
New drugs in ptcl
60
Newer drugs in PTCL Joydeep SR, medical oncology
-
Upload
joydeep-ghosh -
Category
Documents
-
view
45 -
download
2
Transcript of New drugs in ptcl

Newer drugs in PTCL
Joydeep SR, medical oncology

• Pralatrexate• Denileukin diftitox• Alemtuzumab

Pralatrexate…

Chemistry..
• Novel 10-de-aza-aminopterin analogue of methotrexate consisting of a mixture of R- and S- dia-stereomeric folate derivatives

Mechanism of action..
• Pralatrexate selectively enters cells expressing reduced folate carrier type 1 (RFC-1), a protein that is overexpressed on certain cancer cells compared to normal cells



PK/PD
• The total systemic clearance of pralatrexate diastereomers was – 417 mL/min (S-diastereomer)– 191 mL/min (R-diastereomer)
• T ½ : 12-18 hours• AUC and Cmax changed proportionately with
the dose• No long term accumulation seen• 67% bound to plasma protein

Metabolism..
• Not significantly metabolized by the phase I hepatic CYP450 isozymes or phase II hepatic glucuronidases.
• Has low potential to induce or inhibit the activity of CYP450 isozymes
• About 34% of pralatrexate was excreted unchanged into urine

Dosing
• 30 mg/m² IV push over 3-5 minutes via the side port of a free-flowing 0.9% NS
• once weekly for 6 weeks in 7-week cycles
• Continued till disease progression or unacceptable toxicity

Vitamin supplementation
• Folic acid: – 1mg PO OD , starting 10 days before and
continued upto 30 days after the last dose.• Vit B12– 1mg IM starting not more that 10 weeks before
and continued every 8-10 weeks– Can be given on the same day of dosing of
FOLOTYN

Monitoring
• CBC and mucositis should be monitored weekly
• RFT, LFT: prior to 1st and 4th dose of a given cycle
• Dose modifications:– Mucositis </= grade 1– Plt ≥ 100,000/μL for first dose and ≥ 50,000/μL for
all subsequent doses– Absolute neutrophil count (ANC) should be
≥1,000/μL.

Special populations..
• Pregnancy:– Category D – embryotoxic and fetotoxic– Can cause dose dependant decrease in fetal
viability• Not established for pediatric use

• Renal:– not been formally tested in patients with renal
impairment, caution is advised with moderate to severe impairment
• Hepatic:– Formal studies have not been performed– Better to avoid when • total bilirubin > 1.5 mg/dL; • AST or ALT > 2.5 × (ULN); • and AST or ALT > 5 ×ULN if documented hepatic
involvement with lymphoma.

Adverse effects..
• Bone marrow suppression• Mucositis• Skin toxicity:– include skin exfoliation, ulceration, and toxic
epidermal necrolysis (TEN)• TLS• Deranged LFTs


• Phase II, single-arm, open-label, international multicenter study
• August 2006 and April 2008• 111 pts• Primary end point:– ORR (CR+ CR unconfirmed +PR)
• Secondary end points:– DoR, PFS, OS

• Seventy-six percent of these patients (n=67) exhibited a decrease in tumor volume, with 18% of patients experiencing an increase in their disease volume after pralatrexate


Denileukin diftitox..

Chemistry..
• Ontak (denileukin diftitox), is a recombinant DNA-derived cytotoxic protein composed of the amino acid sequences for diphtheria toxin fragments A and B (Met1-Thr387)-His and the sequences for human interleukin-2
• Produced in E.coli• has a molecular weight of 58 kD
Mechanism of action…
• Denileukin diftitox is a fusion protein designed to direct the cytocidal action of diphtheria toxin to cells which express the IL-2 receptor.
• After binding to IL-2, denileukin is internalized• The fusion protein is cleaved, releasing toxin
enzymatic and translocation domains from the IL-2 fragment, resulting in the inhibition of protein synthesis and ultimately, cell death
PK..
• Following the first dose, denileukin diftitox displayed 2-compartment behavior – with a distribution phase (half-life approximately 2
to 5 minutes) – and a terminal phase (half-life approximately 70 to
80 minutes)• Mean volume of distribution was similar to
that of circulating blood • No accumulation was seen along the course
Dosage..
• Pre-medicate with an antihistamine and acetaminophen prior to each infusion.
• Administer at 9 or 18 mcg/kg/day by intravenous infusion over 30-60 minutes for 5 consecutive days every 21 days for 8 cycles
• Do not administer as a bolus injection• W/h if albumin is less than 3.0gm/dl

