohepatic circulation inorder to prevent reabsorption of pruritogens (unidentifiedthus far) and their precursors which is primarily usefulin noncirrhotic children with low-GGT PFIC permanentcholestasis andor intense refractory pruritus and orthotopicLTX which is still the ultimate treatment modality for manyPFIC patients [91] However as well as the risks associatedwith these invasive procedures other serious postoperative-related complications have been reported particularly inPFIC1 patients with extradigestive symptoms which canpersist or even worsen most likely due to extrahepaticexpression of FIC1 [47]Moreover the development of steato-sis and steatohepatitis leading to progressive liver allograftfibrosis in PFIC1 patients [48] and recurrence of the PFIC2phenotype in ABCB11 deficiency may represent other seriouscomplications after LTX and for some patients may evennecessitate retransplantation [54ndash57]
Importantly because of the shortage of cadaveric donorsparental living-related LTX is often considered in PFICpatients As heterozygous conditions can cause mild-to-moderate disease expression under certain circumstancesthe use of blood relatives as donors is seen as controversial Insuch cases it is likely that the heterozygous status of the donorallograft could pose a risk of complications during the lateposttransplant period such as lithiasis or cholestasis whichcan be precipitated by infections or by drugs administeredto the patient However the results of a recent study indicatethat the PFIC heterozygote status of the organ donor does notincrease the risk of liver dysfunction [94]
The limited effectiveness of current conservative proce-dures along with the complications of invasive methods par-ticularly LTX stress the need for the development and intro-duction of new treatment options Total biliary diversionpharmacological diversion of BS and hepatocyte transplanta-tion as well as gene- and mutation-targeted pharmacothera-pies represent promising future therapeutic approaches Thelatter two methods provide the basis for personalised treat-ment strategies in FIC patients Pharmacological chaperones(eg 4-phenylbutyrate) agonists of nuclear receptors (egstatins fibrates 6-ethyl chenodeoxycholic acid) endoplasmicreticulum-associated degradation inhibitors (MG132) andseveral other mutation-specific drugs can be used to increasethe expression of functional proteins and mitigate or eveneliminate deficient phenotypes [95ndash97]
Nevertheless despite the indisputable progress in thetherapy of FIC patients the increased risks of hepatobiliarymalignancies particularly in relation to ABCB11 deficiencystill remain serious life-threatening complications Furtherstudies are required in order to elucidate the complex patho-genesis of cholestasis unlock the mechanism of cholestatic
pruritus and improve the clinical management of bothhereditary and acquired cholestatic liver diseases
Abbreviations
ABC ATP-binding cassette subfamilyABCB4 ATP-binding cassette subfamily B
member 4ABCB11 ATP-binding cassette subfamily B
member 11AIBD Autoimmune BSEP DiseaseASBT Apical sodium-dependent bile acid
transporterATP8B1 ATPase aminophospholipid transporter
class I type 8B member 1BRIC Benign Recurrent Intrahepatic CholestasisBS Bile saltsBSEP Bile salt export pumpCYP7A1 Cholesterol 7 alpha-hydroxylaseCYP27A1 Sterol-27 hydroxylaseFGF19 Fibroblast growth factor 19FGFR4 Fibroblast growth factor receptor 4FIC Familial intrahepatic cholestasisFXR Farnesoid X-activated receptorGGT rsaquo-Glutamyl transferaseHNF4120572 Hepatocyte nuclear factor 4120572IBABP Intestinal bile acid-binding proteinICP Intrahepatic cholestasis of pregnancyIR-1 Inverted repeat DNA element with 1
nucleotide spacingLPAC Low Phospholipid-Associated
Cholelithiasis SyndromeLTX Liver allograft transplantationLXR Liver X receptorMDR3 Multidrug resistance protein 3MRP Multidrug resistance-associated proteinNR1H4 Nuclear receptor subfamily 1 group H
member 4NTCP Na+-taurocholate cotransporting
polypeptidesolute carrier family 10member 1
OATP Organic anion-transporting polypeptideOMIM Electronic database Online Mendelian
Inheritance in ManTMOST Organic solute transporterPFIC Progressive Familial Intrahepatic
CholestasisPXR Pregnane X receptorRXR Retinoid X receptorSHP Small heterodimer partnerSLC22A Solute carrier family 22 (organic cation
transporter) member 1SLCO Solute carrier organic anion transporter
familyTJP2 Tight junction protein 2 zona occludens-2UDCA Ursodeoxycholic acidUGT2B4 Uridine
51015840-diphosphate-glucuronosyltransferase2B4
Canadian Journal of Gastroenterology and Hepatology 9
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
Milan Jirsa was supported by Ministry of Health CzechRepublicmdashConceptual Development of Research Organiza-tion (ldquoInstitute for Clinical and Experimental MedicinendashIKEM IN 00023001rdquo)
References
[1] N B Javitt ldquoBile acid synthesis from cholesterol regulatory andauxiliary pathwaysrdquoThe FASEB Journal vol 8 no 15 pp 1308ndash1311 1994
[2] J Y L Chiang ldquoBile acids regulation of synthesisrdquo Journal ofLipid Research vol 50 no 10 pp 1955ndash1966 2009
[3] J L Boyer ldquoBile formation and secretionrdquo ComprehensivePhysiology vol 3 no 3 pp 1035ndash1078 2013
[4] B Hagenbuch and P J Meier ldquoSinusoidal (basolateral) bile saltuptake systems of hepatocytesrdquo Seminars in Liver Disease vol16 no 2 pp 129ndash136 1996
[5] B Hagenbuch B Stieger M Foguet H Lubbert and P JMeier ldquoFunctional expression cloning and characterization ofthe hepatocyte Na+bile acid cotransport systemrdquo Proceedingsof the National Acadamy of Sciences of the United States ofAmerica vol 88 no 23 pp 10629ndash10633 1991
[6] F M Vaz C C Paulusma H Huidekoper et al ldquoSodiumtaurocholate cotransporting polypeptide (SLC10A1) deficiencyConjugated hypercholanemia without a clear clinical pheno-typerdquo Hepatology vol 61 no 1 pp 260ndash267 2015
[7] B Hagenbuch and P J Meier ldquoOrganic anion transportingpolypeptides of the OATPSLC21 family Phylogenetic classi-fication as OATPSLCO super-family new nomenclature andmolecularfunctional propertiesrdquo Pflugers Archiv - EuropeanJournal of Physiology vol 447 no 5 pp 653ndash665 2004
[8] B Hagenbuch and B Stieger ldquoThe SLCO (former SLC21)superfamily of transportersrdquoMolecular Aspects of Medicine vol34 no 2-3 pp 396ndash412 2013
[9] M Muller and P L M Jansen ldquoThe secretory function ofthe liver New aspects of hepatobiliary transportrdquo Journal ofHepatology vol 28 no 2 pp 344ndash354 1998
[10] G J E J Hooiveld J E Van Montfoort D K F Meijerand M Muller ldquoFunction and regulation of ATP-bindingcassette transport proteins involved in hepatobiliary transportrdquoEuropean Journal of Pharmaceutical Sciences vol 12 no 4 pp525ndash543 2001
[11] J Konig D Rost Y Cui and D Keppler ldquoCharacterizationof the human multidrug resistance protein isoform MRP3localized to the basolateral hepatocyte membranerdquoHepatologyvol 29 no 4 pp 1156ndash1163 1999
[12] H Zeng G Liu P A Rea and G D Kruh ldquoTransport ofamphipathic anions by human multidrug resistance protein 3rdquoCancer Research vol 60 pp 4779ndash4784 2000
[13] Y-M A Lee Y Cui J Konig et al ldquoIdentification and func-tional characterization of the natural variantMRP3-Arg1297Hisof human multidrug resistance protein 3 (MRP3ABCC3)rdquoPharmacogenetics vol 14 no 4 pp 213ndash223 2004
[14] M Donner ldquoUp-regulation of basolateral multidrug resistanceprotein 3 (Mrp3) in cholestatic rat liverrdquoHepatology vol 34 no2 pp 351ndash359 2001
[15] M L Ruiz J P Rigalli A Arias et al ldquoInduction of hepaticmultidrug resistance-associated protein 3 by ethynylestradiol isindependent of cholestasis and mediated by estrogen receptorrdquoDrug Metabolism and Disposition vol 41 no 2 pp 275ndash2802013
[16] N J Cherrington D P Hartley N Li D R Johnson and C DKlaassen ldquoOrgan distribution of multidrug resistance proteins1 2 and 3 (Mrp1 2 and 3) mRNA and hepatic induction ofMrp3 by constitutive androstane receptor activators in ratsrdquoTheJournal of Pharmacology and Experimental Therapeutics vol300 no 1 pp 97ndash104 2002
[17] C A Ritter G Jedlitschky H Meyer Zu Schwabedissen MGrube K Kock and H K Kroemer ldquoCellular export ofdrugs and signaling molecules by the ATP-binding cassettetransporters MRP4 (ABCC4) and MRP5 (ABCC5)rdquo DrugMetabolism Reviews vol 37 no 1 pp 253ndash278 2005
[18] F G M Russel J B Koenderink and R Masereeuw ldquoMul-tidrug resistance protein 4 (MRP4ABCC4) a versatile effluxtransporter for drugs and signalling moleculesrdquo Trends inPharmacological Sciences vol 29 no 4 pp 200ndash207 2008
[19] D Keppler ldquoProgress in the molecular characterization ofhepatobiliary transportersrdquoDigestive Diseases vol 35 no 3 pp197ndash202 2017
[20] V Keitel M Burdelski U Warskulat et al ldquoExpression andlocalization of hepatobiliary transport proteins in progressivefamilial intrahepatic cholestasisrdquo Hepatology vol 41 no 5 pp1160ndash1172 2005
[21] N Ballatori F FangWV Christian N Li andC LHammondldquoOst120572-Ost120573 is required for bile acid and conjugated steroiddisposition in the intestine kidney and liverrdquoAmerican Journalof Physiology-Gastrointestinal and Liver Physiology vol 295 no1 pp G179ndashG186 2008
[22] J L Boyer M Trauner A Mennone et al ldquoUpregulationof a basolateral FXR-dependent bile acid efflux transporterOSTalpha-OSTbeta in cholestasis in humans and rodentsrdquoAmerican Journal of Physiology-Gastrointestinal and Liver Phys-iology vol 290 no 6 pp G1124ndashG1130 2006
[23] T Gerloff B Stieger B Hagenbuch et al ldquoThe sister of P-glycoprotein represents the canalicular bile salt export pump ofmammalian liverrdquoThe Journal of Biological Chemistry vol 273no 16 pp 10046ndash10050 1998
[24] A M van der Bliek F Baas T Ten Houte de Lange P MKooiman T van der Velde-Koerts and P Borst ldquoThe humanmdr3 gene encodes a novel P-glycoprotein homologue and givesrise to alternatively splicedmRNAs in liverrdquo EMBO Journal vol6 no 11 pp 3325ndash3331 1987
[25] A J Smith J L Timmermans-Hereijgers and B RoelofsenldquoThe human MDR3 P-glycoprotein promotes translocation ofphosphatidylcholine through the plasma membrane of fibrob-lasts from transgenic micerdquo FEBS Letters vol 354 no 3 pp263ndash266 1994
[26] J M L de Vree E Jacquemin E Sturm et al ldquoMutations in theMDR3 gene cause progressive familial intrahepatic cholestasisrdquoProceedings of the National Acadamy of Sciences of the UnitedStates of America vol 95 no 1 pp 282ndash287 1998
[27] A Groen M R Romero C Kunne et al ldquoComplementaryfunctions of the flippase ATP8B1 and the floppase ABCB4 inmaintaining canalicular membrane integrityrdquoGastroenterologyvol 141 no 5 pp 1927ndash1937 2011
10 Canadian Journal of Gastroenterology and Hepatology
[28] P A Dawson T Lan and A Rao ldquoThematic review series Bileacids Bile acid transportersrdquo Journal of Lipid Research vol 50no 12 pp 2340ndash2357 2009
[29] E Halilbasic T Claudel andM Trauner ldquoBile acid transportersand regulatory nuclear receptors in the liver and beyondrdquoJournal of Hepatology vol 58 no 1 pp 155ndash168 2013
[30] B L Shneider ldquoIntestinal bile acid transport Biology physiol-ogy and pathophysiologyrdquo Journal of Pediatric Gastroenterologyand Nutrition vol 32 no 4 pp 407ndash417 2001
[31] T Claudel G Zollner M Wagner and M Trauner ldquoRoleof nuclear receptors for bile acid metabolism bile secretioncholestasis and gallstone diseaserdquoBiochimica et Biophysica Acta(BBA) - Molecular Basis of Disease vol 1812 no 8 pp 867ndash8782011
[32] J J Eloranta and G A Kullak-Ublick ldquoThe role of FXR indisorders of bile acid homeostasisrdquo Physiology Journal vol 23no 5 pp 286ndash295 2008
[33] B Goodwin S A Jones R R Price et al ldquoA regulatory cascadeof the nuclear receptors FXR SHP-1 and LRH-1 represses bileacid biosynthesisrdquo Molecular Cell vol 6 no 3 pp 517ndash5262000
[34] M Muller P L M Jansen K N Faber et al ldquoFarnesoid Xreceptor and bile salts are involved in transcriptional regulationof the gene encoding the human bile salt export pumprdquoHepatology vol 35 no 3 pp 589ndash596 2002
[35] M Ananthanarayanan N BalasubramanianMMakishima DJ Mangelsdorf and F J Suchy ldquoHuman bile salt export pumppromoter is transactivated by the farnesoid X receptorbile acidreceptorrdquo The Journal of Biological Chemistry vol 276 no 31pp 28857ndash28865 2001
[36] L Huang A Zhao J L Lew et al ldquoFarnesoid X receptoractivates transcription of the phospholipid pump MDR3rdquo TheJournal of Biological Chemistry vol 278 no 51 pp 51085ndash510902003
[37] M Wagner G Zollner and M Trauner ldquoNuclear receptorregulation of the adaptive response of bile acid transporters incholestasisrdquo Seminars in Liver Disease vol 30 no 2 pp 160ndash1772010
[38] Y Zhang H R Kast-Woelbern and P A Edwards ldquoNaturalstructural variants of the nuclear receptor farnesoid X recep-tor affect transcriptional activationrdquo The Journal of BiologicalChemistry vol 278 no 1 pp 104ndash110 2003
[39] SW C VanMil R H J Houwen and LW J Klomp ldquoGeneticsof familial intrahepatic cholestasis syndromesrdquo Journal of Med-ical Genetics vol 42 no 6 pp 449ndash463 2005
[40] V E H Carlton L Pawlikowska and L N Bull ldquoMolecularbasis of intrahepatic cholestasisrdquoAnnals ofMedicine vol 36 no8 pp 606ndash617 2004
[41] R J Clayton F L Iber B H Ruebner and V A MckusickldquoByler Disease Fatal Familial Intrahepatic Cholestasis in anAmish Kindredrdquo American Journal of Diseases of Children vol117 no 1 pp 112ndash124 1969
[42] E Jacquemin ldquoProgressive familial intrahepatic cholestasisrdquoClinics andResearch inHepatology andGastroenterology vol 36supplement 1 pp S26ndashS35 2012
[43] L N Bull M J T Van Eijk L Pawlikowska et al ldquoA geneencoding a P-type ATPase mutated in two forms of hereditarycholestasisrdquo Nature Genetics vol 18 no 3 pp 219ndash224 1998
[44] L W J Klomp J C Vargas S W C Van Mil et al ldquoCharac-terization of mutations in ATP8B1 associated with hereditarycholestasisrdquo Hepatology vol 40 no 1 pp 27ndash38 2004
[45] P Ujhazy D Ortiz S Misra et al ldquoFamilial intrahepaticcholestasis 1 Studies of localization and functionrdquo Hepatologyvol 34 no 4 I pp 768ndash775 2001
[46] C C Paulusma A Groen C Kunne et al ldquoAtp8b1 deficiencyin mice reduces resistance of the canalicular membrane tohydrophobic bile salts and impairs bile salt transportrdquo Hepatol-ogy vol 44 no 1 pp 195ndash204 2006
[47] SW C VanMil LW J Klomp L N Bull and RH J HouwenldquoFIC1 disease A spectrumof intrahepatic cholestatic disordersrdquoSeminars in Liver Disease vol 21 no 4 pp 535ndash544 2001
[48] A Miyahawa-Hayashino H Egawa T Yorifuji et al ldquoAllograftsteatohepatitis in progressive familial intrahepatic cholestasistype 1 after living donor liver transplantationrdquo Liver Transplan-tation vol 15 no 6 pp 610ndash618 2009
[49] E Nicastro X Stephenne F Smets et al ldquoRecovery of graftsteatosis and protein-losing enteropathy after biliary diversionin a PFIC 1 liver transplanted childrdquo Pediatric Transplantationvol 16 no 5 pp E177ndashE182 2012
[50] K Evason K E Bove M J Finegold et al ldquoMorphologic find-ings in progressive familial intrahepatic cholestasis 2 (PFIC2)Correlation with genetic and immunohistochemical studiesrdquoThe American Journal of Surgical Pathology vol 35 no 5 pp687ndash696 2011
[51] S S Strautnieks L N Bull A S Knisely et al ldquoA gene encodinga liver-specific ABC transporter is mutated in progressivefamilial intrahepatic cholestasisrdquo Nature Genetics vol 20 no3 pp 233ndash238 1998
[52] A S Knisely S S Strautnieks Y Meier et al ldquoHepatocellularcarcinoma in ten children under five years of age with bile saltexport pumpdeficiencyrdquoHepatology vol 44 no 2 pp 478ndash4862006
[53] A O Scheimann S S Strautnieks A S Knisely J A Byrne RJ Thompson andM J Finegold ldquoMutations in Bile Salt ExportPump (ABCB11) in Two Children with Progressive FamilialIntrahepatic Cholestasis and Cholangiocarcinomardquo Journal ofPediatrics vol 150 no 5 pp 556ndash559 2007
[54] V Keitel M Burdelski Z Vojnisek L Schmitt D HaussingerandRKubitz ldquoDe novo bile salt transporter antibodies as a pos-sible cause of recurrent graft failure after liver transplantationA novel mechanism of cholestasisrdquo Hepatology vol 50 no 2pp 510ndash517 2009
[55] P Jara L Hierro P Martınez-Fernandez et al ldquoRecurrence ofbile salt export pump deficiency after liver transplantationrdquoTheNew England Journal of Medicine vol 361 no 14 pp 1359ndash13672009
[56] R Kubitz C Droge S Kluge et al ldquoAutoimmune BSEPDiseaseDisease Recurrence After Liver Transplantation for ProgressiveFamilial Intrahepatic Cholestasisrdquo Clinical Reviews in Allergy ampImmunology vol 48 no 2-3 pp 273ndash284 2015
[57] J Stindt S Kluge C Droge et al ldquoBile salt export pump-reactive antibodies form a polyclonal multi-inhibitoryresponse in antibody-induced bile salt export pump deficiencyrdquoHepatology vol 63 no 2 pp 524ndash537 2016
[58] E Jacquemin J M DeVree D Cresteil et al ldquoThe widespectrum of multidrug resistance 3 deficiency from neonatalcholestasis to cirrhosis of adulthoodrdquoGastroenterology vol 120no 6 pp 1448ndash1458 2001
[59] O Rosmorduc and R Poupon ldquoLow phospholipid associatedcholelithiasis association with mutation in the MDR3ABCB4generdquo Orphanet Journal of Rare Diseases vol 2 article 29 2007
Canadian Journal of Gastroenterology and Hepatology 11
[60] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoThe spectrum of liver diseases related to ABCB4 gene muta-tions Pathophysiology and clinical aspectsrdquo Seminars in LiverDisease vol 30 no 2 pp 134ndash146 2010
[61] DWendumV BarbuO Rosmorduc L Arrive J-F Flejou andR Poupon ldquoAspects of liver pathology in adult patients withMDR3ABCB4 gene mutationsrdquo Virchows Archiv vol 460 no3 pp 291ndash298 2012
[62] R P J Oude Elferink andC C Paulusma ldquoFunction and patho-physiological importance of ABCB4 (MDR3 P-glycoprotein)rdquoPflugers Archiv - European Journal of Physiology vol 453 no 5pp 601ndash610 2007
[63] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoProgressive familial intrahepatic cholestasisrdquo Clinical Pedi-atrics vol 51 pp 689ndash691 2012
[64] S Boga D Jain andM L Schilsky ldquoPresentation of progressivefamilial intrahepatic cholestasis type 3 mimicking wilson dis-ease molecular genetic diagnosis and response to treatmentrdquoPediatric Gastroenterology Hepatology amp Nutrition vol 18 no3 p 202 2015
[65] M Sambrotta S Strautnieks E Papouli et al ldquoMutationsin TJP2 cause progressive cholestatic liver diseaserdquo NatureGenetics vol 46 no 4 pp 326ndash328 2014
[66] M Sambrotta and R J Thompson ldquoMutations in TJP2 encod-ing zona occludens 2 and liver diseaserdquo Tissue Barriers vol 3no 3 Article ID e1026537 2015
[67] S Zhou P M Hertel M J Finegold et al ldquoHepatocellularcarcinoma associated with tight-junction protein 2 deficiencyrdquoHepatology vol 62 no 6 pp 1914ndash1916 2015
[68] V EH Carlton B ZHarris E G Puffenberger et al ldquoComplexinheritance of familial hypercholanemia with associated muta-tions in TJP2 and BAATrdquo Nature Genetics vol 34 no 1 pp 91ndash96 2003
[69] N Gomez-Ospina C J Potter R Xiao et al ldquoMutations inthe nuclear bile acid receptor FXR cause progressive familialintrahepatic cholestasisrdquoNature Communications vol 7 ArticleID 10713 2016
[70] I Koutsounas S Theocharis I Delladetsima E Patsouris andC Giaginis ldquoFarnesoid x receptor in human metabolism anddisease the interplay between gene polymorphisms clinicalphenotypes and disease susceptibilityrdquo Expert Opinion on DrugMetabolism amp Toxicology vol 11 no 4 pp 523ndash532 2015
[71] S W C van Mil A Milona P H Dixon et al ldquoFunctionalVariants of the Central Bile Acid Sensor FXR Identified inIntrahepatic Cholestasis of Pregnancyrdquo Gastroenterology vol133 no 2 pp 507ndash516 2007
[72] C Droge M Bonus U Baumann et al ldquoSequencing of FIC1BSEP and MDR3 in a large cohort of patients with cholestasisrevealed a high number of different genetic variantsrdquo Journal ofHepatology vol 67 no 6 pp 1253ndash1264 2017
[73] L N Bull V E H Carlton N L Stricker et al ldquoGeneticand morphological findings in progressive familial intrahepaticcholestasis (Byler disease [PFIC-1] and Byler syndrome) Evi-dence for heterogeneityrdquo Hepatology vol 26 no 1 pp 155ndash1641997
[74] S W C Van Mil W L Van Der Woerd G Van Der Brugge etal ldquoBenign recurrent intrahepatic cholestasis type 2 is causedby mutations in ABCB11rdquo Gastroenterology vol 127 no 2 pp379ndash384 2004
[75] N A M Van Ooteghem L W J Klomp G P Van Berge-Henegouwen andRH JHouwen ldquoBenign recurrent intrahep-atic cholestasis progressing to progressive familial intrahepatic
cholestasis Low GGT cholestasis is a clinical continuumrdquoJournal of Hepatology vol 36 no 3 pp 439ndash443 2002
[76] F Balsells R Wyllie R Steffen and M Kay ldquoBenign recurrentintrahepatic cholestasis Improvement of pruritus and shorten-ing of the symptomatic phase with rifampin therapy A casereportrdquo Clinical Pediatrics vol 36 no 8 pp 483ndash485 1997
[77] U Beuers M Trauner P Jansen and R Poupon ldquoNewparadigms in the treatment of hepatic cholestasis FromUDCAto FXR PXR and beyondrdquo Journal of Hepatology vol 62 no 1pp S25ndashS37 2015
[78] L Bachs A Pares M Elena C Piera and J Rodes ldquoEffectsof long-term rifampicin administration in primary biliarycirrhosisrdquoGastroenterology vol 102 no 6 pp 2077ndash2080 1992
[79] J M Stapelbroek K J Van Erpecum L W J Klomp et alldquoNasobiliary drainage induces long-lasting remission in benignrecurrent intrahepatic cholestasisrdquoHepatology vol 43 no 1 pp51ndash53 2006
[80] F Lammert H-U Marschall A Glantz and S MaternldquoIntrahepatic cholestasis of pregnancymolecular pathogenesisdiagnosis and managementrdquo Journal of Hepatology vol 33 no6 pp 1012ndash1021 2000
[81] P H Dixon and C Williamson ldquoThe pathophysiology ofintrahepatic cholestasis of pregnancyrdquo Clinics and Research inHepatology and Gastroenterology vol 40 no 2 pp 141ndash1532016
[82] M G Martineau C Raker P H Dixon et al ldquoThe metabolicprofile of intrahepatic cholestasis of pregnancy is associatedwith impaired glucose tolerance dyslipidemia and increasedfetal growthrdquo Diabetes Care vol 38 no 2 pp 243ndash248 2015
[83] D G Goulis I A LWalkerMDe Swiet CWG Redman andC Williamson ldquoPreeclampsia with Abnormal Liver FunctionTests Is Associated with Cholestasis in a Subgroup of CasesrdquoHypertension in Pregnancy vol 23 no 1 pp 19ndash27 2004
[84] A Glantz H-U Marschall F Lammert and L-A MattssonldquoIntrahepatic cholestasis of pregnancy A randomized con-trolled trial comparing dexamethasone and ursodeoxycholicacidrdquo Hepatology vol 42 no 6 pp 1399ndash1405 2005
[85] R Zapata L Sandoval J Palma et al ldquoUrsodeoxycholic acidin the treatment of intrahepatic cholestasis of pregnancy A 12-year experiencerdquo Liver International vol 25 no 3 pp 548ndash5542005
[86] T Binder P Salaj T Zima and L Vıtek ldquoRandomized prospec-tive comparative study of ursodeoxycholic acid and S-adenosyl-L-methionine in the treatment of intrahepatic cholestasis ofpregnancyrdquo Journal of PerinatalMedicine vol 34 no 5 pp 383ndash391 2006
[87] P H Dixon N Weerasekera K J Linton et al ldquoHeterozy-gous MDR3 missense mutation associated with intrahepaticcholestasis of pregnancy Evidence for a defect in proteintraffickingrdquo Human Molecular Genetics vol 9 no 8 pp 1209ndash1217 2000
[88] C Gendrot Y Bacq M-C Brechot J Lansac and C AndresldquoA second heterozygous MDR3 nonsense mutation associatedwith intrahepatic cholestasis of pregnancyrdquo Journal of MedicalGenetics vol 40 no 3 article e32 2003
[89] A Floreani I Carderi D Paternoster et al ldquoIntrahepaticcholestasis of pregnancy Three novel MDR3 gene mutationsrdquoAlimentary Pharmacology amp Therapeutics vol 23 no 11 pp1649ndash1653 2006
[90] J N Painter M Savander A Ropponen et al ldquoSequencevariation in the ATP8B1 gene and intrahepatic cholestasis of
12 Canadian Journal of Gastroenterology and Hepatology
pregnancyrdquo European Journal of Human Genetics vol 13 no 4pp 435ndash439 2005
[91] W L Van Der Woerd R H J Houwen and S F J Van DeGraaf ldquoCurrent and future therapies for inherited cholestaticliver diseasesrdquoWorld Journal of Gastroenterology vol 23 no 5pp 763ndash775 2017
[92] A Thebaut D Habes F Gottrand et al ldquoSertraline as an addi-tional treatment for cholestatic pruritus in childrenrdquo Journal ofPediatric Gastroenterology and Nutrition vol 64 no 3 pp 431ndash435 2017
[93] U Ołdakowska-Jedynak I JankowskaM Hartleb et al ldquoTreat-ment of pruritus with Prometheus dialysis and absorption sys-tem in a patient with benign recurrent intrahepatic cholestasisrdquoHepatology Research vol 44 no 10 pp E304ndashE308 2014
[94] L Cutillo M Najimi F Smets et al ldquoSafety of living-related liver transplantation for progressive familial intrahep-atic cholestasisrdquo Pediatric Transplantation vol 10 no 5 pp570ndash574 2006
[95] E Gonzales B Grosse B Schuller et al ldquoTargeted phar-macotherapy in progressive familial intrahepatic cholestasistype 2 Evidence for improvement of cholestasis with 4-phenylbutyraterdquo Hepatology vol 62 no 2 pp 558ndash566 2015
[96] E Gonzales and E Jacquemin ldquoMutation specific drug ther-apy for progressive familial or benign recurrent intrahepaticcholestasis A new tool in a near futurerdquo Journal of Hepatologyvol 53 no 2 pp 385ndash387 2010
[97] M Trauner C D Fuchs E Halilbasic and G PaumgartnerldquoNew therapeutic concepts in bile acid transport and signalingfor management of cholestasisrdquo Hepatology vol 65 no 4 pp1393ndash1404 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Canadian Journal of Gastroenterology and Hepatology 3
upregulated during cholestasis and independently of anycholestaticmanifestation in individuals withDubin-Johnsonsyndrome or after repeated administration of ethinylestradiol[11 14 15] As well as in hepatocytes Northern blotting ofvarious human tissues indicates the presence of MRP3 inthe bile duct epithelium gallbladder intestine pancreas andkidney [16]
MRP4 (gene ABCC4) is an inducible basolateral trans-porter that cotransports taurine and glycine conjugates ofcholic acid with glutathione It is also a high-affinity trans-porter of sulphated BS dehydroepiandrosterone sulphateeicosanoids and uric acid as well as signalling moleculessuch as cAMP and cGMP [17] Although MRP4 expressionin the liver is low it can be induced by BS in cholestasis [1819] Strong upregulation of human MRP4 has been demon-strated in patients with BS export pump (BSEP) deficiency[20]
The heterodimeric organic solute transporter OST120572-OST120573 initially identified as a basolateral BS efflux systemin enterocytes (see below) is also localised in the sinusoidalmembrane of hepatocytes [21] Hepatic OST120572-OST120573 expres-sion increases in patients with primary biliary cirrhosis andin bile duct-ligated rodents [22] Thus during cholestasisMRP3 MRP4 and OST120572-OST120573 may provide effective pro-tection against hepatocellular BS overload
The transfer of BS from the liver to the bile canaliculus isdetermined by several transport proteins in the canalicular(apical) membrane of hepatocytes mainly ATP-dependentBSEP and MRPs
BSEP encoded by ABCB11 is responsible for the ATP-dependent transport of predominantly monovalent conju-gated BS across the hepatocyte canalicular membrane It isexclusively expressed in the liver and localised predominantlyin the canalicular microvillar (but not the intermicrovillar)membrane and to a lesser extent in subcanalicular (subapical)vesicles [23] Expression of BSEP is sensitive to the flux ofBS through hepatocytes The BSEP promoter contains aninverted repeat DNA element (IR-1) a binding site for thefarnesoid X receptor (FXR) which plays an important rolein maintaining BS homeostasis (see below)
Multidrug resistance protein 3 (MDR3 gene ABCB4) isunderstood to act as a floppase which translocates phospho-lipids from the inner to the outer leaflet of the lipid bilayer ofthe canalicular membrane [24] Mutations in ABCB4 causecholestasis which is characterised by the decreased biliarylecithin output impaired formation of mixed micelles andthe production ofmore hydrophilic bilewith potent detergentproperties resulting in membrane damage [25 26]
Familial intrahepatic cholestasis type 1 transporter (FIC1gene ATP8B1) a member of the type 4 subfamily of P-typeATPases (P4 ATPase) is a flippase that mediates the translo-cation of aminophospholipids from the outer (exoplasmic)to the inner (cytoplasmic) leaflet of the plasma membrane[27] In most eukaryotic cells phosphatidylcholine andsphingolipids are concentrated in the exoplasmic leafletwhereas the aminophospholipids (phosphatidylserine andphosphatidylethanolamine) are largely confined to the cyto-plasmic leaflet FIC1 thus helps in maintaining asymmetry
and fluidity characteristics of plasma membranes the essen-tial prerequisites for proper function of transmembraneembedded pumps [27]
Cholangiocytes are important modifiers of bile com-position Conjugated BS need to be actively transportedinto cholangiocytes via apical sodium-dependent bile acidtransporter (ASBT gene SLC10A2) and are exported into theperibiliary capillary plexus via the heterodimeric transporterOST120572-OST120573 and via MRP3 [28 29] Under physiologicalconditions BS transporters in cholangiocytes can play amajor role in the regulation of intracellular concentrationsof BS as signalling molecules In obstructive cholestasischolangiocellular BS receptors may facilitate the removal ofBS from stagnant bile [3 28 29]
An important step in maintaining BS homeostasis is thereabsorption of BS in the intestinal lumen predominantlyin the ileum Intestinal epithelial cells reabsorb the majorityof secreted BS through ASBT localised in the brush bordermembrane of enterocytes Human ASBT also called ileal bileacid transporter or ileal sodium-dependent bile acid trans-porter consists of 348 amino acids It transports conjugatedand unconjugated BS with a higher affinity for chenodeoxy-cholic and deoxycholic acid than for taurocholate [30] Afteruptake into the enterocyte the transcellular movement of BSis mediated by cytosolic ileal bile acid-binding protein alsoknown as fatty acid-binding protein 6 or gastrotropin (IBABPFABP6 gene FABP6) that is cytoplasmically attached toASBT [30]
The heterodimeric organic solute transporter OST120572-OST120573 (OST120572 gene SLC51A OST120573 gene SLC51B) is expressedin the basolateral membrane of enterocytes and effluxes BSto the portal blood In humans OST120572-OST120573 is expressed athigh levels in a variety of tissues and is the primary trans-porter of BS into the systemic circulation [21 22 30]
Furthermore MRP3 may also participate in the basolat-eral transport of BS in human enterocytes although its overallcontribution is small [10]
4 Regulation of Bile SaltSynthesis and Trafficking
The BS biosynthesis and enterohepatic circulation are tightlyregulated at many levels but particularly by transcriptionaland posttranscriptionalmechanisms [2 3] A key regulator ofBS synthesis and enterohepatic flow is the nuclear farnesoidX receptor (FXR) a major BS-responsive ligand-activatedtranscription factor with a high affinity for several majorendogenous BS [2 31 32] Expression levels of the FXRgene (also known as the NR1H4 genemdashnuclear receptorsubfamily 1 group H member 4) are highest in the intestinepredominantly in the ileal epithelium liver and kidneys [3132]
FXR acts as an agonist-dependent transcriptional acti-vator of its direct target genes The preferred DNA-bindingsequence for FXR within its target promoters is a variantof inverted repeat-1 motif (IR-1) to which FXR binds as aheterodimer with the retinoid X receptor (RXR) FXR canalso downregulate the transcription of specific target genesindirectly via another nuclear receptor the small heterodimer
4 Canadian Journal of Gastroenterology and Hepatology
partner (SHP the NR0B2 gene) SHP is an atypical orphannuclear receptor without a DNA-binding domain It acts asa repressor of nuclear receptors as well as of transcriptionfactors belonging to other protein families [2 31 33]
FXR plays a key role in controlling the enterohepaticcirculation of BS largely by directly regulating the expressionof several hepatobiliary transporters (Figure 1) In the liverthe heterodimer FXR-RXR induces the expression of BSEPby binding to an IR-1 element at the promoter [34 35]Likewise FXR can directly transactivate the ABCC2 ABCB4and SLCO1B3 genes [36 37]
The FXR-RXR complex directly induces the expressionof OST120572-OST120573 (in ileal enterocytes and in the basolateralmembrane of hepatocytes) as well as intestinal expression ofthe intestinal bile acid-binding protein (IBABP) [22 37]
In addition to directly activating the main BS effluxsystems under cholestatic conditions FXR concurrentlydownregulates the main BS uptake systems primarily NTCPin the basolateral membrane of hepatocytes and ASBT inthe ileal epithelium OATP1B1 is also suppressed by anFXR-dependent pathway during cholestasis FXR-mediatedrepression of target genes is indirect and mainly effected viaSHP [2 33 37]
As well as regulating transport systems involved in theenterohepatic flow of BS FXR represses the transcription ofgenes that encode regulatory enzymes in both classical andalternative BS biosynthetic pathways predominantlyCYP7A1and CYP27A1 [2 33]
There are two important FXR-dependent mechanismsfor BS-induced inhibition of CYP7A1 gene transcription theFXRSHP pathway in the liver and the FXRFGF19FGFR4pathway in the intestine [2 37]
In the liver the heterodimer FXRRXR after bindingretinoic acid andBS induces the expression of SHPThe inter-action of SHP with liver receptor homologue-1 (LRH-1 alsoNR5A2 gene NR5A2) and hepatocyte nuclear factor-4120572(HNF4120572 also NR2A1 gene HNF4A) inhibits CYP7A1 tran-scription [2 32 33] In the CYP27A1 gene the BS responseelement contains a DNA-binding site for HNF4120572 only notfor LRH-1 [2 31]
In the intestine FXR induces an intestinal hormonefibroblast growth factor 19 (FGF19 gene FGF19) whichactivates hepatic FGF receptor 4 (FGFR4 gene FGFR4) anddownregulates BS synthesis by inhibitingCYP71A expressionThe FXRFGF19FGFR4 pathway seems to be the physiolog-ical mechanism for feedback regulation of BS biosynthesisFurthermore the FGF19 autocrine pathway exists in thehuman liver [2 31 37 38]
Along with FXR-related regulation of BS biosynthesisthere are several FXR-independent mechanisms of CYP7A1inhibition mediated by pregnane X receptor (PXR) vitaminD receptor (VDR) the cytokines tumour necrosis factor120572 (TNF120572) and interleukin 1120573 (IL-1120573) transforming growthfactor 1205731 (TGF1205731) epidermal growth factor receptor (EGFR)and others These factors activate signalling pathways whichplay roles in protecting against BS toxicity during cholestaticliver injury [2 31 32 37]
Finally FXR also directly transactivates genes encod-ing enzymes that metabolise BS such as human uri-dine 5rsquo-diphosphate-glucuronosyltransferase 2B4 (UGT2B4encoded by UGT2B4) Interestingly FXR binds the UGT2B4promoter as amonomerwithout previous heterodimerisationwith RXR [32]
Several nuclear receptors such as FXR RXR LXR andSHP are also expressed in cholangiocytes but their role in bileduct biology remains to be elucidated [29]
5 Familial Intrahepatic Cholestasis
Up- and downregulation of transport systems involved inbile formation can explain the impaired liver uptake andexcretion of biliary constituents which result in cholestasisand jaundice in some hereditary andmany common acquiredliver disorders Hereditary diseases characterised by hepato-canalicular cholestasis which is caused by defects in hepato-biliary transporters their regulator FXR and in tightness ofthe liver epithelium include progressive familial intrahepaticcholestasis (PFIC) types 1 to 5 benign recurrent intrahepaticcholestasis (BRIC) 1 and 2 familial cholelithiasis caused by alack of biliary secretion of phospholipids (Low Phospholipid-AssociatedCholelithiasis orGallbladderDisease-1) intrahep-atic cholestasis of pregnancy (ICP) and several other raredisorders Hereditary predisposition also plays an impor-tant role in drug-induced intrahepatic cholestasis includingcholestasis induced by hormonal contraceptives [39 40]
51 Progressive Familial Intrahepatic Cholestasis PFIC firstdescribed in 1969 [41] is a genetically heterogeneous group ofautosomal recessive disorders caused by mutations in genesthat encode hepatocanalicular transporters of BS and phos-pholipids their regulator FXR andTJP2which is essential fortightness of cell junctions between the epithelial cells liningthe bile ducts The exact incidence of PFIC is not knownbut it is estimated to be in the region of 150000 to 1100000births Both genders are equally affected [42] Clinically PFICusuallymanifests in the first year of life and is characterised byjaundice severe pruritus hepatosplenomegaly steatorrhoeaand retardation of growth and mental development Furthersymptoms caused by a deficit of fat-soluble vitamins includecoagulopathy osteopaenia and neuromuscular disordersWithout adequate treatment the disease progresses to liverfibrosis and cirrhosis and usually ends in death due to liverfailure in the first or more rarely in the second decade of life[40 42]
The PFIC group consists of five representatives (PFIC 1-5) which are classified into two main categories according tolevels of serum rsaquo-glutamyl transferase (GGT) activity GGTis considered a cholestatic enzyme and when elevated isassociated with damage to the apical membranes of bile ductsand the disruption of intercellular connections due to highconcentrations of BS in bile However in some cholestaticdiseases synthesis or canalicular secretion of BS is virtuallyabsent and there are no conditions that predispose eitherto the release of membrane GGT from damaged cholan-giocytes or to leakage of bile into the extracellular spaceand subsequently the blood This explains why in hereditary
Canadian Journal of Gastroenterology and Hepatology 5
(a) (b)
Figure 2 Histopathology of ABCB11 disease (a) Giant-cell hepatitis (arrows) with hepatocanalicular cholestasis and (b) complete absenceof ABCB11BSEP protein are typical findings in PFIC2 patients Inset immunohistochemical positivity of BSEP in the apical (canalicular)domain of hepatocytes in a healthy control (a) Hematoxylin and eosin original magnification x200 (b inset) Immunohistochemical stainingwith ABCB11 Rabbit Polyclonal Antibody (NBP1-89319 Novus Biologicals USA) original magnification x200 (b) x400 (inset)
cholestasis GGT activity is increased only in disorders ofphospholipid secretion (PFIC3)
511 Progressive Familial Intrahepatic Cholestasis Type 1(PFIC1) PFIC1 (ATP8B1 disease OMIM 211600) formerlyBylerrsquos disease [41] is the consequence of a severe defect in thegene encoding ATPase ATP8B1FIC1 (familial intrahepaticcholestasis 1) localised in the long arm of the 18th chro-mosome (18q21) [43 44] ATP8B1 deficiency which causesmembrane phospholipid asymmetry of the canalicular mem-brane reduces the capacity of the liver to secrete bile [45 46]In addition to the previously described common symptomsof PFIC clinical manifestation of PFIC1 also includes awide range of extrahepatic symptoms Extrahepatic mani-festations of ATP8B1 disease include elevated sweat chlorideconcentrations delayed pubescence and growth and waterydiarrhoea as well as impaired hearing andor pancreatitis[47] These symptoms often persist while diarrhoea eventends to worsen after liver transplantation (LTX) Liverallografts in PFIC1 patients may display diffuse steatosis witha variable necroinflammatory component with subsequentfibrosis [48] Both diarrhoea and steatosissteatohepatitismay improve after biliary diversion [49]