Adverse effects….
• Infusion reactions:– Infusion reactions, defined as symptoms occurring
within 24 hours of infusion and resolving within 48 hours of the last infusion (70.5%)
– Immediately stop and permanently discontinue denileukin for serious infusion reactions

Capillary leak syndrome..
• Defined by any 2/3 :– Hypotension– Edema– Serum albumin less than 3.0 At any time during denileukin therapy
• Incidence: 32.5%• Onset : may be delayed upto 2 weeks• May be severe even after discontinuation
• Visual loss: mostly permanent
• Hepatic dysfunction:– Increase in AST/ALT in 84% cases– Mostly during first and second cycles.– Resolves spontaneously– Did not require stoppage of drug

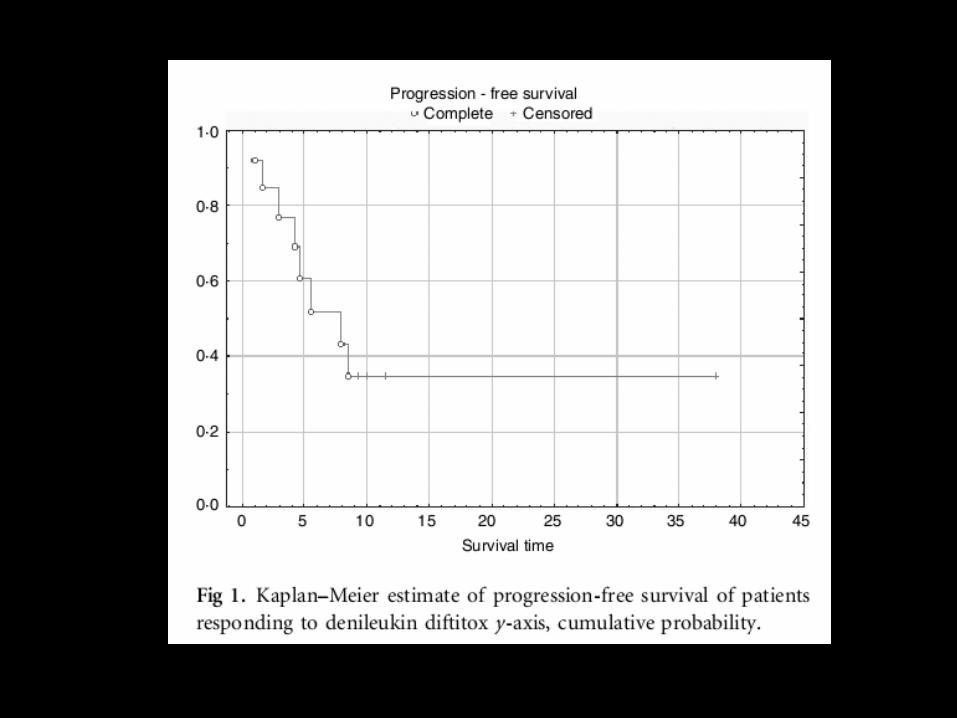
Clinical studies..

• Phase II study, relapsed/refractory T cell NHL
• 27 pts. 2001-2005
• Dose : 18microg/kg once daily as an intravenous (i.v.) infusion over 45–60 min for five consecutive days, repeated every 3 weeks, for up to eight cycles
• Primary end point: – CR + PR


• This phase III, placebo-controlled, randomized trial
• Compared 2 doses of DD– DD 9micg/kg/d (n45), DD 18micg/kg/d (n55), or placebo
infusions (n44), administered for 5 consecutive days every 3 weeks for up to eight cycles
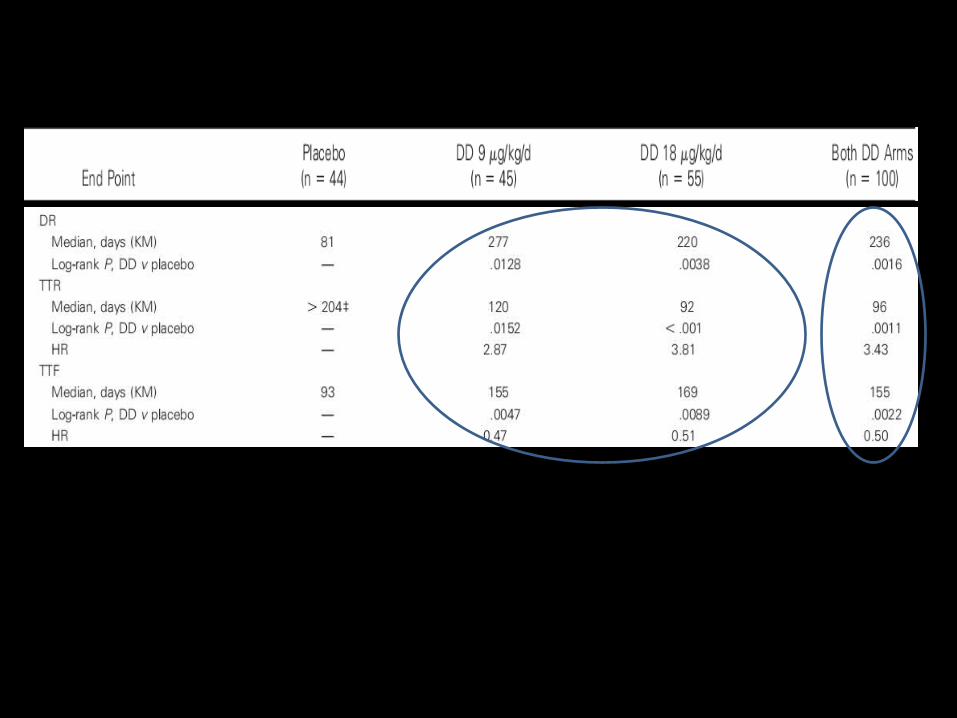
• CD 25 + CTCl, post >/= 3 lines of chemotherapy• N : 144• Primary end point: ORR• Secondary end point: PFS, DoR, TTR, TTF,