Laboratory findings with regard to PFIC1 have reportedcholestasis with low serum levels of GGT increased serumconcentrations of primary BS and normal levels of choles-terol Aminotransferases are initially within the referencerange but during disease progression they gradually increaseby up to tenfold [41] Histopathological changes predomi-nantly involve canalicular cholestasis accentuated around thecentral veins The interlobular ducts can be hypoplastic dueto subnormal bile flow Giant-cell changes of hepatocytes aregenerally not observed in biopsies Liver fibrosis progressioncorresponds with the respective stage of the disease and canterminate in cirrhosis A typical ultrastructural finding isthe presence of Byler-type coarsely granular bile in the bilecanaliculi [50] Molecular diagnosis is based on the detectionof pathogenic mutations in both alleles of the ATP8B1 gene
The milder intermittent nonprogressive form of ATP8B1deficiency is called BRIC1 (see below)
512 Progressive Familial Intrahepatic Cholestasis Type 2(PFIC2) PFIC2 (ABCB11 disease OMIM 601847) is causedby mutations in ABCB11 which is located on the longarm of the second chromosome (2q24) and encodes thecanalicular transport proteinABCB11BSEP [51] Clinical andlaboratory findings with regard to PFIC2 are similar to PFIC1but extrahepatic symptoms are not present Additionally inPFIC2 the formation of gallstones and the early elevation ofserum aminotransferase activity can occurThe developmentof hepatobiliarymalignancies both hepatocellular carcinomaand cholangiocarcinoma can be a serious complication ofPFIC2 which is not observed in PFIC1 [52 53] Screening forliver tumours is recommended from the first year of life inPFIC2 patients
Except for PFIC2 mutations in ABCB11 may result in amilder nonprogressive formof PFIC2 known asBRIC2 aswellas other forms of cholestasis such as ICP andor drug-inducedcholestasis (see below)
Histologically the typical findings in the liver biopsies ofPFIC2 patients are giant-cell (syncycial) hepatitis with hepa-tocanalicular cholestasis while extramedullary haemopoiesisis frequently discernible within lobules Interlobular bileducts can be hypoplastic and ductular proliferation at theperipheries of portal triads is commonly observed TheABCB11BSEP protein is usually undetectable immunohis-tochemically (Figure 2) Ultrastructurally canalicular bilecan be either amorphous or filamentous but is not coarselygranular [51]
Untreated PFIC2 usually leads to progressive liver fibrosisand cirrhosis the development of which ismore rapid than inPFIC1 One curative method for patients with PFIC2 is LTXUnlike in PFIC1 steatosis and steatohepatitis are not presentin liver allografts in the case of PFIC2 However in somepatients a recurrence of the PFIC2 phenotype accompaniedby elevated serum levels of BS and bilirubin with almost
6 Canadian Journal of Gastroenterology and Hepatology
normal GGT activity has been observed after LTX [54 55] Ithas been shown that canalicular immunostaining of the BSEPMDR3 and MRP2 proteins is preserved in the liver graftbiopsies and no discernible changes in BSEP immunoreactiv-ity distribution between the apical membrane and the cyto-plasm have been reported nonetheless de novo polyclonalinhibitory antibodies directed against the first extracellularloop of BSEP have been observed in the posttransplant serumof patients a condition known as Autoimmune BSEPDisease(AIBD) [56 57] The exact mechanism by which BS trans-port is inhibited by anti-BSEP antibodies is still unknownIt is supposed that the cross-linking of BSEP moleculeswhich in turn disrupts the structure and function ofcanalicular membranes andor the direct mechanical occlu-sion of the BSEP pore might explain the inhibitory effectsof the antibodies [56 57] It is estimated that up to 8 oftransplanted PFIC2 patients develop anti-BSEP antibodies[56] This may be explained by the insufficient autotoleranceagainst BSEP exhibited in some patients with severe ABCB11mutations resulting in the complete absence of the BSEPproteinThe causal relationship between recurrent cholestasisin the liver grafts of PFIC2 patients and the occurrence of denovo antibodies directed against BSEP is further supportedby observations that plasmapheresis and the administrationof anti-CD20 antibodies (rituximab) may alleviate symptomsof cholestasis [54ndash57]
Interestingly posttransplant development of inhibitoryautoantibodies directed against FIC1 andMDR3 transporterswith corresponding phenotypes has not yet been docu-mented in patients with PFIC1 and PFIC3 respectively[44]
513 Progressive Familial Intrahepatic Cholestasis Type 3(PFIC3) PFIC3 (ABCB4 disease OMIM 602347) is causedby mutations in both alleles of the ABCB4MDR3 gene thatencode phospholipid transporter MDR3 expressed in thecanalicular (apical) membrane of hepatocytes [26] As wellas PFIC3 there is evidence that either biallelic or monoal-lelic ABCB4 defects may cause or predispose patients to awide spectrum of human liver diseases such as LowPhospholipid-Associated Cholelithiasis Syndrome (LPACOMIM 600803) Intrahepatic Cholestasis of Pregnancy(ICP OMIM 147480) drug-induced liver injury transientneonatal cholestasis small duct sclerosing cholangitis andadult biliary fibrosis or cirrhosis [58ndash61] Moreover hepa-tocellular carcinoma and intrahepatic cholangiocarcinomahave been documented in patients withABCB4MDR3muta-tions [61]
Clinical and laboratory findings associated with PFIC3correspond to the other two forms of PFIC but are charac-terised by the absence of extrahepatic symptoms (except forcholelithiasis) Unlike PFIC1 and PFIC2 elevated serumGGTactivity and normal cholesterol levels are typically observedas exhibited by the MDR3 deficit [26 62]
Histopathological findings in connection with ABCB4disease are variable Syncytial (giant-cell) changes cholesta-sis portal inflammatory infiltrate and periportal ductularproliferation accompanied by various stages of fibrosis have
been observed in liver tissue Lipid crystals within bile ductsand fibroobliterative bile duct lesions can be seen Immuno-histochemistry has indicated the absence of the canalicularMDR3 protein predominantly in early onset forms howeverits use is limited compared to PFIC2 Ultrastructurally bile isdense and amorphous in PFIC3 [26 61]
Prolonged cholestasis in PFIC3 is associated with signifi-cant accumulation of copper in liver tissue andwith increasedurine copper excretion ie findings that overlap with thediagnostic criteria for Wilsonrsquos disease [63 64]
514 Progressive Familial Intrahepatic Cholestasis Type 4(PFIC4) The fourth form of PFIC (PFIC4 TJP2 deficiencyOMIM 615878) first described in 2014 [65] is clinicallysimilar to PFIC2 and caused by homozygous or compoundheterozygous mutations in the TJP2 gene located in the9q12 chromosome Tight junction protein 2 (TJP2 also zonaoccludens-2) is a cytoplasmic component of cell-cell junc-tional complexes expressed in most epithelia and creates alink between transmembrane tight junction proteins and theactin cytoskeleton Complete TJP2 deficiency is associatedwith a significant reduction in an integral tight junction pro-tein claudin-1 predominantly in the canalicular membranesof liver cells which subsequently leads to the disruption ofintercellular connections and the leakage of bile through theparacellular space into the liver parenchyma [65 66]
Patients with TJP2 deficiency display severe progressivecholestatic liver disease in early childhood which puts themat increased risk of developing hepatocellular carcinoma [67]Serum GGT activity is normal or at most slightly increasedwhile expression of the canalicular proteins BSEP andMDR3is maintained In addition to liver impairment extrahepaticfeatures have been identified in PFIC4 patients includ-ing neurological and respiratory disorders [66] A singlehomozygous missense mutation in TJP2 has been previouslydescribed as causing benign familial hypercholanemia a raredisorder of oligogenic inheritance which usually manifestsin elevated serum BS concentrations pruritus and fat mal-absorption but which does not lead to the development ofliver disease [68]
515 Progressive Familial Intrahepatic Cholestasis Type 5(PFIC5) PFIC5 (OMIM 617049) first described in 2016[69] is a cholestatic disorder caused by mutations in NR1H4a gene located at 12q231 which encodes FXR the keyregulator of BS metabolism (see above) Homozygous loss ofFXR function is associated with severe neonatal cholestasisand early onset vitamin K-independent coagulopathy whichrapidly progresses to end-stage liver disease The nonrespon-siveness of coagulopathy to vitamin K treatment is likelya direct consequence of the loss of FXR function repre-senting an important distinguishing diagnostic feature ofNR1H4-related cholestasis In addition to low (or normal)GGT activity serum levels of alpha-fetoprotein are typicallyelevated [69]
Liver biopsies have shown diffuse giant-cell transforma-tion of hepatocytes with hepatocellular cholestasis and ductu-lar proliferation Progressive fibrosis and even micronodularcirrhosis are evident at later stages BSEP is undetectable in
Canadian Journal of Gastroenterology and Hepatology 7
the apical domains of hepatocytes which is consistent withlow activity of GGT MDR3 expression on the other hand ismaintained [69]
Since FXR affects several metabolic pathways someNR1H4 variations may be associated with susceptibility tovarious human diseases NR1H4 single-nucleotide polymor-phisms seem to be correlated with differences in glucosehomeostasis gallstone formation ICP inflammatory boweldisease and several other disorders [70 71]
52 Benign Recurrent Intrahepatic Cholestasis (BRIC) BRICis a group of genetically heterogeneous autosomal recessivediseases characterised by intermittent episodes of cholesta-sis They are caused by mutations in the ATP8B1 and ABCB11genes (the same as in PFIC1 and PFIC2) and probably inat least one other as yet unidentified gene [72] Thereare two genetically characterised forms of BRIC BRIC1(Summerskill-Walshe-Tygstrup syndrome OMIM 243300)and BRIC2 (OMIM 605479) caused by partial deficiency inATP8B1 [39 73] and ABCB11 [74] respectively The diseasetypically manifests before the second decade of life but theage of the first manifestation can vary greatly The samevariability has been documented in the duration of cholestaticepisodes (several days to several months) and their intensityInfection or pregnancy may act as a triggering factor Theclinical manifestations include jaundice pruritus fatigueanorexia and steatorrhoea Increase of bilirubin and BS levelsin serum has been observed during cholestatic attacks butGGT activity and serum cholesterol levels tend to be normalAminotransferase activity is usually normal or only slightlyelevated while biochemical parameters fall within normalranges Liver biopsies performed during cholestatic attackshave demonstrated hepatocanalicular cholestasis withoutfibrosis During the asymptomatic period the histologicalpicture is completely normal Since canalicular expression ofBSEP protein in hepatocytes is mostly maintained immuno-histology is of limited significance in these cases Diagnosisof BRIC1 and BRIC2 is based on demonstrating evidence ofmutations in both alleles of the corresponding genesATP8B1and ABCB11
While mutations causing PFIC are often located in theconserved regions of the genes that encode conserved func-tional domains of the corresponding proteins mutations inBRIC only partially impact protein function and expressionHowever several cases of initially benign episodic cholestasisthat have subsequently transitioned to a persistent progres-sive form of the disease have been reported [75] Thus BRICand PFIC seem to represent two extremes of a continuousspectrum of phenotypes of the one disease
The administration of statins corticosteroids cholestyra-mine or ursodeoxycholic acid (UDCA) is usually not veryeffective in BRIC patients Improvement of pruritus andshortening of symptomatic phase has been described inBRIC patients treated with the antibiotic rifampicin a potenthuman activator of PXR [76 77] However severe hepa-totoxicity after long-term administration of rifampicin hasbeen reported in patients with cholestatic disorders [77 78]Nasobiliary drainage seems to have a prompt effect during
cholestatic episodes but the mechanism of action remainsunclear [79]
53 Intrahepatic Cholestasis of Pregnancy (ICP) ICP (OMIM147480) also known as obstetric cholestasis is characterisedby cholestasis and prurituswith onset in pregnancy usually inthe third trimester It is associated with abnormal liverfunction in the absence of other liver diseases and resolvescompletely after delivery [80 81]The incidence of ICP varieswith geographical location and ethnicity Seasonal variationsindicate higher incidence in winter months as reported insome countries and it more commonly occurs in associationwith multiple pregnancies and following in vitro fertilisationIn Europe ICP affects about 1 of all pregnancies [81] Atypical symptom is intense pruritus commonly localised inthe palms and the soles which progresses during pregnancyElevated levels of serum BS and increased liver aminotrans-ferase activity are typical laboratory findings in such casesIncreased serum bilirubin levels have been observed in asmall proportion of cases while jaundice only rarely occursin affected women [81]
ICP usually resolves soon after delivery Although thedisease is considered relatively benign for themother there isan increased rate of adverse foetal outcomes including foetaldistress foetal asphyxia stillbirth or even intrauterine deathall known complications of ICP [81 82] ICPmay also be asso-ciated with an abnormalmetabolic profile in afflictedwomenespecially higher prevalence of dyslipidaemia impaired glu-cose tolerance and maternal comorbidities eg gestationaldiabetes and preeclampsia [82 83] Administration of UDCAimproves clinical symptoms predominantly pruritus andmay even reduce the risk of premature birth [84ndash86]
Mutations in ABCB4 ABCB11 and ATP8B1 have beenidentified in some patients suffering from ICP [87ndash90]Additionally variations in NR1H4 may be implicated in ICPpossibly via downregulation of BSEP expression [71]
6 Conclusions and Perspectives
Identification of the genes involved in hereditary cholestasishas advanced our understanding of the molecular mecha-nisms behind bile formation and transport
Recently mutations in TJP2 and NR1H4 have been foundin patients with apparent BSEP deficiency normal serumGGT activity and no mutations in ABCB11 However thereare rare cases of genetic cholestasis causes of which haveyet to be identified Therefore it seems likely that other yetunidentified genes involved in secretion andor transport ofcholephiles may be responsible for FIC-like phenotypes
Current therapeutic regimens in FIC patients compriseboth nonsurgical and surgical approaches Nonsurgical ther-apy includes drugs predominantly UDCA and rifampicinand nasobiliary drainage the latter being predominantly usedin BRIC patients with intractable pruritus during long-lastingcholestatic episodes [76 77 79] However the mechanismresponsible for the instant and complete relief from pruritusis still unclear
In addition to cholestyramine phenobarbital S-adeno-sylmethionine opiate antagonists UDCA rifampicin and
8 Canadian Journal of Gastroenterology and Hepatology
serotonin antagonists and its reuptake inhibitors seem to bebeneficial in managing refractory pruritus in patients withPFIC [77 91 92] Furthermore clinical and biochemicalimprovements have been observed in BRIC patients withintractable pruritus after using the molecular adsorbentrecirculating system (MARS) and the Prometheus system anextracorporeal liver support therapy based on fractionatedplasma separation and adsorption [93]
Surgical therapies include partial biliary diversion iemechanical interruption of BS enterohepatic circulation inorder to prevent reabsorption of pruritogens (unidentifiedthus far) and their precursors which is primarily usefulin noncirrhotic children with low-GGT PFIC permanentcholestasis andor intense refractory pruritus and orthotopicLTX which is still the ultimate treatment modality for manyPFIC patients [91] However as well as the risks associatedwith these invasive procedures other serious postoperative-related complications have been reported particularly inPFIC1 patients with extradigestive symptoms which canpersist or even worsen most likely due to extrahepaticexpression of FIC1 [47]Moreover the development of steato-sis and steatohepatitis leading to progressive liver allograftfibrosis in PFIC1 patients [48] and recurrence of the PFIC2phenotype in ABCB11 deficiency may represent other seriouscomplications after LTX and for some patients may evennecessitate retransplantation [54ndash57]
Importantly because of the shortage of cadaveric donorsparental living-related LTX is often considered in PFICpatients As heterozygous conditions can cause mild-to-moderate disease expression under certain circumstancesthe use of blood relatives as donors is seen as controversial Insuch cases it is likely that the heterozygous status of the donorallograft could pose a risk of complications during the lateposttransplant period such as lithiasis or cholestasis whichcan be precipitated by infections or by drugs administeredto the patient However the results of a recent study indicatethat the PFIC heterozygote status of the organ donor does notincrease the risk of liver dysfunction [94]
The limited effectiveness of current conservative proce-dures along with the complications of invasive methods par-ticularly LTX stress the need for the development and intro-duction of new treatment options Total biliary diversionpharmacological diversion of BS and hepatocyte transplanta-tion as well as gene- and mutation-targeted pharmacothera-pies represent promising future therapeutic approaches Thelatter two methods provide the basis for personalised treat-ment strategies in FIC patients Pharmacological chaperones(eg 4-phenylbutyrate) agonists of nuclear receptors (egstatins fibrates 6-ethyl chenodeoxycholic acid) endoplasmicreticulum-associated degradation inhibitors (MG132) andseveral other mutation-specific drugs can be used to increasethe expression of functional proteins and mitigate or eveneliminate deficient phenotypes [95ndash97]
Nevertheless despite the indisputable progress in thetherapy of FIC patients the increased risks of hepatobiliarymalignancies particularly in relation to ABCB11 deficiencystill remain serious life-threatening complications Furtherstudies are required in order to elucidate the complex patho-genesis of cholestasis unlock the mechanism of cholestatic
pruritus and improve the clinical management of bothhereditary and acquired cholestatic liver diseases
Abbreviations
ABC ATP-binding cassette subfamilyABCB4 ATP-binding cassette subfamily B
member 4ABCB11 ATP-binding cassette subfamily B
member 11AIBD Autoimmune BSEP DiseaseASBT Apical sodium-dependent bile acid
transporterATP8B1 ATPase aminophospholipid transporter
class I type 8B member 1BRIC Benign Recurrent Intrahepatic CholestasisBS Bile saltsBSEP Bile salt export pumpCYP7A1 Cholesterol 7 alpha-hydroxylaseCYP27A1 Sterol-27 hydroxylaseFGF19 Fibroblast growth factor 19FGFR4 Fibroblast growth factor receptor 4FIC Familial intrahepatic cholestasisFXR Farnesoid X-activated receptorGGT rsaquo-Glutamyl transferaseHNF4120572 Hepatocyte nuclear factor 4120572IBABP Intestinal bile acid-binding proteinICP Intrahepatic cholestasis of pregnancyIR-1 Inverted repeat DNA element with 1
nucleotide spacingLPAC Low Phospholipid-Associated
Cholelithiasis SyndromeLTX Liver allograft transplantationLXR Liver X receptorMDR3 Multidrug resistance protein 3MRP Multidrug resistance-associated proteinNR1H4 Nuclear receptor subfamily 1 group H
member 4NTCP Na+-taurocholate cotransporting
polypeptidesolute carrier family 10member 1
OATP Organic anion-transporting polypeptideOMIM Electronic database Online Mendelian
Inheritance in ManTMOST Organic solute transporterPFIC Progressive Familial Intrahepatic
CholestasisPXR Pregnane X receptorRXR Retinoid X receptorSHP Small heterodimer partnerSLC22A Solute carrier family 22 (organic cation
transporter) member 1SLCO Solute carrier organic anion transporter
familyTJP2 Tight junction protein 2 zona occludens-2UDCA Ursodeoxycholic acidUGT2B4 Uridine
51015840-diphosphate-glucuronosyltransferase2B4
Canadian Journal of Gastroenterology and Hepatology 9
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
Milan Jirsa was supported by Ministry of Health CzechRepublicmdashConceptual Development of Research Organiza-tion (ldquoInstitute for Clinical and Experimental MedicinendashIKEM IN 00023001rdquo)
References
[1] N B Javitt ldquoBile acid synthesis from cholesterol regulatory andauxiliary pathwaysrdquoThe FASEB Journal vol 8 no 15 pp 1308ndash1311 1994
[2] J Y L Chiang ldquoBile acids regulation of synthesisrdquo Journal ofLipid Research vol 50 no 10 pp 1955ndash1966 2009
[3] J L Boyer ldquoBile formation and secretionrdquo ComprehensivePhysiology vol 3 no 3 pp 1035ndash1078 2013
[4] B Hagenbuch and P J Meier ldquoSinusoidal (basolateral) bile saltuptake systems of hepatocytesrdquo Seminars in Liver Disease vol16 no 2 pp 129ndash136 1996
[5] B Hagenbuch B Stieger M Foguet H Lubbert and P JMeier ldquoFunctional expression cloning and characterization ofthe hepatocyte Na+bile acid cotransport systemrdquo Proceedingsof the National Acadamy of Sciences of the United States ofAmerica vol 88 no 23 pp 10629ndash10633 1991
[6] F M Vaz C C Paulusma H Huidekoper et al ldquoSodiumtaurocholate cotransporting polypeptide (SLC10A1) deficiencyConjugated hypercholanemia without a clear clinical pheno-typerdquo Hepatology vol 61 no 1 pp 260ndash267 2015
[7] B Hagenbuch and P J Meier ldquoOrganic anion transportingpolypeptides of the OATPSLC21 family Phylogenetic classi-fication as OATPSLCO super-family new nomenclature andmolecularfunctional propertiesrdquo Pflugers Archiv - EuropeanJournal of Physiology vol 447 no 5 pp 653ndash665 2004
[8] B Hagenbuch and B Stieger ldquoThe SLCO (former SLC21)superfamily of transportersrdquoMolecular Aspects of Medicine vol34 no 2-3 pp 396ndash412 2013
[9] M Muller and P L M Jansen ldquoThe secretory function ofthe liver New aspects of hepatobiliary transportrdquo Journal ofHepatology vol 28 no 2 pp 344ndash354 1998
[10] G J E J Hooiveld J E Van Montfoort D K F Meijerand M Muller ldquoFunction and regulation of ATP-bindingcassette transport proteins involved in hepatobiliary transportrdquoEuropean Journal of Pharmaceutical Sciences vol 12 no 4 pp525ndash543 2001
[11] J Konig D Rost Y Cui and D Keppler ldquoCharacterizationof the human multidrug resistance protein isoform MRP3localized to the basolateral hepatocyte membranerdquoHepatologyvol 29 no 4 pp 1156ndash1163 1999
[12] H Zeng G Liu P A Rea and G D Kruh ldquoTransport ofamphipathic anions by human multidrug resistance protein 3rdquoCancer Research vol 60 pp 4779ndash4784 2000
[13] Y-M A Lee Y Cui J Konig et al ldquoIdentification and func-tional characterization of the natural variantMRP3-Arg1297Hisof human multidrug resistance protein 3 (MRP3ABCC3)rdquoPharmacogenetics vol 14 no 4 pp 213ndash223 2004
[14] M Donner ldquoUp-regulation of basolateral multidrug resistanceprotein 3 (Mrp3) in cholestatic rat liverrdquoHepatology vol 34 no2 pp 351ndash359 2001
[15] M L Ruiz J P Rigalli A Arias et al ldquoInduction of hepaticmultidrug resistance-associated protein 3 by ethynylestradiol isindependent of cholestasis and mediated by estrogen receptorrdquoDrug Metabolism and Disposition vol 41 no 2 pp 275ndash2802013
[16] N J Cherrington D P Hartley N Li D R Johnson and C DKlaassen ldquoOrgan distribution of multidrug resistance proteins1 2 and 3 (Mrp1 2 and 3) mRNA and hepatic induction ofMrp3 by constitutive androstane receptor activators in ratsrdquoTheJournal of Pharmacology and Experimental Therapeutics vol300 no 1 pp 97ndash104 2002
[17] C A Ritter G Jedlitschky H Meyer Zu Schwabedissen MGrube K Kock and H K Kroemer ldquoCellular export ofdrugs and signaling molecules by the ATP-binding cassettetransporters MRP4 (ABCC4) and MRP5 (ABCC5)rdquo DrugMetabolism Reviews vol 37 no 1 pp 253ndash278 2005
[18] F G M Russel J B Koenderink and R Masereeuw ldquoMul-tidrug resistance protein 4 (MRP4ABCC4) a versatile effluxtransporter for drugs and signalling moleculesrdquo Trends inPharmacological Sciences vol 29 no 4 pp 200ndash207 2008
[19] D Keppler ldquoProgress in the molecular characterization ofhepatobiliary transportersrdquoDigestive Diseases vol 35 no 3 pp197ndash202 2017
[20] V Keitel M Burdelski U Warskulat et al ldquoExpression andlocalization of hepatobiliary transport proteins in progressivefamilial intrahepatic cholestasisrdquo Hepatology vol 41 no 5 pp1160ndash1172 2005
[21] N Ballatori F FangWV Christian N Li andC LHammondldquoOst120572-Ost120573 is required for bile acid and conjugated steroiddisposition in the intestine kidney and liverrdquoAmerican Journalof Physiology-Gastrointestinal and Liver Physiology vol 295 no1 pp G179ndashG186 2008
[22] J L Boyer M Trauner A Mennone et al ldquoUpregulationof a basolateral FXR-dependent bile acid efflux transporterOSTalpha-OSTbeta in cholestasis in humans and rodentsrdquoAmerican Journal of Physiology-Gastrointestinal and Liver Phys-iology vol 290 no 6 pp G1124ndashG1130 2006
[23] T Gerloff B Stieger B Hagenbuch et al ldquoThe sister of P-glycoprotein represents the canalicular bile salt export pump ofmammalian liverrdquoThe Journal of Biological Chemistry vol 273no 16 pp 10046ndash10050 1998
[24] A M van der Bliek F Baas T Ten Houte de Lange P MKooiman T van der Velde-Koerts and P Borst ldquoThe humanmdr3 gene encodes a novel P-glycoprotein homologue and givesrise to alternatively splicedmRNAs in liverrdquo EMBO Journal vol6 no 11 pp 3325ndash3331 1987
[25] A J Smith J L Timmermans-Hereijgers and B RoelofsenldquoThe human MDR3 P-glycoprotein promotes translocation ofphosphatidylcholine through the plasma membrane of fibrob-lasts from transgenic micerdquo FEBS Letters vol 354 no 3 pp263ndash266 1994
[26] J M L de Vree E Jacquemin E Sturm et al ldquoMutations in theMDR3 gene cause progressive familial intrahepatic cholestasisrdquoProceedings of the National Acadamy of Sciences of the UnitedStates of America vol 95 no 1 pp 282ndash287 1998
[27] A Groen M R Romero C Kunne et al ldquoComplementaryfunctions of the flippase ATP8B1 and the floppase ABCB4 inmaintaining canalicular membrane integrityrdquoGastroenterologyvol 141 no 5 pp 1927ndash1937 2011
10 Canadian Journal of Gastroenterology and Hepatology
[28] P A Dawson T Lan and A Rao ldquoThematic review series Bileacids Bile acid transportersrdquo Journal of Lipid Research vol 50no 12 pp 2340ndash2357 2009
[29] E Halilbasic T Claudel andM Trauner ldquoBile acid transportersand regulatory nuclear receptors in the liver and beyondrdquoJournal of Hepatology vol 58 no 1 pp 155ndash168 2013
[30] B L Shneider ldquoIntestinal bile acid transport Biology physiol-ogy and pathophysiologyrdquo Journal of Pediatric Gastroenterologyand Nutrition vol 32 no 4 pp 407ndash417 2001
[31] T Claudel G Zollner M Wagner and M Trauner ldquoRoleof nuclear receptors for bile acid metabolism bile secretioncholestasis and gallstone diseaserdquoBiochimica et Biophysica Acta(BBA) - Molecular Basis of Disease vol 1812 no 8 pp 867ndash8782011
[32] J J Eloranta and G A Kullak-Ublick ldquoThe role of FXR indisorders of bile acid homeostasisrdquo Physiology Journal vol 23no 5 pp 286ndash295 2008
[33] B Goodwin S A Jones R R Price et al ldquoA regulatory cascadeof the nuclear receptors FXR SHP-1 and LRH-1 represses bileacid biosynthesisrdquo Molecular Cell vol 6 no 3 pp 517ndash5262000
[34] M Muller P L M Jansen K N Faber et al ldquoFarnesoid Xreceptor and bile salts are involved in transcriptional regulationof the gene encoding the human bile salt export pumprdquoHepatology vol 35 no 3 pp 589ndash596 2002
[35] M Ananthanarayanan N BalasubramanianMMakishima DJ Mangelsdorf and F J Suchy ldquoHuman bile salt export pumppromoter is transactivated by the farnesoid X receptorbile acidreceptorrdquo The Journal of Biological Chemistry vol 276 no 31pp 28857ndash28865 2001
[36] L Huang A Zhao J L Lew et al ldquoFarnesoid X receptoractivates transcription of the phospholipid pump MDR3rdquo TheJournal of Biological Chemistry vol 278 no 51 pp 51085ndash510902003
[37] M Wagner G Zollner and M Trauner ldquoNuclear receptorregulation of the adaptive response of bile acid transporters incholestasisrdquo Seminars in Liver Disease vol 30 no 2 pp 160ndash1772010
[38] Y Zhang H R Kast-Woelbern and P A Edwards ldquoNaturalstructural variants of the nuclear receptor farnesoid X recep-tor affect transcriptional activationrdquo The Journal of BiologicalChemistry vol 278 no 1 pp 104ndash110 2003
[39] SW C VanMil R H J Houwen and LW J Klomp ldquoGeneticsof familial intrahepatic cholestasis syndromesrdquo Journal of Med-ical Genetics vol 42 no 6 pp 449ndash463 2005
[40] V E H Carlton L Pawlikowska and L N Bull ldquoMolecularbasis of intrahepatic cholestasisrdquoAnnals ofMedicine vol 36 no8 pp 606ndash617 2004
[41] R J Clayton F L Iber B H Ruebner and V A MckusickldquoByler Disease Fatal Familial Intrahepatic Cholestasis in anAmish Kindredrdquo American Journal of Diseases of Children vol117 no 1 pp 112ndash124 1969
[42] E Jacquemin ldquoProgressive familial intrahepatic cholestasisrdquoClinics andResearch inHepatology andGastroenterology vol 36supplement 1 pp S26ndashS35 2012
[43] L N Bull M J T Van Eijk L Pawlikowska et al ldquoA geneencoding a P-type ATPase mutated in two forms of hereditarycholestasisrdquo Nature Genetics vol 18 no 3 pp 219ndash224 1998
[44] L W J Klomp J C Vargas S W C Van Mil et al ldquoCharac-terization of mutations in ATP8B1 associated with hereditarycholestasisrdquo Hepatology vol 40 no 1 pp 27ndash38 2004
[45] P Ujhazy D Ortiz S Misra et al ldquoFamilial intrahepaticcholestasis 1 Studies of localization and functionrdquo Hepatologyvol 34 no 4 I pp 768ndash775 2001
[46] C C Paulusma A Groen C Kunne et al ldquoAtp8b1 deficiencyin mice reduces resistance of the canalicular membrane tohydrophobic bile salts and impairs bile salt transportrdquo Hepatol-ogy vol 44 no 1 pp 195ndash204 2006
[47] SW C VanMil LW J Klomp L N Bull and RH J HouwenldquoFIC1 disease A spectrumof intrahepatic cholestatic disordersrdquoSeminars in Liver Disease vol 21 no 4 pp 535ndash544 2001
[48] A Miyahawa-Hayashino H Egawa T Yorifuji et al ldquoAllograftsteatohepatitis in progressive familial intrahepatic cholestasistype 1 after living donor liver transplantationrdquo Liver Transplan-tation vol 15 no 6 pp 610ndash618 2009
[49] E Nicastro X Stephenne F Smets et al ldquoRecovery of graftsteatosis and protein-losing enteropathy after biliary diversionin a PFIC 1 liver transplanted childrdquo Pediatric Transplantationvol 16 no 5 pp E177ndashE182 2012
[50] K Evason K E Bove M J Finegold et al ldquoMorphologic find-ings in progressive familial intrahepatic cholestasis 2 (PFIC2)Correlation with genetic and immunohistochemical studiesrdquoThe American Journal of Surgical Pathology vol 35 no 5 pp687ndash696 2011
[51] S S Strautnieks L N Bull A S Knisely et al ldquoA gene encodinga liver-specific ABC transporter is mutated in progressivefamilial intrahepatic cholestasisrdquo Nature Genetics vol 20 no3 pp 233ndash238 1998
[52] A S Knisely S S Strautnieks Y Meier et al ldquoHepatocellularcarcinoma in ten children under five years of age with bile saltexport pumpdeficiencyrdquoHepatology vol 44 no 2 pp 478ndash4862006
[53] A O Scheimann S S Strautnieks A S Knisely J A Byrne RJ Thompson andM J Finegold ldquoMutations in Bile Salt ExportPump (ABCB11) in Two Children with Progressive FamilialIntrahepatic Cholestasis and Cholangiocarcinomardquo Journal ofPediatrics vol 150 no 5 pp 556ndash559 2007
[54] V Keitel M Burdelski Z Vojnisek L Schmitt D HaussingerandRKubitz ldquoDe novo bile salt transporter antibodies as a pos-sible cause of recurrent graft failure after liver transplantationA novel mechanism of cholestasisrdquo Hepatology vol 50 no 2pp 510ndash517 2009
[55] P Jara L Hierro P Martınez-Fernandez et al ldquoRecurrence ofbile salt export pump deficiency after liver transplantationrdquoTheNew England Journal of Medicine vol 361 no 14 pp 1359ndash13672009
[56] R Kubitz C Droge S Kluge et al ldquoAutoimmune BSEPDiseaseDisease Recurrence After Liver Transplantation for ProgressiveFamilial Intrahepatic Cholestasisrdquo Clinical Reviews in Allergy ampImmunology vol 48 no 2-3 pp 273ndash284 2015
[57] J Stindt S Kluge C Droge et al ldquoBile salt export pump-reactive antibodies form a polyclonal multi-inhibitoryresponse in antibody-induced bile salt export pump deficiencyrdquoHepatology vol 63 no 2 pp 524ndash537 2016
[58] E Jacquemin J M DeVree D Cresteil et al ldquoThe widespectrum of multidrug resistance 3 deficiency from neonatalcholestasis to cirrhosis of adulthoodrdquoGastroenterology vol 120no 6 pp 1448ndash1458 2001
[59] O Rosmorduc and R Poupon ldquoLow phospholipid associatedcholelithiasis association with mutation in the MDR3ABCB4generdquo Orphanet Journal of Rare Diseases vol 2 article 29 2007
Canadian Journal of Gastroenterology and Hepatology 11
[60] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoThe spectrum of liver diseases related to ABCB4 gene muta-tions Pathophysiology and clinical aspectsrdquo Seminars in LiverDisease vol 30 no 2 pp 134ndash146 2010
[61] DWendumV BarbuO Rosmorduc L Arrive J-F Flejou andR Poupon ldquoAspects of liver pathology in adult patients withMDR3ABCB4 gene mutationsrdquo Virchows Archiv vol 460 no3 pp 291ndash298 2012
[62] R P J Oude Elferink andC C Paulusma ldquoFunction and patho-physiological importance of ABCB4 (MDR3 P-glycoprotein)rdquoPflugers Archiv - European Journal of Physiology vol 453 no 5pp 601ndash610 2007
[63] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoProgressive familial intrahepatic cholestasisrdquo Clinical Pedi-atrics vol 51 pp 689ndash691 2012
[64] S Boga D Jain andM L Schilsky ldquoPresentation of progressivefamilial intrahepatic cholestasis type 3 mimicking wilson dis-ease molecular genetic diagnosis and response to treatmentrdquoPediatric Gastroenterology Hepatology amp Nutrition vol 18 no3 p 202 2015
[65] M Sambrotta S Strautnieks E Papouli et al ldquoMutationsin TJP2 cause progressive cholestatic liver diseaserdquo NatureGenetics vol 46 no 4 pp 326ndash328 2014
[66] M Sambrotta and R J Thompson ldquoMutations in TJP2 encod-ing zona occludens 2 and liver diseaserdquo Tissue Barriers vol 3no 3 Article ID e1026537 2015
[67] S Zhou P M Hertel M J Finegold et al ldquoHepatocellularcarcinoma associated with tight-junction protein 2 deficiencyrdquoHepatology vol 62 no 6 pp 1914ndash1916 2015
[68] V EH Carlton B ZHarris E G Puffenberger et al ldquoComplexinheritance of familial hypercholanemia with associated muta-tions in TJP2 and BAATrdquo Nature Genetics vol 34 no 1 pp 91ndash96 2003
[69] N Gomez-Ospina C J Potter R Xiao et al ldquoMutations inthe nuclear bile acid receptor FXR cause progressive familialintrahepatic cholestasisrdquoNature Communications vol 7 ArticleID 10713 2016
[70] I Koutsounas S Theocharis I Delladetsima E Patsouris andC Giaginis ldquoFarnesoid x receptor in human metabolism anddisease the interplay between gene polymorphisms clinicalphenotypes and disease susceptibilityrdquo Expert Opinion on DrugMetabolism amp Toxicology vol 11 no 4 pp 523ndash532 2015
[71] S W C van Mil A Milona P H Dixon et al ldquoFunctionalVariants of the Central Bile Acid Sensor FXR Identified inIntrahepatic Cholestasis of Pregnancyrdquo Gastroenterology vol133 no 2 pp 507ndash516 2007
[72] C Droge M Bonus U Baumann et al ldquoSequencing of FIC1BSEP and MDR3 in a large cohort of patients with cholestasisrevealed a high number of different genetic variantsrdquo Journal ofHepatology vol 67 no 6 pp 1253ndash1264 2017
[73] L N Bull V E H Carlton N L Stricker et al ldquoGeneticand morphological findings in progressive familial intrahepaticcholestasis (Byler disease [PFIC-1] and Byler syndrome) Evi-dence for heterogeneityrdquo Hepatology vol 26 no 1 pp 155ndash1641997
[74] S W C Van Mil W L Van Der Woerd G Van Der Brugge etal ldquoBenign recurrent intrahepatic cholestasis type 2 is causedby mutations in ABCB11rdquo Gastroenterology vol 127 no 2 pp379ndash384 2004
[75] N A M Van Ooteghem L W J Klomp G P Van Berge-Henegouwen andRH JHouwen ldquoBenign recurrent intrahep-atic cholestasis progressing to progressive familial intrahepatic
cholestasis Low GGT cholestasis is a clinical continuumrdquoJournal of Hepatology vol 36 no 3 pp 439ndash443 2002
[76] F Balsells R Wyllie R Steffen and M Kay ldquoBenign recurrentintrahepatic cholestasis Improvement of pruritus and shorten-ing of the symptomatic phase with rifampin therapy A casereportrdquo Clinical Pediatrics vol 36 no 8 pp 483ndash485 1997
[77] U Beuers M Trauner P Jansen and R Poupon ldquoNewparadigms in the treatment of hepatic cholestasis FromUDCAto FXR PXR and beyondrdquo Journal of Hepatology vol 62 no 1pp S25ndashS37 2015
[78] L Bachs A Pares M Elena C Piera and J Rodes ldquoEffectsof long-term rifampicin administration in primary biliarycirrhosisrdquoGastroenterology vol 102 no 6 pp 2077ndash2080 1992
[79] J M Stapelbroek K J Van Erpecum L W J Klomp et alldquoNasobiliary drainage induces long-lasting remission in benignrecurrent intrahepatic cholestasisrdquoHepatology vol 43 no 1 pp51ndash53 2006
[80] F Lammert H-U Marschall A Glantz and S MaternldquoIntrahepatic cholestasis of pregnancymolecular pathogenesisdiagnosis and managementrdquo Journal of Hepatology vol 33 no6 pp 1012ndash1021 2000
[81] P H Dixon and C Williamson ldquoThe pathophysiology ofintrahepatic cholestasis of pregnancyrdquo Clinics and Research inHepatology and Gastroenterology vol 40 no 2 pp 141ndash1532016
[82] M G Martineau C Raker P H Dixon et al ldquoThe metabolicprofile of intrahepatic cholestasis of pregnancy is associatedwith impaired glucose tolerance dyslipidemia and increasedfetal growthrdquo Diabetes Care vol 38 no 2 pp 243ndash248 2015
[83] D G Goulis I A LWalkerMDe Swiet CWG Redman andC Williamson ldquoPreeclampsia with Abnormal Liver FunctionTests Is Associated with Cholestasis in a Subgroup of CasesrdquoHypertension in Pregnancy vol 23 no 1 pp 19ndash27 2004
[84] A Glantz H-U Marschall F Lammert and L-A MattssonldquoIntrahepatic cholestasis of pregnancy A randomized con-trolled trial comparing dexamethasone and ursodeoxycholicacidrdquo Hepatology vol 42 no 6 pp 1399ndash1405 2005
[85] R Zapata L Sandoval J Palma et al ldquoUrsodeoxycholic acidin the treatment of intrahepatic cholestasis of pregnancy A 12-year experiencerdquo Liver International vol 25 no 3 pp 548ndash5542005
[86] T Binder P Salaj T Zima and L Vıtek ldquoRandomized prospec-tive comparative study of ursodeoxycholic acid and S-adenosyl-L-methionine in the treatment of intrahepatic cholestasis ofpregnancyrdquo Journal of PerinatalMedicine vol 34 no 5 pp 383ndash391 2006
[87] P H Dixon N Weerasekera K J Linton et al ldquoHeterozy-gous MDR3 missense mutation associated with intrahepaticcholestasis of pregnancy Evidence for a defect in proteintraffickingrdquo Human Molecular Genetics vol 9 no 8 pp 1209ndash1217 2000
[88] C Gendrot Y Bacq M-C Brechot J Lansac and C AndresldquoA second heterozygous MDR3 nonsense mutation associatedwith intrahepatic cholestasis of pregnancyrdquo Journal of MedicalGenetics vol 40 no 3 article e32 2003
[89] A Floreani I Carderi D Paternoster et al ldquoIntrahepaticcholestasis of pregnancy Three novel MDR3 gene mutationsrdquoAlimentary Pharmacology amp Therapeutics vol 23 no 11 pp1649ndash1653 2006
[90] J N Painter M Savander A Ropponen et al ldquoSequencevariation in the ATP8B1 gene and intrahepatic cholestasis of
12 Canadian Journal of Gastroenterology and Hepatology
pregnancyrdquo European Journal of Human Genetics vol 13 no 4pp 435ndash439 2005
[91] W L Van Der Woerd R H J Houwen and S F J Van DeGraaf ldquoCurrent and future therapies for inherited cholestaticliver diseasesrdquoWorld Journal of Gastroenterology vol 23 no 5pp 763ndash775 2017
[92] A Thebaut D Habes F Gottrand et al ldquoSertraline as an addi-tional treatment for cholestatic pruritus in childrenrdquo Journal ofPediatric Gastroenterology and Nutrition vol 64 no 3 pp 431ndash435 2017
[93] U Ołdakowska-Jedynak I JankowskaM Hartleb et al ldquoTreat-ment of pruritus with Prometheus dialysis and absorption sys-tem in a patient with benign recurrent intrahepatic cholestasisrdquoHepatology Research vol 44 no 10 pp E304ndashE308 2014
[94] L Cutillo M Najimi F Smets et al ldquoSafety of living-related liver transplantation for progressive familial intrahep-atic cholestasisrdquo Pediatric Transplantation vol 10 no 5 pp570ndash574 2006
[95] E Gonzales B Grosse B Schuller et al ldquoTargeted phar-macotherapy in progressive familial intrahepatic cholestasistype 2 Evidence for improvement of cholestasis with 4-phenylbutyraterdquo Hepatology vol 62 no 2 pp 558ndash566 2015
[96] E Gonzales and E Jacquemin ldquoMutation specific drug ther-apy for progressive familial or benign recurrent intrahepaticcholestasis A new tool in a near futurerdquo Journal of Hepatologyvol 53 no 2 pp 385ndash387 2010
[97] M Trauner C D Fuchs E Halilbasic and G PaumgartnerldquoNew therapeutic concepts in bile acid transport and signalingfor management of cholestasisrdquo Hepatology vol 65 no 4 pp1393ndash1404 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

4 Canadian Journal of Gastroenterology and Hepatology
partner (SHP the NR0B2 gene) SHP is an atypical orphannuclear receptor without a DNA-binding domain It acts asa repressor of nuclear receptors as well as of transcriptionfactors belonging to other protein families [2 31 33]
FXR plays a key role in controlling the enterohepaticcirculation of BS largely by directly regulating the expressionof several hepatobiliary transporters (Figure 1) In the liverthe heterodimer FXR-RXR induces the expression of BSEPby binding to an IR-1 element at the promoter [34 35]Likewise FXR can directly transactivate the ABCC2 ABCB4and SLCO1B3 genes [36 37]
The FXR-RXR complex directly induces the expressionof OST120572-OST120573 (in ileal enterocytes and in the basolateralmembrane of hepatocytes) as well as intestinal expression ofthe intestinal bile acid-binding protein (IBABP) [22 37]
In addition to directly activating the main BS effluxsystems under cholestatic conditions FXR concurrentlydownregulates the main BS uptake systems primarily NTCPin the basolateral membrane of hepatocytes and ASBT inthe ileal epithelium OATP1B1 is also suppressed by anFXR-dependent pathway during cholestasis FXR-mediatedrepression of target genes is indirect and mainly effected viaSHP [2 33 37]
As well as regulating transport systems involved in theenterohepatic flow of BS FXR represses the transcription ofgenes that encode regulatory enzymes in both classical andalternative BS biosynthetic pathways predominantlyCYP7A1and CYP27A1 [2 33]
There are two important FXR-dependent mechanismsfor BS-induced inhibition of CYP7A1 gene transcription theFXRSHP pathway in the liver and the FXRFGF19FGFR4pathway in the intestine [2 37]
In the liver the heterodimer FXRRXR after bindingretinoic acid andBS induces the expression of SHPThe inter-action of SHP with liver receptor homologue-1 (LRH-1 alsoNR5A2 gene NR5A2) and hepatocyte nuclear factor-4120572(HNF4120572 also NR2A1 gene HNF4A) inhibits CYP7A1 tran-scription [2 32 33] In the CYP27A1 gene the BS responseelement contains a DNA-binding site for HNF4120572 only notfor LRH-1 [2 31]
In the intestine FXR induces an intestinal hormonefibroblast growth factor 19 (FGF19 gene FGF19) whichactivates hepatic FGF receptor 4 (FGFR4 gene FGFR4) anddownregulates BS synthesis by inhibitingCYP71A expressionThe FXRFGF19FGFR4 pathway seems to be the physiolog-ical mechanism for feedback regulation of BS biosynthesisFurthermore the FGF19 autocrine pathway exists in thehuman liver [2 31 37 38]
Along with FXR-related regulation of BS biosynthesisthere are several FXR-independent mechanisms of CYP7A1inhibition mediated by pregnane X receptor (PXR) vitaminD receptor (VDR) the cytokines tumour necrosis factor120572 (TNF120572) and interleukin 1120573 (IL-1120573) transforming growthfactor 1205731 (TGF1205731) epidermal growth factor receptor (EGFR)and others These factors activate signalling pathways whichplay roles in protecting against BS toxicity during cholestaticliver injury [2 31 32 37]
Finally FXR also directly transactivates genes encod-ing enzymes that metabolise BS such as human uri-dine 5rsquo-diphosphate-glucuronosyltransferase 2B4 (UGT2B4encoded by UGT2B4) Interestingly FXR binds the UGT2B4promoter as amonomerwithout previous heterodimerisationwith RXR [32]
Several nuclear receptors such as FXR RXR LXR andSHP are also expressed in cholangiocytes but their role in bileduct biology remains to be elucidated [29]
5 Familial Intrahepatic Cholestasis
Up- and downregulation of transport systems involved inbile formation can explain the impaired liver uptake andexcretion of biliary constituents which result in cholestasisand jaundice in some hereditary andmany common acquiredliver disorders Hereditary diseases characterised by hepato-canalicular cholestasis which is caused by defects in hepato-biliary transporters their regulator FXR and in tightness ofthe liver epithelium include progressive familial intrahepaticcholestasis (PFIC) types 1 to 5 benign recurrent intrahepaticcholestasis (BRIC) 1 and 2 familial cholelithiasis caused by alack of biliary secretion of phospholipids (Low Phospholipid-AssociatedCholelithiasis orGallbladderDisease-1) intrahep-atic cholestasis of pregnancy (ICP) and several other raredisorders Hereditary predisposition also plays an impor-tant role in drug-induced intrahepatic cholestasis includingcholestasis induced by hormonal contraceptives [39 40]
51 Progressive Familial Intrahepatic Cholestasis PFIC firstdescribed in 1969 [41] is a genetically heterogeneous group ofautosomal recessive disorders caused by mutations in genesthat encode hepatocanalicular transporters of BS and phos-pholipids their regulator FXR andTJP2which is essential fortightness of cell junctions between the epithelial cells liningthe bile ducts The exact incidence of PFIC is not knownbut it is estimated to be in the region of 150000 to 1100000births Both genders are equally affected [42] Clinically PFICusuallymanifests in the first year of life and is characterised byjaundice severe pruritus hepatosplenomegaly steatorrhoeaand retardation of growth and mental development Furthersymptoms caused by a deficit of fat-soluble vitamins includecoagulopathy osteopaenia and neuromuscular disordersWithout adequate treatment the disease progresses to liverfibrosis and cirrhosis and usually ends in death due to liverfailure in the first or more rarely in the second decade of life[40 42]
The PFIC group consists of five representatives (PFIC 1-5) which are classified into two main categories according tolevels of serum rsaquo-glutamyl transferase (GGT) activity GGTis considered a cholestatic enzyme and when elevated isassociated with damage to the apical membranes of bile ductsand the disruption of intercellular connections due to highconcentrations of BS in bile However in some cholestaticdiseases synthesis or canalicular secretion of BS is virtuallyabsent and there are no conditions that predispose eitherto the release of membrane GGT from damaged cholan-giocytes or to leakage of bile into the extracellular spaceand subsequently the blood This explains why in hereditary
Canadian Journal of Gastroenterology and Hepatology 5
(a) (b)
Figure 2 Histopathology of ABCB11 disease (a) Giant-cell hepatitis (arrows) with hepatocanalicular cholestasis and (b) complete absenceof ABCB11BSEP protein are typical findings in PFIC2 patients Inset immunohistochemical positivity of BSEP in the apical (canalicular)domain of hepatocytes in a healthy control (a) Hematoxylin and eosin original magnification x200 (b inset) Immunohistochemical stainingwith ABCB11 Rabbit Polyclonal Antibody (NBP1-89319 Novus Biologicals USA) original magnification x200 (b) x400 (inset)
cholestasis GGT activity is increased only in disorders ofphospholipid secretion (PFIC3)
511 Progressive Familial Intrahepatic Cholestasis Type 1(PFIC1) PFIC1 (ATP8B1 disease OMIM 211600) formerlyBylerrsquos disease [41] is the consequence of a severe defect in thegene encoding ATPase ATP8B1FIC1 (familial intrahepaticcholestasis 1) localised in the long arm of the 18th chro-mosome (18q21) [43 44] ATP8B1 deficiency which causesmembrane phospholipid asymmetry of the canalicular mem-brane reduces the capacity of the liver to secrete bile [45 46]In addition to the previously described common symptomsof PFIC clinical manifestation of PFIC1 also includes awide range of extrahepatic symptoms Extrahepatic mani-festations of ATP8B1 disease include elevated sweat chlorideconcentrations delayed pubescence and growth and waterydiarrhoea as well as impaired hearing andor pancreatitis[47] These symptoms often persist while diarrhoea eventends to worsen after liver transplantation (LTX) Liverallografts in PFIC1 patients may display diffuse steatosis witha variable necroinflammatory component with subsequentfibrosis [48] Both diarrhoea and steatosissteatohepatitismay improve after biliary diversion [49]
Laboratory findings with regard to PFIC1 have reportedcholestasis with low serum levels of GGT increased serumconcentrations of primary BS and normal levels of choles-terol Aminotransferases are initially within the referencerange but during disease progression they gradually increaseby up to tenfold [41] Histopathological changes predomi-nantly involve canalicular cholestasis accentuated around thecentral veins The interlobular ducts can be hypoplastic dueto subnormal bile flow Giant-cell changes of hepatocytes aregenerally not observed in biopsies Liver fibrosis progressioncorresponds with the respective stage of the disease and canterminate in cirrhosis A typical ultrastructural finding isthe presence of Byler-type coarsely granular bile in the bilecanaliculi [50] Molecular diagnosis is based on the detectionof pathogenic mutations in both alleles of the ATP8B1 gene
The milder intermittent nonprogressive form of ATP8B1deficiency is called BRIC1 (see below)
512 Progressive Familial Intrahepatic Cholestasis Type 2(PFIC2) PFIC2 (ABCB11 disease OMIM 601847) is causedby mutations in ABCB11 which is located on the longarm of the second chromosome (2q24) and encodes thecanalicular transport proteinABCB11BSEP [51] Clinical andlaboratory findings with regard to PFIC2 are similar to PFIC1but extrahepatic symptoms are not present Additionally inPFIC2 the formation of gallstones and the early elevation ofserum aminotransferase activity can occurThe developmentof hepatobiliarymalignancies both hepatocellular carcinomaand cholangiocarcinoma can be a serious complication ofPFIC2 which is not observed in PFIC1 [52 53] Screening forliver tumours is recommended from the first year of life inPFIC2 patients
Except for PFIC2 mutations in ABCB11 may result in amilder nonprogressive formof PFIC2 known asBRIC2 aswellas other forms of cholestasis such as ICP andor drug-inducedcholestasis (see below)
Histologically the typical findings in the liver biopsies ofPFIC2 patients are giant-cell (syncycial) hepatitis with hepa-tocanalicular cholestasis while extramedullary haemopoiesisis frequently discernible within lobules Interlobular bileducts can be hypoplastic and ductular proliferation at theperipheries of portal triads is commonly observed TheABCB11BSEP protein is usually undetectable immunohis-tochemically (Figure 2) Ultrastructurally canalicular bilecan be either amorphous or filamentous but is not coarselygranular [51]
Untreated PFIC2 usually leads to progressive liver fibrosisand cirrhosis the development of which ismore rapid than inPFIC1 One curative method for patients with PFIC2 is LTXUnlike in PFIC1 steatosis and steatohepatitis are not presentin liver allografts in the case of PFIC2 However in somepatients a recurrence of the PFIC2 phenotype accompaniedby elevated serum levels of BS and bilirubin with almost
6 Canadian Journal of Gastroenterology and Hepatology
normal GGT activity has been observed after LTX [54 55] Ithas been shown that canalicular immunostaining of the BSEPMDR3 and MRP2 proteins is preserved in the liver graftbiopsies and no discernible changes in BSEP immunoreactiv-ity distribution between the apical membrane and the cyto-plasm have been reported nonetheless de novo polyclonalinhibitory antibodies directed against the first extracellularloop of BSEP have been observed in the posttransplant serumof patients a condition known as Autoimmune BSEPDisease(AIBD) [56 57] The exact mechanism by which BS trans-port is inhibited by anti-BSEP antibodies is still unknownIt is supposed that the cross-linking of BSEP moleculeswhich in turn disrupts the structure and function ofcanalicular membranes andor the direct mechanical occlu-sion of the BSEP pore might explain the inhibitory effectsof the antibodies [56 57] It is estimated that up to 8 oftransplanted PFIC2 patients develop anti-BSEP antibodies[56] This may be explained by the insufficient autotoleranceagainst BSEP exhibited in some patients with severe ABCB11mutations resulting in the complete absence of the BSEPproteinThe causal relationship between recurrent cholestasisin the liver grafts of PFIC2 patients and the occurrence of denovo antibodies directed against BSEP is further supportedby observations that plasmapheresis and the administrationof anti-CD20 antibodies (rituximab) may alleviate symptomsof cholestasis [54ndash57]
Interestingly posttransplant development of inhibitoryautoantibodies directed against FIC1 andMDR3 transporterswith corresponding phenotypes has not yet been docu-mented in patients with PFIC1 and PFIC3 respectively[44]
513 Progressive Familial Intrahepatic Cholestasis Type 3(PFIC3) PFIC3 (ABCB4 disease OMIM 602347) is causedby mutations in both alleles of the ABCB4MDR3 gene thatencode phospholipid transporter MDR3 expressed in thecanalicular (apical) membrane of hepatocytes [26] As wellas PFIC3 there is evidence that either biallelic or monoal-lelic ABCB4 defects may cause or predispose patients to awide spectrum of human liver diseases such as LowPhospholipid-Associated Cholelithiasis Syndrome (LPACOMIM 600803) Intrahepatic Cholestasis of Pregnancy(ICP OMIM 147480) drug-induced liver injury transientneonatal cholestasis small duct sclerosing cholangitis andadult biliary fibrosis or cirrhosis [58ndash61] Moreover hepa-tocellular carcinoma and intrahepatic cholangiocarcinomahave been documented in patients withABCB4MDR3muta-tions [61]
Clinical and laboratory findings associated with PFIC3correspond to the other two forms of PFIC but are charac-terised by the absence of extrahepatic symptoms (except forcholelithiasis) Unlike PFIC1 and PFIC2 elevated serumGGTactivity and normal cholesterol levels are typically observedas exhibited by the MDR3 deficit [26 62]
Histopathological findings in connection with ABCB4disease are variable Syncytial (giant-cell) changes cholesta-sis portal inflammatory infiltrate and periportal ductularproliferation accompanied by various stages of fibrosis have
been observed in liver tissue Lipid crystals within bile ductsand fibroobliterative bile duct lesions can be seen Immuno-histochemistry has indicated the absence of the canalicularMDR3 protein predominantly in early onset forms howeverits use is limited compared to PFIC2 Ultrastructurally bile isdense and amorphous in PFIC3 [26 61]
Prolonged cholestasis in PFIC3 is associated with signifi-cant accumulation of copper in liver tissue andwith increasedurine copper excretion ie findings that overlap with thediagnostic criteria for Wilsonrsquos disease [63 64]
514 Progressive Familial Intrahepatic Cholestasis Type 4(PFIC4) The fourth form of PFIC (PFIC4 TJP2 deficiencyOMIM 615878) first described in 2014 [65] is clinicallysimilar to PFIC2 and caused by homozygous or compoundheterozygous mutations in the TJP2 gene located in the9q12 chromosome Tight junction protein 2 (TJP2 also zonaoccludens-2) is a cytoplasmic component of cell-cell junc-tional complexes expressed in most epithelia and creates alink between transmembrane tight junction proteins and theactin cytoskeleton Complete TJP2 deficiency is associatedwith a significant reduction in an integral tight junction pro-tein claudin-1 predominantly in the canalicular membranesof liver cells which subsequently leads to the disruption ofintercellular connections and the leakage of bile through theparacellular space into the liver parenchyma [65 66]
Patients with TJP2 deficiency display severe progressivecholestatic liver disease in early childhood which puts themat increased risk of developing hepatocellular carcinoma [67]Serum GGT activity is normal or at most slightly increasedwhile expression of the canalicular proteins BSEP andMDR3is maintained In addition to liver impairment extrahepaticfeatures have been identified in PFIC4 patients includ-ing neurological and respiratory disorders [66] A singlehomozygous missense mutation in TJP2 has been previouslydescribed as causing benign familial hypercholanemia a raredisorder of oligogenic inheritance which usually manifestsin elevated serum BS concentrations pruritus and fat mal-absorption but which does not lead to the development ofliver disease [68]
515 Progressive Familial Intrahepatic Cholestasis Type 5(PFIC5) PFIC5 (OMIM 617049) first described in 2016[69] is a cholestatic disorder caused by mutations in NR1H4a gene located at 12q231 which encodes FXR the keyregulator of BS metabolism (see above) Homozygous loss ofFXR function is associated with severe neonatal cholestasisand early onset vitamin K-independent coagulopathy whichrapidly progresses to end-stage liver disease The nonrespon-siveness of coagulopathy to vitamin K treatment is likelya direct consequence of the loss of FXR function repre-senting an important distinguishing diagnostic feature ofNR1H4-related cholestasis In addition to low (or normal)GGT activity serum levels of alpha-fetoprotein are typicallyelevated [69]
Liver biopsies have shown diffuse giant-cell transforma-tion of hepatocytes with hepatocellular cholestasis and ductu-lar proliferation Progressive fibrosis and even micronodularcirrhosis are evident at later stages BSEP is undetectable in
Canadian Journal of Gastroenterology and Hepatology 7
the apical domains of hepatocytes which is consistent withlow activity of GGT MDR3 expression on the other hand ismaintained [69]
Since FXR affects several metabolic pathways someNR1H4 variations may be associated with susceptibility tovarious human diseases NR1H4 single-nucleotide polymor-phisms seem to be correlated with differences in glucosehomeostasis gallstone formation ICP inflammatory boweldisease and several other disorders [70 71]
52 Benign Recurrent Intrahepatic Cholestasis (BRIC) BRICis a group of genetically heterogeneous autosomal recessivediseases characterised by intermittent episodes of cholesta-sis They are caused by mutations in the ATP8B1 and ABCB11genes (the same as in PFIC1 and PFIC2) and probably inat least one other as yet unidentified gene [72] Thereare two genetically characterised forms of BRIC BRIC1(Summerskill-Walshe-Tygstrup syndrome OMIM 243300)and BRIC2 (OMIM 605479) caused by partial deficiency inATP8B1 [39 73] and ABCB11 [74] respectively The diseasetypically manifests before the second decade of life but theage of the first manifestation can vary greatly The samevariability has been documented in the duration of cholestaticepisodes (several days to several months) and their intensityInfection or pregnancy may act as a triggering factor Theclinical manifestations include jaundice pruritus fatigueanorexia and steatorrhoea Increase of bilirubin and BS levelsin serum has been observed during cholestatic attacks butGGT activity and serum cholesterol levels tend to be normalAminotransferase activity is usually normal or only slightlyelevated while biochemical parameters fall within normalranges Liver biopsies performed during cholestatic attackshave demonstrated hepatocanalicular cholestasis withoutfibrosis During the asymptomatic period the histologicalpicture is completely normal Since canalicular expression ofBSEP protein in hepatocytes is mostly maintained immuno-histology is of limited significance in these cases Diagnosisof BRIC1 and BRIC2 is based on demonstrating evidence ofmutations in both alleles of the corresponding genesATP8B1and ABCB11
While mutations causing PFIC are often located in theconserved regions of the genes that encode conserved func-tional domains of the corresponding proteins mutations inBRIC only partially impact protein function and expressionHowever several cases of initially benign episodic cholestasisthat have subsequently transitioned to a persistent progres-sive form of the disease have been reported [75] Thus BRICand PFIC seem to represent two extremes of a continuousspectrum of phenotypes of the one disease
The administration of statins corticosteroids cholestyra-mine or ursodeoxycholic acid (UDCA) is usually not veryeffective in BRIC patients Improvement of pruritus andshortening of symptomatic phase has been described inBRIC patients treated with the antibiotic rifampicin a potenthuman activator of PXR [76 77] However severe hepa-totoxicity after long-term administration of rifampicin hasbeen reported in patients with cholestatic disorders [77 78]Nasobiliary drainage seems to have a prompt effect during
cholestatic episodes but the mechanism of action remainsunclear [79]
53 Intrahepatic Cholestasis of Pregnancy (ICP) ICP (OMIM147480) also known as obstetric cholestasis is characterisedby cholestasis and prurituswith onset in pregnancy usually inthe third trimester It is associated with abnormal liverfunction in the absence of other liver diseases and resolvescompletely after delivery [80 81]The incidence of ICP varieswith geographical location and ethnicity Seasonal variationsindicate higher incidence in winter months as reported insome countries and it more commonly occurs in associationwith multiple pregnancies and following in vitro fertilisationIn Europe ICP affects about 1 of all pregnancies [81] Atypical symptom is intense pruritus commonly localised inthe palms and the soles which progresses during pregnancyElevated levels of serum BS and increased liver aminotrans-ferase activity are typical laboratory findings in such casesIncreased serum bilirubin levels have been observed in asmall proportion of cases while jaundice only rarely occursin affected women [81]
ICP usually resolves soon after delivery Although thedisease is considered relatively benign for themother there isan increased rate of adverse foetal outcomes including foetaldistress foetal asphyxia stillbirth or even intrauterine deathall known complications of ICP [81 82] ICPmay also be asso-ciated with an abnormalmetabolic profile in afflictedwomenespecially higher prevalence of dyslipidaemia impaired glu-cose tolerance and maternal comorbidities eg gestationaldiabetes and preeclampsia [82 83] Administration of UDCAimproves clinical symptoms predominantly pruritus andmay even reduce the risk of premature birth [84ndash86]
Mutations in ABCB4 ABCB11 and ATP8B1 have beenidentified in some patients suffering from ICP [87ndash90]Additionally variations in NR1H4 may be implicated in ICPpossibly via downregulation of BSEP expression [71]
6 Conclusions and Perspectives
Identification of the genes involved in hereditary cholestasishas advanced our understanding of the molecular mecha-nisms behind bile formation and transport
Recently mutations in TJP2 and NR1H4 have been foundin patients with apparent BSEP deficiency normal serumGGT activity and no mutations in ABCB11 However thereare rare cases of genetic cholestasis causes of which haveyet to be identified Therefore it seems likely that other yetunidentified genes involved in secretion andor transport ofcholephiles may be responsible for FIC-like phenotypes
Current therapeutic regimens in FIC patients compriseboth nonsurgical and surgical approaches Nonsurgical ther-apy includes drugs predominantly UDCA and rifampicinand nasobiliary drainage the latter being predominantly usedin BRIC patients with intractable pruritus during long-lastingcholestatic episodes [76 77 79] However the mechanismresponsible for the instant and complete relief from pruritusis still unclear
In addition to cholestyramine phenobarbital S-adeno-sylmethionine opiate antagonists UDCA rifampicin and
8 Canadian Journal of Gastroenterology and Hepatology
serotonin antagonists and its reuptake inhibitors seem to bebeneficial in managing refractory pruritus in patients withPFIC [77 91 92] Furthermore clinical and biochemicalimprovements have been observed in BRIC patients withintractable pruritus after using the molecular adsorbentrecirculating system (MARS) and the Prometheus system anextracorporeal liver support therapy based on fractionatedplasma separation and adsorption [93]
Surgical therapies include partial biliary diversion iemechanical interruption of BS enterohepatic circulation inorder to prevent reabsorption of pruritogens (unidentifiedthus far) and their precursors which is primarily usefulin noncirrhotic children with low-GGT PFIC permanentcholestasis andor intense refractory pruritus and orthotopicLTX which is still the ultimate treatment modality for manyPFIC patients [91] However as well as the risks associatedwith these invasive procedures other serious postoperative-related complications have been reported particularly inPFIC1 patients with extradigestive symptoms which canpersist or even worsen most likely due to extrahepaticexpression of FIC1 [47]Moreover the development of steato-sis and steatohepatitis leading to progressive liver allograftfibrosis in PFIC1 patients [48] and recurrence of the PFIC2phenotype in ABCB11 deficiency may represent other seriouscomplications after LTX and for some patients may evennecessitate retransplantation [54ndash57]
Importantly because of the shortage of cadaveric donorsparental living-related LTX is often considered in PFICpatients As heterozygous conditions can cause mild-to-moderate disease expression under certain circumstancesthe use of blood relatives as donors is seen as controversial Insuch cases it is likely that the heterozygous status of the donorallograft could pose a risk of complications during the lateposttransplant period such as lithiasis or cholestasis whichcan be precipitated by infections or by drugs administeredto the patient However the results of a recent study indicatethat the PFIC heterozygote status of the organ donor does notincrease the risk of liver dysfunction [94]
The limited effectiveness of current conservative proce-dures along with the complications of invasive methods par-ticularly LTX stress the need for the development and intro-duction of new treatment options Total biliary diversionpharmacological diversion of BS and hepatocyte transplanta-tion as well as gene- and mutation-targeted pharmacothera-pies represent promising future therapeutic approaches Thelatter two methods provide the basis for personalised treat-ment strategies in FIC patients Pharmacological chaperones(eg 4-phenylbutyrate) agonists of nuclear receptors (egstatins fibrates 6-ethyl chenodeoxycholic acid) endoplasmicreticulum-associated degradation inhibitors (MG132) andseveral other mutation-specific drugs can be used to increasethe expression of functional proteins and mitigate or eveneliminate deficient phenotypes [95ndash97]
Nevertheless despite the indisputable progress in thetherapy of FIC patients the increased risks of hepatobiliarymalignancies particularly in relation to ABCB11 deficiencystill remain serious life-threatening complications Furtherstudies are required in order to elucidate the complex patho-genesis of cholestasis unlock the mechanism of cholestatic
pruritus and improve the clinical management of bothhereditary and acquired cholestatic liver diseases
Abbreviations
ABC ATP-binding cassette subfamilyABCB4 ATP-binding cassette subfamily B
member 4ABCB11 ATP-binding cassette subfamily B
member 11AIBD Autoimmune BSEP DiseaseASBT Apical sodium-dependent bile acid
transporterATP8B1 ATPase aminophospholipid transporter
class I type 8B member 1BRIC Benign Recurrent Intrahepatic CholestasisBS Bile saltsBSEP Bile salt export pumpCYP7A1 Cholesterol 7 alpha-hydroxylaseCYP27A1 Sterol-27 hydroxylaseFGF19 Fibroblast growth factor 19FGFR4 Fibroblast growth factor receptor 4FIC Familial intrahepatic cholestasisFXR Farnesoid X-activated receptorGGT rsaquo-Glutamyl transferaseHNF4120572 Hepatocyte nuclear factor 4120572IBABP Intestinal bile acid-binding proteinICP Intrahepatic cholestasis of pregnancyIR-1 Inverted repeat DNA element with 1
nucleotide spacingLPAC Low Phospholipid-Associated
Cholelithiasis SyndromeLTX Liver allograft transplantationLXR Liver X receptorMDR3 Multidrug resistance protein 3MRP Multidrug resistance-associated proteinNR1H4 Nuclear receptor subfamily 1 group H
member 4NTCP Na+-taurocholate cotransporting
polypeptidesolute carrier family 10member 1
OATP Organic anion-transporting polypeptideOMIM Electronic database Online Mendelian
Inheritance in ManTMOST Organic solute transporterPFIC Progressive Familial Intrahepatic
CholestasisPXR Pregnane X receptorRXR Retinoid X receptorSHP Small heterodimer partnerSLC22A Solute carrier family 22 (organic cation
transporter) member 1SLCO Solute carrier organic anion transporter
familyTJP2 Tight junction protein 2 zona occludens-2UDCA Ursodeoxycholic acidUGT2B4 Uridine
51015840-diphosphate-glucuronosyltransferase2B4
Canadian Journal of Gastroenterology and Hepatology 9
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
Milan Jirsa was supported by Ministry of Health CzechRepublicmdashConceptual Development of Research Organiza-tion (ldquoInstitute for Clinical and Experimental MedicinendashIKEM IN 00023001rdquo)
References
[1] N B Javitt ldquoBile acid synthesis from cholesterol regulatory andauxiliary pathwaysrdquoThe FASEB Journal vol 8 no 15 pp 1308ndash1311 1994
[2] J Y L Chiang ldquoBile acids regulation of synthesisrdquo Journal ofLipid Research vol 50 no 10 pp 1955ndash1966 2009
[3] J L Boyer ldquoBile formation and secretionrdquo ComprehensivePhysiology vol 3 no 3 pp 1035ndash1078 2013
[4] B Hagenbuch and P J Meier ldquoSinusoidal (basolateral) bile saltuptake systems of hepatocytesrdquo Seminars in Liver Disease vol16 no 2 pp 129ndash136 1996
[5] B Hagenbuch B Stieger M Foguet H Lubbert and P JMeier ldquoFunctional expression cloning and characterization ofthe hepatocyte Na+bile acid cotransport systemrdquo Proceedingsof the National Acadamy of Sciences of the United States ofAmerica vol 88 no 23 pp 10629ndash10633 1991
[6] F M Vaz C C Paulusma H Huidekoper et al ldquoSodiumtaurocholate cotransporting polypeptide (SLC10A1) deficiencyConjugated hypercholanemia without a clear clinical pheno-typerdquo Hepatology vol 61 no 1 pp 260ndash267 2015
[7] B Hagenbuch and P J Meier ldquoOrganic anion transportingpolypeptides of the OATPSLC21 family Phylogenetic classi-fication as OATPSLCO super-family new nomenclature andmolecularfunctional propertiesrdquo Pflugers Archiv - EuropeanJournal of Physiology vol 447 no 5 pp 653ndash665 2004
[8] B Hagenbuch and B Stieger ldquoThe SLCO (former SLC21)superfamily of transportersrdquoMolecular Aspects of Medicine vol34 no 2-3 pp 396ndash412 2013
[9] M Muller and P L M Jansen ldquoThe secretory function ofthe liver New aspects of hepatobiliary transportrdquo Journal ofHepatology vol 28 no 2 pp 344ndash354 1998
[10] G J E J Hooiveld J E Van Montfoort D K F Meijerand M Muller ldquoFunction and regulation of ATP-bindingcassette transport proteins involved in hepatobiliary transportrdquoEuropean Journal of Pharmaceutical Sciences vol 12 no 4 pp525ndash543 2001
[11] J Konig D Rost Y Cui and D Keppler ldquoCharacterizationof the human multidrug resistance protein isoform MRP3localized to the basolateral hepatocyte membranerdquoHepatologyvol 29 no 4 pp 1156ndash1163 1999
[12] H Zeng G Liu P A Rea and G D Kruh ldquoTransport ofamphipathic anions by human multidrug resistance protein 3rdquoCancer Research vol 60 pp 4779ndash4784 2000
[13] Y-M A Lee Y Cui J Konig et al ldquoIdentification and func-tional characterization of the natural variantMRP3-Arg1297Hisof human multidrug resistance protein 3 (MRP3ABCC3)rdquoPharmacogenetics vol 14 no 4 pp 213ndash223 2004
[14] M Donner ldquoUp-regulation of basolateral multidrug resistanceprotein 3 (Mrp3) in cholestatic rat liverrdquoHepatology vol 34 no2 pp 351ndash359 2001
[15] M L Ruiz J P Rigalli A Arias et al ldquoInduction of hepaticmultidrug resistance-associated protein 3 by ethynylestradiol isindependent of cholestasis and mediated by estrogen receptorrdquoDrug Metabolism and Disposition vol 41 no 2 pp 275ndash2802013
[16] N J Cherrington D P Hartley N Li D R Johnson and C DKlaassen ldquoOrgan distribution of multidrug resistance proteins1 2 and 3 (Mrp1 2 and 3) mRNA and hepatic induction ofMrp3 by constitutive androstane receptor activators in ratsrdquoTheJournal of Pharmacology and Experimental Therapeutics vol300 no 1 pp 97ndash104 2002
[17] C A Ritter G Jedlitschky H Meyer Zu Schwabedissen MGrube K Kock and H K Kroemer ldquoCellular export ofdrugs and signaling molecules by the ATP-binding cassettetransporters MRP4 (ABCC4) and MRP5 (ABCC5)rdquo DrugMetabolism Reviews vol 37 no 1 pp 253ndash278 2005
[18] F G M Russel J B Koenderink and R Masereeuw ldquoMul-tidrug resistance protein 4 (MRP4ABCC4) a versatile effluxtransporter for drugs and signalling moleculesrdquo Trends inPharmacological Sciences vol 29 no 4 pp 200ndash207 2008
[19] D Keppler ldquoProgress in the molecular characterization ofhepatobiliary transportersrdquoDigestive Diseases vol 35 no 3 pp197ndash202 2017
[20] V Keitel M Burdelski U Warskulat et al ldquoExpression andlocalization of hepatobiliary transport proteins in progressivefamilial intrahepatic cholestasisrdquo Hepatology vol 41 no 5 pp1160ndash1172 2005
[21] N Ballatori F FangWV Christian N Li andC LHammondldquoOst120572-Ost120573 is required for bile acid and conjugated steroiddisposition in the intestine kidney and liverrdquoAmerican Journalof Physiology-Gastrointestinal and Liver Physiology vol 295 no1 pp G179ndashG186 2008
[22] J L Boyer M Trauner A Mennone et al ldquoUpregulationof a basolateral FXR-dependent bile acid efflux transporterOSTalpha-OSTbeta in cholestasis in humans and rodentsrdquoAmerican Journal of Physiology-Gastrointestinal and Liver Phys-iology vol 290 no 6 pp G1124ndashG1130 2006
[23] T Gerloff B Stieger B Hagenbuch et al ldquoThe sister of P-glycoprotein represents the canalicular bile salt export pump ofmammalian liverrdquoThe Journal of Biological Chemistry vol 273no 16 pp 10046ndash10050 1998
[24] A M van der Bliek F Baas T Ten Houte de Lange P MKooiman T van der Velde-Koerts and P Borst ldquoThe humanmdr3 gene encodes a novel P-glycoprotein homologue and givesrise to alternatively splicedmRNAs in liverrdquo EMBO Journal vol6 no 11 pp 3325ndash3331 1987
[25] A J Smith J L Timmermans-Hereijgers and B RoelofsenldquoThe human MDR3 P-glycoprotein promotes translocation ofphosphatidylcholine through the plasma membrane of fibrob-lasts from transgenic micerdquo FEBS Letters vol 354 no 3 pp263ndash266 1994
[26] J M L de Vree E Jacquemin E Sturm et al ldquoMutations in theMDR3 gene cause progressive familial intrahepatic cholestasisrdquoProceedings of the National Acadamy of Sciences of the UnitedStates of America vol 95 no 1 pp 282ndash287 1998
[27] A Groen M R Romero C Kunne et al ldquoComplementaryfunctions of the flippase ATP8B1 and the floppase ABCB4 inmaintaining canalicular membrane integrityrdquoGastroenterologyvol 141 no 5 pp 1927ndash1937 2011
10 Canadian Journal of Gastroenterology and Hepatology
[28] P A Dawson T Lan and A Rao ldquoThematic review series Bileacids Bile acid transportersrdquo Journal of Lipid Research vol 50no 12 pp 2340ndash2357 2009
[29] E Halilbasic T Claudel andM Trauner ldquoBile acid transportersand regulatory nuclear receptors in the liver and beyondrdquoJournal of Hepatology vol 58 no 1 pp 155ndash168 2013
[30] B L Shneider ldquoIntestinal bile acid transport Biology physiol-ogy and pathophysiologyrdquo Journal of Pediatric Gastroenterologyand Nutrition vol 32 no 4 pp 407ndash417 2001
[31] T Claudel G Zollner M Wagner and M Trauner ldquoRoleof nuclear receptors for bile acid metabolism bile secretioncholestasis and gallstone diseaserdquoBiochimica et Biophysica Acta(BBA) - Molecular Basis of Disease vol 1812 no 8 pp 867ndash8782011
[32] J J Eloranta and G A Kullak-Ublick ldquoThe role of FXR indisorders of bile acid homeostasisrdquo Physiology Journal vol 23no 5 pp 286ndash295 2008
[33] B Goodwin S A Jones R R Price et al ldquoA regulatory cascadeof the nuclear receptors FXR SHP-1 and LRH-1 represses bileacid biosynthesisrdquo Molecular Cell vol 6 no 3 pp 517ndash5262000
[34] M Muller P L M Jansen K N Faber et al ldquoFarnesoid Xreceptor and bile salts are involved in transcriptional regulationof the gene encoding the human bile salt export pumprdquoHepatology vol 35 no 3 pp 589ndash596 2002
[35] M Ananthanarayanan N BalasubramanianMMakishima DJ Mangelsdorf and F J Suchy ldquoHuman bile salt export pumppromoter is transactivated by the farnesoid X receptorbile acidreceptorrdquo The Journal of Biological Chemistry vol 276 no 31pp 28857ndash28865 2001
[36] L Huang A Zhao J L Lew et al ldquoFarnesoid X receptoractivates transcription of the phospholipid pump MDR3rdquo TheJournal of Biological Chemistry vol 278 no 51 pp 51085ndash510902003
[37] M Wagner G Zollner and M Trauner ldquoNuclear receptorregulation of the adaptive response of bile acid transporters incholestasisrdquo Seminars in Liver Disease vol 30 no 2 pp 160ndash1772010
[38] Y Zhang H R Kast-Woelbern and P A Edwards ldquoNaturalstructural variants of the nuclear receptor farnesoid X recep-tor affect transcriptional activationrdquo The Journal of BiologicalChemistry vol 278 no 1 pp 104ndash110 2003
[39] SW C VanMil R H J Houwen and LW J Klomp ldquoGeneticsof familial intrahepatic cholestasis syndromesrdquo Journal of Med-ical Genetics vol 42 no 6 pp 449ndash463 2005
[40] V E H Carlton L Pawlikowska and L N Bull ldquoMolecularbasis of intrahepatic cholestasisrdquoAnnals ofMedicine vol 36 no8 pp 606ndash617 2004
[41] R J Clayton F L Iber B H Ruebner and V A MckusickldquoByler Disease Fatal Familial Intrahepatic Cholestasis in anAmish Kindredrdquo American Journal of Diseases of Children vol117 no 1 pp 112ndash124 1969
[42] E Jacquemin ldquoProgressive familial intrahepatic cholestasisrdquoClinics andResearch inHepatology andGastroenterology vol 36supplement 1 pp S26ndashS35 2012
[43] L N Bull M J T Van Eijk L Pawlikowska et al ldquoA geneencoding a P-type ATPase mutated in two forms of hereditarycholestasisrdquo Nature Genetics vol 18 no 3 pp 219ndash224 1998
[44] L W J Klomp J C Vargas S W C Van Mil et al ldquoCharac-terization of mutations in ATP8B1 associated with hereditarycholestasisrdquo Hepatology vol 40 no 1 pp 27ndash38 2004