• ORR was 44% for all participants treated with DD (n100; 10% complete response [CR] and 34% partial response [PR]) compared with 15.9% for placebo-treated patients (2% CR and 13.6% PR)
• ORR was higher in the 18g/kg/d group versus the 9g/kg/d group (49.1% vs 37.8%, respectively)
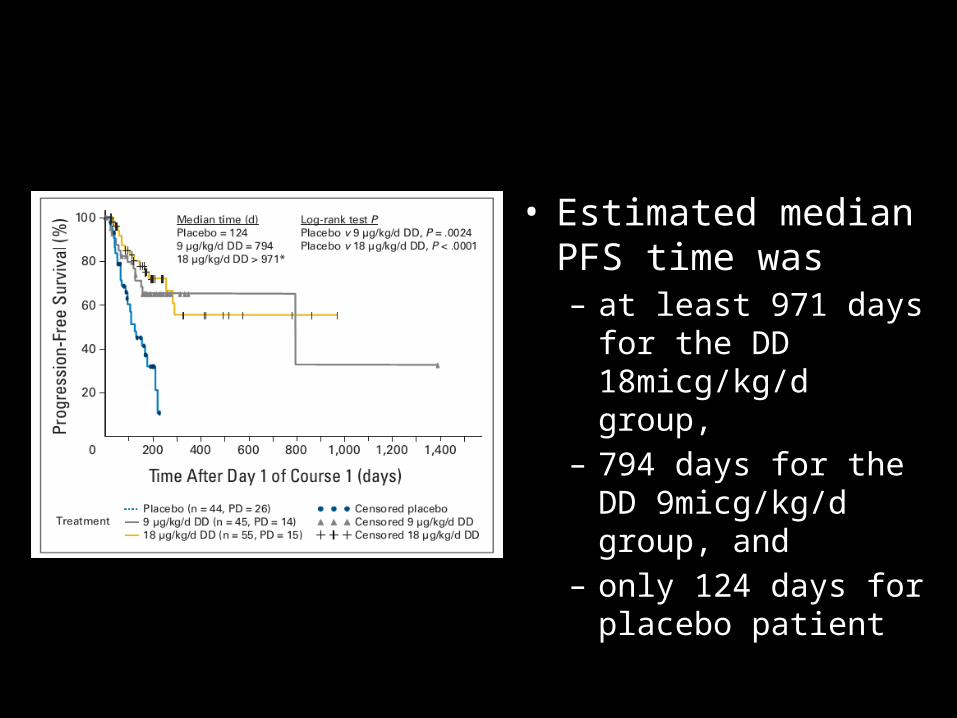
• Estimated median PFS time was – at least 971 days for the
DD 18micg/kg/d group, – 794 days for the DD
9micg/kg/d group, and – only 124 days for
placebo patient

• A: study drug related adverse events
• B: serious adverse events

Conclusions from this study..
• Highly significant difference in efficacy• No significant effects of stage, sex, race, age,
or number of prior CTCL therapies on the primary end point
• Superior outcome for the DD 18microg/kg/d group
• Favorable AE profile

Alemtuzumab…
Chemistry..
• Recombinant DNA-derived humanized monoclonal antibody (Campath-1H) directed against the 21-28 kD cell surface glycoprotein, CD52
• IgG1 kappa antibody with human variable framework and constant regions
• Derived from rat
Mechanism of action
• Binds to CD52 present on the surface of the cell
• Cell kill brought about by – Antibody dependant cell mediated cytotoxicity– Apoptosis