[45] P Ujhazy D Ortiz S Misra et al ldquoFamilial intrahepaticcholestasis 1 Studies of localization and functionrdquo Hepatologyvol 34 no 4 I pp 768ndash775 2001
[46] C C Paulusma A Groen C Kunne et al ldquoAtp8b1 deficiencyin mice reduces resistance of the canalicular membrane tohydrophobic bile salts and impairs bile salt transportrdquo Hepatol-ogy vol 44 no 1 pp 195ndash204 2006
[47] SW C VanMil LW J Klomp L N Bull and RH J HouwenldquoFIC1 disease A spectrumof intrahepatic cholestatic disordersrdquoSeminars in Liver Disease vol 21 no 4 pp 535ndash544 2001
[48] A Miyahawa-Hayashino H Egawa T Yorifuji et al ldquoAllograftsteatohepatitis in progressive familial intrahepatic cholestasistype 1 after living donor liver transplantationrdquo Liver Transplan-tation vol 15 no 6 pp 610ndash618 2009
[49] E Nicastro X Stephenne F Smets et al ldquoRecovery of graftsteatosis and protein-losing enteropathy after biliary diversionin a PFIC 1 liver transplanted childrdquo Pediatric Transplantationvol 16 no 5 pp E177ndashE182 2012
[50] K Evason K E Bove M J Finegold et al ldquoMorphologic find-ings in progressive familial intrahepatic cholestasis 2 (PFIC2)Correlation with genetic and immunohistochemical studiesrdquoThe American Journal of Surgical Pathology vol 35 no 5 pp687ndash696 2011
[51] S S Strautnieks L N Bull A S Knisely et al ldquoA gene encodinga liver-specific ABC transporter is mutated in progressivefamilial intrahepatic cholestasisrdquo Nature Genetics vol 20 no3 pp 233ndash238 1998
[52] A S Knisely S S Strautnieks Y Meier et al ldquoHepatocellularcarcinoma in ten children under five years of age with bile saltexport pumpdeficiencyrdquoHepatology vol 44 no 2 pp 478ndash4862006
[53] A O Scheimann S S Strautnieks A S Knisely J A Byrne RJ Thompson andM J Finegold ldquoMutations in Bile Salt ExportPump (ABCB11) in Two Children with Progressive FamilialIntrahepatic Cholestasis and Cholangiocarcinomardquo Journal ofPediatrics vol 150 no 5 pp 556ndash559 2007
[54] V Keitel M Burdelski Z Vojnisek L Schmitt D HaussingerandRKubitz ldquoDe novo bile salt transporter antibodies as a pos-sible cause of recurrent graft failure after liver transplantationA novel mechanism of cholestasisrdquo Hepatology vol 50 no 2pp 510ndash517 2009
[55] P Jara L Hierro P Martınez-Fernandez et al ldquoRecurrence ofbile salt export pump deficiency after liver transplantationrdquoTheNew England Journal of Medicine vol 361 no 14 pp 1359ndash13672009
[56] R Kubitz C Droge S Kluge et al ldquoAutoimmune BSEPDiseaseDisease Recurrence After Liver Transplantation for ProgressiveFamilial Intrahepatic Cholestasisrdquo Clinical Reviews in Allergy ampImmunology vol 48 no 2-3 pp 273ndash284 2015
[57] J Stindt S Kluge C Droge et al ldquoBile salt export pump-reactive antibodies form a polyclonal multi-inhibitoryresponse in antibody-induced bile salt export pump deficiencyrdquoHepatology vol 63 no 2 pp 524ndash537 2016
[58] E Jacquemin J M DeVree D Cresteil et al ldquoThe widespectrum of multidrug resistance 3 deficiency from neonatalcholestasis to cirrhosis of adulthoodrdquoGastroenterology vol 120no 6 pp 1448ndash1458 2001
[59] O Rosmorduc and R Poupon ldquoLow phospholipid associatedcholelithiasis association with mutation in the MDR3ABCB4generdquo Orphanet Journal of Rare Diseases vol 2 article 29 2007
Canadian Journal of Gastroenterology and Hepatology 11
[60] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoThe spectrum of liver diseases related to ABCB4 gene muta-tions Pathophysiology and clinical aspectsrdquo Seminars in LiverDisease vol 30 no 2 pp 134ndash146 2010
[61] DWendumV BarbuO Rosmorduc L Arrive J-F Flejou andR Poupon ldquoAspects of liver pathology in adult patients withMDR3ABCB4 gene mutationsrdquo Virchows Archiv vol 460 no3 pp 291ndash298 2012
[62] R P J Oude Elferink andC C Paulusma ldquoFunction and patho-physiological importance of ABCB4 (MDR3 P-glycoprotein)rdquoPflugers Archiv - European Journal of Physiology vol 453 no 5pp 601ndash610 2007
[63] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoProgressive familial intrahepatic cholestasisrdquo Clinical Pedi-atrics vol 51 pp 689ndash691 2012
[64] S Boga D Jain andM L Schilsky ldquoPresentation of progressivefamilial intrahepatic cholestasis type 3 mimicking wilson dis-ease molecular genetic diagnosis and response to treatmentrdquoPediatric Gastroenterology Hepatology amp Nutrition vol 18 no3 p 202 2015
[65] M Sambrotta S Strautnieks E Papouli et al ldquoMutationsin TJP2 cause progressive cholestatic liver diseaserdquo NatureGenetics vol 46 no 4 pp 326ndash328 2014
[66] M Sambrotta and R J Thompson ldquoMutations in TJP2 encod-ing zona occludens 2 and liver diseaserdquo Tissue Barriers vol 3no 3 Article ID e1026537 2015
[67] S Zhou P M Hertel M J Finegold et al ldquoHepatocellularcarcinoma associated with tight-junction protein 2 deficiencyrdquoHepatology vol 62 no 6 pp 1914ndash1916 2015
[68] V EH Carlton B ZHarris E G Puffenberger et al ldquoComplexinheritance of familial hypercholanemia with associated muta-tions in TJP2 and BAATrdquo Nature Genetics vol 34 no 1 pp 91ndash96 2003
[69] N Gomez-Ospina C J Potter R Xiao et al ldquoMutations inthe nuclear bile acid receptor FXR cause progressive familialintrahepatic cholestasisrdquoNature Communications vol 7 ArticleID 10713 2016
[70] I Koutsounas S Theocharis I Delladetsima E Patsouris andC Giaginis ldquoFarnesoid x receptor in human metabolism anddisease the interplay between gene polymorphisms clinicalphenotypes and disease susceptibilityrdquo Expert Opinion on DrugMetabolism amp Toxicology vol 11 no 4 pp 523ndash532 2015
[71] S W C van Mil A Milona P H Dixon et al ldquoFunctionalVariants of the Central Bile Acid Sensor FXR Identified inIntrahepatic Cholestasis of Pregnancyrdquo Gastroenterology vol133 no 2 pp 507ndash516 2007
[72] C Droge M Bonus U Baumann et al ldquoSequencing of FIC1BSEP and MDR3 in a large cohort of patients with cholestasisrevealed a high number of different genetic variantsrdquo Journal ofHepatology vol 67 no 6 pp 1253ndash1264 2017
[73] L N Bull V E H Carlton N L Stricker et al ldquoGeneticand morphological findings in progressive familial intrahepaticcholestasis (Byler disease [PFIC-1] and Byler syndrome) Evi-dence for heterogeneityrdquo Hepatology vol 26 no 1 pp 155ndash1641997
[74] S W C Van Mil W L Van Der Woerd G Van Der Brugge etal ldquoBenign recurrent intrahepatic cholestasis type 2 is causedby mutations in ABCB11rdquo Gastroenterology vol 127 no 2 pp379ndash384 2004
[75] N A M Van Ooteghem L W J Klomp G P Van Berge-Henegouwen andRH JHouwen ldquoBenign recurrent intrahep-atic cholestasis progressing to progressive familial intrahepatic
cholestasis Low GGT cholestasis is a clinical continuumrdquoJournal of Hepatology vol 36 no 3 pp 439ndash443 2002
[76] F Balsells R Wyllie R Steffen and M Kay ldquoBenign recurrentintrahepatic cholestasis Improvement of pruritus and shorten-ing of the symptomatic phase with rifampin therapy A casereportrdquo Clinical Pediatrics vol 36 no 8 pp 483ndash485 1997
[77] U Beuers M Trauner P Jansen and R Poupon ldquoNewparadigms in the treatment of hepatic cholestasis FromUDCAto FXR PXR and beyondrdquo Journal of Hepatology vol 62 no 1pp S25ndashS37 2015
[78] L Bachs A Pares M Elena C Piera and J Rodes ldquoEffectsof long-term rifampicin administration in primary biliarycirrhosisrdquoGastroenterology vol 102 no 6 pp 2077ndash2080 1992
[79] J M Stapelbroek K J Van Erpecum L W J Klomp et alldquoNasobiliary drainage induces long-lasting remission in benignrecurrent intrahepatic cholestasisrdquoHepatology vol 43 no 1 pp51ndash53 2006
[80] F Lammert H-U Marschall A Glantz and S MaternldquoIntrahepatic cholestasis of pregnancymolecular pathogenesisdiagnosis and managementrdquo Journal of Hepatology vol 33 no6 pp 1012ndash1021 2000
[81] P H Dixon and C Williamson ldquoThe pathophysiology ofintrahepatic cholestasis of pregnancyrdquo Clinics and Research inHepatology and Gastroenterology vol 40 no 2 pp 141ndash1532016
[82] M G Martineau C Raker P H Dixon et al ldquoThe metabolicprofile of intrahepatic cholestasis of pregnancy is associatedwith impaired glucose tolerance dyslipidemia and increasedfetal growthrdquo Diabetes Care vol 38 no 2 pp 243ndash248 2015
[83] D G Goulis I A LWalkerMDe Swiet CWG Redman andC Williamson ldquoPreeclampsia with Abnormal Liver FunctionTests Is Associated with Cholestasis in a Subgroup of CasesrdquoHypertension in Pregnancy vol 23 no 1 pp 19ndash27 2004
[84] A Glantz H-U Marschall F Lammert and L-A MattssonldquoIntrahepatic cholestasis of pregnancy A randomized con-trolled trial comparing dexamethasone and ursodeoxycholicacidrdquo Hepatology vol 42 no 6 pp 1399ndash1405 2005
[85] R Zapata L Sandoval J Palma et al ldquoUrsodeoxycholic acidin the treatment of intrahepatic cholestasis of pregnancy A 12-year experiencerdquo Liver International vol 25 no 3 pp 548ndash5542005
[86] T Binder P Salaj T Zima and L Vıtek ldquoRandomized prospec-tive comparative study of ursodeoxycholic acid and S-adenosyl-L-methionine in the treatment of intrahepatic cholestasis ofpregnancyrdquo Journal of PerinatalMedicine vol 34 no 5 pp 383ndash391 2006
[87] P H Dixon N Weerasekera K J Linton et al ldquoHeterozy-gous MDR3 missense mutation associated with intrahepaticcholestasis of pregnancy Evidence for a defect in proteintraffickingrdquo Human Molecular Genetics vol 9 no 8 pp 1209ndash1217 2000
[88] C Gendrot Y Bacq M-C Brechot J Lansac and C AndresldquoA second heterozygous MDR3 nonsense mutation associatedwith intrahepatic cholestasis of pregnancyrdquo Journal of MedicalGenetics vol 40 no 3 article e32 2003
[89] A Floreani I Carderi D Paternoster et al ldquoIntrahepaticcholestasis of pregnancy Three novel MDR3 gene mutationsrdquoAlimentary Pharmacology amp Therapeutics vol 23 no 11 pp1649ndash1653 2006
[90] J N Painter M Savander A Ropponen et al ldquoSequencevariation in the ATP8B1 gene and intrahepatic cholestasis of
12 Canadian Journal of Gastroenterology and Hepatology
pregnancyrdquo European Journal of Human Genetics vol 13 no 4pp 435ndash439 2005
[91] W L Van Der Woerd R H J Houwen and S F J Van DeGraaf ldquoCurrent and future therapies for inherited cholestaticliver diseasesrdquoWorld Journal of Gastroenterology vol 23 no 5pp 763ndash775 2017
[92] A Thebaut D Habes F Gottrand et al ldquoSertraline as an addi-tional treatment for cholestatic pruritus in childrenrdquo Journal ofPediatric Gastroenterology and Nutrition vol 64 no 3 pp 431ndash435 2017
[93] U Ołdakowska-Jedynak I JankowskaM Hartleb et al ldquoTreat-ment of pruritus with Prometheus dialysis and absorption sys-tem in a patient with benign recurrent intrahepatic cholestasisrdquoHepatology Research vol 44 no 10 pp E304ndashE308 2014
[94] L Cutillo M Najimi F Smets et al ldquoSafety of living-related liver transplantation for progressive familial intrahep-atic cholestasisrdquo Pediatric Transplantation vol 10 no 5 pp570ndash574 2006
[95] E Gonzales B Grosse B Schuller et al ldquoTargeted phar-macotherapy in progressive familial intrahepatic cholestasistype 2 Evidence for improvement of cholestasis with 4-phenylbutyraterdquo Hepatology vol 62 no 2 pp 558ndash566 2015
[96] E Gonzales and E Jacquemin ldquoMutation specific drug ther-apy for progressive familial or benign recurrent intrahepaticcholestasis A new tool in a near futurerdquo Journal of Hepatologyvol 53 no 2 pp 385ndash387 2010
[97] M Trauner C D Fuchs E Halilbasic and G PaumgartnerldquoNew therapeutic concepts in bile acid transport and signalingfor management of cholestasisrdquo Hepatology vol 65 no 4 pp1393ndash1404 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Canadian Journal of Gastroenterology and Hepatology 5
(a) (b)
Figure 2 Histopathology of ABCB11 disease (a) Giant-cell hepatitis (arrows) with hepatocanalicular cholestasis and (b) complete absenceof ABCB11BSEP protein are typical findings in PFIC2 patients Inset immunohistochemical positivity of BSEP in the apical (canalicular)domain of hepatocytes in a healthy control (a) Hematoxylin and eosin original magnification x200 (b inset) Immunohistochemical stainingwith ABCB11 Rabbit Polyclonal Antibody (NBP1-89319 Novus Biologicals USA) original magnification x200 (b) x400 (inset)
cholestasis GGT activity is increased only in disorders ofphospholipid secretion (PFIC3)
511 Progressive Familial Intrahepatic Cholestasis Type 1(PFIC1) PFIC1 (ATP8B1 disease OMIM 211600) formerlyBylerrsquos disease [41] is the consequence of a severe defect in thegene encoding ATPase ATP8B1FIC1 (familial intrahepaticcholestasis 1) localised in the long arm of the 18th chro-mosome (18q21) [43 44] ATP8B1 deficiency which causesmembrane phospholipid asymmetry of the canalicular mem-brane reduces the capacity of the liver to secrete bile [45 46]In addition to the previously described common symptomsof PFIC clinical manifestation of PFIC1 also includes awide range of extrahepatic symptoms Extrahepatic mani-festations of ATP8B1 disease include elevated sweat chlorideconcentrations delayed pubescence and growth and waterydiarrhoea as well as impaired hearing andor pancreatitis[47] These symptoms often persist while diarrhoea eventends to worsen after liver transplantation (LTX) Liverallografts in PFIC1 patients may display diffuse steatosis witha variable necroinflammatory component with subsequentfibrosis [48] Both diarrhoea and steatosissteatohepatitismay improve after biliary diversion [49]
Laboratory findings with regard to PFIC1 have reportedcholestasis with low serum levels of GGT increased serumconcentrations of primary BS and normal levels of choles-terol Aminotransferases are initially within the referencerange but during disease progression they gradually increaseby up to tenfold [41] Histopathological changes predomi-nantly involve canalicular cholestasis accentuated around thecentral veins The interlobular ducts can be hypoplastic dueto subnormal bile flow Giant-cell changes of hepatocytes aregenerally not observed in biopsies Liver fibrosis progressioncorresponds with the respective stage of the disease and canterminate in cirrhosis A typical ultrastructural finding isthe presence of Byler-type coarsely granular bile in the bilecanaliculi [50] Molecular diagnosis is based on the detectionof pathogenic mutations in both alleles of the ATP8B1 gene
The milder intermittent nonprogressive form of ATP8B1deficiency is called BRIC1 (see below)
512 Progressive Familial Intrahepatic Cholestasis Type 2(PFIC2) PFIC2 (ABCB11 disease OMIM 601847) is causedby mutations in ABCB11 which is located on the longarm of the second chromosome (2q24) and encodes thecanalicular transport proteinABCB11BSEP [51] Clinical andlaboratory findings with regard to PFIC2 are similar to PFIC1but extrahepatic symptoms are not present Additionally inPFIC2 the formation of gallstones and the early elevation ofserum aminotransferase activity can occurThe developmentof hepatobiliarymalignancies both hepatocellular carcinomaand cholangiocarcinoma can be a serious complication ofPFIC2 which is not observed in PFIC1 [52 53] Screening forliver tumours is recommended from the first year of life inPFIC2 patients
Except for PFIC2 mutations in ABCB11 may result in amilder nonprogressive formof PFIC2 known asBRIC2 aswellas other forms of cholestasis such as ICP andor drug-inducedcholestasis (see below)
Histologically the typical findings in the liver biopsies ofPFIC2 patients are giant-cell (syncycial) hepatitis with hepa-tocanalicular cholestasis while extramedullary haemopoiesisis frequently discernible within lobules Interlobular bileducts can be hypoplastic and ductular proliferation at theperipheries of portal triads is commonly observed TheABCB11BSEP protein is usually undetectable immunohis-tochemically (Figure 2) Ultrastructurally canalicular bilecan be either amorphous or filamentous but is not coarselygranular [51]
Untreated PFIC2 usually leads to progressive liver fibrosisand cirrhosis the development of which ismore rapid than inPFIC1 One curative method for patients with PFIC2 is LTXUnlike in PFIC1 steatosis and steatohepatitis are not presentin liver allografts in the case of PFIC2 However in somepatients a recurrence of the PFIC2 phenotype accompaniedby elevated serum levels of BS and bilirubin with almost
6 Canadian Journal of Gastroenterology and Hepatology
normal GGT activity has been observed after LTX [54 55] Ithas been shown that canalicular immunostaining of the BSEPMDR3 and MRP2 proteins is preserved in the liver graftbiopsies and no discernible changes in BSEP immunoreactiv-ity distribution between the apical membrane and the cyto-plasm have been reported nonetheless de novo polyclonalinhibitory antibodies directed against the first extracellularloop of BSEP have been observed in the posttransplant serumof patients a condition known as Autoimmune BSEPDisease(AIBD) [56 57] The exact mechanism by which BS trans-port is inhibited by anti-BSEP antibodies is still unknownIt is supposed that the cross-linking of BSEP moleculeswhich in turn disrupts the structure and function ofcanalicular membranes andor the direct mechanical occlu-sion of the BSEP pore might explain the inhibitory effectsof the antibodies [56 57] It is estimated that up to 8 oftransplanted PFIC2 patients develop anti-BSEP antibodies[56] This may be explained by the insufficient autotoleranceagainst BSEP exhibited in some patients with severe ABCB11mutations resulting in the complete absence of the BSEPproteinThe causal relationship between recurrent cholestasisin the liver grafts of PFIC2 patients and the occurrence of denovo antibodies directed against BSEP is further supportedby observations that plasmapheresis and the administrationof anti-CD20 antibodies (rituximab) may alleviate symptomsof cholestasis [54ndash57]
Interestingly posttransplant development of inhibitoryautoantibodies directed against FIC1 andMDR3 transporterswith corresponding phenotypes has not yet been docu-mented in patients with PFIC1 and PFIC3 respectively[44]
513 Progressive Familial Intrahepatic Cholestasis Type 3(PFIC3) PFIC3 (ABCB4 disease OMIM 602347) is causedby mutations in both alleles of the ABCB4MDR3 gene thatencode phospholipid transporter MDR3 expressed in thecanalicular (apical) membrane of hepatocytes [26] As wellas PFIC3 there is evidence that either biallelic or monoal-lelic ABCB4 defects may cause or predispose patients to awide spectrum of human liver diseases such as LowPhospholipid-Associated Cholelithiasis Syndrome (LPACOMIM 600803) Intrahepatic Cholestasis of Pregnancy(ICP OMIM 147480) drug-induced liver injury transientneonatal cholestasis small duct sclerosing cholangitis andadult biliary fibrosis or cirrhosis [58ndash61] Moreover hepa-tocellular carcinoma and intrahepatic cholangiocarcinomahave been documented in patients withABCB4MDR3muta-tions [61]
Clinical and laboratory findings associated with PFIC3correspond to the other two forms of PFIC but are charac-terised by the absence of extrahepatic symptoms (except forcholelithiasis) Unlike PFIC1 and PFIC2 elevated serumGGTactivity and normal cholesterol levels are typically observedas exhibited by the MDR3 deficit [26 62]
Histopathological findings in connection with ABCB4disease are variable Syncytial (giant-cell) changes cholesta-sis portal inflammatory infiltrate and periportal ductularproliferation accompanied by various stages of fibrosis have
been observed in liver tissue Lipid crystals within bile ductsand fibroobliterative bile duct lesions can be seen Immuno-histochemistry has indicated the absence of the canalicularMDR3 protein predominantly in early onset forms howeverits use is limited compared to PFIC2 Ultrastructurally bile isdense and amorphous in PFIC3 [26 61]
Prolonged cholestasis in PFIC3 is associated with signifi-cant accumulation of copper in liver tissue andwith increasedurine copper excretion ie findings that overlap with thediagnostic criteria for Wilsonrsquos disease [63 64]
514 Progressive Familial Intrahepatic Cholestasis Type 4(PFIC4) The fourth form of PFIC (PFIC4 TJP2 deficiencyOMIM 615878) first described in 2014 [65] is clinicallysimilar to PFIC2 and caused by homozygous or compoundheterozygous mutations in the TJP2 gene located in the9q12 chromosome Tight junction protein 2 (TJP2 also zonaoccludens-2) is a cytoplasmic component of cell-cell junc-tional complexes expressed in most epithelia and creates alink between transmembrane tight junction proteins and theactin cytoskeleton Complete TJP2 deficiency is associatedwith a significant reduction in an integral tight junction pro-tein claudin-1 predominantly in the canalicular membranesof liver cells which subsequently leads to the disruption ofintercellular connections and the leakage of bile through theparacellular space into the liver parenchyma [65 66]
Patients with TJP2 deficiency display severe progressivecholestatic liver disease in early childhood which puts themat increased risk of developing hepatocellular carcinoma [67]Serum GGT activity is normal or at most slightly increasedwhile expression of the canalicular proteins BSEP andMDR3is maintained In addition to liver impairment extrahepaticfeatures have been identified in PFIC4 patients includ-ing neurological and respiratory disorders [66] A singlehomozygous missense mutation in TJP2 has been previouslydescribed as causing benign familial hypercholanemia a raredisorder of oligogenic inheritance which usually manifestsin elevated serum BS concentrations pruritus and fat mal-absorption but which does not lead to the development ofliver disease [68]
515 Progressive Familial Intrahepatic Cholestasis Type 5(PFIC5) PFIC5 (OMIM 617049) first described in 2016[69] is a cholestatic disorder caused by mutations in NR1H4a gene located at 12q231 which encodes FXR the keyregulator of BS metabolism (see above) Homozygous loss ofFXR function is associated with severe neonatal cholestasisand early onset vitamin K-independent coagulopathy whichrapidly progresses to end-stage liver disease The nonrespon-siveness of coagulopathy to vitamin K treatment is likelya direct consequence of the loss of FXR function repre-senting an important distinguishing diagnostic feature ofNR1H4-related cholestasis In addition to low (or normal)GGT activity serum levels of alpha-fetoprotein are typicallyelevated [69]
Liver biopsies have shown diffuse giant-cell transforma-tion of hepatocytes with hepatocellular cholestasis and ductu-lar proliferation Progressive fibrosis and even micronodularcirrhosis are evident at later stages BSEP is undetectable in
Canadian Journal of Gastroenterology and Hepatology 7
the apical domains of hepatocytes which is consistent withlow activity of GGT MDR3 expression on the other hand ismaintained [69]
Since FXR affects several metabolic pathways someNR1H4 variations may be associated with susceptibility tovarious human diseases NR1H4 single-nucleotide polymor-phisms seem to be correlated with differences in glucosehomeostasis gallstone formation ICP inflammatory boweldisease and several other disorders [70 71]
52 Benign Recurrent Intrahepatic Cholestasis (BRIC) BRICis a group of genetically heterogeneous autosomal recessivediseases characterised by intermittent episodes of cholesta-sis They are caused by mutations in the ATP8B1 and ABCB11genes (the same as in PFIC1 and PFIC2) and probably inat least one other as yet unidentified gene [72] Thereare two genetically characterised forms of BRIC BRIC1(Summerskill-Walshe-Tygstrup syndrome OMIM 243300)and BRIC2 (OMIM 605479) caused by partial deficiency inATP8B1 [39 73] and ABCB11 [74] respectively The diseasetypically manifests before the second decade of life but theage of the first manifestation can vary greatly The samevariability has been documented in the duration of cholestaticepisodes (several days to several months) and their intensityInfection or pregnancy may act as a triggering factor Theclinical manifestations include jaundice pruritus fatigueanorexia and steatorrhoea Increase of bilirubin and BS levelsin serum has been observed during cholestatic attacks butGGT activity and serum cholesterol levels tend to be normalAminotransferase activity is usually normal or only slightlyelevated while biochemical parameters fall within normalranges Liver biopsies performed during cholestatic attackshave demonstrated hepatocanalicular cholestasis withoutfibrosis During the asymptomatic period the histologicalpicture is completely normal Since canalicular expression ofBSEP protein in hepatocytes is mostly maintained immuno-histology is of limited significance in these cases Diagnosisof BRIC1 and BRIC2 is based on demonstrating evidence ofmutations in both alleles of the corresponding genesATP8B1and ABCB11
While mutations causing PFIC are often located in theconserved regions of the genes that encode conserved func-tional domains of the corresponding proteins mutations inBRIC only partially impact protein function and expressionHowever several cases of initially benign episodic cholestasisthat have subsequently transitioned to a persistent progres-sive form of the disease have been reported [75] Thus BRICand PFIC seem to represent two extremes of a continuousspectrum of phenotypes of the one disease
The administration of statins corticosteroids cholestyra-mine or ursodeoxycholic acid (UDCA) is usually not veryeffective in BRIC patients Improvement of pruritus andshortening of symptomatic phase has been described inBRIC patients treated with the antibiotic rifampicin a potenthuman activator of PXR [76 77] However severe hepa-totoxicity after long-term administration of rifampicin hasbeen reported in patients with cholestatic disorders [77 78]Nasobiliary drainage seems to have a prompt effect during
cholestatic episodes but the mechanism of action remainsunclear [79]
53 Intrahepatic Cholestasis of Pregnancy (ICP) ICP (OMIM147480) also known as obstetric cholestasis is characterisedby cholestasis and prurituswith onset in pregnancy usually inthe third trimester It is associated with abnormal liverfunction in the absence of other liver diseases and resolvescompletely after delivery [80 81]The incidence of ICP varieswith geographical location and ethnicity Seasonal variationsindicate higher incidence in winter months as reported insome countries and it more commonly occurs in associationwith multiple pregnancies and following in vitro fertilisationIn Europe ICP affects about 1 of all pregnancies [81] Atypical symptom is intense pruritus commonly localised inthe palms and the soles which progresses during pregnancyElevated levels of serum BS and increased liver aminotrans-ferase activity are typical laboratory findings in such casesIncreased serum bilirubin levels have been observed in asmall proportion of cases while jaundice only rarely occursin affected women [81]
ICP usually resolves soon after delivery Although thedisease is considered relatively benign for themother there isan increased rate of adverse foetal outcomes including foetaldistress foetal asphyxia stillbirth or even intrauterine deathall known complications of ICP [81 82] ICPmay also be asso-ciated with an abnormalmetabolic profile in afflictedwomenespecially higher prevalence of dyslipidaemia impaired glu-cose tolerance and maternal comorbidities eg gestationaldiabetes and preeclampsia [82 83] Administration of UDCAimproves clinical symptoms predominantly pruritus andmay even reduce the risk of premature birth [84ndash86]
Mutations in ABCB4 ABCB11 and ATP8B1 have beenidentified in some patients suffering from ICP [87ndash90]Additionally variations in NR1H4 may be implicated in ICPpossibly via downregulation of BSEP expression [71]
6 Conclusions and Perspectives
Identification of the genes involved in hereditary cholestasishas advanced our understanding of the molecular mecha-nisms behind bile formation and transport
Recently mutations in TJP2 and NR1H4 have been foundin patients with apparent BSEP deficiency normal serumGGT activity and no mutations in ABCB11 However thereare rare cases of genetic cholestasis causes of which haveyet to be identified Therefore it seems likely that other yetunidentified genes involved in secretion andor transport ofcholephiles may be responsible for FIC-like phenotypes
Current therapeutic regimens in FIC patients compriseboth nonsurgical and surgical approaches Nonsurgical ther-apy includes drugs predominantly UDCA and rifampicinand nasobiliary drainage the latter being predominantly usedin BRIC patients with intractable pruritus during long-lastingcholestatic episodes [76 77 79] However the mechanismresponsible for the instant and complete relief from pruritusis still unclear
In addition to cholestyramine phenobarbital S-adeno-sylmethionine opiate antagonists UDCA rifampicin and
8 Canadian Journal of Gastroenterology and Hepatology
serotonin antagonists and its reuptake inhibitors seem to bebeneficial in managing refractory pruritus in patients withPFIC [77 91 92] Furthermore clinical and biochemicalimprovements have been observed in BRIC patients withintractable pruritus after using the molecular adsorbentrecirculating system (MARS) and the Prometheus system anextracorporeal liver support therapy based on fractionatedplasma separation and adsorption [93]
Surgical therapies include partial biliary diversion iemechanical interruption of BS enterohepatic circulation inorder to prevent reabsorption of pruritogens (unidentifiedthus far) and their precursors which is primarily usefulin noncirrhotic children with low-GGT PFIC permanentcholestasis andor intense refractory pruritus and orthotopicLTX which is still the ultimate treatment modality for manyPFIC patients [91] However as well as the risks associatedwith these invasive procedures other serious postoperative-related complications have been reported particularly inPFIC1 patients with extradigestive symptoms which canpersist or even worsen most likely due to extrahepaticexpression of FIC1 [47]Moreover the development of steato-sis and steatohepatitis leading to progressive liver allograftfibrosis in PFIC1 patients [48] and recurrence of the PFIC2phenotype in ABCB11 deficiency may represent other seriouscomplications after LTX and for some patients may evennecessitate retransplantation [54ndash57]
Importantly because of the shortage of cadaveric donorsparental living-related LTX is often considered in PFICpatients As heterozygous conditions can cause mild-to-moderate disease expression under certain circumstancesthe use of blood relatives as donors is seen as controversial Insuch cases it is likely that the heterozygous status of the donorallograft could pose a risk of complications during the lateposttransplant period such as lithiasis or cholestasis whichcan be precipitated by infections or by drugs administeredto the patient However the results of a recent study indicatethat the PFIC heterozygote status of the organ donor does notincrease the risk of liver dysfunction [94]
The limited effectiveness of current conservative proce-dures along with the complications of invasive methods par-ticularly LTX stress the need for the development and intro-duction of new treatment options Total biliary diversionpharmacological diversion of BS and hepatocyte transplanta-tion as well as gene- and mutation-targeted pharmacothera-pies represent promising future therapeutic approaches Thelatter two methods provide the basis for personalised treat-ment strategies in FIC patients Pharmacological chaperones(eg 4-phenylbutyrate) agonists of nuclear receptors (egstatins fibrates 6-ethyl chenodeoxycholic acid) endoplasmicreticulum-associated degradation inhibitors (MG132) andseveral other mutation-specific drugs can be used to increasethe expression of functional proteins and mitigate or eveneliminate deficient phenotypes [95ndash97]
Nevertheless despite the indisputable progress in thetherapy of FIC patients the increased risks of hepatobiliarymalignancies particularly in relation to ABCB11 deficiencystill remain serious life-threatening complications Furtherstudies are required in order to elucidate the complex patho-genesis of cholestasis unlock the mechanism of cholestatic
pruritus and improve the clinical management of bothhereditary and acquired cholestatic liver diseases
Abbreviations
ABC ATP-binding cassette subfamilyABCB4 ATP-binding cassette subfamily B
member 4ABCB11 ATP-binding cassette subfamily B
member 11AIBD Autoimmune BSEP DiseaseASBT Apical sodium-dependent bile acid
transporterATP8B1 ATPase aminophospholipid transporter
class I type 8B member 1BRIC Benign Recurrent Intrahepatic CholestasisBS Bile saltsBSEP Bile salt export pumpCYP7A1 Cholesterol 7 alpha-hydroxylaseCYP27A1 Sterol-27 hydroxylaseFGF19 Fibroblast growth factor 19FGFR4 Fibroblast growth factor receptor 4FIC Familial intrahepatic cholestasisFXR Farnesoid X-activated receptorGGT rsaquo-Glutamyl transferaseHNF4120572 Hepatocyte nuclear factor 4120572IBABP Intestinal bile acid-binding proteinICP Intrahepatic cholestasis of pregnancyIR-1 Inverted repeat DNA element with 1
nucleotide spacingLPAC Low Phospholipid-Associated
Cholelithiasis SyndromeLTX Liver allograft transplantationLXR Liver X receptorMDR3 Multidrug resistance protein 3MRP Multidrug resistance-associated proteinNR1H4 Nuclear receptor subfamily 1 group H
member 4NTCP Na+-taurocholate cotransporting
polypeptidesolute carrier family 10member 1
OATP Organic anion-transporting polypeptideOMIM Electronic database Online Mendelian
Inheritance in ManTMOST Organic solute transporterPFIC Progressive Familial Intrahepatic
CholestasisPXR Pregnane X receptorRXR Retinoid X receptorSHP Small heterodimer partnerSLC22A Solute carrier family 22 (organic cation
transporter) member 1SLCO Solute carrier organic anion transporter
familyTJP2 Tight junction protein 2 zona occludens-2UDCA Ursodeoxycholic acidUGT2B4 Uridine
51015840-diphosphate-glucuronosyltransferase2B4
Canadian Journal of Gastroenterology and Hepatology 9
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
Milan Jirsa was supported by Ministry of Health CzechRepublicmdashConceptual Development of Research Organiza-tion (ldquoInstitute for Clinical and Experimental MedicinendashIKEM IN 00023001rdquo)
References
[1] N B Javitt ldquoBile acid synthesis from cholesterol regulatory andauxiliary pathwaysrdquoThe FASEB Journal vol 8 no 15 pp 1308ndash1311 1994
[2] J Y L Chiang ldquoBile acids regulation of synthesisrdquo Journal ofLipid Research vol 50 no 10 pp 1955ndash1966 2009
[3] J L Boyer ldquoBile formation and secretionrdquo ComprehensivePhysiology vol 3 no 3 pp 1035ndash1078 2013
[4] B Hagenbuch and P J Meier ldquoSinusoidal (basolateral) bile saltuptake systems of hepatocytesrdquo Seminars in Liver Disease vol16 no 2 pp 129ndash136 1996
[5] B Hagenbuch B Stieger M Foguet H Lubbert and P JMeier ldquoFunctional expression cloning and characterization ofthe hepatocyte Na+bile acid cotransport systemrdquo Proceedingsof the National Acadamy of Sciences of the United States ofAmerica vol 88 no 23 pp 10629ndash10633 1991
[6] F M Vaz C C Paulusma H Huidekoper et al ldquoSodiumtaurocholate cotransporting polypeptide (SLC10A1) deficiencyConjugated hypercholanemia without a clear clinical pheno-typerdquo Hepatology vol 61 no 1 pp 260ndash267 2015
[7] B Hagenbuch and P J Meier ldquoOrganic anion transportingpolypeptides of the OATPSLC21 family Phylogenetic classi-fication as OATPSLCO super-family new nomenclature andmolecularfunctional propertiesrdquo Pflugers Archiv - EuropeanJournal of Physiology vol 447 no 5 pp 653ndash665 2004
[8] B Hagenbuch and B Stieger ldquoThe SLCO (former SLC21)superfamily of transportersrdquoMolecular Aspects of Medicine vol34 no 2-3 pp 396ndash412 2013
[9] M Muller and P L M Jansen ldquoThe secretory function ofthe liver New aspects of hepatobiliary transportrdquo Journal ofHepatology vol 28 no 2 pp 344ndash354 1998
[10] G J E J Hooiveld J E Van Montfoort D K F Meijerand M Muller ldquoFunction and regulation of ATP-bindingcassette transport proteins involved in hepatobiliary transportrdquoEuropean Journal of Pharmaceutical Sciences vol 12 no 4 pp525ndash543 2001
[11] J Konig D Rost Y Cui and D Keppler ldquoCharacterizationof the human multidrug resistance protein isoform MRP3localized to the basolateral hepatocyte membranerdquoHepatologyvol 29 no 4 pp 1156ndash1163 1999
[12] H Zeng G Liu P A Rea and G D Kruh ldquoTransport ofamphipathic anions by human multidrug resistance protein 3rdquoCancer Research vol 60 pp 4779ndash4784 2000
[13] Y-M A Lee Y Cui J Konig et al ldquoIdentification and func-tional characterization of the natural variantMRP3-Arg1297Hisof human multidrug resistance protein 3 (MRP3ABCC3)rdquoPharmacogenetics vol 14 no 4 pp 213ndash223 2004
[14] M Donner ldquoUp-regulation of basolateral multidrug resistanceprotein 3 (Mrp3) in cholestatic rat liverrdquoHepatology vol 34 no2 pp 351ndash359 2001
[15] M L Ruiz J P Rigalli A Arias et al ldquoInduction of hepaticmultidrug resistance-associated protein 3 by ethynylestradiol isindependent of cholestasis and mediated by estrogen receptorrdquoDrug Metabolism and Disposition vol 41 no 2 pp 275ndash2802013
[16] N J Cherrington D P Hartley N Li D R Johnson and C DKlaassen ldquoOrgan distribution of multidrug resistance proteins1 2 and 3 (Mrp1 2 and 3) mRNA and hepatic induction ofMrp3 by constitutive androstane receptor activators in ratsrdquoTheJournal of Pharmacology and Experimental Therapeutics vol300 no 1 pp 97ndash104 2002
[17] C A Ritter G Jedlitschky H Meyer Zu Schwabedissen MGrube K Kock and H K Kroemer ldquoCellular export ofdrugs and signaling molecules by the ATP-binding cassettetransporters MRP4 (ABCC4) and MRP5 (ABCC5)rdquo DrugMetabolism Reviews vol 37 no 1 pp 253ndash278 2005
[18] F G M Russel J B Koenderink and R Masereeuw ldquoMul-tidrug resistance protein 4 (MRP4ABCC4) a versatile effluxtransporter for drugs and signalling moleculesrdquo Trends inPharmacological Sciences vol 29 no 4 pp 200ndash207 2008
[19] D Keppler ldquoProgress in the molecular characterization ofhepatobiliary transportersrdquoDigestive Diseases vol 35 no 3 pp197ndash202 2017
[20] V Keitel M Burdelski U Warskulat et al ldquoExpression andlocalization of hepatobiliary transport proteins in progressivefamilial intrahepatic cholestasisrdquo Hepatology vol 41 no 5 pp1160ndash1172 2005
[21] N Ballatori F FangWV Christian N Li andC LHammondldquoOst120572-Ost120573 is required for bile acid and conjugated steroiddisposition in the intestine kidney and liverrdquoAmerican Journalof Physiology-Gastrointestinal and Liver Physiology vol 295 no1 pp G179ndashG186 2008
[22] J L Boyer M Trauner A Mennone et al ldquoUpregulationof a basolateral FXR-dependent bile acid efflux transporterOSTalpha-OSTbeta in cholestasis in humans and rodentsrdquoAmerican Journal of Physiology-Gastrointestinal and Liver Phys-iology vol 290 no 6 pp G1124ndashG1130 2006
[23] T Gerloff B Stieger B Hagenbuch et al ldquoThe sister of P-glycoprotein represents the canalicular bile salt export pump ofmammalian liverrdquoThe Journal of Biological Chemistry vol 273no 16 pp 10046ndash10050 1998
[24] A M van der Bliek F Baas T Ten Houte de Lange P MKooiman T van der Velde-Koerts and P Borst ldquoThe humanmdr3 gene encodes a novel P-glycoprotein homologue and givesrise to alternatively splicedmRNAs in liverrdquo EMBO Journal vol6 no 11 pp 3325ndash3331 1987
[25] A J Smith J L Timmermans-Hereijgers and B RoelofsenldquoThe human MDR3 P-glycoprotein promotes translocation ofphosphatidylcholine through the plasma membrane of fibrob-lasts from transgenic micerdquo FEBS Letters vol 354 no 3 pp263ndash266 1994
[26] J M L de Vree E Jacquemin E Sturm et al ldquoMutations in theMDR3 gene cause progressive familial intrahepatic cholestasisrdquoProceedings of the National Acadamy of Sciences of the UnitedStates of America vol 95 no 1 pp 282ndash287 1998
[27] A Groen M R Romero C Kunne et al ldquoComplementaryfunctions of the flippase ATP8B1 and the floppase ABCB4 inmaintaining canalicular membrane integrityrdquoGastroenterologyvol 141 no 5 pp 1927ndash1937 2011
10 Canadian Journal of Gastroenterology and Hepatology
[28] P A Dawson T Lan and A Rao ldquoThematic review series Bileacids Bile acid transportersrdquo Journal of Lipid Research vol 50no 12 pp 2340ndash2357 2009
[29] E Halilbasic T Claudel andM Trauner ldquoBile acid transportersand regulatory nuclear receptors in the liver and beyondrdquoJournal of Hepatology vol 58 no 1 pp 155ndash168 2013
[30] B L Shneider ldquoIntestinal bile acid transport Biology physiol-ogy and pathophysiologyrdquo Journal of Pediatric Gastroenterologyand Nutrition vol 32 no 4 pp 407ndash417 2001
[31] T Claudel G Zollner M Wagner and M Trauner ldquoRoleof nuclear receptors for bile acid metabolism bile secretioncholestasis and gallstone diseaserdquoBiochimica et Biophysica Acta(BBA) - Molecular Basis of Disease vol 1812 no 8 pp 867ndash8782011
[32] J J Eloranta and G A Kullak-Ublick ldquoThe role of FXR indisorders of bile acid homeostasisrdquo Physiology Journal vol 23no 5 pp 286ndash295 2008
[33] B Goodwin S A Jones R R Price et al ldquoA regulatory cascadeof the nuclear receptors FXR SHP-1 and LRH-1 represses bileacid biosynthesisrdquo Molecular Cell vol 6 no 3 pp 517ndash5262000
[34] M Muller P L M Jansen K N Faber et al ldquoFarnesoid Xreceptor and bile salts are involved in transcriptional regulationof the gene encoding the human bile salt export pumprdquoHepatology vol 35 no 3 pp 589ndash596 2002
[35] M Ananthanarayanan N BalasubramanianMMakishima DJ Mangelsdorf and F J Suchy ldquoHuman bile salt export pumppromoter is transactivated by the farnesoid X receptorbile acidreceptorrdquo The Journal of Biological Chemistry vol 276 no 31pp 28857ndash28865 2001
[36] L Huang A Zhao J L Lew et al ldquoFarnesoid X receptoractivates transcription of the phospholipid pump MDR3rdquo TheJournal of Biological Chemistry vol 278 no 51 pp 51085ndash510902003
[37] M Wagner G Zollner and M Trauner ldquoNuclear receptorregulation of the adaptive response of bile acid transporters incholestasisrdquo Seminars in Liver Disease vol 30 no 2 pp 160ndash1772010
[38] Y Zhang H R Kast-Woelbern and P A Edwards ldquoNaturalstructural variants of the nuclear receptor farnesoid X recep-tor affect transcriptional activationrdquo The Journal of BiologicalChemistry vol 278 no 1 pp 104ndash110 2003
[39] SW C VanMil R H J Houwen and LW J Klomp ldquoGeneticsof familial intrahepatic cholestasis syndromesrdquo Journal of Med-ical Genetics vol 42 no 6 pp 449ndash463 2005
[40] V E H Carlton L Pawlikowska and L N Bull ldquoMolecularbasis of intrahepatic cholestasisrdquoAnnals ofMedicine vol 36 no8 pp 606ndash617 2004
[41] R J Clayton F L Iber B H Ruebner and V A MckusickldquoByler Disease Fatal Familial Intrahepatic Cholestasis in anAmish Kindredrdquo American Journal of Diseases of Children vol117 no 1 pp 112ndash124 1969
[42] E Jacquemin ldquoProgressive familial intrahepatic cholestasisrdquoClinics andResearch inHepatology andGastroenterology vol 36supplement 1 pp S26ndashS35 2012
[43] L N Bull M J T Van Eijk L Pawlikowska et al ldquoA geneencoding a P-type ATPase mutated in two forms of hereditarycholestasisrdquo Nature Genetics vol 18 no 3 pp 219ndash224 1998
[44] L W J Klomp J C Vargas S W C Van Mil et al ldquoCharac-terization of mutations in ATP8B1 associated with hereditarycholestasisrdquo Hepatology vol 40 no 1 pp 27ndash38 2004
[45] P Ujhazy D Ortiz S Misra et al ldquoFamilial intrahepaticcholestasis 1 Studies of localization and functionrdquo Hepatologyvol 34 no 4 I pp 768ndash775 2001
[46] C C Paulusma A Groen C Kunne et al ldquoAtp8b1 deficiencyin mice reduces resistance of the canalicular membrane tohydrophobic bile salts and impairs bile salt transportrdquo Hepatol-ogy vol 44 no 1 pp 195ndash204 2006
[47] SW C VanMil LW J Klomp L N Bull and RH J HouwenldquoFIC1 disease A spectrumof intrahepatic cholestatic disordersrdquoSeminars in Liver Disease vol 21 no 4 pp 535ndash544 2001
[48] A Miyahawa-Hayashino H Egawa T Yorifuji et al ldquoAllograftsteatohepatitis in progressive familial intrahepatic cholestasistype 1 after living donor liver transplantationrdquo Liver Transplan-tation vol 15 no 6 pp 610ndash618 2009
[49] E Nicastro X Stephenne F Smets et al ldquoRecovery of graftsteatosis and protein-losing enteropathy after biliary diversionin a PFIC 1 liver transplanted childrdquo Pediatric Transplantationvol 16 no 5 pp E177ndashE182 2012
[50] K Evason K E Bove M J Finegold et al ldquoMorphologic find-ings in progressive familial intrahepatic cholestasis 2 (PFIC2)Correlation with genetic and immunohistochemical studiesrdquoThe American Journal of Surgical Pathology vol 35 no 5 pp687ndash696 2011
[51] S S Strautnieks L N Bull A S Knisely et al ldquoA gene encodinga liver-specific ABC transporter is mutated in progressivefamilial intrahepatic cholestasisrdquo Nature Genetics vol 20 no3 pp 233ndash238 1998
[52] A S Knisely S S Strautnieks Y Meier et al ldquoHepatocellularcarcinoma in ten children under five years of age with bile saltexport pumpdeficiencyrdquoHepatology vol 44 no 2 pp 478ndash4862006
[53] A O Scheimann S S Strautnieks A S Knisely J A Byrne RJ Thompson andM J Finegold ldquoMutations in Bile Salt ExportPump (ABCB11) in Two Children with Progressive FamilialIntrahepatic Cholestasis and Cholangiocarcinomardquo Journal ofPediatrics vol 150 no 5 pp 556ndash559 2007
[54] V Keitel M Burdelski Z Vojnisek L Schmitt D HaussingerandRKubitz ldquoDe novo bile salt transporter antibodies as a pos-sible cause of recurrent graft failure after liver transplantationA novel mechanism of cholestasisrdquo Hepatology vol 50 no 2pp 510ndash517 2009
[55] P Jara L Hierro P Martınez-Fernandez et al ldquoRecurrence ofbile salt export pump deficiency after liver transplantationrdquoTheNew England Journal of Medicine vol 361 no 14 pp 1359ndash13672009
[56] R Kubitz C Droge S Kluge et al ldquoAutoimmune BSEPDiseaseDisease Recurrence After Liver Transplantation for ProgressiveFamilial Intrahepatic Cholestasisrdquo Clinical Reviews in Allergy ampImmunology vol 48 no 2-3 pp 273ndash284 2015
[57] J Stindt S Kluge C Droge et al ldquoBile salt export pump-reactive antibodies form a polyclonal multi-inhibitoryresponse in antibody-induced bile salt export pump deficiencyrdquoHepatology vol 63 no 2 pp 524ndash537 2016
[58] E Jacquemin J M DeVree D Cresteil et al ldquoThe widespectrum of multidrug resistance 3 deficiency from neonatalcholestasis to cirrhosis of adulthoodrdquoGastroenterology vol 120no 6 pp 1448ndash1458 2001
[59] O Rosmorduc and R Poupon ldquoLow phospholipid associatedcholelithiasis association with mutation in the MDR3ABCB4generdquo Orphanet Journal of Rare Diseases vol 2 article 29 2007
Canadian Journal of Gastroenterology and Hepatology 11
[60] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoThe spectrum of liver diseases related to ABCB4 gene muta-tions Pathophysiology and clinical aspectsrdquo Seminars in LiverDisease vol 30 no 2 pp 134ndash146 2010
[61] DWendumV BarbuO Rosmorduc L Arrive J-F Flejou andR Poupon ldquoAspects of liver pathology in adult patients withMDR3ABCB4 gene mutationsrdquo Virchows Archiv vol 460 no3 pp 291ndash298 2012
[62] R P J Oude Elferink andC C Paulusma ldquoFunction and patho-physiological importance of ABCB4 (MDR3 P-glycoprotein)rdquoPflugers Archiv - European Journal of Physiology vol 453 no 5pp 601ndash610 2007
[63] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoProgressive familial intrahepatic cholestasisrdquo Clinical Pedi-atrics vol 51 pp 689ndash691 2012
[64] S Boga D Jain andM L Schilsky ldquoPresentation of progressivefamilial intrahepatic cholestasis type 3 mimicking wilson dis-ease molecular genetic diagnosis and response to treatmentrdquoPediatric Gastroenterology Hepatology amp Nutrition vol 18 no3 p 202 2015
[65] M Sambrotta S Strautnieks E Papouli et al ldquoMutationsin TJP2 cause progressive cholestatic liver diseaserdquo NatureGenetics vol 46 no 4 pp 326ndash328 2014
[66] M Sambrotta and R J Thompson ldquoMutations in TJP2 encod-ing zona occludens 2 and liver diseaserdquo Tissue Barriers vol 3no 3 Article ID e1026537 2015
[67] S Zhou P M Hertel M J Finegold et al ldquoHepatocellularcarcinoma associated with tight-junction protein 2 deficiencyrdquoHepatology vol 62 no 6 pp 1914ndash1916 2015
[68] V EH Carlton B ZHarris E G Puffenberger et al ldquoComplexinheritance of familial hypercholanemia with associated muta-tions in TJP2 and BAATrdquo Nature Genetics vol 34 no 1 pp 91ndash96 2003
[69] N Gomez-Ospina C J Potter R Xiao et al ldquoMutations inthe nuclear bile acid receptor FXR cause progressive familialintrahepatic cholestasisrdquoNature Communications vol 7 ArticleID 10713 2016
[70] I Koutsounas S Theocharis I Delladetsima E Patsouris andC Giaginis ldquoFarnesoid x receptor in human metabolism anddisease the interplay between gene polymorphisms clinicalphenotypes and disease susceptibilityrdquo Expert Opinion on DrugMetabolism amp Toxicology vol 11 no 4 pp 523ndash532 2015
[71] S W C van Mil A Milona P H Dixon et al ldquoFunctionalVariants of the Central Bile Acid Sensor FXR Identified inIntrahepatic Cholestasis of Pregnancyrdquo Gastroenterology vol133 no 2 pp 507ndash516 2007
[72] C Droge M Bonus U Baumann et al ldquoSequencing of FIC1BSEP and MDR3 in a large cohort of patients with cholestasisrevealed a high number of different genetic variantsrdquo Journal ofHepatology vol 67 no 6 pp 1253ndash1264 2017
[73] L N Bull V E H Carlton N L Stricker et al ldquoGeneticand morphological findings in progressive familial intrahepaticcholestasis (Byler disease [PFIC-1] and Byler syndrome) Evi-dence for heterogeneityrdquo Hepatology vol 26 no 1 pp 155ndash1641997
[74] S W C Van Mil W L Van Der Woerd G Van Der Brugge etal ldquoBenign recurrent intrahepatic cholestasis type 2 is causedby mutations in ABCB11rdquo Gastroenterology vol 127 no 2 pp379ndash384 2004
[75] N A M Van Ooteghem L W J Klomp G P Van Berge-Henegouwen andRH JHouwen ldquoBenign recurrent intrahep-atic cholestasis progressing to progressive familial intrahepatic
cholestasis Low GGT cholestasis is a clinical continuumrdquoJournal of Hepatology vol 36 no 3 pp 439ndash443 2002
[76] F Balsells R Wyllie R Steffen and M Kay ldquoBenign recurrentintrahepatic cholestasis Improvement of pruritus and shorten-ing of the symptomatic phase with rifampin therapy A casereportrdquo Clinical Pediatrics vol 36 no 8 pp 483ndash485 1997
[77] U Beuers M Trauner P Jansen and R Poupon ldquoNewparadigms in the treatment of hepatic cholestasis FromUDCAto FXR PXR and beyondrdquo Journal of Hepatology vol 62 no 1pp S25ndashS37 2015
[78] L Bachs A Pares M Elena C Piera and J Rodes ldquoEffectsof long-term rifampicin administration in primary biliarycirrhosisrdquoGastroenterology vol 102 no 6 pp 2077ndash2080 1992
[79] J M Stapelbroek K J Van Erpecum L W J Klomp et alldquoNasobiliary drainage induces long-lasting remission in benignrecurrent intrahepatic cholestasisrdquoHepatology vol 43 no 1 pp51ndash53 2006
[80] F Lammert H-U Marschall A Glantz and S MaternldquoIntrahepatic cholestasis of pregnancymolecular pathogenesisdiagnosis and managementrdquo Journal of Hepatology vol 33 no6 pp 1012ndash1021 2000
[81] P H Dixon and C Williamson ldquoThe pathophysiology ofintrahepatic cholestasis of pregnancyrdquo Clinics and Research inHepatology and Gastroenterology vol 40 no 2 pp 141ndash1532016
[82] M G Martineau C Raker P H Dixon et al ldquoThe metabolicprofile of intrahepatic cholestasis of pregnancy is associatedwith impaired glucose tolerance dyslipidemia and increasedfetal growthrdquo Diabetes Care vol 38 no 2 pp 243ndash248 2015
[83] D G Goulis I A LWalkerMDe Swiet CWG Redman andC Williamson ldquoPreeclampsia with Abnormal Liver FunctionTests Is Associated with Cholestasis in a Subgroup of CasesrdquoHypertension in Pregnancy vol 23 no 1 pp 19ndash27 2004
[84] A Glantz H-U Marschall F Lammert and L-A MattssonldquoIntrahepatic cholestasis of pregnancy A randomized con-trolled trial comparing dexamethasone and ursodeoxycholicacidrdquo Hepatology vol 42 no 6 pp 1399ndash1405 2005
[85] R Zapata L Sandoval J Palma et al ldquoUrsodeoxycholic acidin the treatment of intrahepatic cholestasis of pregnancy A 12-year experiencerdquo Liver International vol 25 no 3 pp 548ndash5542005
[86] T Binder P Salaj T Zima and L Vıtek ldquoRandomized prospec-tive comparative study of ursodeoxycholic acid and S-adenosyl-L-methionine in the treatment of intrahepatic cholestasis ofpregnancyrdquo Journal of PerinatalMedicine vol 34 no 5 pp 383ndash391 2006
[87] P H Dixon N Weerasekera K J Linton et al ldquoHeterozy-gous MDR3 missense mutation associated with intrahepaticcholestasis of pregnancy Evidence for a defect in proteintraffickingrdquo Human Molecular Genetics vol 9 no 8 pp 1209ndash1217 2000
[88] C Gendrot Y Bacq M-C Brechot J Lansac and C AndresldquoA second heterozygous MDR3 nonsense mutation associatedwith intrahepatic cholestasis of pregnancyrdquo Journal of MedicalGenetics vol 40 no 3 article e32 2003
[89] A Floreani I Carderi D Paternoster et al ldquoIntrahepaticcholestasis of pregnancy Three novel MDR3 gene mutationsrdquoAlimentary Pharmacology amp Therapeutics vol 23 no 11 pp1649ndash1653 2006
[90] J N Painter M Savander A Ropponen et al ldquoSequencevariation in the ATP8B1 gene and intrahepatic cholestasis of
12 Canadian Journal of Gastroenterology and Hepatology
pregnancyrdquo European Journal of Human Genetics vol 13 no 4pp 435ndash439 2005
[91] W L Van Der Woerd R H J Houwen and S F J Van DeGraaf ldquoCurrent and future therapies for inherited cholestaticliver diseasesrdquoWorld Journal of Gastroenterology vol 23 no 5pp 763ndash775 2017
[92] A Thebaut D Habes F Gottrand et al ldquoSertraline as an addi-tional treatment for cholestatic pruritus in childrenrdquo Journal ofPediatric Gastroenterology and Nutrition vol 64 no 3 pp 431ndash435 2017
[93] U Ołdakowska-Jedynak I JankowskaM Hartleb et al ldquoTreat-ment of pruritus with Prometheus dialysis and absorption sys-tem in a patient with benign recurrent intrahepatic cholestasisrdquoHepatology Research vol 44 no 10 pp E304ndashE308 2014
[94] L Cutillo M Najimi F Smets et al ldquoSafety of living-related liver transplantation for progressive familial intrahep-atic cholestasisrdquo Pediatric Transplantation vol 10 no 5 pp570ndash574 2006
[95] E Gonzales B Grosse B Schuller et al ldquoTargeted phar-macotherapy in progressive familial intrahepatic cholestasistype 2 Evidence for improvement of cholestasis with 4-phenylbutyraterdquo Hepatology vol 62 no 2 pp 558ndash566 2015
[96] E Gonzales and E Jacquemin ldquoMutation specific drug ther-apy for progressive familial or benign recurrent intrahepaticcholestasis A new tool in a near futurerdquo Journal of Hepatologyvol 53 no 2 pp 385ndash387 2010
[97] M Trauner C D Fuchs E Halilbasic and G PaumgartnerldquoNew therapeutic concepts in bile acid transport and signalingfor management of cholestasisrdquo Hepatology vol 65 no 4 pp1393ndash1404 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

6 Canadian Journal of Gastroenterology and Hepatology
normal GGT activity has been observed after LTX [54 55] Ithas been shown that canalicular immunostaining of the BSEPMDR3 and MRP2 proteins is preserved in the liver graftbiopsies and no discernible changes in BSEP immunoreactiv-ity distribution between the apical membrane and the cyto-plasm have been reported nonetheless de novo polyclonalinhibitory antibodies directed against the first extracellularloop of BSEP have been observed in the posttransplant serumof patients a condition known as Autoimmune BSEPDisease(AIBD) [56 57] The exact mechanism by which BS trans-port is inhibited by anti-BSEP antibodies is still unknownIt is supposed that the cross-linking of BSEP moleculeswhich in turn disrupts the structure and function ofcanalicular membranes andor the direct mechanical occlu-sion of the BSEP pore might explain the inhibitory effectsof the antibodies [56 57] It is estimated that up to 8 oftransplanted PFIC2 patients develop anti-BSEP antibodies[56] This may be explained by the insufficient autotoleranceagainst BSEP exhibited in some patients with severe ABCB11mutations resulting in the complete absence of the BSEPproteinThe causal relationship between recurrent cholestasisin the liver grafts of PFIC2 patients and the occurrence of denovo antibodies directed against BSEP is further supportedby observations that plasmapheresis and the administrationof anti-CD20 antibodies (rituximab) may alleviate symptomsof cholestasis [54ndash57]
Interestingly posttransplant development of inhibitoryautoantibodies directed against FIC1 andMDR3 transporterswith corresponding phenotypes has not yet been docu-mented in patients with PFIC1 and PFIC3 respectively[44]
513 Progressive Familial Intrahepatic Cholestasis Type 3(PFIC3) PFIC3 (ABCB4 disease OMIM 602347) is causedby mutations in both alleles of the ABCB4MDR3 gene thatencode phospholipid transporter MDR3 expressed in thecanalicular (apical) membrane of hepatocytes [26] As wellas PFIC3 there is evidence that either biallelic or monoal-lelic ABCB4 defects may cause or predispose patients to awide spectrum of human liver diseases such as LowPhospholipid-Associated Cholelithiasis Syndrome (LPACOMIM 600803) Intrahepatic Cholestasis of Pregnancy(ICP OMIM 147480) drug-induced liver injury transientneonatal cholestasis small duct sclerosing cholangitis andadult biliary fibrosis or cirrhosis [58ndash61] Moreover hepa-tocellular carcinoma and intrahepatic cholangiocarcinomahave been documented in patients withABCB4MDR3muta-tions [61]
Clinical and laboratory findings associated with PFIC3correspond to the other two forms of PFIC but are charac-terised by the absence of extrahepatic symptoms (except forcholelithiasis) Unlike PFIC1 and PFIC2 elevated serumGGTactivity and normal cholesterol levels are typically observedas exhibited by the MDR3 deficit [26 62]
Histopathological findings in connection with ABCB4disease are variable Syncytial (giant-cell) changes cholesta-sis portal inflammatory infiltrate and periportal ductularproliferation accompanied by various stages of fibrosis have
been observed in liver tissue Lipid crystals within bile ductsand fibroobliterative bile duct lesions can be seen Immuno-histochemistry has indicated the absence of the canalicularMDR3 protein predominantly in early onset forms howeverits use is limited compared to PFIC2 Ultrastructurally bile isdense and amorphous in PFIC3 [26 61]
Prolonged cholestasis in PFIC3 is associated with signifi-cant accumulation of copper in liver tissue andwith increasedurine copper excretion ie findings that overlap with thediagnostic criteria for Wilsonrsquos disease [63 64]
514 Progressive Familial Intrahepatic Cholestasis Type 4(PFIC4) The fourth form of PFIC (PFIC4 TJP2 deficiencyOMIM 615878) first described in 2014 [65] is clinicallysimilar to PFIC2 and caused by homozygous or compoundheterozygous mutations in the TJP2 gene located in the9q12 chromosome Tight junction protein 2 (TJP2 also zonaoccludens-2) is a cytoplasmic component of cell-cell junc-tional complexes expressed in most epithelia and creates alink between transmembrane tight junction proteins and theactin cytoskeleton Complete TJP2 deficiency is associatedwith a significant reduction in an integral tight junction pro-tein claudin-1 predominantly in the canalicular membranesof liver cells which subsequently leads to the disruption ofintercellular connections and the leakage of bile through theparacellular space into the liver parenchyma [65 66]
Patients with TJP2 deficiency display severe progressivecholestatic liver disease in early childhood which puts themat increased risk of developing hepatocellular carcinoma [67]Serum GGT activity is normal or at most slightly increasedwhile expression of the canalicular proteins BSEP andMDR3is maintained In addition to liver impairment extrahepaticfeatures have been identified in PFIC4 patients includ-ing neurological and respiratory disorders [66] A singlehomozygous missense mutation in TJP2 has been previouslydescribed as causing benign familial hypercholanemia a raredisorder of oligogenic inheritance which usually manifestsin elevated serum BS concentrations pruritus and fat mal-absorption but which does not lead to the development ofliver disease [68]
515 Progressive Familial Intrahepatic Cholestasis Type 5(PFIC5) PFIC5 (OMIM 617049) first described in 2016[69] is a cholestatic disorder caused by mutations in NR1H4a gene located at 12q231 which encodes FXR the keyregulator of BS metabolism (see above) Homozygous loss ofFXR function is associated with severe neonatal cholestasisand early onset vitamin K-independent coagulopathy whichrapidly progresses to end-stage liver disease The nonrespon-siveness of coagulopathy to vitamin K treatment is likelya direct consequence of the loss of FXR function repre-senting an important distinguishing diagnostic feature ofNR1H4-related cholestasis In addition to low (or normal)GGT activity serum levels of alpha-fetoprotein are typicallyelevated [69]
Liver biopsies have shown diffuse giant-cell transforma-tion of hepatocytes with hepatocellular cholestasis and ductu-lar proliferation Progressive fibrosis and even micronodularcirrhosis are evident at later stages BSEP is undetectable in
Canadian Journal of Gastroenterology and Hepatology 7
the apical domains of hepatocytes which is consistent withlow activity of GGT MDR3 expression on the other hand ismaintained [69]
Since FXR affects several metabolic pathways someNR1H4 variations may be associated with susceptibility tovarious human diseases NR1H4 single-nucleotide polymor-phisms seem to be correlated with differences in glucosehomeostasis gallstone formation ICP inflammatory boweldisease and several other disorders [70 71]
52 Benign Recurrent Intrahepatic Cholestasis (BRIC) BRICis a group of genetically heterogeneous autosomal recessivediseases characterised by intermittent episodes of cholesta-sis They are caused by mutations in the ATP8B1 and ABCB11genes (the same as in PFIC1 and PFIC2) and probably inat least one other as yet unidentified gene [72] Thereare two genetically characterised forms of BRIC BRIC1(Summerskill-Walshe-Tygstrup syndrome OMIM 243300)and BRIC2 (OMIM 605479) caused by partial deficiency inATP8B1 [39 73] and ABCB11 [74] respectively The diseasetypically manifests before the second decade of life but theage of the first manifestation can vary greatly The samevariability has been documented in the duration of cholestaticepisodes (several days to several months) and their intensityInfection or pregnancy may act as a triggering factor Theclinical manifestations include jaundice pruritus fatigueanorexia and steatorrhoea Increase of bilirubin and BS levelsin serum has been observed during cholestatic attacks butGGT activity and serum cholesterol levels tend to be normalAminotransferase activity is usually normal or only slightlyelevated while biochemical parameters fall within normalranges Liver biopsies performed during cholestatic attackshave demonstrated hepatocanalicular cholestasis withoutfibrosis During the asymptomatic period the histologicalpicture is completely normal Since canalicular expression ofBSEP protein in hepatocytes is mostly maintained immuno-histology is of limited significance in these cases Diagnosisof BRIC1 and BRIC2 is based on demonstrating evidence ofmutations in both alleles of the corresponding genesATP8B1and ABCB11
While mutations causing PFIC are often located in theconserved regions of the genes that encode conserved func-tional domains of the corresponding proteins mutations inBRIC only partially impact protein function and expressionHowever several cases of initially benign episodic cholestasisthat have subsequently transitioned to a persistent progres-sive form of the disease have been reported [75] Thus BRICand PFIC seem to represent two extremes of a continuousspectrum of phenotypes of the one disease
The administration of statins corticosteroids cholestyra-mine or ursodeoxycholic acid (UDCA) is usually not veryeffective in BRIC patients Improvement of pruritus andshortening of symptomatic phase has been described inBRIC patients treated with the antibiotic rifampicin a potenthuman activator of PXR [76 77] However severe hepa-totoxicity after long-term administration of rifampicin hasbeen reported in patients with cholestatic disorders [77 78]Nasobiliary drainage seems to have a prompt effect during
cholestatic episodes but the mechanism of action remainsunclear [79]
53 Intrahepatic Cholestasis of Pregnancy (ICP) ICP (OMIM147480) also known as obstetric cholestasis is characterisedby cholestasis and prurituswith onset in pregnancy usually inthe third trimester It is associated with abnormal liverfunction in the absence of other liver diseases and resolvescompletely after delivery [80 81]The incidence of ICP varieswith geographical location and ethnicity Seasonal variationsindicate higher incidence in winter months as reported insome countries and it more commonly occurs in associationwith multiple pregnancies and following in vitro fertilisationIn Europe ICP affects about 1 of all pregnancies [81] Atypical symptom is intense pruritus commonly localised inthe palms and the soles which progresses during pregnancyElevated levels of serum BS and increased liver aminotrans-ferase activity are typical laboratory findings in such casesIncreased serum bilirubin levels have been observed in asmall proportion of cases while jaundice only rarely occursin affected women [81]
ICP usually resolves soon after delivery Although thedisease is considered relatively benign for themother there isan increased rate of adverse foetal outcomes including foetaldistress foetal asphyxia stillbirth or even intrauterine deathall known complications of ICP [81 82] ICPmay also be asso-ciated with an abnormalmetabolic profile in afflictedwomenespecially higher prevalence of dyslipidaemia impaired glu-cose tolerance and maternal comorbidities eg gestationaldiabetes and preeclampsia [82 83] Administration of UDCAimproves clinical symptoms predominantly pruritus andmay even reduce the risk of premature birth [84ndash86]
Mutations in ABCB4 ABCB11 and ATP8B1 have beenidentified in some patients suffering from ICP [87ndash90]Additionally variations in NR1H4 may be implicated in ICPpossibly via downregulation of BSEP expression [71]
6 Conclusions and Perspectives
Identification of the genes involved in hereditary cholestasishas advanced our understanding of the molecular mecha-nisms behind bile formation and transport
Recently mutations in TJP2 and NR1H4 have been foundin patients with apparent BSEP deficiency normal serumGGT activity and no mutations in ABCB11 However thereare rare cases of genetic cholestasis causes of which haveyet to be identified Therefore it seems likely that other yetunidentified genes involved in secretion andor transport ofcholephiles may be responsible for FIC-like phenotypes
Current therapeutic regimens in FIC patients compriseboth nonsurgical and surgical approaches Nonsurgical ther-apy includes drugs predominantly UDCA and rifampicinand nasobiliary drainage the latter being predominantly usedin BRIC patients with intractable pruritus during long-lastingcholestatic episodes [76 77 79] However the mechanismresponsible for the instant and complete relief from pruritusis still unclear
In addition to cholestyramine phenobarbital S-adeno-sylmethionine opiate antagonists UDCA rifampicin and
8 Canadian Journal of Gastroenterology and Hepatology
serotonin antagonists and its reuptake inhibitors seem to bebeneficial in managing refractory pruritus in patients withPFIC [77 91 92] Furthermore clinical and biochemicalimprovements have been observed in BRIC patients withintractable pruritus after using the molecular adsorbentrecirculating system (MARS) and the Prometheus system anextracorporeal liver support therapy based on fractionatedplasma separation and adsorption [93]
Surgical therapies include partial biliary diversion iemechanical interruption of BS enterohepatic circulation inorder to prevent reabsorption of pruritogens (unidentifiedthus far) and their precursors which is primarily usefulin noncirrhotic children with low-GGT PFIC permanentcholestasis andor intense refractory pruritus and orthotopicLTX which is still the ultimate treatment modality for manyPFIC patients [91] However as well as the risks associatedwith these invasive procedures other serious postoperative-related complications have been reported particularly inPFIC1 patients with extradigestive symptoms which canpersist or even worsen most likely due to extrahepaticexpression of FIC1 [47]Moreover the development of steato-sis and steatohepatitis leading to progressive liver allograftfibrosis in PFIC1 patients [48] and recurrence of the PFIC2phenotype in ABCB11 deficiency may represent other seriouscomplications after LTX and for some patients may evennecessitate retransplantation [54ndash57]
Importantly because of the shortage of cadaveric donorsparental living-related LTX is often considered in PFICpatients As heterozygous conditions can cause mild-to-moderate disease expression under certain circumstancesthe use of blood relatives as donors is seen as controversial Insuch cases it is likely that the heterozygous status of the donorallograft could pose a risk of complications during the lateposttransplant period such as lithiasis or cholestasis whichcan be precipitated by infections or by drugs administeredto the patient However the results of a recent study indicatethat the PFIC heterozygote status of the organ donor does notincrease the risk of liver dysfunction [94]
The limited effectiveness of current conservative proce-dures along with the complications of invasive methods par-ticularly LTX stress the need for the development and intro-duction of new treatment options Total biliary diversionpharmacological diversion of BS and hepatocyte transplanta-tion as well as gene- and mutation-targeted pharmacothera-pies represent promising future therapeutic approaches Thelatter two methods provide the basis for personalised treat-ment strategies in FIC patients Pharmacological chaperones(eg 4-phenylbutyrate) agonists of nuclear receptors (egstatins fibrates 6-ethyl chenodeoxycholic acid) endoplasmicreticulum-associated degradation inhibitors (MG132) andseveral other mutation-specific drugs can be used to increasethe expression of functional proteins and mitigate or eveneliminate deficient phenotypes [95ndash97]
Nevertheless despite the indisputable progress in thetherapy of FIC patients the increased risks of hepatobiliarymalignancies particularly in relation to ABCB11 deficiencystill remain serious life-threatening complications Furtherstudies are required in order to elucidate the complex patho-genesis of cholestasis unlock the mechanism of cholestatic
pruritus and improve the clinical management of bothhereditary and acquired cholestatic liver diseases
Abbreviations
ABC ATP-binding cassette subfamilyABCB4 ATP-binding cassette subfamily B
member 4ABCB11 ATP-binding cassette subfamily B
member 11AIBD Autoimmune BSEP DiseaseASBT Apical sodium-dependent bile acid
transporterATP8B1 ATPase aminophospholipid transporter
class I type 8B member 1BRIC Benign Recurrent Intrahepatic CholestasisBS Bile saltsBSEP Bile salt export pumpCYP7A1 Cholesterol 7 alpha-hydroxylaseCYP27A1 Sterol-27 hydroxylaseFGF19 Fibroblast growth factor 19FGFR4 Fibroblast growth factor receptor 4FIC Familial intrahepatic cholestasisFXR Farnesoid X-activated receptorGGT rsaquo-Glutamyl transferaseHNF4120572 Hepatocyte nuclear factor 4120572IBABP Intestinal bile acid-binding proteinICP Intrahepatic cholestasis of pregnancyIR-1 Inverted repeat DNA element with 1
nucleotide spacingLPAC Low Phospholipid-Associated
Cholelithiasis SyndromeLTX Liver allograft transplantationLXR Liver X receptorMDR3 Multidrug resistance protein 3MRP Multidrug resistance-associated proteinNR1H4 Nuclear receptor subfamily 1 group H
member 4NTCP Na+-taurocholate cotransporting
polypeptidesolute carrier family 10member 1
OATP Organic anion-transporting polypeptideOMIM Electronic database Online Mendelian
Inheritance in ManTMOST Organic solute transporterPFIC Progressive Familial Intrahepatic
CholestasisPXR Pregnane X receptorRXR Retinoid X receptorSHP Small heterodimer partnerSLC22A Solute carrier family 22 (organic cation
transporter) member 1SLCO Solute carrier organic anion transporter
familyTJP2 Tight junction protein 2 zona occludens-2UDCA Ursodeoxycholic acidUGT2B4 Uridine
51015840-diphosphate-glucuronosyltransferase2B4
Canadian Journal of Gastroenterology and Hepatology 9
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
Milan Jirsa was supported by Ministry of Health CzechRepublicmdashConceptual Development of Research Organiza-tion (ldquoInstitute for Clinical and Experimental MedicinendashIKEM IN 00023001rdquo)
References
[1] N B Javitt ldquoBile acid synthesis from cholesterol regulatory andauxiliary pathwaysrdquoThe FASEB Journal vol 8 no 15 pp 1308ndash1311 1994
[2] J Y L Chiang ldquoBile acids regulation of synthesisrdquo Journal ofLipid Research vol 50 no 10 pp 1955ndash1966 2009
[3] J L Boyer ldquoBile formation and secretionrdquo ComprehensivePhysiology vol 3 no 3 pp 1035ndash1078 2013
[4] B Hagenbuch and P J Meier ldquoSinusoidal (basolateral) bile saltuptake systems of hepatocytesrdquo Seminars in Liver Disease vol16 no 2 pp 129ndash136 1996
[5] B Hagenbuch B Stieger M Foguet H Lubbert and P JMeier ldquoFunctional expression cloning and characterization ofthe hepatocyte Na+bile acid cotransport systemrdquo Proceedingsof the National Acadamy of Sciences of the United States ofAmerica vol 88 no 23 pp 10629ndash10633 1991
[6] F M Vaz C C Paulusma H Huidekoper et al ldquoSodiumtaurocholate cotransporting polypeptide (SLC10A1) deficiencyConjugated hypercholanemia without a clear clinical pheno-typerdquo Hepatology vol 61 no 1 pp 260ndash267 2015
[7] B Hagenbuch and P J Meier ldquoOrganic anion transportingpolypeptides of the OATPSLC21 family Phylogenetic classi-fication as OATPSLCO super-family new nomenclature andmolecularfunctional propertiesrdquo Pflugers Archiv - EuropeanJournal of Physiology vol 447 no 5 pp 653ndash665 2004
[8] B Hagenbuch and B Stieger ldquoThe SLCO (former SLC21)superfamily of transportersrdquoMolecular Aspects of Medicine vol34 no 2-3 pp 396ndash412 2013
[9] M Muller and P L M Jansen ldquoThe secretory function ofthe liver New aspects of hepatobiliary transportrdquo Journal ofHepatology vol 28 no 2 pp 344ndash354 1998
[10] G J E J Hooiveld J E Van Montfoort D K F Meijerand M Muller ldquoFunction and regulation of ATP-bindingcassette transport proteins involved in hepatobiliary transportrdquoEuropean Journal of Pharmaceutical Sciences vol 12 no 4 pp525ndash543 2001
[11] J Konig D Rost Y Cui and D Keppler ldquoCharacterizationof the human multidrug resistance protein isoform MRP3localized to the basolateral hepatocyte membranerdquoHepatologyvol 29 no 4 pp 1156ndash1163 1999
[12] H Zeng G Liu P A Rea and G D Kruh ldquoTransport ofamphipathic anions by human multidrug resistance protein 3rdquoCancer Research vol 60 pp 4779ndash4784 2000
[13] Y-M A Lee Y Cui J Konig et al ldquoIdentification and func-tional characterization of the natural variantMRP3-Arg1297Hisof human multidrug resistance protein 3 (MRP3ABCC3)rdquoPharmacogenetics vol 14 no 4 pp 213ndash223 2004
[14] M Donner ldquoUp-regulation of basolateral multidrug resistanceprotein 3 (Mrp3) in cholestatic rat liverrdquoHepatology vol 34 no2 pp 351ndash359 2001
[15] M L Ruiz J P Rigalli A Arias et al ldquoInduction of hepaticmultidrug resistance-associated protein 3 by ethynylestradiol isindependent of cholestasis and mediated by estrogen receptorrdquoDrug Metabolism and Disposition vol 41 no 2 pp 275ndash2802013
[16] N J Cherrington D P Hartley N Li D R Johnson and C DKlaassen ldquoOrgan distribution of multidrug resistance proteins1 2 and 3 (Mrp1 2 and 3) mRNA and hepatic induction ofMrp3 by constitutive androstane receptor activators in ratsrdquoTheJournal of Pharmacology and Experimental Therapeutics vol300 no 1 pp 97ndash104 2002
[17] C A Ritter G Jedlitschky H Meyer Zu Schwabedissen MGrube K Kock and H K Kroemer ldquoCellular export ofdrugs and signaling molecules by the ATP-binding cassettetransporters MRP4 (ABCC4) and MRP5 (ABCC5)rdquo DrugMetabolism Reviews vol 37 no 1 pp 253ndash278 2005
[18] F G M Russel J B Koenderink and R Masereeuw ldquoMul-tidrug resistance protein 4 (MRP4ABCC4) a versatile effluxtransporter for drugs and signalling moleculesrdquo Trends inPharmacological Sciences vol 29 no 4 pp 200ndash207 2008
[19] D Keppler ldquoProgress in the molecular characterization ofhepatobiliary transportersrdquoDigestive Diseases vol 35 no 3 pp197ndash202 2017
[20] V Keitel M Burdelski U Warskulat et al ldquoExpression andlocalization of hepatobiliary transport proteins in progressivefamilial intrahepatic cholestasisrdquo Hepatology vol 41 no 5 pp1160ndash1172 2005
[21] N Ballatori F FangWV Christian N Li andC LHammondldquoOst120572-Ost120573 is required for bile acid and conjugated steroiddisposition in the intestine kidney and liverrdquoAmerican Journalof Physiology-Gastrointestinal and Liver Physiology vol 295 no1 pp G179ndashG186 2008
[22] J L Boyer M Trauner A Mennone et al ldquoUpregulationof a basolateral FXR-dependent bile acid efflux transporterOSTalpha-OSTbeta in cholestasis in humans and rodentsrdquoAmerican Journal of Physiology-Gastrointestinal and Liver Phys-iology vol 290 no 6 pp G1124ndashG1130 2006
[23] T Gerloff B Stieger B Hagenbuch et al ldquoThe sister of P-glycoprotein represents the canalicular bile salt export pump ofmammalian liverrdquoThe Journal of Biological Chemistry vol 273no 16 pp 10046ndash10050 1998
[24] A M van der Bliek F Baas T Ten Houte de Lange P MKooiman T van der Velde-Koerts and P Borst ldquoThe humanmdr3 gene encodes a novel P-glycoprotein homologue and givesrise to alternatively splicedmRNAs in liverrdquo EMBO Journal vol6 no 11 pp 3325ndash3331 1987
[25] A J Smith J L Timmermans-Hereijgers and B RoelofsenldquoThe human MDR3 P-glycoprotein promotes translocation ofphosphatidylcholine through the plasma membrane of fibrob-lasts from transgenic micerdquo FEBS Letters vol 354 no 3 pp263ndash266 1994
[26] J M L de Vree E Jacquemin E Sturm et al ldquoMutations in theMDR3 gene cause progressive familial intrahepatic cholestasisrdquoProceedings of the National Acadamy of Sciences of the UnitedStates of America vol 95 no 1 pp 282ndash287 1998
[27] A Groen M R Romero C Kunne et al ldquoComplementaryfunctions of the flippase ATP8B1 and the floppase ABCB4 inmaintaining canalicular membrane integrityrdquoGastroenterologyvol 141 no 5 pp 1927ndash1937 2011
10 Canadian Journal of Gastroenterology and Hepatology
[28] P A Dawson T Lan and A Rao ldquoThematic review series Bileacids Bile acid transportersrdquo Journal of Lipid Research vol 50no 12 pp 2340ndash2357 2009
[29] E Halilbasic T Claudel andM Trauner ldquoBile acid transportersand regulatory nuclear receptors in the liver and beyondrdquoJournal of Hepatology vol 58 no 1 pp 155ndash168 2013
[30] B L Shneider ldquoIntestinal bile acid transport Biology physiol-ogy and pathophysiologyrdquo Journal of Pediatric Gastroenterologyand Nutrition vol 32 no 4 pp 407ndash417 2001
[31] T Claudel G Zollner M Wagner and M Trauner ldquoRoleof nuclear receptors for bile acid metabolism bile secretioncholestasis and gallstone diseaserdquoBiochimica et Biophysica Acta(BBA) - Molecular Basis of Disease vol 1812 no 8 pp 867ndash8782011