Pharmacokinetics..
• Systemic clearance decreased with repeated administration due to decreased receptor-mediated clearance
• Mean half-life was – 11 hours (range 2 to 32 hours) after the first 30 mg
dose – 6 days (range 1 to 14 days) after the last 30 mg
dose

Adverse effects
• Severe, including fatal, autoimmune anemia and thrombocytopenia, and prolonged myelosuppression have been reported in patients receiving Campath
• Pure red cell aplasia, bone marrow aplasia, and hypoplasia
• Discontinue for autoimmune cytopenias or recurrent/persistent severe cytopenias

• Lymphopenia:– In previously untreated patients, the median CD4+
was cells/μL at one month after treatment and 238 cells/μL to 418 cells/μL at 6 months post-treatment
• Neutropenia:– the incidence of Grade 3 or 4 neutropenia was
42% with a median time to onset of 31 days and a median duration of 37 days

• Anemia:– In previously untreated patients, the incidence of
Grade 3 or 4 anemia was 12% with a median time to onset of 31 days and a median duration of 8 days
• Thrombocytopenia:– In previously untreated patients, the incidence of
Grade 3 or 4 thrombocytopenia was 14% with a median time to onset of 9 days and a median duration of 14 days

• Infections:– CMV infection occurred in 16%– Other infections were reported in approximately 50% of
patients across all studies– Epstein-Barr Virus (EBV) including EBV-associated
lymphoproliferative disorder, progressive multifocal leukoencephalopathy (PML), re-activation of latent viruses
• Cardiac dysrhythmias occurred in approximately 14% of previously untreated patients– mostly tachycardias

Dosing..
• As a continuous IV infusion over 2 hours• Premedicate with diphenhydramine (50 mg)
and acetaminophen (500-1000 mg) 30minutes prior to first infusion and each dose escalation
• Appropriate antiviral/PCP prophylaxis• Usual dose is 30mg three times a weeks, after
an initial incremental dosing of 3mg, 10gm.

• Flow cytometry in 78 untreated patients including – 34 adult T-cell leukemia /lymphomas (ATLL), – 2 anaplastic large cell lymphomas (ALCL), – 3 angioimmunoblastic T-cell lymphomas (AITL), – 16 cutaneous T-cell lymphomas (CTCL), – 4 extra-nodal T/NK cell lymphomas (ENT/NKCL), – 4 hepatosplenic T-cell lymphomas (HSTCL), – 13 peripheral T-cell lymphomas (PTCL-NOS),– 2 T-prolymphocytic leukemia (T-PLL

Results..
• AITL, HSTCL, and T-PLL: – 100% positive
• Other:– PTL-NOS : 92.3%– ATLL: 94.1%– CTCL: 87.5%
• Expression was low in:– ALCL: 50%– NK/T cell: 25%


• Phase 2, open-label study in patients with advanced MF/SS who did not respond adequately to treatment with at least PUVA, radiotherapy, or chemotherapy
• Dose: 30mg thrice weekly after initial dose escalation, for total 12 weeks
• Primary objective:– ORR
• Secondary objective:– Safety profile – Clinical benefit

Results…
• N- 22, multiply treated before
• Most pts were stage III/IV
• ORR – skin: 55%– LN: 55%– Blood: 80%

• Itching was reduced from a median of 8 (at baseline) to 2 (at the end of the treatment period)
• Median time to treatment failure in responding patients was 12 months (range, 5-32months)


• Single centre phase II study• January 2003 and December 2005• 24 consecutive patients with PTCL entered the
study and received 8 CHOP courses• Alemtuzumab was added at 30 mg
subcutaneously at day1 initially to the first 4 courses (4 patients), and then to all 8 courses (20 patients).

• Among 24 evaluable patients, – 17 (71%) reached CR, – overall response rate
(CP+PR) of 75%
• All the patients affected by AILD-T , ALCL , and EATCL entered CR

• OS curve is projected to 70% and 53% at 1 and 2 years, respectively
• FFS curve is projected to 54% and 48% at 1 and 2 years, respectively
• Hematologic:– Anemia: 25%– Neutropenia: 34%– Thrombocytopenia: 2%
• Infections:– CMV: 9%– Others: JC virus reactivation, PCP, bacterial sepsis
Conclusions..
• Is a feasible chemoimmunotherapy regimen
• Is effective in PTCL with a high rate of CR achievement
• Associated with mostly manageable infectious complications

Thankyou…


