[32] J J Eloranta and G A Kullak-Ublick ldquoThe role of FXR indisorders of bile acid homeostasisrdquo Physiology Journal vol 23no 5 pp 286ndash295 2008
[33] B Goodwin S A Jones R R Price et al ldquoA regulatory cascadeof the nuclear receptors FXR SHP-1 and LRH-1 represses bileacid biosynthesisrdquo Molecular Cell vol 6 no 3 pp 517ndash5262000
[34] M Muller P L M Jansen K N Faber et al ldquoFarnesoid Xreceptor and bile salts are involved in transcriptional regulationof the gene encoding the human bile salt export pumprdquoHepatology vol 35 no 3 pp 589ndash596 2002
[35] M Ananthanarayanan N BalasubramanianMMakishima DJ Mangelsdorf and F J Suchy ldquoHuman bile salt export pumppromoter is transactivated by the farnesoid X receptorbile acidreceptorrdquo The Journal of Biological Chemistry vol 276 no 31pp 28857ndash28865 2001
[36] L Huang A Zhao J L Lew et al ldquoFarnesoid X receptoractivates transcription of the phospholipid pump MDR3rdquo TheJournal of Biological Chemistry vol 278 no 51 pp 51085ndash510902003
[37] M Wagner G Zollner and M Trauner ldquoNuclear receptorregulation of the adaptive response of bile acid transporters incholestasisrdquo Seminars in Liver Disease vol 30 no 2 pp 160ndash1772010
[38] Y Zhang H R Kast-Woelbern and P A Edwards ldquoNaturalstructural variants of the nuclear receptor farnesoid X recep-tor affect transcriptional activationrdquo The Journal of BiologicalChemistry vol 278 no 1 pp 104ndash110 2003
[39] SW C VanMil R H J Houwen and LW J Klomp ldquoGeneticsof familial intrahepatic cholestasis syndromesrdquo Journal of Med-ical Genetics vol 42 no 6 pp 449ndash463 2005
[40] V E H Carlton L Pawlikowska and L N Bull ldquoMolecularbasis of intrahepatic cholestasisrdquoAnnals ofMedicine vol 36 no8 pp 606ndash617 2004
[41] R J Clayton F L Iber B H Ruebner and V A MckusickldquoByler Disease Fatal Familial Intrahepatic Cholestasis in anAmish Kindredrdquo American Journal of Diseases of Children vol117 no 1 pp 112ndash124 1969
[42] E Jacquemin ldquoProgressive familial intrahepatic cholestasisrdquoClinics andResearch inHepatology andGastroenterology vol 36supplement 1 pp S26ndashS35 2012
[43] L N Bull M J T Van Eijk L Pawlikowska et al ldquoA geneencoding a P-type ATPase mutated in two forms of hereditarycholestasisrdquo Nature Genetics vol 18 no 3 pp 219ndash224 1998
[44] L W J Klomp J C Vargas S W C Van Mil et al ldquoCharac-terization of mutations in ATP8B1 associated with hereditarycholestasisrdquo Hepatology vol 40 no 1 pp 27ndash38 2004
[45] P Ujhazy D Ortiz S Misra et al ldquoFamilial intrahepaticcholestasis 1 Studies of localization and functionrdquo Hepatologyvol 34 no 4 I pp 768ndash775 2001
[46] C C Paulusma A Groen C Kunne et al ldquoAtp8b1 deficiencyin mice reduces resistance of the canalicular membrane tohydrophobic bile salts and impairs bile salt transportrdquo Hepatol-ogy vol 44 no 1 pp 195ndash204 2006
[47] SW C VanMil LW J Klomp L N Bull and RH J HouwenldquoFIC1 disease A spectrumof intrahepatic cholestatic disordersrdquoSeminars in Liver Disease vol 21 no 4 pp 535ndash544 2001
[48] A Miyahawa-Hayashino H Egawa T Yorifuji et al ldquoAllograftsteatohepatitis in progressive familial intrahepatic cholestasistype 1 after living donor liver transplantationrdquo Liver Transplan-tation vol 15 no 6 pp 610ndash618 2009
[49] E Nicastro X Stephenne F Smets et al ldquoRecovery of graftsteatosis and protein-losing enteropathy after biliary diversionin a PFIC 1 liver transplanted childrdquo Pediatric Transplantationvol 16 no 5 pp E177ndashE182 2012
[50] K Evason K E Bove M J Finegold et al ldquoMorphologic find-ings in progressive familial intrahepatic cholestasis 2 (PFIC2)Correlation with genetic and immunohistochemical studiesrdquoThe American Journal of Surgical Pathology vol 35 no 5 pp687ndash696 2011
[51] S S Strautnieks L N Bull A S Knisely et al ldquoA gene encodinga liver-specific ABC transporter is mutated in progressivefamilial intrahepatic cholestasisrdquo Nature Genetics vol 20 no3 pp 233ndash238 1998
[52] A S Knisely S S Strautnieks Y Meier et al ldquoHepatocellularcarcinoma in ten children under five years of age with bile saltexport pumpdeficiencyrdquoHepatology vol 44 no 2 pp 478ndash4862006
[53] A O Scheimann S S Strautnieks A S Knisely J A Byrne RJ Thompson andM J Finegold ldquoMutations in Bile Salt ExportPump (ABCB11) in Two Children with Progressive FamilialIntrahepatic Cholestasis and Cholangiocarcinomardquo Journal ofPediatrics vol 150 no 5 pp 556ndash559 2007
[54] V Keitel M Burdelski Z Vojnisek L Schmitt D HaussingerandRKubitz ldquoDe novo bile salt transporter antibodies as a pos-sible cause of recurrent graft failure after liver transplantationA novel mechanism of cholestasisrdquo Hepatology vol 50 no 2pp 510ndash517 2009
[55] P Jara L Hierro P Martınez-Fernandez et al ldquoRecurrence ofbile salt export pump deficiency after liver transplantationrdquoTheNew England Journal of Medicine vol 361 no 14 pp 1359ndash13672009
[56] R Kubitz C Droge S Kluge et al ldquoAutoimmune BSEPDiseaseDisease Recurrence After Liver Transplantation for ProgressiveFamilial Intrahepatic Cholestasisrdquo Clinical Reviews in Allergy ampImmunology vol 48 no 2-3 pp 273ndash284 2015
[57] J Stindt S Kluge C Droge et al ldquoBile salt export pump-reactive antibodies form a polyclonal multi-inhibitoryresponse in antibody-induced bile salt export pump deficiencyrdquoHepatology vol 63 no 2 pp 524ndash537 2016
[58] E Jacquemin J M DeVree D Cresteil et al ldquoThe widespectrum of multidrug resistance 3 deficiency from neonatalcholestasis to cirrhosis of adulthoodrdquoGastroenterology vol 120no 6 pp 1448ndash1458 2001
[59] O Rosmorduc and R Poupon ldquoLow phospholipid associatedcholelithiasis association with mutation in the MDR3ABCB4generdquo Orphanet Journal of Rare Diseases vol 2 article 29 2007
Canadian Journal of Gastroenterology and Hepatology 11
[60] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoThe spectrum of liver diseases related to ABCB4 gene muta-tions Pathophysiology and clinical aspectsrdquo Seminars in LiverDisease vol 30 no 2 pp 134ndash146 2010
[61] DWendumV BarbuO Rosmorduc L Arrive J-F Flejou andR Poupon ldquoAspects of liver pathology in adult patients withMDR3ABCB4 gene mutationsrdquo Virchows Archiv vol 460 no3 pp 291ndash298 2012
[62] R P J Oude Elferink andC C Paulusma ldquoFunction and patho-physiological importance of ABCB4 (MDR3 P-glycoprotein)rdquoPflugers Archiv - European Journal of Physiology vol 453 no 5pp 601ndash610 2007
[63] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoProgressive familial intrahepatic cholestasisrdquo Clinical Pedi-atrics vol 51 pp 689ndash691 2012
[64] S Boga D Jain andM L Schilsky ldquoPresentation of progressivefamilial intrahepatic cholestasis type 3 mimicking wilson dis-ease molecular genetic diagnosis and response to treatmentrdquoPediatric Gastroenterology Hepatology amp Nutrition vol 18 no3 p 202 2015
[65] M Sambrotta S Strautnieks E Papouli et al ldquoMutationsin TJP2 cause progressive cholestatic liver diseaserdquo NatureGenetics vol 46 no 4 pp 326ndash328 2014
[66] M Sambrotta and R J Thompson ldquoMutations in TJP2 encod-ing zona occludens 2 and liver diseaserdquo Tissue Barriers vol 3no 3 Article ID e1026537 2015
[67] S Zhou P M Hertel M J Finegold et al ldquoHepatocellularcarcinoma associated with tight-junction protein 2 deficiencyrdquoHepatology vol 62 no 6 pp 1914ndash1916 2015
[68] V EH Carlton B ZHarris E G Puffenberger et al ldquoComplexinheritance of familial hypercholanemia with associated muta-tions in TJP2 and BAATrdquo Nature Genetics vol 34 no 1 pp 91ndash96 2003
[69] N Gomez-Ospina C J Potter R Xiao et al ldquoMutations inthe nuclear bile acid receptor FXR cause progressive familialintrahepatic cholestasisrdquoNature Communications vol 7 ArticleID 10713 2016
[70] I Koutsounas S Theocharis I Delladetsima E Patsouris andC Giaginis ldquoFarnesoid x receptor in human metabolism anddisease the interplay between gene polymorphisms clinicalphenotypes and disease susceptibilityrdquo Expert Opinion on DrugMetabolism amp Toxicology vol 11 no 4 pp 523ndash532 2015
[71] S W C van Mil A Milona P H Dixon et al ldquoFunctionalVariants of the Central Bile Acid Sensor FXR Identified inIntrahepatic Cholestasis of Pregnancyrdquo Gastroenterology vol133 no 2 pp 507ndash516 2007
[72] C Droge M Bonus U Baumann et al ldquoSequencing of FIC1BSEP and MDR3 in a large cohort of patients with cholestasisrevealed a high number of different genetic variantsrdquo Journal ofHepatology vol 67 no 6 pp 1253ndash1264 2017
[73] L N Bull V E H Carlton N L Stricker et al ldquoGeneticand morphological findings in progressive familial intrahepaticcholestasis (Byler disease [PFIC-1] and Byler syndrome) Evi-dence for heterogeneityrdquo Hepatology vol 26 no 1 pp 155ndash1641997
[74] S W C Van Mil W L Van Der Woerd G Van Der Brugge etal ldquoBenign recurrent intrahepatic cholestasis type 2 is causedby mutations in ABCB11rdquo Gastroenterology vol 127 no 2 pp379ndash384 2004
[75] N A M Van Ooteghem L W J Klomp G P Van Berge-Henegouwen andRH JHouwen ldquoBenign recurrent intrahep-atic cholestasis progressing to progressive familial intrahepatic
cholestasis Low GGT cholestasis is a clinical continuumrdquoJournal of Hepatology vol 36 no 3 pp 439ndash443 2002
[76] F Balsells R Wyllie R Steffen and M Kay ldquoBenign recurrentintrahepatic cholestasis Improvement of pruritus and shorten-ing of the symptomatic phase with rifampin therapy A casereportrdquo Clinical Pediatrics vol 36 no 8 pp 483ndash485 1997
[77] U Beuers M Trauner P Jansen and R Poupon ldquoNewparadigms in the treatment of hepatic cholestasis FromUDCAto FXR PXR and beyondrdquo Journal of Hepatology vol 62 no 1pp S25ndashS37 2015
[78] L Bachs A Pares M Elena C Piera and J Rodes ldquoEffectsof long-term rifampicin administration in primary biliarycirrhosisrdquoGastroenterology vol 102 no 6 pp 2077ndash2080 1992
[79] J M Stapelbroek K J Van Erpecum L W J Klomp et alldquoNasobiliary drainage induces long-lasting remission in benignrecurrent intrahepatic cholestasisrdquoHepatology vol 43 no 1 pp51ndash53 2006
[80] F Lammert H-U Marschall A Glantz and S MaternldquoIntrahepatic cholestasis of pregnancymolecular pathogenesisdiagnosis and managementrdquo Journal of Hepatology vol 33 no6 pp 1012ndash1021 2000
[81] P H Dixon and C Williamson ldquoThe pathophysiology ofintrahepatic cholestasis of pregnancyrdquo Clinics and Research inHepatology and Gastroenterology vol 40 no 2 pp 141ndash1532016
[82] M G Martineau C Raker P H Dixon et al ldquoThe metabolicprofile of intrahepatic cholestasis of pregnancy is associatedwith impaired glucose tolerance dyslipidemia and increasedfetal growthrdquo Diabetes Care vol 38 no 2 pp 243ndash248 2015
[83] D G Goulis I A LWalkerMDe Swiet CWG Redman andC Williamson ldquoPreeclampsia with Abnormal Liver FunctionTests Is Associated with Cholestasis in a Subgroup of CasesrdquoHypertension in Pregnancy vol 23 no 1 pp 19ndash27 2004
[84] A Glantz H-U Marschall F Lammert and L-A MattssonldquoIntrahepatic cholestasis of pregnancy A randomized con-trolled trial comparing dexamethasone and ursodeoxycholicacidrdquo Hepatology vol 42 no 6 pp 1399ndash1405 2005
[85] R Zapata L Sandoval J Palma et al ldquoUrsodeoxycholic acidin the treatment of intrahepatic cholestasis of pregnancy A 12-year experiencerdquo Liver International vol 25 no 3 pp 548ndash5542005
[86] T Binder P Salaj T Zima and L Vıtek ldquoRandomized prospec-tive comparative study of ursodeoxycholic acid and S-adenosyl-L-methionine in the treatment of intrahepatic cholestasis ofpregnancyrdquo Journal of PerinatalMedicine vol 34 no 5 pp 383ndash391 2006
[87] P H Dixon N Weerasekera K J Linton et al ldquoHeterozy-gous MDR3 missense mutation associated with intrahepaticcholestasis of pregnancy Evidence for a defect in proteintraffickingrdquo Human Molecular Genetics vol 9 no 8 pp 1209ndash1217 2000
[88] C Gendrot Y Bacq M-C Brechot J Lansac and C AndresldquoA second heterozygous MDR3 nonsense mutation associatedwith intrahepatic cholestasis of pregnancyrdquo Journal of MedicalGenetics vol 40 no 3 article e32 2003
[89] A Floreani I Carderi D Paternoster et al ldquoIntrahepaticcholestasis of pregnancy Three novel MDR3 gene mutationsrdquoAlimentary Pharmacology amp Therapeutics vol 23 no 11 pp1649ndash1653 2006
[90] J N Painter M Savander A Ropponen et al ldquoSequencevariation in the ATP8B1 gene and intrahepatic cholestasis of
12 Canadian Journal of Gastroenterology and Hepatology
pregnancyrdquo European Journal of Human Genetics vol 13 no 4pp 435ndash439 2005
[91] W L Van Der Woerd R H J Houwen and S F J Van DeGraaf ldquoCurrent and future therapies for inherited cholestaticliver diseasesrdquoWorld Journal of Gastroenterology vol 23 no 5pp 763ndash775 2017
[92] A Thebaut D Habes F Gottrand et al ldquoSertraline as an addi-tional treatment for cholestatic pruritus in childrenrdquo Journal ofPediatric Gastroenterology and Nutrition vol 64 no 3 pp 431ndash435 2017
[93] U Ołdakowska-Jedynak I JankowskaM Hartleb et al ldquoTreat-ment of pruritus with Prometheus dialysis and absorption sys-tem in a patient with benign recurrent intrahepatic cholestasisrdquoHepatology Research vol 44 no 10 pp E304ndashE308 2014
[94] L Cutillo M Najimi F Smets et al ldquoSafety of living-related liver transplantation for progressive familial intrahep-atic cholestasisrdquo Pediatric Transplantation vol 10 no 5 pp570ndash574 2006
[95] E Gonzales B Grosse B Schuller et al ldquoTargeted phar-macotherapy in progressive familial intrahepatic cholestasistype 2 Evidence for improvement of cholestasis with 4-phenylbutyraterdquo Hepatology vol 62 no 2 pp 558ndash566 2015
[96] E Gonzales and E Jacquemin ldquoMutation specific drug ther-apy for progressive familial or benign recurrent intrahepaticcholestasis A new tool in a near futurerdquo Journal of Hepatologyvol 53 no 2 pp 385ndash387 2010
[97] M Trauner C D Fuchs E Halilbasic and G PaumgartnerldquoNew therapeutic concepts in bile acid transport and signalingfor management of cholestasisrdquo Hepatology vol 65 no 4 pp1393ndash1404 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Canadian Journal of Gastroenterology and Hepatology 7
the apical domains of hepatocytes which is consistent withlow activity of GGT MDR3 expression on the other hand ismaintained [69]
Since FXR affects several metabolic pathways someNR1H4 variations may be associated with susceptibility tovarious human diseases NR1H4 single-nucleotide polymor-phisms seem to be correlated with differences in glucosehomeostasis gallstone formation ICP inflammatory boweldisease and several other disorders [70 71]
52 Benign Recurrent Intrahepatic Cholestasis (BRIC) BRICis a group of genetically heterogeneous autosomal recessivediseases characterised by intermittent episodes of cholesta-sis They are caused by mutations in the ATP8B1 and ABCB11genes (the same as in PFIC1 and PFIC2) and probably inat least one other as yet unidentified gene [72] Thereare two genetically characterised forms of BRIC BRIC1(Summerskill-Walshe-Tygstrup syndrome OMIM 243300)and BRIC2 (OMIM 605479) caused by partial deficiency inATP8B1 [39 73] and ABCB11 [74] respectively The diseasetypically manifests before the second decade of life but theage of the first manifestation can vary greatly The samevariability has been documented in the duration of cholestaticepisodes (several days to several months) and their intensityInfection or pregnancy may act as a triggering factor Theclinical manifestations include jaundice pruritus fatigueanorexia and steatorrhoea Increase of bilirubin and BS levelsin serum has been observed during cholestatic attacks butGGT activity and serum cholesterol levels tend to be normalAminotransferase activity is usually normal or only slightlyelevated while biochemical parameters fall within normalranges Liver biopsies performed during cholestatic attackshave demonstrated hepatocanalicular cholestasis withoutfibrosis During the asymptomatic period the histologicalpicture is completely normal Since canalicular expression ofBSEP protein in hepatocytes is mostly maintained immuno-histology is of limited significance in these cases Diagnosisof BRIC1 and BRIC2 is based on demonstrating evidence ofmutations in both alleles of the corresponding genesATP8B1and ABCB11
While mutations causing PFIC are often located in theconserved regions of the genes that encode conserved func-tional domains of the corresponding proteins mutations inBRIC only partially impact protein function and expressionHowever several cases of initially benign episodic cholestasisthat have subsequently transitioned to a persistent progres-sive form of the disease have been reported [75] Thus BRICand PFIC seem to represent two extremes of a continuousspectrum of phenotypes of the one disease
The administration of statins corticosteroids cholestyra-mine or ursodeoxycholic acid (UDCA) is usually not veryeffective in BRIC patients Improvement of pruritus andshortening of symptomatic phase has been described inBRIC patients treated with the antibiotic rifampicin a potenthuman activator of PXR [76 77] However severe hepa-totoxicity after long-term administration of rifampicin hasbeen reported in patients with cholestatic disorders [77 78]Nasobiliary drainage seems to have a prompt effect during
cholestatic episodes but the mechanism of action remainsunclear [79]
53 Intrahepatic Cholestasis of Pregnancy (ICP) ICP (OMIM147480) also known as obstetric cholestasis is characterisedby cholestasis and prurituswith onset in pregnancy usually inthe third trimester It is associated with abnormal liverfunction in the absence of other liver diseases and resolvescompletely after delivery [80 81]The incidence of ICP varieswith geographical location and ethnicity Seasonal variationsindicate higher incidence in winter months as reported insome countries and it more commonly occurs in associationwith multiple pregnancies and following in vitro fertilisationIn Europe ICP affects about 1 of all pregnancies [81] Atypical symptom is intense pruritus commonly localised inthe palms and the soles which progresses during pregnancyElevated levels of serum BS and increased liver aminotrans-ferase activity are typical laboratory findings in such casesIncreased serum bilirubin levels have been observed in asmall proportion of cases while jaundice only rarely occursin affected women [81]
ICP usually resolves soon after delivery Although thedisease is considered relatively benign for themother there isan increased rate of adverse foetal outcomes including foetaldistress foetal asphyxia stillbirth or even intrauterine deathall known complications of ICP [81 82] ICPmay also be asso-ciated with an abnormalmetabolic profile in afflictedwomenespecially higher prevalence of dyslipidaemia impaired glu-cose tolerance and maternal comorbidities eg gestationaldiabetes and preeclampsia [82 83] Administration of UDCAimproves clinical symptoms predominantly pruritus andmay even reduce the risk of premature birth [84ndash86]
Mutations in ABCB4 ABCB11 and ATP8B1 have beenidentified in some patients suffering from ICP [87ndash90]Additionally variations in NR1H4 may be implicated in ICPpossibly via downregulation of BSEP expression [71]
6 Conclusions and Perspectives
Identification of the genes involved in hereditary cholestasishas advanced our understanding of the molecular mecha-nisms behind bile formation and transport
Recently mutations in TJP2 and NR1H4 have been foundin patients with apparent BSEP deficiency normal serumGGT activity and no mutations in ABCB11 However thereare rare cases of genetic cholestasis causes of which haveyet to be identified Therefore it seems likely that other yetunidentified genes involved in secretion andor transport ofcholephiles may be responsible for FIC-like phenotypes
Current therapeutic regimens in FIC patients compriseboth nonsurgical and surgical approaches Nonsurgical ther-apy includes drugs predominantly UDCA and rifampicinand nasobiliary drainage the latter being predominantly usedin BRIC patients with intractable pruritus during long-lastingcholestatic episodes [76 77 79] However the mechanismresponsible for the instant and complete relief from pruritusis still unclear
In addition to cholestyramine phenobarbital S-adeno-sylmethionine opiate antagonists UDCA rifampicin and
8 Canadian Journal of Gastroenterology and Hepatology
serotonin antagonists and its reuptake inhibitors seem to bebeneficial in managing refractory pruritus in patients withPFIC [77 91 92] Furthermore clinical and biochemicalimprovements have been observed in BRIC patients withintractable pruritus after using the molecular adsorbentrecirculating system (MARS) and the Prometheus system anextracorporeal liver support therapy based on fractionatedplasma separation and adsorption [93]
Surgical therapies include partial biliary diversion iemechanical interruption of BS enterohepatic circulation inorder to prevent reabsorption of pruritogens (unidentifiedthus far) and their precursors which is primarily usefulin noncirrhotic children with low-GGT PFIC permanentcholestasis andor intense refractory pruritus and orthotopicLTX which is still the ultimate treatment modality for manyPFIC patients [91] However as well as the risks associatedwith these invasive procedures other serious postoperative-related complications have been reported particularly inPFIC1 patients with extradigestive symptoms which canpersist or even worsen most likely due to extrahepaticexpression of FIC1 [47]Moreover the development of steato-sis and steatohepatitis leading to progressive liver allograftfibrosis in PFIC1 patients [48] and recurrence of the PFIC2phenotype in ABCB11 deficiency may represent other seriouscomplications after LTX and for some patients may evennecessitate retransplantation [54ndash57]
Importantly because of the shortage of cadaveric donorsparental living-related LTX is often considered in PFICpatients As heterozygous conditions can cause mild-to-moderate disease expression under certain circumstancesthe use of blood relatives as donors is seen as controversial Insuch cases it is likely that the heterozygous status of the donorallograft could pose a risk of complications during the lateposttransplant period such as lithiasis or cholestasis whichcan be precipitated by infections or by drugs administeredto the patient However the results of a recent study indicatethat the PFIC heterozygote status of the organ donor does notincrease the risk of liver dysfunction [94]
The limited effectiveness of current conservative proce-dures along with the complications of invasive methods par-ticularly LTX stress the need for the development and intro-duction of new treatment options Total biliary diversionpharmacological diversion of BS and hepatocyte transplanta-tion as well as gene- and mutation-targeted pharmacothera-pies represent promising future therapeutic approaches Thelatter two methods provide the basis for personalised treat-ment strategies in FIC patients Pharmacological chaperones(eg 4-phenylbutyrate) agonists of nuclear receptors (egstatins fibrates 6-ethyl chenodeoxycholic acid) endoplasmicreticulum-associated degradation inhibitors (MG132) andseveral other mutation-specific drugs can be used to increasethe expression of functional proteins and mitigate or eveneliminate deficient phenotypes [95ndash97]
Nevertheless despite the indisputable progress in thetherapy of FIC patients the increased risks of hepatobiliarymalignancies particularly in relation to ABCB11 deficiencystill remain serious life-threatening complications Furtherstudies are required in order to elucidate the complex patho-genesis of cholestasis unlock the mechanism of cholestatic
pruritus and improve the clinical management of bothhereditary and acquired cholestatic liver diseases
Abbreviations
ABC ATP-binding cassette subfamilyABCB4 ATP-binding cassette subfamily B
member 4ABCB11 ATP-binding cassette subfamily B
member 11AIBD Autoimmune BSEP DiseaseASBT Apical sodium-dependent bile acid
transporterATP8B1 ATPase aminophospholipid transporter
class I type 8B member 1BRIC Benign Recurrent Intrahepatic CholestasisBS Bile saltsBSEP Bile salt export pumpCYP7A1 Cholesterol 7 alpha-hydroxylaseCYP27A1 Sterol-27 hydroxylaseFGF19 Fibroblast growth factor 19FGFR4 Fibroblast growth factor receptor 4FIC Familial intrahepatic cholestasisFXR Farnesoid X-activated receptorGGT rsaquo-Glutamyl transferaseHNF4120572 Hepatocyte nuclear factor 4120572IBABP Intestinal bile acid-binding proteinICP Intrahepatic cholestasis of pregnancyIR-1 Inverted repeat DNA element with 1
nucleotide spacingLPAC Low Phospholipid-Associated
Cholelithiasis SyndromeLTX Liver allograft transplantationLXR Liver X receptorMDR3 Multidrug resistance protein 3MRP Multidrug resistance-associated proteinNR1H4 Nuclear receptor subfamily 1 group H
member 4NTCP Na+-taurocholate cotransporting
polypeptidesolute carrier family 10member 1
OATP Organic anion-transporting polypeptideOMIM Electronic database Online Mendelian
Inheritance in ManTMOST Organic solute transporterPFIC Progressive Familial Intrahepatic
CholestasisPXR Pregnane X receptorRXR Retinoid X receptorSHP Small heterodimer partnerSLC22A Solute carrier family 22 (organic cation
transporter) member 1SLCO Solute carrier organic anion transporter
familyTJP2 Tight junction protein 2 zona occludens-2UDCA Ursodeoxycholic acidUGT2B4 Uridine
51015840-diphosphate-glucuronosyltransferase2B4
Canadian Journal of Gastroenterology and Hepatology 9
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
Milan Jirsa was supported by Ministry of Health CzechRepublicmdashConceptual Development of Research Organiza-tion (ldquoInstitute for Clinical and Experimental MedicinendashIKEM IN 00023001rdquo)
References
[1] N B Javitt ldquoBile acid synthesis from cholesterol regulatory andauxiliary pathwaysrdquoThe FASEB Journal vol 8 no 15 pp 1308ndash1311 1994
[2] J Y L Chiang ldquoBile acids regulation of synthesisrdquo Journal ofLipid Research vol 50 no 10 pp 1955ndash1966 2009
[3] J L Boyer ldquoBile formation and secretionrdquo ComprehensivePhysiology vol 3 no 3 pp 1035ndash1078 2013
[4] B Hagenbuch and P J Meier ldquoSinusoidal (basolateral) bile saltuptake systems of hepatocytesrdquo Seminars in Liver Disease vol16 no 2 pp 129ndash136 1996
[5] B Hagenbuch B Stieger M Foguet H Lubbert and P JMeier ldquoFunctional expression cloning and characterization ofthe hepatocyte Na+bile acid cotransport systemrdquo Proceedingsof the National Acadamy of Sciences of the United States ofAmerica vol 88 no 23 pp 10629ndash10633 1991
[6] F M Vaz C C Paulusma H Huidekoper et al ldquoSodiumtaurocholate cotransporting polypeptide (SLC10A1) deficiencyConjugated hypercholanemia without a clear clinical pheno-typerdquo Hepatology vol 61 no 1 pp 260ndash267 2015
[7] B Hagenbuch and P J Meier ldquoOrganic anion transportingpolypeptides of the OATPSLC21 family Phylogenetic classi-fication as OATPSLCO super-family new nomenclature andmolecularfunctional propertiesrdquo Pflugers Archiv - EuropeanJournal of Physiology vol 447 no 5 pp 653ndash665 2004
[8] B Hagenbuch and B Stieger ldquoThe SLCO (former SLC21)superfamily of transportersrdquoMolecular Aspects of Medicine vol34 no 2-3 pp 396ndash412 2013
[9] M Muller and P L M Jansen ldquoThe secretory function ofthe liver New aspects of hepatobiliary transportrdquo Journal ofHepatology vol 28 no 2 pp 344ndash354 1998
[10] G J E J Hooiveld J E Van Montfoort D K F Meijerand M Muller ldquoFunction and regulation of ATP-bindingcassette transport proteins involved in hepatobiliary transportrdquoEuropean Journal of Pharmaceutical Sciences vol 12 no 4 pp525ndash543 2001
[11] J Konig D Rost Y Cui and D Keppler ldquoCharacterizationof the human multidrug resistance protein isoform MRP3localized to the basolateral hepatocyte membranerdquoHepatologyvol 29 no 4 pp 1156ndash1163 1999
[12] H Zeng G Liu P A Rea and G D Kruh ldquoTransport ofamphipathic anions by human multidrug resistance protein 3rdquoCancer Research vol 60 pp 4779ndash4784 2000
[13] Y-M A Lee Y Cui J Konig et al ldquoIdentification and func-tional characterization of the natural variantMRP3-Arg1297Hisof human multidrug resistance protein 3 (MRP3ABCC3)rdquoPharmacogenetics vol 14 no 4 pp 213ndash223 2004
[14] M Donner ldquoUp-regulation of basolateral multidrug resistanceprotein 3 (Mrp3) in cholestatic rat liverrdquoHepatology vol 34 no2 pp 351ndash359 2001
[15] M L Ruiz J P Rigalli A Arias et al ldquoInduction of hepaticmultidrug resistance-associated protein 3 by ethynylestradiol isindependent of cholestasis and mediated by estrogen receptorrdquoDrug Metabolism and Disposition vol 41 no 2 pp 275ndash2802013
[16] N J Cherrington D P Hartley N Li D R Johnson and C DKlaassen ldquoOrgan distribution of multidrug resistance proteins1 2 and 3 (Mrp1 2 and 3) mRNA and hepatic induction ofMrp3 by constitutive androstane receptor activators in ratsrdquoTheJournal of Pharmacology and Experimental Therapeutics vol300 no 1 pp 97ndash104 2002
[17] C A Ritter G Jedlitschky H Meyer Zu Schwabedissen MGrube K Kock and H K Kroemer ldquoCellular export ofdrugs and signaling molecules by the ATP-binding cassettetransporters MRP4 (ABCC4) and MRP5 (ABCC5)rdquo DrugMetabolism Reviews vol 37 no 1 pp 253ndash278 2005
[18] F G M Russel J B Koenderink and R Masereeuw ldquoMul-tidrug resistance protein 4 (MRP4ABCC4) a versatile effluxtransporter for drugs and signalling moleculesrdquo Trends inPharmacological Sciences vol 29 no 4 pp 200ndash207 2008
[19] D Keppler ldquoProgress in the molecular characterization ofhepatobiliary transportersrdquoDigestive Diseases vol 35 no 3 pp197ndash202 2017
[20] V Keitel M Burdelski U Warskulat et al ldquoExpression andlocalization of hepatobiliary transport proteins in progressivefamilial intrahepatic cholestasisrdquo Hepatology vol 41 no 5 pp1160ndash1172 2005
[21] N Ballatori F FangWV Christian N Li andC LHammondldquoOst120572-Ost120573 is required for bile acid and conjugated steroiddisposition in the intestine kidney and liverrdquoAmerican Journalof Physiology-Gastrointestinal and Liver Physiology vol 295 no1 pp G179ndashG186 2008
[22] J L Boyer M Trauner A Mennone et al ldquoUpregulationof a basolateral FXR-dependent bile acid efflux transporterOSTalpha-OSTbeta in cholestasis in humans and rodentsrdquoAmerican Journal of Physiology-Gastrointestinal and Liver Phys-iology vol 290 no 6 pp G1124ndashG1130 2006
[23] T Gerloff B Stieger B Hagenbuch et al ldquoThe sister of P-glycoprotein represents the canalicular bile salt export pump ofmammalian liverrdquoThe Journal of Biological Chemistry vol 273no 16 pp 10046ndash10050 1998
[24] A M van der Bliek F Baas T Ten Houte de Lange P MKooiman T van der Velde-Koerts and P Borst ldquoThe humanmdr3 gene encodes a novel P-glycoprotein homologue and givesrise to alternatively splicedmRNAs in liverrdquo EMBO Journal vol6 no 11 pp 3325ndash3331 1987
[25] A J Smith J L Timmermans-Hereijgers and B RoelofsenldquoThe human MDR3 P-glycoprotein promotes translocation ofphosphatidylcholine through the plasma membrane of fibrob-lasts from transgenic micerdquo FEBS Letters vol 354 no 3 pp263ndash266 1994
[26] J M L de Vree E Jacquemin E Sturm et al ldquoMutations in theMDR3 gene cause progressive familial intrahepatic cholestasisrdquoProceedings of the National Acadamy of Sciences of the UnitedStates of America vol 95 no 1 pp 282ndash287 1998
[27] A Groen M R Romero C Kunne et al ldquoComplementaryfunctions of the flippase ATP8B1 and the floppase ABCB4 inmaintaining canalicular membrane integrityrdquoGastroenterologyvol 141 no 5 pp 1927ndash1937 2011
10 Canadian Journal of Gastroenterology and Hepatology
[28] P A Dawson T Lan and A Rao ldquoThematic review series Bileacids Bile acid transportersrdquo Journal of Lipid Research vol 50no 12 pp 2340ndash2357 2009
[29] E Halilbasic T Claudel andM Trauner ldquoBile acid transportersand regulatory nuclear receptors in the liver and beyondrdquoJournal of Hepatology vol 58 no 1 pp 155ndash168 2013
[30] B L Shneider ldquoIntestinal bile acid transport Biology physiol-ogy and pathophysiologyrdquo Journal of Pediatric Gastroenterologyand Nutrition vol 32 no 4 pp 407ndash417 2001
[31] T Claudel G Zollner M Wagner and M Trauner ldquoRoleof nuclear receptors for bile acid metabolism bile secretioncholestasis and gallstone diseaserdquoBiochimica et Biophysica Acta(BBA) - Molecular Basis of Disease vol 1812 no 8 pp 867ndash8782011
[32] J J Eloranta and G A Kullak-Ublick ldquoThe role of FXR indisorders of bile acid homeostasisrdquo Physiology Journal vol 23no 5 pp 286ndash295 2008
[33] B Goodwin S A Jones R R Price et al ldquoA regulatory cascadeof the nuclear receptors FXR SHP-1 and LRH-1 represses bileacid biosynthesisrdquo Molecular Cell vol 6 no 3 pp 517ndash5262000
[34] M Muller P L M Jansen K N Faber et al ldquoFarnesoid Xreceptor and bile salts are involved in transcriptional regulationof the gene encoding the human bile salt export pumprdquoHepatology vol 35 no 3 pp 589ndash596 2002
[35] M Ananthanarayanan N BalasubramanianMMakishima DJ Mangelsdorf and F J Suchy ldquoHuman bile salt export pumppromoter is transactivated by the farnesoid X receptorbile acidreceptorrdquo The Journal of Biological Chemistry vol 276 no 31pp 28857ndash28865 2001
[36] L Huang A Zhao J L Lew et al ldquoFarnesoid X receptoractivates transcription of the phospholipid pump MDR3rdquo TheJournal of Biological Chemistry vol 278 no 51 pp 51085ndash510902003
[37] M Wagner G Zollner and M Trauner ldquoNuclear receptorregulation of the adaptive response of bile acid transporters incholestasisrdquo Seminars in Liver Disease vol 30 no 2 pp 160ndash1772010
[38] Y Zhang H R Kast-Woelbern and P A Edwards ldquoNaturalstructural variants of the nuclear receptor farnesoid X recep-tor affect transcriptional activationrdquo The Journal of BiologicalChemistry vol 278 no 1 pp 104ndash110 2003
[39] SW C VanMil R H J Houwen and LW J Klomp ldquoGeneticsof familial intrahepatic cholestasis syndromesrdquo Journal of Med-ical Genetics vol 42 no 6 pp 449ndash463 2005
[40] V E H Carlton L Pawlikowska and L N Bull ldquoMolecularbasis of intrahepatic cholestasisrdquoAnnals ofMedicine vol 36 no8 pp 606ndash617 2004
[41] R J Clayton F L Iber B H Ruebner and V A MckusickldquoByler Disease Fatal Familial Intrahepatic Cholestasis in anAmish Kindredrdquo American Journal of Diseases of Children vol117 no 1 pp 112ndash124 1969
[42] E Jacquemin ldquoProgressive familial intrahepatic cholestasisrdquoClinics andResearch inHepatology andGastroenterology vol 36supplement 1 pp S26ndashS35 2012
[43] L N Bull M J T Van Eijk L Pawlikowska et al ldquoA geneencoding a P-type ATPase mutated in two forms of hereditarycholestasisrdquo Nature Genetics vol 18 no 3 pp 219ndash224 1998
[44] L W J Klomp J C Vargas S W C Van Mil et al ldquoCharac-terization of mutations in ATP8B1 associated with hereditarycholestasisrdquo Hepatology vol 40 no 1 pp 27ndash38 2004
[45] P Ujhazy D Ortiz S Misra et al ldquoFamilial intrahepaticcholestasis 1 Studies of localization and functionrdquo Hepatologyvol 34 no 4 I pp 768ndash775 2001
[46] C C Paulusma A Groen C Kunne et al ldquoAtp8b1 deficiencyin mice reduces resistance of the canalicular membrane tohydrophobic bile salts and impairs bile salt transportrdquo Hepatol-ogy vol 44 no 1 pp 195ndash204 2006
[47] SW C VanMil LW J Klomp L N Bull and RH J HouwenldquoFIC1 disease A spectrumof intrahepatic cholestatic disordersrdquoSeminars in Liver Disease vol 21 no 4 pp 535ndash544 2001
[48] A Miyahawa-Hayashino H Egawa T Yorifuji et al ldquoAllograftsteatohepatitis in progressive familial intrahepatic cholestasistype 1 after living donor liver transplantationrdquo Liver Transplan-tation vol 15 no 6 pp 610ndash618 2009
[49] E Nicastro X Stephenne F Smets et al ldquoRecovery of graftsteatosis and protein-losing enteropathy after biliary diversionin a PFIC 1 liver transplanted childrdquo Pediatric Transplantationvol 16 no 5 pp E177ndashE182 2012
[50] K Evason K E Bove M J Finegold et al ldquoMorphologic find-ings in progressive familial intrahepatic cholestasis 2 (PFIC2)Correlation with genetic and immunohistochemical studiesrdquoThe American Journal of Surgical Pathology vol 35 no 5 pp687ndash696 2011
[51] S S Strautnieks L N Bull A S Knisely et al ldquoA gene encodinga liver-specific ABC transporter is mutated in progressivefamilial intrahepatic cholestasisrdquo Nature Genetics vol 20 no3 pp 233ndash238 1998
[52] A S Knisely S S Strautnieks Y Meier et al ldquoHepatocellularcarcinoma in ten children under five years of age with bile saltexport pumpdeficiencyrdquoHepatology vol 44 no 2 pp 478ndash4862006
[53] A O Scheimann S S Strautnieks A S Knisely J A Byrne RJ Thompson andM J Finegold ldquoMutations in Bile Salt ExportPump (ABCB11) in Two Children with Progressive FamilialIntrahepatic Cholestasis and Cholangiocarcinomardquo Journal ofPediatrics vol 150 no 5 pp 556ndash559 2007
[54] V Keitel M Burdelski Z Vojnisek L Schmitt D HaussingerandRKubitz ldquoDe novo bile salt transporter antibodies as a pos-sible cause of recurrent graft failure after liver transplantationA novel mechanism of cholestasisrdquo Hepatology vol 50 no 2pp 510ndash517 2009
[55] P Jara L Hierro P Martınez-Fernandez et al ldquoRecurrence ofbile salt export pump deficiency after liver transplantationrdquoTheNew England Journal of Medicine vol 361 no 14 pp 1359ndash13672009
[56] R Kubitz C Droge S Kluge et al ldquoAutoimmune BSEPDiseaseDisease Recurrence After Liver Transplantation for ProgressiveFamilial Intrahepatic Cholestasisrdquo Clinical Reviews in Allergy ampImmunology vol 48 no 2-3 pp 273ndash284 2015
[57] J Stindt S Kluge C Droge et al ldquoBile salt export pump-reactive antibodies form a polyclonal multi-inhibitoryresponse in antibody-induced bile salt export pump deficiencyrdquoHepatology vol 63 no 2 pp 524ndash537 2016
[58] E Jacquemin J M DeVree D Cresteil et al ldquoThe widespectrum of multidrug resistance 3 deficiency from neonatalcholestasis to cirrhosis of adulthoodrdquoGastroenterology vol 120no 6 pp 1448ndash1458 2001
[59] O Rosmorduc and R Poupon ldquoLow phospholipid associatedcholelithiasis association with mutation in the MDR3ABCB4generdquo Orphanet Journal of Rare Diseases vol 2 article 29 2007
Canadian Journal of Gastroenterology and Hepatology 11
[60] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoThe spectrum of liver diseases related to ABCB4 gene muta-tions Pathophysiology and clinical aspectsrdquo Seminars in LiverDisease vol 30 no 2 pp 134ndash146 2010
[61] DWendumV BarbuO Rosmorduc L Arrive J-F Flejou andR Poupon ldquoAspects of liver pathology in adult patients withMDR3ABCB4 gene mutationsrdquo Virchows Archiv vol 460 no3 pp 291ndash298 2012
[62] R P J Oude Elferink andC C Paulusma ldquoFunction and patho-physiological importance of ABCB4 (MDR3 P-glycoprotein)rdquoPflugers Archiv - European Journal of Physiology vol 453 no 5pp 601ndash610 2007
[63] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoProgressive familial intrahepatic cholestasisrdquo Clinical Pedi-atrics vol 51 pp 689ndash691 2012
[64] S Boga D Jain andM L Schilsky ldquoPresentation of progressivefamilial intrahepatic cholestasis type 3 mimicking wilson dis-ease molecular genetic diagnosis and response to treatmentrdquoPediatric Gastroenterology Hepatology amp Nutrition vol 18 no3 p 202 2015
[65] M Sambrotta S Strautnieks E Papouli et al ldquoMutationsin TJP2 cause progressive cholestatic liver diseaserdquo NatureGenetics vol 46 no 4 pp 326ndash328 2014
[66] M Sambrotta and R J Thompson ldquoMutations in TJP2 encod-ing zona occludens 2 and liver diseaserdquo Tissue Barriers vol 3no 3 Article ID e1026537 2015
[67] S Zhou P M Hertel M J Finegold et al ldquoHepatocellularcarcinoma associated with tight-junction protein 2 deficiencyrdquoHepatology vol 62 no 6 pp 1914ndash1916 2015
[68] V EH Carlton B ZHarris E G Puffenberger et al ldquoComplexinheritance of familial hypercholanemia with associated muta-tions in TJP2 and BAATrdquo Nature Genetics vol 34 no 1 pp 91ndash96 2003
[69] N Gomez-Ospina C J Potter R Xiao et al ldquoMutations inthe nuclear bile acid receptor FXR cause progressive familialintrahepatic cholestasisrdquoNature Communications vol 7 ArticleID 10713 2016
[70] I Koutsounas S Theocharis I Delladetsima E Patsouris andC Giaginis ldquoFarnesoid x receptor in human metabolism anddisease the interplay between gene polymorphisms clinicalphenotypes and disease susceptibilityrdquo Expert Opinion on DrugMetabolism amp Toxicology vol 11 no 4 pp 523ndash532 2015
[71] S W C van Mil A Milona P H Dixon et al ldquoFunctionalVariants of the Central Bile Acid Sensor FXR Identified inIntrahepatic Cholestasis of Pregnancyrdquo Gastroenterology vol133 no 2 pp 507ndash516 2007
[72] C Droge M Bonus U Baumann et al ldquoSequencing of FIC1BSEP and MDR3 in a large cohort of patients with cholestasisrevealed a high number of different genetic variantsrdquo Journal ofHepatology vol 67 no 6 pp 1253ndash1264 2017
[73] L N Bull V E H Carlton N L Stricker et al ldquoGeneticand morphological findings in progressive familial intrahepaticcholestasis (Byler disease [PFIC-1] and Byler syndrome) Evi-dence for heterogeneityrdquo Hepatology vol 26 no 1 pp 155ndash1641997
[74] S W C Van Mil W L Van Der Woerd G Van Der Brugge etal ldquoBenign recurrent intrahepatic cholestasis type 2 is causedby mutations in ABCB11rdquo Gastroenterology vol 127 no 2 pp379ndash384 2004
[75] N A M Van Ooteghem L W J Klomp G P Van Berge-Henegouwen andRH JHouwen ldquoBenign recurrent intrahep-atic cholestasis progressing to progressive familial intrahepatic
cholestasis Low GGT cholestasis is a clinical continuumrdquoJournal of Hepatology vol 36 no 3 pp 439ndash443 2002
[76] F Balsells R Wyllie R Steffen and M Kay ldquoBenign recurrentintrahepatic cholestasis Improvement of pruritus and shorten-ing of the symptomatic phase with rifampin therapy A casereportrdquo Clinical Pediatrics vol 36 no 8 pp 483ndash485 1997
[77] U Beuers M Trauner P Jansen and R Poupon ldquoNewparadigms in the treatment of hepatic cholestasis FromUDCAto FXR PXR and beyondrdquo Journal of Hepatology vol 62 no 1pp S25ndashS37 2015
[78] L Bachs A Pares M Elena C Piera and J Rodes ldquoEffectsof long-term rifampicin administration in primary biliarycirrhosisrdquoGastroenterology vol 102 no 6 pp 2077ndash2080 1992
[79] J M Stapelbroek K J Van Erpecum L W J Klomp et alldquoNasobiliary drainage induces long-lasting remission in benignrecurrent intrahepatic cholestasisrdquoHepatology vol 43 no 1 pp51ndash53 2006
[80] F Lammert H-U Marschall A Glantz and S MaternldquoIntrahepatic cholestasis of pregnancymolecular pathogenesisdiagnosis and managementrdquo Journal of Hepatology vol 33 no6 pp 1012ndash1021 2000
[81] P H Dixon and C Williamson ldquoThe pathophysiology ofintrahepatic cholestasis of pregnancyrdquo Clinics and Research inHepatology and Gastroenterology vol 40 no 2 pp 141ndash1532016
[82] M G Martineau C Raker P H Dixon et al ldquoThe metabolicprofile of intrahepatic cholestasis of pregnancy is associatedwith impaired glucose tolerance dyslipidemia and increasedfetal growthrdquo Diabetes Care vol 38 no 2 pp 243ndash248 2015
[83] D G Goulis I A LWalkerMDe Swiet CWG Redman andC Williamson ldquoPreeclampsia with Abnormal Liver FunctionTests Is Associated with Cholestasis in a Subgroup of CasesrdquoHypertension in Pregnancy vol 23 no 1 pp 19ndash27 2004
[84] A Glantz H-U Marschall F Lammert and L-A MattssonldquoIntrahepatic cholestasis of pregnancy A randomized con-trolled trial comparing dexamethasone and ursodeoxycholicacidrdquo Hepatology vol 42 no 6 pp 1399ndash1405 2005
[85] R Zapata L Sandoval J Palma et al ldquoUrsodeoxycholic acidin the treatment of intrahepatic cholestasis of pregnancy A 12-year experiencerdquo Liver International vol 25 no 3 pp 548ndash5542005
[86] T Binder P Salaj T Zima and L Vıtek ldquoRandomized prospec-tive comparative study of ursodeoxycholic acid and S-adenosyl-L-methionine in the treatment of intrahepatic cholestasis ofpregnancyrdquo Journal of PerinatalMedicine vol 34 no 5 pp 383ndash391 2006
[87] P H Dixon N Weerasekera K J Linton et al ldquoHeterozy-gous MDR3 missense mutation associated with intrahepaticcholestasis of pregnancy Evidence for a defect in proteintraffickingrdquo Human Molecular Genetics vol 9 no 8 pp 1209ndash1217 2000
[88] C Gendrot Y Bacq M-C Brechot J Lansac and C AndresldquoA second heterozygous MDR3 nonsense mutation associatedwith intrahepatic cholestasis of pregnancyrdquo Journal of MedicalGenetics vol 40 no 3 article e32 2003
[89] A Floreani I Carderi D Paternoster et al ldquoIntrahepaticcholestasis of pregnancy Three novel MDR3 gene mutationsrdquoAlimentary Pharmacology amp Therapeutics vol 23 no 11 pp1649ndash1653 2006
[90] J N Painter M Savander A Ropponen et al ldquoSequencevariation in the ATP8B1 gene and intrahepatic cholestasis of
12 Canadian Journal of Gastroenterology and Hepatology
pregnancyrdquo European Journal of Human Genetics vol 13 no 4pp 435ndash439 2005
[91] W L Van Der Woerd R H J Houwen and S F J Van DeGraaf ldquoCurrent and future therapies for inherited cholestaticliver diseasesrdquoWorld Journal of Gastroenterology vol 23 no 5pp 763ndash775 2017
[92] A Thebaut D Habes F Gottrand et al ldquoSertraline as an addi-tional treatment for cholestatic pruritus in childrenrdquo Journal ofPediatric Gastroenterology and Nutrition vol 64 no 3 pp 431ndash435 2017
[93] U Ołdakowska-Jedynak I JankowskaM Hartleb et al ldquoTreat-ment of pruritus with Prometheus dialysis and absorption sys-tem in a patient with benign recurrent intrahepatic cholestasisrdquoHepatology Research vol 44 no 10 pp E304ndashE308 2014
[94] L Cutillo M Najimi F Smets et al ldquoSafety of living-related liver transplantation for progressive familial intrahep-atic cholestasisrdquo Pediatric Transplantation vol 10 no 5 pp570ndash574 2006
[95] E Gonzales B Grosse B Schuller et al ldquoTargeted phar-macotherapy in progressive familial intrahepatic cholestasistype 2 Evidence for improvement of cholestasis with 4-phenylbutyraterdquo Hepatology vol 62 no 2 pp 558ndash566 2015
[96] E Gonzales and E Jacquemin ldquoMutation specific drug ther-apy for progressive familial or benign recurrent intrahepaticcholestasis A new tool in a near futurerdquo Journal of Hepatologyvol 53 no 2 pp 385ndash387 2010
[97] M Trauner C D Fuchs E Halilbasic and G PaumgartnerldquoNew therapeutic concepts in bile acid transport and signalingfor management of cholestasisrdquo Hepatology vol 65 no 4 pp1393ndash1404 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

8 Canadian Journal of Gastroenterology and Hepatology
serotonin antagonists and its reuptake inhibitors seem to bebeneficial in managing refractory pruritus in patients withPFIC [77 91 92] Furthermore clinical and biochemicalimprovements have been observed in BRIC patients withintractable pruritus after using the molecular adsorbentrecirculating system (MARS) and the Prometheus system anextracorporeal liver support therapy based on fractionatedplasma separation and adsorption [93]
Surgical therapies include partial biliary diversion iemechanical interruption of BS enterohepatic circulation inorder to prevent reabsorption of pruritogens (unidentifiedthus far) and their precursors which is primarily usefulin noncirrhotic children with low-GGT PFIC permanentcholestasis andor intense refractory pruritus and orthotopicLTX which is still the ultimate treatment modality for manyPFIC patients [91] However as well as the risks associatedwith these invasive procedures other serious postoperative-related complications have been reported particularly inPFIC1 patients with extradigestive symptoms which canpersist or even worsen most likely due to extrahepaticexpression of FIC1 [47]Moreover the development of steato-sis and steatohepatitis leading to progressive liver allograftfibrosis in PFIC1 patients [48] and recurrence of the PFIC2phenotype in ABCB11 deficiency may represent other seriouscomplications after LTX and for some patients may evennecessitate retransplantation [54ndash57]
Importantly because of the shortage of cadaveric donorsparental living-related LTX is often considered in PFICpatients As heterozygous conditions can cause mild-to-moderate disease expression under certain circumstancesthe use of blood relatives as donors is seen as controversial Insuch cases it is likely that the heterozygous status of the donorallograft could pose a risk of complications during the lateposttransplant period such as lithiasis or cholestasis whichcan be precipitated by infections or by drugs administeredto the patient However the results of a recent study indicatethat the PFIC heterozygote status of the organ donor does notincrease the risk of liver dysfunction [94]
The limited effectiveness of current conservative proce-dures along with the complications of invasive methods par-ticularly LTX stress the need for the development and intro-duction of new treatment options Total biliary diversionpharmacological diversion of BS and hepatocyte transplanta-tion as well as gene- and mutation-targeted pharmacothera-pies represent promising future therapeutic approaches Thelatter two methods provide the basis for personalised treat-ment strategies in FIC patients Pharmacological chaperones(eg 4-phenylbutyrate) agonists of nuclear receptors (egstatins fibrates 6-ethyl chenodeoxycholic acid) endoplasmicreticulum-associated degradation inhibitors (MG132) andseveral other mutation-specific drugs can be used to increasethe expression of functional proteins and mitigate or eveneliminate deficient phenotypes [95ndash97]
Nevertheless despite the indisputable progress in thetherapy of FIC patients the increased risks of hepatobiliarymalignancies particularly in relation to ABCB11 deficiencystill remain serious life-threatening complications Furtherstudies are required in order to elucidate the complex patho-genesis of cholestasis unlock the mechanism of cholestatic
pruritus and improve the clinical management of bothhereditary and acquired cholestatic liver diseases
Abbreviations
ABC ATP-binding cassette subfamilyABCB4 ATP-binding cassette subfamily B
member 4ABCB11 ATP-binding cassette subfamily B
member 11AIBD Autoimmune BSEP DiseaseASBT Apical sodium-dependent bile acid
transporterATP8B1 ATPase aminophospholipid transporter
class I type 8B member 1BRIC Benign Recurrent Intrahepatic CholestasisBS Bile saltsBSEP Bile salt export pumpCYP7A1 Cholesterol 7 alpha-hydroxylaseCYP27A1 Sterol-27 hydroxylaseFGF19 Fibroblast growth factor 19FGFR4 Fibroblast growth factor receptor 4FIC Familial intrahepatic cholestasisFXR Farnesoid X-activated receptorGGT rsaquo-Glutamyl transferaseHNF4120572 Hepatocyte nuclear factor 4120572IBABP Intestinal bile acid-binding proteinICP Intrahepatic cholestasis of pregnancyIR-1 Inverted repeat DNA element with 1
nucleotide spacingLPAC Low Phospholipid-Associated
Cholelithiasis SyndromeLTX Liver allograft transplantationLXR Liver X receptorMDR3 Multidrug resistance protein 3MRP Multidrug resistance-associated proteinNR1H4 Nuclear receptor subfamily 1 group H
member 4NTCP Na+-taurocholate cotransporting
polypeptidesolute carrier family 10member 1
OATP Organic anion-transporting polypeptideOMIM Electronic database Online Mendelian
Inheritance in ManTMOST Organic solute transporterPFIC Progressive Familial Intrahepatic
CholestasisPXR Pregnane X receptorRXR Retinoid X receptorSHP Small heterodimer partnerSLC22A Solute carrier family 22 (organic cation
transporter) member 1SLCO Solute carrier organic anion transporter
familyTJP2 Tight junction protein 2 zona occludens-2UDCA Ursodeoxycholic acidUGT2B4 Uridine
51015840-diphosphate-glucuronosyltransferase2B4
Canadian Journal of Gastroenterology and Hepatology 9
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
Milan Jirsa was supported by Ministry of Health CzechRepublicmdashConceptual Development of Research Organiza-tion (ldquoInstitute for Clinical and Experimental MedicinendashIKEM IN 00023001rdquo)
References
[1] N B Javitt ldquoBile acid synthesis from cholesterol regulatory andauxiliary pathwaysrdquoThe FASEB Journal vol 8 no 15 pp 1308ndash1311 1994
[2] J Y L Chiang ldquoBile acids regulation of synthesisrdquo Journal ofLipid Research vol 50 no 10 pp 1955ndash1966 2009
[3] J L Boyer ldquoBile formation and secretionrdquo ComprehensivePhysiology vol 3 no 3 pp 1035ndash1078 2013
[4] B Hagenbuch and P J Meier ldquoSinusoidal (basolateral) bile saltuptake systems of hepatocytesrdquo Seminars in Liver Disease vol16 no 2 pp 129ndash136 1996
[5] B Hagenbuch B Stieger M Foguet H Lubbert and P JMeier ldquoFunctional expression cloning and characterization ofthe hepatocyte Na+bile acid cotransport systemrdquo Proceedingsof the National Acadamy of Sciences of the United States ofAmerica vol 88 no 23 pp 10629ndash10633 1991
[6] F M Vaz C C Paulusma H Huidekoper et al ldquoSodiumtaurocholate cotransporting polypeptide (SLC10A1) deficiencyConjugated hypercholanemia without a clear clinical pheno-typerdquo Hepatology vol 61 no 1 pp 260ndash267 2015
[7] B Hagenbuch and P J Meier ldquoOrganic anion transportingpolypeptides of the OATPSLC21 family Phylogenetic classi-fication as OATPSLCO super-family new nomenclature andmolecularfunctional propertiesrdquo Pflugers Archiv - EuropeanJournal of Physiology vol 447 no 5 pp 653ndash665 2004
[8] B Hagenbuch and B Stieger ldquoThe SLCO (former SLC21)superfamily of transportersrdquoMolecular Aspects of Medicine vol34 no 2-3 pp 396ndash412 2013
[9] M Muller and P L M Jansen ldquoThe secretory function ofthe liver New aspects of hepatobiliary transportrdquo Journal ofHepatology vol 28 no 2 pp 344ndash354 1998
[10] G J E J Hooiveld J E Van Montfoort D K F Meijerand M Muller ldquoFunction and regulation of ATP-bindingcassette transport proteins involved in hepatobiliary transportrdquoEuropean Journal of Pharmaceutical Sciences vol 12 no 4 pp525ndash543 2001
[11] J Konig D Rost Y Cui and D Keppler ldquoCharacterizationof the human multidrug resistance protein isoform MRP3localized to the basolateral hepatocyte membranerdquoHepatologyvol 29 no 4 pp 1156ndash1163 1999
[12] H Zeng G Liu P A Rea and G D Kruh ldquoTransport ofamphipathic anions by human multidrug resistance protein 3rdquoCancer Research vol 60 pp 4779ndash4784 2000
[13] Y-M A Lee Y Cui J Konig et al ldquoIdentification and func-tional characterization of the natural variantMRP3-Arg1297Hisof human multidrug resistance protein 3 (MRP3ABCC3)rdquoPharmacogenetics vol 14 no 4 pp 213ndash223 2004
[14] M Donner ldquoUp-regulation of basolateral multidrug resistanceprotein 3 (Mrp3) in cholestatic rat liverrdquoHepatology vol 34 no2 pp 351ndash359 2001
[15] M L Ruiz J P Rigalli A Arias et al ldquoInduction of hepaticmultidrug resistance-associated protein 3 by ethynylestradiol isindependent of cholestasis and mediated by estrogen receptorrdquoDrug Metabolism and Disposition vol 41 no 2 pp 275ndash2802013
[16] N J Cherrington D P Hartley N Li D R Johnson and C DKlaassen ldquoOrgan distribution of multidrug resistance proteins1 2 and 3 (Mrp1 2 and 3) mRNA and hepatic induction ofMrp3 by constitutive androstane receptor activators in ratsrdquoTheJournal of Pharmacology and Experimental Therapeutics vol300 no 1 pp 97ndash104 2002
[17] C A Ritter G Jedlitschky H Meyer Zu Schwabedissen MGrube K Kock and H K Kroemer ldquoCellular export ofdrugs and signaling molecules by the ATP-binding cassettetransporters MRP4 (ABCC4) and MRP5 (ABCC5)rdquo DrugMetabolism Reviews vol 37 no 1 pp 253ndash278 2005
[18] F G M Russel J B Koenderink and R Masereeuw ldquoMul-tidrug resistance protein 4 (MRP4ABCC4) a versatile effluxtransporter for drugs and signalling moleculesrdquo Trends inPharmacological Sciences vol 29 no 4 pp 200ndash207 2008
[19] D Keppler ldquoProgress in the molecular characterization ofhepatobiliary transportersrdquoDigestive Diseases vol 35 no 3 pp197ndash202 2017
[20] V Keitel M Burdelski U Warskulat et al ldquoExpression andlocalization of hepatobiliary transport proteins in progressivefamilial intrahepatic cholestasisrdquo Hepatology vol 41 no 5 pp1160ndash1172 2005
[21] N Ballatori F FangWV Christian N Li andC LHammondldquoOst120572-Ost120573 is required for bile acid and conjugated steroiddisposition in the intestine kidney and liverrdquoAmerican Journalof Physiology-Gastrointestinal and Liver Physiology vol 295 no1 pp G179ndashG186 2008
[22] J L Boyer M Trauner A Mennone et al ldquoUpregulationof a basolateral FXR-dependent bile acid efflux transporterOSTalpha-OSTbeta in cholestasis in humans and rodentsrdquoAmerican Journal of Physiology-Gastrointestinal and Liver Phys-iology vol 290 no 6 pp G1124ndashG1130 2006
[23] T Gerloff B Stieger B Hagenbuch et al ldquoThe sister of P-glycoprotein represents the canalicular bile salt export pump ofmammalian liverrdquoThe Journal of Biological Chemistry vol 273no 16 pp 10046ndash10050 1998
[24] A M van der Bliek F Baas T Ten Houte de Lange P MKooiman T van der Velde-Koerts and P Borst ldquoThe humanmdr3 gene encodes a novel P-glycoprotein homologue and givesrise to alternatively splicedmRNAs in liverrdquo EMBO Journal vol6 no 11 pp 3325ndash3331 1987
[25] A J Smith J L Timmermans-Hereijgers and B RoelofsenldquoThe human MDR3 P-glycoprotein promotes translocation ofphosphatidylcholine through the plasma membrane of fibrob-lasts from transgenic micerdquo FEBS Letters vol 354 no 3 pp263ndash266 1994
[26] J M L de Vree E Jacquemin E Sturm et al ldquoMutations in theMDR3 gene cause progressive familial intrahepatic cholestasisrdquoProceedings of the National Acadamy of Sciences of the UnitedStates of America vol 95 no 1 pp 282ndash287 1998
[27] A Groen M R Romero C Kunne et al ldquoComplementaryfunctions of the flippase ATP8B1 and the floppase ABCB4 inmaintaining canalicular membrane integrityrdquoGastroenterologyvol 141 no 5 pp 1927ndash1937 2011
10 Canadian Journal of Gastroenterology and Hepatology
[28] P A Dawson T Lan and A Rao ldquoThematic review series Bileacids Bile acid transportersrdquo Journal of Lipid Research vol 50no 12 pp 2340ndash2357 2009
[29] E Halilbasic T Claudel andM Trauner ldquoBile acid transportersand regulatory nuclear receptors in the liver and beyondrdquoJournal of Hepatology vol 58 no 1 pp 155ndash168 2013
[30] B L Shneider ldquoIntestinal bile acid transport Biology physiol-ogy and pathophysiologyrdquo Journal of Pediatric Gastroenterologyand Nutrition vol 32 no 4 pp 407ndash417 2001
[31] T Claudel G Zollner M Wagner and M Trauner ldquoRoleof nuclear receptors for bile acid metabolism bile secretioncholestasis and gallstone diseaserdquoBiochimica et Biophysica Acta(BBA) - Molecular Basis of Disease vol 1812 no 8 pp 867ndash8782011
[32] J J Eloranta and G A Kullak-Ublick ldquoThe role of FXR indisorders of bile acid homeostasisrdquo Physiology Journal vol 23no 5 pp 286ndash295 2008
[33] B Goodwin S A Jones R R Price et al ldquoA regulatory cascadeof the nuclear receptors FXR SHP-1 and LRH-1 represses bileacid biosynthesisrdquo Molecular Cell vol 6 no 3 pp 517ndash5262000
[34] M Muller P L M Jansen K N Faber et al ldquoFarnesoid Xreceptor and bile salts are involved in transcriptional regulationof the gene encoding the human bile salt export pumprdquoHepatology vol 35 no 3 pp 589ndash596 2002
[35] M Ananthanarayanan N BalasubramanianMMakishima DJ Mangelsdorf and F J Suchy ldquoHuman bile salt export pumppromoter is transactivated by the farnesoid X receptorbile acidreceptorrdquo The Journal of Biological Chemistry vol 276 no 31pp 28857ndash28865 2001
[36] L Huang A Zhao J L Lew et al ldquoFarnesoid X receptoractivates transcription of the phospholipid pump MDR3rdquo TheJournal of Biological Chemistry vol 278 no 51 pp 51085ndash510902003
[37] M Wagner G Zollner and M Trauner ldquoNuclear receptorregulation of the adaptive response of bile acid transporters incholestasisrdquo Seminars in Liver Disease vol 30 no 2 pp 160ndash1772010
[38] Y Zhang H R Kast-Woelbern and P A Edwards ldquoNaturalstructural variants of the nuclear receptor farnesoid X recep-tor affect transcriptional activationrdquo The Journal of BiologicalChemistry vol 278 no 1 pp 104ndash110 2003
[39] SW C VanMil R H J Houwen and LW J Klomp ldquoGeneticsof familial intrahepatic cholestasis syndromesrdquo Journal of Med-ical Genetics vol 42 no 6 pp 449ndash463 2005
[40] V E H Carlton L Pawlikowska and L N Bull ldquoMolecularbasis of intrahepatic cholestasisrdquoAnnals ofMedicine vol 36 no8 pp 606ndash617 2004
[41] R J Clayton F L Iber B H Ruebner and V A MckusickldquoByler Disease Fatal Familial Intrahepatic Cholestasis in anAmish Kindredrdquo American Journal of Diseases of Children vol117 no 1 pp 112ndash124 1969
[42] E Jacquemin ldquoProgressive familial intrahepatic cholestasisrdquoClinics andResearch inHepatology andGastroenterology vol 36supplement 1 pp S26ndashS35 2012
[43] L N Bull M J T Van Eijk L Pawlikowska et al ldquoA geneencoding a P-type ATPase mutated in two forms of hereditarycholestasisrdquo Nature Genetics vol 18 no 3 pp 219ndash224 1998
[44] L W J Klomp J C Vargas S W C Van Mil et al ldquoCharac-terization of mutations in ATP8B1 associated with hereditarycholestasisrdquo Hepatology vol 40 no 1 pp 27ndash38 2004
[45] P Ujhazy D Ortiz S Misra et al ldquoFamilial intrahepaticcholestasis 1 Studies of localization and functionrdquo Hepatologyvol 34 no 4 I pp 768ndash775 2001
[46] C C Paulusma A Groen C Kunne et al ldquoAtp8b1 deficiencyin mice reduces resistance of the canalicular membrane tohydrophobic bile salts and impairs bile salt transportrdquo Hepatol-ogy vol 44 no 1 pp 195ndash204 2006
[47] SW C VanMil LW J Klomp L N Bull and RH J HouwenldquoFIC1 disease A spectrumof intrahepatic cholestatic disordersrdquoSeminars in Liver Disease vol 21 no 4 pp 535ndash544 2001
[48] A Miyahawa-Hayashino H Egawa T Yorifuji et al ldquoAllograftsteatohepatitis in progressive familial intrahepatic cholestasistype 1 after living donor liver transplantationrdquo Liver Transplan-tation vol 15 no 6 pp 610ndash618 2009
[49] E Nicastro X Stephenne F Smets et al ldquoRecovery of graftsteatosis and protein-losing enteropathy after biliary diversionin a PFIC 1 liver transplanted childrdquo Pediatric Transplantationvol 16 no 5 pp E177ndashE182 2012
[50] K Evason K E Bove M J Finegold et al ldquoMorphologic find-ings in progressive familial intrahepatic cholestasis 2 (PFIC2)Correlation with genetic and immunohistochemical studiesrdquoThe American Journal of Surgical Pathology vol 35 no 5 pp687ndash696 2011
[51] S S Strautnieks L N Bull A S Knisely et al ldquoA gene encodinga liver-specific ABC transporter is mutated in progressivefamilial intrahepatic cholestasisrdquo Nature Genetics vol 20 no3 pp 233ndash238 1998
[52] A S Knisely S S Strautnieks Y Meier et al ldquoHepatocellularcarcinoma in ten children under five years of age with bile saltexport pumpdeficiencyrdquoHepatology vol 44 no 2 pp 478ndash4862006
[53] A O Scheimann S S Strautnieks A S Knisely J A Byrne RJ Thompson andM J Finegold ldquoMutations in Bile Salt ExportPump (ABCB11) in Two Children with Progressive FamilialIntrahepatic Cholestasis and Cholangiocarcinomardquo Journal ofPediatrics vol 150 no 5 pp 556ndash559 2007
[54] V Keitel M Burdelski Z Vojnisek L Schmitt D HaussingerandRKubitz ldquoDe novo bile salt transporter antibodies as a pos-sible cause of recurrent graft failure after liver transplantationA novel mechanism of cholestasisrdquo Hepatology vol 50 no 2pp 510ndash517 2009
[55] P Jara L Hierro P Martınez-Fernandez et al ldquoRecurrence ofbile salt export pump deficiency after liver transplantationrdquoTheNew England Journal of Medicine vol 361 no 14 pp 1359ndash13672009
[56] R Kubitz C Droge S Kluge et al ldquoAutoimmune BSEPDiseaseDisease Recurrence After Liver Transplantation for ProgressiveFamilial Intrahepatic Cholestasisrdquo Clinical Reviews in Allergy ampImmunology vol 48 no 2-3 pp 273ndash284 2015
[57] J Stindt S Kluge C Droge et al ldquoBile salt export pump-reactive antibodies form a polyclonal multi-inhibitoryresponse in antibody-induced bile salt export pump deficiencyrdquoHepatology vol 63 no 2 pp 524ndash537 2016
[58] E Jacquemin J M DeVree D Cresteil et al ldquoThe widespectrum of multidrug resistance 3 deficiency from neonatalcholestasis to cirrhosis of adulthoodrdquoGastroenterology vol 120no 6 pp 1448ndash1458 2001
[59] O Rosmorduc and R Poupon ldquoLow phospholipid associatedcholelithiasis association with mutation in the MDR3ABCB4generdquo Orphanet Journal of Rare Diseases vol 2 article 29 2007
Canadian Journal of Gastroenterology and Hepatology 11
[60] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoThe spectrum of liver diseases related to ABCB4 gene muta-tions Pathophysiology and clinical aspectsrdquo Seminars in LiverDisease vol 30 no 2 pp 134ndash146 2010
[61] DWendumV BarbuO Rosmorduc L Arrive J-F Flejou andR Poupon ldquoAspects of liver pathology in adult patients withMDR3ABCB4 gene mutationsrdquo Virchows Archiv vol 460 no3 pp 291ndash298 2012
[62] R P J Oude Elferink andC C Paulusma ldquoFunction and patho-physiological importance of ABCB4 (MDR3 P-glycoprotein)rdquoPflugers Archiv - European Journal of Physiology vol 453 no 5pp 601ndash610 2007
[63] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoProgressive familial intrahepatic cholestasisrdquo Clinical Pedi-atrics vol 51 pp 689ndash691 2012
[64] S Boga D Jain andM L Schilsky ldquoPresentation of progressivefamilial intrahepatic cholestasis type 3 mimicking wilson dis-ease molecular genetic diagnosis and response to treatmentrdquoPediatric Gastroenterology Hepatology amp Nutrition vol 18 no3 p 202 2015
[65] M Sambrotta S Strautnieks E Papouli et al ldquoMutationsin TJP2 cause progressive cholestatic liver diseaserdquo NatureGenetics vol 46 no 4 pp 326ndash328 2014
[66] M Sambrotta and R J Thompson ldquoMutations in TJP2 encod-ing zona occludens 2 and liver diseaserdquo Tissue Barriers vol 3no 3 Article ID e1026537 2015
[67] S Zhou P M Hertel M J Finegold et al ldquoHepatocellularcarcinoma associated with tight-junction protein 2 deficiencyrdquoHepatology vol 62 no 6 pp 1914ndash1916 2015
[68] V EH Carlton B ZHarris E G Puffenberger et al ldquoComplexinheritance of familial hypercholanemia with associated muta-tions in TJP2 and BAATrdquo Nature Genetics vol 34 no 1 pp 91ndash96 2003
[69] N Gomez-Ospina C J Potter R Xiao et al ldquoMutations inthe nuclear bile acid receptor FXR cause progressive familialintrahepatic cholestasisrdquoNature Communications vol 7 ArticleID 10713 2016
[70] I Koutsounas S Theocharis I Delladetsima E Patsouris andC Giaginis ldquoFarnesoid x receptor in human metabolism anddisease the interplay between gene polymorphisms clinicalphenotypes and disease susceptibilityrdquo Expert Opinion on DrugMetabolism amp Toxicology vol 11 no 4 pp 523ndash532 2015
[71] S W C van Mil A Milona P H Dixon et al ldquoFunctionalVariants of the Central Bile Acid Sensor FXR Identified inIntrahepatic Cholestasis of Pregnancyrdquo Gastroenterology vol133 no 2 pp 507ndash516 2007
[72] C Droge M Bonus U Baumann et al ldquoSequencing of FIC1BSEP and MDR3 in a large cohort of patients with cholestasisrevealed a high number of different genetic variantsrdquo Journal ofHepatology vol 67 no 6 pp 1253ndash1264 2017
[73] L N Bull V E H Carlton N L Stricker et al ldquoGeneticand morphological findings in progressive familial intrahepaticcholestasis (Byler disease [PFIC-1] and Byler syndrome) Evi-dence for heterogeneityrdquo Hepatology vol 26 no 1 pp 155ndash1641997
[74] S W C Van Mil W L Van Der Woerd G Van Der Brugge etal ldquoBenign recurrent intrahepatic cholestasis type 2 is causedby mutations in ABCB11rdquo Gastroenterology vol 127 no 2 pp379ndash384 2004
[75] N A M Van Ooteghem L W J Klomp G P Van Berge-Henegouwen andRH JHouwen ldquoBenign recurrent intrahep-atic cholestasis progressing to progressive familial intrahepatic
cholestasis Low GGT cholestasis is a clinical continuumrdquoJournal of Hepatology vol 36 no 3 pp 439ndash443 2002
[76] F Balsells R Wyllie R Steffen and M Kay ldquoBenign recurrentintrahepatic cholestasis Improvement of pruritus and shorten-ing of the symptomatic phase with rifampin therapy A casereportrdquo Clinical Pediatrics vol 36 no 8 pp 483ndash485 1997
[77] U Beuers M Trauner P Jansen and R Poupon ldquoNewparadigms in the treatment of hepatic cholestasis FromUDCAto FXR PXR and beyondrdquo Journal of Hepatology vol 62 no 1pp S25ndashS37 2015
[78] L Bachs A Pares M Elena C Piera and J Rodes ldquoEffectsof long-term rifampicin administration in primary biliarycirrhosisrdquoGastroenterology vol 102 no 6 pp 2077ndash2080 1992
[79] J M Stapelbroek K J Van Erpecum L W J Klomp et alldquoNasobiliary drainage induces long-lasting remission in benignrecurrent intrahepatic cholestasisrdquoHepatology vol 43 no 1 pp51ndash53 2006
[80] F Lammert H-U Marschall A Glantz and S MaternldquoIntrahepatic cholestasis of pregnancymolecular pathogenesisdiagnosis and managementrdquo Journal of Hepatology vol 33 no6 pp 1012ndash1021 2000
[81] P H Dixon and C Williamson ldquoThe pathophysiology ofintrahepatic cholestasis of pregnancyrdquo Clinics and Research inHepatology and Gastroenterology vol 40 no 2 pp 141ndash1532016
[82] M G Martineau C Raker P H Dixon et al ldquoThe metabolicprofile of intrahepatic cholestasis of pregnancy is associatedwith impaired glucose tolerance dyslipidemia and increasedfetal growthrdquo Diabetes Care vol 38 no 2 pp 243ndash248 2015
[83] D G Goulis I A LWalkerMDe Swiet CWG Redman andC Williamson ldquoPreeclampsia with Abnormal Liver FunctionTests Is Associated with Cholestasis in a Subgroup of CasesrdquoHypertension in Pregnancy vol 23 no 1 pp 19ndash27 2004
[84] A Glantz H-U Marschall F Lammert and L-A MattssonldquoIntrahepatic cholestasis of pregnancy A randomized con-trolled trial comparing dexamethasone and ursodeoxycholicacidrdquo Hepatology vol 42 no 6 pp 1399ndash1405 2005
[85] R Zapata L Sandoval J Palma et al ldquoUrsodeoxycholic acidin the treatment of intrahepatic cholestasis of pregnancy A 12-year experiencerdquo Liver International vol 25 no 3 pp 548ndash5542005
[86] T Binder P Salaj T Zima and L Vıtek ldquoRandomized prospec-tive comparative study of ursodeoxycholic acid and S-adenosyl-L-methionine in the treatment of intrahepatic cholestasis ofpregnancyrdquo Journal of PerinatalMedicine vol 34 no 5 pp 383ndash391 2006
[87] P H Dixon N Weerasekera K J Linton et al ldquoHeterozy-gous MDR3 missense mutation associated with intrahepaticcholestasis of pregnancy Evidence for a defect in proteintraffickingrdquo Human Molecular Genetics vol 9 no 8 pp 1209ndash1217 2000
[88] C Gendrot Y Bacq M-C Brechot J Lansac and C AndresldquoA second heterozygous MDR3 nonsense mutation associatedwith intrahepatic cholestasis of pregnancyrdquo Journal of MedicalGenetics vol 40 no 3 article e32 2003
[89] A Floreani I Carderi D Paternoster et al ldquoIntrahepaticcholestasis of pregnancy Three novel MDR3 gene mutationsrdquoAlimentary Pharmacology amp Therapeutics vol 23 no 11 pp1649ndash1653 2006
[90] J N Painter M Savander A Ropponen et al ldquoSequencevariation in the ATP8B1 gene and intrahepatic cholestasis of
12 Canadian Journal of Gastroenterology and Hepatology
pregnancyrdquo European Journal of Human Genetics vol 13 no 4pp 435ndash439 2005
[91] W L Van Der Woerd R H J Houwen and S F J Van DeGraaf ldquoCurrent and future therapies for inherited cholestaticliver diseasesrdquoWorld Journal of Gastroenterology vol 23 no 5pp 763ndash775 2017
[92] A Thebaut D Habes F Gottrand et al ldquoSertraline as an addi-tional treatment for cholestatic pruritus in childrenrdquo Journal ofPediatric Gastroenterology and Nutrition vol 64 no 3 pp 431ndash435 2017
[93] U Ołdakowska-Jedynak I JankowskaM Hartleb et al ldquoTreat-ment of pruritus with Prometheus dialysis and absorption sys-tem in a patient with benign recurrent intrahepatic cholestasisrdquoHepatology Research vol 44 no 10 pp E304ndashE308 2014
[94] L Cutillo M Najimi F Smets et al ldquoSafety of living-related liver transplantation for progressive familial intrahep-atic cholestasisrdquo Pediatric Transplantation vol 10 no 5 pp570ndash574 2006
[95] E Gonzales B Grosse B Schuller et al ldquoTargeted phar-macotherapy in progressive familial intrahepatic cholestasistype 2 Evidence for improvement of cholestasis with 4-phenylbutyraterdquo Hepatology vol 62 no 2 pp 558ndash566 2015
[96] E Gonzales and E Jacquemin ldquoMutation specific drug ther-apy for progressive familial or benign recurrent intrahepaticcholestasis A new tool in a near futurerdquo Journal of Hepatologyvol 53 no 2 pp 385ndash387 2010
[97] M Trauner C D Fuchs E Halilbasic and G PaumgartnerldquoNew therapeutic concepts in bile acid transport and signalingfor management of cholestasisrdquo Hepatology vol 65 no 4 pp1393ndash1404 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Canadian Journal of Gastroenterology and Hepatology 9
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Acknowledgments
Milan Jirsa was supported by Ministry of Health CzechRepublicmdashConceptual Development of Research Organiza-tion (ldquoInstitute for Clinical and Experimental MedicinendashIKEM IN 00023001rdquo)
References
[1] N B Javitt ldquoBile acid synthesis from cholesterol regulatory andauxiliary pathwaysrdquoThe FASEB Journal vol 8 no 15 pp 1308ndash1311 1994
[2] J Y L Chiang ldquoBile acids regulation of synthesisrdquo Journal ofLipid Research vol 50 no 10 pp 1955ndash1966 2009
[3] J L Boyer ldquoBile formation and secretionrdquo ComprehensivePhysiology vol 3 no 3 pp 1035ndash1078 2013
[4] B Hagenbuch and P J Meier ldquoSinusoidal (basolateral) bile saltuptake systems of hepatocytesrdquo Seminars in Liver Disease vol16 no 2 pp 129ndash136 1996
[5] B Hagenbuch B Stieger M Foguet H Lubbert and P JMeier ldquoFunctional expression cloning and characterization ofthe hepatocyte Na+bile acid cotransport systemrdquo Proceedingsof the National Acadamy of Sciences of the United States ofAmerica vol 88 no 23 pp 10629ndash10633 1991
[6] F M Vaz C C Paulusma H Huidekoper et al ldquoSodiumtaurocholate cotransporting polypeptide (SLC10A1) deficiencyConjugated hypercholanemia without a clear clinical pheno-typerdquo Hepatology vol 61 no 1 pp 260ndash267 2015
[7] B Hagenbuch and P J Meier ldquoOrganic anion transportingpolypeptides of the OATPSLC21 family Phylogenetic classi-fication as OATPSLCO super-family new nomenclature andmolecularfunctional propertiesrdquo Pflugers Archiv - EuropeanJournal of Physiology vol 447 no 5 pp 653ndash665 2004
[8] B Hagenbuch and B Stieger ldquoThe SLCO (former SLC21)superfamily of transportersrdquoMolecular Aspects of Medicine vol34 no 2-3 pp 396ndash412 2013
[9] M Muller and P L M Jansen ldquoThe secretory function ofthe liver New aspects of hepatobiliary transportrdquo Journal ofHepatology vol 28 no 2 pp 344ndash354 1998
[10] G J E J Hooiveld J E Van Montfoort D K F Meijerand M Muller ldquoFunction and regulation of ATP-bindingcassette transport proteins involved in hepatobiliary transportrdquoEuropean Journal of Pharmaceutical Sciences vol 12 no 4 pp525ndash543 2001
[11] J Konig D Rost Y Cui and D Keppler ldquoCharacterizationof the human multidrug resistance protein isoform MRP3localized to the basolateral hepatocyte membranerdquoHepatologyvol 29 no 4 pp 1156ndash1163 1999
[12] H Zeng G Liu P A Rea and G D Kruh ldquoTransport ofamphipathic anions by human multidrug resistance protein 3rdquoCancer Research vol 60 pp 4779ndash4784 2000
[13] Y-M A Lee Y Cui J Konig et al ldquoIdentification and func-tional characterization of the natural variantMRP3-Arg1297Hisof human multidrug resistance protein 3 (MRP3ABCC3)rdquoPharmacogenetics vol 14 no 4 pp 213ndash223 2004
[14] M Donner ldquoUp-regulation of basolateral multidrug resistanceprotein 3 (Mrp3) in cholestatic rat liverrdquoHepatology vol 34 no2 pp 351ndash359 2001
[15] M L Ruiz J P Rigalli A Arias et al ldquoInduction of hepaticmultidrug resistance-associated protein 3 by ethynylestradiol isindependent of cholestasis and mediated by estrogen receptorrdquoDrug Metabolism and Disposition vol 41 no 2 pp 275ndash2802013
[16] N J Cherrington D P Hartley N Li D R Johnson and C DKlaassen ldquoOrgan distribution of multidrug resistance proteins1 2 and 3 (Mrp1 2 and 3) mRNA and hepatic induction ofMrp3 by constitutive androstane receptor activators in ratsrdquoTheJournal of Pharmacology and Experimental Therapeutics vol300 no 1 pp 97ndash104 2002
[17] C A Ritter G Jedlitschky H Meyer Zu Schwabedissen MGrube K Kock and H K Kroemer ldquoCellular export ofdrugs and signaling molecules by the ATP-binding cassettetransporters MRP4 (ABCC4) and MRP5 (ABCC5)rdquo DrugMetabolism Reviews vol 37 no 1 pp 253ndash278 2005
[18] F G M Russel J B Koenderink and R Masereeuw ldquoMul-tidrug resistance protein 4 (MRP4ABCC4) a versatile effluxtransporter for drugs and signalling moleculesrdquo Trends inPharmacological Sciences vol 29 no 4 pp 200ndash207 2008
[19] D Keppler ldquoProgress in the molecular characterization ofhepatobiliary transportersrdquoDigestive Diseases vol 35 no 3 pp197ndash202 2017
[20] V Keitel M Burdelski U Warskulat et al ldquoExpression andlocalization of hepatobiliary transport proteins in progressivefamilial intrahepatic cholestasisrdquo Hepatology vol 41 no 5 pp1160ndash1172 2005
[21] N Ballatori F FangWV Christian N Li andC LHammondldquoOst120572-Ost120573 is required for bile acid and conjugated steroiddisposition in the intestine kidney and liverrdquoAmerican Journalof Physiology-Gastrointestinal and Liver Physiology vol 295 no1 pp G179ndashG186 2008
[22] J L Boyer M Trauner A Mennone et al ldquoUpregulationof a basolateral FXR-dependent bile acid efflux transporterOSTalpha-OSTbeta in cholestasis in humans and rodentsrdquoAmerican Journal of Physiology-Gastrointestinal and Liver Phys-iology vol 290 no 6 pp G1124ndashG1130 2006
[23] T Gerloff B Stieger B Hagenbuch et al ldquoThe sister of P-glycoprotein represents the canalicular bile salt export pump ofmammalian liverrdquoThe Journal of Biological Chemistry vol 273no 16 pp 10046ndash10050 1998
[24] A M van der Bliek F Baas T Ten Houte de Lange P MKooiman T van der Velde-Koerts and P Borst ldquoThe humanmdr3 gene encodes a novel P-glycoprotein homologue and givesrise to alternatively splicedmRNAs in liverrdquo EMBO Journal vol6 no 11 pp 3325ndash3331 1987
[25] A J Smith J L Timmermans-Hereijgers and B RoelofsenldquoThe human MDR3 P-glycoprotein promotes translocation ofphosphatidylcholine through the plasma membrane of fibrob-lasts from transgenic micerdquo FEBS Letters vol 354 no 3 pp263ndash266 1994
[26] J M L de Vree E Jacquemin E Sturm et al ldquoMutations in theMDR3 gene cause progressive familial intrahepatic cholestasisrdquoProceedings of the National Acadamy of Sciences of the UnitedStates of America vol 95 no 1 pp 282ndash287 1998
[27] A Groen M R Romero C Kunne et al ldquoComplementaryfunctions of the flippase ATP8B1 and the floppase ABCB4 inmaintaining canalicular membrane integrityrdquoGastroenterologyvol 141 no 5 pp 1927ndash1937 2011
10 Canadian Journal of Gastroenterology and Hepatology
[28] P A Dawson T Lan and A Rao ldquoThematic review series Bileacids Bile acid transportersrdquo Journal of Lipid Research vol 50no 12 pp 2340ndash2357 2009
[29] E Halilbasic T Claudel andM Trauner ldquoBile acid transportersand regulatory nuclear receptors in the liver and beyondrdquoJournal of Hepatology vol 58 no 1 pp 155ndash168 2013
[30] B L Shneider ldquoIntestinal bile acid transport Biology physiol-ogy and pathophysiologyrdquo Journal of Pediatric Gastroenterologyand Nutrition vol 32 no 4 pp 407ndash417 2001
[31] T Claudel G Zollner M Wagner and M Trauner ldquoRoleof nuclear receptors for bile acid metabolism bile secretioncholestasis and gallstone diseaserdquoBiochimica et Biophysica Acta(BBA) - Molecular Basis of Disease vol 1812 no 8 pp 867ndash8782011
[32] J J Eloranta and G A Kullak-Ublick ldquoThe role of FXR indisorders of bile acid homeostasisrdquo Physiology Journal vol 23no 5 pp 286ndash295 2008
[33] B Goodwin S A Jones R R Price et al ldquoA regulatory cascadeof the nuclear receptors FXR SHP-1 and LRH-1 represses bileacid biosynthesisrdquo Molecular Cell vol 6 no 3 pp 517ndash5262000
[34] M Muller P L M Jansen K N Faber et al ldquoFarnesoid Xreceptor and bile salts are involved in transcriptional regulationof the gene encoding the human bile salt export pumprdquoHepatology vol 35 no 3 pp 589ndash596 2002
[35] M Ananthanarayanan N BalasubramanianMMakishima DJ Mangelsdorf and F J Suchy ldquoHuman bile salt export pumppromoter is transactivated by the farnesoid X receptorbile acidreceptorrdquo The Journal of Biological Chemistry vol 276 no 31pp 28857ndash28865 2001
[36] L Huang A Zhao J L Lew et al ldquoFarnesoid X receptoractivates transcription of the phospholipid pump MDR3rdquo TheJournal of Biological Chemistry vol 278 no 51 pp 51085ndash510902003
[37] M Wagner G Zollner and M Trauner ldquoNuclear receptorregulation of the adaptive response of bile acid transporters incholestasisrdquo Seminars in Liver Disease vol 30 no 2 pp 160ndash1772010
[38] Y Zhang H R Kast-Woelbern and P A Edwards ldquoNaturalstructural variants of the nuclear receptor farnesoid X recep-tor affect transcriptional activationrdquo The Journal of BiologicalChemistry vol 278 no 1 pp 104ndash110 2003
[39] SW C VanMil R H J Houwen and LW J Klomp ldquoGeneticsof familial intrahepatic cholestasis syndromesrdquo Journal of Med-ical Genetics vol 42 no 6 pp 449ndash463 2005
[40] V E H Carlton L Pawlikowska and L N Bull ldquoMolecularbasis of intrahepatic cholestasisrdquoAnnals ofMedicine vol 36 no8 pp 606ndash617 2004
[41] R J Clayton F L Iber B H Ruebner and V A MckusickldquoByler Disease Fatal Familial Intrahepatic Cholestasis in anAmish Kindredrdquo American Journal of Diseases of Children vol117 no 1 pp 112ndash124 1969
[42] E Jacquemin ldquoProgressive familial intrahepatic cholestasisrdquoClinics andResearch inHepatology andGastroenterology vol 36supplement 1 pp S26ndashS35 2012
[43] L N Bull M J T Van Eijk L Pawlikowska et al ldquoA geneencoding a P-type ATPase mutated in two forms of hereditarycholestasisrdquo Nature Genetics vol 18 no 3 pp 219ndash224 1998
[44] L W J Klomp J C Vargas S W C Van Mil et al ldquoCharac-terization of mutations in ATP8B1 associated with hereditarycholestasisrdquo Hepatology vol 40 no 1 pp 27ndash38 2004
[45] P Ujhazy D Ortiz S Misra et al ldquoFamilial intrahepaticcholestasis 1 Studies of localization and functionrdquo Hepatologyvol 34 no 4 I pp 768ndash775 2001
[46] C C Paulusma A Groen C Kunne et al ldquoAtp8b1 deficiencyin mice reduces resistance of the canalicular membrane tohydrophobic bile salts and impairs bile salt transportrdquo Hepatol-ogy vol 44 no 1 pp 195ndash204 2006
[47] SW C VanMil LW J Klomp L N Bull and RH J HouwenldquoFIC1 disease A spectrumof intrahepatic cholestatic disordersrdquoSeminars in Liver Disease vol 21 no 4 pp 535ndash544 2001
[48] A Miyahawa-Hayashino H Egawa T Yorifuji et al ldquoAllograftsteatohepatitis in progressive familial intrahepatic cholestasistype 1 after living donor liver transplantationrdquo Liver Transplan-tation vol 15 no 6 pp 610ndash618 2009
[49] E Nicastro X Stephenne F Smets et al ldquoRecovery of graftsteatosis and protein-losing enteropathy after biliary diversionin a PFIC 1 liver transplanted childrdquo Pediatric Transplantationvol 16 no 5 pp E177ndashE182 2012
[50] K Evason K E Bove M J Finegold et al ldquoMorphologic find-ings in progressive familial intrahepatic cholestasis 2 (PFIC2)Correlation with genetic and immunohistochemical studiesrdquoThe American Journal of Surgical Pathology vol 35 no 5 pp687ndash696 2011
[51] S S Strautnieks L N Bull A S Knisely et al ldquoA gene encodinga liver-specific ABC transporter is mutated in progressivefamilial intrahepatic cholestasisrdquo Nature Genetics vol 20 no3 pp 233ndash238 1998
[52] A S Knisely S S Strautnieks Y Meier et al ldquoHepatocellularcarcinoma in ten children under five years of age with bile saltexport pumpdeficiencyrdquoHepatology vol 44 no 2 pp 478ndash4862006
[53] A O Scheimann S S Strautnieks A S Knisely J A Byrne RJ Thompson andM J Finegold ldquoMutations in Bile Salt ExportPump (ABCB11) in Two Children with Progressive FamilialIntrahepatic Cholestasis and Cholangiocarcinomardquo Journal ofPediatrics vol 150 no 5 pp 556ndash559 2007
[54] V Keitel M Burdelski Z Vojnisek L Schmitt D HaussingerandRKubitz ldquoDe novo bile salt transporter antibodies as a pos-sible cause of recurrent graft failure after liver transplantationA novel mechanism of cholestasisrdquo Hepatology vol 50 no 2pp 510ndash517 2009
[55] P Jara L Hierro P Martınez-Fernandez et al ldquoRecurrence ofbile salt export pump deficiency after liver transplantationrdquoTheNew England Journal of Medicine vol 361 no 14 pp 1359ndash13672009
[56] R Kubitz C Droge S Kluge et al ldquoAutoimmune BSEPDiseaseDisease Recurrence After Liver Transplantation for ProgressiveFamilial Intrahepatic Cholestasisrdquo Clinical Reviews in Allergy ampImmunology vol 48 no 2-3 pp 273ndash284 2015
[57] J Stindt S Kluge C Droge et al ldquoBile salt export pump-reactive antibodies form a polyclonal multi-inhibitoryresponse in antibody-induced bile salt export pump deficiencyrdquoHepatology vol 63 no 2 pp 524ndash537 2016
[58] E Jacquemin J M DeVree D Cresteil et al ldquoThe widespectrum of multidrug resistance 3 deficiency from neonatalcholestasis to cirrhosis of adulthoodrdquoGastroenterology vol 120no 6 pp 1448ndash1458 2001
[59] O Rosmorduc and R Poupon ldquoLow phospholipid associatedcholelithiasis association with mutation in the MDR3ABCB4generdquo Orphanet Journal of Rare Diseases vol 2 article 29 2007
Canadian Journal of Gastroenterology and Hepatology 11
[60] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoThe spectrum of liver diseases related to ABCB4 gene muta-tions Pathophysiology and clinical aspectsrdquo Seminars in LiverDisease vol 30 no 2 pp 134ndash146 2010
[61] DWendumV BarbuO Rosmorduc L Arrive J-F Flejou andR Poupon ldquoAspects of liver pathology in adult patients withMDR3ABCB4 gene mutationsrdquo Virchows Archiv vol 460 no3 pp 291ndash298 2012
[62] R P J Oude Elferink andC C Paulusma ldquoFunction and patho-physiological importance of ABCB4 (MDR3 P-glycoprotein)rdquoPflugers Archiv - European Journal of Physiology vol 453 no 5pp 601ndash610 2007
[63] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoProgressive familial intrahepatic cholestasisrdquo Clinical Pedi-atrics vol 51 pp 689ndash691 2012
[64] S Boga D Jain andM L Schilsky ldquoPresentation of progressivefamilial intrahepatic cholestasis type 3 mimicking wilson dis-ease molecular genetic diagnosis and response to treatmentrdquoPediatric Gastroenterology Hepatology amp Nutrition vol 18 no3 p 202 2015
[65] M Sambrotta S Strautnieks E Papouli et al ldquoMutationsin TJP2 cause progressive cholestatic liver diseaserdquo NatureGenetics vol 46 no 4 pp 326ndash328 2014
[66] M Sambrotta and R J Thompson ldquoMutations in TJP2 encod-ing zona occludens 2 and liver diseaserdquo Tissue Barriers vol 3no 3 Article ID e1026537 2015
[67] S Zhou P M Hertel M J Finegold et al ldquoHepatocellularcarcinoma associated with tight-junction protein 2 deficiencyrdquoHepatology vol 62 no 6 pp 1914ndash1916 2015
[68] V EH Carlton B ZHarris E G Puffenberger et al ldquoComplexinheritance of familial hypercholanemia with associated muta-tions in TJP2 and BAATrdquo Nature Genetics vol 34 no 1 pp 91ndash96 2003
[69] N Gomez-Ospina C J Potter R Xiao et al ldquoMutations inthe nuclear bile acid receptor FXR cause progressive familialintrahepatic cholestasisrdquoNature Communications vol 7 ArticleID 10713 2016
[70] I Koutsounas S Theocharis I Delladetsima E Patsouris andC Giaginis ldquoFarnesoid x receptor in human metabolism anddisease the interplay between gene polymorphisms clinicalphenotypes and disease susceptibilityrdquo Expert Opinion on DrugMetabolism amp Toxicology vol 11 no 4 pp 523ndash532 2015
[71] S W C van Mil A Milona P H Dixon et al ldquoFunctionalVariants of the Central Bile Acid Sensor FXR Identified inIntrahepatic Cholestasis of Pregnancyrdquo Gastroenterology vol133 no 2 pp 507ndash516 2007
[72] C Droge M Bonus U Baumann et al ldquoSequencing of FIC1BSEP and MDR3 in a large cohort of patients with cholestasisrevealed a high number of different genetic variantsrdquo Journal ofHepatology vol 67 no 6 pp 1253ndash1264 2017
[73] L N Bull V E H Carlton N L Stricker et al ldquoGeneticand morphological findings in progressive familial intrahepaticcholestasis (Byler disease [PFIC-1] and Byler syndrome) Evi-dence for heterogeneityrdquo Hepatology vol 26 no 1 pp 155ndash1641997
[74] S W C Van Mil W L Van Der Woerd G Van Der Brugge etal ldquoBenign recurrent intrahepatic cholestasis type 2 is causedby mutations in ABCB11rdquo Gastroenterology vol 127 no 2 pp379ndash384 2004
[75] N A M Van Ooteghem L W J Klomp G P Van Berge-Henegouwen andRH JHouwen ldquoBenign recurrent intrahep-atic cholestasis progressing to progressive familial intrahepatic
cholestasis Low GGT cholestasis is a clinical continuumrdquoJournal of Hepatology vol 36 no 3 pp 439ndash443 2002
[76] F Balsells R Wyllie R Steffen and M Kay ldquoBenign recurrentintrahepatic cholestasis Improvement of pruritus and shorten-ing of the symptomatic phase with rifampin therapy A casereportrdquo Clinical Pediatrics vol 36 no 8 pp 483ndash485 1997
[77] U Beuers M Trauner P Jansen and R Poupon ldquoNewparadigms in the treatment of hepatic cholestasis FromUDCAto FXR PXR and beyondrdquo Journal of Hepatology vol 62 no 1pp S25ndashS37 2015
[78] L Bachs A Pares M Elena C Piera and J Rodes ldquoEffectsof long-term rifampicin administration in primary biliarycirrhosisrdquoGastroenterology vol 102 no 6 pp 2077ndash2080 1992
[79] J M Stapelbroek K J Van Erpecum L W J Klomp et alldquoNasobiliary drainage induces long-lasting remission in benignrecurrent intrahepatic cholestasisrdquoHepatology vol 43 no 1 pp51ndash53 2006
[80] F Lammert H-U Marschall A Glantz and S MaternldquoIntrahepatic cholestasis of pregnancymolecular pathogenesisdiagnosis and managementrdquo Journal of Hepatology vol 33 no6 pp 1012ndash1021 2000
[81] P H Dixon and C Williamson ldquoThe pathophysiology ofintrahepatic cholestasis of pregnancyrdquo Clinics and Research inHepatology and Gastroenterology vol 40 no 2 pp 141ndash1532016
[82] M G Martineau C Raker P H Dixon et al ldquoThe metabolicprofile of intrahepatic cholestasis of pregnancy is associatedwith impaired glucose tolerance dyslipidemia and increasedfetal growthrdquo Diabetes Care vol 38 no 2 pp 243ndash248 2015
[83] D G Goulis I A LWalkerMDe Swiet CWG Redman andC Williamson ldquoPreeclampsia with Abnormal Liver FunctionTests Is Associated with Cholestasis in a Subgroup of CasesrdquoHypertension in Pregnancy vol 23 no 1 pp 19ndash27 2004
[84] A Glantz H-U Marschall F Lammert and L-A MattssonldquoIntrahepatic cholestasis of pregnancy A randomized con-trolled trial comparing dexamethasone and ursodeoxycholicacidrdquo Hepatology vol 42 no 6 pp 1399ndash1405 2005
[85] R Zapata L Sandoval J Palma et al ldquoUrsodeoxycholic acidin the treatment of intrahepatic cholestasis of pregnancy A 12-year experiencerdquo Liver International vol 25 no 3 pp 548ndash5542005
[86] T Binder P Salaj T Zima and L Vıtek ldquoRandomized prospec-tive comparative study of ursodeoxycholic acid and S-adenosyl-L-methionine in the treatment of intrahepatic cholestasis ofpregnancyrdquo Journal of PerinatalMedicine vol 34 no 5 pp 383ndash391 2006
[87] P H Dixon N Weerasekera K J Linton et al ldquoHeterozy-gous MDR3 missense mutation associated with intrahepaticcholestasis of pregnancy Evidence for a defect in proteintraffickingrdquo Human Molecular Genetics vol 9 no 8 pp 1209ndash1217 2000
[88] C Gendrot Y Bacq M-C Brechot J Lansac and C AndresldquoA second heterozygous MDR3 nonsense mutation associatedwith intrahepatic cholestasis of pregnancyrdquo Journal of MedicalGenetics vol 40 no 3 article e32 2003
[89] A Floreani I Carderi D Paternoster et al ldquoIntrahepaticcholestasis of pregnancy Three novel MDR3 gene mutationsrdquoAlimentary Pharmacology amp Therapeutics vol 23 no 11 pp1649ndash1653 2006
[90] J N Painter M Savander A Ropponen et al ldquoSequencevariation in the ATP8B1 gene and intrahepatic cholestasis of
12 Canadian Journal of Gastroenterology and Hepatology
pregnancyrdquo European Journal of Human Genetics vol 13 no 4pp 435ndash439 2005
[91] W L Van Der Woerd R H J Houwen and S F J Van DeGraaf ldquoCurrent and future therapies for inherited cholestaticliver diseasesrdquoWorld Journal of Gastroenterology vol 23 no 5pp 763ndash775 2017
[92] A Thebaut D Habes F Gottrand et al ldquoSertraline as an addi-tional treatment for cholestatic pruritus in childrenrdquo Journal ofPediatric Gastroenterology and Nutrition vol 64 no 3 pp 431ndash435 2017
[93] U Ołdakowska-Jedynak I JankowskaM Hartleb et al ldquoTreat-ment of pruritus with Prometheus dialysis and absorption sys-tem in a patient with benign recurrent intrahepatic cholestasisrdquoHepatology Research vol 44 no 10 pp E304ndashE308 2014
[94] L Cutillo M Najimi F Smets et al ldquoSafety of living-related liver transplantation for progressive familial intrahep-atic cholestasisrdquo Pediatric Transplantation vol 10 no 5 pp570ndash574 2006
[95] E Gonzales B Grosse B Schuller et al ldquoTargeted phar-macotherapy in progressive familial intrahepatic cholestasistype 2 Evidence for improvement of cholestasis with 4-phenylbutyraterdquo Hepatology vol 62 no 2 pp 558ndash566 2015
[96] E Gonzales and E Jacquemin ldquoMutation specific drug ther-apy for progressive familial or benign recurrent intrahepaticcholestasis A new tool in a near futurerdquo Journal of Hepatologyvol 53 no 2 pp 385ndash387 2010
[97] M Trauner C D Fuchs E Halilbasic and G PaumgartnerldquoNew therapeutic concepts in bile acid transport and signalingfor management of cholestasisrdquo Hepatology vol 65 no 4 pp1393ndash1404 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

10 Canadian Journal of Gastroenterology and Hepatology
[28] P A Dawson T Lan and A Rao ldquoThematic review series Bileacids Bile acid transportersrdquo Journal of Lipid Research vol 50no 12 pp 2340ndash2357 2009
[29] E Halilbasic T Claudel andM Trauner ldquoBile acid transportersand regulatory nuclear receptors in the liver and beyondrdquoJournal of Hepatology vol 58 no 1 pp 155ndash168 2013
[30] B L Shneider ldquoIntestinal bile acid transport Biology physiol-ogy and pathophysiologyrdquo Journal of Pediatric Gastroenterologyand Nutrition vol 32 no 4 pp 407ndash417 2001
[31] T Claudel G Zollner M Wagner and M Trauner ldquoRoleof nuclear receptors for bile acid metabolism bile secretioncholestasis and gallstone diseaserdquoBiochimica et Biophysica Acta(BBA) - Molecular Basis of Disease vol 1812 no 8 pp 867ndash8782011
[32] J J Eloranta and G A Kullak-Ublick ldquoThe role of FXR indisorders of bile acid homeostasisrdquo Physiology Journal vol 23no 5 pp 286ndash295 2008
[33] B Goodwin S A Jones R R Price et al ldquoA regulatory cascadeof the nuclear receptors FXR SHP-1 and LRH-1 represses bileacid biosynthesisrdquo Molecular Cell vol 6 no 3 pp 517ndash5262000
[34] M Muller P L M Jansen K N Faber et al ldquoFarnesoid Xreceptor and bile salts are involved in transcriptional regulationof the gene encoding the human bile salt export pumprdquoHepatology vol 35 no 3 pp 589ndash596 2002
[35] M Ananthanarayanan N BalasubramanianMMakishima DJ Mangelsdorf and F J Suchy ldquoHuman bile salt export pumppromoter is transactivated by the farnesoid X receptorbile acidreceptorrdquo The Journal of Biological Chemistry vol 276 no 31pp 28857ndash28865 2001
[36] L Huang A Zhao J L Lew et al ldquoFarnesoid X receptoractivates transcription of the phospholipid pump MDR3rdquo TheJournal of Biological Chemistry vol 278 no 51 pp 51085ndash510902003
[37] M Wagner G Zollner and M Trauner ldquoNuclear receptorregulation of the adaptive response of bile acid transporters incholestasisrdquo Seminars in Liver Disease vol 30 no 2 pp 160ndash1772010
[38] Y Zhang H R Kast-Woelbern and P A Edwards ldquoNaturalstructural variants of the nuclear receptor farnesoid X recep-tor affect transcriptional activationrdquo The Journal of BiologicalChemistry vol 278 no 1 pp 104ndash110 2003
[39] SW C VanMil R H J Houwen and LW J Klomp ldquoGeneticsof familial intrahepatic cholestasis syndromesrdquo Journal of Med-ical Genetics vol 42 no 6 pp 449ndash463 2005
[40] V E H Carlton L Pawlikowska and L N Bull ldquoMolecularbasis of intrahepatic cholestasisrdquoAnnals ofMedicine vol 36 no8 pp 606ndash617 2004
[41] R J Clayton F L Iber B H Ruebner and V A MckusickldquoByler Disease Fatal Familial Intrahepatic Cholestasis in anAmish Kindredrdquo American Journal of Diseases of Children vol117 no 1 pp 112ndash124 1969
[42] E Jacquemin ldquoProgressive familial intrahepatic cholestasisrdquoClinics andResearch inHepatology andGastroenterology vol 36supplement 1 pp S26ndashS35 2012
[43] L N Bull M J T Van Eijk L Pawlikowska et al ldquoA geneencoding a P-type ATPase mutated in two forms of hereditarycholestasisrdquo Nature Genetics vol 18 no 3 pp 219ndash224 1998
[44] L W J Klomp J C Vargas S W C Van Mil et al ldquoCharac-terization of mutations in ATP8B1 associated with hereditarycholestasisrdquo Hepatology vol 40 no 1 pp 27ndash38 2004
[45] P Ujhazy D Ortiz S Misra et al ldquoFamilial intrahepaticcholestasis 1 Studies of localization and functionrdquo Hepatologyvol 34 no 4 I pp 768ndash775 2001
[46] C C Paulusma A Groen C Kunne et al ldquoAtp8b1 deficiencyin mice reduces resistance of the canalicular membrane tohydrophobic bile salts and impairs bile salt transportrdquo Hepatol-ogy vol 44 no 1 pp 195ndash204 2006
[47] SW C VanMil LW J Klomp L N Bull and RH J HouwenldquoFIC1 disease A spectrumof intrahepatic cholestatic disordersrdquoSeminars in Liver Disease vol 21 no 4 pp 535ndash544 2001
[48] A Miyahawa-Hayashino H Egawa T Yorifuji et al ldquoAllograftsteatohepatitis in progressive familial intrahepatic cholestasistype 1 after living donor liver transplantationrdquo Liver Transplan-tation vol 15 no 6 pp 610ndash618 2009
[49] E Nicastro X Stephenne F Smets et al ldquoRecovery of graftsteatosis and protein-losing enteropathy after biliary diversionin a PFIC 1 liver transplanted childrdquo Pediatric Transplantationvol 16 no 5 pp E177ndashE182 2012
[50] K Evason K E Bove M J Finegold et al ldquoMorphologic find-ings in progressive familial intrahepatic cholestasis 2 (PFIC2)Correlation with genetic and immunohistochemical studiesrdquoThe American Journal of Surgical Pathology vol 35 no 5 pp687ndash696 2011
[51] S S Strautnieks L N Bull A S Knisely et al ldquoA gene encodinga liver-specific ABC transporter is mutated in progressivefamilial intrahepatic cholestasisrdquo Nature Genetics vol 20 no3 pp 233ndash238 1998
[52] A S Knisely S S Strautnieks Y Meier et al ldquoHepatocellularcarcinoma in ten children under five years of age with bile saltexport pumpdeficiencyrdquoHepatology vol 44 no 2 pp 478ndash4862006
[53] A O Scheimann S S Strautnieks A S Knisely J A Byrne RJ Thompson andM J Finegold ldquoMutations in Bile Salt ExportPump (ABCB11) in Two Children with Progressive FamilialIntrahepatic Cholestasis and Cholangiocarcinomardquo Journal ofPediatrics vol 150 no 5 pp 556ndash559 2007
[54] V Keitel M Burdelski Z Vojnisek L Schmitt D HaussingerandRKubitz ldquoDe novo bile salt transporter antibodies as a pos-sible cause of recurrent graft failure after liver transplantationA novel mechanism of cholestasisrdquo Hepatology vol 50 no 2pp 510ndash517 2009
[55] P Jara L Hierro P Martınez-Fernandez et al ldquoRecurrence ofbile salt export pump deficiency after liver transplantationrdquoTheNew England Journal of Medicine vol 361 no 14 pp 1359ndash13672009
[56] R Kubitz C Droge S Kluge et al ldquoAutoimmune BSEPDiseaseDisease Recurrence After Liver Transplantation for ProgressiveFamilial Intrahepatic Cholestasisrdquo Clinical Reviews in Allergy ampImmunology vol 48 no 2-3 pp 273ndash284 2015
[57] J Stindt S Kluge C Droge et al ldquoBile salt export pump-reactive antibodies form a polyclonal multi-inhibitoryresponse in antibody-induced bile salt export pump deficiencyrdquoHepatology vol 63 no 2 pp 524ndash537 2016
[58] E Jacquemin J M DeVree D Cresteil et al ldquoThe widespectrum of multidrug resistance 3 deficiency from neonatalcholestasis to cirrhosis of adulthoodrdquoGastroenterology vol 120no 6 pp 1448ndash1458 2001
[59] O Rosmorduc and R Poupon ldquoLow phospholipid associatedcholelithiasis association with mutation in the MDR3ABCB4generdquo Orphanet Journal of Rare Diseases vol 2 article 29 2007
Canadian Journal of Gastroenterology and Hepatology 11
[60] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoThe spectrum of liver diseases related to ABCB4 gene muta-tions Pathophysiology and clinical aspectsrdquo Seminars in LiverDisease vol 30 no 2 pp 134ndash146 2010
[61] DWendumV BarbuO Rosmorduc L Arrive J-F Flejou andR Poupon ldquoAspects of liver pathology in adult patients withMDR3ABCB4 gene mutationsrdquo Virchows Archiv vol 460 no3 pp 291ndash298 2012
[62] R P J Oude Elferink andC C Paulusma ldquoFunction and patho-physiological importance of ABCB4 (MDR3 P-glycoprotein)rdquoPflugers Archiv - European Journal of Physiology vol 453 no 5pp 601ndash610 2007
[63] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoProgressive familial intrahepatic cholestasisrdquo Clinical Pedi-atrics vol 51 pp 689ndash691 2012
[64] S Boga D Jain andM L Schilsky ldquoPresentation of progressivefamilial intrahepatic cholestasis type 3 mimicking wilson dis-ease molecular genetic diagnosis and response to treatmentrdquoPediatric Gastroenterology Hepatology amp Nutrition vol 18 no3 p 202 2015
[65] M Sambrotta S Strautnieks E Papouli et al ldquoMutationsin TJP2 cause progressive cholestatic liver diseaserdquo NatureGenetics vol 46 no 4 pp 326ndash328 2014
[66] M Sambrotta and R J Thompson ldquoMutations in TJP2 encod-ing zona occludens 2 and liver diseaserdquo Tissue Barriers vol 3no 3 Article ID e1026537 2015
[67] S Zhou P M Hertel M J Finegold et al ldquoHepatocellularcarcinoma associated with tight-junction protein 2 deficiencyrdquoHepatology vol 62 no 6 pp 1914ndash1916 2015
[68] V EH Carlton B ZHarris E G Puffenberger et al ldquoComplexinheritance of familial hypercholanemia with associated muta-tions in TJP2 and BAATrdquo Nature Genetics vol 34 no 1 pp 91ndash96 2003
[69] N Gomez-Ospina C J Potter R Xiao et al ldquoMutations inthe nuclear bile acid receptor FXR cause progressive familialintrahepatic cholestasisrdquoNature Communications vol 7 ArticleID 10713 2016
[70] I Koutsounas S Theocharis I Delladetsima E Patsouris andC Giaginis ldquoFarnesoid x receptor in human metabolism anddisease the interplay between gene polymorphisms clinicalphenotypes and disease susceptibilityrdquo Expert Opinion on DrugMetabolism amp Toxicology vol 11 no 4 pp 523ndash532 2015
[71] S W C van Mil A Milona P H Dixon et al ldquoFunctionalVariants of the Central Bile Acid Sensor FXR Identified inIntrahepatic Cholestasis of Pregnancyrdquo Gastroenterology vol133 no 2 pp 507ndash516 2007
[72] C Droge M Bonus U Baumann et al ldquoSequencing of FIC1BSEP and MDR3 in a large cohort of patients with cholestasisrevealed a high number of different genetic variantsrdquo Journal ofHepatology vol 67 no 6 pp 1253ndash1264 2017
[73] L N Bull V E H Carlton N L Stricker et al ldquoGeneticand morphological findings in progressive familial intrahepaticcholestasis (Byler disease [PFIC-1] and Byler syndrome) Evi-dence for heterogeneityrdquo Hepatology vol 26 no 1 pp 155ndash1641997
[74] S W C Van Mil W L Van Der Woerd G Van Der Brugge etal ldquoBenign recurrent intrahepatic cholestasis type 2 is causedby mutations in ABCB11rdquo Gastroenterology vol 127 no 2 pp379ndash384 2004
[75] N A M Van Ooteghem L W J Klomp G P Van Berge-Henegouwen andRH JHouwen ldquoBenign recurrent intrahep-atic cholestasis progressing to progressive familial intrahepatic
cholestasis Low GGT cholestasis is a clinical continuumrdquoJournal of Hepatology vol 36 no 3 pp 439ndash443 2002
[76] F Balsells R Wyllie R Steffen and M Kay ldquoBenign recurrentintrahepatic cholestasis Improvement of pruritus and shorten-ing of the symptomatic phase with rifampin therapy A casereportrdquo Clinical Pediatrics vol 36 no 8 pp 483ndash485 1997
[77] U Beuers M Trauner P Jansen and R Poupon ldquoNewparadigms in the treatment of hepatic cholestasis FromUDCAto FXR PXR and beyondrdquo Journal of Hepatology vol 62 no 1pp S25ndashS37 2015
[78] L Bachs A Pares M Elena C Piera and J Rodes ldquoEffectsof long-term rifampicin administration in primary biliarycirrhosisrdquoGastroenterology vol 102 no 6 pp 2077ndash2080 1992
[79] J M Stapelbroek K J Van Erpecum L W J Klomp et alldquoNasobiliary drainage induces long-lasting remission in benignrecurrent intrahepatic cholestasisrdquoHepatology vol 43 no 1 pp51ndash53 2006
[80] F Lammert H-U Marschall A Glantz and S MaternldquoIntrahepatic cholestasis of pregnancymolecular pathogenesisdiagnosis and managementrdquo Journal of Hepatology vol 33 no6 pp 1012ndash1021 2000
[81] P H Dixon and C Williamson ldquoThe pathophysiology ofintrahepatic cholestasis of pregnancyrdquo Clinics and Research inHepatology and Gastroenterology vol 40 no 2 pp 141ndash1532016
[82] M G Martineau C Raker P H Dixon et al ldquoThe metabolicprofile of intrahepatic cholestasis of pregnancy is associatedwith impaired glucose tolerance dyslipidemia and increasedfetal growthrdquo Diabetes Care vol 38 no 2 pp 243ndash248 2015
[83] D G Goulis I A LWalkerMDe Swiet CWG Redman andC Williamson ldquoPreeclampsia with Abnormal Liver FunctionTests Is Associated with Cholestasis in a Subgroup of CasesrdquoHypertension in Pregnancy vol 23 no 1 pp 19ndash27 2004
[84] A Glantz H-U Marschall F Lammert and L-A MattssonldquoIntrahepatic cholestasis of pregnancy A randomized con-trolled trial comparing dexamethasone and ursodeoxycholicacidrdquo Hepatology vol 42 no 6 pp 1399ndash1405 2005
[85] R Zapata L Sandoval J Palma et al ldquoUrsodeoxycholic acidin the treatment of intrahepatic cholestasis of pregnancy A 12-year experiencerdquo Liver International vol 25 no 3 pp 548ndash5542005
[86] T Binder P Salaj T Zima and L Vıtek ldquoRandomized prospec-tive comparative study of ursodeoxycholic acid and S-adenosyl-L-methionine in the treatment of intrahepatic cholestasis ofpregnancyrdquo Journal of PerinatalMedicine vol 34 no 5 pp 383ndash391 2006
[87] P H Dixon N Weerasekera K J Linton et al ldquoHeterozy-gous MDR3 missense mutation associated with intrahepaticcholestasis of pregnancy Evidence for a defect in proteintraffickingrdquo Human Molecular Genetics vol 9 no 8 pp 1209ndash1217 2000
[88] C Gendrot Y Bacq M-C Brechot J Lansac and C AndresldquoA second heterozygous MDR3 nonsense mutation associatedwith intrahepatic cholestasis of pregnancyrdquo Journal of MedicalGenetics vol 40 no 3 article e32 2003
[89] A Floreani I Carderi D Paternoster et al ldquoIntrahepaticcholestasis of pregnancy Three novel MDR3 gene mutationsrdquoAlimentary Pharmacology amp Therapeutics vol 23 no 11 pp1649ndash1653 2006
[90] J N Painter M Savander A Ropponen et al ldquoSequencevariation in the ATP8B1 gene and intrahepatic cholestasis of
12 Canadian Journal of Gastroenterology and Hepatology
pregnancyrdquo European Journal of Human Genetics vol 13 no 4pp 435ndash439 2005
[91] W L Van Der Woerd R H J Houwen and S F J Van DeGraaf ldquoCurrent and future therapies for inherited cholestaticliver diseasesrdquoWorld Journal of Gastroenterology vol 23 no 5pp 763ndash775 2017
[92] A Thebaut D Habes F Gottrand et al ldquoSertraline as an addi-tional treatment for cholestatic pruritus in childrenrdquo Journal ofPediatric Gastroenterology and Nutrition vol 64 no 3 pp 431ndash435 2017
[93] U Ołdakowska-Jedynak I JankowskaM Hartleb et al ldquoTreat-ment of pruritus with Prometheus dialysis and absorption sys-tem in a patient with benign recurrent intrahepatic cholestasisrdquoHepatology Research vol 44 no 10 pp E304ndashE308 2014
[94] L Cutillo M Najimi F Smets et al ldquoSafety of living-related liver transplantation for progressive familial intrahep-atic cholestasisrdquo Pediatric Transplantation vol 10 no 5 pp570ndash574 2006
[95] E Gonzales B Grosse B Schuller et al ldquoTargeted phar-macotherapy in progressive familial intrahepatic cholestasistype 2 Evidence for improvement of cholestasis with 4-phenylbutyraterdquo Hepatology vol 62 no 2 pp 558ndash566 2015
[96] E Gonzales and E Jacquemin ldquoMutation specific drug ther-apy for progressive familial or benign recurrent intrahepaticcholestasis A new tool in a near futurerdquo Journal of Hepatologyvol 53 no 2 pp 385ndash387 2010
[97] M Trauner C D Fuchs E Halilbasic and G PaumgartnerldquoNew therapeutic concepts in bile acid transport and signalingfor management of cholestasisrdquo Hepatology vol 65 no 4 pp1393ndash1404 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Canadian Journal of Gastroenterology and Hepatology 11
[60] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoThe spectrum of liver diseases related to ABCB4 gene muta-tions Pathophysiology and clinical aspectsrdquo Seminars in LiverDisease vol 30 no 2 pp 134ndash146 2010
[61] DWendumV BarbuO Rosmorduc L Arrive J-F Flejou andR Poupon ldquoAspects of liver pathology in adult patients withMDR3ABCB4 gene mutationsrdquo Virchows Archiv vol 460 no3 pp 291ndash298 2012
[62] R P J Oude Elferink andC C Paulusma ldquoFunction and patho-physiological importance of ABCB4 (MDR3 P-glycoprotein)rdquoPflugers Archiv - European Journal of Physiology vol 453 no 5pp 601ndash610 2007
[63] A Davit-Spraul E Gonzales C Baussan and E JacqueminldquoProgressive familial intrahepatic cholestasisrdquo Clinical Pedi-atrics vol 51 pp 689ndash691 2012
[64] S Boga D Jain andM L Schilsky ldquoPresentation of progressivefamilial intrahepatic cholestasis type 3 mimicking wilson dis-ease molecular genetic diagnosis and response to treatmentrdquoPediatric Gastroenterology Hepatology amp Nutrition vol 18 no3 p 202 2015
[65] M Sambrotta S Strautnieks E Papouli et al ldquoMutationsin TJP2 cause progressive cholestatic liver diseaserdquo NatureGenetics vol 46 no 4 pp 326ndash328 2014
[66] M Sambrotta and R J Thompson ldquoMutations in TJP2 encod-ing zona occludens 2 and liver diseaserdquo Tissue Barriers vol 3no 3 Article ID e1026537 2015
[67] S Zhou P M Hertel M J Finegold et al ldquoHepatocellularcarcinoma associated with tight-junction protein 2 deficiencyrdquoHepatology vol 62 no 6 pp 1914ndash1916 2015
[68] V EH Carlton B ZHarris E G Puffenberger et al ldquoComplexinheritance of familial hypercholanemia with associated muta-tions in TJP2 and BAATrdquo Nature Genetics vol 34 no 1 pp 91ndash96 2003
[69] N Gomez-Ospina C J Potter R Xiao et al ldquoMutations inthe nuclear bile acid receptor FXR cause progressive familialintrahepatic cholestasisrdquoNature Communications vol 7 ArticleID 10713 2016
[70] I Koutsounas S Theocharis I Delladetsima E Patsouris andC Giaginis ldquoFarnesoid x receptor in human metabolism anddisease the interplay between gene polymorphisms clinicalphenotypes and disease susceptibilityrdquo Expert Opinion on DrugMetabolism amp Toxicology vol 11 no 4 pp 523ndash532 2015
[71] S W C van Mil A Milona P H Dixon et al ldquoFunctionalVariants of the Central Bile Acid Sensor FXR Identified inIntrahepatic Cholestasis of Pregnancyrdquo Gastroenterology vol133 no 2 pp 507ndash516 2007
[72] C Droge M Bonus U Baumann et al ldquoSequencing of FIC1BSEP and MDR3 in a large cohort of patients with cholestasisrevealed a high number of different genetic variantsrdquo Journal ofHepatology vol 67 no 6 pp 1253ndash1264 2017
[73] L N Bull V E H Carlton N L Stricker et al ldquoGeneticand morphological findings in progressive familial intrahepaticcholestasis (Byler disease [PFIC-1] and Byler syndrome) Evi-dence for heterogeneityrdquo Hepatology vol 26 no 1 pp 155ndash1641997
[74] S W C Van Mil W L Van Der Woerd G Van Der Brugge etal ldquoBenign recurrent intrahepatic cholestasis type 2 is causedby mutations in ABCB11rdquo Gastroenterology vol 127 no 2 pp379ndash384 2004
[75] N A M Van Ooteghem L W J Klomp G P Van Berge-Henegouwen andRH JHouwen ldquoBenign recurrent intrahep-atic cholestasis progressing to progressive familial intrahepatic
cholestasis Low GGT cholestasis is a clinical continuumrdquoJournal of Hepatology vol 36 no 3 pp 439ndash443 2002
[76] F Balsells R Wyllie R Steffen and M Kay ldquoBenign recurrentintrahepatic cholestasis Improvement of pruritus and shorten-ing of the symptomatic phase with rifampin therapy A casereportrdquo Clinical Pediatrics vol 36 no 8 pp 483ndash485 1997
[77] U Beuers M Trauner P Jansen and R Poupon ldquoNewparadigms in the treatment of hepatic cholestasis FromUDCAto FXR PXR and beyondrdquo Journal of Hepatology vol 62 no 1pp S25ndashS37 2015
[78] L Bachs A Pares M Elena C Piera and J Rodes ldquoEffectsof long-term rifampicin administration in primary biliarycirrhosisrdquoGastroenterology vol 102 no 6 pp 2077ndash2080 1992
[79] J M Stapelbroek K J Van Erpecum L W J Klomp et alldquoNasobiliary drainage induces long-lasting remission in benignrecurrent intrahepatic cholestasisrdquoHepatology vol 43 no 1 pp51ndash53 2006
[80] F Lammert H-U Marschall A Glantz and S MaternldquoIntrahepatic cholestasis of pregnancymolecular pathogenesisdiagnosis and managementrdquo Journal of Hepatology vol 33 no6 pp 1012ndash1021 2000
[81] P H Dixon and C Williamson ldquoThe pathophysiology ofintrahepatic cholestasis of pregnancyrdquo Clinics and Research inHepatology and Gastroenterology vol 40 no 2 pp 141ndash1532016
[82] M G Martineau C Raker P H Dixon et al ldquoThe metabolicprofile of intrahepatic cholestasis of pregnancy is associatedwith impaired glucose tolerance dyslipidemia and increasedfetal growthrdquo Diabetes Care vol 38 no 2 pp 243ndash248 2015
[83] D G Goulis I A LWalkerMDe Swiet CWG Redman andC Williamson ldquoPreeclampsia with Abnormal Liver FunctionTests Is Associated with Cholestasis in a Subgroup of CasesrdquoHypertension in Pregnancy vol 23 no 1 pp 19ndash27 2004
[84] A Glantz H-U Marschall F Lammert and L-A MattssonldquoIntrahepatic cholestasis of pregnancy A randomized con-trolled trial comparing dexamethasone and ursodeoxycholicacidrdquo Hepatology vol 42 no 6 pp 1399ndash1405 2005
[85] R Zapata L Sandoval J Palma et al ldquoUrsodeoxycholic acidin the treatment of intrahepatic cholestasis of pregnancy A 12-year experiencerdquo Liver International vol 25 no 3 pp 548ndash5542005
[86] T Binder P Salaj T Zima and L Vıtek ldquoRandomized prospec-tive comparative study of ursodeoxycholic acid and S-adenosyl-L-methionine in the treatment of intrahepatic cholestasis ofpregnancyrdquo Journal of PerinatalMedicine vol 34 no 5 pp 383ndash391 2006
[87] P H Dixon N Weerasekera K J Linton et al ldquoHeterozy-gous MDR3 missense mutation associated with intrahepaticcholestasis of pregnancy Evidence for a defect in proteintraffickingrdquo Human Molecular Genetics vol 9 no 8 pp 1209ndash1217 2000
[88] C Gendrot Y Bacq M-C Brechot J Lansac and C AndresldquoA second heterozygous MDR3 nonsense mutation associatedwith intrahepatic cholestasis of pregnancyrdquo Journal of MedicalGenetics vol 40 no 3 article e32 2003
[89] A Floreani I Carderi D Paternoster et al ldquoIntrahepaticcholestasis of pregnancy Three novel MDR3 gene mutationsrdquoAlimentary Pharmacology amp Therapeutics vol 23 no 11 pp1649ndash1653 2006
[90] J N Painter M Savander A Ropponen et al ldquoSequencevariation in the ATP8B1 gene and intrahepatic cholestasis of
12 Canadian Journal of Gastroenterology and Hepatology
pregnancyrdquo European Journal of Human Genetics vol 13 no 4pp 435ndash439 2005
[91] W L Van Der Woerd R H J Houwen and S F J Van DeGraaf ldquoCurrent and future therapies for inherited cholestaticliver diseasesrdquoWorld Journal of Gastroenterology vol 23 no 5pp 763ndash775 2017
[92] A Thebaut D Habes F Gottrand et al ldquoSertraline as an addi-tional treatment for cholestatic pruritus in childrenrdquo Journal ofPediatric Gastroenterology and Nutrition vol 64 no 3 pp 431ndash435 2017
[93] U Ołdakowska-Jedynak I JankowskaM Hartleb et al ldquoTreat-ment of pruritus with Prometheus dialysis and absorption sys-tem in a patient with benign recurrent intrahepatic cholestasisrdquoHepatology Research vol 44 no 10 pp E304ndashE308 2014
[94] L Cutillo M Najimi F Smets et al ldquoSafety of living-related liver transplantation for progressive familial intrahep-atic cholestasisrdquo Pediatric Transplantation vol 10 no 5 pp570ndash574 2006
[95] E Gonzales B Grosse B Schuller et al ldquoTargeted phar-macotherapy in progressive familial intrahepatic cholestasistype 2 Evidence for improvement of cholestasis with 4-phenylbutyraterdquo Hepatology vol 62 no 2 pp 558ndash566 2015
[96] E Gonzales and E Jacquemin ldquoMutation specific drug ther-apy for progressive familial or benign recurrent intrahepaticcholestasis A new tool in a near futurerdquo Journal of Hepatologyvol 53 no 2 pp 385ndash387 2010
[97] M Trauner C D Fuchs E Halilbasic and G PaumgartnerldquoNew therapeutic concepts in bile acid transport and signalingfor management of cholestasisrdquo Hepatology vol 65 no 4 pp1393ndash1404 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

12 Canadian Journal of Gastroenterology and Hepatology
pregnancyrdquo European Journal of Human Genetics vol 13 no 4pp 435ndash439 2005
[91] W L Van Der Woerd R H J Houwen and S F J Van DeGraaf ldquoCurrent and future therapies for inherited cholestaticliver diseasesrdquoWorld Journal of Gastroenterology vol 23 no 5pp 763ndash775 2017
[92] A Thebaut D Habes F Gottrand et al ldquoSertraline as an addi-tional treatment for cholestatic pruritus in childrenrdquo Journal ofPediatric Gastroenterology and Nutrition vol 64 no 3 pp 431ndash435 2017
[93] U Ołdakowska-Jedynak I JankowskaM Hartleb et al ldquoTreat-ment of pruritus with Prometheus dialysis and absorption sys-tem in a patient with benign recurrent intrahepatic cholestasisrdquoHepatology Research vol 44 no 10 pp E304ndashE308 2014
[94] L Cutillo M Najimi F Smets et al ldquoSafety of living-related liver transplantation for progressive familial intrahep-atic cholestasisrdquo Pediatric Transplantation vol 10 no 5 pp570ndash574 2006
[95] E Gonzales B Grosse B Schuller et al ldquoTargeted phar-macotherapy in progressive familial intrahepatic cholestasistype 2 Evidence for improvement of cholestasis with 4-phenylbutyraterdquo Hepatology vol 62 no 2 pp 558ndash566 2015
[96] E Gonzales and E Jacquemin ldquoMutation specific drug ther-apy for progressive familial or benign recurrent intrahepaticcholestasis A new tool in a near futurerdquo Journal of Hepatologyvol 53 no 2 pp 385ndash387 2010
[97] M Trauner C D Fuchs E Halilbasic and G PaumgartnerldquoNew therapeutic concepts in bile acid transport and signalingfor management of cholestasisrdquo Hepatology vol 65 no 4 pp1393ndash1404 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom














![[2015] post lt cholestasis](https://static.fdocuments.in/doc/165x107/58ee0ee21a28ab92198b4665/2015-post-lt-cholestasis.jpg)